






γλώσσες
Σελίδες
Νομικός


Impact of Preoperative a-Fetoprotein Level on Disease-FreeSurvival After Liver Transplantation for HepatocellularCarcinoma
Fabrice Muscari • Jean-Pascal Guinard •
Nassim Kamar • Jean-Marie Peron •
Philippe Otal • Bertrand Suc
Published online: 25 April 2012
� Societe Internationale de Chirurgie 2012
Abstract
Background Preoperative a-fetoprotein (AFP) levels may
have an influence on disease-free survival (DFS) of patients
after liver transplantation for hepatocellular carcinoma
(HCC) located on a cirrhotic liver.
Methods Between 2000 and 2009, two groups were dis-
tinguished according to preoperative AFP level: normal-
level group (\10 ng/ml) and increased-level group
([10 ng/ml). The increased-level group was further divi-
ded into three levels of preoperative AFP: 10–150,
150–500, and C500 ng/ml. DFS and recurrence rates were
compared. All patients underwent transplantation using the
preoperative 5/5 criteria.
Results Of the 122 patients in this study, 63 had normal
and 59 had increased preoperative AFP. There were no
differences between the two groups concerning periopera-
tive or pathologic data. Those with an increased preoper-
ative AFP level had a significantly shorter 5-year DFS, and
their recurrence rate was higher than that of the normal
AFP group. The 5-year DFS and recurrence rates were 71
and 4 %, respectively, for those with normal AFP; 57 and
10 %, respectively, for those with AFP 10–150 ng/ml; 46
and 24 %, respectively, for those with AFP 150–500 ng/
ml; and 28 and 62 %, respectively, for those with AFP
C500 ng/ml.
Conclusions This study shows the prognostic value of
preoperative AFP levels on DFS after a liver transplant for
HCC in a population of patients undergoing transplantation
with the same preoperative criteria.
Introduction
Hepatocellular carcinoma (HCC) on a cirrhotic liver is one
of the most common indications for liver transplantation
(LT). The overall 5-year survival rate for this procedure
ranges from 65 to 75 % [1–4]. These good results have
been achieved by using precise selection criteria for
patients. The Milan criteria [3, 5–8] are used as a reference
for LT teams and health systems and are currently used by
the United Network for Organ Sharing (UNOS). However,
during the last decade, the incidence of HCC has increased,
and thus more patients currently need treatment [9, 10].
Therefore, several LT teams have tried to extend the Milan
criteria with the objective of treating more patients [7, 11–
14]. At our center, we use the 5/5 criteria (B5 nodules,
B5 cm), which in a previous study showed good results in
terms of survival and recurrence [15]. These good results
have been confirmed by other teams [16, 17]. This criterion
(5/5) allows to patients to undergo transplantation [17] with
a low recurrence rate and good survival. It is important that
any extension of the HCC selection criteria does not
increase the recurrence rate after LT. The recurrence rate
F. Muscari (&) � J.-P. Guinard � B. Suc
Department of Digestive Surgery and Liver Transplantation,
CHU Rangueil, 1 Avenue Jean Poulhes, 31059 Toulouse Cedex,
France
e-mail: [email protected]
F. Muscari
Department of Epidemiology and Inserm U1027,
Toulouse, France
N. Kamar
Department of Organ Transplantation and Nephrology,
CHU Rangueil, Toulouse, France
J.-M. Peron
Department of Hepatology, CHU Purpan, Toulouse, France
P. Otal
Department of Radiology, CHU Rangueil, Toulouse, France
123
World J Surg (2012) 36:1824–1831
DOI 10.1007/s00268-012-1587-z

needs to remain low to offer equity between all patients on
a waiting list, whatever their type of disease. Extensions to
the selection criteria have concerned only the number and
size of nodules [7, 11–15].
It has been shown that other criteria could influence the
recurrence rate after LT, particularly histologic criteria
(i.e., poor differentiation, satellite nodules, microvascular
invasion) [4, 18–22]. The main problem with the histologic
criteria is that they are difficult to obtain during the pre-
operative period as there is poor correlation between tumor
analysis performed on the preoperative biopsy and the final
analysis of the operative specimen. There is also a risk of
tumor seeding during percutaneous biopsy [19, 23]. Indeed,
only the analysis of a specimen at resection has a good
correlation with the histologic analysis of the liver explant
[19]. Thus, these criteria do not improve selection of
patients beyond the size and number of nodules, with the
exception of patients who have had a resection before LT.
Another factor is that the preoperative a-fetoprotein (AFP)
level seems to be well correlated with the recurrence of
HCC after LT. The AFP level is increased by 20 to 80 % in
patients with HCC and is strongly related to tumor
aggressiveness [24–26]. The AFP level also seems to be
related to survival and recurrence rates after LT [27–32].
The advantage of the AFP level is that it is easy to obtain
before surgery at all LT centers.
The aim of our study was to evaluate the influence of
preoperative AFP levels on DFS of patients undergoing
liver transplantation for HCC and to assess if this evalua-
tion meets the preoperative 5/5 criteria.
Patients and methods
Patients
Data from all HCC patients who received a full-size liver
graft from a deceased donor between 2000 and 2009 in our
department were enrolled in this study. Two groups of
patients were distinguished: one with normal preoperative
AFP levels (\10 ng/ml) and the other with increased pre-
operative levels ([10 ng/ml).
Inclusion criteria
All patients’ records were analyzed at a multidisciplinary
meeting before registration on to the LT waiting list. A
diagnosis of HCC was assigned in accordance with the
Barcelona criteria [33]. A preoperative biopsy was per-
formed in cases of atypical appearance of lesions on
imaging and/or when the size of the nodule was \2 cm.
Patients were registered for the waiting list if they fell
within the 5/5 criteria (i.e., up to five nodules with a
maximum size of 5 cm [15]) as assessed by imaging
studies. The serum AFP was determined at least once in all
patients before the LT. The last determination of AFP
before liver transplantation was considered in this study.
Data collection
Data were collected prospectively. (1) Perioperative crite-
ria were the recipient’s age, sex, blood type, underlying
liver disease, Child-Pugh score, preoperative AFP levels—
normal (\10), 10–150, 150–500 or [500 ng/ml—a pre-
operative biopsy or not, tumor size and number of nodules
found on imaging, pre-LT treatment (for alcoholization,
resection, radiofrequency, or transarterial chemoemboli-
zation), waiting time on list, donor age, number of preop-
erative red blood cells and frozen fresh-plasma
transfusions, use of perioperative autotransfusion, amount
of blood transfused, and duration of graft cold ischemia. (2)
Pathologic criteria were the size and number of nodules,
macroscopic vascular invasion, degree of tumor differen-
tiation, presence of microvascular invasion, and presence
of satellite nodules. (3) Postoperative criteria were com-
plications (during hospitalization), death (during hospital-
ization), and/or recurrence (including the date and site of
the recurrence and its treatment).
Follow-up
While on the waiting list, AFP was determined each month,
and morphologic examinations [computed tomography
(CT) or magnetic resonance imaging (MRI)] were per-
formed every 3 months. Treatment while on the waiting list
was decided upon during a multidisciplinary meeting on a
case-by-case basis, depending on blood group and expected
waiting time. Data collection was completed on June 1,
2010—one year after the first inclusion.
After transplantation, the same team of pathologists
(two persons) performed the explant analyses. Follow-up,
after transplantation, was done in the outpatient clinic
every 3 months for the first year and then every 6 months
in the absence of any adverse events. Standard laboratory
tests, liver function tests, and determination of residual
anticalcineurins were done each time. An AFP assay was
performed every 6 months after LT for HCC. Ultrasonog-
raphy (US) was performed at 1 month, 6 months, 1 year,
and then every 6 months thereafter. CT/MRI was not per-
formed routinely but was used liberally for follow-up of
biliary and arterial complications; it was also used if
recurrence of HCC was suspected on the basis of history,
physical examination, laboratory findings, or US imaging.
An HCC recurrence was diagnosed during a multidis-
ciplinary meeting that included the same radiologist,
World J Surg (2012) 36:1824–1831 1825
123

surgeons, and hepatologists who treated the patient. The
recurrence was established based on imaging studies, the
AFP value, and the histology of a percutaneous biopsy.
Methods
Liver transplantation
The procedure used for orthotopic liver transplantation was
inferior vena cava (IVC) conservation. The cava–caval
anastomosis was fashioned by either a side-to-side tech-
nique or the ‘‘piggy-back’’ technique, using the three main
hepatic veins, as described previously [34]. No systematic
temporary portocaval anastomosis was done. An intraop-
erative blood-salvage autotransfusion was done using a
Cell-Saver 5 (Haemonetics) with the addition of an an-
tiaggregate filter (the same as that used for massive
homologue transfusions). We decided to use the Cell Saver
because it does not appear to increase the risk of postop-
erative recurrence [35].
Immunosuppression protocol
At induction, patients received either rabbit anti-thymocyte
globulin (RATG) or antagonists of receptors for interleukin
2 (basiliximab and daclizumab), or they had no induction
therapy. For maintenance treatment, almost all patients
were given anticalcineurin therapy (tacrolimus or cyclo-
sporine A). From 2003, patients received mycophenolate
mofetil. When HCC recurrence was diagnosed before 2001
anticalcineurin doses were decreased, whereas after 2001
the therapy was switched to rapamycin.
Statistical analyses
Statistical analyses were done with Statview software.
Analyses to estimate survival used the Kaplan-Meier esti-
mation, and the log-rank test was used to compare survival
curves. The v2 test and Student’s t test were used to
compare data between groups of patients.
Results
Perioperative data
Between 2000 and 2009, a total of 122 patients, meeting
the preoperative 5/5 criteria received a liver graft for HCC.
In all, 80 patients (65 %) underwent transplantation after
January 1, 2005 and 42 (35 %) before that date. A total of
63 patients had a normal preoperative AFP level, and 59
patients had an increased AFP level. The perioperative
characteristics of these two groups of patients are listed in
Table 1. There were no significant differences between the
two groups, with the exception of a more advanced age for
patients who had normal preoperative AFP levels. The
mean size of the largest HCC nodule was greater in the
group with increased preoperative AFP levels, but this
difference did not reach significance.
Correlation between preoperative AFP level
and preoperative selection criteria
The numbers of patients with increased AFP levels before
surgery were similar regardless to the selection criteria
applied at the time of registration [Milan, University of
California at San Francisco (UCSF), and 5/5] (Table 1).
There was no difference in the levels of abnormal preop-
erative AFP levels between the patients subgrouped
according to the number and size of their largest tumor
(44 % for the subgroup with one nodule B3 cm versus
43 % for the subgroup with fewer than five nodules
B5 cm) (Table 2).
Pathologic data
The specimen analyses data are shown in Table 3. All
patients were shown to have HCC on specimen analysis.
The maximum size and number of HCC nodules were
significantly greater in patients with increased AFP levels
before surgery. Altogether, 29 patients (24 %) had disease
that was underestimated by the initial imaging technique,
so they were beyond the 5/5 criteria based on the final
specimen analysis.
Immunosuppressive protocol
In all, 25 % of patients underwent induction with RATG,
28 % received anti-interleukin-2 receptor blockers (basil-
iximab or daclizumab), and 47 % had no induction therapy.
Additionally, patients were treated with calcineurin inhib-
itors (CNIs); 87 % received tacrolimus to target trough
levels of 5 to 10 ng/ml until month 3 and from 5 to 8 ng/ml
thereafter; 23 % received cyclosporine A to target C2
levels of 1,000 to 1,200 ng/ml until month 3 and from 500
to 800 ng/ml thereafter. In addition, half received myco-
phenolate mofetil, and 84 % received steroids. If HCC
recurred before 2001, the CNI doses of were reduced. If
recurrence occurred after 2001, CNIs were switched to
sirolimus. No significant differences between the immu-
nosuppressive protocols were found according to preoper-
ative AFP levels.
1826 World J Surg (2012) 36:1824–1831
123

Table 1 Perioperative data
Parameter All
patients
Normal
preop. AFP
Abnormal
preop. AFP
p
(n = 122) (n = 63) (n = 59)
Recipient age (years)a 58 58 55 0.030
Sex
Male 107 (88 %) 56 (89 %) 51 (86 %) 0.680
Female 15 (12 %) 7 (11 %) 8 (14 %)
Child–Pugh class
A 76 (62 %) 33 (53 %) 43 (73 %) 0.059
B 28 (23 %) 19 (30 %) 9 (15 %)
C 18 (15 %) 11 (17 %) 7 (12 %)
Meld scorea 18 17 18 0.653
Etiology of cirrhosis
Alcoholism 48 (39 %) 28 (44 %) 20 (34 %) 0.168
Viral C 49 (40 %) 24 (38 %) 25 (42 %)
Viral B 12 (10 %) 4 (7 %) 8 (14 %)
Others 7 (11 %) 6 (10 %)
Biopsy for HCC
Yes 36 (29 %) 17 (27 %) 19 (32 %) 0.661
No 86 (71 %) 46 (73 %) 40 (68 %)
Preoperative treatment
None 64 (52 %) 30 (48 %) 34 (58 %) 0.443
TACE 44 (36 %) 25 (40 %) 19 (32 %)
RFA 10 (9 %) 6 (9 %) 4 (7 %)
Resection 4 (3 %) 2 (3 %) 2 (3 %)
Size of nodule (cm)* 2.7 2.4 3 0.057
No. of nodule(s)a 2 2 2 0.728
Preoperative selection criteria
Milan criteria
Yes 89 (73 %) 42 (48 %) 47 (42 %) 0.158
No 33 (27 %) 21 (64 %) 12 (36 %)
UCSF criteria
Yes 98 (80 %) 52 (53 %) 46 (47 %) 0.882
No 24 (20 %) 11 (46 %)
AFP (ng/ml)
10–150 15 (12 %) – 15 (25 %)
150–500 27 (22 %) – 27 (46 %)
C 500 17 (14 %) – 17 (29 %)
Time on waiting
list (months)a2.7 3.0 2.5 0.483
Donor age (years)a 46 46 45 0.623
Cold ischemia
time (min)
472 478 465 0.601
No. of RBCsa 3.6 3.6 3.6 0.978
No. of FFPsa 5 5 6 0.381
IBSA
Yes 65 (53 %) 32 (51 %) 33 (56 %) 0.936
No 57 (47 %) 31 (49 %) 26 (44 %)
Table 2 Percentage of patients with abnormal preoperative AFP
levels ([10 ng/ml) according to the size and number of preoperative
HCC tumors
No. of
nodules
No. of patients with abnormal preop. AFP levels, by size
of largest nodule
B3.0 cm B4.5 cm B5.0 cm
1 11/25 (44 %),
AFP 229a22/38 (58 %),
AFP 204
27/44 (61 %),
AFP 180
B3 31/70 (44 %),
AFP 78
44/94 (47 %),
AFP 150)
52/106 (49 %),
AFP 136
B5 37/80 (46 %),
AFP 78
50/107 (47 %),
AFP 51
52/122 (43 %),
AFP 229
HCC hepatocellular carcinomaa Median of AFP measurements (ng/ml) in the subgroup
Table 3 Pathology data
Parameter All
patients
Normal
preop. AFP
Abnormal
preop. AFP
p
(n = 122) (n = 63) (n = 59)
Size of largest
nodule (cm)a3.3 2.8 3.7 0.016
No. of nodulesa 3.2 2.7 3.8 0.032
Differentiation
Poor 7 (6 %) 3 (4 %) 4 (7 %) 0.519
Middle 58 (46 %) 30 (48 %) 28 (47 %)
Good 44 (36 %) 25 (40 %) 19 (33 %)
Necrosis 13 (12 % 5 (8 %) 8 (13 %)
Microscopic
vascular
invasion
29 (24 %) 13 (21 %) 16 (27 %) 0.400
Satellite nodules 21 (17 %) 10 (10 %) 11 (19 %) 0.440
Selection criteria
5/5 93 (86 %) 52 (83 %) 41 (70 %) 0.901
[ 5/5 29 (24 %) 11 (17 %) 18 (30 %)
a Median
Table 1 continued
Parameter All
patients
Normal
preop. AFP
Abnormal
preop. AFP
p
(n = 122) (n = 63) (n = 59)
IBSA (ml)a 553 607 500 0.622
AFP a-fetoprotein, TACE transarterial chemoembolizationm, RFA radio-
frequency ablation, USCF University of California at San Francisco, RBCsred blood cells, FFP frozen fresh plasma, IBSA intraoperative blood sal-
vage autotransfusiona Median
World J Surg (2012) 36:1824–1831 1827
123

Postoperative data
The postoperative mortality rate (3 months) was 6 % (7/
122). Causes of death were fungal infection, cerebral
infarction, intraabdominal hemorrhage, and mesenteric
infarction. The postoperative morbidity rate was 34.5 %
(42/122). Causes of morbidity were surgical in 21 cases
and medical in 21 cases. There was no difference in terms
of mortality and morbidity according to the AFP level.
Follow-up period
The median follow-up time of patients was 38 months
(1–123 months): 39 months for normal preoperative AFP
level patients and 38 months for increased preoperative
AFP level patients.
The HCC recurred in 16 patients (13 %) after LT. There
was no significant difference in recurrence before or after
2005: 16 versus 11 % (p = 0.406). Recurrence was sig-
nificantly more frequent in patients who had an increased
preoperative AFP level compared to those with a normal
level: 22 % (n = 13) versus 4 % (n = 3) (p = 0.003).
Depending on the threshold level of preoperative AFP
studied, we observed a 10 % recurrence rate when preop-
erative AFP levels were 10 to 150 ng/ml, 24 % when levels
were 150 to 500 ng/ml, and 62 % with AFP levels
[500 ng/ml.
The median time from a LT to recurrence was
20 months for patients with normal preoperative AFP
levels and 22 months for patients with increased AFP
levels (p = 0,849). The median time until death after
diagnosis of recurrence was 7 months (1–19 months) with
no difference between the two groups.
The treatments of HCC recurrence were symptomatic
for 11 cases, palliative chemotherapy (sorafenib) in 2
cases, surgical resection in 2 cases, and alcoholization in 1
case.
At the end of the study period, 83 patients were alive
without recurrence (68 %), 4 patients were alive with
recurrence (3 %), and 35 patients had died (28 %). Causes
of death for the 35 patients were HCC recurrence (n = 12),
fungal and bacteria infection (n = 15), other neoplasm
induced by immunosuppressive treatment (n = 4), hepatic
(loss of graft) (n = 2), cardiac arrest (n = 2).
Disease-free survival
The DFS rates at 1, 3, and 5 years, for the entire popula-
tion, were, respectively, 91.5, 67.0, and 60.0 %. There
were no significant differences in the 5-year DFS before
and after 2005: 64 versus 57 % (p = 0.398).
The DFS according to the ‘‘classic’’ selection criteria
(Milan criteria and UCSF criteria) was not significantly
different. The 5-year DFS was 63.5 % within the preop-
erative Milan criteria (n = 89) and 50 % beyond them
(n = 33) (p = 0.164). The 5-year DFS was 58 % within
the preoperative UCSF criteria (n = 98) and 66 % beyond
them (n = 24) (p = 0.914).
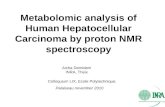
The DFS was significantly decreased in patients with
increased AFP levels, with a significant decrease at 5 years
according to the different threshold levels of preoperative
AFP (Fig. 1): 71 % for normal preoperative AFP levels,
57 % for AFP levels of 10 to 150 ng/ml, 46 % for AFP
levels of 150 to 500 ng/ml, and 28 % for AFP levels
[500 ng/ml. The recurrence rate was higher and the delay
to recurrence was shorter, depending on the preoperative
AFP levels (Fig. 2).
0
,2
,4
,6
,8
1
Sur
vie
Cum
.
0 10 20 30 40 50 60
p = 0.045
Patients at risk:1.2. 3.4.
63 53 33 28 26 18 30 15 21 10 8 6 6
6 4 1
(1)
(2)
(3)
(4)
Time (months)
419910
2 1
29 2116 12
8 6
Fig. 1 Disease-free survival according to preoperative a-fetoprotein
(AFP) levels. (1) Normal preoperative AFP (\10 ng/ml) (n = 63). (2)
Preoperative AFP 10–150 ng/ml (n = 30). (3) Preoperative AFP
150–500 ng/ml (n = 21). (4) Preoperative AFP [500 ng/ml (n = 8)
0
,2
,4
,6
,8
1
1,2
1,4
Tau
x d’
Evé
n C
um.
0 10 20 30 40 50 60
p = 0.045
(1)
(3)
(4)
(2)
Time (months)
Fig. 2 Recurrence of hepatocellular carcinoma according to preop-
erative AFP levels. See Fig. 1 for explanation of the curves
1828 World J Surg (2012) 36:1824–1831
123

Overall survival
The overall survival (OS) rates for the entire population at
1, 3, and 5 years were, respectively, 91.5, 67.5, and 62 %.
There was no significant difference in the 5- year OS rates
after and before 2005: 64 versus 61 % (p = 0.601).
The OS according to the ‘‘classic’’ selection criteria
(Milan criteria and UCSF criteria) was not significantly
different. The 5-year OS was 66 % within the preoperative
Milan criteria (n = 89) and 50 % beyond them (n = 33)
(p = 0.102). The 5-year OS was 61 % within the preop-
erative UCSF criteria (n = 98) and 66 % beyond them
(n = 24) (p = 0.914).
The OS rates were worse in patients with increased AFP
levels before surgery, whereas there was no significant
difference according to the various thresholds of the pre-
operative AFP levels (Fig. 3). However, we did observe a
significant difference in terms of OS when the preoperative
AFP levels were [150 ng/ml, with the 5-year OS rates of
40 % when it was [150 ng/ml versus 66 % when it was
\150 ng/ml (p = 0.032) (Fig. 4).
Discussion
Our study shows that in a population of patients with the
same radiologic preoperative criteria the preoperative AFP
level was significantly associated with a change in DFS
after LT for HCC. This impact seems to be related to the
preoperative AFP level, resulting in a change in 5-year
DFS that ranges from 71 % when the level was normal
(\10 ng/ml) to 28 % when AFP was [500 ng/ml.
We observed that increased AFP levels before surgery
did not correlate with the size and number of HCC nodules
(Table 2). Indeed, 44 to 61 % of patients had increased
AFP levels before surgery regardless of the chosen selec-
tion criteria of the number of nodules and size of the largest
tumor. This probably helps to explain the recurrence rate of
10 % after LT as reported for the Milan criteria [3, 5–8] but
also the stable results in terms of survival and recurrence
rates observed using extensive selection criteria with
regard to number and size of the tumors [7, 11–15]. This
means that the restriction of selection criteria in terms of
size and number of HCC tumors does not decrease the
number of patients with an increased AFP level and
therefore does not improve the DFS.
All patients in this study underwent transplantation
within the 5/5 criteria (B5 nodules, B5 cm) and we have
recently reported the results obtained using the 5/5 criteria
in terms of recurrence and survival compared to the Milan
criteria [15]. In the population of patients reported here, we
determined three thresholds of prognostic preoperative
AFP levels: 10 to 150 ng/ml with a 5-year DFS of 57 %;
150 to 500 ng/ml with a DFS of 46 %;[500 ng/ml with a
5-year DFS of 28 %. Differences in DFS observed between
these three levels were statistically significant. The recur-
rence rate was 4 % when the preoperative AFP was normal
and ranged from 10 to 62 % depending on the elevation of
the AFP levels before surgery. The higher the AFP level,
the earlier did a recurrence appear. Our data confirmed that
AFP can be used as a serum marker for tumor aggres-
siveness [24–26, 29–32]. This marker is correlated with the
presence of histologic markers of poor prognosis, such as
microscopic vascular invasion, presence of satellite nod-
ules, or a poorly differentiated tumor [24–27]. In our study,
the number of patients presenting with poor histologic
criteria was higher in the group with increased preoperative
AFP levels, but this difference was not significant probably
because of the small number of patients in the ‘‘elevated
AFP-level group.’’ However, our patients with abnormal
preoperative AFP levels had significantly more nodules and
larger size of nodules on histologic analyses, which are
well known to be poor prognostic factors. This marker,
0
,2
,4
,6
,8
1
Sur
vie
Cum
.
0 10 20 30 40 50 60
(1)
(2)
(3) (4)
Patients at risk:1. 63 18 2. 303. 214.
p = 0.325
Time (months)
29 21 1553 42 33
16 12 10 8 6 6 2 1 1
28 26
6 48 6
10 10 9
Fig. 3 Overall survival according to preoperative AFP levels. See
Fig. 1 for explanation of the curves
0
,2
,4
,6
,8
1
Sur
vie
Cum
.
0 10 20 30 40 50 60
p = 0.032
AFP < 150 ng/ml (n = 101)
AFP > 150 ng/ml (n = 21)
Patients at risk: < 150 ng/ml. 101 69 53 42 83 30> 150 ng/ml. 21
Time (months) 8616 12 9 6 4 4
Fig. 4 Overall survival according to preoperative AFP levels greater
or less than 150 ng/ml
World J Surg (2012) 36:1824–1831 1829
123

however, was not related to preoperative size or number of
HCC nodules in our study because there was probably an
underestimation of these parameters during the preopera-
tive imaging studies. This underestimation of size and
number of HCC nodules was previously reported by many
studies and for all preoperative selection criteria [8, 11, 15,
36, 37]. In this context, the preoperative AFP value could
balance the radiologic preoperative underestimation of size
and number.
The predictive value of the AFP level for survival after
LT for HCC has been described in previous studies, with
preoperative AFP levels varying from 8.5 to 1000 ng/ml
[11, 29, 30, 32, 38–43]. Even with intention-to-treat anal-
ysis, it has been shown that high AFP levels are associated
with more patients dropping out of the waiting list [38, 39].
It has also been shown [28] that preoperative AFP levels of
[400 ng/ml that are associated with a tumor volume
\115 cm3 had a poor prognosis. Recently, studies [27, 31]
demonstrated that progression of preoperative AFP at [15
or [50 ng/ml per month was associated with worse sur-
vival and a higher risk of recurrence. AFP level also seems
to be a good marker of tumor response to various treat-
ments, including transarterial chemoembolization [44–46].
Until now, no study has compared increased AFP with the
preoperative cutoff in terms of survival and recurrence.
The mean weakness of our study was our long period of
inclusion. However, analysis of periods before and after
2005 did not find any significant difference for recurrence,
DFS, or OS. The choice of 2005 as a cutoff was justified by
our liver transplantation activity for HCC that was twice as
large (65 %) during 2005–2009 than during 2000–2004
(35 %). We could not analyze the effect of treatments on
the waiting list regarding the AFP level because this test
was not available to all patients before this time. The
heterogeneity of immunosuppressive protocols could be
explained by our long period of study. None of the various
immunosuppression protocols seemed to promote recur-
rence of HCC after transplantation. There was no differ-
ence in the use of anticalcineurin agents or the use of
induction therapies, whether by thymocyte globulin or
monoclonal antibodies, in this study (data not shown).
Rapamycin was used in our study only when recurrence of
HCC was suspected. We have not used other prognostic
markers (e.g., PIVKA-II, des-c-carboxyprothrombin)
because they were not easily available in our hospital.
Another limitation of our work was the absence of routine
CT or MRI for looking at HCC recurrence after orthotopic
liver transplantation. In our hospital, all liver transplant
patients are regularly followed and reviewed by the doctors
of the organ transplantation department. No patient was
lost to follow-up. The only distinctive feature of patients
who underwent transplantation for HCC was more regular
US examinations and AFP assays. In fact, we have
considered that there was no real benefit for the patient to
detect an early recurrence because therapeutic resources
are poor. Thus, the recurrence in our work was not
underestimated but was probably detected not early. In the
end, however, the recurrence rate is the same. In recent
studies on this topic, routine surveillance imaging has used
as well as US imaging [47].
Conclusions
This study confirms the prognostic value of preoperative
AFP levels on determining the DFS after LT for HCC.
With the objective of respecting equity among patients
waiting for LT for benign or malignant disease, it seems
necessary to us to select those HCC patients who are most
likely to benefit from LT. Therefore, it seems important to
consider preoperative AFP levels, which are easy to obtain.
One of the problems could be how to integrate the AFP
preoperative level with classic selection criteria for HCC—
how the preoperative AFP level could influence indications
for treatment while on the waiting list and possibly treat-
ment to downstage before LT.
Conflict of interest None.
References
1. Yoo HY, Patt CH, Geschwind JF et al (2003) The outcome of
liver transplantation in patients with hepatocellular carcinoma in
the United States between 1988 and 2001: 5-year survival has
improved significantly with time. J Clin Oncol 21:4329–4335
2. Hemming AW, Cattral MS, Reed AI et al (2001) Liver trans-
plantation for hepatocellular carcinoma. Ann Surg 5:652–659
3. Mazzaferro V, Regalia E, Doci R et al (1996) Liver transplan-
tation for the treatment of small hepatocellular carcinomas in
patients with cirrhosis. N Engl J Med 334:693–699
4. Jonas S, Bechstein WO, Steinmueller T et al (2001) Vascular
invasion and histopathologic grading determine outcome after
liver transplantation for hepatocellular carcinoma in cirrhosis.
Hepatology 33:1080–1086
5. Figueras J, Jaurrieta E, Valls C et al (1997) Survival after liver
transplantation in cirrhotic patients with and without hepatocel-
lular carcinoma: a comparative study. Hepatology 25:1485–1489
6. Llovet JM, Bruix J, Fuster J et al (1998) Liver transplantation for
small hepatocellular carcinoma: the tumour-node-metastasis
classification does not have prognostic power. Hepatology 27:
1572–1577
7. Herrero JI, Sangro B, Quiroga J et al (2001) Influence of tumour
characteristic on the outcome of liver transplantation among
patients with liver cirrhosis and hepatocellular carcinoma. Liver
Transpl 7:631–636
8. Duffy JP, Vardanian A, Benjamin E et al (2007) Liver trans-
plantation criteria for hepatocellular carcinoma should be
expanded: a 22-year experience with 467 patients at UCLA. Ann
Surg 246:502–511
9. Llovet JM, Burroughs A, Bruix J (2003) Hepatocellular carci-
noma. Lancet 362:1907–1917
1830 World J Surg (2012) 36:1824–1831
123

10. El-Serag HB, Mason AL (1999) Rising incidence of hepatocel-
lular carcinoma in the United States. N Engl J Med 340:745–750
11. Yao FY, Ferrell L, Bass NM et al (2001) Liver transplantation for
hepatocellular carcinoma: an expansion of the tumour size limits
does not adversely impact survival. Hepatology 33:1394–1403
12. Sue C, Kris V (2002) Expansion of criteria for liver transplan-
tation in HCC: a slippery slope? Gastroenterology 122:579–582
13. Roayaie S, Frischer JS, Emre SH et al (2002) Long-term results
with multimodal adjuvant therapy and liver transplantation for
the treatment of hepatocellular carcinomas larger than 5 cm. Ann
Surg 235:533–539
14. Onaca N, Davis GL, Goldstein RM et al (2007) Expanded criteria
for liver transplantation in patients with hepatocellular carci-
noma: a report from the International Registry of Hepatic Tumor
in Liver Transplantation. Liver Transpl 13:391–399
15. Muscari F, Foppa B, Kamar N et al (2009) Liberal selection
criteria for liver transplantation for hepatocellular carcinoma. Br J
Surg 96:785–791
16. Sugawara Y, Tamura S, Makuuchi M (2007) Living donor liver
transplantation for hepatocellular: Tokyo University series. Dig
Dis 25:310–312
17. Toso C, Kneteman NM, Shapiro AMJ et al (2009) The estimated
number of patients with hepatocellular carcinoma selected for
liver transplantation using expanded selection criteria. Transpl Int
22:869–875
18. Cha C, Fong Y, Jarnagin WR et al (2003) Predictors and patterns
of recurrence after resection of hepatocellular carcinoma. J Am
Coll Surg 197:753–758
19. Scatton O, Zalinski S, Terris B et al (2008) Hepatocellular car-
cinoma developed on compensated cirrhosis: resection as a
selection tool for liver transplantation. Liver Transpl 14:779–788
20. Regimbeau JM, Abdalla EK, Vauthey JN et al (2004) Risk factors
for early death due to recurrence after liver resection for hepa-
tocellular carcinoma: results of a multicenter study. J Surg Oncol
85:36–41
21. Wang CC, Iyer SI, Low JK et al (2009) Perioperative factors
affecting long term outcomes of 473 consecutive patients
undergoing hepatectomy for hepatocellular carcinoma. Ann Surg
Oncol 16:1832–1842
22. Ng KK, Lo CM, Liu CL et al (2008) Survival analysis of patients
with transplantable recurrent hepatocellular carcinoma. Arch
Surg 143:68–74
23. Pawlik TM, Gleisner AL, Anders RA et al (2007) Preoperative
assessment of hepatocellular carcinoma tumor grade using needle
biopsy: implications for transplant eligibility. Ann Surg 245:435–442
24. Sherman M (2010) The resurrection of alphafetoprotein. J Hepa-
tol 52:939–940
25. Fujioka M, Nakashima Y, Nakashima O et al (2001) Immuno-
histologic study on the expressions of alpha-fetoprotein and
protein induced by vitamin K absence or antagonist II in surgi-
cally resected small hepatocellular carcinoma (abstract). Hepa-
tology 34:1128–1134
26. Farinati F, Marino D, De Giorgo M et al (2006) Diagnostic and
prognostic role of alpha-fetoprotein in hepatocellular carcinoma:
both or neither? Am J Gastroenterol 101:524–532
27. Vibert E, Azoulay D, Hoti E et al (2010) Progression of alpha-
fetoprotein before liver transplantation for hepatocellular carci-
noma in cirrhotic patients: a critical factor. Am J Transpl
10:129–137
28. Toso C, Asthana S, Bigam DL et al (2009) Reassessing selection
criteria prior to liver transplantation for hepatocellular carcinoma
utilizing the Scientific Registry of Transplant Recipients data-
base. Hepatology 49:832–838
29. Wang ZX, Song SH, Teng F et al (2010) A single-center retro-
spective analysis of liver transplantation on 225 patients with
hepatocellular carcinoma. Clin Transpl 24:752–757
30. Onaca N, Davis GL, Jennings LW et al (2009) Improved results
of transplantation for hepatocellular carcinoma: a report from the
International Registry of Hepatic Tumors in liver transplantation.
Liver Transpl 15:574–580
31. Han K, Tzimas GN, Barkun JS et al (2007) Preoperative alpha-
fetoprotein slope is predictive of hepatocellular carcinoma
recurrence after liver transplantation. Can J Gastroenterol
21:39–45
32. Chen CL, Concejero AM (2010) Liver transplantation for hepa-
tocellular carcinoma in the world: the Taiwan experience. J He-
patobiliary Pancreat Sci 17:555–558
33. Bruix J, Sherman M, Llovet JM et al (2001) Clinical management
of hepatocellular carcinoma: conclusions of the Barcelona–2000
EASL Conference—European Association for the Study of Liver.
J Hepatol 35:421–430
34. Muscari F, Suc B, Aguirre J et al (2005) Orthotopic liver trans-
plantation with vena cava preservation in cirrhotic patients: is
systematic temporary portocaval anastomosis a justified proce-
dure? Transpl Proc 37:2159–2162
35. Muscari F, Suc B, Vigouroux D et al (2005) Blood salvage
autotransfusion during transplantation for hepatocarcinoma: does
it increase the risk of neoplastic recurrence? Transpl Int
18:1236–1239
36. Decaens T, Roudot-Thoroval F, Hadni-Bresson S et al (2006)
Impact of UCSF criteria according to pre- and post-OLT tumor
features: analysis of 479 patients listed for HCC with a short
waiting time. Liver Transpl 12:1769–1791
37. Sotiropoulos GC, Malago M, Molmenti EP et al (2005) Liver
transplantation for hepatocellular carcinoma in cirrosis: is clinical
tumor classification before transplantation realistic? Transplan-
tation 79:483–487
38. Figueras J, Ibanez L, Ramos E et al (2001) Selection criteria for
liver transplantation in early-stage hepatocellular carcinoma with
cirrhosis: results of a multicenter study. Liver Transpl 7:877–883
39. Shetty K, Timmins K, Brensinger C et al (2004) Liver transplan-
tation for hepatocellular carcinoma: validation of present selection
criteria in predicting outcome. Liver Transpl 10:911–918
40. De Carlis L, Giacomoni A, Pirotta V et al (2003) Surgical
treatment of hepatocellular cancer in the era of hepatic trans-
plantation. J Am Coll Surg 196:887–897
41. Stuart KE, Anand AJ, Jenkins RL (1996) Hepatocellular carci-
noma in the United States: prognostic features, treatment, out-
come and survival. Cancer 77:2217–2222
42. Llovet JM, Fuster J, Bruix J (1999) Intention-to-treat analysis of
surgical treatment for early hepatocellular carcinoma: resection
versus transplantation. Hepatology 30:1434–1440
43. Yamashiki N, Gaynor JJ, Kato T et al (2004) Competing risks
analysis of predictors of delisting owing to tumor progression in
liver transplantation candidates with hepatocellular carcinoma.
Am J Transpl 4:774–781
44. Shan SL, Mo FK, Johnson PJ et al (2009) New utility of an old
marker: serial alpha-fetoprotein measurement in predicting
radiologic response and survival of patients with hepatocellular
carcinoma undergoing systemic chemotherapy. J Clin Oncol
27:446–452
45. Riaz A, Ryu RK, Kulik LM et al (2009) Alpha-fetoprotein
response after locoregional therapy for hepatocellular carcinoma:
oncologic marker of radiologic response, progression, and sur-
vival. J Clin Oncol 27:5734–5742
46. Chen LT, Shiah HS, Chao Y et al (2009) Alpha-fetoproteinresponse in advanced hepatocellular carcinoma receiving cyto-
static agent. J Clin Oncol 27:e271
47. Sandhu L, Sandroussi C, Guba M, et al (2011) Live donor versus
decreased donor liver transplantation for hepatocellular carci-
noma: comparative survival and recurrence. Liver Transpl Dec 5
World J Surg (2012) 36:1824–1831 1831
123
Top Related