Arg347Cys polymorphism of α1a-adrenergic receptor in vasovagal syncope. Case–control study in a...
6
Arg347Cys polymorphism of α 1a -adrenergic receptor in vasovagal syncope. Case–control study in a Mexican population Guadalupe Hernández-Pacheco a,b, ⁎, Antonio González-Hermosillo c , Chiharu Murata d , Petra Yescas e , Nilda Espínola-Zavaleta f , Martín Martínez a , Héctor Serrano g a Department of Physiology, Instituto Nacional de Cardiología “Ignacio Chávez”, Mexico b PhD Program in Biological Sciences and Health, Universidad Autónoma Metropolitana, Mexico c Medical Branch, Instituto Nacional de Cardiología “Ignacio Chávez”, Mexico d Department of Methodology, Instituto Nacional de Pediatría, Mexico e Department of Genetics, Instituto Nacional de Neurología y Neurocirugía “Manuel Velasco Suárez”, Mexico f Department of Echocardiography, Instituto Nacional de Cardiología “Ignacio Chávez”, Mexico g Department of Health Sciences, Universidad Autónoma Metropolitana-Iztapalapa, Mexico abstract article info Article history: Received 15 July 2013 Received in revised form 26 December 2013 Accepted 13 January 2014 Available online xxxx Keywords: Autonomic nervous system Syncope Adrenergic receptor Genes Background: Vasovagal syncope is a common clinical condition, consequential to reduced cerebral blood flow resulting from a failure in cardiovascular homeostasis during orthostasis. Blood pressure regulation is the basis for syncope development. In this regulation, the α 1a -adrenergic receptor plays a major role. Some studies have found a positive correlation between the Arg347Cys polymorphism of the α 1a -adrenergic receptor to hyperten- sion and heart autonomic control. The goal of this study is to evaluate the possible association between the Arg347Cys α 1a -adrenergic receptor polymorphism and vasovagal syncope in a Mexican population. Methods/major findings: A sample of 89 vasovagal syncope patients and 40 healthy controls were studied. Arg347Cys α 1a -adrenergic receptor polymorphism was determined by the PCR-RFLP method. We found an in- creased frequency of genotype ArgArg in vasovagal syncope patients. In a logistic regression model significant as- sociations were found in two genetic models, in codominant model (OR = 13.21: CI 95% 3.69–54.99, p b 0.001) and in additive model (OR = 12.68: CI 95% 3.5–53.07, p b 0.001) for ArgArg genotype with CysCys as reference. Conclusions: Our data suggests an important participation of Arg347Cys polymorphism as susceptibility factor in patients with vasovagal syncope. ArgArg genotype could be a marker for vasovagal syncope susceptibility in the Mexican population. © 2014 Elsevier B.V. All rights reserved. 1. Introduction Vasovagal syncope (VVS) is the commonest cause of transient loss of consciousness, accounting for 1.6% of all admissions to the emergency department (Cárdenas et al., 2009). It is associated with a transient fail- ure of the autonomic mechanisms that regulate cardiovascular function. The pathophysiology of VVS remains incompletely understood. Never- theless, one consistent observation is that evolving vasovagal episodes are preceded by an apparent transient period of increased sympathetic activity (Moya et al., 2009). The initial phase of sympathetic stimulation occurs in response to a stressor, which may either be orthostatic, phys- ical or emotional. VVS has been observed more frequently on those in the 10 to 30 year range (Ganzeboom et al., 2003; Sheldon et al., 2006; Moya et al., 2009). The evaluation of this condition is difficult due to the transitory state and its diagnosis is based on clinical history. From its introduction in 1986, the head-up tilt test (HUT) is used to study the hemodynamic changes and symptom reproduction of vasovagal syncope (Kenny et al., 1986). In its familial form, it is commonly ob- served that more than one family member is affected (Camfield and Camfield, 1990; Mathias et al., 1998; Newton et al., 2003; Márquez et al., 2005) suggesting a possible genetic component (Azevedo et al., 2009; OldeNordkamp et al., 2009). According to cardiovascular homeostasis some studies of gene poly- morphism have been conducted in renin–angiotensin and serotonin system (Newton et al., 2007; Mudraková et al., 2009), in endothelin sys- tem (Sorrentino et al., 2009), in genes encoding G-proteins (Lelonek et al., 2009; Huang et al., 2010) and sympathetic nervous system (Sorrentino et al., 2010). Cardiac output and sympathetic vasoconstrictor responses are crucial for the cardiovascular homeostasis during orthostasis. Short- time adjustments in the regulation of circulation produced by heart rate changes, cardiac contractility, vasoconstriction and ultimately, ce- rebral blood flow depend on the autonomic nervous system. In previous studies from our group, we found an association between Arg389Gly polymorphism β 1 -adrenergic receptor and positive HUT response in Autonomic Neuroscience: Basic and Clinical xxx (2014) xxx–xxx ⁎ Corresponding author at: Instituto Nacional de Cardiología “Ignacio Chávez”, Juan Badiano 1, Col. Sección XVI, Tlalpan, México 14080, DF, México. Tel.: +52 55 55732911; fax: +52 55 55730994. E-mail address: [email protected] (G. Hernández-Pacheco). AUTNEU-01624; No of Pages 6 1566-0702/$ – see front matter © 2014 Elsevier B.V. All rights reserved. http://dx.doi.org/10.1016/j.autneu.2014.01.005 Contents lists available at ScienceDirect Autonomic Neuroscience: Basic and Clinical journal homepage: www.elsevier.com/locate/autneu Please cite this article as: Hernández-Pacheco, G., et al., Arg347Cys polymorphism of α 1a -adrenergic receptor in vasovagal syncope. Case–control study in a Mexican population, Auton. Neurosci. (2014), http://dx.doi.org/10.1016/j.autneu.2014.01.005
Transcript of Arg347Cys polymorphism of α1a-adrenergic receptor in vasovagal syncope. Case–control study in a...

Autonomic Neuroscience: Basic and Clinical xxx (2014) xxx–xxx
AUTNEU-01624; No of Pages 6
Contents lists available at ScienceDirect
Autonomic Neuroscience: Basic and Clinical
j ourna l homepage: www.e lsev ie r .com/ locate /autneu
Arg347Cys polymorphism of α1a-adrenergic receptor in vasovagalsyncope. Case–control study in a Mexican population
Guadalupe Hernández-Pacheco a,b,⁎, Antonio González-Hermosillo c, Chiharu Murata d, Petra Yescas e,Nilda Espínola-Zavaleta f, Martín Martínez a, Héctor Serrano g
a Department of Physiology, Instituto Nacional de Cardiología “Ignacio Chávez”, Mexicob PhD Program in Biological Sciences and Health, Universidad Autónoma Metropolitana, Mexicoc Medical Branch, Instituto Nacional de Cardiología “Ignacio Chávez”, Mexicod Department of Methodology, Instituto Nacional de Pediatría, Mexicoe Department of Genetics, Instituto Nacional de Neurología y Neurocirugía “Manuel Velasco Suárez”, Mexicof Department of Echocardiography, Instituto Nacional de Cardiología “Ignacio Chávez”, Mexicog Department of Health Sciences, Universidad Autónoma Metropolitana-Iztapalapa, Mexico
⁎ Corresponding author at: Instituto Nacional de CardBadiano 1, Col. Sección XVI, Tlalpan, México 14080, DF, Mfax: +52 55 55730994.
E-mail address: [email protected] (G. Hernández-P
1566-0702/$ – see front matter © 2014 Elsevier B.V. All rihttp://dx.doi.org/10.1016/j.autneu.2014.01.005
Please cite this article as: Hernández-Pachecstudy in a Mexican population, Auton. Neuro
a b s t r a c t
a r t i c l e i n f oArticle history:
Received 15 July 2013Received in revised form 26 December 2013Accepted 13 January 2014Available online xxxxKeywords:Autonomic nervous systemSyncopeAdrenergic receptorGenes
Background: Vasovagal syncope is a common clinical condition, consequential to reduced cerebral blood flowresulting from a failure in cardiovascular homeostasis during orthostasis. Blood pressure regulation is the basisfor syncope development. In this regulation, the α1a-adrenergic receptor plays a major role. Some studies havefound a positive correlation between the Arg347Cys polymorphism of the α1a-adrenergic receptor to hyperten-sion and heart autonomic control. The goal of this study is to evaluate the possible association between theArg347Cys α1a-adrenergic receptor polymorphism and vasovagal syncope in a Mexican population.Methods/major findings: A sample of 89 vasovagal syncope patients and 40 healthy controls were studied.Arg347Cys α1a-adrenergic receptor polymorphism was determined by the PCR-RFLP method. We found an in-creased frequency of genotype ArgArg in vasovagal syncope patients. In a logistic regressionmodel significant as-sociations were found in two genetic models, in codominant model (OR = 13.21: CI 95% 3.69–54.99, p b 0.001)
and in additive model (OR = 12.68: CI 95% 3.5–53.07, p b 0.001) for ArgArg genotype with CysCys as reference.Conclusions: Our data suggests an important participation of Arg347Cys polymorphism as susceptibility factor inpatients with vasovagal syncope. ArgArg genotype could be a marker for vasovagal syncope susceptibility in theMexican population.© 2014 Elsevier B.V. All rights reserved.
1. Introduction
Vasovagal syncope (VVS) is the commonest cause of transient loss ofconsciousness, accounting for 1.6% of all admissions to the emergencydepartment (Cárdenas et al., 2009). It is associated with a transient fail-ure of the autonomicmechanisms that regulate cardiovascular function.The pathophysiology of VVS remains incompletely understood. Never-theless, one consistent observation is that evolving vasovagal episodesare preceded by an apparent transient period of increased sympatheticactivity (Moya et al., 2009). The initial phase of sympathetic stimulationoccurs in response to a stressor, which may either be orthostatic, phys-ical or emotional. VVS has been observed more frequently on those inthe 10 to 30 year range (Ganzeboom et al., 2003; Sheldon et al., 2006;Moya et al., 2009). The evaluation of this condition is difficult due tothe transitory state and its diagnosis is based on clinical history. From
iología “Ignacio Chávez”, Juanéxico. Tel.: +52 55 55732911;
acheco).
ghts reserved.
o, G., et al., Arg347Cys polymosci. (2014), http://dx.doi.org
its introduction in 1986, the head-up tilt test (HUT) is used to studythe hemodynamic changes and symptom reproduction of vasovagalsyncope (Kenny et al., 1986). In its familial form, it is commonly ob-served that more than one family member is affected (Camfield andCamfield, 1990; Mathias et al., 1998; Newton et al., 2003; Márquezet al., 2005) suggesting a possible genetic component (Azevedo et al.,2009; OldeNordkamp et al., 2009).
According to cardiovascular homeostasis some studies of gene poly-morphism have been conducted in renin–angiotensin and serotoninsystem (Newton et al., 2007;Mudraková et al., 2009), in endothelin sys-tem (Sorrentino et al., 2009), in genes encoding G-proteins (Leloneket al., 2009; Huang et al., 2010) and sympathetic nervous system(Sorrentino et al., 2010).
Cardiac output and sympathetic vasoconstrictor responses arecrucial for the cardiovascular homeostasis during orthostasis. Short-time adjustments in the regulation of circulation produced by heartrate changes, cardiac contractility, vasoconstriction and ultimately, ce-rebral blood flowdepend on the autonomic nervous system. In previousstudies from our group, we found an association between Arg389Glypolymorphism β1-adrenergic receptor and positive HUT response in
rphism ofα1a-adrenergic receptor in vasovagal syncope. Case–control/10.1016/j.autneu.2014.01.005

2 G. Hernández-Pacheco et al. / Autonomic Neuroscience: Basic and Clinical xxx (2014) xxx–xxx
patientswith VVS (Hernández-Pacheco et al., 2008). Theα1a-adrenergicreceptor has been proven to be important in blood pressure regulationin knock-outmice (Rokosh and Simpson, 2002), and it is expressed pre-dominantly in the human vascular system (Rudner et al., 1999).
The human ADRA1A gene is located in chromosome 8q21.2, and itbears a single base polymorphism (SNP rs1048101) at the 1441 positionwhere the change of Thymidine instead of Cytosine originatesthe change of Arginine to Cysteine as the 347 amino acid residue(Arg347Cys) in the carboxy-terminal end of the receptor protein(Hoehe et al., 1992). This polymorphism has been associated with hy-pertension and autonomic heart control in some populations (Snapiret al., 2003; Jiang et al., 2005, Gu et al., 2006; Iacoviello et al., 2006;Freitas et al., 2008; Zhang et al., 2009).
The ultimate cause of syncope is the reduction in brain blood flowsecondary to decreased cardiac output and low blood pressure. In thisscenario, blood pressure regulation is determinant of syncope develop-ment, due to the vast expression of the α1a-adrenergic receptor in thevascular system along with its polymorphic character. The goal of thisstudy was to explore the possible association between the Arg347Cyspolymorphism of α1a-adrenergic receptor and the occurrence of vaso-vagal syncope in the Mexican population.
2. Methods
We carried out a case–control study according to the Declaration ofHelsinki. All participants gave a written consent after the study charac-teristics were explained. When participants were younger than18 years old, the responsible adult gave his/her consent as above. The“Bioethics Commission of Instituto Nacional de Cardiología IgnacioChávez” approved this study. All chemicals were from Sigma Chemicalsunless otherwise indicated or of the highest quality available.
2.1. Participants
All cases were patients attending the syncope unit at the InstitutoNacional de Cardiologia, aged 10 to 50 years old, both sexes with atleast 2 syncope or presyncope episodes with a probable vasovagal ori-gin, recruited within the previous 12 months. Presyncope was deter-mined clinically as the experience of weakness, diaphoresis, chills,dizziness and nausea without loss of consciousness. The cases thatwere considered were those that met the criteria mentioned above,without any previous disease or condition that could explain syncope.
Controls were healthy volunteers with no familial relationship tocases, with no syncope or presyncope history. They usually were theguardians of the patients attending diverse services of the InstitutoNacional de Cardiologia. Both cases and controls came from diverse re-gions of the country.
2.2. Head-up Tilt Fainting Protocol (HUT)
The HUT in both cases and controls was performed according to thepreviously reported Institutional protocol (Hermosillo et al., 2000). Allparticipants were tested after a 10 to 12 h fasting period in a speciallyadapted room with facilities for blood pressure and heart monitoring.Prior to baseline recording, there was a stabilization period thatconsisted in at least 20min of rest in supine position. The protocol com-prised three stages: supine, 70° head up tilt and recovery in supine po-sition. The head-up tilt period was performed under two conditions:passive (in the absence of any provocative drugs), and pharmacological(with drug challenge). In the passive phase, upright posture was main-tained until either development of syncope or intolerable near syncopesymptoms or completion of maximum 45 min tilt duration. If syncopeoccurred the table was promptly returned to the supine position. If syn-cope or presyncope did not occur, subjects were given a single sublin-gual 5 mg isosorbide dinitrate dose (Hermosillo et al., 2000) andupright posture was maintained for 15 min or earlier if syncope or
Please cite this article as: Hernández-Pacheco, G., et al., Arg347Cys polymostudy in a Mexican population, Auton. Neurosci. (2014), http://dx.doi.org
presyncope occurs. Cases were studied in both passive and pharmaco-logical phases, whereas control individuals were submitted to the pas-sive phase only if they completed a 45 min , 70° upright tilt withoutsyncope or presyncope, to ensure that they were true controls(Hermosillo et al., 2010). The test was considered positive when synco-pe or near-syncope symptoms were developed (dizziness, diaphoresisor nausea) with arterial hypotension (systolic blood pressureb80 mm Hg or a fall larger or equal to 30% of basal values) and/or bra-dycardia (heart rate lower than 50 beats per minute or a reductionhigher than 20% of the basal level). A test was considered negativewhen subjects did not show vasovagal symptoms.
2.3. DNA isolation
Before the HUT test, a peripheral blood sample was taken in anEDTA-containing Vacutainer. Samples were maintained at 4 °C for upto 2 days before processing. DNA was isolated in a guanidine-phenolfree protocol (Lahiri and Nurnberger, 1991). In short, erythrocytesunderwent lysis in a low salt solution and chromatin complexes werefreed in a high salt buffer. After protein removal, DNA was ethanol pre-cipitated and washed by centrifugation; concentration and integritywere determined by spectrophotometry and electrophoresis.
2.4. Determination of the α1a-adrenergic receptor polymorphism
Samples for genotypingwere handled in a blind codewith no partic-ular order for case or controls. The polymorphism was determined bypolymerase chain reaction-restriction fragment length polymorphisms(PCR-RFLP) (Shibata et al., 1996). A 502 bp fragment was obtained byusing 12.5 μl JumpStartREDtaq (SIGMA), 100 ng DNA and 2 μl [10 μM]primers P1: 5′-ATGCTCCAGCCAAGAGTTCA-3′ and P2: 5′-TCCCAAGAAGAGCTGGCCTTC-3′ in aGeneAmpPCR System2700 (Applied Biosystems)programmed with 30 cycles of 94 °C 1 min, 30 s 55 °C annealing and1min extension at 72 °C. After amplification, amplicons were evaluatedby 1.5% agarose gel electrophoresis. Amplified material was thendigested with PstI (New England Biolabs) for 1 h at 37 °C. Fragmentswere identified in an 8% polyacrylamide gel and visualized by ethidiumbromide stain. Allele identificationwas registered and then associated tothe corresponding code.
3. Statistical analysis
Categorical variables were expressed as percentages. The age distri-bution was not normal; therefore it was expressed asmedian and quar-tile one and three. Association of genotype and vasovagal syncope wasassessed by a logistic regression model adjusted for age and sex. Weused three genetic models of inheritance; recessive, codominant andadditive form. Genotype and hemodynamic response was evaluatedby correspondence analysis.
Supplemental analysis was made, from the group of cases and con-trols, we randomly formed subgroups of 15 men and 15 women ineach group, with age greater than 18 years. In these subgroups, logisticregression analysiswasmade in twomodels of inheritance, codominantand additive. Results from the logistic regression were expressed asodds ratio (OR) with a 95% confidence interval (CI 95%). Statistical sig-nificance was taken at p b 0.05. Analyses were conducted by using theJMP9 facility software (SAS Institute, Inc., Cary, NC).
4. Results
4.1. General characteristics of participants
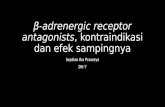
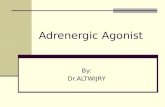
Fig. 1 shows the strategy for participant selection. We were able tocollect a sample of 241 participants attending the syncope until an18 month period. From them, 89 non-related cases were identified, asdiagnosed VVS with a positive HUT test. Also, in this period, 81
rphism ofα1a-adrenergic receptor in vasovagal syncope. Case–control/10.1016/j.autneu.2014.01.005

Fig. 1. Experimental strategy for study participation and patient selection.
3G. Hernández-Pacheco et al. / Autonomic Neuroscience: Basic and Clinical xxx (2014) xxx–xxx
potentially healthy volunteers were contacted but, after the applicationof the exclusion criteria, only 40 control individuals were considered forthe study.
From 89 cases, there were 59 (66.3%) females and 30 (33.7%) maleswith a median of 22 years (IQR: 15.0; 29.5 years). In the control groupthere were 15 (37.5%) females and 25 (62.5%) males with a median of24 years (IQR: 21.5; 29.0 years). Therewas statistical difference by gen-der between groups (p= 0.003) and no statistical differencewas foundwhen age was analyzed (p= 0.23). Allelic and genotype frequencies ofArg347Cys polymorphism of the α1a-adrenergic receptor in groups areshown in Table 1. Table 2 shows the genotype coding to evaluate thedifferent models of inheritance.
Table 1Genotype and allelic frequencies of Arg347Cys polymorphism of the study participants.
Cases (n = 89) Controls (n = 40)
Genotype ArgArg (n = 43) 34 (38.2%) 9 (22.5%)ArgCys (n = 62) 45 (50.7%) 17 (42.5%)CysCys (n = 24) 10 (11.2%) 14 (35.0%)
Allele Arg 113 (63.5%) 35 (43.8%)Cys 65 (36.5%) 45 (56.3%)
Please cite this article as: Hernández-Pacheco, G., et al., Arg347Cys polymostudy in a Mexican population, Auton. Neurosci. (2014), http://dx.doi.org
4.2. Gender, age, VVS, and genotype association analysis
Genotype distribution was not found to be different from those pre-dicted by the Hardy–Weinberg equilibrium in the control (p = 0.17)group.
Table 3 shows the results of the multiple logistic regression analysison the codominant and additive genetic models adjusted for age andgender. The ArgArg genotype had a positive association for bothmodels(codominant OR= 13.2: CI 95% 3.7–55.0, p b 0.001 and additive OR=12.7: CI 95% 3.5–53.0, p b 0.001) with CysCys as reference. Age showedno association. No additional association was found for variableinteractions.
Table 2Genotype coding to evaluate different models of inheritance.
Genotype Codominant Recessive Additive
ArgArg 0 1 1 2ArgCys 1 0 0 1CysCys 0 0 0 0
rphism ofα1a-adrenergic receptor in vasovagal syncope. Case–control/10.1016/j.autneu.2014.01.005

Table 3Adjusted association for sex, age and genotype with vasovagal syncope developmentaccording to the logistic regression model in two genetic models.
Variable Codominant Additive
OR [CI 95%] p OR [CI 95%] p
Gender (female) 6.12 [2.45–17.07] b0.001a 6.11 [2.48–16.57] b0.001a
Age (per year) 0.97 [0.92–1.01] 0.15b 0.97 [0.92–1.01] 0.15Genotype Arg/Arg 13.21 [3.69–54.99] b0.001a 12.68 [3.5–53.07] b0.001a
Arg/Cys 0.44 [0.15–1.20] 0.11Cys/Cys 0.75 [0.018–0.27] b0.001a
a Indicates statistically significant association.b Post-hoc power analysis was performed: 1 − β N 0.80.
4 G. Hernández-Pacheco et al. / Autonomic Neuroscience: Basic and Clinical xxx (2014) xxx–xxx
4.3. Complementary analysis
When homogenized by age and gender, although the sample is evensmaller, the positive association is maintained in both inheritancemodels. The ArgArg genotype was a positive association in the modelscodominant, OR = 5.33: CI 95% 1.03–34.2, p = 0.04, and additiveOR = 5.2: CI 95% 1.02–32.5, p = 0.04, with CysCys as reference.
5. Discussion
Themain findings in this study are: a) ArgArg genotype is a potentialrisk factor for VVS, b) CysCys genotype can be considered as a possibleprotection factor for VVS.
Distribution frequency for the Arg347Cys polymorphism found incontrols was similar to those found in another studymade in aMexicanpopulation (ArgArg 27%, ArgCys 40%, CysCys 35% vs 22.5%, 42.5% and35.0% in our study) (Vargas-Alarcón et al., 2009). The highest VVS prev-alence in females shown in this study is in full agreement with thosealready reported in the literature in other populations (Moya et al.,2009; Park et al., 2010).
Some genes have been studied to look for a genetic association withVVS. Sorrentino et al. studied patients with recurrent syncope, findingno association between ADRA1A polymorphism and VVS in an Italianpopulation (Sorrentino et al., 2010). One major difference is the kindof study, they studied one group of patients with syncope while westudied cases and controls. One small difference is that in our studythe number of female cases was greater than in their study; the meanage for VVS development in our study was closer to those already avail-able in the literature (10 to 30 year range) (Colman et al., 2004; Sheldonet al., 2006;Moya et al., 2009). The differences between their populationand ours could explain these controversial results. However theArg347Cys frequency in the Italian group with a positive HUT test wassimilar to our findings (ArgArg 32%, ArgCys 49%, CysCys 19% vs 38.2%,50.6% and 11.2% in our study). Also, in our study, subjects with no clin-ical history of VVS or presyncope butwithHUT positive resultswere ex-cluded, as well as subjects with a clinical history of VVS and presyncopebut with HUT negative test.
The Arg347Cys polymorphism is located at the carboxy-terminalend of the α1a-adrenergic receptor (Jiang et al., 2005) and has severalprotein isoforms originated by the alternative splicing of the respectivemRNAs. All these protein isoforms are relatively similar except in the se-quence and extension of the C-terminal (Hirasawa et al., 1995; Changet al., 1998; Daniels et al., 1999).
Some proteins interact with the C-terminal region of the receptorsand modulate several functions, like availability, localization andamount of receptor in a determined membrane domain (Hall et al.,1998; Brzostowski and Kimmel, 2001; Diviani et al., 2003). In some re-ceptors, density is maintained by recycling (Morris et al., 2004), there-fore, internalization or receptor removal is a constitutive pathway.
A metalloprotease from the astacin family from amammalian originknown asmTolloid interacts with residues 322 to 359 at the C-terminalend of the α1a-adrenergic receptor (Xu et al., 2006). This interaction
Please cite this article as: Hernández-Pacheco, G., et al., Arg347Cys polymostudy in a Mexican population, Auton. Neurosci. (2014), http://dx.doi.org
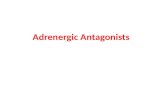
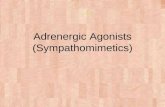
allows receptor internalization. Since the Arg347Cys polymorphismlies in the interacting region with the mTolloid protein, it is reasonableto suggest the possibility that this interaction can be affected by poly-morphism and so the interaction of these proteins can have a differen-tial dynamics depending on the amino acid present in this position.This polymorphism lies on the limits of a transmembrane domainwhere it can interact with both integral membrane proteins as well ascytoplasmatic ones. If an alternative size and charge amino acid ispresent in this region, a different coupling could be done. We hypothe-size that in presence of the agonist, an ArgArg individual could have abetter interaction between the adrenergic receptor and the mTolloidprotein giving place to a faster and more efficient receptor internaliza-tion. This interaction decreases intracellular Ca2+, caused by the sympa-thetic stimuli of the agonist, producing vasodilatation, decrease ofvenous return, increasing the risk of VVS development in ArgArg pa-tients. In the case of CysCys genotype, the interaction with themTolloidprotein is less effective, thus, the internalization of the receptor takeslonger, and therefore, the vasoconstriction state is maintained for a lon-ger period of time,with amore efficient blood return,maintaining bloodpressure and brain perfusion. Given that it is possible to detect asymp-tomatic VVS patients, all subjects without history of presyncope andsyncope positiveHUT,were excluded in order to guarantee that subjectsin the control group did not become cases. Fig. 2 summarizes the pro-posed interaction model.
As in this study, it has been reported that there is a higher affectednumber of women than men (Colman et al., 2004; Moya et al., 2009).Gender differences in blood pressure regulation have been reportedand vascular resistance is an important factor in their regulation. Inmen, the key factor is the equilibrium between cardiac output and sym-pathetic control of the peripheral vasculature resistance (Charkoudianet al., 2005). However, premenopausal women have a diminished sen-sibility to the norepinephrine vasoconstrictor effect in the adrenergicreceptor stimulation and, β2-receptors have a higher adrenalin affinityand possibly have a major role in vasodilatation regulation in women(Kneale et al., 2000; Hart et al., 2009). According to the proposedmodel, it can be suggested that even though women have a lower sup-port for theα adrenergic response for blood pressure regulation, if theyhave an ArgArg genotype, it makes them more susceptible to developVVS due to a vasodilatation increased tendency, explaining the morefrequent and longer lasting VVS episodes (Park et al., 2010). Vascular re-sistance is a decisive factor in blood pressure regulation in men; thispolymorphism could participate in lowering vascular resistance for in-dividuals according to this model.
It is clear that these and other genetic polymorphisms could give riseto a more comprehensible and detailed understanding of the factorsthat control hypotension and bradycardia development, despite thefact that most of the human population is susceptible or has actuallyexperienced a VVS episode during their lifetime. Up to now, it is clearthat VVS is a multifactorial disorder and includes other autonomicresponse-associated genes like β2-adrenergic receptors and otherbody functions like breathing, brain blood flow and other autonomicfunctional modulation along environmental and psychological factors,should be considered.
5.1. Study limitations
In this report, we found a significant association between the α1a-adrenergic receptor and VVS. The simple size was reduced in ourstudy and it is necessary to keep increasing it, because it is importantto estimate parameters with more precision. Although we could evi-dence the association because we homogenized the subjects by ageand gender, the associationwasmaintain in spite of the smaller sample,indicating that the association magnitude is enough to be detected andpost-hoc statistical power was N0.8.
We can only give a general overview of the complex interactions ofall these factorswith the limited data available up to now.More detailed
rphism ofα1a-adrenergic receptor in vasovagal syncope. Case–control/10.1016/j.autneu.2014.01.005

Fig. 2.Possiblemechanism of the participation of Arg347Cys polymorphismwith themTolloid in the receptor internalization. Abbreviations used: PCL: Phospholipase, IP3: Inositol triphos-phate, DAG: diacyl glycerol, PIP2: Phosphatidyl inositol, ER: endoplasmic reticulum, mTolloid: mammalian Tolloid.
5G. Hernández-Pacheco et al. / Autonomic Neuroscience: Basic and Clinical xxx (2014) xxx–xxx
studies are required, and they need to include several other variables fora more precise comprehension of the effect of protein polymorphismsassociated with blood pressure modulation.
6. Conclusions
Arg347Cys polymorphism in α1a-adrenergic receptor is associatedwith the susceptibility for VVS in a group of Mexican subjects. ArgArggenotype could be a potential susceptibility factor in the developmentof VVS and CysCys variable is a potential protective factor for VVS inthe Mexican population.
Acknowledgments
We thank PhD. H. Moreno and R. González Camarena for his com-ments, Betty Lou Chinn RN Bs for language correction and SelmaSánchez for graphic illustration.
References
Azevedo, M.C., Barbisan, J.N., Silva, E.O., 2009. Neurocardiogenic syncope and hereditarity.Rev. Assoc. Med. Bras. 55 (1), 19–21.
Brzostowski, J.A., Kimmel, A.R., 2001. Signaling at zero G: G-protein-independent func-tions for 7-TM receptors. Trends Biochem. Sci. 26 (5), 291–297.
Camfield, P.R., Camfield, C., 1990. Syncope in childhood: a case control clinical study offamily tendency to faint. Can. J. Neurol. Sci. 17, 306–308.
Cárdenas, M., Vallejo, M., Martínez-Palomino, G., Paredes-Balderas, G., Sandoval-Rubio,L.A., Maldonado-Gallardo, E., et al., 2009. Prevalence of syncope in a simple of Mexi-can women residents in Mexico city. Arch. Cardiol. Mex. 79 (3), 197–200.
Chang, D.J., Chang, T.K., Yamanishi, S.S., Salazar, F.H.R., Kosaka, A.H., Khare, R., et al., 1998.Molecular cloning, genomic characterization and expression of novel human α1A-adrenoceptor isoforms. FEBS Lett. 422 (2), 279–283.
Charkoudian, N., Joyner, M.J., Johson, C.P., Eisenach, J.H., Dietz, N.M., Wallin, B.G., 2005.Balance between cardiac output and sympathetic nerve activity in resting humans:role in arterial pressure regulation. J. Physiol. 568 (Pt 1), 315–321.
Colman, N., Nahm, K., Ganzeboom, K.S., Shen, W.K., Reitsma, J.B., Linzer, M., et al., 2004.Epidemiology of reflex syncope. Clin. Auton. Res. 14 (Suppl. 1), I/9–17.
Please cite this article as: Hernández-Pacheco, G., et al., Arg347Cys polymostudy in a Mexican population, Auton. Neurosci. (2014), http://dx.doi.org
Daniels, D.V., Gever, J.R., Jasper, J.R., Kava, M.S., Lesnick, J.D., Meloy, T.D., et al., 1999.Human cloned α1A-adrenoceptor isoforms display α1L-adrenoceptor pharmacologyin functional studies. Eur. J. Pharmacol. 370, 337.
Diviani, D., Lattion, A.L., Abuin, L., Staub, O., Cotecchia, S., 2003. The adaptor complex 2 di-rectly interacts with the alpha 1b-adrenergic receptor and plays a role in receptor en-docytosis. J. Biol. Chem. 278 (21), 19331–19340.
Freitas, S.R., Pereira, A.C., Floriano, M.S., Mill, J.G., Krieger, J.E., 2008. Association of alpha1a-adrenergic receptor polymorphism and blood pressure phenotypes in theBrazilian population. BMC Cardiovasc. Disord. 8, 40.
Ganzeboom, K.S., Colman, N., Reitsma, J.B., Shen, W.K., Weiling, W., 2003. Prevalence andtriggers of syncope in medical students. Am. J. Cardiol. 91, 1006–1008.
Gu, D.G.D., Snieder, H., He, J., Chen, S., Huang, J., Li, B., et al., 2006. Association of alpha 1aadrenergic receptor gene variants on chromosome 8q21 with human stage 2 hyper-tension. J. Hypertens. 24, 1049–1056.
Hall, R.A., Premort, R.T., Chow, C.W., Blitzer, J.T., Pitcher, J.A., Claing, A., et al., 1998. Thebeta2-adrenergic receptor interacts with the Na+/H+-exchanger regulatory factorto control Na+/H+-exchange. Nature 392 (6676), 626–630.
Hart, E.C., Charkoudian, N., Wallin, B.G., Curry, T.B., Eisenbach, J.H., Joyner, M.J., 2009. Sexdifferences in sympathetic neural–hemodynamic balance: implications for humanblood pressure regulation. Hypertension (53), 571–576.
Hermosillo, A.G., Marquez, M.F., Jauregui-Renaud, K., Falcon, J.C., Casanova, J.M., Guevara,M., et al., 2000. Tilt testing in neurocardiogenic syncope: isosorbide versus isoproter-enol. Acta Cardiol. 55 (6), 351–355.
Hermosillo, A.G., Vallejo, M., Covarrubias, F., Rodríguez, A., Kostine, A., Salas, E., et al., 2010.Mecanismos de síncope en nadadoras de Elite. Rev. Iberoam. Arritmol.—RIA 1 (1),74–84.
Hernández-Pacheco, G., Serrano, H., Márquez, M.F., Hermosillo, A.G., Pérez-Vielma, N.,Sotomayor, A., et al., 2008. Genetic study of the vasovagal syncope associated to theArg389Gly polymorphism of the beta1 adrenergic receptor. Arch. Cardiol. Mex. 78(2), 134–138.
Hirasawa, A., Shibata, K., Horie, K., Takei, Y., Obika, K., Tanaka, T., et al., 1995. Cloning func-tional expression and tissue distribution of human αac-adrenoceptor splice variants.FEBS Lett. 363 (3), 256–260.
Hoehe, M.R., Berrettini, W.H., Schwinn, D.A., Hsieh, W.T., 1992. A two-allele PstI RFLPfor the alpha-1c adrenergic receptor gene (ADRA1C). Hum. Mol. Genet. 1 (5),349.
Huang, Y.J., Bao, L.M.,Wang, J.Y., Huang, M., 2010. Association between the polymorphismof GNB3C825T gene and vasovagal syncope in children. Zhonghua Er Ke Za Zhi 48(12), 896–899.
Iacoviello, M., Forleo, C., Sorrentino, S., Romito, R., De Tommmasi, E., Lucarelli, K., et al.,2006. Alpha- and beta-adrenergic receptor polymorphisms in hypertensive and nor-motensive offspring. J. Cardiovasc. Med. 7 (5), 316–321.
Jiang, S., Mao, G., Zhang, S., Hong, X., Tang, G., Li, Z., et al., 2005. Individual and joint asso-ciation of alpha 1A-adrenergic receptor Arg347Cys polymorphism and plasma
rphism ofα1a-adrenergic receptor in vasovagal syncope. Case–control/10.1016/j.autneu.2014.01.005

6 G. Hernández-Pacheco et al. / Autonomic Neuroscience: Basic and Clinical xxx (2014) xxx–xxx
irbersartan concentration with blood pressure therapeutic response in Chinese hy-pertensive subjects. Clin. Pharmacol. Ther. 78 (3), 239–248.
Kenny, R.A., Ingram, A., Bayliss, J., Sutton, R., 1986. Head up tilt: a useful test for investigat-ing unexplained syncope. Lancet 1, 1352–1354.
Kneale, B.J., Chowienczyk, J.P., Brent, S.E., Coltar, D.J., Ritter, J.M., 2000. Gender differences insensitivity to adrenergic agonists of forearm resistance vasculature. JACC 36, 1233–1238.
Lahiri, D.K., Nurnberger, J.I., 1991. A rapid non-enzymatic method for the preparation ofHMW DNA from blood for RFLP studies. Nucleic Acids Res. 19 (19), 5444.
Lelonek, M., Pietrucha, T., Matyjaszczyk, M., Goch, J.H., 2009. Genetic insight into syncopaltilted population with severe clinical presentation. Auton. Neurosci. 147 (1–2), 97–100.
Márquez, M.F., Urías, K.I., Hermosillo, A.G., Jardón, J.L., Iturralde, P., Colín, L., et al., 2005.Familial vasovagal syncope. Europace 7, 472–474.
Mathias, C.J., Deguchi, K., Bleadsdale-Barr, K., Kimber, J.R., 1998. Frequency of family his-tory in vasovagal syncope. Lancet 352, 33–34.
Morris, D.P., Price, R.R., Smith, M.P., Lei, B., Schwinn, D.A., 2004. Cellular trafficking ofhuman α1a-adrenergic receptors is continuous and primarily agonist-independent.Mol. Pharmacol. 66, 843–854.
Moya, A., Sutton, R., Ammirati, F., BlancJJ, Brignole M., Dham, J.B., Deharo, J.C., et al., 2009.Guidelines for the diagnosis and management of syncope (version 2009). The taskforce for the diagnosis andmanagement of syncope of the European Society of Cardi-ology (ESC). Eur. Heart J. 30 (21), 2631–2671.
Mudraková, K., Mitro, P., Salagovic, J., Habalova, V., Kirsch, P., Tkac, I., 2009. Gene polymor-phisms of renin angiotensin system and serotonin transporter gene in patients withvasovagal syncope. Bratisl. Lek. Listy 110 (2), 73–76.
Newton, J.L., Kenny, R., Lawson, J., Frearson, R., Donaldson, P., 2003. Prevalence of familialhistory in vasovagal syncope and haemodynamic response to head up tilt in first de-gree relatives. Clin. Auton. Res. 13, 22–26.
Newton, J.L., Donaldson, P., Parry, S., Kenny, R.A., Smith, J., Gibson, A.M., Morris, Ch., 2007.Angiotensin converting enzyme insertion/deletion polymorphism in vasovagal syn-cope. Europace 7, 396–399.
OldeNordkamp, L.R., Wieling, W., Zwinderman, A.H., Wilde, A.A., van Dijk, N., 2009. Ge-netic aspects of vasovagal syncope: a systematic review of current evidence.Europace 11 (4), 414–420.
Park, J., Jang, S.Y., Yim, H.R., On, Y.K., Shin, D.H., Kim, J.S., 2010. Gender difference inpatients with recurrent neutrally mediated syncope. Yonsei Med. J. 51 (4),499–503.
Please cite this article as: Hernández-Pacheco, G., et al., Arg347Cys polymostudy in a Mexican population, Auton. Neurosci. (2014), http://dx.doi.org
Rokosh, D.G., Simpson, P.C., 2002. Knockout of the α1A/C-adrenergic receptor subtype:the α1A/C is expressed in resistance arteries and is required to maintain arterialblood pressure. Proc. Natl. Acad. Sci. U. S. A. 99 (14), 9474–9479.
Rudner, X.L., Berkowitz, D.E., Booth, J.V., Funk, B.L., Cozart, K.L., DÁmico, E.B., et al., 1999.Subtype specific regulation of human vascular alpha (1)-adrenergic receptors by ves-sel bed and age. Circulation 100 (23), 2336–2343.
Sheldon, R.S., Sheldon, A.G., Connolly, S.J., Morillo, C.A., Klingenheben, T., Krahn, A.D., et al.,2006. Age of first faint in patients with vasovagal syncope. J. Cardiovasc.Electrophysiol. 17, 49–54.
Shibata, H.A., Moriyama, N., Kawabe, K., Ogawa, S., Tsujimoto, G., 1996. α1a-Adrenoceptorpolymorphism: pharmacological characterization and association with benign pros-tatic hypertrophy. Br. J. Pharmacol. 118, 1403–1408.
Snapir, A., Koskenvuo, J., Toikka, J., Ortho-Melander, M., Hinkka, S., Saraste, M., et al., 2003.Effects of common polymorphism in the alpha 1A-, alpha 2b-, beta 1 and beta 2-adrenoreceptors on haemodynamic responses to adrenaline. Clin. Sci. 104 (5),509–520.
Sorrentino, S., Forleo, C., Iacovello, M., Guida, P., DÁndria, V., Favale, S., 2009. Endothelinsystem polymorphisms in tilt test-induced vasovagal syncope. Clin. Auton. Res. 19(6), 347–354.
Sorrentino, S., Forleo, C., Iacoviello, M., Guida, P., Dándria, V., Favale, S., 2010. Lack of asso-ciation between genetic polymorphism affecting sympathetic activity and tilt-induced vasovagal syncope. Auton. Neurosci. 155, 98–103.
Vargas-Alarcón, G., Fragoso, J.M., Cruz-Robles, D., Vargas, A., Martínez, A., Lao-Villadóniga,J.I., et al., 2009. Association of adrenergic receptor gene polymorphism with differentfibromyalgia syndrome domains. Arthritis Rheum. 60 (7), 2169–2173.
Xu, Q., Xu, N., Zhang, T., Li, Z., Yin, F., Han, Q., et al., 2006. Mammalian Tolloid alters sub-cellular localization, internalization, and signaling of α1a-adrenergic receptors. Mol.Pharmacol. 70, 532–540.
Zhang, Y., Hong, X., Liu, H., Huo, Y., Xu, X., 2009. Arg347Cys polymorphism of alpha1A-adrenoceptor gene is associated with blood pressure response to nifedipine GITS inChinese hypertensive patients. J. Hum. Genet. 54 (6), 360–364.
rphism ofα1a-adrenergic receptor in vasovagal syncope. Case–control/10.1016/j.autneu.2014.01.005