




γλώσσες
Σελίδες
Νομικός


Corneal Iron Ring After Hyperopic LASIK
Grand Rounds April 2005
Jay C. Bradley, MD
David L. McCartney, MD

Report of Case:
• 56 year old male
• Pre-operative refraction
+6.00 –2.50 x 7
+6.00 –1.75 x 165
• Pre-operative pachymetry
OD – 516 μm
OS – 525 μm

Operative Summary (2001):
• LADARVision 4000
• Laser-assisted in situ keratomileusis
• Blend Radius 1.50 mm
• Zone Size 6.00 mm
• Ablation depth OD – 91.0 microns
OS – 90.8 microns
• No flap or ablation complications

Follow-up (2004)
• Returns to clinic with complaints of decreased near vision OU
• Does not use distance Rx
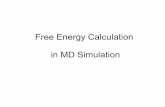
• Normal exam except for trace NSC OU and prominent corneal iron ring OU (~ 5 mm diameter)
• Patient given Rx for reading glasses

Corneal Iron Ring Photo

Prior Reports of Corneal Iron Ring After Hyperopic LASIK
• Ozdamar A et al. Cornea. 1999 Mar; 18(2):243-5.
• 3 patients with pre-op spherical equivalent refraction of +3.37 to +6.50
• Paracentral iron ring OU at 6 – 7 months after surgery
• Localized to outside border of central steep zone• No change in ring at 1 year follow-up

Prior Reports of Corneal Iron Ring After Hyperopic LASIK
• Probst LE et al. JCRS. 1999 May; 25:868-870.
• 1 patient with pre-op Rx of +7.00 –1.50 x 153 OD and +7.50 –1.50 x 165 OS
• Paracentral corneal iron ring OU at 6 months after surgery (5 mm diameter)
• 6.0 mm optical zone with 9.5 mm blend zone• Ring corresponded to base of hyperopic ablation on
corneal topography• Increased mean pre-operative SE and ablation depth
associated with deposition

Histology
• Hemosiderin deposition in basal corneal epithelial cells
• Iron deposits when there is an abrupt change in corneal surface curvature in area of diminished tear flow and hydrodynamic stasis
(Hyperopic PRK)

Pathogenesis: Tear-pool hypothesis
• Proposed by Gass (1964)• Sequestered iron in the tear film is
preferentially deposited in areas of the cornea with pooling of the tear film
• Explains Hudson-Stahli lines corresponding to the lid position at rest
• Low [iron] in tears, protective effect of mucus, and occurrence of iron lines in eyes without tears question this theory

Pathogenesis: Basal-Cell-Migration Theory
• Proposed by Rose and Lavin (1987)
• Abrasive lid action on corneal surface induces enhanced mitotic activity
• Dividing, nonmigrating, basal cells become mature and accumulate iron

Pathogenesis: Tear Desiccation Hypothesis
• Proposed by Assil (1993)
• Iron deposits occur in areas of initial tear breakup

Pathogenesis: Senescent Basal Cell Hypothesis
• Proposed by Assil (1993)
• Iron accumulates in the epithelial cells where there are diminished rates of cell turnover

Iron Lines Associated with Rx / Tx Corneal Procedures
• Arcuate along anterior suture border after PK• Lamellar keratoplasty • Ring adjacent to margin of donor lenticule after epikeratophakia• Central stellate pattern after RK (~ 80 %)• Inferior line or midperipheral arcuate after intrastromal corneal
ring segment (ICRS) placement• Central line after uneventful PRK (myopic and hyperopic)• Small central ring associated with steep central islands after
PRK• Myopic and hyperopic LASIK• Overnight orthokeratology• Conductive keratoplasty



Iron ring associated with overnight ortho-K


Other Corneal Iron Lines
• Fleischer ring– Associated with
keratoconus– First reported in 1906– Partial or complete ring
encircling base of cone– Yellowish to dark brown– Best seen with cobalt
blue light

Other Corneal Iron Lines
• Hudson-Stähli– Iron line along lower
third of cornea in otherwise normal eyes
– Associated with age– Area of tear pooling
when eye lids at rest

Other Corneal Iron Lines
• Stocker-Busacca line– Associated with
pterygia– Anterior to leading edge– Yellow to golden brown

Other Corneal Iron Lines
• Ferry’s line– Associated with
filtering blebs– First reported in 1968

Other Corneal Iron Lines
• Elevated corneal scars
• Salzmann’s nodular degeneration
• Corneal foreign body
• Coats’ white ring
• Juvenile corneal arcus lipoides

Coat’s White Ring

Salzmann’s Nodular Degeneration

Importance of Corneal Iron Lines
• Diagnosis of associated ocular condition
• Identification of corneal donor tissue with prior refractive surgery (ie LASIK flap)
• Possible estimation of optical size and centration of ablation with hyperopic LASIK

Any Questions?
Top Related