

![Brucella Six species of Brucella B.melitensis, B.abortus, B.suis, B.canis Sir David Bruce [brucellosis], Bernhard Bang [Bang's disease] Undulant.](https://static.fdocument.org/doc/165x107/56649d885503460f94a6d4e6/brucella-six-species-of-brucella-bmelitensis-babortus-bsuis-bcanis.jpg)


γλώσσες
Σελίδες
Νομικός


- Mycoplasma and Ureaplasma
- Rickettsia
Mycoplasma and Ureaplasma
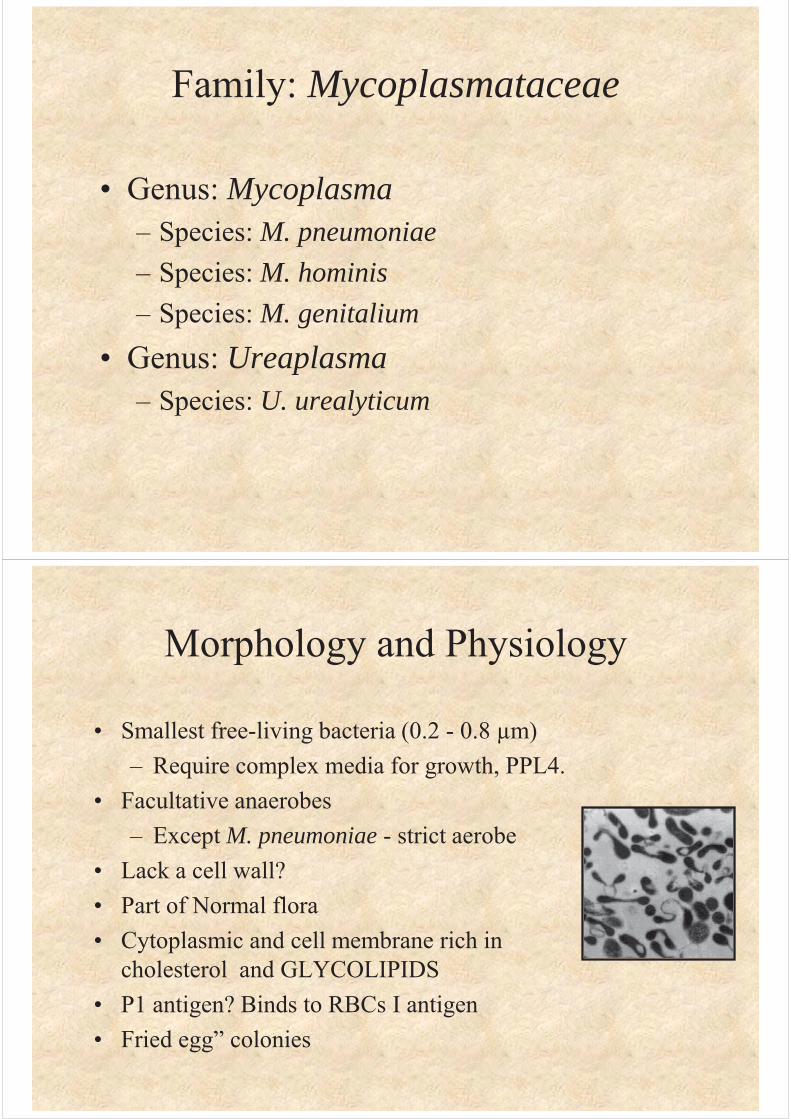
Family: Mycoplasmataceae
• Genus: Mycoplasma– Species: M. pneumoniae– Species: M. hominis– Species: M. genitalium
• Genus: Ureaplasma– Species: U. urealyticum
Morphology and Physiology
• Smallest free-living bacteria (0.2 - 0.8 μm)– Require complex media for growth, PPL4.
• Facultative anaerobes– Except M. pneumoniae - strict aerobe
• Lack a cell wall?• Part of Normal flora • Cytoplasmic and cell membrane rich in
cholesterol and GLYCOLIPIDS• P1 antigen? Binds to RBCs I antigen• Fried egg” colonies
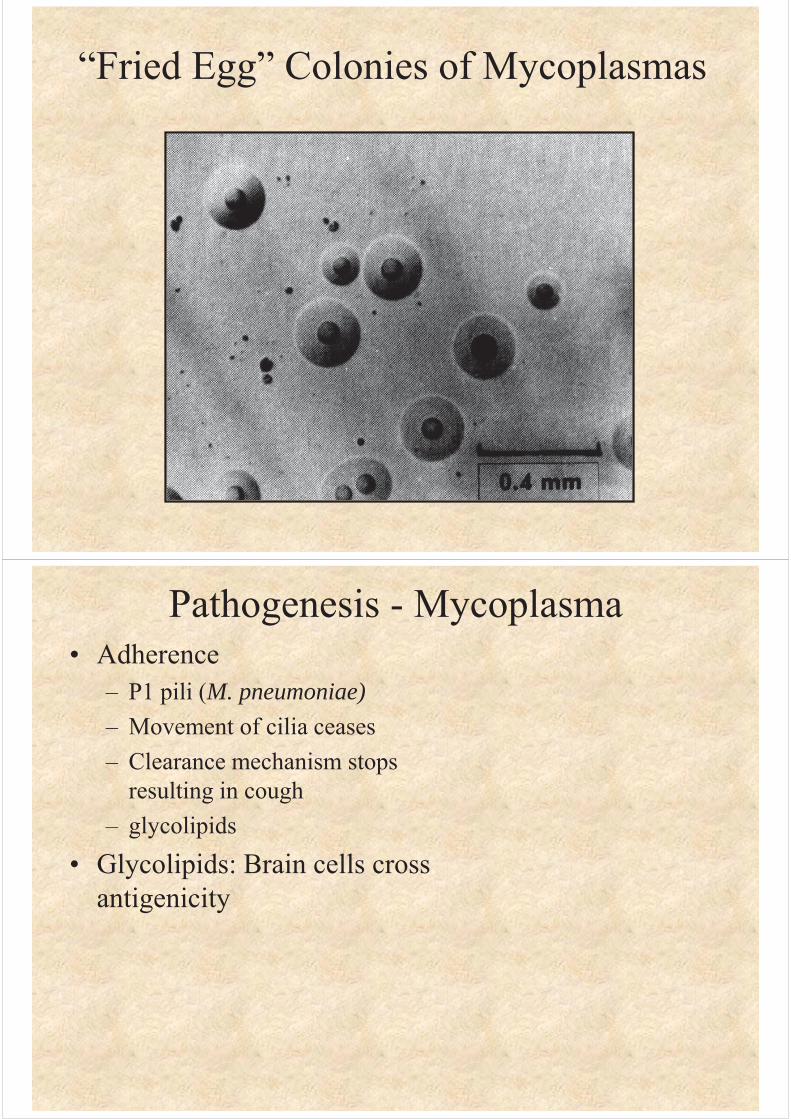
“Fried Egg” Colonies of Mycoplasmas
Pathogenesis - Mycoplasma• Adherence
– P1 pili (M. pneumoniae)– Movement of cilia ceases– Clearance mechanism stops
resulting in cough– glycolipids
• Glycolipids: Brain cells cross antigenicity
Organism Disease
M. pneumoniae Upper respiratory tract disease,tracheobronchitis, atypicalpneumonia, (chronic asthma??)
M. hominis Pyleonephritis, pelvicinflammatory disease,postpartum fever
M. genitalium Nongonococcal urethritis
U. urealyticum Nongonococcal urethritis,(pneumonia and chronic lungdisease in premature infants??)
Diseases Caused by Mycoplasma
N.B. Other organisms infect humans but their disease association is not known.
Mycoplasma pneumoniae
• Tracheobronchitis• Atypical pneumonia (walking pneumonia)
Epidemiology - M. pneumoniae
• Occurs worldwide• No seasonal
variation– Proportionally
higher in summer and fall
Clinical Syndrome - M. pneumoniae
• Incubation - 2-3 weeks• Fever, headache and malaise• Persistent non-productive cough• Respiratory symptoms
– Radiological signs precede symptoms• Slow resolution• Rarely fatal
Laboratory Diagnosis - M. pneumoniae
• Microscopy– Difficult to stain– Can help eliminate other organisms
• Culture (definitive diagnosis)• May take 2-3 weeks• Serology • PCR
Treatment and PreventionM. pneumoniae
• Treatment – Tetracycline or erythromycin
• Newer fluoroquinolones– Can’t use cell wall synthesis inhibitors
• Prevention– Avoid close contact– No vaccine
Rickettsia and Orientia
• Small obligate intracellular parasites • Once considered to be viruses • Gram-negative bacteria
– Stain poorly with Gram stain (Giemsa)• Reservoirs - animals, insects and humans• Arthropod vectors
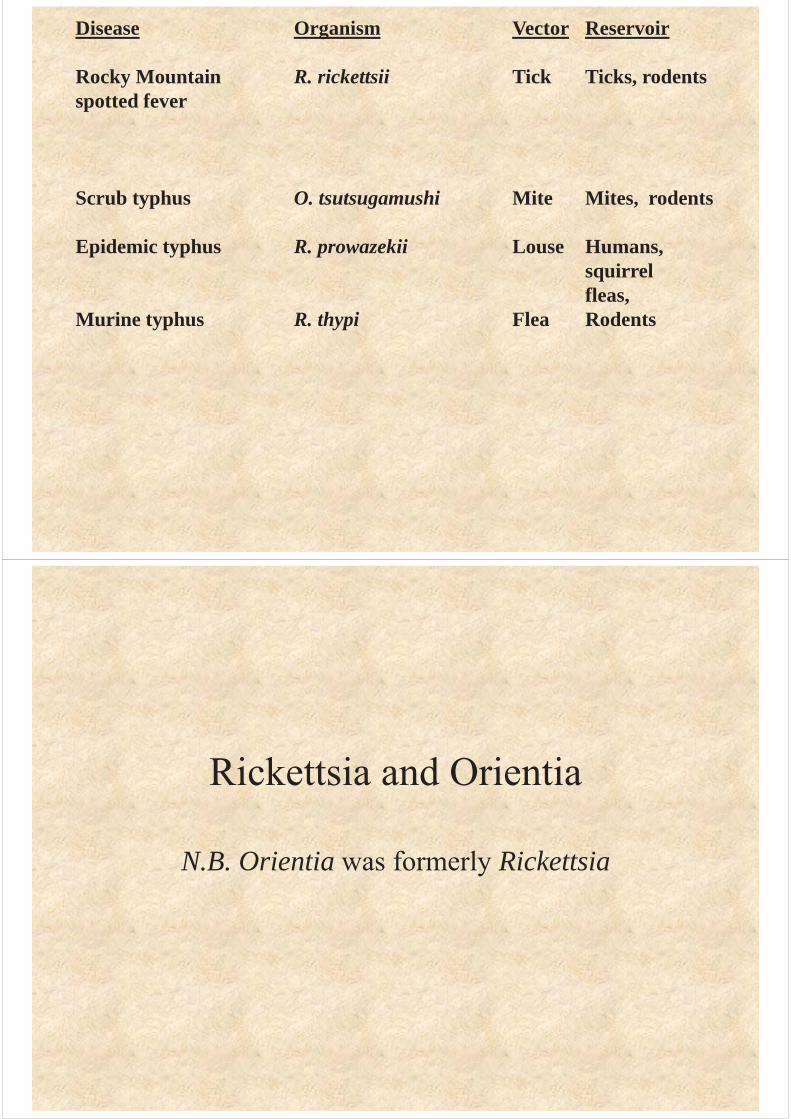
Disease Organism Vector Reservoir
Rocky Mountain R. rickettsii Tick Ticks, rodentsspotted fever
Scrub typhus O. tsutsugamushi Mite Mites, rodents
Epidemic typhus R. prowazekii Louse Humans, squirrelfleas,
Murine typhus R. thypi Flea Rodents
Rickettsia and Orientia
N.B. Orientia was formerly Rickettsia
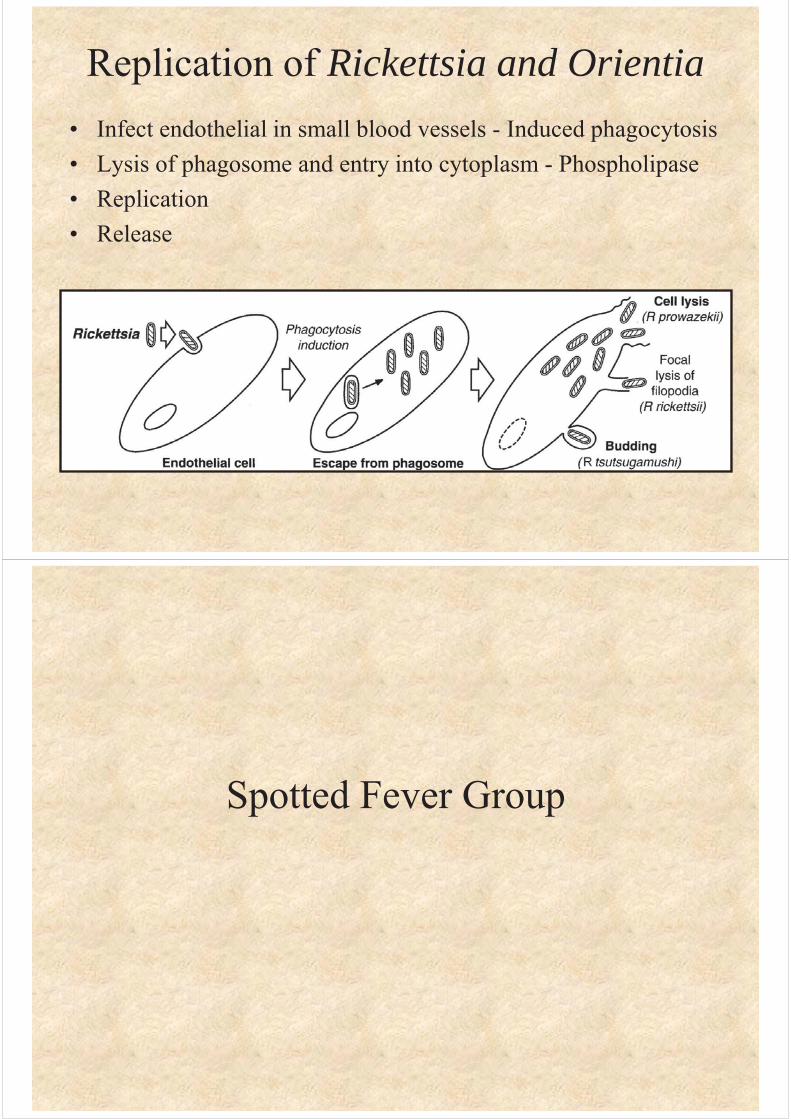
Replication of Rickettsia and Orientia• Infect endothelial in small blood vessels - Induced phagocytosis• Lysis of phagosome and entry into cytoplasm - Phospholipase• Replication• Release
Spotted Fever Group
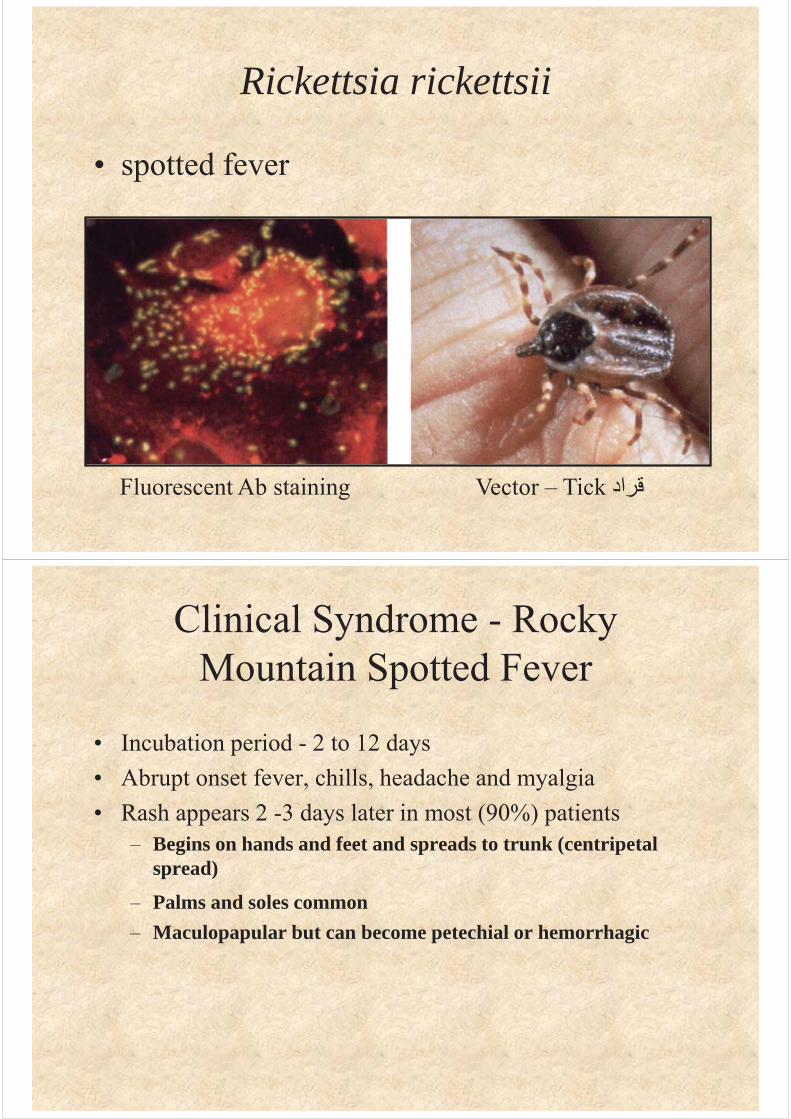
Rickettsia rickettsii
• spotted fever
Vector – Tick قرادFluorescent Ab staining
Clinical Syndrome - Rocky Mountain Spotted Fever
• Incubation period - 2 to 12 days• Abrupt onset fever, chills, headache and myalgia• Rash appears 2 -3 days later in most (90%) patients
– Begins on hands and feet and spreads to trunk (centripetal spread)
– Palms and soles common– Maculopapular but can become petechial or hemorrhagic
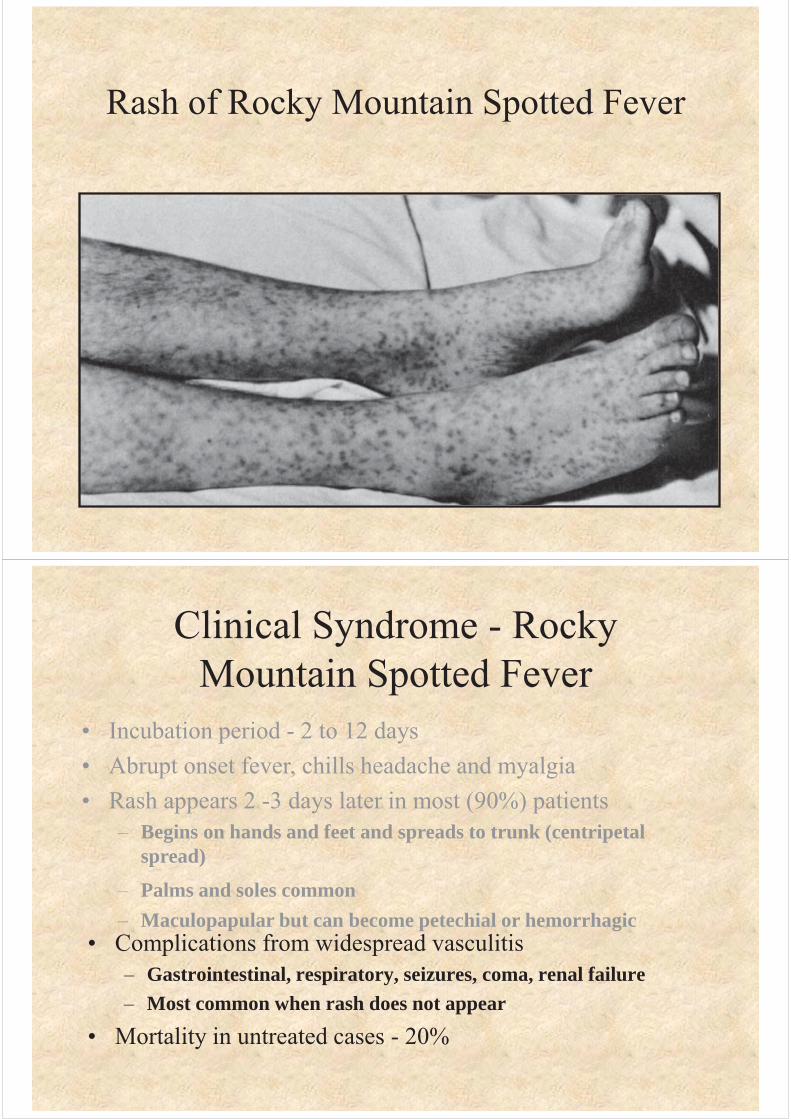
Rash of Rocky Mountain Spotted Fever
Clinical Syndrome - Rocky Mountain Spotted Fever
• Complications from widespread vasculitis– Gastrointestinal, respiratory, seizures, coma, renal failure– Most common when rash does not appear
• Mortality in untreated cases - 20%
• Incubation period - 2 to 12 days• Abrupt onset fever, chills headache and myalgia• Rash appears 2 -3 days later in most (90%) patients
– Begins on hands and feet and spreads to trunk (centripetal spread)
– Palms and soles common– Maculopapular but can become petechial or hemorrhagic
Laboratory Diagnosis - R. rickettsii
• Initial diagnosis - clinical grounds• Fluorescent Ab test for Ag in punch biopsy
- reference labs• PCR based tests - reference labs• Serology
– Indirect fluorescent Ab test for Ab– Latex agglutination test for Ab
Treatment, Prevention and ControlR. rickettsii
• Tetracycline– Prompt treatment reduces morbidity and
mortality• No vaccine• Prevention of tick bites (protective clothing,
insect repellents)• Prompt removal of ticks• Can’t control the reservoir
Typhus Group
Rickettsia prowazekii• Epidemic typhus• Brill-Zinsser disease
Fluorescent-Ab staining Vector - Louse
From: G. Wistreich, Microbiology Perspectives, Prentice Hall
Clinical Syndrome - Epidemic typhus• Incubation period approximately 1 week• Sudden onset of fever, chills, headache and myalgia• After 1 week rash
– Maculopapular progressing to petechial or hemorrhagic– First on trunk and spreads to extremities (centrifugal
spread)• Complications
– Myocarditis, stupor, delirium (Greek “typhos” = smoke)• Recovery may take months• Mortality rate can be high (60-70%)
Laboratory Diagnosis - R. prowazekii
• Isolation possible but dangerous• Serology
Treatment, prevention and ControlR. prowazekii
• Tetracycline
Rickettsia typhi
• Murine or endemic typhus
Epidemiology - R. typhiMurine or endemic typhus
• Occurs worldwide• Vector - rat flea برغوث
– Bacteria in feces• Reservoir - rats
– No transovarian transmission– Normal cycle - rat to flea to rat
• Humans accidentally infected
Flea
Clinical Syndrome- Murine Typhus
• Incubation period 1 - 2 weeks• Sudden onset of fever, chills, headache and
myalgia• Rash in most cases
– Begins on trunk and spreads to extremities (centrifugal spread)
• Mild disease - resolves even if untreated
Laboratory Diagnosis - R. typhi
• Serology– Indirect fluorescent antibody test
– Treatment: doxycycline
END
Top Related