Adora2b Adenosine Receptor Signaling Protects during Acute Kidney Injury via Inhibition of...
9
of October 4, 2012. This information is current as Release α Inhibition of Neutrophil-Dependent TNF- Protects during Acute Kidney Injury via Adora2b Adenosine Receptor Signaling Tak, Holger K. Eltzschig and Eric T. Clambey Almut Grenz, Jae-Hwan Kim, Jessica D. Bauerle, Eunyoung ol.1201651 http://www.jimmunol.org/content/early/2012/09/26/jimmun published online 1 October 2012 J Immunol Subscriptions http://jimmunol.org/subscriptions is online at: The Journal of Immunology Information about subscribing to Permissions http://www.aai.org/ji/copyright.html Submit copyright permission requests at: Email Alerts http://jimmunol.org/cgi/alerts/etoc Receive free email-alerts when new articles cite this article. Sign up at: Print ISSN: 0022-1767 Online ISSN: 1550-6606. Immunologists, Inc. All rights reserved. Copyright © 2012 by The American Association of 9650 Rockville Pike, Bethesda, MD 20814-3994. The American Association of Immunologists, Inc., is published twice each month by The Journal of Immunology at Univ of Calgary Hlth Sci Ctr/Hlth Sci Lib/Per on October 4, 2012 http://jimmunol.org/ Downloaded from
Transcript of Adora2b Adenosine Receptor Signaling Protects during Acute Kidney Injury via Inhibition of...

of October 4, 2012.This information is current as
ReleaseαInhibition of Neutrophil-Dependent TNF-
Protects during Acute Kidney Injury via Adora2b Adenosine Receptor Signaling
Tak, Holger K. Eltzschig and Eric T. ClambeyAlmut Grenz, Jae-Hwan Kim, Jessica D. Bauerle, Eunyoung
ol.1201651http://www.jimmunol.org/content/early/2012/09/26/jimmun
published online 1 October 2012J Immunol
Subscriptionshttp://jimmunol.org/subscriptions
is online at: The Journal of ImmunologyInformation about subscribing to
Permissionshttp://www.aai.org/ji/copyright.htmlSubmit copyright permission requests at:
Email Alertshttp://jimmunol.org/cgi/alerts/etocReceive free email-alerts when new articles cite this article. Sign up at:
Print ISSN: 0022-1767 Online ISSN: 1550-6606. Immunologists, Inc. All rights reserved.Copyright © 2012 by The American Association of9650 Rockville Pike, Bethesda, MD 20814-3994.The American Association of Immunologists, Inc.,
is published twice each month byThe Journal of Immunology
at Univ of C
algary Hlth Sci C
tr/Hlth Sci L
ib/Per on October 4, 2012
http://jimm
unol.org/D
ownloaded from

The Journal of Immunology
Adora2b Adenosine Receptor Signaling Protects during AcuteKidney Injury via Inhibition of Neutrophil-Dependent TNF-aRelease
Almut Grenz,* Jae-Hwan Kim,† Jessica D. Bauerle,‡ Eunyoung Tak,*
Holger K. Eltzschig,* and Eric T. Clambey*
Renal ischemia is among the leading causes of acute kidney injury (AKI). Previous studies have shown that extracellular adenosine is
a prominent tissue-protective cue elicited during ischemia, including signaling events through the adenosine receptor 2b (Adora2b).
To investigate the functional role of Adora2b signaling in cytokine-mediated inflammatory pathways, we screened wild-type and
Adora2b-deficient mice undergoing renal ischemia for expression of a range of inflammatory cytokines. These studies demon-
strated a selective and robust increase of TNF-a levels in Adora2b-deficient mice following renal ischemia and reperfusion. Based
on these findings, we next sought to understand the contribution of TNF-a on ischemic AKI through a combination of loss- and
gain-of-function studies. Loss of TNF-a, through either Ab blockade or study of Tnf-a–deficient animals, resulted in significantly
attenuated tissue injury and improved kidney function following renal ischemia. Conversely, transgenic mice with overexpression
of TNF-a had significantly pronounced susceptibility to AKI. Furthermore, neutrophil depletion or reconstitution of Adora2b2/2
mice with Tnf-a–deficient neutrophils rescued their phenotype. In total, these data demonstrate a critical role of adenosine
signaling in constraining neutrophil-dependent production of TNF-a and implicate therapies targeting TNF-a in the treatment
of ischemic AKI. The Journal of Immunology, 2012, 189: 000–000.
Acute kidney injury (AKI) is clinically defined as an abruptreduction in kidney function (e.g., a decrease in glo-merular filtration rate [GFR]) over minutes to days (1).
AKI can result from multiple etiologies, including sepsis andsurgical procedures (both of the kidney and other tissues includingthe heart) (2–5). Although the rate of mortality associated withAKI varies depending on the specific combination of etiology withAKI, even moderate levels of kidney injury are associated with a70% greater risk of death than in patients without evidence of AKI(3). Notably, individuals who survive AKI are at an increased riskfor long-term sequelae, including progression to chronic kidneydisease and end-stage renal disease (6, 7). Despite the signifi-cant medical challenge of AKI, therapeutic approaches to preventor treat AKI are limited; to date, the majority of clinical trialsfor AKI have failed (8, 9). Because of this unmet medical need,there is significant interest in further understanding the path-ogenesis of AKI and developing novel therapeutic approachesfor AKI.
Although there are multiple etiologies for AKI, a commonoccurrence contributing to AKI is obstruction of renal blood flow,which results in renal ischemia (10). The pathogenesis of AKIfollowing renal ischemia is multifactorial, involving the impairedfunction and apoptosis of tissue-resident epithelial and endo-thelial cells, followed by the resulting inflammatory cascade thatsequentially recruits neutrophils, monocytes, and T cells to thepostischemic kidney (10). The outcome of AKI is regulated bythe balance of pathogenic mechanisms (e.g., prolonged ischemia,cell death, and the elicitation of proinflammatory cytokines includingTNF-a) relative to protective mechanisms (e.g., extracellular aden-osine, heme oxygenase, and the production of proresolving leu-kotrienes) (10).Among tissue-protective factors elicited during ischemia, there
is clear evidence that the generation and signaling of extracellularadenosine can function as a primary mechanism that limits ischemictissue injury and inflammation (11, 12). These suppressive functionsof extracellular adenosine signaling are exemplified by seminalstudies by Sitkovsky et al. (13), in which the adenosine receptor2a (Adora2a) was identified as a potent anti-inflammatory receptorin vivo. During tissue ischemia, there is a transient accumulationof extracellular adenosine, generated by the stepwise degradationof precursor molecules (nucleotides including ATP, ADP, or AMP)(14, 15). Extracellular adenosine signals through four distinctadenosine receptors (Adora1, Adora2a, Adora2b, Adora3) (16, 17),and studies show that hypoxia also enhances adenosine signalingby transcriptional increases of adenosine receptor levels (15). Al-though the mechanisms by which extracellular adenosine mediateprotective effects remain only partially understood, adenosine re-ceptor signaling can potently limit inflammation by influencing bothparenchymal and bone marrow-derived compartments (11, 18). Inthe context of Adora2b, the focus of this research, multiple studieshave demonstrated that adenosine generation and signaling viaAdora2b protects against ischemic injury in the heart (19, 20),liver (21), and intestine (22, 23).
*Mucosal Inflammation Program, Department of Anesthesiology, University of Col-orado Denver, Aurora, CO 80045; †Department of Anesthesiology, Korea UniversityCollege of Medicine, Seoul 136-701, Korea; and ‡Department of Anesthesiology,Perioperative, and Pain Medicine, Brigham and Women’s Hospital, Harvard MedicalSchool, Boston, MA 02115
Received for publication June 14, 2012. Accepted for publication August 23, 2012.
This work was supported by the Juvenile Diabetes Research Foundation and anAmerican Heart Association grant (to A.G.), National Institutes of Health GrantsR01-HL092188, R01-DK083385, and R01-HL098294, and a grant from the Crohn’sand Colitis Foundation of America (to H.K.E.).
Address correspondence and reprint requests to Dr. Eric T. Clambey, Mucosal In-flammation Program, Department of Anesthesiology, University of Colorado Denver,12700 East 19th Avenue, Mailstop B112, Research Complex 2, Room 7118, Aurora,CO 80045. E-mail address: [email protected]
Abbreviations used in this article: Adora2b, adenosine receptor 2b; AKI, acute kid-ney injury; ARE, AU-rich element; GFR, glomerular filtration rate.
Copyright� 2012 by The American Association of Immunologists, Inc. 0022-1767/12/$16.00
www.jimmunol.org/cgi/doi/10.4049/jimmunol.1201651
Published October 1, 2012, doi:10.4049/jimmunol.1201651 at U
niv of Calgary H
lth Sci Ctr/H
lth Sci Lib/Per on O
ctober 4, 2012http://jim
munol.org/
Dow
nloaded from

Previous studies identified that extracellular adenosine genera-tion and signaling through adenosine receptors can potently limitAKI (24–29). Although protective effects of adenosine involvesignaling through multiple adenosine receptors (including Adora1,Adora2a, and Adora2b), each of which influences discrete celltypes and phases of AKI (as reviewed in Refs. 26, 30), thehypoxia-inducible nature of Adora2b (also known as the A2Badenosine receptor) places it as a prominent pathway affordingrenovascular protection during ischemia (31). Recent studies haveshown that one protective mechanism elicited by Adora2b sig-naling is to restore optimal blood flow to the postischemic kidney(32). In this study, we sought to investigate the contribution ofAdora2b in limiting inflammation and tissue damage during AKI,with a particular focus on leukocyte regulation. These studiesdemonstrated that Adora2b has a critical role in specifically reg-ulating TNF-a production and that Adora2b restricts tissue dam-age mediated by neutrophils via this pathway.
Materials and MethodsMice generation and breeding
All mice were housed in a 12-h light/dark cycle and were gender-, age-, andweight-matched between 12 and 16 wk. In transcript and pharmacologicalstudies, C57BL/6J mice obtained from The Jackson Laboratory were used.Mice deficient in TNF-a (33) were obtained from The Jackson Laboratory(B6;129S-Tnftm1Gkl/J, stock number 003008). TNFD AU-rich elements(ARE) mice (34) were kindly provided by Dr. Jesus Rivera-Nieves(University of California, San Diego, La Jolla, CA) and generated, vali-dated, and characterized as previously described (35). Adora2b-deficient(Adora2b2/2) mice were characterized as previously described (31).
Murine model for renal ischemia
Mice underwent right nephrectomy followed by left renal artery ischemia(0, 10, 30, and 40 min of ischemia) using a hanging weight system, aspreviously described (24, 25, 31, 36). Briefly, a right nephrectomy isperformed, and then the left kidney is carefully isolated and the left adrenalgland dissected away. The kidney is placed in a lucite cup, and a 7–0 nylonsuture is threaded under the renal artery. Weights are attached at both endsof the suture, and ischemia is performed for indicated time points. Ischemiais confirmed by color change of the kidney from red to pale white. At theend of the designated ischemic time period, the weights are resupported,and reperfusion ensues. Inulin clearance was performed 1 h followingreperfusion.
Inulin clearance
Inulin clearance was measured 1 h after renal ischemia (40 min) as de-scribed previously (31). Briefly, mice were anesthetized using 50 mg/kgi.p. pentobarbital. Animals were then placed on a temperature-controlledoperating table to keep rectal temperature at 37˚C. The right jugular veinwas cannulated for continuous infusion. Blood samples were taken viaretro-orbital vein plexus puncture. A catheter was placed in the urinarybladder for timed urine collection after removal of the right kidney. Aftersurgery, mice received a bolus of 0.45% sodium chloride solution in anamount equal to 20% body weight. Continuous infusion was maintained ata rate of 800 ml/h/25 g body weight, and FITC-labeled inulin (0.75 g/100ml; Sigma-Aldrich) was added to the infusion for evaluation of whole-kidney GFR as described before (37, 38). After stabilization of the animalsfor 20 min, 20-min timed urine collections were performed. Blood wasobtained in the middle of every urine collection period for measurement ofFITC-inulin. Concentration of inulin in plasma and urine was performedby measurement of wavelength using a spectophotometer (Biotek Synergy2), and GFR was calculated by standard formulas.
Renal histology
Kidneys were excised and harvested 24 h following 40 min of renal ischemia.Renal tissues were fixed in 4.5% buffered formalin, dehydrated, and em-bedded in paraffin. Sections (3 mm) were stained with H&E (31). Exami-nation and scoring of three representative sections of each kidney (n = 4–6for each condition) were carried out blinded.
Cytokine ELISA
To quantify renal cytokine content, we performed cytokine ELISA andfollowed the manufacturer’s instructions (Meso Scale Discovery).
Transcriptional analysis
Total RNA was isolated from mouse kidneys using the TRIzol Reagentaccording to the manufacturer’s instructions (Invitrogen). Therefore, frozentissue was homogenized in TRIzol Reagent (Invitrogen) and chloroform.After spinning at 12,000 3 g for 15 min, the aqueous phase was removed,and the RNAwas precipitated with isopropanol. RNAwas pelleted, washedwith ethanol, treated with DNAse, and the concentration was quantified.The PCR reactions contained 1 mM sense and 1 mM antisense oligonu-cleotides with SYBR Green (Bio-Rad). Each target sequence was ampli-fied using increasing numbers of cycles of 94˚C for 1 min, 58˚C for 0.5min, and 72˚C for 1 min. Quantification of transcript levels was measuredby real-time RT-PCR (iCycler; Bio-Rad). Primers for TNF were: forward59-CCC ACT CTG ACC CCT TTA CT-39 and reverse 59-TTT GAG TCCTTG ATG GTG GT-39.
Ab-based studies
To neutralize TNF-a in vivo, mice were treated with infliximab (Remicade;Jannsen Biotech), a TNF-a–specific mAb therapy, at a dose of 10 mg/kgbody weight by i.p. injection 60 min prior renal ischemia. To depleteneutrophils, mice were injected with 150 mg anti-Gr1 Ab (clone RB6-8C5;BioXCell). This Ab results in .90% depletion of neutrophils for at least24 h (data not shown and Ref. 39).
Neutrophil adoptive transfer
Neutrophils were enriched from Adora2b2/2 or Tnf-a2/2 mice using mag-netic bead-based enrichment (Ly6G beads; Miltenyi Biotec) for positiveenrichment for neutrophils. A total of 33 106 enriched neutrophils were thenadoptively transferred by i.v. transfer into the indicated recipient mice.
Statistical analysis
A grading scale of 0–4, as outlined by Jablonski et al. (40), was used for thehistopathological assessment of proximal tubular damage. These renalinjury score data are given as median and range; all other data are pre-sented as mean 6 SD. Renal injury was analyzed with the Kruskal-Wallistest, with follow-up pairwise comparisons by Wilcoxon Mann–WhitneyU test. Jablonski index results are shown as box-and-whisker plots. Thelines within the boxes show the median, the bounds of the boxes show theupper and lower median, and the whiskers extend out to the data’s smallestand largest number. For all other outcomes, data were compared by two-factor ANOVA with Bonferroni’s posttest or by two-tailed Student t testwhen appropriate. Data are expressed as mean6 SD. A p value,0.05 wasconsidered statistically significant. For all statistical analyses, GraphPadPrism 5.0 software (GraphPad) for Windows XP was used.
Study approval
All animal protocols were in accordance with the United States Guidelinesof the International Animal Care and Use Committee for use of livinganimals and approved by the Institutional Animal Care and Use Committeeof the University of Colorado guidelines for animal care.
ResultsAdora2b2/2 mice have a selective and profound induction ofTNF-a during AKI
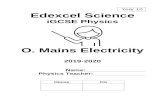
Previous studies had implicated Adora2b signaling in tissue pro-tection from ischemia and reperfusion injury (32, 41, 42). Based onthese studies, we exposed wild-type C57BL/6J (Adora2b+/+) andAdora2b2/2 mice to ischemic kidney injury using a well-established hanging-weight model (36); following reperfusion,kidney function was assessed by measuring the GFR. As expected,Adora2b2/2 mice had more pronounced kidney injury, as measuredby an impaired GFR following renal ischemia (Fig. 1A). Next, wesought to define how Adora2b regulates inflammatory cytokineprofiles following renal ischemia, comparing Adora2b+/+ andAdora2b2/2 mice subjected to AKI. Ischemic kidney tissue wasthen screened for the relative abundance of a panel of cytokines. Inthis screen, we found that Adora2b2/2 mice had a pronounced in-crease in TNF-a protein, whereas other cytokines (IL-1, IL-2, IL-4,and IL-12) had less pronounced differences in expression betweenAdora2b+/+ and Adora2b2/2 mice (Fig. 1B). These data identifyelevated levels of TNF-a in Adora2b2/2 mice as one potentialpathogenic player contributing to the worse AKI in these mice.
2 Adora2b REGULATES NEUTROPHIL TNF IN RENAL ISCHEMIA
at Univ of C
algary Hlth Sci C
tr/Hlth Sci L
ib/Per on October 4, 2012
http://jimm
unol.org/D
ownloaded from

Adora2b-dependent regulation of TNF-a occurs followingprolonged periods of ischemia
To better understand the contribution of Adora2b-dependent in-hibition of TNF-a production, we defined the kinetics of TNF-aregulation by Adora2b. To do this, we exposed Adora2b+/+ andAdora2b2/2 mice to various periods of ischemia followed bymeasurement of TNF-a transcript levels. Animals exposed to aslittle as 10 or 30 min of ischemia had no difference in TNF-alevels between Adora2b+/+ and Adora2b2/2 mice (Fig. 2). Incontrast, with 40 min of renal ischemia, Adora2b2/2 mice hadincreased levels of TNF-a relative to their wild-type counterparts(Fig. 2). Given the temporal regulation of TNF-a following pro-longed ischemia, we focused our further studies on 40 min ofischemia, the time at which there is a maximal difference betweenAdora2b+/+ and Adora2b2/2 mice.
Ab blockade of TNF-a limits AKI following renal ischemia inAdora2b2/2 mice
Based on the worse AKI in Adora2b-deficient mice (31, 32)and identification of elevated TNF-a in Adora2b2/2 mice, wetested the outcome of blocking TNF-a during renal ischemia inAdora2b2/2 mice through treatment of animals with infliximab(Remicade; Janssen), a TNF-a–specific mAb therapy used for thetreatment of inflammatory diseases including rheumatoid arthri-tis and inflammatory bowel disease (43). In untreated animals,infliximab treatment had no effect on renal histology (Fig. 3A–C).Infliximab-treated Adora2b2/2 mice subjected to renal ischemiahad reduced renal injury relative to control-treated animals (Fig.3A–C). Mice treated with infliximab before renal ischemia hadreduced kidney injury as demonstrated by reduced acute tubularnecrosis, less destruction of the brush border, and attenuated hy-aline cast formation (Fig. 3B). Semiquantitative histological anal-ysis demonstrated a reduction in the Jablonski index with infliximabtreatment (Fig. 3C). These data identify that TNF-a elicited duringrenal ischemia in Adora2b2/2 mice contributes to the enhancedseverity of AKI in these animals.
Ab blockade of TNF-a limits AKI in wild-type mice followingrenal ischemia
The previous studies focused primarily on the role of TNF-a inthe enhanced tissue injury in Adora2b2/2 mice. To extend thesefindings to the context of wild-type C57BL/6J mice, we admin-istered the TNF-a–blocking Ab (infliximab) to either control miceor mice experiencing renal ischemia. Infliximab treatment did notalter baseline renal histology in control animals not subjected toischemia (Fig. 3D–F). However, when animals were subjected torenal ischemia, infliximab-treated animals had pronounced histo-logical protection from renal ischemia with less tubular acutenecrosis, reduced brush border injury, and attenuated cast forma-tion (Fig. 3D–F).
Genetic ablation of TNF-a limits AKI following renal ischemia
Based on the efficacy of Ab blocking against TNF-a in amelioratingAKI, we next tested the outcome of AKI in mice genetically defi-cient in TNF-a (Tnf2/2). When Tnf2/2 mice were subjected to40 min of ischemia, Tnf2/2 mice had reduced AKI, as measured by
FIGURE 1. Adora2b2/2 mice have a selective and profound induction
of TNF-a during AKI. (A) GFR following 40 min of renal ischemia and
1 h of reperfusion in wild-type (WT; black bars) and Adora2b2/2 (white
bars) mice (n = 4–6). (B) Measurement of TNF-a, IL-1, IL-2, IL-4, and IL-
12 protein levels after 40 min of renal ischemia and 2 h of reperfusion from
WT and Adora2b2/2 mice by ELISA (n = 3–4).2I, Animals not subjected
to renal ischemia; +I, animals subjected to renal ischemia. KW, Kidney
weight.
FIGURE 2. Adora2b-dependent regulation of TNF-a
occurs following prolonged periods of ischemic injury.
Measurement of TNF-a transcript levels in wild-type
(WT, black bars) and Adora2b2/2 (white bars) mice
after different ischemia times (0, 10, 30, and 40 min)
and 2 h of reperfusion (n = 2).
The Journal of Immunology 3
at Univ of C
algary Hlth Sci C
tr/Hlth Sci L
ib/Per on October 4, 2012
http://jimm
unol.org/D
ownloaded from

improved kidney function (characterized by a higher GFR) andimproved tissue integrity as analyzed by histology (Fig. 4). Thesegenetic data provide compelling evidence for a critical role for el-evated TNF-a as a primary driver of renal injury during ischemia/reperfusion injury in mice.
Mice with genetic overexpression of TNF-a have exacerbatedAKI following renal ischemia
Given the correlation among Adora2b deficiency, increased TNF-alevels, and worse AKI, we tested what consequence elevatedlevels of TNF-a in normal mice might have on AKI. To do this,we analyzed AKI in TNFDARE mice, a mouse model in which theARE that confers TNF-a mRNA instability has been geneticallyablated through homologous recombination (34). Notably, thesemice have elevated levels of TNF-a both in the resting state and
following an inflammatory insult (34). When TNFDARE micewere exposed to 40 min of ischemia, TNFDARE mice had sig-nificantly worse AKI than wild-type controls, measured by re-duced GFR (Fig. 5A), and worse tissue integrity by histology (Fig.5B, 5C). Based on these studies, mice with a genetic lesion thatresults in elevated TNF-a levels have worse AKI. These geneticdata demonstrate that appropriate control of TNF-a protein ex-pression levels are required to mitigate excessive tissue injuryduring ischemia/reperfusion and AKI in mice.
Neutrophils contribute to the increased AKI ofAdora2b-deficient mice
Given the important role of both TNF-a and neutrophils in ischemicinjury, we next sought to test the contribution of neutrophils to the
FIGURE 3. TNF-a contributes to AKI following renal ischemia in wild-
type (WT) and Adora2b2/2 mice. (A) GFR following 40 min of renal
ischemia and 1 h of reperfusion in Adora2b2/2 untreated (black bar) or
treated with the anti-TNF Ab infliximab (white bars, 10 mg/kg body
weight i.p. 60 min prior renal ischemia; n = 4–6). (B) Renal histology
(H&E staining) following 40 min of renal ischemia and 24 h of reperfusion
(original magnification 3400; one of three to five representative slides is
shown) in Adora2b2/2 animals untreated (black bar) or treated with the
anti-TNF Ab infliximab (white bars). (C) Quantification of renal tissue
injury using the Jablonski index (n = 3–5). (D) GFR following 40 min of
renal ischemia and 1 h of reperfusion in WT mice untreated (black bar)
or treated with the anti-TNF Ab infliximab (white bars, 10 mg/kg body
weight i.p. 60 min prior renal ischemia; n = 4–6). (E) Renal histology
(H&E staining) following 40 min of renal ischemia and 24 h of reperfusion
in WT mice without (black bars) or with (white bars) infliximab treatment
(original magnification 3400; one of three to five representative slides is
shown). (F) Quantification of renal tissue injury in WT mice without (black
bars) or with (white bars) infliximab treatment by using the Jablonski index
(n = 3–5). 2I, Animals not subjected to renal ischemia; +I, animals sub-
jected to renal ischemia. KW, Kidney weight.
FIGURE 4. Genetic ablation of TNF-a limits AKI following renal is-
chemia. (A) GFR following 40 min of renal ischemia and 1 h of reper-
fusion in wild-type (WT; black bars) and Tnf-a2/2 gene-targeted mice
(white bars) (n = 4–6). (B) Renal histology (H&E staining) following 40
min of renal ischemia and 24 h of reperfusion (original magnification
3400; one of three to five representative slides is shown). (C) Quantifi-
cation of renal tissue injury using the Jablonski index (n = 3–5). 2I,
Animals not subjected to renal ischemia; +I, animals subjected to renal
ischemia. KW, Kidney weight.
FIGURE 5. Mice with genetic overexpression of TNF-a have exacer-
bated AKI following renal ischemia. (A) GFR following 40 min of renal
ischemia and 1 h of reperfusion in wild-type (WT; black bars) and
TNFDARE (white bars) gene-targeted mice (n = 4–6). (B) Renal histology
(H&E staining) following 40 min of renal ischemia and 24 h of reperfusion
(original magnification 3400; one of three to five representative slides is
shown). (C) Quantification of renal tissue injury using the Jablonski index
(n = 3–5). 2I, Animals not subjected to renal ischemia; +I, animals sub-
jected to renal ischemia. KW, Kidney weight.
4 Adora2b REGULATES NEUTROPHIL TNF IN RENAL ISCHEMIA
at Univ of C
algary Hlth Sci C
tr/Hlth Sci L
ib/Per on October 4, 2012
http://jimm
unol.org/D
ownloaded from

worse AKI in Adora2b2/2 mice. To do this, Adora2b2/2 mice weresubjected to Ab-mediated depletion of neutrophils, followingtreatment with an anti-Gr1 Ab (39). Following deletion of neu-trophils, Adora2b2/2 mice were subjected to renal ischemia. Inthese studies, we found that neutropenic mice had improved renalfunction (measured by increased GFR relative to controls, Fig. 6A)and reduced histological damage (Fig. 6B, 6C). Further, when weanalyzed TNF-a levels in animals depleted of neutrophils, we foundthat neutrophil depletion resulted in a profound decrease in theamount of TNF-a detected during AKI (Fig. 6D). These data in-dicate that neutrophils contribute to the exacerbated AKI followingrenal ischemia in Adora2b2/2 mice. Moreover, these data identifyneutrophils as a major source of TNF-a during AKI followingprolonged renal ischemia.To investigate the role of neutrophil-derived TNF-a as a factor
contributing to Adora2b2/2 AKI, we next performed adoptivetransfer studies of magnetically enriched neutrophils from eitherAdora2b2/2 or Tnf2/2 mice into Adora2b2/2 recipients previ-ously depleted of neutrophils. Notably, whereas adoptive transferof neutrophils from Adora2b2/2 mice into Adora2b2/2 mice hadimpaired renal function (as measured by GFR, Fig. 6E), adoptive
transfer of neutrophils from Tnf2/2 mice was associated withattenuated AKI and a relatively improved GFR (Fig. 6E). Basedon these data, neutrophil-derived TNF-a is an important contrib-utor to AKI in Adora2b2/2 mice. In total, these studies demon-strate a central role for TNF-a as a molecular mediator of tissueinjury during renal ischemia in both wild-type and Adora2b2/2
mice.
DiscussionThe pathogenesis of AKI following renal ischemia is a complexprocess, involving the impaired function and apoptosis of tissue-resident epithelial and endothelial cells, coupled with a resultinginflammatory cascade that recruits multiple leukocyte subsets to thepostischemic kidney (10). The outcome of renal ischemia is tightlyregulated by the relative balance of pathogenic versus protectivemechanisms (10). One potent protective mechanism elicited duringischemia is extracellular adenosine generation (generated by thestepwise degradation of extracellular ATP through the extracellularenzymes CD39 and CD73) and signaling through adenosine re-ceptors (24–26). Notably, evidence for the potent anti-inflammatoryproperties mediated by adenosine receptor signaling came frompioneering studies by Sitkovsky’s group (13, 44), in which Adora2asignaling was identified as a primary anti-inflammatory pathwaythat constrains tissue injury during inflammation and ischemiain multiple organ systems. Although the adenosine receptor canbe a potent, tissue-protective pathway, it is important to note thatexcess extracellular adenosine signaling, whether in the contextof adenosine deaminase deficiency or in states of repeated ische-mic events (e.g., sickle cell), can induce profound pathologies(45–47).In the context of AKI following renal ischemia, the adenosine
receptors Adora1 (A1), Adora2a (A2a), and Adora2b (A2b) haveeach been demonstrated to play protective roles to limit AKI (27,28, 31). In contrast, Adora3 (A3) has a detrimental role in thiscontext, such that Adora3-deficient mice are protected againstrenal ischemia-induced AKI (48). Although multiple adenosinereceptors participate in protection of the kidney against ischemia,it is notable that different adenosine receptors are thought to elicitdistinct mechanisms of protection, ranging from primary modu-lation of parenchymal cells within the kidney (via Adora1 sig-naling) (26) to inhibition of the recruitment and activation ofmultiple bone marrow-derived cell types including neutrophils,NK T cells, and T cells (via Adora2a signaling) (11, 49, 50). Inthis context, it is worth noting that Adora2a signaling has previ-ously been demonstrated to regulate TNF-a production fromisolated human neutrophils in vitro and in murine neutrophils in anair pouch model of inflammation (49). Adora2a can also influencethe extent of adenosine receptor signaling beyond its own signalingcapacity. In particular, careful studies by Sitkovsky’s laboratory (51)have demonstrated that optimal cell-surface expression of Adora2brelies on coexpression with Adora2a, revealing an unanticipatedinterconnectedness between these two receptors. Whether theAdora2b-dependent regulation observed in this current study isinfluenced by integration with Adora2a-dependent signaling dur-ing AKI remains to be determined. In the context of AKI fol-lowing ischemia/reperfusion, Adora2a constrains tissue damageboth by limiting neutrophil transmigration and inhibiting T cells(29, 52).Although Adora2a is thought to primarily target leukocytes in its
anti-inflammatory actions, Adora2b signaling appears to be moremultifactorial, with examples of Adora2b inhibition in both pa-renchymal and leukocyte subsets. Adora2b is expressed bymultiplecell types and tissues, including expression in the vasculature and inleukocyte subsets such as macrophages (31, 53). To date, studies
FIGURE 6. Neutrophils contribute to the increased AKI of Adora2b2/2
mice. (A) GFR following 40 min of renal ischemia and 1 h of reperfusion
in Adora2b2/2 mice without (black bars) or with neutrophil depletion via
anti-Gr1 Ab treatment (white bars) 24 h prior to renal ischemia (n = 3–5).
(B) Renal histology (H&E staining) following 40 min of renal ischemia
and 24 h of reperfusion (original magnification 3400; one of three to five
representative slides is shown). (C) Quantification of renal tissue injury
using the Jablonski index (n = 3–5). (D) TNF-a protein levels following 40
min of renal ischemia and 2 h of reperfusion by ELISA. (E) Neutrophils
were isolated from either Adora2b2/2 mice (black bars) or Tnf-a2/2 mice
(white bars) and injected into Adora2b2/2 mice that had been previously
depleted of neutrophils by anti-Gr1 Ab treatment. GFR was performed
following 40 min of renal ischemia and 1 h of reperfusion in the recipient
Adora2b2/2 mice. KW, Kidney weight; n.s., no statistically significant
difference.
The Journal of Immunology 5
at Univ of C
algary Hlth Sci C
tr/Hlth Sci L
ib/Per on October 4, 2012
http://jimm
unol.org/D
ownloaded from

analyzing the protective effects of Adora2b in limiting AKI havefocused primarily on a renovascular function for Adora2b inlimiting AKI (31, 32); this focus was based largely on bonemarrow chimera studies that demonstrated Adora2b can mediateprotective effects when it is expressed on nonhematopoietic cells(31). Notably, however, there is clear evidence that Adora2b sig-naling can regulate diverse components of the inflammatory re-sponse, including neutrophils, macrophages, dendritic cells, andeven lymphocytes (53–57). In this manuscript, we have focused oneffector mechanisms regulated by Adora2b within the hemato-poietic system, with a focus on the role of Adora2b following alonger ischemic insult (40 min relative to previous studies using30 min of ischemia). In these studies, we found that Adora2b hasa pronounced effect, limiting the production of TNF-a followingrenal ischemia, and that neutrophil-derived TNF-a contributes toAKI in Adora2b2/2 mice. These data are consistent with reportsidentifying that Adora2b limits TNF-a production from macro-phages (53–55), as well as a recent report demonstrating Adora2bcan restrict TNF-a production from neutrophils in the context ofmyocardial ischemia (58).Though our studies have focused on the protective role of
adenosine receptor signaling in AKI following renal ischemia, it isimportant to note that the etiology of AKI can profoundly influencethe contribution of adenosine receptor signaling in either protectingagainst or exacerbating AKI. For example, studies by Lee et al. (27)have clearly shown that the Adora1 adenosine receptor has di-vergent effects in AKI with different modes of renal injury. Inthe context of renal ischemia, Adora1 has a protective role, andAdora1-deficient mice have worse AKI following renal ischemia(27). Conversely, in the context of nephrotoxic and radiocontrastagent-induced AKI, Adora1 has a detrimental role such thatAdora1-deficient mice are protected against this form of AKI (59).These data exemplify the complex interplay between AKI etiologyand adenosine receptor signaling to ultimately influence kidneyfunction.Our data in this study, and elsewhere, demonstrate a protective
role for Adora2b in limiting acute, ischemic tissue injury (23, 31,58). In these contexts, the hypoxia-inducible nature of Adora2bplaces it as a central mediator affording tissue-protective effectsduring ischemia (31). However, it is important to note that in othercontexts, Adora2b signaling has been associated with proin-flammatory roles, such as the induction of IL-6 in dendritic cells(60). Moreover, depending on the duration and context of Adora2bsignaling, this receptor can be a primary driver of pathobiology.Notably, rigorous studies from the laboratories of Xia and Blackburn(47, 61, 62) have clearly demonstrated that Adora2b is respon-sible for pathogenic outcomes in priaprism, sickle cell disease,and bleomycin-induced lung fibrosis.The outcome of AKI is regulated at multiple stages, from
mechanisms that function rapidly (within minutes to hours of in-jury) to the later involvement of components of the adaptive im-mune response including T cells that can contribute to tissue injuryand repair days after the initial insult (10). In this larger context,it is important to note that Adora2b induces multiple protectiveeffects during ischemic injury. For example, by analyzing the roleof Adora2b within the renal vasculature, we recently showed thatAdora2b promotes optimal postischemic blood flow within thekidney, thereby ensuring maximal return of blood flow, tissueoxygenation, and the removal of waste products from the ischemickidney (32). This mechanism functions through cross talk ofAdora2b with ENT1, the equilibrative nucleoside transporter, atransporter protein that controls the extent and timing of extra-cellular adenosine. Based on the data presented in this study,demonstrating that Adora2b-regulated TNF-a directly impacts
AKI, it is worth noting that TNF-a can have profound effects onthe vasculature, raising the possibility that the mechanism iden-tified in this study may integrate with the Adora2b–ENT1 pathwayto regulate postischemic blood flow to the kidney (32). AlthoughAdora2b signaling can mediate protective effects during renalischemia [using either nephrectomy and unilateral ischemia orsimultaneous, bilateral renal ischemia (32)], it remains to be seenwhat contribution Adora2b has in the context of AKI followingnephrotoxin exposure [e.g., cisplatin (63)] or following sepsis[a context in which Adora2b deficiency is beneficial in limitingbacterial colonization (55)]. This is an important question forfuture investigation because different forms of AKI are char-acterized by distinct kinetics and effector mechanisms (e.g.,ischemia/reperfusion, nephrotoxin, or sepsis) (2, 10, 63). A notablecontrast between our model and that of cisplatin-induced AKIis that parenchymal cells are the prominent source of TNF-a(64, 65), in contrast to our renal ischemia model in which neu-trophils are a prominent source of TNF-a. Because Adora2b canmediate protective effects on both parenchymal and bone marrow-derived cell types, it is possible that the contribution of Adora2bsignaling in AKI will vary depending on the etiology of AKI understudy.Beyond the kidney, Adora2b has been shown to mediate ad-
ditional tissue-protective effects in models of acute inflammation.For example, Adora2b signaling can elicit cardioprotective effectsthrough the circadian rhythm protein Period2, which in turn pro-motes metabolic adaptation in the ischemic heart (41). In acutecolitis and following hypoxia, Adora2b also functions as an es-sential receptor for the anti-inflammatory properties of netrin-1,a neuronal guidance molecule (66). Adora2b signaling can alsoregulate the superoxide burst in neutrophils (67), which wouldlimit neutrophil-derived production of potentially toxic reactiveoxygen species. Finally, Adora2b has been shown to limit theinflammatory properties of macrophages and T cells (53, 55, 57).Given that these cell types can influence regulate AKI (52, 68, 69),Adora2b-mediated protection in AKI may arise by altering thefunction of multiple leukocyte subsets.The multiple etiologies of AKI, combined with the paucity
of therapeutic interventions, continue to be a significant unmetmedical challenge. Given the weight of evidence that extracellularadenosine generation and signaling are tissue-protective duringAKI, this pathway is of significant therapeutic interest. To opti-mally harness the potential of Adora2b in limiting AKI, it will beimportant for future studies to define how the multiple protectivemechanisms of Adora2b integrate to induce maximal protectionduring AKI. In addition, it will be equally important to determinehow to therapeutically activate the beneficial effects of Adora2bsignaling without triggering deleterious consequences of prolongedAdora2b signaling (47, 70).
AcknowledgmentsWe thank Dr. Jesus Rivera-Nieves for kindly providing the TNFDARE
mice and members of the Eltzschig laboratory for critical discussion.
DisclosuresThe authors have no financial conflicts of interest.
References1. Mehta, R. L., J. A. Kellum, S. V. Shah, B. A. Molitoris, C. Ronco,
D. G. Warnock, and A. Levin; Acute Kidney Injury Network. 2007. AcuteKidney Injury Network: report of an initiative to improve outcomes in acutekidney injury. Crit. Care 11: R31.
2. Schrier, R. W., and W. Wang. 2004. Acute renal failure and sepsis. N. Engl.J. Med. 351: 159–169.
6 Adora2b REGULATES NEUTROPHIL TNF IN RENAL ISCHEMIA
at Univ of C
algary Hlth Sci C
tr/Hlth Sci L
ib/Per on October 4, 2012
http://jimm
unol.org/D
ownloaded from

3. Abuelo, J. G. 2007. Normotensive ischemic acute renal failure. N. Engl. J. Med.357: 797–805.
4. Gelman, S. 1995. The pathophysiology of aortic cross-clamping and unclamp-ing. Anesthesiology 82: 1026–1060.
5. Mehta, R. L. 2005. Acute renal failure and cardiac surgery: marching in place ormoving ahead? J. Am. Soc. Nephrol. 16: 12–14.
6. Ishani, A., J. L. Xue, J. Himmelfarb, P. W. Eggers, P. L. Kimmel, B. A. Molitoris,and A. J. Collins. 2009. Acute kidney injury increases risk of ESRD amongelderly. J. Am. Soc. Nephrol. 20: 223–228.
7. Coca, S. G., S. Singanamala, and C. R. Parikh. 2012. Chronic kidney diseaseafter acute kidney injury: a systematic review and meta-analysis. Kidney Int. 81:442–448.
8. Bove, T., G. Landoni, M. G. Calabro, G. Aletti, G. Marino, E. Cerchierini,G. Crescenzi, and A. Zangrillo. 2005. Renoprotective action of fenoldopam inhigh-risk patients undergoing cardiac surgery: a prospective, double-blind, ran-domized clinical trial. Circulation 111: 3230–3235.
9. Kumar, A. B., and M. Suneja. 2011. Cardiopulmonary bypass-associated acutekidney injury. Anesthesiology 114: 964–970.
10. Bonventre, J. V., and L. Yang. 2011. Cellular pathophysiology of ischemic acutekidney injury. J. Clin. Invest. 121: 4210–4221.
11. Sitkovsky, M. V., D. Lukashev, S. Apasov, H. Kojima, M. Koshiba, C. Caldwell,A. Ohta, and M. Thiel. 2004. Physiological control of immune response andinflammatory tissue damage by hypoxia-inducible factors and adenosine A2Areceptors. Annu. Rev. Immunol. 22: 657–682.
12. Gladwin, M. T. 2011. Adenosine receptor crossroads in sickle cell disease. Nat.Med. 17: 38–40.
13. Ohta, A., and M. Sitkovsky. 2001. Role of G-protein-coupled adenosine recep-tors in downregulation of inflammation and protection from tissue damage.Nature 414: 916–920.
14. Zeiser, R., O. Penack, E. Holler, and M. Idzko. 2011. Danger signals activatinginnate immunity in graft-versus-host disease. J. Mol. Med. 89: 833–845.
15. Eltzschig, H. K., and P. Carmeliet. 2011. Hypoxia and inflammation. N. Engl.J. Med. 364: 656–665.
16. Fredholm, B. B., A. P. IJzerman, K. A. Jacobson, J. Linden, and C. E. Muller.2011. International Union of Basic and Clinical Pharmacology. LXXXI. No-menclature and classification of adenosine receptors—an update. Pharmacol.Rev. 63: 1–34.
17. Fredholm, B. B. 2007. Adenosine, an endogenous distress signal, modulatestissue damage and repair. Cell Death Differ. 14: 1315–1323.
18. Hasko, G., J. Linden, B. Cronstein, and P. Pacher. 2008. Adenosine receptors:therapeutic aspects for inflammatory and immune diseases. Nat. Rev. DrugDiscov. 7: 759–770.
19. Eckle, T., D. Kohler, R. Lehmann, K. C. El Kasmi, and H. K. Eltzschig. 2008.Hypoxia-inducible factor-1 is central to cardioprotection: a new paradigm forischemic preconditioning. Circulation 118: 166–175.
20. Kohler, D., T. Eckle, M. Faigle, A. Grenz, M. Mittelbronn, S. Laucher,M. L. Hart, S. C. Robson, C. E. Muller, and H. K. Eltzschig. 2007. CD39/ectonucleoside triphosphate diphosphohydrolase 1 provides myocardial protec-tion during cardiac ischemia/reperfusion injury. Circulation 116: 1784–1794.
21. Hart, M. L., C. Much, I. C. Gorzolla, J. Schittenhelm, D. Kloor, G. L. Stahl, andH. K. Eltzschig. 2008. Extracellular adenosine production by ecto-5’-nucleo-tidase protects during murine hepatic ischemic preconditioning. Gastroenterol-ogy 135: 1739–1750.e3.
22. Hart, M. L., M. Henn, D. Kohler, D. Kloor, M. Mittelbronn, I. C. Gorzolla,G. L. Stahl, and H. K. Eltzschig. 2008. Role of extracellular nucleotide phos-phohydrolysis in intestinal ischemia-reperfusion injury. FASEB J. 22: 2784–2797.
23. Hart, M. L., B. Jacobi, J. Schittenhelm, M. Henn, and H. K. Eltzschig. 2009.Cutting Edge: A2B Adenosine receptor signaling provides potent protectionduring intestinal ischemia/reperfusion injury. J. Immunol. 182: 3965–3968.
24. Grenz, A., H. Zhang, T. Eckle, M. Mittelbronn, M. Wehrmann, C. Kohle,D. Kloor, L. F. Thompson, H. Osswald, and H. K. Eltzschig. 2007. Protectiverole of ecto-59-nucleotidase (CD73) in renal ischemia. J. Am. Soc. Nephrol. 18:833–845.
25. Grenz, A., H. Zhang, M. Hermes, T. Eckle, K. Klingel, D. Y. Huang,C. E. Muller, S. C. Robson, H. Osswald, and H. K. Eltzschig. 2007. Contributionof E-NTPDase1 (CD39) to renal protection from ischemia-reperfusion injury.FASEB J. 21: 2863–2873.
26. Yap, S. C., and H. T. Lee. 2012. Adenosine and protection from acute kidneyinjury. Curr. Opin. Nephrol. Hypertens. 21: 24–32.
27. Lee, H. T., H. Xu, S. H. Nasr, J. Schnermann, and C. W. Emala. 2004. A1adenosine receptor knockout mice exhibit increased renal injury following is-chemia and reperfusion. Am. J. Physiol. Renal Physiol. 286: F298–F306.
28. Day, Y. J., L. Huang, M. J. McDuffie, D. L. Rosin, H. Ye, J. F. Chen,M. A. Schwarzschild, J. S. Fink, J. Linden, and M. D. Okusa. 2003. Renalprotection from ischemia mediated by A2A adenosine receptors on bonemarrow-derived cells. J. Clin. Invest. 112: 883–891.
29. Awad, A. S., M. Rouse, L. Huang, A. L. Vergis, J. Reutershan, H. P. Cathro,J. Linden, and M. D. Okusa. 2009. Compartmentalization of neutrophils in thekidney and lung following acute ischemic kidney injury. Kidney Int. 75: 689–698.
30. Bauerle, J. D., A. Grenz, J. H. Kim, H. T. Lee, and H. K. Eltzschig. 2011.Adenosine generation and signaling during acute kidney injury. J. Am. Soc.Nephrol. 22: 14–20.
31. Grenz, A., H. Osswald, T. Eckle, D. Yang, H. Zhang, Z. V. Tran, K. Klingel,K. Ravid, and H. K. Eltzschig. 2008. The reno-vascular A2B adenosine receptorprotects the kidney from ischemia. PLoS Med. 5: e137.
32. Grenz, A., J. D. Bauerle, J. H. Dalton, D. Ridyard, A. Badulak, E. Tak,E. N. McNamee, E. Clambey, R. Moldovan, G. Reyes, et al. 2012. Equilibrativenucleoside transporter 1 (ENT1) regulates postischemic blood flow during acutekidney injury in mice. J. Clin. Invest. 122: 693–710.
33. Pasparakis, M., L. Alexopoulou, V. Episkopou, and G. Kollias. 1996. Immuneand inflammatory responses in TNF alpha-deficient mice: a critical requirementfor TNF alpha in the formation of primary B cell follicles, follicular dendriticcell networks and germinal centers, and in the maturation of the humoral im-mune response. J. Exp. Med. 184: 1397–1411.
34. Kontoyiannis, D., M. Pasparakis, T. T. Pizarro, F. Cominelli, and G. Kollias.1999. Impaired on/off regulation of TNF biosynthesis in mice lacking TNF AU-rich elements: implications for joint and gut-associated immunopathologies.Immunity 10: 387–398.
35. Ho, J., C. C. Kurtz, M. Naganuma, P. B. Ernst, F. Cominelli, and J. Rivera-Nieves. 2008. A CD8+/CD103high T cell subset regulates TNF-mediatedchronic murine ileitis. J. Immunol. 180: 2573–2580.
36. Grenz, A., T. Eckle, H. Zhang, D. Y. Huang, M. Wehrmann, C. Kohle, K. Unertl,H. Osswald, and H. K. Eltzschig. 2007. Use of a hanging-weight system forisolated renal artery occlusion during ischemic preconditioning in mice. Am. J.Physiol. Renal Physiol. 292: F475–F485.
37. Lorenz, J. N., and E. Gruenstein. 1999. A simple, nonradioactive method forevaluating single-nephron filtration rate using FITC-inulin. Am. J. Physiol. 276:F172–F177.
38. Conger, J. D., S. A. Falk, B. H. Yuan, and R. W. Schrier. 1989. Atrial natriureticpeptide and dopamine in a rat model of ischemic acute renal failure. Kidney Int.35: 1126–1132.
39. Rogers, H. W., and E. R. Unanue. 1993. Neutrophils are involved in acute,nonspecific resistance to Listeria monocytogenes in mice. Infect. Immun. 61:5090–5096.
40. Jablonski, P., B. O. Howden, D. A. Rae, C. S. Birrell, V. C. Marshall, andJ. Tange. 1983. An experimental model for assessment of renal recovery fromwarm ischemia. Transplantation 35: 198–204.
41. Eckle, T., K. Hartmann, S. Bonney, S. Reithel, M. Mittelbronn, L. A. Walker,B. D. Lowes, J. Han, C. H. Borchers, P. M. Buttrick, et al. 2012. Adora2b-elicited Per2 stabilization promotes a HIF-dependent metabolic switch crucialfor myocardial adaptation to ischemia. Nat. Med. 18: 774–782.
42. Eltzschig, H. K., and T. Eckle. 2011. Ischemia and reperfusion—from mecha-nism to translation. Nat. Med. 17: 1391–1401.
43. Siddiqui, M. A., and L. J. Scott. 2005. Infliximab: a review of its use in Crohn’sdisease and rheumatoid arthritis. Drugs 65: 2179–2208.
44. Ohta, A., D. Lukashev, E. K. Jackson, B. B. Fredholm, and M. Sitkovsky. 2007.1,3,7-trimethylxanthine (caffeine) may exacerbate acute inflammatory liver in-jury by weakening the physiological immunosuppressive mechanism. J. Immu-nol. 179: 7431–7438.
45. Wakamiya, M., M. R. Blackburn, R. Jurecic, M. J. McArthur, R. S. Geske,J. Cartwright, Jr., K. Mitani, S. Vaishnav, J. W. Belmont, R. E. Kellems, et al.1995. Disruption of the adenosine deaminase gene causes hepatocellular im-pairment and perinatal lethality in mice. Proc. Natl. Acad. Sci. USA 92: 3673–3677.
46. Blackburn, M. R., J. B. Volmer, J. L. Thrasher, H. Zhong, J. R. Crosby, J. J. Lee,and R. E. Kellems. 2000. Metabolic consequences of adenosine deaminase de-ficiency in mice are associated with defects in alveogenesis, pulmonary in-flammation, and airway obstruction. J. Exp. Med. 192: 159–170.
47. Zhang, Y., Y. Dai, J. Wen, W. Zhang, A. Grenz, H. Sun, L. Tao, G. Lu,D. C. Alexander, M. V. Milburn, et al. 2011. Detrimental effects of adenosinesignaling in sickle cell disease. Nat. Med. 17: 79–86.
48. Lee, H. T., A. Ota-Setlik, H. Xu, V. D. D’Agati, M. A. Jacobson, andC. W. Emala. 2003. A3 adenosine receptor knockout mice are protected againstischemia- and myoglobinuria-induced renal failure. Am. J. Physiol. RenalPhysiol. 284: F267–F273.
49. McColl, S. R., M. St-Onge, A. A. Dussault, C. Laflamme, L. Bouchard,J. Boulanger, and M. Pouliot. 2006. Immunomodulatory impact of the A2Aadenosine receptor on the profile of chemokines produced by neutrophils. FASEBJ. 20: 187–189.
50. Lappas, C. M., Y. J. Day, M. A. Marshall, V. H. Engelhard, and J. Linden. 2006.Adenosine A2A receptor activation reduces hepatic ischemia reperfusion injuryby inhibiting CD1d-dependent NKT cell activation. J. Exp. Med. 203: 2639–2648.
51. Moriyama, K., and M. V. Sitkovsky. 2010. Adenosine A2A receptor is involvedin cell surface expression of A2B receptor. J. Biol. Chem. 285: 39271–39288.
52. Day, Y. J., L. Huang, H. Ye, L. Li, J. Linden, and M. D. Okusa. 2006. Renalischemia-reperfusion injury and adenosine 2A receptor-mediated tissue protec-tion: the role of CD4+ T cells and IFN-gamma. J. Immunol. 176: 3108–3114.
53. Yang, D., Y. Zhang, H. G. Nguyen, M. Koupenova, A. K. Chauhan, M. Makitalo,M. R. Jones, C. St Hilaire, D. C. Seldin, P. Toselli, et al. 2006. The A2Badenosine receptor protects against inflammation and excessive vascular adhe-sion. J. Clin. Invest. 116: 1913–1923.
54. Chen, H., D. Yang, S. H. Carroll, H. K. Eltzschig, and K. Ravid. 2009. Activationof the macrophage A2b adenosine receptor regulates tumor necrosis factor-alphalevels following vascular injury. Exp. Hematol. 37: 533–538.
55. Belikoff, B. G., S. Hatfield, P. Georgiev, A. Ohta, D. Lukashev, J. A. Buras,D. G. Remick, and M. Sitkovsky. 2011. A2B adenosine receptor blockade en-hances macrophage-mediated bacterial phagocytosis and improves poly-microbial sepsis survival in mice. J. Immunol. 186: 2444–2453.
56. Wilson, J. M., W. G. Ross, O. N. Agbai, R. Frazier, R. A. Figler, J. Rieger,J. Linden, and P. B. Ernst. 2009. The A2B adenosine receptor impairs thematuration and immunogenicity of dendritic cells. J. Immunol. 182: 4616–4623.
The Journal of Immunology 7
at Univ of C
algary Hlth Sci C
tr/Hlth Sci L
ib/Per on October 4, 2012
http://jimm
unol.org/D
ownloaded from

57. Ehrentraut, H., J. A. Westrich, H. K. Eltzschig, and E. T. Clambey. 2012.Adora2b adenosine receptor engagement enhances regulatory T cell abundanceduring endotoxin-induced pulmonary inflammation. PLoS ONE 7: e32416.
58. Koeppen, M., P. N. Harter, S. Bonney, M. Bonney, S. Reithel, C. Zachskorn,M. Mittelbronn, and T. Eckle. 2012. Adora2b signaling on bone marrow derivedcells dampens myocardial ischemia-reperfusion injury. Anesthesiology 116:1245–1257.
59. Lee, H. T., M. Jan, S. C. Bae, J. D. Joo, F. R. Goubaeva, J. Yang, and M. Kim.2006. A1 adenosine receptor knockout mice are protected against acuteradiocontrast nephropathy in vivo. Am. J. Physiol. Renal Physiol. 290: F1367–F1375.
60. Wilson, J. M., C. C. Kurtz, S. G. Black, W. G. Ross, M. S. Alam, J. Linden, andP. B. Ernst. 2011. The A2B adenosine receptor promotes Th17 differentiation viastimulation of dendritic cell IL-6. J. Immunol. 186: 6746–6752.
61. Mi, T., S. Abbasi, H. Zhang, K. Uray, J. L. Chunn, L. W. Xia, J. G. Molina,N. W. Weisbrodt, R. E. Kellems, M. R. Blackburn, and Y. Xia. 2008. Excessadenosine in murine penile erectile tissues contributes to priapism via A2Badenosine receptor signaling. J. Clin. Invest. 118: 1491–1501.
62. Wen, J., X. Jiang, Y. Dai, Y. Zhang, Y. Tang, H. Sun, T. Mi, P. V. Phatarpekar,R. E. Kellems, M. R. Blackburn, and Y. Xia. 2010. Increased adenosine con-tributes to penile fibrosis, a dangerous feature of priapism, via A2B adenosinereceptor signaling. FASEB J. 24: 740–749.
63. Miller, R. P., R. K. Tadagavadi, G. Ramesh, and W. B. Reeves. 2010. Mecha-nisms of Cisplatin nephrotoxicity. Toxins (Basel) 2: 2490–2518.
64. Ramesh, G., and W. B. Reeves. 2002. TNF-alpha mediates chemokine and cy-tokine expression and renal injury in cisplatin nephrotoxicity. J. Clin. Invest.110: 835–842.
65. Zhang, B., G. Ramesh, C. C. Norbury, and W. B. Reeves. 2007. Cisplatin-induced nephrotoxicity is mediated by tumor necrosis factor-alpha producedby renal parenchymal cells. Kidney Int. 72: 37–44.
66. Aherne, C. M., C. B. Collins, J. C. Masterson, M. Tizzano, T. A. Boyle,J. A. Westrich, J. A. Parnes, G. T. Furuta, J. Rivera-Nieves, and H. K. Eltzschig.2012. Neuronal guidance molecule netrin-1 attenuates inflammatory cell traf-ficking during acute experimental colitis. Gut 61: 695–705.
67. van der Hoeven, D., T. C. Wan, E. T. Gizewski, L. M. Kreckler, J. E. Maas,J. Van Orman, K. Ravid, and J. A. Auchampach. 2011. A role for the low-affinityA2B adenosine receptor in regulating superoxide generation by murine neu-trophils. J. Pharmacol. Exp. Ther. 338: 1004–1012.
68. Day, Y. J., L. Huang, H. Ye, J. Linden, and M. D. Okusa. 2005. Renal ischemia-reperfusion injury and adenosine 2A receptor-mediated tissue protection: role ofmacrophages. Am. J. Physiol. Renal Physiol. 288: F722–F731.
69. Gandolfo, M. T., H. R. Jang, S. M. Bagnasco, G. J. Ko, P. Agreda, S. R. Satpute,M. T. Crow, L. S. King, and H. Rabb. 2009. Foxp3+ regulatory T cells participatein repair of ischemic acute kidney injury. Kidney Int. 76: 717–729.
70. Zhou, Y., D. J. Schneider, E. Morschl, L. Song, M. Pedroza, H. Karmouty-Quintana, T. Le, C. X. Sun, and M. R. Blackburn. 2011. Distinct roles for theA2B adenosine receptor in acute and chronic stages of bleomycin-induced lunginjury. J. Immunol. 186: 1097–1106.
8 Adora2b REGULATES NEUTROPHIL TNF IN RENAL ISCHEMIA
at Univ of C
algary Hlth Sci C
tr/Hlth Sci L
ib/Per on October 4, 2012
http://jimm
unol.org/D
ownloaded from