Anti-tumor necrosis factor-α induced systemic lupus erythematosus in a patient with metastatic...
3
SHORT REPORT Anti-tumor necrosis factor-α induced systemic lupus erythematosus in a patient with metastatic Crohn's disease—what is the role of anti-TNF antibody? Klaudia Farkas a , Ferenc Nagy a , László Kovács b , Tibor Wittmann a , Tamás Molnár a , ⁎ a First Department of Medicine, University of Szeged, Szeged, Hungary b Department of Rheumatology, University of Szeged, Szeged, Hungary Received 11 May 2012; received in revised form 30 May 2012; accepted 25 June 2012 KEYWORDS Crohn's disease; Infliximab; TNF-α antagonist-induced lupus-like syndrome; Autoantibodies; Cross reactivity Abstract Biological therapies are supposed to trigger the development of autoimmune diseases. We report a case of a 27-year old woman presenting with drug induced systemic lupus erythematosus (SLE) associated with infliximab therapy. The development of paradoxical inflammation in immune-mediated inflammatory diseases patients treated with anti TNF-α suggests that an unknown inflammatory pathway may be provoked by inhibiting TNF-α. We suppose that in our case a cross reactivity between anti-infliximab antibodies and autoanti- bodies may lead to the development of TNF-induced immune disease. © 2012 European Crohn's and Colitis Organisation. Published by Elsevier B.V. All rights reserved. 1. Introduction Drug induced lupus erythematosus like syndrome is a rarely described condition in Crohn's disease; however patients treated with biological therapy are slightly more susceptible for developing such an adverse reaction. 1 The use of anti-TNF agents has been associated with an increasing number of autoimmune diseases, mainly lupus, vasculitis, and intestinal lung disease. 2 Biological therapies are supposed to trigger the development of autoimmune diseases, although allergic reac- tion or loss of response due to the production of antibodies against the TNF blockers may also play role in the development of these complications. From another point of view, the mechanism in the background of this effect may be stimulated humoral immunity: production of autoantibodies due to the neutralization of TNF-α or inhibition of cytotoxic T lymphocytes by TNF blockade. 3,4 Although the development of autoanti- bodies is common during infliximab therapy; drug induced lupus erythematosus like syndrome is still rare. A study of 500 Crohn's disease patients from the Mayo Clinic revealed only three patients who developed drug induced lupus during the ⁎ Corresponding author at: Tamás Molnár, First Department of Medicine, University of Szeged, H-6720, Korányi fasor 8, Szeged, Hungary. Tel.: + 36 62 545186; fax: + 36 62 545185. E-mail address: [email protected] (T. Molnár). 1873-9946/$ - see front matter © 2012 European Crohn's and Colitis Organisation. Published by Elsevier B.V. All rights reserved. doi:10.1016/j.crohns.2012.06.016 Available online at www.sciencedirect.com Journal of Crohn's and Colitis (2013) 7, e143–e145
Transcript of Anti-tumor necrosis factor-α induced systemic lupus erythematosus in a patient with metastatic...

Ava i l ab l e on l i ne a t www.sc i enced i r ec t . com
Journal of Crohn's and Colitis (2013) 7, e143–e145
SHORT REPORT
Anti-tumor necrosis factor-α induced systemic lupuserythematosus in a patient with metastatic Crohn'sdisease—what is the role of anti-TNF antibody?Klaudia Farkas a, Ferenc Nagy a, László Kovács b,Tibor Wittmann a, Tamás Molnár a,⁎
a First Department of Medicine, University of Szeged, Szeged, Hungaryb Department of Rheumatology, University of Szeged, Szeged, Hungary
Received 11 May 2012; received in revised form 30 May 2012; accepted 25 June 2012
⁎ Corresponding author at: TamásMedicine, University of Szeged, H-67Hungary. Tel.: +36 62 545186; fax: +3
E-mail address: molnar.tamas@me
1873-9946/$ - see front matter © 2012doi:10.1016/j.crohns.2012.06.016
KEYWORDSCrohn's disease;Infliximab;TNF-α antagonist-inducedlupus-like syndrome;Autoantibodies;Cross reactivity
Abstract
Biological therapies are supposed to trigger the development of autoimmune diseases. Wereport a case of a 27-year old woman presenting with drug induced systemic lupuserythematosus (SLE) associated with infliximab therapy. The development of paradoxicalinflammation in immune-mediated inflammatory diseases patients treated with anti TNF-αsuggests that an unknown inflammatory pathway may be provoked by inhibiting TNF-α. Wesuppose that in our case a cross reactivity between anti-infliximab antibodies and autoanti-
bodies may lead to the development of TNF-induced immune disease.© 2012 European Crohn's and Colitis Organisation. Published by Elsevier B.V. All rights reserved.Molnár, First Department of20, Korányi fasor 8, Szeged,6 62 545185.d.u-szeged.hu (T. Molnár).
European Crohn's and Colitis
1. Introduction
Drug induced lupus erythematosus like syndrome is a rarelydescribed condition in Crohn's disease; however patientstreated with biological therapy are slightly more susceptiblefor developing such an adverse reaction.1 The use of anti-TNFagents has been associated with an increasing number ofautoimmune diseases, mainly lupus, vasculitis, and intestinal
Org
lung disease.2 Biological therapies are supposed to trigger thedevelopment of autoimmune diseases, although allergic reac-tion or loss of response due to the production of antibodiesagainst the TNF blockers may also play role in the developmentof these complications. From another point of view, themechanism in the background of this effect may be stimulatedhumoral immunity: production of autoantibodies due to theneutralization of TNF-α or inhibition of cytotoxic T lymphocytesby TNF blockade.3,4 Although the development of autoanti-bodies is common during infliximab therapy; drug induced lupuserythematosus like syndrome is still rare. A study of 500 Crohn'sdisease patients from the Mayo Clinic revealed only threepatients who developed drug induced lupus during the
anisation. Published by Elsevier B.V. All rights reserved.

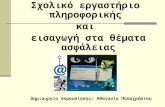
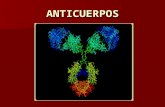
Figure 2 Closed preauricular fistula after infliximab inductiontherapy.
e144 K. Farkas et al.
therapy.5 In Hungary infliximabwas approved for the treatmentof moderate to severe Crohn's disease in 2001. We report a caseof a 27-year old woman presenting with drug induced systemiclupus erythematosus (SLE) associated with infliximab therapy.In the past 10 years, the present is the only case of the morethan 230 patients who have been on biological therapy whenanti-TNF α therapy provoked the occurrence of SLE at ourcenter.
2. Case report
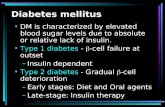
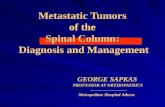
Crohn's disease of our female patient was diagnosed in 2007at age 22 years when she was presented with fever, diarrhea,aphthous stomatitis and a painful mass in the preauricularregion requiring surgical intervention. Ileocolonoscopy iden-tified aphthous lesions in the ileum, the right side of thecolon and the transverse colon. After initiating the treatmentwith mesalazine and corticosteroids her symptoms graduallyimproved. Two years later she developed active symptomsand perianal abscess. Mesalazine was stopped because ofloss of efficacy. After adding azathioprine and draining theabscess the patient shortly achieved remission. However, inJanuary 2010 she presented with recently activated 2×1-cmdischarging preauricular and perianal fistula; thereforeinfliximab therapy was started (Fig. 1). The histology offacial skin manifestation showed epitheloid histiocytes andmassive mononuclear infiltration. The activity-related pre-auricular fistula was suspected as metastatic Crohn's disease.With the infusion regimen of 5 mg/kg at 8-week intervals thepreauricular fistula remitted (Fig. 2) and the discharge of theperianal fistula reduced significantly. However, at the end ofthe one-year treatment period, the patient presented withswelling and pain in her fingers, wrists, elbows, knees andankles and her walking became difficult. Her bowel symp-toms were still in remission, although the perianal fistulastarted to discharge again.
Physical examination revealed swollen and tender shoul-ders, fingers, knees and toes without cutaneous symptoms.Laboratory investigation showed elevated C-reactive protein(24.5 mg/l) and erythrocyte sedimentation rate (66 mm/h),a positive serum anti-nuclear antibody, significantly elevatedanti-Sjogren's syndrome A antibody (181 U/ml) and anti-Sjogren's syndrome B antibody (N200 U/ml). Anti-double-stranded (ds)DNA, anti-ribonuclear protein/anti-Smith anti-body and anti-histone antibodies were also positive. C3 andC4 levels were normal. The patient was negative for anti
Figure 1 Preauricular fistula before infliximab therapy.
cardiolipin antibodies (IgG, IgM, IgA) and anti Beta-2-glycoprotein-1 (IgG, IgM, IgA). She did not have any sign ofrenal involvement; urea and creatinine levels were in normalrage. The pharmacokinetic examinations revealed low inflix-imab trough levels (2.75 ng/ml) and high levels of antibodiesagainst infliximab (ATI-3194 ng/ml). On the basis of the clinicalsymptoms, the autoimmune and pharmacokinetic measure-ments the diagnosis of infliximab induced SLE was established.Infliximab was stopped and low dose oral methylprednisolone(8 mg daily) was administered. Her symptoms resolvedcompletely within 2 months after stopping infliximab and hergastrointestinal symptoms also remained in remission withazathioprine monotherapy. Methylprednisolone was graduallytapered and stopped after 4 months of therapy. Because of herdischarging perianal fistula, Seton placement was performed inJanuary 2012.
3. Discussion
Metastatic Crohn's disease presents as cutaneous manifesta-tion of Crohn's disease characterized by ulcerative lesions. Theskin lesions may precede the diagnosis of Crohn's disease andusually show simultaneous activity with the clinical course.The presence of granulomas in MCD is the most prominenthistopathologic finding, and Langerhans giant cells arefrequently seen along with epithelioid histiocytes and anaccompanying lymphoplasmacytic infiltrate.6
Biopsies of these lesions show noncaseating granulomasthat are characteristic of Crohn's disease.7 In our case, thesimultaneous appearance of preauricular fistula and theintestinal symptoms suggested the diagnosis of metastaticCrohn's disease, although metastatic Crohn's disease on theface is a rare entity.8,9 Infliximab has not only proven itsefficacy in the treatment of metastatic Crohn's disease;furthermore, it seems to be the most beneficial in themanagement of mucocutaneous manifestations.10,11
In the last two decades anti-tumor necrosis factor(TNF)-α has been extensively used for the treatment ofimmune-mediated diseases. However, with the increasing useof anti TNF-α therapy, the number of anti TNF-α related sideeffect is also increasing. Paradoxical inflammatory reactionshave been described in patients with immune-mediatedinflammatory diseases receiving biological therapy. The reviewof Fiorino et al.12 revealed the onset of psoriasis in 18 cases ofpatients with inflammatory bowel disease treated with anti

e145Anti-tumor necrosis factor-α induced SLE in a patient with metastatic Crohn's disease
TNF therapy. In the majority of the patients, psoriatic lesionsresolved after cessation of biological therapy. The develop-ment of paradoxical inflammation in immune-mediated in-flammatory diseases patients treated with anti TNF-α suggeststhat an unknown inflammatory pathway is provoked byinhibiting TNF-α. According to the hypothesis of Fiorino et al.interferon (IFN) α may play an important role in thedevelopment of TNF-α induced psoriasis. Withdrawing biolog-ical therapy or switching to another anti TNF agent may beconsidered in these very rare conditions.
The least rigorous criteria for diagnosis of drug inducedlupus need one or more symptoms compatible with lupuserythematosus, ongoing exposure to a drug known to causedrug induced lupus, no prior history of lupus erythematosus,and resolution of symptoms when the offending drug isdiscontinued.13 In our case, the patient suffered fromarthritis, had antibodies to dsDNA and ANA positivity (threesymptoms compatible with SLE) was also detected; shereceived infliximab which had been shown to provoke druginduced lupus, never had SLE before and her symptomsresolved after discontinuing anti TNF therapy.
Treatment with infliximab can cause immunogenicity andthe formation of ATI.14 Detectable infliximab in the serumpredicts higher rates of remission and endoscopic improve-ment,15 while ATI positive patients are associated withlower response to infliximab and with the development ofadverse reactions.16 Infliximab-treated patients also devel-op autoantibodies in some cases, including ANA andanti-dsDNA antibodies that may be associated with SLE.17
Patients with ANA positivity before infliximab therapy aremore susceptible to develop dsDNA antibodies and druginduced lupus. Compared to drug-related lupus, dsDNA ispositive in 100% of TNF-α antagonist-induced lupus-likesyndrome.18 The concept of TNF-α antagonist-inducedlupus-like syndrome (TAILS) was first referred in a publicationof Williams and Cohen.13 They postulated some hypotheses forthe development of TAILS, including the role of anti TNF-αinduced apoptosis, the activation B lymphocytes and thereforethe increased autoantibody production, and finally thesuppression of cytotoxic T-lymphocytes.18 In our case, ATIand autoantibodies like anti dsDNA and ANA antibodies weredetected simultaneously. The results of a recent study19
suggest a role for autoantibodies in the development of ATIand the development of loss of response under treatment withinfliximab in psoriasis. It has been previously shown thatmicrobial stimulation of the immune system may provoke theproduction of auto-antibodies.20,21 The study of Zhang andReichlin22 demonstrated that anti-dsDNA antibodies from lupuspatients can react with burkholderia fungorum bacterialcell lysates. This supports the hypothesis that the origin ofanti-dsDNA antibodies in SLE may be associated with burkhol-deria bacterial infection and this crossreactivitymay play a rolein the development of autoimmunity. We suppose that in ourcase a cross reactivity between ATI and the autoantibodiesmayalso lead to the development of TNF induced immune disease.
References
1. Zella GC,Weinblatt ME,Winter HS. Drug-induced lupus associatedwith infliximab and adalimumab in an adolescent with Crohndisease. J Pediatr Gastroenterol Nutr 2009;49:355–8.
2. Ramos-Casals M, Brito-Zerón P, Muñoz S, Soria N, Galiana D,Bertolaccini L, et al. Autoimmune diseases induced byTNF-targeted therapies. Analysis of 233 cases. Medicine2007;86:242–51.
3. Eriksson C, Engstrand S, Sundqvist KG, Rantapää-Dahlqvist S.Autoantibody formation in patients with rheumatoid arthritistreated with anti-TNF alpha. Ann Rheum Dis 2005;64:403–7.
4. Via CS, Shustov A, Rus V, Lang T, Nguyen P, Finkelman FD. Invivo neutralization of TNF-alpha promotes humoral autoimmu-nity by preventing the induction of CTL. J Immunol 2001;167:6821–6.
5. Colombel JF, Loftus EV, Tremaine WJ, Egan LJ, Harmsen WS,Schleck CD, et al. The safety profile of infliximab in patientswith Crohn's disease: the Mayo clinic experience in 500 patients.Gastroenterology 2004;126:19–31.
6. Guest GD, Fink RLW. Metastatic Crohn's disease. Case report ofan unusual variant and review of the literature. Dis ColonRectum 2000;43:1764–6.
7. Chuah JH, Kim DS, Allen C, Hollis L. Metastatic Crohn's diseaseof the ear. Int J Otolaryngol 2009;2009:871567.
8. Graham DB, Jager DL, Borum ML. Metastatic Crohn's disease ofthe face. Dig Dis Sci 2006;51:2062–3.
9. McCallum DI, Gray WM. Metastatic Crohn's disease. BrJ Dermatol 1976;95:551–4.
10. Kaufman I, Caspi D, Yeshurum D, Dotan I, Yaron M, Elkayam O.The effect of infliximab on extraintestinal manifestations ofCrohn's disease. Rheumatol Int 2005;25:406–10.
11. Fiorino G, Allez M, Malesci A, Danese S. Review article: antiTNF-a induced psoriasis in patients with inflammatory boweldisease. Aliment Pharmacol Ther 2009;29:921–7.
12. Williams VL, Cohen PR. TNF alpha antagonist-induced lupus-likesyndrome: report and review of the literature with implicationsfor treatment with alternative TNF alpha antagonists. IntJ Dermatol 2011;50:619–25.
13. Baert F, Noman M, Vermeire S, Van Assche G, D' Haens G,Carbonez A, et al. Influence of immunogenicity on the long-termefficacy of infliximab in Crohn's disease. N Engl J Med 2003;348:601–8.
14. Seow CH, Newman A, Irwin SP, Steinhart AH, Silverberg MS,Greenberg GR. Trough serum infliximab: a predictive factor ofclinical outcome for infliximab therapy in acute ulcerativecolitis. Gut 2010;59:49–54.
15. Pariente B, de Chambrun GP, Krzysiek R, Desroches M, Louis G,De Cassan C, et al. Trough levels and antibodies to infliximabmay not predict response to intensification of infliximabtherapy in patients with inflammatory bowel disease. InflammBowel Dis 2012;18:1199–206.
16. Klapman JB, Ene-Stroescu D, Becker MA, Hanauer SB. Alupus-like syndrome associated with infliximab therapy.Inflamm Bowel Dis 2003;9:176–8.
17. Costa MF, Said NR, Zimmermann B. Drug-induced lupus due toanti-tumor necrosis factor alpha agents. Semin Arthritis Rheum2008;37:381–7.
18. Hoffmann JH, Hartmann M, Enk AH, Hadaschik EN. Autoantibodiesin psoriasis as predictors for loss of response and anti-infliximabantibody induction. Br J Dermatol 2011;165:1355–8.
19. El-Roiey A, Sela O, Isenberg DA, Feldman R, Colaco BC, KennedyRC, et al. The sera of patients with Klebsiella infections containa common anti-DNA idiotype (16/6) Id and anti-polynucleotideactivity. Clin Exp Immunol 1987;67:507–15.
20. Unni KK, Holley KE, McDuffie FC, Titus JL. Comparative studyof NZB mice under germ-free and conventional conditions.J Rheumatol 1975;2:36–44.
21. Zhang W, Reichlin M. A possible link between infection withBurkholderia bacteria and systemic lupus erythematosus basedon epitope mimicry. Clin Dev Immunol 2008;2008:683489.
22. Siroy A, Wasman J. Metastatic Crohn's disease: a rare cutaneousentity. Arch Pathol Lab Med 2012;136:329–32.