





γλώσσες
Σελίδες
Νομικός


Jotimul o/iVeurochemistry Raven Press, Ltd., New York (c) 1993 International Society for Neurochemistry
Brain a-Ketoglutarate Dehydrogenase Complex Activity in Alzheimer’s Disease
Frank Mastrogiacomo, *Catherine Bergeron, and Stephen J. Kish
Human Neurochemical Pathology Luborutory, Clarke Instifute of Psychiutry; and Tentrefor Reseurch in Neurodegenerative Diseases, Toronto, Ontario, Canada
Abstract: We measured the activity of the a-ketoglutarate dehydrogenase complex (a-KGDHC), a rate-limiting Krebs cycle enzyme, in postmortem brain samples from 38 con- trols and 30 neuropathologically confirmed Alzheimer’s disease (AD) cases, in both the presence and absence of thiamine pyrophosphate (TPP), the enzyme’s cofactor. Statistically significant correlations between brain pH and lactate levels and a-KGDHC activity in the controls were observed, suggesting an influence of agonal status on the activity of a-KGDHC. As compared with the controls, mean a-KGDHC activity, with added TPP, was signifi- cantly @ < 0.005) reduced in AD brain in frontal (-56%), temporal (-6O%), and parietal (-68%) cortices, with the reductions (-25 to -53%) in the occipital cortex, hippo- campus, amygdala, and caudate failing to reach statistical significance. In the absence of exogenously administered TPP, mean a-KGDHC activity was reduced to a slightly greater extent in all seven AD brain areas (-39 to -83%), with the reductions now reaching statistical significance in the four cerebral cortical areas and hippocampus. A statis- tically significant negative correlation was observed be- tween a-KGDHC activity and neurofibrillary tangle count in AD parietal cortex, the brain area exhibiting the most marked reduction in enzyme activity; this suggests that the enzyme activity reduction in AD brain may be related to the disease process and severity. In each brain area examined, TPP produced a greater stimulatory effect on a-KGDHC activity in the AD group (23-280% mean stimu- lation) as compared with the controls (-4 to +50°/o); this TPP effect could be explained by reduced endogenous TPP levels in AD brain. Reduced brain a-KGDHC activity could be consequent to loss of neurons preferentially enriched in a-KGDHC, a premortem reduction in TPP lev- els (which may have affected enzyme stability), elevated brain levels of the a-KGDHC inhibitor ammonia, or an ac- tual failure in the expression of the gene encoding the en- zyme. We suggest that a defect in this key Krebs cycle enzyme could contribute to an impairment of cerebral en- ergy metabolism and the brain dysfunction in AD. Key Words: a-Ketoglutarate dehydrogenase complex-Krebs cycle enzyme-Alzheimer’s disease-Thiamine pyro- phosphate-Thiamine. J. Neurochern. 61,2007-201 4 (1 993).
Various possible etiological mechanisms have been proposed for Alzheimer’s disease (AD), including ab-
normal amyloidogenic proteins (Selkoe, 1989; Katz- man and Saitoh, 1991), deficient levels of neurotro- phic factors (Hefti et al., 1989), excitatory amino acid neurotoxicity (Greenamyre and Young, I989), envi- ronmental toxins such as aluminum (Gautrin and Gauthier, 1989), and abnormal phospholipid metabo- lism (Pettegrew et al., 1988; Blusztajn et al., 1990; Farooqui and Horrocks, 199 1 ; Nitsch et al., 1992). In addition, circumstantial evidence has suggested that a defect in brain energy metabolism might be involved in the neurodegenerative process of AD (for review, see Blass et al., 19886), either as a primary event or possibly interacting with one or more of the above- mentioned mechanisms.
The a-ketoglutarate dehydrogenase complex (a- KGDHC; EC 1.2.4.2, EC 2.3.1.61, and EC 1.6.4.3) is a multicomponent mitochondria1 enzyme complex that catalyzes the oxidative decarboxylation of a-keto- glutarate (a-KG) to succinyl-CoA in the tricarboxylic acid cycle. Because a-KGDHC is a key rate-limiting enzyme of the Krebs cycle (Gibson et al., 1984), a defect of this enzyme in brain would, if severe enough, lead to a depletion of energy stores and neuro- nal death. Gibson et al. (1 988) have reported near-to- tal reductions (-75 to -100%) in the activity of a- KGDHC in both degenerated and intact areas of post- mortem AD brain, suggesting the possibility of a global brain phenomenon. Similarly, Buttenvorth and Besnard (1 990) recently demonstrated a 70% re- duction in a-KGDHC activity in AD temporal cor- tex. However, the above studies used only a limited sample size of control and AD patients and number of brain areas examined, and, in a preliminary study
Received November 12, 1992; revised manuscript received March 22, 1993; accepted March 30, 1993.
Address correspondence and reprint requests to Dr. S . J. Kish at Human Neurochemical Pathology Laboratory, Clarke Institute of Psychiatry, 250 College Street, Toronto, Ontario, Canada M5T 1 R8.
Abbreviations used: AD, Alzheimer’s disease; CS, citrate syn- thase; GDH, glutamate dehydrogenase; a-KG, a-ketoglutarate; a- KGDHC, a-ketoglutarate dehydrogenase complex; NFT, neurofi- brillary tangle; NP, neuritic plaque; TPP, thiamine pyrophosphate.
2007

2008 F. MASTROGIACOMO ET AL.
(Kish and Mastrogiacomo, 199 I ), we observed marked intersubject variability in brain enzyme val- ues for both the control and AD groups, which might have been accounted for by agonal status differences. The purpose of the present study was to extend the above investigations in a comprehensive and system- atic manner by using an expanded sample size and number of brain areas examined and by paying spe- cial attention to premortem agonal status.
PATIENTS AND METHODS Autopsied brain was obtained from 30 clinically de-
mented and histopathologically confirmed patients with ADand 38 control subjectsdyingwithout evidenceofneuro- logical or psychiatric disease or brain pathology. The con- trols were selected so that all had, like the AD patients, a protracted illness before death [carcinoma, pulmonary dis- ease, chronic cardiac insufficiency, or bronchopneumonia; criteria of Spokes (1979) and Perry et al. (1982)] and were matched with respect to age (controls, 69 f 2 years; AD, 73 f I years; mean I SE), postmortem interval (controls, 13 t 1 h; AD, 10 * 1 h), and sex ratio (controls, M/F = 2 1/17; AD, MJF = 19/ 1 1 ; p > 0.05). At autopsy, one half brain was fixed in formalin, whereas the other half was frozen at -80°C.
A detailed neuropathological examination was per- formed on all AD cases as previously described (Bergeron and Pollanen, 1989). The criteria for the diagnosis of AD included the presence of both neuritic plaques (NPs) and neurofibrillary tangles (NFTs) in both neocortex and hippo- campus in the absence of any other degenerative process. Four AD cases were found to contain either abundant Lewy bodies or evidence of hypoxic changes and were not in- cluded in the study. The density of NPs and NFTs in the middle temporal gyrus (Brodmann area 2 1) was recorded in each case using the CERAD scale (Mirra et al., 1991) for NPs and the following scale for NFTs (per X250 field): 0, no N F T ; I , less than one NFT per field; 2, one to five NFTs per field; and 3, more than five NFTs in most fields. For the 30 AD patients the NP scores were as follows: 0 (none), n = 0; 1 (sparse), n = 1: 2 (moderate), n = 10; and 3 (frequent), n = 19. The NFT scores were as follows: 0, n = 0; 1, n = 5; 2, n = 12; and 3, n = 13.
No significant differences were observed in the control and AD groups with respect to two brain indices of agonal status (measured in frontal cortex), whic‘h are altered in brain of patients dying with a protracted illness and which could influence enzyme activity (Perry et al., 1982; Hardy et al.. 1985; Butterworth and Tennant, 1989; Yates et at., 1990), namely, pH (controls, 6.30 k 0.05; AD, 6.34 k 0.05; mean ? SE; p > 0.05 by two-tailed Student’s test) and lactic acid levels (controls, 290 -+ 12 nmol/mg of protein; AD. 309 f 1 I nmol/mg of protein; p > 0.05). Postmortem pH and lactate levels measured in human cerebral cortex arc highly correlated with values in striatum (Butterworth and Tennant. 1989).
Frozen brain tissue was dissected and homogenized (7.5% solution) i n ice-cold homogenizing solution containing 50 mM KH,PO,. I mM potassium EDTA, 1 mM 2-mercap- toethanol, and 0.2% Triton X-I00 (pH 7.8) usinga Bronwill Biosonik sonicator ( I X 20 strokes on ice; probe intensity of 70). a-KGDHC activity was determined by a spectrophoto- metric procedure (minor modifications of the procedure of
Gibson et al., 1988) which measured the formation of NADH at 30°C and 340 nm. The final reaction mixture contained 63 mMTris buffer (pH 8.0), 0.63 mMpotassium EDTA, 0.63 m M 2-mercaptoethanol, 0.13% Triton X-100, 3.9 1 m M NAD, 0.19 m M thiamine pyrophosphate (TPP), 0.63 m M dithiothreitol, 1.25 m M CaCI,, 0.30 mM CoA, and 10 mM a-KG, with 100 pI of tissue homogenate, in a final volume of 2.1 ml. The reaction was initiated with addi- tion of substrate, and after a stabilizing period of 3 min, the reaction was monitored for 7 min. Blanks contained 100 pl of distilled water in place of a-KG. Enzyme activity was linear with respect to time and protein concentration. In a preliminary study, the concentrations of a-KG, CoA, NAD, TPP, dithiothreitol, and CaCI, were optimized. No enzyme activity was present in brain homogenates in the absence of a-KG, CoA, or NAD. As expected, a-KGDHC activity (frontal cortex; n = 3 per test, except where indicated) was inhibited by 5 mM NH,CI [53 f 5%; mean f SE percent inhibition (Lai and Cooper, 1986)], 5 mM 0-NADH [I00 k 0% (Koike and Koike, 1976; Gohil and Jones, 198311, 5 niM L-aspartate [ 100 t 0%) (Lai and Cooper, 1986)], 5 mM succinyl-CoA [ 100%; n = 2 (Koike and Koike, 1976)], and 5 mM a-keto-/3-methyl-n-valerate [85 f 3% (Patel, 1974; Koike and Kolke, 1976)]. Preliminary observations on frontal cortical samples revealed no differences in enzyme activity between fresh (unfrozen) tissue and frozen tissue.
To examine the influence of pH on the stability of human brain a-KGDHC in vitro, tissue (control occipital cortex, n = 3) was homogenized in buffer at various pH values (5.5- 9.0, at 0.5-unit increments) and then stored at room temper- ature for 2 h before determination of enzyme activity, all at optimal assay pH (8.0). Enzyme activity in occipital cortex (n = 3) was also determined in both the presence and ab- sence of 1 mM L-lactic acid, pH 8.0.
Activity of two “control” mitochondria1 enzymes, gluta- mate dehydrogenase (GDH) and citrate synthase (CS), was determined by the spectrophotometric procedures of Filla et al. (1986) and Coore et al. ( 1 97 I ) , respectively, in frontal cortex of the control and AD groups. Brain pH and lactic acid levels were determined according to the procedures of Yates et al. ( 1990) and Hohorst ( 1 965), respectively.
RESULTS
Influence of postmortem time and age Biochemical analysis of whole brain of adult Wistar
rats allowed to remain, in a refrigerated (9°C) cold room, at various times after death (1,30, or 60 min or 3,6, 12, or 24 h; n = 4 per group) revealed only a slight but statistically significant influence of postmortem time on enzyme activity 07 < 0.05 by one-way AN- OVA), with a 15% decrease in a-KGDHC activity be- tween the I-min (19.6 f 0.6 nmol/min/mg ofprotein; mean k SE) and 24-h (16.6 f 0.9 nmol/min/mg of protein) groups. These data are similar to the observa- tions of Gibson et al. ( 1 988) of a 29% decrease of a- KGDHC activity in (whole) mouse brain over a 24-h period. As previously reported (Gibson et al., 1988), a-KGDHC activity in autopsied human brain (7.5 k 0.9 nmol/min/mg of protein, mean -t SE; frontal cortex; n = 38) was much lower than in (whole, fresh) brain of the rodent (adult Wistar rats) (20.0 +- 0.6 nmol/min/mg of protein: n = 4).

2009 BRAIN a-KGDI€C IN ALZHEIMER'S DISEASE
5 G 20 s 2 1 5 -
r = 0.58
- r = -0.80
\
5 U 0 6 2 6 4 0 6 8 8 7 . Brain pH
Brain Lactate (nmol/mg protein)
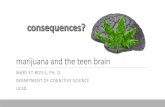
FIG. 1 . Relationship between pH and lactic acid concentrations and temporal cortical a-KGDHC activity in autopsied brain of 35 control subjects @ < 0.002 for both pH and lactic acid).
Brain a-KGDHC activity values for both the con- trol and AD subjects did not fit a normal distribution (p < 0.05 by Kolmogorov-Smirnov-Lilliefors test; see also Fig. 3). Consequently, nonparametric statisti- cal analyses were performed on all comparisons (Mann-Whitney U test) and correlations (Spearman rank order) directly involving a-KGDHC activity. Spearman rank correlation analyses revealed no sta- tistically significant correlation (p > 0.05) between a- KGDHC activity and postmortem interval or age of the patient in all brain areas examined for the control group. In the AD group, slight but statistically signifi- cant positive correlations (p < 0.05) were observed between a-KGDHC activity and patient age (parietal cortex, r = 0.37) and postmortem interval (caudate, Y = 0.40) (p > 0.05 for other brain regions).
Brain pH and lactate Statistically significant correlations were observed
between a-KGDHC activity and both frontal cortical pH ( r = 0.55-0.7 1, p < 0.0 1 by Spearman rank corre- lation) and lactic acid levels ( r = -0.64 to -0.82, p < 0.002) in all seven brain areas examined in the con- trols (temporal cortex is shown in Fig. 1). As previ- ously reported (Butterworth and Tennant, 1989; Yates et al., 1990), a statistically significant negative correlation ( r = -0.65, p < 0.0001 by Pearson correla- tion) was also evident between frontal cortical pH and lactic acid levels in the controls. In the AD group,
statistically significant positive correlations between a-KGDHC activity and pH were observed in tem- poral, parietal, and occipital cortices, as well as the amygdala and caudate ( r = 0.38-0.52, p < 0.05 by Spearman rank correlation) (p > 0.05 for the frontal cortex and hippocampus), whereas statistically signifi- cant negative correlations between a-KGDHC activ- ity and lactic acid levels were demonstrated in all seven AD brain areas (Y = -0.42 to -0.6 I , p < 0.05). A statistically significant negative correlation ( r = -0.48, p < 0.01 by Pearson correlation) was ob- served between frontal cortical pH and lactic acid lev- els for the AD group.
Following the procedure of Yates et al. (1990), we examined the influence of pH and lactic acid on the stability of a-KGDHC activity in (occipital cortical) brain homogenates (n = 3 per group) in vitro. Activity of a-KGDHC in homogenate stored at room tempera- ture at various pHs for 2 h and later measured at opti- mal assay pH was reduced by 100% at pH 5.5 and 73% at pH 6.0 as compared with maximal levels occurring between pH values of 6.5 and 9.0. Enzyme activity was also significantly inhibited by 44% k 6% by addi- tion of 1 m M L-lactic acid, pH 8.0.
a-KGDHC in control versus AD As shown in Fig. 2, mean a-KGDHC activity, in
the presence of exogenously administered TPP, in AD brain was significantly 0, < 0.005 by Mann-Whitney U test) reduced in frontal (-56%), temporal (-60%), and parietal (-68%) cortices, as compared with the controls, with the reductions in the occipital cortex
0 Control with TPP
I AD with TPP Control without TFP
10
h
$ 6
2 4
9
0 Frontal Tenpwal Parietal oCciF#d Hippo- Amypdale Caudate Cutex Cwtex Cortex Cortex c a w s
FIG. 2. Activity of a-KGDHC in cerebral cortex (frontal, Brod- mann area 10; temporal, area 21; parietal, area 7b; and occipital, area 17). hippocampus, amygdala, and caudate nucleus. Data are mean k SE (bars) values from 29-38 control subjects and 26-30 patients with AD. "p < 0.005 by Mann-Whitney U test, control versus AD groups with TPP added to the incubation medium; "p < 0.05, control versus AD groups without TPP. Enzyme activity was also significantly greater (p < 0.05 by paired two-tailed Stu- dent's t test) in the presence of exogenous TPP as compared with its absence in five of seven control brain areas (frontal, tern- poral, parietal, and occipital cortex and hippocampus) and in all seven AD brain areas (p < 0.001).
J Neurochem., Vol. 61, No. 6, 1993

2010
i
F. MASTROGIACOMO ET AL.
Control AD
FIG. 3. Individual patient values for a-KGDHC activity in control (n = 35) and AD (n = 30) temporal cortex (Brodmann area 21) measured in the presence of TPP. Note the large intersubject variance in the controls (0-13.5 nmol/min/mg of protein). Four of the five control subjects with enzyme activity of tl .O nmol/min/ mg of protein had frontal cortical pH and lactic acid levels in the bottom 20th and top 23rd percentile of pH and lactic acid values measured, respectively.
(-35%), hippocampus ( - 5 3 % ; ~ = 0.053,just missing statistical significance), amygdala (-34%), and cau- date (-25%) failing to reach statistical significance @ > 0.05). In the absence of exogenous TPP, a- KGDHC activity in the AD patients was significantly reduced @ < 0.05) in all four cerebral cortical brain areas (-50 to -83%) as well as in hippocampus (-76%), with statistically nonsignificant reductions in the amygdala (-57%) and caudate (-39%). The mag- nitude of the enzyme reduction in the absence of TPP was - 10-23% greater than in its presence in the seven AD brain areas.
An analysis of the individual data revealed that most of the AD patients had enzyme values within the bottom half of the control range for all seven brain areas (individual control and patient enzyme values for temporal cortex are shown in Fig. 3). Mean en- zyme activity was significantly greater in the presence of a maximally stimulatory concentration of exoge- nous TPP as compared with its absence in five of seven control brain areas (frontal, temporal, parietal, and occipital cortices and amygdala; p < 0.05 by paired two-tailed Student's t test) and in all seven AD brain areas (p < 0.001) (see Fig. 2).
Figure 4 shows that TPP produced, on average, a greater stirnulatory effect on a-KGDHC activity in the AD group (23-280%) as compared with the con- trols (-4 to +50%) in all of the brain areas examined. Differences in the stimulatory effect of TPP between the control and AD groups were statistically signifi- cant @ < 0.05 by Mann-Whitney U test) in all brain areas except the amygdala. In a preliminary study, the K, values for a-KG and CoA in frontal cortex were determined by Eadie-Hofstee analysis. No significant differences @ > 0.05 by two-tailed Student's t test) between the control and AD patients were observed for K, values calculated for either a-KG [controls, 1.4
k 0.3 mM(n = 5); AD, 1.7 k 0.6 mM(n = 3)] or CoA [controls, 64 t 14 ,uM (n = 4); AD, 29 * 4 pM (n = 3)]. GDH and CS
Mean activities of GDH and CS, as control mito- chondrial enzymes, were also measured in frontal cor- tex of both control and AD groups. Mean t SEM activity of GDH in the AD group (2 13 k 18 pmol/ min/g of protein, n = 18) was not significantly (p > 0.05 by two-tailed Student's t test) different from the controls (194 +- 8 pmol/min/g of protein, n = 26), whereas mean CS activity, on average, was slightly but significantly reduced by 14% (AD, 154 +_ 6 nmol/ min/mg of protein, n = 30; controls, 179 k 6 nmol/ min/mg of protein, n = 37; p < 0.0001 by Mann- Whitney U test). In control frontal cortex, there was no significant correlation between a-KGDHC activ- ity and GDH activity (p > 0.05 by Spearman rank correlation), whereas a slight but statistically signifi- cant positive correlation (Y = 0.49, p < 0.01) was ob- served between a-KGDHC activity and CS activity. No significant correlations were demonstrated be- tween a-KGDHC activity and either GDH or CS ac- tivities @ > 0.05) in AD frontal cortex. Neuropathological correlations of a-KGDHC
Spearman rank correlation analyses revealed a sta- tistically significant negative correlation ( r = -0.46, p < 0.05) between a-KGDHC activity (with TPP) and NFT count in parietal cortex, with no significant correlation in any other brain area examined @ > 0.05). No significant correlation was observed be- tween a-KGDHC activity and NP count in any exam- ined brain area @ > 0.05).
DISCUSSION We observed reduced mean a-KGDHC activity in
four cerebral cortical and three subcortical brain areas
Frontal Temporal Parietal Occipital H i Amy& Caudate Cortex Cortex Cortex Cortex campus - 1M1 t
FIG. 4. TPP stimulation of a-KGDHC activity in cerebral cortex (frontal, Brodmann area 10; temporal, area 21 : parietal, area 7b; and occipital, area 17), hippocampus, amygdala, and caudate nu- cleus of controls and patients with AD. Data are mean * SE (bars) values, expressed as percent TPP stimulation of a-KGDHC activ- ity, in 19-30 control subjects and 15-22 AD patients having mea- surable enzyme activity in the absence of TPP. "p I 0.05 by Mann-Whitney U-test, control versus AD groups; "p < 0.01: NS, p > 0.05.
J. Neurochem., Vol. 61, No. 6, 1993

BRAIN a-KGDHC IN ALZHEIMER’S DISEASE 201 1
of AD patients, with statistically significant reduc- tions in the frontal, temporal, and parietal cortices when the enzyme activity was measured in the pres- ence of exogenous TPP and significant reductions in five of the seven AD brain areas examined for the enzyme activity measured in the absence of exoge- nous TPP. Our observation of below-normal enzyme activity in all of the AD brain areas examined is con- sistent with the suggestion of Gibson et al. (1988) that reduced a-KGDHC activity in AD brain may be a generalized brain phenomenon. However, unlike the former study, in which a near-total (-75 to - 100%) and generally uniform reduction of a-KGDHC activ- ity was observed in the four cerebral cortical and sub- cortical areas examined, we observed a marked, but less severe, and regionally nonuniform reduction of a-KGDHC activity, with the most severe reductions occurring in the cerebral cortex and hippocampus. Our data also indicate that because all of the individ- ual AD values fell within the range of the controls, e.g. see Fig. 3, brain a-KGDHC activity cannot be used as a reliable marker of AD.
a-KGDHC activity and agonal status The large range of individual a-KGDHC activity
values in all brain regions examined of the controls, e.g., in temporal cortex ranging from 0 to 13.5 nmol/ min/mg of protein (see Fig. 3) , is similar to the obser- vations of Gibson et al. (1988), who also reported a large variation in control autopsied brain enzyme ac- tivities (SE values representing 22 to 57% of mean enzyme activities; see Table 1 of Gibson et al., 1988). This indicates that interpretation of the actual signifi- cance of mean differences between a-KGDHC values in a control versus patient group will be difficult be- cause all of the patient values will likely fall within the (large) range of the controls. The high degree of inter- subject variance in control a-KGDHC activity (with some neurologically normal controls having no detect- able brain enzyme activity; see Fig. 3 ) is unlikely to be due to either the age of the patient or postmortem interval, as neither variable was significantly corre- lated with a-KGDHC activity. The absence of a marked influence of postmortem time on brain en- zyme activity in our rodent study further supports this argument. This large variance in the controls is likely to be explained in part by differences in the terminal hypoxic state of the brain, as suggested both by the highly statistically significant correlations between a- KGDHC activity and both lactic acid and pH levels in the control and AD brain and by the irreversibly inhib- itory influence of lactic acid and low pH on enzyme activity in vitro (see Results). This indicates that in future autopsied brain studies of a-KGDHC, agonal status, as assessed by brain pH or lactate levels, should be taken into account.
Several interpretations of this correlation are possi- ble. First, a patient’s premortem agonal status may directly influence the a-KGDHC activity measured
postmortem. Thus, in highly debilitating and chroni- cally terminal illnesses, such as coma, bronchopneu- monia, cerebral hypoxia, and malnutrition (Spokes, 1979), prolonged acidosis or other metabolic changes associated with hypoxia, e.g., altered protein synthesis and catabolism, could result in low postmortem levels of the enzyme. On the other hand, the alternate possi- bility has to be considered, especially for the AD group, that reduced a-KGDHC activity, occumng as a more primary event, could actually have influenced brain pH and lactate levels by inhibiting flow through the Krebs cycle (Bonnefont et al., 1992), thereby pro- moting the conversion of pyruvate to lactate and thus reducing pH levels.
a-KGDHC activity in AD brain The reduction of a-KGDHC activity in AD brain is
unlikely to be due to differences from the controls in brain pH and lactic acid concentrations as the mean brain pH and lactate levels were not significantly dif- ferent in the AD and control groups. Because the con- trol and patient enzyme values were not normally dis- tributed, we used a nonparametric statistical test for group comparisons; this procedure did not permit us to factor out the influence of pH and lactate on en- zyme activity. However, application of the paramet- ric analysis of covariance test (using pH and lactate as covariates to remove any influence on enzyme activ- ity), which may be appropriate if large sample sizes are used and the deviation from normality is not ex- treme (see McCall, 1970), revealed that the enzyme activity reduction in AD was still highly significant (p < 0.000 1 for frontal, temporal, and parietal cortices; p > 0.05 for other brain areas).
The enzyme activity reduction is also unlikely to be due primarily to loss of mitochondria containing the enzyme, as the decreased enzyme activity in AD cere- bral (frontal) cortex (-56%) greatly exceeded the re- duction (-14%) in frontal cortical activity of CS [a Krebs cycle marker for mitochondrial mass (see Scha- pira et al., 1990a,b)], and a statistical analysis using enzyme data corrected for CS activity (a-KGDHC/ CS activity ratio: control, 0.040 k 0.005; AD, 0.021 + 0.004; mean f SE) revealed that the enzyme activ- ity reduction in AD frontal cortex was still statistically significant (p < 0.02 by Mann-Whitney U test). Re- ports of normal or near-normal activities of two other Krebs cycle enzymes-namely, fumarase (Sorbi et al., 1983) and succinate dehydrogenase (Yates et al., 1990)-as well as of GDH, a mitochondria1 enzyme (see Results and Butterworth and Besnard, 1990) fur- ther support the specificity of the a-KGDHC change in AD brain. Part of the reduction in a-KGDHC activ- ity could be explained by neuronal loss, as the enzyme reductions were greater in those brain areas that suffer the most severe degeneration in AD (frontal, tem- poral, and parietal cortices and hippocampus) than in areas generally spared (caudate).
The neuronal localization of a-KGDHC appears to
J . Neurochem., Vol. 61, NO. 6, 1993

2012 F. MASTROGIACOMO ET AL.
be presently unknown and requires investigation. Should a-KGDHC be preferentially contained in a subgroup of neurons more severely affected in AD, e.g., nucleus basalis-cerebral cortical cholinergic neu- rons (Perry, 1986), then neuronal loss could, in fact, account for the observed reduction in a-KGDHC ac- tivity. Because activity of the enzyme is inhibited by ammonia (see Patients and Methods; Faff-Michalak et al., 199 1: Lai and Cooper, 199 l), reduced activity of a-KGDHC could also be consequent to elevated cerebral levels of ammonia, which have been reported in AD (Hoyer et al., 1990). However, brain a- KGDHC levels have been reported to be normal in patients dying in hepatic coma who were presumably hyperammonemic (Gigukre et al., 1988). Finally, it is possible that a failure in the expression of the gene that encodes any of the three component enzymes of a-KGDHC, including component 1 (E I) , for which TPP is the prosthetic group (Koike and Koike, 1976; Yeaman, 1986). has occurred in AD brain, as sug- gested by the preliminary study of Sheu et al. ( 1992).
Of particular interest is our finding that exoge- nously administered TPP, the enzyme’s cofactor, has, on average, a greater stimulatory effect on brain a- KGDHC activity in the AD group, as compared with the controls. This ability of TPP to stimulate enzyme activity, the TPP effect, has been regarded as a reliable and sensitive criterion for the diagnosis of thiamine deficiency (Kuriyama et al., 1980; McLaren et al., 1981; Graudal et al., 1985). Hence, a greater TPP ef- fect in the AD group is suggestive of lower endoge- nous TPP levels in AD brain than in control brain, a possibility consistent with a preliminary observation of reduced TPP levels in postmortem AD brain (Hkoux et al., 1991). Our observation that a- KGDHC activity remains reduced even with the ad- dition of a maximally stimulatory concentration of exogenous TPP in the in vitro assay may be related to a possible cofactor stabilization role of TPP for its dependent enzyme in vivo (Blass et al., 1988a). We directly explored this possibility using an in vitro as- say to examine the rate of inactivation of purified a- KGDHC (from bovine heart) when incubated at 37°C in both the presence and absence of TPP. Our preliminary observations (data not shown) demon- strate a slightly slower rate of a-KGDHC inactivation when incubated in the presence (-65%; percent inac- tivation of a-KGDHC activity in 10 min) than in the absence (-76%) of TPP. Hence, lower TPP levels in AD brain due to elevated TPP degradation and/or reduced TPP synthesis, reduced thiamine transport across the blood-brain barrier, or a general lack of dietary thiamine intake and/or absorption across the intestinal wall could lead to irreversible inactivation of a-KGDHC. However, the latter possibility appears unlikely in light of evidence from several studies that have directly examined the thiamine status of AD pa- tients in a clinical setting (Scileppi et al., 1984; Wino- grad et al.. 199 1 ) and reported normal blood thiamine
levels in AD. Previous observations from Gibson et al. (1 988) and Butterworth and Besnard ( 1990) of re- duced activity of two other TPP-dependent enzymes in AD brain-namely, pyruvate dehydrogenase com- plex and transketolase-further reinforce the notion that decreased a-KGDHC activity in AD brain could be related to altered thiamine neurochemistry.
Functional significance of a-KGDHC activity reduction
Spearman rank correlation analyses revealed a sta- tistically significant negative correlation ( r = -0.46) between a-KGDHC activity and N F T count in AD parietal cortex, the brain area showing the greatest reduction in a-KGDHC activity. No correlation be- tween enzyme activity and NPs was evident in any examined brain area. In light of recent findings by Arriagada et al. ( 1992), that NFTs (and not NPs) paral- lel the duration and severity of AD, the reduction in a-KGDHC activity may have been related to the de- velopment and/or severity of the disease.
The functional significance of the moderate to se- vere reduction in brain a-KGDHC activity in AD brain is uncertain. A deficiency of this rate-limiting Krebs cycle enzyme in brain would be expected to result in reduced energy stores in the form of ATP, which, if severe enough, would lead to neuronal death. Because ATP is the pyrophosphate donor in the process of TPP synthesis (Sanioto et al., 1977), reduced ATP levels would also compromise the syn- thesis of TPP, leading to lowered a-KGDHC activity and, consequently, lowered ATP levels as a positive feedback phenomenon. Reduced energy metabolism in AD brain is suggested by the observations in living patients of decreased brain glucose utilization by posi- tron emission tomography (Duara et al., 1986; Haxby et al., 1986: McGeer et al., 1986; Nyback et al., I99 I). However, in an in vitro study of biopsied neocortex from AD patients (Sims et al., 1983), CO, production from glucose was increased, suggesting a partial un- coupling of oxidation to ATP production (Blass et al., 1988b), and was associated with only a slight reduc- tion (-2 1%) in ATP levels. Thus, the possibility must also be considered that the a-KGDHC deficit in AD brain might not be sufficient, by itself, to produce any impairment in energy metabolism but could still sig- nificantly compromise the ability of the brain to re- spond adequately to age-related or other neuronal in- sults, e.g. excitotoxic (see Novelli et al., 1988).
In conclusion, we have demonstrated a moderate to marked reduction in the activity of a rate-limiting thiamine-dependent Krebs cycle enzyme in postmor- tem brain of AD patients. Future studies should exam- ine the status of TPP and relevant thiamine-metabo- lizing enzymes in AD brain, an abnormality of which could explain the above changes. Such studies should also determine whether the enzyme changes are spe- cific to AD or occur in brain of patients with other neurodegenerative conditions in which altered thia-
J. Nnirochem., V d 6 1 . No. 6, 19413

BRAIN CE-KGDHC IN ALZHEIMER’S DISEASE 201 3
mine dynamics may be present, namely, Wernicke- Korsakoff syndrome (Adams and Victor, 1981; But- tenvorth, 1989), spinocerebellar disorders (Pedraza and Botez, 1992; Poloni et al., 1992), and amyotro- phic lateral sclerosis and variant (Poloni et al., 1982). Finally, in light of the above evidence indirectly sug- gestive of reduced TPP levels in AD brain, the possibil- ity has to be considered that pharmacologic interven- tion in AD designed to elevate brain TPP levels might prove to be of some clinical benefit (see also Nolan et al., 1991).
Acknowledgment: This study was supported by grant NS26034 from the U.S. National Institute of Neurological Disorders and Stroke. S.J.K. is a Career Scientist of the On- tario Ministry of Health. Some autopsied brain tissue was obtained from the Canadian Brain Tissue Bank.
REFERENCES Adams R. D. and Victor M. ( 1 98 1) Diseases of the nervous system
due to nutritional deficiency, in Principles ofNeirrology, 2nd ed., pp. 709-7 1 1. McGraw-Hill, New York.
Arriagada P. V., Growdon J. H., Hedley-Whyte E. T., and Hyman B. T. (1 992) Neurofibrillary tangles but not senile plaques par- allel duration and severity of Alzheimer’s disease. Neurology 42,63 1-639.
Bergeron C. and Pollanen M. (1989) Lewy bodies in Alzheimer’s disease-one or two diseases? Alzheimer Dis. Assoc. Disord. 4, 197-204.
Blass J. P., Gleason P., Brush D., DiPonte P., and Thaler H. (1988~) Thiamine and Alzheimer’s disease. Arch. Nezrrol. 45,833-835.
Blass J. P., Sheu K.-F. R., and Cedarbaum J. M. (1988h) Energy metabolism in disorders of the nervous system. Rev. Neurol.
Blusztajn J. K., Gonzales-Coviella I . L., Logue M., Growdon J. H., and Wurtman R. J. (1990) Levels of phospholipid catabolic intermediates, glycerophosphocholine and glycerophos- phoethanolamine, are elevated in brains of Alzheimer’s disease but not of Down’s syndrome patients. Brain Rex 536, 240- 244.
Bonnefont J.-P., Chretien D., Rustin P., Robinson B., Vassault A,, Aupetit J., Charpentier C., Rabier D., Saudubray J.-M., and Munnich A. (1992) Alpha-ketoglutarate dehydrogenase defi- ciency presenting as congenital lactic acidosis. J. Pediatr. 121,
Butterworth R. F. ( I 989) Effects of thiamine deficiency on brain metabolism: implications for the pathogenesis of the Wer- nicke-Korsakoff syndrome. Alcohol Alcohol. 24,27 1-279.
Butterworth R. F. and Besnard A. M. (1990) Thiamine-dependent enzyme changes in temporal cortex of patients with Alz- heimer’s disease. Merub. Bruin Dis. 4, 179- 184.
Butterworth J. and Tennant M. C. (1989) Postmortem human brain pH and lactate in sudden infant death syndrome. J. Netirochem. 53, 1494- 1499.
Coore H. G., Denton R. M., Martin B. R., and Randle P. J. (197 I ) Regulation of adipose tissue pyruvate dehydrogenase by insu- lin and other hormones. Biochern. J . 125, 1 15-127.
Duara R., Grady C., Haxby J., Sundaram M., Cutler N. R., Heston L.. Moore A,, Schlageter N., Larson S., and Rapoport S. I . ( 1986) Positron emission tomography in Alzheimer’s disease. Neurology 36, 879-887.
Faff-Michalak L., Wysmyk-Cybula U., and Albrecht J. (1991) Dif- ferent responses of rat cerebral mitochondria1 2-oxoglutarate dehydrogenase activity to ammonia and hepatic encephalopa- thy in synaptic and nonsynaptic mitochondria. Neurochem. Int. 19, 573-579.
Farooqui A. and Horrocks L. A. (1991) Excitatory amino acid re-
144,543-563.
25 5-25 8.
ceptors. neural membrane phospholipid metabolism and neu- rologic disorders. Bruin Re.s. Rev. 16, 17 I - I9 1 .
Filla A,, De Michele G., Brescia Morra V., Palma V., Di Lauro A,, Di Geronimo G., and Campanella G. (1986) Glutamate dehy- drogenase in human brain: regional distribution and proper- ties. J. Neicrochem. 46, 422-424.
Gautrin D. and Gauthier S. (1989) Alzheimer’s disease: environ- mental factors and etiologic hypothesis. Can. J. Neiirol. Sci.
Gibson G. E., Ksiezak-Reding H., Sheu K.-F. R., Mykytyn V., and Blass J. P. (1984) Correlation of enzymatic, metabolic, and behavioral deficits in thiamin deficiency and its reversal. Nezc- rochem. Res. 9, 803-8 14.
Gibson G. E., Sheu K.-F. R., Blass J. P., Baker A.. Carlson K. C., Harding B., and Perrino P. (1988) Reduced activities of thia- mine-dependent enzymes in the brains and peripheral tissues of patients with Alzheimer’s disease. Arch. Nezrrol. 45, 836- 840.
Gigut.re J.-F., Besnard A.-M., Lavoie J., Layrargues G. P., and But- tenvorth R. F. (1989) Activities of glutamate-related enzymes in autopsied brain tissue from cirrhotic patients with hepatic encephalopathy. in Hepulic Encephuloputhy: Pathophysiology und Treatment, pp. 435-445. Humana Press, Clifton, New Jer- sey.
Gohil K. and Jones D. A. (1983) A sensitive spectrophotometric analysis for pyruvate dehydrogenase and oxoglutarate dehydro- genase complex. Biosci. Rep. 3, 1-9.
Graudal N., Torp-Pedersen K., Hanel H., Kristensen M., Thomsen A. C., and Norgird G. (1985) An assessment ofthiamine nutri- tional status. An evaluation of erythrocyte transketolase activ- ity, the stimulated erythrocyte transketolase activity and the thiamine pyrophosphate effect. Int. J . Virum. Xzcrr. Res. 55, 399-403.
Greenamyre J. T. and Young A. B. (1989) Excitatory amino acids and Alzheimer’s disease. Nezrrohiol. .4gin,q 10, 593-602.
Hardy J. A,, Wester P., Winblad B.. Gezelius C., Bring G., and Eriksson A. (1985) The patients dying after long terminal phase have acidotic brain: implications for biochemical mea- surements on autopsy tissue. J. Nmrul Trunsm. 61, 253-264.
Haxby J. V., Grady C. L., Duara R., Schlageter N., Berg G., and Rapoport S. I. (1986) Neocortical metabolic abnormalities precede nonmemory cognitive defects in early Alzheimer’s- type dementia. Arch. Neurol. 43, 882-885.
Hefti F., Hartikka J., and Knusel B. (1989) Function of neurotro- phic factors in the adult and aging brain and their possible use in the treatment of neurodegenerative diseases. Neiirohiol. A p ing 10,5 15-533.
HCroux M., Besnard A.-M., and Butterworth R. F. (1991) Evidence for altered thiamine neurochemistry in Alzheimer’s disease. Soc. Neurosci. Ahsrr. 17, 726.
Hohorst H. J. (1965) L-(+)-Lactate determination with lactic dehy- drogenase and DPN. in Met1iod.s in Enqwutic Anulysis (Berg- meyer H. U., ed), pp. 266-270. Academic Press, New York.
Hoyer S., Nitsch R., and Oestereich K. (1990) Ammonia is endoge- nously generated in the brain in the presence of presumed and verified dementia of Alzheimer type. Neurosci. L w . 117,358- 362.
Katzman R. and Saitoh T. (199 I ) Advances in Alzheimer’s disease. FASEB J. 5,278-286.
Kish S. J. and Mastrogiacomo F. (1991) Brain alpha-ketoglutarate dehydrogenase activity i n Alzheimer’s disease. Soc. Nezrrosci. Abstr. 17, 726.
Koike M. and Koike K. (1976) Structure, assembly and function of mammalian a-keto acid dehydrogenase complexes. Adv. Biophjls. 9, 187-227.
Kuriyama M., Yokomine R., Arima H., Hamda R., and Igata A. (1980) Blood vitamin B,, transketolase and thiamine pyro- phosphate (TPP) effect in beriberi patients, with studies em- ploying discriminant analysis. Clin. Chim. Acru 108, 159-168.
Lai J. C. K. and Cooper A. J. L. ( I 986) Brain a-ketoglutarate dehy-
16,375-387.
J. Neurochem., Vol. 61. No. 6, 1993

2014 F. MASTROGIACOMO ET AL.
drogenase complex: kinetic properties, regional distribution, and effects of inhibitors. J . Nmrocl7em. 47, 1376-1386.
Lai J. C. K. and Cooper A. J. L. (199 I ) Neurotoxicity ofammonia and fatty acids: differential inhibition of mitochondria1 dehy- drogenases by ammonia and fatty acyl coenzyme A deriva- tives. Ncurochcm. Res. 16, 795-803.
McCall R. B. ( 1970) Fundamenla1 Statistics fbr P.sychology. Har- court, Brace and World. New York.
McGeer P. L., Kamo H., Harrop R., Li D. K. B., Tuokko H., McGeer E. G., Adam M. J., and Ammann W. (1986) Positron emmission tomography in patients with clinically diagnosed Alzheimer’s disease. Cun. Med. Assoc. J . 134, 597-607.
McLaren D. S., Docherty M. A., and Boyd D. H. A. (198 1) Plasma thiamine pyrophosphate and erythrocyte transketolase in chronic alcoholism. Am. J. Clin. Nutr. 34, 1031-1033.
Mirra S. S., Heyman A., McKeel D., Sumi S. M., Crain B. J., Brownlee L. M.. Vogel F. S., Hughes J. P., van Belle G., Berg L.. and participating CERAD neuropathologists (199 1) The Consortium to Establish Assessment of Alzheimer’s Disease (CERAD). Part 11. Standardization of the neuropathologic as- sessment of Alzheimer’s disease. Neurology 41, 479-486.
Nitsch R. M., Blusztajn J. K., Pittas A. G., Slack B. E., Growdon J. H., and Wurtman R. J. (1992) Evidence for a membrane defect in Alzheimer’s disease brain. Proc. Natl. Acad. Sci. USA
Nolan K. A., Black R. S . , Sheu K.-F. R., Langberg J., and Blass J. P. ( 1 99 I ) A trial of thiaminc in Alzheimer’s disease. Arch. Neurol.
Novelli A,, Reilly J. A., Lysko P. G.. and Henneberry R. C. (1988) Glutamate becomes neurotoxic via the N-methyl- aspar art ate receptor when intracellular energy levels are reduced. Bruin Rev. 451, 205-2 12.
Nyback H., Nyman H., Blomqvist G., Sjogren I., and Stone- Elander s. (1991) Brain metabolism in Alzheimer’s dementia: studies of “C-deoxyglucose accumulation. CSF monoamine metabolites and neuropsychological test performance in pa- tients and healthy subjects. .I. Ncwrol. Neurosurg. Psychiatry
Patel M. S. (1974) Inhibition by the branched-chain 2-0x0 acids of the 2-oxoglutarate dehydrogenase complex in developing rat and human brain. Biochem. J . 144, 91-97.
Pedraza 0. L. and Botez M. I. ( I 992) Thiamine status in inherited degenerative ataxias. J . Neurol. Neuroswg. Psychiatry 55,
Perry E. K. (1986) The cholinergic hypothesis-ten years on. Br.
Perry E. K.. Perry R. H.. and Tomlinson B. E. (1982) The influence of agonal status on some neurochemical activities of postmor- tem human brain tissue. Neiirosci. Lett. 29, 303-307.
Pettegrew J. W., Panchalingam K., Moossy J. , Martinez J., Rao G., and Boller F. (1988) Correlation of phosphorus-31 magnetic
89, 1671-1675.
48,8143.
54,672-678.
136-137.
bled. Bull. 42, 63-69.
resonance spectroscopy and morphologic findings in Alz- heimer’s disease. Arch. Neurol. 45, 1093- 1096.
Poloni M., Patrini C., Rocchelli B., and Rindi G. (1982) Thiamine monophosphate in the CSF of patients with amyotrophic lat- eral sclerosis. Arch. Neurol. 39, 507-509.
Poloni M., Mazzarello P., Laforenza U., Caramella C., and Patrini C. (1992) Thiamine contents of cerebrospinal fluid, plasma and erythrocytes in cerebellar ataxias. Eur. Neurol. 32, 154- 158.
Sanioto S. M. L., Reinauer H., and Hollmann S. (1977) Thiamine pyrophosphokinase activity in liver, heart, and brain crude ex- tracts of control and thiamine deficient rats. Int. J . Vitam. Nutr. Res. 47, 3 15-324.
Schapira A. H. V., Cooper J. M., Dexter D., Clark J. B., Jenner P.. and Marsden C. D. ( I 9900) Mitochondria1 complex 1 defi- ciency in Parkinson’s disease. J. Neurochem. 54, 823-827.
Schapira A. H. V.. Mann V. M., Cooper J. M., Dexter D., Daniel S. E., Jenner P., Clark J. B., and Marsden C. D. (l990b) Ana- tomic and disease specificity of NADH CoQ, reductase (com- plex I) deficiency in Parkinson’s disease. J . Neurochem. 55, 2 142-2 145.
Scileppi K. P., Blass J. P., and Baker H. G. (1984) Circulating vita- mins in Alzheimer’s dementia as compared to other demen- tias. J . Am. Geriatr. Soc. 32, 709-71 1.
Selkoe D. J. ( I 989) Molecular pathology ofamyloidogenic proteins and the role of vascular amyloidosis in Alzheimer’s disease. Neurobiol. A ~ i n g 10, 387-395.
Sheu K.-F. R., Cooper A. J . L., Ali G., Blass J. P., and Lindsay J. G. ( 1992) Mitochondrial a-kctoglutarate dehydrogenase abnor- mality in Alzheimer disease fibroblasts. Neurobiol. Aging 13 (Suppl.), S64.
Sims N. R., Bowen D. M., Neary D., and Davison A. N. (1983) Metabolic process in Alzheimer's disease: adenine nucleotide content and production of I4CO, from [U-14C]glucose in wfro in human neocortex. .I. Nmrot~hem. 41, 1329-1334.
Sorbi S., Bird E. D., and Blass J. P. ( I 983) Decreased pyruvate dehydrogenase complex activity in Huntington and Alzheimer brain. Ann. Neirrol. 13, 72-78.
Spokes E. G. S. (1979) An analysis of factors influencing measure- ments of dopamine, noradrenaline, glutamate decarboxylase and choline acetylase in human post-mortem brain tissue. Brain 102, 333-346.
Winograd C. H., Jacobson D. H., Butterfield G. E., Cragen E., Edler L. A., Taylor B. S., and Yesavage J. A. (1991) Nutritional in- take in patients with senile dementia of the Alzheimer type. Alzheimu Dis. Assoc. Disord. 5, 173- 180.
Yates C. M., Buttenvorth J., Tennant M. C., andGordon A. (1990) Enzyme activities in relation to pH and lactate i n postmortem brain in Alzheimer-type and other dementias. J . Nc.tirochcm. 55, 1624-1630.
Yeaman S. J. (1986) The mammalian 2-oxoacid dehydrogenases: a complex family. Trend.v Biochern. Sci. 11, 293-296.
J. Nrirrochem , Vol 61. No. 6. I993
Top Related