A Guide for Dental Practices - BMJ Quality & Safety€¦ · · 2012-07-27Standard 3: Preventing...
83
National Safety and Quality Health Service Standards A Guide for Dental Practices Part B Consultation Draft July 2012
Transcript of A Guide for Dental Practices - BMJ Quality & Safety€¦ · · 2012-07-27Standard 3: Preventing...
National Safety and Quality Health Service Standards
A Guide for Dental PracticesPart B
Consultation DraftJuly 2012
Australian Commission on Safety and Quality in Health Care
Table of Contents: A Guide for Dental Practices-Part B Introduction ................................................................................................................. 2
Standard 1: Governance for Safety and Quality in Health Service Organisations ...... 3
Standard 2: Partnering with Consumers ................................................................... 23
Standard 3: Preventing and Controlling Healthcare Associated Infections............... 31
Standard 4: Medication Safety .................................................................................. 53
Standard 5: Patient Identification and Procedure Matching ...................................... 70
Standard 6: Clinical Handover .................................................................................. 76
Consultation Draft Ι A Guide for Dental Practices Ι Part B
Australian Commission on Safety and Quality in Health Care
Introduction Part B of the Guide for Dental Practices contains information specific to each Standard and includes:
• A description of the Standard
• A statement of intent or the desired outcome for the Standard
• The context in which the Standard must be applied
• Key criteria of the Standard
• A series of actions relevant to each criterion
• Reflective questions to clarify the intent of each criterion
• Examples of evidence
• A column to assist health services identify if further action is required.
The purpose of the evidence list is to assist a dental practice determine how it can show safety and quality processes and systems are in place, that they are reviewed, evaluated and practices are changed when necessary.
Each dental practice should interpret the evidence listed with respect to its own model of service delivery and care.
If a dental practice finds there is insufficient evidence available to demonstrate an action has been met, the ‘No’ box in the last column of the tables in the Guide is there to prompt further action that may be required to address identified gaps.
Dental practices are not expected to have every form of evidence provided as examples. You are strongly encouraged to only use enough evidence to show actions are being addressed. The evidence used would typically come from the usual improvement and business processes of the practice rather than created specifically for accreditation.
Part B should be read in conjunction with Part A of the Guide for Dental Practices. Part A contains information about the accreditation process and resources to assist dental practices prepare for accreditation.
Consultation Draft Ι A Guide for Dental Practices Ι Part B 2
Australian Commission on Safety and Quality in Health Care Standard 1: Governance for Safety and Quality in Health Service Organisations
Standard 1: Governance for Safety and Quality in Health Service Organisations Health service organisation leaders implement governance systems to set, monitor and improve the performance of the organisation and communicate the importance of the patient experience and quality management to all members of the workforce. Clinicians and other members of the workforce use the governance systems.
The intention of this Standard is to:
Create integrated governance systems that maintain and improve the reliability and quality of patient care, as well as improve patient outcomes.
Context
This Standard provides the safety and quality governance framework for health service organisations. It is expected that this Standard will apply to the implementation of all other Standards in conjunction with Standard 2, ‘Partnering with Consumers’.
Criteria to achieve the Governance for Safety and Quality in Health Service Organisations Standard:
• Governance and quality improvement systems
• Clinical practice
• Performance and skills management
• Incident and complaints management
• Patient rights and engagement
Consultation Draft Ι A Guide for Dental Practices Ι Part B 3
Australian Commission on Safety and Quality in Health Care Standard 1: Governance for Safety and Quality in Health Service Organisations
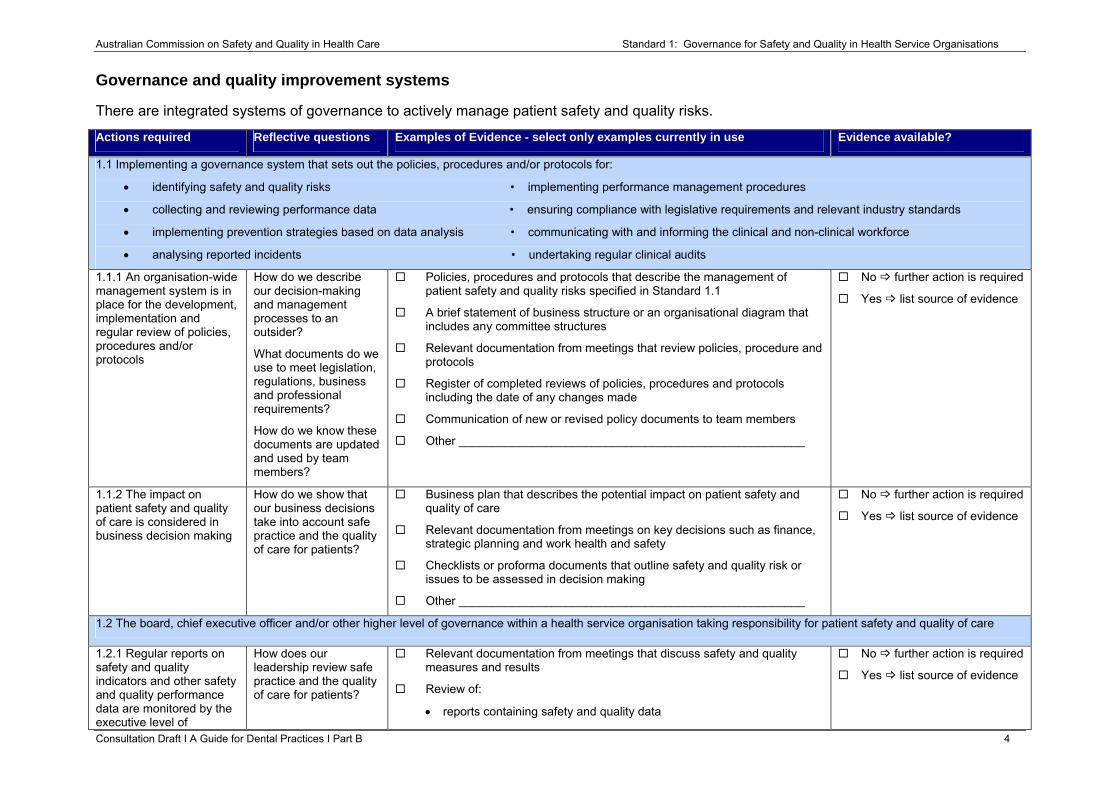
Governance and quality improvement systems
There are integrated systems of governance to actively manage patient safety and quality risks.
Consultation Draft Ι A Guide for Dental Practices Ι Part B 4
Actions required Reflective questions Examples of Evidence - select only examples currently in use Evidence available?
1.1 Implementing a governance system that sets out the policies, procedures and/or protocols for:
• identifying safety and quality risks • implementing performance management procedures
• collecting and reviewing performance data • ensuring compliance with legislative requirements and relevant industry standards
• implementing prevention strategies based on data analysis • communicating with and informing the clinical and non-clinical workforce
• analysing reported incidents • undertaking regular clinical audits
1.1.1 An organisation-wide management system is in place for the development, implementation and regular review of policies, procedures and/or protocols
How do we describe our decision-making and management processes to an outsider?
What documents do we use to meet legislation, regulations, business and professional requirements?
How do we know these documents are updated and used by team members?
Policies, procedures and protocols that describe the management of patient safety and quality risks specified in Standard 1.1
A brief statement of business structure or an organisational diagram that includes any committee structures
Relevant documentation from meetings that review policies, procedure and protocols
Register of completed reviews of policies, procedures and protocols including the date of any changes made
Communication of new or revised policy documents to team members
Other ____________________________________________________
No further action is required
Yes list source of evidence
1.1.2 The impact on patient safety and quality of care is considered in business decision making
How do we show that our business decisions take into account safe practice and the quality of care for patients?
Business plan that describes the potential impact on patient safety and quality of care
Relevant documentation from meetings on key decisions such as finance, strategic planning and work health and safety
Checklists or proforma documents that outline safety and quality risk or issues to be assessed in decision making
Other ____________________________________________________
No further action is required
Yes list source of evidence
1.2 The board, chief executive officer and/or other higher level of governance within a health service organisation taking responsibility for patient safety and quality of care
1.2.1 Regular reports on safety and quality indicators and other safety and quality performance data are monitored by the executive level of
How does our leadership review safe practice and the quality of care for patients?
Relevant documentation from meetings that discuss safety and quality measures and results
Review of:
• reports containing safety and quality data
No further action is required
Yes list source of evidence
Australian Commission on Safety and Quality in Health Care Standard 1: Governance for Safety and Quality in Health Service Organisations
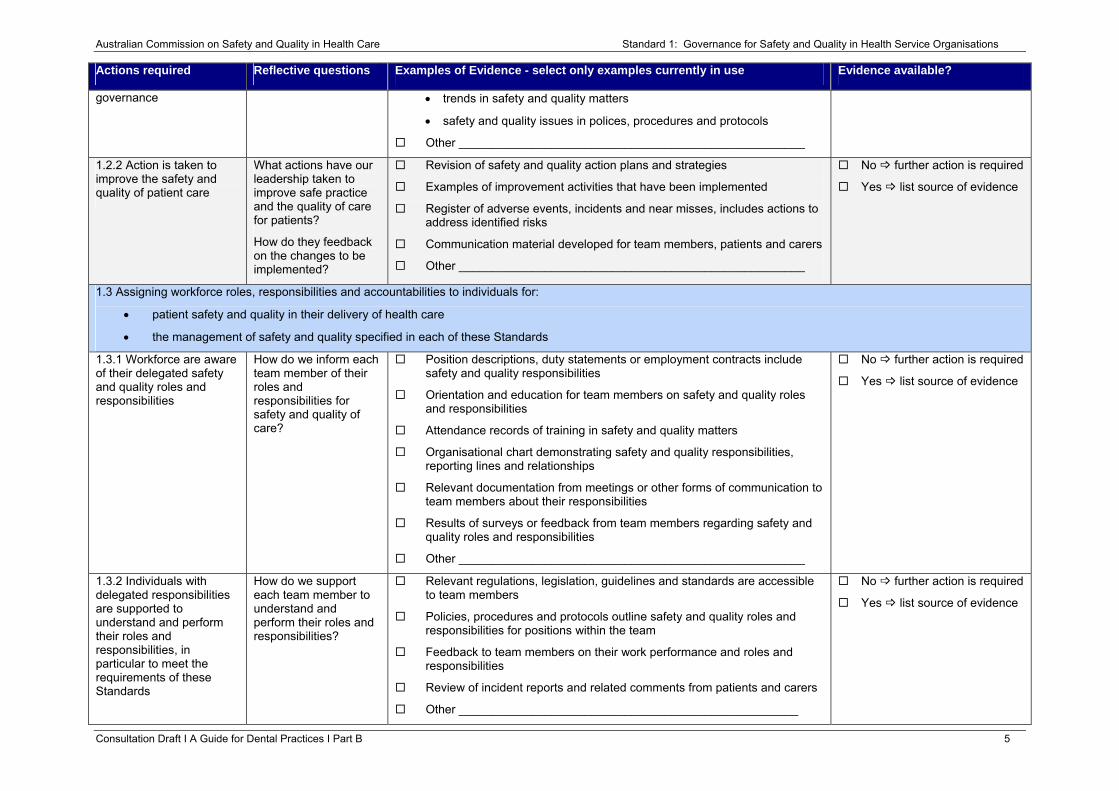
Actions required Reflective questions Examples of Evidence - select only examples currently in use Evidence available?
governance • trends in safety and quality matters
• safety and quality issues in polices, procedures and protocols
Other ____________________________________________________
1.2.2 Action is taken to improve the safety and quality of patient care
What actions have our leadership taken to improve safe practice and the quality of care for patients?
How do they feedback on the changes to be implemented?
Revision of safety and quality action plans and strategies
Examples of improvement activities that have been implemented
Register of adverse events, incidents and near misses, includes actions to address identified risks
Communication material developed for team members, patients and carers
Other ____________________________________________________
No further action is required
Yes list source of evidence
1.3 Assigning workforce roles, responsibilities and accountabilities to individuals for:
• patient safety and quality in their delivery of health care
• the management of safety and quality specified in each of these Standards
1.3.1 Workforce are aware of their delegated safety and quality roles and responsibilities
How do we inform each team member of their roles and responsibilities for safety and quality of care?
Position descriptions, duty statements or employment contracts include safety and quality responsibilities
Orientation and education for team members on safety and quality roles and responsibilities
Attendance records of training in safety and quality matters
Organisational chart demonstrating safety and quality responsibilities, reporting lines and relationships
Relevant documentation from meetings or other forms of communication to team members about their responsibilities
Results of surveys or feedback from team members regarding safety and quality roles and responsibilities
Other ____________________________________________________
No further action is required
Yes list source of evidence
1.3.2 Individuals with delegated responsibilities are supported to understand and perform their roles and responsibilities, in particular to meet the requirements of these Standards
How do we support each team member to understand and perform their roles and responsibilities?
Relevant regulations, legislation, guidelines and standards are accessible to team members
Policies, procedures and protocols outline safety and quality roles and responsibilities for positions within the team
Feedback to team members on their work performance and roles and responsibilities
Review of incident reports and related comments from patients and carers
Other ___________________________________________________
No further action is required
Yes list source of evidence
Consultation Draft Ι A Guide for Dental Practices Ι Part B 5
Australian Commission on Safety and Quality in Health Care Standard 1: Governance for Safety and Quality in Health Service Organisations
Actions required Reflective questions Examples of Evidence - select only examples currently in use Evidence available?
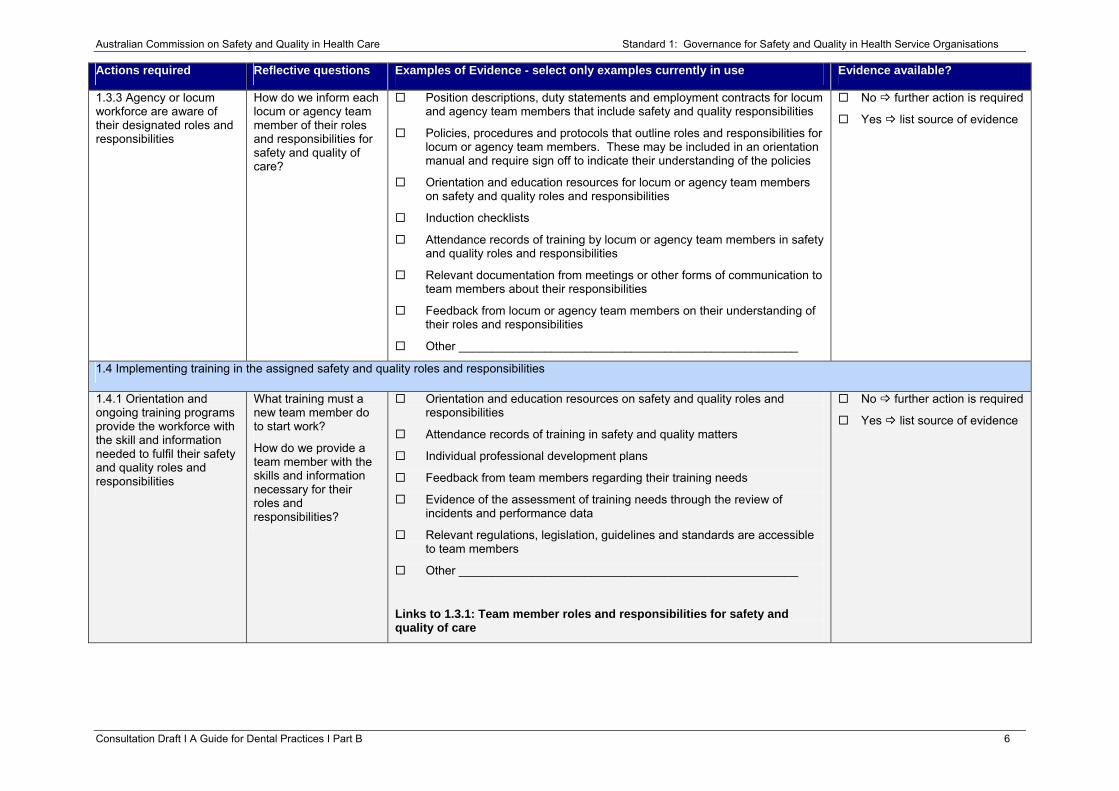
1.3.3 Agency or locum workforce are aware of their designated roles and responsibilities
How do we inform each locum or agency team member of their roles and responsibilities for safety and quality of care?
Position descriptions, duty statements and employment contracts for locum and agency team members that include safety and quality responsibilities
Policies, procedures and protocols that outline roles and responsibilities for locum or agency team members. These may be included in an orientation manual and require sign off to indicate their understanding of the policies
Orientation and education resources for locum or agency team members on safety and quality roles and responsibilities
Induction checklists
Attendance records of training by locum or agency team members in safety and quality roles and responsibilities
Relevant documentation from meetings or other forms of communication to team members about their responsibilities
Feedback from locum or agency team members on their understanding of their roles and responsibilities
Other ___________________________________________________
No further action is required
Yes list source of evidence
1.4 Implementing training in the assigned safety and quality roles and responsibilities
1.4.1 Orientation and ongoing training programs provide the workforce with the skill and information needed to fulfil their safety and quality roles and responsibilities
What training must a new team member do to start work?
How do we provide a team member with the skills and information necessary for their roles and responsibilities?
Orientation and education resources on safety and quality roles and responsibilities
Attendance records of training in safety and quality matters
Individual professional development plans
Feedback from team members regarding their training needs
Evidence of the assessment of training needs through the review of incidents and performance data
Relevant regulations, legislation, guidelines and standards are accessible to team members
Other ___________________________________________________
Links to 1.3.1: Team member roles and responsibilities for safety and quality of care
No further action is required
Yes list source of evidence
Consultation Draft Ι A Guide for Dental Practices Ι Part B 6
Australian Commission on Safety and Quality in Health Care Standard 1: Governance for Safety and Quality in Health Service Organisations
Actions required Reflective questions Examples of Evidence - select only examples currently in use Evidence available?
1.4.2 Annual mandatory training programs to meet the requirements of these Standards
What training must team members do each year?
List of essential annual education and training opportunities, including on-the-job training, to be current with any new equipment, procedures or protocols
Audit of team member education and training needs matched against the requirements of the NSQHS Standards
Policy that outlines mandatory training requirements for team members in areas such as:
• work health and safety
• infection control
• medical emergency training or
• other training as required by the dental practice
Education resources and attendance records for mandatory training requirements
Other ___________________________________________________
No further action is required
Yes list source of evidence
1.4.3 Locum and agency workforce have the necessary information, training and orientation to the workplace to fulfil their safety and quality roles and responsibilities
How do we provide a locum or agency team member with the necessary skills and information to undertake their role and responsibilities?
Policies, procedures and protocols that are readily accessible to locum and agency team members
Orientation and education resources for locum and agency team members
Attendance records of training for locum or agency team members
Contracts and position descriptions for locum and agency team members
Skills appraisals of locum and agency team members
Register of locum and agency team member credentials (qualifications)
Policy, procedures and protocols for clinical supervision of locum and agency team members
Internal communication system that is accessible to locum and agency team members with information about safety and quality (for example, intranet or memos)
Other ___________________________________________________
No further action is required
Yes list source of evidence
1.4.4 Competency-based training is provided to the clinical workforce to improve safety and quality
How do we provide competency based training to clinical team members to improve our safety and quality care in the practice?
Orientation and education resources in competency based training for clinical team members to enhance safety and quality
Schedule of training for clinical team members
Attendance records and results of competency based training for clinical team members
Communication to clinical team members regarding annual mandatory
No further action is required
Yes list source of evidence
Consultation Draft Ι A Guide for Dental Practices Ι Part B 7
Australian Commission on Safety and Quality in Health Care Standard 1: Governance for Safety and Quality in Health Service Organisations
Actions required Reflective questions Examples of Evidence - select only examples currently in use Evidence available?
training requirements
Other ___________________________________________________
Links to 1.4.1: Orientation and ongoing training programs for team members
1.5 Establishing an organisation-wide risk management system that incorporates identification, assessment, rating, controls and monitoring for patient safety and quality
1.5.1 An organisation-wide risk register is used and regularly monitored
How do we identify, record and implement changes to reduce the risks to safe practice and quality of care for our patients?
Register of adverse events, incidents and near misses includes actions taken to address identified risks
Completed risk assessments
Review of comments and complaints, and use of these results for improvement purposes
Relevant documentation from meetings or other forms of communication to team members about risk matters
Reports of trends in safety and quality risks
Feedback from team members
Other ___________________________________________________
No further action is required
Yes list source of evidence
1.5.2 Actions are taken to minimise risks to patient safety and quality of care
What action do we take to reduce safety risks and improve the quality of care for our patients?
Relevant documentation from meetings or other forms of communication to team members about risk matters
Reviews of safety and quality measures or performance indicators with recommendations for improvement, including action plans and outcomes
Examples of improvement activities that have been implemented and evaluated
Other ___________________________________________________
No further action is required
Yes list source of evidence
1.6 Establishing an organisation-wide quality management system that monitors and reports on the safety and quality of patient care and informs changes in practice
1.6.1 An organisation-wide quality management system is used and regularly monitored
How do we plan our work, then measure our success against what we do and do it better?
How do we use quality management methods in our practice?
Policies, procedures, protocols or plans that describe a quality approach in key areas such as:
• leadership
• planning activities and introduction of changes
• roles and responsibilities
• dissemination of information and documents
No further action is required
Yes list source of evidence
Consultation Draft Ι A Guide for Dental Practices Ι Part B 8
Australian Commission on Safety and Quality in Health Care Standard 1: Governance for Safety and Quality in Health Service Organisations
Actions required Reflective questions Examples of Evidence - select only examples currently in use Evidence available?
• work and administrative activities
• measurement and observation of performance
• review and improvement of activities
Evaluation reports on the safety and quality of patient care and any introduced changes in practice
Reports, presentations and analysis of performance data
Position descriptions or employment contracts that require participation in quality management systems
Feedback to team members on their work performance in safety and quality matters
Use of quality management tools such as the Plan–Do–Check–Act (PDCA) cycle
Other ___________________________________________________
1.6 Establishing an organisation-wide quality management system that monitors and reports on the safety and quality of patient care and informs changes in practice
1.6.2 Actions are taken to maximise patient quality of care
What actions have we taken to ensure the highest quality of care for our patients?
Policies, procedures and protocols that that have been developed to identify and address deficiencies in care
Register of adverse events, incidents and near misses, including actions to address identified issues
Analysis of patient and carer feedback or satisfaction survey results
Review of identified areas requiring action in patient quality of care
Examples of improvement activities that have been implemented
Other ___________________________________________________
No further action is required
Yes list source of evidence
Consultation Draft Ι A Guide for Dental Practices Ι Part B 9
Australian Commission on Safety and Quality in Health Care Standard 1: Governance for Safety and Quality in Health Service Organisations
Clinical practice
Care provided by the clinical workforce is guided by current best practice.
Actions required Reflective questions Examples of Evidence - select only examples currently in use Evidence available?
1.7 Developing and/or applying clinical guidelines or pathways that are supported by the best available evidence
1.7.1 Agreed and documented clinical guidelines and/or pathways are available to the clinical workforce
Which clinical guidelines do we use, where do they come from and how do our team members access them?
Policies, procedures and protocols for accessing clinical guidelines
Register of clinical guidelines used by the practice
Current guidelines accessible to team members
Audit of the availability and currency of clinical guidelines to team members
Other ___________________________________________________
No further action is required
Yes list source of evidence
1.7.2 The use of agreed clinical guidelines by the clinical workforce is monitored
How do we find out if clinical team members are using agreed clinical guidelines?
Declaration of compliance by dental practitioners
Feedback to dental practitioners on their work performance
Observation of clinical practice
Other ___________________________________________________
No further action is required
Yes list source of evidence
1.8 Adopting processes to support the early identification, early intervention and appropriate management of patients at increased risk of harm
1.8.1 Mechanisms are in place to identify patients at increased risk of harm
How do we identify patients at increased risk of harm?
Audits of patient medical and dental history or other information such as whether they have a significant disability or are from a culturally and linguistically diverse (CALD) background
Policies, procedures and protocols that outline how a dental practitioner is alerted to patients at increased risk of harm
Risk profile of the dental practice that details the most likely risks and their potential impact
Completed risk assessments
Register of adverse events, incidents and near misses including actions to address identified issues
Review of patient and carer complaints
Other ___________________________________________________
No further action is required
Yes list source of evidence
1.8.2 Early action is taken to reduce the risks for at-risk patients
What action have we taken to decrease the risk of harm to our vulnerable patients?
Action plans implemented for patients identified at increased risk of harm
Declaration of compliance with measures and procedures by dental practitioners
Feedback to dental practitioners on their work performance
No further action is required
Yes list source of evidence
Consultation Draft Ι A Guide for Dental Practices Ι Part B 10
Australian Commission on Safety and Quality in Health Care Standard 1: Governance for Safety and Quality in Health Service Organisations
Actions required Reflective questions Examples of Evidence - select only examples currently in use Evidence available?
Observation of clinical practice
Other ___________________________________________________
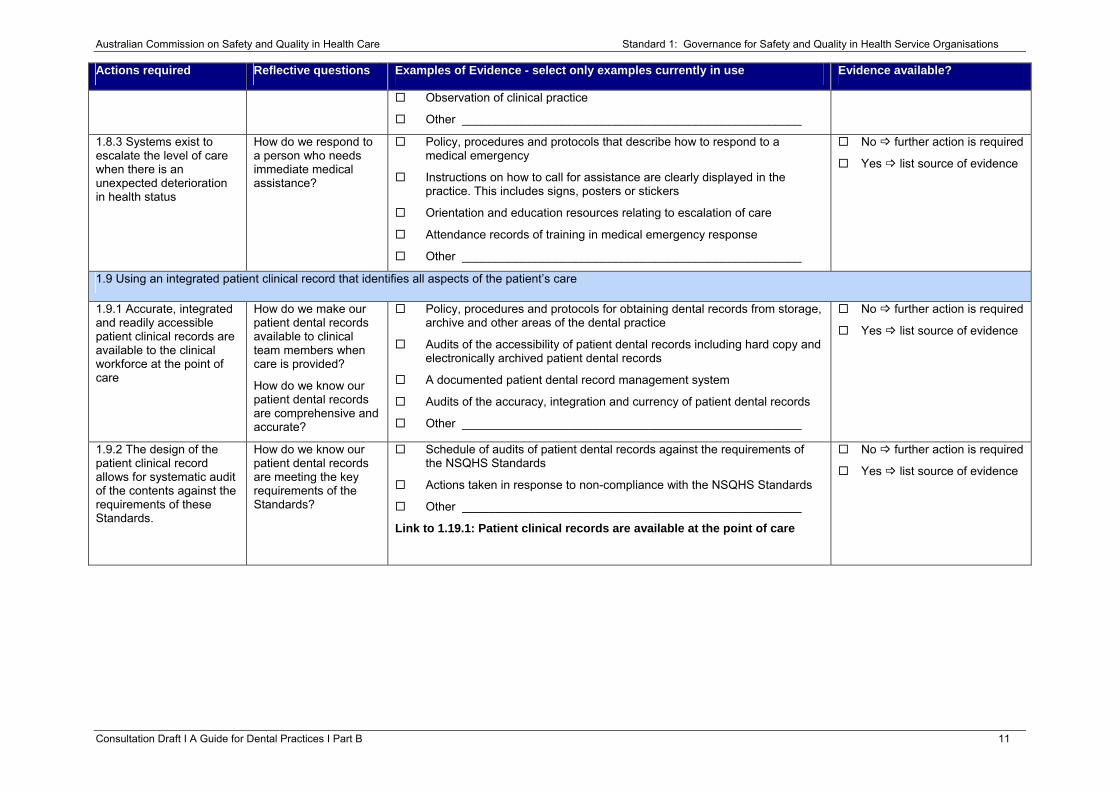
1.8.3 Systems exist to escalate the level of care when there is an unexpected deterioration in health status
How do we respond to a person who needs immediate medical assistance?
Policy, procedures and protocols that describe how to respond to a medical emergency
Instructions on how to call for assistance are clearly displayed in the practice. This includes signs, posters or stickers
Orientation and education resources relating to escalation of care
Attendance records of training in medical emergency response
Other ___________________________________________________
No further action is required
Yes list source of evidence
1.9 Using an integrated patient clinical record that identifies all aspects of the patient’s care
1.9.1 Accurate, integrated and readily accessible patient clinical records are available to the clinical workforce at the point of care
How do we make our patient dental records available to clinical team members when care is provided?
How do we know our patient dental records are comprehensive and accurate?
Policy, procedures and protocols for obtaining dental records from storage, archive and other areas of the dental practice
Audits of the accessibility of patient dental records including hard copy and electronically archived patient dental records
A documented patient dental record management system
Audits of the accuracy, integration and currency of patient dental records
Other ___________________________________________________
No further action is required
Yes list source of evidence
1.9.2 The design of the patient clinical record allows for systematic audit of the contents against the requirements of these Standards.
How do we know our patient dental records are meeting the key requirements of the Standards?
Schedule of audits of patient dental records against the requirements of the NSQHS Standards
Actions taken in response to non-compliance with the NSQHS Standards
Other ___________________________________________________
Link to 1.19.1: Patient clinical records are available at the point of care
No further action is required
Yes list source of evidence
Consultation Draft Ι A Guide for Dental Practices Ι Part B 11
Australian Commission on Safety and Quality in Health Care Standard 1: Governance for Safety and Quality in Health Service Organisations
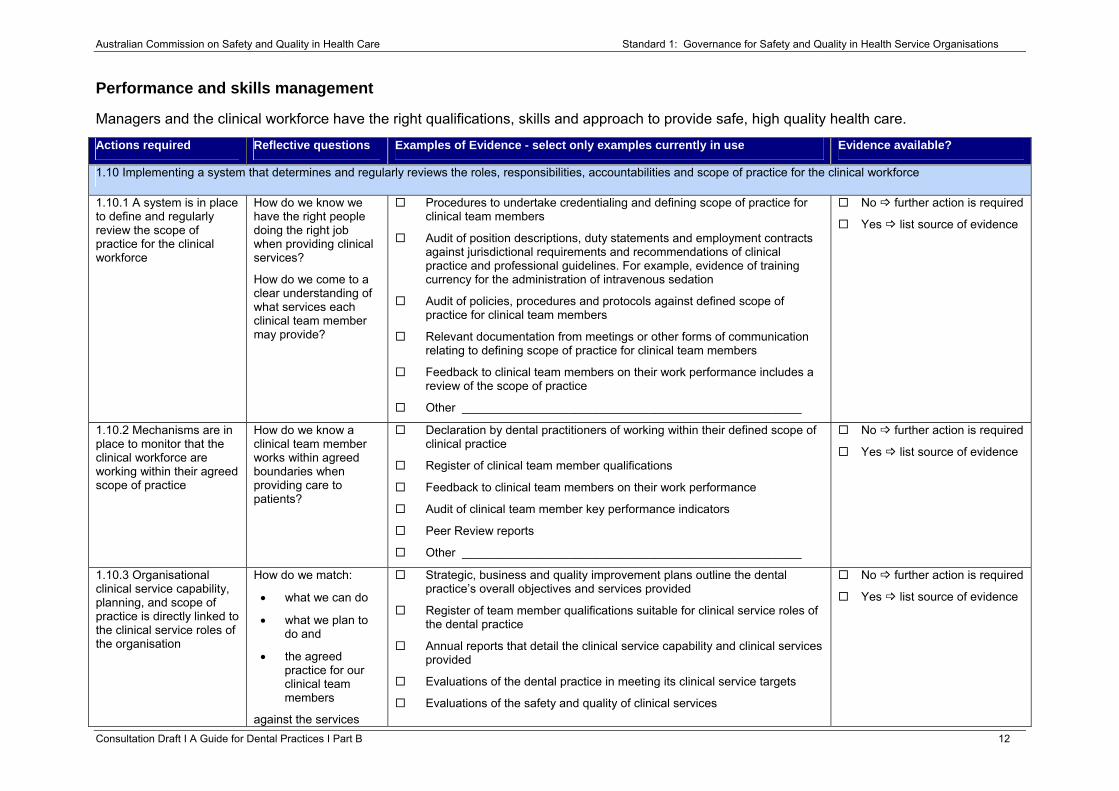
Performance and skills management
Managers and the clinical workforce have the right qualifications, skills and approach to provide safe, high quality health care.
Consultation Draft Ι A Guide for Dental Practices Ι Part B 12
Actions required Reflective questions Examples of Evidence - select only examples currently in use Evidence available?
1.10 Implementing a system that determines and regularly reviews the roles, responsibilities, accountabilities and scope of practice for the clinical workforce
1.10.1 A system is in place to define and regularly review the scope of practice for the clinical workforce
How do we know we have the right people doing the right job when providing clinical services?
How do we come to a clear understanding of what services each clinical team member may provide?
Procedures to undertake credentialing and defining scope of practice for clinical team members
Audit of position descriptions, duty statements and employment contracts against jurisdictional requirements and recommendations of clinical practice and professional guidelines. For example, evidence of training currency for the administration of intravenous sedation
Audit of policies, procedures and protocols against defined scope of practice for clinical team members
Relevant documentation from meetings or other forms of communication relating to defining scope of practice for clinical team members
Feedback to clinical team members on their work performance includes a review of the scope of practice
Other ___________________________________________________
No further action is required
Yes list source of evidence
1.10.2 Mechanisms are in place to monitor that the clinical workforce are working within their agreed scope of practice
How do we know a clinical team member works within agreed boundaries when providing care to patients?
Declaration by dental practitioners of working within their defined scope of clinical practice
Register of clinical team member qualifications
Feedback to clinical team members on their work performance
Audit of clinical team member key performance indicators
Peer Review reports
Other ___________________________________________________
No further action is required
Yes list source of evidence
1.10.3 Organisational clinical service capability, planning, and scope of practice is directly linked to the clinical service roles of the organisation
How do we match:
• what we can do
• what we plan to do and
• the agreed practice for our clinical team members
against the services
Strategic, business and quality improvement plans outline the dental practice’s overall objectives and services provided
Register of team member qualifications suitable for clinical service roles of the dental practice
Annual reports that detail the clinical service capability and clinical services provided
Evaluations of the dental practice in meeting its clinical service targets
Evaluations of the safety and quality of clinical services
No further action is required
Yes list source of evidence
Australian Commission on Safety and Quality in Health Care Standard 1: Governance for Safety and Quality in Health Service Organisations
Actions required Reflective questions Examples of Evidence - select only examples currently in use Evidence available?
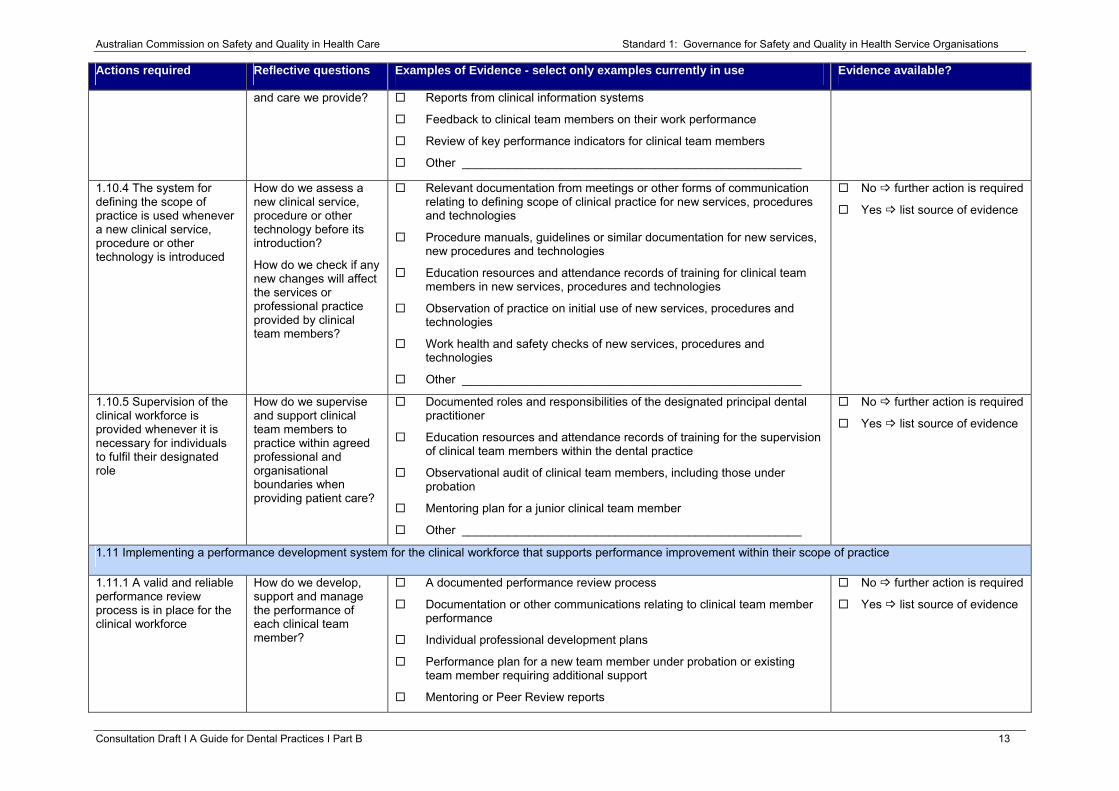
and care we provide? Reports from clinical information systems
Feedback to clinical team members on their work performance
Review of key performance indicators for clinical team members
Other ___________________________________________________
1.10.4 The system for defining the scope of practice is used whenever a new clinical service, procedure or other technology is introduced
How do we assess a new clinical service, procedure or other technology before its introduction?
How do we check if any new changes will affect the services or professional practice provided by clinical team members?
Relevant documentation from meetings or other forms of communication relating to defining scope of clinical practice for new services, procedures and technologies
Procedure manuals, guidelines or similar documentation for new services, new procedures and technologies
Education resources and attendance records of training for clinical team members in new services, procedures and technologies
Observation of practice on initial use of new services, procedures and technologies
Work health and safety checks of new services, procedures and technologies
Other ___________________________________________________
No further action is required
Yes list source of evidence
1.10.5 Supervision of the clinical workforce is provided whenever it is necessary for individuals to fulfil their designated role
How do we supervise and support clinical team members to practice within agreed professional and organisational boundaries when providing patient care?
Documented roles and responsibilities of the designated principal dental practitioner
Education resources and attendance records of training for the supervision of clinical team members within the dental practice
Observational audit of clinical team members, including those under probation
Mentoring plan for a junior clinical team member
Other ___________________________________________________
No further action is required
Yes list source of evidence
1.11 Implementing a performance development system for the clinical workforce that supports performance improvement within their scope of practice
1.11.1 A valid and reliable performance review process is in place for the clinical workforce
How do we develop, support and manage the performance of each clinical team member?
A documented performance review process
Documentation or other communications relating to clinical team member performance
Individual professional development plans
Performance plan for a new team member under probation or existing team member requiring additional support
Mentoring or Peer Review reports
No further action is required
Yes list source of evidence
Consultation Draft Ι A Guide for Dental Practices Ι Part B 13
Australian Commission on Safety and Quality in Health Care Standard 1: Governance for Safety and Quality in Health Service Organisations
Actions required Reflective questions Examples of Evidence - select only examples currently in use Evidence available?
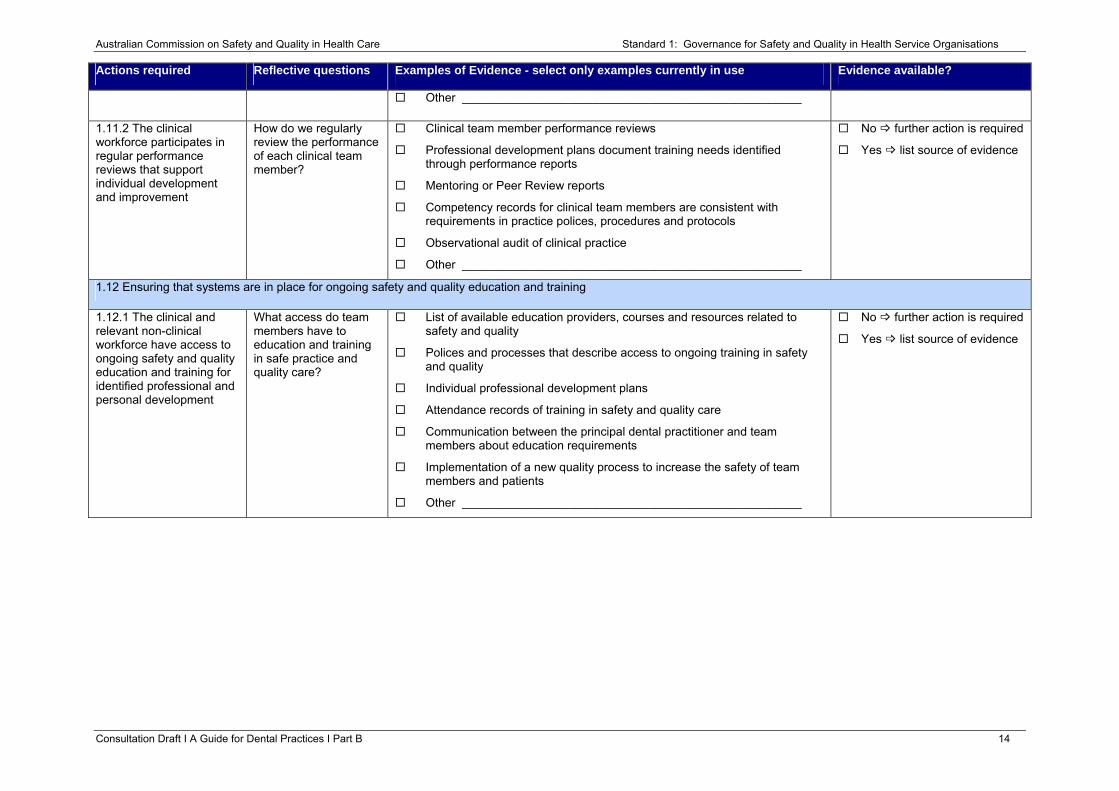
Other ___________________________________________________
1.11.2 The clinical workforce participates in regular performance reviews that support individual development and improvement
How do we regularly review the performance of each clinical team member?
Clinical team member performance reviews
Professional development plans document training needs identified through performance reports
Mentoring or Peer Review reports
Competency records for clinical team members are consistent with requirements in practice polices, procedures and protocols
Observational audit of clinical practice
Other ___________________________________________________
No further action is required
Yes list source of evidence
1.12 Ensuring that systems are in place for ongoing safety and quality education and training
1.12.1 The clinical and relevant non-clinical workforce have access to ongoing safety and quality education and training for identified professional and personal development
What access do team members have to education and training in safe practice and quality care?
List of available education providers, courses and resources related to safety and quality
Polices and processes that describe access to ongoing training in safety and quality
Individual professional development plans
Attendance records of training in safety and quality care
Communication between the principal dental practitioner and team members about education requirements
Implementation of a new quality process to increase the safety of team members and patients
Other ___________________________________________________
No further action is required
Yes list source of evidence
Consultation Draft Ι A Guide for Dental Practices Ι Part B 14
Australian Commission on Safety and Quality in Health Care Standard 1: Governance for Safety and Quality in Health Service Organisations
Actions required Reflective questions Examples of Evidence - select only examples currently in use Evidence available?
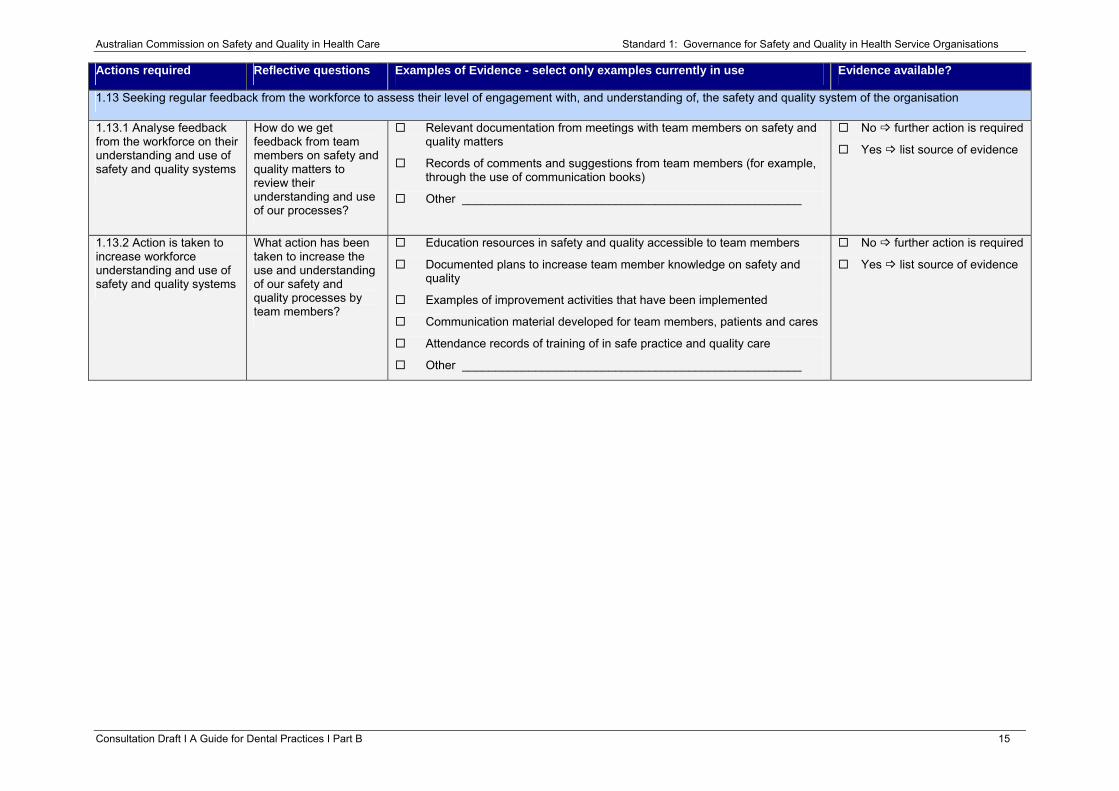
1.13 Seeking regular feedback from the workforce to assess their level of engagement with, and understanding of, the safety and quality system of the organisation
1.13.1 Analyse feedback from the workforce on their understanding and use of safety and quality systems
How do we get feedback from team members on safety and quality matters to review their understanding and use of our processes?
Relevant documentation from meetings with team members on safety and quality matters
Records of comments and suggestions from team members (for example, through the use of communication books)
Other ___________________________________________________
No further action is required
Yes list source of evidence
1.13.2 Action is taken to increase workforce understanding and use of safety and quality systems
What action has been taken to increase the use and understanding of our safety and quality processes by team members?
Education resources in safety and quality accessible to team members
Documented plans to increase team member knowledge on safety and quality
Examples of improvement activities that have been implemented
Communication material developed for team members, patients and cares
Attendance records of training of in safe practice and quality care
Other ___________________________________________________
No further action is required
Yes list source of evidence
Consultation Draft Ι A Guide for Dental Practices Ι Part B 15
Australian Commission on Safety and Quality in Health Care Standard 1: Governance for Safety and Quality in Health Service Organisations
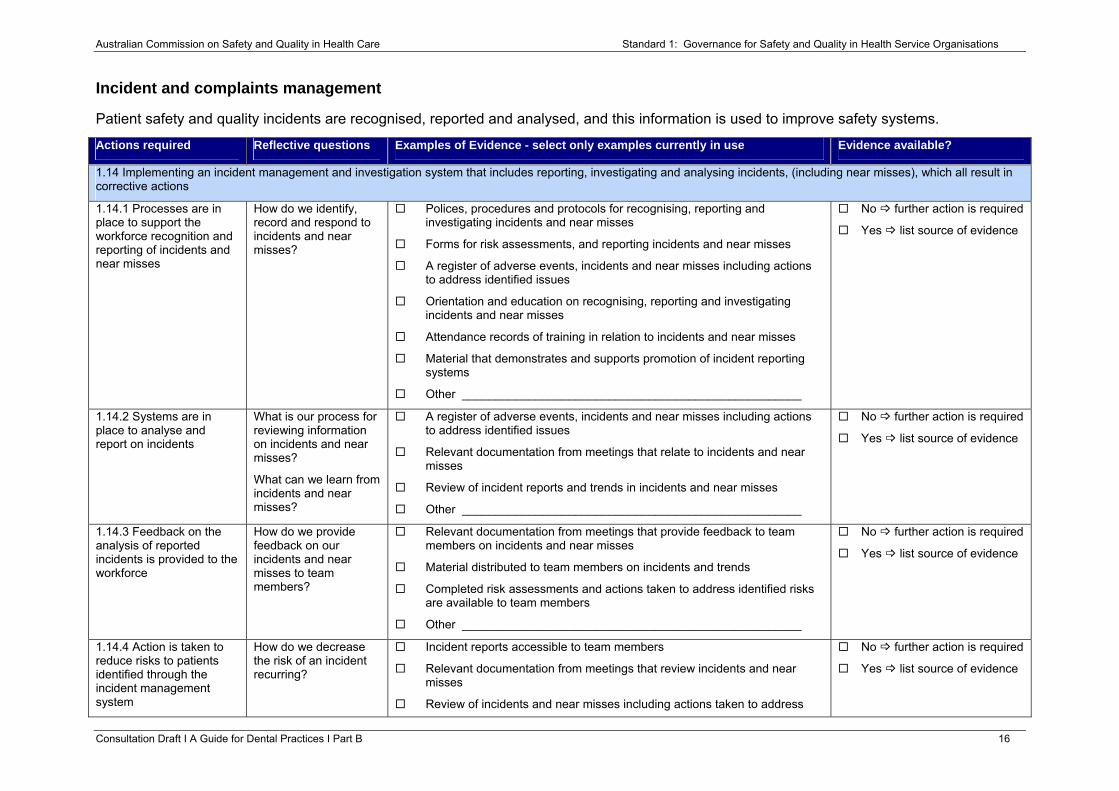
Incident and complaints management
Patient safety and quality incidents are recognised, reported and analysed, and this information is used to improve safety systems.
Actions required Reflective questions Examples of Evidence - select only examples currently in use Evidence available?
1.14 Implementing an incident management and investigation system that includes reporting, investigating and analysing incidents, (including near misses), which all result in corrective actions
1.14.1 Processes are in place to support the workforce recognition and reporting of incidents and near misses
How do we identify, record and respond to incidents and near misses?
Polices, procedures and protocols for recognising, reporting and investigating incidents and near misses
Forms for risk assessments, and reporting incidents and near misses
A register of adverse events, incidents and near misses including actions to address identified issues
Orientation and education on recognising, reporting and investigating incidents and near misses
Attendance records of training in relation to incidents and near misses
Material that demonstrates and supports promotion of incident reporting systems
Other ___________________________________________________
No further action is required
Yes list source of evidence
1.14.2 Systems are in place to analyse and report on incidents
What is our process for reviewing information on incidents and near misses?
What can we learn from incidents and near misses?
A register of adverse events, incidents and near misses including actions to address identified issues
Relevant documentation from meetings that relate to incidents and near misses
Review of incident reports and trends in incidents and near misses
Other ___________________________________________________
No further action is required
Yes list source of evidence
1.14.3 Feedback on the analysis of reported incidents is provided to the workforce
How do we provide feedback on our incidents and near misses to team members?
Relevant documentation from meetings that provide feedback to team members on incidents and near misses
Material distributed to team members on incidents and trends
Completed risk assessments and actions taken to address identified risks are available to team members
Other ___________________________________________________
No further action is required
Yes list source of evidence
1.14.4 Action is taken to reduce risks to patients identified through the incident management system
How do we decrease the risk of an incident recurring?
Incident reports accessible to team members
Relevant documentation from meetings that review incidents and near misses
Review of incidents and near misses including actions taken to address
No further action is required
Yes list source of evidence
Consultation Draft Ι A Guide for Dental Practices Ι Part B 16
Australian Commission on Safety and Quality in Health Care Standard 1: Governance for Safety and Quality in Health Service Organisations
Actions required Reflective questions Examples of Evidence - select only examples currently in use Evidence available?
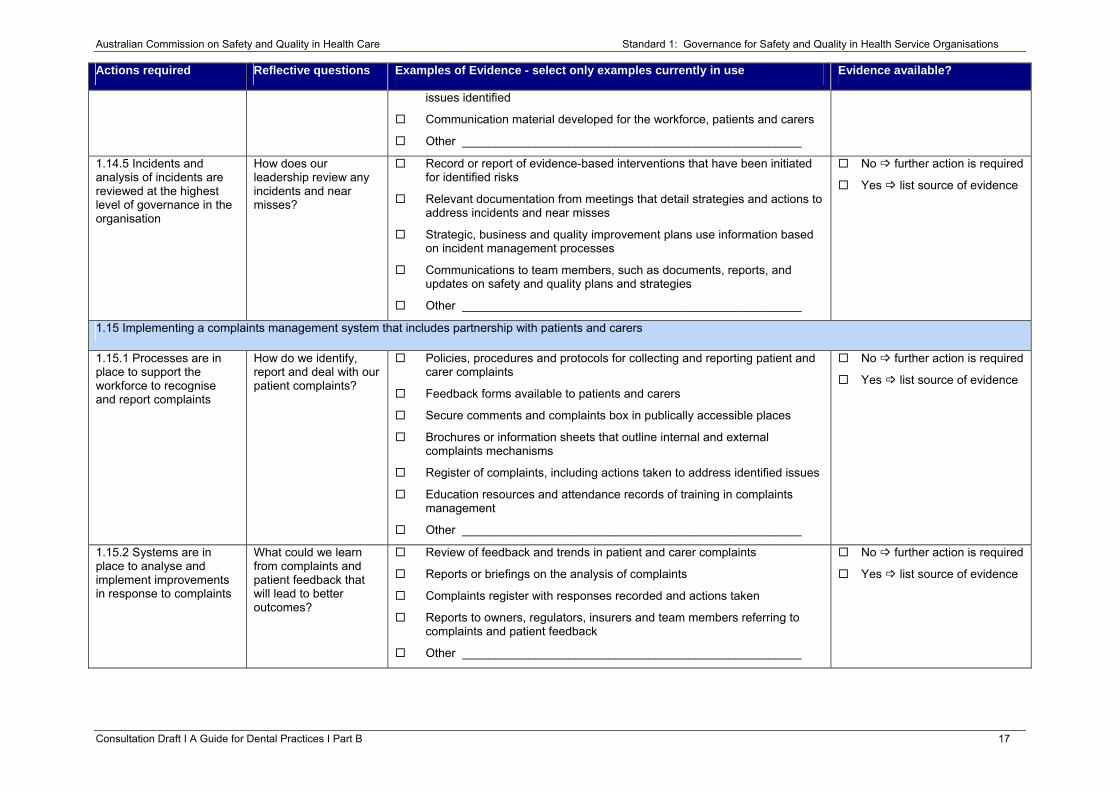
issues identified
Communication material developed for the workforce, patients and carers
Other ___________________________________________________
1.14.5 Incidents and analysis of incidents are reviewed at the highest level of governance in the organisation
How does our leadership review any incidents and near misses?
Record or report of evidence-based interventions that have been initiated for identified risks
Relevant documentation from meetings that detail strategies and actions to address incidents and near misses
Strategic, business and quality improvement plans use information based on incident management processes
Communications to team members, such as documents, reports, and updates on safety and quality plans and strategies
Other ___________________________________________________
No further action is required
Yes list source of evidence
1.15 Implementing a complaints management system that includes partnership with patients and carers
1.15.1 Processes are in place to support the workforce to recognise and report complaints
How do we identify, report and deal with our patient complaints?
Policies, procedures and protocols for collecting and reporting patient and carer complaints
Feedback forms available to patients and carers
Secure comments and complaints box in publically accessible places
Brochures or information sheets that outline internal and external complaints mechanisms
Register of complaints, including actions taken to address identified issues
Education resources and attendance records of training in complaints management
Other ___________________________________________________
No further action is required
Yes list source of evidence
1.15.2 Systems are in place to analyse and implement improvements in response to complaints
What could we learn from complaints and patient feedback that will lead to better outcomes?
Review of feedback and trends in patient and carer complaints
Reports or briefings on the analysis of complaints
Complaints register with responses recorded and actions taken
Reports to owners, regulators, insurers and team members referring to complaints and patient feedback
Other ___________________________________________________
No further action is required
Yes list source of evidence
Consultation Draft Ι A Guide for Dental Practices Ι Part B 17
Australian Commission on Safety and Quality in Health Care Standard 1: Governance for Safety and Quality in Health Service Organisations
Actions required Reflective questions Examples of Evidence - select only examples currently in use Evidence available?
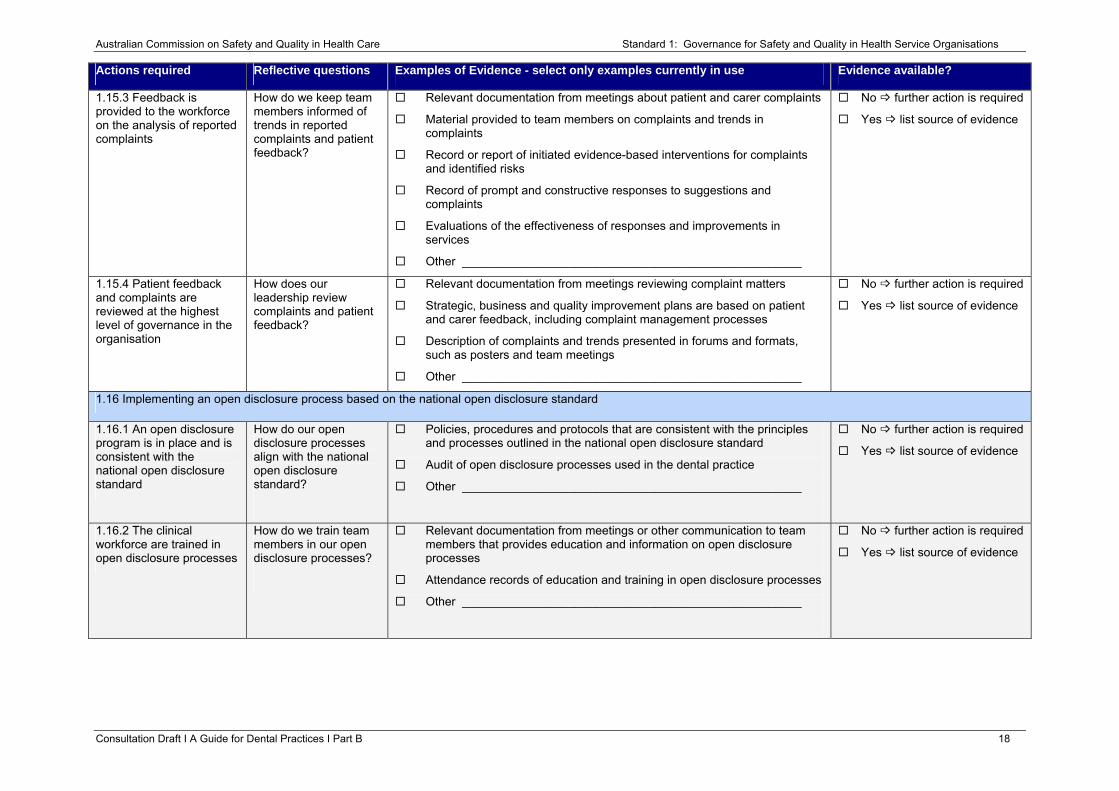
1.15.3 Feedback is provided to the workforce on the analysis of reported complaints
How do we keep team members informed of trends in reported complaints and patient feedback?
Relevant documentation from meetings about patient and carer complaints
Material provided to team members on complaints and trends in complaints
Record or report of initiated evidence-based interventions for complaints and identified risks
Record of prompt and constructive responses to suggestions and complaints
Evaluations of the effectiveness of responses and improvements in services
Other ___________________________________________________
No further action is required
Yes list source of evidence
1.15.4 Patient feedback and complaints are reviewed at the highest level of governance in the organisation
How does our leadership review complaints and patient feedback?
Relevant documentation from meetings reviewing complaint matters
Strategic, business and quality improvement plans are based on patient and carer feedback, including complaint management processes
Description of complaints and trends presented in forums and formats, such as posters and team meetings
Other ___________________________________________________
No further action is required
Yes list source of evidence
1.16 Implementing an open disclosure process based on the national open disclosure standard
1.16.1 An open disclosure program is in place and is consistent with the national open disclosure standard
How do our open disclosure processes align with the national open disclosure standard?
Policies, procedures and protocols that are consistent with the principles and processes outlined in the national open disclosure standard
Audit of open disclosure processes used in the dental practice
Other ___________________________________________________
No further action is required
Yes list source of evidence
1.16.2 The clinical workforce are trained in open disclosure processes
How do we train team members in our open disclosure processes?
Relevant documentation from meetings or other communication to team members that provides education and information on open disclosure processes
Attendance records of education and training in open disclosure processes
Other ___________________________________________________
No further action is required
Yes list source of evidence
Consultation Draft Ι A Guide for Dental Practices Ι Part B 18
Australian Commission on Safety and Quality in Health Care Standard 1: Governance for Safety and Quality in Health Service Organisations
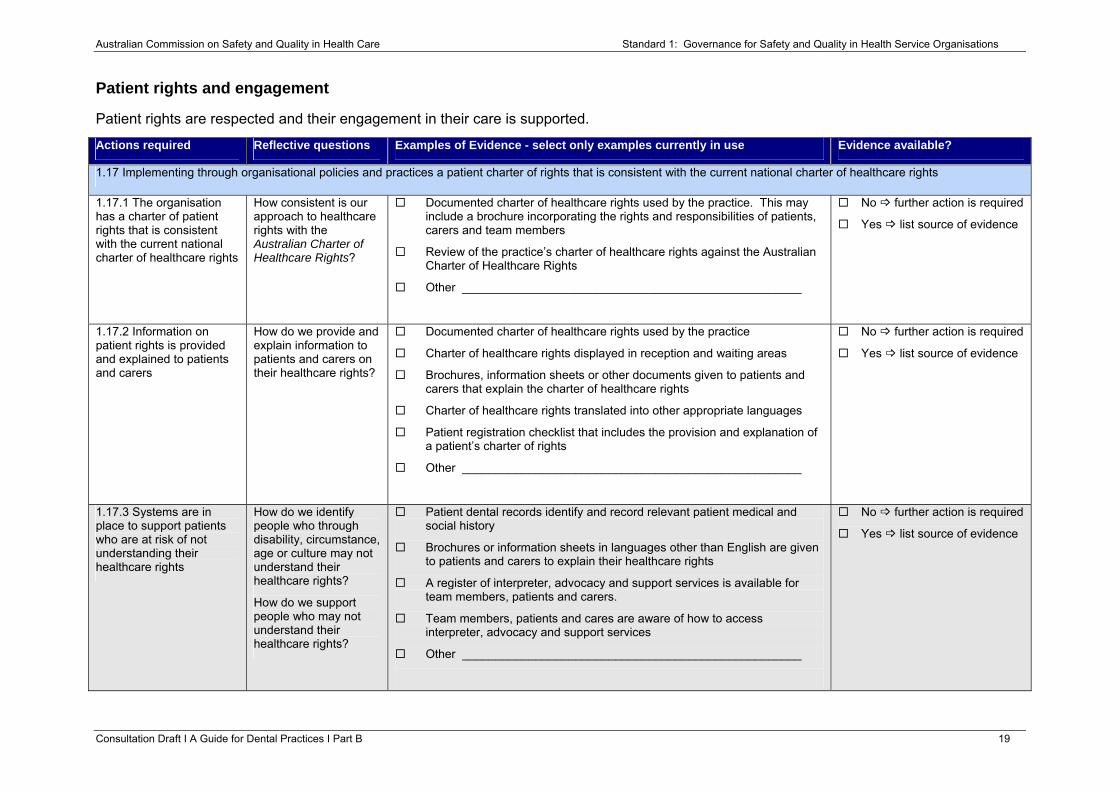
Patient rights and engagement
Patient rights are respected and their engagement in their care is supported.
Actions required Reflective questions Examples of Evidence - select only examples currently in use Evidence available?
1.17 Implementing through organisational policies and practices a patient charter of rights that is consistent with the current national charter of healthcare rights
1.17.1 The organisation has a charter of patient rights that is consistent with the current national charter of healthcare rights
How consistent is our approach to healthcare rights with the Australian Charter of Healthcare Rights?
Documented charter of healthcare rights used by the practice. This may include a brochure incorporating the rights and responsibilities of patients, carers and team members
Review of the practice’s charter of healthcare rights against the Australian Charter of Healthcare Rights
Other ___________________________________________________
No further action is required
Yes list source of evidence
1.17.2 Information on patient rights is provided and explained to patients and carers
How do we provide and explain information to patients and carers on their healthcare rights?
Documented charter of healthcare rights used by the practice
Charter of healthcare rights displayed in reception and waiting areas
Brochures, information sheets or other documents given to patients and carers that explain the charter of healthcare rights
Charter of healthcare rights translated into other appropriate languages
Patient registration checklist that includes the provision and explanation of a patient’s charter of rights
Other ___________________________________________________
No further action is required
Yes list source of evidence
1.17.3 Systems are in place to support patients who are at risk of not understanding their healthcare rights
How do we identify people who through disability, circumstance, age or culture may not understand their healthcare rights?
How do we support people who may not understand their healthcare rights?
Patient dental records identify and record relevant patient medical and social history
Brochures or information sheets in languages other than English are given to patients and carers to explain their healthcare rights
A register of interpreter, advocacy and support services is available for team members, patients and carers.
Team members, patients and cares are aware of how to access interpreter, advocacy and support services
Other ___________________________________________________
No further action is required
Yes list source of evidence
Consultation Draft Ι A Guide for Dental Practices Ι Part B 19
Australian Commission on Safety and Quality in Health Care Standard 1: Governance for Safety and Quality in Health Service Organisations
Actions required Reflective questions Examples of Evidence - select only examples currently in use Evidence available?
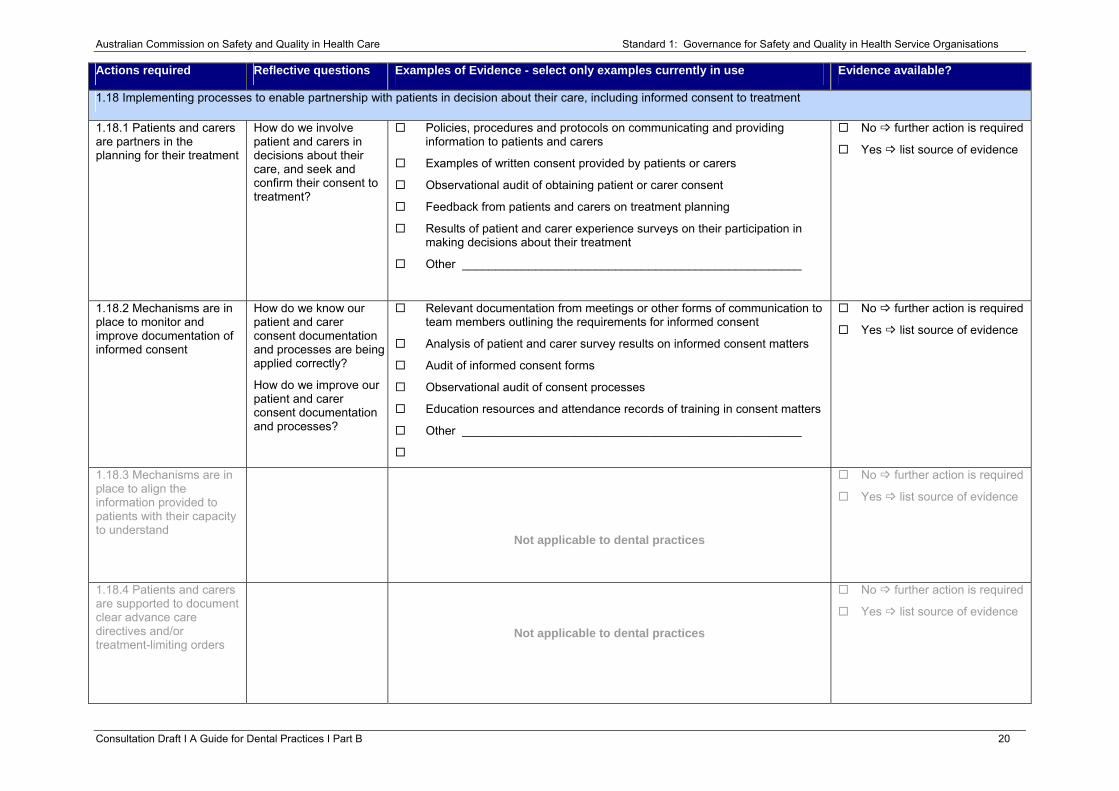
1.18 Implementing processes to enable partnership with patients in decision about their care, including informed consent to treatment
1.18.1 Patients and carers are partners in the planning for their treatment
How do we involve patient and carers in decisions about their care, and seek and confirm their consent to treatment?
Policies, procedures and protocols on communicating and providing information to patients and carers
Examples of written consent provided by patients or carers
Observational audit of obtaining patient or carer consent
Feedback from patients and carers on treatment planning
Results of patient and carer experience surveys on their participation in making decisions about their treatment
Other ___________________________________________________
No further action is required
Yes list source of evidence
1.18.2 Mechanisms are in place to monitor and improve documentation of informed consent
How do we know our patient and carer consent documentation and processes are being applied correctly?
How do we improve our patient and carer consent documentation and processes?
Relevant documentation from meetings or other forms of communication to team members outlining the requirements for informed consent
Analysis of patient and carer survey results on informed consent matters
Audit of informed consent forms
Observational audit of consent processes
Education resources and attendance records of training in consent matters
Other ___________________________________________________
No further action is required
Yes list source of evidence
1.18.3 Mechanisms are in place to align the information provided to patients with their capacity to understand
Not applicable to dental practices
No further action is required
Yes list source of evidence
1.18.4 Patients and carers are supported to document clear advance care directives and/or treatment-limiting orders
Not applicable to dental practices
No further action is required
Yes list source of evidence
Consultation Draft Ι A Guide for Dental Practices Ι Part B 20
Australian Commission on Safety and Quality in Health Care Standard 1: Governance for Safety and Quality in Health Service Organisations
Actions required Reflective questions Examples of Evidence - select only examples currently in use Evidence available?
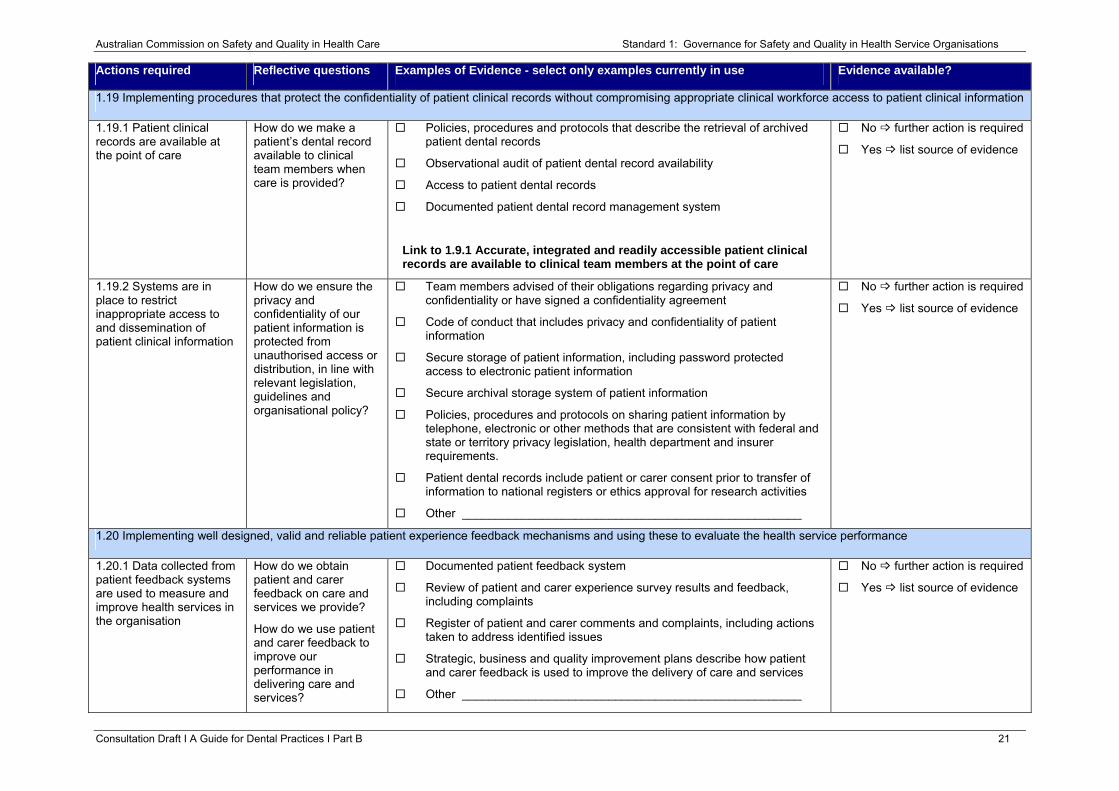
1.19 Implementing procedures that protect the confidentiality of patient clinical records without compromising appropriate clinical workforce access to patient clinical information
1.19.1 Patient clinical records are available at the point of care
How do we make a patient’s dental record available to clinical team members when care is provided?
Policies, procedures and protocols that describe the retrieval of archived patient dental records
Observational audit of patient dental record availability
Access to patient dental records
Documented patient dental record management system
Link to 1.9.1 Accurate, integrated and readily accessible patient clinical records are available to clinical team members at the point of care
No further action is required
Yes list source of evidence
1.19.2 Systems are in place to restrict inappropriate access to and dissemination of patient clinical information
How do we ensure the privacy and confidentiality of our patient information is protected from unauthorised access or distribution, in line with relevant legislation, guidelines and organisational policy?
Team members advised of their obligations regarding privacy and confidentiality or have signed a confidentiality agreement
Code of conduct that includes privacy and confidentiality of patient information
Secure storage of patient information, including password protected access to electronic patient information
Secure archival storage system of patient information
Policies, procedures and protocols on sharing patient information by telephone, electronic or other methods that are consistent with federal and state or territory privacy legislation, health department and insurer requirements.
Patient dental records include patient or carer consent prior to transfer of information to national registers or ethics approval for research activities
Other ___________________________________________________
No further action is required
Yes list source of evidence
1.20 Implementing well designed, valid and reliable patient experience feedback mechanisms and using these to evaluate the health service performance
1.20.1 Data collected from patient feedback systems are used to measure and improve health services in the organisation
How do we obtain patient and carer feedback on care and services we provide?
How do we use patient and carer feedback to improve our performance in delivering care and services?
Documented patient feedback system
Review of patient and carer experience survey results and feedback, including complaints
Register of patient and carer comments and complaints, including actions taken to address identified issues
Strategic, business and quality improvement plans describe how patient and carer feedback is used to improve the delivery of care and services
Other ___________________________________________________
No further action is required
Yes list source of evidence
Consultation Draft Ι A Guide for Dental Practices Ι Part B 21
Australian Commission on Safety and Quality in Health Care Standard 1: Governance for Safety and Quality in Health Service Organisations
Resources
1. Australian Charter of Healthcare Rights. Commonwealth of Australia, 2008. (Accessed 8 June 2012, at http://www.safetyandquality.gov.au/our-work/national-perspectives/charter-of-healthcare-rights/.)
2. Australian Safety and Quality Framework for Health Care. ACSQHC, 2010. (Accessed 8 June, 2012, at http://www.safetyandquality.gov.au/our-work/national-perspectives/australian-safety-and-quality-framework-for-health-care/.)
3. Guidelines for Good Practice on Consent for Care in Dentistry. Australian Dental Association Inc. 2005 (Accessed 28 June 2012, at http://www.ada.org.au/app_cmslib/media/lib/0703/m52394_v1_ggp2consentforcareindentistry.pdf.)
4. Guidelines for Good Practice on Emergencies in Dental Practice. Australian Dental Association Inc. 2005 (Accessed 28 June 2012, at http://www.ada.org.au/app_cmslib/media/lib/0703/m52398_v1_ggp3emergencies.pdf.)
5. Guidelines for Good Practice on Patient Information and Records. Australian Dental Association Inc. 2006 (Accessed 28 June 2012, at http://www.ada.org.au/app_cmslib/media/lib/0703/m52390_v1_ggp1patientiforecordsamended.pdf.)
6. Open Disclosure Standard: A National Standard for Open Communication in Public and Private Hospitals, Following an Adverse Event in Health Care. Canberra, 2003. (Accessed 8 June, 2012, at http://www.safetyandquality.gov.au/our-work/open-disclosure/the-open-disclosure-standard/)
7. Standard for Credentialling and Defining the Scope of Clinical Practice for Medical Practitioners. Australian Council for Safety and Quality in Health Care (Accessed 8 June 2012, 08June, at http://www.health.gov.au/internet/safety/publishing.nsf/Content/a-zpublicationss-u/$File/credentl.pdf)
Consultation Draft Ι A Guide for Dental Practices Ι Part B 22
Australian Commission on Safety and Quality in Health Care Standard 3 Preventing and Controlling Healthcare Associated Infections
Standard 2: Partnering with Consumers Leaders of a health service organisation implement systems to support partnering with patients, carers and other consumers to improve the
safety and quality of care. Patients, carers, consumers, clinicians and other members of the workforce use the systems for partnering with
consumers.
The intention of this Standard is to:
Create a health service that is responsive to patient, carer and consumer input and needs.
Context
This Standard provides the framework for active partnership with consumers by health service organisations. It is expected that this Standard will apply in conjunction with Standard 1, ‘Governance for Safety and Quality in Health Service Organisations’, in the implementation of all other Standards.
Criteria to achieve the Partnering with Consumers Standard:
• Consumer partnership in service planning
• Consumer partnership in designing care
• Consumer partnership in service measurement and evaluation
Consultation Draft Ι A Guide for Dental Practices Ι Part B 23
Australian Commission on Safety and Quality in Health Care Standard 3 Preventing and Controlling Healthcare Associated Infections
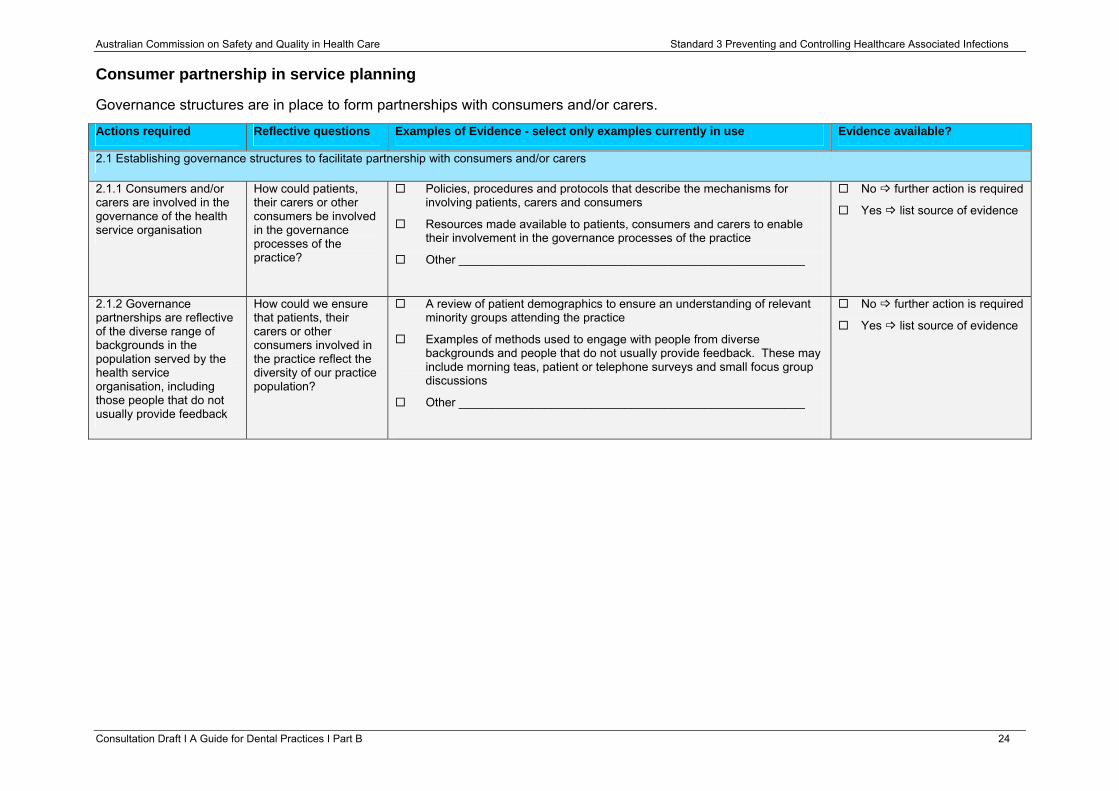
Consumer partnership in service planning
Governance structures are in place to form partnerships with consumers and/or carers.
Actions required Reflective questions Examples of Evidence - select only examples currently in use Evidence available?
2.1 Establishing governance structures to facilitate partnership with consumers and/or carers
2.1.1 Consumers and/or carers are involved in the governance of the health service organisation
How could patients, their carers or other consumers be involved in the governance processes of the practice?
Policies, procedures and protocols that describe the mechanisms for involving patients, carers and consumers
Resources made available to patients, consumers and carers to enable their involvement in the governance processes of the practice
Other ____________________________________________________
No further action is required
Yes list source of evidence
2.1.2 Governance partnerships are reflective of the diverse range of backgrounds in the population served by the health service organisation, including those people that do not usually provide feedback
How could we ensure that patients, their carers or other consumers involved in the practice reflect the diversity of our practice population?
A review of patient demographics to ensure an understanding of relevant minority groups attending the practice
Examples of methods used to engage with people from diverse backgrounds and people that do not usually provide feedback. These may include morning teas, patient or telephone surveys and small focus group discussions
Other ____________________________________________________
No further action is required
Yes list source of evidence
Consultation Draft Ι A Guide for Dental Practices Ι Part B 24
Australian Commission on Safety and Quality in Health Care Standard 3 Preventing and Controlling Healthcare Associated Infections
Actions required Reflective questions Examples of Evidence - select only examples currently in use Evidence available?
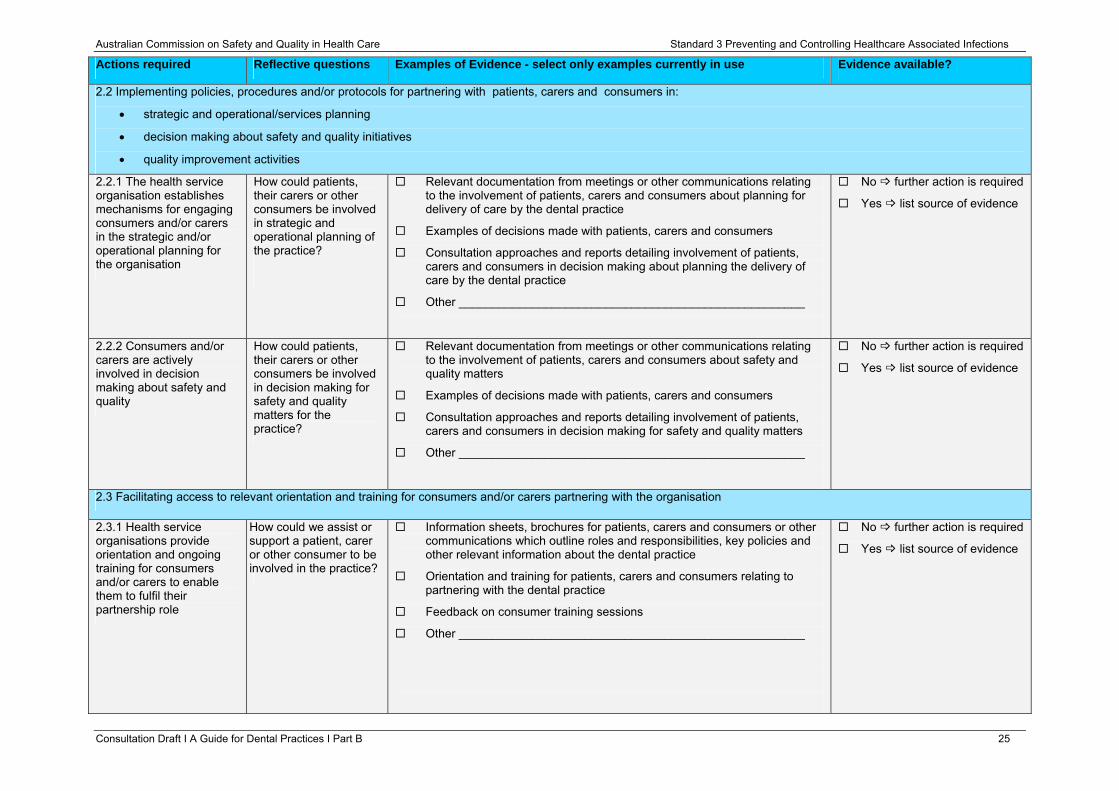
2.2 Implementing policies, procedures and/or protocols for partnering with patients, carers and consumers in:
• strategic and operational/services planning
• decision making about safety and quality initiatives
• quality improvement activities
2.2.1 The health service organisation establishes mechanisms for engaging consumers and/or carers in the strategic and/or operational planning for the organisation
How could patients, their carers or other consumers be involved in strategic and operational planning of the practice?
Relevant documentation from meetings or other communications relating to the involvement of patients, carers and consumers about planning for delivery of care by the dental practice
Examples of decisions made with patients, carers and consumers
Consultation approaches and reports detailing involvement of patients, carers and consumers in decision making about planning the delivery of care by the dental practice
Other ____________________________________________________
No further action is required
Yes list source of evidence
2.2.2 Consumers and/or carers are actively involved in decision making about safety and quality
How could patients, their carers or other consumers be involved in decision making for safety and quality matters for the practice?
Relevant documentation from meetings or other communications relating to the involvement of patients, carers and consumers about safety and quality matters
Examples of decisions made with patients, carers and consumers
Consultation approaches and reports detailing involvement of patients, carers and consumers in decision making for safety and quality matters
Other ____________________________________________________
No further action is required
Yes list source of evidence
2.3 Facilitating access to relevant orientation and training for consumers and/or carers partnering with the organisation
2.3.1 Health service organisations provide orientation and ongoing training for consumers and/or carers to enable them to fulfil their partnership role
How could we assist or support a patient, carer or other consumer to be involved in the practice?
Information sheets, brochures for patients, carers and consumers or other communications which outline roles and responsibilities, key policies and other relevant information about the dental practice
Orientation and training for patients, carers and consumers relating to partnering with the dental practice
Feedback on consumer training sessions
Other ____________________________________________________
No further action is required
Yes list source of evidence
Consultation Draft Ι A Guide for Dental Practices Ι Part B 25
Australian Commission on Safety and Quality in Health Care Standard 3 Preventing and Controlling Healthcare Associated Infections
Actions required Reflective questions Examples of Evidence - select only examples currently in use Evidence available?
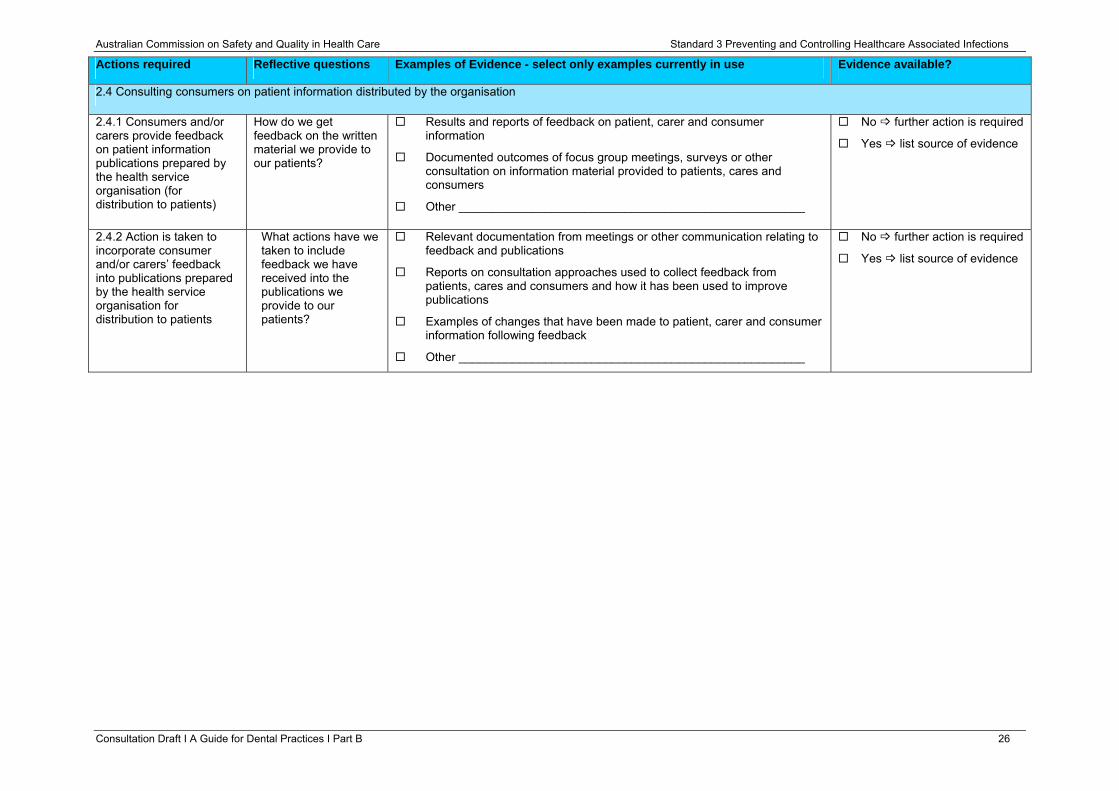
2.4 Consulting consumers on patient information distributed by the organisation
2.4.1 Consumers and/or carers provide feedback on patient information publications prepared by the health service organisation (for distribution to patients)
How do we get feedback on the written material we provide to our patients?
Results and reports of feedback on patient, carer and consumer information
Documented outcomes of focus group meetings, surveys or other consultation on information material provided to patients, cares and consumers
Other ____________________________________________________
No further action is required
Yes list source of evidence
2.4.2 Action is taken to incorporate consumer and/or carers’ feedback into publications prepared by the health service organisation for distribution to patients
What actions have we taken to include feedback we have received into the publications we provide to our patients?
Relevant documentation from meetings or other communication relating to feedback and publications
Reports on consultation approaches used to collect feedback from patients, cares and consumers and how it has been used to improve publications
Examples of changes that have been made to patient, carer and consumer information following feedback
Other ____________________________________________________
No further action is required
Yes list source of evidence
Consultation Draft Ι A Guide for Dental Practices Ι Part B 26
Australian Commission on Safety and Quality in Health Care Standard 3 Preventing and Controlling Healthcare Associated Infections
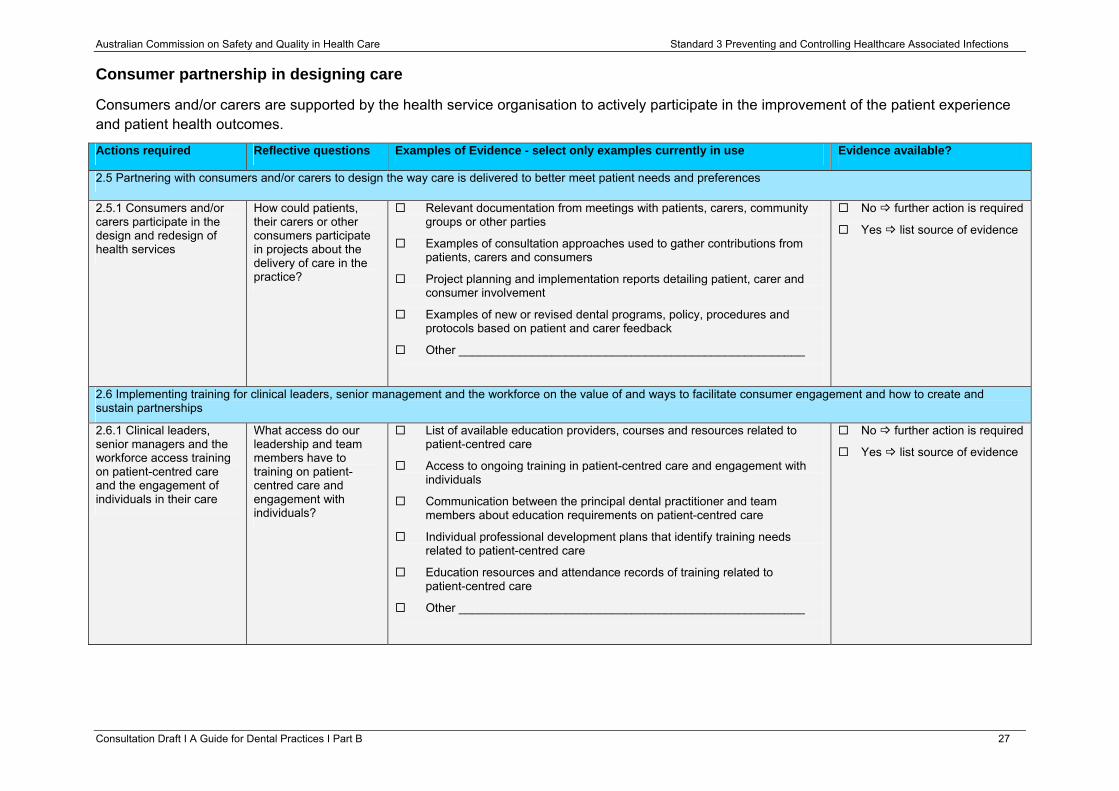
Consumer partnership in designing care
Consumers and/or carers are supported by the health service organisation to actively participate in the improvement of the patient experience and patient health outcomes.
Actions required Reflective questions Examples of Evidence - select only examples currently in use Evidence available?
2.5 Partnering with consumers and/or carers to design the way care is delivered to better meet patient needs and preferences
2.5.1 Consumers and/or carers participate in the design and redesign of health services
How could patients, their carers or other consumers participate in projects about the delivery of care in the practice?
Relevant documentation from meetings with patients, carers, community groups or other parties
Examples of consultation approaches used to gather contributions from patients, carers and consumers
Project planning and implementation reports detailing patient, carer and consumer involvement
Examples of new or revised dental programs, policy, procedures and protocols based on patient and carer feedback
Other ____________________________________________________
No further action is required
Yes list source of evidence
2.6 Implementing training for clinical leaders, senior management and the workforce on the value of and ways to facilitate consumer engagement and how to create and sustain partnerships
2.6.1 Clinical leaders, senior managers and the workforce access training on patient-centred care and the engagement of individuals in their care
What access do our leadership and team members have to training on patient-centred care and engagement with individuals?
List of available education providers, courses and resources related to patient-centred care
Access to ongoing training in patient-centred care and engagement with individuals
Communication between the principal dental practitioner and team members about education requirements on patient-centred care
Individual professional development plans that identify training needs related to patient-centred care
Education resources and attendance records of training related to patient-centred care
Other ____________________________________________________
No further action is required
Yes list source of evidence
Consultation Draft Ι A Guide for Dental Practices Ι Part B 27
Australian Commission on Safety and Quality in Health Care Standard 3 Preventing and Controlling Healthcare Associated Infections
Actions required Reflective questions Examples of Evidence - select only examples currently in use Evidence available?
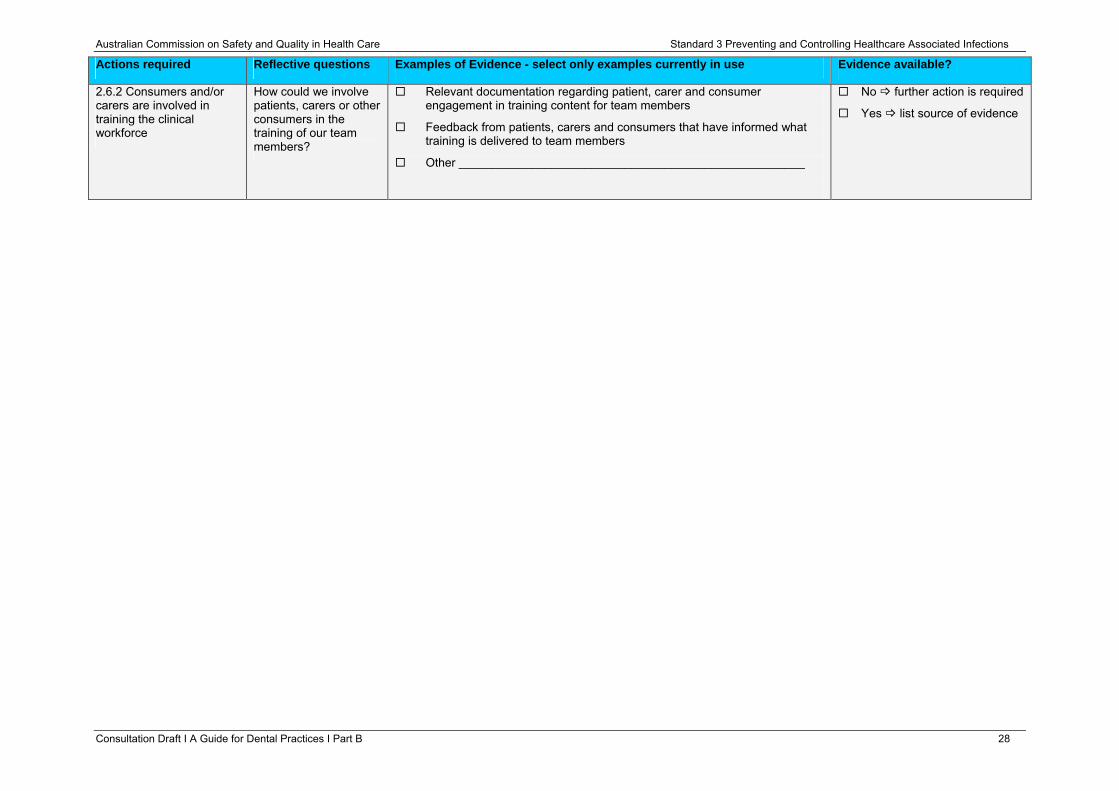
2.6.2 Consumers and/or carers are involved in training the clinical workforce
How could we involve patients, carers or other consumers in the training of our team members?
Relevant documentation regarding patient, carer and consumer engagement in training content for team members
Feedback from patients, carers and consumers that have informed what training is delivered to team members
Other ____________________________________________________
No further action is required
Yes list source of evidence
Consultation Draft Ι A Guide for Dental Practices Ι Part B 28
Australian Commission on Safety and Quality in Health Care Standard 3 Preventing and Controlling Healthcare Associated Infections
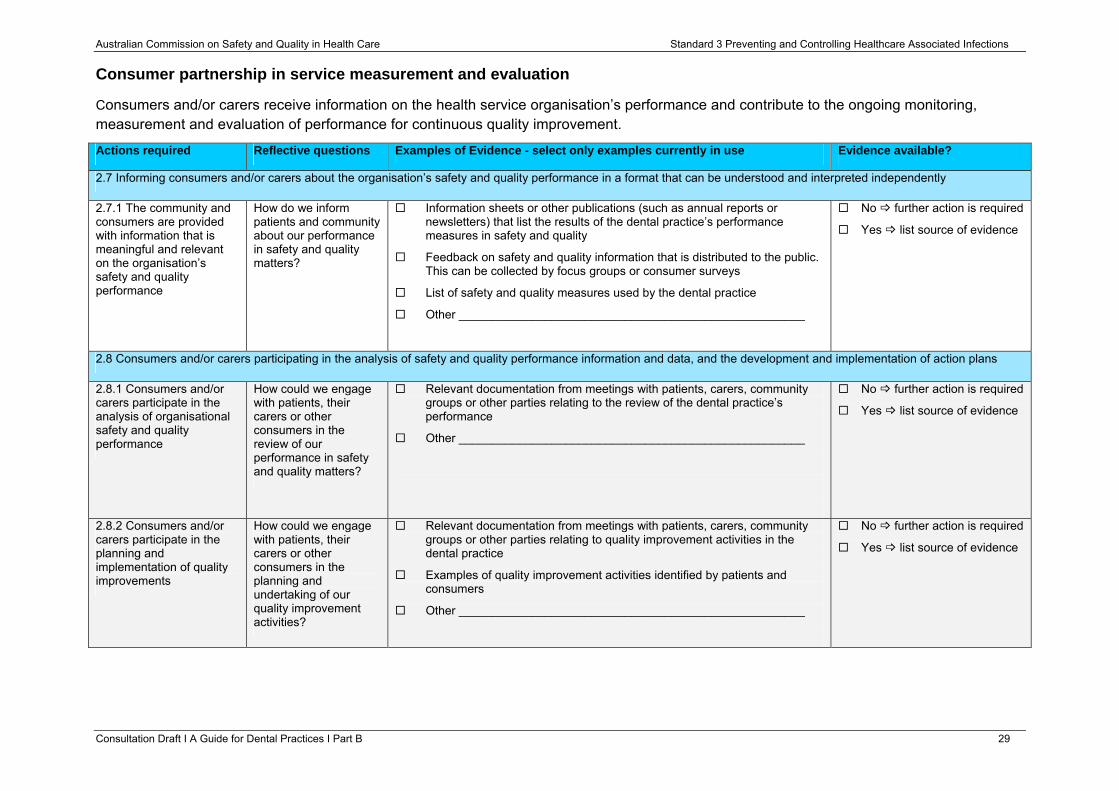
Consumer partnership in service measurement and evaluation
Consumers and/or carers receive information on the health service organisation’s performance and contribute to the ongoing monitoring, measurement and evaluation of performance for continuous quality improvement.
Actions required Reflective questions Examples of Evidence - select only examples currently in use Evidence available?
2.7 Informing consumers and/or carers about the organisation’s safety and quality performance in a format that can be understood and interpreted independently
2.7.1 The community and consumers are provided with information that is meaningful and relevant on the organisation’s safety and quality performance
How do we inform patients and community about our performance in safety and quality matters?
Information sheets or other publications (such as annual reports or newsletters) that list the results of the dental practice’s performance measures in safety and quality
Feedback on safety and quality information that is distributed to the public. This can be collected by focus groups or consumer surveys
List of safety and quality measures used by the dental practice
Other ____________________________________________________
No further action is required
Yes list source of evidence
2.8 Consumers and/or carers participating in the analysis of safety and quality performance information and data, and the development and implementation of action plans
2.8.1 Consumers and/or carers participate in the analysis of organisational safety and quality performance
How could we engage with patients, their carers or other consumers in the review of our performance in safety and quality matters?
Relevant documentation from meetings with patients, carers, community groups or other parties relating to the review of the dental practice’s performance
Other ____________________________________________________
No further action is required
Yes list source of evidence
2.8.2 Consumers and/or carers participate in the planning and implementation of quality improvements
How could we engage with patients, their carers or other consumers in the planning and undertaking of our quality improvement activities?
Relevant documentation from meetings with patients, carers, community groups or other parties relating to quality improvement activities in the dental practice
Examples of quality improvement activities identified by patients and consumers
Other ____________________________________________________
No further action is required
Yes list source of evidence
Consultation Draft Ι A Guide for Dental Practices Ι Part B 29
Australian Commission on Safety and Quality in Health Care Standard 3 Preventing and Controlling Healthcare Associated Infections
Actions required Reflective questions Examples of Evidence - select only examples currently in use Evidence available?
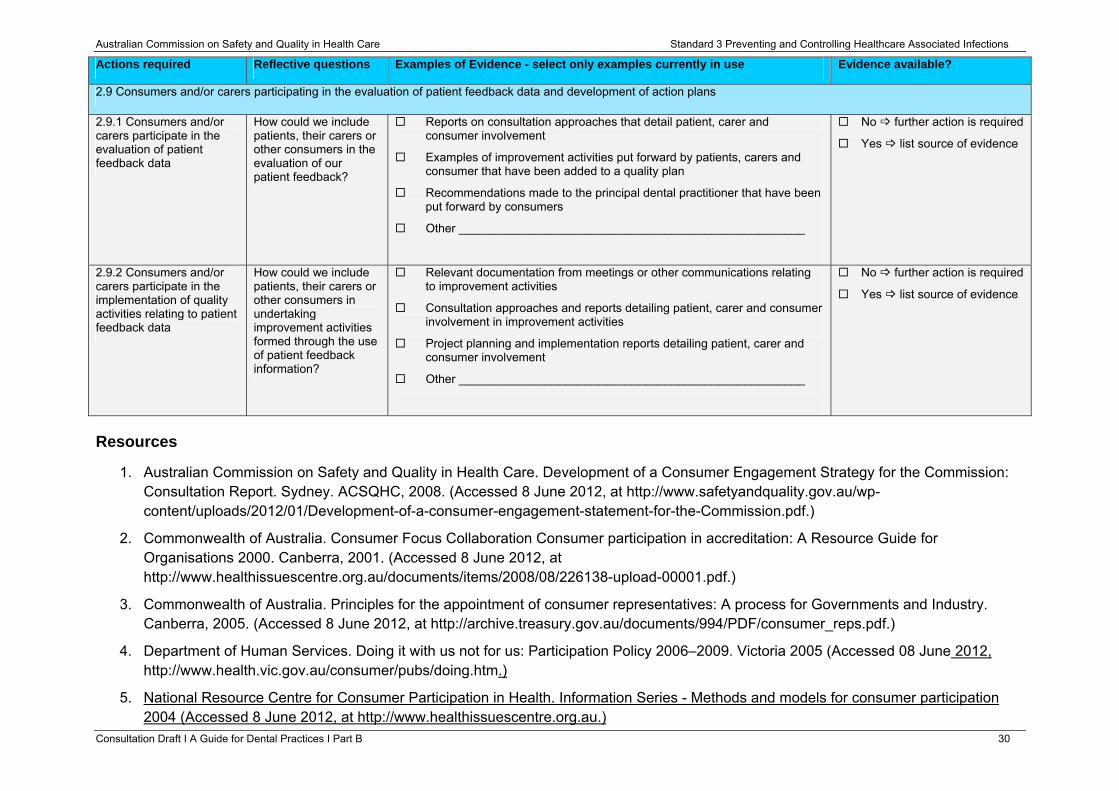
2.9 Consumers and/or carers participating in the evaluation of patient feedback data and development of action plans
2.9.1 Consumers and/or carers participate in the evaluation of patient feedback data
How could we include patients, their carers or other consumers in the evaluation of our patient feedback?
Reports on consultation approaches that detail patient, carer and consumer involvement
Examples of improvement activities put forward by patients, carers and consumer that have been added to a quality plan
Recommendations made to the principal dental practitioner that have been put forward by consumers
Other ____________________________________________________
No further action is required
Yes list source of evidence
2.9.2 Consumers and/or carers participate in the implementation of quality activities relating to patient feedback data
How could we include patients, their carers or other consumers in undertaking improvement activities formed through the use of patient feedback information?
Relevant documentation from meetings or other communications relating to improvement activities
Consultation approaches and reports detailing patient, carer and consumer involvement in improvement activities
Project planning and implementation reports detailing patient, carer and consumer involvement
Other ____________________________________________________
No further action is required
Yes list source of evidence
Resources
1. Australian Commission on Safety and Quality in Health Care. Development of a Consumer Engagement Strategy for the Commission: Consultation Report. Sydney. ACSQHC, 2008. (Accessed 8 June 2012, at http://www.safetyandquality.gov.au/wp-content/uploads/2012/01/Development-of-a-consumer-engagement-statement-for-the-Commission.pdf.)
2. Commonwealth of Australia. Consumer Focus Collaboration Consumer participation in accreditation: A Resource Guide for Organisations 2000. Canberra, 2001. (Accessed 8 June 2012, at http://www.healthissuescentre.org.au/documents/items/2008/08/226138-upload-00001.pdf.)
3. Commonwealth of Australia. Principles for the appointment of consumer representatives: A process for Governments and Industry. Canberra, 2005. (Accessed 8 June 2012, at http://archive.treasury.gov.au/documents/994/PDF/consumer_reps.pdf.)
4. Department of Human Services. Doing it with us not for us: Participation Policy 2006–2009. Victoria 2005 (Accessed 08 June 2012, http://www.health.vic.gov.au/consumer/pubs/doing.htm.)
5. National Resource Centre for Consumer Participation in Health. Information Series - Methods and models for consumer participation 2004 (Accessed 8 June 2012, at http://www.healthissuescentre.org.au.)
Consultation Draft Ι A Guide for Dental Practices Ι Part B 30
Australian Commission on Safety and Quality in Health Care Standard 3 Preventing and Controlling Healthcare Associated Infections
Standard 3: Preventing and Controlling Healthcare Associated Infections: Clinical leaders and senior managers of a health service organisation implement systems to prevent and manage healthcare associated infections and communicate these to all workforce to achieve appropriate outcomes. Clinicians and other members of the workforce use the healthcare associated infection prevention and control systems.
The intention of this Standard is to:
Prevent patients from acquiring preventable healthcare associated infections and effectively manage infections when they occur by using evidence-based strategies.
Context
It is expected that this Standard will be applied in conjunction with Standard 1, ‘Governance for Safety and Quality in Health Service Organisations requirements’ and Standard 2, ‘Partnering with Consumers’.
Criteria to achieve the Preventing and Controlling Healthcare Associated Infections Standard:
• Governance and systems for infection prevention, control and surveillance
• Infection prevention and control strategies
• Managing patients with infections or colonisations
• Antimicrobial stewardship
• Cleaning, disinfection and sterilisation
• Communicating with patients and carers
Consultation Draft Ι A Guide for Dental Practices Ι Part B 31
Australian Commission on Safety and Quality in Health Care Standard 3 Preventing and Controlling Healthcare Associated Infections
Governance and systems for infection prevention, control and surveillance
Effective governance and management systems for healthcare associated infections are implemented and maintained.
Actions required Reflective questions Examples of Evidence - select only examples currently in use Evidence available?
3.1 Developing and implementing governance systems for effective infection prevention and control to minimise the risk to patients of healthcare associated infections
3.1.1 A risk management approach is taken when implementing policies, procedures and/or protocols for:
• standard infection control precautions
• transmission-based precautions
• aseptic technique
• safe handling and disposal of sharps
• prevention and management of occupational exposure to blood and body substances
• environmental cleaning and disinfection
• antimicrobial prescribing
• outbreaks or unusual clusters of communicable infection
• processing of reusable medical devices
• single-use devices
• surveillance and reporting of data
Are our infection prevention and control policies, procedures and protocols consistent with national guidelines?
How do our policies, procedures and protocols for infection prevention and control ensure risks are identified and managed?
Policies, procedures and protocols that address items listed in 3.1.1 are accessible to team members and included in the practice infection prevention and control manual. They:
• are referenced to the Australian Guidelines for the Prevention and Control of Infections in Health Care, best practice, regulatory and legislative requirements, and relevant jurisdictional protocols
• provide links to relevant resource materials
• include a register of completed reviews and the date of any changes made
Risk assessment tools used in the dental practice
Other _____________________________________________________
Links to Standards 1: Governance for Safety and Quality in Health Service Organisations
No further action is required
Yes list source of evidence
Consultation Draft Ι A Guide for Dental Practices Ι Part B 32
Australian Commission on Safety and Quality in Health Care Standard 3 Preventing and Controlling Healthcare Associated Infections
Actions required Reflective questions Examples of Evidence - select only examples currently in use Evidence available?
where relevant
• reporting of communicable and notifiable diseases
• provision of risk assessment guidelines to workforce
• exposure-prone procedures
3.1.2 The use of policies, procedures and/or protocols is regularly monitored
How do we find out if our infection prevention and control measures are being used by our team?
Relevant documentation from meetings or other communications relating to monitoring of infection control measures
Audit checklist, or other documentation, that demonstrates the dental practice is monitoring compliance with its infection control policy on a periodic basis
Declaration by team members that they comply with infection control measures
Observational audit of infection control measures in use
Other _____________________________________________________
No further action is required
Yes list source of evidence
3.1.3 The effectiveness of the infection prevention and control systems is regularly reviewed at the highest level of governance in the organisation
How does our leadership know about our performance in infection prevention and control measures?
Relevant documentation from meetings or other communications to leadership that relate to monitoring of infection prevention and control measures
Checklists, memos or other documentation that demonstrates the principal dental practitioner monitors and reviews the effectiveness of the practice’s systems
Reports of interventions that have been initiated for identified risks in infection prevention and control systems
Other _____________________________________________________
No further action is required
Yes list source of evidence
3.1.4 Action is taken to improve the effectiveness of infection prevention and control policies, procedures and/or protocols
What action have we taken to improve the outcomes of our infection prevention and control performance?
Policies, procedures and protocols on infection control are accessible to team members
Infrastructure (such as hand basins), instruments (such as sterile packs) and other equipment (such as solutions, sharp containers) necessary to comply with practice polices, procedures and protocols are available to team members
Register of quality improvement actions and activities undertaken in infection control practices
No further action is required
Yes list source of evidence
Consultation Draft Ι A Guide for Dental Practices Ι Part B 33
Australian Commission on Safety and Quality in Health Care Standard 3 Preventing and Controlling Healthcare Associated Infections
Actions required Reflective questions Examples of Evidence - select only examples currently in use Evidence available?
Attendance records for education and training in infection control updates
Other _____________________________________________________
3.2 Undertaking surveillance of healthcare associated infections
3.2.1 Surveillance systems for healthcare associated infections are in place
How do we identify our health care associated infections?
Reports of specific trends relating to healthcare associated infections, for example:
• Needle stick injuries reported over a period
• Surveillance systems for infections on discharge for specified practice surgical procedures (if appropriate)
• Non line-associated blood stream infections (this may be applicable in a dental practice, however the patient may need medical management in a hospital setting)
• Antimicrobial resistant organisms (this may be applicable in a dental practice and will require medical management)
Other _____________________________________________________
No further action is required
Yes list source of evidence
3.2.2 Healthcare associated infections surveillance data are regularly monitored by the delegated workforce and/or committees
How is healthcare associated infection data reported in the practice?
Relevant documentation from meetings and other communications that relate to healthcare associated infection surveillance. This can include meetings with team members or the work health and safety committee
Reports or reviews for the principal dental practitioner on the frequency of exposure incidents, such as sharps injuries
Indicator reports on occupational exposures reviewed by leadership or the work health and safety committee
Other _____________________________________________________
No further action is required
Yes list source of evidence
Consultation Draft Ι A Guide for Dental Practices Ι Part B 34
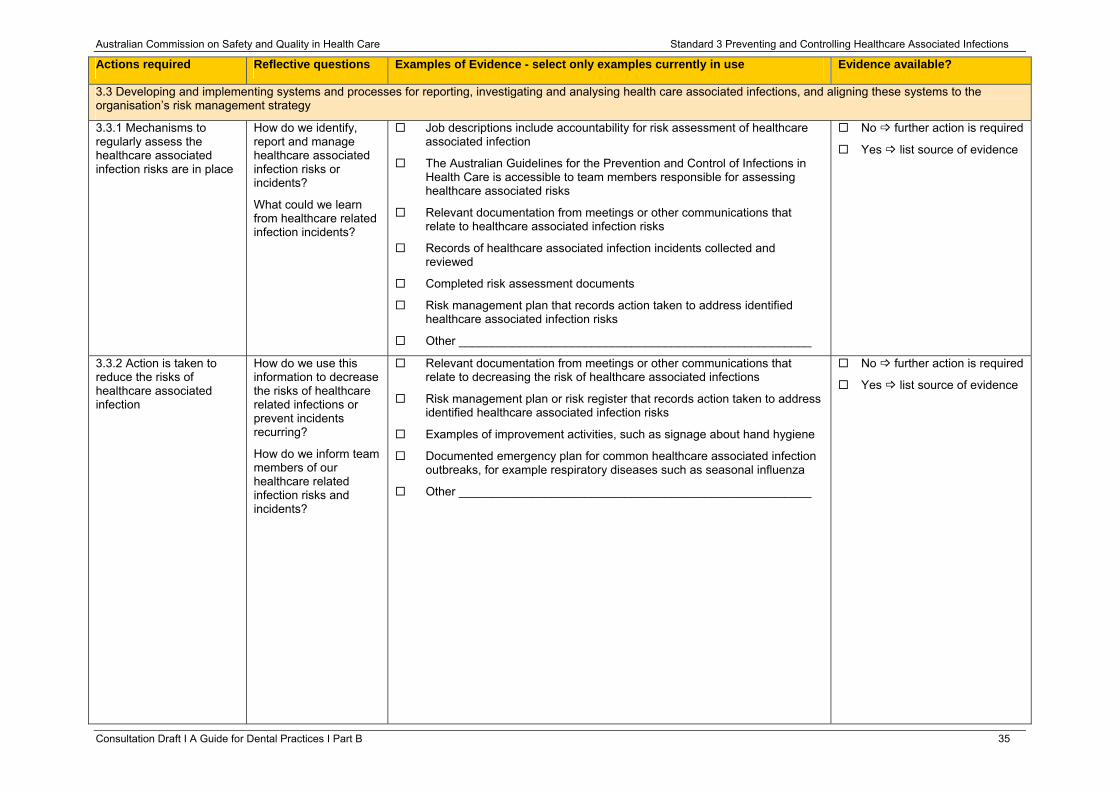
Australian Commission on Safety and Quality in Health Care Standard 3 Preventing and Controlling Healthcare Associated Infections
Actions required Reflective questions Examples of Evidence - select only examples currently in use Evidence available?
3.3 Developing and implementing systems and processes for reporting, investigating and analysing health care associated infections, and aligning these systems to the organisation’s risk management strategy
3.3.1 Mechanisms to regularly assess the healthcare associated infection risks are in place
How do we identify, report and manage healthcare associated infection risks or incidents?
What could we learn from healthcare related infection incidents?
Job descriptions include accountability for risk assessment of healthcare associated infection
The Australian Guidelines for the Prevention and Control of Infections in Health Care is accessible to team members responsible for assessing healthcare associated risks
Relevant documentation from meetings or other communications that relate to healthcare associated infection risks
Records of healthcare associated infection incidents collected and reviewed
Completed risk assessment documents
Risk management plan that records action taken to address identified healthcare associated infection risks
Other _____________________________________________________
No further action is required
Yes list source of evidence
3.3.2 Action is taken to reduce the risks of healthcare associated infection
How do we use this information to decrease the risks of healthcare related infections or prevent incidents recurring?
How do we inform team members of our healthcare related infection risks and incidents?
Relevant documentation from meetings or other communications that relate to decreasing the risk of healthcare associated infections
Risk management plan or risk register that records action taken to address identified healthcare associated infection risks
Examples of improvement activities, such as signage about hand hygiene
Documented emergency plan for common healthcare associated infection outbreaks, for example respiratory diseases such as seasonal influenza
Other _____________________________________________________
No further action is required
Yes list source of evidence
Consultation Draft Ι A Guide for Dental Practices Ι Part B 35
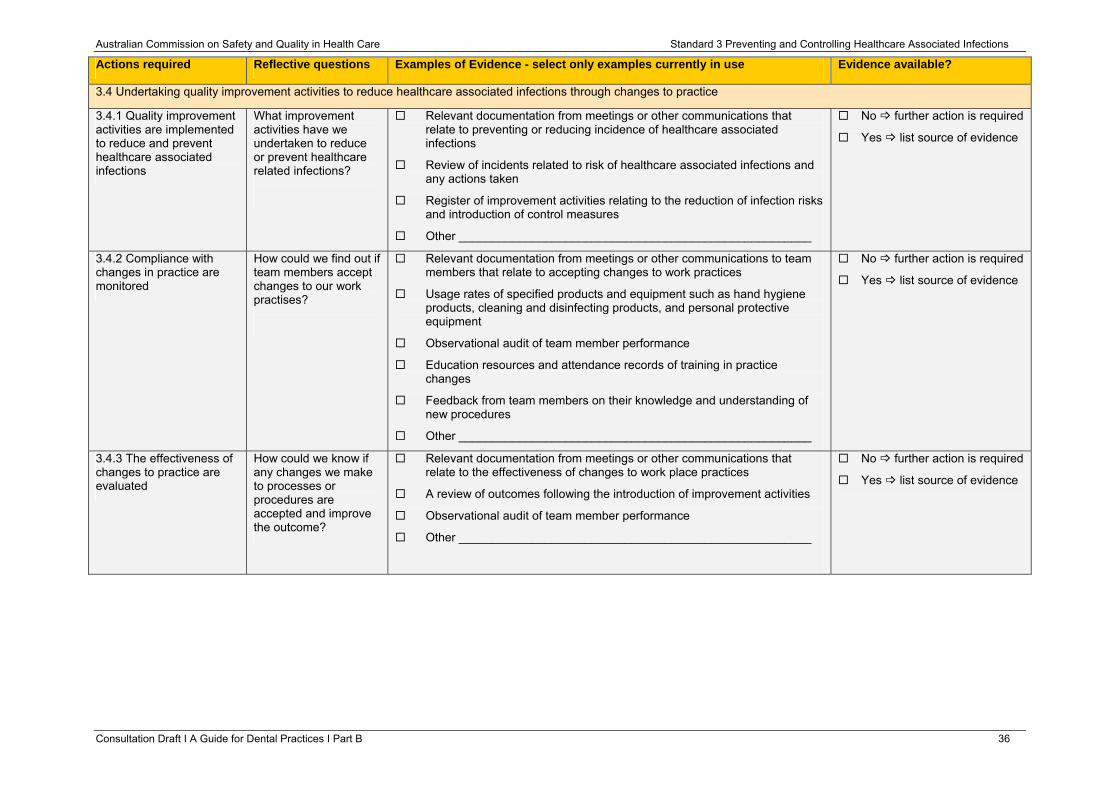
Australian Commission on Safety and Quality in Health Care Standard 3 Preventing and Controlling Healthcare Associated Infections
Actions required Reflective questions Examples of Evidence - select only examples currently in use Evidence available?
3.4 Undertaking quality improvement activities to reduce healthcare associated infections through changes to practice
3.4.1 Quality improvement activities are implemented to reduce and prevent healthcare associated infections
What improvement activities have we undertaken to reduce or prevent healthcare related infections?
Relevant documentation from meetings or other communications that relate to preventing or reducing incidence of healthcare associated infections
Review of incidents related to risk of healthcare associated infections and any actions taken
Register of improvement activities relating to the reduction of infection risks and introduction of control measures
Other _____________________________________________________
No further action is required
Yes list source of evidence
3.4.2 Compliance with changes in practice are monitored
How could we find out if team members accept changes to our work practises?
Relevant documentation from meetings or other communications to team members that relate to accepting changes to work practices
Usage rates of specified products and equipment such as hand hygiene products, cleaning and disinfecting products, and personal protective equipment
Observational audit of team member performance
Education resources and attendance records of training in practice changes
Feedback from team members on their knowledge and understanding of new procedures
Other _____________________________________________________
No further action is required
Yes list source of evidence
3.4.3 The effectiveness of changes to practice are evaluated
How could we know if any changes we make to processes or procedures are accepted and improve the outcome?
Relevant documentation from meetings or other communications that relate to the effectiveness of changes to work place practices
A review of outcomes following the introduction of improvement activities
Observational audit of team member performance
Other _____________________________________________________
No further action is required
Yes list source of evidence
Consultation Draft Ι A Guide for Dental Practices Ι Part B 36
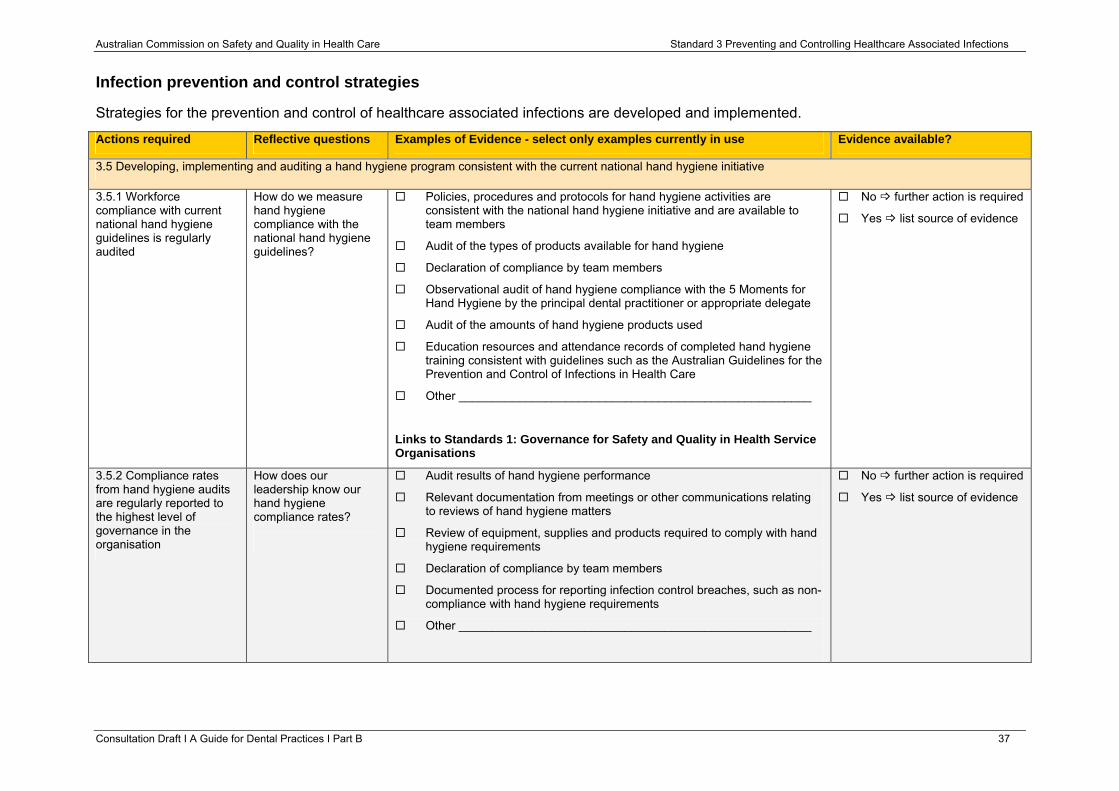
Australian Commission on Safety and Quality in Health Care Standard 3 Preventing and Controlling Healthcare Associated Infections
Infection prevention and control strategies
Strategies for the prevention and control of healthcare associated infections are developed and implemented.
Actions required Reflective questions Examples of Evidence - select only examples currently in use Evidence available?
3.5 Developing, implementing and auditing a hand hygiene program consistent with the current national hand hygiene initiative
3.5.1 Workforce compliance with current national hand hygiene guidelines is regularly audited
How do we measure hand hygiene compliance with the national hand hygiene guidelines?
Policies, procedures and protocols for hand hygiene activities are consistent with the national hand hygiene initiative and are available to team members
Audit of the types of products available for hand hygiene
Declaration of compliance by team members
Observational audit of hand hygiene compliance with the 5 Moments for Hand Hygiene by the principal dental practitioner or appropriate delegate
Audit of the amounts of hand hygiene products used
Education resources and attendance records of completed hand hygiene training consistent with guidelines such as the Australian Guidelines for the Prevention and Control of Infections in Health Care
Other _____________________________________________________
Links to Standards 1: Governance for Safety and Quality in Health Service Organisations
No further action is required
Yes list source of evidence
3.5.2 Compliance rates from hand hygiene audits are regularly reported to the highest level of governance in the organisation
How does our leadership know our hand hygiene compliance rates?
Audit results of hand hygiene performance
Relevant documentation from meetings or other communications relating to reviews of hand hygiene matters
Review of equipment, supplies and products required to comply with hand hygiene requirements
Declaration of compliance by team members
Documented process for reporting infection control breaches, such as non-compliance with hand hygiene requirements
Other _____________________________________________________
No further action is required
Yes list source of evidence
Consultation Draft Ι A Guide for Dental Practices Ι Part B 37
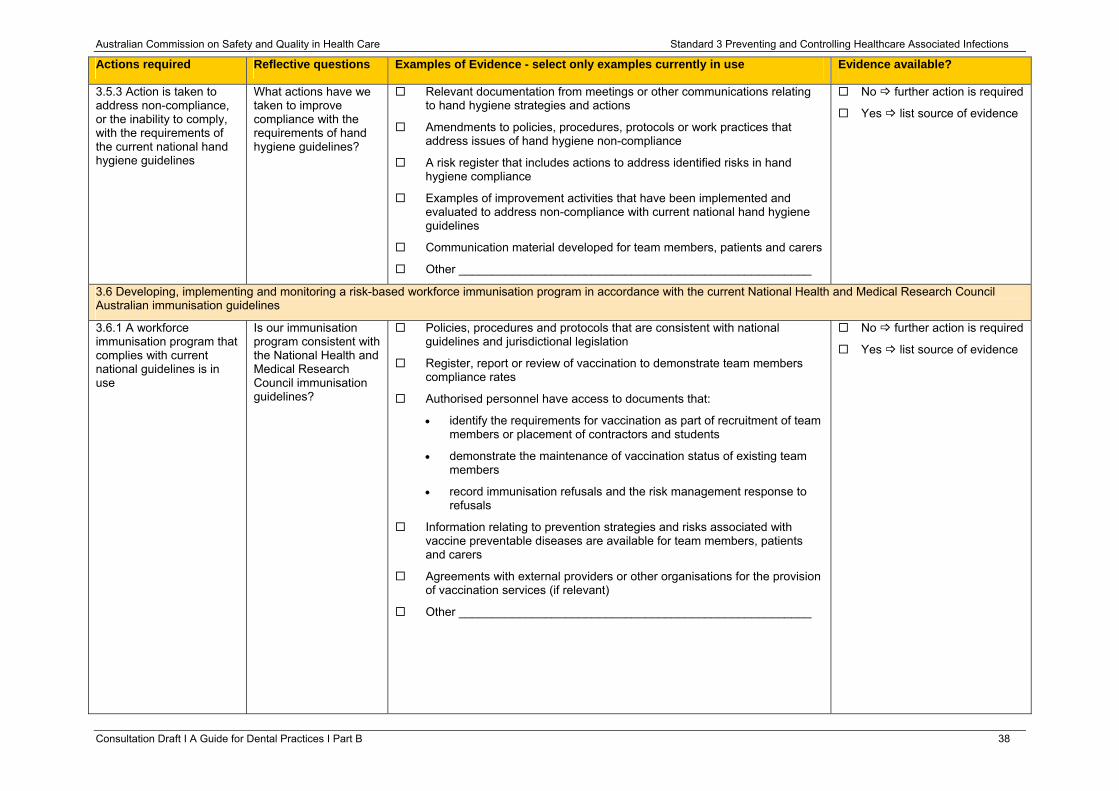
Australian Commission on Safety and Quality in Health Care Standard 3 Preventing and Controlling Healthcare Associated Infections
Actions required Reflective questions Examples of Evidence - select only examples currently in use Evidence available?
3.5.3 Action is taken to address non-compliance, or the inability to comply, with the requirements of the current national hand hygiene guidelines
What actions have we taken to improve compliance with the requirements of hand hygiene guidelines?
Relevant documentation from meetings or other communications relating to hand hygiene strategies and actions
Amendments to policies, procedures, protocols or work practices that address issues of hand hygiene non-compliance
A risk register that includes actions to address identified risks in hand hygiene compliance
Examples of improvement activities that have been implemented and evaluated to address non-compliance with current national hand hygiene guidelines
Communication material developed for team members, patients and carers
Other _____________________________________________________
No further action is required
Yes list source of evidence
3.6 Developing, implementing and monitoring a risk-based workforce immunisation program in accordance with the current National Health and Medical Research Council Australian immunisation guidelines
3.6.1 A workforce immunisation program that complies with current national guidelines is in use
Is our immunisation program consistent with the National Health and Medical Research Council immunisation guidelines?
Policies, procedures and protocols that are consistent with national guidelines and jurisdictional legislation
Register, report or review of vaccination to demonstrate team members compliance rates
Authorised personnel have access to documents that:
• identify the requirements for vaccination as part of recruitment of team members or placement of contractors and students
• demonstrate the maintenance of vaccination status of existing team members
• record immunisation refusals and the risk management response to refusals
Information relating to prevention strategies and risks associated with vaccine preventable diseases are available for team members, patients and carers
Agreements with external providers or other organisations for the provision of vaccination services (if relevant)
Other _____________________________________________________
No further action is required
Yes list source of evidence
Consultation Draft Ι A Guide for Dental Practices Ι Part B 38
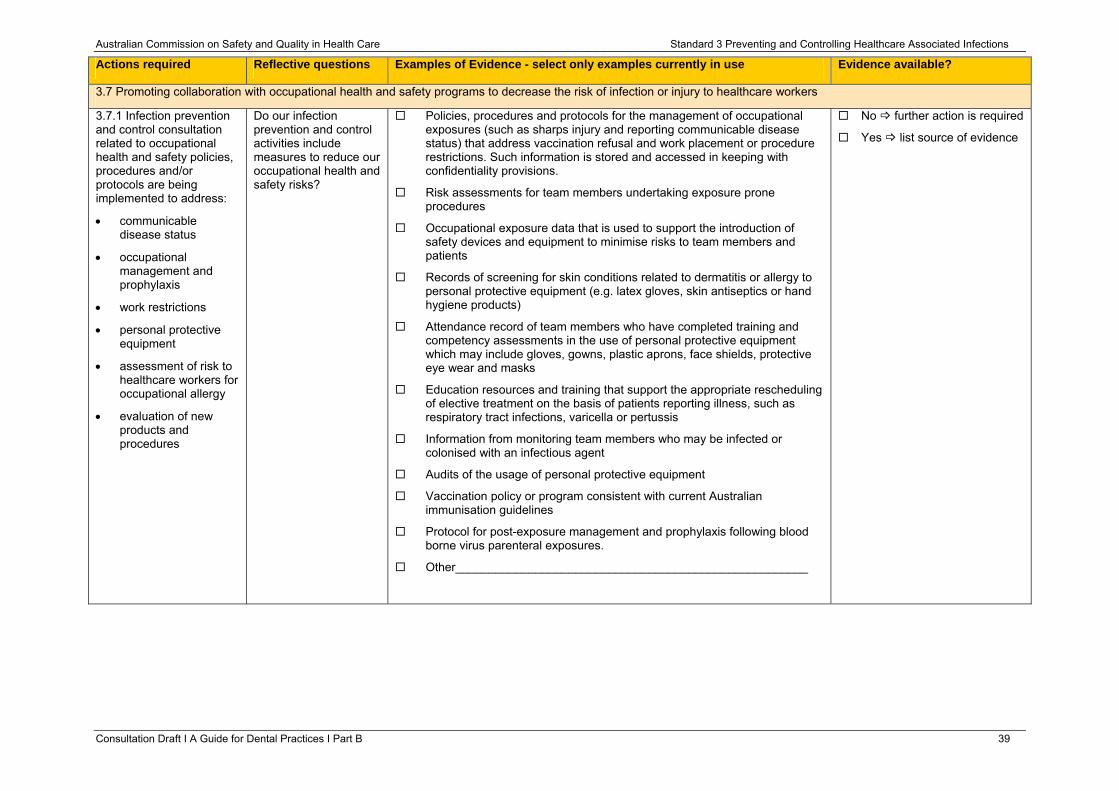
Australian Commission on Safety and Quality in Health Care Standard 3 Preventing and Controlling Healthcare Associated Infections
Actions required Reflective questions Examples of Evidence - select only examples currently in use Evidence available?
3.7 Promoting collaboration with occupational health and safety programs to decrease the risk of infection or injury to healthcare workers
3.7.1 Infection prevention and control consultation related to occupational health and safety policies, procedures and/or protocols are being implemented to address:
• communicable disease status
• occupational management and prophylaxis
• work restrictions
• personal protective equipment
• assessment of risk to healthcare workers for occupational allergy
• evaluation of new products and procedures
Do our infection prevention and control activities include measures to reduce our occupational health and safety risks?
Policies, procedures and protocols for the management of occupational exposures (such as sharps injury and reporting communicable disease status) that address vaccination refusal and work placement or procedure restrictions. Such information is stored and accessed in keeping with confidentiality provisions.
Risk assessments for team members undertaking exposure prone procedures
Occupational exposure data that is used to support the introduction of safety devices and equipment to minimise risks to team members and patients
Records of screening for skin conditions related to dermatitis or allergy to personal protective equipment (e.g. latex gloves, skin antiseptics or hand hygiene products)
Attendance record of team members who have completed training and competency assessments in the use of personal protective equipment which may include gloves, gowns, plastic aprons, face shields, protective eye wear and masks
Education resources and training that support the appropriate rescheduling of elective treatment on the basis of patients reporting illness, such as respiratory tract infections, varicella or pertussis
Information from monitoring team members who may be infected or colonised with an infectious agent
Audits of the usage of personal protective equipment
Vaccination policy or program consistent with current Australian immunisation guidelines
Protocol for post-exposure management and prophylaxis following blood borne virus parenteral exposures.
Other_____________________________________________________
No further action is required
Yes list source of evidence
Consultation Draft Ι A Guide for Dental Practices Ι Part B 39
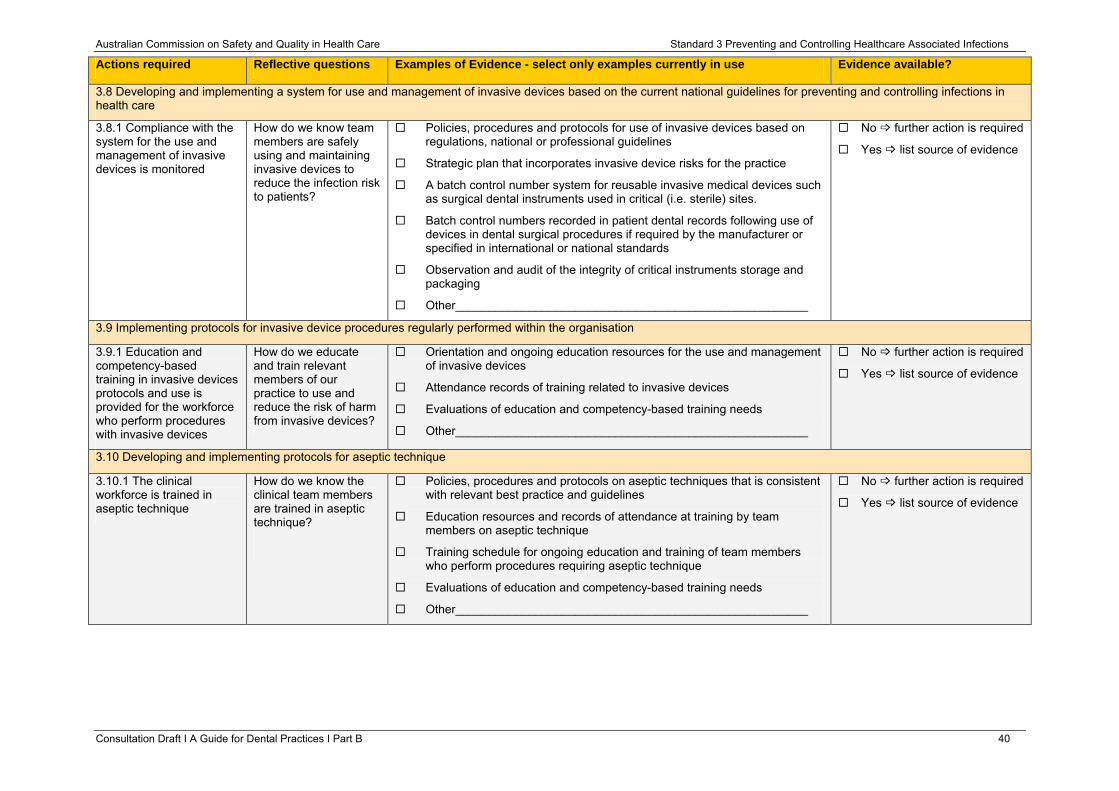
Australian Commission on Safety and Quality in Health Care Standard 3 Preventing and Controlling Healthcare Associated Infections
Actions required Reflective questions Examples of Evidence - select only examples currently in use Evidence available?
3.8 Developing and implementing a system for use and management of invasive devices based on the current national guidelines for preventing and controlling infections in health care
3.8.1 Compliance with the system for the use and management of invasive devices is monitored
How do we know team members are safely using and maintaining invasive devices to reduce the infection risk to patients?
Policies, procedures and protocols for use of invasive devices based on regulations, national or professional guidelines
Strategic plan that incorporates invasive device risks for the practice
A batch control number system for reusable invasive medical devices such as surgical dental instruments used in critical (i.e. sterile) sites.
Batch control numbers recorded in patient dental records following use of devices in dental surgical procedures if required by the manufacturer or specified in international or national standards
Observation and audit of the integrity of critical instruments storage and packaging
Other_____________________________________________________
No further action is required
Yes list source of evidence
3.9 Implementing protocols for invasive device procedures regularly performed within the organisation
3.9.1 Education and competency-based training in invasive devices protocols and use is provided for the workforce who perform procedures with invasive devices
How do we educate and train relevant members of our practice to use and reduce the risk of harm from invasive devices?
Orientation and ongoing education resources for the use and management of invasive devices
Attendance records of training related to invasive devices
Evaluations of education and competency-based training needs
Other_____________________________________________________
No further action is required
Yes list source of evidence
3.10 Developing and implementing protocols for aseptic technique
3.10.1 The clinical workforce is trained in aseptic technique
How do we know the clinical team members are trained in aseptic technique?
Policies, procedures and protocols on aseptic techniques that is consistent with relevant best practice and guidelines
Education resources and records of attendance at training by team members on aseptic technique
Training schedule for ongoing education and training of team members who perform procedures requiring aseptic technique
Evaluations of education and competency-based training needs
Other_____________________________________________________
No further action is required
Yes list source of evidence
Consultation Draft Ι A Guide for Dental Practices Ι Part B 40
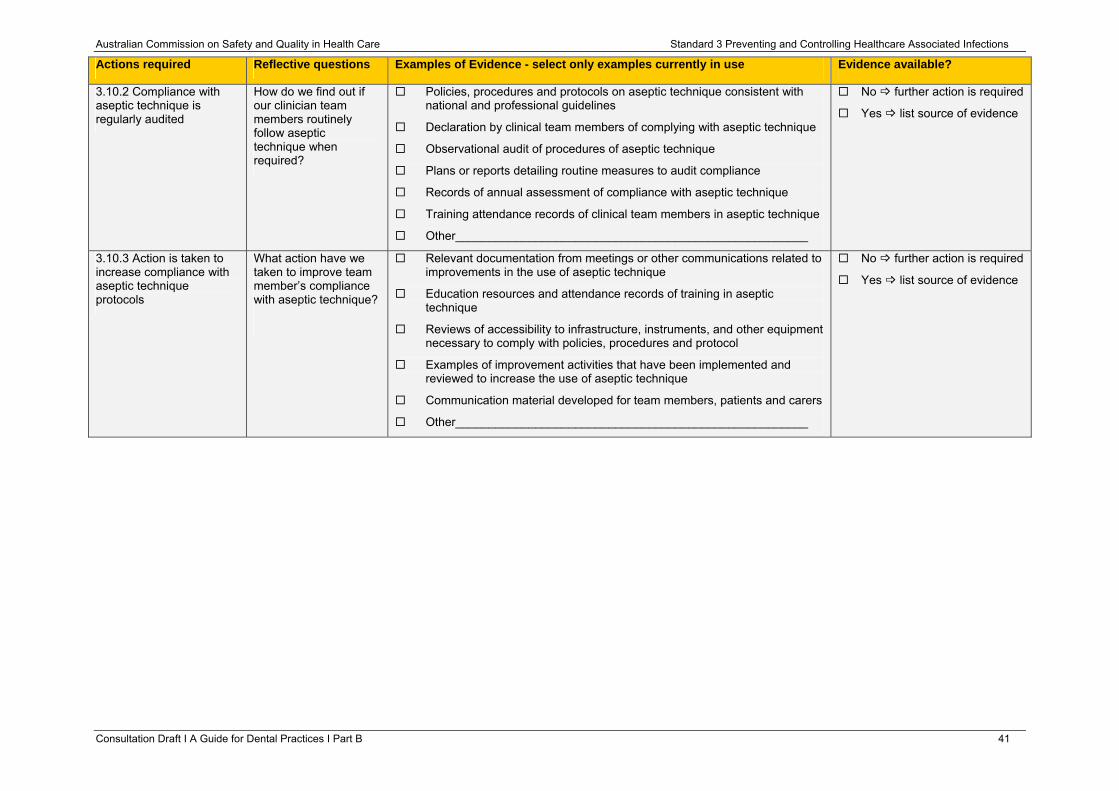
Australian Commission on Safety and Quality in Health Care Standard 3 Preventing and Controlling Healthcare Associated Infections
Actions required Reflective questions Examples of Evidence - select only examples currently in use Evidence available?
3.10.2 Compliance with aseptic technique is regularly audited
How do we find out if our clinician team members routinely follow aseptic technique when required?
Policies, procedures and protocols on aseptic technique consistent with national and professional guidelines
Declaration by clinical team members of complying with aseptic technique
Observational audit of procedures of aseptic technique
Plans or reports detailing routine measures to audit compliance
Records of annual assessment of compliance with aseptic technique
Training attendance records of clinical team members in aseptic technique
Other_____________________________________________________
No further action is required
Yes list source of evidence
3.10.3 Action is taken to increase compliance with aseptic technique protocols
What action have we taken to improve team member’s compliance with aseptic technique?
Relevant documentation from meetings or other communications related to improvements in the use of aseptic technique
Education resources and attendance records of training in aseptic technique
Reviews of accessibility to infrastructure, instruments, and other equipment necessary to comply with policies, procedures and protocol
Examples of improvement activities that have been implemented and reviewed to increase the use of aseptic technique
Communication material developed for team members, patients and carers
Other_____________________________________________________
No further action is required
Yes list source of evidence
Consultation Draft Ι A Guide for Dental Practices Ι Part B 41
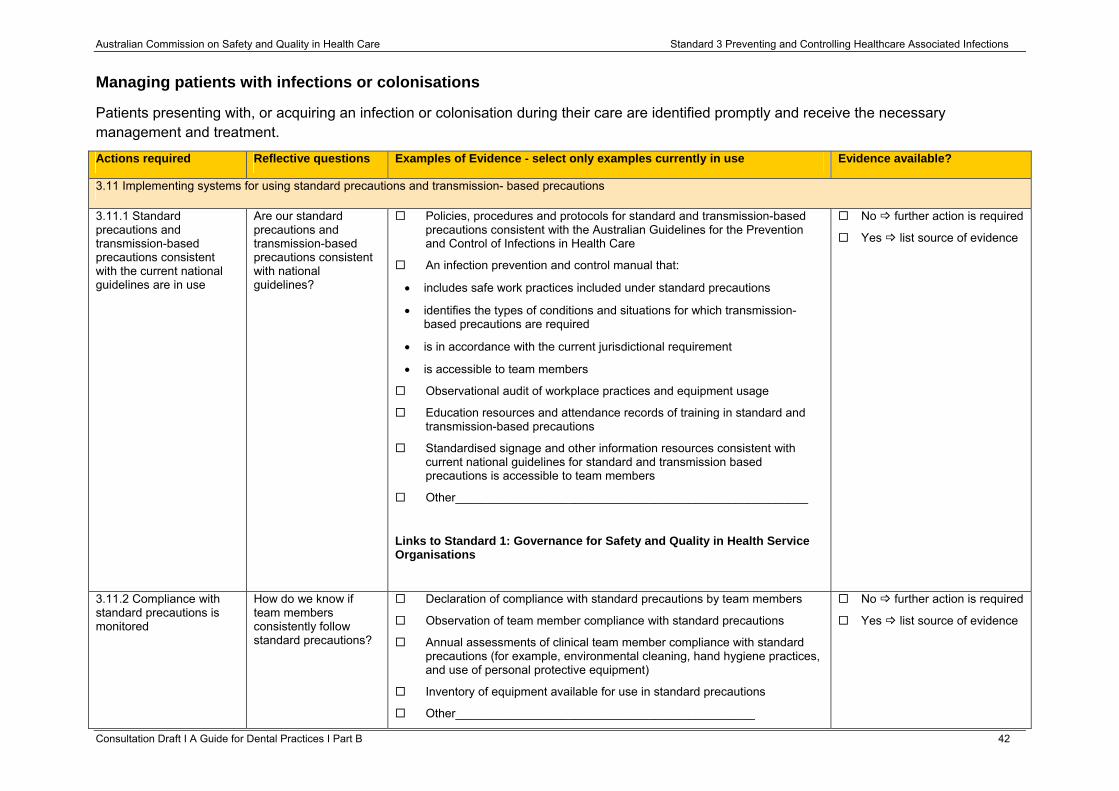
Australian Commission on Safety and Quality in Health Care Standard 3 Preventing and Controlling Healthcare Associated Infections
Managing patients with infections or colonisations
Patients presenting with, or acquiring an infection or colonisation during their care are identified promptly and receive the necessary management and treatment.
Consultation Draft Ι A Guide for Dental Practices Ι Part B 42
Actions required Reflective questions Examples of Evidence - select only examples currently in use Evidence available?
3.11 Implementing systems for using standard precautions and transmission- based precautions
3.11.1 Standard precautions and transmission-based precautions consistent with the current national guidelines are in use
Are our standard precautions and transmission-based precautions consistent with national guidelines?
Policies, procedures and protocols for standard and transmission-based precautions consistent with the Australian Guidelines for the Prevention and Control of Infections in Health Care
An infection prevention and control manual that:
• includes safe work practices included under standard precautions
• identifies the types of conditions and situations for which transmission-based precautions are required
• is in accordance with the current jurisdictional requirement
• is accessible to team members
Observational audit of workplace practices and equipment usage
Education resources and attendance records of training in standard and transmission-based precautions
Standardised signage and other information resources consistent with current national guidelines for standard and transmission based precautions is accessible to team members
Other_____________________________________________________
Links to Standard 1: Governance for Safety and Quality in Health Service Organisations
No further action is required
Yes list source of evidence
3.11.2 Compliance with standard precautions is monitored
How do we know if team members consistently follow standard precautions?
Declaration of compliance with standard precautions by team members
Observation of team member compliance with standard precautions
Annual assessments of clinical team member compliance with standard precautions (for example, environmental cleaning, hand hygiene practices, and use of personal protective equipment)
Inventory of equipment available for use in standard precautions
Other_____________________________________________
No further action is required
Yes list source of evidence
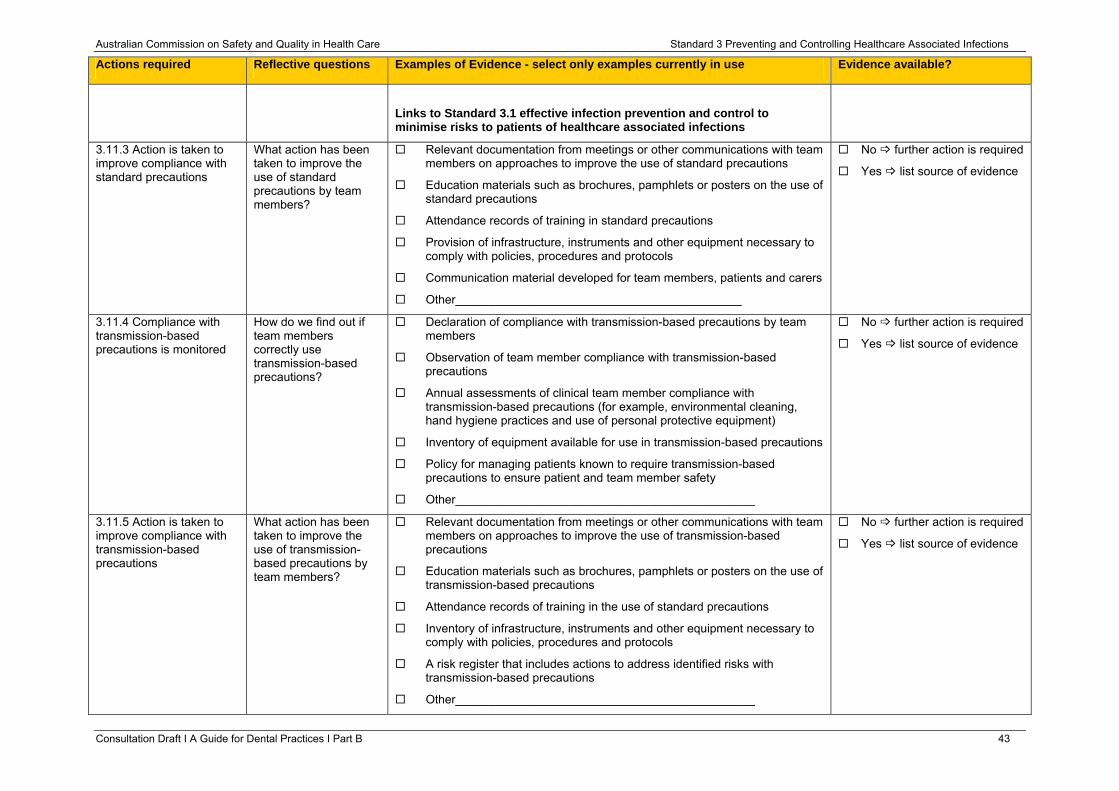
Australian Commission on Safety and Quality in Health Care Standard 3 Preventing and Controlling Healthcare Associated Infections
Actions required Reflective questions Examples of Evidence - select only examples currently in use Evidence available?
Links to Standard 3.1 effective infection prevention and control to minimise risks to patients of healthcare associated infections
3.11.3 Action is taken to improve compliance with standard precautions
What action has been taken to improve the use of standard precautions by team members?
Relevant documentation from meetings or other communications with team members on approaches to improve the use of standard precautions
Education materials such as brochures, pamphlets or posters on the use of standard precautions
Attendance records of training in standard precautions
Provision of infrastructure, instruments and other equipment necessary to comply with policies, procedures and protocols
Communication material developed for team members, patients and carers
Other___________________________________________
No further action is required
Yes list source of evidence
3.11.4 Compliance with transmission-based precautions is monitored
How do we find out if team members correctly use transmission-based precautions?
Declaration of compliance with transmission-based precautions by team members
Observation of team member compliance with transmission-based precautions
Annual assessments of clinical team member compliance with transmission-based precautions (for example, environmental cleaning, hand hygiene practices and use of personal protective equipment)
Inventory of equipment available for use in transmission-based precautions
Policy for managing patients known to require transmission-based precautions to ensure patient and team member safety
Other_____________________________________________
No further action is required
Yes list source of evidence
3.11.5 Action is taken to improve compliance with transmission-based precautions
What action has been taken to improve the use of transmission-based precautions by team members?
Relevant documentation from meetings or other communications with team members on approaches to improve the use of transmission-based precautions
Education materials such as brochures, pamphlets or posters on the use of transmission-based precautions
Attendance records of training in the use of standard precautions
Inventory of infrastructure, instruments and other equipment necessary to comply with policies, procedures and protocols
A risk register that includes actions to address identified risks with transmission-based precautions
Other_____________________________________________
No further action is required
Yes list source of evidence
Consultation Draft Ι A Guide for Dental Practices Ι Part B 43
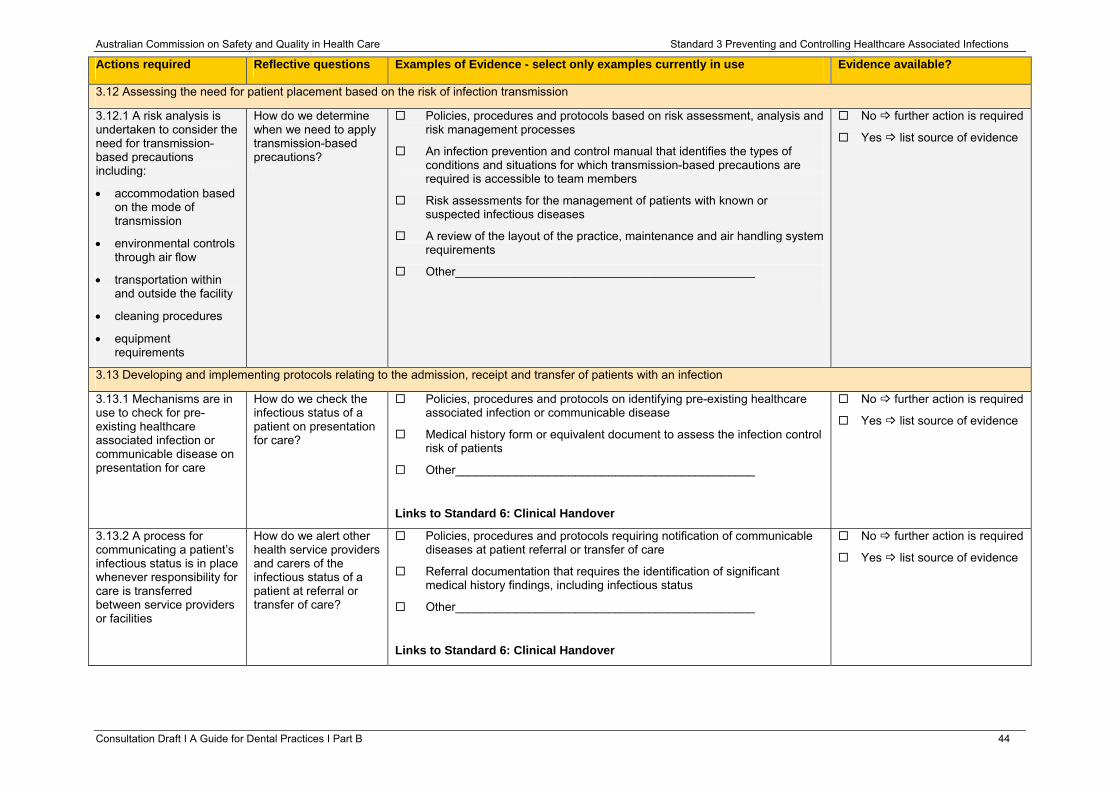
Australian Commission on Safety and Quality in Health Care Standard 3 Preventing and Controlling Healthcare Associated Infections
Actions required Reflective questions Examples of Evidence - select only examples currently in use Evidence available?
3.12 Assessing the need for patient placement based on the risk of infection transmission
3.12.1 A risk analysis is undertaken to consider the need for transmission-based precautions including:
• accommodation based on the mode of transmission
• environmental controls through air flow
• transportation within and outside the facility
• cleaning procedures
• equipment requirements
How do we determine when we need to apply transmission-based precautions?
Policies, procedures and protocols based on risk assessment, analysis and risk management processes
An infection prevention and control manual that identifies the types of conditions and situations for which transmission-based precautions are required is accessible to team members
Risk assessments for the management of patients with known or suspected infectious diseases
A review of the layout of the practice, maintenance and air handling system requirements
Other_____________________________________________
No further action is required
Yes list source of evidence
3.13 Developing and implementing protocols relating to the admission, receipt and transfer of patients with an infection
3.13.1 Mechanisms are in use to check for pre-existing healthcare associated infection or communicable disease on presentation for care
How do we check the infectious status of a patient on presentation for care?
Policies, procedures and protocols on identifying pre-existing healthcare associated infection or communicable disease
Medical history form or equivalent document to assess the infection control risk of patients
Other_____________________________________________
Links to Standard 6: Clinical Handover
No further action is required
Yes list source of evidence
3.13.2 A process for communicating a patient’s infectious status is in place whenever responsibility for care is transferred between service providers or facilities
How do we alert other health service providers and carers of the infectious status of a patient at referral or transfer of care?
Policies, procedures and protocols requiring notification of communicable diseases at patient referral or transfer of care
Referral documentation that requires the identification of significant medical history findings, including infectious status
Other_____________________________________________
Links to Standard 6: Clinical Handover
No further action is required
Yes list source of evidence
Consultation Draft Ι A Guide for Dental Practices Ι Part B 44
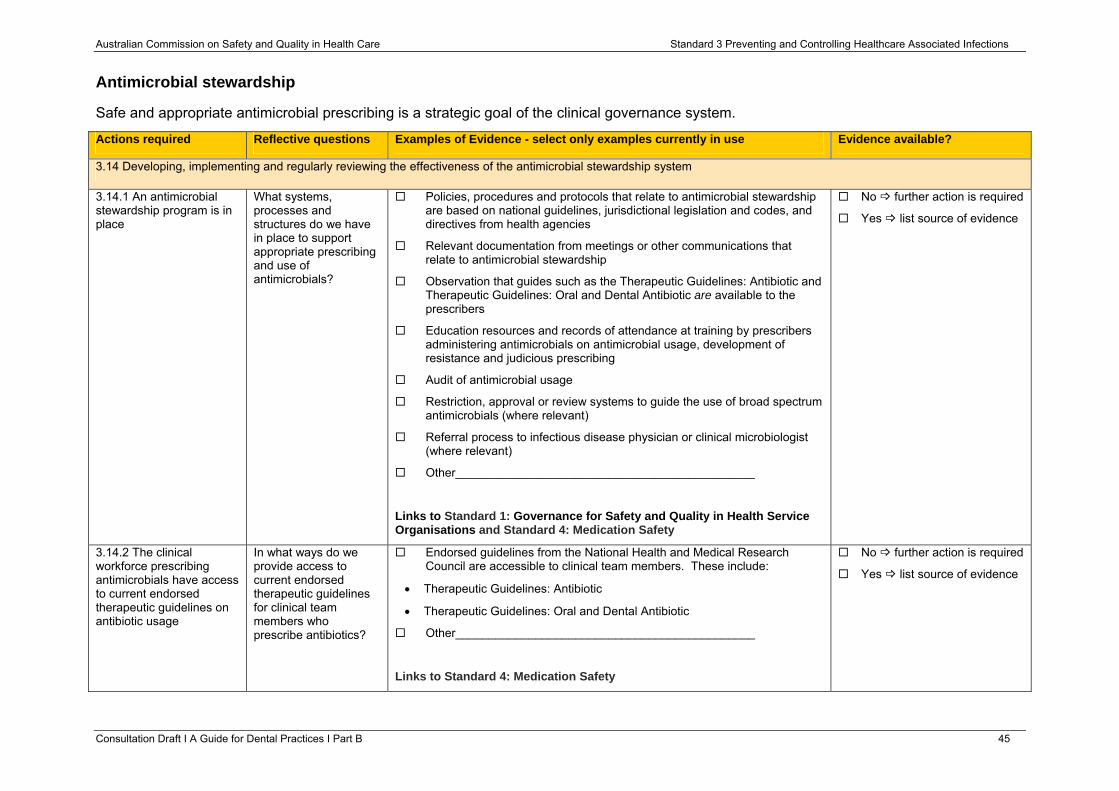
Australian Commission on Safety and Quality in Health Care Standard 3 Preventing and Controlling Healthcare Associated Infections
Antimicrobial stewardship
Safe and appropriate antimicrobial prescribing is a strategic goal of the clinical governance system.
Actions required Reflective questions Examples of Evidence - select only examples currently in use Evidence available?
3.14 Developing, implementing and regularly reviewing the effectiveness of the antimicrobial stewardship system
3.14.1 An antimicrobial stewardship program is in place
What systems, processes and structures do we have in place to support appropriate prescribing and use of antimicrobials?
Policies, procedures and protocols that relate to antimicrobial stewardship are based on national guidelines, jurisdictional legislation and codes, and directives from health agencies
Relevant documentation from meetings or other communications that relate to antimicrobial stewardship
Observation that guides such as the Therapeutic Guidelines: Antibiotic and Therapeutic Guidelines: Oral and Dental Antibiotic are available to the prescribers
Education resources and records of attendance at training by prescribers administering antimicrobials on antimicrobial usage, development of resistance and judicious prescribing
Audit of antimicrobial usage
Restriction, approval or review systems to guide the use of broad spectrum antimicrobials (where relevant)
Referral process to infectious disease physician or clinical microbiologist (where relevant)
Other_____________________________________________
Links to Standard 1: Governance for Safety and Quality in Health Service Organisations and Standard 4: Medication Safety
No further action is required
Yes list source of evidence
3.14.2 The clinical workforce prescribing antimicrobials have access to current endorsed therapeutic guidelines on antibiotic usage
In what ways do we provide access to current endorsed therapeutic guidelines for clinical team members who prescribe antibiotics?
Endorsed guidelines from the National Health and Medical Research Council are accessible to clinical team members. These include:
• Therapeutic Guidelines: Antibiotic
• Therapeutic Guidelines: Oral and Dental Antibiotic
Other_____________________________________________
Links to Standard 4: Medication Safety
No further action is required
Yes list source of evidence
Consultation Draft Ι A Guide for Dental Practices Ι Part B 45
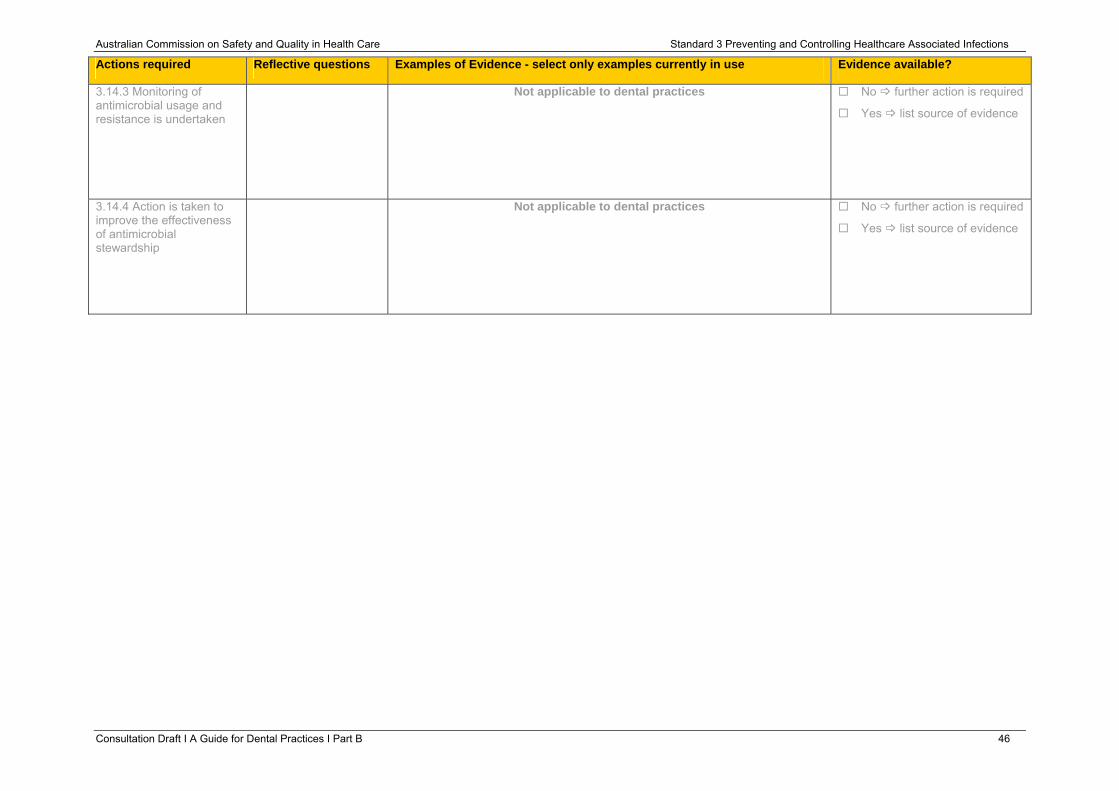
Australian Commission on Safety and Quality in Health Care Standard 3 Preventing and Controlling Healthcare Associated Infections
Actions required Reflective questions Examples of Evidence - select only examples currently in use Evidence available?
3.14.3 Monitoring of antimicrobial usage and resistance is undertaken
Not applicable to dental practices No further action is required
Yes list source of evidence
3.14.4 Action is taken to improve the effectiveness of antimicrobial stewardship
Not applicable to dental practices No further action is required
Yes list source of evidence
Consultation Draft Ι A Guide for Dental Practices Ι Part B 46
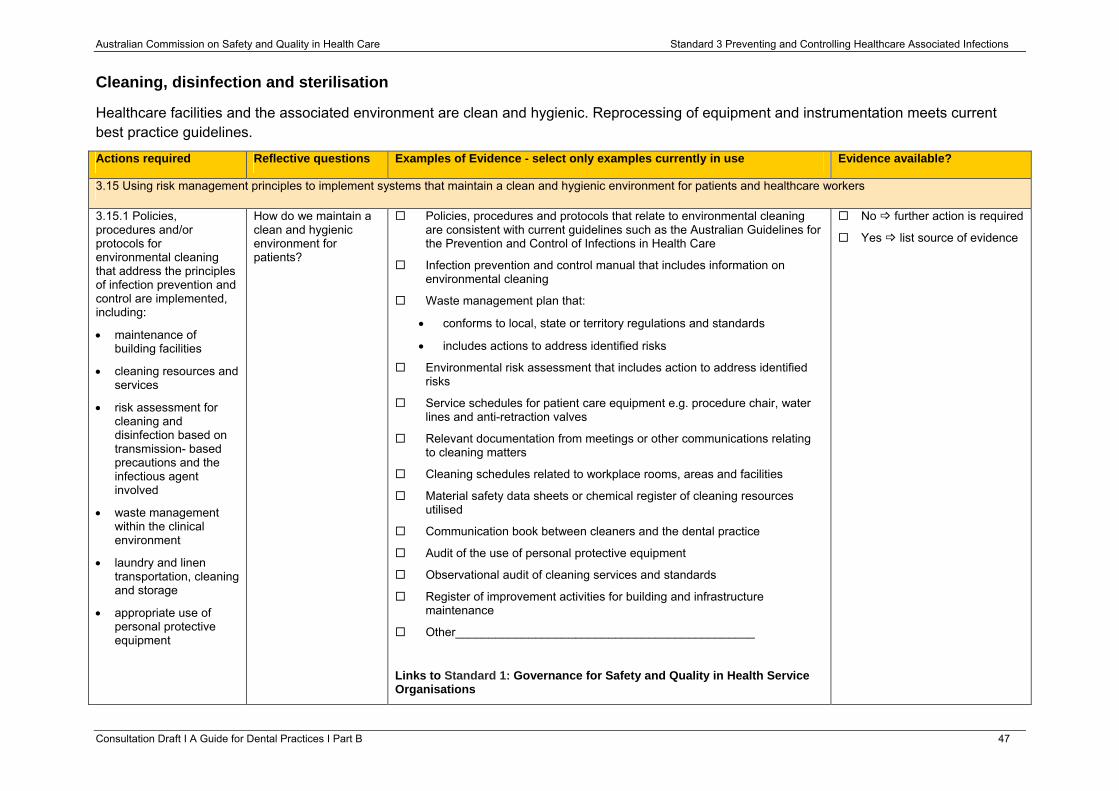
Australian Commission on Safety and Quality in Health Care Standard 3 Preventing and Controlling Healthcare Associated Infections
Cleaning, disinfection and sterilisation
Healthcare facilities and the associated environment are clean and hygienic. Reprocessing of equipment and instrumentation meets current best practice guidelines.
Actions required Reflective questions Examples of Evidence - select only examples currently in use Evidence available?
3.15 Using risk management principles to implement systems that maintain a clean and hygienic environment for patients and healthcare workers
3.15.1 Policies, procedures and/or protocols for environmental cleaning that address the principles of infection prevention and control are implemented, including:
• maintenance of building facilities
• cleaning resources and services
• risk assessment for cleaning and disinfection based on transmission- based precautions and the infectious agent involved
• waste management within the clinical environment
• laundry and linen transportation, cleaning and storage
• appropriate use of personal protective equipment
How do we maintain a clean and hygienic environment for patients?
Policies, procedures and protocols that relate to environmental cleaning are consistent with current guidelines such as the Australian Guidelines for the Prevention and Control of Infections in Health Care
Infection prevention and control manual that includes information on environmental cleaning
Waste management plan that:
• conforms to local, state or territory regulations and standards
• includes actions to address identified risks
Environmental risk assessment that includes action to address identified risks
Service schedules for patient care equipment e.g. procedure chair, water lines and anti-retraction valves
Relevant documentation from meetings or other communications relating to cleaning matters
Cleaning schedules related to workplace rooms, areas and facilities
Material safety data sheets or chemical register of cleaning resources utilised
Communication book between cleaners and the dental practice
Audit of the use of personal protective equipment
Observational audit of cleaning services and standards
Register of improvement activities for building and infrastructure maintenance
Other_____________________________________________
Links to Standard 1: Governance for Safety and Quality in Health Service Organisations
No further action is required
Yes list source of evidence
Consultation Draft Ι A Guide for Dental Practices Ι Part B 47
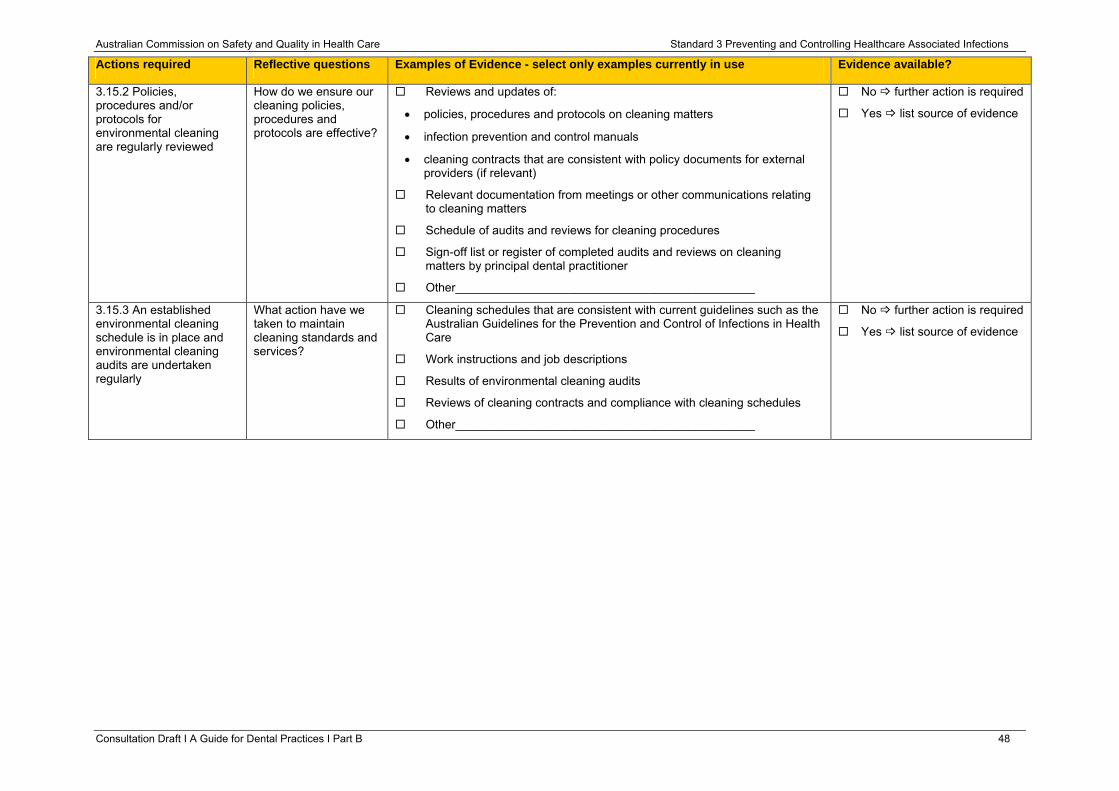
Australian Commission on Safety and Quality in Health Care Standard 3 Preventing and Controlling Healthcare Associated Infections
Actions required Reflective questions Examples of Evidence - select only examples currently in use Evidence available?
3.15.2 Policies, procedures and/or protocols for environmental cleaning are regularly reviewed
How do we ensure our cleaning policies, procedures and protocols are effective?
Reviews and updates of:
• policies, procedures and protocols on cleaning matters
• infection prevention and control manuals
• cleaning contracts that are consistent with policy documents for external providers (if relevant)
Relevant documentation from meetings or other communications relating to cleaning matters
Schedule of audits and reviews for cleaning procedures
Sign-off list or register of completed audits and reviews on cleaning matters by principal dental practitioner
Other_____________________________________________
No further action is required
Yes list source of evidence
3.15.3 An established environmental cleaning schedule is in place and environmental cleaning audits are undertaken regularly
What action have we taken to maintain cleaning standards and services?
Cleaning schedules that are consistent with current guidelines such as the Australian Guidelines for the Prevention and Control of Infections in Health Care
Work instructions and job descriptions
Results of environmental cleaning audits
Reviews of cleaning contracts and compliance with cleaning schedules
Other_____________________________________________
No further action is required
Yes list source of evidence
Consultation Draft Ι A Guide for Dental Practices Ι Part B 48
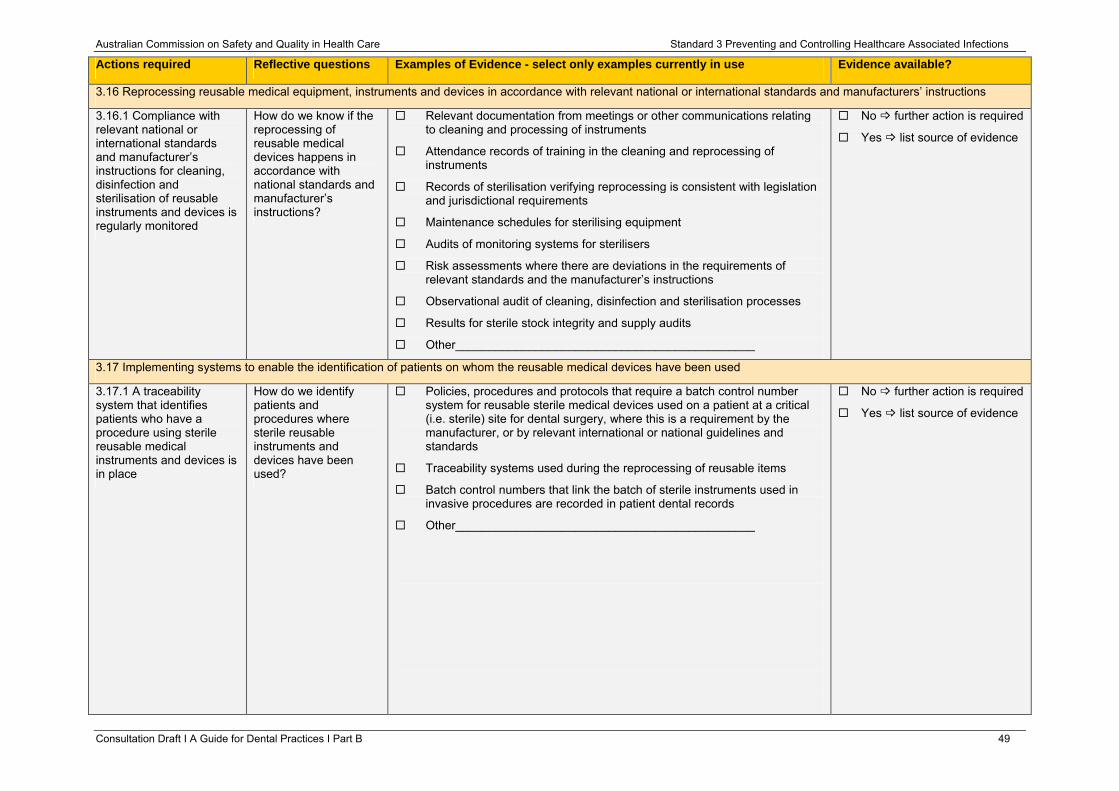
Australian Commission on Safety and Quality in Health Care Standard 3 Preventing and Controlling Healthcare Associated Infections
Actions required Reflective questions Examples of Evidence - select only examples currently in use Evidence available?
3.16 Reprocessing reusable medical equipment, instruments and devices in accordance with relevant national or international standards and manufacturers’ instructions
3.16.1 Compliance with relevant national or international standards and manufacturer’s instructions for cleaning, disinfection and sterilisation of reusable instruments and devices is regularly monitored
How do we know if the reprocessing of reusable medical devices happens in accordance with national standards and manufacturer’s instructions?
Relevant documentation from meetings or other communications relating to cleaning and processing of instruments
Attendance records of training in the cleaning and reprocessing of instruments
Records of sterilisation verifying reprocessing is consistent with legislation and jurisdictional requirements
Maintenance schedules for sterilising equipment
Audits of monitoring systems for sterilisers
Risk assessments where there are deviations in the requirements of relevant standards and the manufacturer’s instructions
Observational audit of cleaning, disinfection and sterilisation processes
Results for sterile stock integrity and supply audits
Other_____________________________________________
No further action is required
Yes list source of evidence
3.17 Implementing systems to enable the identification of patients on whom the reusable medical devices have been used
3.17.1 A traceability system that identifies patients who have a procedure using sterile reusable medical instruments and devices is in place
How do we identify patients and procedures where sterile reusable instruments and devices have been used?
Policies, procedures and protocols that require a batch control number system for reusable sterile medical devices used on a patient at a critical (i.e. sterile) site for dental surgery, where this is a requirement by the manufacturer, or by relevant international or national guidelines and standards
Traceability systems used during the reprocessing of reusable items
Batch control numbers that link the batch of sterile instruments used in invasive procedures are recorded in patient dental records
Other_____________________________________________
No further action is required
Yes list source of evidence
Consultation Draft Ι A Guide for Dental Practices Ι Part B 49
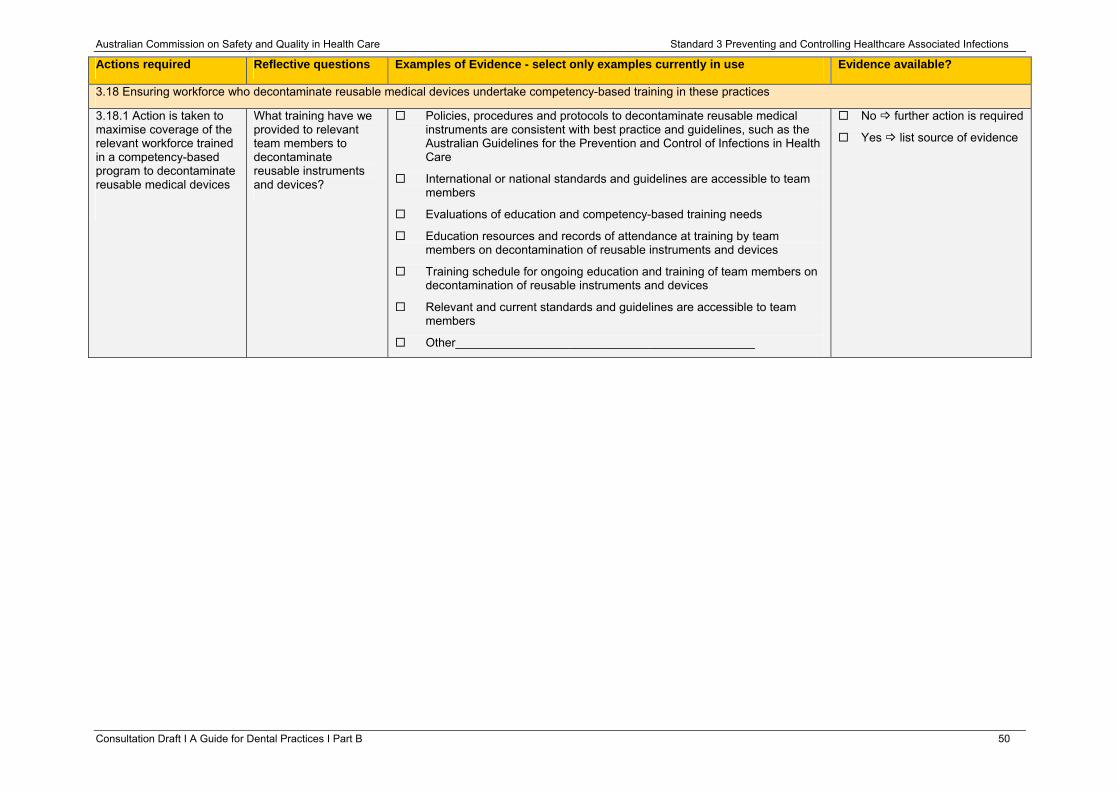
Australian Commission on Safety and Quality in Health Care Standard 3 Preventing and Controlling Healthcare Associated Infections
Actions required Reflective questions Examples of Evidence - select only examples currently in use Evidence available?
3.18 Ensuring workforce who decontaminate reusable medical devices undertake competency-based training in these practices
3.18.1 Action is taken to maximise coverage of the relevant workforce trained in a competency-based program to decontaminate reusable medical devices
What training have we provided to relevant team members to decontaminate reusable instruments and devices?
Policies, procedures and protocols to decontaminate reusable medical instruments are consistent with best practice and guidelines, such as the Australian Guidelines for the Prevention and Control of Infections in Health Care
International or national standards and guidelines are accessible to team members
Evaluations of education and competency-based training needs
Education resources and records of attendance at training by team members on decontamination of reusable instruments and devices
Training schedule for ongoing education and training of team members on decontamination of reusable instruments and devices
Relevant and current standards and guidelines are accessible to team members
Other_____________________________________________
No further action is required
Yes list source of evidence
Consultation Draft Ι A Guide for Dental Practices Ι Part B 50
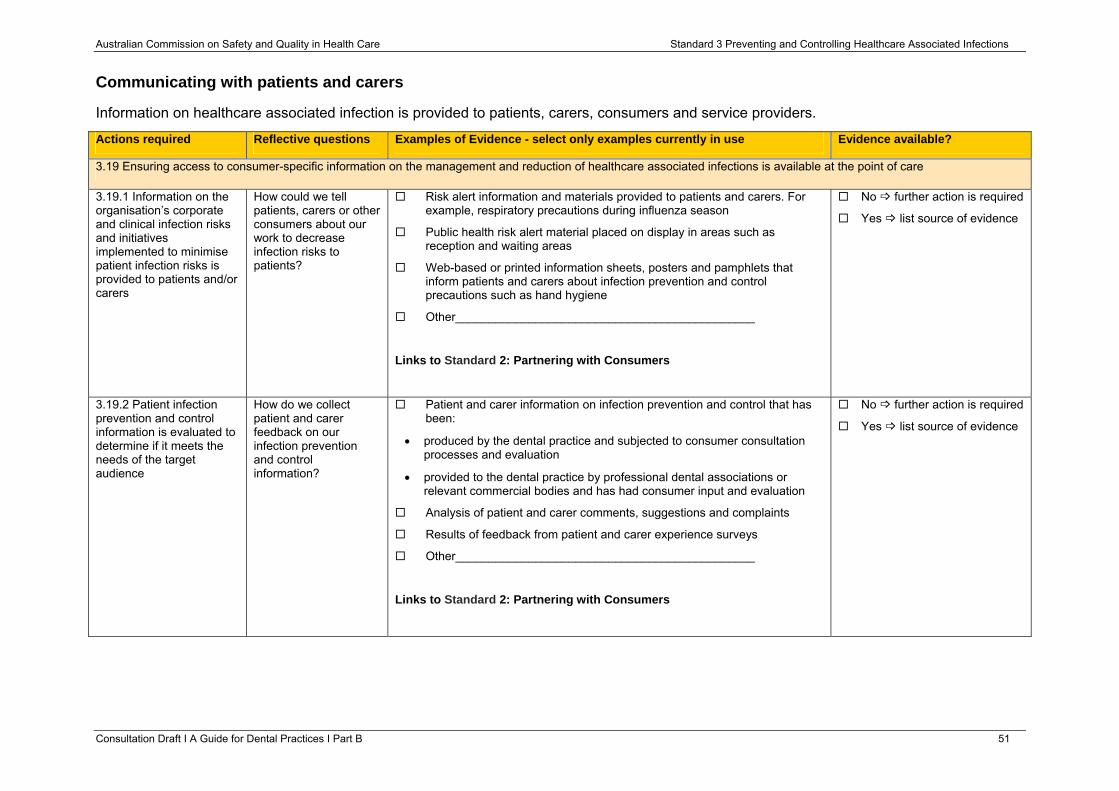
Australian Commission on Safety and Quality in Health Care Standard 3 Preventing and Controlling Healthcare Associated Infections
Communicating with patients and carers
Information on healthcare associated infection is provided to patients, carers, consumers and service providers.
Actions required Reflective questions Examples of Evidence - select only examples currently in use Evidence available?
3.19 Ensuring access to consumer-specific information on the management and reduction of healthcare associated infections is available at the point of care
3.19.1 Information on the organisation’s corporate and clinical infection risks and initiatives implemented to minimise patient infection risks is provided to patients and/or carers
How could we tell patients, carers or other consumers about our work to decrease infection risks to patients?
Risk alert information and materials provided to patients and carers. For example, respiratory precautions during influenza season
Public health risk alert material placed on display in areas such as reception and waiting areas
Web-based or printed information sheets, posters and pamphlets that inform patients and carers about infection prevention and control precautions such as hand hygiene
Other_____________________________________________
Links to Standard 2: Partnering with Consumers
No further action is required
Yes list source of evidence
3.19.2 Patient infection prevention and control information is evaluated to determine if it meets the needs of the target audience
How do we collect patient and carer feedback on our infection prevention and control information?
Patient and carer information on infection prevention and control that has been:
• produced by the dental practice and subjected to consumer consultation processes and evaluation
• provided to the dental practice by professional dental associations or relevant commercial bodies and has had consumer input and evaluation
Analysis of patient and carer comments, suggestions and complaints
Results of feedback from patient and carer experience surveys
Other_____________________________________________
Links to Standard 2: Partnering with Consumers
No further action is required
Yes list source of evidence
Consultation Draft Ι A Guide for Dental Practices Ι Part B 51
Australian Commission on Safety and Quality in Health Care Standard 3 Preventing and Controlling Healthcare Associated Infections
Resources
1. Antibiotic Expert Group. Therapeutic guidelines: antibiotic. Version 14. Melbourne: Therapeutic Guidelines Limited; 2010.
2. Australian College of Operating Room Nurses. Aseptic Non-Touch Technique (ANTT) Standards for Periooperative Nursing 2010-2011. South Australia. ACORN. 2010. (Copies can be purchased from ACORN website http://www.acorn.org.au/about-acorn-standards.html.)
3. Australian Commission on Safety and Quality in Health Care. Antimicrobial Stewardship in Australian Hospitals, 2010.
4. ADA Guidelines for Infection Control. Second Edition. Australian Dental Association. (Accessed 4 July 2012, at http://www.ada.org.au/publications/guideinfectcont.aspx)
5. Australian/New Zealand Standard AS/NZS 4815 2006 Office-based health care facilities – Reprocessing of reusable medical and surgical instruments and equipment, and maintenance of the associated environment (currently under review). Available for purchase at www.standards.co.nz
6. Australian/New Zealand Standard AS/NZS 4187 2003. Cleaning, disinfecting and sterilising reusable medical and surgical instruments and equipment, and maintenance of associated environments in health care facilities (currently under review). Available for purchase at www.standards.co.nz
7. Duguid M, Cruickshank M, editors. Antimicrobial Stewardship in Australian Hospitals. Sydney: Australian Commission on Safety and Quality in Health Care, 2011.
8. 5 Moments for Hand Hygiene. Hand Hygiene Australia, 2011. (Accessed 8 June 2012, at http://www.hha.org.au/home/5-moments-for-hand-hygiene.aspx.)
9. Guidelines on Infection Control. Dental Board of Australia. (Accessed 08 June 2012, at http://www.dentalboard.gov.au)
10. Healthcare Associated Infection (HAI) Program. Australian Commission on Safety and Quality in Health Care (Accessed 08 June 2012, at http://www.safetyandquality.gov.au/our-work/healthcare-associated-infection/)
11. National Health and Medical Research Council. Australian Guidelines for the Prevention and Control of Infections in Healthcare. Canberra: NHMRC, 2010.
12. National Health and Medical Research Council. The Australian Immunisation Handbook 9th Edition Canberra, ACT. Australian Government 2008.
13. Oral and Dental Expert Group. Therapeutic guidelines: oral and dental. Version 2. Melbourne: Therapeutic Guidelines Limited; 2012
Consultation Draft Ι A Guide for Dental Practices Ι Part B 52
Australian Commission on Safety and Quality in Health Care Standard 4: Medication Safety
Consultation Draft Ι A Guide for Dental Practices Ι Part B 53
Standard 4: Medication Safety Clinical leaders and senior managers of a health service organisation implement systems to reduce the occurrence of medication incidents, and improve the safety and quality of medicine use. Clinicians and other members of the workforce use the systems to safely manage medicines.
The intention of this Standard is to:
Ensure competent clinicians safely prescribe, dispense and administer appropriate medicines to informed patients and carers.
Context
It is expected that this Standard will be applied in conjunction with Standard 1 ‘Governance for Safety and Quality in Health Service Organisations’ and Standard 2 ‘Partnering with Consumers’.
Criteria to achieve the Medication Safety Standard:
• Governance and systems for medication safety
• Documentation of patient information
• Medication management processes
• Continuity of medication management
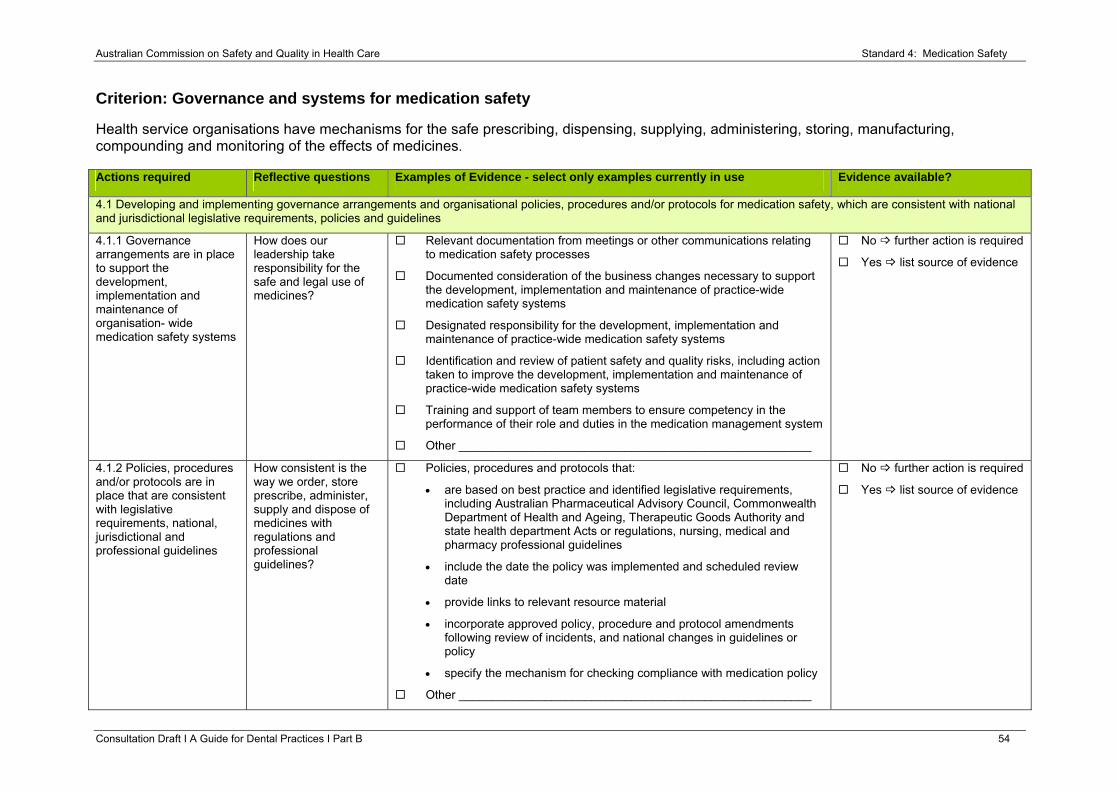
Australian Commission on Safety and Quality in Health Care Standard 4: Medication Safety
Consultation Draft Ι A Guide for Dental Practices Ι Part B 54
Criterion: Governance and systems for medication safety
Health service organisations have mechanisms for the safe prescribing, dispensing, supplying, administering, storing, manufacturing, compounding and monitoring of the effects of medicines. Actions required Reflective questions Examples of Evidence - select only examples currently in use Evidence available?
4.1 Developing and implementing governance arrangements and organisational policies, procedures and/or protocols for medication safety, which are consistent with national and jurisdictional legislative requirements, policies and guidelines
4.1.1 Governance arrangements are in place to support the development, implementation and maintenance of organisation- wide medication safety systems
How does our leadership take responsibility for the safe and legal use of medicines?
Relevant documentation from meetings or other communications relating to medication safety processes
Documented consideration of the business changes necessary to support the development, implementation and maintenance of practice-wide medication safety systems
Designated responsibility for the development, implementation and maintenance of practice-wide medication safety systems
Identification and review of patient safety and quality risks, including action taken to improve the development, implementation and maintenance of practice-wide medication safety systems
Training and support of team members to ensure competency in the performance of their role and duties in the medication management system
Other _____________________________________________________
No further action is required
Yes list source of evidence
4.1.2 Policies, procedures and/or protocols are in place that are consistent with legislative requirements, national, jurisdictional and professional guidelines
How consistent is the way we order, store prescribe, administer, supply and dispose of medicines with regulations and professional guidelines?
Policies, procedures and protocols that:
• are based on best practice and identified legislative requirements, including Australian Pharmaceutical Advisory Council, Commonwealth Department of Health and Ageing, Therapeutic Goods Authority and state health department Acts or regulations, nursing, medical and pharmacy professional guidelines
• include the date the policy was implemented and scheduled review date
• provide links to relevant resource material
• incorporate approved policy, procedure and protocol amendments following review of incidents, and national changes in guidelines or policy
specif• y the mechanism for checking compliance with medication policy
Other _____________________________________________________
No further action is required
Yes list source of evidence
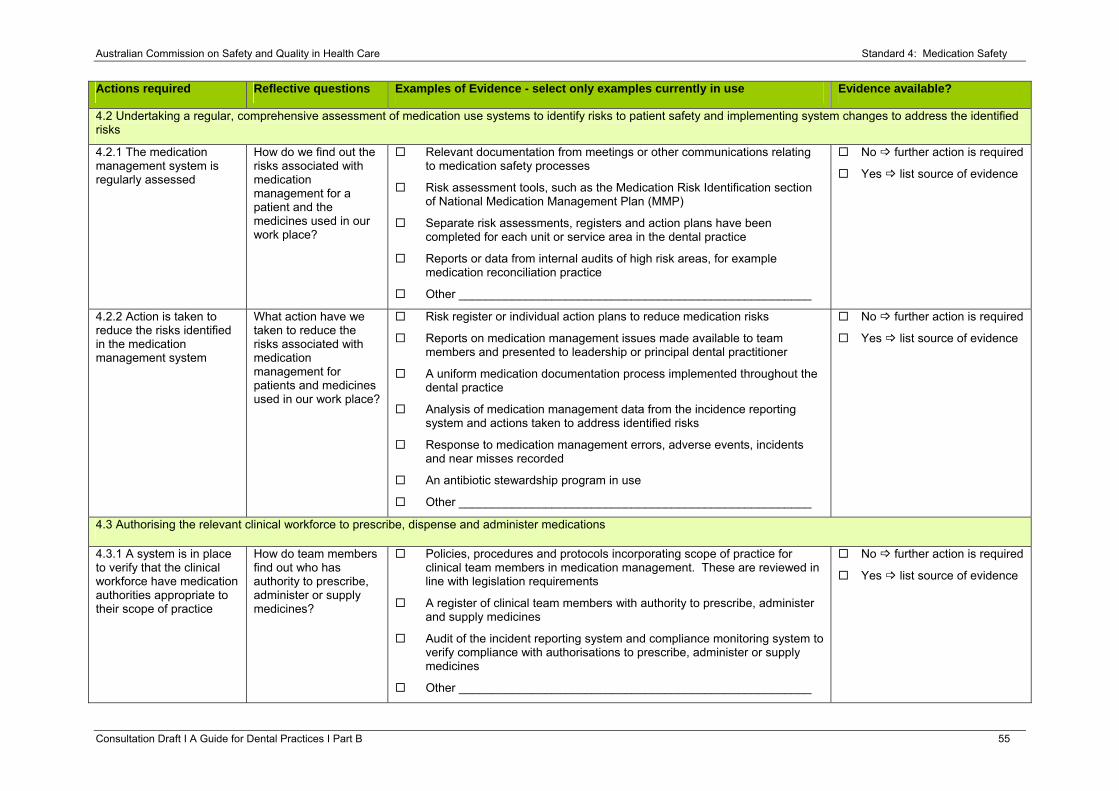
Australian Commission on Safety and Quality in Health Care Standard 4: Medication Safety
Consultation Draft Ι A Guide for Dental Practices Ι Part B 55
Actions required Reflective questions Examples of Evidence - select only examples currently in use Evidence available?
4.2 Undertaking a regular, comprehensive assessment of medication use systems to identify risks to patient safety and implementing system changes to address the identified risks
4.2.1 The medication management system is regularly assessed
How do we find out the risks associated with medication management for a patient and the medicines used in our work place?
Relevant documentation from meetings or other communications relating to medication safety processes
Risk assessment tools, such as the Medication Risk Identification section of National Medication Management Plan (MMP)
Separate risk assessments, registers and action plans have been completed for each unit or service area in the dental practice
Reports or data from internal audits of high risk areas, for example medication reconciliation practice
Other _____________________________________________________
No further action is required
Yes list source of evidence
4.2.2 Action is taken to reduce the risks identified in the medication management system
What action have we taken to reduce the risks associated with medication management for patients and medicines used in our work place?
Risk register or individual action plans to reduce medication risks
Reports on medication management issues made available to team members and presented to leadership or principal dental practitioner
A uniform medication documentation process implemented throughout the dental practice
Analysis of medication management data from the incidence reporting system and actions taken to address identified risks
Response to medication management errors, adverse events, incidents and near misses recorded
An antibiotic stewardship program in use
Other _____________________________________________________
No further action is required
Yes list source of evidence
4.3 Authorising the relevant clinical workforce to prescribe, dispense and administer medications
4.3.1 A system is in place to verify that the clinical workforce have medication authorities appropriate to their scope of practice
How do team members find out who has authority to prescribe, administer or supply medicines?
Policies, procedures and protocols incorporating scope of practice for clinical team members in medication management. These are reviewed in line with legislation requirements
A register of clinical team members with authority to prescribe, administer and supply medicines
Audit of the incident reporting system and compliance monitoring system to verify compliance with authorisations to prescribe, administer or supply medicines
Other _____________________________________________________
No further action is required
Yes list source of evidence
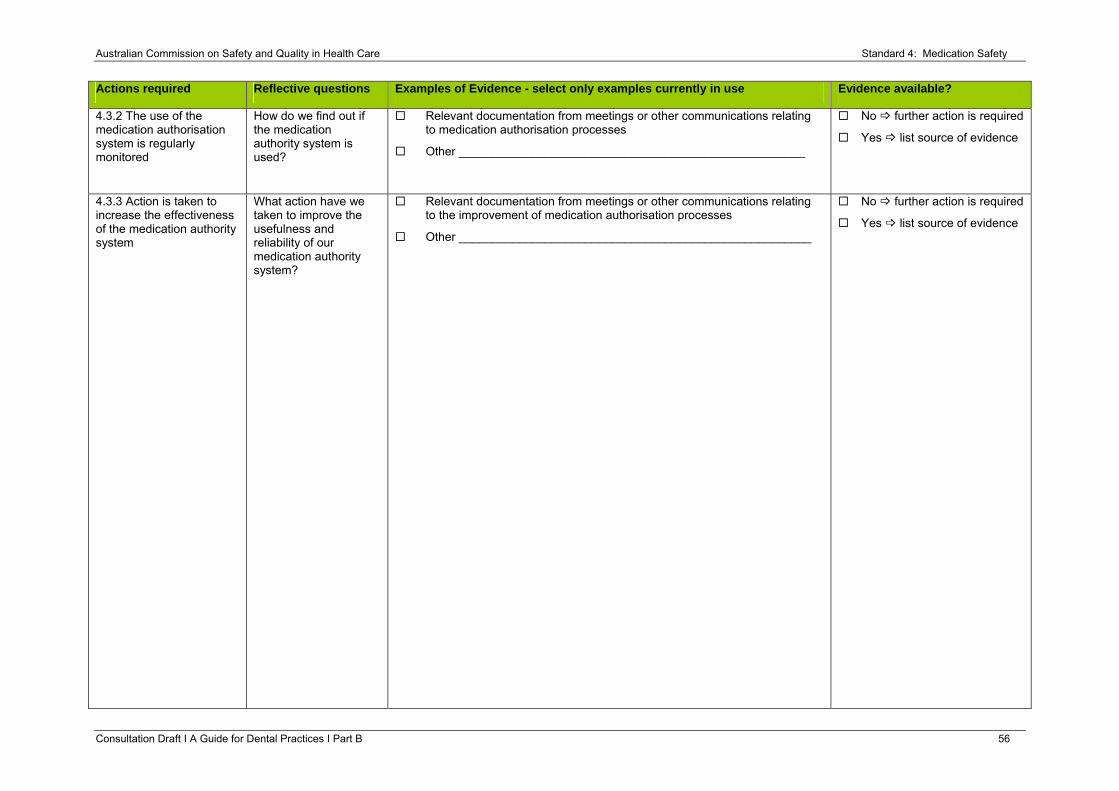
Australian Commission on Safety and Quality in Health Care Standard 4: Medication Safety
Consultation Draft Ι A Guide for Dental Practices Ι Part B 56
Actions required Reflective questions Examples of Evidence - select only examples currently in use Evidence available?
4.3.2 The use of the medication authorisation system is regularly monitored
How do we find out if the medication authority system is used?
Relevant documentation from meetings or other communications relating to medication authorisation processes
Other ____________________________________________________
No further action is required
Yes list source of evidence
4.3.3 Action is taken to increase the effectiveness of the medication authority system
What action have we taken to improve the usefulness and reliability of our medication authority system?
Relevant documentation from meetings or other communications relating to the improvement of medication authorisation processes
Other _____________________________________________________
No further action is required
Yes list source of evidence
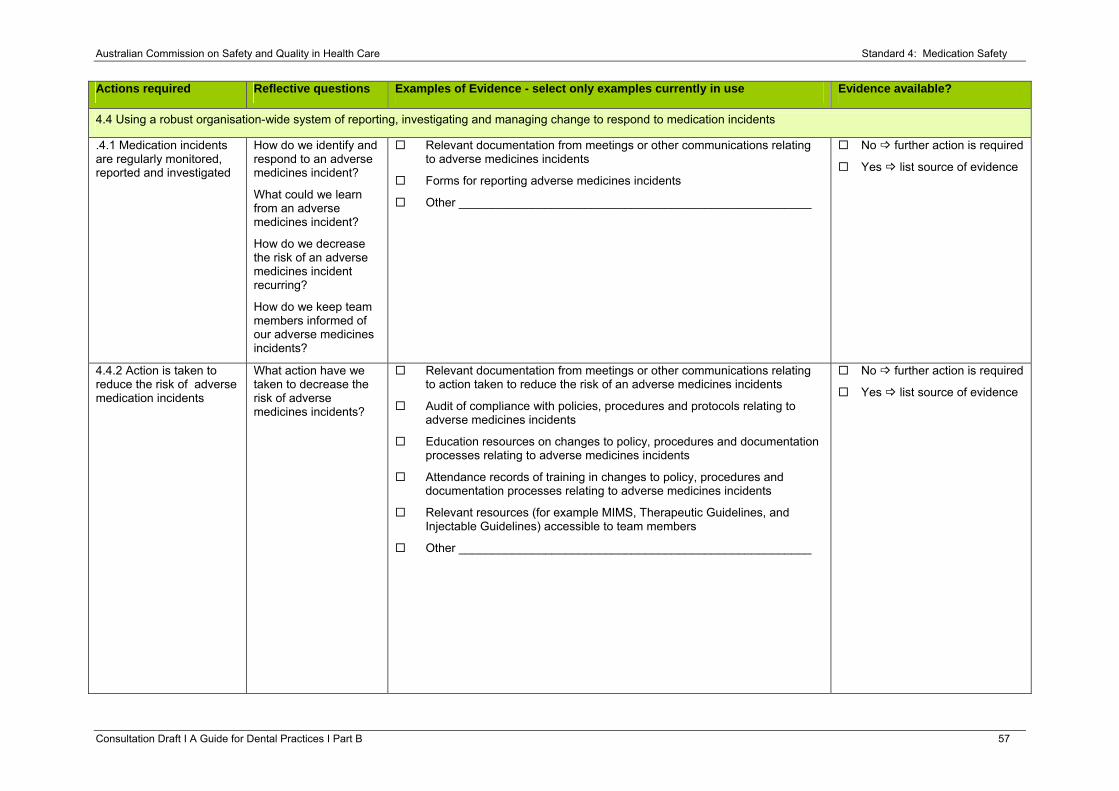
Australian Commission on Safety and Quality in Health Care Standard 4: Medication Safety
Consultation Draft Ι A Guide for Dental Practices Ι Part B 57
Actions required Reflective questions Examples of Evidence - select only examples currently in use Evidence available?
4.4 Using a robust organisation-wide system of reporting, investigating and managing change to respond to medication incidents
.4.1 Medication incidents are regularly monitored, reported and investigated
How do we identify and respond to an adverse medicines incident?
What could we learn from an adverse medicines incident?
How do we decrease the risk of an adverse medicines incident recurring?
How do we keep team members informed of our adverse medicines incidents?
Relevant documentation from meetings or other communications relating to adverse medicines incidents
Forms for reporting adverse medicines incidents
Other _____________________________________________________
No further action is required
Yes list source of evidence
4.4.2 Action is taken to reduce the risk of adverse medication incidents
What action have we taken to decrease the risk of adverse medicines incidents?
Relevant documentation from meetings or other communications relating to action taken to reduce the risk of an adverse medicines incidents
Audit of compliance with policies, procedures and protocols relating to adverse medicines incidents
Education resources on changes to policy, procedures and documentation processes relating to adverse medicines incidents
Attendance records of training in changes to policy, procedures and documentation processes relating to adverse medicines incidents
Relevant resources (for example MIMS, Therapeutic Guidelines, and Injectable Guidelines) accessible to team members
Other _____________________________________________________
No further action is required
Yes list source of evidence
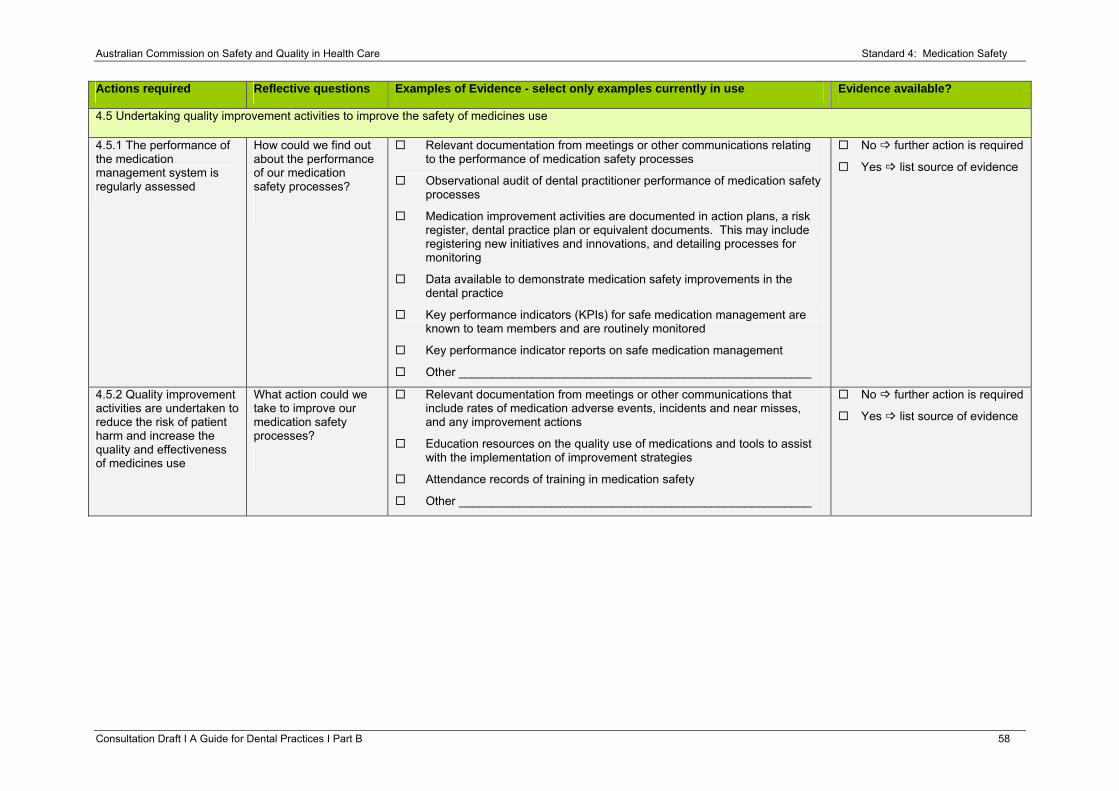
Australian Commission on Safety and Quality in Health Care Standard 4: Medication Safety
Consultation Draft Ι A Guide for Dental Practices Ι Part B 58
Actions required Reflective questions Examples of Evidence - select only examples currently in use Evidence available?
4.5 Undertaking quality improvement activities to improve the safety of medicines use
4.5.1 The performance of the medication management system is regularly assessed
How could we find out about the performance of our medication safety processes?
Relevant documentation from meetings or other communications relating to the performance of medication safety processes
Observational audit of dental practitioner performance of medication safety processes
Medication improvement activities are documented in action plans, a risk register, dental practice plan or equivalent documents. This may include registering new initiatives and innovations, and detailing processes for monitoring
Data available to demonstrate medication safety improvements in the dental practice
Key performance indicators (KPIs) for safe medication management are known to team members and are routinely monitored
Key performance indicator reports on safe medication management
Other _____________________________________________________
No further action is required
Yes list source of evidence
4.5.2 Quality improvement activities are undertaken to reduce the risk of patient harm and increase the quality and effectiveness of medicines use
What action could we take to improve our medication safety processes?
Relevant documentation from meetings or other communications that include rates of medication adverse events, incidents and near misses, and any improvement actions
Education resources on the quality use of medications and tools to assist with the implementation of improvement strategies
Attendance records of training in medication safety
Other _____________________________________________________
No further action is required
Yes list source of evidence
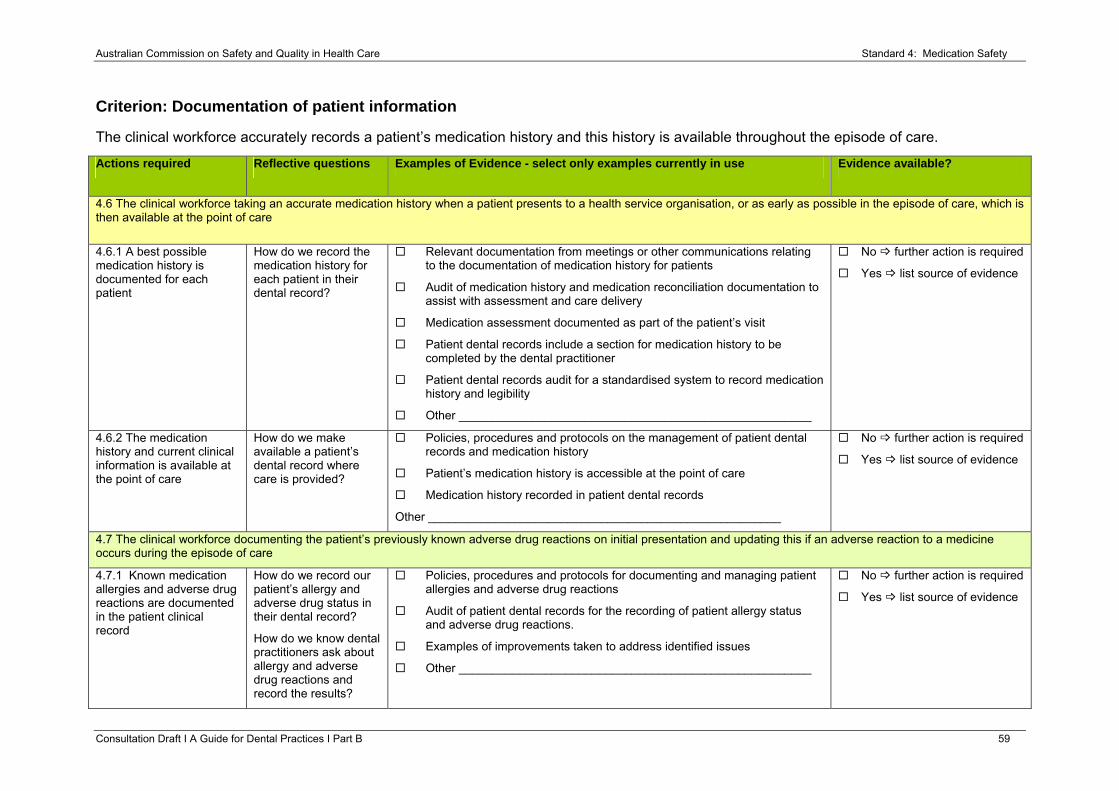
Australian Commission on Safety and Quality in Health Care Standard 4: Medication Safety
Consultation Draft Ι A Guide for Dental Practices Ι Part B 59
Criterion: Documentation of patient information
The clinical workforce accurately records a patient’s medication history and this history is available throughout the episode of care.
Actions required Reflective questions Examples of Evidence - select only examples currently in use Evidence available?
4.6 The clinical workforce taking an accurate medication history when a patient presents to a health service organisation, or as early as possible in the episode of care, which is then available at the point of care
4.6.1 A best possible medication history is documented for each patient
How do we record the medication history for each patient in their dental record?
Relevant documentation from meetings or other communications relating to the documentation of medication history for patients
Audit of medication history and medication reconciliation documentation to assist with assessment and care delivery
Medication assessment documented as part of the patient’s visit
Patient dental records include a section for medication history to be completed by the dental practitioner
Patient dental records audit for a standardised system to record medication history and legibility
Other _____________________________________________________
No further action is required
Yes list source of evidence
4.6.2 The medication history and current clinical information is available at the point of care
How do we make available a patient’s dental record where care is provided?
Policies, procedures and protocols on the management of patient dental records and medication history
Patient’s medication history is accessible at the point of care
Medication history recorded in patient dental records
Other _____________________________________________________
No further action is required
Yes list source of evidence
4.7 The clinical workforce documenting the patient’s previously known adverse drug reactions on initial presentation and updating this if an adverse reaction to a medicine occurs during the episode of care
4.7.1 Known medication allergies and adverse drug reactions are documented in the patient clinical record
How do we record our patient’s allergy and adverse drug status in their dental record?
How do we know dental practitioners ask about allergy and adverse drug reactions and record the results?
Policies, procedures and protocols for documenting and managing patient allergies and adverse drug reactions
Audit of patient dental records for the recording of patient allergy status and adverse drug reactions.
Examples of improvements taken to address identified issues
Other _____________________________________________________
No further action is required
Yes list source of evidence
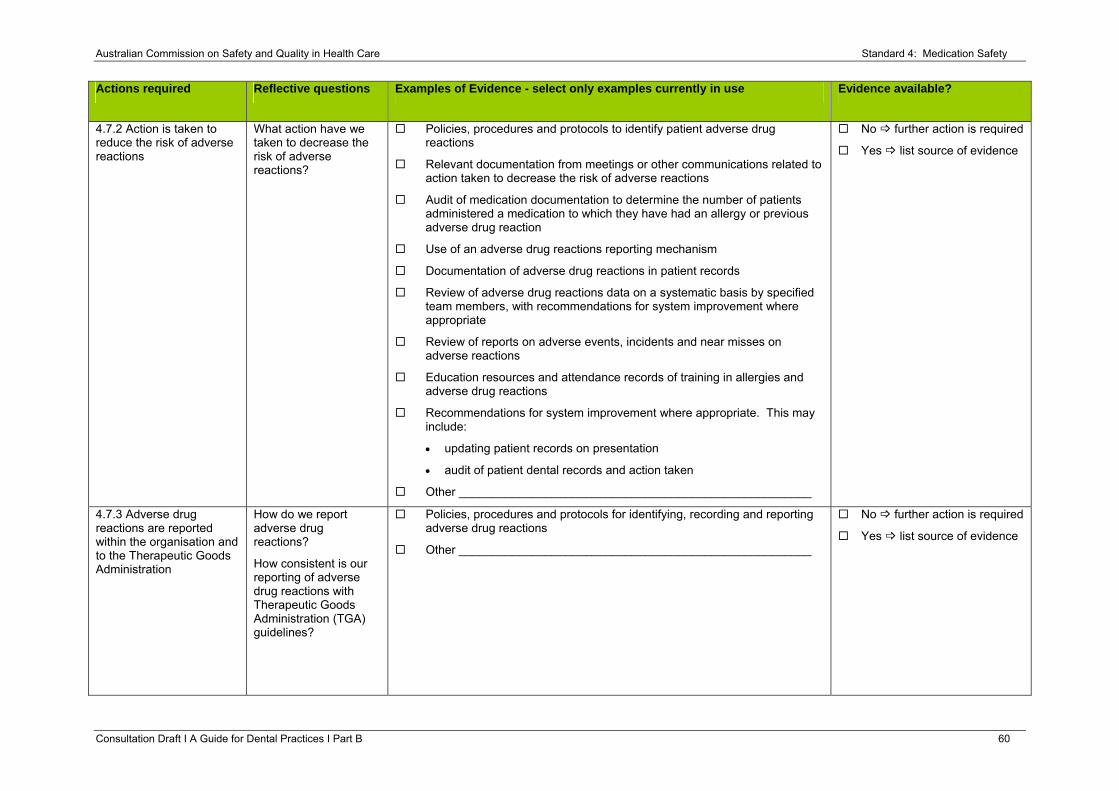
Australian Commission on Safety and Quality in Health Care Standard 4: Medication Safety
Consultation Draft Ι A Guide for Dental Practices Ι Part B 60
Actions required Reflective questions Examples of Evidence - select only examples currently in use Evidence available?
4.7.2 Action is taken to reduce the risk of adverse reactions
What action have we taken to decrease the risk of adverse reactions?
Policies, procedures and protocols to identify patient adverse drug reactions
Relevant documentation from meetings or other communications related to action taken to decrease the risk of adverse reactions
Audit of medication documentation to determine the number of patients administered a medication to which they have had an allergy or previous adverse drug reaction
Use of an adverse drug reactions reporting mechanism
Documentation of adverse drug reactions in patient records
Review of adverse drug reactions data on a systematic basis by specified team members, with recommendations for system improvement where appropriate
Review of reports on adverse events, incidents and near misses on adverse reactions
Education resources and attendance records of training in allergies and adverse drug reactions
Recommendations for system improvement where appropriate. This may include:
• updating patient records on presentation
• audit of patient dental records and action taken
Other _____________________________________________________
No further action is required
Yes list source of evidence
4.7.3 Adverse drug reactions are reported within the organisation and to the Therapeutic Goods Administration
How do we report adverse drug reactions?
How consistent is our reporting of adverse drug reactions with Therapeutic Goods Administration (TGA) guidelines?
Policies, procedures and protocols for identifying, recording and reporting adverse drug reactions
Other _____________________________________________________
No further action is required
Yes list source of evidence
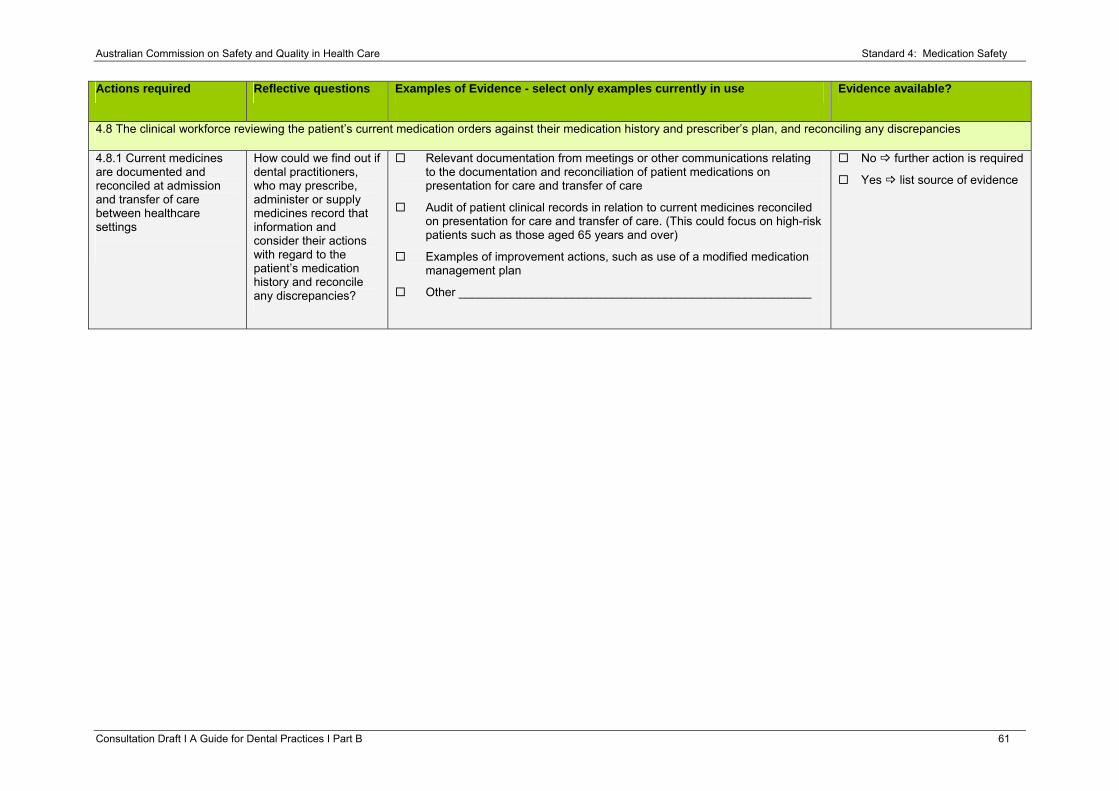
Australian Commission on Safety and Quality in Health Care Standard 4: Medication Safety
Consultation Draft Ι A Guide for Dental Practices Ι Part B 61
Actions required Reflective questions Examples of Evidence - select only examples currently in use Evidence available?
4.8 The clinical workforce reviewing the patient’s current medication orders against their medication history and prescriber’s plan, and reconciling any discrepancies
4.8.1 Current medicines are documented and reconciled at admission and transfer of care between healthcare settings
How could we find out if dental practitioners, who may prescribe, administer or supply medicines record that information and consider their actions with regard to the patient’s medication history and reconcile any discrepancies?
Relevant documentation from meetings or other communications relating to the documentation and reconciliation of patient medications on presentation for care and transfer of care
Audit of patient clinical records in relation to current medicines reconciled on presentation for care and transfer of care. (This could focus on high-risk patients such as those aged 65 years and over)
Examples of improvement actions, such as use of a modified medication management plan
Other _____________________________________________________
No further action is required
Yes list source of evidence
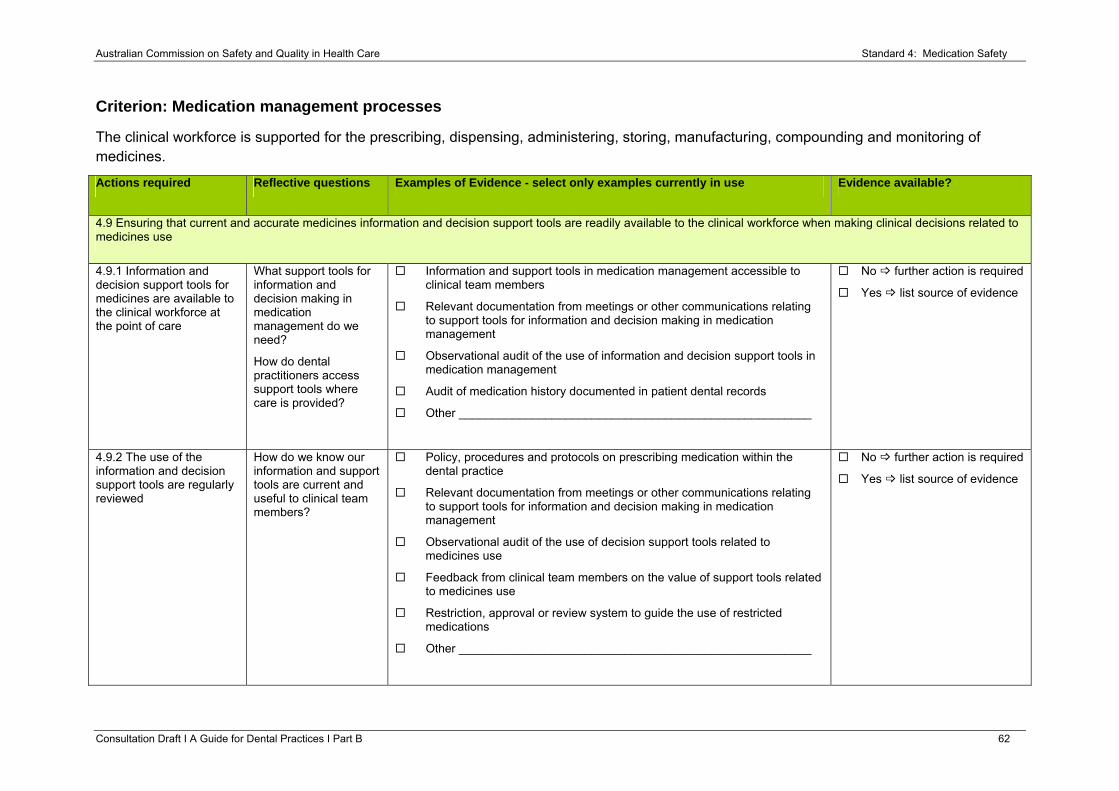
Australian Commission on Safety and Quality in Health Care Standard 4: Medication Safety
Consultation Draft Ι A Guide for Dental Practices Ι Part B 62
Criterion: Medication management processes
The clinical workforce is supported for the prescribing, dispensing, administering, storing, manufacturing, compounding and monitoring of medicines.
Actions required Reflective questions Examples of Evidence - select only examples currently in use Evidence available?
4.9 Ensuring that current and accurate medicines information and decision support tools are readily available to the clinical workforce when making clinical decisions related to medicines use
4.9.1 Information and decision support tools for medicines are available to the clinical workforce at the point of care
What support tools for information and decision making in medication management do we need?
How do dental practitioners access support tools where care is provided?
Information and support tools in medication management accessible to clinical team members
Relevant documentation from meetings or other communications relating to support tools for information and decision making in medication management
Observational audit of the use of information and decision support tools in medication management
Audit of medication history documented in patient dental records
Other _____________________________________________________
No further action is required
Yes list source of evidence
4.9.2 The use of the information and decision support tools are regularly reviewed
How do we know our information and support tools are current and useful to clinical team members?
Policy, procedures and protocols on prescribing medication within the dental practice
Relevant documentation from meetings or other communications relating to support tools for information and decision making in medication management
Observational audit of the use of decision support tools related to medicines use
Feedback from clinical team members on the value of support tools related to medicines use
Restriction, approval or review system to guide the use of restricted medications
Other _____________________________________________________
No further action is required
Yes list source of evidence
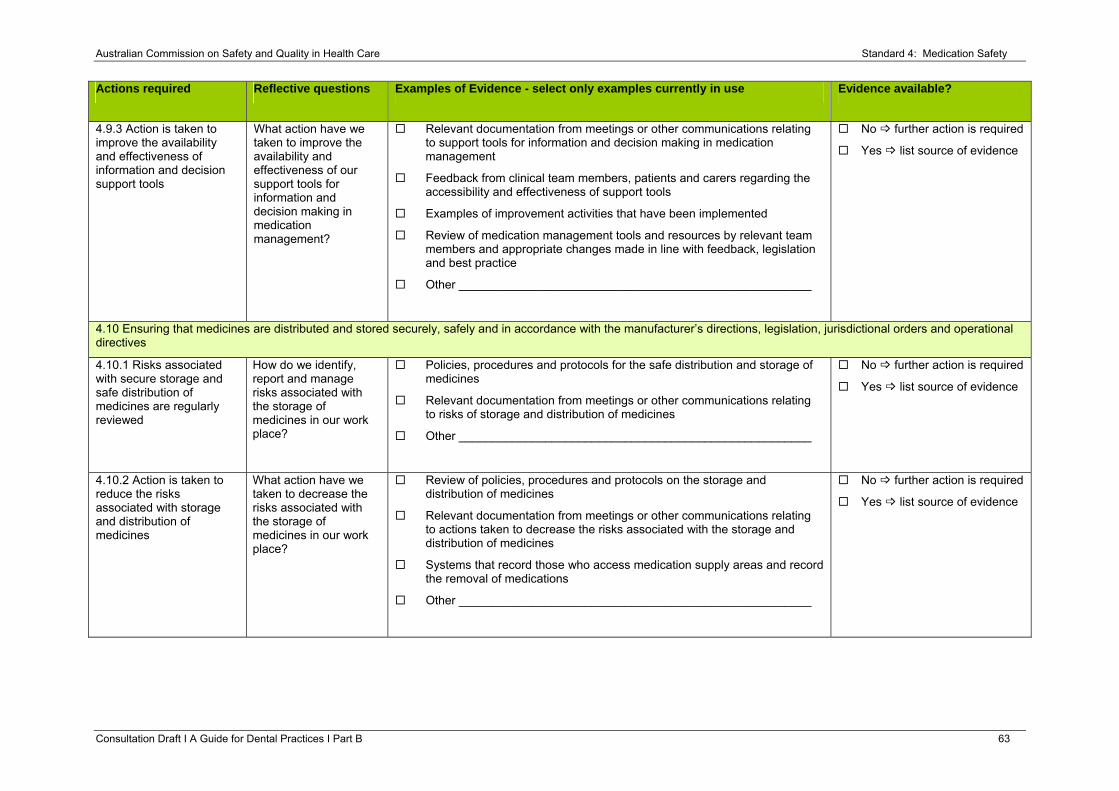
Australian Commission on Safety and Quality in Health Care Standard 4: Medication Safety
Consultation Draft Ι A Guide for Dental Practices Ι Part B 63
Actions required Reflective questions Examples of Evidence - select only examples currently in use Evidence available?
4.9.3 Action is taken to improve the availability and effectiveness of information and decision support tools
What action have we taken to improve the availability and effectiveness of our support tools for information and decision making in medication management?
Relevant documentation from meetings or other communications relating to support tools for information and decision making in medication management
Feedback from clinical team members, patients and carers regarding the accessibility and effectiveness of support tools
Examples of improvement activities that have been implemented
Review of medication management tools and resources by relevant team members and appropriate changes made in line with feedback, legislation and best practice
Other _____________________________________________________
No further action is required
Yes list source of evidence
4.10 Ensuring that medicines are distributed and stored securely, safely and in accordance with the manufacturer’s directions, legislation, jurisdictional orders and operational directives
4.10.1 Risks associated with secure storage and safe distribution of medicines are regularly reviewed
How do we identify, report and manage risks associated with the storage of medicines in our work place?
Policies, procedures and protocols for the safe distribution and storage of medicines
Relevant documentation from meetings or other communications relating to risks of storage and distribution of medicines
Other _____________________________________________________
No further action is required
Yes list source of evidence
4.10.2 Action is taken to reduce the risks associated with storage and distribution of medicines
What action have we taken to decrease the risks associated with the storage of medicines in our work place?
Review of policies, procedures and protocols on the storage and distribution of medicines
Relevant documentation from meetings or other communications relating to actions taken to decrease the risks associated with the storage and distribution of medicines
Systems that record those who access medication supply areas and record the removal of medications
Other _____________________________________________________
No further action is required
Yes list source of evidence
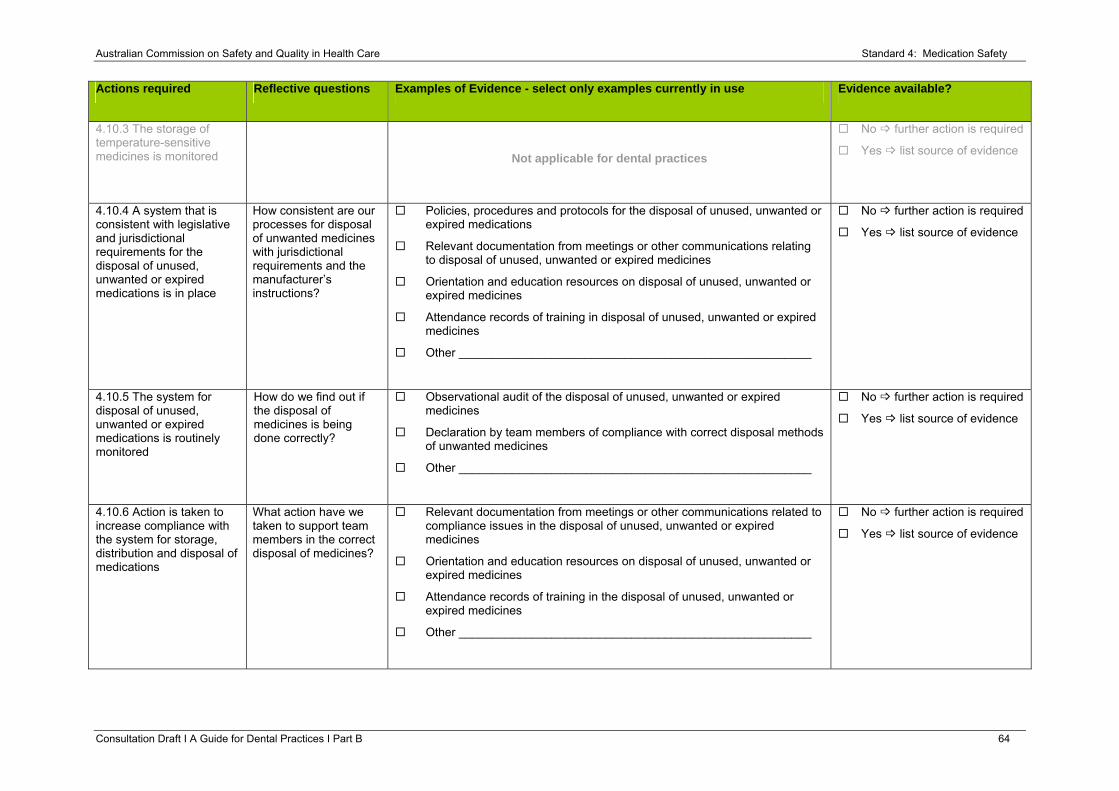
Australian Commission on Safety and Quality in Health Care Standard 4: Medication Safety
Consultation Draft Ι A Guide for Dental Practices Ι Part B 64
Actions required Reflective questions Examples of Evidence - select only examples currently in use Evidence available?
4.10.3 The storage of temperature-sensitive medicines is monitored
Not applicable for dental practices
No further action is required
Yes list source of evidence
4.10.4 A system that is consistent with legislative and jurisdictional requirements for the disposal of unused, unwanted or expired medications is in place
How consistent are our processes for disposal of unwanted medicines with jurisdictional requirements and the manufacturer’s instructions?
Policies, procedures and protocols for the disposal of unused, unwanted or expired medications
Relevant documentation from meetings or other communications relating to disposal of unused, unwanted or expired medicines
Orientation and education resources on disposal of unused, unwanted or expired medicines
Attendance records of training in disposal of unused, unwanted or expired medicines
Other _____________________________________________________
No further action is required
Yes list source of evidence
4.10.5 The system for disposal of unused, unwanted or expired medications is routinely monitored
How do we find out if the disposal of medicines is being done correctly?
Observational audit of the disposal of unused, unwanted or expired medicines
Declaration by team members of compliance with correct disposal methods of unwanted medicines
Other _____________________________________________________
No further action is required
Yes list source of evidence
4.10.6 Action is taken to increase compliance with the system for storage, distribution and disposal of medications
What action have we taken to support team members in the correct disposal of medicines?
Relevant documentation from meetings or other communications related to compliance issues in the disposal of unused, unwanted or expired medicines
Orientation and education resources on disposal of unused, unwanted or expired medicines
Attendance records of training in the disposal of unused, unwanted or expired medicines
Other _____________________________________________________
No further action is required
Yes list source of evidence
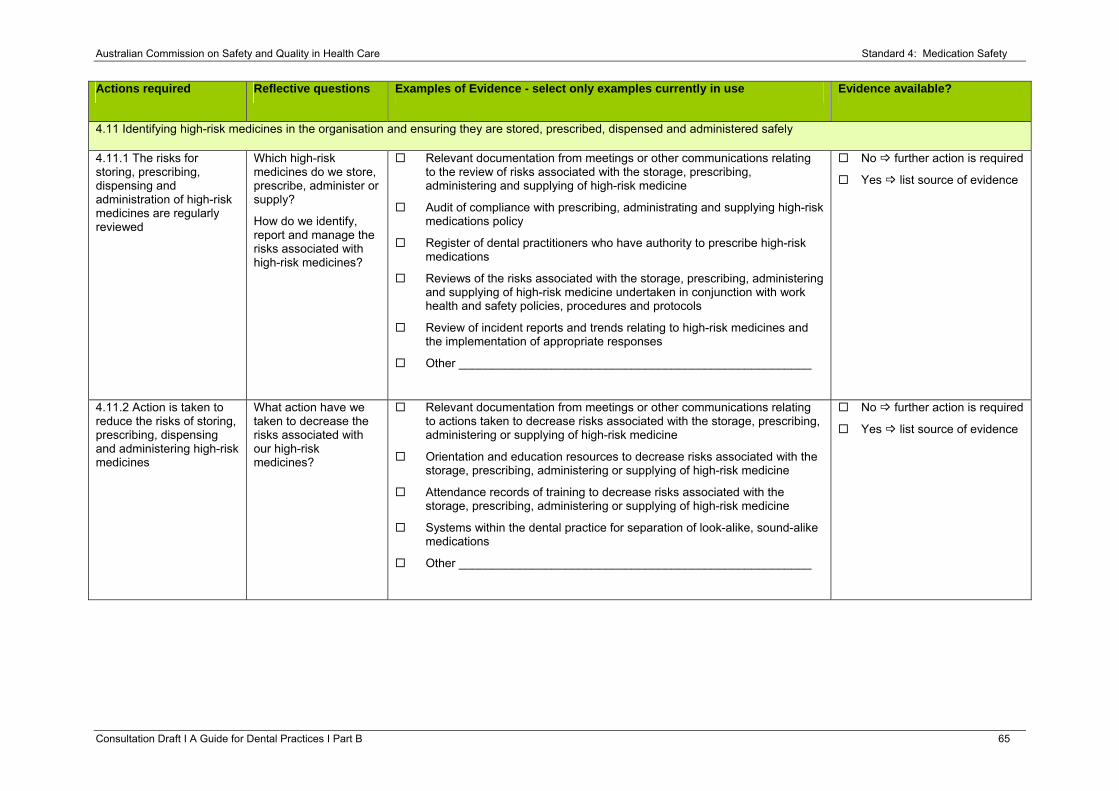
Australian Commission on Safety and Quality in Health Care Standard 4: Medication Safety
Consultation Draft Ι A Guide for Dental Practices Ι Part B 65
Actions required Reflective questions Examples of Evidence - select only examples currently in use Evidence available?
4.11 Identifying high-risk medicines in the organisation and ensuring they are stored, prescribed, dispensed and administered safely
4.11.1 The risks for storing, prescribing, dispensing and administration of high-risk medicines are regularly reviewed
Which high-risk medicines do we store, prescribe, administer or supply?
How do we identify, report and manage the risks associated with high-risk medicines?
Relevant documentation from meetings or other communications relating to the review of risks associated with the storage, prescribing, administering and supplying of high-risk medicine
Audit of compliance with prescribing, administrating and supplying high-risk medications policy
Register of dental practitioners who have authority to prescribe high-risk medications
Reviews of the risks associated with the storage, prescribing, administering and supplying of high-risk medicine undertaken in conjunction with work health and safety policies, procedures and protocols
Review of incident reports and trends relating to high-risk medicines and the implementation of appropriate responses
Other _____________________________________________________
No further action is required
Yes list source of evidence
4.11.2 Action is taken to reduce the risks of storing, prescribing, dispensing and administering high-risk medicines
What action have we taken to decrease the risks associated with our high-risk medicines?
Relevant documentation from meetings or other communications relating to actions taken to decrease risks associated with the storage, prescribing, administering or supplying of high-risk medicine
Orientation and education resources to decrease risks associated with the storage, prescribing, administering or supplying of high-risk medicine
Attendance records of training to decrease risks associated with the storage, prescribing, administering or supplying of high-risk medicine
Systems within the dental practice for separation of look-alike, sound-alike medications
Other _____________________________________________________
No further action is required
Yes list source of evidence
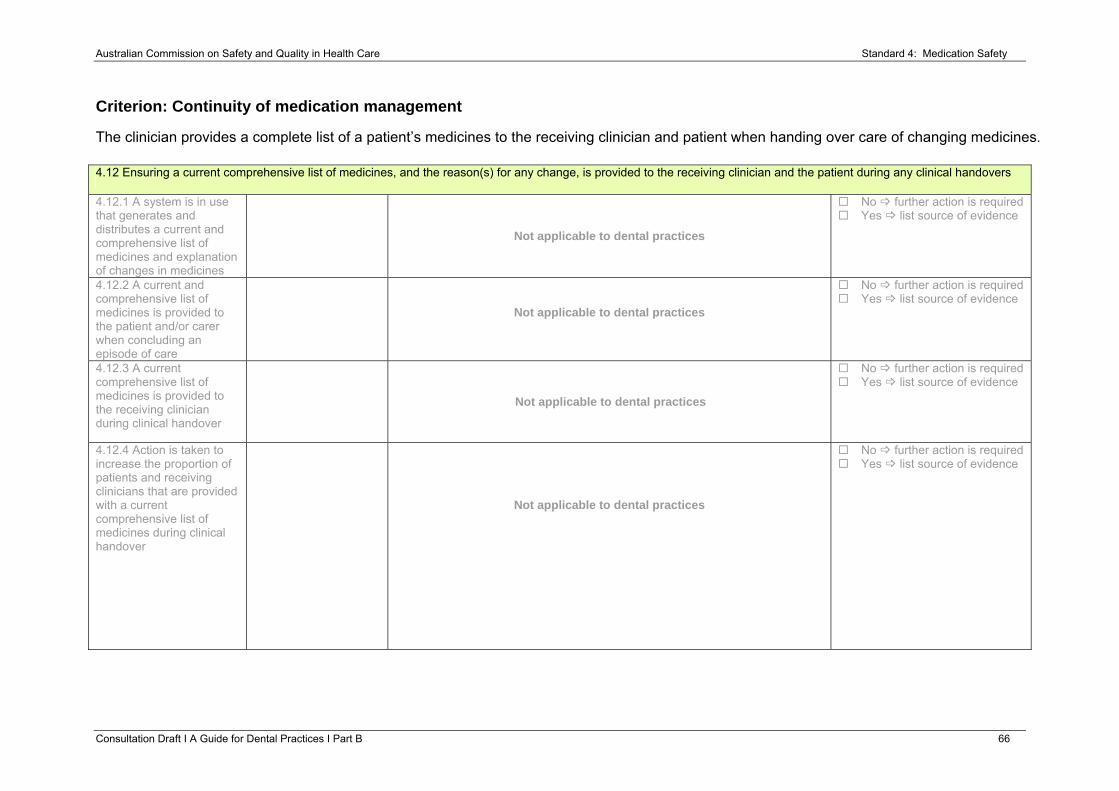
Australian Commission on Safety and Quality in Health Care Standard 4: Medication Safety
Consultation Draft Ι A Guide for Dental Practices Ι Part B 66
Criterion: Continuity of medication management
The clinician provides a complete list of a patient’s medicines to the receiving clinician and patient when handing over care of changing medicines. 4.12 Ensuring a current comprehensive list of medicines, and the reason(s) for any change, is provided to the receiving clinician and the patient during any clinical handovers
4.12.1 A system is in use that generates and distributes a current and comprehensive list of medicines and explanation of changes in medicines
Not applicable to dental practices
No further action is required Yes list source of evidence
4.12.2 A current and comprehensive list of medicines is provided to the patient and/or carer when concluding an episode of care
Not applicable to dental practices
No further action is required Yes list source of evidence
4.12.3 A current comprehensive list of medicines is provided to the receiving clinician during clinical handover
Not applicable to dental practices
No further action is required Yes list source of evidence
4.12.4 Action is taken to increase the proportion of patients and receiving clinicians that are provided with a current comprehensive list of medicines during clinical handover
Not applicable to dental practices
No further action is required Yes list source of evidence
Australian Commission on Safety and Quality in Health Care Standard 4: Medication Safety
Consultation Draft Ι A Guide for Dental Practices Ι Part B 67
Criterion: Communication with patients and carers
The clinical workforce informs patients about their options, risks and responsibilities for an agreed medication management plan.
Actions required Reflective questions Examples of Evidence - select only examples currently in use Evidence available?
4.13 The clinical workforce informing patients and carers about medication treatment options, benefits and associated risks
4.13.1 The clinical workforce provides patients with patient-specific medicine information, including medical treatment options, benefits and associated risks
How do we inform our patients about their care options including the use of medicines?
Relevant documentation from meetings or other communications relating to the provision of patient-specific medicine information, including medication treatment options, benefits and associated risks
Patient dental records show that medicines information was provided to patients
Examples of material provided to patients and carers on medicines, such as brochures, fact sheets and appropriate websites
Audit of documentation provided to patients and carers that may be contained in patient dental records or stored on computer systems
Feedback from patients and carers on the provision of patient-specific medicine information, including medication treatment options, benefits and associated risks
Other _____________________________________________________
No further action is required
Yes list source of evidence
4.13.2 Information that is designed for distribution to patients is readily available to the clinical workforce
How do we make available information to a patient or carer about care options?
Education materials and resources provided to patients and carers by team members such as brochures, handouts and fact sheets
Observational audit of the availability or patient and carer information material
Feedback from patients and carers on the suitability of information provided by the dental practice
Orientation and education resources on patient and carer information material
Other _____________________________________________________
No further action is required
Yes list source of evidence
Australian Commission on Safety and Quality in Health Care Standard 4: Medication Safety
Consultation Draft Ι A Guide for Dental Practices Ι Part B 68
Actions required Reflective questions Examples of Evidence - select only examples currently in use Evidence available?
4.14 Developing a medication management plan in partnership with patients and carers
4.14.1 An agreed medication management plan is documented and available in the patient’s clinical record
Not applicable to dental practices
No further action is required
Yes list source of evidence
4.15 Providing current medicines information to patients in a format that meets their needs whenever new medicines are prescribed or dispensed
4.15.1 Information on medicines is provided to patients and carers in a format that is understood and meaningful
Not applicable to dental practices
No further action is required
Yes list source of evidence
4.15.2 Action is taken in response to patient feedback to improve medicines information distributed by the health service organisation to patients
Not applicable to dental practices
No further action is required
Yes list source of evidence
Australian Commission on Safety and Quality in Health Care Standard 4: Medication Safety
Resources
1. Australian Pharmaceutical Advisory Council (APAC), Guiding principles for medication management in the community. Canberra: Commonwealth of Australia 2006
2. Australian Pharmaceutical Advisory Council (APAC), Guiding principles to achieve continuity in medication management. Canberra: Commonwealth of Australia 2005
3. Group Medication Safety Self Assessment for Australian Hospitals. Clinical Excellence Commission and NSW Therapeutic Advisory (Accessed 2012, 08 June, at http://www.cec.health.nsw.gov.au/programs/mssa.)
4. Indicators for Quality Use of Medicines in Australian Hospitals. NSW Therapeutic Advisory Group (Accessed 2012, 08 June, http://www.cec.health.nsw.gov.au/programs/medication-safety.)
5. Medication Safety Self Assessment for Antithrombotic Therapy in Australian Hospitals. Clinical Excellence Commission and NSW Therapeutic Advisory Group (Accessed 2012, 08 June, at http://mssa.cec.health.nsw.gov.au/at2/MSSAT_introduction.html.)
6. National Medicines Policy (2000) (Accessed 2012, 08 June, http://www.health.gov.au/internet/publishing.nsf/content/nmp-objectives-policy.htm.)
7. Additional information on high risk medications can be found at the Institute for Safe Medication Practices (ISMP) http://www.ismp.org
Consultation Draft Ι A Guide for Dental Practices Ι Part B 69
Australian Commission on Safety and Quality in Health Care Standard 5: Patient Identification and Procedure Matching
Standard 5: Patient Identification and Procedure Matching Clinical leaders and senior managers of a health service organisation establish systems to ensure the correct identification of patients and correct matching of patients with their intended treatment. Clinicians and other members of the workforce use the patient identification and procedure matching systems.
The intention of this Standard is to:
Correctly identify all patients whenever care is provided and correctly match patients to their intended treatment.
Context
It is expected that this Standard will be applied in conjunction with Standard 1, ‘Governance for Safety and Quality in Health Service Organisations’ and Standard 2, ‘Partnering with Consumers’.
Criteria to achieve the Patient Identification and Procedure Matching Standard:
• Identification of individual patients
• Processes to transfer care
• Processes to match patients and their care
Consultation Draft Ι A Guide for Dental Practices Ι Part B 70
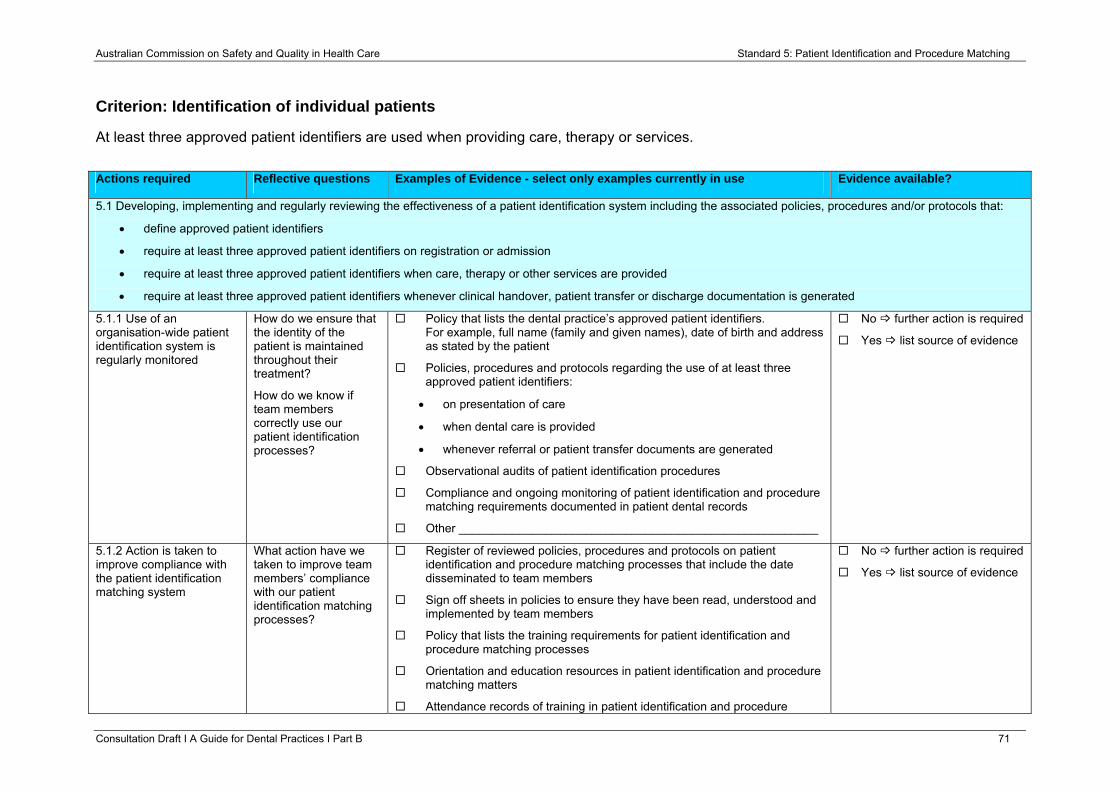
Australian Commission on Safety and Quality in Health Care Standard 5: Patient Identification and Procedure Matching
Criterion: Identification of individual patients
At least three approved patient identifiers are used when providing care, therapy or services.
Actions required Reflective questions Examples of Evidence - select only examples currently in use Evidence available?
5.1 Developing, implementing and regularly reviewing the effectiveness of a patient identification system including the associated policies, procedures and/or protocols that:
• define approved patient identifiers
• require at least three approved patient identifiers on registration or admission
• require at least three approved patient identifiers when care, therapy or other services are provided
• require at least three approved patient identifiers whenever clinical handover, patient transfer or discharge documentation is generated
5.1.1 Use of an organisation-wide patient identification system is regularly monitored
How do we ensure that the identity of the patient is maintained throughout their treatment?
How do we know if team members correctly use our patient identification processes?
Policy that lists the dental practice’s approved patient identifiers. For example, full name (family and given names), date of birth and address as stated by the patient
Policies, procedures and protocols regarding the use of at least three approved patient identifiers:
• on presentation of care
• when dental care is provided
• whenever referral or patient transfer documents are generated
Observational audits of patient identification procedures
Compliance and ongoing monitoring of patient identification and procedure matching requirements documented in patient dental records
Other ______________________________________________________
No further action is required
Yes list source of evidence
5.1.2 Action is taken to improve compliance with the patient identification matching system
What action have we taken to improve team members’ compliance with our patient identification matching processes?
Register of reviewed policies, procedures and protocols on patient identification and procedure matching processes that include the date disseminated to team members
Sign off sheets in policies to ensure they have been read, understood and implemented by team members
Policy that lists the training requirements for patient identification and procedure matching processes
Orientation and education resources in patient identification and procedure matching matters
Attendance records of training in patient identification and procedure
No further action is required
Yes list source of evidence
Consultation Draft Ι A Guide for Dental Practices Ι Part B 71
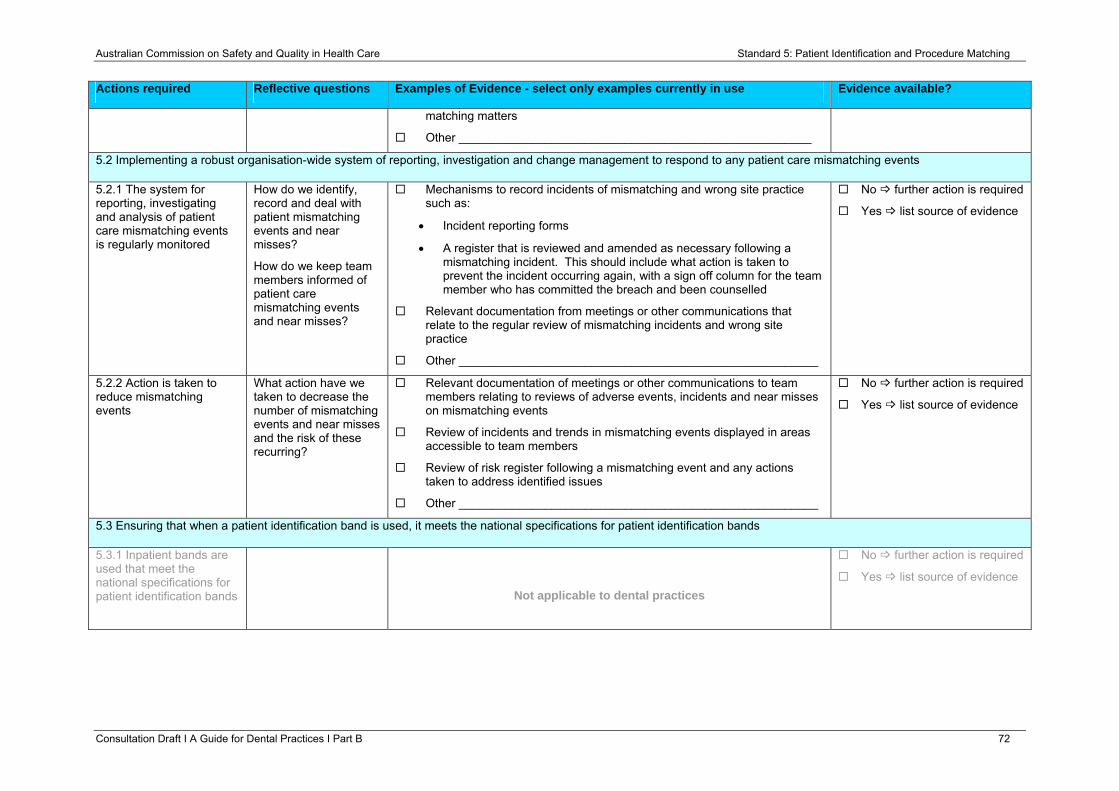
Australian Commission on Safety and Quality in Health Care Standard 5: Patient Identification and Procedure Matching
Actions required Reflective questions Examples of Evidence - select only examples currently in use Evidence available?
matching matters
Other _____________________________________________________
5.2 Implementing a robust organisation-wide system of reporting, investigation and change management to respond to any patient care mismatching events
5.2.1 The system for reporting, investigating and analysis of patient care mismatching events is regularly monitored
How do we identify, record and deal with patient mismatching events and near misses?
How do we keep team members informed of patient care mismatching events and near misses?
Mechanisms to record incidents of mismatching and wrong site practice such as:
• Incident reporting forms
• A register that is reviewed and amended as necessary following a mismatching incident. This should include what action is taken to prevent the incident occurring again, with a sign off column for the team member who has committed the breach and been counselled
Relevant documentation from meetings or other communications that relate to the regular review of mismatching incidents and wrong site practice
Other ______________________________________________________
No further action is required
Yes list source of evidence
5.2.2 Action is taken to reduce mismatching events
What action have we taken to decrease the number of mismatching events and near misses and the risk of these recurring?
Relevant documentation of meetings or other communications to team members relating to reviews of adverse events, incidents and near misses on mismatching events
Review of incidents and trends in mismatching events displayed in areas accessible to team members
Review of risk register following a mismatching event and any actions taken to address identified issues
Other ______________________________________________________
No further action is required
Yes list source of evidence
5.3 Ensuring that when a patient identification band is used, it meets the national specifications for patient identification bands
5.3.1 Inpatient bands are used that meet the national specifications for patient identification bands
Not applicable to dental practices
No further action is required
Yes list source of evidence
Consultation Draft Ι A Guide for Dental Practices Ι Part B 72
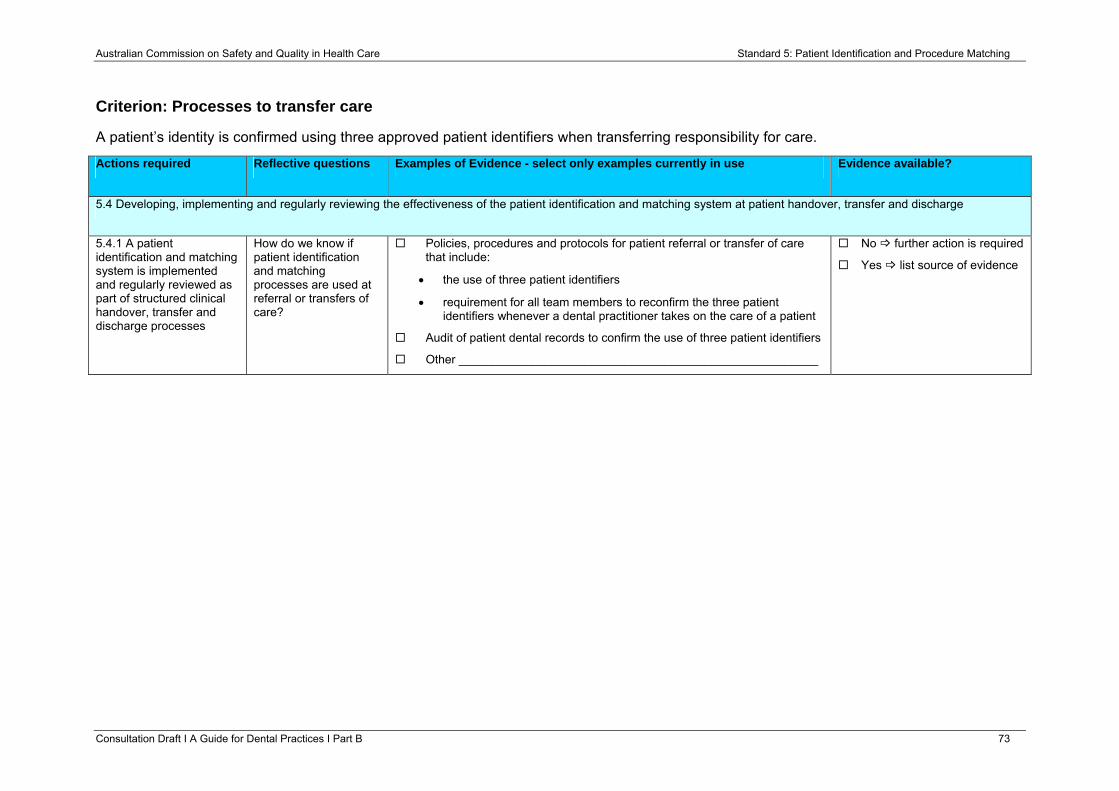
Australian Commission on Safety and Quality in Health Care Standard 5: Patient Identification and Procedure Matching
Criterion: Processes to transfer care
A patient’s identity is confirmed using three approved patient identifiers when transferring responsibility for care.
Actions required Reflective questions Examples of Evidence - select only examples currently in use Evidence available?
5.4 Developing, implementing and regularly reviewing the effectiveness of the patient identification and matching system at patient handover, transfer and discharge
5.4.1 A patient identification and matching system is implemented and regularly reviewed as part of structured clinical handover, transfer and discharge processes
How do we know if patient identification and matching processes are used at referral or transfers of care?
Policies, procedures and protocols for patient referral or transfer of care that include:
• the use of three patient identifiers
• requirement for all team members to reconfirm the three patient identifiers whenever a dental practitioner takes on the care of a patient
Audit of patient dental records to confirm the use of three patient identifiers
Other ______________________________________________________
No further action is required
Yes list source of evidence
Consultation Draft Ι A Guide for Dental Practices Ι Part B 73
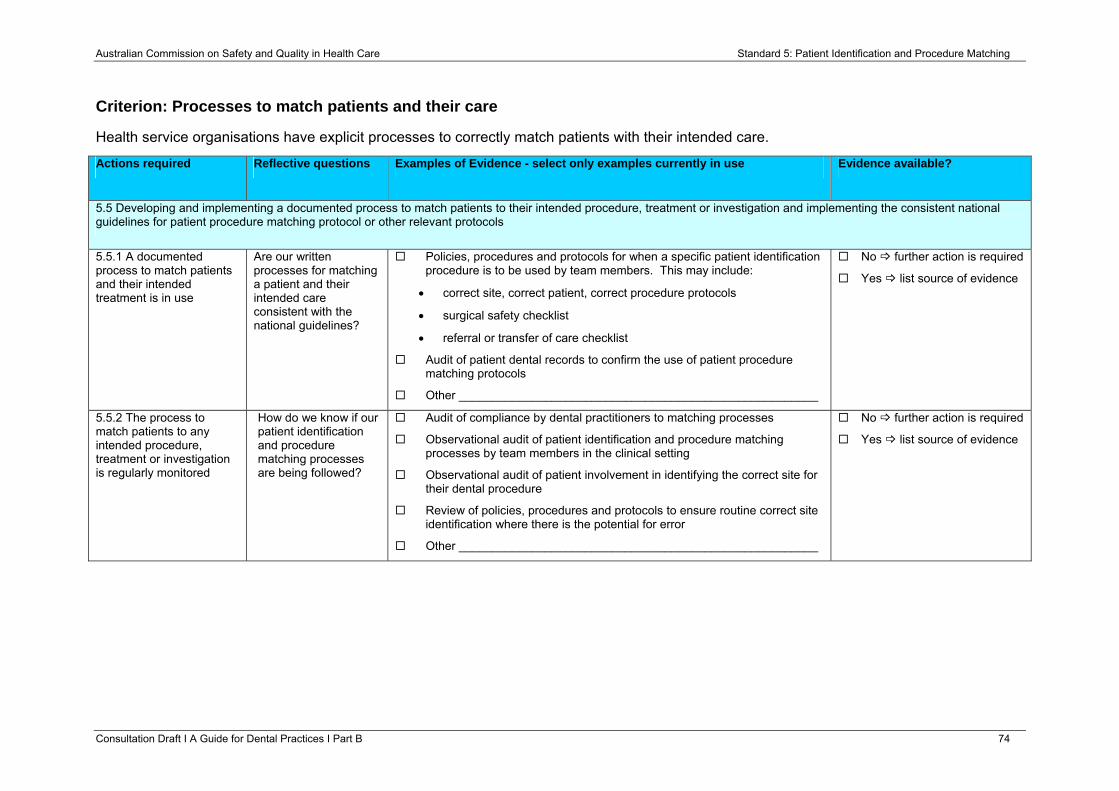
Australian Commission on Safety and Quality in Health Care Standard 5: Patient Identification and Procedure Matching
Criterion: Processes to match patients and their care
Health service organisations have explicit processes to correctly match patients with their intended care.
Actions required Reflective questions Examples of Evidence - select only examples currently in use Evidence available?
5.5 Developing and implementing a documented process to match patients to their intended procedure, treatment or investigation and implementing the consistent national guidelines for patient procedure matching protocol or other relevant protocols
5.5.1 A documented process to match patients and their intended treatment is in use
Are our written processes for matching a patient and their intended care consistent with the national guidelines?
Policies, procedures and protocols for when a specific patient identification procedure is to be used by team members. This may include:
• correct site, correct patient, correct procedure protocols
• surgical safety checklist
• referral or transfer of care checklist
Audit of patient dental records to confirm the use of patient procedure matching protocols
Other ______________________________________________________
No further action is required
Yes list source of evidence
5.5.2 The process to match patients to any intended procedure, treatment or investigation is regularly monitored
How do we know if our patient identification and procedure matching processes are being followed?
Audit of compliance by dental practitioners to matching processes
Observational audit of patient identification and procedure matching processes by team members in the clinical setting
Observational audit of patient involvement in identifying the correct site for their dental procedure
Review of policies, procedures and protocols to ensure routine correct site identification where there is the potential for error
Other ______________________________________________________
No further action is required
Yes list source of evidence
Consultation Draft Ι A Guide for Dental Practices Ι Part B 74
Australian Commission on Safety and Quality in Health Care Standard 5: Patient Identification and Procedure Matching
Consultation Draft Ι A Guide for Dental Practices Ι Part B 75
Actions required Reflective questions Examples of Evidence - select only examples currently in use Evidence available?
5.5.3 Action is taken to improve the effectiveness of the process for matching patients to their intended procedure, treatment or investigation
What action has been taken to improve our patient identification and procedure matching processes?
Policies, procedures and protocols for patient identification and procedure matching are reviewed and updated
Register of patient identification and procedure matching improvement activities and action plans
Examples of improvement activities that have been implemented and evaluated to improve patient identification and procedure matching processes
Relevant documentation from meetings or other communications to team members about patient identification and procedure matching improvement activities
Other ______________________________________________________
No further action is required
Yes list source of evidence
Resources
1. Ensuring Correct Patient, Correct Site, Correct Procedure in Oral Surgery, 2008. (Accessed 12 June 2012, at
http://www.safetyandquality.gov.au/wp-content/uploads/2012/01/Protocol_OralSurgery.pdf.)
2. Standards Australia. HB 222-2006 Australian Health Care Client and Provider Identification Handbook. Sydney: Standards Australia, 2006.
3. Standards Australia. AS5017-2006 Health Care Client Identification. Sydney: Standards Australia, 2006.
Australian Commission on Safety and Quality in Health Care Standard 6: Clinical Handover
Standard 6: Clinical Handover Clinical leaders and senior managers of a health service organisation implement documented systems for effective and structured clinical handover. Clinicians and other members of the workforce use the clinical handover systems.
Clinical handover is the transfer of professional responsibility and accountability for some or all aspects of care for a patient or group of patients, to another person or professional group on a temporary or permanent basis12.
The intention of this Standard is to:
Ensure there is timely, relevant and structured clinical handover that supports safe patient care.
Context
It is expected that this Standard will be applied in conjunction with Standard 1, ‘Governance for Safety and Quality in Health Service Organisations’ and Standard 2, ‘Partnering with Consumers’.
Criteria to achieve the Clinical Handover Standard:
• Governance and leadership for effective clinical handover
• Clinical handover processes
• Patient and carer involvement in clinical handover
Consultation Draft Ι A Guide for Dental Practices Ι Part B 76
Australian Commission on Safety and Quality in Health Care Standard 6: Clinical Handover
Criterion: Governance and leadership for effective clinical handover
Health Service organisations implement clinical handover systems.
Actions required Reflective questions Examples of Evidence - select only examples currently in use Evidence available?
6.1 Developing and implementing an organisational system for structured clinical handover that is relevant to the healthcare setting and specialities, including:
• documented policy, procedures and/or protocols
• agreed tools and guides
6.1.1 Clinical handover policies, procedures and/or protocols are used by the workforce and regularly monitored
How do we describe our process for clinical handover resulting in a transfer of care and accountability to another healthcare practitioner or organisation?
How do we know that our clinical handovers are being done correctly?
Policies, procedures and protocols for clinical handover occuring between practitioners within the practice and outside of the dental practice
Audit of the use of clinical handover tools and processes such as:
• checklists
• transfer forms
• referral proforma documents
• database entries
Other ______________________________________________________
No further action is required
Yes list source of evidence
6.1.2 Action is taken to maximise the effectiveness of clinical handover policies, procedures and/or protocols
What action have we taken to improve the guidance to team members on clinical handover?
Relevant documentation from meetings or other communications to team members regarding clinical handover matters
Education resources and training sessions on referral or patient transfer matters
Other ______________________________________________________
No further action is required
Yes list source of evidence
6.1.3 Tools and guides are periodically reviewed
What tools and guides do we use to assist in clinical handover and how often do we review them?
A system for checking patient dental records for clinical handover processes
Tools and guides on clinical handover are reviewed, updated or modified in line with best practice guides or emerging information
Other ______________________________________________________
No further action is required
Yes list source of evidence
Consultation Draft Ι A Guide for Dental Practices Ι Part B 77
Australian Commission on Safety and Quality in Health Care Standard 6: Clinical Handover
Criterion: Clinical handover processes
Health service organisations have in place documented and structured clinical handover processes in place.
Actions required Reflective questions Examples of Evidence - select only examples currently in use Evidence available?
6.2 Establishing and maintaining structured and documented processes for clinical handover
6.2.1 The workforce has access to documented structured processes for clinical handover that include:
• preparing for handover, including setting the location and time whilst maintaining continuity of patient care
• organising relevant workforce members to participate
• being aware of the clinical context and patient needs
• participating in effective handover resulting in transfer of responsibility and accountability for care
What could be the best clinical handover processes to use for our patients?
How could we document and keep our clinical handover processes current?
Policy and guideline documentation on clinical handover included in orientation resources or manuals
Education resources and attendance records of training clinical handover processes
Tools and resources associated with the structured clinical handover process are available to team members. For example clinical handover sheets in patient dental records
Other ______________________________________________________
No further action is required
Yes list source of evidence
Consultation Draft Ι A Guide for Dental Practices Ι Part B 78
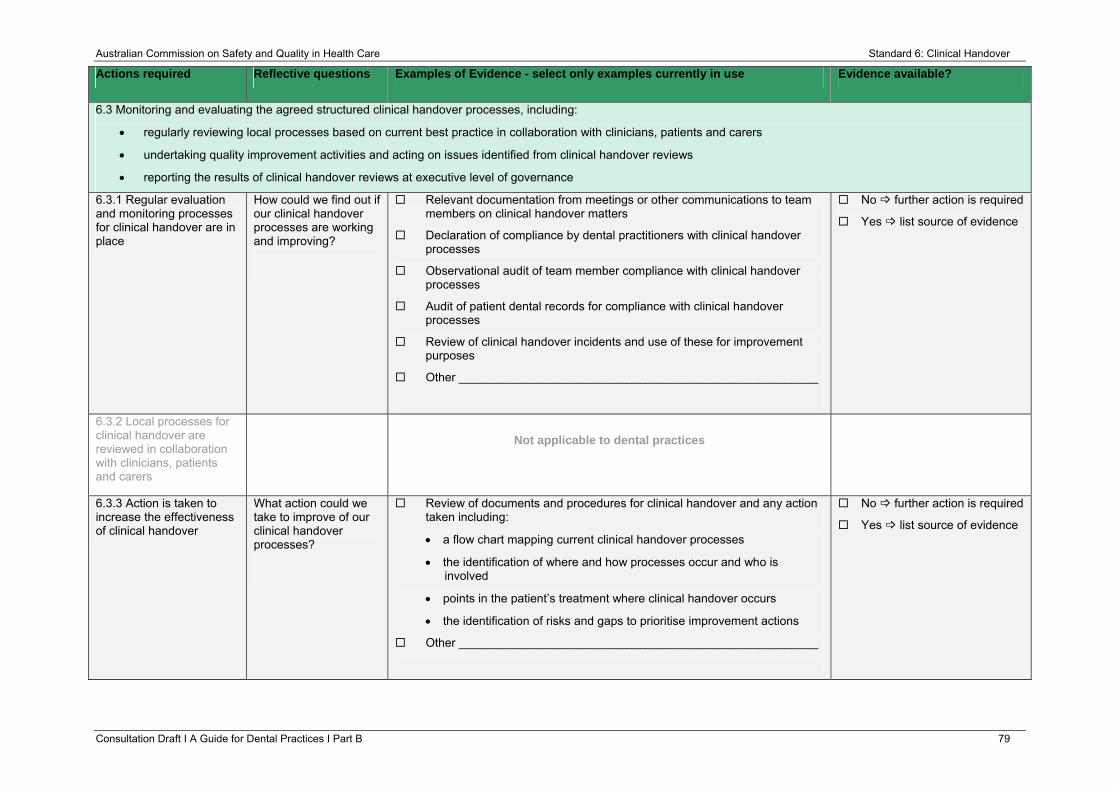
Australian Commission on Safety and Quality in Health Care Standard 6: Clinical Handover
Actions required Reflective questions Examples of Evidence - select only examples currently in use Evidence available?
6.3 Monitoring and evaluating the agreed structured clinical handover processes, including:
• regularly reviewing local processes based on current best practice in collaboration with clinicians, patients and carers
• undertaking quality improvement activities and acting on issues identified from clinical handover reviews
• reporting the results of clinical handover reviews at executive level of governance
6.3.1 Regular evaluation and monitoring processes for clinical handover are in place
How could we find out if our clinical handover processes are working and improving?
Relevant documentation from meetings or other communications to team members on clinical handover matters
Declaration of compliance by dental practitioners with clinical handover processes
Observational audit of team member compliance with clinical handover processes
Audit of patient dental records for compliance with clinical handover processes
Review of clinical handover incidents and use of these for improvement purposes
Other ______________________________________________________
No further action is required
Yes list source of evidence
6.3.2 Local processes for clinical handover are reviewed in collaboration with clinicians, patients and carers
Not applicable to dental practices
6.3.3 Action is taken to increase the effectiveness of clinical handover
What action could we take to improve of our clinical handover processes?
Review of documents and procedures for clinical handover and any action taken including:
• a flow chart mapping current clinical handover processes
• the identification of where and how processes occur and who is involved
• points in the patient’s treatment where clinical handover occurs
• the identification of risks and gaps to prioritise improvement actions
Other ______________________________________________________
No further action is required
Yes list source of evidence
Consultation Draft Ι A Guide for Dental Practices Ι Part B 79
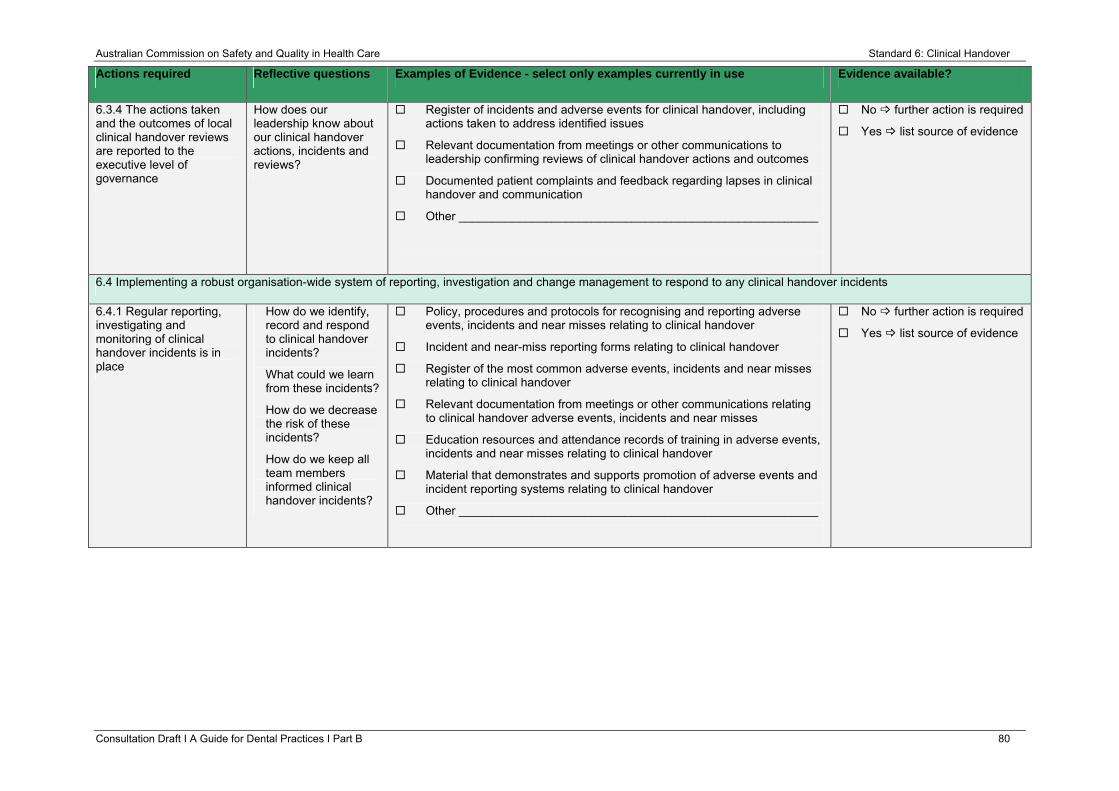
Australian Commission on Safety and Quality in Health Care Standard 6: Clinical Handover
Actions required Reflective questions Examples of Evidence - select only examples currently in use Evidence available?
6.3.4 The actions taken and the outcomes of local clinical handover reviews are reported to the executive level of governance
How does our leadership know about our clinical handover actions, incidents and reviews?
Register of incidents and adverse events for clinical handover, including actions taken to address identified issues
Relevant documentation from meetings or other communications to leadership confirming reviews of clinical handover actions and outcomes
Documented patient complaints and feedback regarding lapses in clinical handover and communication
Other ______________________________________________________
No further action is required
Yes list source of evidence
6.4 Implementing a robust organisation-wide system of reporting, investigation and change management to respond to any clinical handover incidents
6.4.1 Regular reporting, investigating and monitoring of clinical handover incidents is in place
How do we identify, record and respond to clinical handover incidents?
What could we learn from these incidents?
How do we decrease the risk of these incidents?
How do we keep all team members informed clinical handover incidents?
Policy, procedures and protocols for recognising and reporting adverse events, incidents and near misses relating to clinical handover
Incident and near-miss reporting forms relating to clinical handover
Register of the most common adverse events, incidents and near misses relating to clinical handover
Relevant documentation from meetings or other communications relating to clinical handover adverse events, incidents and near misses
Education resources and attendance records of training in adverse events, incidents and near misses relating to clinical handover
Material that demonstrates and supports promotion of adverse events and incident reporting systems relating to clinical handover
Other ______________________________________________________
No further action is required
Yes list source of evidence
Consultation Draft Ι A Guide for Dental Practices Ι Part B 80
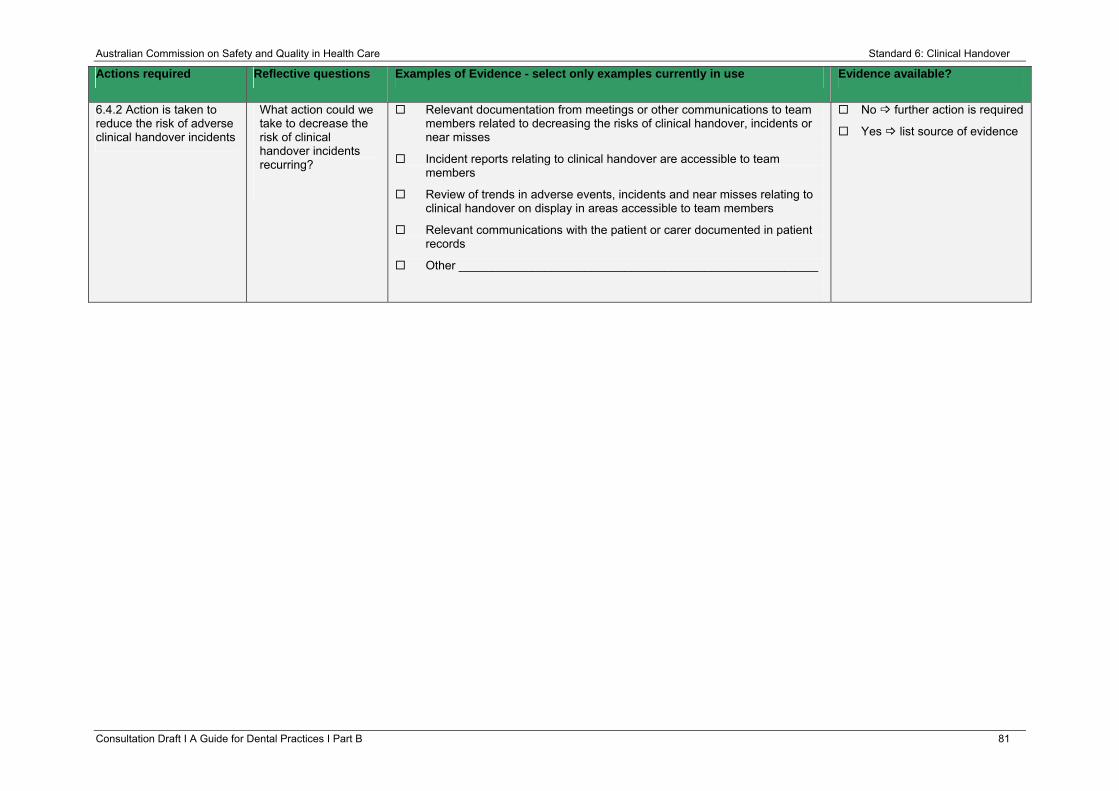
Australian Commission on Safety and Quality in Health Care Standard 6: Clinical Handover
Actions required Reflective questions Examples of Evidence - select only examples currently in use Evidence available?
6.4.2 Action is taken to reduce the risk of adverse clinical handover incidents
What action could we take to decrease the risk of clinical handover incidents recurring?
Relevant documentation from meetings or other communications to team members related to decreasing the risks of clinical handover, incidents or near misses
Incident reports relating to clinical handover are accessible to team members
Review of trends in adverse events, incidents and near misses relating to clinical handover on display in areas accessible to team members
Relevant communications with the patient or carer documented in patient records
Other ______________________________________________________
No further action is required
Yes list source of evidence
Consultation Draft Ι A Guide for Dental Practices Ι Part B 81
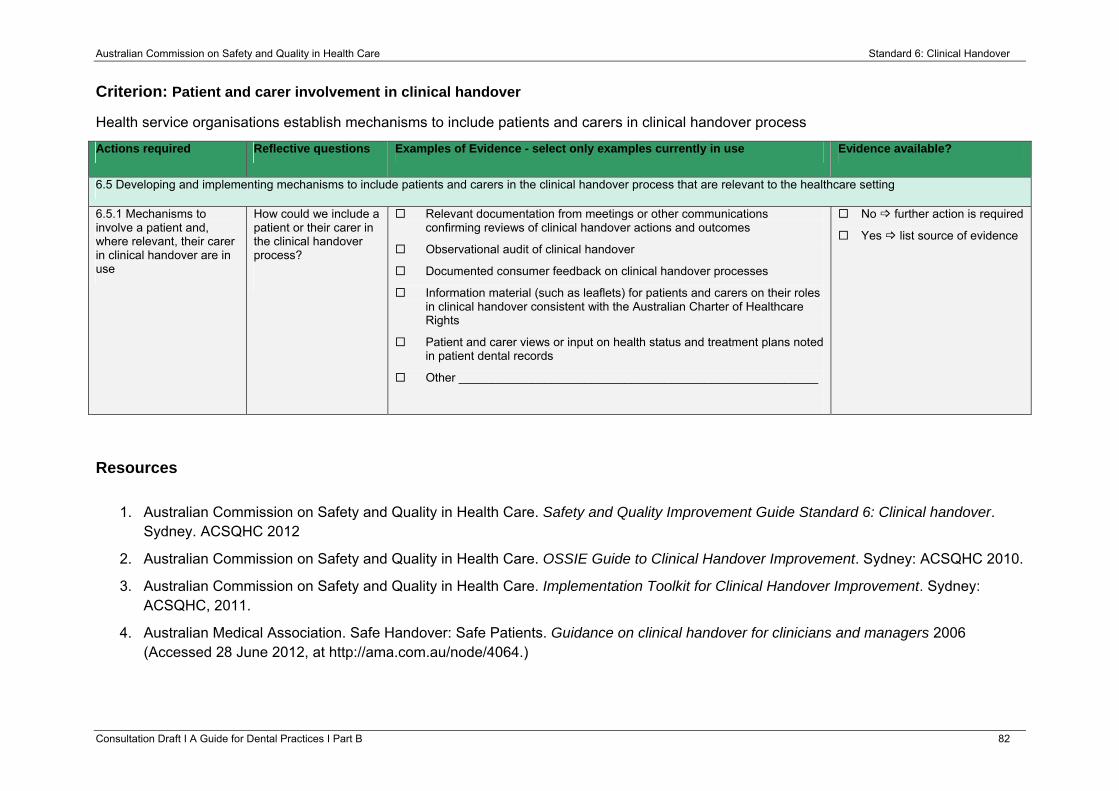
Australian Commission on Safety and Quality in Health Care Standard 6: Clinical Handover
Criterion: Patient and carer involvement in clinical handover
Health service organisations establish mechanisms to include patients and carers in clinical handover process
Actions required Reflective questions Examples of Evidence - select only examples currently in use Evidence available?
6.5 Developing and implementing mechanisms to include patients and carers in the clinical handover process that are relevant to the healthcare setting
6.5.1 Mechanisms to involve a patient and, where relevant, their carer in clinical handover are in use
How could we include a patient or their carer in the clinical handover process?
Relevant documentation from meetings or other communications confirming reviews of clinical handover actions and outcomes
Observational audit of clinical handover
Documented consumer feedback on clinical handover processes
Information material (such as leaflets) for patients and carers on their roles in clinical handover consistent with the Australian Charter of Healthcare Rights
Patient and carer views or input on health status and treatment plans noted in patient dental records
Other ______________________________________________________
No further action is required
Yes list source of evidence
Resources
1. Australian Commission on Safety and Quality in Health Care. Safety and Quality Improvement Guide Standard 6: Clinical handover.
Sydney. ACSQHC 2012
2. Australian Commission on Safety and Quality in Health Care. OSSIE Guide to Clinical Handover Improvement. Sydney: ACSQHC 2010.
3. Australian Commission on Safety and Quality in Health Care. Implementation Toolkit for Clinical Handover Improvement. Sydney: ACSQHC, 2011.
4. Australian Medical Association. Safe Handover: Safe Patients. Guidance on clinical handover for clinicians and managers 2006 (Accessed 28 June 2012, at http://ama.com.au/node/4064.)
Consultation Draft Ι A Guide for Dental Practices Ι Part B 82