β-adrenergic signaling in heart failure—adapt or die
3
Click here to load reader
Transcript of β-adrenergic signaling in heart failure—adapt or die

N E W S A N D V I E W S
individuals can optimally regulate the excita-tory input from cortical areas and specific intralaminar thalamic nuclei (Fig. 1a).
In advanced Parkinson’s disease, pyra-midal cells with Lewy pathology appear in the deep cortical layers (V–VI), where the cell bodies of the corticostriatal projection are located. The most plausible explanation for both the dendritic spine loss by striatal projection cells and the occurrence of Lewy pathology in the cortical pyramidal cells is that the neurons generating the corticostria-tal pathway become affected. Impairment of the corticostriatal input can be inferred from the loss of striatal spines12.
Should physical contacts between projection neurons in different regions prove to be cru-cial for the pathogenesis of Parkinson’s disease, the pattern of synaptic contacts on dendritic spines of striatal projection cells may have broader implications for surgical interventions
than previously realized: if synaptic contacts from grafted neurons are too close to degener-ating synaptic contacts of the host nigrostria-tal pathway (Fig. 1b), the grafted nerve cells might become affected by an entity capable of inducing Lewy pathology (Fig. 1c,d).
Remarkably, the synaptic contacts from all fiber tracts whose neurons develop Lewy pathology during Parkinson’s disease con-verge on or near dendritic spines of striatal projection cells (the corticostriatal, nigro-striatal and thalamostriatal tracts; Fig. 1c). The loss of dendritic spines causes an insidi-ously progressive disconnection between the cerebral cortex and striatum (Fig. 1d) and, in so doing, results in drastic impairment of the cortico–basal ganglia–cortical circuitry, that is, far-reaching loss of cortical control of movement14. For this reason alone, suc-cessfully transplanted dopaminergic neurons might become, years later, incapable of regu-
lating increasingly ‘spineless’ striatal projec-tion neurons (Fig. 1d).
1. Olanow, C.W. et al. Ann. Neurol. 54, 403–414 (2003).
2. Mendez, I. et al. Nat. Med. published online, doi:10.1038/nm1752 (6 April 2008).
3. Kordower, J.H. et al. Nat. Med. published online, doi:10.1038/nm1747 (6 April 2008).
4. Li, J.-Y. et al. Nat. Med. published online, doi:10.1038/nm1746 (6 April 2008).
5. Spillantini, M.G. et al. Nature 388, 839–840 (1997).6. Lang, A.E. & Obeso, J.A. Lancet Neurol. 3, 309–316
(2004).7. Ahlskog, J.E. Neurology 69, 1701–1711 (2007).8. Langston, J.W. Ann. Neurol. 59, 591–596 (2006).9. Bloch, A. et al. Neuropathol. Appl. Neurobiol. 32,
284–295 (2006).10. Freed, C.R. et al. N. Engl. J. Med. 344, 710–719
(2001).11. Snyder, B.J. & Olanow, C.E. Curr. Opin. Neurol. 18,
376–385 (2005).12. Braak, H. & Del Tredici, K. Neurology (in the press).13. Stephens, B. et al. Neuroscience 132, 741–754
(2005).14. Tepper, J.M. et al. Prog. Brain Res. 160, 3–7 (2007).15. Deutch, A.Y. J. Neural Transm. Suppl. 70 67–70
(2006).
β-adrenergic signaling in heart failure—adapt or dieThomas Eschenhagen
About 25% of the African-American population carries a gene variant that seems to protect against heart failure. The findings may have implications for the use of β-blockers (pages 510–517).
Thomas Eschenhagen is at the Institute of
Experimental and Clinical Pharmacology, University
Medical Center Hamburg-Eppendorf, Martinistrasse
52, 20246 Hamburg, Germany.
e-mail: [email protected]
A report in this issue of Nature Medicine1 identifies a gene variant that seems to protect against the progression of heart failure. The gene, GRK5, encodes a G protein–coupled receptor kinase (GRK) that participates in signaling through β-adrenergic receptors, the targets of β-blockers. The protective gene vari-ant, identified in one quarter of the African-American population, was associated with improved survival in individuals with chronic heart failure.
The pathophysiology of heart failure is complex, and drug development in this field a particular challenge. Indeed, the current com-bination of heart failure drugs that prolongs life expectancy in millions of patients has emerged from a process involving frequent misconcep-tions and failures—and rare successes, which can often be attributed to the stubborn con-victions of a few individuals. An example is the story of β-blockers—drugs that compete with the stress hormones norepinephrine and
epinephrine for binding to their receptors, thereby dampening the ‘fight or flight’ reaction of the heart. The development of these now widely used drugs defied prevailing scientific concepts, with clinical studies weighing in with the final say.
Waagstein et al.2 reported their first expe-riences with β-blockers in people with severe heart failure in 1975. At the time, this class of drugs was strictly contraindicated in heart failure. Instead, the industry was looking for the ‘ideal inotrope’, a drug that makes hearts beat more strongly. This goal emerged from an apparently straightforward idea—to target the main deficit in the failing heart, the reduction in pumping force (Fig. 1). Researchers were looking for inotropes that were as effective as digoxin—a mainstay then for more than 200 years—but with a better therapeutic index and additional vasodilator properties to reduce the resistance against which the heart has to eject blood.
One class of drugs that fulfilled these criteria was inhibitors of phosphodiesterases, such as milrinone; these drugs have powerful effects on both the heart and on blood vessels by inhibit-ing degradation of cAMP, the second messen-ger downstream of β-adrenergic receptors that
stimulates force in the heart (Fig. 1) and reduces it in blood vessels. With much accompanying optimism, these drugs entered clinical trials.
β-blockers, in contrast, seemed to have all the wrong properties. They reduce the pump-ing force acutely, can precipitate acute heart failure and tend to constrict, rather than dilate, blood vessels. The idea of treating heart failure with β-blockers provoked fierce objection in the scientific community.
Years later, after numerous clinical studies, it finally became clear that cAMP-dependent inotropes, despite their undisputed short-term benefits, increase mortality when administered chronically. In contrast, β-blockers, despite their acute force-reducing effects, decrease mortality in subjects with heart failure when given at slowly increasing doses and, in fact, increase the pumping force of the heart after several months of treatment.
What explains these apparently paradoxical findings? Clearly, it is a matter not only of dos-ing and timing (‘start low, go slow’), but also of concept. The lesson learned is that the heart is a biological system that adapts to prolonged stimulation and its withdrawal3.
Adaptation in heart failure occurs on several levels (Fig. 1). On the systemic level, reductions
NATURE MEDICINE VOLUME 14 | NUMBER 5 | MAY 2008 485
©20
08 N
atur
e P
ublis
hing
Gro
up
http
://w
ww
.nat
ure.
com
/nat
urem
edic
ine

N E W S A N D V I E W S
in pumping capacity—such as after myocardial infarction—initiate sustained activation of the sympathetic nervous system with a chronically elevated plasma concentration of norepineph-rine.
Norepinephrine binds to cardiac β-adren-ergic receptors, which activate stimulatory G proteins and thereby adenylyl cyclase, leading to increased production of the intracellular second messenger cAMP. Increased concen-trations of cAMP stimulate heart rate and, via activation of the cAMP-dependent protein kinase, phosphorylation of proteins that deter-mine force. As a result, norepinephrine pow-erfully and instantaneously stimulates heart function, although at the cost of overpropor-tional increases in energy consumption.
This signaling system is not rigid and adapts to continuous stimulation by a process termed ‘desensitization’3,4. Within minutes, norepi-nephrine-occupied β-adrenergic receptors are phosphorylated by GRKs, uncoupled from
the stimulatory G protein and subjected to internalization. In the longer term, the abun-dance of β-adrenergic receptors5 and a small intracellular amplifier, protein phosphatase inhibitor-1 (ref. 6), is stably decreased and that of GRK2 (ref. 7) and inhibitory G proteins8 is increased.
As a result of these adaptations, cardiac myocytes in failing hearts lose their respon-siveness to norepinephrine over time. Whether these adaptations are predominantly ‘good’ or ‘bad’ has long been a matter of debate. On the one hand, β-adrenergic desensitization exag-gerates exercise intolerance in heart failure. On the other hand, desensitization protects myocytes against the consequences of sus-tained β-adrenergic overstimulation, namely, arrhythmias, energy depletion, hypertrophy and apoptosis4. Accordingly, catecholamines and phosphodiesterase inhibitors—drugs that further stimulate the heart by overcoming desensitization—cause increased mortality. In
contrast, β-blockers reduce adrenergic respon-siveness and decrease mortality in individuals with heart failure. Additionally, mouse strains that efficiently downregulate their cardiac β-adrenergic receptor density exhibit lower car-diac toxicity in response to the β-adrenergic agonist isoprenaline than strains that do not9.
People differ genetically in their adrenergic responsiveness, as proposed 15 years ago when the first β-adrenergic receptor polymorphism was identified by Liggett and his colleagues10. Since then, it has become clear that people are equipped with α- and β-adrenergic receptors that, when assayed in recombinant cell systems, differ substantially in their signaling efficacy and propensity to be downregulated by pro-longed exposure to norepinephrine11. To what degree the biochemical variability translates into clinically meaningful differences remains a matter of debate12.
In this issue, Dorn, Liggett and their col-leagues1 add a new facet to the picture. They identified a polymorphism in GRK5 that gives rise to a variant (GRK5-Leu41) with higher kinase activity than the wild-type enzyme (GRK5-Gln41). The GRK5-Leu41 variant is common in African Americans (allele fre-quency ∼25%) and rare in European Americans (∼2%).
GRKs phosphorylate agonist-occupied receptors and uncouple them from down-stream G proteins. This mechanism suggests that a high-activity GRK5 variant confers faster desensitization and lower responses to ago-nists such as norepinephrine. GRKs basically switch off the β-adrenergic and other receptor signaling pathways. Indeed, cells overexpress-ing GRK5-Leu41 showed subnormal isoprena-line-stimulated cAMP production over time. What’s more, GRK5-Leu41–expressing trans-genic mice showed accelerated desensitization to a continuous infusion of isoprenaline. This desensitization was associated with partial pro-tection from chronic isoprenaline toxicity, an effect similar to that seen in mice treated with a β-blocker1.
The data in people dovetailed with the findings in mice. The authors examined an African-American population of subjects with heart failure treated with or without β-blockers1. β-blocker–naive individuals with heart failure who had at least one GRK5-Leu41–encoding allele showed markedly better transplant-free survival compared to individuals with two wild-type alleles. They also had the same rate of transplant-free survival as people homozygous for the gene encoding GRK5-GlnQ41 and taking β-block-ers. Thus, the presence of at least one GRK5-Leu41–encoding allele conferred the same marked protection as did β-blockers, which,
Injury,e.g. infarct
Acuteimprovement
Pumpingcapacity
Chronic accelerationof vicious cycle
Digoxin
Norepinephrine
β-blockers
GRK
cAMP
Phosphodiesteraseinhibitors
G AC
PDE5´AMP
Sympathetic nervous system
↑ Force ↑ Frequency
↑ Energy consumption ↑ Apoptosis
↑ Hypertrophy ↑ Arrhythmia
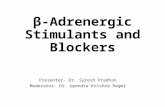
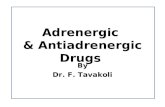
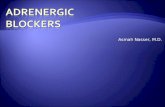
Figure 1 Vicious cycle in heart failure. Any major injury that reduces cardiac pumping capacity activates neurohumoral mechanisms, including the sympathetic nervous system. The acute increase in norepinephrine serves as a fast and powerful mechanism that stabilizes perfusion of crucial organs by redirecting blood flow away from skin, muscles, kidney and gut and stimulating heart rate and force. If the primary pumping defect of the heart continues, however, the sustained increase in sympathetic tone turns from friend to foe for two reasons. First, peripheral vasoconstriction imposes increased load on the failing heart, which further reduces cardiac output (the reason to prescribe vasodilators, not shown here). Second, continued stimulation of cardiac myocytes leads to adverse effects including overproportional increases in energy consumption, cell death, fibrosis, cardiac myocyte hypertrophy and arrhythmia. Norepinephrine operates through β-adrenergic receptors (βARs), stimulatory G proteins (Gs), adenylyl cyclase (AC) and the second messenger cAMP. Collectively, these changes accelerate the decline of the heart—or cause sudden death—and constitute a vicious cycle. The speed of the cycle is determined, at least in part, by the sensitivity at which the β-adrenergic signaling cascade translates the extracellular signal norepinephrine into a cellular response. In heart failure, the signaling cascade is normally desensitized in response to chronic norepinephrine stimulation, an adaptation that can be viewed as mainly beneficial. The new findings from Dorn and his colleagues1 suggest that individual differences in the capacity to adapt to chronic norepinephrine stimulation depend, at least in part, on different GRK5 variants. These variants can thus affect the prognosis in the case of heart failure. PDE, phosphodiesterase.
Kim
Cae
sar
486 VOLUME 14 | NUMBER 5 | MAY 2008 NATURE MEDICINE
©20
08 N
atur
e P
ublis
hing
Gro
up
http
://w
ww
.nat
ure.
com
/nat
urem
edic
ine

N E W S A N D V I E W S
in this cohort, had no additional effect. These data suggest that patients with a robust adap-tational response—through GRK5—may not need β-blocker treatment.
The present study spanned the experi-mental gamut, from the identification of a new gene polymorphism to well-controlled experiments in recombinant cells and trans-genic mice, to studies in humans1. Of course, even with this impressive breadth, there are limitations.
The clinical study is historically prospective in design and, despite a total number of 375 subjects, differences in outcome relied mainly on individuals homozygous for the gene encod-ing GRK5-Gln41 and not taking β-blockers (n = 34, 17 events). The mouse studies are complicated by the fact that the GRK5 isoforms were expressed in addition to the two normal GRK5 alleles. The GRK5-Leu41 transgenic mice showed accelerated desensitization to isoprenaline infusion, but the maximal reduc-tion in response was normal. This observation is not easily compatible with the long term role
of GRK5 in the regulation of adrenergic sensi-tivity, as proposed by the authors1.
Finally, it is not clear which receptors, in addition to β-adrenergic receptors, are targets of GRK5 in cardiac myocytes. For instance, GRK5-knockout mice show neuronal13 and bronchial14 muscarinic supersensitivity. Because cardiac muscarinic M2 receptors antagonize the effect of adrenergic stimula-tion, increased desensitization of M2 recep-tors in cardiac myocytes would cause net stimulation of the heart, opposite the effect of β-blockers.
Despite these limitations, the findings provide strong support for the idea that adaptation of β-adrenergic signaling is key to survival in heart failure. Given that one-fourth of the African-American population carries what seems to be a protective geno-type that may affect their responsiveness to β-blockers, the findings could have direct practical implications. Before this conclu-sion is reached, however, the present find-ings need to be independently confirmed in
a large prospective study—which will hope-fully take less time than the 24 years from the first documented treatment of heart failure with β-blockers to the first convincing end-point study.
1. Liggett, S.B. et al. Nat. Med. 14, 510–517 (2008).2. Waagstein, F., Hjalmarson, A., Varnauskas, E. &
Wallentin, I. Br. Heart J. 37, 1022–1036 (1975).3. Collins, S. et al. Biochem. Soc. Trans. 18, 541–544
(1990).4. Lohse, M.J., Engelhardt, S. & Eschenhagen, T. Circ.
Res. 93, 896–906 (2003).5. Bristow, M.R. et al. N. Engl. J. Med. 307, 205–211
(1982).6. El-Armouche, A., Pamminger, T., Ditz, D., Zolk, O. &
Eschenhagen, T. Cardiovasc. Res. 61, 87–93 (2004).7. Ungerer, M., Bohm, M., Elce, J.S., Erdmann, E. &
Lohse, M.J. Circulation 87, 454–463 (1993).8. Feldman, A.M. et al. J. Clin. Invest. 82, 189–197
(1988).9. Faulx, M.D. et al. Am. J. Physiol. Heart Circ. Physiol.
289, H30–H36 (2005).10. Reihsaus, E., Innis, M., MacIntyre, N. & Liggett, S.B.
Am. J. Respir. Cell Mol. Biol. 8, 334–339 (1993).11. Liggett, S.B. Am. J. Med. 117, 525–527 (2004).12. Brodde, O.E. Pharmacol. Ther. 117, 1–29 (2008).13. Gainetdinov, R.R. et al. Neuron 24, 1029–1036
(1999).14. Walker, J.K. et al. Am. J. Physiol. Lung Cell. Mol.
Physiol. 286, L312–L319 (2004).
Dust mites’ dirty dealings with dendritic cellsDean Sheppard
Allergens stimulate lymphocytes to become factories for secreted proteins that cause organ dysfunction in allergic diseases. Allergens are now shown to target dendritic cells, the cells responsible for processing and presenting antigens to T cells (pages 565–573).
Dean Sheppard is in the Department of Medicine,
University of California, San Francisco, UCSF Box
2922, San Francisco, California 94143-2922, USA.
e-mail: [email protected]
The immune system has evolved to identify and kill a variety of threatening microorgan-isms, and distinct patterns of response have emerged to effectively nullify distinct groups of invaders. The response pattern used to defend against parasites involves the generation of T lymphocytes called T helper type 2 (TH2) cells that secrete potent cytokines required for walling off and expelling parasites. However, no defense is perfect, and in some people the same response pattern is mounted to defend against otherwise innocuous environmental agents, such as house dust mites, resulting in allergic diseases such as asthma.
Another helper T lymphocyte, the TH17 cell, which secretes interleukin-17, also con-tributes to allergic responses1. Although much has been learned about how T lymphocytes
differentiate into TH2 cells2or TH17 cells3, less is known about how the immune system rec-ognizes allergens and initiates the pattern of response. Krishnamoorthy et al.4 begin to fill in this gap. They examine a multicellular path-way in which allergens act directly on dendritic cells to drive differentiation of both TH2 and TH17 cells.
Cells of the innate immune system detect viruses and bacteria and initiate responses that result in the destruction of these organ-isms and the protection and repair of the infected host. The first step in this process is recognition of common components of viruses and bacteria by so-called pattern rec-ognition receptors expressed on several types of immune cells, including dendritic cells5. Dendritic cells ingest foreign particles and microorganisms and present fragments of these organisms to adjacent T lymphocytes to initiate adaptive immune responses needed for long-term defense. Interactions between viruses and bacteria and the pattern recog-nition receptors expressed by dendritic cells
initiate immune defense against these organisms. In experimental models, aller-gic responses to usually innocuous foreign antigens can be induced by the conditions of immunization, for example, by addition of cholera toxin to an immunizing antigen6 or by immunization with the common asthma-inducing allergen, house dust mite7. However, the molecular steps linking these specific immunization conditions to differentiation of T cells have been largely unknown.
Krishnamoorthy et al.4 initially approached this problem by using expression microarrays to identify genes induced in dendritic cells by cholera toxin. Two of the most highly induced genes were those encoding the trans-membrane tyrosine kinase receptor c-Kit and the cytokine interleukin-6 (IL-6). IL-6 has previously been shown to induce TH17 cells3,8 and to contribute to the induction of TH2 cells9. The authors incubated dendritic cells with either cholera toxin or a standard experimental allergen, house dust mites. Both substances potently induced IL-6 secretion
NATURE MEDICINE VOLUME 14 | NUMBER 5 | MAY 2008 487
©20
08 N
atur
e P
ublis
hing
Gro
up
http
://w
ww
.nat
ure.
com
/nat
urem
edic
ine