Υπέρταση, Κολπική μαρμαρυγή και νέα αντιθρομβωτικά...
85
Director of Cardiology Dept, Asklepeion General Hospital, Athens Greece. New Generation of Anticoagulant Drugs In Cardiovascular Diseases Athanasios J. Manolis
-
Upload
cardio-asklepeion -
Category
Documents
-
view
238 -
download
0
description
Υπέρταση,Κολπική μαρμαρυγή
Transcript of Υπέρταση, Κολπική μαρμαρυγή και νέα αντιθρομβωτικά...
Director of Cardiology Dept, Asklepeion General Hospital,
Athens Greece.
New Generation of Anticoagulant Drugs In Cardiovascular Diseases
Athanasios J. Manolis

Congress set aside $ 1.1 billion last year for head-to-head testing of drugs and treatment to determine which work best and for which type of patient
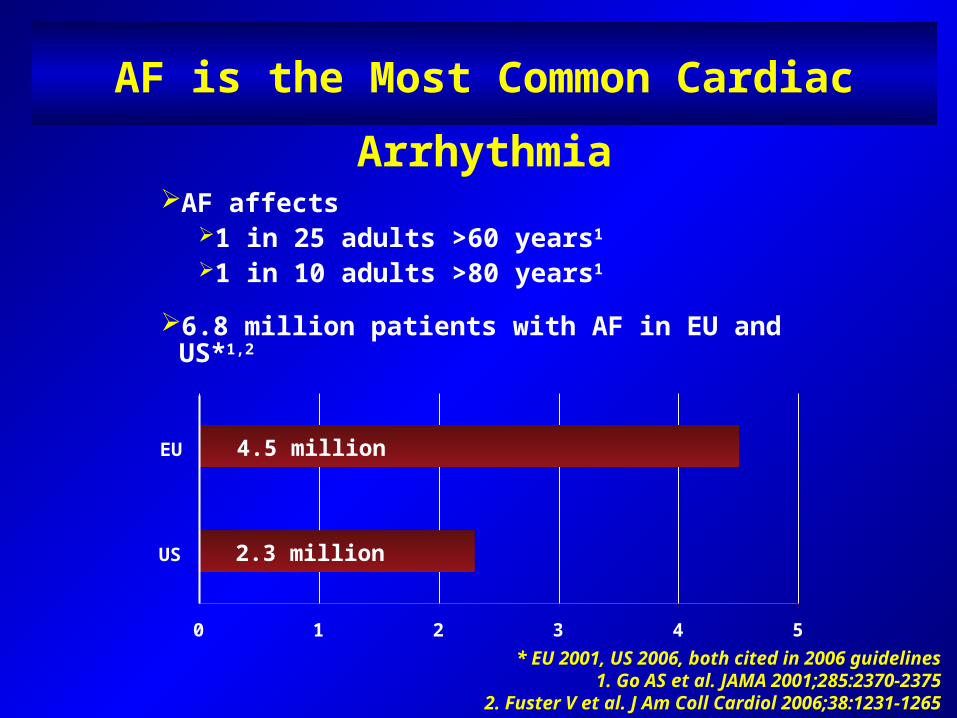
AF is the Most Common Cardiac Arrhythmia
AF affects 1 in 25 adults >60 years1 1 in 10 adults >80 years1
6.8 million patients with AF in EU and US*1,2
* EU 2001, US 2006, both cited in 2006 guidelines1. Go AS et al. JAMA 2001;285:2370-2375
2. Fuster V et al. J Am Coll Cardiol 2006;38:1231-1265
4.5 million
2.3 million
0 1 2 3 4 5
US
EU
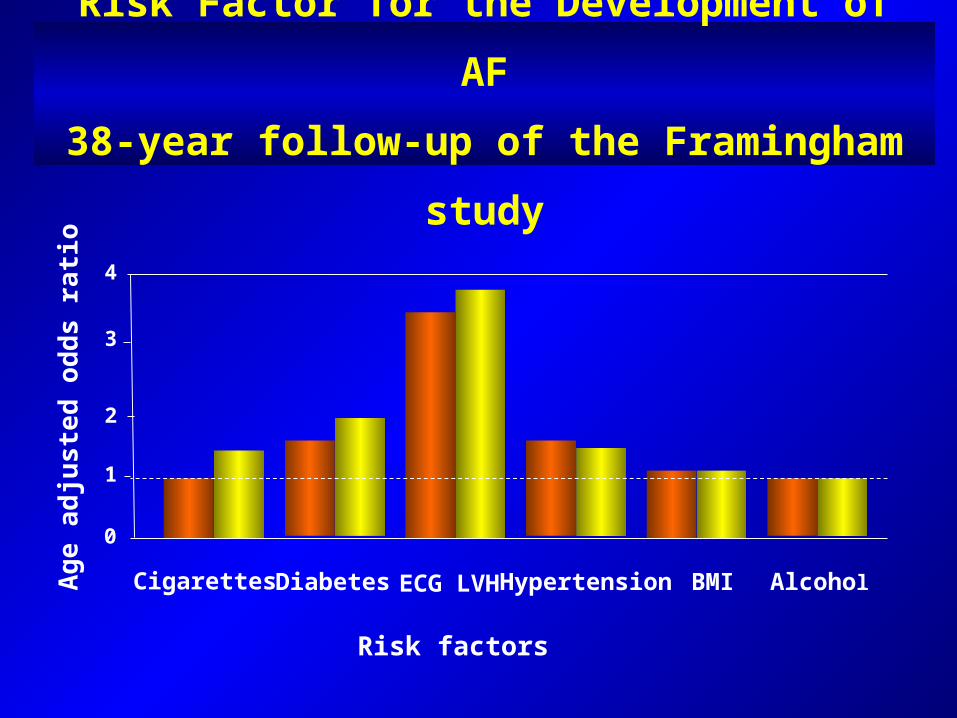
Risk Factor for the Development of AF
38-year follow-up of the Framingham study
Risk factors
Age
adj
uste
d od
ds r
atio
Cigarettes
1
2
3
4
0
Diabetes ECG LVH Hypertension BMI Alcohol
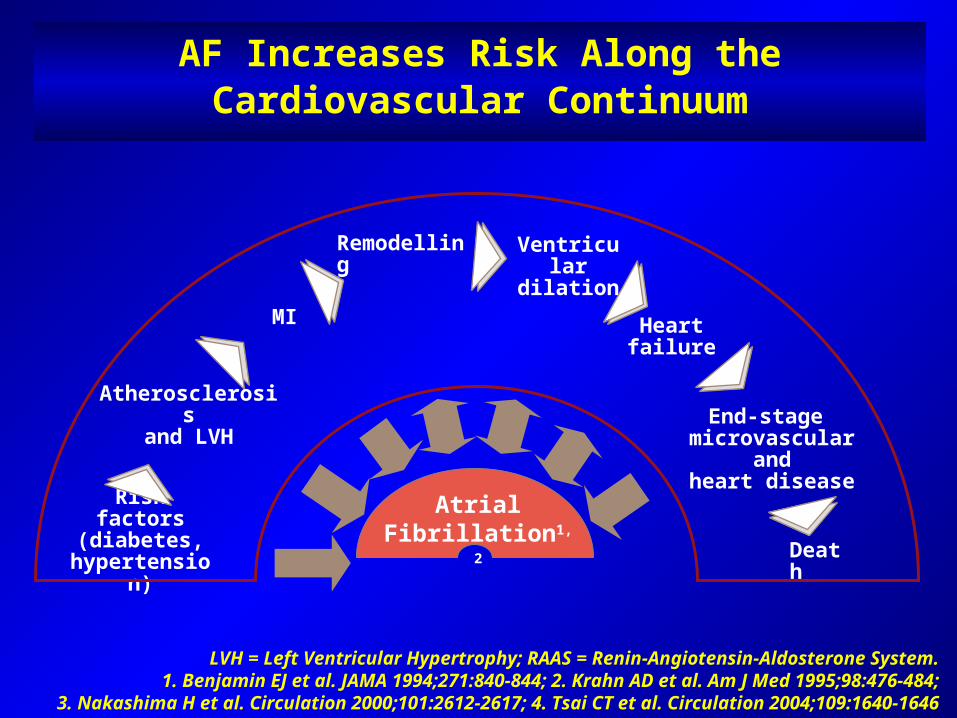
AF Increases Risk Along the Cardiovascular Continuum
LVH = Left Ventricular Hypertrophy; RAAS = Renin-Angiotensin-Aldosterone System.1. Benjamin EJ et al. JAMA 1994;271:840-844; 2. Krahn AD et al. Am J Med 1995;98:476-484;
3. Nakashima H et al. Circulation 2000;101:2612-2617; 4. Tsai CT et al. Circulation 2004;109:1640-1646
Risk factors(diabetes,
hypertension)
Atrial Fibrillation1,2
MI
Atherosclerosisand LVH
Remodelling Ventriculardilation
Heart failure
End-stage microvascular
andheart disease
Death
26/04/23 05:24 a.m.11760 M11760 M
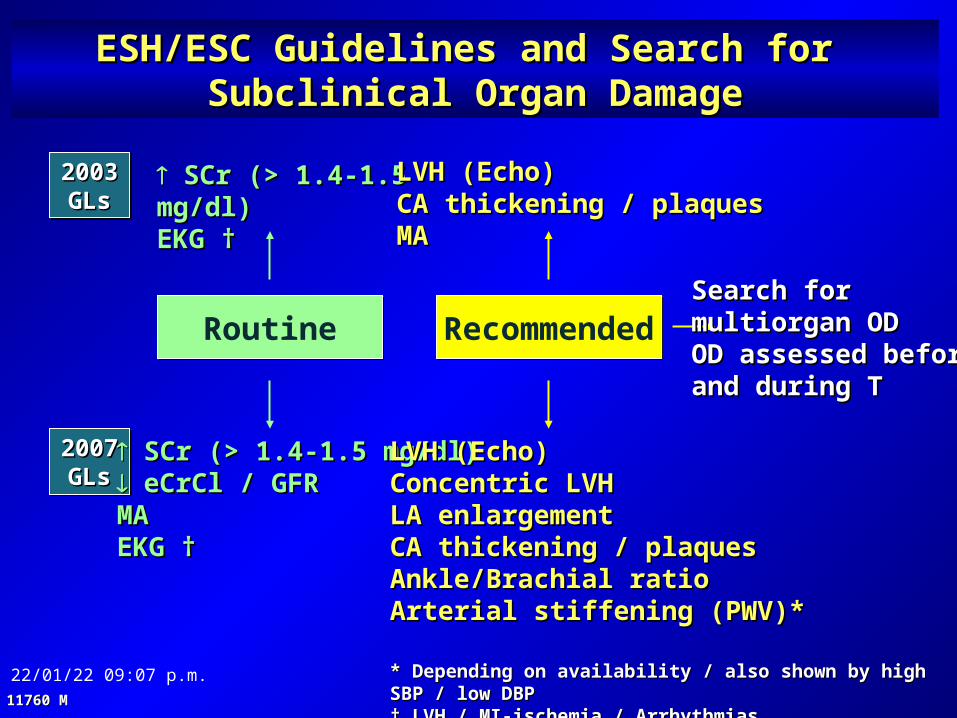
ESH/ESC Guidelines and Search for ESH/ESC Guidelines and Search for Subclinical Organ DamageSubclinical Organ Damage
20032003GLsGLs
20072007GLsGLs
SCr (> 1.4-1.5 mg/dl)SCr (> 1.4-1.5 mg/dl) eCrCl / GFReCrCl / GFRMAMAEKG †EKG †
SCr (> 1.4-1.5 mg/dl)SCr (> 1.4-1.5 mg/dl)EKG †EKG †
LVH (Echo)LVH (Echo)Concentric LVHConcentric LVHLA enlargementLA enlargementCA thickening / plaquesCA thickening / plaquesAnkle/Brachial ratioAnkle/Brachial ratioArterial stiffening (PWV)*Arterial stiffening (PWV)*
LVH (Echo)LVH (Echo)CA thickening / plaquesCA thickening / plaquesMAMA
Routine RecommendedSearch for Search for multiorgan ODmultiorgan ODOD assessed before OD assessed before and during Tand during T
* * Depending on availability / also shown by high SBP / low Depending on availability / also shown by high SBP / low DBPDBP† † LVH / MI-ischemia / ArrhythmiasLVH / MI-ischemia / Arrhythmias
What is Atrial Fibrillation?
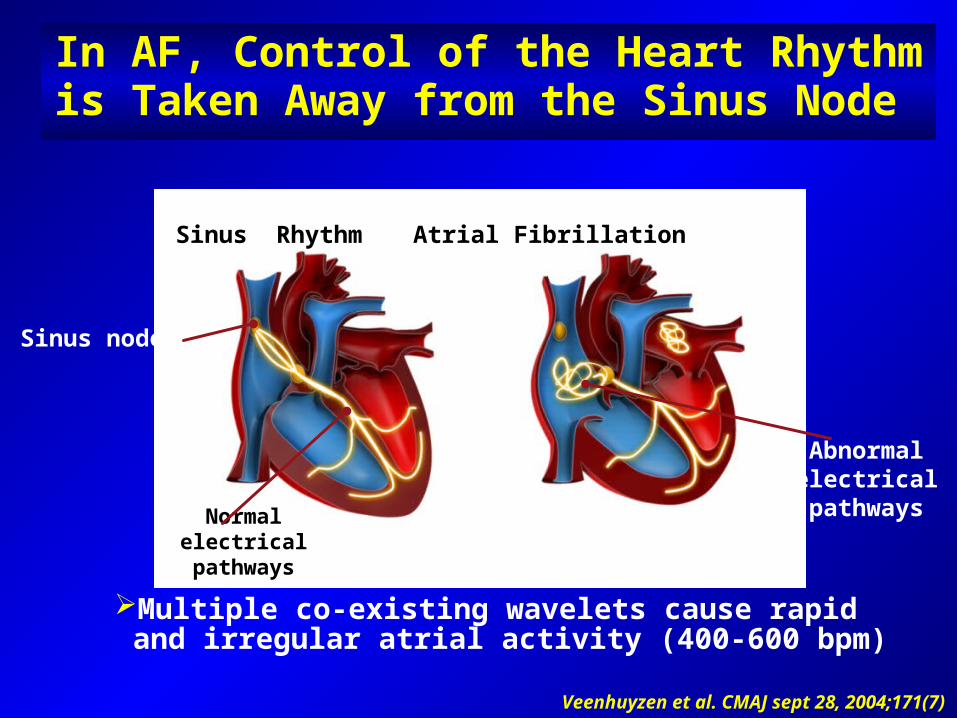
In AF, Control of the Heart Rhythm is Taken Away from the Sinus Node
Veenhuyzen et al. CMAJ sept 28, 2004;171(7)
Normal electrical pathways
Abnormal electrical pathways
Sinus Rhythm Atrial Fibrillation
Multiple co-existing wavelets cause rapid and irregular atrial activity (400-600 bpm)
Sinus node
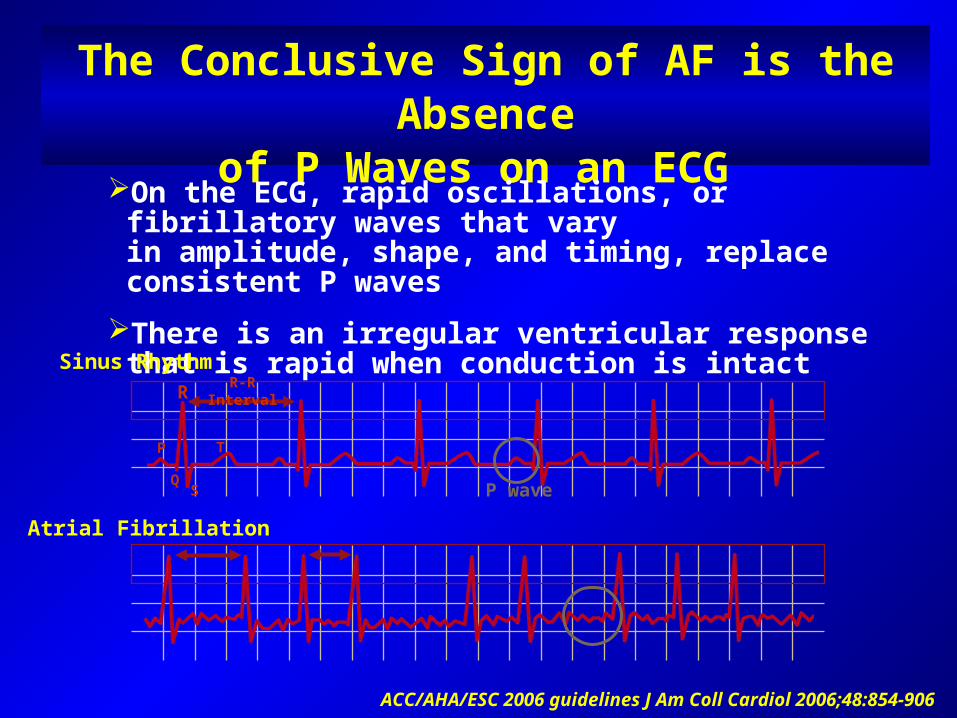
The Conclusive Sign of AF is the Absenceof P Waves on an ECG
On the ECG, rapid oscillations, or fibrillatory waves that varyin amplitude, shape, and timing, replace consistent P waves
There is an irregular ventricular response that is rapid when conduction is intact
Atrial Fibrillation
P T
QS
R
ACC/AHA/ESC 2006 guidelines J Am Coll Cardiol 2006;48:854-906
Sinus Rhythm
P wave
R-R Interval
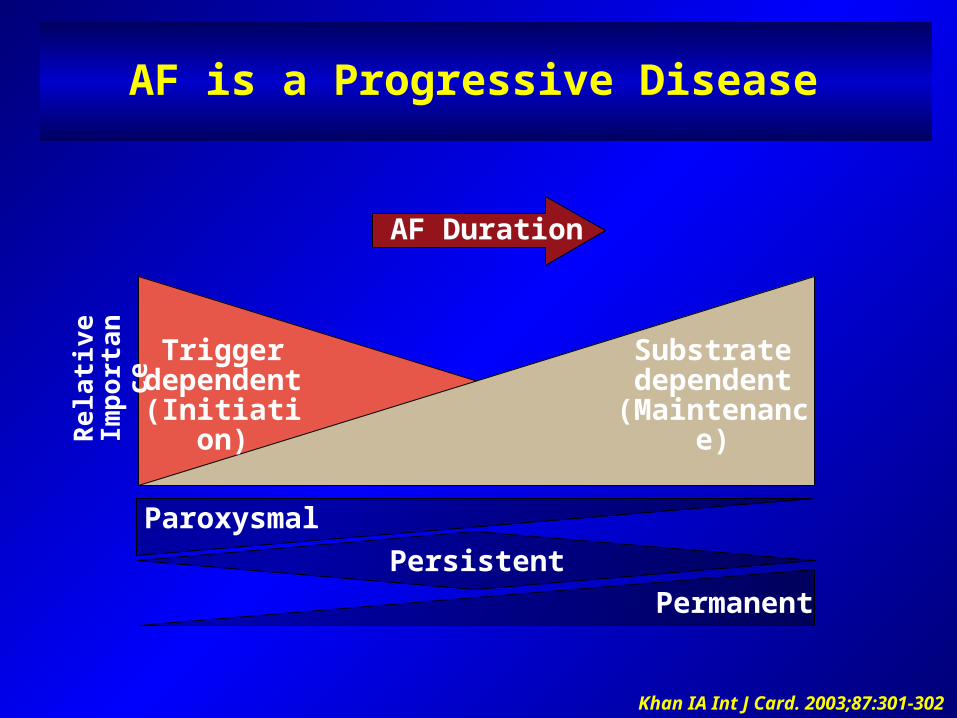
AF Duration
AF is a Progressive Disease
Paroxysmal
Trigger dependent(Initiation)
Permanent
Substrate dependent
(Maintenance)Rel
ativ
e Im
port
ance
Khan IA Int J Card. 2003;87:301-302
Persistent
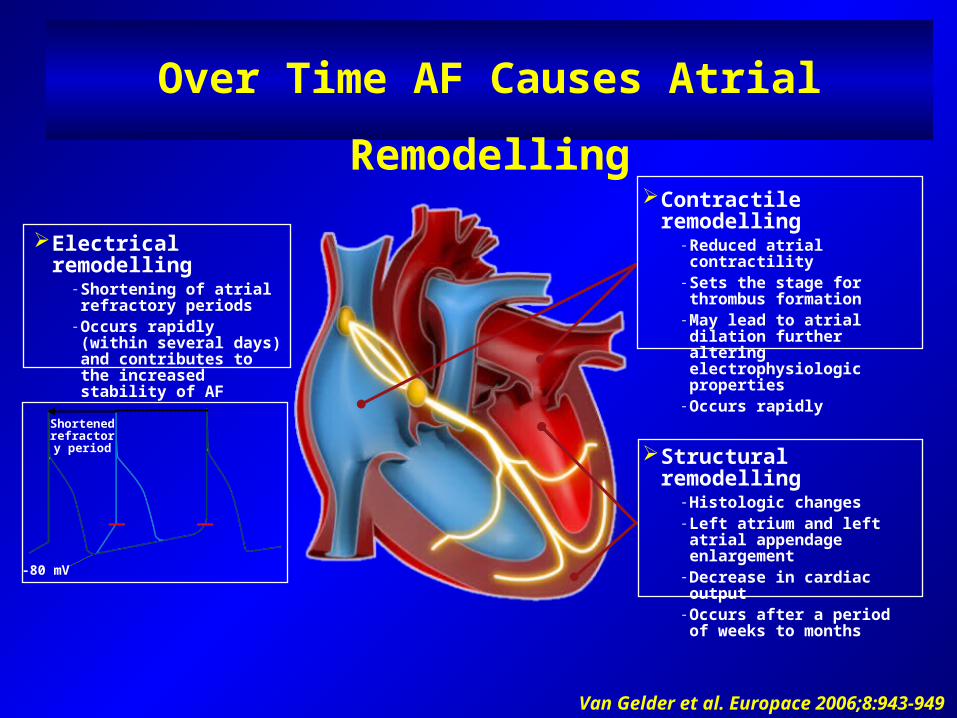
Over Time AF Causes Atrial Remodelling
Contractile remodelling-Reduced atrial contractility-Sets the stage for thrombus
formation-May lead to atrial dilation
further altering electrophysiologic properties
-Occurs rapidly
Structural remodelling-Histologic changes-Left atrium and left atrial
appendage enlargement-Decrease in cardiac output-Occurs after a period of
weeks to months
Shortened refractory
period
-80 mV
Electrical remodelling-Shortening of atrial
refractory periods-Occurs rapidly (within
several days) and contributes to the increased stability of AF
Van Gelder et al. Europace 2006;8:943-949
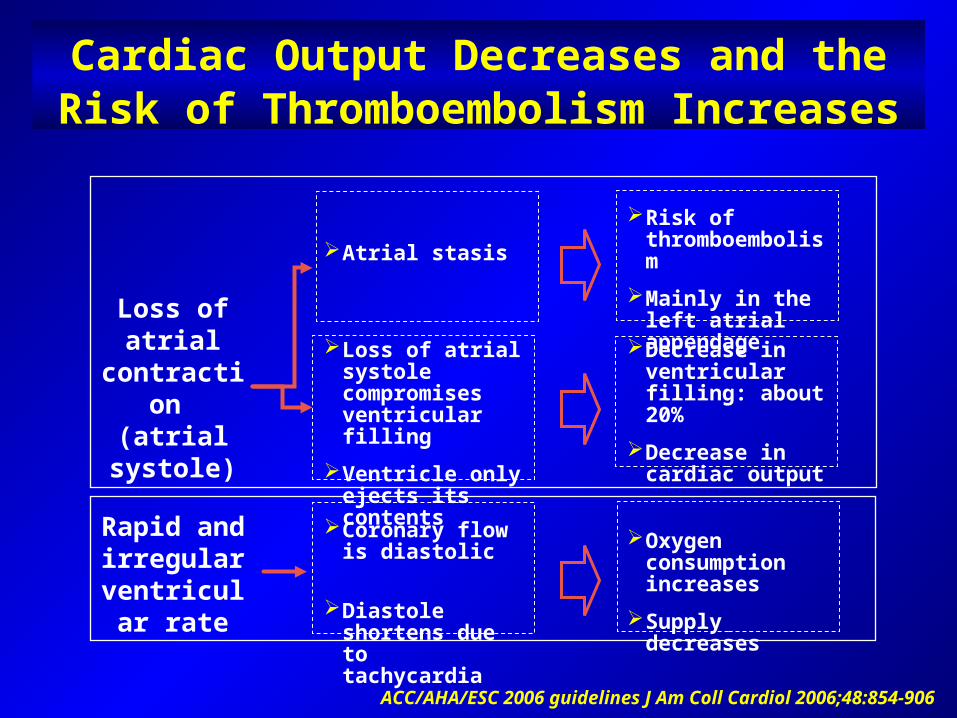
Cardiac Output Decreases and the Risk of Thromboembolism Increases
Atrial stasis
Loss of atrial systole compromises ventricular filling
Ventricle only ejects its contents
Risk of thromboembolism
Mainly in the left atrial appendage
Decrease in ventricular filling: about 20%
Decrease in cardiac output
Rapid and irregular
ventricular rate
Coronary flow is diastolic
Diastole shortens due to tachycardia
Oxygen consumption increases
Supply decreases
ACC/AHA/ESC 2006 guidelines J Am Coll Cardiol 2006;48:854-906
Loss of atrial contraction
(atrial systole)
What are the consequences of AF?
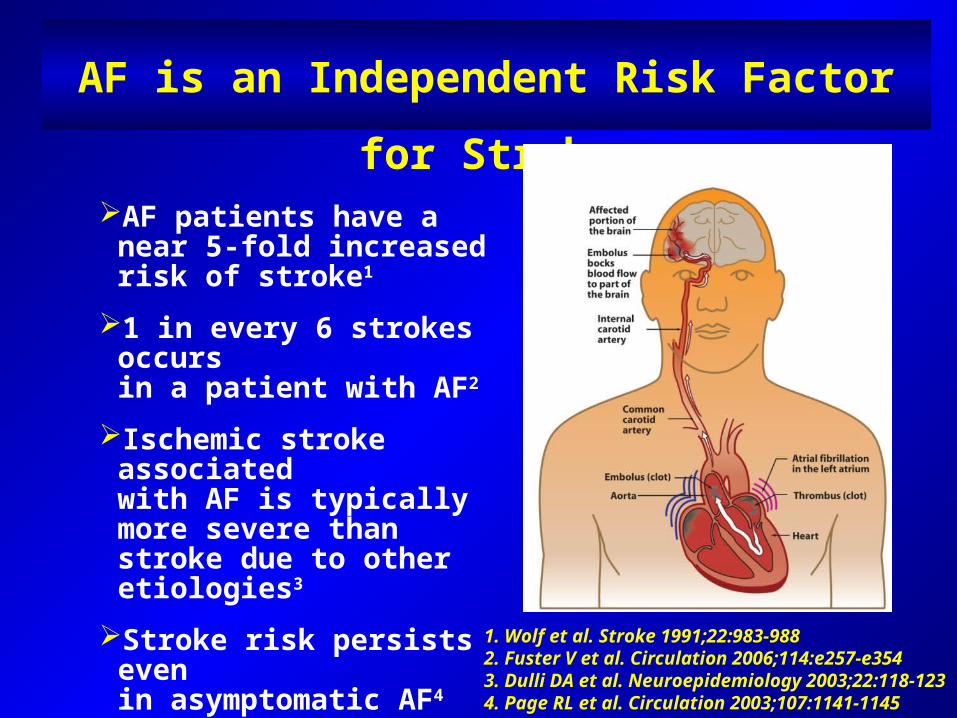
AF is an Independent Risk Factor for Stroke
AF patients have a near 5-fold increased risk of stroke1
1 in every 6 strokes occursin a patient with AF2
Ischemic stroke associatedwith AF is typically more severe than stroke due to other etiologies3
Stroke risk persists evenin asymptomatic AF4
1. Wolf et al. Stroke 1991;22:983-9882. Fuster V et al. Circulation 2006;114:e257-e354 3. Dulli DA et al. Neuroepidemiology 2003;22:118-1234. Page RL et al. Circulation 2003;107:1141-1145
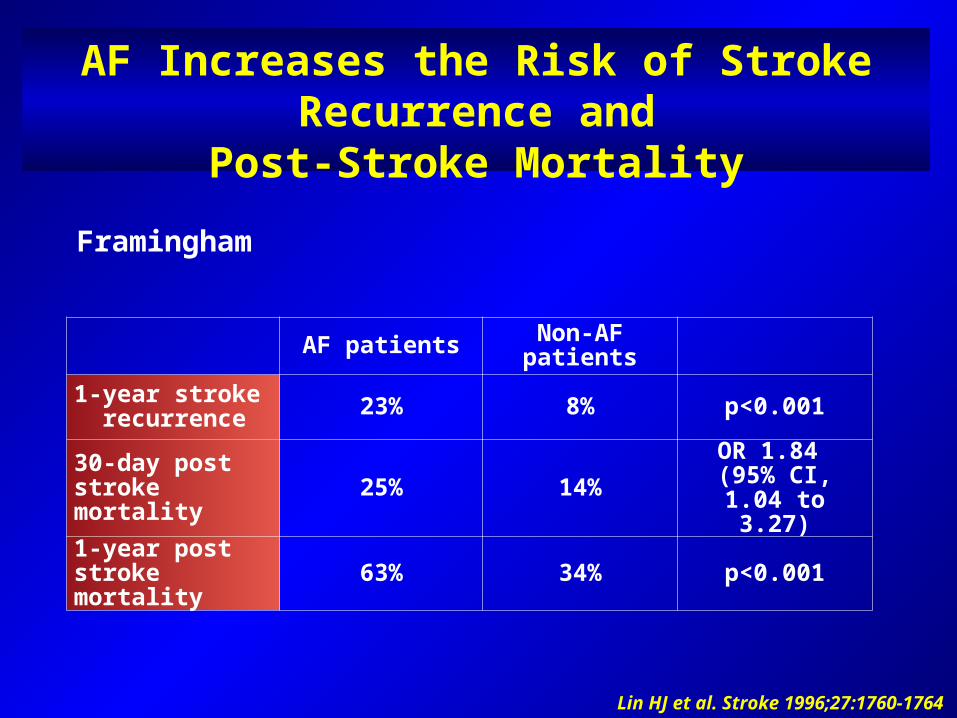
AF Increases the Risk of Stroke Recurrence andPost-Stroke Mortality
AF patients Non-AF patients
1-year stroke recurrence 23% 8% p<0.001
30-day post stroke mortality 25% 14%
OR 1.84 (95% CI, 1.04 to
3.27)1-year post stroke mortality 63% 34% p<0.001
Lin HJ et al. Stroke 1996;27:1760-1764
Framingham
What are the current treatment strategies
for AF?
Atrial fibrillation is easy to find,
but evidence on how best to treat it isn’t
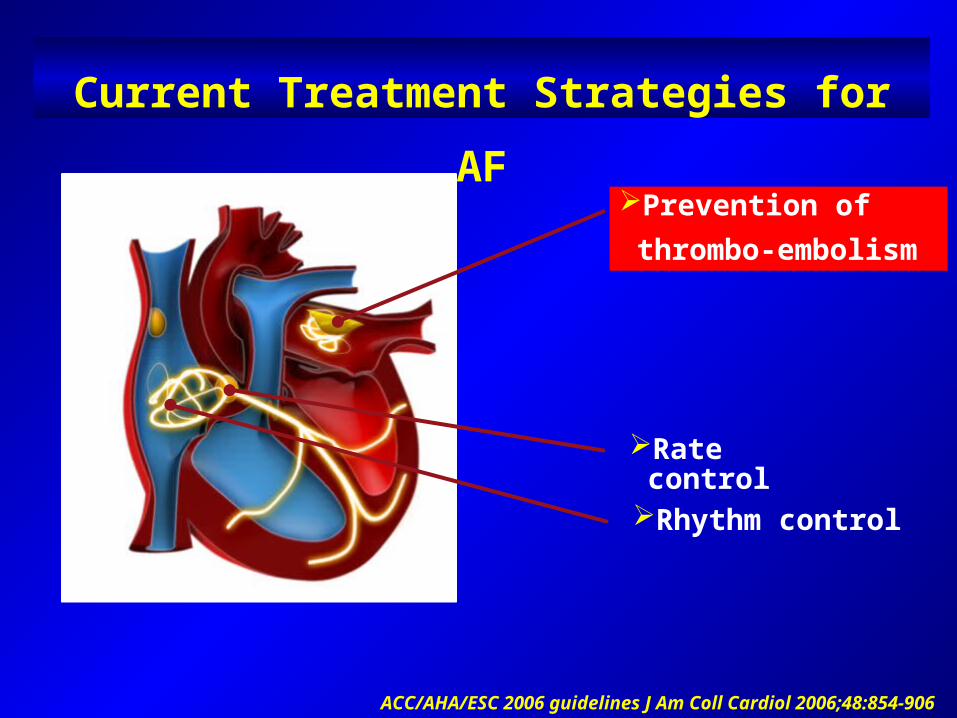
Current Treatment Strategies for AF
Prevention of thrombo-embolism
Rhythm control
Rate control
ACC/AHA/ESC 2006 guidelines J Am Coll Cardiol 2006;48:854-906
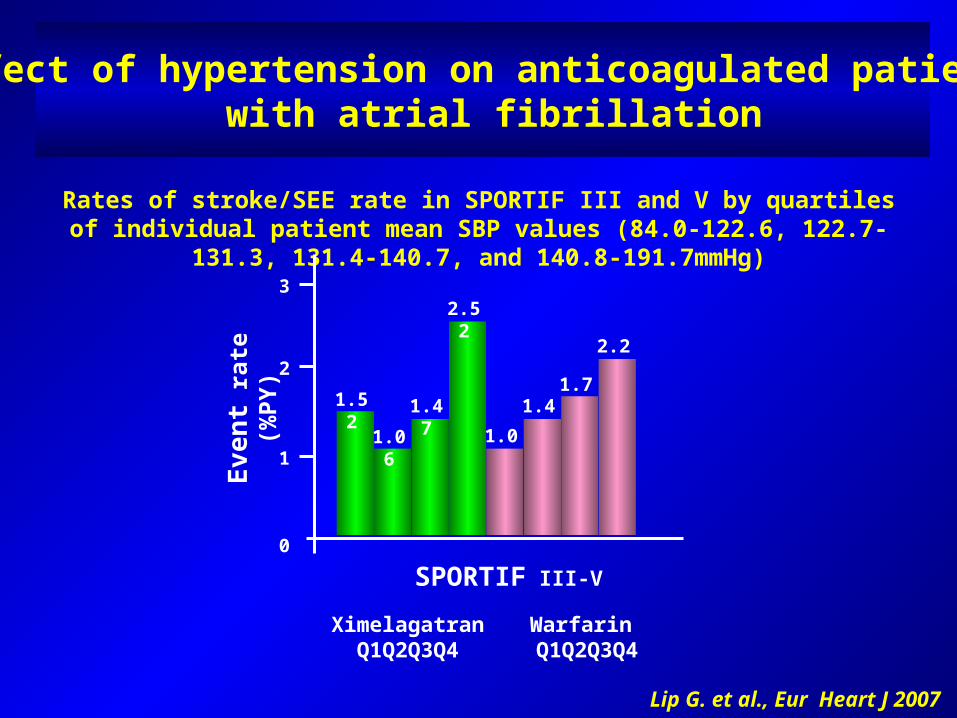
Effect of hypertension on anticoagulated patients with atrial fibrillation
Rates of stroke/SEE rate in SPORTIF III and V by quartiles of individual patient mean SBP values (84.0-122.6, 122.7-131.3, 131.4-140.7, and 140.8-191.7mmHg)
Lip G. et al., Eur Heart J 2007
0
1
2
3
SPORTIF III-V
XimelagatranQ1Q2Q3Q4
Warfarin Q1Q2Q3Q4
Eve
nt ra
te (%
PY)
1.52
1.061.47
2.52
1.061.47
1.77
2.26
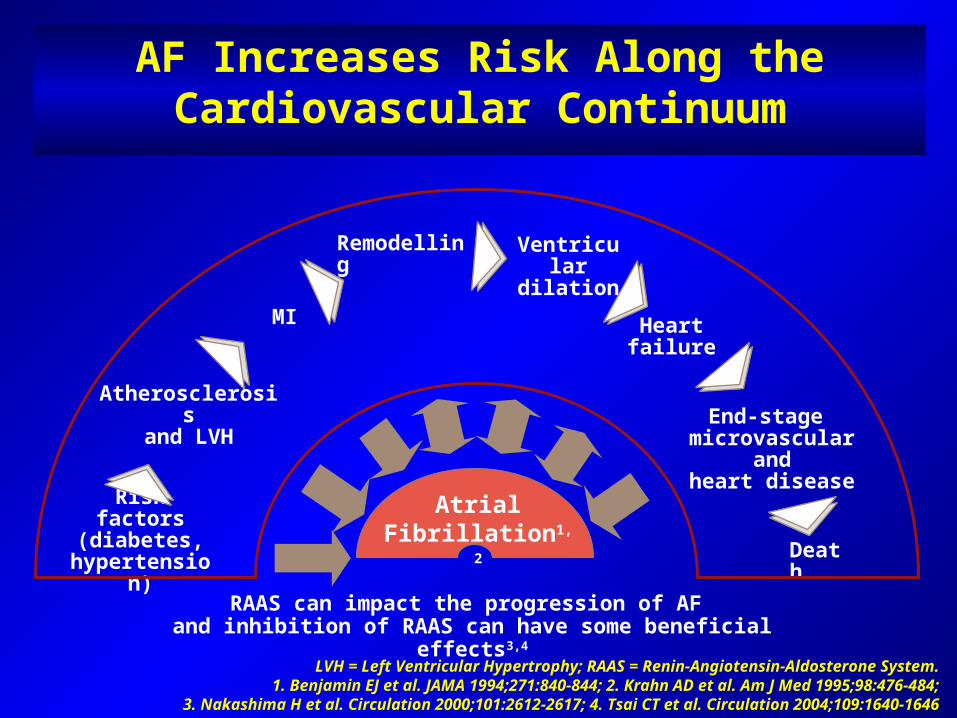
AF Increases Risk Along the Cardiovascular Continuum
RAAS can impact the progression of AF and inhibition of RAAS can have some beneficial effects3,4
LVH = Left Ventricular Hypertrophy; RAAS = Renin-Angiotensin-Aldosterone System.1. Benjamin EJ et al. JAMA 1994;271:840-844; 2. Krahn AD et al. Am J Med 1995;98:476-484;
3. Nakashima H et al. Circulation 2000;101:2612-2617; 4. Tsai CT et al. Circulation 2004;109:1640-1646
Risk factors(diabetes,
hypertension)
Atrial Fibrillation1,2
MI
Atherosclerosisand LVH
Remodelling Ventriculardilation
Heart failure
End-stage microvascular
andheart disease
Death
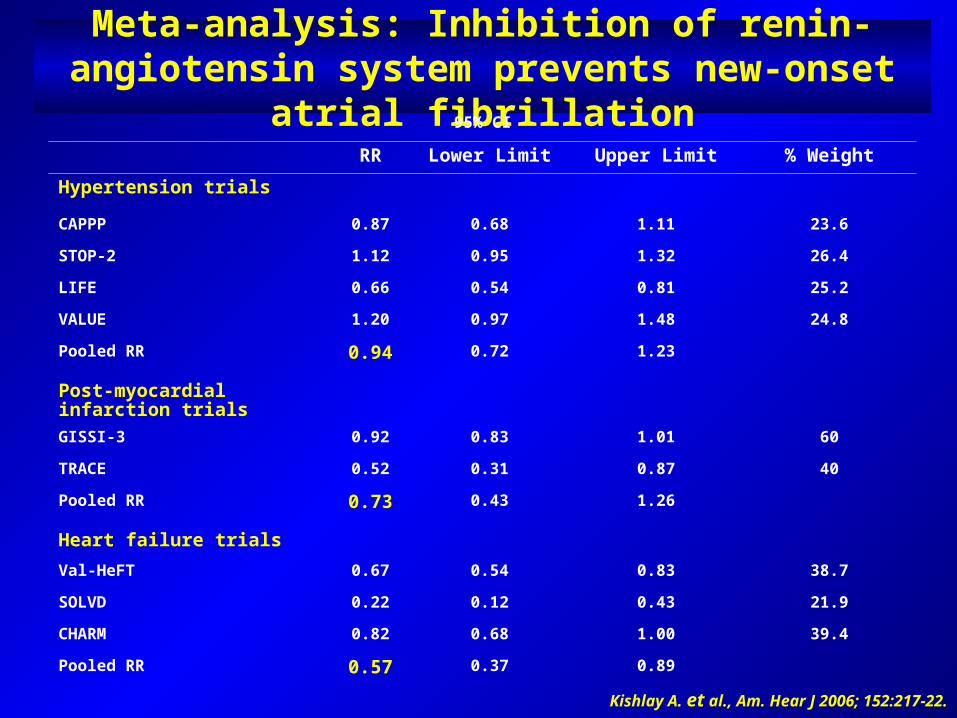
Meta-analysis: Inhibition of renin-angiotensin system prevents new-onset atrial fibrillation
95% CI
RR Lower Limit Upper Limit % Weight
Hypertension trials
CAPPP 0.87 0.68 1.11 23.6
STOP-2 1.12 0.95 1.32 26.4
LIFE 0.66 0.54 0.81 25.2
VALUE 1.20 0.97 1.48 24.8
Pooled RR 0.94 0.72 1.23
Post-myocardial infarction trialsGISSI-3 0.92 0.83 1.01 60
TRACE 0.52 0.31 0.87 40
Pooled RR 0.73 0.43 1.26
Heart failure trialsVal-HeFT 0.67 0.54 0.83 38.7
SOLVD 0.22 0.12 0.43 21.9
CHARM 0.82 0.68 1.00 39.4
Pooled RR 0.57 0.37 0.89
Kishlay A. et al., Am. Hear J 2006; 152:217-22.
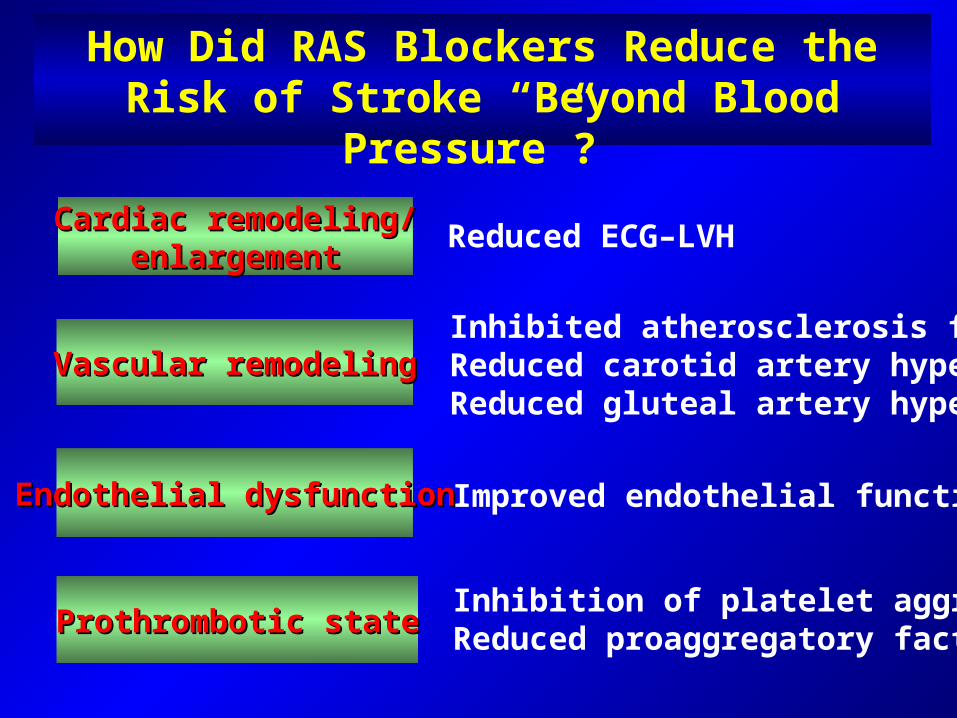
How Did RAS Blockers Reduce the Risk of Stroke “Beyond Blood Pressure”?
Cardiac remodeling/Cardiac remodeling/enlargementenlargement
Endothelial dysfunctionEndothelial dysfunction
Prothrombotic stateProthrombotic state
Vascular remodelingVascular remodeling
Reduced ECG–LVH
Improved endothelial function
Inhibition of platelet aggregationReduced proaggregatory factors
Inhibited atherosclerosis formationReduced carotid artery hypertrophy Reduced gluteal artery hypertrophy
Anti-thrombotic Therapy is Essential forReducing Risk of Stroke
Current clinical practice recommends that anticoagulation should be continued for life in patients at high risk of thrombo-embolism or with risk factors for atrial fibrillation recurrence
The CHADS2 (Cardiac Failure, Hypertension, Age, Diabetes, Stroke [Doubled]) is a points based system for predicting risk of stroke in AF, based on key risk factors and serves as a guideline for anticoagulation treatment
Prior stroke or TIA 2 pointsAge >75 years 1 pointHypertension 1 pointDiabetes mellitus 1 point Heart failure 1 point
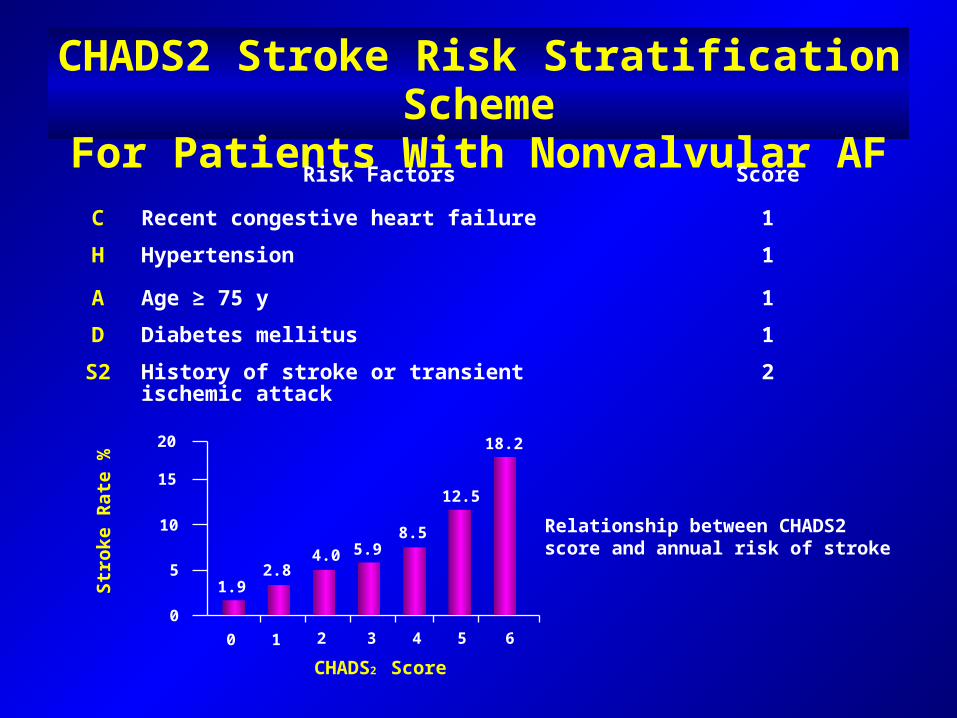
CHADS2 Stroke Risk Stratification SchemeFor Patients With Nonvalvular AF
Risk Factors Score
C Recent congestive heart failure 1H Hypertension 1
A Age ≥ 75 y 1D Diabetes mellitus 1S2 History of stroke or transient ischemic attack 2
CHADS2 Score
Stro
ke R
ate
%
20
15
10
5
0
1.92.8
4.0 5.98.5
12.5
18.2
1 2 30 4 5 6
Relationship between CHADS2 score and annual risk of stroke
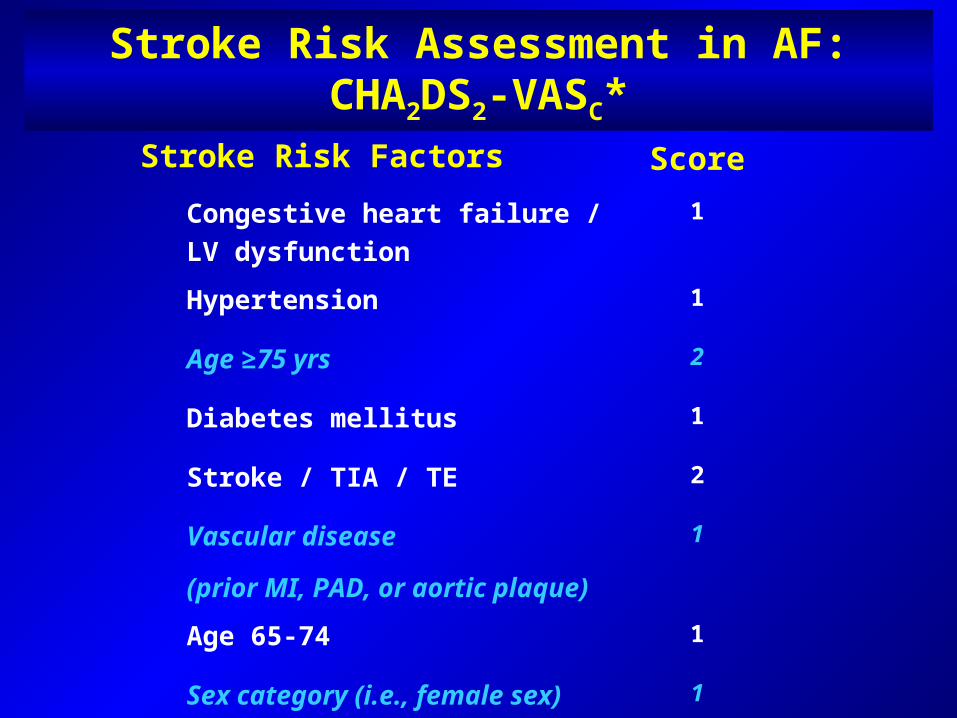
Stroke Risk Assessment in AF:CHA2DS2-VASC*
Stroke Risk Factors Score
Congestive heart failure / LV dysfunction
1
Hypertension 1
Age ≥75 yrs 2
Diabetes mellitus 1
Stroke / TIA / TE 2
Vascular disease
(prior MI, PAD, or aortic plaque)
1
Age 65-74 1
Sex category (i.e., female sex) 1
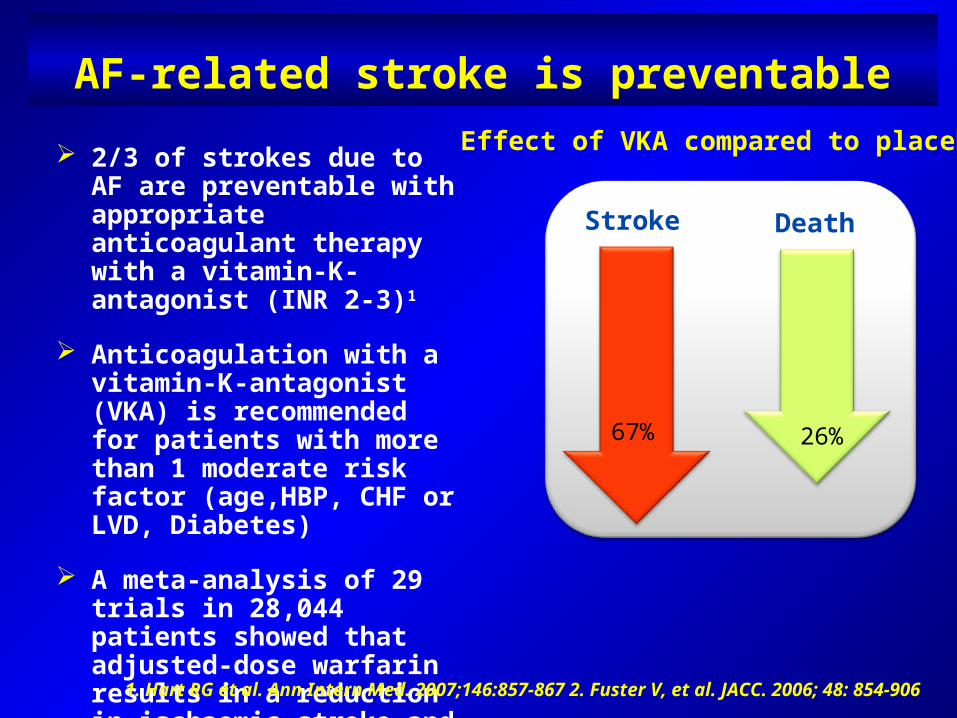
AF-related stroke is preventable
2/3 of strokes due to AF are preventable with appropriate anticoagulant therapy with a vitamin-K-antagonist (INR 2-3)1
Anticoagulation with a vitamin-K-antagonist (VKA) is recommended for patients with more than 1 moderate risk factor (age,HBP, CHF or LVD, Diabetes)
A meta-analysis of 29 trials in 28,044 patients showed that adjusted-dose warfarin results in a reduction in ischaemic stroke and in all-cause mortality1
Stroke Death
67% 26%
1. Hart RG et al. Ann Intern Med. 2007;146:857-867 2. Fuster V, et al. JACC. 2006; 48: 854-906
Effect of VKA compared to placebo
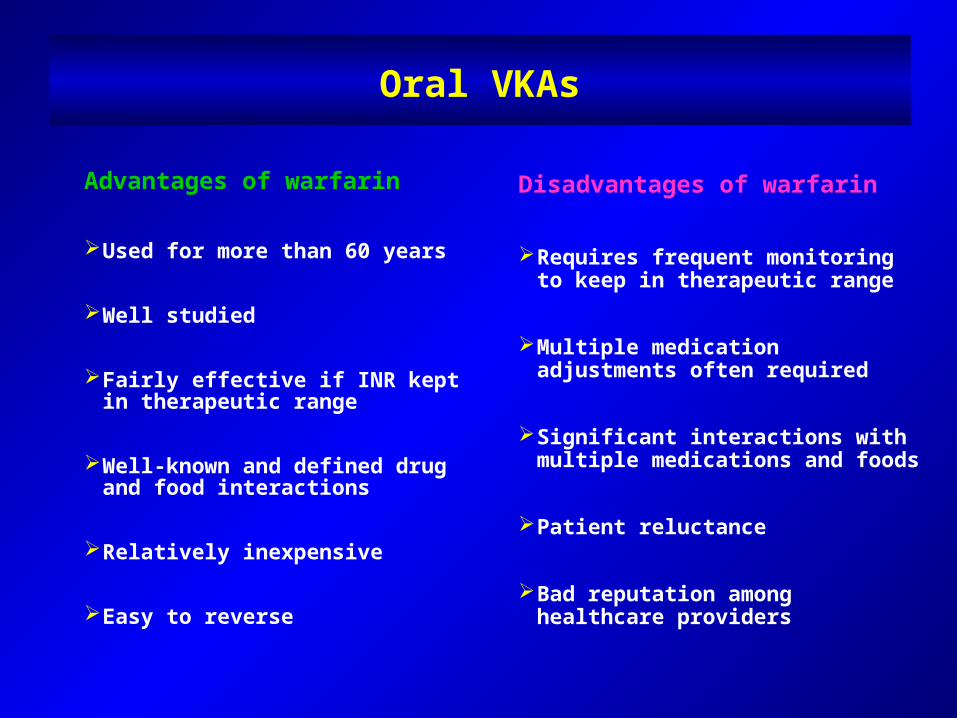
Oral VKAs
Advantages of warfarin
Used for more than 60 years
Well studied
Fairly effective if INR kept in therapeutic range
Well-known and defined drug and food interactions
Relatively inexpensive
Easy to reverse
Disadvantages of warfarin
Requires frequent monitoring to keep in therapeutic range
Multiple medication adjustments often required
Significant interactions with multiple medications and foods
Patient reluctance
Bad reputation among healthcare providers
Underuse of oral anticoagulants in AF:A Systematic Review
Ogilvie I et al Am J Med 2010;123:638
Underuse of oral anticoagulants for high-risk atrial fibrillation patients was found in most of the 54 studies (1998-2008) reporting both patient stroke risk and patients treated.
Over two thirds of studies of atrial fibrillation patients with prior stroke or transient ischemic attack reported treatment levels of under 60% of eligible patients.
Most studies based on CHADS2 score reported oral anticoagulant treatment levels of high-risk subjects below 70%.
Key features of a “new contender” in the prevention of CV events in AF
Freedom from coagulation monitoring
Simpler kinetic profile
More rapid onset and offset
Reduced or absent drug-drug and drug-food interactions
More “user-friendly” than Warfarin
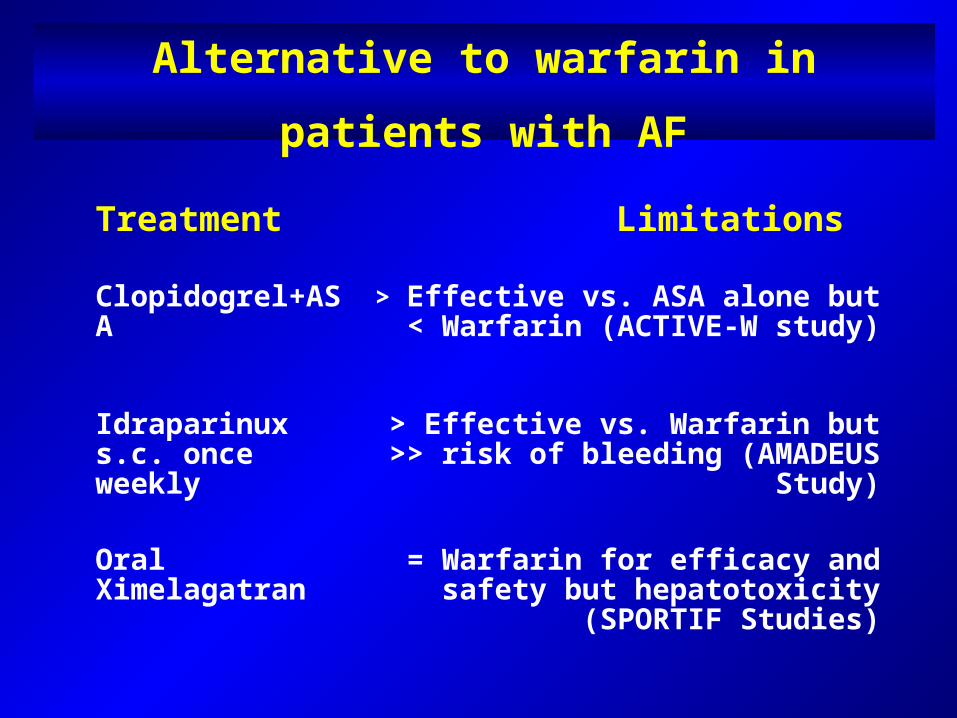
Alternative to warfarin in patients with AF
Treatment Limitations
Clopidogrel+ASA > Effective vs. ASA alone but < Warfarin (ACTIVE-W study)
Idraparinux s.c. once weekly
> Effective vs. Warfarin but >> risk of bleeding (AMADEUS Study)
Oral Ximelagatran = Warfarin for efficacy and safety but hepatotoxicity (SPORTIF Studies)
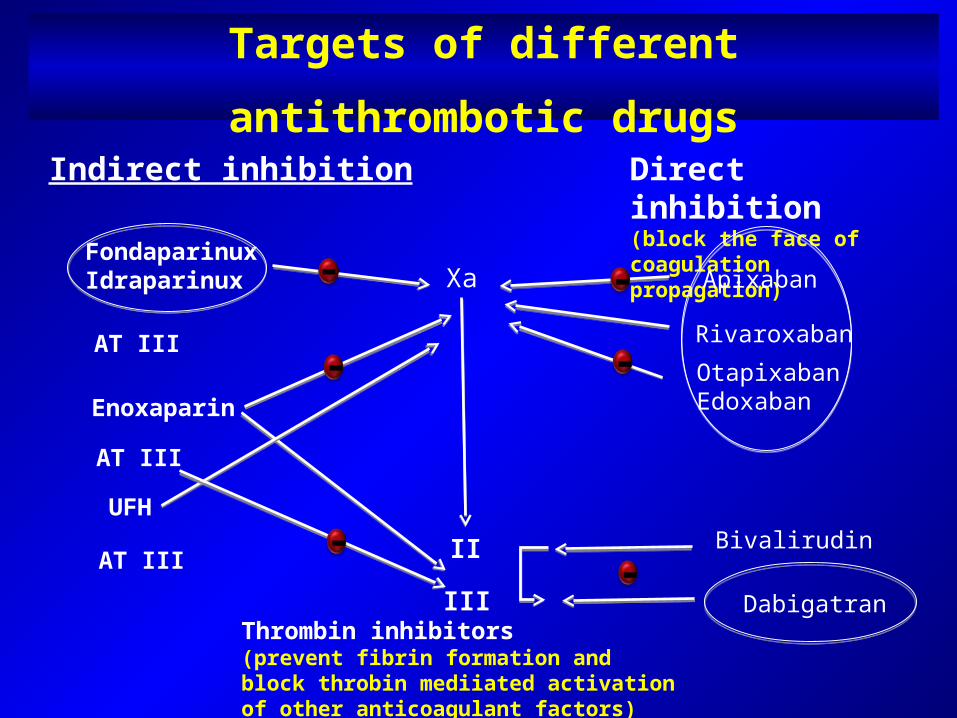
Targets of different antithrombotic drugs
Indirect inhibition Direct inhibition(block the face of coagulation propagation)
FondaparinuxIdraparinux
AT III
Enoxaparin
AT III
UFH
AT III
Xa
IIIII
Apixaban
Bivalirudin
Dabigatran
-
-
-
RivaroxabanOtapixabanEdoxaban
--
-Thrombin inhibitors(prevent fibrin formation andblock throbin mediiated activationof other anticoagulant factors)
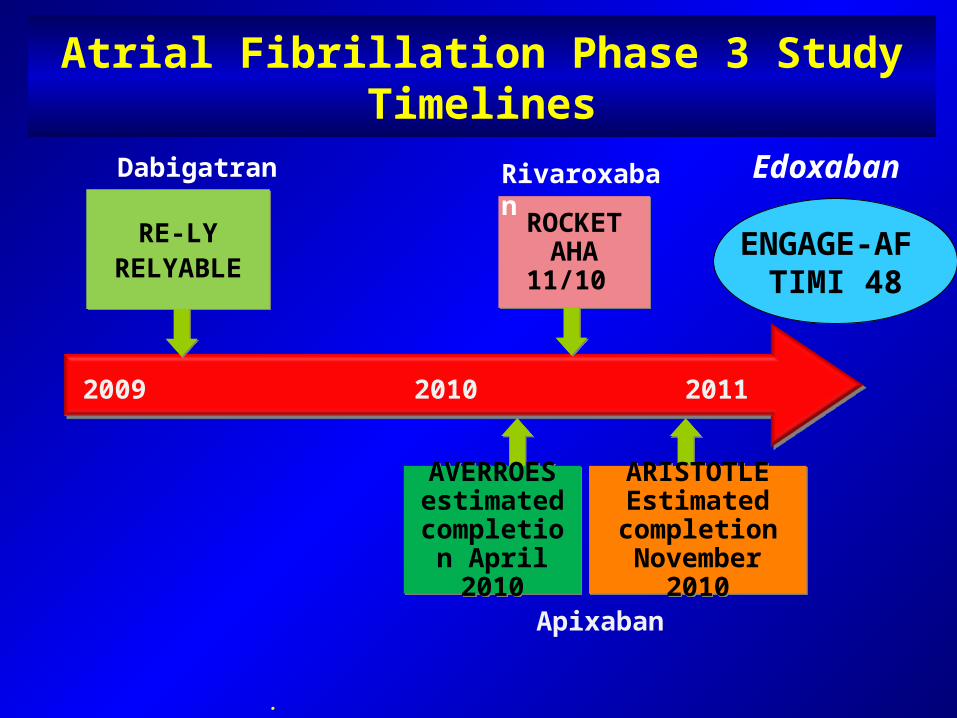
Apixaban
.
ROCKETAHA 11/10
Rivaroxaban
RE-LYRELYABLE
Dabigatran
2009 2010 2011
AVERROES estimated
completion April 2010
ARISTOTLEEstimated completion
November 2010
Atrial Fibrillation Phase 3 Study Timelines
ENGAGE-AF TIMI 48
Edoxaban
Oral Factor Xa inhibitors
Parenteral Factor Xa inhibitors(modified idraparinux)
New oral direct thrombin inhibitors(other than ximelagatran)
NEW PERSPECTIVES
Antithrombotic Prophylaxis in AF

Rivaroxaban Bayer Phase III
Apixaban Bristol-Myers Squibb Phase III
Edoxaban Daiichi Sankyo Phase III
YM 150 Astellas Pharma Planned
LY 517717 Lilly Planned
PRT 054021 Portola Planned
New Oral Direct FXa Inhibitors Under Investigation for Stroke Prevention in Atrial Fibrillation
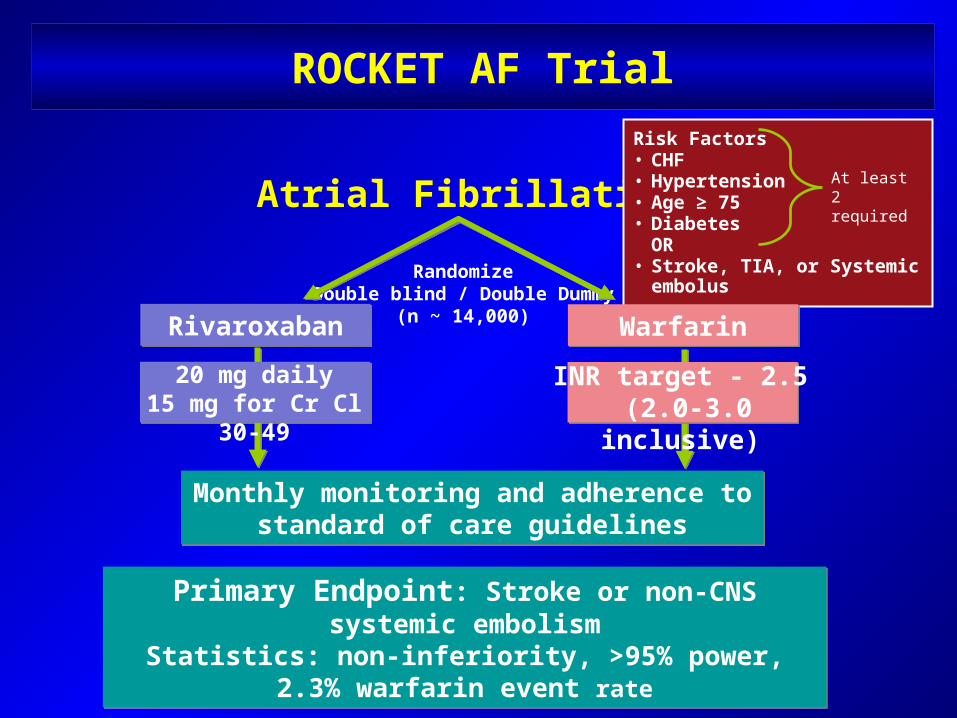
ROCKET AF Trial
Rivaroxaban
Primary Endpoint: Stroke or non-CNS systemic embolismStatistics: non-inferiority, >95% power, 2.3% warfarin event
rate
Atrial Fibrillation
RandomizeDouble blind / Double Dummy
(n ~ 14,000)
Risk Factors• CHF • Hypertension • Age ≥ 75 • Diabetes
OR• Stroke, TIA, or Systemic embolus
At least 2 required
Monthly monitoring and adherence to standard of care guidelines
20 mg daily15 mg for Cr Cl 30-49
Warfarin
INR target - 2.5 (2.0-3.0 inclusive)
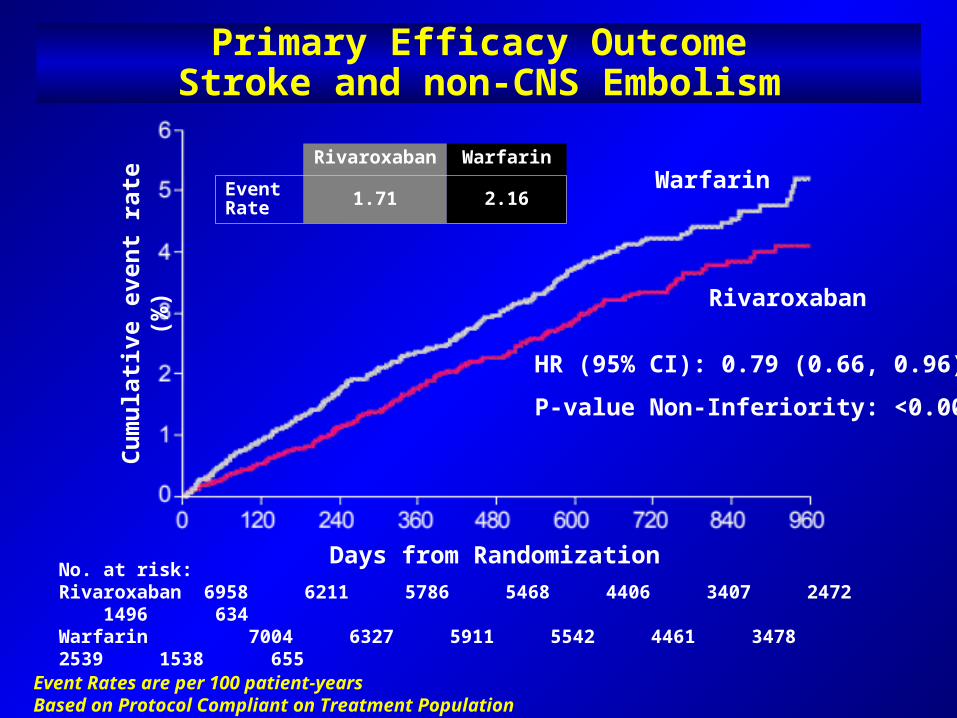
Primary Efficacy OutcomeStroke and non-CNS Embolism
Event Rates are per 100 patient-yearsBased on Protocol Compliant on Treatment Population
No. at risk:Rivaroxaban 6958 6211 5786 5468 4406 3407 2472 1496 634Warfarin 7004 6327 5911 5542 4461 3478 2539 1538 655
Warfarin
HR (95% CI): 0.79 (0.66, 0.96)
P-value Non-Inferiority: <0.001
Days from Randomization
Cum
ulat
ive
even
t rat
e (%
)
Rivaroxaban
Rivaroxaban WarfarinEvent Rate 1.71 2.16
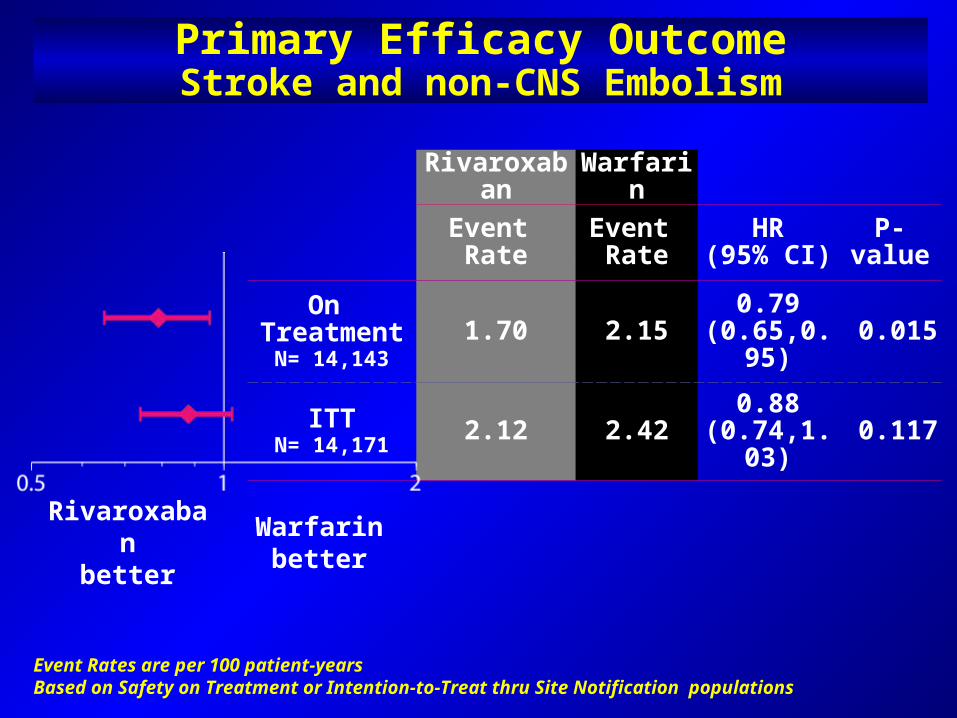
Rivaroxaban Warfarin Event Rate
Event Rate
HR(95% CI) P-value
On TreatmentN= 14,143
1.70 2.15 0.79 (0.65,0.95) 0.015
ITTN= 14,171 2.12 2.42 0.88
(0.74,1.03) 0.117
Rivaroxabanbetter
Warfarinbetter
Primary Efficacy OutcomeStroke and non-CNS Embolism
Event Rates are per 100 patient-yearsBased on Safety on Treatment or Intention-to-Treat thru Site Notification populations
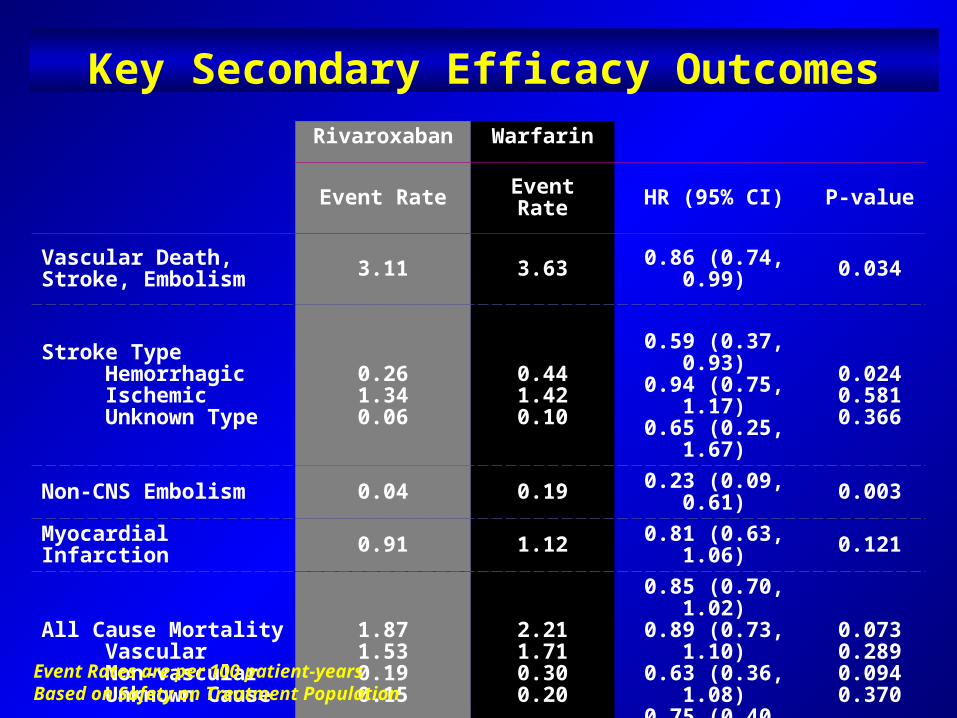
Key Secondary Efficacy OutcomesRivaroxaban Warfarin
Event Rate Event Rate HR (95% CI) P-value
Vascular Death, Stroke, Embolism 3.11 3.63 0.86 (0.74, 0.99) 0.034
Stroke Type Hemorrhagic Ischemic Unknown Type
0.261.340.06
0.441.420.10
0.59 (0.37, 0.93)0.94 (0.75, 1.17)0.65 (0.25, 1.67)
0.0240.5810.366
Non-CNS Embolism 0.04 0.19 0.23 (0.09, 0.61) 0.003
Myocardial Infarction 0.91 1.12 0.81 (0.63, 1.06) 0.121
All Cause Mortality Vascular Non-vascular Unknown Cause
1.871.530.190.15
2.211.710.300.20
0.85 (0.70, 1.02)0.89 (0.73, 1.10)0.63 (0.36, 1.08)0.75 (0.40, 1.41)
0.0730.2890.0940.370
Event Rates are per 100 patient-yearsBased on Safety on Treatment Population
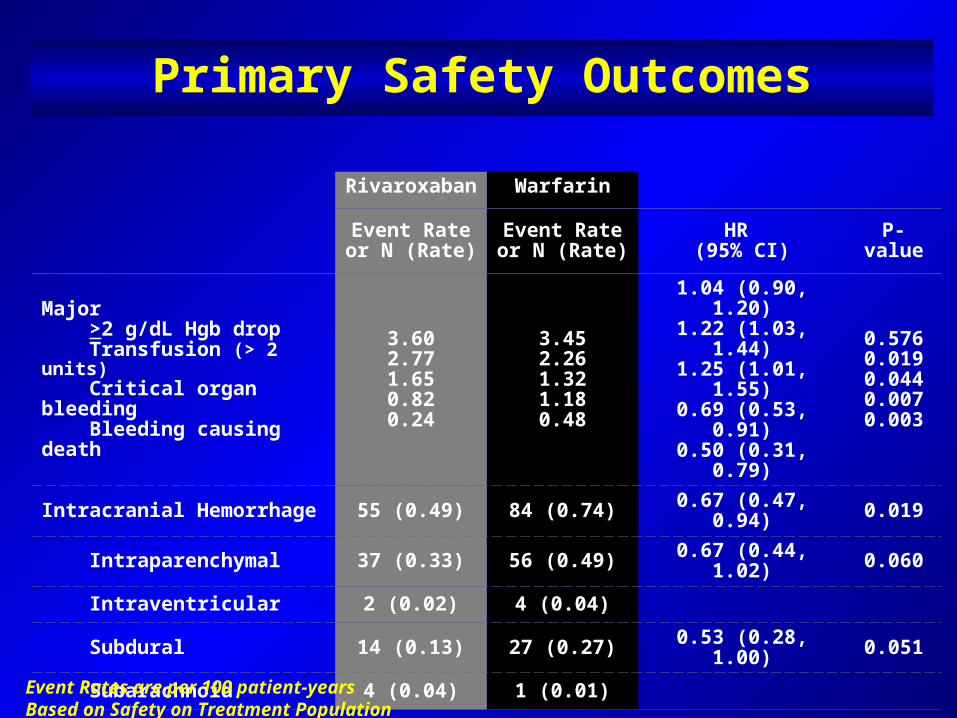
Rivaroxaban Warfarin
Event Rate or N (Rate)
Event Rate or N (Rate)
HR (95% CI) P-value
Major >2 g/dL Hgb drop Transfusion (> 2 units) Critical organ bleeding Bleeding causing death
3.602.771.650.820.24
3.452.261.321.180.48
1.04 (0.90, 1.20)1.22 (1.03, 1.44)1.25 (1.01, 1.55)0.69 (0.53, 0.91)0.50 (0.31, 0.79)
0.5760.0190.0440.0070.003
Intracranial Hemorrhage 55 (0.49) 84 (0.74) 0.67 (0.47, 0.94) 0.019
Intraparenchymal 37 (0.33) 56 (0.49) 0.67 (0.44, 1.02) 0.060
Intraventricular 2 (0.02) 4 (0.04)
Subdural 14 (0.13) 27 (0.27) 0.53 (0.28, 1.00) 0.051
Subarachnoid 4 (0.04) 1 (0.01)
Event Rates are per 100 patient-yearsBased on Safety on Treatment Population
Primary Safety Outcomes
Summary
Efficacy: Rivaroxaban was non-inferior to warfarin for prevention of
stroke and non-CNS embolism. Rivaroxaban was superior to warfarin while patients were
taking study drug. By intention-to-treat, rivaroxaban was non-inferior to
warfarin but did not achieve superiority. Safety:
Similar rates of bleeding and adverse events. Less ICH and fatal bleeding with rivaroxaban.
Conclusion: Rivaroxaban is a proven alternative to warfarin for
moderate or high risk patients with AF.
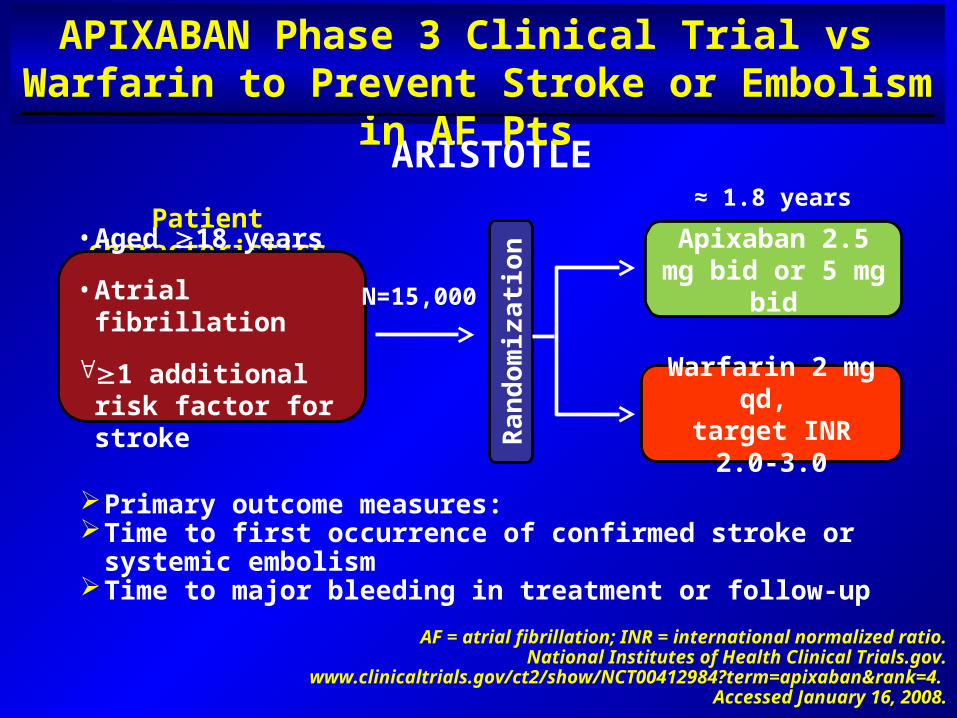
ARISTOTLE
APIXABAN Phase 3 Clinical Trial vs Warfarin to Prevent Stroke or Embolism in AF Pts
AF = atrial fibrillation; INR = international normalized ratio.National Institutes of Health Clinical Trials.gov.
www.clinicaltrials.gov/ct2/show/NCT00412984?term=apixaban&rank=4. Accessed January 16, 2008.
Apixaban 2.5 mg bid or 5 mg bid
Warfarin 2 mg qd, target INR 2.0-3.0
Primary outcome measures: Time to first occurrence of confirmed stroke or systemic embolismTime to major bleeding in treatment or follow-up
Patient characteristics
Ran
dom
izat
ion
≈ 1.8 years
• Aged 18 years
• Atrial fibrillation
1 additional risk factor for stroke
N=15,000
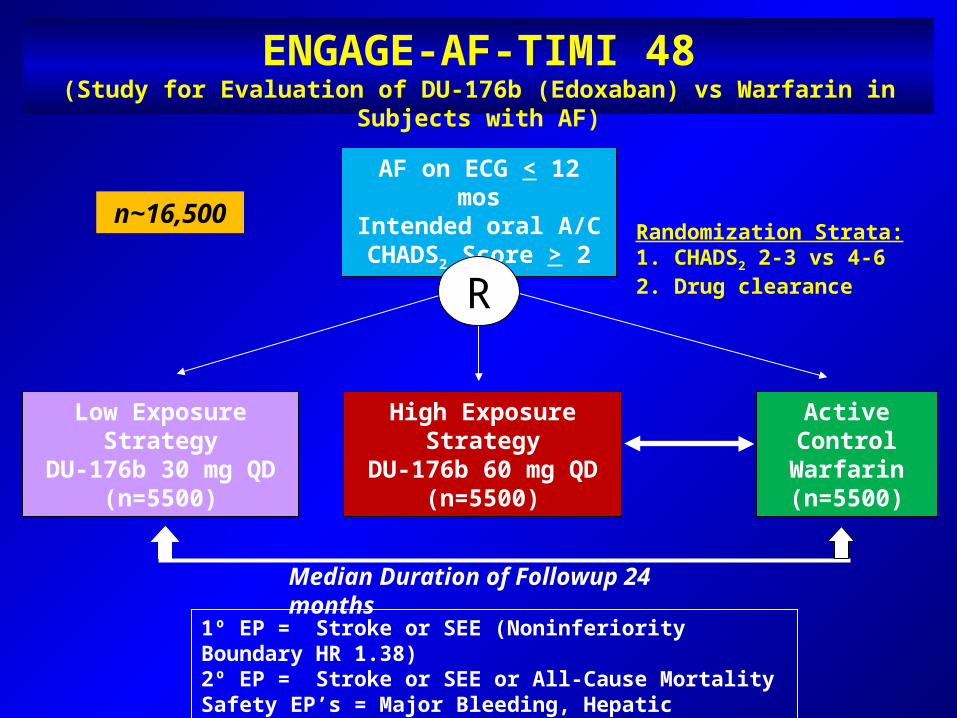
ENGAGE-AF-TIMI 48(Study for Evaluation of DU-176b (Edoxaban) vs Warfarin in Subjects with AF)
Low Exposure StrategyDU-176b 30 mg QD
(n=5500)
Active ControlWarfarin(n=5500)
High Exposure StrategyDU-176b 60 mg QD
(n=5500)
1º EP = Stroke or SEE (Noninferiority Boundary HR 1.38)2º EP = Stroke or SEE or All-Cause MortalitySafety EP’s = Major Bleeding, Hepatic Function
AF on ECG < 12 mosIntended oral A/CCHADS2 Score > 2
RRandomization Strata:1. CHADS2 2-3 vs 4-62. Drug clearance
Median Duration of Followup 24 months
n~16,500
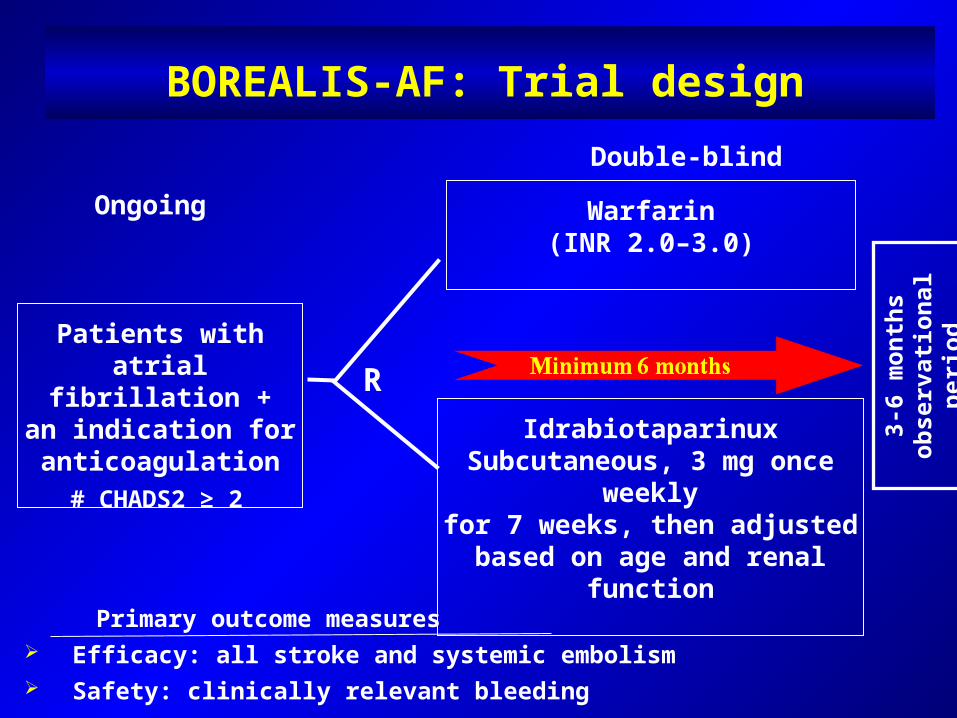
Patients with atrial fibrillation +
an indication for anticoagulation
IdrabiotaparinuxSubcutaneous, 3 mg once weekly
for 7 weeks, then adjusted based on age and renal function
Warfarin(INR 2.0–3.0)
R
BOREALIS-AF: Trial design
Primary outcome measures Efficacy: all stroke and systemic embolism Safety: clinically relevant bleeding
Ongoing
Double-blind
# CHADS2 ≥ 2
3-6
mon
ths
obse
rvat
iona
l per
iod
Anti-Thrombotic Prophylaxis in AF
Oral Factor Xa inhibitors
Parenteral Factor Xa inhibitors(modified idraparinux)
New oral direct thrombin inhibitors(other than ximelagatran)
NEW PERSPECTIVES
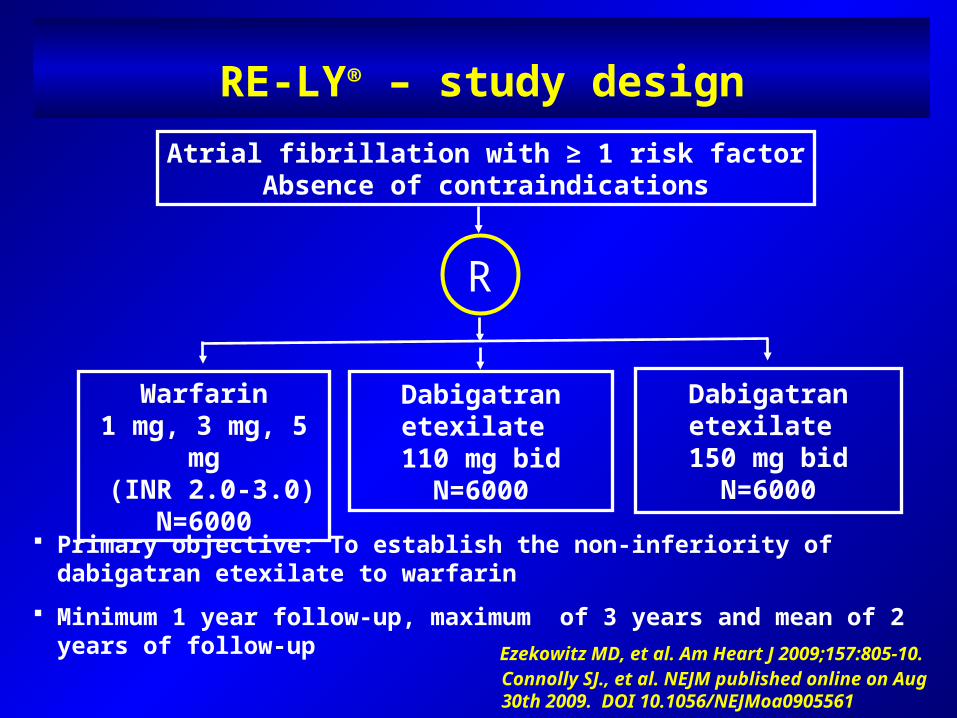
RE-LY® – study designAtrial fibrillation with ≥ 1 risk factor
Absence of contraindications
R
Warfarin1 mg, 3 mg, 5 mg
(INR 2.0-3.0)N=6000
Dabigatran etexilate 110 mg bid
N=6000
Dabigatran etexilate 150 mg bid
N=6000
Primary objective: To establish the non-inferiority of dabigatran etexilate to warfarin
Minimum 1 year follow-up, maximum of 3 years and mean of 2 years of follow-up
Ezekowitz MD, et al. Am Heart J 2009;157:805-10.Connolly SJ., et al. NEJM published online on Aug 30th 2009. DOI 10.1056/NEJMoa0905561
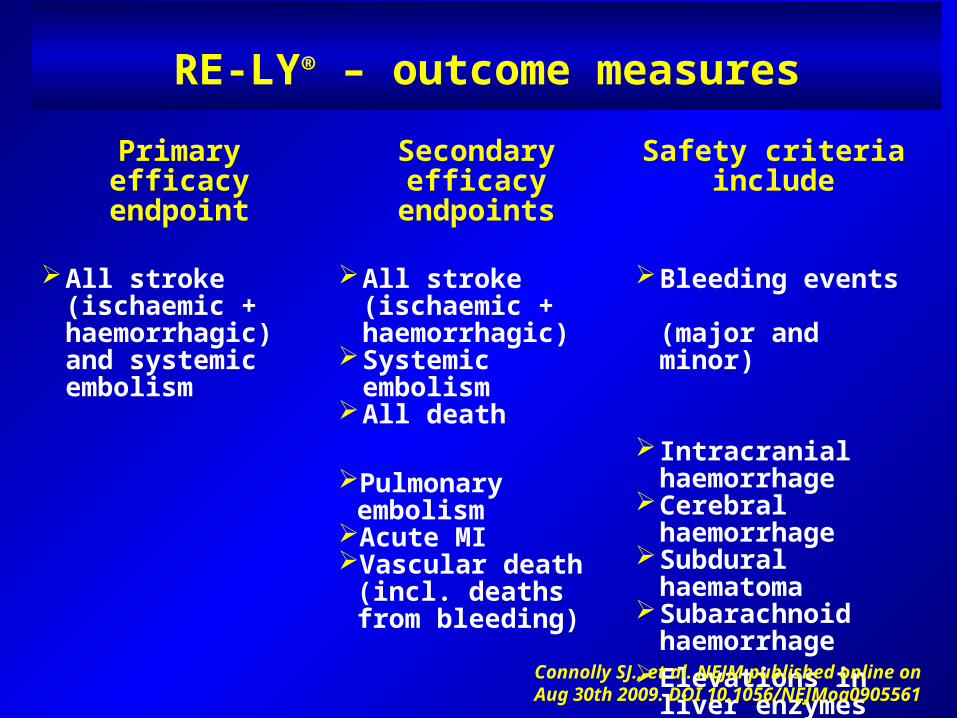
RE-LY® – outcome measures
Primary efficacy endpoint
Secondary efficacy endpoints
Safety criteria include
All stroke (ischaemic + haemorrhagic) and systemic embolism
All stroke (ischaemic + haemorrhagic)
Systemic embolismAll death
Bleeding events (major and minor)
Pulmonary embolismAcute MIVascular death (incl.
deaths from bleeding)
Intracranial haemorrhage
Cerebral haemorrhage
Subdural haematomaSubarachnoid
haemorrhageElevations in liver
enzymes or hepatic dysfunction
Connolly SJ., et al. NEJM published online on Aug 30th 2009. DOI 10.1056/NEJMoa0905561
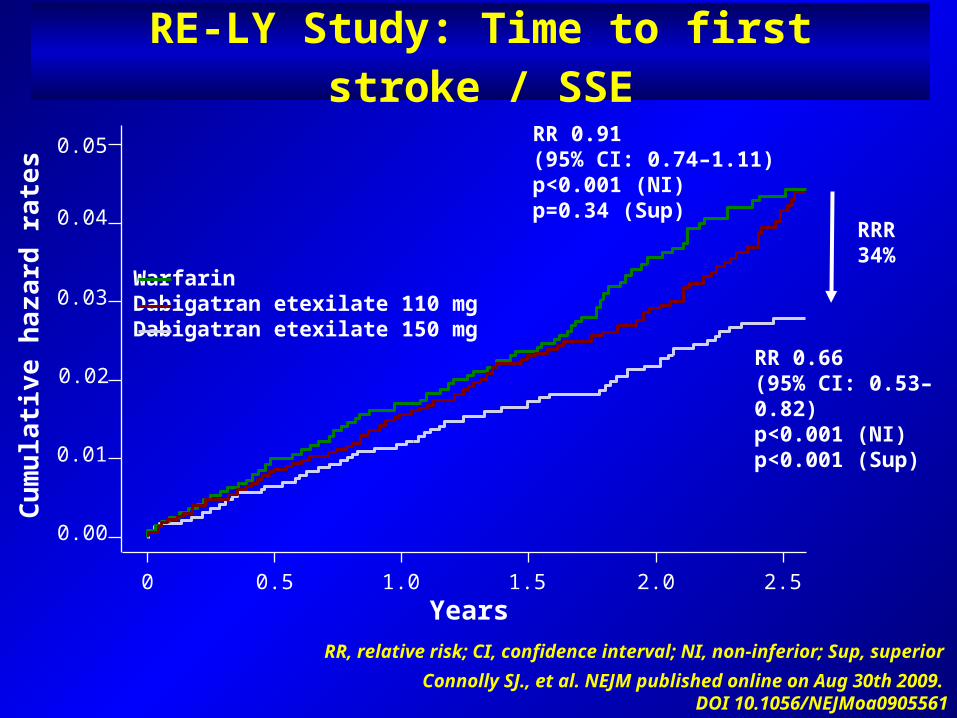
RE-LY Study: Time to first stroke / SSE
RR, relative risk; CI, confidence interval; NI, non-inferior; Sup, superiorConnolly SJ., et al. NEJM published online on Aug 30th 2009.
DOI 10.1056/NEJMoa0905561
0.01
0.02
0.03
0.05
0.04
Cum
ulat
ive
haza
rd r
ates
RR 0.91(95% CI: 0.74–1.11)p<0.001 (NI)p=0.34 (Sup)
RR 0.66(95% CI: 0.53–0.82)p<0.001 (NI)p<0.001 (Sup)
Years0 0.5 1.0 1.5 2.0 2.5
0.00
WarfarinDabigatran etexilate 110 mgDabigatran etexilate 150 mg
RRR34%
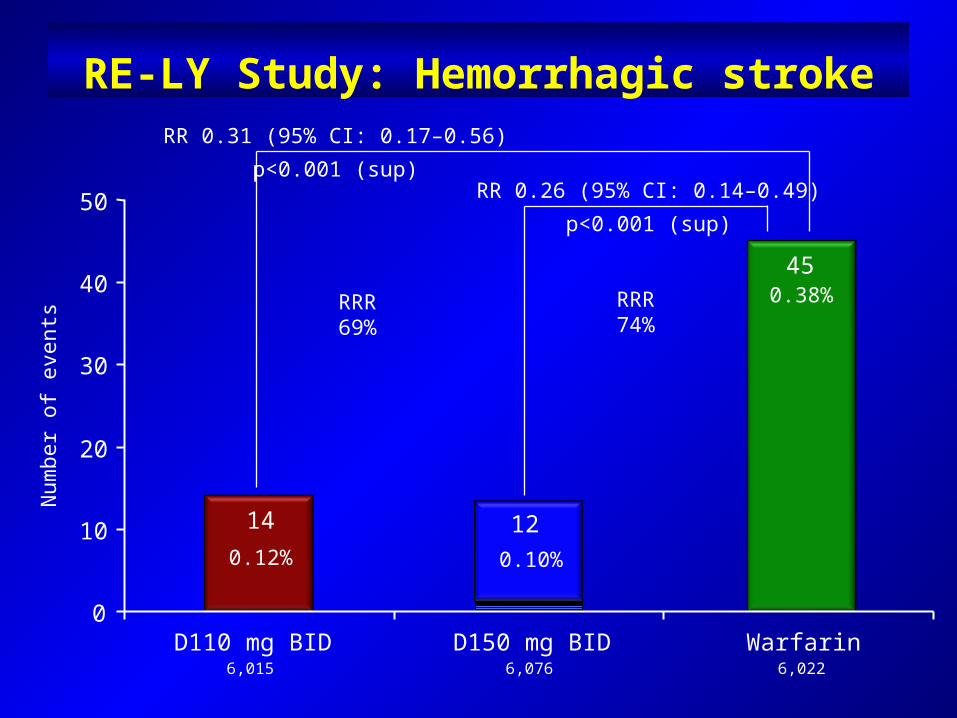
RE-LY Study: Hemorrhagic stroke
RR 0.26 (95% CI: 0.14–0.49)p<0.001 (sup)
RR 0.31 (95% CI: 0.17–0.56)p<0.001 (sup)
Num
ber o
f eve
nts
6,015 6,076 6,022
14 12
45
0
10
20
30
40
50
D110 mg BID D150 mg BID Warfarin
0.10%
0.38%
RRR69%
RRR74%
0.12%
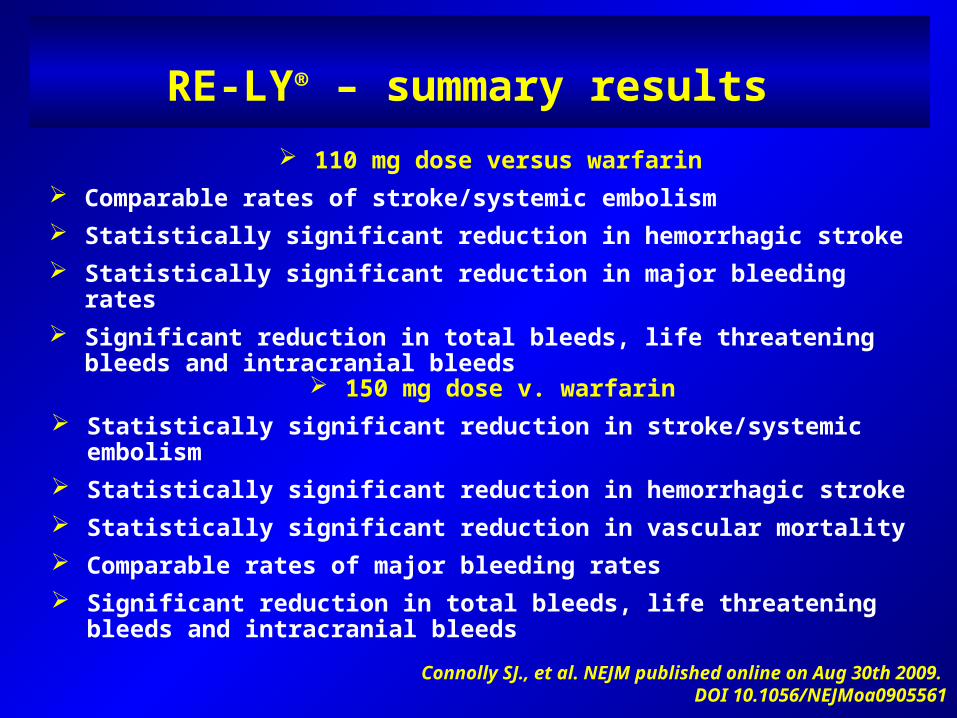
RE-LY® – summary results
150 mg dose v. warfarin Statistically significant reduction in stroke/systemic embolism Statistically significant reduction in hemorrhagic stroke Statistically significant reduction in vascular mortality Comparable rates of major bleeding rates Significant reduction in total bleeds, life threatening bleeds and intracranial bleeds
110 mg dose versus warfarin Comparable rates of stroke/systemic embolism Statistically significant reduction in hemorrhagic stroke Statistically significant reduction in major bleeding rates Significant reduction in total bleeds, life threatening bleeds and intracranial bleeds
Connolly SJ., et al. NEJM published online on Aug 30th 2009. DOI 10.1056/NEJMoa0905561
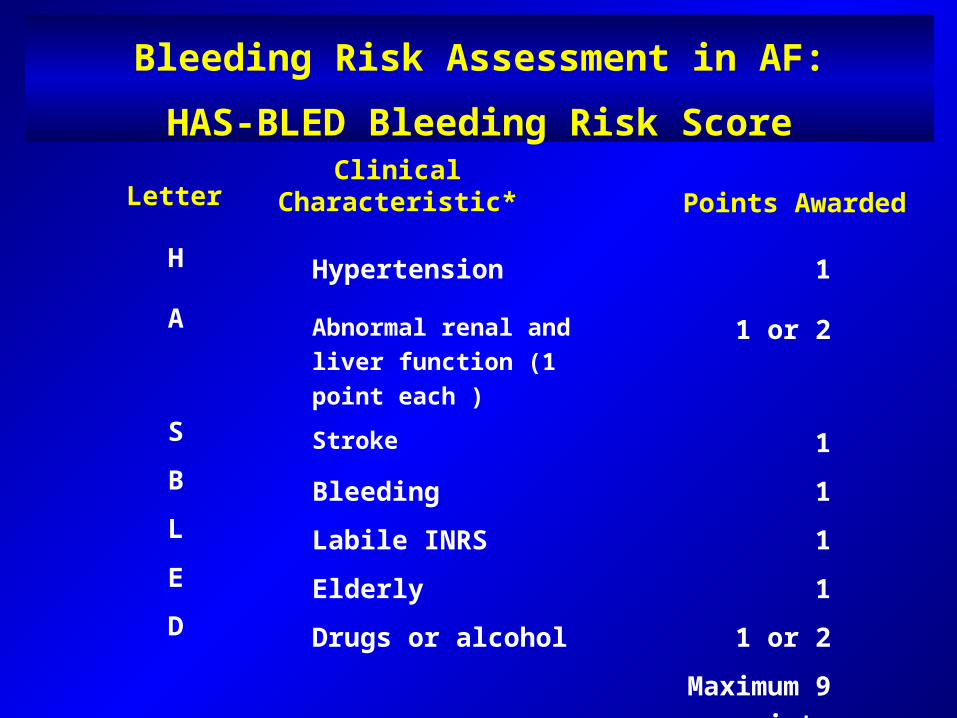
Bleeding Risk Assessment in AF:
HAS-BLED Bleeding Risk ScoreClinical
Characteristic* Points Awarded
H Hypertension 1
A Abnormal renal and liver function (1 point each )
1 or 2
S Stroke 1B Bleeding 1L Labile INRS 1E Elderly 1D Drugs or alcohol 1 or 2
Maximum 9 points
Letter
Ideal candidates for the use of Dabigatran among
patients with AF
Warfarin-naïve
Hard to maintain the therapeutic range
Previous bleeding complication with Warfarin
Multiple medications (high risk of interactions)
Open issues in the RE-LY study
Short follow-up (safety requires longer observations)
Small but significant excess of MI in high dose of Dabigatran
vs. Warfarin
The risk/benefit of combining Warfarin with antiplatelet agents
(only 20% of study patients)
Safety and efficacy in patients with renal failure
(<30 ml/min excluded from study)
No known antidote or reversal agent for Dabigatran
Dabigatran: FDA approval
FDA advisory panel in September voted 9-0 to recommend that dabigatran be approved
FDA approved October 20,2010
Doses approved: 150 mg twice daily
75 mg twice daily (severe renal impairment)
Canadian Cardiovascular Guidelines for AF
Based on its safety and efficacy profile, dabigatran is preferred over warfarin. Overall, the 150 mg dose of dabigatran is preferred over the 110 mg dose.
For patients at low risk of stroke (CHADS2 score=1), treatment should include either warfarin or dabigatran. However, based on individual risk/benefit considerations, aspirin is a resonable alternative.
For patients at moderate to high risk of stroke (CHADS2 >2), treatment should include either warfarin or dabigatran
October 26,2010
How can we make a strong recommendation
from one trial?
That single trial includes more patients than all the trials with warfarin combined (18.000 patients)
Comprehensive Management of AF Should Addressits Multiple Impacts
In addition to stroke prevention and reduction of AF burden*, successful management of AF should also aim at further reducing
hospitalisations as well as CV morbidity and mortality
Prevention of
thrombo-embolism
Reduction of AF burden*↑ QoL↓ Symptoms
Reduction in the risk
of CV events and
hospitalisations
Reductionin
mortality
Current Treatment Strategies for AF
Rhythm control
Rate control
Prevention of thromboembolism
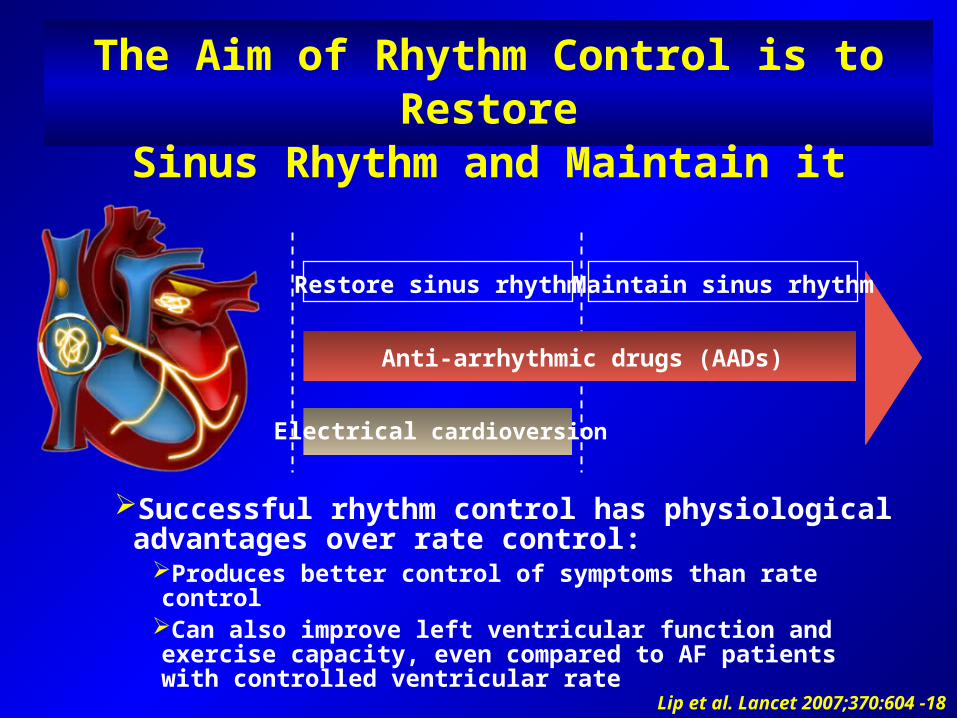
The Aim of Rhythm Control is to RestoreSinus Rhythm and Maintain it
Restore sinus rhythm Maintain sinus rhythm
Successful rhythm control has physiological advantages over rate control:
Produces better control of symptoms than rate controlCan also improve left ventricular function and exercise capacity, even compared to AF patients with controlled ventricular rate
Lip et al. Lancet 2007;370:604 -18
Anti-arrhythmic drugs (AADs)
Electrical cardioversion
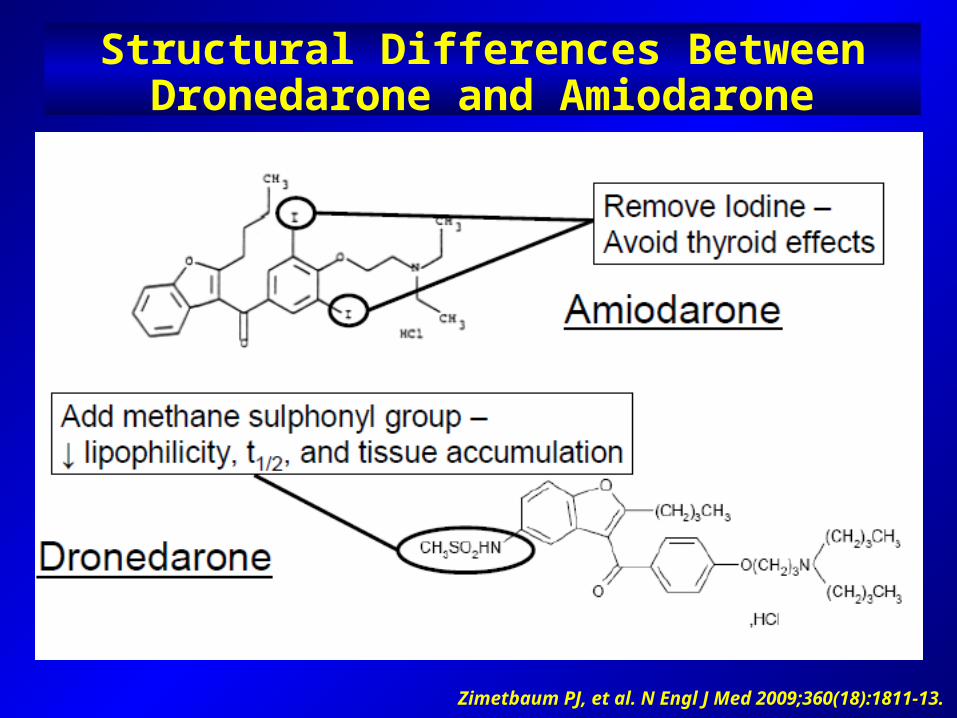
Structural Differences Between Dronedarone and Amiodarone
Zimetbaum PJ, et al. N Engl J Med 2009;360(18):1811-13.
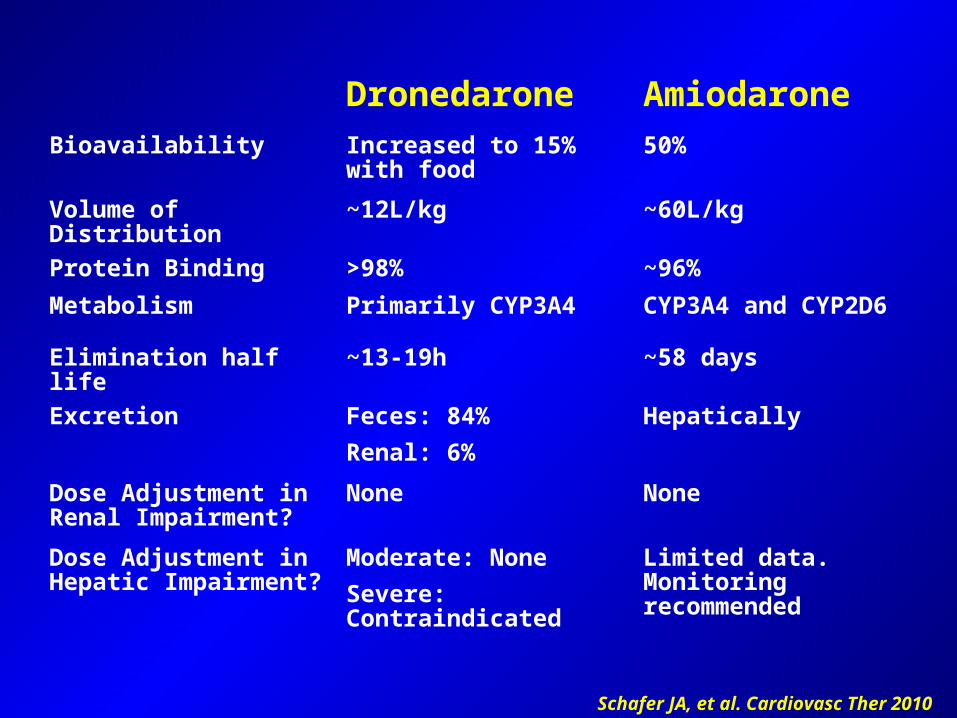
Schafer JA, et al. Cardiovasc Ther 2010
Dronedarone AmiodaroneBioavailability Increased to 15% with
food50%
Volume of Distribution ~12L/kg ~60L/kgProtein Binding >98% ~96%Metabolism Primarily CYP3A4 CYP3A4 and CYP2D6
Elimination half life ~13-19h ~58 daysExcretion Feces: 84%
Renal: 6%Hepatically
Dose Adjustment in Renal Impairment?
None None
Dose Adjustment in Hepatic Impairment?
Moderate: NoneSevere: Contraindicated
Limited data. Monitoring recommended
Dronedarone has Multiple Properties
Extensive anti-arrhythmic efficacy at atrial and ventricular level1, 2
Rate controlling effects1
Vasodilatory effects2
Anti-adrenergic effects3
Blood pressure lowering properties4
1 Gautier P, et al. J Cardiovasc Pharmacol. 2003;41(2):191-202. 2 Hodeige D, et al. European Journal of Pharmacology 1995;279:25-32.
3 Guiraudou P, et al. European Journal of Pharmacology 2004;496:119-127.4 Hohnloser SH et al. N Engl J Med 2009;360:668-78.
Multaq [package insert]. Bridgewater, NJ: Sanofi Aventis; 2009
• Dronedarone increases serum creatinine levels~0.1 mg/dl increaseInhibits tubular secretion of creatinineNo effect on GFRRapid onset, plateaus after 7 days, reversible upon drug discontinuation
Dronedarone – Warnings
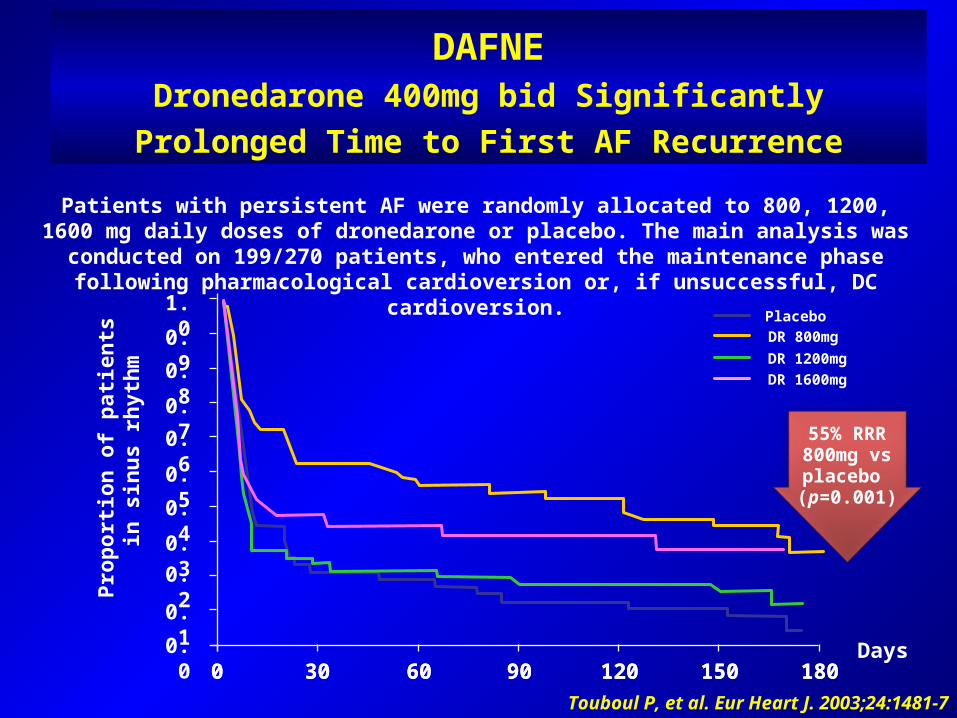
DAFNEDronedarone 400mg bid Significantly
Prolonged Time to First AF Recurrence
Touboul P, et al. Eur Heart J. 2003;24:1481-7.
0 30 60 90 120 150 180Days0.0
0.1
0.20.30.40.50.60.70.80.91.0
Prop
ortio
n of
pat
ient
s in
sin
us rh
ythm
0 30 60 90 120 150 180
PlaceboDR 800mgDR 1200mgDR 1600mg
55% RRR800mg vsplacebo (p=0.001)
Patients with persistent AF were randomly allocated to 800, 1200, 1600 mg daily doses of dronedarone or placebo. The main analysis was conducted on 199/270 patients, who
entered the maintenance phase following pharmacological cardioversion or, if unsuccessful, DC cardioversion.
EURIDIS and ADONISObjective
EURIDIS and ADONIS investigated whether dronedarone is superior to placebo on top of standard therapy* for maintaining sinus rhythm after electrical, pharmacologic, or spontaneous conversion from atrial fibrillation or atrial flutter
Singh BN, et al. N Engl J Med. 2007;357:987-99.
* Standard therapy may have included rate control agents (beta-blockers, and/or Ca-antagonists and/or digoxin) and/or anti-
thrombotic therapy (oral anticoagulation and/or long-term antiplatelet therapy) and/or other cardiovascular therapy such as ACE inhibitors and statins
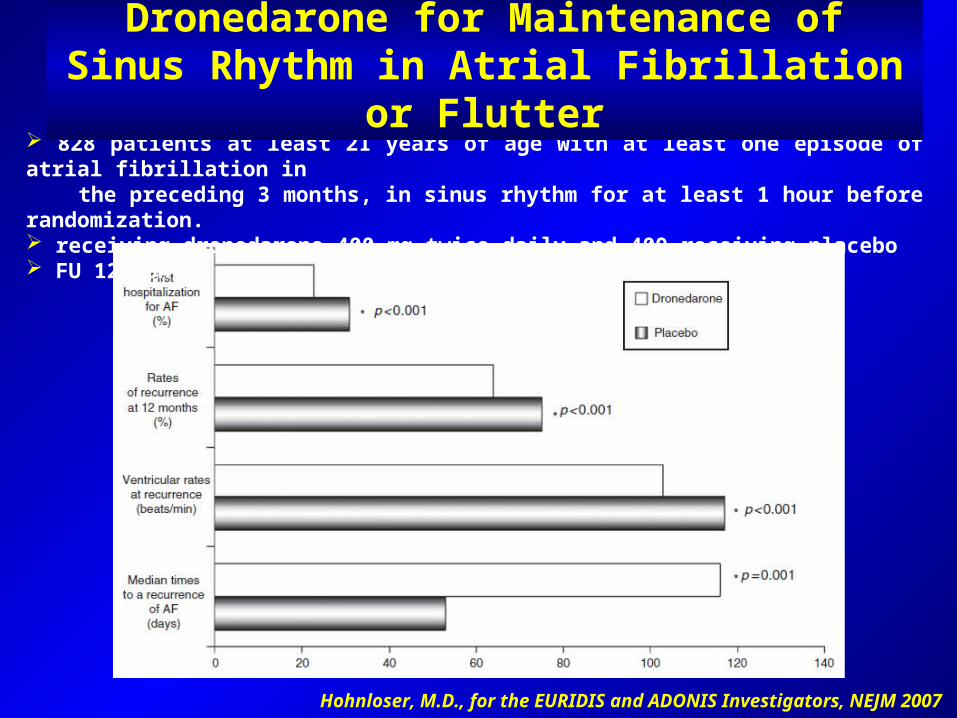
Hohnloser, M.D., for the EURIDIS and ADONIS Investigators, NEJM 2007
828 patients at least 21 years of age with at least one episode of atrial fibrillation in the preceding 3 months, in sinus rhythm for at least 1 hour before randomization. receiving dronedarone 400 mg twice daily and 409 receiving placebo FU 12 months
Dronedarone for Maintenance of Sinus Rhythm in Atrial Fibrillation or Flutter
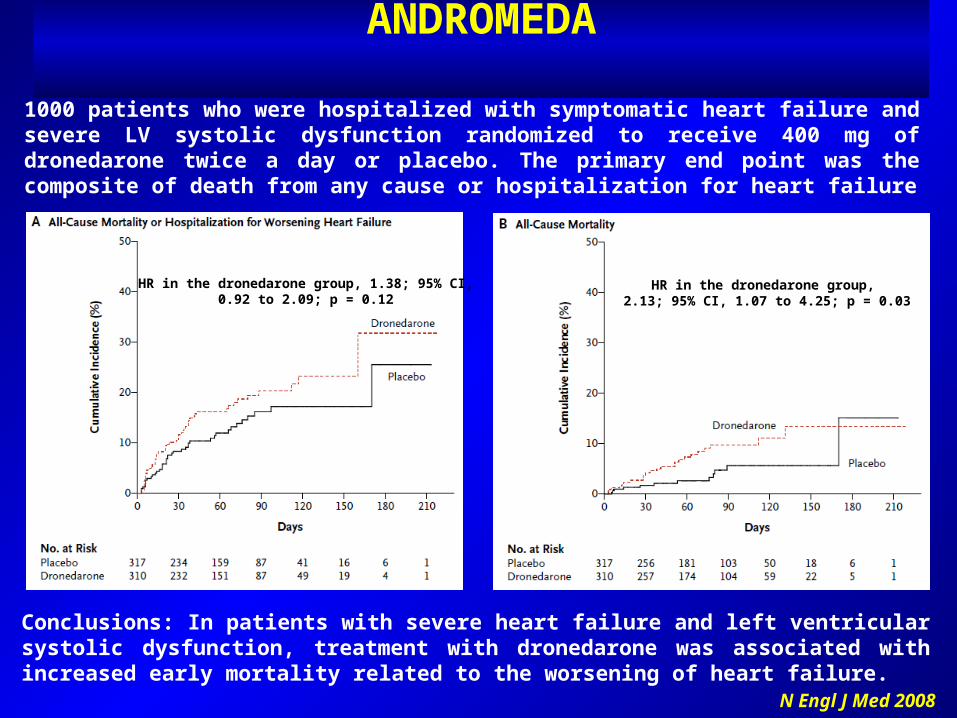
1000 patients who were hospitalized with symptomatic heart failure and severe LV systolic dysfunction randomized to receive 400 mg of dronedarone twice a day or placebo. The primary end point was the composite of death from any cause or hospitalization for heart failure
Conclusions: In patients with severe heart failure and left ventricular systolic dysfunction, treatment with dronedarone was associated with increased early mortality related to the worsening of heart failure.
HR in the dronedarone group, 1.38; 95% CI,0.92 to 2.09; p = 0.12
HR in the dronedarone group, 2.13; 95% CI, 1.07 to 4.25; p = 0.03
N Engl J Med 2008
ANDROMEDA
0
10
20
30
40
Primaryendpoint
Firsthospitalization for CV causes
%
p<0.001
p<0.001
DronedaronePlacebo
p<0.001
p=0.18p=0.03
p=0.01
Firsthospitalization
for AF
Death fromany cause
Death fromCV
causes
Death fromcardiac
arrhythmias
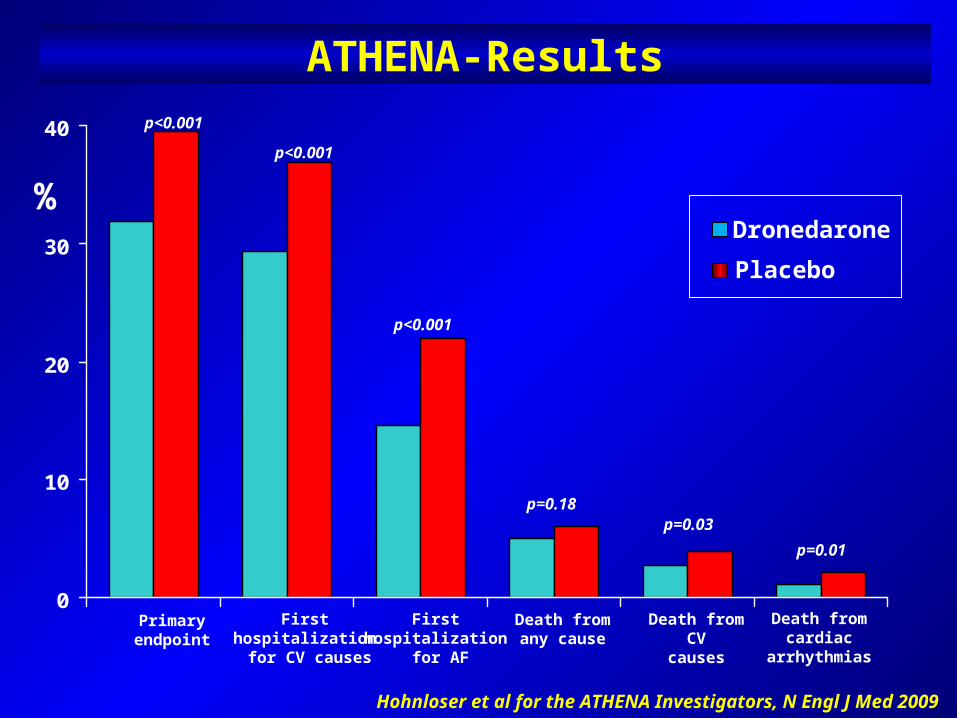
Hohnloser et al for the ATHENA Investigators, N Engl J Med 2009
ATHENA-Results
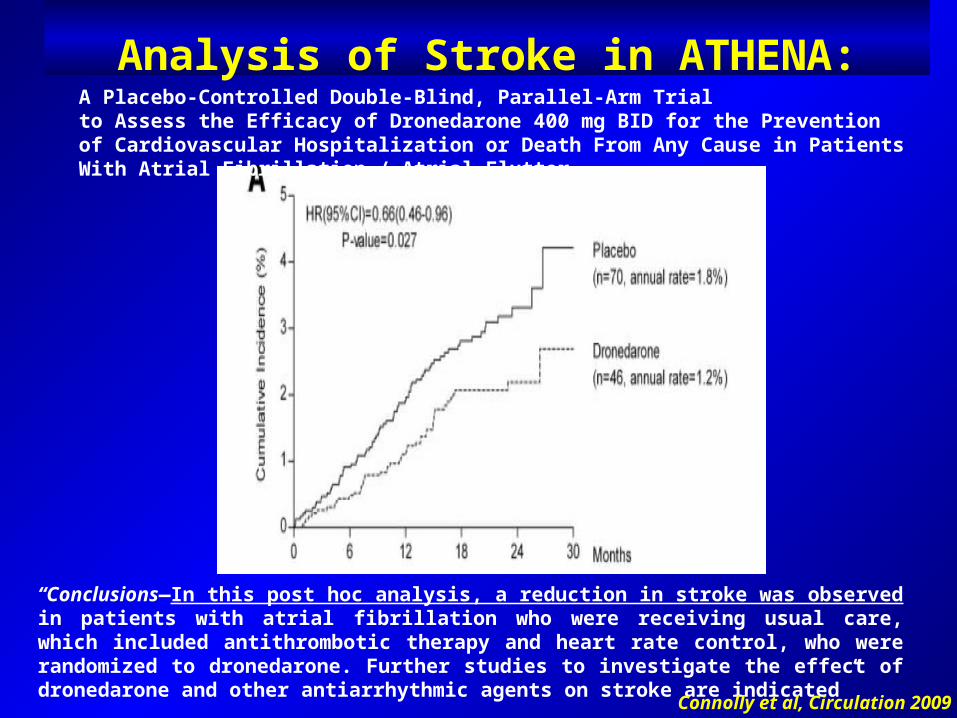
“Conclusions—In this post hoc analysis, a reduction in stroke was observed in patients with atrial fibrillation who were receiving usual care, which included antithrombotic therapy and heart rate control, who were randomized to dronedarone. Further studies to investigate the effect of dronedarone and other antiarrhythmic agents on stroke are indicated” Connolly et al, Circulation 2009
Analysis of Stroke in ATHENA:A Placebo-Controlled Double-Blind, Parallel-Arm Trial to Assess the Efficacy of Dronedarone 400 mg BID for the Prevention of Cardiovascular Hospitalization or Death From Any Cause in Patients With Atrial Fibrillation / Atrial Flutter
Five hundred and four amiodarone-naıve patients were randomized to receive dronedarone 400 mg bid (n = 249) or amiodarone 600 mg qd for 28 days then 200 mg qd (n = 255) for at least 6 months.
Primary composite endpoint was recurrence of AF (including unsuccessful electrical cardioversion, no spontaneous conversion and no electrical cardioversion) or premature study discontinuation.
Main safety endpoint (MSE) was occurrence of thyroid-, hepatic-, pulmonary-, neurologic-, skin-, eye-, or gastrointestinal-specific events, or premature study drug discontinuation following an adverse event.
J Cardiovasc Electrophysiol, Vol. 21, pp. 597-605, June 2010
A Short-Term, Randomized, Double-Blind, Parallel-Group Study to Evaluate the Efficacy and Safety of Dronedarone
versus Amiodarone in Patients with Persistent Atrial Fibrillation:
The DIONYSOS Study
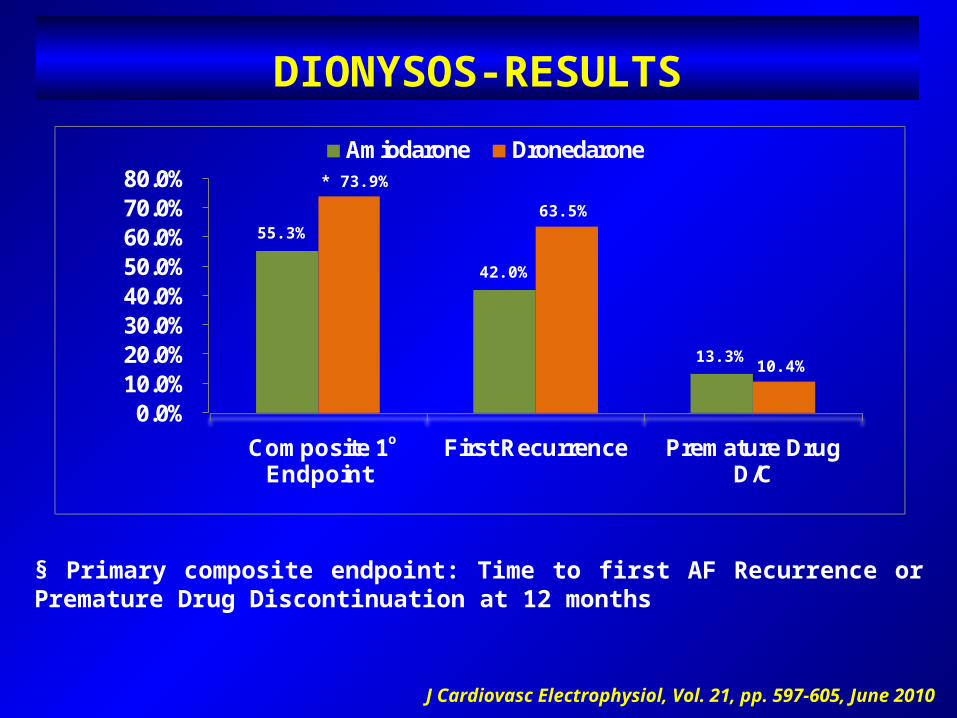
§ Primary composite endpoint: Time to first AF Recurrence or Premature Drug Discontinuation at 12 months
DIONYSOS-RESULTS
J Cardiovasc Electrophysiol, Vol. 21, pp. 597-605, June 2010
0.0%10.0%20.0%30.0%40.0%50.0%60.0%70.0%80.0%
Composite 1 Endpoint
First Recurrence Premature Drug D/C
Amiodarone Dronedarone
55.3%
* 73.9%
42.0%
63.5%
13.3% 10.4%
o
J Cardiovasc Electrophysiol, Vol. 21, pp. 597-605, June 2010
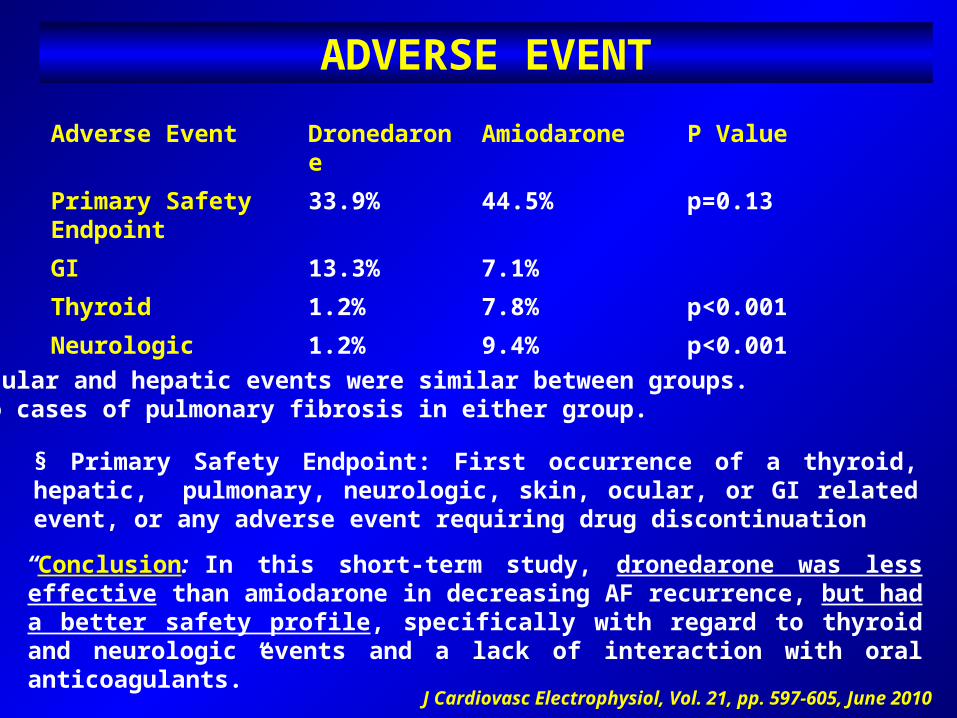
§ Primary Safety Endpoint: First occurrence of a thyroid, hepatic, pulmonary, neurologic, skin, ocular, or GI related event, or any adverse event requiring drug discontinuation
“Conclusion: In this short-term study, dronedarone was less effective than amiodarone in decreasing AF recurrence, but had a better safety profile, specifically with regard to thyroid and neurologic events and a lack of interaction with oral anticoagulants.”
Adverse Event Dronedarone Amiodarone P ValuePrimary SafetyEndpoint
33.9% 44.5% p=0.13
GI 13.3% 7.1%Thyroid 1.2% 7.8% p<0.001Neurologic 1.2% 9.4% p<0.001
Ocular and hepatic events were similar between groups.No cases of pulmonary fibrosis in either group.
ADVERSE EVENT
Piccini et al, J Am Coll Cardiol 2009
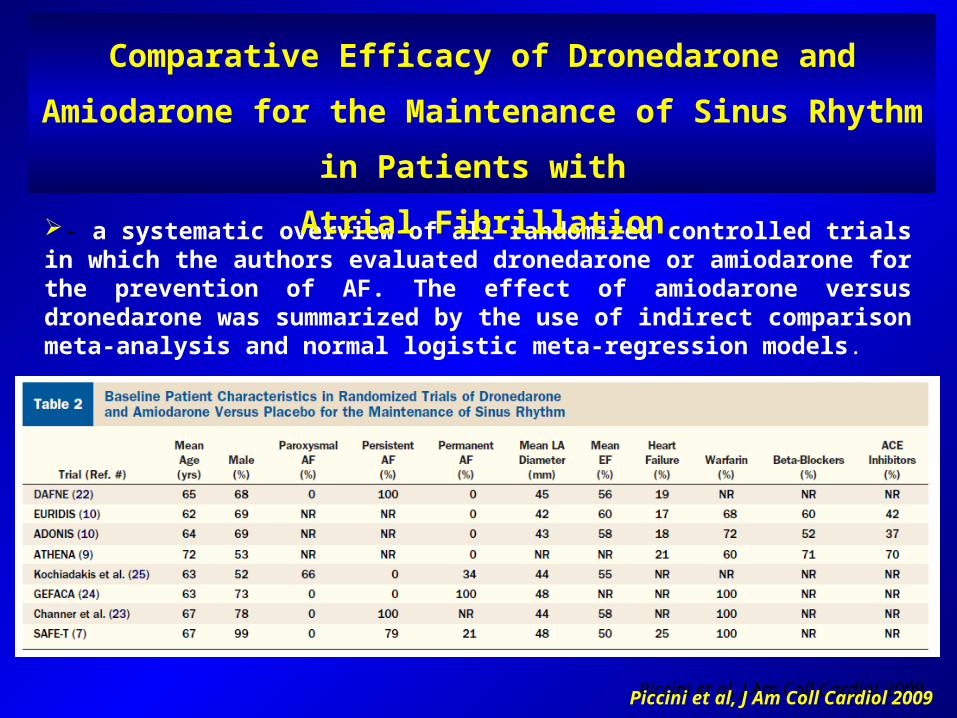
- a systematic overview of all randomized controlled trials in which the authors evaluated dronedarone or amiodarone for the prevention of AF. The effect of amiodarone versus dronedarone was summarized by the use of indirect comparison meta-analysis and normal logistic meta-regression models.
Piccini et al, J Am Coll Cardiol 2009
Comparative Efficacy of Dronedarone and Amiodarone for the Maintenance of Sinus Rhythm in Patients with
Atrial Fibrillation
”…A normal logistic regression model incorporating all trial evidence found amiodarone superior to dronedarone (OR: 0.49; 95% CI: 0.37 to 0.63; p 0.001) for the prevention of recurrent AF. In contrast, these models also found a trend toward greater all-cause mortality (OR: 1.61; 95% CI: 0.97 to 2.68; p 0.066) and greater overall adverse events requiring drug discontinuation with amiodarone versus dronedarone (OR: 1.81; 95% CI: 1.33 to 2.46; p 0.001).
”Conclusion: Dronedarone is less effective than amiodarone for the maintenance of sinus rhythm, but has fewer adverse effects. For every 1,000 patients treated with dronedarone instead of amiodarone, we estimate approximately 228 more recurrences of AF in exchange for 9.6 fewer deaths and 62 fewer adverse events requiring discontinuation of drug.”
Piccini et al, J Am Coll Cardiol 2009
Comparative Efficacy of Dronedarone and Amiodarone for the Maintenance of Sinus Rhythm
in Patients with Atrial Fibrillation
• Indicated to reduce the risk of CV hospitalization in patients with paroxysmal or persistent atrial fibrillation (AF) or atrial flutter (AFL). Dose: 400mg po BID• Patients:
In sinus rhythm or who will be cardioverted Recent episode of AF/AFL CV risk factors
Age > 70yrsHypertensionDiabetesPrior CVALeft Atrial Diameter > 55 mm EF < 40%
Dronedarone: FDA Approval: July 2009
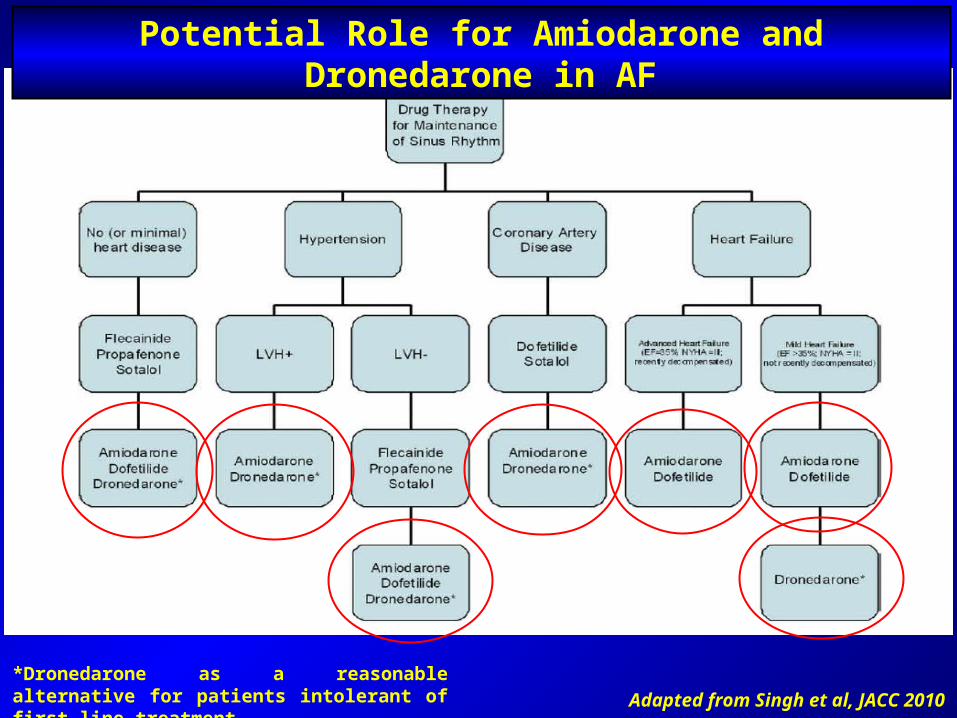
Potential Role for Amiodarone and Dronedarone in AF
*Dronedarone as a reasonable alternative for patients intolerant of first-line treatment. Adapted from Singh et al, JACC 2010
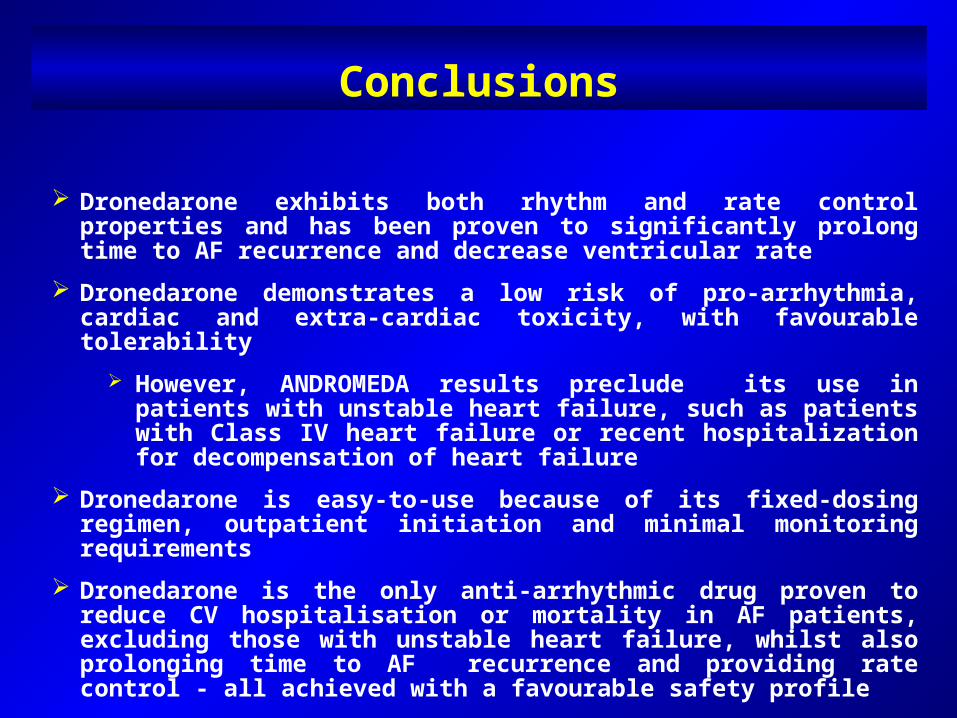
Conclusions
Dronedarone exhibits both rhythm and rate control properties and has been proven to significantly prolong time to AF recurrence and decrease ventricular rate
Dronedarone demonstrates a low risk of pro-arrhythmia, cardiac and extra-cardiac toxicity, with favourable tolerability
However, ANDROMEDA results preclude its use in patients with unstable heart failure, such as patients with Class IV heart failure or recent hospitalization for decompensation of heart failure
Dronedarone is easy-to-use because of its fixed-dosing regimen, outpatient initiation and minimal monitoring requirements
Dronedarone is the only anti-arrhythmic drug proven to reduce CV hospitalisation or mortality in AF patients, excluding those with unstable heart failure, whilst also prolonging time to AF recurrence and providing rate control - all achieved with a favourable safety profile
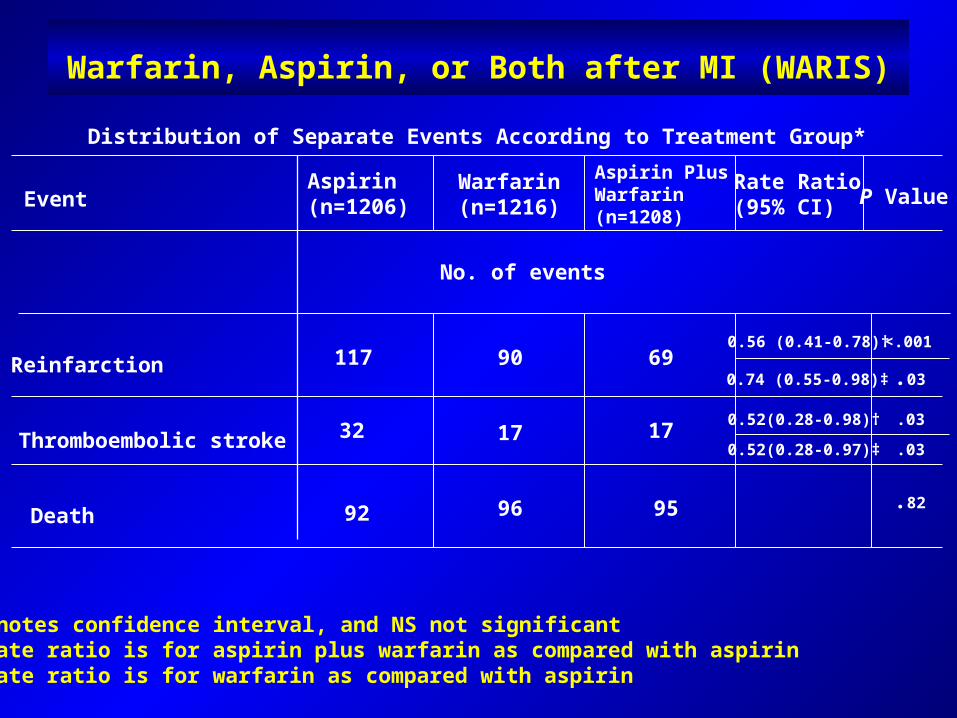
Warfarin, Aspirin, or Both after MI (WARIS)
Distribution of Separate Events According to Treatment Group*
*CI denotes confidence interval, and NS not significant†The rate ratio is for aspirin plus warfarin as compared with aspirin‡The rate ratio is for warfarin as compared with aspirin
Event
Thromboembolic stroke
Death
Reinfarction
No. of events
Aspirin(n=1206)
Aspirin PlusWarfarin(n=1208)
Warfarin(n=1216)
Rate Ratio(95% CI) P Value
17
69
96
17
90117
32
92 95
0.74 (0.55-0.98)‡
0.56 (0.41-0.78)†
0.52(0.28-0.98)†
0.52(0.28-0.97)‡ .03
.82
.03
.03
<.001
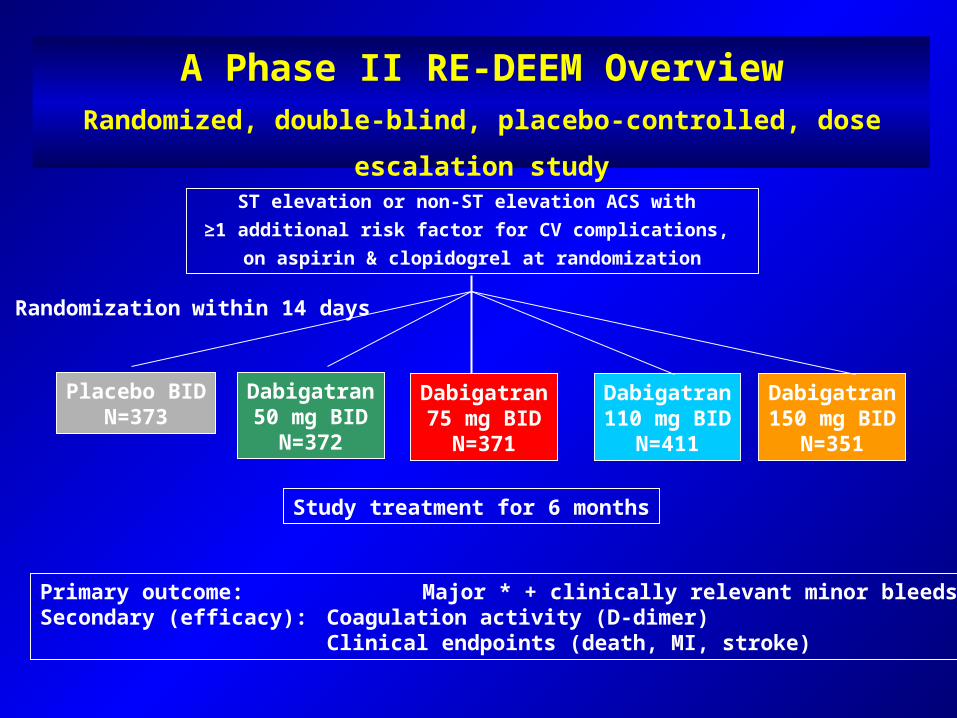
A Phase II RE-DEEM OverviewRandomized, double-blind, placebo-controlled, dose escalation
studyST elevation or non-ST elevation ACS with
≥1 additional risk factor for CV complications, on aspirin & clopidogrel at randomization
Placebo BIDN=373
Dabigatran50 mg BID
N=372
Dabigatran75 mg BID
N=371
Dabigatran110 mg BID
N=411
Dabigatran150 mg BID
N=351
Randomization within 14 days
Study treatment for 6 months
Primary outcome: Major * + clinically relevant minor bleedsSecondary (efficacy): Coagulation activity (D-dimer)
Clinical endpoints (death, MI, stroke)
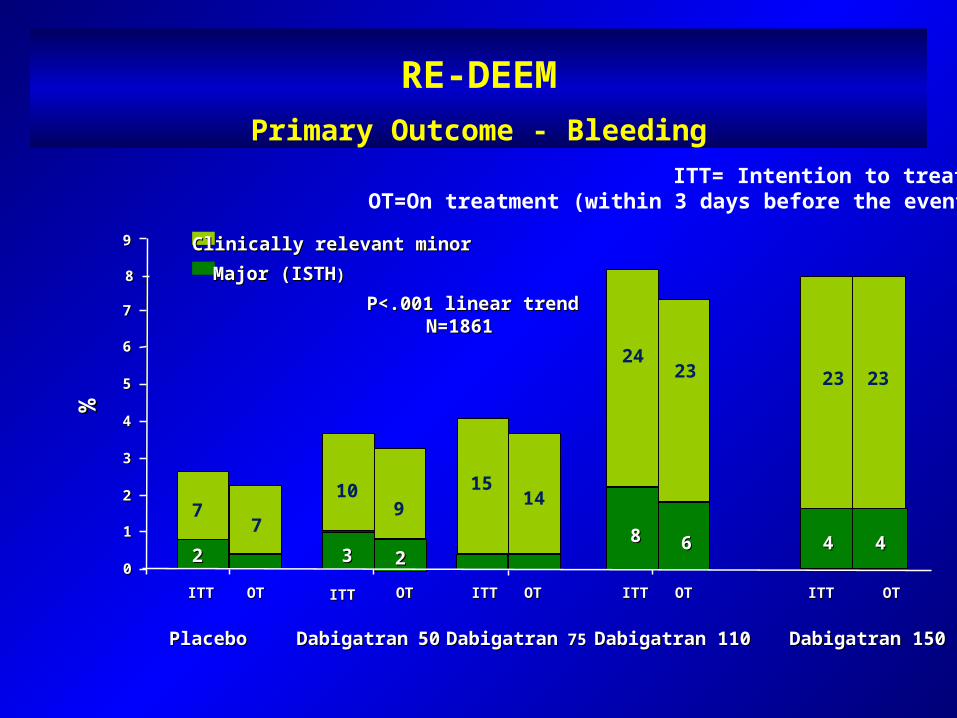
RE-DEEMPrimary Outcome - Bleeding
ITT= Intention to treat;OT=On treatment (within 3 days before the event)
00
11
22
33
44
55
66
77
88
%%
ITTITT OOTT
Clinically relevant minorClinically relevant minor99
Major (ISTHMajor (ISTH))
OOTT
OTOT OOTT
ITTITT ITTITTITTITT
7
P<.001 linear trendP<.001 linear trendN=1861N=1861
Dabigatran 110Dabigatran 110PlaceboPlacebo DabigatranDabigatran 75 75DabigatranDabigatran 5050
722
Dabigatran 150Dabigatran 150
33
OOTT
ITTITT
22
109
23 23
6688
1514
44 44
2324
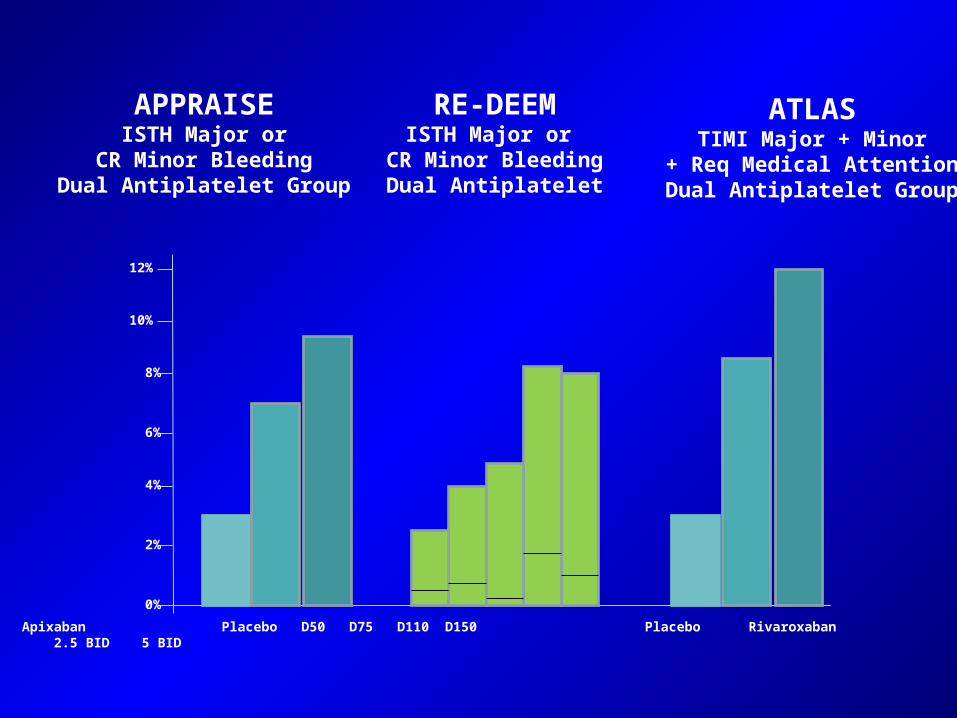
APPRAISEISTH Major or
CR Minor BleedingDual Antiplatelet Group
RE-DEEMISTH Major or
CR Minor BleedingDual Antiplatelet
ATLASTIMI Major + Minor
+ Req Medical AttentionDual Antiplatelet Group
12%
10%
8%
6%
4%
2%
0% Placebo Apixaban Placebo D50 D75 D110 D150 Placebo Rivaroxaban 2.5 BID 5 BID 2.5 BID 5 BID
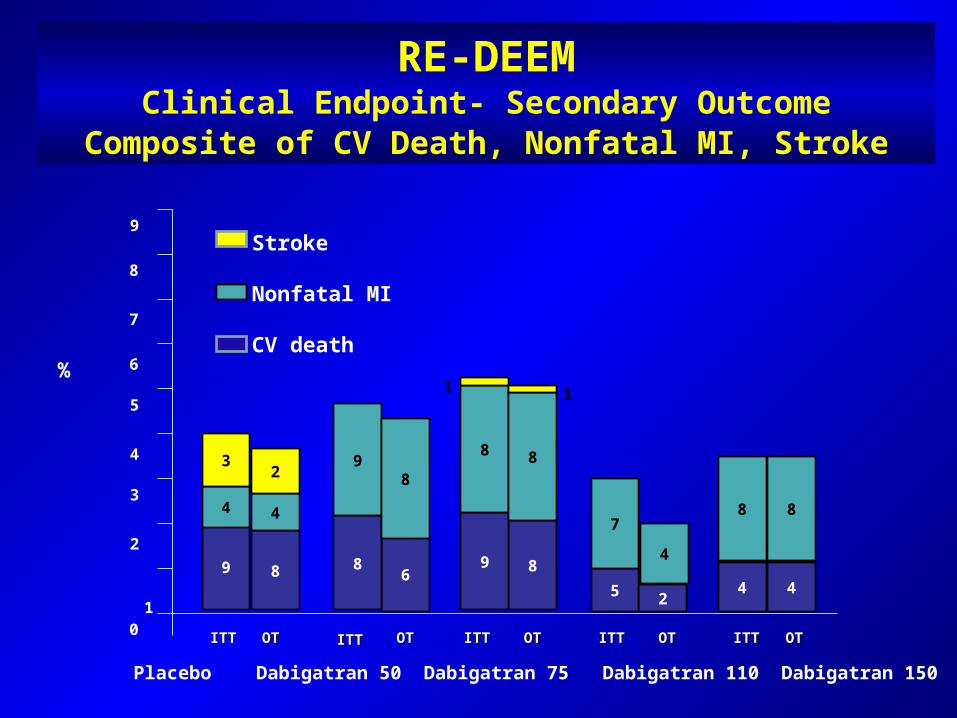
RE-DEEMClinical Endpoint- Secondary Outcome
Composite of CV Death, Nonfatal MI, Stroke
9 6884425
9
5
4
3
2
0
8
7
6
1
89
4
3
4
2 98
8 8
8 87
4
ITTITT OOTT
OOTT
OTOT OOTT
ITTITT ITTITTITTITT OOTT
ITTITT
1 1%
Placebo Dabigatran 50 Dabigatran 75 Dabigatran 110 Dabigatran 150
Stroke
Nonfatal MI
CV death
Consequences of AF
Hospitalizations:Most common arrhythmia requiring hospitalization2-3 risk for hospitalization
Thromboembolism:Stroke: 4.5x riskMicroemboli: reduced cognitive functionProthrombotic state
Reduced QoL:Palpitations, dyspnea, fatigue, exercise tolerance
Mortality:2x risk independent of comorbid CV diseaseSudden death in heart failure and HCM
Impaired Hemodynamics:Loss of atrial kickIrregular ventricular contractionsHeart failureTachycardia-induced cardiomyopathy
Sinus Rhythm Strategy:Who Are Appropriate Candidates?
Highly symptomatic with AFFirst episodeReversible causeYoung ageSymptomatic despite rate controlRate-related cardiomyopathyLV dysfunction / CHFDiastolic dysfunction with symptomsHCM or aortic stenosisPrior embolic stroke or TIA
New Pharmacologic Agents for AF
Multi-ion channel blockers:
DronedaroneBudiodarone
Atrial-selective AADs:
I Kur -, Ito and I KACh - blockerAtrial-selective Na channel blockerHistamine (5-HT4) receptor antagonist
Other ion channel blockersOther mechanismsUpstream therapies:
StatinsACEI / ARBOmega -3 fatty acidsAnti-inflammatory drugs