ΙΑΤΡΙΚΟ ΙΣΤΟΡΙΚΟ...Intra-Aortic Balloon Pump - Pros and Cons PROs: • Mature...
74
Transcript of ΙΑΤΡΙΚΟ ΙΣΤΟΡΙΚΟ...Intra-Aortic Balloon Pump - Pros and Cons PROs: • Mature...


ΙΑΤΡΙΚΟ ΙΣΤΟΡΙΚΟ
1997 Αντικατάσταση αορτικής βαλβίδας -μεταλλική (σοβαρού
βαθμού στένωση δίπτυχης αορτικής βαλβίδας)
1997 Βαλβιδική καρδιακή ανεπάρκεια (EF=35%)
2009 PCI LAD
2011 Εμφύτευση απινιδωτή για πρωτογενή πρόληψη (EF=25%)
ΑΙΤΙΑ ΕΙΣΑΓΩΓΗΣ ΓΙΑ ΝΟΣΗΛΕΙΑ ΑΝΔΡΑΣ 61 χρονών, υπερτασικός, μη διαβητικός, με μετρίου
βαθμού νεφρική ανεπάρκεια.
Καρδιακή ανεπάρκεια: περιφερικό οίδημα και δύσπνοια
Ηλεκτρική θύελλα: 3 εκφορτίσεις απινιδωτή για κοιλιακή
μαρμαρυγή

EF=15%

Mitral Valve: moderate to severe regurgitation

Metallic Aortic Valve: normal function

CORONARY ANGIOGRAPHY
RCA: normal AVR: normal

CORONARY ANGIOGRAPHY
severe heavily calcified distal LMS ostial LAD
ostial CX (MEDINA 1,1,1)

ΕΠΙΛΟΓΕΣ
CABG – αποκλειόμενη από χειρουργούς STS score >10
PCI – Rotablation χωρίς υποστήριξη
PCI – Rotablation με μηχανική υποστήριξη
ΑΠΟΦΑΣΗ
PCI – Rotablation με μηχανική υποστήριξη

Goals of Percutaneous Circulatory SupportDepend on the Clinical Application
• Cardiogenic shock (±AMI)/ Decompensated heart failure
–
–
–
–
–
Normalize CO, BP, Cardiac Power Output (CPO=MAP x CO)
Decrease PCWP
Optimize blood oxygen saturation
‘Bridge to Decision’ enabling
Minimize myocardial damage and optimizerecovery•
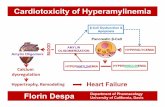
Decrease myocardial work and oxygen consumption while optimizing myocardial perfusion
• High Risk PCI– Maintain BP and CO during proximal coronary occlusion to maximize CBF to other myocardial regions
and blood flow to the body
• Myocardial Salvage in Setting of AMI
– Reduce LV workload (and oxygen demand) to minimize necrosis and optimize myocardial recovery

Metrics for Comparing Different Methods ofPercutaneous Circulatory Support
• Amount of hemodynamic support
–
–
Ability to increase CPO and decrease PCWP
Single vs Biventricular Support
• Degree of myocardial protection
– Ability to offload the LV while providing support
•
•
•
Ease of use: insertion & operation
Risk of complications (vascular, valvular, hemolysis…)
Contraindications (or limitations)

Right Ventricle
Left Ventricle
Varying Mechanisms of Hemodynamic Support

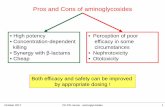
Intra-Aortic Balloon Pump
- Pros and ConsPROs:
• Mature technology
• Increases Stroke Volume up to 30%
• Increase Coronary Perfusion
• Ease of Use
• Lower Complication rate over time
CONs:
• Does not unload the heart
• Require a minimum LV function
• Require a stable rhythm
• No proven mortality benefit
• only modestly augments cardiac output
and is unable to provide circulatory support
if hemodynamic collapse occurs
LV diastole
LV systole



LV dysfunction

LM occlusion

IABC






IMPELLA

Thiele H et al, N Engl J Med 2012;367:1287-96.

IABP SHOCK II Trial: 1-year Mortality
Thiele H et al. Lancet 2013; 382:1638-45
52%51%

30-day Survival in Patients with Cardiogenic ShockTreated in the Impella-EUROSHOCK Registry
46%43.7%
24.5%18.2%
Lauten A et al, Circ Heart Fail. 2013;6;23-30




Selected Trials of Circulatory Device Therapy and Indications
Trial Study Device Indication Primary Outcome
IABP SHOCK IABP Cardiogenic ShockNo difference in 30-day
mortality or secondaryendpoints
CRISP IABPAcute Anterior Myocardial
Infarction
Trend toward higher infarctsize and vascular
complications with IABP
PROTECT IIvsImpella 2.5
IABPHigh Risk PCI
No difference in 30-day MAE;halted for futility and DSMBconcerns for safety trends
BCIS IABP High Risk PCINo difference in in-hospitalMACCE; improved 5-year
survival
IMPRESSImpella CP vs
IABPCardiogenic Shock
No difference in 30-daymortality or secondary
endpoints


TandemHeart PV Loop Performance
The combination of left atrial cannulation with a high-flowcentrifugal pump enables up to 80% work reduction
On File, Cardiac Assist, Inc.





Veno-Venous/Arterial Extra
Corporeal Membrane Oxygenation
Indications
➢ Cardiogenic shock
➢ Pulmonary support
➢ Post cardiotomy
➢ Post heart/lung
transplant
Reported in-hospital survival 24-38%
In pediatric patients - up to 80%

ECMO
Percutaneous femoral cannulation of both the common femoral
vein (24 Fr cannula) and artery (18 Fr cannula with added distal
leg perfusion branch)
the circuit was connected to a third generation (magnetically
levitated) centrifugal pump (Centrimag, Levitronix) and to a long term (low pressure) membrane oxygenator (Medtronic)
cardiopulmonary support with flows up to
5.5 l/min

DECISION
PCI – Rotablation with MECHANICAL SUPPORT
IABP: Inadequte support
IMPELLA: Non applicable (AVR)
ECMO


PILOT 50 LAD - FINECROSS IVUS CANNOT CROSS
PTCA: Rotablation LAD, CX, CULOTTE technique

ROTAWIRE THROUGH FINECROSS ROTABURR 1.25mm 140000rpm
PTCA: Rotablation LAD, CX, CULOTTE technique

ROTABURR 1.5mm 140000rpm POST ROTA LAD
PTCA: Rotablation LAD, CX, CULOTTE technique

ROTABURR 1.5 mm CX 140000rpm POST ROTA CX
PTCA: Rotablation LAD, CX, CULOTTE technique

BALLOON LAD BALLOON CX
PTCA: Rotablation LAD, CX, CULOTTE technique

STENT CX WIRE LAD
PTCA: Rotablation LAD, CX, CULOTTE technique

FIRST KISSING STENT LAD
PTCA: Rotablation LAD, CX, CULOTTE technique

STENT LAD DEPLOYED FINAL KISSING
PTCA: Rotablation LAD, CX, CULOTTE technique

PTCA: Rotablation LAD, CX, CULOTTE technique
FINAL POT 4.5 BALLOON 26 Atm

PTCA: Rotablation LAD, CX, CULOTTE technique
FINAL RESULT

PTCA: Rotablation LAD, CX, CULOTTE technique
FINAL IVUS RESULT

DAY 1: patient completely dependent on ECMO –
pressure tracing direct line – iv inotropes

DAY 1: patient completely dependent on ECMO – pressure
tracing direct line – iv inotropes

DAY 5: ECMO REMOVED
DAY 8: PATIENT DISCHARGED – NYHA I – EF 35%

MR improved grade II

PRE POST
EF

Conclusions (I)
PCI in patient with severe hemodynamic compromise is feasible if facilitated by MCS
IABP remains the old fashioned gold-standard
ECMO is indicated for life threatening pulmonary or cardiac failure, when any other forms of treatment have been failed
ECMO provides full hemodynamic support although at the expense of a higher complication rate due to the increased invasiveness of the procedure in the femoral vessels and the presence of an oxygenator which increases the inflammatory response

Sintek and Joseph et al J Card Fail 2015
The more dysfunction the ventricle,
the less functional an IABP becomes
Counterpulsation Requires Native Left Ventricular Pulsation

Conclusions (I)
PCI in patient with severe hemodynamic compromise is feasible if facilitated by MCS
IABP remains the old fashioned gold-standard
ECMO is indicated for life threatening pulmonary or cardiac failure, when any other forms of treatment have been failed
ECMO provides full hemodynamic support although at the expense of a higher complication rate due to the increased invasiveness of the procedure in the femoral vessels and the presence of an oxygenator which increases the inflammatory response


Conclusions (II)Identification of high risk patients who most likely will benefit from MCS is crucial
Type of MCS depends on:
LV-circulatory status
type and duration of procedure
It is important to utilize the expertise of the surgeons in this field


Conclusions (II)Identification of high risk patients who most likely will benefit from MCS is crucial
Type of MCS depends on:
LV-circulatory status
type and duration of procedure
It is important to utilize the expertise of the surgeons in this field


Rota-Kurs Gaul I/2002
Rotablator:
Catheter Components
drive shaft
guide wire
diamond coated burr1.25 mm - 2.5 mm
(0.25 mm increments)
sheath 4.3 french O.D.

• Differential Cutting
• The Orthogonal Displacement of Friction
Key Principles of Operation for the
Rotablator System

Principle of Operation
Differential Cutting
All diseased plaque is inelastic
High speed rotational ablation differentiates healthy elastic vessel wall from plaque
High speed rotational ablation preferentially cuts all types of plaque morphology

Differential Cutting
Elastic Tissue In-elastic Tissue

Rotablator
Micro
Particles
Rotablator
Micro
Particles
Red Blood CellsRed Blood Cells
5 Micron Bead5 Micron Bead
tt
ss
Plaque is ablated
into small particles
removed by RES
RotablatorTM: Benefits

• Minimises vessel wall stretch and elastic recoil
• Eliminates vessel barotrauma
• Removes all plaque morphologies; Soft, fibrotic,
calcified
• Produces a smooth lumen channel for improved
hemodynamic flow
Rotablator: Benefits

post-PTCA procedure post-Rotablator® procedure

System
Components
Overview
Disposable’s and Hardware

Rotablator System Components
Disposables:
• Advancer
• Burr Catheter
• WireClip Torquer
• Guide Wire

Rotablator System
ComponentsHardware
• Air Supply
Compressed Air
Compressed Nitrogen
• Console
• Dynaglide Foot Pedal