Page 1 of 35 Diabetes · 2014. 2. 6. · combined with islet autoantigen-specific approaches to...
35
1 Combination therapy with an anti-IL-1β antibody and GAD65 DNA vaccine can reverse recent- onset diabetes in the RIP-GP mouse model Philippe P. Pagni a , Damien Bresson a,b , Teresa Rodriguez-Calvo a , Amira Bel Hani a , Yulia Manenkova a , Natalie Amirian a , Alecia Blaszczak a , Sina Faton a , Sowbarnika Sachithanantham a , Matthias G. von Herrath a, # Affiliations: a Type 1 Diabetes Center, La Jolla Institute for Allergy and Immunology, 9420 Athena Circle, La Jolla, California, United States, 92037. b Current address: Ambrx, Inc. 10975 N Torrey Pines Rd, San Diego, CA 92121. Short running title : Diabetes reversal on IL-1β blockade/GAD65 DNA vaccine. Word count: 3,915 words; 6 figures; 4 online supplementary figures. Abbreviations: GAD65, Glutamic acid decarboxylase of 65kDa; T1D, type 1 diabetes; NOD, nonobese diabetic; LCMV, lymphocytic choriomeningitis virus; RIP-GP, rat insulin promoter- glycoprotein; BGV, blood glucose value; TNF, tumor necrosis factor; IFN-γ, interferon-γ; IL, interleukin; Th, T-helper; PBMC, peripheral blood mononuclear cells; IL-1Ra, interleukin-1 receptor antagonist. #Corresponding author: Type 1 Diabetes Center, La Jolla Institute for Allergy and Immunology, 9420 Athena Circle, La Jolla, California, United States, 92037. Tel: 001-858-205-0646. Fax: 001- 858-752-6993. Email: [email protected] Page 1 of 35 Diabetes Diabetes Publish Ahead of Print, published online February 11, 2014
Transcript of Page 1 of 35 Diabetes · 2014. 2. 6. · combined with islet autoantigen-specific approaches to...

1
Combination therapy with an anti-IL-1β antibody and GAD65 DNA vaccine can reverse recent-
onset diabetes in the RIP-GP mouse model
Philippe P. Pagnia, Damien Bresson
a,b, Teresa Rodriguez-Calvo
a, Amira Bel Hani
a, Yulia
Manenkovaa, Natalie Amirian
a, Alecia Blaszczak
a, Sina Faton
a , Sowbarnika Sachithanantham
a,
Matthias G. von Herratha, #
Affiliations: aType 1 Diabetes Center, La Jolla Institute for Allergy and Immunology, 9420
Athena Circle, La Jolla, California, United States, 92037.
bCurrent address: Ambrx, Inc. 10975 N Torrey Pines Rd, San Diego, CA 92121.
Short running title : Diabetes reversal on IL-1β blockade/GAD65 DNA vaccine.
Word count: 3,915 words; 6 figures; 4 online supplementary figures.
Abbreviations: GAD65, Glutamic acid decarboxylase of 65kDa; T1D, type 1 diabetes; NOD,
nonobese diabetic; LCMV, lymphocytic choriomeningitis virus; RIP-GP, rat insulin promoter-
glycoprotein; BGV, blood glucose value; TNF, tumor necrosis factor; IFN-γ, interferon-γ; IL,
interleukin; Th, T-helper; PBMC, peripheral blood mononuclear cells; IL-1Ra, interleukin-1
receptor antagonist.
#Corresponding author: Type 1 Diabetes Center, La Jolla Institute for Allergy and Immunology,
9420 Athena Circle, La Jolla, California, United States, 92037. Tel: 001-858-205-0646. Fax: 001-
858-752-6993. Email: [email protected]
Page 1 of 35 Diabetes
Diabetes Publish Ahead of Print, published online February 11, 2014

2
Type 1 diabetes is thought to be an autoimmune condition in which self-reactive T cells attack
insulin-secreting pancreatic β-cells. As a proinflammatory cytokine produced by β-cells or
macrophages, interleukin (IL)-1β represents a potential therapeutic target in diabetes. We
reasoned IL-1β blockade could be combined with islet antigen-specific approaches involving
glutamic acid decarboxylase of 65kDa (GAD65)-expressing plasmids, as previously shown in
combination therapies (CT) with anti-CD3. Thus, we investigated whether anti-IL-1β antibody
alone or combined with GAD65 vaccine could reverse diabetes development in a virus-induced
mouse model. Given alone, anti-IL-1β had no effect on diabetes while GAD65 plasmid resulted
in 33% disease reversal after 5-week observation. However, CT cured 53% of animals and
prevented worsening of glycemic control in non-protected individuals for up to 12 weeks. While
the GAD65 vaccine arm of the CT was associated with increased Foxp3+ regulatory T-cell
frequency in pancreatic lymph nodes, islet infiltration by CD11b+/high
cells was less frequent upon
CT and its extent correlated with treatment success or failure. Altogether, our CT provided
prolonged improvement of clinical and immunological features. Despite unsuccessful clinical
trials using anti-IL-1β monotherapy, these data hold promise for treatment of type 1 diabetic
patients with IL-1β blockade combined with antigen-specific vaccines.
200 words.
Keywords
Type 1 diabetes; IL-1β; GAD65 DNA vaccine; Immunotherapy; RIP-LCMV
Page 2 of 35Diabetes

3
INTRODUCTION
Inflammation of the pancreatic islets is observed in patients with type 1 and type 2 diabetes (1-3).
Islets are sensitive to proinflammatory cytokines and the combination of IFN-γ, TNF and IL-1β
can act synergistically to lead to β-cell demise (4-6). IL-1β can be produced by cells such as
monocytes, macrophages, dendritic cells or neurons (1; 7). In β-cells, IL-1β secretion in
conditions of high glucose concentrations can have cytotoxic effects such as altered insulin
secretion and β-cell apoptosis (8-10). Therefore, IL-1β blockade as a means to prevent or reverse
type 1 and type 2 diabetes onset has become a potential therapeutic target.
In type 2 diabetes, neutralization of IL-1β signaling has resulted in improved glycemic control
and insulin secretion in murine (11) and human studies (12-13). Microarray analyses have shown
that compared to healthy controls, IL-1β gene expression was increased 3-fold in peripheral
blood mononuclear cells (PBMCs) from both type 1 and type 2 recent-onset diabetic patients but
significantly declined upon a 4-month course of insulin therapy and adjusted glycemic control
(14). In type 1 diabetic patients, Pfleger et al. found a positive association at 1- and 6-month post-
diagnosis, between levels of C-peptide and that of interleukin-1 receptor antagonist (IL-1Ra), the
natural antagonist to pro-inflammatory cytokines IL-1α/β and the foot-print of earlier IL-1 action
(15). Moreover, short-term neutralization of IL-1β resulted in reduced chemokine receptor
expression on CD11b+ circulating monocytes (16) in people with type 1 diabetes. More recently,
two randomized, placebo-controlled Phase 2a trials both enrolling 69 type 1 diabetic patients
have evaluated whether IL-1 blockade could improve β-cell function in recent-onset type 1
diabetes (17). One used a human monoclonal anti-IL-1β antibody (Canakinumab) whereas the
other used a recombinant human IL-1Ra (Anakinra). Despite no severe safety issues, neither trial
met its primary or secondary endpoints. Thus, despite good scientific rationale, the effect of IL-
Page 3 of 35 Diabetes

4
1β blockade alone in overt type 1 diabetes is, if any, minor and combination with other agents
will be needed. Antigen-specific therapies, due to their lack of inducing systemic side effects, are
preferable to using additional systemic immunosuppressants.
Along these lines, while IL-1 receptor-deficient nonobese diabetic (NOD) mice display slowed
progression to diabetes but normal incidence (18), Ablamunits et al. have recently shown
synergistic reversal of type 1 diabetes after combined anti-IL-1β (using blocking antibody or IL-
1Ra) and anti-CD3 antibody treatments (19). Furthermore, preclinical studies in our laboratory
also demonstrated synergistic reversal of type 1 diabetes using similar anti-CD3 antibody
combined with islet autoantigen-specific approaches to induce and maintain tolerance to β-cell
antigens (20-22). Oral and nasal (pro)insulin were proved efficacious as part of the CT in the
NOD model (20; 21) whereas pCMV-encoded human glutamic acid decarboxylase of 65kDa
(pCMV-hGAD65) DNA plasmid was efficacious in the RIP-LCMV-GP model (22). RIP-LCMV-
GP mice express the glycoprotein (GP) from lymphocytic choriomeningitis virus (LCMV) as a
transgene under the rat insulin promoter (RIP) and turn diabetic within 2 weeks post-LCMV
infection (23). Other plasmid DNA vaccines encoding mouse proinsulin II or GAD65-IgFc and
IL-4 have also been shown to prevent and/or reverse hyperglycemia in NOD mice (24; 25).
Herein, we investigated whether an IL1-β neutralizing antibody alone or combined with an islet
antigen GAD65-specific vaccine could reverse recent-onset diabetes development in the RIP-GP
model. For this, we chose two main time-points for our studies: (i) 5 weeks post-treatment, i.e.,
one week after the last administration of anti-IL-1β antibody, and (ii) 12 weeks post-treatment
i.e., up to 2 months after the treatments have been stopped.
Page 4 of 35Diabetes

5
RESEARCH DESIGN AND METHODS
Mice. Transgenic rat insulin promoter (RIP)-lymphocytic choriomeningitis virus (LCMV)-
glycoprotein (GP) mice on the C57Bl/6 background have been described (26). Mice were bred in-
house under specific pathogen free conditions at the La Jolla Institute for Allergy and
Immunology (LIAI). A dose of 1x104 plaque-forming units of LCMV Armstrong was injected
intraperitoneally. Blood glucose values (BGVs) were recorded with an AccuCheck Glucometer
(LifeScan Inc., Milpitas, CA).
Treatments. From day 7 post-infection, BGV was assessed for all mice and when above
250mg/dl, mice were included in one treatment group. Novartis (Basel, Switzerland) kindly
provided us with a monoclonal anti-mouse IL-1β antibody and its corresponding IgG2a isotype
(anti-cyclosporin B) control antibody. Both kinds of antibodies were administered
intraperitoneally (200µg) similar to Osborn et al. (11), once a week for 4 weeks and GAD65
DNA vaccine was given as described previously in our laboratory (22), i.e., intramuscularly
(100µg per leg) at day 0, 4 and 11 post-onset. At the end of different periods of observation, mice
were sacrificed and blood, spleen, pancreatic lymph nodes (PLNs) as well as pancreata were
collected and processed for analyses (27).
Histology. Mouse pancreata were embedded in optimum cutting temperature compound (VWR)
and stored at -80C. Six-micron-thick sections were stained for insulin and surface markers.
Staining for CD4, CD8 and CD11b was performed using biotinylated primary antibodies (1/100,
BD) followed by the addition of streptavidin coupled-horseradish peroxidase (1/1,000, Vector)
and developed using NovaRed Peroxidase substrate kit (Vector). Sections were simultaneously
stained with guinea pig anti-insulin primary antibody (Dako), followed by staining with goat anti-
guinea pig alkaline phosphatase antibody (Sigma) and developed using Vector Blue AP III
Page 5 of 35 Diabetes

6
(Vector). Sections were mounted with aqueous mounting solution (Lerner Lab.). Pictures were
taken with a Nikon 80i fluorescence microscope. The criteria for scoring islet infiltration were as
follows: (i) no insulitis, (ii) peri-insulitis with no islet destruction or a few (less than 10)
infiltrating cells, and (iii) infiltrating insulitis with extensive islet destruction (or islet destroyed).
The readings were performed in a blinded fashion by three different co-authors, S.F., A.B. and
N.A. at 1, 5 and 12 weeks post-onset, respectively.
Flow cytometry staining. After various periods of observations post-treatment onset, blood,
spleen and PLNs were collected from euthanized mice and processed for further staining as
previously described (27). Db/GP33, and Db/NP396 pentamers were purchased from Proimmune
(Sarasota, FL). Isolated cells were submitted to a Fc block incubation for 10 minutes at +4C,
followed by pentamer staining (3ul per 50ul reaction) at room temperature for at least 20 minutes.
Last, surface antibodies were added and incubated for 20 minutes at 4C. After acquisition of data
on a LSRII cytometer (Beckton Dickinson), events were analyzed with FlowJo software (Tree
Star), gating on Aqua live/dead dye (Life Tech) negative cells as well as CD19-CD8
+ T cells.
Statistics. Data are expressed as mean ± standard error of the mean. Diabetes incidences were
assessed using the Gehan-Breslow and Log-rank tests. Graphs were plotted and statistics
calculated with GraphPad Prism® (versions 4 and 5). Comparisons between the different groups
were performed with two-tailed, unpaired Mann-Whitneytests. A 2-way ANOVA test was used
for hisotological data analyses. The Wilcoxon signed rank test was used to determine statistical
significance for paired values. *P < 0.05, **P < 0.01, ***P < 0.001.
Ethics. These studies were performed at LIAI upon approval of Institutional Animal Care and
Use Committee.
Page 6 of 35Diabetes

7
RESULTS
Anti-IL1β/GAD65 DNA vaccine combination, but not anti-IL1β treatment alone, can
reverse hyperglycemia in diabetic RIP-GP mice. To determine the efficacy of IL-1β
neutralization as a monotherapy in the RIP-LCMV-GP diabetes model, we treated diabetic mice
once weekly for 4 weeks with an anti-IL-1β antibody or an isotype control. After 5 weeks, all
isotype-treated animals remained hyperglycemic whereas 16.7% (1/6) of anti-IL-1β-treated mice
reverted to euglycemia (Fig. 1A left panels, 1B). This difference did not reach statistical
significance, suggesting that monotherapy based upon IL-1β blockade was inefficacious in the
rapid-onset RIP-GP mouse model, paralleling the recent clinical trial experience (17).
Previous studies by our laboratory had shown success in curing diabetic RIP-GP mice combining
anti-CD3 and pCMV-GAD65 DNA vaccines (22). Thus, we questioned whether the same DNA
vaccine could be associated with IL-1β blocking antibody to induce immunological tolerance to
GAD65. In accordance with Bresson et al. (22) and reflecting the initial success of DNA vaccines
in preserving β-cell mass in a trial in recent-onset diabetes (28), 33% (4/12) of mice treated with
GAD65 DNA plasmid and isotype antibody (below referred to as the isot/GAD group) reverted
to euglycemia after 5 weeks, providing some limited protection compared to isotype-treated
counterparts. However, when using a combination therapy (CT) with both the GAD65 DNA
vaccine and anti-IL-1β antibody (also referred to as the a-IL-1β/GAD group), we found a
significantly higher proportion of cured mice (9/17, 53%) (Fig. 1A right panels, 1B). In addition,
we observed a significantly faster reversal in the a-IL-1β/GAD group compared to the isot/GAD
group (Fig. 1C), as reflected by the Gehan-Breslow statistical test that gives more weight to
earlier events (Fig. 1B).
Page 7 of 35 Diabetes

8
Overall, the average glycemia levels at entry were comparable among all groups, therefore
excluding a bias in this regard (supplementary Fig. 1B). Moreover, the combination of anti-IL-
1β antibody with either empty pCMV plasmid or pCMV expressing the B chain of insulin
resulted in reversal rates similar to anti-IL-1β-treated mice (supplementary Fig. 1C), excluding
non-specific effects as observed previously (20-21) and indicating MHC restriction of GAD65-
based induction of tolerance. Supporting the point that antigenic vaccines will operate in an
MHC-restricted manner, earlier studies have shown that DNA vaccines expressing proinsulin but
not GAD65 can protect NOD and Balb/c, but not B6, mice from diabetes due to differences in
insulin B chain presentation on the H-2b background (20; 22; 29).
Anti-IL1β/GAD65 DNA vaccine combination prevents worsening of glycemic control in
non-protected mice. Glycemic control is evaluated in diabetic individuals by measuring the
percentage of glycated haemoglobin (% HbA1c). Importantly, uncontrolled, severe,
hyperglycemia (HG) steeply increases the risk to develop complications such as retinopathy or
neuropathy (30). Moreover, there is evidence for decreased responsiveness to anti-CD3-induced
decline in C-peptide after 2 years in type 1 diabetic patients with poorly controlled glycemia
(Protégé Trial) (31). Therefore, we examined closely the glycemic status of non-protected mice,
distinguishsing mice with mild and severe hyperglycemia, i.e., with final BGVs comprised
between 251-400mg/dl and 401-600mg/dl, respectively. The isot/GAD and CT groups both
presented 8 non-protected mice, out of which 12.5% (1/8) versus 75% (6/8) mice had mild
hyperglycemia, respectively (Fig. 1D, 1E). These data demonstrate that in cases where IL-1β
blockade as an add-on to GAD65-based tolerance induction does not cure mice from diabetes, it
can nevertheless stabilizethe extent of hyperglycemia in RIP-GP mice.
Page 8 of 35Diabetes

9
Effector CD8 T-cell responses are reduced and regulatory T-cell responses are improved
after GAD65 DNA vaccine and combination therapy. Next, we assessed immunological
parameters systemically (in the spleen) and locally (in PLNs) in mice. Cells were isolated and
restimulated with LCMV immunodominant CD8 T-cell epitope, GP33-41 peptide, in order to
evaluate cytokine production. No significant difference was observed between isotype- and anti-
IL-1β-treated animals, consistent with the absence of efficacy of IL-1β monotherapy (Fig. 2A,
2B). In comparison to isotype antibody treatment, the isot/GAD group presented diminished
frequencies of IFN-γ and TNF-secreting cells in the spleen (Fig. 2A), but not in PLNs (Fig. 2B).
Likewise, compared to anti-IL-1β treatment, we observed reduced fractions of cytokine-secreting
cells in the spleen of the CT group (Fig. 2A), and also in PLNs regarding TNF (Fig. 2B).
The effect of IL-1β on the development and/or function of Foxp3-expressing regulatory T cells
(Tregs) is not completely understood. Indeed, while some argued for a role of IL-1β in breaking
immunological tolerance via expansion of CD25+ effector T cells (32) and in differentiating Th17
cells at the expense of Tregs (33), others argued for a costimulatory effect of IL-1β on the
expansion of Tregs and their maintenance of Foxp3 expression (34; 35). Here, the frequencies of
CD4+CD25
+Foxp3
+ Tregs were comparable between isotype- and anti-IL-1β-treated animals in
the spleen and PLNs (Fig. 2C, D). Of note, the CT group displayed a higher percentage of
Foxp3-expressing Tregs in PLNs (Fig. 2D), but not in the spleen (Fig. 2C). Interestingly, effector
(Fig. 2A, B) and regulatory (Fig. 2C, D) T-cell responses were similar upon GAD65 plasmid
treatment with or without anti-IL-1β antibody. This indicates that the beneficial neutralization of
IL-1β in the CT does not act through the inhibition of cytokine production by GP33-specific
(‘autoreactive’ in the RIP-LCMV model) CD8 T cells nor increased Foxp3+ Treg fractions.
Page 9 of 35 Diabetes

10
Anti-IL1β/GAD65 DNA combination therapy can reverse hyperglycemia up to 8 weeks
after the treatment has been stopped. From a translational point of view, one important issue is
to know whether the benefitial effect provided by the CT is durable on extended periods of time,
notably several weeks after the treatment has been stopped. Thus, we followed BGVs in mice up
to 12 weeks post-onset, i.e., up to 8 weeks after the last antibody administration. Given our data
at 5 weeks post-onset, monotherapies with anti-IL-1β or isotype antibody alone were not tested
here. We observed a higher frequency of mice cured by the CT (6/14, 43%) than by the isot/GAD
treatment (2/11, 18%). This difference was not significant by Log-rank test analysis (p=0.059)
(Fig. 3A, supplementary Fig. 1E) but mean BGVs in CT-treated mice were significantly lower
than that in their isot/GAD-treated counterparts (p<0.001) (Fig. 3B). Then, we performed
analyses on non-protected mice and found that CT reduced the frequencies of mice with severe
hyperglycemia at the end of the study (Fig. 3C), reminiscent of our findings at 5 weeks post-
onset. Likewise, 75% (6/8) of mice that were not cured by the CT at 12 weeks post-onset
nonetheless maintained glycemia levels comparable to those measured at entry (Fig. 3D). In
isot/GAD-treated mice, this proportion was lower (33%, 3/9) and BGVs at euthanasia were
significantly higher than at entry (Fig. 3D). Finally, we assessed how many non-protected mice
presented one or several episodes of transient reversal to euglycemia, defined by one BGV
reading lower than 250mg/dl during the course of our observation. Compared to the isot/GAD
group, CT induced transient reversal to euglycemia more frequently (6/8, 75% versus 3/9, 33%)
and more durably (4.16 versus 1.67 weeks in average, p=0.049) (Fig. 3E).
Page 10 of 35Diabetes

11
Effector CD8 and CD4 T-cell responses at 12 weeks post-onset are largely unaffected by the
CT in spleen, PLNs and blood. In the perspective of unveiling potential immune biomarkers
that would be relevant for human clinical trials, the assessment of the presence of CD8 T cells
specific for islet antigens via multimer (e.g., Quantum-dot) flow cytometry staining has gained
importance, is now technically achievable and could thus be considered as possible secondary
end-point in the future (28; 36; 37). Here, we took advantage of the RIP-GP model to monitor
frequencies of CD8 T cells specific for LCMV GP33-41 (Fig. 4A) and NP396-404 (Fig. 4B) epitopes
via pentamer staining in the blood, as this is the main accessible compartment in human patients.
Our results after 12-week follow up did not reveal any differences in terms of LCMV-specific
CD8 T-cell frequencies for either epitope in the blood (Fig. 4) or spleen (supplementary Fig. 2).
Furthermore, intracellular cytokine staining in CT-treated animals showed decreased frequencies
of GP33-41-specific CD8 effector T cells producing TNF in PLNs (Fig. 4B, left panels). However,
this effect was limited as this was not observed regarding IFN-γ (Fig. 4B, right panels) nor was
it observed in the spleen. Effector and regulatory CD4 T-cell responses in the spleen and PLNs of
isot/GAD- and CT-treated mice were also comparable (supplementary Fig. 3). Altogether, these
results suggest that some, but not all, CD8 and CD4 T-cell responses in the spleen and PLNs are
consitent with the improved mean glycemia levels and diabetes incidence in CT-treated mice.
Islet infiltration by CD8+ and CD11b
+ cells is reduced after CT at 5 and/or 12 weeks post-
onset. Immune cell infiltrates in the pancreas of RIP-LCMV mice contain (CD4 and CD8) T cells
as well as innate immune cells such as CD11b+ macrophages and CD11c
+ dendritic cells. It is
noteworthy that diabetes onset is preceded by an early MHC class II upregulation and infiltration
of macrophages in mouse islets (38) while macrophages also count among the different
Page 11 of 35 Diabetes

12
inflammatory cell infiltrates in human type 1 diabetic patients (39). Thus, we assessed the extent
of overall insulitis and islet infiltration by CD11b+ cells (presumably macrophages) together with
CD4+ and CD8
+ T cells. We found that in accordance with diabetes incidence curves at 5-week
follow up, anti-IL-1β/GAD-treated animals presented significantly reduced insulitis compared to
isot/GAD- and anti-IL-1β-treated groups (supplementary Fig. 1D). In isot/GAD- and CT-treated
groups, we found that overall CD4+ and CD8
+ cell infiltration was similar at 1 and 5 weeks post-
treatment onset (Fig. 5A, middle and lower panels). However, mice treated with anti-
IL1β/GAD65 DNA vaccine displayed less severe infiltration by CD11b+ cells compared to
isot/GAD65-treated mice at 1, 5 and 12 weeks post-treatment onset (Fig. 5A, upper panels). In
accordance with histological data, flow cytometry data (Fig. 5B) revealed that islet CD8+
and
CD11bhigh
cells were decreased upon CT compared to isot/GAD treatment, although this was not
statistically significant for CD11bhigh
cells (p=0.052) but may be explained by the stringency of
our gating strategy (Fig. 5B, upper panel).
The extent of islet infiltration by CD11bhigh
but not T cells correlates with efficacy of the
CT. We then assessed the extent of different immune cell infiltrations distinguishing mice that
were, or failed to be, cured by their respective treatment. Doing so, we found that CT-treated
mice that reverted to euglycemia presented a significantly lower fraction of islet CD11bhigh
cells
than mice that were also treated with the CT but stayed hyperglycemic (Fig. 6A). Of note, this
dichotomy was not observed in the case of isot/GAD treatment, suggesting that this phenotype
was likely due to the IL-1β blockade component of the CT. Moreover, we assessed on a per-
mouse basis the correlation between pancreas-derived CD11bhigh
macrophage infiltration in
relation to mouse glycemia. In accordance with our findings in Figure 6A, the positive linear
Page 12 of 35Diabetes

13
relationship between these two parameters was strong (Pearson r=+0.78) and significant (p=0.01)
in the CT group, but not in the isot/GAD group (Pearson r=+0.27; p=0.55) (Fig. 6B). In contrast,
no significant association was found when correlating mouse glycemia to pancreas infiltration by
CD8 T cells (Fig. 6C, D), CD4 T cells (data not shown) or Foxp3+ Tregs (Fig. 6E, F). We
conclude that on a per-mouse basis, the extent of islet infiltration specifically by CD11bhigh
macrophages, but not T cells, might serve as a biological marker for success or failure of the anti-
IL-1β/GAD65 CT.
Page 13 of 35 Diabetes

14
DISCUSSION
In accordance with the minor effect of IL-1R deficiency on diabetes development in the RIP-
LCMV and NOD models (18; 40), our present results showed no protective effect of anti-IL-1β
therapy alone. This lack of efficacy is in line with the negative outcome of two recently published
placebo-controlled Phase IIa trials in recent-onset type 1 diabetes patients (17). Similarly to a
recently published trial using DNA vaccines (28), we found that GAD65 plasmid alone provided
some efficacy, albeit limited. Thus, the enhanced effect of the CT indicates utility of anti-IL-1β
antibody as an induction agent rather than a monotherapy.
In human trials, it appeared that higher C-peptide levels at study enrollment, reflective of better
preserved β-cell function, was associated with increased responsiveness to drugs such as anti-
CD3 (31; 41). Following the same reasoning, we stratified glycemia levels at treatment onset and
found that CT induced disease reversal in more than half of the treated mice if glycemia at
enrollment was comprised between 250-400mg/dl (Fig. 1, 3) but not any more if above 400mg/dl
(supplementary Fig. 1A). This suggests that a minimal residual β-cell mass is necessary for
protection. Subsequently, we closely analyzed the clinical outcome of non-protected mice,
creating subsets with mild (BGV 251-400mg/dl) versus severe (BGV 401-600mg/dl)
hyperglycemia. This refined analysis allowed us to discover that the CT maintained BGVs to a
milder HG status compared to the isot/GAD group. It is noteworthy that maintenance of glycemic
control was not observed upon monotherapy with anti-IL-1β antibody alone (Fig. 1A). We
showed that compared to anti-IL-1β-treated mice, CT acted by increasing Treg frequencies in
PLNs (Fig. 2). However, in comparison to GAD65 DNA treatment alone, CT did not further
increase Treg fractions. We cannot exclude however, that the Treg pool presented better
regulatory properties or a higher fraction of cells with specificity to GAD65. Of note, we have
Page 14 of 35Diabetes

15
previsouly shown that when given with anti-CD3, the same pCMV-hGAD65 DNA plasmid
promoted the expansion of T cells specific for the C-terminal domain of the GAD65 protein (22).
Consistent with this, we also observed a similar reactivity to this domain upon treatment of RIP-
GP mice with Alum-formulated GAD65 protein (27). Depending on the context, regulatory cells
displayed an IL-10 producing or Th2-biased, IL-5-secreting phenotype. Here, we analyzed by
ELISpot whether protection induced by the CT could be associated with increased
immunomodulatory cytokines levels (IL-10, TGF-β or IL-4), whose elevation can be protective
in animal models of diabetes (42-44). However, we did not detect significant differences in the
spleen (supplementary Fig. 3C) or PLNs (supplementary Fig. 3D).
Upon treatment with anti-IL-1β/anti-CD3, Ablamunits et al. have observed an augmentation in
splenic M2-type CD11b+ and CD11c
+ cells with increased arginase-1, and decreased nitric oxide,
production (19). In our case, fewer CD11bhigh
cells were observed in the pancreas of CT-treated
mice but further phenotypic characterization of these cells will be warranted. Since myeloid
dendritic cells can also under some circumstances express the CD11b integrin marker, the exact
nature of these CD11bhigh
(presumably) macrophages needs to be defined. Sanda et al. have
shown that short-term neutralization of IL-1β in type 1 diabetic patients resulted in a decrease of
CD11b expression on monocytes isolated from PBMCs, which is consistent with our
observations (16). Although the phenotype of CD11bhigh
cells present in anti-IL-1β/GAD65-
treated mice is still unclear, our data rather argue for a diminished cell infiltration degree.
We found a significant correlation between mouse glycemia and the extent of islet infiltration by
CD11bhigh
cells, but not T-cell populations (Fig. 6). We believe such findings could be of
importance in regard to establishing biomarkers tailored for a given treatment. In addition to
simultaneous correlations between an individual’s glycemic status and a defined immune marker,
Page 15 of 35 Diabetes

16
predictive correlations will yield a major advantage in that these would allow to predict
responsiveness to (a) tested drug(s) either before enrollment or early post-treatment. Because of
the inaccessibility of the target organ in type 1 diabetic patients, it will be invaluable to identify
biomarkers that can be measured in the peripheral blood. In our case, although the mechanism(s)
underlying such an impaired recruitment/infiltration of CD11b+/high
and CD8+ cells to the target
organ are unclear, it will be interesting to track the behavior of those cells at, or early after, onset
in PBMCs. Preliminary data 4 days post-treatment onset in the blood tend to exclude a role for
CXCR3 or costimulatory molecule CD40, CD80 and CD86 expression on CD11bhigh
cells
(supplementary Fig. 4).
Four recent Phase II/III clinical trials, two aiming at IL-1β blockade (17) and two promoting
induction of tolerance to GAD65 (45; 46) have failed to meet their primary endpoints. In all
cases, later studies in mouse models indicated that there would be no effect (19; 27). We have
shown here that compared to isot/GAD-treated mice, CT increased the frequency of diabetes
reversal albeit more modestly than other CTs involving synergistic effects of anti-CD3 treatments
(19-22). Additionally however, most of non-protected mice still maintained comparable glycemic
levels compared to baseline, suggesting a subtle but discernable effect of the IL-1β blockade arm
of the CT. Altogether, this suggests that two such therapies that target IL-1β blockade and
tolerance induction to GAD65, yielding sub-optimal outcome when given separately, might be
promising candidates for combination in future human trials. We believe that such trials could
begin soon, since it has been established that DNA vaccines encoding islet antigens such as
proinsulin, can preserve C-peptide secretion and are well tolerated by type 1 diabetic patients
(28).
Page 16 of 35Diabetes

17
ACKNOWLEDGEMENTS
P.P.P., D.B. and M.G.v.H. designed study. P.P.P. and M.G.v.H. are the guarantors of this work
and, as such, had full access to all the data in the study and take responsibility for the integrity of
the data and the accuracy of the data analysis. P.P.P., A.B.H., Y.M., N.A., A.B., T.R.C, S.S. and
S.F. researched data. P.P.P. and M.G.v.H. wrote the manuscript. D.B. generated the
pCMV/hGAD65, contributed to discussion and reviewed/edited manuscript.
The authors are thankful to Priscilla Colby and Malina McClure from the von Herrath lab for the
administrative and mouse work, respectively. We thank Carmen Baca Jones, Sowbarnika
Sachithanantham and Jackie Miller from the von Herrath lab for the preparation of LCMV
Armstrong stocks. We also thank Ambima Buzhyason from the von Herrath lab for his technical
help. We are thankful to Dr. Hermann Gram (Novartis, Basel, Switzerland) for kindly providing
us with anti-IL-1β and isotype (anti-cyclosporin B) monoclonal antibodies.
Preliminary results from this manuscript were presented at the American Diabetes Association’s
71st Scientific Sessions in 2011 in San Diego (Abstract Number: 331-OR).
P.P.P. received funding from the American Diabetes Association (Mentor-Based Postdoctoral
Fellowship 7-09-MN-54) and The Philippe Foundation, Inc. D.B. was the recipient of a funding
from the Juvenile Diabetes Research Foundation (Grant 36-2008-921). This work was funded by
U prevention center grant (U01 DK078013-05S1). The funding sources had no involvement in
the study design, interpretation of data, or decision to submit the article for publication.
All authors declare no conflict of interest.
Page 17 of 35 Diabetes

18
FIGURE LEGENDS
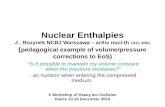
Figure 1: Anti-IL1β/GAD65 DNA combination, but not anti-IL1β treatment alone, can
reverse hyperglycemia in recent-onset diabetic RIP-GP mice. (A) Individual blood glucose
values (BGV) in mg/dl in groups of recent-onset diabetic mice upon different treatments: isotype
antibody (open circles), anti-IL-1β antibody (open squares), isotype antibody plus GAD65 DNA
vaccine (closed circles) or anti-IL-1β antibody plus GAD65 DNA vaccine (closed squares).
Dashed horizontal lines represent threshold for enrollment (250mg/dl). (B) Cumulative diabetes
incidence after 5-week follow up in mice enrolled with BGV between 250-400mg/dl.
Significance from Gehan-Breslow test, which gives more weight to early reversals, is depicted in
grey on the graph whereas that of Log-rank test is depicted in black. (C) Time to reversal to
normoglycemia. Only one mouse reverted in the anti-IL-1β treated group and was not depicted.
Mean ± SEM is represented. (D) Fractions of mice 5 weeks post-treatment that were cured (Final
BGV < 250mg/dl, white), mildly hyperglycemic (HG) (Final BGV 251-400mg/dl, grey) and
severely HG (Final BGV > 401mg/dl, black). (E) BGV at, and 5 weeks after, treatment onset in
those mice that were not cured by their respective treatment. The Wilcoxon signed rank test was
used to determine statistical significance for paired values. Data pooled from seven independent
experiments are shown. *p<0.05. **p<0.01.
Figure 2: Effector CD8 T-cell responses are reduced and regulatory T-cell responses are
improved after GAD65 DNA vaccine and combination therapy. (A, B) Frequencies of IFN-γ-
and TNF-producing GP33-41-specific CD8+ effector T cells in spleen (A) and PLNs (B) of treated
mice. After 5-week treatment, spleens and PLNs were mashed onto 70µm cell strainers to obtain
single-cell suspensions. Cells were then plated in round bottom 96-well plates and left
Page 18 of 35Diabetes

19
unstimulated, or stimulated for 4 to 5 hours with 5µg/ml (CD8 T-cell specific) GP33 peptide in
the presence of brefeldin A (10µg/ml). Cells were then stained in surface with fluorochrome-
coupled CD8 antibodies, fixed, permeabilized and stained with fluorochrome-coupled IFN-γ and
TNF antibodies. Data are expressed as % of gated CD8+ cells. (C, D) Frequencies of Foxp3-
expressing CD4+CD25
+ T regulatory cells in spleen (C) and PLNs (D) of treated mice. In parallel
to the intracellular cytokine staining, cells were stained for CD4, CD25 and intracellular Foxp3.
Data are expressed as % of gated CD25+Foxp3
+ within CD4+ cells. Results from 2-3 pooled
experiments with 2-3 mice per group are shown. *p<0.05.
Figure 3: Anti-IL1β/GAD65 DNA combination therapy can reverse hyperglycemia until 8
weeks after the treatment has been stopped. (A) Individual blood glucose values (BGV) in
mg/dl in groups of recent-onset diabetic mice upon different treatments: isotype antibody plus
GAD65 DNA vaccine (closed circles) or anti-IL-1β antibody plus GAD65 DNA vaccine (closed
squares). (B) Mean BGV in mice depicted in (A). Mean ± SEM is represented. Data pooled from
four independent experiments are shown. ***p<0.0001 (2-tailed paired t-test). (C) Fractions of
mice 12 weeks post-treatment that were cured (Final BGV < 250mg/dl, white), mildly
hyperglycemic (HG) (Final BGV 251-400mg/dl, grey) and severely HG (Final BGV > 401mg/dl,
black). (D) BGV at, and 12 weeks after, treatment onset in those mice that were not cured by
their respective treatment. The Wilcoxon signed rank test was used to determine statistical
significance for paired values. Data pooled from five independent experiments are shown.
*p<0.05. (E) Duration assessment of transient disease reversal observed in those mice that were
not cured by isot/GAD treatment (3/9, 33%) and CT (6/8, 75%). *p<0.05.
�
Page 19 of 35 Diabetes

20
Figure 4: Effector CD8 and CD4 T-cell responses at 12 weeks post-onset are largely
unaffected by the CT in spleen, PLNs and blood. (A) Left panel, frequencies of gp33/Db
pentamer-positive CD8 T cells in the blood of treated mice. Right panel, representative FACS
plots depicting frequencies of np396/Db pentamer-positive CD8 T cells in the blood of treated
mice. Cells were pre-gated on Live/dead Aqua-negative, and CD8+CD19
- cells. (B) Frequencies
of TNF-producing GP33-41-specific CD8+ effector T cells in spleen (upper left panel) and PLNs
(lower left panel) of treated mice after 12 weeks of observation, as well as representative FACS
plots for frequencies of IFN-γ-producing cells (right panels). Data are expressed as % of gated
CD8+ cells. Results from 2 pooled experiments with 2-4 mice per group are shown. *p<0.05.
Figure 5: Islet infiltration by CD8+ and CD11b
+ cells is reduced after CT at 5 and/or 12
weeks post-onset. (A, left panels) CD4+, CD8
+ and CD11b
+ cell infiltration in mice treated with
GAD65 DNA with isotype or anti-IL-1β antibody. Pancreas sections from treated mice were
stained for insulin as well as CD4, CD8 and CD11b in parallel. Classification was performed as
follows: (i) no insulitis (white), (ii) peri-insulitis with no islet destruction or a few (less than 10)
infiltrating cells (grey), and (iii) infiltrating insulitis with extensive islet destruction (or islet
destroyed) (black). (A, right panels) Representative pictures at 20X. Two-way ANOVA tests
determined statistically significant differences (*P<0.05). (B) At 12 weeks post-onset, the
pancreas of mice was processed and cells stained for FACS analyses to confirm histological
analyses (*P<0.05 upon Mann-Whitney test). The extent of CD4+, CD8
+ or CD11b
+ cell
infiltration was counted as follows: 1 week post-onset: 29-134 islets from 3 mice per group; 5
weeks post-onset: 16-111 islets from 2-5 mice per group; 12 weeks post-onset: 13-39 islets from
3 mice per group.
Page 20 of 35Diabetes

21
Figure 6: The extent of islet infiltration by CD11bhigh
but not T cells correlates with efficacy
of the CT. (A, C, E) Frequencies of CD11bhigh
(A), CD8 T (C) and CD4+CD25
+Foxp3
+ Treg (E)
cells found in the pancreas of mice upon indicated treatment. (B, D, F) Correlation between
mouse glycemia at 12 weeks post-treatment and the percentage of CD11bhigh
(B), CD8 T (D) and
CD4+CD25
+Foxp3
+ Treg (F) cell infiltration in mouse pancreata. Note that using Pearson
correlation test, r values between 0.3 and 0.7 (0.3 and -0.7) indicate a moderate positive
(negative) linear relationship.
Page 21 of 35 Diabetes

22
REFERENCES
1. Dinarello CA, Simon A, van der Meer JW: Treating inflammation by blocking
interleukin-1 in a broad spectrum of diseases. Nature reviews Drug discovery 2012;11:633-652
2. Mandrup-Poulsen T, Pickersgill L, Donath MY: Blockade of interleukin 1 in type 1
diabetes mellitus. Nature reviews Endocrinology 2010;6:158-166
3. Willcox A, Richardson SJ, Bone AJ, Foulis AK, Morgan NG: Analysis of islet
inflammation in human type 1 diabetes. Clinical and experimental immunology 2009;155:173-
181
4. Mandrup-Poulsen T, Bendtzen K, Dinarello CA, Nerup J: Human tumor necrosis factor
potentiates human interleukin 1 mediated rat pancreatic beta cell cytotoxicity. Journal of
immunology 1987;139: 4077-82
5. Thomas HE, Darwiche R, Corbett JA, Kay TW: Interleukin-1 plus gamma-interferon-
induced pancreatic beta-cell dysfunction is mediated by beta-cell nitric oxide production.
Diabetes 2002;51:311-316
6. Eizirik DL, Colli ML, Ortis F: The role of inflammation in insulitis and beta-cell loss in
type 1 diabetes. Nature reviews Endocrinology 2009;5:219-226
7. Shaftel SS, Griffin WS, O'Banion MK: The role of interleukin-1 in neuroinflammation
and Alzheimer disease: an evolving perspective. Journal of neuroinflammation 2008;5:7
8. Mandrup-Poulsen T, Bendtzen K, Nerup J, Dinarello CA, Svenson M, Nielsen JH:
Affinity-purified human interleukin I is cytotoxic to isolated islets of Langerhans. Diabetologia
1986;29:63-67
9. Maedler K, Sergeev P, Ris F, Oberholzer J, Joller-Jemelka HI, Spinas GA, Kaiser N,
Halban PA, Donath MY: Glucose-induced beta cell production of IL-1beta contributes to
glucotoxicity in human pancreatic islets. The Journal of clinical investigation 2002;110:851-860
10. Maedler K, Storling J, Sturis J, Zuellig RA, Spinas GA, Arkhammar PO, Mandrup-
Poulsen T, Donath MY: Glucose- and interleukin-1beta-induced beta-cell apoptosis requires
Ca2+ influx and extracellular signal-regulated kinase (ERK) 1/2 activation and is prevented by a
sulfonylurea receptor 1/inwardly rectifying K+ channel 6.2 (SUR/Kir6.2) selective potassium
channel opener in human islets. Diabetes 2004;53:1706-1713
11. Osborn O, Brownell SE, Sanchez-Alavez M, Salomon D, Gram H, Bartfai T: Treatment
with an Interleukin 1 beta antibody improves glycemic control in diet-induced obesity. Cytokine
2008;44:141-148
12. Cavelti-Weder C, Babians-Brunner A, Keller C, Stahel MA, Kurz-Levin M, Zayed H,
Solinger AM, Mandrup-Poulsen T, Dinarello CA, Donath MY: Effects of gevokizumab on
glycemia and inflammatory markers in type 2 diabetes. Diabetes care 2012;35:1654-1662
13. Larsen CM, Faulenbach M, Vaag A, Volund A, Ehses JA, Seifert B, Mandrup-Poulsen
T, Donath MY: Interleukin-1-receptor antagonist in type 2 diabetes mellitus. The New England
journal of medicine 2007;356:1517-1526
14. Kaizer EC, Glaser CL, Chaussabel D, Banchereau J, Pascual V, White PC: Gene
expression in peripheral blood mononuclear cells from children with diabetes. The Journal of
clinical endocrinology and metabolism 2007;92:3705-3711
15. Pfleger C, Mortensen HB, Hansen L, Herder C, Roep BO, Hoey H, Aanstoot HJ, Kocova
M, Schloot NC, Hvidore Study Group on Childhood D: Association of IL-1ra and adiponectin
with C-peptide and remission in patients with type 1 diabetes. Diabetes 2008;57:929-937
Page 22 of 35Diabetes

23
16. Sanda S, Bollyky J, Standifer N, Nepom G, Hamerman JA, Greenbaum C: Short-term
IL-1beta blockade reduces monocyte CD11b integrin expression in an IL-8 dependent fashion in
patients with type 1 diabetes. Clinical immunology 2010;136:170-173
17. Moran A, Bundy B, Becker DJ, DiMeglio LA, Gitelman SE, Goland R, Greenbaum CJ,
Herold KC, Marks JB, Raskin P, Sanda S, Schatz D, Wherrett DK, Wilson DM, Krischer JP,
Skyler JS, Pickersgill L, de Koning E, Ziegler AG, Boehm B, Badenhoop K, Schloot N, Bak JF,
Pozzilli P, Mauricio D, Donath MY, Castano L, Wagner A, Lervang HH, Perrild H, Mandrup-
Poulsen T, for the Type 1 Diabetes TrialNet Canakinumab Study Group, for the AIDA Study
Group: Interleukin-1 antagonism in type 1 diabetes of recent onset: two multicentre, randomised,
double-blind, placebo-controlled trials. Lancet 2013;381:1905-1915
18. Thomas HE, Irawaty W, Darwiche R, Brodnicki TC, Santamaria P, Allison J, Kay TW:
IL-1 receptor deficiency slows progression to diabetes in the NOD mouse. Diabetes 2004;53:113-
121
19. Ablamunits V, Henegariu O, Hansen JB, Opare-Addo L, Preston-Hurlburt P, Santamaria
P, Mandrup-Poulsen T, Herold KC: Synergistic reversal of type 1 diabetes in NOD mice with
anti-CD3 and interleukin-1 blockade: evidence of improved immune regulation. Diabetes
2012;61:145-154
20. Bresson D, Togher L, Rodrigo E, Chen Y, Bluestone JA, Herold KC, von Herrath M:
Anti-CD3 and nasal proinsulin combination therapy enhances remission from recent-onset
autoimmune diabetes by inducing Tregs. The Journal of clinical investigation 2006;116:1371-
1381
21. Mamchak AA, Manenkova Y, Leconet W, Zheng Y, Chan JR, Stokes CL, Shoda LK,
von Herrath M, Bresson D: Preexisting autoantibodies predict efficacy of oral insulin to cure
autoimmune diabetes in combination with anti-CD3. Diabetes 2012;61:1490-1499
22. Bresson D, Fradkin M, Manenkova Y, Rottembourg D, von Herrath M: Genetic-induced
variations in the GAD65 T-cell repertoire governs efficacy of anti-CD3/GAD65 combination
therapy in new-onset type 1 diabetes. Molecular therapy : the journal of the American Society of
Gene Therapy 2010;18:307-316
23. Oldstone MB, Nerenberg M, Southern P, Price J, Lewicki H: Virus infection triggers
insulin-dependent diabetes mellitus in a transgenic model: role of anti-self (virus) immune
response. Cell 1991;65:319-331
24. Solvason N, Lou YP, Peters W, Evans E, Martinez J, Ramirez U, Ocampo A, Yun R,
Ahmad S, Liu E, Yu L, Eisenbarth G, Leviten M, Steinman L, Garren H: Improved efficacy of a
tolerizing DNA vaccine for reversal of hyperglycemia through enhancement of gene expression
and localization to intracellular sites. Journal of immunology 2008;181:8298-8307
25. Tisch R, Wang B, Weaver DJ, Liu B, Bui T, Arthos J, Serreze DV: Antigen-specific
mediated suppression of beta cell autoimmunity by plasmid DNA vaccination. Journal of
immunology 2001;166:2122-2132
26. von Herrath MG, Dockter J, Oldstone MB: How virus induces a rapid or slow onset
insulin-dependent diabetes mellitus in a transgenic model. Immunity 1994;1:231-242
27. Boettler T, Pagni PP, Jaffe R, Cheng Y, Zerhouni P, von Herrath M: The clinical and
immunological significance of GAD-specific autoantibody and T-cell responses in type 1
diabetes. Journal of autoimmunity 2013;
28. Roep BO, Solvason N, Gottlieb PA, Abreu JR, Harrison LC, Eisenbarth GS, Yu L,
Leviten M, Hagopian WA, Buse JB, von Herrath M, Quan J, King RS, Robinson WH, Utz PJ,
Garren H, Investigators BHT, Steinman L: Plasmid-Encoded Proinsulin Preserves C-Peptide
While Specifically Reducing Proinsulin-Specific CD8+ T Cells in Type 1 Diabetes. Science
translational medicine 2013;5:191ra182
Page 23 of 35 Diabetes

24
29. Abiru N, Maniatis AK, Yu L, Miao D, Moriyama H, Wegmann D, Eisenbarth GS:
Peptide and major histocompatibility complex-specific breaking of humoral tolerance to native
insulin with the B9-23 peptide in diabetes-prone and normal mice. Diabetes 2001;50:1274-1281
30. Lind M, Oden A, Fahlen M, Eliasson B: The true value of HbA1c as a predictor of
diabetic complications: simulations of HbA1c variables. PloS one 2009;4:e4412
31. Hagopian W, Ferry RJ, Jr., Sherry N, Carlin D, Bonvini E, Johnson S, Stein KE, Koenig
S, Daifotis AG, Herold KC, Ludvigsson J, for the Protege Trial I: Teplizumab preserves C-
peptide in recent-onset type 1 diabetes: 2-year results from the randomized, placebo-controlled
Protege trial. Diabetes 2013;
32. O'Sullivan BJ, Thomas HE, Pai S, Santamaria P, Iwakura Y, Steptoe RJ, Kay TW,
Thomas R: IL-1 beta breaks tolerance through expansion of CD25+ effector T cells. Journal of
immunology 2006;176:7278-7287
33. Bertin-Maghit S, Pang D, O'Sullivan B, Best S, Duggan E, Paul S, Thomas H, Kay TW,
Harrison LC, Steptoe R, Thomas R: Interleukin-1beta produced in response to islet autoantigen
presentation differentiates T-helper 17 cells at the expense of regulatory T-cells: Implications for
the timing of tolerizing immunotherapy. Diabetes 2011;60:248-257
34. Brinster C, Shevach EM: Costimulatory effects of IL-1 on the expansion/differentiation
of CD4+CD25+Foxp3+ and CD4+CD25+Foxp3- T cells. Journal of leukocyte biology
2008;84:480-487
35. Ganesh BB, Bhattacharya P, Gopisetty A, Sheng J, Vasu C, Prabhakar BS: IL-1beta
promotes TGF-beta1 and IL-2 dependent Foxp3 expression in regulatory T cells. PloS one
2011;6:e21949
36. Trudeau JD, Kelly-Smith C, Verchere CB, Elliott JF, Dutz JP, Finegood DT, Santamaria
P, Tan R: Prediction of spontaneous autoimmune diabetes in NOD mice by quantification of
autoreactive T cells in peripheral blood. The Journal of clinical investigation 2003;111:217-223
37. Velthuis JH, Unger WW, Abreu JR, Duinkerken G, Franken K, Peakman M, Bakker AH,
Reker-Hadrup S, Keymeulen B, Drijfhout JW, Schumacher TN, Roep BO: Simultaneous
detection of circulating autoreactive CD8+ T-cells specific for different islet cell-associated
epitopes using combinatorial MHC multimers. Diabetes 2010;59:1721-1730
38. von Herrath M, Holz A: Pathological changes in the islet milieu precede infiltration of
islets and destruction of beta-cells by autoreactive lymphocytes in a transgenic model of virus-
induced IDDM. Journal of autoimmunity 1997;10:231-238
39. Itoh N, Hanafusa T, Miyazaki A, Miyagawa J, Yamagata K, Yamamoto K, Waguri M,
Imagawa A, Tamura S, Inada M, et al.: Mononuclear cell infiltration and its relation to the
expression of major histocompatibility complex antigens and adhesion molecules in pancreas
biopsy specimens from newly diagnosed insulin-dependent diabetes mellitus patients. The
Journal of clinical investigation 1993;92:2313-2322
40. Barral AM, Thomas HE, Ling EM, Darwiche R, Rodrigo E, Christen U, Ejrnaes M,
Wolfe T, Kay TW, von Herrath MG: SOCS-1 protects from virally-induced CD8 T cell mediated
type 1 diabetes. Journal of autoimmunity 2006;27:166-173
41. Bresson D, von Herrath M: Immunotherapy for the prevention and treatment of type 1
diabetes: optimizing the path from bench to bedside. Diabetes care 2009;32:1753-1768
42. Bot A, Smith D, Bot S, Hughes A, Wolfe T, Wang L, Woods C, von Herrath M: Plasmid
vaccination with insulin B chain prevents autoimmune diabetes in nonobese diabetic mice.
Journal of immunology 2001;167:2950-2955
43. Homann D, Holz A, Bot A, Coon B, Wolfe T, Petersen J, Dyrberg TP, Grusby MJ, von
Herrath MG: Autoreactive CD4+ T cells protect from autoimmune diabetes via bystander
suppression using the IL-4/Stat6 pathway. Immunity 1999;11:463-472
Page 24 of 35Diabetes

25
44. King C, Mueller Hoenger R, Malo Cleary M, Murali-Krishna K, Ahmed R, King E,
Sarvetnick N: Interleukin-4 acts at the locus of the antigen-presenting dendritic cell to counter-
regulate cytotoxic CD8+ T-cell responses. Nature medicine 2001;7:206-214
45. Ludvigsson J, Krisky D, Casas R, Battelino T, Castano L, Greening J, Kordonouri O,
Otonkoski T, Pozzilli P, Robert JJ, Veeze HJ, Palmer J, Samuelsson U, Elding Larsson H, Aman
J, Kardell G, Neiderud Helsingborg J, Lundstrom G, Albinsson E, Carlsson A, Nordvall M, Fors
H, Arvidsson CG, Edvardson S, Hanas R, Larsson K, Rathsman B, Forsgren H, Desaix H,
Forsander G, Nilsson NO, Akesson CG, Keskinen P, Veijola R, Talvitie T, Raile K, Kapellen T,
Burger W, Neu A, Engelsberger I, Heidtmann B, Bechtold S, Leslie D, Chiarelli F, Cicognani A,
Chiumello G, Cerutti F, Zuccotti GV, Gomez Gila A, Rica I, Barrio R, Clemente M, Lopez
Garcia MJ, Rodriguez M, Gonzalez I, Lopez JP, Oyarzabal M, Reeser HM, Nuboer R, Stouthart
P, Bratina N, Bratanic N, de Kerdanet M, Weill J, Ser N, Barat P, Bertrand AM, Carel JC,
Reynaud R, Coutant R, Baron S: GAD65 antigen therapy in recently diagnosed type 1 diabetes
mellitus. The New England journal of medicine 2012;366:433-442
46. Wherrett DK, Bundy B, Becker DJ, DiMeglio LA, Gitelman SE, Goland R, Gottlieb PA,
Greenbaum CJ, Herold KC, Marks JB, Monzavi R, Moran A, Orban T, Palmer JP, Raskin P,
Rodriguez H, Schatz D, Wilson DM, Krischer JP, Skyler JS, Type 1 Diabetes TrialNet GADSG:
Antigen-based therapy with glutamic acid decarboxylase (GAD) vaccine in patients with recent-
onset type 1 diabetes: a randomised double-blind trial. Lancet 2011;378:319-327
Page 25 of 35 Diabetes

*
Pagni et al. Fig 1.
B C
ns
* *
*
A Isotype Ab Anti-IL1β Ab Anti-IL1β/GAD Isot/GAD
Diabetes incidence for E2-8BGVs 250-400
0 1 2 3 4 50
20
40
60
80
100 anti-isot Ab (n=7)
anti-IL1b Ab (n=6)
anti-isot Ab / GAD (n=12)
anti-IL1b Ab / GAD (n=17)
Weeks post treatment onset
Dia
bete
s incid
ence (
%)
Diabetes incidence for E2-8BGVs 250-400
0 1 2 3 4 50
20
40
60
80
100 anti-isot Ab (n=7)
anti-IL1b Ab (n=6)
anti-isot Ab / GAD (n=12)
anti-IL1b Ab / GAD (n=17)
Weeks post treatment onset
Dia
bete
s incid
ence (
%)
Diabetes incidence for E2-8BGVs 250-400
0 1 2 3 4 50
20
40
60
80
100 anti-isot Ab (n=7)
anti-IL1b Ab (n=6)
anti-isot Ab / GAD (n=12)
anti-IL1b Ab / GAD (n=17)
Weeks post treatment onset
Dia
bete
s incid
ence (
%)
Diabetes incidence for E2-8BGVs 250-400
0 1 2 3 4 50
20
40
60
80
100 anti-isot Ab (n=7)
anti-IL1b Ab (n=6)
anti-isot Ab / GAD (n=12)
anti-IL1b Ab / GAD (n=17)
Weeks post treatment onset
Dia
bete
s incid
ence (
%)
Time to reversion to normoglycemia (weeks)
anti-
isot
Ab
+ GAD (n
=4)
anti-
IL1b
Ab
+ GAD (
n=9)
0
2
4
6
0.0466
I also have a significant diff with Gehan-Breslow graph.This graph may not be needed to make my point then.
Tim
e to r
evers
ion
(weeks p
ost-
treatm
ent sta
rt)
*
5-week follow up
E2-9, BGVs 250-400
0 1 2 3 4 50
200
400
600
Weeks post treatment start
BG
V (
mg/d
l)
E2-9, BGVs 250-400
0 1 2 3 4 5Weeks post treatment start
0/6 (0%) 9/17 (53%) 4/12 (33%) 1/6 (17%)
Diabetes incidence for E2-8BGVs 250-400
0 1 2 3 4 50
20
40
60
80
100 anti-isot Ab (n=6)
anti-IL1b Ab (n=6)
anti-isot Ab / GAD (n=12)
anti-IL1b Ab / GAD (n=17)
Weeks post treatment onset
Dia
bete
s incid
ence (
%)
E2-9, BGVs 250-400
0 1 2 3 4 5Weeks post treatment start
E2-9, BGVs 250-400
0 1 2 3 4 5Weeks post treatment start
% cured (Final BGV < 250mg/dl)
% mild HG (Final BGV 251-400mg/dl)
% severe HG (Final BGV > 401mg/dl)
Diabetes incidence for E2-8BGVs 250-400
0 1 2 3 4 50
20
40
60
80
100 anti-isot Ab (n=7)
anti-IL1b Ab (n=6)
anti-isot Ab / GAD (n=12)
anti-IL1b Ab / GAD (n=17)
Weeks post treatment onset
Dia
bete
s incid
ence (
%)
Diabetes incidence for E2-8BGVs 250-400
0 1 2 3 4 50
20
40
60
80
100 anti-isot Ab (n=7)
anti-IL1b Ab (n=6)
anti-isot Ab / GAD (n=12)
anti-IL1b Ab / GAD (n=17)
Weeks post treatment onset
Dia
bete
s incid
ence (
%)
Diabetes incidence for E2-8BGVs 250-400
0 1 2 3 4 50
20
40
60
80
100 anti-isot Ab (n=7)
anti-IL1b Ab (n=6)
anti-isot Ab / GAD (n=12)
anti-IL1b Ab / GAD (n=17)
Weeks post treatment onset
Dia
bete
s incid
ence (
%)
Diabetes incidence for E2-8BGVs 250-400
0 1 2 3 4 50
20
40
60
80
100 anti-isot Ab (n=7)
anti-IL1b Ab (n=6)
anti-isot Ab / GAD (n=12)
anti-IL1b Ab / GAD (n=17)
Weeks post treatment onset
Dia
bete
s incid
ence (
%)
D % mice cured vs mild vs high BG
anti-
isot
Ab
(n=6
)
anti-
IL1b
Ab
(n=6
)
anti-
isot
Ab
+ GAD (n
=12)
anti-
IL1b
Ab
+ GAD (n
=17)
0
20
40
60
80
100
% cured (Final BG < 250mg/dl)% mild HG (Final BG 251-400)% high HG (Final BG >401)
% e
nro
lled m
ice
% mice cured vs mild vs high BG
anti-
isot
Ab
(n=6
)
anti-
IL1b
Ab
(n=6
)
anti-
isot
Ab
+ GAD (n
=12)
anti-
IL1b
Ab
+ GAD (n
=17)
0
20
40
60
80
100
% cured (Final BG < 250mg/dl)% mild HG (Final BG 251-400)% high HG (Final BG >401)
% e
nro
lled m
ice
* *
E Anti-IL1β/GAD Isot/GAD
At onset 5 wks At onset 5 wks
Diabetes incidence for E2-8BGVs 250-400
0 1 2 3 4 50
20
40
60
80
100 anti-isot Ab (n=7)
anti-IL1b Ab (n=6)
anti-isot Ab / GAD (n=12)
anti-IL1b Ab / GAD (n=17)
Weeks post treatment onset
Dia
bete
s incid
ence (
%)
Diabetes incidence for E2-8BGVs 250-400
0 1 2 3 4 50
20
40
60
80
100 anti-isot Ab (n=7)
anti-IL1b Ab (n=6)
anti-isot Ab / GAD (n=12)
anti-IL1b Ab / GAD (n=17)
Weeks post treatment onset
Dia
bete
s incid
ence (
%)
BGV at entry vs 5wks post-onset (ANTI-IL-1b/GAD)
Ant
i-IL-
1b/G
AD a
t ent
ry
Ant
i-IL-
1b 5
wks
pos
t-ons
et200
300
400
500
600
BG
V (
mg/d
l)
BGV at entry vs 5wks post-onset (ANTI-ISOT/GAD)
Ant
i-iso
t/GAD a
t ent
ry
Ant
i-iso
t/GAD 5
wks
pos
t-ons
et200
300
400
500
600
BG
V (
mg/d
l)
% mice cured vs mild vs high BG
anti-
isot
Ab
(n=6
)
anti-
IL1b
Ab
(n=6
)
anti-
isot
Ab
+ GAD (n
=12)
anti-
IL1b
Ab
+ GAD (n
=17)
0
20
40
60
80
100
% cured (Final BG < 250mg/dl)% mild HG (Final BG 251-400)% high HG (Final BG >401)
% e
nro
lled m
ice
% mice cured vs mild vs high BG
anti-
isot
Ab
(n=6
)
anti-
IL1b
Ab
(n=6
)
anti-
isot
Ab
+ GAD (n
=12)
anti-
IL1b
Ab
+ GAD (n
=17)
0
20
40
60
80
100
% cured (Final BG < 250mg/dl)% mild HG (Final BG 251-400)% high HG (Final BG >401)
% e
nro
lled m
ice
% mice cured vs mild vs high BG
anti-
isot
Ab
(n=6
)
anti-
IL1b
Ab
(n=6
)
anti-
isot
Ab
+ GAD (n
=12)
anti-
IL1b
Ab
+ GAD (n
=17)
0
20
40
60
80
100
% cured (Final BG < 250mg/dl)% mild HG (Final BG 251-400)% high HG (Final BG >401)
% e
nro
lled m
ice
% mice cured vs mild vs high BG
anti-
isot
Ab
(n=6
)
anti-
IL1b
Ab
(n=6
)
anti-
isot
Ab
+ GAD (n
=12)
anti-
IL1b
Ab
+ GAD (n
=17)
0
20
40
60
80
100
% cured (Final BG < 250mg/dl)% mild HG (Final BG 251-400)% high HG (Final BG >401)
% e
nro
lled m
ice
% mice cured vs mild vs high BG
anti-
isot
Ab
(n=6
)
anti-
IL1b
Ab
(n=6
)
anti-
isot
Ab
+ GAD (n
=12)
anti-
IL1b
Ab
+ GAD (n
=17)
0
20
40
60
80
100
% cured (Final BG < 250mg/dl)% mild HG (Final BG 251-400)% high HG (Final BG >401)
% e
nro
lled m
ice
% mice cured vs mild vs high BG
anti-
isot
Ab
(n=6
)
anti-
IL1b
Ab
(n=6
)
anti-
isot
Ab
+ GAD (n
=12)
anti-
IL1b
Ab
+ GAD (n
=17)
0
20
40
60
80
100
% cured (Final BG < 250mg/dl)% mild HG (Final BG 251-400)% high HG (Final BG >401)
% e
nro
lled m
ice
** ns
Anti-IL1β/GAD Isot/GAD
Page 26 of 35Diabetes

% C
D8+
IFN
-γ+
% C
D8+
TNF+
GP33 peptide in vitro stimulation S
plee
n P
LNs
*
% C
D4+
CD
25+ F
oxp3
+
C
5-week follow up
% C
D8+
IFN
-γ+
% C
D8+
TNF+
% C
D4+
CD
25+ F
oxp3
+
Anti-IL1β Ab Anti-IL1β/GAD
A Sp- E2-4 Total IFNg+ in CD8+Sp-
anti-i
sot A
b (n=
6)
anti-I
L1b A
b (n=
7)
Anti-is
ot+GAD (n
=3)
anti-I
L1b A
b+GAD (n
=7)
0
5
10
15
0.0112%
IFN
g+ in
CD
8+
Sp- E2-4 Total IFNg+ in CD8+Sp-
*
Sp- E2-4 Total TNFa+ in CD8+Sp-
anti-i
sot A
b (n=
6)
anti-I
L1b A
b (n=
7)
Anti-is
ot+GAD (n
=3)
anti-I
L1b A
b+GAD (n
=7)
0
10
20
30
% T
NF+
in C
D8+
Sp- E2-4 Total TNFa+ in CD8+Sp-
* *
PLNs- Total IFNg+ in CD8+
anti-i
sot A
b (n=
6)
anti-I
L1b A
b (n=
7)
Anti-is
ot+GAD (n
=3)
anti-I
L1b A
b+GAD (n
=7)
0
2
4
6
% IF
Ng+
in C
D8+
PLNs- Total IFNg+ in CD8+
Sp- E2-4 CD4+CD25+Foxp3+
anti-i
sot A
b (n=
6)
anti-I
L1b A
b (n=
7)
Anti-is
ot+GAD (n
=3)
anti-I
L1b A
b+GAD (n
=7)
0
5
10
15
20
% C
D4+
CD
25+F
oxp3
+
Sp- E2-4 CD4+CD25+Foxp3+
PLNs- E2-4 CD4+CD25+Foxp3+
anti-i
sot A
b (n=
6)
anti-I
L1b A
b (n=
7)
Anti-is
ot+GAD (n
=3)
anti-I
L1b A
b+GAD (n
=7)
0
5
10
15
20
0.0358
% C
D4+
CD
25+F
oxp3
+
PLNs- E2-4 CD4+CD25+Foxp3+
PLNs- Total TNFa+ in CD8+
anti-i
sot A
b (n=
6)
anti-I
L1b A
b (n=
7)
Anti-is
ot+GAD (n
=3)
anti-I
L1b A
b+GAD (n
=7)
0
1
2%
TN
F+ in
CD
8+
PLNs- Total TNFa+ in CD8+
* *
d4pi bld- MFI CXCR3 in CD4+
a-iso
t (n=
7)
a-IL1
b (n=
7)
a-iso
t/GAD (n
=7)
a-IL1
b/GAD (n
=7)
0
1000
2000
3000a-isot (n=7)a-IL1b (n=7)a-isot/GAD (n=7)a-IL1b/GAD (n=7)
MFI
CX
CR
3 in
CD
4+
d4pi bld- MFI CXCR3 in CD4+
a-iso
t (n=
7)
a-IL1
b (n=
7)
a-iso
t/GAD (n
=7)
a-IL1
b/GAD (n
=7)
0
1000
2000
3000a-isot (n=7)a-IL1b (n=7)a-isot/GAD (n=7)a-IL1b/GAD (n=7)
MFI
CX
CR
3 in
CD
4+
d4pi bld- MFI CXCR3 in CD4+
a-iso
t (n=
7)
a-IL1
b (n=
7)
a-iso
t/GAD (n
=7)
a-IL1
b/GAD (n
=7)
0
1000
2000
3000a-isot (n=7)a-IL1b (n=7)a-isot/GAD (n=7)a-IL1b/GAD (n=7)
MFI
CX
CR
3 in
CD
4+
d4pi bld- MFI CXCR3 in CD4+
a-iso
t (n=
7)
a-IL1
b (n=
7)
a-iso
t/GAD (n
=7)
a-IL1
b/GAD (n
=7)
0
1000
2000
3000a-isot (n=7)a-IL1b (n=7)a-isot/GAD (n=7)a-IL1b/GAD (n=7)
MFI
CX
CR
3 in
CD
4+
d4pi bld- MFI CXCR3 in CD4+
a-iso
t (n=
7)
a-IL1
b (n=
7)
a-iso
t/GAD (n
=7)
a-IL1
b/GAD (n
=7)
0
1000
2000
3000a-isot (n=7)a-IL1b (n=7)a-isot/GAD (n=7)a-IL1b/GAD (n=7)
MFI
CX
CR
3 in
CD
4+
d4pi bld- MFI CXCR3 in CD4+
a-iso
t (n=
7)
a-IL1
b (n=
7)
a-iso
t/GAD (n
=7)
a-IL1
b/GAD (n
=7)
0
1000
2000
3000a-isot (n=7)a-IL1b (n=7)a-isot/GAD (n=7)a-IL1b/GAD (n=7)
MFI
CX
CR
3 in
CD
4+
d4pi bld- MFI CXCR3 in CD4+
a-iso
t (n=
7)
a-IL1
b (n=
7)
a-iso
t/GAD (n
=7)
a-IL1
b/GAD (n
=7)
0
1000
2000
3000a-isot (n=7)a-IL1b (n=7)a-isot/GAD (n=7)a-IL1b/GAD (n=7)
MFI
CX
CR
3 in
CD
4+
d4pi bld- MFI CXCR3 in CD4+
a-iso
t (n=
7)
a-IL1
b (n=
7)
a-iso
t/GAD (n
=7)
a-IL1
b/GAD (n
=7)
0
1000
2000
3000a-isot (n=7)a-IL1b (n=7)a-isot/GAD (n=7)a-IL1b/GAD (n=7)
MFI
CX
CR
3 in
CD
4+Pagni et al. Fig 2.
D B
Isot/GAD Isotype Ab
Page 27 of 35 Diabetes

% mice cured vs mild vs high BG
anti-
isot
Ab
+ GAD
(n=1
1)
anti-
IL1b
Ab
+ GAD (n
=14)
0
20
40
60
80
100
% cured (Final BG < 250mg/dl)% mild HG (Final BG 251-400)% high HG (Final BG >401)
% e
nro
lled m
ice
B A
12-week follow up Anti-IL1β/GAD Isot/GAD
Diabetes incidence for E2-8BGVs 250-400
0 1 2 3 4 50
20
40
60
80
100 anti-isot Ab (n=7)
anti-IL1b Ab (n=6)
anti-isot Ab / GAD (n=12)
anti-IL1b Ab / GAD (n=17)
Weeks post treatment onset
Dia
bete
s incid
ence (
%)
Diabetes incidence for E2-8BGVs 250-400
0 1 2 3 4 50
20
40
60
80
100 anti-isot Ab (n=7)
anti-IL1b Ab (n=6)
anti-isot Ab / GAD (n=12)
anti-IL1b Ab / GAD (n=17)
Weeks post treatment onset
Dia
bete
s incid
ence (
%)
C
***
Pagni et al. Fig 3.
E5+6+7+8 GP- BGVs
0 2 4 6 8 10 120
200
400
600E5_Anti-IL1b/GAD #3570
E5_Anti-IL1b/GAD #3542
E5_Anti-IL1b/GAD #3544
E5_Anti-IL1b/GAD #3583
E6_Anti-IL1b/GAD #3981
E6_Anti-IL1b/GAD #3977
E7_a-IL1/GAD #5350
E7_a-IL1/GAD #5327
E8_a-IL1/GAD #5355
E8_a-IL1/GAD #5320
E8_a-IL1/GAD #5331
E8_a-IL1/GAD #5340
E9_a-IL1/GAD #6001
E9_a-IL1/GAD #6003
E9_a-IL1/GAD #6015
Weeks post-treatment
BG
V (
mg/d
l)
E5+6+7+8 GP- BGVs
0 2 4 6 8 10 120
200
400
600
E5_Anti-isot/GAD #3590
E5_Anti-isot/GAD #3543
E6_Anti-isot/GAD #3980
E6_Anti-isot/GAD #3978
E7_a-isot/GAD #5329
E7_a-isot/GAD #5358
E8_a-isot/GAD #5363
E8_a-isot/GAD #5370
E8_a-isot/GAD #5371
E9_a-isot/GAD #6008
E9_a-isot/GAD #6009
Weeks post-treatment
BG
V (
mg/d
l)
E5+6+7+8+9 GP- BGVs
0 2 4 6 8 10 120
200
400
600
Anti-iso/GAD (n=9)+5
Anti-IL1b/GAD (n=14+5)
Weeks post-treatment
Mean B
GV
(m
g/d
l)
6/14 (43%) 2/11 (18%)
% cured (Final BGV < 250mg/dl)
% mild HG (Final BGV 251-400mg/dl)
% severe HG (Final BGV > 401mg/dl)
E
% mice cured vs mild vs high BG
anti-
isot
Ab
(n=6
)
anti-
IL1b
Ab
(n=6
)
anti-
isot
Ab
+ GAD (n
=12)
anti-
IL1b
Ab
+ GAD (n
=17)
0
20
40
60
80
100
% cured (Final BG < 250mg/dl)% mild HG (Final BG 251-400)% high HG (Final BG >401)
% e
nro
lled m
ice
*
Anti-IL1β/GAD
At onset 12 wks At onset 12 wks
Diabetes incidence for E2-8BGVs 250-400
0 1 2 3 4 50
20
40
60
80
100 anti-isot Ab (n=7)
anti-IL1b Ab (n=6)
anti-isot Ab / GAD (n=12)
anti-IL1b Ab / GAD (n=17)
Weeks post treatment onset
Dia
bete
s incid
ence (
%)
Diabetes incidence for E2-8BGVs 250-400
0 1 2 3 4 50
20
40
60
80
100 anti-isot Ab (n=7)
anti-IL1b Ab (n=6)
anti-isot Ab / GAD (n=12)
anti-IL1b Ab / GAD (n=17)
Weeks post treatment onset
Dia
bete
s incid
ence (
%)
% mice cured vs mild vs high BG
anti-
isot
Ab
(n=6
)
anti-
IL1b
Ab
(n=6
)
anti-
isot
Ab
+ GAD (n
=12)
anti-
IL1b
Ab
+ GAD (n
=17)
0
20
40
60
80
100
% cured (Final BG < 250mg/dl)% mild HG (Final BG 251-400)% high HG (Final BG >401)
% e
nro
lled m
ice
% mice cured vs mild vs high BG
anti-
isot
Ab
(n=6
)
anti-
IL1b
Ab
(n=6
)
anti-
isot
Ab
+ GAD (n
=12)
anti-
IL1b
Ab
+ GAD (n
=17)
0
20
40
60
80
100
% cured (Final BG < 250mg/dl)% mild HG (Final BG 251-400)% high HG (Final BG >401)
% e
nro
lled m
ice
% mice cured vs mild vs high BG
anti-
isot
Ab
(n=6
)
anti-
IL1b
Ab
(n=6
)
anti-
isot
Ab
+ GAD (n
=12)
anti-
IL1b
Ab
+ GAD (n
=17)
0
20
40
60
80
100
% cured (Final BG < 250mg/dl)% mild HG (Final BG 251-400)% high HG (Final BG >401)
% e
nro
lled m
ice
% mice cured vs mild vs high BG
anti-
isot
Ab
(n=6
)
anti-
IL1b
Ab
(n=6
)
anti-
isot
Ab
+ GAD (n
=12)
anti-
IL1b
Ab
+ GAD (n
=17)
0
20
40
60
80
100
% cured (Final BG < 250mg/dl)% mild HG (Final BG 251-400)% high HG (Final BG >401)
% e
nro
lled m
ice
% mice cured vs mild vs high BG
anti-
isot
Ab
(n=6
)
anti-
IL1b
Ab
(n=6
)
anti-
isot
Ab
+ GAD (n
=12)
anti-
IL1b
Ab
+ GAD (n
=17)
0
20
40
60
80
100
% cured (Final BG < 250mg/dl)% mild HG (Final BG 251-400)% high HG (Final BG >401)
% e
nro
lled m
ice
% mice cured vs mild vs high BG
anti-
isot
Ab
(n=6
)
anti-
IL1b
Ab
(n=6
)
anti-
isot
Ab
+ GAD (n
=12)
anti-
IL1b
Ab
+ GAD (n
=17)
0
20
40
60
80
100
% cured (Final BG < 250mg/dl)% mild HG (Final BG 251-400)% high HG (Final BG >401)
% e
nro
lled m
ice
* ns BGV at entry vs 12wks post-onset (ANTI-ISOT/GAD)
Ant
i-iso
t/GAD a
t ent
ry
Ant
i-iso
t/GAD 1
2wks
pos
t-ons
et
200
300
400
500
600
BG
V (
mg/d
l)
0.0391
BGV at entry vs 12wks post-onset (ANTI-ISOT/GAD)
Ant
i-IL-
1b/G
AD a
t ent
ry
Ant
i-IL-
1b 1
2wks
pos
t-ons
et
200
300
400
500
600
BG
V (
mg/d
l)
0.5469
D
# of weeks spent <250mg/dl
anti-
isot
Ab
+ GAD (n
=3)
anti-
IL1b
Ab
+ GAD (n
=6)
0
2
4
6
8
# o
f w
eeks s
pent
with B
GV
< 2
50m
g/d
l
*
Isot/GAD
Dura
tion o
f tr
ansie
nt
revers
ion (
weeks)
a-IL1β/GAD Isot/GAD
Anti-IL1β/GAD Isot/GAD
Page 28 of 35Diabetes

% n
p396
/Db+
C
D8+
T c
ells
E5+6+8_spl_GP33stim- Total TNFa+
Anti-is
ot / G
AD65 (n
=7)
Anti-IL
-1b /
GAD65
(n=1
0)
0
2
4
6
8
% T
NF+
in C
D8+
E5+6+8_spl_GP33stim- Total TNFa+
Anti-is
ot / G
AD65 (n
=7)
Anti-IL
-1b /
GAD65
(n=1
0)*
A
B
12-week follow up %
CD
8+TN
F+
Spl
een
PLN
s
% C
D8+
TNF+
CD8
% g
p33-
31/D
b+
CD
8+ T
cel
ls
IFN
-γ+
CD8
PLN GP33- %CD8+TNF+
E8_Anti
-isot/
GAD (n=5
)
E8_Anti
-IL-1
b/GAD (n
=5)
0
1
2
3
4*
%TN
F+ in
CD
8+
PLN GP33- %CD8+TNF+
E8_Anti
-isot/
GAD (n=5
)
E8_Anti
-IL-1
b/GAD (n
=5)
*
GP33-41 peptide in vitro stimulation
E5+6_Bld_GP33 pentamer
Anti-is
ot / G
AD65 (n
=4)
Anti-IL
-1b /
GAD65
(n=6
)
0
1
2
3
4
% o
f gp3
3-31
/Db+
C
D8
T ce
lls
E5+6_Bld_GP33 pentamer
Blo
od
Isot/GAD Anti-IL-1β/GAD
0102 103 104 105
0102
103
104
105
<APC-A>: CD8
<PE
-A>:
NP
396
pent
amer 3.41
0102 103 104 105
0102
103
104
105
<APC-A>: CD8
<PE
-A>:
NP
396
pent
amer 4.41
Isot/GAD Anti-IL-1β/GAD
Anti-IL1β/GAD
d4pi bld- MFI CXCR3 in CD4+
a-iso
t (n=
7)
a-IL1
b (n=
7)
a-iso
t/GAD (n
=7)
a-IL1
b/GAD (n
=7)
0
1000
2000
3000a-isot (n=7)a-IL1b (n=7)a-isot/GAD (n=7)a-IL1b/GAD (n=7)
MFI
CX
CR
3 in
CD
4+
d4pi bld- MFI CXCR3 in CD4+
a-iso
t (n=
7)
a-IL1
b (n=
7)
a-iso
t/GAD (n
=7)
a-IL1
b/GAD (n
=7)
0
1000
2000
3000a-isot (n=7)a-IL1b (n=7)a-isot/GAD (n=7)a-IL1b/GAD (n=7)
MFI
CX
CR
3 in
CD
4+
d4pi bld- MFI CXCR3 in CD4+
a-iso
t (n=
7)
a-IL1
b (n=
7)
a-iso
t/GAD (n
=7)
a-IL1
b/GAD (n
=7)
0
1000
2000
3000a-isot (n=7)a-IL1b (n=7)a-isot/GAD (n=7)a-IL1b/GAD (n=7)
MFI
CX
CR
3 in
CD
4+
d4pi bld- MFI CXCR3 in CD4+
a-iso
t (n=
7)
a-IL1
b (n=
7)
a-iso
t/GAD (n
=7)
a-IL1
b/GAD (n
=7)
0
1000
2000
3000a-isot (n=7)a-IL1b (n=7)a-isot/GAD (n=7)a-IL1b/GAD (n=7)
MFI
CX
CR
3 in
CD
4+
0102 103 104 105
0102
103
104
105
<PE-Texas Red-A>: CD8
<Ale
xa F
luor
700
-A>:
IFN
g
0.705
0102 103 104 105
0102
103
104
105
<PE-Texas Red-A>: CD8
<Ale
xa F
luor
700
-A>:
IFN
g
1.13
0102 103 104 105
0102
103
104
105
<PE-Texas Red-A>: CD8<A
lexa
Flu
or 7
00-A
>: IF
Ng
4.62
0102 103 104 105
0102
103
104
105
<PE-Texas Red-A>: CD8
<Ale
xa F
luor
700
-A>:
IFN
g
6.37
Pagni et al. Fig 4.
Isot/GAD
Page 29 of 35 Diabetes

Weeks post-onset CD11b infiltration, 12wks p.t.s
Anti-iso
t / G
AD65
(n=3
; 39i)
Anti-IL-1b / G
AD65
(n=3
; 20i)
Anti-iso
t (n=
2; 56i)
Anti-IL-1b (n=1
; 23i)
0
20
40
60
80
100no infiltrationmild infiltrationheavy infiltration
ns
# mice: 3 and 3, resp. ; # counted islets: 39 and 20, resp.
% o
f counte
d isle
ts
CD4 infiltration, 12wks p.t.s
Anti-iso
t / G
AD65
(n=3
; 36i)
Anti-IL-1b / G
AD65
(n=3
; 13i)
Anti-iso
t (n=
2; 39i)
Anti-IL-1b (n=1
; 13i)
0
20
40
60
80
100no infiltrationmild infiltrationheavy infiltration
# mice:
% o
f counte
d isle
ts
CD8 infiltration, 12wks p.t.s
Anti-iso
t / G
AD65
(n=3
; 31i)
Anti-IL-1b / G
AD65
(n=3
; 15i)
Anti-iso
t (n=
2; 44i)
Anti-IL-1b (n=1
; 16i)
0
20
40
60
80
100no infiltrationmild infiltrationheavy infiltration
# mice:
% o
f counte
d isle
ts
%CD8+ Infiltration
anti-i
sotyp
e + G
AD (n=3
, 43 i
slets)
anti I
L1B +
GAD (n=3
, 42 i
slets)
0
20
40
60
80
100no infiltration mild infiltrationheavy infiltration
% o
f cou
nted
isle
ts
Cel
ls
CD
4+
CD
8+
CD11b insulin
No infiltration
Mild (peri) infiltration
Heavy (intra) infiltration
*
Ant
i-IL-
1β
Ab/
GA
D65
CD
11b+
5 12 CD11b infiltration
Anti-iso
t / G
AD65
Anti-IL-1b / G
AD65
Anti-iso
t
Anti-IL-1b
0
20
40
60
80
100no infiltrationmild infiltrationheavy infiltration
ns
# mice: 2 and 4, resp. ; # counted islets: 16 and 61, resp.
% o
f counte
d isle
ts
CD8 infiltration
Anti-iso
t / G
AD65
Anti-IL-1b / G
AD65
Anti-iso
t
Anti-IL-1b
0
20
40
60
80
100no infiltrationmild infiltrationheavy infiltration
# mice: 3 and 3, resp. ; # counted islets: 43 and 42, resp.
% o
f counte
d isle
ts
CD4 infiltration
Anti-iso
t / G
AD65
Anti-IL-1b / G
AD65
Anti-iso
t
Anti-IL-1b
0
20
40
60
80
100no infiltrationmild infiltrationheavy infiltration
# mice: 5 and 5, resp. ; # counted islets: 63 and 111, resp.
% o
f counte
d isle
ts*
Ant
i-IL-
1β
Ab/
GA
D65
A B
*
Ant
i-IL-
1β
Ab/
GA
D65
*
CD11b infiltration
Anti-iso
t / G
AD65
Anti-IL-1b / G
AD65
Anti-iso
t
Anti-IL-1b
0
20
40
60
80
100no infiltrationmild infiltrationheavy infiltration
**
# mice: 3, resp. ; # counted islets: 43iso, 31IL1, 47isoGAD, 29IL1GAD
% o
f counte
d isle
ts
CD8 infiltration
Anti-iso
t / G
AD65
Anti-IL-1b / G
AD65
Anti-iso
t
Anti-IL-1b
0
20
40
60
80
100
no infiltrationmild infiltrationheavy infiltration
# mice: 3 and 3, resp. ; # counted islets: 84 and 47, resp.
% o
f counte
d isle
ts
CD4 infiltration
Anti-iso
t / G
AD65
Anti-IL-1b / G
AD65
Anti-iso
t
Anti-IL-1b
0
20
40
60
80
100
no infiltrationmild infiltrationheavy infiltration
# mice: 5 and 5, resp. ; # counted islets: 63 and 111, resp.
% o
f counte
d isle
ts
1
Isot
/ G
AD
65
Ant
i-IL-
1β
Ab/
GA
D65
Weeks post-onset
12
% C
D4+
CD
25+ F
oxp3
+
1
Pc- %CD11b+
E568_
Anti-is
ot/GAD (n
=7)
E568_
Anti-IL
-1b/G
AD (n=1
0)0
20
40
60
80
0.0520
%C
D11
bhigh
Pc- %CD11b+0.0520
Pc- % total CD8+
E6_Anti
-isot/
GAD (n=7
)
E6_Anti
-IL-1
b/GAD (n
=10)
0
10
20
30
40
E6_Anti-isot/GAD (n=7)E6_Anti-IL-1b/GAD (n=10)
*
% C
D8+
Pc- % total CD8+
Pc- %CD4+
E568_
Anti-is
ot/GAD (n
=7)
E568_
Anti-IL
-1b/G
AD (n=1
0)0
5
10
15
20
25
%C
D4+
Pc- %CD4+
% C
D4+
%
CD
8+
% C
D11
bhig
h
Pagni et al. Fig 5.
Isot
/ G
AD
65
Isot
/ G
AD
65
Isot
/ G
AD
65
E5+6+8_Pc- %CD25+Foxp3+
E5+6+
8_Anti
-isot/
GAD (n=6
)
E5+6+
8_Anti
-IL-1
b/GAD (n
=10)
0
10
20
30
Within these cells, similar MFI for CTLA-4, Helios, PD-1, Neuropilin-1 and LAP
%C
D25
+Fox
p3+
in C
D4+
E5+6+8_Pc- %CD25+Foxp3+
Page 30 of 35Diabetes

A B *
1
Pagni et al. Fig 6.
Isot/GAD
12-week follow up
BGV at 12wks vs %CD11b in Pc (cured vs sick)
%CD8+
(isot/
GAD): Cur
ed
%CD8+
(isot/
GAD): Sick
%CD8+
(CT):
Cured
%CD8+
(CT):
Sick
0
10
20
30
% C
D8+
in p
ancr
eas
a-IL-1β/GAD
Data 1
200 300 400 500 6000
20
40
60
%CD11b+ in Pc (CT)%CD11b+ in Pc (isot/GAD)
BGV at 12 wks post-onset
% C
D11
bhigh
in
pan
crea
s
Pearson r95% confidence intervalP value (two-tailed)
%CD11b+ in Pc (CT)0.77990.2401 to 0.95130.0132
%CD11b+ in Pc (isot/GAD)0.2711-0.6057 to 0.85060.5564
Isot/GAD Pearson r = 0.27 P value = 0.55
aIL-1β/GAD Pearson r = 0.78 *P value = 0.01
Isot/GAD Pearson r = -0.36 P value = 0.43
aIL-1β/GAD Pearson r = 0.38 P value = 0.32
Isot/GAD Pearson r = -0.59 P value = 0.16
aIL-1β/GAD Pearson r = 0.27 P value = 0.48
Data 1
200 300 400 500 6000
20
40
60
%CD11b+ in Pc (CT)%CD11b+ in Pc (isot/GAD)
BGV at 12 wks post-onset
% C
D11
bhigh
in
pan
crea
s
Pearson r95% confidence intervalP value (two-tailed)
%CD11b+ in Pc (CT)0.77990.2401 to 0.95130.0132
%CD11b+ in Pc (isot/GAD)0.2711-0.6057 to 0.85060.5564
Data 1
200 300 400 500 6000
20
40
60
%CD11b+ in Pc (CT)%CD11b+ in Pc (isot/GAD)
BGV at 12 wks post-onset
% C
D11
bhigh
in
pan
crea
s
Pearson r95% confidence intervalP value (two-tailed)
%CD11b+ in Pc (CT)0.77990.2401 to 0.95130.0132
%CD11b+ in Pc (isot/GAD)0.2711-0.6057 to 0.85060.5564
BGV at 12wks vs %CD11b in Pc (cured vs sick)
%CD11
b+ (is
ot/GAD):
Cured
%CD11
b+ (is
ot/GAD):
Sick
%CD11
b+ (C
T): Cur
ed
%CD11
b+ (C
T): Sick
0
20
40
60
% C
D11
bhigh
in
pan
crea
s
C D
E F BGV at 12wks vs %CD11b in Pc (cured vs sick)
%CD25
+Fox
p3+ (
isot/G
AD): Cur
ed
%CD25
+Fox
p3+ (
isot/G
AD): Sick
%CD25
+Fox
p3+ (
CT): Cur
ed
%CD25
+Fox
p3+ (
CT): Sick
0
10
20
30
% C
D25
+ Fox
p3+
in
CD
4+ in
pan
crea
s
Data 1
200 300 400 500 6000
20
40
60
%CD11b+ in Pc (CT)%CD11b+ in Pc (isot/GAD)
Pearson r95% confidence intervalP value (two-tailed)
%CD11b+ in Pc (CT)0.77990.2401 to 0.95130.0132
%CD11b+ in Pc (isot/GAD)0.2711-0.6057 to 0.85060.5564
BGV at 12 wks post-onset%
CD
11bhi
gh
in p
ancr
eas
Data 1
200 300 400 500 6000
20
40
60
%CD11b+ in Pc (CT)%CD11b+ in Pc (isot/GAD)
Pearson r95% confidence intervalP value (two-tailed)
%CD11b+ in Pc (CT)0.77990.2401 to 0.95130.0132
%CD11b+ in Pc (isot/GAD)0.2711-0.6057 to 0.85060.5564
BGV at 12 wks post-onset
% C
D11
bhigh
in
pan
crea
s
Data 1
200 300 400 500 6000
20
40
60
%CD11b+ in Pc (CT)%CD11b+ in Pc (isot/GAD)
Pearson r95% confidence intervalP value (two-tailed)
%CD11b+ in Pc (CT)0.77990.2401 to 0.95130.0132
%CD11b+ in Pc (isot/GAD)0.2711-0.6057 to 0.85060.5564
BGV at 12 wks post-onset
% C
D11
bhigh
in
pan
crea
sData 1
200 300 400 500 6000
10
20
30
Pearson r95% confidence intervalP value (two-tailed)
%CD8+ in Pc (CT)-0.2713-0.7927 to 0.47930.4802
%CD8+ in Pc (isot/GAD)-0.5884-0.9296 to 0.29590.1646
BGV at 12 wks post-onset
% C
D8+
in p
ancr
eas
Data 1
200 300 400 500 6000
20
40
60
%CD11b+ in Pc (CT)%CD11b+ in Pc (isot/GAD)
Pearson r95% confidence intervalP value (two-tailed)
%CD11b+ in Pc (CT)0.77990.2401 to 0.95130.0132
%CD11b+ in Pc (isot/GAD)0.2711-0.6057 to 0.85060.5564
BGV at 12 wks post-onset
% C
D11
bhigh
in
pan
crea
s
Data 1
200 300 400 500 6000
10
20
30
%CD4+25+Foxp3+ in Pc (CT)%CD4+25+Foxp3+ in Pc (isot/GAD
Pearson r95% confidence intervalP value (two-tailed)
%CD4+25+Foxp3+ in Pc (CT)0.3783-0.3819 to 0.83320.3155
%CD4+25+Foxp3+ in Pc (isot/GAD-0.3609-0.8759 to 0.53870.4265
BGV at 12 wks post-onset
% C
D25
+ Fox
p3+
in C
D4+
in p
ancr
eas
Page 31 of 35 Diabetes

Page 32 of 35Diabetes

Page 33 of 35 Diabetes

#Ghanashyam Sarikonda, Sowbarnika Sachithanantham, Yulia Manenkova, Tinalyn Kupfer, Amanda Posgai,
Clive Wasserfall, Philip Bernstein, Laura Straub, Philippe P. Pagni, Darius Schneider, Teresa Rodriguez Calvo,
Marilyne Coulombe, Kevan Herold, Ronald G. Gill, Mark Atkinson, Gerald Nepom, Mario Ehlers, Teodora
Staeva, Hideki Garren, Lawrence Steinman, Andrew C. Chan, Matthias von Herrath. Transient B-Cell
Depletion with Anti-CD20 in Combination with Proinsulin DNA Vaccine or Oral Insulin: Immunologic Effects
and Efficacy in NOD Mice. PLoS One. 2013;8(2):e54712. doi: 10.1371/journal.pone.0054712. Epub 2013 Feb
6.
Page 34 of 35Diabetes

Page 35 of 35 Diabetes