6 min Walking Test -...
40
6 min Walking Test: η σημασία του στην κλινική πράξη Καρακώστας Γεώργιος Διευθυντής Καρδιολογικής Κλινικής, Γ.Ν. Κιλκίς
Transcript of 6 min Walking Test -...

6 min Walking Test:η σημασία του στην κλινική πράξη
Καρακώστας ΓεώργιοςΔιευθυντής Καρδιολογικής Κλινικής, Γ.Ν. Κιλκίς
Definition
The 6 minute walking test (6MWT) is a
sub-maximal exercise test used to evaluate
the functional capacity in patients with
cardiovascular and pulmonary diseases.
Background
• The 6MWT was first described by Balke in 1963, mostly to evaluatethe exercise capacity in healthy populations.
• For years it was used to evaluate patients with chronic respiratorydiseases.
• Guyatt in 1985 and Lipkin in 1986 reported that the 6MWT canidentify the most compromised patients suffering from heartfailure.
• Bittner in 1993 reported that the distance walked during the6MWT is a strong and independent predictor of mortality andmorbidity in patients with left ventricular dysfunction.
Indications Evaluation of functional capacity Chronic obstructive pulmonary disease Heart failure Cystic fibrosis Peripheral vascular disease Older subjects
Evaluation of effects of therapeutic interventions Chronic obstructive pulmonary disease Heart failure Lung resection Lung volume reduction surgery Pulmonary rehabilitation Pulmonary hypertension
Prognostic stratification Heart failure Chronic obstructive pulmonary disease Primary pulmonary hypertension
Contraindications for walking tests (1) Absolute Acute myocardial myocardial infarction (3-5 days)
Unstable Angina
Exercise induced uncontrolled arrythmias
Active endocarditis, Acute myocarditis or pericarditis
Uncontrolled heart failure and pulmonary oedema
Acute pulmonary embolus
Thrombosis of lower extremeties
Suspected dissecting aneurysm
Acute respiratory failure
Acute non cardiopulmonary disorder that may affect exercise performance or be aggravated by exercise (i.e. infection, renal failure, thyrotoxicosis)
Mental impairment leading to inability to cooparate
Contraindications for walking tests (2)
Relative Resting heart rate > 120 bpm
Systolic blood pressure > 180 mmHg
Diastolic blood pressure > 100 mmHg
Left main coronary stenosis or its equivalent
Severe aortic stenosis
Tachyarrhythmias or Bradyarrhythmias
Advanced pregnancy
Severe orthopaedic impairment that prevents walking
ERS/ATS (2014)
Indentifying a space for the 6MWT• A 30 meters long corridor, straight, with no obstacles with a level
floor.
• The space should be quiet enough for the participant to clearlyhear your instructions.
• Any clock or timers should not be visible to the participant.
• A chair should be available for the participant to test during orafter the test.
• There should be easy access to a telephone and appropriateequipment in case of emergency. The person administrating thetest is not necessarily a physician, but he should be trained inbasic life support.
Required Equipment
• Two cones to mark the turning points at the either end
• Stopwatch or countdown timer
• Measuring tape
• Pen and paper
Before the test
• The participant should wear comfortable clothing and appropriate footwear.
• He should continue with his normal medical treatment.
• If he usually walks with an aid, he should use it during the test.
• If he usually uses a GTN spray, chronic oxygen or any other inhaler, he should have them with him and use them during the test if necessary.
Instructions• The text approved by the ATS is the following:
“The object of this test is to walk as far as possible for 6 minutes. You
will walk back and forth in this hallway. Six minutes is a long time to
walk, so you will be exerting yourself. You will probably get out of
breath or become exhausted. You are permitted to slow down, to stop,
and to rest as necessary. You may lean against the wall while resting,
but resume walking as soon as you are able. You will be walking back
and forth around the cones. You should pivot briskly around the cones
and continue back the other way without hesitation. Now I’m going to
show you. Please watch the way I turn without hesitation. Remember
that the object is to walk AS FAR AS POSSIBLE for 6 minutes, but don’t
run or jog. Start now, or whenever you are ready.”ATS 2002
Performing the 6MWT
• Set the timer to 6 minutes.
• Demonstrate by walking one lap yourself.
• Start the timer as soon as the participant starts walking
• Record the number of laps.
• Record the additional distance walked from the final
partial lap.
• Calculate the total distance.
Reasons for immediate stopping
• Chest pain
• Intolerable dyspnea
• Leg cramps
• Staggering
• Diaphoresis
• Pale or ashen appearance
ATS 2002
Encouragement
• Encouragement significantly increases the distance
walked.
• Participants are told when 2, 4, and 6 minutes have
elapsed.
• Words like ‘‘keep up the good work’’ or ‘‘you’re doing
fine’’ are provided with even voice at 1 minute
intervals.
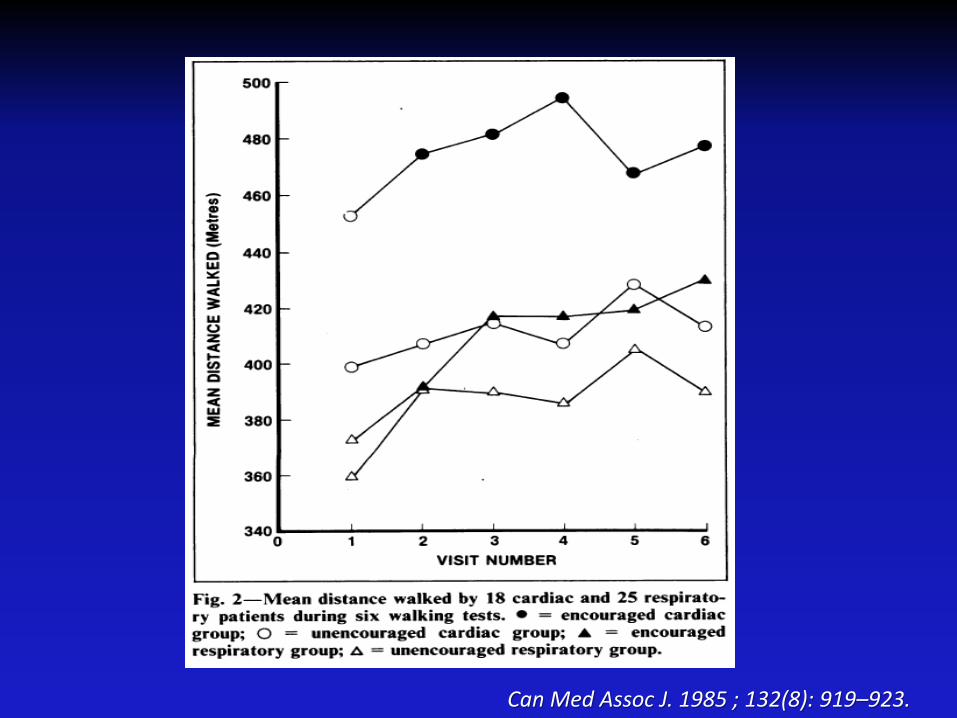
Can Med Assoc J. 1985 ; 132(8): 919–923.
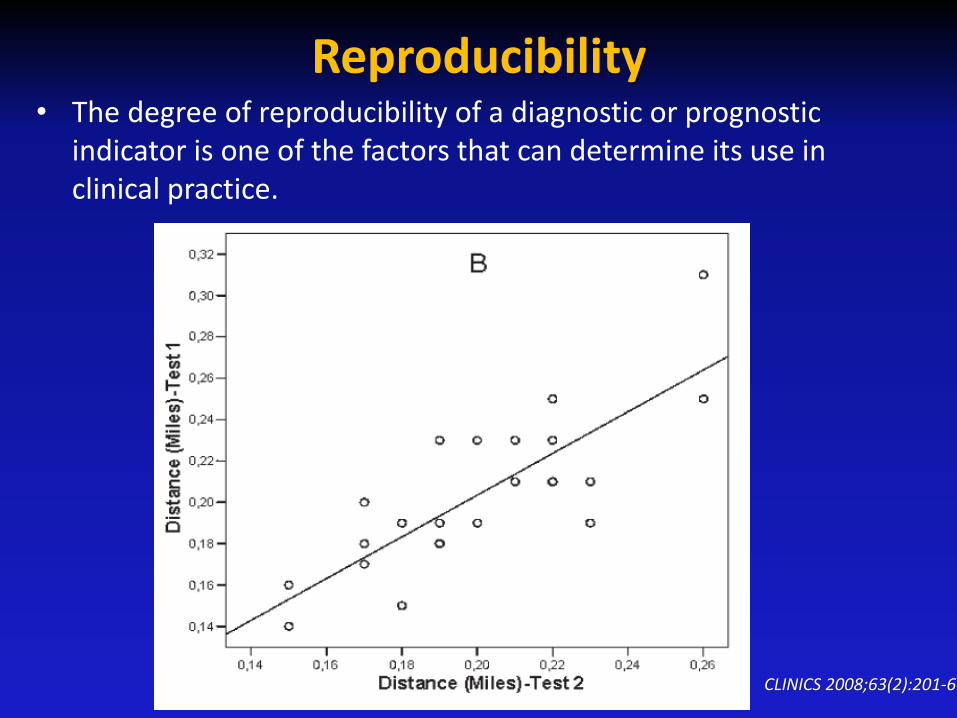
Reproducibility• The degree of reproducibility of a diagnostic or prognostic
indicator is one of the factors that can determine its use in clinical practice.
CLINICS 2008;63(2):201-6
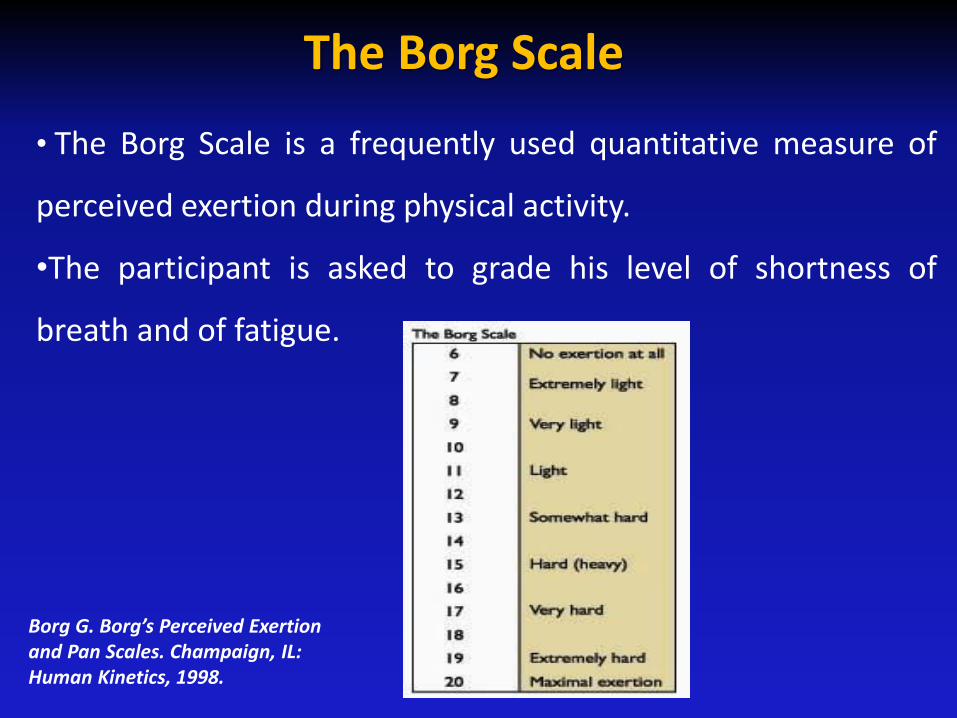
The Borg Scale
• The Borg Scale is a frequently used quantitative measure of
perceived exertion during physical activity.
•The participant is asked to grade his level of shortness of
breath and of fatigue.
Borg G. Borg’s Perceived Exertion and Pan Scales. Champaign, IL: Human Kinetics, 1998.
Advantages of the method
• Easy to administer
• Easy to repeat
• Does not require expensive equipment
• Does not require advanced training for technicians
• Has a good correlation with objective measures of effort
tolerance, such as oxygen uptake at the peak of exercise
• Well tolerated because it is similar to the activities of
daily living
Limitations of the method
• Does not determine peak oxygen uptake
• Does not provide specific information on the function of
each of the different organs and systems involved in
exercise
• Does not diagnose the cause of dyspnea on exertion
• Does not evaluate the causes or mechanisms of exercise
limitation
• Results can be affected by a number of factors ATS 2002
6MWT sources of Variability (1)
Factors reducing the 6MWT :
Shorter height
Older age
Higher body weight
Female sex
Impaired cognition
A shorter corridor
Pulmonary disease
Cardiovascular disease
Musculoskeletal disorders
6MWT sources of Variability (2)
Factors increasing the 6MWT :
Taller height
Male sex
Encouragement
A patient who has previously performed the test
Medication for a disabling disease taken just before the test
Oxygen supplementation in patients with exercise-induced hypoxemia
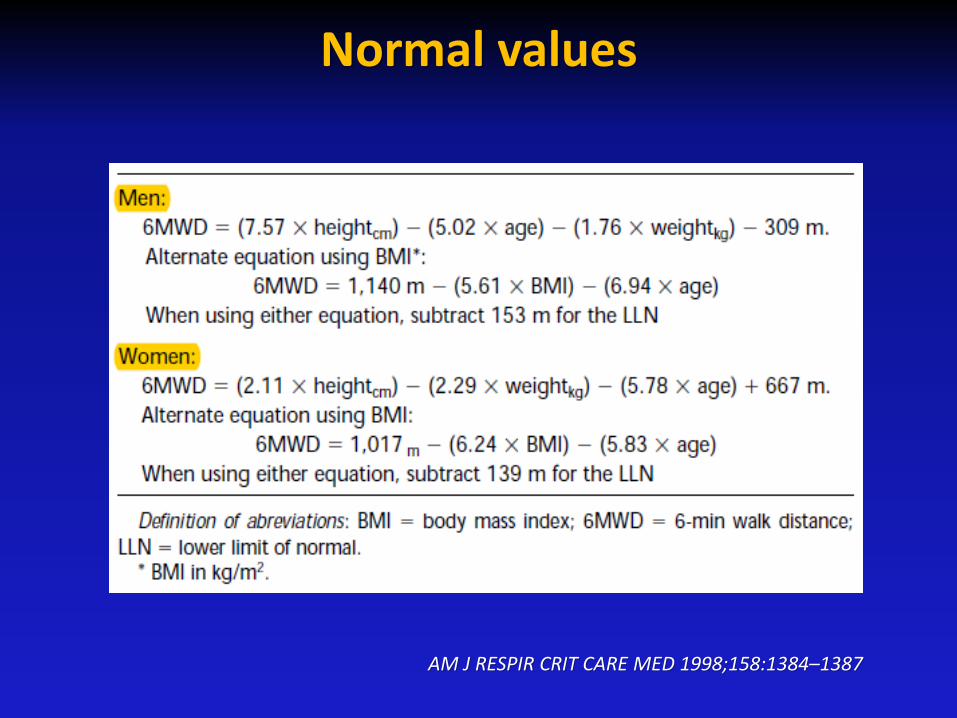
Normal values
AM J RESPIR CRIT CARE MED 1998;158:1384–1387
6MWT
• Evaluation of functional capacity
• Evaluation of effects of therapeutic interventions
• Prognostic stratification
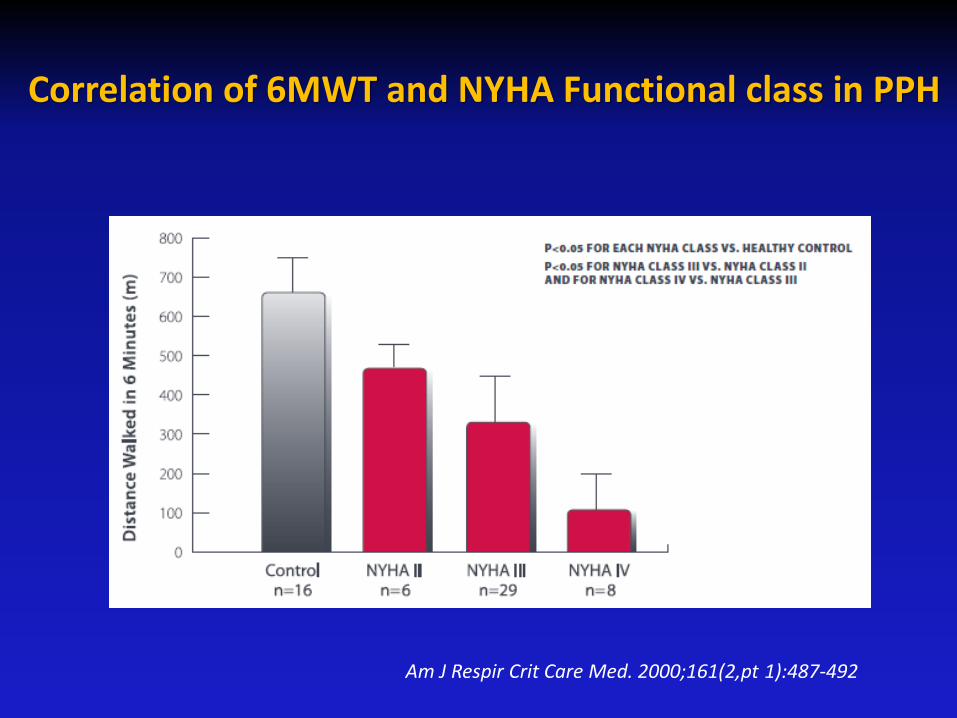
Correlation of 6MWT and NYHA Functional class in PPH
Am J Respir Crit Care Med. 2000;161(2,pt 1):487-492
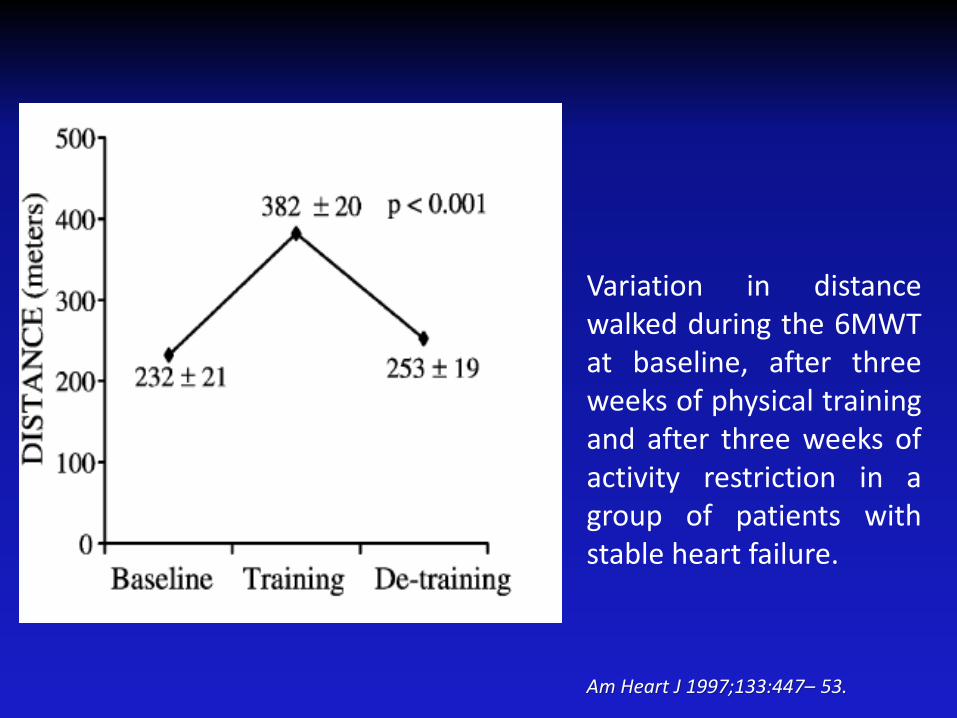
Am Heart J 1997;133:447– 53.
Variation in distancewalked during the 6MWTat baseline, after threeweeks of physical trainingand after three weeks ofactivity restriction in agroup of patients withstable heart failure.
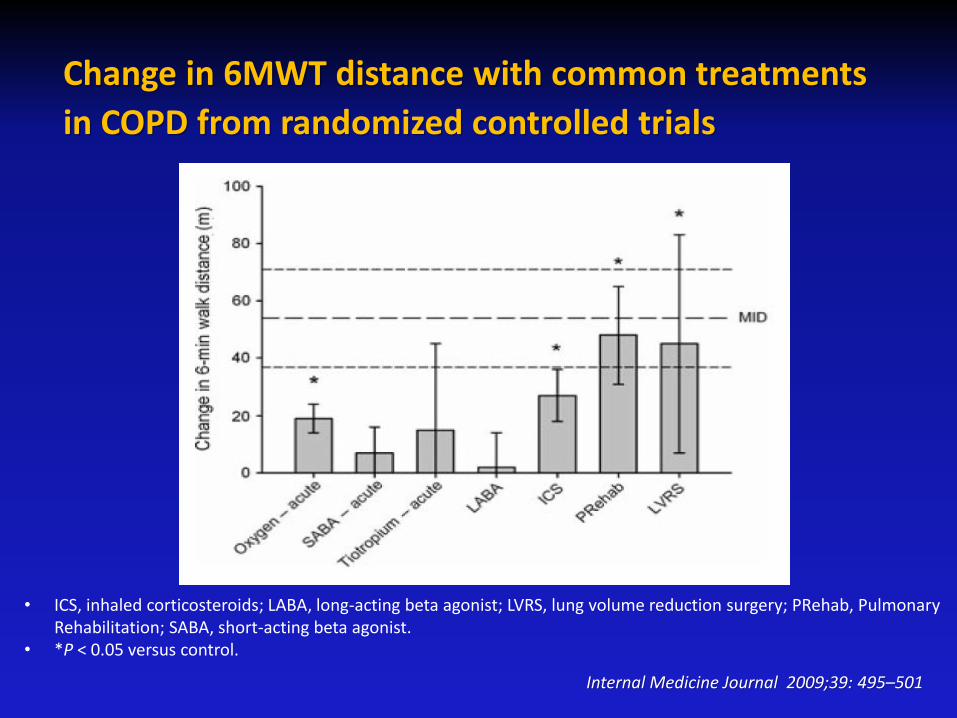
Change in 6MWT distance with common treatments
in COPD from randomized controlled trials
• ICS, inhaled corticosteroids; LABA, long-acting beta agonist; LVRS, lung volume reduction surgery; PRehab, Pulmonary Rehabilitation; SABA, short-acting beta agonist.
• *P < 0.05 versus control.
Internal Medicine Journal 2009;39: 495–501
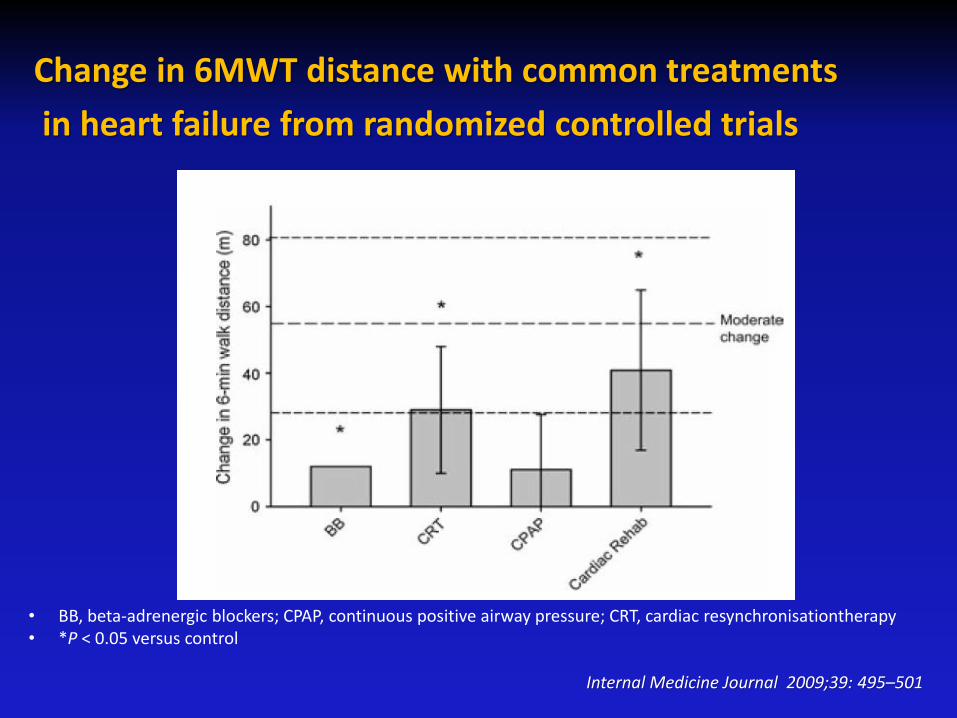
Change in 6MWT distance with common treatments
in heart failure from randomized controlled trials
• BB, beta-adrenergic blockers; CPAP, continuous positive airway pressure; CRT, cardiac resynchronisationtherapy• *P < 0.05 versus control
Internal Medicine Journal 2009;39: 495–501
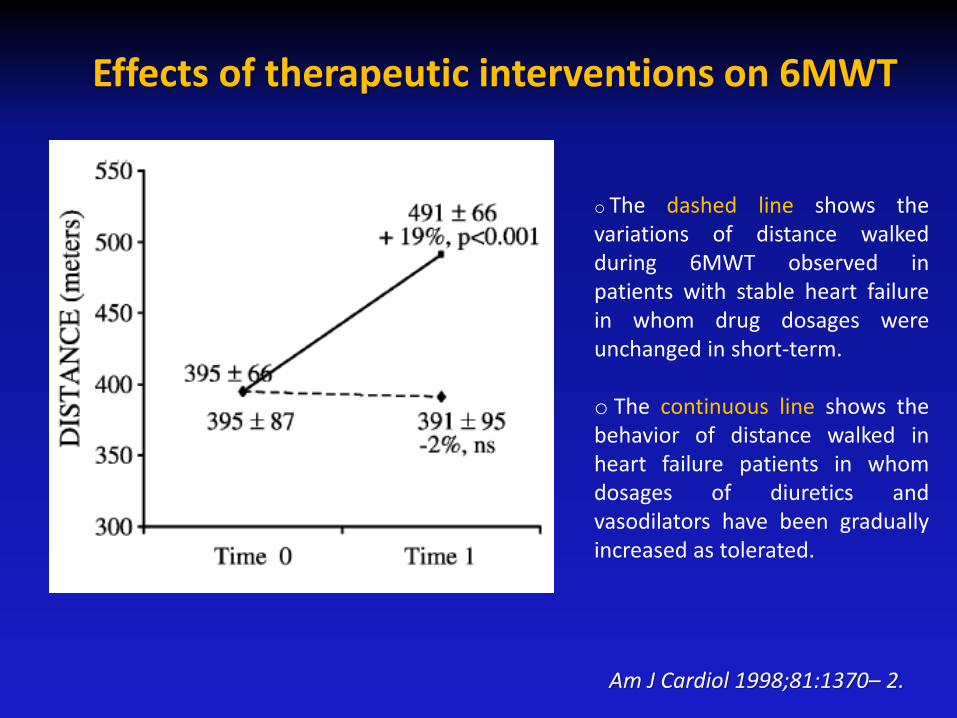
Effects of therapeutic interventions on 6MWT
o The dashed line shows thevariations of distance walkedduring 6MWT observed inpatients with stable heart failurein whom drug dosages wereunchanged in short-term.
o The continuous line shows thebehavior of distance walked inheart failure patients in whomdosages of diuretics andvasodilators have been graduallyincreased as tolerated.
Am J Cardiol 1998;81:1370– 2.
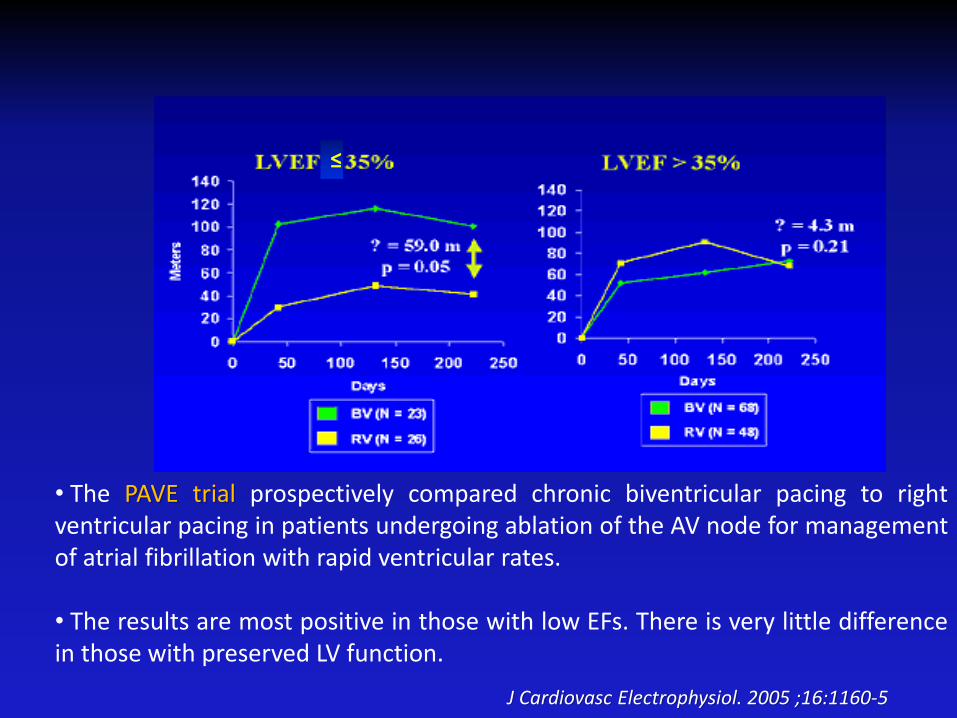
• The PAVE trial prospectively compared chronic biventricular pacing to rightventricular pacing in patients undergoing ablation of the AV node for managementof atrial fibrillation with rapid ventricular rates.
• The results are most positive in those with low EFs. There is very little differencein those with preserved LV function.
≤
J Cardiovasc Electrophysiol. 2005 ;16:1160-5
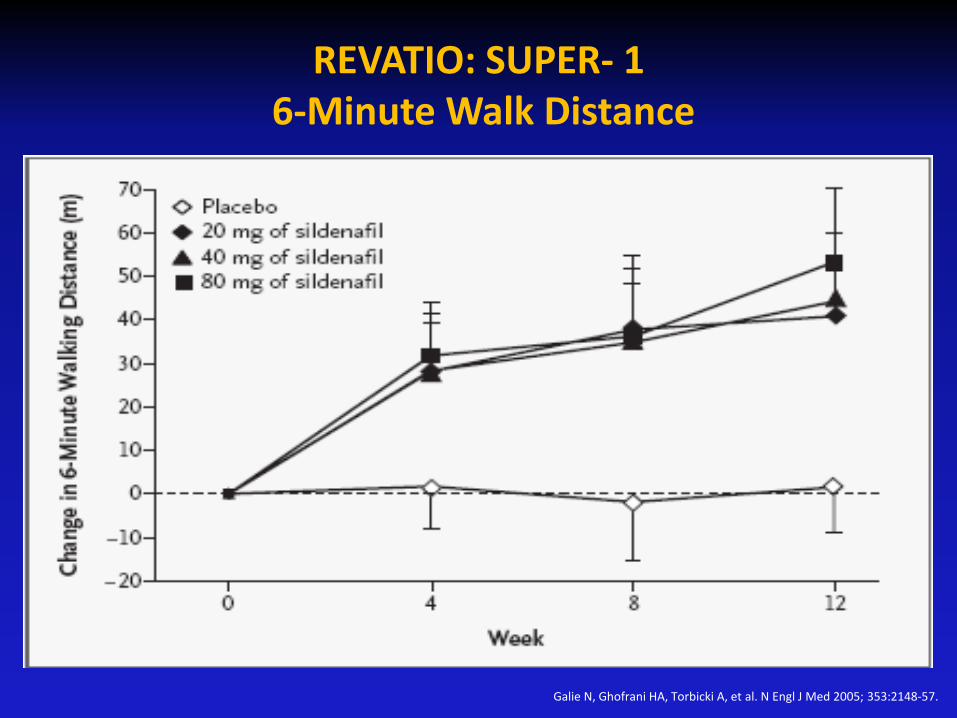
Galie N, Ghofrani HA, Torbicki A, et al. N Engl J Med 2005; 353:2148-57.
REVATIO: SUPER- 16-Minute Walk Distance
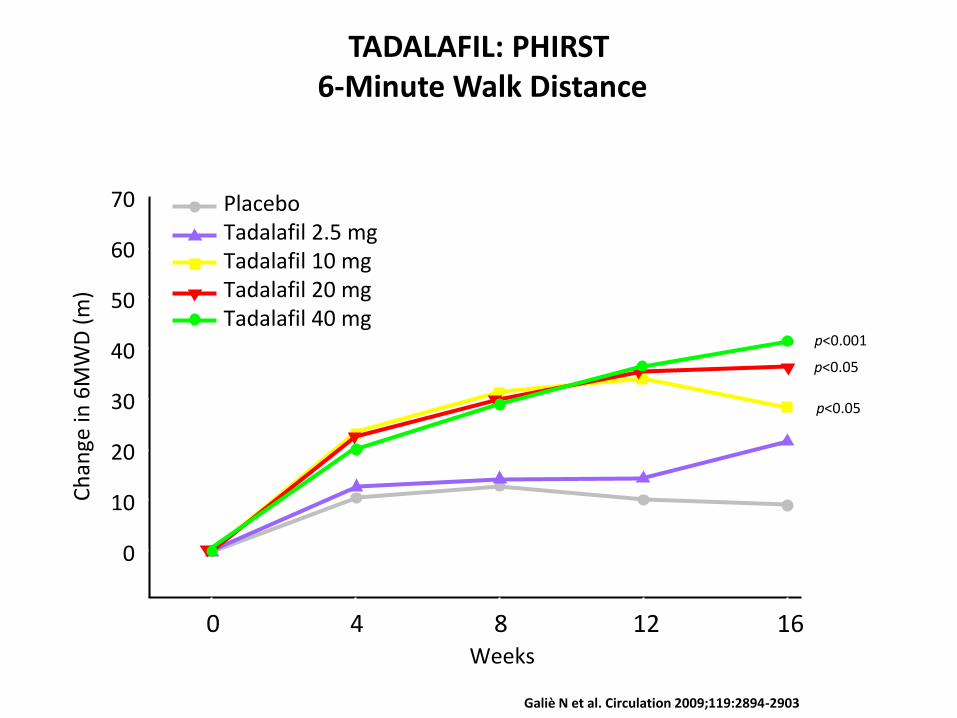
Galiè N et al. Circulation 2009;119:2894-2903
TADALAFIL: PHIRST6-Minute Walk Distance
PlaceboTadalafil 2.5 mgTadalafil 10 mgTadalafil 20 mgTadalafil 40 mg
70
60
50
40
30
20
10
0
4 8 12 160
Ch
ange
in 6
MW
D (
m)
Weeks
p<0.001
p<0.05
p<0.05
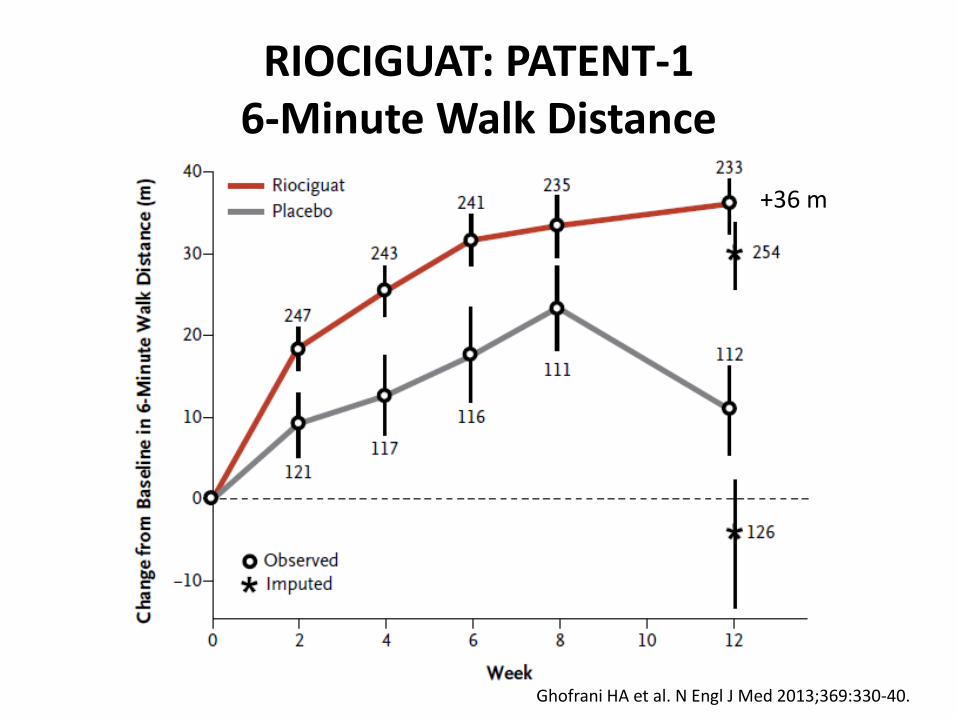
RIOCIGUAT: PATENT-16-Minute Walk Distance
Ghofrani HA et al. N Engl J Med 2013;369:330-40.
+36 m
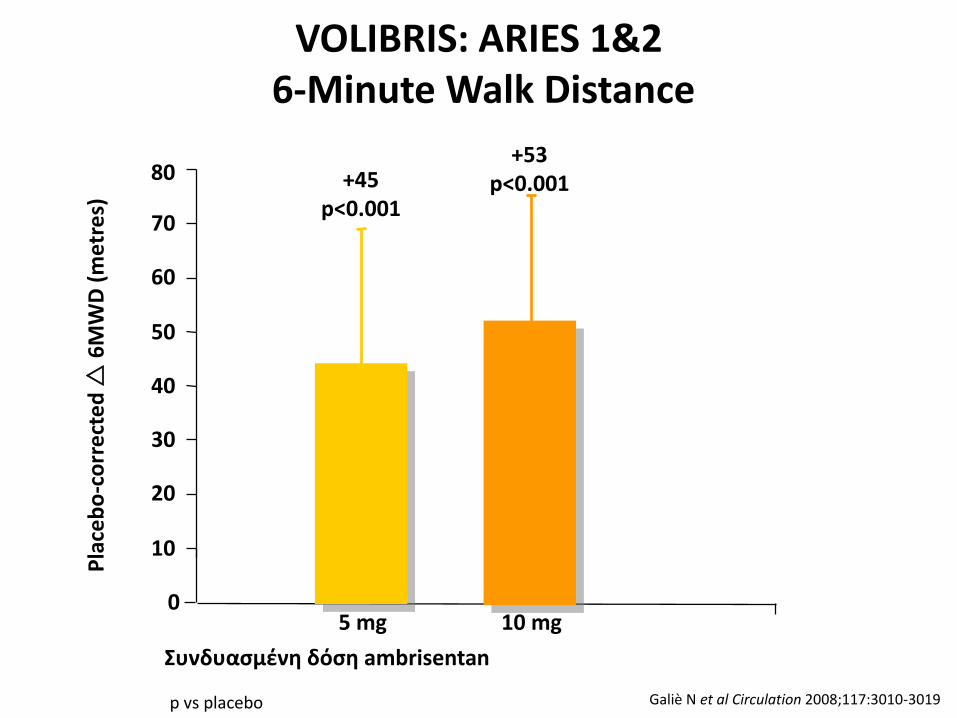
VOLIBRIS: ARIES 1&26-Minute Walk Distance
p vs placebo
20
0
10
30
40
50
60
70
80 +45p<0.001
+53p<0.001
5 mg 10 mg
Συνδυασμένη δόση ambrisentan
Pla
ceb
o-c
orr
ect
ed
6
MW
D (
me
tre
s)
Galiè N et al Circulation 2008;117:3010-3019
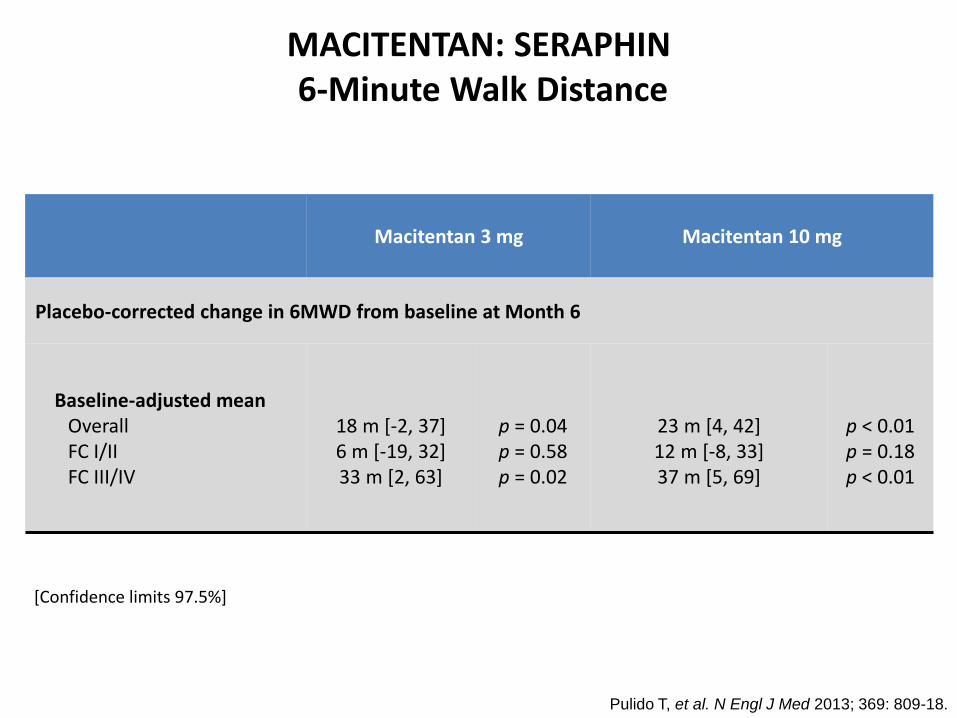
MACITENTAN: SERAPHIN6-Minute Walk Distance
Macitentan 3 mg Macitentan 10 mg
Placebo-corrected change in 6MWD from baseline at Month 6
Baseline-adjusted meanOverallFC I/IIFC III/IV
18 m [-2, 37]6 m [-19, 32]33 m [2, 63]
p = 0.04p = 0.58p = 0.02
23 m [4, 42]12 m [-8, 33]37 m [5, 69]
p < 0.01p = 0.18p < 0.01
[Confidence limits 97.5%]
Pulido T, et al. N Engl J Med 2013; 369: 809-18.Pulido T, et al. N Engl J Med 2013; 369: 809-18.Pulido T, et al. N Engl J Med 2013; 369: 809-18.
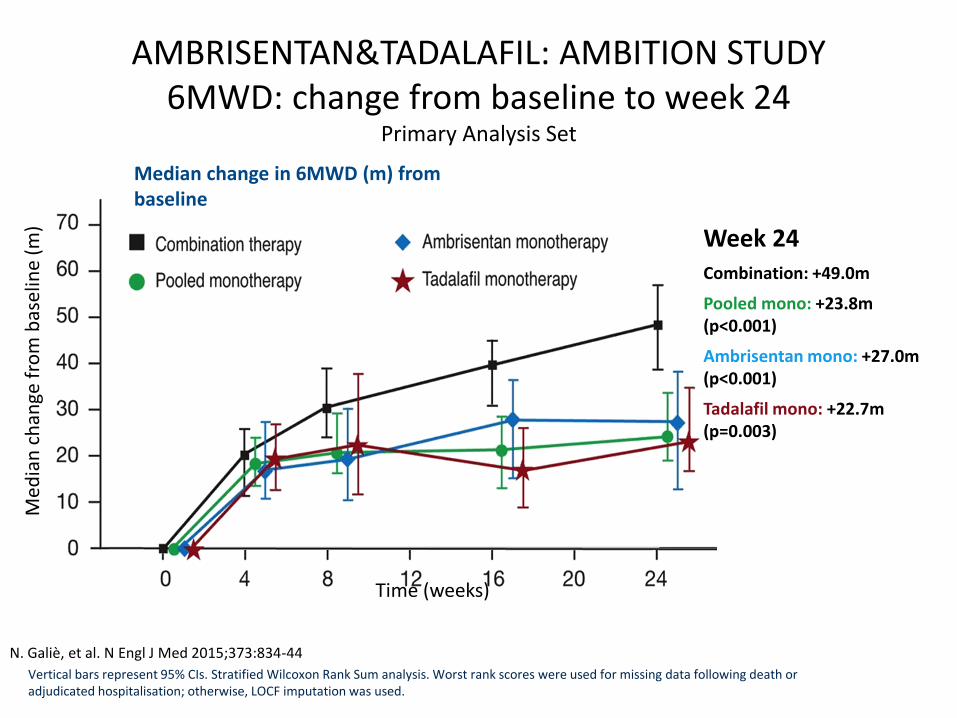
Median change in 6MWD (m) from baseline
Vertical bars represent 95% CIs. Stratified Wilcoxon Rank Sum analysis. Worst rank scores were used for missing data following death or adjudicated hospitalisation; otherwise, LOCF imputation was used.
Week 24Combination: +49.0m
Pooled mono: +23.8m (p<0.001)
Ambrisentan mono: +27.0m (p<0.001)
Tadalafil mono: +22.7m (p=0.003)
Med
ian
ch
ange
fro
m b
asel
ine
(m)
Time (weeks)
AMBRISENTAN&TADALAFIL: AMBITION STUDY 6MWD: change from baseline to week 24
Primary Analysis Set
N. Galiè, et al. N Engl J Med 2015;373:834-44
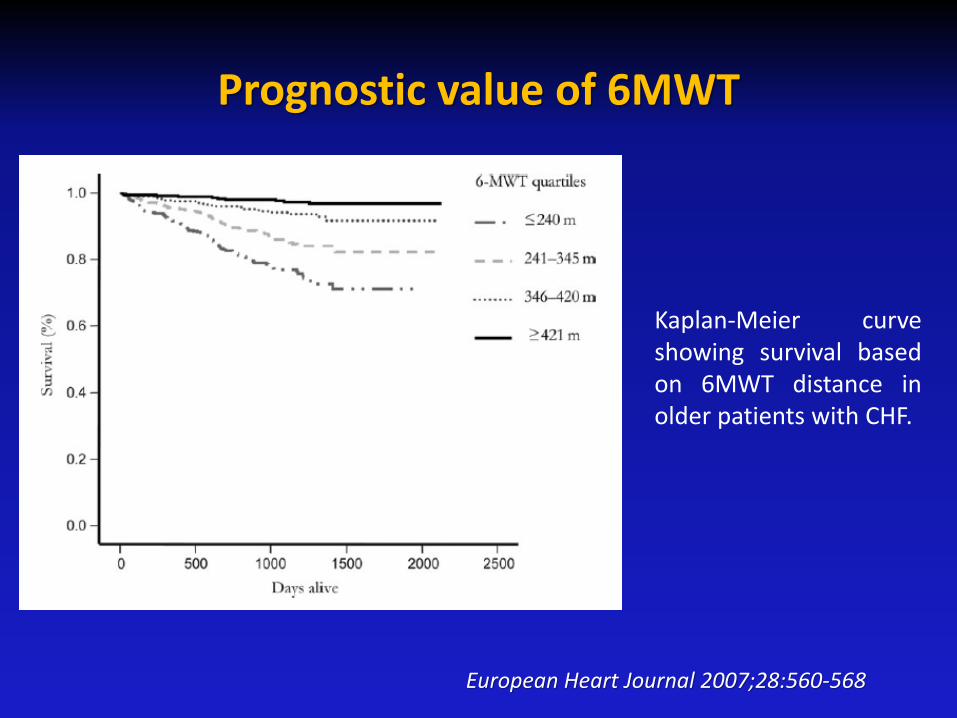
Prognostic value of 6MWT
European Heart Journal 2007;28:560-568
Kaplan-Meier curveshowing survival basedon 6MWT distance inolder patients with CHF.
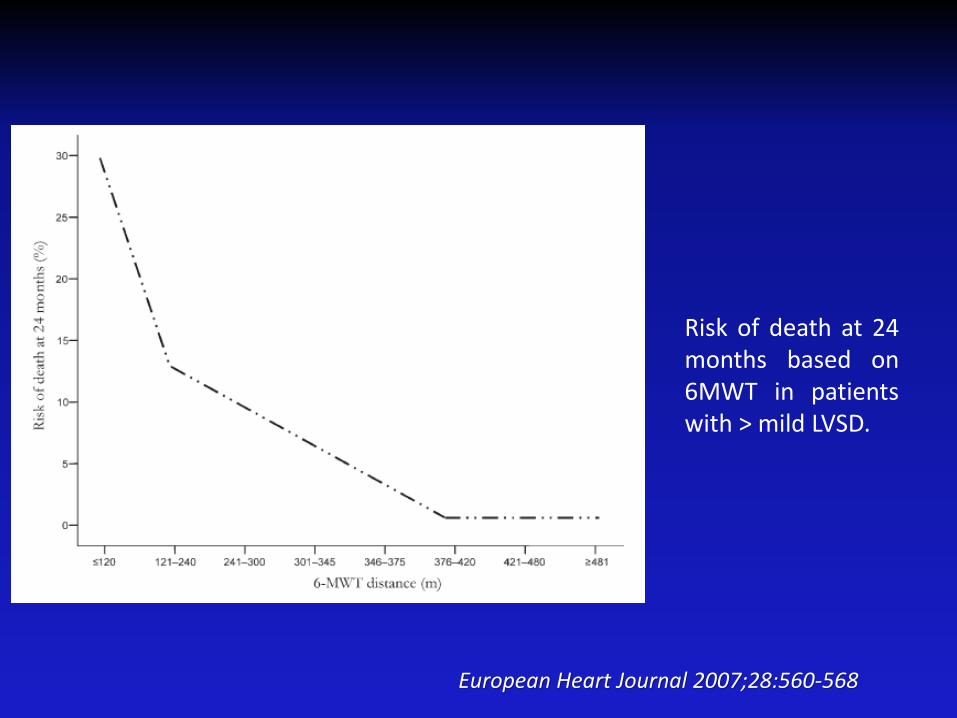
European Heart Journal 2007;28:560-568
Risk of death at 24months based on6MWT in patientswith > mild LVSD.
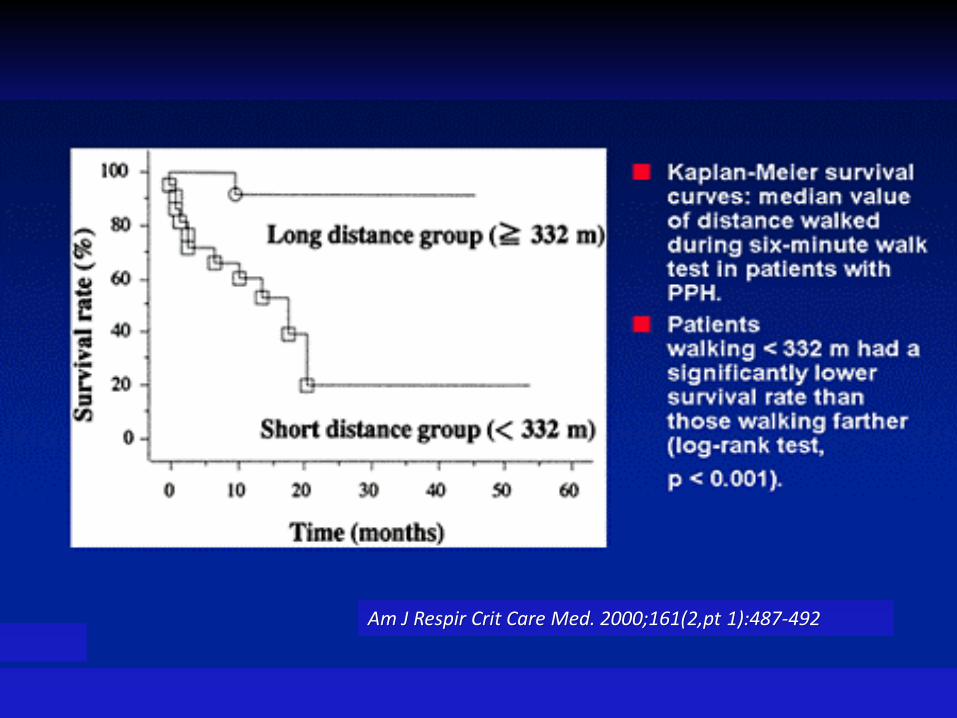
Am J Respir Crit Care Med. 2000;161(2,pt 1):487-492
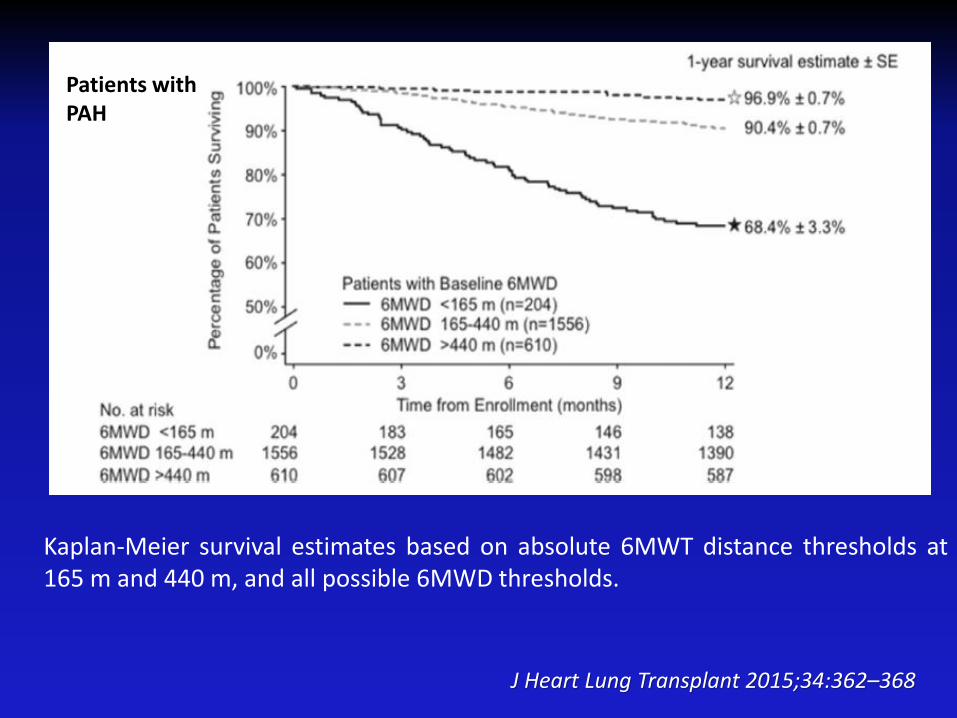
J Heart Lung Transplant 2015;34:362–368
Kaplan-Meier survival estimates based on absolute 6MWT distance thresholds at165 m and 440 m, and all possible 6MWD thresholds.
Patients with PAH
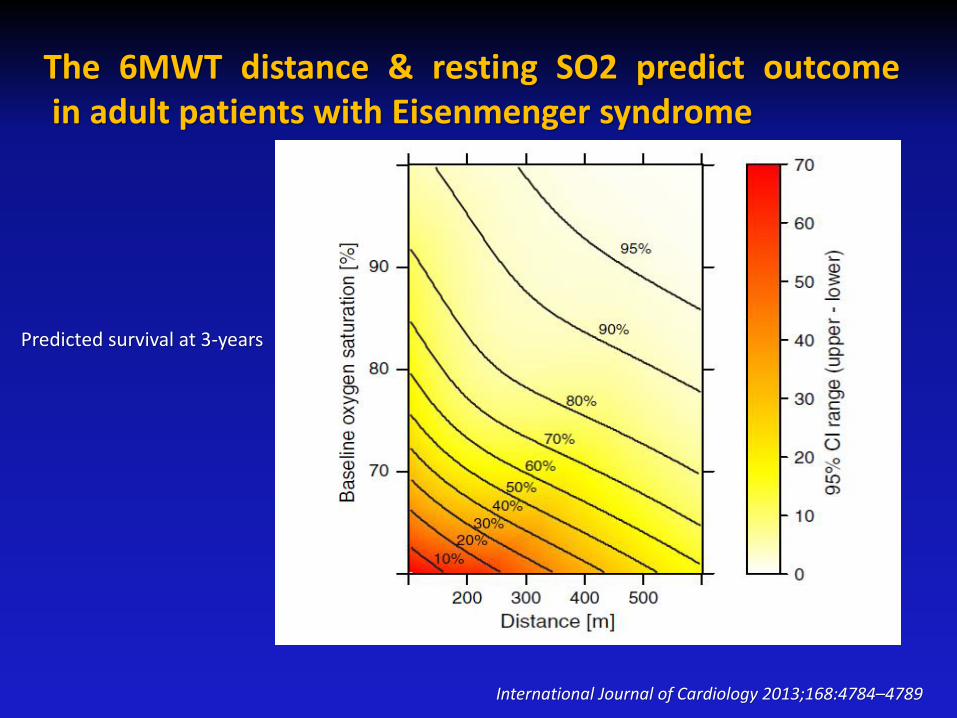
The 6MWT distance & resting SO2 predict outcomein adult patients with Eisenmenger syndrome
International Journal of Cardiology 2013;168:4784–4789
Predicted survival at 3-years