



γλώσσες
Σελίδες
Νομικός

DIABETES MELLITUS

OBJECTIVES• INTRODUCTION• TYPES OF DIABETES• CLINICAL FEATURES• DIAGNOSIS• TREATMENT
• global pandemic principally involves type 2 diabetes• a clinical syndrome characterized by an increase in plasma blood glucose
(hyperglycaemia)• Type 1 diabetes is caused by autoimmune destruction of insulin-producing cells (β
cells) in the pancreas• type 2 diabetes is characterised by resistance to the action of insulin• The diagnostic criteria for diabetes (a fasting plasma glucose ≥ 7.0 mmol/L (126
mg/dL) or glucose 2 hours after an oral glucose challenge ≥ 11.1 mmol/L (200 mg/dL)
• associated with genetic as well as environmental factors such as greater longevity, obesity, unsatisfactory diet, sedentary lifestyle, increasing urbanisation
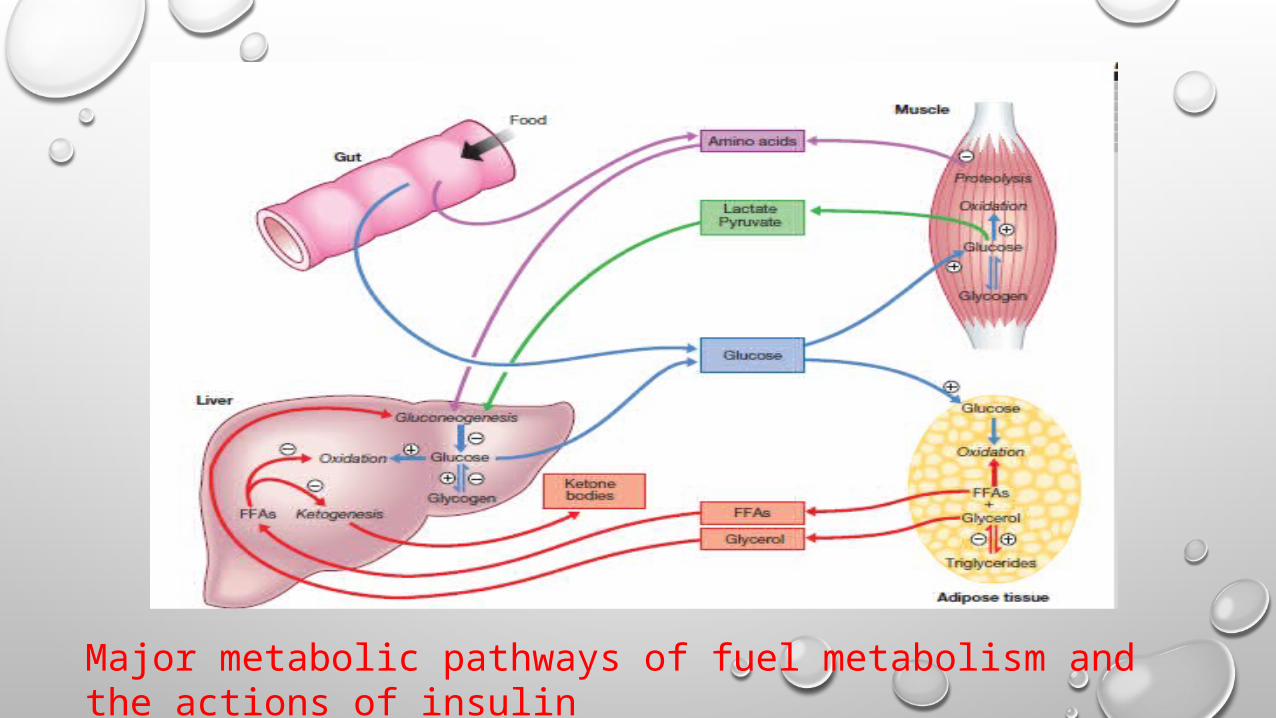
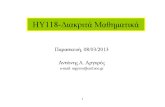
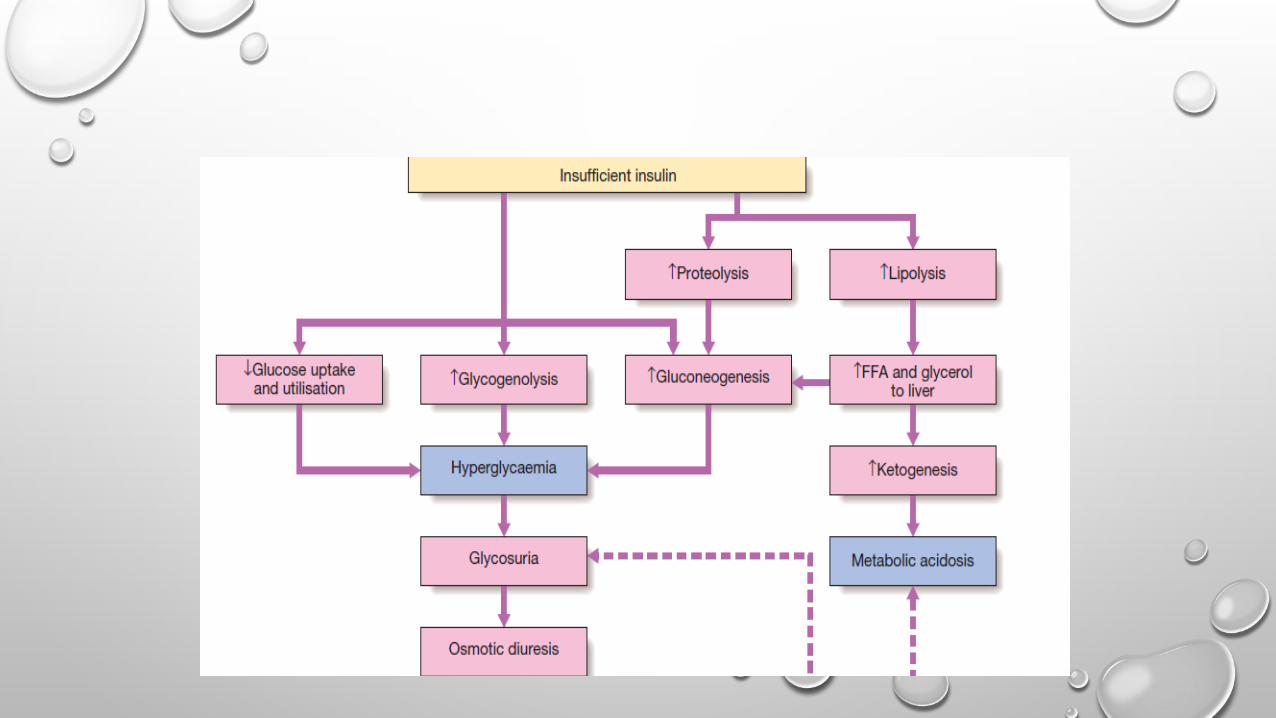
Major metabolic pathways of fuel metabolism and the actions of insulin
AETIOLOGY AND PATHOGENESIS
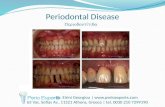
• TYPE 1 DIABETES• type 1 diabetes is a t cell-mediated autoimmune diseasedestruction of the insulin-secreting β cells in the pancreatic islets.,
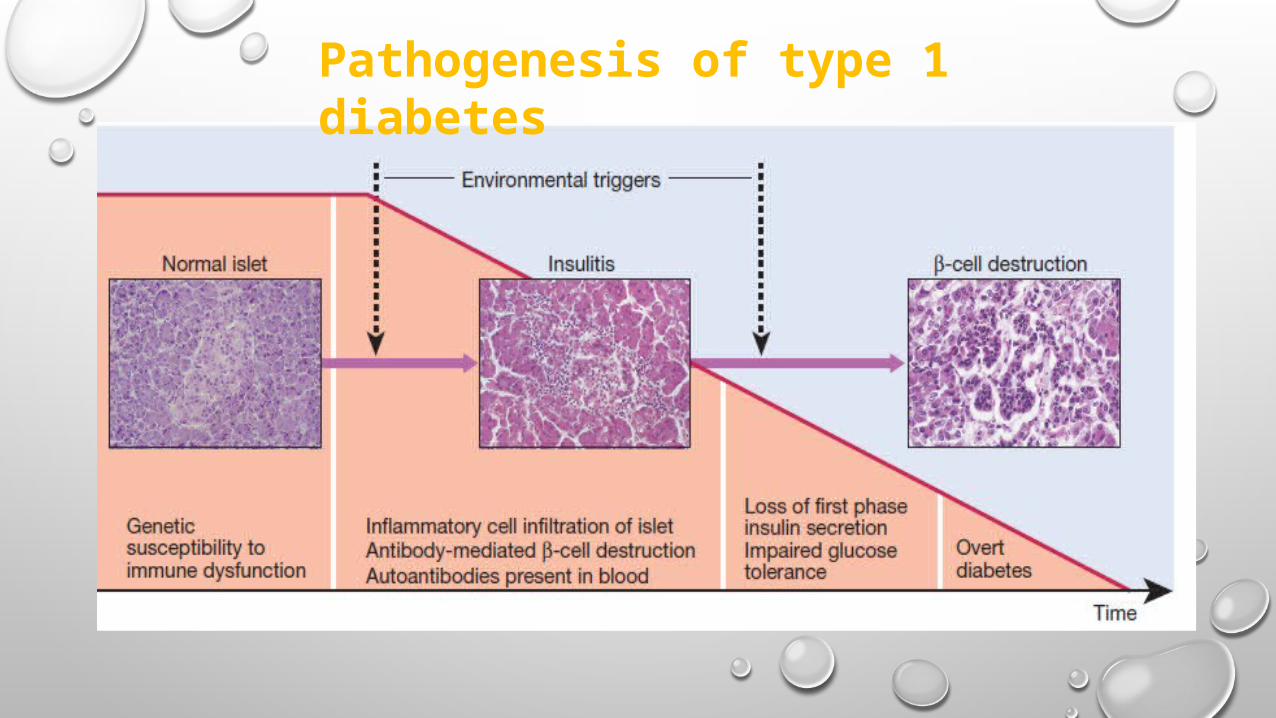
Pathogenesis of type 1 diabetes
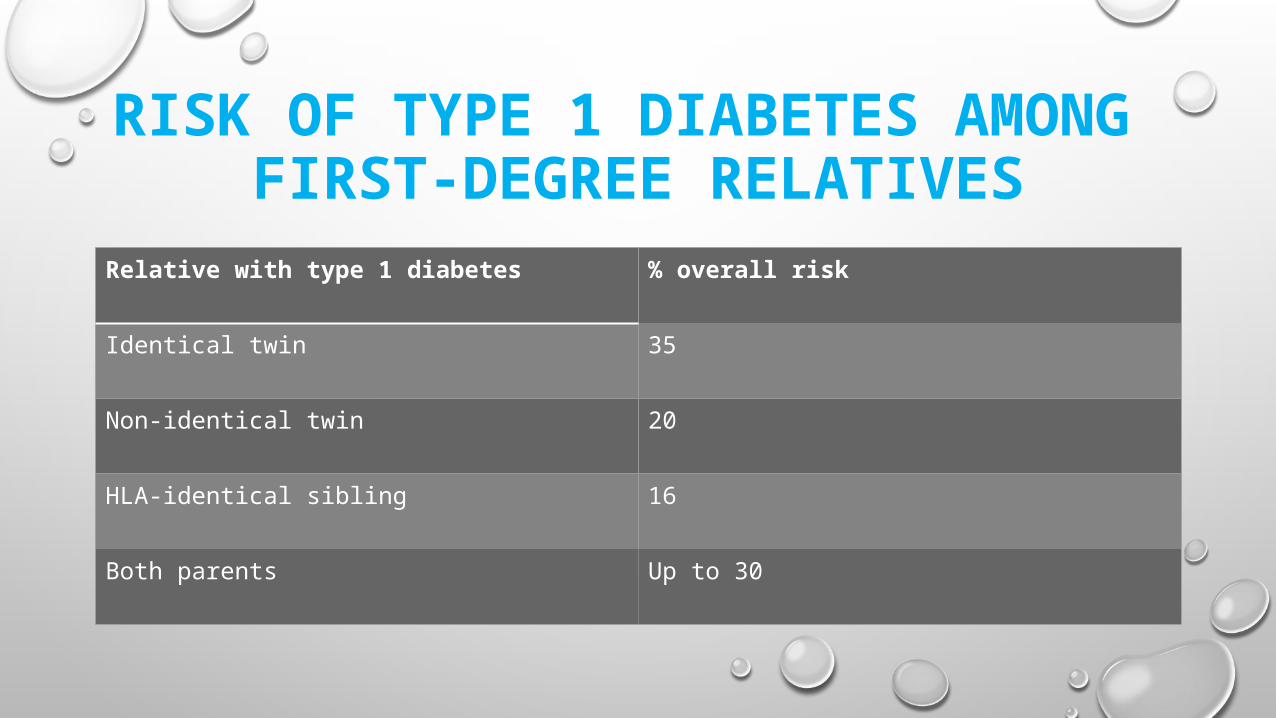
RISK OF TYPE 1 DIABETES AMONG FIRST-DEGREE RELATIVES
Relative with type 1 diabetes % overall risk
Identical twin 35
Non-identical twin 20
HLA-identical sibling 16
Both parents Up to 30
GENETIC PREDISPOSITION• the inheritance is polygenic• Genes on the short arm of chromosome 6; this locus is designated IDDM 1• The HLA haplotypes DR3 and/or DR4 are associated with increased
susceptibility to type 1 diabetes
ENVIRONMENTAL PREDISPOSITION
• direct toxicity to β cells or by stimulating an autoimmune reaction directed against β cells.
• Viruses: mumps, Coxsackie B4, retroviruses,rubella (in utero), cytomegalovirus and Epstein–Barr
• virus.• dietary nitrosamines, coffee, Bovine serum albumin(BSA),
TYPE 2 DIABETES• initially, insulin resistance leads to elevated insulin secretion• the pancreatic β cells are unable to sustain the increased demand for insulin
and a slowly progressive insulin deficiency develops.• ‘insulin resistance syndrome’ or ‘metabolic syndrome’,:• ‘adipokines’:• Pancreatic β-cell failure• Genetic predisposition
ENVIRONMENTAL ANDOTHER RISK FACTORS
• DIET AND OBESITY• Overeating, underactivity
• AGE• more common in the middle-aged and elderly
• At diagnosis, patients are often asymptomatic or give a long history of fatigue, with or
without ‘osmotic symptoms’ (thirst and polyuria)
OTHER FORMS OF DIABETES
• ‘maturity-onset diabetes of the young’ (MODY) • latent autoimmune diabetes of adults (LADA).
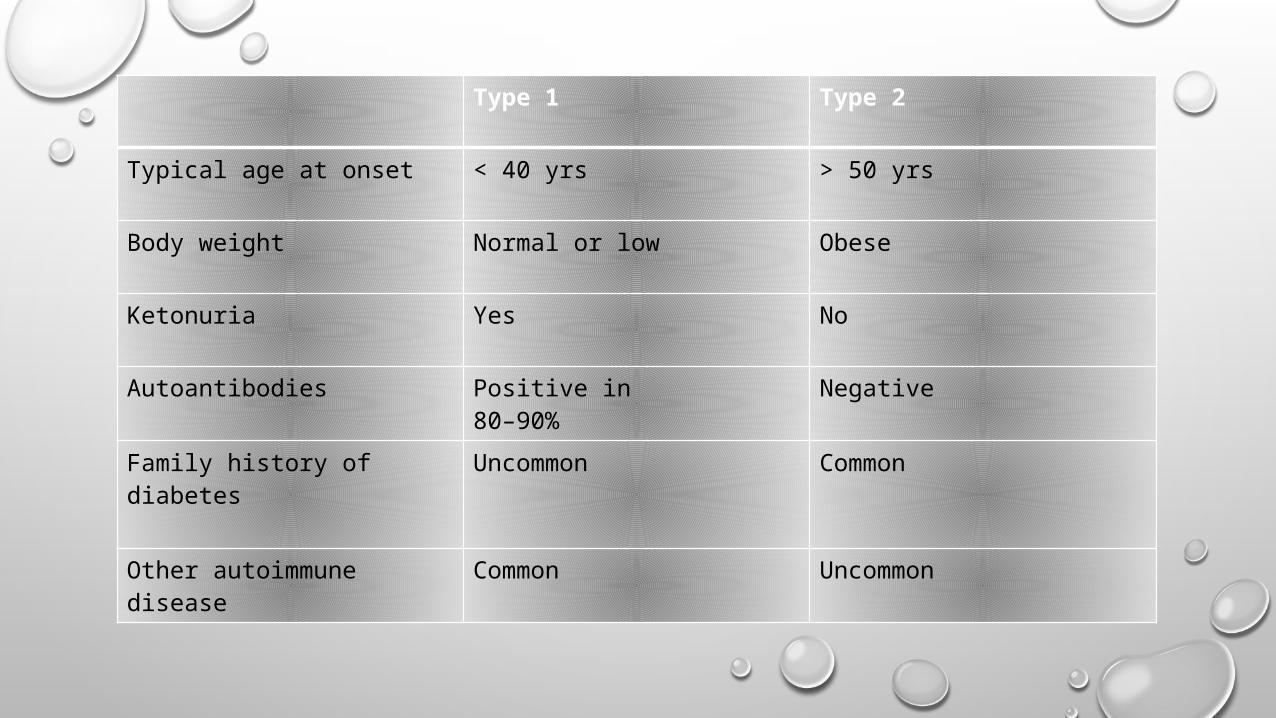
Type 1 Type 2
Typical age at onset < 40 yrs > 50 yrs
Body weight Normal or low Obese
Ketonuria Yes No
Autoantibodies Positive in80–90%
Negative
Family history ofdiabetes
Uncommon Common
Other autoimmunedisease
Common Uncommon
SYMPTOMS OF HYPERGLYCAEMIA
• THIRST, DRY MOUTH• POLYURIA• NOCTURIA• TIREDNESS, FATIGUE, LETHARGY• CHANGE IN WEIGHT (USUALLY WEIGHT LOSS)• BLURRING OF VISION• PRURITUS VULVAE, BALANITIS (GENITAL CANDIDIASIS)• HYPERPHAGIA; PREDILECTION FOR SWEET FOODS• MOOD CHANGE, IRRITABILITY, DIFFICULTY IN CONCENTRATING, APATHY
INVESTIGATIONS• BLOOD GLUCOSE:• to make the diagnosis of diabetes, the blood glucose concentration
should be estimated using• an accurate laboratory method rather than a glucometer• Whole blood glucose concentrations are lower than plasma
concentrations because red blood cells contain relatively little glucose
• Venous plasma values are usually the most reliable • BLOOD KETONE:• detects β-OHB the major ketone in blood during DKA
• URINE TESTING• For Glucose with dipsticksdisadvantage of urinary glucose
measurement is the individual variation in renal threshold for glucose.; • albumin (both macro- and micro-albuminuria)• KETONES
• GLYCATED HAEMOGLOBIN• Glycated haemoglobin provides an accurate and objective measure of
glycaemic control integrated over a period of weeks to months.• HbA1c estimates may be erroneously diminished in anaemia or during
pregnancy, and may be difficult to interpret with some assay methods in patients who have uraemia or a haemoglobinopathy.
• DIABETES• FASTING ≥ 7.0 MMOL/L (126 MG/DL) OR• A RANDOM GLUCOSE ≥ 11.1 MMOL/L (200 MG/DL) (• IFCC HBA1C OF MORE THAN 48 MOLL/MOL• PRE-DIABETES:• IFG OR IGT,BASED UPON THE FASTING PLASMA GLUCOSE ≥ 6.0 (108 MG/DL) AND < 7.0 MMOL/L (126
MG/DL) AND 2-HOUR ORAL GLUCOSE TOLERANCE TEST RESULTS (OGTT) AFTER 75 G ORAL GLUCOSE DRINK 7.8–11.1 MMOL/L (140–200 MG/DL)
• ‘STRESS HYPERGLYCAEMIA: DURING SEVERE STRESS, OR DURING TREATMENT WITH DIABETOGENIC DRUGS
DIABETES IN PREGNANCY• HIGH-RISK WOMEN SHOULD HAVE A 75 G ORAL GLUCOSE TOLERANCE TEST
BEFORE 28 WEEKS’ GESTATION• GESTATIONAL DIABETES IS DIAGNOSED WHEN:• FASTING PLASMA GLUCOSE ≥ 5.1 MMOL/L (92 MG/DL) OR• 1-HR PLASMA GLUCOSE (AFTER GLUCOSE LOAD) ≥ 10 MMOL/L• (180 MG/DL) OR• 2-HR PLASMA GLUCOSE (AFTER GLUCOSE LOAD) ≥ 8 MMOL/L(144 MG/DL)• CONSIDER TESTING HIGH-RISK WOMEN AT FIRST BOOKING VISIT WITH AN HBA1C
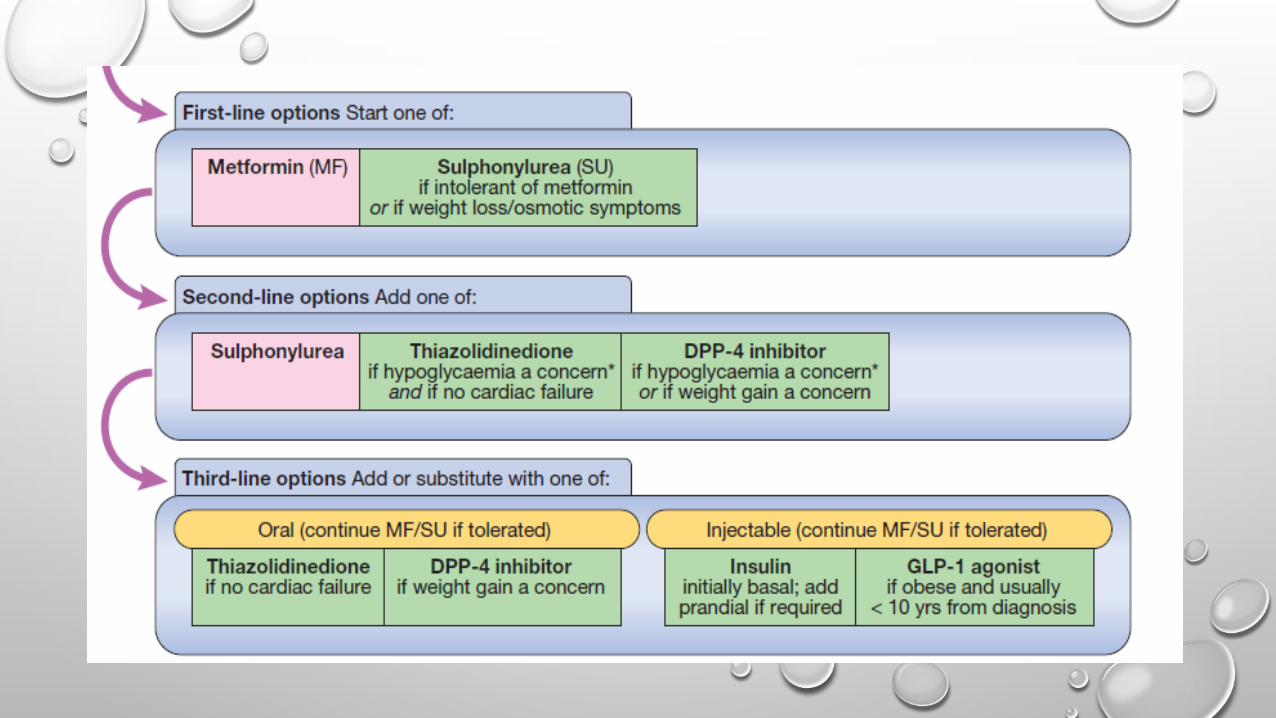
MANAGEMENT• DIETARY• LIFESTYLE MODIFICATION• ORAL ANTI-DIABETIC DRUGS AND• INJECTED THERAPIESINSULINS• BLOOD GLUCOSE TARGETS:PRE-MEAL VALUES BETWEEN 4 AND 7 MMOL/L (72
AND 126 MG/DL) AND 2-HOUR POST-MEAL VALUES BETWEEN 4 AND 8 MMOL/L REPRESENT OPTIMAL CONTROL
• THE TARGET HBA1C: 6.5% -7.5%
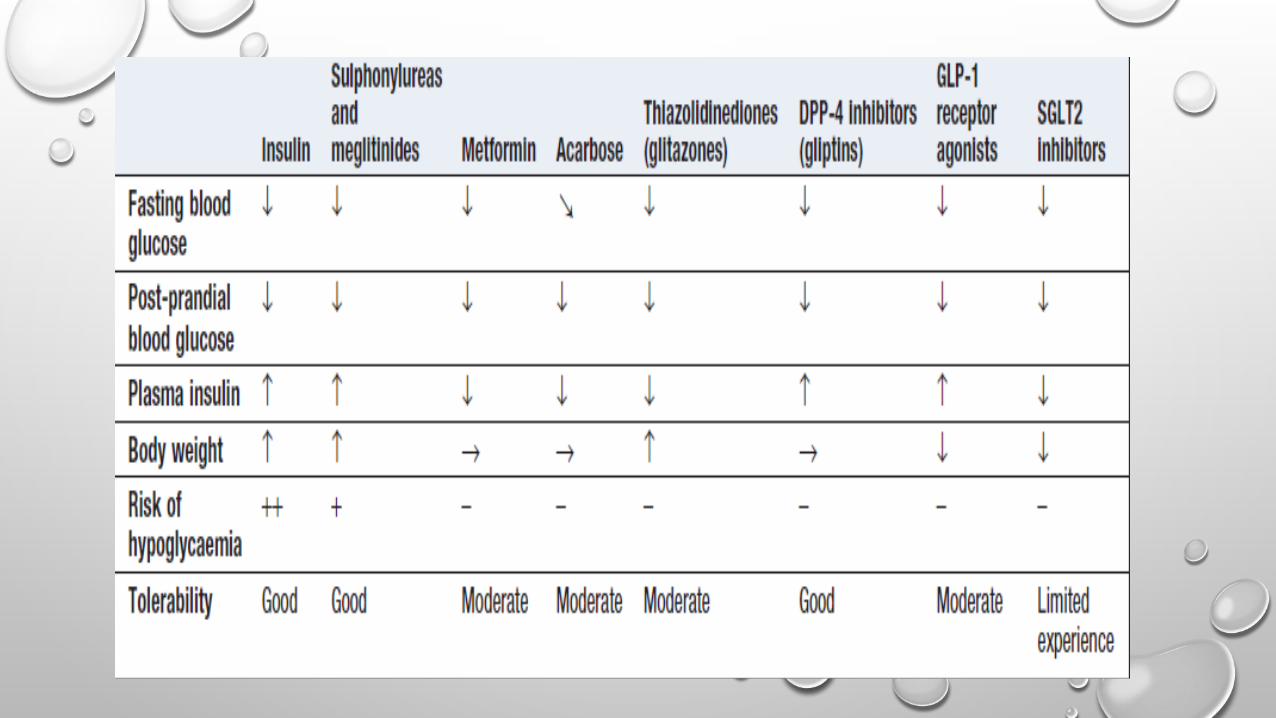
DRUGS• BIGUANIDES• METFORMIN FIRST-LINE THERAPY FOR TYPE 2 DIABETES• THE MAIN SIDE-EFFECTS ARE DIARRHOEA, ABDOMINAL CRAMPS, BLOATING AND
NAUSEA.• AN‘INSULIN SENSITISER’ , ITS MAIN EFFECTS ARE ON FASTING GLUCOSE• DOES NOT CAUSE HYPOGLYCAEMIA• HAS ESTABLISHED BENEFITS IN MICROVASCULAR DISEASE• INTRODUCED AT LOW DOSE (500 MG TWICE DAILY)• THE USUAL MAINTENANCE DOSE IS 1 G TWICE DAILY• CAN INCREASE SUSCEPTIBILITY TO LACTIC ACIDOSIS
• SULPHONYLUREAS:gliclazide, glibenclamide, glimepiride, glipizide• ‘insulin secretagogues’, long-term benefits in lowering microvascular complications• act by closing the pancreatic β-cell ATP-sensitive potaglimepiridessium (KATP)
channel, decreasing K+ efflux, which ultimately triggers insulin secretion.• used as an add-on to metformin• The main adverse effects of sulphonylureas are weight gain and hypoglycaemia
• ALPHA-GLUCOSIDASE INHIBITORS:acarbose, miglitol• delay carbohydrate absorption in the gut by inhibiting disaccharidases• lower post-prandial blood glucose• The main side-effects are flatulence, abdominal bloating and diarrhea
• THIAZOLIDINEDIONES:pioglitazone• TZDs enhance the actions of endogenous insulin, in part directly (in the
adipose cells) and in part indirectly (by altering release of ‘adipokines’,such as adiponectin, which alter insulin sensitivity in the liver)
• hypoglycaemia does not occur
DPP-4 INHIBITORS AND GLP-1 ANALOGUES
• INCRETIN EFFECT:
• THE ‘GLIPTINS’, OR DPP-4 INHIBITORS:sitagliptin, vildagliptin, saxagliptin and linagliptin
• PREVENT BREAKDOWN AND THEREFORE ENHANCE CONCENTRATIONS OF ENDOGENOUS GLP-1 AND GIP
• WEIGHT-NEUTRAL
• INJECTABLE GLP-1 ANALOGUESEXENATIDE (TWICE DAILY), EXENATIDE MR (ONCE WEEKLY) AND LIRAGLUTIDE (ONCE DAILY).
• lower blood glucose and result in weight loss, these agents do not cause hypoglycaemia
SGLT2 INHIBITORS• DAPAGLIFLOZIN• sglt2 is involved in reabsorption of glucose. inhibition results in
approximately 25% of the filtered glucose not being reabsorbed, with consequent glycosuria.
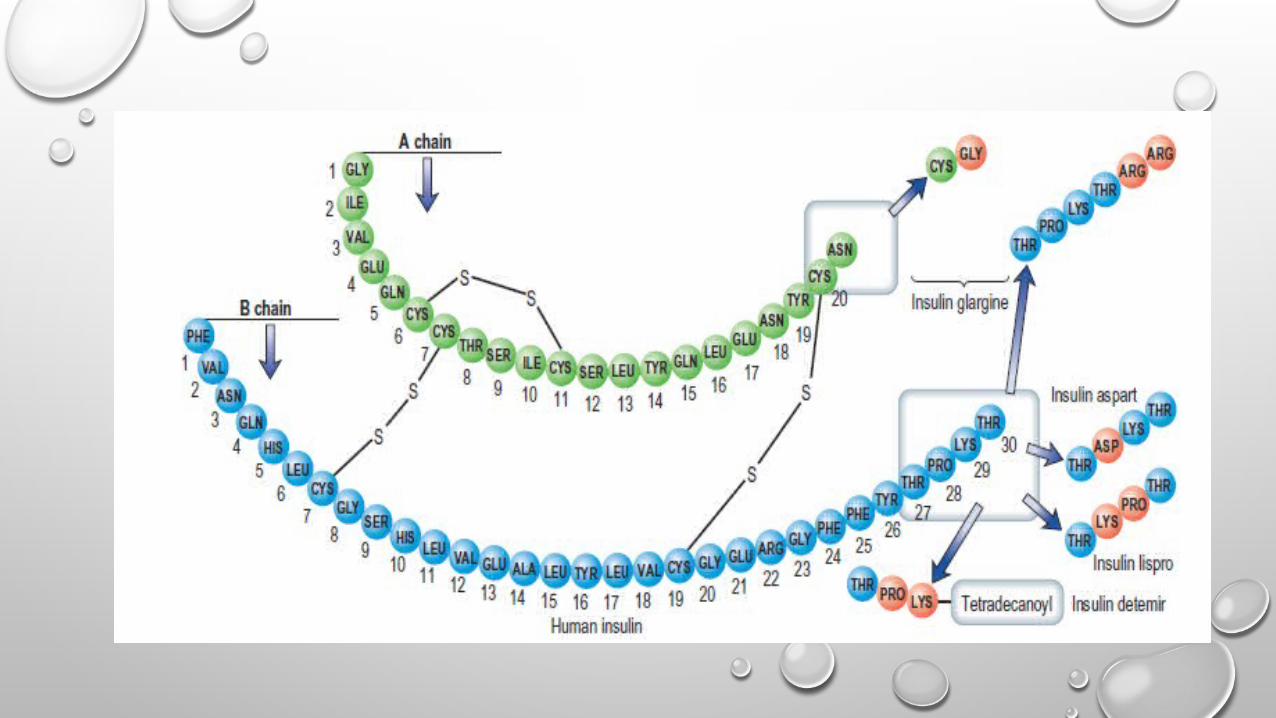
INSULIN THERAPY• SHORT-ACTING INSULIN'S• RAPID-ACTING INSULINS :INSULIN LISPRO,INSULIN
ASPART AND INSULIN GLULISINE• INTERMEDIATE ACTING INSULINS• LONGER-ACTING INSULINS:GLARGINE, DETEMIR• INHALED INSULIN

Thank You
Top Related