Antiadrenergic drugs - drdhriti
38
Antiadrenergic Drugs Dr. D. K. Brahma Department of Pharmacology NEIGRIHMS, Shillong
-
Upload
dr-dhriti-brahma -
Category
Health & Medicine
-
view
3.401 -
download
6
description
A PowerPoint presentation on "Antiadrenergic Drugs" suitable for undergraduate level Medical Students
Transcript of Antiadrenergic drugs - drdhriti

Antiadrenergic Drugs
Dr. D. K. Brahma
Department of Pharmacology
NEIGRIHMS, Shillong

Introduction
Drugs which antagonize the receptor action of Adrenaline and other related drugs at the receptor level
They occupy adrenergic receptors (α and β ) but do not produce signal transduction – affinity is there but without IA - - competitive antagonists
For pharmacologic research, adrenoceptor antagonist drugs have been very useful in the experimental exploration of autonomic nervous system function
Effects vary according to the drug's selectivity for and receptors - α and its subtype specific or β and its subtype specific

Antiadrenergic Drugs - Background Clinically – to modify the responses of endogenous catecholamines
(Adrenaline and Noradrenaline) - physiologic and pathophysiologic
Nonselective α-antagonists: have been used in the treatment of pheochromocytoma (tumors that secrete catecholamines), and alpha-1 selective antagonists are used in primary hypertension and benign prostatic hyperplasia (BHP)
β-receptor antagonist: hypertension, ischemic heart disease, arrhythmias, endocrinologic and neurologic disorders, and many other conditions
Blockade of peripheral dopamine receptors is of no recognized clinical importance at present
In contrast, blockade of central nervous system dopamine receptors is very important – antiemetic, antipsychotic and TCAs

Drugs – Classification
Nonequilibrium type: β-haloalkylamines: Phenoxybenzamine
Equilibrium:I. Nonselective:
1. Ergots: Ergotamine and Ergotoxine2. Hydrogenated ergot alkaloids: DHE, Dihydroergotoxine3. Imidazolines: Tolazoline, Phentolamine4. Miscellaneous: Chlorpromazine, Histamine and Serotonin
II. Selective α-1: Prazosin, Terazosin, Doxazosin and Tamsulosin
III. Selective α-2: Yohimbine

Ergot Images (Claviceps purpurea)
Sclerotium – St Anthony`s Fire
Ergotism

Ergots
Natural: considered derivatives of Lysergic acid (LSD) Amine alkaloid: Ergometrine (ergonovine) Amino acid alkaloids: Ergotamine and ergotoxine –
vasoconstrictor, partial agonist and antagonist at α receptors and 5-HT receptors (1 and 2)
Semisynthetic derivatives: Dihydroergotamine (DHE) and Dihydroergotoxine – more α blocking property

General Effects of alpha Blockade - CVS
Arteriolar and venous tone are determined to a large extent by receptors on vascular smooth muscle
Reduction in Blood Pressure: Blockade of α-1 (also α-2) receptor causes – pooling of blood in capacitance vessels – reduced venous return and Cardiac output – fall in mean BP Postural Reflex is interfered – dizziness and Syncope on
standing Reason: Normally 700 ml of blood is pooled to legs when a person
stands up, and therefore syncope should occur. But do not occur in case of normal person because of Baroreceptor reflex which stimulates VMC and sympathetic system is activated. Contraction of veins occur via α-1 receptor. Blockade of such receptor may therefore may lead to Postural hypotension
Vasopressor effects of Adrenaline is not found - Vasomotor reversal of Dale

Effects of alpha Blockade - Others Reflex tachycardia due to fall in - BP and increased
NA release due to presynaptic alpha-2 blockade Nasal stuffiness and Miosis Increased Intestinal Motility - diarrhoea Reduced GFR: Sodium retention and increase in blood
volume – also reflex renin release Tone of the Bladder trigone, sphincter and prostate is
maintained by α1A sympathetic Blockade produces increased urine flow Inhibition of Ejaculation – due to inhibition of contraction
of vas deferens and others

Individual Agents - Phenoxybenzamine Non specific, long acting irreversible alpha antagonist MOA: Spontaneously cyclizes in the body to give ethyleniminium
intermediate – forms a strong covalent bond with α receptors – blockade of alpha receptor (lasts for 3 – 4 days) Also blockade of 5-HT, histaminergic and cholinergic receptors
Clinically: Postural hypotension: Venodilatation>arteriolar In recumbent position, however:
Blood flow to many organ increased due to reduction in peripheral resistance and increased venous return
Shifts blood from pulmonary to systemic circulation Shifts blood from extravascular to vascular compartment
CNS stimulation – nausea, vomiting on IV injection but oral doses cause depression, tiredness and lethargy

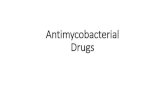
DRC
100% _
50% _
0.1 1 10 100
Log dose
A
A+1XC
A+10XC
A = AgonistC = antagonist

Phenoxybenzamine Pharmacokinetics:
Erratic oral absorption and painful on IM or SC injections Most of the administered drug Excretes in urine in 24 Hrs Small amount may remain in tissue bound covalently – leading to
accumulation in adipose tissue Uses:
Phechromocytoma, Secondary shock and Peripheral vascular disease (Raynaud`s disease)
ADRs: Postural hypotension, nasal stuffiness, miosis and inhibition of ejaculation
Preparation and dosage: 20-60 mg orally 1 mg/kg IV infusion for 1 Hr.

Phentolamine Non specific, short acting reversible alpha antagonist Potent competitive antagonist at both 1 and 2 receptors Quick acting (in minutes) Reduction in Peripheral Resistance - blocking both α-1 and α-2
receptors - causes NA release and venodilatation more than arteriolar
Cardiac stimulation: Enhanced NA release due to alpha-2 blockade Inhibits serotonin release – muscarinic agonist (?)
Uses: Pheochromocytoma, clonidine withdrawal, cheese reaction and in extravasations of NA and Adr injection
Dose: 5 mg IV injection as and when needed

Prazosin Highly selective alpha-1 blocker (1:1000) Non-specific blockade of all subtypes - α1A, α1B and α1D Blockade of sympathetic vasoconstriction - fall in BP NA is not released as α-2 is not blocked (only mild tachycardia) Dilates arterioles more than veins – Postural hypotension is less –
only 1st dose effect (dizziness and fainting) Also inhibits PDE – rise in smooth muscle cAMP - vasodilatation Kinetics: effective orally (70%), metabolized in liver and half life is
6-8 Hrs Uses:
Hypertension Raynaud`s disease BHP
Dose: start with 0.5 mg bed time and then 1-4 mg tds.

Other alpha Blockers Terazosin:
Similar to Prazosin but better bioavailability (90%) Duration of action is longer – 24 Hrs Use: Preferred in BHP – single dose and apoptosis, also in
hypertension Similar is Doxazosin
Tamsulosin: Uroselective (vasicoselective) - α1A and α1D but not α1B No change in BP and HR at therapeutic doses and
Postural hypotension Preferred drug in BHP Only once dosing regime (MR caps) ADRs: Retrograde ejaculation and dizziness

Comparison of alpha blockers
Receptor affinity

Uses of α-blockers
Pheochromocytoma: Tumor of medullary cells of Adrenals VMA and normetanephrine estimation is diagnostic Phentolamine test: Injection of 5mg IV over 1 minute
(recumbent) 35 mm (Systolic) and 25 mm (Diastolic) of Hg
Treatment: Surgery Phenoxybenzamine in preoperatively and intra-operative because:
To Normalize blood volume: Excess CA shifts blood from vascular to extra vascular
To prevent outpouring of CA during surgery To prevent unwanted hypotension due to dilatation of blood vessels
following removal of tumor
(Previously - Clonidine suppression test – Measurement of plasma CA levels)

Uses of α-blockers – contd.
Hypertension: Not useful except Prazosin due to
Compensated cardiac stimulation Postural hypotension, Impotence, nasal blockage etc. Phentolamine and Phenoxybenzamine – in clonidine withdrawal and cheese
reaction
BHP: Static component: Size of prostate (5-alpha reductase) Dynamic component: Tone of Prostate and bladder neck (alpha-1
mediated) Converts testosterone to active dihydrotestosterone)
Effects of α blocking – relaxation of neck and prostate structures – reduction in obstruction
5-α reductase inhibitors like Finesteride decreases size of the prostate – better voiding
α blockers – 2 weeks and 5-alpha reductase inhibitors – 6 months Remember – BHP is a progressive disease

Other uses of α-blockers
Secondary Shock – Phenoxybenzamine Peripheral vascular disease – beneficial in
Raynaud`s disease Congestive Heart Failure – short term Papaverine/Phentolamine induced penile
erection (PIPE) for impotence

Postural Hypotension and 1st dose effect
Remember !

Next Class
β-adrenergic Receptor Blockers

β-adrenergic Blockers
Cardioselective: Metoprolol, atenolol, acebutalol, bisoprolol,
esmolol, betaxolol, celiprolol, nebivolol Nonselective (β1 and β2):
Without intrinsic sympathomimetic activity: Propranolol (membrane stabilizing action), Sotalol and Timolol
With intrinsic sympathomimetic activity (ISA): Pindolol and Oxprenolol
Additional alpha blocking property: Labetolol and Carvedilol

Actions - Propranolol Heart:
Decrease in Heart rate, decrease in cardiac output, decrease in force of contraction
Prolongs systole- synergy of contraction disturbed Not prominent in Normal persons, but in presence of sympathetic
over activity (exercise, emotion) Decreased ventricular size in normal subject – dilatation in low
cardiac reserve patients Cardiac work and oxygen consumption - reduced Total coronary flow reduction (aortic pressure) – subepicardial
region but not subendocardial region – benefit in angina Delayed AV conduction At high doses membrane stabilizing and direct depressant action

Propranolol – Blood Pressure No direct and acute action on Blood Pressure In fact blocks vasodilatation fall in BP by Isoprenaline and enhances
rise in BP by adrenaline – re-reversal of vasomotor reversal But beneficial in hypertensives on prolonged administration Normally, propranolol would block CA induced vasodilatation and
cause increase in TPR and decrease in cardiac output – but negligible change in BP
ADAPTATION: But chronic exposure will lead the resistance vessels to adapt to chronically low CO – TPR falls (Most possible explanation of antihypertensive effect) Other explanations may be:
Decreased Renin release (β1) Central reduction of sympathetic outflow Blockade of NA release – blockade of beta recptors

Re-reversal of Vasomotor reversal

Actions - Propranolol Respiratory:
Bronchoconstriction due to blockade of dilator beta-2 receptors Not considerable in normal individual - May be dangerous in
presence of asthma (avoid) Beta-1 selective drugs are preferred Contrary: COPD patients tolerate
Eye: Decreases IOP by reducing production of aqueous humor – glaucoma
CNS: No considerable CNS effect except – behavioural, forgetfulness and nightmare etc. Suppresses anxiety
Skeletal Muscle: Reduction of Tremor Reduction of exercise capacity: reduction in blood flow,
glycogenolysis and lipolysis

Propranolol Actions – Metabolic Lipid: Inhibits sympathetic stimulation of lipolysis and
consequent increase in free fatty acid level – triglyceride level increased
Carbohydrate: Inhibition of glycogenolysis in heart, muscle and liver – β2 mediated Recovery from insulin action delayed Warning signs are masked
But, Glucagon is the main hormone that responses to hypoglycaemia
Still, beta blockers should be used in caution in patients with diabetes and low glucagon reserve patients and in pancreatectomized patients
β1 selective are much safer

Pharmacokinetics (Propranolol as prototype) - absorption Most of the drugs are well absorbed after oral administration;
peak concentrations occur 1–3 hours after ingestion including propranolol
Propranolol undergoes extensive hepatic (first-pass) metabolism High oral:parenteral ratio – 40:1 Interindividiual and equieffective dose bioavailability variation Metabolism dependent on hepatic blood flow – itself decreases
hepatic blood flow – higher bioavailability on chronic administration – saturation of hepatic extraction mechanism
Higher bioavailability if taken with food Dose available as 10-80 mg tabs. (40 – 160 mg /day) Sustained-release preparations of propranolol and metoprolol are
available

Propranolol - ADRs1. Precipitation of CCF/Oedema –
loss of sympathetic support – careful addition of beta-1 selective
2. Bradycardia3. Respiratory: COAD and Bronchial
asthma (life threatening asthma)4. Risk of Coronary Heart Disease
(triglyceride and LDL increase and fall in HDL)
5. Tiredness and reduced exercise capacity – beta-2 muscle
6. Variant angina exacerbation – unopposed coronary constriction by alpha receptor
7. Cold hands and feet – worsening of Peripheral vascular disease
8. Withdrawal9. Others: GIT upset, nightmare,
forgetfulness and sexual distress

Drug Interactions
Propranolol and insulin: Delayed recovery of hypoglycemia by insulin Warning signs are suppressed
Propranolol + alpha agonists: Rise in BP NSAIDs + Propranolol: Attenuation of
antihypertensive action of beta-blockers

Other Drugs – beta blockers
Cardioselectivity: More selective in blocking β1 receptors than β2
Advantages: Lower propensity to cause Bronchoconstriction Lesser interference with carbohydrate metabolism – safer in diabetics Lower incidence of cold hand and feet – no/less β2 block Lesser suppression of essential tremor Lesser impairment of exercise capacity
Intrinsic sympathomimetic activity: Pindolol, celiprolol Advantages: Partial agonist action
Lesser bradycardia and depression of contractility – preferred in elderly, sick sinus syndrome etc.
Favourable withdrawal, less/no interference with lipid profile

Other beta blockers – contd.
Membrane stabilizing effect: like lidocaine Local anaesthetic action Typically blocks Na+ channel – antiarrhythmic
action Lipid insolubility: Atenolol, celiprolol,
bisoprolol etc. Less likely to produce sleep disturbances Longer acting – incompletely absorbed, no first
pass metabolism, excreted unchanged in urine – t1/2 – 6-2 Hrs Vs 2-6 Hrs

Other Beta Blockers Metoprolol:
Prototype of cardioselective blockers - β1 selective (also inverse agonist)
Safer in patients with bronchoconstriction and preferred in patients with insulin
Less first pass metabolism Slow and fast hydroxylators (CYP2D6 substrate) Used:
In Diabetics and patients in OHs Cold hands and feet with Propranolol
Available as tab – 25/50/100/ mg and IV injection Atenolol:
Selective β1 and low lipid solubility Longer duration of action – once daily dosing No lipid profile adverse effects - Hypertension and angina

Other Beta Blockers Partial beta-agonist: Pindolol, acebutalol, celiprolol,
carteolol, bopindolol, oxprenolol, and penbutolol: Major CVS applications – less plasma lipid action and
bradycardia Intrinsic sympathomimetic activity However, doubtful clinical benefit
Esmolol: partial agonist and MSA Ultra short acting (less than 10 minutes) - inactivated by
esterases in blood Degree of blockade can be titrated - Steady dose can be
maintained Given as IV infusion in SVT, AF, Atrial flutter, arrhythmia
during anaesthesia and cardiac surgery etc. Available as injections IV: 100 – 500 mg/10 ml inj.

Other Beta Blockers Celiprolol:
Selective beta-1 with additional beta-2 agonistic activity Safe in asthmatics Causes vasodilatation by NO production (NA receptor mediated)
– additional benefit as antihypertensive. Dose: 200-600 mg Nebivolol:
Highly selective beta-1 blocker Acts as NO donor - Improves endothelial function and delay of
atheroschlerosis No deleterious effects on carbohydrate, lipid metabolism In CHF and hypertension Dose: 2.5/5 mg

Uses of Beta Blockers1. Hypertension: 1st line of agent (JNC 7)2. Angina pectoris – not in vasospastic3. Myocardia infarction:
Prevent reinfarction Prevent ventricular fibrillation Myocardial salvage: reduction in infarct size
4. Cardiac arrhythmias: Class II type of agent – Propranolol IV (digitalis and anaesthesia induced)
5. Congestive Heart failure6. Phaeochromocytoma7. Hyperthyroidism: T4-T3 + sympathetic symptoms8. Migraine9. Anxiety: social phobia10. Essential Tremor11. Glaucoma

α + β blockers Labetolol:
Alpha + beta blocker (4 diastereomers) Commercially – α1 + β1 + β2 block + β2 agonistic Beta blockade – 1/3rd of Propranolol and alpha – 1/10th of
Phentolamine Beta: alpha = 1: 5 Clinically: Low dose – like propranolol and high dose like
Propranolol + Prazosin Fall in BP (Syst + diast) + vasodilatation (beta-2)
Moderately potent and Used in Phaechromocytoma, clonidine withdrawal
Carvedilol: β1 + β2 and α1 blocker and also Ca+ channel block Vasodilatation – α + Ca++ channel block + antioxidant Uses: Hypertension and especially preferred in CHF as
cardioprotective

Summary Usefulness and actions of β blockers shall be discussed
later - in relation to their use in the particular CVS disease conditions
Remember: Effects of alpha blockade - Phenoxybenzamine, Phentolamine
Test (Phaechromocytoma) Selective alpha-1 blockers and uses - Prazosin, Terazosin and
Tamsulosine Name with selectivity of β blockers as per classification given Pharmacological actions and ADRs of Propranolol as discussed Overall therapeutic uses of beta-blockers – general Idea Individual drugs - Metoprolol, atenolol, esmolol and carvedilol
etc.

Thank you





![Cardiovascular Drugs[1]_ppt [Compatibility Mode]](https://static.fdocument.org/doc/165x107/54506cf8b1af9f19098b4d5a/cardiovascular-drugs1ppt-compatibility-mode.jpg)