A CASE OF ALLOIMMUNIZATION IN A PATIENT OF …Microsoft PowerPoint - Dr. Sonani Hb E Beta Thal...
17
A CASE OF ALLOIMMUNIZATION IN A PATIENT OF HBE BETA THALASSEMIA Dr Rajesh Sonani (Presenting Author) Dr Jaymin Bhatt Dr Shweta Gupta Dr Pritesh Rajani Dr Nidhi Bhatnagar Dr M D Gajjar
Transcript of A CASE OF ALLOIMMUNIZATION IN A PATIENT OF …Microsoft PowerPoint - Dr. Sonani Hb E Beta Thal...

A CASE OF ALLOIMMUNIZATION IN
A PATIENT OF HBE BETA
THALASSEMIA
Dr Rajesh Sonani (Presenting Author)
Dr Jaymin Bhatt
Dr Shweta Gupta
Dr Pritesh Rajani
Dr Nidhi Bhatnagar
Dr M D Gajjar

INTRODUCTION
� HbE Beta Thalassemia occurs due to
substitution of Glutamic acid by Lysine at
position 26 of the β chain.
� After HbS, it is the second most prevalent
abnormal Hemoglobin in the world, mainly in
the South-East Asian countries.

PATHOPHYSIOLOGY
� The β chain of Hemoglobin E is synthesized at a
reduced rate compared with that of Hemoglobin
A because the mutation creates an alternate
splicing site within an exon.
� This results in reduced rate of synthesis βE
chain and therefore, of HbE.

Continued..
� HbE may be present in the heterozygous
(genotype AE), homozygous ( EE or Hemoglobin
E disease) and compound heterozygous (
hemoglobin E/ β Thalassemia, Sickle
cell/hemoglobin E or SE genotype) states.
� HbE may therefore be regarded as β+
thalassemic hemoglobinopathy.

CASE REPORT
� A 23 year old female, primigravida , with history
of 7.5 months of amenorrhea was admitted to
Civil Hospital, Ahmedabad with chief complains
of abdominal pain.

PAST HISTORY
� Patient was hospitalized for anemia before 1
year where investigations showed a Positive
NESTROFT (Naked Eye Single Tube Red cell
Osmotic Fragility Test).
� Further work-up of the patient led to the
diagnosis of HbE β-Thalassemia (on High
Performance Liquid Chromatography-HPLC).
� So, at that time the patient was transfused 3
units of Packed Cell Volume at a private clinic.

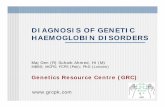
Here, HbF is 53.8 % and HbA2 is 42.4% which is consistent with HbE β
Thalassemia.
HPLC of the patient

PHYSICAL EXAMINATION(At the time of admission)
� Pallor : ++
� Vitals (Temperature, Pulse, Respiratory Rate
and BP ) : within normal range
� RS : NAD
� CVS : NAD
� CNS : NAD
� Per Abdomen : Uterine size corresponding to 30
weeks of gestation with Fetal Heart Sounds
(FHS) well heard.

Laboratory findings(At the time of admission)
� Hemoglobin : 6.6 gm/dL
� Red Cell Count : 2.96 million/cmm
� Total & Differential Count : in normal reference range
� Platelet count : 1.03 lacs/cmm
� MCV : 72 fl
� MCH : 25.1 pg
� MCHC : 34.8 gm/dL
� P / S : RBCs predominantly microcytic, mild hypochromic

ULTRASONOGRAPHY FINDINGS:
� Confirmed the findings of P/A examination.
� Also revealed hepato-splenomegaly.

� Patient delivered a live, pre-term baby
vaginally weighing 1.48 Kgs after which
patient was transfused 2 units of group
compatible Packed Cell Volume (PCV) with no
adverse reaction.
� On 10th Post-partum day, patient developed
fever with Hb falling to 3.7 gm/dL for which
she was advised by treating physician to
transfuse 4 units of PCV
� But on major Cross-match, no group
compatible units were found.

SEROLOGICAL INVESTIGATIONS
� Fresh sample was obtained which was not haemolysed with no auto-clumps.
� Cell and Serum Grouping (at room temperature)
� Direct and Indirect Antiglobulin Test : Both were Grade 3 Positive
Anti
A
Anti
B
Anti
D1
Anti
D2
A Cell B Cell O
Cell
+3 0 +3 +3 0 +3 0

Antibody Screening with DiaMed 3 and 11 Cell
Panels
Cell 1 Cell 2 Cell 3
+3 0 +3
Results of 3 cell panel as follows:
Results of 11 cell panel as follows:
1 2 3 4 5 6 7 8 9 10 11
0 4+ 4+ 0 0 4+ 4+ 4+ 0 4+ 4+

RESULTS
� The above results showed the presence of Anti K
and Anti M which might have developed as a
result of allo-immunization due to previous
blood transfusions.
� The presence of Anti M antibodies was further
confirmed by using papain which turned the
previously positive result of cell 1 in 3 cell panel
negative.

MANAGEMENT
� M antigen & K Antigen negative blood was
searched using commercial Anti M & Anti K sera.
� Patient was started on steroids
(Methylprednisone) daily.
� Subsequently, the patient underwent
splenectomy during which she was transfused
same group major cross match compatible units
with no adverse reactions to transfusion noted.
� On discharge, pt’s Hb was 10.1 gm/dL and
further follow-up has shown no significant fall in
Hb.

DISCUSSION
� After development of significant antibodies,
patients receiving multiple transfusions
present challenging task in management.
� When specific antibody is identified as in this
case, that particular antigen negative blood can
be given.
� Steroids forms the first line of treatment in
these patients followed by immuno-suppresion
with azathioprine or cyclophosphamide.
� Use of IVIg and spelenectomy is indicated in
refractory cases.

THANK YOU



![1t Hb N ojKD$F JOLIS-L X 1 K · §1.]1t}HNJDM*KXoj ⊲ Plan §0. J](https://static.fdocument.org/doc/165x107/5f78167e9c3078094e6827b3/1t-hb-n-ojkdf-jolis-l-x-1-k-11thnjdmkxoj-a-plan-0-j.jpg)