Άρης ?ιάκος, MD MScpromesi.med.auth.gr/mathimata/28_RCT_Workshop.pdf · Άρης...
23
Μάθημα: Ιατρική Βασισμένη στην Τεκμηρίωση Κριτική αξιολόγηση τυχαιοποιημένης κλινικής δοκιμής Άρης Λιάκος, MD MSc Ειδικευόμενος Παθολογίας, Υποψήφιος Διδάκτωρ e-mail: [email protected] Αριστοτέλειο Πανεπιστήμιο Θεσσαλονίκης Σχολή Επιστημών Υγείας – Τμήμα Ιατρικής Πρόγραμμα Μεταπτυχιακών Σπουδών «Ερευνητική Μεθοδολογία στην Ιατρική και τις Επιστήμες Υγείας»
Transcript of Άρης ?ιάκος, MD MScpromesi.med.auth.gr/mathimata/28_RCT_Workshop.pdf · Άρης...
Μάθημα: Ιατρική Βασισμένη στην Τεκμηρίωση
Κριτική αξιολόγηση τυχαιοποιημένης κλινικής δοκιμήςΆρης Λιάκος, MD MScΕιδικευόμενος Παθολογίας, Υποψήφιος Διδάκτωρe-mail: [email protected]
Αριστοτέλειο Πανεπιστήμιο ΘεσσαλονίκηςΣχολή Επιστημών Υγείας – Τμήμα ΙατρικήςΠρόγραμμα Μεταπτυχιακών Σπουδών«Ερευνητική Μεθοδολογία στην Ιατρική και τις Επιστήμες Υγείας»
Connolly et al. N Engl J Med 2009;361(12):1139-51

Critical Appraisal Skills Programme (2017) CASP Randomised Controlled Trial Checklist [online]
1. Did the trial address a clearly focused issue?
HINT: An issue can be “focused” in terms of
• The population studied
• The intervention given
• The comparator given
• The outcomes considered

Critical Appraisal Skills Programme (2017) CASP Randomised Controlled Trial Checklist [online]
2. Was the assignment of patients to treatments randomised?
HINT: Consider
• How this was carried out?
• Was the allocation sequence concealed from researchers and patients?

Randomisation
• Minimises selection bias
• Types
– Simple
– Blocked randomization (e.g. AABB, BBAA, ABAB, ABBA, BAAB, e.t.c.)
– Stratified randomisation

Critical Appraisal Skills Programme (2017) CASP Randomised Controlled Trial Checklist [online]
3. Were all of the patients who entered the trial properly accounted for at its conclusion?
HINT: Consider
• Was the trial stopped early?
• Were patients analysed in the groups to which they were randomised?
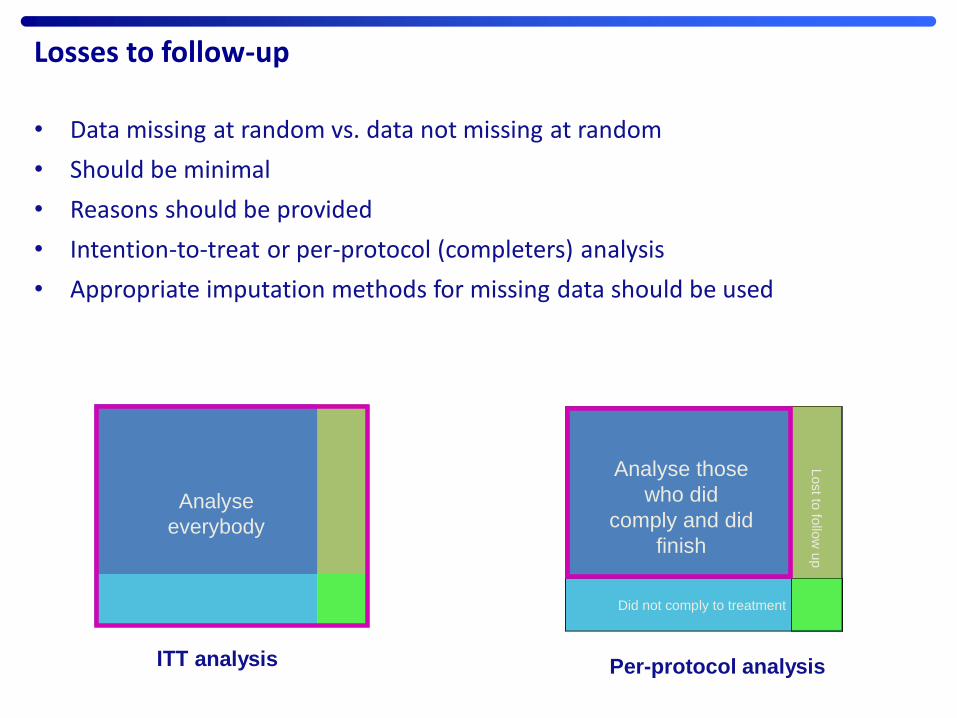
Losses to follow-up
• Data missing at random vs. data not missing at random
• Should be minimal
• Reasons should be provided
• Intention-to-treat or per-protocol (completers) analysis
• Appropriate imputation methods for missing data should be used
True ITT
Analyse
everybody
Because we want to estimate the effectiveness of the intervention
under real circumstances and not the efficacy of the chemical
substance or the nature of the intervention
Per-protocol or treatment-received
Did not comply to treatment
Lost to
follo
w u
p
Analyse those
who did
comply and did
finish
ΙΤΤ analysis Per-protocol analysis
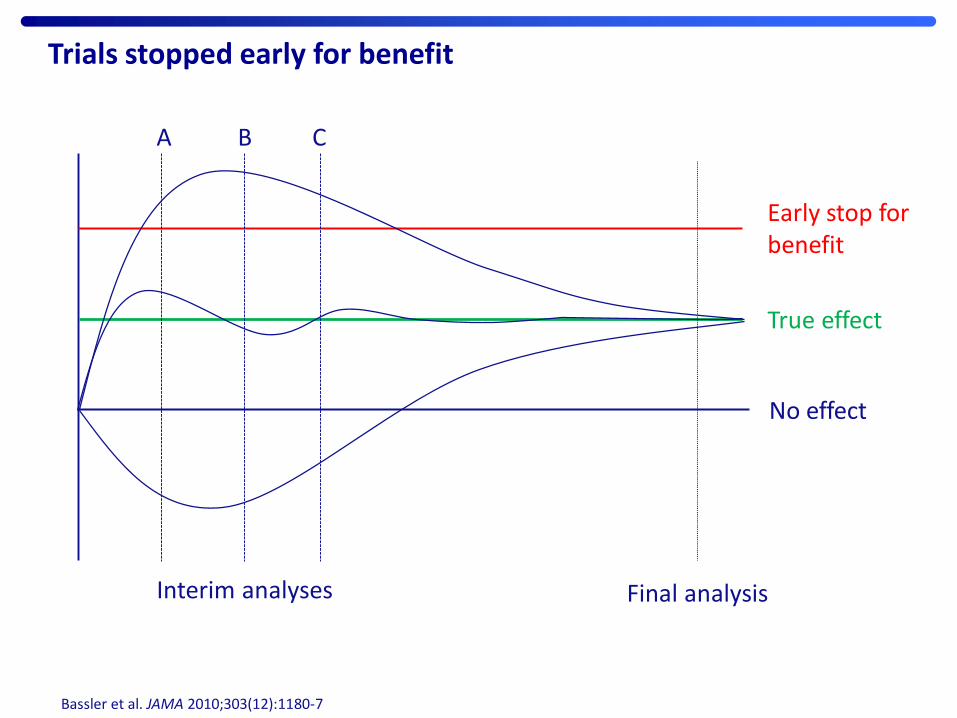
Trials stopped early for benefit
Bassler et al. JAMA 2010;303(12):1180-7
True effect
No effect
Early stop for benefit
Interim analyses Final analysis
Α Β C

Critical Appraisal Skills Programme (2017) CASP Randomised Controlled Trial Checklist [online]
4. Were patients, health workers and study personnel “blind” to treatment?
HINT: Think about
• Patients?
• Health workers?
• Study personnel?
Allocation concealment vs. blinding
• Allocation concealment
– sealed, opaque, sequentially numbered envelopes
– IVRS
– web-based computer system
– independent pharmacist
• Blinding
– participants (single)
– study personnel (double)
– outcome assesors (triple)
– study statistician (quadra)
– minimises ascertainment bias, might be impractical
Critical Appraisal Skills Programme (2017) CASP Randomised Controlled Trial Checklist [online]
5. Were the groups similar at the start of the trial?
HINT: Look at
• Other factors that might affect the outcome such as age, sex, social class

Critical Appraisal Skills Programme (2017) CASP Randomised Controlled Trial Checklist [online]
6. Aside from the experimental intervention were the groups treated equally?
Critical Appraisal Skills Programme (2017) CASP Randomised Controlled Trial Checklist [online]
7. How large was the treatment effect?
HINT: Consider
• What outcomes were measured?
• Is the primary outcome clearly specified?
• What results were found for each outcome?

Critical Appraisal Skills Programme (2017) CASP Randomised Controlled Trial Checklist [online]
8. How precise was the estimate of the treatment effect?
HINT: Consider
• What are the confidence limits?

Critical Appraisal Skills Programme (2017) CASP Randomised Controlled Trial Checklist [online]
9. Can the results be applied in your context (or to the local population)?
HINT: Consider whether
• Do you think that the patients covered by the trial are similar enough to the
patients to whom you will apply this?, if not how do they differ?

Critical Appraisal Skills Programme (2017) CASP Randomised Controlled Trial Checklist [online]
10. Were all clinically important outcomes considered?
HINT: Consider
• Is there other information you would like to have seen?
• If not, does this affect the decision?

Critical Appraisal Skills Programme (2017) CASP Randomised Controlled Trial Checklist [online]
11. Are the benefits worth the harms and costs?
HINT: Consider
• Even if this is not addressed by the trial, what do you think?

Sun et al. BMJ 2012;344
Subgroup analyses
• Looking for “effect modification”
• Exploratory in nature (hypothesis generating)
• Credibility based upon:
– Is the subgroup variable a characteristic measured at baseline or after
randomisation?
– Was the hypothesis specified a priori?
– Was the subgroup effect one of a small number of hypothesised effects tested?
– Is the size of the subgroup effect large?
– Is the interaction consistent across closely related outcomes within the study?
– Is the significant subgroup effect independent?

Sample size calculation
• If the sample size it too small:
– a statistically significant difference between the study arms cannot be detected (wide confidence intervals)
– resources will be wasted
– it is unethical for participants to enroll in a trial that is not adequately powered to answer the research question
• If the sample size is too large:
– resources will be unnecessarily wasted
– the research proposal is unlikely to receive funding
Sample size calculation (continued…)
• Sample size is usually calculated based on the primary outcome
• Sample size depends on:
– Level of significance (type I error rate)
– Power of the study (type II error rate)
– The minimally clinically important difference
– Standard deviation in the population
– The underlying event (rate) prevalence in the population
• Other parameters to consider for sample size calculation:
– The expected drop-out rate
– The allocation ratio
– Secondary outcomes or subgroup analyses

Non-inferiority trial design
• Test whether an experimental treatment is not substantially worse than a control treatment
• Incremental benefits of newly developed treatments may be only marginal or use of placebo unethical
• Null hypothesis: effects of treatments differ by no more than a tolerable amount (i.e. equivalence margin)
• Including dropouts in the analysis (ITT analysis) tends to bias the results toward equivalence

Tips for interpreting medical trials
• Do not rely solely on the pathophysiologic mechanism of action
• Be critical to surrogate endpoints
• Be critical to comparisons against placebo – For active comparators check that therapeutic levels have been used
• Beware of publication bias
Adapted from Greenhalgh Τ. How to read a paper. 2001

Tips for interpreting medical trials (continued…)
• Always look for confidence intervals in the results (statistical versus clinical significance)
• Respect the hierarchy of the evidence
• Be critical to claims presented by key opinion leaders
Adapted from Greenhalgh Τ. How to read a paper. 2001




![Πού είναι ο άρης [all]](https://static.fdocument.org/doc/165x107/568c34b61a28ab023591802a/-all568c34b61a28ab023591802a.jpg)