UvA-DARE (Digital Academic Repository) Subunit specific ... · Subunit specific modulation of...
145
UvA-DARE is a service provided by the library of the University of Amsterdam (http://dare.uva.nl) UvA-DARE (Digital Academic Repository) Subunit specific modulation of sodium channels by anti-epileptic drugs Sun, G. Link to publication Citation for published version (APA): Sun, G. (2007). Subunit specific modulation of sodium channels by anti-epileptic drugs Zutphen: Wohrmann Print General rights It is not permitted to download or to forward/distribute the text or part of it without the consent of the author(s) and/or copyright holder(s), other than for strictly personal, individual use, unless the work is under an open content license (like Creative Commons). Disclaimer/Complaints regulations If you believe that digital publication of certain material infringes any of your rights or (privacy) interests, please let the Library know, stating your reasons. In case of a legitimate complaint, the Library will make the material inaccessible and/or remove it from the website. Please Ask the Library: http://uba.uva.nl/en/contact, or a letter to: Library of the University of Amsterdam, Secretariat, Singel 425, 1012 WP Amsterdam, The Netherlands. You will be contacted as soon as possible. Download date: 06 Jun 2018
Transcript of UvA-DARE (Digital Academic Repository) Subunit specific ... · Subunit specific modulation of...

UvA-DARE is a service provided by the library of the University of Amsterdam (http://dare.uva.nl)
UvA-DARE (Digital Academic Repository)
Subunit specific modulation of sodium channels by anti-epileptic drugs
Sun, G.
Link to publication
Citation for published version (APA):Sun, G. (2007). Subunit specific modulation of sodium channels by anti-epileptic drugs Zutphen: WohrmannPrint
General rightsIt is not permitted to download or to forward/distribute the text or part of it without the consent of the author(s) and/or copyright holder(s),other than for strictly personal, individual use, unless the work is under an open content license (like Creative Commons).
Disclaimer/Complaints regulationsIf you believe that digital publication of certain material infringes any of your rights or (privacy) interests, please let the Library know, statingyour reasons. In case of a legitimate complaint, the Library will make the material inaccessible and/or remove it from the website. Please Askthe Library: http://uba.uva.nl/en/contact, or a letter to: Library of the University of Amsterdam, Secretariat, Singel 425, 1012 WP Amsterdam,The Netherlands. You will be contacted as soon as possible.
Download date: 06 Jun 2018

Subunit specific modulation of sodium channels by anti-epileptic drugs
Guangchun Sun

ii
© Guangchun Sun, Shanghai, China, 2007 Printed by Wohrmann Print Service, Zutphen, The Netherlands Cover design: Annelies Olijslagers

Subunit specific modulation of sodium channels by anti-epileptic drugs
ACADEMISCH PROEFSCHRIFT
ter verkrijging van de graad van doctor aan de Universiteit van Amsterdam,
op gezag van de Rector Magnificus prof. dr. D.C. van den Boom, ten overstaan van een door het
college voor promoties ingestelde commissie, in het openbaar te verdedigen in de Agnietenkapel
op dinsdag 16 oktober 2007, te 12.00 uur
door
Guangchun Sun
geboren te Guizhou, Volksrepubliek China

iv
Promotiecommissie: Promotor: Prof. dr. W.J. Wadman Co-promotor: Dr. T.R.Werkman Overige leden: Prof. dr. P.A.J.M. Boon
Dr. J.J. Clare Prof. dr. M. Joëls Prof. dr. C.G. Kruse Prof. dr. F.H. Lopes da Silva Prof. dr. M.C. Michel Dr. R.A.Voskuyl
Faculteit der Natuurwetenschappen, Wiskunde en Informatica The research described in this thesis was carried out at the Center for Neuroscience of the Swammerdam Institute for Life Sciences, Universiteit van Amsterdam, The Netherlands. The research was financially supported by the Dutch National Epilepsy Foundation “The Power of the Small”.

v
ABBREVIATIONS 4-AP------------------ 4-aminopyridine AEDs ----------------- anti-epileptic drugs Cm -------------------- membrane capacitance CBZ ------------------ carbamazepine CHO ----------------- Chinese hamster ovary CNS ------------------ central nervous system DMSO --------------- dimethylsulfoxide DPH ------------------ phenytoin DRG ------------------ dorsal root ganglion EC50 ------------------ the concentration that causes half-maximal effect EGTA ---------------- ethylene glycol-bis(2-aminoethyl-ether)N,N,N’,N’-tetraacetic acid gmax ------------------- maximal conductance GABA ----------------γ-aminobutyric acid GEFS+ --------------- febrile seizures plus GHK ----------------- Goldman-Hodgkin-Katz H & H ---------------- Hodgkin and Huxley HCL ------------------ human chromosomal localization HEK ------------------ human embryonic kidney HEPES --------------- N-(2-hydroxyethyl)piperazine-N’-(2-ethanesulfanic acid) KA -------------------- kainate LTG ------------------ lamotrigine P0 ---------------------- maximal permeability P ---------------------- at postnatal day PIPES ---------------- piperazine- N,N’-bis(2-ethanesulfanic acid) disodium salt PN -------------------- peripheral neuron S.E.M ---------------- standard error of the mean SKM ------------------ skeletal muscle SMEI ----------------- severe myoclonic epilepsy of infancy TEA ------------------ tetraethylammonium mTLE ---------------- mesial temporal lobe epilepsy TPM ------------------ topiramate TTX ------------------ tetrodotoxin

vi
CONTENTS Chapter 1 1 General introduction Chapter 2 17 Sodium current properties in different models of epilepsy Chapter 3 25 A comparison of Biophysical and Pharmacological Properties of Human Brain Sodium Channel α-subunits NaV1.1, NaV1.2, NaV1.3 and NaV1.6 Expressed in HEK293 Cells Chapter 4 47 Sodium channel properties and functional changes by carbamazepine in rat hippocampal CA1 neurons during development Chapter 5 63 Kinetic changes and modulation by carbamazepine on voltage-gated sodium channels in rat CA1 neurons after epilepsy Chapter 6 79 Carbamazepine and topiramate modulation of transient and persistent sodium currents studied in HEK293 cells expressing the NaV1.3 α-subunit Chapter 7 93 General discussion References 107 Nederlandse Samenvatting (Summary in Dutch) 123 中文摘要 (Summary in Chinese) 133 Curriculum Vitae 135 Dankwoord/Acknowledgements 137

CHAPTER 1
General Introduction

Chapter 1
2
Functional role of the sodium channel, action potential generation
Action potentials are the rapidly propagated electrical messages that speed along the axons of the nervous system and over the surface membrane of many muscle and glandular cells. In axons they are brief, travel at constant velocity, and maintain constant amplitude in an all or none fashion. The action potential is a membrane potential change causing a change in conductance that results in the flow of ions through ion channels in the membrane (Hille, 2001). Voltage-gated sodium channels are responsible for the rising phase of the action potential in the membranes of neurons, whereas voltage-gated potassium channels mediate the repolarization process (Hodgkin and Huxley, 1952b, Hodgkin and Huxley, 1952a, Hodgkin and Huxley, 1952c, Hodgkin and Huxley, 1952d) (Fig. 1).
Hodgkin and Huxley recorded sodium currents, using the voltage clamp technique and described their features in a new classical formalism, based on: (1) selective ion conductance, (2) voltage-dependent activation, and (3) rapid inactivation (Hodgkin and Huxley, 1952d), see Box 1. Detailed analysis of sodium channel function during the 1960s and 1970s using the voltage clamp method applied to invertebrate giant axons and vertebrate myelinated nerve fibers yielded mechanistic models for sodium channel function (Armstrong, 1981, Hille, 2001). The sodium channel protein was characterized in 1980, by biochemical approaches- e.g. measurement of ion flux through the channel, high affinity binding of neurotoxins, and detergent solubilization and purification of sodium channel proteins labeled by neurotoxins (Ritchie and Rogart, 1977). The sodium channel protein undergoes voltage-dependent conformation changes that regulate pore conductance and the Hodgkin and Huxley’s (H&H) model accounts for ion fluxes and voltage dependent permeability changes of the excitable membrane (Hille, 2001) (box-1). Box-1: The Hodgkin and Huxley formalism for voltage dependent ion channels
In their original papers H&H stated three important assumptions that underlie
their analysis 1) Ionic currents for Na+ and K+ are independent of each other; 2) The ion channels that control the currents can be in several distinct conformational states. The kinetics of the currents are mainly determined by the number of states and the transitions between these states; 3) The voltage dependence arises because all rate constants that determine the transitions between different states are voltage dependent. This set of assumptions was sufficient to characterize the essentials that were known at that time and it also correctly predicted the propagation of an action potential along an axon (Hodgkin and Huxley, 1952d, Hodgkin and Huxley, 1952a).
In this box the formalism for the Na+ current is discussed, which can easily be expanded to describe the kinetics of all voltage dependent channels. Even to date the H&H formalism is still sufficient to describe the macroscopic currents through voltage dependent channels. The sodium current can activate and inactivate so that we need at least three different states to describe it: an open state (O), a closed state (C) and an inactivated state (I).
The transition between the closed and the open state models the process of activation. Assume that a fraction m of the channels is in the open state O and therefore

General Introduction
3
the fraction 1-m is in the closed state C:
mmOCVV
−⇔
1
)(),( βα
α(V) and β(V) are the voltage dependent rate constants for respectively opening and closing. If the equilibrium between closed and open state can be described as a simple first order chemical reaction the time course of the opening of the channels should obey the following differential equation:
)()()1( VmVmdtdm βα ×−×−=
which for a constant voltage V leads to the equilibrium distribution (m∞) and time constant ( τ ):
)()(
1)()()(
)()(VV
VVV
VVmβα
τβα
α+
=+
=∞
which are determined at a certain membrane voltage under “voltage clamp” experimental conditions, keeping the voltage constant, to get a better estimation.
In a similar manner the occupancy of the inactivated state can be described from the transition of channels between the inactivated state (I) and the closed state (C), with its own specific rate constants γ(V) and δV), where h is the fraction of the channels in the closed state C and therefore 1-h defines the fraction in the inactivated state I:
hhIC
−⇔
δγ
1
)V(),V(
which leads to:
)()(1)(
)()()()(
VVV
VVVVh
δγτ
δγγ
+=
+=∞
Finally H & H empirically determined that the actual sodium conductance was best described by: max
3 ghmg Na ××= which for a driving force described by the Nernst equation (ENa) leads to a current of: )(max
3NaNa EVghmI −×××=
in which g max is the maximum conductance and ENa is the equilibrium potential of sodium. Or, when using the Goldman-Hodgkin Katz current equation, to:
)exp(1
)exp()][][(
)( max3
V
VNaNa
VghmNaI out
in
α
α
−−
−−++
××××= with RTF
=α
With this model the following sequence of events during an action potential (Fig. 1) is described in mathematical terms. At resting membrane potentials, most channels are in the closed state. In response to membrane depolarization, channels activate within a few hundred microseconds, and will quickly move into the open state. Channels cannot open

Chapter 1
4
from the inactivated state, so the maximum current that is generated strongly depends on the voltage at which activation starts. Once open and at a depolarized potential most channels will quickly (within a few milliseconds) convert to the non-conducting inactivated state. The membrane voltage has to repolarize to a relatively low voltage in order for the channel inactivation to be removed; the channels then transit from the inactivated to the closed state and are available for opening again. This takes time, which limits the firing frequency. During the depolarization, m rises rapidly and h falls slowly. Taking the cube of m sets up a small delay in the rise, and multiplying it by the slowly falling h makes m3h eventually fall to a low value again. After depolarization, m recovers rapidly and h slowly to the original values.
Brain sodium channels cycle through these three functional states within the few milliseconds that an action potential lasts. This characteristic is essential for sustaining rapid trains of action potentials necessary for brain function (Ragsdale and Avoli, 1998).
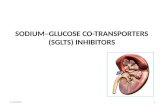
Figure 1. Action potential and underlying changes in Na and K conductions calculated from the H&H model at 18.5oC. After membrane depolarization, sodium currents activate rapidly and the depolarization becomes regenerative, but even before the peak of the action potential, inactivation starts and the sodium permeability falls back to its original value. The strong depolarization (slowly) activates potassium current, which is needed to repolarize the membrane. The time course of repolarization depends on the rate of sodium channel inactivation and the rate of potassium channel activation. For a brief period after the action potential, the membrane is absolute refractory as a fraction of the sodium channels is inactivated, thereafter the large potassium conductance results in a relative refractory period (Hille, 2001). Molecular properties of the sodium channel
Sodium channel proteins in the mammalian brain consist of аn α-subunit of approximately 260 kDa in association with auxiliary subunits of 33 to 36 kDa - β1, β2, β3 and β4 (Catterall, 1984, Catterall, 1992, Catterall, 2000, Yu et al., 2003) (Table 1). So far nine α-subunits have been shown to form functional sodium channels— NaV1.1 to NaV1.9 (Goldin et al., 2000) (Table 1). These subunits consist of four homologous domains (I–IV), each of which contains six α -helical transmembrane segments (S1–S6) and a membrane re-entrant loop that dips into the trans-membrane region of the protein between transmembrane segments S5 and S6. The N-terminal and C-terminal domains are intracellular (Noda et al., 1984, Numa and Noda, 1986, Catterall, 2000) (Fig.2). The

General Introduction
5
S4 segments in each domain serve as the voltage sensors, the S5 and S6 segments and the re-entrant loop between them form the lining of the pore, and the short intracellular loop between domains Ш and IV forms the inactivation gate (Figs. 2 and 3). Auxiliary β 1 and β 2 subunits contain immunoglobulin-like folds. The immunoglobulin-like fold is a sandwich of two β sheets held together by hydrophobic interactions and forms the interface with the α subunit (Fig. 2).
Even coexpression of the β subunit is required for full reconstitution of the properties of native sodium channels, as these auxiliary subunits modify the kinetics and voltage-dependence of the gating (that is, opening and closing) of the channel (Isom et al., 1994, Catterall, 2000, Cantrell and Catterall, 2001, Yu and Catterall, 2003, Yu et al., 2005). The ion-conducting aqueous pore is contained entirely within the α subunit, and the essential elements of sodium-channel function – channel opening, ion selectivity and rapid inactivation – can be demonstrated when α subunits are expressed alone in cells (Goldin et al., 1986, Noda et al., 1986b, Scheuer et al., 1990, Catterall, 2000, Cantrell and Catterall, 2001, Yu and Catterall, 2003).
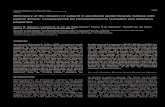
Figure 2. The primary structures of the subunits of the voltage-gated sodium channels are illustrated as transmembrane folding diagrams. The extracellular domains of the β1 and β 2 subunits are shown as immunoglobulin-like folds, which interact with the loops in the α subunits as shown. Roman numerals indicate the domains of the α subunit; segments 1-5 indicate the transmembrane spanning regions of each domain. Segments 5 and 6 are the pore-lining segments and the S4 helices make up the voltage sensors. Circles in the intracellular loops of domains III and IV indicate the inactivation gate IFM (I1488, F1489 and M1490) motif and its receptor (h, inactivation gate); P, phosphorylation sites (in circles, sites for protein kinase A; in diamonds, sites for protein kinase C); ψ, probable N-linked glycosylation site. The circles in the re-entrant loops (segment 5 and 6) in each domain represent the amino acids that form the ion selectivity filter (Catterall, 2000, Yu and Catterall, 2003).

Chapter 1
6
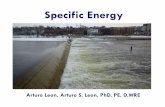
Figure 3. The hinged-lid mechanism of inactivation of sodium channels. The intracellular loop connecting domains III and IV of the sodium channel is depicted as forming a hinged lid with the critical phenylalanine (F1489) within the IFM (I1488, F1489 and M1490) motif shown occluding the mouth of the pore during the inactivation process. The circles represent the transmembrane helices (Catterall, 2000, Yu and Catterall, 2003). So far four different sodium channel subtypes have been identified in rat brain:
NaV1.1, NaV1.2, NaV1.3 and NaV1.6 (Noda et al., 1986a, Kayano et al., 1988, Schaller et al., 1995) (Table 1). The originally identified as cardiac sodium channel NaV1.5 subtype also appears to be present in the brain (mainly in limbic structures but not in hippocampus) (Hartmann et al., 1999, Wu et al., 2002). Moreover, type NaV1.2, NaV1.3 and NaV1.6 genes encode two isoforms, termed A (for adult) and N (for neonatal), as a result of a mutually exclusive splicing (developmentally regulated) of a single exon (Auld et al., 1988, Sarao et al., 1991, Gustafson et al., 1993, Plummer et al., 1998).
The human sodium channel α subunit proteins exhibits a distinct subcellular localization patterns. Types NaV1.1, NaV1.3 and NaV1.6 immunoreactivity are predominantly in neuronal cell bodies and proximal processes, whereas type NaV1.2 is concentrated along axons (Whitaker et al., 2001b). This is similar to rat brain and suggests that different sodium channel subtypes have distinct functions that are highly conserved between human and rodents. However, a recent study indicated that NaV1.1 channels may also be predominantly located on axons (Ogiwara et al., 2007). There is a broader expression of type NaV1.3 in adult human brain than in adult rat brain (Whitaker et al., 2001b). Generally, Nav1.1 and Nav1.3 control neuronal excitability through integration of synaptic impulses to set the threshold for action potential initiation and propagation to the dendritic and axonal compartments, whereas NaV1.2 conducts the action potential (Westenbroek et al., 1989, Trimmer and Rhodes, 2004). During development, NaV1.6 has been shown to replace NaV1.2 in maturing nodes of Ranvier, the gaps in the myelin sheaths of myelinated axons where saltatory action potential conduction takes place (Boiko et al., 2001, Kaplan et al., 2001, Yu and Catterall, 2003).

General Introduction
7
Table 1. Voltage-gated sodium channel family (Catterall, 2000, Morgan et al., 2000, Hille, 2001, Isom, 2001, Whitaker et al., 2001b, Yu et al., 2003, Birch et al., 2004, Catterall et al., 2005, Yu et al., 2005).
α subunit
other names
Gene name HCL Auxiliary
subunits Key tissue
distribution
Nav1.1 type I SCN1A 2q24 β1,β2,β3,β4 Brain, spinal cord
Nav1.2 type II SCN2A 2q23–24 β1,β2,β3,β4 Brain, spinal cord
Nav1.3 type III SCN3A 2q24 β1,β3 Brain
(embryonic in rat)
Nav1.6 type VI /NaCh6
/PN4 SCN8A 12q13 β1,β2
Brain, spinal cord, glia, DRG
Nav1.4 SKM1 SCN4A 17q23–25 β1 Skeletal muscle
Nav1.5 h1 SCN5A 3p21 β1,β2,β3,β4 Heart muscle (Brain)
Nav1.7 PN1 /hNE /NaS
SCN9A 2q24 β1,β2
DRG, neuroendocrine
cells
Nav1.8 SNS /PN3 SCN10A 3p22-24 Unknown DRG
Nav1.9 SNS2 /NaN /PN5
SCN11A 3p21-24 Unknown DRG
β
subunit
Navβ1 SCN1B 19q13 Brain, muscle, DRG
Navβ2 SCN2B 11q22 Brain
Navβ3 SCN3B 11q24 Brain
Navβ4 SCN4B 11q23 Brain, spinal cord
Abbreviations: DRG, dorsal root ganglion; HCL, human chromosomal localization; PN, peripheral neuron; SNS, sensory neuron specific; SKM, Skeletal muscle.

Chapter 1
8
Box-2: The relation between single channels and macroscopic current
In their original papers H&H did not explicitly state what the molecular form of the “channels” and the “gates” was. Since the great advances in molecular biology we now know that “channels” are membrane proteins and what these proteins look like. Many of them have been cloned and can now be investigated in isolation. This also implies that we have a much better concept of how the real channels operate at the molecular level. In this thesis a description at the level of ionic currents suffices, but in this box we will shortly explain how the macroscopic properties of the currents are related to the molecular properties of the channels. The basic mechanisms of the currents explained in Box-1 are a description of phenomena that are based on real molecular assumptions. The large channel proteins are folded in the membrane in such a way that they indeed form a watery channel, just big enough to let single ions pass. The sodium channel was one of the earliest ones to be cloned (Noda et al., 1984) and many of the details of its structure-function relations are known. In recent years a lot of knowledge has been gathered about the selectivity filter that determines the selective permeability of the channel, about the voltage sensors of ion channels (see specific facts on voltage-gated K+ channels (Gulbis and Doyle, 2004, Yu et al., 2005)) and about mechanisms responsible for properties like inactivation. The easiest way to translate the H&H model of the ionic current into channel properties is illustrated in Fig 4. The channel is presented as a conducting pore when the channel is in the open state, depending on voltage depolarization.
Figure 4. The sodium channel state and the sodium channel current under the cell-attached voltage clamp condition. When the membrane voltage is depolarized, the channel opens and sodium influx occurs (Bear et al., 2006).
The relation between the properties at the single channel level and the ones of the

General Introduction
9
macroscopic current are illustrated in Fig. 5, where an ensemble of 10 single channel sodium currents recorded in response to a depolarizing voltage step from –80 mV to –40 mV is shown and averaged (bottom trace). Their response is stochastic. After the depolarizing step, the channel can be open, but the time it takes until the first opening is stochastic; in fact a detailed analysis of the distribution of the intervals to first opening appears to follow a Poisson distribution, characterized by a mean time that is exactly equal to the time constant of activation obtained from the whole cell current shown as the bottom trace. Also the mean opening time of the channel, measured as the duration during which the channel is in the conducting state follows a Poisson distribution and its characteristic time is related to the time constant of inactivation in the current trace.
Generalizing we can conclude that whenever we encounter rate constant in the H&H state model, it represents a transition between distinct stochastic states in the single channel model.
(A) UNITARY SODIUM CURRENTS
Figure 5. Relation between single channels and macroscopic current (A) Ten consecutive trials of sodium currents are recorded during a voltage step from -80 to -40 mV. The open sodium channel has a conductance of about 2.2 pA. Dashed line indicates the current level when sodium channels are closed. (B) The ensemble average of 352 repeats of the same protocol (Hille, 2001).

Chapter 1
10
Many studies have shown that sodium channels in the brain have distinct
expression patterns depending on the distinct brain regions as well as the stages of development. For example, types NaV1.1, NaV1.2 and NaV1.6 are abundant in adult brain whereas type NaV1.3 was supposed to be mainly expressed at late embryonic and early postnatal time points (Felts et al., 1997, Chen et al., 2000), although more recently it has been shown that type NaV1.3 immunoreactivity is present in the adult rat brain (Lindia and Abbadie, 2003). In addition, in the human brain type NaV1.3 is detectable in many different brain structures (Chen et al., 2000, Whitaker et al., 2001b). All subtypes are detectable in the rat hippocampus (Black et al., 1994, Krzemien et al., 2000). For β subunits, β1 and β2 subunits only occurred after postnatal day 3 (P3), whereas the β3 subunit is already present in embryonic tissues (Shah et al., 2001).
The somato-dendritic localization of NaV1.1, NaV1.3 and NaV1.6 sodium channels (see above), which activate at sub-threshold membrane potentials, may be important for generating the non-inactivating or ‘persistent’ sodium currents, and may boost EPSPs originating in distal dendrites as they spread to the cell soma (Whitaker et al., 2001b). Interestingly, when expressed in HEK293 mammalian cells the cloned human type NaV1.1, NaV1.3 and NaV1.6 α-subunits give rise to substantially higher levels of spontaneous persistent current than the type NaV1.2 channel (Chen et al., 2000). Modulation of the sodium channel
Modulation of sodium currents is very important in the brain, although specific deficits that directly affect sodium channel regulation are not yet known. Mutations that subtly alter neuronal voltage-gated sodium channel function can lead to human diseases of hyperexcitability, like epilepsy (Armijo et al., 2005, Meisler and Kearney, 2005, Koopmann et al., 2006, Yamakawa, 2006, Avanzini et al., 2007, Waxman, 2007). The SCN1A gene encoding the NaV1.1 neuronal sodium channel α subunit is currently the most clinically relevant of all the known epilepsy genes (Mulley et al., 2005) and a number of epilepsy syndromes are associated with SCN1A gene mutations (Escayg et al., 2000, Claes et al., 2001, Fujiwara et al., 2003), e.g. febrile seizures plus (GEFS+) and severe myoclonic epilepsy of infancy (SMEI) (Vanoye et al., 2006).
SCN1A mutations could alter channel inactivation, resulting in persistent inward sodium current which will likely enhance excitability of neuronal membranes by causing prolonged membrane depolarization (Escayg et al., 2000, Lossin et al., 2002). The persistent sodium current and window current
The persistent sodium current is a noninactivating component of the tetrodotoxin-sensitive sodium current. It may arise from a modal change in gating of conventional sodium channels (Crill, 1996, Taddese and Bean, 2002). Direct interactions of sodium channels with βγ subunits of G proteins might be one of the mechanism of inducing persistent sodium currents (Ma et al., 1994, Ma et al., 1997). The persistent sodium current is thought to be important for integration of neuronal responses, so the

General Introduction
11
modulation of sodium channel gating by G βγ subunits is expected to have profound effects on neuronal excitability (Ma et al., 1997).
The persistent sodium current might have a key role in regulating excitability near firing threshold because it is largely unopposed by other voltage-activated currents in this range of membrane potentials. Moreover, there is evidence that the persistent sodium current contributes to the initiation and maintenance of epileptiform activity (Segal and Douglas, 1997). The persistent sodium current is greater in animal models of epileptogenesis, (Ketelaars et al., 2001, Agrawal et al., 2003, Ellerkmann et al., 2003). Moreover, sodium channel mutations that are associated with epilepsy in mice and humans have been found to enhance the persistent sodium current (Lossin et al., 2002).
The “window current” is also a noninactivating component of the tetrodotoxin-sensitive sodium current, but comes directly from the model of Hodgkin & Huxley (Hodgkin and Huxley, 1952d). In the Hodgkin-Huxley whole-cell current properties, plots of h∞ (the probability that a sodium channel is not inactivated) and m∞ (the probability that a sodium channel is activated), against membrane potential overlap over a small potential range, predicting a steady sodium conductance over this range. The “window current” should be affected by the shift in voltage dependence of activation and inactivation. Epilepsy
Epilepsy, one of the most common neurologic disorders, is a major public health issue, affecting about 4% of individuals over their lifetime (Browne and Holmes, 2001). The term epilepsy refers to a collection of disorders of the central nervous system (CNS) exhibiting disturbances of brain function characterized by the repeated occurrence of seizure activity. Most epileptic episodes are idiopathic although, occasionally, sympathomatic seizures can be attributed to head trauma, brain tumor, cerebrovascular problems, etc. The classification of seizure disorders has gradually undergone modification over the years, and the latest attempt was published in 1989 by the Commission on Classification and Terminology of the International League Against Epilepsy (Epilepsia, 30(4): 389-399, 1989). Mesial temporal lobe epilepsy (mTLE) is the most common form of adult focal epilepsy (Engel et al., 1989) and is characterized by chronic seizures that often originate in the hippocampal formation (Sloviter, 1994).
Epileptic seizures are induced by abnormal focal or generalized synchronized electrical discharges within the CNS. The equilibrium in communication between neurons is regulated by a network of excitatory and inhibitory circuits. Enhancement of excitatory or impairment of inhibitory mechanisms will disturb this equilibrium, and the intrinsic properties of individual neurons do also contribute. Since ion channels provide the basis for all these processes, any mutation-induced channel malfunction can directly alter brain excitability and can directly or indirectly induce epileptic seizures (Lerche et al., 2001, Armijo et al., 2005).
Epilepsy reflects neuronal hyperexcitability, arising from largely unknown genetic, molecular, cellular and network mechanisms (Avoli et al., 2005, Crino, 2007). Idiopathic epilepsies, which account for up to 40% of all epilepsies, are mainly caused by genetic factors (Steinlein, 2002) and often involve channelopathies, including sodium channel mutations (Armijo et al., 2005, Koopmann et al., 2006, Avanzini et al., 2007, Waxman,

Chapter 1
12
2007). In generalized epilepsy with febrile seizures plus (GEFS+), mutations in three genes coding for voltage-gated sodium channel α or β1 subunits (SCN1A, SCN2A, SCN1B) and one GABA receptor subunit gene (GABRG2) have been identified (Wallace et al., 1998, Escayg et al., 2000, Celesia, 2001, Moulard et al., 2001, Sugawara et al., 2001, Lossin et al., 2002, Steinlein, 2002, Lossin et al., 2003, Mulley et al., 2003, Ceulemans et al., 2004, Armijo et al., 2005). In addition, also mutations in the SCN5A gene (encoding the NaV1.5 channel) have been suggested to underlie inherited epilepsy (Hartmann et al., 1999).
Animal models for temporal lobe epilepsy
Due to the ethical and experimental limitations of human studies, appropriate animal models for epilepsy are essential. Animal models have been developed for studying the basic mechanism(s) of epileptogenesis and the characteristics of chronic epilepsy (Hellier et al., 1998).
There are various experimental animal models for epilepsy that reflect the pathophysiology of human epilepsy. Chronic epilepsy models can be divided into acquired (symptomatic) epilepsy models, including the kindling model of epilepsy, post-status epilepticus models of TLE in which epilepsy develops after an induced sustained status epilepticus; and genetic (idiopathic) models that lead to different types of epilepsy. Currently, the kindling model (Bertram, 2007) and post-status models (kainite (Sun et al., 2006, Cross and Cavazos, 2007), pilocarpine (Borges et al., 2006, Pereira et al., 2007, Pitsch et al., 2007) or stimulus (Magalhaes et al., 2004, Borowicz et al., 2007) induced models) are the most widely used models for studies on epileptogenic processes. The seizures in these models can be used for testing of antiepileptic drug effects (Loscher, 2002), although many other realistic seizure models exist, such as transgenic or knockout mice with induced mutations (Noebels, 1999, Prasad et al., 1999). Pharmacological properties of anti-epileptic drugs
Despite progress in understanding the pathogenesis of seizures and epilepsy (McNamara, 1999), the cellular basis of human epilepsy is not completely understood. In the absence of a specific etiological understanding, approaches to drug therapy of epilepsy have necessarily been directed at the control of symptoms avoiding interference with normal brain function, i.e. the suppression of seizures by chronic administration of antiepileptic (anticonvulsant) drugs (AEDs). Most of these drugs were found empirically and afterwards some of their mechanisms of action have been elucidated. Clinically used AEDs decrease membrane excitability by interacting with ion channels or neurotransmitter receptors. Currently available AEDs appear to act on sodium channels, GABAA receptors, or calcium channels (Macdonald and Kelly, 1993, Macdonald and Kelly, 1994, Macdonald and Kelly, 1995, Meldrum, 1996, Rogawski and Loscher, 2004a, Meldrum and Rogawski, 2007). The pharmacotherapy of epilepsy includes over 20 different medications, mostly divided into older (‘first generation’) drugs e.g. phenobarbital, phenytoin (DPH), carbamazepine (CBZ), and valproate, and new (‘second generation’) drugs such as lamotrigine (LTG), topiramate (TPM), vigabatrin, tiagabine, gabapentin, and levetiracetam (Loscher and Schmidt, 2002). In our research we mainly

General Introduction
13
focused on CBZ, LTG, and DPH which are the most frequently prescribed drugs in the clinic and which all interact with voltage-gated sodium channels.
A short clinically connected description of the drugs used in this thesis is given below:
CBZ is an iminostilbene derivative of tricyclic antidepressants (Fig. 6) with a very short amide side chain. It exhibits a spectrum of anticonvulsant activity very similar to that of DPH (Rogawski and Porter, 1990). In humans, it is effective against partial and generalized tonic–clonic seizures, but not against absence seizures (Ragsdale and Avoli, 1998).
LTG is a phenyltriazine (Fig. 6) that emerged from the screening of putative antifolates as anticonvulsant agents. It is a simple compound composed of only two aromatic rings. LTG has proven to be a promising new treatment for partial and generalized tonic–clonic seizure (Rogawski and Porter, 1990, Yuen, 1994). In addition, it may also have utility in the management of primary generalized epilepsy with absence attacks (Ragsdale and Avoli, 1998).
DPH is a hydantoin containing the ureide structure (Fig. 6), which is traditionally viewed as an important structural motif responsible for antiepileptic activity. It was first described by Merritt and Putman (Merritt and Putnam, 1938) and it has subsequently been shown to be efficacious in treating partial and generalized tonic–clonic seizures in humans. The remarkable property of DPH is that it is capable of preventing seizures without producing sedation. Thus, DPH was the first AED to approach the therapeutic ideal of inhibiting abnormal brain activity characteristic of seizures without appreciably interfering with normal brain activity (Ragsdale and Avoli, 1998).
TPM, a sulfamate-substituted monosaccharide (Fig. 6), is a relatively new AED. It has broad-spectrum activity, being efficacious against partial seizures and various generalized seizure types (Perucca, 2005). Its anticonvulsant action relies on interactions with various neurotransmitter and/or ion channel systems, e.g. inhibition of kainate-evoked currents (Gibbs et al., 2000), enhancement of GABA-evoked currents (White et al., 1997), inhibition of voltage-activated calcium currents (Zhang et al., 2000), but also block of (persistent) sodium currents (Zona et al., 1997, Taverna et al., 1999).
Carbamazepine Lamotrigin

Chapter 1
14
Phenytoin Topiramate
Figure 6. Structures of AEDs used in this study.
CBZ, LTG, and DPH have a similar spectrum of activity in animal seizure models
and in human epilepsies. They all show voltage- and frequency- dependent suppression of sodium currents, which has been implicated as the major mechanism underlying their antiepileptic effect (Rogawski and Porter, 1990, Kuo and Lu, 1997, Ragsdale and Avoli, 1998, Rogawski and Loscher, 2004a). The use-dependent block of discharges is of great mechanistic interest as it readily explains why these nonsedative antiepileptics may effectively inhibit seizure discharges, yet spare most normal activity (Kuo and Lu, 1997). These drugs do not reduce the amplitude or duration of single action potentials but reduce the ability of neurons to fire trains of action potentials at high frequency (Macdonald and Kelly, 1993, Macdonald and Kelly, 1994, Macdonald and Kelly, 1995, Meldrum, 1996). The action of the AEDs appears to be due to a shift of sodium channels to an inactive state that is similar to the normally occurring inactive state but from which recovery is delayed (Macdonald and Kelly, 1993). This stabilization of the inactive form of the channel results in frequency- dependent block of sodium channels and in the blockade of sustained high-frequency repetitive firing of action potentials evoked from reduced membrane potentials (Macdonald and Kelly, 1993).
These three anticonvulsants all have much higher affinity to the inactivated state than to the resting or open state of the sodium channel via a simple bimolecular reaction (a one-to-one binding process) (Macdonald and Kelly, 1993, Kuo, 1998), but long (seconds) depolarizations are needed for drug binding to the channels (Matsuki et al., 1984, Lang et al., 1993, Kuo and Bean, 1994b, Kuo and Bean, 1994a, Xie et al., 1995). They are effective inhibitors of sodium currents only when applied externally, not internally, suggesting that they bind to a common site of the sodium channel located extracellularly (Kuo, 1998).
LTG and DPH may potently inhibit sodium currents by slow binding to the fast inactivated state of sodium channels (Kuo et al., 1997). Compared to DPH, CBZ has 3-fold lower affinity for depolarized channels, but binds to these channels with a five time faster rate (Kuo et al., 1997). Thus, CBZ may be more effective than DPH under epileptic conditions with relatively fast depolarizing shifts. This difference may in part explain why some patients respond better to DPH whereas others are more effectively treated with CBZ (Ragsdale and Avoli, 1998).

General Introduction
15
In addition to effects on the fast voltage-gated sodium current that is responsible for the upstroke of the action potential, AEDs might also act by blocking the persistent sodium current. Several authors have reported that phenytoin (Chao and Alzheimer, 1995, Segal and Douglas, 1997, Lampl et al., 1998, Niespodziany et al., 2004) and topiramate (Taverna et al., 1999) inhibit the persistent sodium current at concentrations lower than those that block fast sodium current. The selective reduction of late, persistent sodium channel openings might contribute to the ability of these drugs to protect against seizures. Pharmacoresistance to AEDs
Although currently available AEDs are effective, at least 30% of all epilepsies are refractory to current AEDs, especially those with complex partial seizures (Macdonald and Kelly, 1993, Loscher and Schmidt, 2002). During recent years, a large number of new AEDs have been marketed worldwide, but the proportion of patients failing to respond to drug treatment has not changed to a significant extent (Brodie and Porter, 1990, Brodie, 2001). Thus, new concepts and original ideas for developing AEDs are urgently needed (Loscher and Schmidt, 2002).
In chronic epilepsy, many patients develop resistance to anticonvulsant drug treatment during the course of their disease, with the underlying mechanisms remaining unclear. Two main concepts have been advanced to explain drug resistance. 1) The overexpression of multidrug transporters, especially P-glycoprotein (Pgp), restricts the access of these drugs to their site of action (Abbott et al., 2002, Loscher and Potschka, 2002, Rizzi et al., 2002, Remy et al., 2003a, Weiss et al., 2003, Remy and Beck, 2006). 2) Molecular drug targets may undergo genetic (see the paragraph “Modulation of the sodium channel”) or functional modification after which they are no longer sensitive to their ligands. It was reported that the composition of sodium channel subunits was changed after epilepsy. For example, the expression of NaV1.3 channels was markedly increased in rat hippocampus following kainic acid-induced seizures (Bartolomei et al., 1997). In human epileptic hippocampus, a markedly up-regulation of NaV1.3 channel was detected, whereas the NaV1.2 channel was significantly down-regulated (Whitaker et al., 2001a). In addition, the increased expression of neonatal isoforms of NaV1.2 and NaV1.3 channels was observed in hippocampal neurons, dentate granule cell layer and microglial cells after electrically-induced status epilepticus (Aronica et al., 2001). Furthermore, the sodium channel β1 subunit was up-regulated in astrocytes of epilepsy model rats (Catania et al., 2003) and in glia of epilepsy patients (Aronica et al., 2003). These results collectively suggest that changes in sodium channel (subunits) might partly underlie the pharmaco-resistence of AEDs. The studies in this thesis were performed based on this hypothesis. Outline of this thesis
The aim of this thesis is to understand the functional role of sodium channels in epilepsy. Since earlier work has shown the changed expression of sodium channel subunits after epilepsy (see above), the question arose whether (subtle) differences of drug sensitivities between sodium channel subunits could be involved in the pharmacoresistance observed in epilepsy. HEK-cell lines stably expressing the human

Chapter 1
16
brain sodium channel α subunits NaV1.1, NaV1.2, NaV1.3 and NaV1.6 comprise a useful tool to study the function of α subunits in a standardized expression system. Furthermore, we translated our studies to the sodium channels in dissociated CA1 hippocampal neurons with different subunit composition, during development and after epilepsy.
In Chapter 2, a background theory is discussed to illustrate the study of sodium channel function (and the interactions of AEDs with these channels) under voltage clamp conditions. The parameters of sodium channel properties are illustrated with a modeling study based on actual experiments in CA1 hippocampal pyramidal neurons.
In Chapter 3, the electrophysiological properties of the human brain sodium channel α subunits NaV1.1, NaV1.2, NaV1.3 and NaV1.6 expressed in HEK293 cells are studied. In addition, the modulation of the four sodium channels α-subunits by the commonly used AEDs CBZ, LTG and DPH is investigated.
In Chapter 4, the sodium channel function as well as its modulation by CBZ in rat neonatal and adult hippocampal CA1 neurons is studied. The purpose of the study is to detect whether changes in the composition of sodium channel α-subunits during development underlie a different sensitivity to CBZ.
In Chapter 5, the sodium channel function as well as its modulation by CBZ in rat hippocampal CA1 neurons after kainate-induced epilepsy is studied. The purpose of the study is to determine whether sodium channels of epileptic tissues display a different CBZ sensitivity as compared with sodium channels of control tissue.
In Chapter 6, the inhibition of the persistent sodium current in NaV1.3 α-subunit expressed in HEK293 cells by CBZ and TMP is compared. Also the effects of these two AEDs on the transient sodium current are compared. The purpose of the study is to determine to what extent the interactions of CBZ and TPM with the two sodium current components contribute to the anti-epileptic profile of these AEDs.
In Chapter 7, we summarize and discuss the conclusions drawn in the preceding chapters and their implications with regard to the efficacy of AEDs on sodium channel (subtypes).

CHAPTER 2
Sodium current properties in different models of epilepsy
Wytse J. WADMAN, Rogier MIN, and Guangchun SUN
In: Corcoran M, Moshe L, eds. Kindling 6. Amsterdam: Springer, 61-70 (2005)

Chapter 2
18
1. INTRODUCTION
The voltage dependent sodium current determines the upstroke of the action potential and it is therefore one of the determinant factor for neuronal excitability. The steep voltage dependence of activation as well as inactivation in combination with it fast kinetics imply that even relatively small changes in sodium current properties will have a significant influence on for example cell firing frequency. It is therefore not surprising that the majority of anti epileptic drugs (AEDs) exert their action by modulating sodium current properties that are relevant for cell firing (for review see Kohling, 2002). The aim of this study is to parameterize the sodium current in CA1 hippocampal pyramidal cells using the classical description originally provided by Hodgkin and Huxley (Hodgkin and Huxley, 1952d, Hodgkin and Huxley, 1952a) employing voltage clamp data obtained from neurons acutely isolated from the rat hippocampus . Such a description does not comprise every possible detail of the present knowledge of the sodium channel. Nevertheless it appears to be sufficient to describe the changes observed in the inactivation function of the sodium current in neurons isolated from the epileptic focus in rats that were either kindled (Vreugdenhil et al., 1998) or in which a status epilepticus model was generated (Ketelaars et al., 2001).
The most effective drugs against epileptic seizures exert their effect by specifically shifting the inactivation function in a hyperpolarizing direction in a concentration dependent manner. This modulation can be incorporated into the kinetic scheme of the sodium current as a binding to the inactivated state based on actual experiments in the cells under study. With the description of the sodium current at hand a model neuron was implemented in the NEURON simulation environment (Hines and Carnevale, 1997) so that its firing properties could be simulated under current clamp conditions. This offers the possibility to predict how carbamazepine binding could affect the firing behavior of these neurons.
2. Na-CURRENT IN CA1 PYRAMIDAL NEURONS
The classical description of the sodium channel (Hodgkin and Huxley, 1952d, Hodgkin and Huxley, 1952a) postulates that the current is controlled by an activation gate (m: the fraction of open gates) and an inactivation gate (h) that together control the voltage and time dependence of the conductance for sodium. The kinetics in the model is determined by the state of the gates, while the voltage dependence is incorporated in the rate constants that define the state transitions: NaNa gthtmtg ××= )()()( 3 (1) where h defines the fraction of the h gates in the open state hh VV hh −⎯⎯ →⎯⎯⎯ ⎯← 1)()( αβ (2) and the change in h is given by
hVhVdtdh
hh ×−−×= )()1()( αβ (3)
The rate constants α and β determine the steady state (h∝) at a certain membrane
voltage and the voltage dependent time constant of h. A similar set of equations (2-3) can

Sodium current properties in different models of epilepsy
19
Figure 1. Examples of fits to sodium currents evoked with various protocols in CA1 pyramidal neurons acutely, enzymatically isolated from the rat hippocampus (for methods see Vreugdenhil and Wadman, 1992). A1 Sodium current evoked by 20 ms depolarization to -40 mV preceded by a 40 ms hyperpolarization to -150 mV. Holding potential is set at -65 mV. The current is fitted with a third order rising exponential and single exponential decay. A2 Same as A1 but now for a depolarization to -25 mV. B Recovery from inactivation measured using a double pulse protocol separated by hyperpolarizations of variable duration and membrane voltage of three different values (-70, -80, and -90 mV). Smooth curves are first order exponential fits to the data points. C Inactivation measured by a standard depolarization to -20 mV, preceded by hyperpolarization to levels between -65 and -150 mV. Smooth curve is the fit to a Boltzmann function (4). D Activation function determined as the peak amplitude of the sodium current evoked by a 20 ms depolarization. Smooth curve is the fit to the Goldman-Hodgkin-Katz current equation (Hille, 2001), using a Boltzmann function to describe the voltage dependence of the permeability (5).
be defined for the activation gate m (which stand for the fraction of m gates in the open state). We used a procedure that directly fitted a complete set of currents observed under experimental conditions (examples in figure 1a and b) in order to estimate the best functions for α and β and found:
41.891.19
1
76.23)( Vm
eV −−
+=α and
30.2657.121
1
36.27)( +
+= Vm
eVβ
and

Chapter 2
20
50.20
66.151
1
856.0)( +
+= Vh
eVα and
71.1208.16
1
917.1)( Vh
eV −−
+=β
Under these conditions the inactivation function is sufficiently fitted by a Boltzmann equation (figure 1c):
c
h
VVV
e
IVI −
+
=
1
)( max (4)
The activation function was fitted with the Goldman-Hodgkin-Katz current equation (Hille, 2001) using a permeability with a Boltzmann type voltage dependence (figure 1d):
V
VNaNa
VcVVh e
e
e
gVVI o
i
α
α
−
−
− −
−×
+×=
+
+
11
)( ][][
max (5)
The sodium current defined by these parameters was implemented in a NEURON simulation model (Hines and Carnevale, 1997), with a single compartment morphology, which resembles the electrotonic shape of the isolated neuron used for the fitting. Applying the standard voltage clamp protocols to the artificial neuron confirmed the correct implementation of the properties of the sodium current. 3. Na-CURRENT INACTIVATION IN EPILEPSY MODELS
The change in excitability that is associated with the process of epileptogenesis is partly resulting from changes in ionic currents. Here we focus on the role of the sodium current properties (for a review see Kohling, 2002). A common observation made in several models of epilepsy is a shift of the inactivation curve in depolarizing direction. In the epilepsy model of classical kindling Vh shifted about 3.1 mV in depolarizing direction (Vreugdenhil et al., 1998). A similar shift (2.5 mV) was found in the SSLSE model of epilepsy (Ketelaars et al., 2001), although in those experiments the variance was larger and the difference did not reach significance (figure 2). The inactivation function is so steep that even a shift of this small magnitude results in a ~25% increase of the number of recruitable sodium channels at resting membrane potential.
4. CBZ MODULATION OF Na-CURRENT INACTIVATION Carbamazepine (CBZ) is one of the drugs of first choice for the treatment of
epileptic patients (Macdonald and Kelly, 1994). Its basic mechanism of action has extensively been studied, in particularly under conditions of voltage clamp in isolated neurons. Extrapolating such results to the effects of the drug under current clamp conditions has proven more difficult than expected and most results are formulated in terms of its effectiveness in the prevention of seizures.
The isolated cell preparation allows to determine which parameters of the sodium current (as defined in figure 1) are modulated by CBZ. CBZ does not affect the activation properties of the sodium current (data not shown, but see Vreugdenhil and Wadman, 1999), but it exerts a highly specific effect on the inactivation of the current (figure 3).

Sodium current properties in different models of epilepsy
21
Figure 2: Inactivation properties of sodium current in rat hippocampal neurons. A. Shift in depolarizing direction in fully kindled animals (adapted from Vreugdenhil et al., 1998). B. A similar shift in neurons isolated from rats in the SSLSE model (adapted from Ketelaars et al., 2001).
The relation between the CBZ concentration and the shift of the inactivation curve
is well described by a Hill relation with a Hill factor of 1 and an EC50 in the range of 40-100 M (figure 3b). In a series of studies Kuo and coworkers (Kuo et al., 1997, Kuo, 1998) have shown that CBZ acts by binding to an extracellular site of the sodium channel. The affinity of binding to the inactivated state is much larger than that to the resting state. This mechanism can be investigated under voltage clamp, and it can be added to the kinetic scheme presented by equations 1-3.
Figure 3: A. Application of carbamazepine shifts the inactivation in hyperpolarizing direction in a dose dependent way. B. The relation between Vh and CBZ can be described by a Hill function, the Hill factor for this cell was 1 and the EC50 for this cell was 94 µM.

Chapter 2
22
The assumption that binding of CBZ predominantly takes place to the inactivated
state of the sodium channel implies the existence of an additional h state (hbound). The distribution of the channels between hclosed and hbound is then determined by a CBZ dependent association constant (CBZ) and a fixed dissociation constant δ: bound
CBZclosed hCBZh hh ⎯⎯⎯ →⎯⎯⎯←+ )(γδ (6)
A protocol was designed in which a depolarizing voltage step of variable duration
allowed CBZ to bind to an increasing fraction of inactivated gates. A standard depolarizing voltage step subsequently applied made it possible to
quantify the bound fraction (figure 5A, voltage protocol given as an inset). The binding rate constant was then obtained from the relation between CBZ and the binding rate. For CBZ in CA1 hippocampal pyramidal cells we obtained a value for (CBZ) of 32 ± 3 mM-1s-1.
Figure 4. Determining the binding rate constant (CBZ) for CBZ to the inactivated state of the sodium channel. A. Slow binding to the inactivated state decreases the current evoked by a test pulse after an inactivating voltage step of variable duration. CBZ concentration for this experiment was 50 µM. The smooth curve is the single exponential fit to the data points with a time constant of 270 ms. The voltage protocol is given as an inset. B. The binding rate constant can be determined from the relation between binding rate and CBZ concentration, using a least square fit.
5. CBZ MODULATION OF NEURONAL FIRING
The addition of a CBZ dependent “bound” state to the model allows illustrating the equilibrium distribution of the h channels over the three states as a function of CBZ (see figure 5 for examples of a low and a high concentration of CBZ). It also confirms the observed shift in Vh of the inactivation function and it allows investigating the changes in time constant of recovery from inactivation that can be anticipated (data not shown). In order to evaluate the possible consequences of CBZ presence on neuronal firing rate we

Sodium current properties in different models of epilepsy
23
implemented the sodium current in a single compartment neuron implemented in the simulation environment NEURON (Hines and Carnevale, 1997). To create realistic firing we had to add at least a voltage dependent potassium current and we implemented the one defined by Hofman and coworkers (Hoffman et al., 1997). Although this oversimplified neuronal model will not demonstrate all the fine variations in firing patterns that are possible (e.g. it will lack properties related to calcium current, calcium accumulation and calcium dependent potassium channels), it will nevertheless demonstrate how CBZ affects basic firing rate of an isolated neuron (for overview see Destexhe and Huguenard, 2000, Destexhe and Huguenard, 2000b).
Figure 5. Distribution of the h gates over the three possible states (open, closed and bound) illustrated for 5 µM (left panel) and 50 µM CBZ (right panel). The Vh of the curve that describes the distribution between hopen and hclosed shifts from -75.2 mV to -83.7 mV when CBZ is increased from 5 to 50 µM.
As is demonstrated in figure 6 the presence of a high concentration of CBZ
(100 µM), considerably above the usual adopted therapeutic dose of 15 µM) blocks all action potentials. At a concentration of 50 µM, CBZ effectively reduces firing rate of the neurons and the difference between figure 6A and B indicates that these properties are use-dependent. 6. CONCLUSIONS
Using a fit procedure that minimizes the collective error of a complete set of current traces describing voltage dependent activation, inactivation, and recovery from inactivation, allowed us to use the classical formalism of Hodgkin and Huxley and model the sodium current with sufficient accuracy to simulate such a set of current traces. Adding one more inactivated state (the one bound to CBZ) also permitted to incorporate

Chapter 2
24
the binding of carbamazepine in a form that catches the essential properties responsible for its anti-epileptic activity.
Figure 6. Firing properties of a hippocampal CA1 neuron investigated in a NEURON simulation model. A. Relation between current injection and firing rate measured over 2000 ms for control and in the presence of 50 and 100 µM CBZ. The latter concentration completely blocked neuronal firing. B. The same relation as illustrated in A, but now firing rate was determined over the first 200 ms. C. sample trace of membrane potential for control and in the presence of 150 µM CBZ.
The changes induced by CBZ are counteracting the changes observed in sodium current inactivation in the classical kindling model of epilepsy (Goddard et al., 1969, Vreugdenhil et al., 1998) and in the SSLSE model (Lothman et al., 1995, Ketelaars et al., 2001, Gorter et al., 2002). Of course the effectiveness of CBZ in preventing seizures cannot be predicted from such a modeling study as many more parameters of currents and neurons might have changed in the epileptic focus. On the other hand it has provided us with a tool that predicts how an AED will affect firing rate under normal conditions. 7. ACKNOWLEDGMENTS
The help of Martin Vreugdenhil, Susan Ketelaars, Kristel Crommentuijn, Jan
Gorter, and Taco Werkman in the experiments is greatly acknowledged. We also thank Hans Kager and Michiel Remme for their help in building and investigating the NEURON model.

CHAPTER 3
A Comparison of Biophysical and Pharmacological Properties of Human Brain Sodium Channel α-subunits NaV1.1, NaV1.2, NaV1.3 and
NaV1.6 Expressed in HEK293 Cells
Guangchun SUN, Taco R. WERKMAN, Jeffrey J. CLARE
and Wytse J. WADMAN
Submitted to Molecular Pharmacology

Chapter 3
26
ABSTRACT The whole cell voltage-clamp technique was used to investigate the biophysical and pharmacological properties of the human Na+ channel NaV1.1, NaV1.2, NaV1.3 and NaV1.6 α-subunits stably expressed in HEK293 cells. Some subtle differences were observed for the properties of voltage-gated Na+ currents carried by the four α-subunits. For instance, the recovery from inactivation of Na+ currents carried by the NaV1.1 and NaV1.6 α-subunits was relatively fast (tau values at –80 mV ~7 and ~ 5 ms, respectively) whereas this was much slower for the NaV1.2 and NaV1.3 currents (~18 ms and ~28 ms, respectively). Furthermore, the anti-epileptic drugs (AEDs) carbamazepine (CBZ), lamotrigine (LTG), and phenytoin (DPH) concentration dependently blocked the Na+ currents in a use- and frequency-dependent manner. Especially the NaV1.1 and NaV1.6 currents were found to be less sensitive to CBZ (EC50 values for shifting the steady-state inactivation curve: NaV1.1, ~345 μM; NaV1.2, ~65 μM; NaV1.3, ~85 μM; NaV1.6, ~195 μM). When comparing the binding kinetics of the three AEDs, we found that CBZ had a much faster binding rate to the α-subunits than LTG and DPH (e.g. for the NaV1.2 subunit: CBZ, 75.1 ± 6.2 mM-1s-1; LTG, 21.0 ± 2.7 mM-1s-1; DPH, 12.9 ± 2.1 M-1s-1). We also observed that all three AEDs displayed slower binding and unbinding rates for the NaV1.3 subunit as compared with the other α-subunits. These findings are discussed in the light of AED efficacy, especially under (epileptic) conditions when expression patterns of voltage-gated Na+ channels are changed. Introduction
Voltage-gated Na+ channels play an important role in cellular excitability. They open upon depolarization of the membrane and their regenerative properties make them responsible for the generation of action potentials. Ultimately they are the key players in the transmission of fast impulses through cell membranes and cellular networks (Catterall, 1984). The brain Na+ channel proteins consist of a pore-forming α-subunit associated with auxiliary β-subunits (Catterall, 2000, Catterall et al., 2005). Expression of the α-subunit alone is sufficient for the formation of functional Na+ channels, but β subunits (so far four types: β1 through β4 have been identified) can modulate the (inactivation) properties of the channel and also have a role in trafficking the channel to the cell membrane (Isom, 2001, Meadows et al., 2002, Goldin, 2003, Ulbricht, 2005). Of the ten different Na+ channel α-subunits known, the NaV1.1, NaV1.2, NaV1.3 and NaV1.6 α-subunits comprise the most prominent brain Na+ channels (Noda et al., 1986a, Kayano et al., 1988, Schaller et al., 1995, Yu and Catterall, 2003). Moreover, various alternatively spliced isoforms of these are known including adult and neonatal isoforms of NaV1.2, NaV1.3 and NaV1.6 which result from developmentally regulated splicing of a single exon (Auld et al., 1988, Sarao et al., 1991, Gustafson et al., 1993, Plummer et al., 1998).
Certain generalizations can be made with respect to the location and function of these four α-subunits (Yu and Catterall, 2003, Trimmer and Rhodes, 2004). NaV1.1 subunits are located on dendrites and cell bodies and are thought to play a role in synaptic signal transfer from dendrite to cell body. NaV1.2 subunits are mainly located in axons and terminals. They contribute to axonal propagation of action potentials. NaV1.3

Pharmacology of α-subunits of human sodium channels
27
subunits are abundant in embryonic and neonatal brain, and also occur in adult brain where they have an expression pattern similar to that of NaV1.1 subunits in the adult brain (Whitaker et al., 2001b, Lindia and Abbadie, 2003, Thimmapaya et al., 2005). Finally, NaV1.6 subunits are expressed at high levels in the nodes of Ranvier of myelinated axons, where they have a function in the characteristic high velocity action potential propagation in these axons.
The most common antiepileptic drugs (AEDs) target voltage-gated Na+ channels in a use- and voltage-dependent manner, a mechanism that selectively dampens pathologic activation of Na+ channels in particularly by preventing high frequency synchronous firing, without interacting with normal Na+ channel function (Macdonald and Kelly, 1995, Clare et al., 2000, Rogawski and Loscher, 2004a, Clare, 2006). Through this action AEDs like carbamazepine (CBZ), phenytoin (DPH) and lamotrigine (LTG) are effective in treating partial and generalized tonic-clonic seizures in humans (Rogawski and Porter, 1990, Ragsdale and Avoli, 1998). The interaction with Na+ channels also underlies therapeutic efficacy of such drugs in the treatment of non-epileptic conditions like neuropathic pain and migraine (Rogawski and Loscher, 2004b). Disturbed function of voltage-gated Na+ channels is implicated in neurological disorders like epilepsy, where in several instances it involves channeloptahies of Na+ channel α- and/or β-subunits (Clare et al., 2000, George, 2005, Meisler and Kearney, 2005, Clare, 2006).
CBZ, LTG, and DPH all have a much higher affinity to the inactivated state than to the resting state of the Na+ channel which implies that they stabilize the inactivated states, effectively blocking the conductance (Ragsdale and Avoli, 1998). The α-helical S6 segments of the III and VI repeats of the α-subunits comprise the site where most AEDs bind to the voltage-gated Na+ channel (Rogawski and Loscher, 2004a). This site is accessible from the extracellular side of the channel via a simple one-to-one binding reaction (Kuo, 1998). AED-Na+ channel interactions have been described in several studies (Ragsdale et al., 1991, Kuo and Bean, 1994b, Xie et al., 1995, Ragsdale et al., 1996, Kuo et al., 1997, Kuo and Lu, 1997, Xie et al., 2001, Liu et al., 2003, Ilyin et al., 2005) but a systematic and detailed comparison of AED effects on the different brain Na+ channel subtypes NaV1.1, NaV1.2, NaV1.3 and NaV1.6 is lacking. In this study we will compare the interaction of the AEDs CBZ, DPH and LTG with the four brain related α-subunits that were stably expressed in HEK293 cell lines. As there is growing evidence that Na+ channel α-subunit expression might undergo modification during or after epileptogensis, understanding of the differences in pharmocological profile of these channel components might be of help in combatting the phenomenon of pharmaco resistance, a condition which affects ~30% of epilepsy patients who do not respond to first-line AEDs (Regesta and Tanganelli, 1999, Remy and Beck, 2006). Materials and Methods
Stably transfected HEK293 cell lines. All experiments were performed in HEK293 cell lines stably expressing the human NaV1.1, NaV1.2, NaV1.3 or NaV1.6 α-subunits that have previously been described (Chen et al., 2000, Burbidge et al., 2002, Mantegazza et al., 2005). The cell lines were generated using the pCIN5 vector (Chen et al., 2000) using the method described by Burbidge et al. (Burbidge et al., 2002).

Chapter 3
28
Cell culture. The HEK293 cell lines stably expressing the human NaV1.1, NaV1.2, NaV1.3 or NaV1.6 sodium channel α-subunits were cultured in minimum essential medium (Gibco), containing 10% fetal calf serum (Gibco), 1% L-glutamine (200 mM, Gibco) and 1% penicillin/streptomycin (Gibco). Cells were grown in a 95/5% O2/CO2 atmosphere at 37oC and with 95% humidity. One to two days prior to electrophysiological recordings, the cells were plated on glass coverslips.
Whole-cell voltage-clamp recordings. Cells grown on glass coverslips were placed into a recording chamber with 0.5 ml extracellular solution which contained (in mM): NaCl 140, KCl 5, CaCl2 2, MgCl2 1, HEPES 10, and glucose 11; pH was adjusted to 7.4. The patch electrodes had resistances of 2-3 MΩ and were filled with pipette solution consisting of (in mM): CsF 140, EGTA 10, HEPES 10, NaCl 5, MgCl2 2; the pH was adjusted to 7.3. Voltage-dependent Na+ currents were measured under whole-cell voltage-clamp conditions at room temperature (20-22oC). After the whole-cell configuration was established, the cell was perfused with extracellular solution for ~13 minutes allowing the current to stabilize, and then moved into either control or drug-containing extracellular solution emitted from the application pipette using the Fast-Step Perfusion system (SF-77B, Warner Instrument Corporation, Hamden, USA). Voltage-step protocols were applied by an Atari (TT030) computer-controlled Axopatch 200A amplifier. The membrane capacitance was read from the amplifier dials and used to indicate membrane surface. Compensation circuitry was used to reduce the series resistance error by at least 75%. The holding membrane potential was set at –70 mV and currents were sampled at a frequency of 5 kHz and analyzed using custom-made software. Each protocol (lasting 2-2.5 min) was performed at least twice in each (control or drug-containing) extracellular solution. The control extracellular solution was applied before and after drug-containing solution to control the stability of the voltage dependence properties in particularly when estimating drug effects. Preferably, more than one concentration per cell was tested (with a maximum of four concentrations per cell). HEK cells are electrotonically compact and rarely escape voltage-clamp. Only cells that showed little current rundown over the recording time, were incorporated in the analysis. The currents were corrected off-line for linear non-specific leak and residual capacitive current.
Drugs and reagents. CBZ, DPH (Sigma) and LTG (Glaxo Wellcome) were dissolved in dimethylsulfoxide (DMSO, Sigma) to make stock solutions of respectively 400 mM, 100 mM and 333 mM. They were then diluted in extracellular solution to reach their final concentrations; DMSO concentrations in CBZ, DPH and LTG containing solutions were respectively 0.05%, 0.2% and 0.3%, for which concentration no effect on Na+ currents could be demonstrated.
Data analysis. Data are given as the mean ± standard error of the mean (S.E.M). Multiple groups were compared using an (one or two factor) ANOVA followed by a post-hoc Fisher test. Unless otherwise stated, Student’s t-test was used for the direct comparison of two groups of parameters. P < 0.05 was considered to indicate a significant difference.

Pharmacology of α-subunits of human sodium channels
29
Results
Biophysical analysis of Na+ currents carried by the NaV1.1, NaV1.2, NaV1.3 and NaV1.6 α-subunits expressed in HEK293 cells. Whole-cell voltage clamp recordings were made of voltage-activated Na+ currents in HEK293 cells expressing the NaV1.1, NaV1.2, NaV1.3 or NaV1.6 α-subunits. Na+ currents were activated by 25-ms depolarization steps to levels between –70 mV and +10 mV from a pre-pulse potential of –120 mV (inset of Fig. 1Aa). The depolarization activated a fast, transient inward Na+ current that increased in amplitude as the channels open with steps to higher potentials and then decreased at even higher potentials due to the reduced driving force (Fig. 1 Aa). We determined the peak amplitude of the current for each step and constructed current-voltage relationships for the four α-subunits which were fitted to the Goldman-Hodgkin-Katz current equation (Hille, 2001) using a Boltzmann function to describe the sodium permeability as a function of membrane voltage (V):
( ) )exp(1)exp(][][
exp1 F P)( 0
VVNaNaVVI outin
VVV
c
h ααα
−−
×+
××=
++
− Eq 1
With α = F/RT where P0 is the maximal permeability of the channel, F is the Faraday constant, R the gas constant and T represents the absolute temperature. The voltage dependence of the conductance is described with a Boltzmann term characterized by the potential of half-maximal activation (Vh) and a slope parameter (Vc). For practical measurements we prefer to substitute gmax = P0 αF [Na+]out where gmax is the maximal membrane conductance. The I-V curves in Fig. 1Ab are fits to the mean data points, but these fits were also performed on the data points measured in the individual cells and the resulting average Vh, Vc and Gmax values for the different subunits can be found in Table 1. In general the Vh and Vc values of the four subunits are in the same range, although the difference of the Vh values for activation and inactivation (ΔVh) of NaV1.1 is smaller than that of the other three subunits (Student’s t-test, p<0.01; Table 1), which will result in a window current that is present over a wider voltage range (see Fig. 2). The different Gmax values are most likely the result of differences in channel densities due to differences in expression efficacies in the four cell lines.
The voltage dependence of steady-state inactivation of the Na+ current was measured by varying a 500-ms hyperpolarizing pre-pulse from –150 to –35 mV followed by a 25-ms depolarization to –10 mV (inset of Fig. 1Ba). The peak amplitude of the current (I) evoked at –10 mV was normalized to Imax and plotted as a function of pre-pulse potential (V). The data points of Fig. 1Bb were fitted with a Boltzmann equation of the form:
⎟⎟⎠
⎞⎜⎜⎝
⎛ −+
=
c
h
VVV
IVI
exp1)( max Eq. 2
where Vh is the potential of half-maximal inactivation and Vc is proportional to the slope of the curve. The data points measured in the individual cells were also fitted with equation 2 and the mean Vh and Vc values can be found in Table 1.
Over the voltage range where the activation and inactivation functions overlap a so-called window current can be present, where the activated current is not completely inactivated (Patlak, 1991, Johnston, 1995). The window currents of the four subunits (for

Chapter 3
30
each cell) were constructed by determining the product of the activation and inactivation functions (Fig. 2), using the Vh and Vc parameters for activation and inactivation. In Fig. 2A as example the activation and inactivation curves of subunit NaV1.1 are shown. The inactivation curve (i.e. the available fraction) is the same as in Fig. 1B and the
0
0.2
0.4
0.6
0.8
1
-120 -100 -80 -60 -40
NaV1.1
NaV1.2
NaV1.3
NaV1.6
Avai
labl
e Fr
actio
n
Voltage (mV)
-7
-6
-5
-4
-3
-2
-1
0
NaV1.1
NaV1.2
NaV1.3
NaV1.6
-80 -60 -40 -20 0 20
Am
plitu
de (n
A)
Voltage (mV)
3 nA
5 ms
3 nA
5 ms
-35 mV
-70 mV
-150 mV500 ms
-10 mV25 ms
A
B
-70 mV
10 mV
500 ms
25 ms
-120 mV
a b
a b
Figure 1. Voltage-dependent activation and steady-state inactivation of Na+ currents carried by human Na+ channel α-subtypes (Nav1.1, Nav1.2, Nav1.3 and Nav1.6) expressed in HEK293 cells. A, Voltage-dependence of activation. (a), Example traces of voltage-activated NaV1.3 Na+ currents. Na+ currents were activated by 25-ms depolarizing voltage steps ranging from –70 mV to +10 mV, following a 500-ms hyperpolarizing pre-pulse to –120 mV (protocol given as inset). (b), The mean peak amplitudes of the Na+ currents carried by the four α-subunits are plotted as a function of membrane potential and fitted with the Goldman-Hodgkin-Katz current equation (Eq. 1). These fits to the averaged data points resulted in the following values for Vh and Vc, respectively: NaV1.1, –30.5 ± 0.4 mV and –5.3 ± 0.3 mV (n=8); NaV1.2, –28.6 ± 0.3 mV and –5.4 ± 0.3 (n=36); NaV1.3, –27.0 ± 0.5 mV and –5.3 ± 0.3 mV (n=30); NaV1.6, –26.6 ± 0.3 mV and –5.4 ± 0.3 mV (n=10). B, Voltage-dependence of steady-state

Pharmacology of α-subunits of human sodium channels
31
inactivation. (a), Example traces of voltage-inactivated NaV1.3 Na+ currents. Na+ currents were evoked with a step depolarization to –10 mV for 25-ms following a 500-ms hyperpolarizing pre-pulse between –150 mV and –35 mV (protocol given as inset). The fraction available current was defined as the normalized peak current (relative to the current amplitude evoked with an inactivating pre-pulse at –150 mV), plotted as a function of membrane potential and fitted with a Boltzmann function (Eq. 2) (b). These fits to the averaged data points resulted in the following values for Vh and Vc, respectively: NaV1.1, –63.4 ± 0.5 and –6.7 ± 0.4 (n=8); NaV1.2, –69.5 ± 0.6 mV and –9.0 ± 0.5 mV (n=36); NaV1.3, –68.1 ± 0.5 mV and –8.2 ± 0.4 mV (n=30); NaV1.6, –66.6 ± 0.5 mV and –7.5 ± 0.4 mV (n=10). Error bars indicate S.E.M.
activation curve is the fitted Boltzmann term from equation 1, which reflects the open fraction of Na+ channels immediately after depolarization to the specific voltage. The resulting mean window currents (Fig. 2B) indicate that the α-subunit NaV1.1 is capable of generating a window current that is present over a relatively wide voltage range as compared to the other three subunits. This is also reflected by the smaller ΔVh value found for the NaV1.1 current (Table 1). Table 1. Activation and steady-state inactivation properties of Na+ currents carried by NaV1.1, NaV1.2, NaV1.3 and NaV1.6 α-subunits expressed in HEK293 cells Activation Inactivation
Subtype
Vh (mV) Vc (mV) Gmax(nS)
Vh (mV) Vc (mV)
ΔVh (mV)
NaV1.1 –29.9±1.7 (8)
–4.7±0.3 (8)
181.5± 21.4 (8)
–63.2±1.6 (8)
–5.9±0.6 (8)
33.2±1.5
(8)
NaV1.2 –28.9±0.9 (36)
–4.7±0.1 (36)
185.7 ± 15.2 (36)
–68.6±1.4 (36)
–6.6±0.2 (36)
40.4±1.1**
(36)
NaV1.3 –27.4±0.9 (30)
–4.4±0.4 (30)
231.5±20.1 (30)
–67.4±1.0 (30)
–6.9±0.2 (30)
39.7±0.9**
(30)
NaV1.6 –25.5±1.1 (10)
–5.4±0.2 (10)
101.8±14.6 (10)
–65.9±1.0 (10)
–6.7±0.2 (10)
40.0±1.0**
(10)
Cell numbers are given in brackets. **p<0.01, compared with NaV1.1 (Student’s t-test)

Chapter 3
32
0.0
0.2
0.4
0.6
0.8
1.0
0.0
0.2
0.4
0.6
0.8
1.0
-120 -100 -80 -60 -40 -20 0
activationinactivationAv
aila
ble
fract
ion
Voltage (mV)
Open fraction
NaV1.1
-0.02
-0.015
-0.01
-0.005
0
NaV1.1
NaV1.2
NaV1.3
NaV1.6
-100 -80 -60 -40 -20 0 20
Am
plitu
de (n
A)
Voltage (mV)A B
Figure 2. Construction of the window current carried by the NaV1.1, NaV1.2, NaV1.3 and NaV1.6 α-subunits. A, Activation and steady-state inactivation curves of the NaV1.1 current. The activation curve is given by the Boltzmann term of equation 1, the inactivation curve is the same as in Fig. 1Bb. B, The absolute window current carried by the four α-subunits was constructed as the product of the inactivation and activation function (see A). Compared with the other three α-subunits the window current carried by the NaV1.1 α-subunits is active over a wider voltage range.
Next the time course of the recovery from inactivation of the Na+ current was
determined using a double-pulse protocol (inset of Fig. 3A). The interval ∆t (during which the current was allowed to recover) between two 25-ms depolarization steps (to–10 mV) was varied between 1 and 200 ms. The recovery time constant was determined at membrane voltages of –80, –90 and –100 mV. The amplitude of the Na+ current activated by the second pulse is plotted as a function of ∆t and fitted with a single-exponential function (Fig. 3Ad) of the form:
⎟⎠⎞
⎜⎝⎛ Δ−−=Δ
τttR exp1)( Eq. 3
where τ is the time constant. The average τ values estimated for the four α-subunits are presented in Fig. 3B where it can be seen that the recovery from inactivation is voltage- and subunit-dependent (two-factor ANOVA, p<0.001). The recovery from inactivation is relatively slow for the NaV1.3 subunit current and to a lesser extent for the current of the NaV1.2 subunit. Na+ currents carried by the NaV1.1 and NaV1.6 subunits display a relatively fast recovery from inactivation process. Pharmacological analysis of the human NaV1.1, NaV1.2, NaV1.3 and NaV1.6 α-subunits expressed in HEK293 cells. Frequency-dependent inhibition by anti-epileptic drugs. Several AEDs are capable of blocking voltage-activated Na+ currents in a frequency and use-dependent manner (Macdonald and Kelly, 1995). The degree of block of voltage-activated Na+ currents that is generated when a Na+ channel is exposed to an AED while depolarizing the cell with different frequencies is an important determinant of channel and AED pharmacology. We illustrated this by investigating the frequency-dependent block of the Na+ current carried by the four α-subunits evoked with two AEDs known to affect Na+ channels, namely CBZ and LTG. CBZ was tested on all

Pharmacology of α-subunits of human sodium channels
33
Δt = 100 ms
30 ms1 nA
Δt = 20 ms
Δt = 2 ms
-80 mV
-10 mV25 ms 25 ms
Δt = 1~200ms
-90 mV-100 mV
0
5
10
15
20
25
30
35
-80 -90 -100
NaV1.1
NaV1.2
NaV1.3
NaV1.6
Tim
ce c
onst
ant (
ms)
Voltage (mV)
****
**
**
******
**
*
*
^^
^^
^^^^
**
-6
-5
-4
-3
-2
-1
00 50 100 150 200
Am
plitu
de (n
A)
Interval (ms)
V = -80 mV
a
b
c
d
A
B
Figure. 3. Voltage dependence of recovery from inactivation of Na+ currents carried by NaV1.1, NaV1.2, NaV1.3 and NaV1.6 α-subunits expressed in HEK293 cells. A, The time course of recovery from inactivation was determined by a double-pulse protocol (given as inset). The variable pulse interval (∆t = 1, 2, 5, 10, 20, 50, 100 or 200 ms, during which the current was allowed to recover) between two 25-ms depolarizing voltage steps to –25 mV was used to determine the recovery from inactivation at the membrane voltages –80 mV, –90 mV, and –100 mV. Example traces of NaV1.3 currents activated by double pulses with different pulse intervals are shown in (a) (∆t = 100 ms), (b) (∆t = 20 ms) and (c) (∆t = 2 ms). With longer inter-pulse duration more channels recover from inactivation. (d), The amplitude of the Na+ current (recorded from a cell expressing the NaV1.3 α-subunit) activated by the second pulse was plotted as a function of ∆t and fitted

Chapter 3
34
with a single-exponential function to give the time constant of recovery from inactivation (Tau, at membrane potential –80 mV). B, Tau values of NaV1.1 (n = 5-6), NaV1.2 (n = 23-26), NaV1.3 (n = 30-33) and NaV1.6 (n = 7-9) currents at the three membrane voltages. The recovery form inactivation was voltage- and subunit-dependent (two-factor ANOVA, p<0.001) and was faster for NaV1.1 and NaV1.6 currents compared with NaV1.2 and NaV1.3 currents. Error bars indicate S.E.M. * and ** indicate p<0.05 and p<0.01, respectively, for comparison between different α-subunits at the same membrane potential and ^^ indicates p<0.01 for comparison of the same α-subunits at different membrane voltages (both Fisher’s post hoc test).
four subunits, whereas LTG was applied only to cells expressing the NaV1.2 or NaV1.3 subunit. The time constant of inhibition was determined by delivering twenty 3-ms depolarizing pulses to –10 mV with pulse intervals of 100 or 20 ms (when the potential was stepped back to –80 mV; inset of Fig. 4A), effectively evoking the Na+ currents with 10 HZ or 50 Hz stimulation trains, respectively. So this frequency reflects the interpulse interval when the potential is stepped back to –80 mV and not the actual pulse frequency (which is ~8 HZ and ~44 Hz, respectively). The blocked current was determined by subtracting the current in the presence of the AED from the control current (thus correcting for the reduction in current amplitude due to inactivation) and plotted as function of time (Fig. 4A). The development of block during time was determined by fitting the blocked current amplitude with a mono-exponential equation (Eq. 3) to give the time constant of this process (Fig. 4Ad). The trains of depolarizing pulses cause the Na+ channels to accumulate in the inactivated state (resulting in more inactivated channels with high frequency stimulations), allowing the AEDs to more effectively block the channels. This was reflected by the observation that with 50 Hz stimulation AED block developed more quickly than with 10 Hz (multi-factor ANOVA P<0.001) (Fig. 4B and D). It is also clear that this development of block occurred faster with higher AED concentrations (multi-factor ANOVA, P<0.001). Furthermore, for the NaV1.2 and NaV1.3 subunits it was observed that CBZ block developed faster than LTG block (Fig. 4B and D; note different Y-axis scales). It also appeared that the frequency sensitivity of LTG block of the NaV1.2 subtype is larger than that of the NaV1.3 α-subunit (Fig. 4E). For example, with 30 µM LTG the development of block of the Na+ current carried by the NaV1.2 subunit was ~7 times faster when the current was evoked with the 50 Hz stimulus train (compared with 10 Hz), whereas for the NaV1.3 subunit this was only ~2 times faster (Fig. 4E). This suggests that with 10 Hz stimulation not enough NaV1.2 channels are long enough in the inactivated state to allow sufficient LTG binding, whereas this binding is considerably increased with the 50 Hz stimulation protocol, due to a larger fraction of inactivated channels. With the 300-μM LTG concentration this difference between NaV1.2 and NaV1.3 was much smaller (~2 vs. ~1.5), indicating that with this (much) higher concentration relatively more NaV1.2 channels get blocked, also with the 10 Hz stimulation protocol. For CBZ it was observed that for all four subunits the frequency sensitivity was not much different (the blocking rate was ~2 times faster with 50 Hz as compared with 10 Hz) for both concentrations (Fig. 4C). This suggests that CBZ is capable of rapidly binding to the inactivated state and that the selected stimulation frequencies are not a rate-limiting factor.

Pharmacology of α-subunits of human sodium channels
35
Figure 4. Frequency-dependent block by CBZ and LTG of Na+ currents carried by NaV1.1, NaV1.2, NaV1.3 and NaV1.6 α-subunits expressed in HEK293 cells. A, Examples of pulse-activated Na+ current traces (evoked with 20 3-ms voltage steps to –10 mV; pulse interval at –80 mV was 20 ms) recorded from a cell expressing the NaV1.1 α-subunit before (a), during (b) and after CBZ (50 μM) (c) application. Protocol is given as inset (pulse interval at –80 mV was 20 ms (“50 Hz”) or 100 ms (“10 Hz”); the protocol was repeated every 5 s). (d) The CBZ-blocked Na+ current amplitudes (i.e. difference of control and CBZ current amplitude) were plotted against the stimulation time and fitted with a mono-exponential equation to yield the time constant describing the rate at which CBZ develops (164 ms in this particular example). B, Time constants describing the development of CBZ (50 and 200 μM) block of Na+ currents evoked with the 10 or 50 Hz stimulation protocol for all four α-subunits (n=5-10). C, Frequency
Control
100 ms
2 nA
50 μM CBZ Wash
-120 mV
-80 mV -80 mV
-10 mV3 ms
x 19
t = 20, 100 ms
t0
0.5
1
1.5
2
0 100 200 300 400 500
Bloc
ked
Cur
rent
(nA)
Time (ms)
τ = 164 ms
50 μM CBZ, 50 Hz
0
100
200
300
400
10 Hz 50 Hz 10 Hz 50 Hz
NaV1.1
NaV1.2
NaV1.3
NaV1.6
Tim
e co
nsta
nt (m
s)
50 μM [CBZ] 200 μM
ac
ac
ac
ac
ac
bc
bc
bc
****
***
***
ac
ac
ac
bc
0
2
4
6
8
50 μM 200 μM
NaV1.1
NaV1.2
NaV1.3
NaV1.6
tau 10
/ ta
u 50
[CBZ]
Aa b c
B C
D
0
200
400
600
800
1000
1200
1400
10 Hz 50 Hz 10 Hz 50 Hz
NaV1.2
NaV1.3
Tim
e co
nsta
nt (m
s)
30μM [LTG] 300μM
ac
ac
a
ac
b
cb
**
0
2
4
6
8Na
V1.2
NaV1.3
tau 10
/tau 50
[LTG]30μM 300μM
****
**
E
d

Chapter 3
36
sensitivity of CBZ block (ratio of tau10 and tau50 values from B) for 50 and 200 μM CBZ for the four α-subunits (n=5-10). D, Time constants describing the development of LTG (30 and 300 μM) block of Na+ currents evoked with the 10 or 50 Hz stimulation protocol for the NaV1.2 and NaV1.3 α-subunits (n=6-7). E, Frequency sensitivity of LTG block (ratio of tau10 and tau50 values from D) for 30 and 300 μM LTG for the NaV1.2 and NaV1.3 α-subunits (n=6-7). Both drugs showed a frequency and concentration-dependent block (multi-factor ANOVA, p<0.001). Error bars indicate S.E.M. In B and D * and ** indicate p<0.05 and p<0.01, respectively, for comparison of different α-subunits. “a” and “b” indicate p<0.01 and p<0.05, respectively, for comparison of the same α-subunit at different stimulation frequencies but at the same concentration; “c” indicates p<0.01 for comparison of the same α-subunit at different concentrations but at the same stimulation frequency; in E ** indicates p<0.01 (all Fisher’s post-hoc test).
These findings show that AEDs can block the Na+ currents in a use-dependent
manner and that subtle differences exist between the interactions of these drugs with the four subunits. We further investigated the mechanisms underlying the interactions of several AEDs with the four subunits in the following sections.
AED effects on the inactivation properties of Na+ currents carried by the NaV1.1, NaV1.2, NaV1.3 and NaV1.6 α-subunits. As shown above, AEDs like CBZ and LTG have a relatively high affinity for inactivated Na+ channels. This is illustrated by the observation that Na+ currents evoked after keeping the membrane potential at a relatively less hyperpolarizing potential of –80 mV are effectively blocked by 300 μM LTG, whereas this block is much less when channel activation occurred after a pre-pulse of –130 mV (Fig. 5Aa). To determine the effects of AEDs on this steady-state inactivation, the protocol described in Fig. 1B was used. In addition to CBZ and LTG we also tested phenytoin (DPH), another AED also known to interact with voltage-gated Na+ channels. LTG and DPH were both tested on the NaV1.2 and NaV1.3 subunits, whereas CBZ was tested on all four subunits. Fig. 5Ab shows that the normalized inactivation curve of Na+ currents carried by the NaV1.2 subunit was shifted to more hyperpolarized direction with increasing concentrations of LTG (10-1000 μM). The absolute shift of the curve midpoints (∆Vh) in Fig. 5Ac was determined in each cell by the difference of Vh in the absence and presence of LTG and plotted as function of the LTG concentration (see Material and Methods). The data points were fitted with a logistic function of the form:
( )
[ ]AEDEC
VAEDV h
h50
max
1+
Δ=Δ − Eq. 4
where ∆Vh-max is the maximal shift of ∆Vh, EC50 is the concentration which causes half-maximal ∆Vh and [AED] is the applied concentration of AED. For LTG this yielded the following values for the NaV1.2 subunit: ∆Vh-max = 25 ± 2 mV and EC50 = 192 ± 33 μM (n=12-14) (Figs. 5Ac and 5B). In this manner LTG effects were tested on the NaV1.2 and NaV1.3 subunits and compared with the effects of CBZ and DPH. It was noticed that LTG induced a relatively large and statistically significant (maximal) shift of Vh (25 mV for NaV1.2 and 30 mV for NaV1.3) compared to CBZ and DPH (p<0.01), which both induced a maximal shift of ~15 mV when tested on these two subunits (Fig. 5BC). In

Pharmacology of α-subunits of human sodium channels
37
addition, EC50 values for CBZ and DPH were for the NaV1.2 and NaV1.3 subunits in the same range (50-90 μM), whereas that of LTG was for both subunits ~200 μM (differences for CBZ and DPH vs. LTG p<0.01 for NaV1.2, p<0.05 for NaV1.3). When determining the effects of CBZ on the four subunits, we observed that the NaV1.1 subunit in particular displayed a relatively low affinity (EC50≈350 μM) compared to NaV1.2 and NaV1.3 (p<0.05), whereas that of the NaV1.6 subunit (EC50≈200) was somewhat in between (also compared to the NaV1.2 and NaV1.3 subunits (p<0.05; Fig. 5D).
Control
1 nA
2 ms
-130 mV
-80 mV
C
0
5
10
15
20
25
10 100 1000
CBZLTGDPH
Δ V hi
(mV)
[AED] (μM)
ΔVh max
(mV)EC50(μM)AED
13±2c67±19aCBZ
25±2c,d192±33a,bLTG
14±1d50±12bDPH
NaV1.2
A
B
0
5
10
15
20
25
10 100 1000
CBZLTGDPH
Δ V hi
(mV)
[AED] (μM)
ΔVh max
(mV)EC50(μM)AED
15±1c86±16aCBZ
30±2c,d215±50a,bLTG
15±1d52±13bDPH
NaV1.3
0
0.2
0.4
0.6
0.8
1
-140 -120 -100 -80 -60 -40
NaV1.2
0 μM10 μM30 μM100 μM300 μM1000 μM
Ava
ilabl
e Fr
actio
n
Voltage (mV)
[LTG]:
0
2
4
6
8
10
12
14
10 100
NaV1.1
NaV1.2
NaV1.3
NaV1.6
Δ V hi
(mV)
[CBZ] (μM)
ΔVh max
(mV)EC50(μM)type
17±4346±129a,bNaV1.1
13±267±19a,dNaV1.2
15±186±16b,cNaV1.3
17±3196±54c,dNaV1.6
CBZ
0
5
10
15
20
25
200 400 600 800 1000
Δ V hi
(mV)
[LTG] (μM)
NaV1.2
( )( )hill
50
maxhihi
]Drug/[EC1
VDrugV
+
Δ=Δ
D
b ca300 μM LTG
-130 mV
-80 mV
Wash
-130 mV
-80 mV
-80 mV
-70 mV
-130 mV500 ms
-10 mV25 ms
Figure 5. Voltage shift of steady-state inactivation by AEDs of Na+ currents carried by the α-subunits NaV1.1, NaV1.2, NaV1.3 and NaV1.6 expressed in HEK293 cells. A, Examples of Na+ currents evoked at the testing potential of –10 mV following a 500-ms hyperpolarizing pre-pulse at –130 mV or –80 mV in a cell expressing the NaV1.2 α-subunit shown in (a) (control, 300 μM LTG and wash; inset shows the voltage protocol). LTG blocked the Na+ current when it was evoked from the pre-potential of –80 mV. (b), The normalized steady-state inactivation curve of the NaV1.2 current was shifted to hyperpolarized potential with increasing concentrations of LTG. Currents were evoked with the voltage protocol described in Fig. 1B. The data points (n=12-14) were fitted with a Boltzmann function (Eq. 2), resulting in Vh values (in mV) of –69.0, –74.9, –79.2, –86.9, –93.8, –108.0 and Vc values (in mV) of –8.8, –9.0, –9.7, –9.4, –8.2, –10.3 for control and 10, 30, 100, 300 and 1000 μM LTG, respectively. (c), The shift of Vh (∆Vh) was determined in each cell by the difference of Vh in the absence and presence of LTG and plotted against the concentration of LTG. The data points were

Chapter 3
38
fitted with a logistic function (see inset; eq. 3). B, The ∆Vh induced by CBZ (10, 20, 50, 100 and 200 μM), LTG (10, 30, 100, 300 and 1000 μM) and DPH (10, 20, 50, 100 and 200 μM) on NaV1.2 currents (n=5-14). The EC50 and ΔVh values obtained by fitting the data point to a logistic equation (eq. 3) are given in the table inset. Values with similar letter superscripts designate a statistical significance (EC50: a and b indicate p<0.01, ΔVh: c and d indicate p<0.01, Students t-test). C, The ∆Vh induced by CBZ, LTG and DPH on NaV1.3 currents (n=8-16). Values with similar letter superscripts designate a statistical significance (EC50: a and b indicate p<0.05, ΔVh: c and d indicate p<0.01, Students t-test). D, The shift of ∆Vh induced by CBZ on all four Na+ channel subtypes (n=8-16). Values with similar letter superscripts designate a statistical significance (EC50: a, b, c and d indicate p<0.05, ΔVh: c and f indicate p<0.05, Students t-test). Error bars indicate S.E.M.
By having a relatively high affinity for the inactivated state of the voltage-
activated Na+ channels (see above) AEDs like CBZ, LTG and DPH are capable of slowing the recovery from inactivation process. This is illustrated in Fig. 6, where the effect of CBZ on the recovery of inactivation of Na+ currents carried by the four α-subunits was tested in a set of experiments with a double-pulse protocol (inset of Fig. 3A). It was observed that CBZ concentration dependently slowed the recovery of inactivation process of Na+ currents carried by the four subunits, at both recovery potentials of –80 mV and –90 mV (multi factor ANOVA, p<0.01; Fig. 6). Although the control time constants for recovery from inactivation are much smaller for the NaV1.1 and NaV1.6 currents (see Fig. 3), also here CBZ was able to evoke a concentration dependent slowing of the recovery process. Similarly, LTG and DPH slowed the recovery from inactivation of NaV1.2 and NaV1.3 currents in a concentration dependent manner (data not shown).
Figure 6. Concentration-dependent effect of CBZ on the recovery from inactivation of the Na+ current carried by NaV1.1, NaV1.2, NaV1.3 and NaV1.6 α-subunits expressed in HEK293 cells. A, Time constants describing the recovery of the inactivation process at the recovery potential of –80 mV (see Fig. 3) in the absence and presence of CBZ (10, 50 and 100 μM). B, Time constants describing the recovery of the inactivation process at the recovery potential of –90 mV (note different Y-axis scales in A and B). Error bars indicate S.E.M. At both potentials CBZ evoked a concentration dependent slowing of the recovery from inactivation for all four α-subunits (two-factor ANOVA, p<0.01; n=4-12).
0
20
40
60
80
100
0 10 50 100
NaV1.1
NaV1.2
NaV1.3
NaV1.6
Tim
e co
nsta
nt (m
s)
[CBZ] (μM)
V = -80 mV
0
10
20
30
40
50
0 10 50 100
NaV1.1
NaV1.2
NaV1.3
NaV1.6
Tim
e co
nsta
nt (m
s)
[CBZ] (μM)
V = -90 mV
BA

Pharmacology of α-subunits of human sodium channels
39
Binding rates of AEDs to inactivated NaV1.1, NaV1.2, NaV1.3 and NaV1.6
α-subunits. Differences in AED efficacy in treating the various forms of epilepsy can possibly be explained by differences in binding rates onto the Na+ channels. Experiments were performed to determine the binding rates at which AEDs bind to the inactivated Na+ channel subtypes by using a voltage protocol described in Fig. 7 (Kuo and Lu, 1997). With such a protocol the channels were exposed to a depolarizing voltage step (to –40 mV) of different durations (30 – 2500 ms) (inset Fig. 7A). Longer depolarizing voltage steps allow more channels to enter the inactivated state and due to the much higher affinity of AEDs for this state more channels will be blocked (Fig. 7A). A 5-ms repolarization step to –120 mV (following the prepulse) was applied to allow the fraction of channels not blocked by the AED to recover from inactivation. In these experiments the current amplitude in the presence of AED was subtracted from control current amplitude, yielding the amplitude of the blocked current. This procedure also corrected for a reduction in current amplitude due to a slow inactivation process (Fig. 7Aa). The blocked current amplitude was expressed as function of the prepulse duration and fitted with a mono-exponential function (eq. 3) (Fig. 7B). For each tested concentration this yielded a time constant describing the time course during which channel block developed. By taking the reciprocal of this time constant the binding rate at each concentration was determined. The binding rates were plotted as function of AED concentration and the slope of the fitted linear relationship equals the so-called binding rate constant (Fig. 7C). The binding rate constants of CBZ, LTG and DPH were determined for the NaV1.2 and NaV1.3 subunits and it appeared that the CBZ binding rate constant was approximately three times faster than that of LTG and DPH (p<0.01) (Fig. 7D). In addition, LTG binding to these channels was faster than that of DPH (p<0.05 for NaV1.2 and p<0.01 for NaV1.3). Furthermore, all three AEDs displayed a smaller binding rate constant when interacting with the NaV1.3 channel subtype compared with the NaV1.2 subtype (Fig. 7D).
Unbinding rates of AEDs from the NaV1.1, NaV1.2, NaV1.3 and NaV1.6
α-subunits. Another important determinant of AED efficacy is the rate at which the drug dissociates from its binding site. The unbinding rates of CBZ (tested for all four subunits) and LTG (NaV1.2 and NaV1.3 subunits) were determined with the voltage protocol shown in the inset of Fig. 8A. The cells were exposed to a depolarizing voltage step (to –40 mV) for 2000 ms permitting a steady-state block in the presence of AED to develop (see Fig. 7). Subsequently the cell was repolarized to –120 mV for various intervals (5-500 ms) during which the drug can unbind from the channel, followed by a test voltage step to –10 mV to determine the fraction of available channels. The currents in the presence of the drug were subtracted from the control currents (so in the absence of the drug), thus yielding the blocked current amplitude. The AED-blocked current was plotted as function of the recovery interval and fitted with a mono-exponential function (eq. 3), yielding the time constant describing the unblocking process, which appeared to be independent of the AED concentration (Fig. 8Ac). Therefore for each cell the time constants determined with both concentrations (50 and 200 μM for CBZ and 30 and 300 μM for LTG) were used to determine the mean time constant per cell. The reciprocal of this time constant represents the rate at which the drug dissociates from the channel (at –120 mV) and was determined for CBZ (for all four subunits) and LTG (for the NaV1.2 and NaV1.3 subunits)

Chapter 3
40
(Fig. 8B). When comparing CBZ and LTG, we observed for the NaV1.2 and NaV1.3 subunits that the CBZ off rate is much faster than that of LTG (p<0.01). Furthermore, when comparing the CBZ off rates for the four different subunits we found that this was the slowest for the NaV1.3 subunit (p<0.01).
Figure 7. AED binding onto the inactivated state of human Na+ channel subtypes (NaV1.1, NaV1.2, NaV1.3 and NaV1.6) expressed in HEK293 cells. A, Examples of NaV1.3 Na+ currents evoked with the test potential step to –10 mV following a 30-, 250-, and 2500-ms pre-pulse to –40 mV (see inset) in the absence (a) and presence (b) of 50 μM DPH. Pre-pulse durations (Δt) were 30, 62.5, 125, 250, 500, 1000, 1500 and 2500 ms. Before the test potential step to –10 mV the voltage was stepped back for 5 ms to –120 mV to allow the drug-free channels to recover from inactivation. The whole protocol given as inset was repeated every 5 s. B, The blocked Na+ current amplitude was determined by subtracting the control current (measured in the absence of DPH) from the current recorded in the
0
0.5
1
1.5
2
2.5
3
0 50 100 150 200 250
Bin
ding
rate
(s-1
)
[DPH] (μM)
7300 M-1s-1
0
1
2
3
4
5
0 0.5 1 1.5 2 2.5 3
10 μM20 μM50 μM100 μM200 μM
Blo
cked
cur
rent
(nA
)
Prepulse duration (s)
[DPH]:
Control
2500 ms
30 ms
250 ms
3 ms
2 nA
A
B
-120 mV
-40 mV
-10 mV
5 ms
25 ms
Δt = 30- 2500 ms
2500 ms
30 ms
250 ms
50 μM DPH
3 ms
2 nA
C
0
20
40
60
80
100
1.1 1.2 1.3 1.6
CBZLTGDPH
Na channel subtype
Bind
ing
rate
con
stan
t
(x10
3 M-1
s-1)
*
****
****
**
***
*D
a b

Pharmacology of α-subunits of human sodium channels
41
presence of DPH and was plotted against Δt. The data points were fitted with a mono-exponential function to determine the time constant (Tau) for development of block in the presence of 10, 20, 50, 100 and 200 μM DPH. C, The binding rates (1/Tau, s-1) in NaV1.3 cells are plotted against the DPH concentration. The slope of the linear regression gives the binding rate constant of 7300 M-1s-1 to Nav1.3 for DPH (n = 8). D, Comparison of the binding rate constants of CBZ, DPH and LTG for the α-subunits NaV1.1, NaV1.2, NaV1.3 and NaV1.6; these values were determined with the procedure described in A-C. The binding of CBZ to NaV1.3 (45.5 ± 5.9 mM-1s-1, n=5) is slower than to the other three α-subunits (NaV1.1: 62.3 ± 6.8 mM-1s-1, n=8; NaV1.2: 75.1 ± 6.2 mM-1s-1, n=5; NaV1.6: 62.1 ± 10.1 mM-1s-1, n=5). Also LTG (12.3 ± 0.8 mM-1s-1, n=5) and DPH (7.3 ± 1.4 mM-1s-1, n=8) binding to NaV1.3 are slower than that to NaV1.2 (21.0 ± 2.7 mM-1s-1 (n=6) and 12.9 ± 2.1 M-1s-1 (n=6), respectively). Furthermore, CBZ binding to NaV1.2 and NaV1.3 is faster than that of LTG and LTG binding to NaV1.2 and NaV1.3 is faster than that of DPH. Error bars indicate S.E.M. * indicates p<0.05 and ** indicates p<0.01. For comparison of the different AED binding rates to the NaV1.2 and NaV1.3 α-subunits the statistical analysis (multi-factor ANOVA with Fisher’s post-hoc test) was performed on the log-transformed data (due to non-homogeneity of variance).
Figure 8. Unbinding rates of AEDs from the inactivated human Na+ channel α-subunits NaV1.1, NaV1.2, NaV1.3 and NaV1.6 expressed in HEK293 cells. A, Examples of NaV1.3 currents evoked with a testing step potential to –10 mV, following 5-, 30-, and 500-ms pre-pulses to –120 mV in the absence (a) and presence (b) of (50 μM CBZ). The cells were held
-120 mV
-40 mV
-10 mV25 ms
Δt =5-500 ms
2000 ms
4 ms
2 nA5 ms
30 ms500 ms
Control
5 ms
30 ms
500 ms
50 μM CBZ
0
1
2
3
4
5
0 100 200 300 400 500
50 μM CBZ200 μM CBZ
Bloc
ked
Cur
rent
(nA)
Time (ms)
18.4 ms
18.2 ms
0
10
20
30
40
50
60
70
1.1 1.2 1.3 1.6
CBZLTG
Off
rate
(s-1
)
Na channel type
****
****
**
Aa b c
B

Chapter 3
42
at –40 mV for 2000 ms to permit drug binding to the inactivated channels, followed by a step to a recovery potential at –120 mV with a variable time duration Δt to facilitate channels to recover from inactivation and to allow drug dissociation. The whole protocol (shown as inset) was repeated every 5 s. The blocked current was determined by subtracting the control current (measured in the absence of CBZ) from the current recorded in the presence of CBZ and plotted against the time duration of the recovery Δt (c). The data points were fitted with a mono-exponential equation to determine the time constant (Tau) of CBZ unbinding, showing that the unbinding rate is concentration-independent (tau ~18 ms for 50 and 200 μM CBZ). B, Comparison of CBZ (all α-subunits) and LTG (NaV1.2 and NaV1.3 α-subunits) unbinding rates. These off rate values were determined with the procedure described in A (see also text). The CBZ off rate from the NaV1.3 channel (36.3 ± 2.7 s-1; n=12) was slower than those of the other three α-subunits (NaV1.1: 62.5 ± 2.7 s-1, n=4; NaV1.2: 53.3 ± 3.4 s-1, n=12; NaV1.6: 52.0 ± 1.1 s-1, n=5) and CBZ off rates from the NaV1.2 and NaV1.3 α-subunits were faster than those for LTG (20.1 ± 1.7, s-1 (n=6) and 18.9 ± 1.7 s-1 (n=9), respectively (multi-factor ANOVA with Fisher’s post-hoc test). * indicates p<0.05 and ** indicates p<0.01. Error bars indicate S.E.M.
Since the ratio of the off rate (k-1) and binding rate constant (k1) equals the
dissociation constant (KD=k-1/k1), it would seem appropriate to compare this ratio with the observed EC50 values of the AEDs for shifting the steady-state inactivation curves to hyperpolarizing potentials (Fig. 5). However, the off rate values were determined at a recovery potential of –120 mV and the binding rate constant experiments were performed at a equilibrium potential of –40 mV. In addition, the relative slow binding rate we found for DPH and LTG (Fig. 7) implicates that the 500-ms duration of the conditioning pulse used for determining the shift of the steady-state inactivation curves was probably too short, resulting in a certain underestimation of the EC50 values for these drugs. This makes it rather awkward to yield a correct estimate of the KD from the k-1/k1 ratios for DPH and LTG. Nevertheless, in the case of CBZ the on rate was found to be relatively fast and the k-1/k1 ratios for this drug displayed the same rank order as we observed for the CBZ EC50 values (NaV1.2≤NaV1.3<NaV1.6<NaV1.1; Fig. 5), indicating that the observed on and off rates at least in a qualitative way shape the CBZ affinities for the different α-subunits. DISCUSSION
Using the whole-cell voltage clamp technique we were able to make a detailed comparison of the biophysical and pharmacological properties of human NaV1.1, NaV1.2, NaV1.3 and NaV1.6 Na+ channels stably expressed in HEK293 cells. Although these have all previously been characterized individually (Goldin, 2001, Catterall et al., 2005), only relatively subtle functional differences have been described and it is unclear from these studies whether these are genuine differences or whether they can be attributed to differences in cell host systems (e.g. CHO cells vs. HEK cells), transfection methods (transient, vs. stable) and/or recording solution compositions. For example, properties of NaV1.3 currents differ considerably when this α-subunit is expressed in HEK293 cells or DRG neurons (Cummins et al., 2001). Contributing to this may be accessory β-subunits (Isom, 2001, Meadows et al., 2002, Goldin, 2003, Ulbricht, 2005) and/or phosphorylation of the channels by the major kinases (e.g. cAMP-dependent protein kinase A and protein

Pharmacology of α-subunits of human sodium channels
43
kinase C) (Cantrell and Catterall, 2001, Diss et al., 2004). This study therefore represents the first detailed study directly comparing the four major brain subtypes using the same expression system and cell background and using identical recording conditions.
The smaller ΔVh value (difference between the values for activation and steady-state inactivation; Table 1) we observed for the NaV1.1 current will result in a larger voltage range where the so-called window current will be active (Patlak, 1991, Johnston, 1995). Indeed we found that the NaV1.1 window current spanned a wider voltage range than those of the other three subunits (Fig. 2). This property may be relevant to the subcellular location of the NaV1.1 subunit in dendrites and cell bodies of neurons (Westenbroek et al., 1989) and would suggest that the window current may facilitate the excitatory synaptic signal transfer from the dendrite to the cell body. Furthermore, we found that the NaV1.3 current displayed the slowest recovery from inactivation time constant, which will result in a reduced excitability level of the neurons expressing the subunit. Thus the presence of NaV1.3 channels in neonatal neurons may help provide new-born mammals with a neuroprotective mechanism against hypoxic conditions (Park and Ahmed, 1991, Cummins et al., 1994). The time constants for the recovery from inactivation for the NaV1.1 and NaV1.6 currents were relatively fast and for NaV1.6, which is present at high densities in the nodes of Ranvier of myelinated axons (Boiko et al., 2001), this is compatible with fast action potential propagation in these axons. The main purpose of the present study was to compare the interactions of CBZ, DPH and LTG with the NaV1.1, NaV1.2, NaV1.3 and NaV1.6 α-subunits. The observed properties and values for the parameters describing these AED effects on the Na+ currents carried by the four α-subunits (e.g. use-dependent block, EC50 and maximal shift of Vh for steady-state inactivation) were in the same range previously reported for a large variety of cloned and native voltage-gated Na+ channels (Ragsdale et al., 1991, Kuo and Bean, 1994b, Xie et al., 1995, Ragsdale et al., 1996, Kuo et al., 1997, Kuo and Lu, 1997, Xie et al., 2001, Liu et al., 2003, Ilyin et al., 2005). All three AEDs were able to concentration-dependently shift the steady-state inactivation curves of the Na+ currents carried by the four α-subunits to more hyperpolarized potentials and to slow the recovery from inactivation process (Figs. 5 and 6). Nevertheless, some differences in the effects of AEDs between the different α-subunits were observed. When comparing the effects on the NaV1.2 and NaV1.3 currents, we observed that – in addition to differences in EC50 values – the maximal shift of the Vh value for steady-state inactivation evoked by LTG was larger than that of CBZ and DPH (~30 mV vs. ~15 mV). Differences in dissociation rates may underlie the latter effect (see below). No appreciable differences in effects of the three AEDs on the NaV1.2 and NaV1.3 currents were observed. However, it appeared that the affinity of CBZ for the NaV1.6 and especially the NaV1.1 subunits was lower (higher EC50 values) than that for the NaV1.2 and NaV1.3 subunits. This indicates that the sensitivity of neurons of different brain areas for AEDs can be distinctly different, dependent on the variant Na+ channel make-up of neurons present in these brain areas (Clare et al., 2000, Trimmer and Rhodes, 2004).
The effects of AEDs on the inactivation properties of voltage-gated Na+ channels that are discussed above will result in a use-dependent block of voltage-gated Na+ channels under high neuronal activity levels (e.g. epileptic events), when the Na+ channels will accumulate in the inactivated state(s) (Macdonald and Kelly, 1995, Rogawski and Loscher, 2004a). This was illustrated by the observation that the

Chapter 3
44
concentration-dependent block of the Na+ currents by CBZ and LTG occurred faster when the currents were evoked with high frequency stimulation trains (50 Hz vs. 10 Hz, Fig. 4). With higher frequency stimulation recovery is inefficient and a larger fraction of the Na+ channels remain in the inactivated state(s), allowing increased binding of CBZ and LTG and more effective channel blockade. It appeared that block by CBZ developed faster than for LTG, suggesting the latter has a slower binding rate. Indeed, it has previously been reported that the binding rate of CBZ to (inactivated) voltage-activated Na+ is faster than that of LTG (Kuo et al., 1997, Kuo and Lu, 1997) (see below). For CBZ the increase in the rate of block seen at 50 Hz versus 10 Hz was not influenced by the concentration of CBZ used, suggesting that, within the concentration range used, the CBZ binding rate is fast enough to effectively block the channels with either stimulation paradigm. Therefore the development of block depends solely on the fraction of available (i.e. inactivated) channels, which is larger in the case of currents evoked with the 50 Hz protocol. This was the case for all four α-subunits showing that with the stimulation frequencies used no differences in CBZ-channel interactions between the subunits could be observed. In contrast, subtype differences in interactions with LTG were observed using these stimulation paradigms. In particular, for NaV1.2 the magnitude of the increase in rate of block seen at 50 Hz versus 10 Hz was dependent on the concentration of LTG used. Thus at 30 μM LTG the development of block was 7-fold faster at 50 Hz than at 10 Hz whereas at 300 μM it was only 2-fold faster (fig 4E). This suggests a relatively slow binding rate of LTG to NaV1.2 such that at lower concentrations, binding is too slow to be fully effective in blocking the channels at the slower stimulation frequency where recovery from inactivation is efficient. However, block is more effective at faster stimulation frequencies, since inactivated channels accumulate due to less efficient recovery, or at lower frequency using a higher drug concentration since the binding rate is accelerated allowing block to develop more rapidly. Such differences in LTG effects were not observed for the NaV1.3 currents. This can be at least partially explained by the slower rate of recovery from inactivation of Nav1.3 compared to 1.2 (Fig. 3) suggesting that when stimulated at the10 Hz protocol, NaV1.3 channels do not recover as efficiently and can be more effectively blocked. Another potential contributory factor could be that the binding of LTG to this α-subunit is even slower than to NaV1.2 such that even at higher concentration it is still too slow to allow effective block at the lower stimulation frequency. In order to test the hypothesis that differences in binding rates to the α-subunits may underlie the different frequency sensitivity of AED block we measured binding rates experimentally. As expected we found that CBZ had a (much) faster binding rate to inactivated Na+ channels than DPH and LTG (Fig. 7) and the magnitude of these rates (CBZ: ~60×103 M-1s-1, DPH: ~8×103 M-1s-1, LTG: 18×103 M-1s-1) are in the range previously described for native voltage-gated Na+ channels (Kuo and Bean, 1994b, Kuo et al., 1997, Kuo and Lu, 1997). Thus the high CBZ binding rate can explain why the development of CBZ block (for all four α-subunits) has a relative small frequency and concentration dependency. The observed faster binding rate of LTG to the NaV1.2 α-subunit compared with that to the NaV1.3 α-subunit (21×103 M-1s-1 and 12×103 M-1s-1, respectively) is also consistent with our explanation for the large acceleration of block seen with Nav1.2 but not Nav1.3 when using higher LTG concentration with the 10 Hz stimulation protocol. Evidently, the slower LTG binding rate to the NaV1.3 α-subunit

Pharmacology of α-subunits of human sodium channels
45
prohibits such an acceleration. The rate of development of channel block is dependent not only on the binding rate of the AED but also on the off rate during the interpulse periods when the potential is stepped back (to –120 mV) and the drug is allowed to dissociate from its binding site (Ragsdale et al., 1996). Since the off rate of LTG for NaV1.2 and NaV1.3 channels was similar (Fig. 8), it seems likely that the higher frequency dependency of LTG (30 μM) block of the NaV1.2 subunit (compared with that of the NaV1.3 subunit) is determined by the faster LTG binding rate to the NaV1.2 subunit. For the NaV1.2 and NaV1.3 α-subunits the dissociation rate of LTG (20 s-1) appeared to be slower than that of CBZ (52 s-1 for NaV1.2 and 38 s-1 for NaV1.3). This lower LTG off rate may explain why LTG is able to induce a larger shift of the steady-state inactivation curve as compared to the effects of CBZ and DPH (Fig. 5) since it occupies its binding site for a longer period, allowing it to evoke a larger block and consequently a larger shift of Vh.
Our data suggest that the NaV1.3 α-subunit displays different CBZ binding and unbinding properties as compared to the other α-subunits (Figs. 7 and 8). This could have important consequences for AED efficacy in cases where epileptic tissues express the NaV1.3 α-subunit. This subunit is mainly present in embryonic and neonatal brain tissues (Felts et al., 1997, Chen et al., 2000), although more recent studies have demonstrated that the NaV1.3 subunit is expressed to some extent in the adult brain (Whitaker et al., 2001b, Lindia and Abbadie, 2003, Thimmapaya et al., 2005). However, there are indications that the NaV1.3 α-subunit is up-regulated in epileptic tissues (Bartolomei et al., 1997, Aronica et al., 2001, Whitaker et al., 2001a, Yu et al., 2006). Due to this increased expression of the NaV1.3 α-subunit Na+ currents in neurons of epileptic tissue may be less sensitive to AED block since the binding rate of AEDs to the NaV1.3 α-subunit is in general slower than that to the other α-subunits (Fig 7). This can especially be of importance in the case of epileptic events with relatively fast depolarization shifts (Kuo and Bean, 1994b, Kuo et al., 1997). Such mechanisms may therefore contribute to the phenomenon of pharmacoresistence in epilepsy where the changed target hypothesis (in this case Na+ channels) explains why a considerable fraction of epilepsy patients (~30%) during time become unresponsive to treatment with AEDs (Remy and Beck, 2006). However, also a reduced drug availability at the CNS targets (the so-called transporter hypothesis) may play a role (Remy and Beck, 2006). In addition, it has to be kept in mind that the biophysical and pharmacological properties of Na+ channel α-subunits may be different in native tissues, e.g. due to the modulatory actions of β-subunits (Meadows et al., 2002, Lenkowski et al., 2003). Nevertheless, our findings supply evidence for the concept that the dynamic shifts in Na+ channel protein expression (in addition to many other cellular proteins involved in shaping neuronal activity) during and after epileptic events (Ellerkmann et al., 2003, Gorter et al., 2006) will affect pharmacosensitivity. Consequently, this has important implications for understanding the role of voltage-gated Na+ channels in epilepsy, the treatment of this disorder and the development of new AEDs with Na+ channel affinity (Clare, 2006).

Chapter 3
46

CHAPTER 4
Sodium channel properties and functional changes by
carbamazepine in rat hippocampal CA1 neurons during development
Guangchun SUN, Taco R. WERKMAN and Wytse J. WADMAN
To be submitted

Chapter 4
48
AbstractThe whole-cell voltage clamp technique was used to investigate the electrophysiological properties of Na+ channels and their sensitivity to the anti-epileptic drug carbamazepine (CBZ) in hippocampal CA1 neurons from neonatal (at postnatal day 2-4) and adult (at postnatal day 36-41) rats. Compared with neonatal neurons, Na+ channels in adult neurons are present in higher channel density, their voltage dependence of steady-state inactivation was shifted to depolarized potentials and they had a faster time course of recovery from inactivation. These characteristics in adult neurons all result in an increased neuronal excitability. Possibly an altered Na+ channel subunits expression underlies this. Furthermore, CBZ had significantly stronger effects on slowing down the recovery from inactivation in neonatal than in adult neurons. But for the voltage shift of the steady-state inactivation, CBZ showed similar efficacy on them (only at 100 μM the shift was slightly larger in adult neurons). The higher sensitivity of neonatal neurons to CBZ maybe due to CBZ’s faster binding rate onto the inactivated channels, which is a consequence of functional properties of Na+ channel in neonatal neurons. The lower neuronal excitability and subsequently higher sensitivity to CBZ for neonatal neurons observed in this study could be helpful to understand the Na+ channel function and the efficacy of drugs under some pathological conditions, including epilepsy.
Introduction
Voltage-gated Na+ channels play an important role in cell excitability. They mediate an increase in Na+ ion permeability thereby transmitting depolarizing impulses rapidly throughout cells and cellular networks (Catterall, 1984). Na+ channel proteins consist of a pore-forming α subunit associated with auxiliary β subunits and to date ten structurally related α subunits and four β subunits have been identified (Catterall, 2000, Goldin, 2001, Yu et al., 2005). Expression of the α subunit alone is sufficient for the formation of functional Na+ channels, but the β subunits can modulate the properties of the channels (Cantrell and Catterall, 2001). So far, four different Na+ channel subtypes have been identified in rat brain: types I, II, III and VI (Noda et al., 1986a, Kayano et al., 1988, Lupa et al., 1995). Moreover, both type II and III genes encode two isoforms, termed A (for adult) and N (for neonatal), as a result of a mutually exclusive splicing of a single exon (Auld et al., 1988, Sarao et al., 1991, Gustafson et al., 1993). This splicing is developmentally regulated.
Many studies have shown that Na+ channels have distinct expression patterns in rat brain both in different brain regions and at different stages of development. For example, type I, II and VI are abundant in adult brain, whereas type III peaks at birth but becomes barely detectable in adult rats (Felts et al., 1997, Chen et al., 2000), although more recently it has been shown that still appreciable type III immunoreactivity is present in the adult rat brain (Lindia and Abbadie, 2003). In addition, in the human brain type III is detectable in many different brain structures (Chen et al., 2000, Whitaker et al., 2001b). All subtypes are detectable in the rat hippocampus (Black et al., 1994, Krzemien et al., 2000).
Drugs that block voltage-gated Na+ channels are well known as local anaesthetics, antiarrhythmics and anticonvulsants (Taylor and Meldrum, 1995). An important pharmacological property of many anticonvulsants (antiepileptic drugs; AEDs) is the use-

Sodium channels during development
49
dependent inhibition of neuronal Na+ currents, so they effectively inhibit only seizure discharges and spare most normal neuronal activities (Kuo, 1998, Yang and Kuo, 2002).
A commonly used AED is carbamezapine (CBZ) a non-sedative tricyclic compound effective in treatment of partial as well as generalized tonic-clonic seizures (Katzung, 2001). It is widely accepted that CBZ produces its antiepileptic effect by blocking (inactivated) Na+ channels which reduces the ability of neurons to conduct high frequency impulse flow (Macdonald and Kelly, 1994). Moreover, CBZ is also known to have a variety of other actions including inhibiting the uptake and release of norepinephrine from brain synaptosomes, and potentiating the postsynaptic action of γ-aminobutyric acid (GABA) (Katzung, 2001), thus decreasing neuronal excitability.
In the absence of a specific etiological understanding, epilepsy is treated with chronic administration of AEDs to suppress the seizures. However, about 30% of epilepsy patients do not respond to the usual AEDs including CBZ despite adequate drug treatment (Regesta and Tanganelli, 1999). Several studies indicate that in epileptic brain tissue expression patterns of α subunits of voltage-activated Na+ channels resemble those of the neonatal brain. For example, it was reported that the neonatal type П and Ш isoforms were induced in adult rat hippocampus by epileptic seizures (Gastaldi et al., 1997, Aronica et al., 2001). If indeed neonatal Na+ expression patterns occur in the epileptic brain, it is of importance to know how the new Na+ channel composition affects excitability and whether the efficacy of AEDs is different in epileptic tissue. Therefore were compared the effect of CBZ on Na+ currents in neonatal and adult rat hippocampal CA1 neurons. We describe that the Na+ currents in neonatal CA1 neurons display different electrophysiological properties and are more sensitive to CBZ.
Experimental procedures Animals
Six neonatal (at postnatal day (P) 2-P4) and six adult (P36-P41) male Wistar rats (Harlan Zeist, The Netherlands) were used in this study. All the animal experiments were performed in accordance with the regulations of the Animal Welfare Committee of the University of Amsterdam, which strives to minimize the use and suffering of experimental animals. Cell preparation
After decapitation, the brain was quickly removed and cooled in an oxygenated PIPES buffered dissociation solution, containing (mM) 120 NaCl, 5 KCl, 1 MgCl2, 20 PIPES, 25 D-glucose; pH 7.0 (adjusted using NaOH). The hippocampus was dissected and transverse slices (300 µm thick) were cut using a tissue chopper. From each slice the CA1 area was cut and transferred to an incubation chamber containing oxygenated dissociation solution and 1 mg/ml trypsin (type XI from bovine pancreas, Sigma) at 32
oC. For the much smaller neonatal rat brains, the dissection of the hippocampus and the cutting of the CA1 area were performed under a microscope. The neonatal and adult tissue cubes were enzymatically treated for 25 min and 45 min respectively. Tissue cubes were then washed with oxygenated dissociation solution and maintained in this solution at room temperature (20o C) until use. Neurons were isolated by trituration of a tissue cube in 0.5 ml extracellular solution (see below) through a series of Pasteur pipettes with

Chapter 4
50
decreasing diameter and brought into a perfusion chamber of an inverted microscope (Nikon). Pyramidal shaped neurons with a clear apical dendrite, a bright and smooth appearance and no visible organelles were selected for electrophysiological measurements (Vreugdenhil et al., 1998). Current recordings
Voltage-dependent Na+ currents were measured under whole-cell voltage clamp conditions with an Axopatch 200A amplifier (Axon Instruments) at room temperature (20-22o C). The patch pipettes (2-3 MΩ) were pulled from thin-wall borosilicate glass capillary tubes (1.5 mm outer diameter; Science Products GmbH, Hofheim, Germany) on a Brown/ Flaming puller (Model-P-87; Sutter Instruments Co.). The pipette solution contained (in mM) 110 CsF, 5 NaCl, 10 EGTA, 10 HEPES, 2 MgCl2, 25 TEACl, 5 MgATP, 0.1 NaGTP, 0.1 leupeptin. The pH was adjusted to 7.3 using CsOH. Neurons were continuously perfused with extracellular solution containing (in mM) 95 Choline-Cl, 20 NaCl, 10 HEPES, 2 CaCl2, 1 MgCl2, 5 KCl, 25 TEACl, 5 4-AP, 100 μM CdCl2 and 25 D-glucose; pH 7.4 (adjusted using HCl). For the neonatal rats, the 95 mM Choline-Cl in extracellular solution was replaced by NaCl to attain a final concentration of 115 mM NaCl because of the relatively lower Na+ current density in neonatal neurons. After gigaseal formation and cell membrane rupturing, series resistance was compensated for 75%. Voltage step protocols were applied by an Atari (TT030) computer controlling the Axopatch 200A amplifier. The membrane capacitance was read from the amplifier dials as a measure of membrane surface. The holding membrane potential was set at –70 mV. The currents were sampled at a frequency of 5 kHz and analyzed using custom-made software. 2-4 Min after establishing the whole-cell configuration, the cell was moved into either control- or drug-containing extracellular solution emitted by the application pipette using the Fast-Step Perfusion system (SF-77B, Warner Instrument Corporation, Hamden, USA). In each extracellular solution (control- or drug-containing) protocols were performed twice, and the control extracellular solution was always applied before and after drug application. A small drift of the voltage dependence of steady-state inactivation and recovery from inactivation with time was usually observed and compensated for when determining the drug effect (see results). The pulse interval was 1 sec and the duration of protocols was 2.5 minutes. Data analysis
Only electrotonically compact cells that did not escape voltage clamp and showed little current rundown during the experiment were incorporated in the analysis. The currents were corrected off-line for linear non-specific leak and residual capacitive current transients. Data are given as the mean ± standard error of the mean (S.E.M). Statistical comparisons were performed with the Student’s t-test. For comparison between multiple groups an ANOVA and the Dunn’s Bonferroni post-hoc test were used (unless otherwise stated). P < 0.05 was considered to indicate a significant difference. Drugs and reagents
Carbamazepine (Sigma) was dissolved in dimethylsulfoxide (DMSO) to make a stock solution of 200 mM. Then it was diluted in extracellular solution to reach the final

Sodium channels during development
51
concentrations required (15, 50 and 100 µM). The final concentration of DMSO was always 0.05 % (also in the control solution), which had no significant effects on Na+ currents. Results
Na+ channel properties of neonatal (P2-P4) and adult (P36-P41) rat hippocampal CA1 neurons were studied using the whole-cell voltage-clamp technique on activation, steady-state inactivation and recovery from inactivation. We also investigated the pharmacological properties of CBZ when interacting with Na+ channels of neonatal and adult neurons. Due to the (much) lower Na+ current density in neonatal CA1 neurons (see below) we measured for these neurons the Na+ currents in an extracellular solution with a high Na+ concentration (115 mM). In order to determine whether the different Na+ ion concentrations in the extracellular solution influence the voltage dependent properties of Na+ channels, we recorded adult CA1 neurons in both extracellular solutions (with 20 mM or 115 mM Na+). We found that with 115 mM Na+ in the extracellular solution the IV-relationship and steady-state inactivation curve were shifted to more depolarized potentials (5-10 mV) as compared to the recordings in 20 mM Na+ (n=2, data not shown). However, the removal from activation properties were hardly affected when recorded in extracellular solutions with different Na+ concentrations. In addition, effects of CBZ on voltage-activated Na+ currents were not different in both intracellular solutions (n=4; data not shown). Na+ channel properties of CA1 neurons from neonatal and adult rats. Activation, steady-state inactivation and recovery from inactivation.
Na+ currents were activated by 25-ms depolarization steps to levels between –70 mV and +10 mV from a pre-pulse potential of –150 mV (inset Fig. 1A). The depolarization activated a fast, transient inward Na+ current that first increased in peak amplitude as the channels open and at higher potentials decreased due to the reduced driving force (Fig. 1A). We determined the peak amplitude of the current for each voltage step and constructed a current-voltage relationship (Fig. 1B). This relationship was fitted to the Goldman-Hodgkin-Katz current equation (Hille, 2001) using a Boltzmann function to describe the Na+ permeability as a function of membrane voltage (V):
)exp(1
)exp()][][(
)Vexp(1
1)(ha
maxV
VNaNa
VV
VgVI out
in
c
α
α
−−
−−++
×−
+××= (1)
With α = F/RT and gmax = αF [Na+]out P0 where P0 is the maximal permeability, F is the Faraday constant, R is the gas constant and T represents the absolute temperature. The maximal conductance of the current is gmax (nS), while the potential of half-maximal activation (Via) and the slope parameter (Vc) characterize its voltage dependence. Compared with neonatal neurons, adult neurons have a larger Na+ channel conductance (gmax: 26.5 ± 3.1 nS, n = 10 for neonatal neurons; 90.9 ± 7.9 nS, n = 14 for adult neurons; p < 0.01). The membrane capacitance (Cm) as a measure of membrane surface was

Chapter 4
52
smaller for neonatal neurons (5.6 ± 0.4 pF) as compared with that of adult neurons (7.2 ± 0.5 pF) (p < 0.05). We calculated the current conductance density that was defined as gmax/Cm (nS/pF), and found that adult neurons had a higher Na+ conductance density (13.3 ± 1.3 nS/pF for adult neurons and 5.1 ± 0.8 nS/pF for neonatal neurons, p < 0.01). The more comparable value gmax/Cm of adult neurons should be bigger than the present value (13.3 nS/pF), because the gmax was even bigger when we used 115 mM Na+ ion concentration (the same as used on neonatal neurons) instead of 20 mM in extracellular solution (data not shown). For the voltage dependence of activation, no differences were found between neonatal (Vha: –29.0 ± 0.4 mV; Vc: –5.3 ± 0.3; n=10) and adult (Vha: –29.1 ± 0.3 mV; Vc: –5.1 ± 0.2; n=14) neurons (Fig. 1B). Nonetheless, since under conditions with low Na+ ion concentrations (20 mM) in adult neurons we observed a shift of the IV-relationship to depolarized potentials (see above), we cannot exclude the possibility that this also occurred in the neonatal neurons, thus making it difficult to compare the activation properties when measured under conditions with different extracellular Na+ concentrations.
A du lt
0 .5 nA
10 m s
N eona ta l
0 .5 nA
10 m s-70 m V -70 m V
10 m V
-15 0 mV
25 ms
500 m s
-3 .0
-2 .5
-2 .0
-1 .5
-1 .0
-0 .5
0 .0
-6 0 -40 -20 0 20
A du ltN eo na ta l
Ampl
itude
(nA)
V o ltag e (m V )
A 1 A 2
B
Figure 1. Voltage dependence of Na+ channel activation in CA1 neurons from neonatal and adult rats. (A) Examples of voltage-activated Na+ currents in CA1 neurons from an adult (A1) and a neonatal rat (A2). Na+ currents were activated by 25-ms depolarizing voltage steps ranging from –70 mV to +10 mV, following a 500-ms hyperpolarizing pre-pulse to –150 mV (see inset). (B) The mean peak amplitudes of the Na+ current in adult (n = 14) and neonatal (n = 10) neurons were plotted as function of membrane potential and fitted with the Goldman-Hodgkin-Katz current equation (Eq. 1). The voltage of half-maximal activation (Vha) and the slope parameter (Vc) obtained from the fitting procedure

Sodium channels during development
53
in neonatal neurons (–29.0 ± 0.4 mV, –5.3 ± 0.3) are similar to those in adult neurons (–29.1 ± 0.3 mV and –5.1 ± 0.2). Error bars indicate S.E.M.
The voltage dependence of steady-state inactivation of the Na+ current was
measured by varying a 500-ms hyperpolarizing pre-pulse from –150 to –35 mV followed by a 25-ms depolarization step to –25 mV (inset Fig. 2A). The peak amplitude of the current (I) evoked at –25 mV was normalized to Imax and plotted as a function of pre-pulse potential (V). The data points were fitted with a Boltzmann equation:
)exp(1
1I/)( m
c
hiax
VVV
VI−
+= (2)
Where Vhi is the potential of half-maximal inactivation and Vc is proportional to the slope of the curve. When comparing these properties it can be seen that the steady-state inactivation curve of Na+ currents in neonatal neurons is shifted towards more hyperpolarized potentials (Fig. 2B). This is reflected by a more negative Vhi value in neonatal neurons as compared to that of adult neurons (–68.4 ± 0.4 mV (n=10) and –62.6 ± 0.3 mV (n=14), respectively, p < 0.01). This difference may be an underestimation, since in solutions with a low Na+ concentration the steady-state inactivation curve (of adult neurons) was found to be shifted to hyperpolarized potentials (see above). The Vc values were also statistically different between the two groups (–7.8 ± 0.4 mV for neonatal neurons and –6.9 ± 0.2 mV for adult neurons, p < 0.05), showing that the curve for the adult neurons is slightly steeper (Fig. 2B).
Adult
0.5 nA
10 m s
Neonatal
0.5 nA
10 m s
-35 mV
-70 mV
-150 mV500 ms
-25 mV25 ms
-70 mV
0
0.2
0.4
0.6
0.8
1
-120 -100 -80 -60 -40 -20
Adult Neonata l
Avai
labl
e fra
ctio
n
Vo ltage (m V)
A1 A2
B
Figure 2. Voltage dependence of Na+ current steady-state inactivation in CA1 neurons from neonatal and adult rats. (A) Examples of voltage-inactivated Na+ currents in CA1

Chapter 4
54
neurons from an adult rat (A1) and a neonatal rat (A2). Na+ currents were evoked with a step depolarization to –25 mV for 25 ms following 500-ms hyperpolarizing pre-pulses between –150 mV and –35 mV. (B) The normalized conductance of steady-state inactivation for both adult and neonatal neurons were plotted as a function of membrane potential and fitted with the Boltzmann function (Eq. 2). The voltage of half-maximal inactivation (Vhi) in adult neurons (–62.6 ± 0.3 mV, n = 14) was 5.8 mV depolarized compared with the Vhi value in neonatal neurons (–68.4 ± 0.4 mV, n = 10), p < 0.01. Also the Vc values for both groups were different (–7.8 ± 0.4 mV for neonatal neurons and –6.9 ± 0.2 mV for adult neurons, p < 0.05). Error bars indicate S.E.M.
The time course of the recovery from inactivation was determined using a double-
pulse protocol (inset Fig. 3A). The interval ∆t (during which the current was allowed to recover) between two 25-ms depolarization steps was varied between 1 and 200 ms. The recovery time constant was determined at membrane voltages of –70, –80, –90 and –100 mV. The amplitude of the Na+ current activated by the second pulse was plotted as a function of ∆t and fitted with a single-exponential function to give the time constant of recovery from inactivation (Tau) (Fig. 3B). Recovery from inactivation of voltage-activated Na+ currents was faster at more hyperpolarized potentials, and this recovery was faster in adult neurons than in neonatal neurons at each membrane potential (two-factor Anova, p < 0.001) (Fig. 3C). Effects of CBZ on Na+ channels in CA1 neurons from neonatal and adult rats
Three concentrations of CBZ (15, 50 and 100 µM) were applied on each cell and every CBZ concentration was always applied between two control recordings. The voltage step protocols were performed twice in each extracellular solution (control or CBZ-containing). There was a certain drift during time of the voltage-dependence of steady-state inactivation to more hyperpolarized potentials and also the time constant of recovery from inactivation showed a small increase during time (data not shown). For both parameters a correction was applied to exclude obscuring effects of these shifts on the CBZ effects.
CBZ did not affect Na+ current activation in both neonatal and adult neurons (Fig. 4A). CBZ effects on steady-state inactivation To determine the effect of CBZ on steady-state inactivation, the protocol described in Fig. 2A was used. CBZ concentration-dependently shifted the steady-state inactivation curves of Na+ currents to more hyperpolarized potentials in both adult and neonatal neurons (the CBZ effect on neonatal neurons is given in Fig. 4A). The absolute shift of curve midpoints (∆Vhi) in Fig. 4A was determined in each cell by the difference of Vhi in the absence and presence of CBZ as a function of CBZ concentration (0, 15, 50, 100 µM; Fig. 4B). The ∆Vhi calculation excludes the interference of the drift of voltage dependence on inactivation during time (~10 mV/30 min). The data points were fitted with a logistic equation:

Sodium channels during development
55
Figure 3. Voltage-dependent properties of recovery from inactivation of Na+ currents in neonatal and adult rat CA1 neurons. The time course of recovery from inactivation was determined by a double-pulse protocol (see inset in A). The variable interval (∆t = 1, 2, 5, 10, 20, 50, 100 or 200 ms, during which the current was allowed to recover) between two 25-ms depolarizing voltage steps to –25 mV was used to determine the recovery from inactivation at the membrane voltages –70 mV, –80 mV, –90 mV, and –100 mV. (A) Three examples of Na+ currents activated by two double pulses applied with different time intervals are shown: (a) ∆t = 200 ms, (b) ∆t = 10 ms and (c) ∆t = 1 ms. (B) The amplitude of the Na+ current activated by the second pulse is plotted as a function of ∆t and fitted with a single-exponential function to give the time constant of recovery from inactivation (Tau, one example at membrane potential –80 mV). C. Tau values of neonatal (n = 17) and adult neurons (n = 17) at different membrane voltages. The recovery was voltage-dependent for both neuron types and faster in adult neurons (two-factor Anova, p < 0.001). Error bars indicate S.E.M. For comparison between neuron types or the recovery voltage for the same neuron type * indicates p < 0.05 and ** indicates p < 0.01; ^ indicates p < 0.01 for the membrane voltage for the same neuron type compared to –70 mV (all Dunn’s Bonferroni post-hoc test).
1 nA
20 ms
a
b
c
-2.0
-1.5
-1.0
-0.5
0.00 20 40 60 80 100
Cur
rent
am
plitu
de (n
A)
Pulse interval, Δt (ms)
-70 mV -70 mV
-25 mV25 ms 25 ms
Δt = 1~200 ms
-70 mV-80 mV
-90 mV
-100 mV
-25 mV
0
5
10
15
20
25
30
35
-70 -80 -90 -100
AdultNeonatal
Tau
(ms)
Potential (mV)
**
^
^^
^
^^
***
*
A B
C

Chapter 4
56
( )
[ ]CBZEC
VCBZV hi
hi50
max
1+
Δ=Δ (4)
where ∆Vhimax is the maximal shift of Vhi, EC50 is the CBZ concentration that causes half-maximal ∆Vhi and [CBZ] is the applied concentration of CBZ. The estimated values of ∆Vhimax and EC50 were 13.8 mV and 74.1 µM, respectively for neonatal neurons (n=14–7) and 24.5 mV and 165.1 µM, respectively for adult neurons (n=14–16) (Fig. 4B). This indicates that with higher concentrations of CBZ in adult neurons a larger voltage shift of steady-state inactivation can be obtained (p < 0.01). It was found that in the presence of 100 µM CBZ the ∆Vhi was slightly larger in adult neurons (compared with neonatal neurons, p < 0.05), but the concentration-response curves were not significantly different (two-factor Anova) (Fig. 4B).
0
0.2
0.4
0.6
0.8
1
-120 -100 -80 -60 -40 -20
control15 μM CBZ50 μM CBZ100 μM CBZ
0
0.2
0.4
0.6
0.8
1
Voltage (mV)
Ava
ilabl
e fra
ctio
n Open fraction
ActivationInactivation
0
2
4
6
8
10
12
0 20 40 60 80 100 120
AdultNeonatal
[CBZ] (μM)
ΔV
hi (m
V)*
A B
Figure 4. Voltage shift of the Na+ current steady-state inactivation relationship by CBZ in CA1 neurons from neonatal and adult rats. (A) The normalized inactivation curve in neonatal neurons was shifted towards more hyperpolarized direction with increasing concentrations of CBZ (n=14-17; see protocol in Fig. 2). The available fraction at a certain voltage of the inactivating pre-pulse was defined as the normalized peak current (relative to the current evoked following an inactivating pre-pulse to –150 mV). The data points were fitted with a Boltzmann function (see Eq. 2) resulting in Vhi values (in mV) of –67.8, –76.7, –83.3, –86.67; and Vc values (in mV) of –8.0, –8.3, –8.0, –7.5 for control and 15, 50, and 100 μM CBZ (from right to left), respectively. To the right, the activation curves of the Na+ current in the absence and presence of the highest CBZ (100 μM) concentration are shown. The conductance (G) at each voltage was determined from the relation G=I/(V-VR), where I is the peak current amplitude, V is the step potential and VR is the reversal potential (calculated to be 79 mV). The conductance values were normalized (to Gmax) to yield the open fraction and fitted to a Boltzmann equation, resulting in Vha values (in mV) of –46.2 and –45.9; and Vc values (in mV) of 6.3 and 6.5

Sodium channels during development
57
for control and 100 μM CBZ, respectively. (B) The shift of Vhi (∆Vhi) was established in each neuron by determining the difference of the Vhi value in the absence and presence of CBZ and was plotted against the concentration of CBZ (neonatal neurons, n = 14-17; adult neurons, n = 14-16). Data points were fitted with a logistic function (Eq. 4) resulting in the estimated values of maximal ∆Vhi (∆Vhimax) and the concentration that causes half-maximal ∆Vhi (EC50) for neonatal (13.8 ± 0.5 mV and 74.1 ± 5.4 µM, respectively) and adult (24.5 ± 1.7 mV and 165.1 ± 17.1 µM, respectively) neurons. The ∆Vhi value only showed a significant difference at 100 μM CBZ between neonatal (n = 14) and adult (n = 14) neurons (* indicates p < 0.05, Student’s t-test). Error bars indicate S.E.M.
CBZ effects on recovery from inactivation
The time course of recovery from inactivation was determined with the same double-pulse protocol as described in Fig. 3A. CBZ concentration dependently slowed down the recovery from inactivation, represented by the increased time constant (Tau) of recovery from inactivation in the presence of different CBZ concentrations (Fig. 5). Like with the voltage-dependent parameters for activation and steady-state inactivation (especially Vh, see above) the Tau values for recovery of inactivation are not constant during time. This recovery becomes slower during the recording period (i.e. the Tau values become larger) and we corrected for this by determining the change of Tau value in the presence of CBZ compared to the Tau values measured during the application with control buffer (shortly before and after the CBZ applications). This ∆Tau calculation excludes the interference of the shift of Tau during time, thus giving a more accurate estimation of the CBZ-induced slowing of the recovery of inactivation (insets Fig. 5). Although the average Tau value for the neonatal neurons under control conditions was slower compared to that of the adult neurons (Fig. 3), stronger effects by CBZ were observed in neonatal neurons, which were also concentration- and voltage-dependent (multi-factor Anova, p < 0.001; Fig. 5), indicating that over the whole tested voltage range (–70 mV through –100 mV, but especially at –70 mV and –80 mV) in neonatal neurons CBZ induces a larger slowing of inactivation of voltage-activated Na+ currents as compared to the adult currents. For instance, in the presences of 15 μM CBZ the recovery of inactivation of neonatal Na+ currents at –80 mV was slowed by 27%, whereas the adult Na+ currents displayed only a decrease of 9%. Binding rate constants of CBZ onto the fast inactivated Na+ channels in CA1 neurons from neonatal and adult rats
Experiments were performed to determine the binding rate at which CBZ binds to the inactivated Na+ channels, and it was assessed by a voltage protocol described in Fig. 6A (Kuo, 1997). With such a protocol the channels were exposed to a depolarizing voltage step (to –40 mV) of different durations (30-2500 ms). Longer depolarizing voltage steps allow more channels to enter the inactivated state and due to the much higher affinity of CBZ to this state more channels will be blocked. Fig. 6B demonstrates that with increasing pre-pulse durations more Na+ current got blocked in the presence of 50 μM CBZ. By subtracting the control current (no CBZ present) from the current in the

Chapter 4
58
presence of CBZ at each pre-pulse duration, the CBZ-blocked current was obtained. This procedure eliminates the contamination by slowly inactivating currents. Expressing the blocked current as function of the pre-pulse duration shows the development of CBZ block, a relationship that can be fitted with a mono-exponential function and the resulting Tau value describes the time course of development of block for each CBZ concentration (Fig. 6C). The 1/Tau value at each CBZ concentration yields the binding rates and these increased linearly with higher CBZ concentrations for adult and neonatal neurons (Fig. 6D). The slopes of these linear relationships give the binding rate constant of CBZ for Na+ channels of neonatal and adult CA1 neurons. The slopes were determined for each individual neuron and the average values were 55.5 ± 6.6 × 103 M-1s-1 for neonatal neurons (n=14) and 33.7 ± 2.3 × 103 M-1s-1 for adult neurons (n=14), a statistically significant difference (p < 0.01, Student’s t-test). This finding indicates that the binding of CBZ to the inactivated Na+ channels is faster in neonatal neurons than in adult neurons.
Figure 5. CBZ slows down the recovery from inactivation at different membrane potentials of Na+ currents in neonatal and adult CA1 neurons. The same voltage step protocol was used as in Fig. 3. The Tau values are expressed against the CBZ concentrations 15, 50 and 100 μM, at membrane potential –70 mV (A), –80 mV (B), –90 mV (C) and –100 mV (D). ∆Tau values (the difference of Tau in the absence and presence
0
10
20
30
40
50
60
15 50 100
-70 mVAdultNeonatal
[CBZ] (μM)
Tau
(ms)
0
10
20
30
40
50
60
15 50 100
-80 mV
AdultNeonatal
[CBZ] (μM)
Tau
(ms)
A B
0
10
20
30
40
50
60
15 50 100
-90 mVAdultNeonatal
[CBZ] (μM)
Tau
(ms)
0
10
20
30
40
50
60
15 50 100
-100 mVAdultNeonatal
[CBZ] (μM)
Tau
(ms)
C D
0
5
10
15 50 100[CBZ] (μM)
ΔTa
u (m
s)
ΔTau
**** *
0
5
10
15 50 100[CBZ] (μM)
ΔTa
u (m
s)
ΔTau
****
**
0
5
10
15 50 100[CBZ] (μM)
ΔTa
u (m
s)
ΔTau
** ***
0
5
10
15 50 100[CBZ] (μM)
ΔTa
u (m
s)
ΔTau
** *

Sodium channels during development
59
of CBZ) are given as insets in the four panels. The effects of CBZ were concentration- and voltage-dependent (multi-factor Anova, p < 0.001). A stronger CBZ effect for almost all concentrations on ΔTau in neonatal neurons (n=6-15) was observed as compared with adult neurons (n=12-15); * indicates p < 0.05 and ** indicates p < 0.01, compared to the effect on adult neurons with the same CBZ concentration. Error bars indicate S.E.M.
50 μM CBZ
2500 ms
30 m s
250 m s
0.5 nA
5 ms
Control
2500 ms
30 m s250 m s
0.5 nA
5 ms
A B
0
0.2
0.4
0.6
0.8
1
1.2
1.4
1.6
0 0.5 1 1.5 2 2.5
15 μM CBZ50 μM CBZ100 μM CBZ
Blo
cked
cur
rent
(nA)
Pre-pulse duration (s)
0
1
2
3
4
5
6
7
0 20 40 60 80 100
AdultNeonatal
Bin
ding
rate
(s-1
)
[CBZ] (μM)
55.5 ± 6.6 x 10 3 M -1s-1
33.7 ± 2.3 x 103 M -1s-1
C D
-150 mV -150 mV
-40 mV-25 mV
5 ms
5 ms
Δ t=30-2500 ms
Figure 6. Binding rates of CBZ onto the fast-inactivated state of Na+ channels in CA1 neurons from neonatal and adult rats. (A) The neurons were held at –150 mV and pre-pulsed to –40 mV with increasing time duration (Δt = 30-2500 ms). After a recovery gap potential at –150 mV for 5 ms (allowing most of the drug-free inactivated Na+ channels to recover), the available current was determined with a 5-ms testing potential to –25 mV. The pulse interval was 5 s. (B) Examples of Na+ currents at the testing potential (to –25 mV) in one adult CA1 neuron with 30, 250, and 2500 ms pre-pulse time durations are shown in the absence (upper traces; control) and presence of 50 μM CBZ (lower traces). (C) Example of how development of block was estimated. The blocked current was determined by subtracting the control current (measured in the absence of CBZ) from the current recorded in the presence of CBZ and this was plotted against the time duration of the pre-pulse Δt. The data points were fitted with a monoexponential equation to determine the time constant (Tau) for development of block in the presence of 15, 50 and

Chapter 4
60
100 μM CBZ. (D) The binding rates (1/Tau, s-1) of CBZ to the inactivated state of the Na+ channel in adult and neonatal neurons are plotted against the CBZ concentration. The slopes of the linear regression fits (determined for each individual neuron) give the binding rate constant for CBZ, which was 55.5 ± 6.6 × 103 M-1s-1 for neonatal neurons (n=14) and 32.3 ± 2.6 × 103 M-1s-1 for adult neurons (n=14). Based on the average slope and intercept values the plotted lines were constructed. Error bars indicate S.E.M.
DISCUSSION
We used the whole-cell voltage-clamp technique to investigate the properties of Na+ channel in CA1 neurons from neonatal (P2-P4) and adult (P36-P41) rats and furthermore to compare the effects of CBZ on these currents. Na+ currents in adult neurons were recorded in an extracellular solution containing a reduced Na+ concentration (20 mM) to avoid poor voltage clamp conditions due to too large Na+ currents. On the other hand, Na+ current density in neonatal CA1 neurons was considerably smaller and therefore we had to record these Na+ currents in an extracellular solution with a high Na+ concentration. We found that the activation and steady-state inactivation properties of adult Na+ currents measured in solutions with 115 mM Na+ were shifted to depolarized potentials, an effect that could be due to different screening properties of Na+ and choline ions and thus affecting the voltage dependent characteristics differently (Hille, 2001). Developmental changes on Na+ channel density, voltage dependence of steady-state inactivation and time course of recovery from inactivation
In excitable cells a dynamic re-arrangement of voltage-gated ion channels (including voltage-activated Na+ channels) underlies the continuously changing excitability modes during development (Moody and Bosma, 2005). We found that adult CA1 neurons have a larger Na+ channel conductance, which is due to the bigger Na+ conductance density (gmax/Cm) and which can only partly be explained by the larger cell capacitance. The increased Na+ current density with development is comparable to what Cummins et al. found in rat neocortical neurons, which is due to changes in the number of functional channels (channel density) (Cummins et al., 1994). A similar finding was also found in Xenopus laevis oocytes injected with mRNA extracted from adult or neonatal rat brains, and in younger and older diencephalic neurons from fetal rats grown in a defined medium (Park and Ahmed, 1991, Virginio and Cherubini, 1995). It was thought that the lower Na+ channel density in neonatal neurons could result in a decreased cell excitability and lower susceptibility to hypoxia which is a kind of protection for newborn mammals (Park and Ahmed, 1991, Cummins et al., 1994). In addition, the developing brain is able to respond to hypoxic conditions by changing its Na+ channel expression patterns (Zhao et al., 2005).
The Vhi of steady-state inactivation in adult neurons shifted 5.8 mV to more depolarized potentials compared with neonatal neurons. A similar shift was also found by Virginio and Cherubini (Virginio and Cherubini, 1995) in Xenopus laevis oocytes injected with mRNA extracted from adult or neonatal rat brains. The depolarized shift of Vhi could result in a higher neuronal excitability of adult neurons because of the higher

Sodium channels during development
61
threshold for Na+ channel inactivation, whereas Na+ currents of neonatal neurons could be more susceptible to steady-state inactivation. Assuming that in neonatal neurons high extracellular Na+ concentrations also result in a shift of activation and steady-state inactivation properties to more depolarized potentials (see above), it is likely that the magnitude of the difference of Vhi values for adult and neonatal Na+ currents is an underestimation.
Interestingly, we observed that the time course of recovery from inactivation significantly became faster with development, a property that was not affected by the different extracellular Na+ concentrations), which has not been reported before. This characteristic also contributes to the enhanced ability of mediating excitability in adult neurons.
Taken together, it is suggested from our study that it is easier to generate action potentials in adult CA1 neurons than in neonatal CA1 neurons. The higher Na+ channel density, the higher threshold for channel inactivation and the decreased time course of recovery from inactivation all support this point.
The expression of Na+ channel α and β subunits that follow a distinct temporal and spatial pattern during development could account for these changes. The expression of Na+ channel α subunits I, П, Ш and VI was examined in developing hippocampus by Felts (Felts et al., 1997) and Brysch (Brysch et al., 1991). They found that type П subunit was abundant and that type VI subunit was detectable at all developmental stages, whereas type Ш subunit was barely detectable at P30 but was mainly expressed at late embryonic and early postnatal time points. However, a more recent study shows that also in the adult rat brain type III Na+ channel subtypes are present, albeit at lower levels than the other subtypes (Lindia and Abbadie, 2003), a finding that resembles the situation in the human brain (Whitaker et al., 2001b). For β subunits, β1 and β2 subunits only occurred after postnatal day 3 (P3), whereas the β3 subunit is already present in embryonic tissues (Shah et al., 2001). Although ion permeability and voltage sensing is primarily determined by α subunits, β subunits are important modulators of Na+ channel function (Yu et al., 2005). For example, co-expression of β1 subunits with type IIA α subunits in Xenopus oocytes shifted the voltage dependence of Na+ channel activation and inactivation to more negative membrane potentials (Isom et al., 1995). Coexpression of β2 with α subunits in Xenopus oocytes increased functional expression, modulated gating, and increased the membrane capacitance (Isom et al., 1995).
The neurons in our study were from P2–P4 and P36–P41 rats and the differences in functional properties of the voltage-dependent Na+ currents we encountered corroborates a shifting expression pattern of Na+ channel subunits during development. Interestingly, in epileptic hippocampus the neonatal type П and Ш isoforms were induced (Gastaldi et al., 1997, Aronica et al., 2001), and our study indicates that neonatal Na+ channels are less excitable. So we hypothesize that the re-expression of the neonatal isoforms of Na+ channel in epileptic tissue is a kind of compensation mechanism, which can protect the normal function of brain from the higher neuronal excitability. Reduced efficacy of CBZ on slowing down the recovery from Na+ channel inactivation during development

Chapter 4
62
We studied the effects of the AED CBZ on both neonatal and adult CA1 neurons. It is well-known that Na+ channel is the major target for most of the anti-epileptic drugs including CBZ, and their effects mostly are evaluated by acting on steady-state inactivation and recovery from inactivation (Macdonald and Kelly, 1994). The (concentration-dependent) shift of the steady-state inactivation curve of the Na+ current by CBZ was not different in neonatal and adult neurons, although at the highest tested concentration (100 μM) CBZ appeared to be more potent in the adult neurons. However, the recovery from inactivation of the voltage-dependent Na+ current was differentially affected by CBZ in neonatal and adult CA1 neurons. In both neuron types CBZ concentration-dependently slowed the recovery of the inactivation process, but especially at membrane voltages of –70 and –80 mV this effect was more pronounced in the neonatal neurons. The underlying mechanism may be the observed faster binding rate of CBZ to the (inactivated) neonatal Na+ currents. This property may result in more blocked (inactivated) Na+ channels in neonatal neurons than in adult neurons with decreasing pulse intervals, thus slowing the recovery of inactivation process more efficiently in the neonatal neurons. These findings suggest that neurons expressing neonatal Na+ currents may be more sensitive to CBZ and that consequently CBZ could more easily reduce hyperactivity in these neurons. This may be of importance for the treatment of epilepsy with AEDs like CBZ, since it has been shown that in epileptic brain tissue different (neonatal) Na+ channels can be expressed (Lombardo et al., 1996, Gastaldi et al., 1997, Aronica et al., 2001, Whitaker et al., 2001a). It remains to be determined whether the epilepsy-induced expressed neonatal Na+ channels resemble the functional and pharmacological profile of the Na+ channels we studied in the neonatal CA1 neurons. Nevertheless, our findings corroborate the possibility that neurons in epileptic brain tissue possess different functional and pharmacological properties as compared to neurons from healthy tissue, which may have important consequences for the understanding of the etiology of epilepsy and its treatment.

CHAPTER 5
Kinetic changes and modulation by carbamazepine on voltage-gated
sodium channels in rat CA1 neurons after epilepsy
Guangchun SUN, Taco. R. WERKMAN, and Wytse. J. WADMAN
Acta Pharmacologica Sinica 2006, 27: 1537-1546

Chapter 5
64
ABSTRACT
AIM: To study whether the functional properties of sodium channel, and subsequently the channel modulation by carbamazepine (CBZ), in hippocampal CA1 neurons can be changed after epileptic seizures. METHODS: We used the acutely dissociated hippocampal CA1 pyramidal cells from epilepsy model rats three-week and three-month after kainate injection, and the whole-cell voltage-clamp techniques. RESULTS: After long-term epileptic seizures, 1) both sodium channel voltage-dependence of activation and steady-state inactivation shifted to more hyperpolarizing potentials, which resulted in the enlarged window current; 2) the membrane density of sodium current decreased; 3) the time constant of recovery from inactivation increased; 4) CBZ displayed unchanged efficacy on sodium channels, with similar binding rate to them, except that at higher concentration the voltage shift of inactivation reduced. For the short-term kainate model rats, no differences were detected between control and epilepsy groups. CONCLUSION: These results indicate that the properties of sodium channel in acutely dissociated hippocampal neurons could be changed following long-term epilepsy, but the alternation might not be enough to induce the channel resistance to CBZ. INTRODUCTION
Epilepsy is a common neurological disorder, affecting approximately 1 – 2% of
the population (Browne and Holmes, 2001). It is a chronic and often progressive brain disorder, characterized by the periodic and unpredictable occurrence of seizures (Lothman, 1996). In the absence of a specific etiological understanding, chronic administration of antiepileptic drugs (AEDs) to suppress the seizures is the treatment in epilepsy. However, about 30% of epilepsy patients do not respond to the usual AEDs despite adequate drug treatment (Regesta and Tanganelli, 1999). Voltage-gated sodium channels are molecular targets of many of the most widely used AEDs, like CBZ, because they mediate regenerative inward currents that are responsible for the initial depolarization of action potentials in brain neurons. The AEDs suppress the abnormal neuronal excitability associated with seizures by means of complex voltage- and frequency-dependent inhibition of ionic currents through sodium channels (Ragsdale and Avoli, 1998).
Voltage-gated sodium channels have three functional states: open, resting and inactivated. Membrane depolarization activates channels from the resting to the open state allowing the rapid influx of sodium ions. During prolonged depolarization (>1 ms), the channels inactivate and sodium influx declines; in this state, the channels remain closed and are refractory unless the membrane is repolarized to allow them to recover to the resting state (Clare et al., 2000). CBZ, as well as phenytoin and lamotrigine, binds to a common receptor located on the extracellular side of the sodium channel, and they all have much higher affinity to the inactivated state than to the resting state of the sodium channel (Kuo, 1998).
The brain sodium channel proteins consist of a pore-forming α subunit associated with auxiliary β subunits - β1, β2, and/or β3 (Catterall, 1995, Catterall, 1999, Catterall, 2000). So far four different sodium channel subtypes have been identified in rat brain: І,

Sodium current properties in the kainate model of epilepsy
65
П, Ш and VI (Noda et al., 1986b, Kayano et al., 1988, Schaller et al., 1995). The expression of α or β subunits in neuron can be altered during the epileptogenic process either in model rats or in human tissue (Bartolomei et al., 1997, Gastaldi et al., 1997, Gastaldi et al., 1998, Whitaker et al., 1999, Whitaker et al., 2000, Aronica et al., 2001, Whitaker et al., 2001a, Aronica et al., 2003). In rodents, systemic administration of kainate, a glutamate receptor agonist, induces the development of the well-described model of limbic seizures which is accompanied with neuronal cell death, axonal sprouting and neosynaptogenesis in hippocampus as well as the induction of specific genes (Ben-Ari and Represa, 1990).
The hippocampus plays a crucial role in the pharmacoresistance of temporal lobe epilepsy in epilepsy patients (Jeub et al., 2002), and the mechanisms underlying pharmacoresistance most likely involve the functional and morphologic changes developing in hippocampus in the course of the disease (Heinemann et al., 1994). So our question rises: whether the properties of the sodium channel in hippocampal neurons could be changed after short-term and long-term kainate-induced epilepsy; whether the efficacy of CBZ might be reduced following epilepsy.
MATERIALS AND METHODS
Animals 26 male Sprague Dawley rats (Harlan Zeist, The Netherlands), weighing 150- 200 gram at the time of kainate injection, were used in this study. 12 rats were for three-week kainate model experiments (6 rats in each control and kainate group) and 14 rats were for three-month one (7 rats in each control and kainate group). The rats were housed in individual cages under a controlled environment (21 ± 1 oC; humidity 60%; light on 08.00-20.00). Food and water were available ad libitum. All the animal experiments were performed in accordance with the regulations of the Animal Welfare Committee of the University of Amsterdam, which strives to minimize the use and suffering of experimental animals. Short-term (3 weeks) and long-term (3 months) kainate model rats of epilepsy Epilepsy was induced with kainate acid (KA) (Biovectra, Charlottetown, Canada) injections according to the protocol of Hellier et al (Hellier and Dudek, 1999), Wuarin and Dudek (Wuarin and Dudek, 1996). The rats were injected intraperitoneally with 10 mg.kg -1 KA dissolved in 0.05 M phosphate-buffered saline (PBS) (pH = 7.4). The animals were monitored throughout SE induction and seizure severity was assessed according to a modified Racine’s scale (Racine, 1972, Ben-Ari, 1985). Motor seizure activity was characterized as follows: class Ш, animals displayed forelimb clonus with a lordotic posture; class IV, animals reared with concomitant forelimb clonus; and class V, animals had a generalized clonic convulsion associated with loss of balance. When rats did not exhibit clear behavioural changes within one hour after injection, additional KA injections (5 mg.kg -1) were given every hour, until a clear change of behaviour (stage П/Ш seizures) was observed. The maximal cumulative dose varied between 10- 25 mg.kg -1. No termination of convulsions by ket/xyl was used to minimize risk of death. A Status Epilepticus (SE) was considered to have been established, if rats experienced more than two stage IV/V seizures within the first hours after injection. Control rats were injected intraperitoneally with 0.05 M PBS (pH = 7.4). Sugar water was supplied to all rats for 24

Chapter 5
66
hours after the KA treatment. The animals were killed three weeks (short-term kainate model) or three months (long-term kainate model) after SE. Cell preparation Each experimental day, a rat was decapitated. The brain was quickly removed and cooled immediately in an oxygenated PIPES buffered dissociation solution, containing (mM) 120 NaCl, 5 KCl, 1 MgCl2, 20 PIPES, 25 D-glucose; pH 7.0 (adjusted using NaOH). From a 300 µm thick transverse slice of the hippocampus, the CA1 area was dissected and cut into 0.5 mm thick slabs, which were incubated for 50 min at 32oC in oxygenated PIPES buffered dissociation solution containing 1 mg. ml -1 trypsin (type XI from bovine pancreas, Sigma). After washing, tissue pieces were kept in dissociation solution at room temperature (20oC) until use. Neurons were isolated by trituration of a tissue piece in 0.5 ml extracellular solution (see below) through a series of Pasteur pipettes with decreasing diameter and brought into a perfusion chamber of an inverted microscope (Nikon). Pyramidal shaped neurons with a clear apical dendrite, a bright and smooth appearance and no visible organelles were selected for electrophysiological measurements (Vreugdenhil et al., 1998). Current recording Voltage-dependent sodium currents were measured under whole-cell voltage-clamp conditions at room temperature (20oC), using patch pipettes of 2-3 MΩ resistance. Pipette solution contained (in mM) 110 CsF, 5 NaCl, 10 EGTA, 10 HEPES, 2 MgCl2, 25 TEACl, 5 MgATP, 0.1 NaGTP, 0.1 LEUPEPTIN. The pH was adjusted to 7.3 using CsOH. Neurons were continuously perfused with extracellular solution containing (in mM) 95 Choline-Cl, 20 NaCl, 10 HEPES, 2 CaCl2, 1 MgCl2, 5 KCl, 25 tetraethylammonium chloride (TEA-Cl), 5 4-aminopyridine (4-AP), 100 μM CdCl2 and 25 D-glucose; pH 7.4 (adjusted using HCl). To avoid space-clamp problems, the sodium gradient was reduced by equimolarly replacing part of the sodium in the extracellular solution by choline. After gigaseal formation and cell membrane rupturing, series resistance was compensated for 75%. The protocols were applied by an Atari (TT030) computer-controlled Axopatch 200A amplifier. The membrane capacitance was read from the amplifier dials as a measure of membrane surface. The holding membrane potential was set at –70 mV. The currents were sampled at a frequency of 5 kHz and analyzed using custom-made software. 2-4 min after the whole-cell configuration, the cell was moved into either control or drug-containing extracellular solution emitted by the application pipette using the Fast-Step Perfusion system (SF-77B, Warner Instrument Corporation, Hamden, USA). In each extracellular solution (control or drug-containing) protocols were performed twice, and the control extracellular solution was always applied before and after drug using. A small drift of the voltage dependence of steady-state inactivation and recovery from inactivation with time was executed when estimated the effects of drug (see results). The interval of protocols was always 2.5 minutes. Current traces were corrected off-line for linear leak using the leak conductance determined by a voltage step of -5 mV and +5 mV around the pre-pulse potential of -150 mV. Data analysis Only electrotonically compact cells that did not escape voltage-clamp and showed little rundown within the recording time were incorporated in the analysis. The currents were corrected off-line for linear non-specific leak and residual capacitive current transients.

Sodium current properties in the kainate model of epilepsy
67
Data are given as the mean ± standard error of the mean (S.E.M). Student’s t-test was used to compare groups of cells. P < 0.05 was considered to indicate a significant difference. Drugs and reagents carbamazepine (CBZ, Sigma) was dissolved in dimethylsulfoxide (DMSO, Sigma) to make a stock solution of 200 mM. Then it was diluted in extracellular solution to reach the final concentrations required (25, 75 and 100 µM). The final concentration of DMSO was always 0.05 %, which had no significant effects on sodium currents. RESULTS
We did experiments using rats three-week (short-term) and three-month (long-term) after kainate injection. All the results presented here were from long-term epileptic rats, except those we stated were from short-term epileptic rats. Functional changes in sodium channels after kainate-induced epilepsy 1. Voltage-dependent activation and steady-state inactivation shifted to the negative potentials
We investigated the sodium channel properties on voltage-dependent activation
and inactivation after epilepsy. Sodium currents were activated by depolarization (25 ms) to levels between -70 mV and + 10 mV from a prepulse potential of -150 mV (Fig 1A). The depolarization activated a fast, transient inward sodium current that first increased in amplitude as the channels open and at higher potentials decreased due to the reduced driving force. The current activated at potentials >-55 mV for control (>-60 mV for epileptic) CA1neuros, and current amplitude increased with membrane potential up to -15 mV.
We determined the peak amplitude of the current for each step and constructed a current-voltage relation. This I-V-curve was fitted to the Goldman-Hodgkin-Katz current equation (Hille, 2001) using a Boltzmann function to describe the sodium permeability as a function of membrane voltage (V):
)exp(1
)exp()][][(
)exp(1
1)( maxV
VNaNa
VVV
VgVI out
in
c
h α
α
−−
−−++
×−
+××=
Eq 1
With α = F/RT and gmax = αF [Na+]outp0 where p0 is the maximal permeability, F is the Faraday constant, R is the gas constant and T represents the absolute temperature. The maximal conductance of the current is gmax (nS), while the potential of half-maximal activation (Vh) and the slope parameter (Vc) characterize its voltage dependence.

Chapter 5
68
The voltage dependence of steady-state inactivation of the sodium current was measured by varying a 500-ms hyperpolarizing pre-pulse from -150 to -35 mV followed by a 25-ms depolarization to -25 mV (Fig 1B). The peak amplitude of the current (I) evoked at -25 mV was normalized to Imax and plotted as a function of pre-pulse potential (V). The curve was fitted by a Boltzmann equation:
)exp(1
I)( m
c
h
ax
VVV
VI−
+= Eq 2
Where Vh is the potential of half-maximal inactivation and Vc is proportional to the slope of the curve.
The sodium channel conductance (gmax) in CA1 neurons decreased after epilepsy, from 114.31 ± 9.93 nS (n = 16) to 88.63 ± 7.26 nS (n = 20), p < 0.05 (Tab 1). In order to exclude the interpretation of cell surface (indicated by membrane capacitance Cm), we calculated the sodium current density (gmax/Cm ) and it was also smaller in neurons after epilepsy, from 16.78 ± 1.29 nS.pF-1 (n = 16) to 12.38 ± 1.09 nS.pF-1 (n = 20), p < 0.05 (Table 1).
Both voltage-dependence of activation and steady-state inactivation shifted to more hyperpolarized direction without changing the slopes after epilepsy, with Vh of activation -43.07 ± 1.20 mV (n = 20; control rat: -39.67 ± 0.97 mV, n = 16; t-test p < 0.05) and Vh of inactivation -69.80 ± 1.41 mV (n = 20; control rat: -66.44 ± 1.04 mV, n = 16; t-test p < 0.05) (Fig 1C and Table 1).
Table.1.Sodium current properties of activation and steady-state inactivation in rat CA1 neurons after kainate-induced epilepsy. bP<0.05 vs control. Error bars indicate S.E.M.
Activation Inactivation Vc Vh(mV) gmax(nS) gmax/Cm(nS.pF-1) Vc Vh(mV) Control (n = 16) 6.4±0.3 -39.6±1.0 114.3±9.9 16.7±1.3 -6.5±0.2 -66.4±1.0
Epilepsy (n = 20) 6.2±0.3 -43.1±1.2b 88.6±7.3b 12.4±1.1b -6.4±0.2 -69.8±1.4b
The voltage-dependent properties of activation and steady-state inactivation from
short-term epilepsy group did not differ from control group (data not shown).

Sodium current properties in the kainate model of epilepsy
69
Figure 1.Voltage-dependence of sodium channel activation and steady-state inactivation in rat CA1 neurons after kainate-induced epilepsy. (A) example of voltage-activated sodium currents in a CA1 neuron. Sodium currents were activated by 25 ms depolarizing voltage step ranging from -70 mV to +10 mV, following a 500 ms hyperpolarizing pre-pulse to -150 mV; (B) example of voltage-inactivated sodium currents in a CA1 neuron. Sodium currents were evoked with a step depolarization to -25 mV for 25 ms following 500 ms hyperpolarizing pre-pulses between -150 mV and -35 mV; (C) The normalized conductance of activation (right curves) and steady-state inactivation (left curves) for both the control (n=16) and epilepsy (n=20) groups were plotted as a function of membrane potential. The data points were fitted with the Goldman-Hodgkin-Katz current equation (Eqn 1, activation) and the Boltzmann function (Eqn 2, steady-state inactivation) to give the values of Vha (the voltage of half-maximal activation), Vhi (the voltage of half-maximal inactivation) and Vc (the slope parameter). Error bars indicate S.E.M.
2. The window current was increased
In the small voltage range where the activation and inactivation curves of the fast
sodium current overlap, a persistent window current exists because current can be activated that will not completely inactivate (Johnston, 1995). The overlap was illustrated in Fig 1 (a). We calculated the absolute window current from the product of the activation
0
0.2
0.4
0.6
0.8
1
1.2
0
0.2
0.4
0.6
0.8
1
1.2
-120 -100 -80 -60 -40 -20
Con.(Inact.)Epi.(Inact.)Con(Act.)Epi(Act.)
Frac
tion
avai
labl
e
Voltage(mV)
Inactivation Activation
Fraction open
5 ms1 nA
-70 mV -70 mV
10 mV
-150 mV,500ms
25 ms5 ms
1 nA
-35 mV
-70 mV
-150 mV 500 ms
-25 mV 25 ms
-70 mV
A B
C

Chapter 5
70
and inactivation function (Eq 1 and Eq 2) using the mean parameters given in Tab 1. After kainate-induced epilepsy, the maximal window current amplitude increased from 6 pA to 9 pA, and it shifted to the hyperpolarizing direction from -46 mV to -52 mV (Fig 2).
Figure 2.Window current in rat CA1 neurons after kainate-induced epilepsy. The absolute window current for the control rats (n=16) and epileptic rats (n=20) was constructed as the product of the fitted activation and inactivation function (Eqn 1,2) using the mean values of the parameters (Vc, Vh, and gmax). The maximal amplitude of the window current was larger in the CA1 neurons after epilepsy. The voltage at which maximal amplitude occurred shifted towards more hyperpolarized potentials in CA1 neurons after epilepsy.
3. Recovery from inactivation was slower
The time course of recovery from inactivation was determined using a double-
pulse protocol (Fig 3A). The interval ∆t (during which the current was allowed to recover) between two 25-ms depolarization steps was varied between 1 and 200 ms. The recovery time constant was determined at membrane voltages of –70, –80 and –90 mV. The amplitude of the sodium current activated by the second pulse was plotted as a function of ∆t and fitted with a single-exponential function to give the time constant of recovery from inactivation (Tau) (Fig 3B).
R (∆t) = 1 – exp ⎟⎠⎞
⎜⎝⎛ Δ−
Taut Eq 3
Recovery from inactivation was faster at more hyperpolarized membrane
potentials, and the recovery was slower after kainate -induced epilepsy, which reached significance at membrane potential -80 and -90 mV (p < 0.05, Fig 3C a). Three-week after kainate injection, the recovery was not changed (Fig 3C b).
-0.01
-0.008
-0.006
-0.004
-0.002
0
ControlEpilepsy
-80 -70 -60 -50 -40 -30 -20 -10 0
Win
dow
cur
rent
(nA
)
Voltage (mV)

Sodium current properties in the kainate model of epilepsy
71
Figure 3. Voltage-dependent properties of recovery from the inactivation of sodium currents in rat CA1 neurons after kainate-induced epilepsy. The time course of recovery from inactivation was determined by a double-pulse protocol (see inset in A). The variable interval (∆t=1, 2, 5, 10, 20, 50, 100, or 200 ms, during which the current was allowed to recover) between two 25-ms depolarizing voltage steps to -25 mV was used to determine the recovery from inactivation at the membrane voltages -70 mV, -80 mV, and -90 mV. (A) 3 examples of sodium currents activated by 2 double pulses applied with different time intervals are shown: (i) ∆t=100 ms, (ii) ∆t=10 ms and (iii) ∆t=2 ms; (B) Amplitude of the sodium current activated by the second pulse is plotted as a function of ∆t and fitted with a single exponential function to give the time constant of recovery from inactivation (Tau, 1 example at membrane potential -80 mV); (C) Tau values of the control group (n=16) and epilepsy group ((n=20) at membrane potentials -70 mV (26.0±1.4 and 30.0±1.4), -80 mV (13.7±0.8 and 17.3±1.3) and -90 mV (8.1± 0.5 and 10.3±0.9) 3 months after kainate injection; (D) Tau values of the control group (n=11) and epilepsy group (n=12) at membrane potentials -70 mV (25.7±1.5 and 29.2±3.5), -80 mV (14.7±1.4 and 15.2±1.8) and -90 mV (8.4±0.7 and 8.5±0.9) 3 weeks after kainite injection. The recovery was voltage-dependent and was slower after long-term epilepsy (ANOVA P<0.05). Error bars indicate S.E.M.
0
5
10
15
20
25
30
35
-70 -80 -90
ControlEpilepsy
Membrane potential (mV)
Tau(
ms)
three-month after kainate injection
i
ii
iii40 ms
2 nA
-70mV -70mV
-25mV 25ms 25ms
Δt = 1~200ms
- 70 mV
- 80 mV
- 90 mV -2.5
-2.0
-1.5
-1.0
-0.5
0.00 50 100 150 200
Interval (ms)
Am
plitu
de (n
A)
0
5
10
15
20
25
30
35
-70 -80 -90
ControlEpilepsy
Membrane potential (mV)
Tau(
ms)
three-week after kainate injection
A B
C D

Chapter 5
72
Sodium channel inhibition by CBZ after kainate-induced epilepsy 1. The voltage shift of the steady-state inactivation by CBZ slightly decreased
The protocol was described in Fig 1C. CBZ concentration-dependently shifted the
sodium channel inactivation curves to more hyperpolarized potentials in rat CA1 neurons after kainate -induced epilepsy (Fig 4A). But in comparison with control group, the absolute shift of the midpoint of the steady-state inactivation curves (∆Vhi, which is the difference between control and presence of CBZ. In this way the small drift with time in voltage dependence of steady-state inactivation was also corrected) by CBZ in epilepsy group was slightly smaller, which reached significance at 100 μM (p < 0.05, Fig 4B). The similar shift by CBZ was also found in rats three-week after kainate injection, but no significant difference between control and epilepsy groups (Fig 4C).
2. The time constant of recovery from inactivation by CBZ was not significantly changed
The time course of recovery from inactivation was determined by the same
double-pulse protocol as described in Fig 3A. CBZ concentration dependently slowed down the recovery from inactivation at each membrane potential, represented by the increased time constant (Tau) of recovery from inactivation in the presence of different CBZ concentrations (Fig 5). The Tau was bigger with higher concentration of CBZ generally, and it was not changed significantly after kainate-induced epilepsy (Fig 5). The binding rate constant of CBZ onto the fast inactivated sodium channels in rat CA1 neurons was not changed significantly after kainate-induced epilepsy
Experiments were performed to determine the binding rate at which CBZ binds to the inactivated sodium channels, and it was assessed by a voltage protocol described in Fig 6A inset (Kuo and Lu, 1997). With such a protocol the channels were exposed to a depolarizing voltage step (to –40 mV) of different durations (30-2500 ms). Longer depolarizing voltage steps allow more channels to enter the inactivated state and due to the much higher affinity of CBZ to this state, more channels will be blocked. Fig 6A demonstrates that with increasing pre-pulse durations more sodium current got blocked in the presence of 75 μM CBZ. By subtracting the control current (no CBZ present) from the current in the presence of CBZ at each pre-pulse duration, the CBZ-blocked current was obtained. This procedure eliminates the contamination by slowly inactivating currents. Expressing the blocked current as function of the pre-pulse duration shows the development of CBZ block, a relationship that can be fitted with a mono-exponential function and the resulting Tau value describes the time course of development of block for each CBZ concentration (Fig 6B). The 1/Tau value at each CBZ concentration yields the binding rates and these increased linearly with higher CBZ concentrations for control and epilepsy neurons (Fig 6C). The slopes of these linear relationships give the binding rate constant of CBZ for sodium channels of control and epilepsy CA1 neurons. These values were 31.3 ± 2.6 × 103 M-1s-1 for control group (n=11) and 28.9 ± 4.7 × 103 M-1s-1 for epilepsy group (n=16), without significant difference between them. This finding

Sodium current properties in the kainate model of epilepsy
73
indicates that the binding of CBZ to the inactivated sodium channels is similar for control and epilepsy groups.
Figure 4.Voltage shift of the sodium channel steady-state inactivation by CBZ in rat CA1 neurons after kainate-induced epilepsy. (A) concentration-dependent shift of inactivation curves by CBZ in epileptic rats 3 months after kainate injection (n=19–22). The cell was held at -70 mV and stepped to the inactivating pre-pulse from -150 mV to -35 mV for 500 ms. The channels which remained available after each inactivating pre-pulse were assessed by the peak currents during the following 25 ms short test pulse at -25 mV. The fraction available was defined as the normalized peak current (relative to the current evoked with an inactivating pre-pulse at -150 mV) and was plotted against the voltage of the inactivating pre-pulse. Four sets of data from right to left were obtained from the control and 25 μM, 75 μM, and 100 μM CBZ. The lines were fitted with a Boltzmann function (Eqn 2) with Vh values (in mV) of -68.8, -77.8, -83.4, and -86.3. Vc values of 6.5, 7.0, 7.4, 7.6 for the control and 25 μM, 75 μM, 100 μM CBZ, respectively; (B) The ∆Vhi shifted by CBZ in the rats 3 months after kainate injection. The significance was found at 100 μM CBZ (t-test P<0.05) between the control (n=12–19) and epilepsy (n=18–20) groups; (C) The ∆Vhi shifted by CBZ in the rats 3 weeks after kainate injection (n=5–9 for the control group and n=10–12 for the epilepsy group). The ∆Vhi was determined in each cell by the difference of Vhi between the control and presence of CBZ, and was plotted against the concentrations of CBZ. The curves were fitted with a logistic function ∆Vhimax/(1+EC50/[D]), where ∆Vhimax is the maximal shift of Vhi , EC50 is the concentration which causes half maximal ∆Vhi and D is the applied concentration of CBZ. Error bars
0
2
4
6
8
10
12
0 20 40 60 80 100 120
ControlEpilepsy
CBZ (μM)
Δ V
hi (m
V)
Three-month after kainate injection
*(*p < 0.05 vs control)
0
0.2
0.4
0.6
0.8
1
-120 -100 -80 -60 -40
Three-months after kainate injection
0μM25μM75μM100μM
Voltage(mV)
Frac
tion
avai
labl
e
Epilepsy group
0
2
4
6
8
10
12
0 20 40 60 80 100 120
ControlEpilepsy
CBZ (μM)
Δ V
hi (m
V)
Three-week after kainate injection
A
B C

Chapter 5
74
indicate S.E.M. The estimated values of EC50 and ∆Vhimax from the curve fittings for each group are as follows: 3 months after kainate injection: control group: EC50 140 μM, ∆Vhimax 20 mV; and epilepsy group: EC50 103 μM, ∆Vhimax 16 mV. Three weeks after kainate injection: control group: EC50 126 μM, ∆Vhimax 23 mV; epilepsy group: EC50 147 μM, ∆Vhimax 24 mV.
Figure 5. CBZ slows down the recovery from inactivation at different membrane potentials of sodium currents in rat CA1 neurons after kainate-induced epilepsy. The same voltage step protocol was used as in Fig. 3. The Tau values are expressed against the CBZ concentrations 0, 25, 75, and 100 μM, at membrane potential of -70 mV (A; n=7–15 for the control group and n=13–18 for the epilepsy group), -80 mV (B; n=10–17 for the control group and n=19–21 for the epilepsy group) and -90 mV (C; n=11–18 for the control group and n=15–21 for the epilepsy group). The effects of CBZ were concentration- and voltage-dependent (ANOVA P<0.01), which were not changed significantly after kainate-induced epilepsy. Error bars indicate S.E.M.
0
10
20
30
40
50
60
0 23 76 100
-80mV
ControlEpilepsy
CBZ(μM)
Tau(
ms)
long-term kainate
n = 17, 14, 13, 10n = 21, 16, 19, 19
0
10
20
30
40
50
0 25 75 100
-70mV
ControlEpilepsy
CBZ(μM)
Tau
(ms)
long-term kainate
n = 15, 12, 11, 7n = 18, 13, 16, 16
0
10
20
30
40
50
60
0 23 76 100
-90mV
ControlEpilepsy
CBZ(μM)
Tau(
ms)
long-term kainate
n = 18, 15, 14, 11n = 21, 15, 19, 19
A
B C

Sodium current properties in the kainate model of epilepsy
75
Figure 6. Binding rates of CBZ onto the fast-inactivated sodium channels in rat CA1 neurons after kainate-induced epilepsy. Cells were held at -150 mV and pre-pulsed to -40 mV with increasing time duration (∆t=30–2500 ms). After a recovery gap potential at -150 mV for 5 ms (allowing most of the drug-free inactivated sodium channels to recover), the available current was determined with a 5 ms testing potential to -25 mV. The whole protocol was repeated every 5 s. Examples of sodium currents at the testing potential in 1 cell with 30, 250, and 2500 ms pre-pulse time durations are shown in A (control) and B (75 μM CBZ); C; The blocked current was determined by subtracting the control current (measured in the absence of CBZ) from the current recorded in the presence of CBZ and was plotted against the time duration of the pre-pulse ∆t. The data points were fitted with a monoexponential equation to determine the time constant (Tau) for the development of the block in the presence of 25, 75, and 100 μM CBZ; D; The binding rates (1/Tau, s-1) for both the control and epilepsy groups are plotted against the CBZ concentration. The slopes of the linear regression give the binding rate constants for CBZ, which was 31.3±2.6 M-1s-1 for the control group (n=11) and 28.9±4.7 M-1s-1 for the epilepsy group (n=16). Error bars indicate S.E.M.
DISCUSSION
In this present study we characterized the properties of the voltage-gated sodium current, and its modulation by CBZ in acutely dissociated hippocampal CA1 neurons from rats three-month and three-week after kainate injection; additionally the binding rate constant of CBZ onto the inactivated channels. Our main findings were the enlarged and
CBZ
5 ms1 nA2500 ms
30 ms
250 ms
Control
5 ms1 nA
2500 ms
30 ms250 ms
-150mV -150mV-150mV
-40mV-25mV
5ms
5ms
Δt = 30- 2500 ms
A B
0
0.5
1
1.5
2
2.5
0 0.5 1 1.5 2 2.5 3
25μM75μM100μM
Blo
cked
cur
rent
(nA
)
Prepulse duration (s)
0
1
2
3
4
5
6
7
0 20 40 60 80 100 120
ControlEpilepsybi
ndin
g ra
te (s
ec-1
)
CBZ(μM)
C D

Chapter 5
76
negative voltage shifted window current that was mainly caused by the negative shift of the voltage-dependent activation; as well as the increased recovery time constant from inactivation after epilepsy. The efficacy of CBZ and its binding rate to the channels did not change markedly. For the short-term (three-week) epileptic rats, we could not detect any differences on sodium current between the control and epilepsy groups. Epilepsy model induced by kainate injection
All the epileptic rats (three-month and three-week after kainate injection) in our
study were wild and showed typical behaviors of epileptic seizures compared with control rats. In hippocampal CA1 area of epileptic rats, there was a significant cell loss found by Gorter et al (Gorter et al., 2003). Functional changes in sodium channels after kainate-induced epilepsy
The overlap of the activation and the inactivation curves gives rise to a voltage-
window in which a persistent current exists, because activation occurs at a voltage where the current will not completely inactivate. When it is of sufficient amplitude, it is important for cellular excitability (Johnston, 1995). In our study, after epilepsy the window current was larger due to the more hyperpolarizing voltage shift of activation than inactivation, and the voltage at which the maximal window current amplitude occurred shifted 6 mV to the negative direction. That means it will drive the membrane voltage closer to the firing threshold, thereby lowering the threshold for epileptic activity. On the other hand, our data showed that the neuron excitability could also be attenuated after epilepsy due to the slowed recovery from inactivation and decreased membrane current density. The slowed recovery from inactivation could be accounted for by the negative voltage shift of activation and inactivation, which could make the inactivated channels accumulated so as to enlarge the refractory period. Regard to the lower membrane current density, our explanation is that it could be a sort of compensation mechanism or the cells we recorded were from surviving cells after seizures. Because we did see the significant cell loss in cell suspension compared with control. We did not detect any differences of channel properties between epilepsy and control groups in short-term epileptic rats. So the sodium channel properties could change secondary to long-term epileptic seizures. Sodium channel inhibition by CBZ after kainate-induced epilepsy
CBZ did display similar sodium channel inhibition on long-term and short-term
epileptic rats as it does usually: shifted the voltage-dependence of inactivation to more negative potentials, with the similar ∆Vhimax and EC50; concentration-dependently slowed down the recovery from inactivation. The only difference we found was at 100 μM CBZ ∆Vhi was reduced after long-term epilepsy. Because 100 μM was much bigger than CBZ’s therapeutically relevant concentration range in human brain (3 – 15 µM (Altafullah et al., 1989)), so we assume that the long-term epileptic seizures might not be the key factor which could cause pharmacoresistance of CBZ in clinical epilepsy treatment, at least conclusion from this epilepsy model study. In additional, CBZ bound

Sodium current properties in the kainate model of epilepsy
77
to the inactivated channels at the similar speed after epilepsy compared with control, which also supported our conclusion.
The possible mechanism for the functional changes of sodium channel associated with epilepsy and the slightly reduced response of channels to CBZ modulation could be as follows: 1) The changed expression of sodium channel subtypes. Even though we do not have direct proof for this suggestion in our study, we can not exclude its involvement. Bartolomei et al (Bartolomei et al., 1997) reported that following kainic acid-induced seizures there was a marked increase in type Ш mRNA expression and a modest increase in type П mRNA expression in rat hippocampus. Furthermore, in human epileptic hippocampus, a significant down-regulation of type П mRNA and a significant up-regulation of type Ш mRNA were observed (Whitaker et al., 2001a). Taken together, there is a higher expression of type Ш mRNA than type П mRNA of sodium channels in hippocampus after epilepsy. In our other study of sodium channel subtypes expressed in HEK-cell and CBZ, we did detect the different pharmacological profiles of CBZ between type П and type Ш, and this observation supports our suggestion in the present study. 2) The changed expression of sodium channel auxiliary β subunits. In a 72 hours observation after kainate injection, the β2 mRNA expression was seen increased transiently in the first 1 hour, and then decreased significantly in hippocampus (Gastaldi et al., 1998). This variation might play a role in cellular excitability changes occurring in the course of seizures, because expression of β2 subunit with neuronal α subunits in oocytes increased current amplitude, modulated gating and increased membrane capacitance (Isom et al., 1995). 3) Mutations in genes encoding sodium channel α or β subunits. In generalized epilepsy with febrile seizure plus, mutations in three genes coding for α (SCN1A, SCN2A) or β1 subunits (SCN1B) have been identified (Wallace et al., 1998, Escayg et al., 2000, Sugawara et al., 2001). In the functional study of mutations in SCN1A by heterologous expression with its known accessory subunits β1 and β2 in cultured mammalian cells, SCN1A mutations could alter channel inactivation, resulting in persistent inward sodium current, which could likely enhance excitability of neuronal membranes by causing prolonged membrane depolarization (Lossin et al., 2002). 4) Sodium channel modulation by G-protein-coupled pathway. Sodium channel in hippocampal neurons could be modulated by guanine nucleotide binding protein (G protein)-coupled pathways under conditions of whole-cell voltage clamp (Ma et al., 1994). Activation of G protein increased the sodium current amplitude, caused by negative shift in the voltage dependence of both activation and inactivation (Ma et al., 1994). Other functional studies on sodium channel after epilepsy
In long-term epileptic rats induced by pilocarpine, sodium channel window
current in dentate granule cells increased due to the positive shift of voltage-dependent inactivation and the negative shift of voltage-dependent activation, and no changes were found in recovery from inactivation (Ellerkmann et al., 2003); Furthermore CBZ completely lost its effects on slowing down the fast recovery from inactivation, so failed to reduce the sodium current availability during high-frequency action potential series (Remy et al., 2003a). In another pilocarpine model, epileptic rats responded to CBZ treatment at very high concentrations (Leite and Cavalheiro, 1995). Our present results

Chapter 5
78
are not consistent with these findings, which may be related to the different induction protocols leading to chronic epilepsy, as well as the different cell types detected. Because the processes underlying epileptogenesis even differ among post-status epilepsy models, like pilocarpine and kainate models, the markedly different antiepileptogenic effects of drugs could exist between models (Loscher, 2002).
Our conclusion is the properties of sodium channel in acutely dissociated hippocampal neurons could change secondary to the chronic epilepsy processes. But the alternation is not enough to destroy the effective targeting of CBZ, so it is not the key factor for pharmacoresistance.

CHAPTER 6
Carbamazepine and topiramate modulation of transient and persistent
sodium currents studied in HEK293 cells expressing the NaV1.3 α-subunit
Guangchun SUN, Taco R. WERKMAN, Arne BATTEFELD, Jeffrey J.
CLARE and Wytse J. WADMAN
Epilepsia 48 (4): 774–782 (2007)

Chapter 6
80
ABSTRACT
Summary: Purpose: The transient and the persistent Na+ current play a distinct role in neuronal excitability. Several antiepileptic drugs (AEDs) modulate the transient Na+ current and block the persistent Na+ current; both effects contribute to their antiepileptic properties. The interactions of the AEDs carbamazepine (CBZ) and topiramate (TPM) with the persistent and transient Na+ current were investigated. Methods: HEK293 cells stably expressing the α-subunit of the Na+ channel NaV1.3 were used to record Na+ currents under voltage-clamp by using the patch-clamp technique in whole-cell configuration and to investigate the effects of CBZ and TPM. Results: The persistent Na+ current was present in all cells and constituted 10.3 ± 3.8% of the total current. CBZ partially blocked the persistent Na+ current in a concentration-dependent manner [median effective concentration (EC50), 16 ± 4 μM]. CBZ also shifted the steady-state inactivation of the transient Na+ current to negative potentials (EC50, 14 ± 11 μM). TPM partially blocked the persistent Na+ current with a much higher affinity (EC50, 61 ± 37 nM) than it affected the steady-state inactivation of the transient Na+ current (EC50, 3.2 ± 1.8 μM). For the latter effect, TPM was at most half as effective as CBZ. Conclusions: The persistent Na+ current flowing through the α-subunit of the NaV1.3 channel is partially blocked by CBZ at about the same therapeutic concentrations at which it modulates the transient Na+ current, adding a distinct aspect to its anticonvulsant profile. The TPM-induced partial block of the persistent Na+ current, already effective at low concentrations, could be the dominant action of this drug on the Na+ current. INTRODUCTION
Sodium currents are responsible for the upstroke of the action potential, and they play a crucial role in determining neuronal excitability. Many neurons possess two types of sodium current: the fast transient Na+ current of the classic Hodgkin and Huxley type and a non-inactivating (persistent) voltage-dependent Na+ current (Taylor, 1993, Crill, 1996). The molecular basis of the persistent Na+ current is not completely clear; it could either be a modal change in gating of the conventional Na+ channel, or alternatively, it could be generated by an unusual Na+-channel subtype that does not inactivate (Alzheimer et al., 1993, Crill, 1996, Ogata and Ohishi, 2002). A recent study of Mantegazza et al. (2005) implicated G-protein βγ-subunits as modulators of the persistent current, without defining the functional conditions where this becomes relevant (Mantegazza et al., 2005). In mammalian hippocampal CA1 neurons, the persistent Na+ current activates at potentials close to resting membrane potential, and because it hardly inactivates, it could play a role in repetitive firing of action potentials caused by prolonged depolarization (French et al., 1990). The persistent Na+ current could thus play a role in brain disorders like hypoxia (Hammarstrom and Gage, 2002) and epilepsy (Segal, 2002). The persistent Na+ current was found increased in neurons of e.g. the entorhinal cortex and hippocampus of epileptic animals and epilepsy patients (Kearney et al., 2001, Lossin et al., 2002, Agrawal et al., 2003, Spampanato et al., 2004, Vreugdenhil et al., 2004). Furthermore, the amplitude of the persistent Na+ current was extremely large in hippocampal CA1 neurons from drug-resistant epileptic patients, up to 53% of the total Na+ current amplitude (Vreugdenhil et al., 2004).

CBZ and TPM modulation of sodium current
81
A broad range of anti-epileptic drugs (AEDs) is able to block the persistent Na+ current at therapeutically relevant doses, examples are phenytoin (Chao and Alzheimer, 1995, Segal and Douglas, 1997), valproic acid (VPA) (Taverna et al., 1998), lamotrigine (LTG) (Spadoni et al., 2002), topiramate (TPM) (Taverna et al., 1999) and ethosuximide (ESM) (Leresche et al., 1998). However, for none of these drugs blocking the persistent Na+ current is considered the dominant mode of action. For the most commonly used AED carbamazepine (CBZ), which predominantly interacts with the fast Na+ channel, information about its interaction with the persistent Na+ current is lacking.
The fast inactivating Na+ channel is the molecular target for many of the most widely used AEDs, including CBZ (Ragsdale and Avoli, 1998). CBZ is a first-line drug in the treatment of most forms of epilepsy, and it is also used in trigeminal neuralgia and bipolar depression (Bertilsson and Tomson, 1986). CBZ produces voltage- and frequency-dependent block of Na+ channels, because it binds to the inactivated channels with higher affinity than to channels in the open or resting state (Macdonald and Kelly, 1995, Kuo, 1998). The stabilization of the inactive state of the Na+ channel by CBZ in a voltage-dependent fashion slows down the recovery from inactivation, it shifts the steady-state inactivation curve to more negative voltages and it prevents sustained high-frequency repetitive firing of action potentials evoked from reduced membrane potentials (Wadman et al., 2005). The AED TPM (Perucca, 1997) also affects voltage-dependent Na+ current (Zona et al., 1997, Taverna et al., 1999, DeLorenzo et al., 2000), although Na+ channel interaction is, most likely, not the only target underlying the anti-epileptic properties of TPM (Shank et al., 2000). In addition, it has been shown that TPM blocks the persistent Na+ current in neocortical neurons at relatively low concentrations (Taverna et al., 1999).
The expression of the pore forming Na+ channel α-subunit NaV1.3 was found to be up-regulated in hippocampal neurons isolated from epileptic human and rat brain (Bartolomei et al., 1997, Aronica et al., 2001, Whitaker et al., 2001b). When this Na+ channel subtype is expressed in HEK293 cells, it conducts Na+ current with a persistent component (Chen et al., 2000). Therefore the persistent component of the Na+ current carried by this channel subtype observed in the neurons from epileptic tissues, may well contribute to the deviant electrical activity in those tissues.
The HEK293 expression system provides an excellent tool to compare the effects of AEDs on the transient and persistent component generated by the same Na+ channel. In the present study we investigated the effects of the AEDs CBZ and TPM and found that both the transient and persistent component of the NaV1.3 Na+ channel are affected by therapeutically relevant concentrations of CBZ, in addition the blocking effects of TPM were more pronounced on the persistent Na+ current. METHODS Stably transfected HEK293 cell line
All experiments were performed in a HEK293 cell line that stably expressed the NaV1.3 α-subunit. It was generated using the pCIN-hIII vector (Chen et al., 2000) using the method described by Burbidge et al. (Burbidge et al., 2002).

Chapter 6
82
Cell culture HEK293 cells stably expressing the human NaV1.3 subunit were cultured in
minimum essential medium, containing 10% fetal calf serum, 1% L-glutamine (200 mM) and 1% penicillin/streptomycin (all reagents from Gibco). Cells were grown at 37 oC in a 5% CO2 atmosphere with 95% humidity. One to two days prior to electrophysiological recordings, the cells were plated on glass coverslips. Whole-cell voltage clamp recordings
Cells grown on glass coverslips were placed into a recording chamber with 0.5 ml
extracellular solution which contained (in mM): NaCl 140, KCl 5, CaCl2 2, MgCl2 1, HEPES 10, and glucose 11. The pH was adjusted to 7.4. The patch electrode had a resistance of 2-3 MΩ when filled with a pipette solution consisting of (in mM): CsCl 135, EGTA 10, HEPES 10, NaCl 5, MgCl2 2, Mg-ATP 2, Na-GTP 1. The pH was adjusted to 7.3. Voltage-dependent Na+ currents were measured under whole-cell voltage clamp conditions at room temperature (20-22oC). After the whole-cell configuration was established, the cell was perfused with extracellular solution for 5 minutes during which the Na+ current amplitudes reached a stable level. Next it was bathed in control or drug-containing extracellular solution ejected from the application pipette using the Fast-Step Perfusion system (SF-77B, Warner Instrument Corporation, Hamden, USA). Series resistance was compensated for at least 75%. Membrane capacitance, as a measure of membrane surface, was read from the amplifier dials. An Atari (TT030) computer-controlled Axopatch 200A amplifier applied the voltage-clamp protocols; the minimum interval between protocols was one second. Membrane potential was held at –70 mV. The currents were sampled at a frequency of 5 kHz and analyzed using custom-made software. Each series of protocols was performed twice in control solution, twice in drug-containing solution (CBZ or TPM) and again twice in control solution as wash. In several cases it was possible to test more than one concentration per cell (with a maximum of four). The interval between each series of protocols was fixed at 1 minute. We confirmed the block of the current by TTX (<0.5 M) as described by for these cell by Chen et al. (Chen et al., 2000) Data analysis
HEK cells were electrotonically compact and rarely escaped voltage clamp. Only
cells that showed little rundown during the recording were incorporated in the analysis. The currents were corrected off-line for linear non-specific leak and residual capacitive current transients. Data are given as the mean ± standard error of the mean (S.E.M). Unless otherwise mentioned, Student’s t-test was used to compare the parameters of groups of n cells. P < 0.05 was considered to indicate a significant difference. Drugs and reagents
CBZ (Sigma) was dissolved in dimethylsulfoxide (DMSO, Sigma) to make a stock solution of 200 mM. This solution was diluted in extracellular solution to reach the

CBZ and TPM modulation of sodium current
83
final concentrations of 1, 10, 50 and 100 µM. The final concentration of DMSO for CBZ was always 0.05 %, which was tested to have no effects on Na+ currents. TPM (Sigma) stock solutions (20 mM) were made in H2O and diluted in extracellular solution to reach the final concentration.
RESULTS Basic properties of transient and persistent Na+ current carried by the NaV1.3 α-subunit.
Na+ currents were activated by 100-ms depolarization steps to levels between –70 mV and +10 mV from a prepulse potential of –120 mV (Fig. 1A; the voltage protocol is given as an inset). The depolarization activated an inward Na+ current with two components: a fast, transient current and a persistent current. The peak amplitude of the transient current was reached within a few milliseconds; it was voltage dependent and increased with larger depolarization; it reached its maximum value around –10 mV, and gradually decreased for depolarization to higher voltages because of the reduction in driving force (Fig. 1A). The peak amplitude of the transient current and the amplitude of the persistent current, measured at the end of the 100-ms depolarization, were determined for each voltage step and used to construct the current–voltage (I-V) relation for both current components (Fig. 1B). Ramp protocols were used only for inspection purposes, but given the impossibility of separating window current from persistent current (see later) with ramps, we analyzed all currents by using voltage-step protocols of 100-ms depolarization, which is very long in respect to the inactivation time of the fast transient Na+ current.
The observed I-V relationship is well fitted by the Goldman-Hodgkin-Katz current equation (Hille, 2001) that relates membrane current (I) to membrane voltage (V) under asymmetric ionic conditions:
)exp(1
)exp(][][
exp1
1)( max V
VNaNa
cVVhV
VgVI out
in
α
α
−−
−−×
−+
××=+
+
with α = F/RT (1)
Where F is the Faraday constant, R is the gas constant and T is the absolute temperature. The maximal conductance of the current (gmax) is related to the maximal permeability (P0) via the relation gmax = P0αF [Na+]out. The voltage dependence of the conductance is well described with a Boltzmann function characterized by the voltage of half-maximal activation (Vh) and a slope parameter (Vc).
The persistent current was present in all cells, and its amplitude constituted 10.3 ± 3.8% (n = 8) of the total current. The mean gmax value for the persistent current was 30.8 ± 0.6 nS, and for the transient Na+ current it was 280 ± 10 nS (n = 8). The voltage-dependence of the two Na+ current components was determined for each cell, which resulted in the mean values of Vh = –13.6 ± 0.4 mV and Vc = –4.1 ± 0.2 mV for the persistent current and Vh = –18.7 ± 0.7 mV and Vc = –5.1 ± 0.5 mV for the transient

Chapter 6
84
current (n = 8). The activation of the persistent current, as defined by Vh, was 5.1 mV more depolarized than the one of the transient current (p < 0.01; Fig. 1B).
The better to judge the shape of the I-V curve, we constructed a normalized mean by scaling each I-V curve to the mean by using a multiplicative scale factor minimizing the least-square error. The same factors were used to scale the persistent current. In this way, the mean amplitude of the I-V relation and the relation between fast and persistent current were preserved, but the errors give a better indication of the shape of the curve instead of representing the variation in absolute amplitude (Fig. 1B). The fitted continuous curve in Fig. 1B is the GHK fit to the mean values of the I-V curves; the obtained parameters (Vh, Vc, gmax) were, however, not significant different from the mean of the parameters obtained from the fits to all single traces, as given earlier. The persistent Na+ current versus the window current
The transient Na+ current can generate a window current arising from overlap of
the steady-state inactivation and activation functions over the voltage range where the activated current is not completely inactivated (Patlak, 1991, Johnston, 1995). To exclude the possibility that the persistent Na+ current is carried mainly by a window current, we determined the amplitude and I-V relation of the window current. For this, we constructed the steady-state inactivation relation of the transient Na+ current by evoking the current with a step potential to –10 mV, after 500−ms conditioning voltage steps (–150 to –35 mV; Fig. 1C, protocol given as an inset). The amplitude of the available Na+ current (as a fraction of the maximal current, Imax) was plotted as function of the voltage of the conditioning pulse, and this relation was well described with a Boltzmann equation (Fig. 1D):
)exp(1)( max
c
h
VVV
IVI
−+
= (2)
The inactivation function was characterized by Vh = −61.9 ± 0.4 mV and Vc = –8.0 ± 0.4 mV (n = 8). The normalized inactivation curve I(V)/Imax is illustrated in Fig. 1D, in combination with the voltage dependence of the activation function: the fitted Boltzmann term from equation (1). The latter equation reflects the open fraction of the Na+ channels, immediately after depolarization to the specific voltage.

CBZ and TPM modulation of sodium current
85
Figure 1. Properties of the transient and persistent Na+ current in HEK293 cells that stably express the Na+ channel subunit NaV1.3. A: Currents activated by 100-ms depolarizing voltage steps ranging from –70 mV to +10 mV, after a 500-ms hyperpolarizing prepulse to –120 mV; cells were held at –70 mV (voltage protocol given in the inset). The transient (peak current) and the persistent Na+ current components (persistent current) are indicated by arrows. B: The amplitude of the persistent current and the peak current as a function of membrane voltage. Data points indicate mean values (n = 8); details on the error bars are explained in the text. The continuous curves are the fits of the Goldman-Hodgkin-Katz current equation to the mean data points (Eq. 1) (n = 8) that characterize the activation function of the transient current component Vh = −18.7 ± 0.7 mV and Vc = −5.1 ± 0.5 mV (for details see text), and of the persistent current Vh = −13.6 ± 0.4 mV and Vc = −4.1 ± 0.2 mV. C: Currents were evoked with a step depolarization to –10 mV for 25 ms after a 500-ms hyperpolarizing prepulse between –150 mV and –35 mV and used to determine the inactivation function. Voltage protocol is given in the inset. D: The steady-state inactivation function (open symbols) and the activation function (solid symbols) of the transient Na+ current. The steady-state inactivation function was determined by dividing the peak current amplitude obtained from a certain prepulse voltage by the maximal current (Imax) and plotting it as a function of the conditioning voltage; see protocol in C. The inactivation function was characterized by Vh = –61.9 ± 0.4 mV and Vc = 8.0 ± 0.4 mV (Eq. 2). The activation function is given by the Boltzmann term in Eq. 1; parameter values are given in 1B. Data points represent the mean values (n = 8), and error bars indicate the SEM values (for further details, see text).

Chapter 6
86
From the voltage dependence of activation and inactivation, we constructed the
window current of the transient-current component as the product of the activation and inactivation function by using the mean parameter values (Fig. 2). The window current for the fast Na+ current is at least one order of magnitude smaller than the persistent current evoked in the same cells; in addition, the window current can only make a relevant contribution for membrane voltages more negative than –20 mV. As expected, the window current disappeared at potentials more positive than –10 mV, where the persistent current was still large and only reduced because of the diminishing driving force (Fig. 2). This result confirms that we are indeed dealing with a persistent Na+ current, which can be easily distinguished from the window current of the fast transient component.
Figure 2. The absolute amplitude of the window current compared with the absolute amplitude of the persistent current. The window current was constructed as the product of the inactivation and activation function (see Fig. 1D). The window current was at least an order of magnitude smaller in amplitude than the persistent current, and it peaked below –20 mV, whereas the persistent current peaked around −10 mV. Data points represent mean values (n = 8); for clarity, error bars were omitted.
Block of the persistent Na+ current by CBZ and TPM
In the presence of 10 μM CBZ, the persistent Na+ current was partly and
reversibly blocked (Fig. 3A). We determined the concentration dependence of the CBZ-induced block by measuring the relative persistent Na+ current (evoked with a depolarizing voltage step to –10 mV) in the presence of 0, 1, 10, 50, and 100 μM CBZ. These values were expressed as a function of the CBZ concentration and fitted to a logistic equation of the form:

CBZ and TPM modulation of sodium current
87
hill
DEC
EIDI
⎟⎟⎠
⎞⎜⎜⎝
⎛+
−=
][1
1)(
50
max
0
(3)
where I(D) is the amplitude of the current in the presence of the drug (CBZ or TPM) with concentration [D], I0 is the amplitude of the persistent Na+ current in the absence of drug, Emax is the fraction of the current that can maximally be blocked, EC50 is the drug concentration that causes a half-maximal block, and hill is a slope factor analogous to the Hill coefficient. Our first fits indicated that hill is not different from 1, implying a one-to-one interaction of the drug with the blocking site; therefore we set hill to 1 in all fits. For CBZ, we observed a concentration-dependent block of the persistent Na+ current; the EC50 value was 16 ± 4 μM, and the maximal block Emax was 46 ± 4% (n = 5–8) (Fig. 3C).
Figure 3. Modulation of the transient and persistent Na+ current by carbamazepine (CBZ) measured in HEK293 cells that stably express the NaV1.3 subunit. A: Recordings of Na+ current before (a, control), during (b, CBZ) and after (c, wash) the application of 10 μM CBZ. All recordings are from the same cell; voltage protocol as explained in Fig. 1A. B: Concentration-dependent shift of the steady-state inactivation curve of the transient Na+ current induced by CBZ (0–100 μM) to more-hyperpolarized potentials. CBZ concentrations tested: 0 μM (n = 8), 1 μM (n = 7), 10 μM (n = 6), 50 μM (n = 5), 100 μM (n = 5). Two to four concentrations per cell were tested. Steady-state inactivation curves were constructed as described in Fig. 1C and D. C: Concentration–response relations for the CBZ-induced block of the persistent Na+ current and the CBZ-induced shift of the steady-state inactivation curve. The shift in the inactivation function induced by CBZ characterized by ΔVhi (see Eq. 2) was determined in each cell as the difference of the parameter Vh of the inactivation function in the absence and presence of CBZ (solid

Chapter 6
88
symbols). Two to four concentrations per cell were tested (see B). Next, the concentration dependence was fitted with the logistic equation (Eq. 4, continuous line) and yielded an EC50 of 14 μM and a maximal shift of 7.9 mV. The slope parameter Vc was hardly dependent on the CBZ concentration. The relative amplitude of the persistent Na+ current (at –10 mV) as a function of the CBZ concentration (measured in the same set of experiments as in B) is given by the open symbols and fitted also with a logistic function (Eq. 3, dotted line) to give an EC50 value of 16 μM and a maximal effect (Emax) of 46%. Data points represent mean values (n = 5–8), and error bars indicate SEM values.
TPM was able to evoke a partial and reversal block of the persistent Na+ current (Fig. 4A). Although the maximally attainable block (Emax) was only 30 ± 4% and smaller than that obtained with CBZ, TPM blocked the persistent Na+ current at a relatively low concentration: EC50 = 61 ± 37 nM (n = 3–6) (Fig. 4B).
Figure 4. Modulation of the transient and persistent Na+ current by topiramate (TPM) measured in HEK293 cells that stably express the NaV1.3 subunit. A: Recordings of Na+ current before (a, control), during (b, TPM) and after (c, wash) the application of 0.1 μM TPM. All recordings are from the same cell; the voltage protocol is illustrated in Fig. 1A. B: Concentration–response relations for the TPM-induced block of the persistent Na+ current and the TPM-induced shift of the steady-state inactivation curve of the transient Na+ current. One to four concentrations per cell were tested. Note the log concentration

CBZ and TPM modulation of sodium current
89
scale to incorporate the large effective concentration range of TPM. The concentration dependence of the shift in Vh of the inactivation function (ΔVh) was determined as described in Fig. 3B and C and fitted with a logistic function (Eq. 4, solid symbols, continuous line). The maximal shift was 2.9 mV, and the concentration of half-maximal effect (EC50) was 3.2 μM (n = 5–11). The relative persistent Na+ current (at –10 mV) was plotted against the concentration of TPM (5 nM–100 μM), and also fitted with a logistic equation (Eq. 3, open symbols, dotted line) to give an EC50 of 61 nM and a maximal effect (Emax) of 30% (n = 3–6). Data points represent mean values (n = 3–11); error bars indicate SEM values.
CBZ and TPM shift the steady-state inactivation curve of the transient Na+ current.
It is widely accepted that CBZ has a high affinity for the inactivated state of the
transient Na+ current and that this shifts the steady-state inactivation curve of the transient Na+ current to hyperpolarizing potentials. TPM also can interact with the inactivated state. To compare the effects of CBZ and TPM on the persistent Na+ current (see earlier) with the effect on Na+ channel inactivation, we determined the effect of CBZ and TPM on the voltage dependence of steady-state inactivation. For this, the same protocol as described in Fig. 1C and D was used. With increasing CBZ concentrations, the steady-state inactivation curve was shifted to more-negative potentials, which resulted in more-negative Vh values (Fig. 3B; Eq. 2). The absolute voltage shift of inactivation (ΔVh) by CBZ in Fig. 3B was calculated by taking the difference of Vh in the absence and presence of CBZ, and this value was expressed as a function of the CBZ concentration (Fig. 3C). The data points were fitted to a logistic function of the form:
( )
[ ]
hill
hh
DEC
VDV
⎟⎟⎠
⎞⎜⎜⎝
⎛+
Δ=Δ
50
max
1
(4)
where ΔVh is the shift of Vh evoked by the drug (CBZ or TPM) with concentration [D], ΔVhmax is the maximal attainable shift, EC50 is the concentration of the drug inducing half-maximal effect, and hill is a slope factor analogous to the Hill coefficient. Our first series of fits showed that hill was not different from 1, indicating a one-to-one interaction of the drug with the blocking site. Therefore we decided to set hill equal to 1 for all fits. With the fitting procedure, we obtained a maximal shift of 7.9 ± 1.6 mV and an EC50 value of 14 ± 11 μM (n = 5–8), which was not different from the EC50 value (16 μM) found for the CBZ effect on the persistent Na+ current.
The same analysis was performed with TPM, and we found that it evoked a relatively small shift of the steady-state inactivation curve [2.9 ± 0.3 mV (n = 5–11); Fig. 4B]. In addition, the EC50 value of 3.2 ± 1.8 μM (n = 5–11) shows that this effect is obtained at relatively high concentrations compared with the TPM-induced block of the persistent current (61 nM).
DISCUSSION
Several AEDs (ethosuximide, phenytoin, valproate, topiramate and lamotrigine) block the persistent Na+ current in acutely dissociated rat neurons of e.g. the neocortex, neostriatum and hippocampus (Chao and Alzheimer, 1995, Taverna et al., 1998, Taverna

Chapter 6
90
et al., 1999, Spadoni et al., 2002). In general, the block of the persistent Na+ current by AEDs could be achieved with lower concentrations than the concentrations needed to shift the steady-state inactivation curve of the transient Na+ current. In the present study, we compared the effects of CBZ and TPM on the transient and persistent Na+ current in HEK293 cells stably expressing the α−subunit of the Na+ channel NaV1.3. It was reported before that, in addition to a transient Na+ current, a prominent persistent Na+ current is present in this cell line and that both current components are TTX sensitive (Chen et al., 2000). Because only one molecular type of Na+ channel is expressed in this cell line, it is likely that a switch in gating modes of the channel accounts for the two Na+ current components, as was demonstrated before in native tissue (Alzheimer et al., 1993).
Our HEK293 cell line showed a stable and consistent expression of Na+ channels that gave a persistent current large enough to investigate systematically the effect of CBZ and TPM on the transient as well as the persistent component in cells under the same conditions. For CBZ, a commonly used first-line AED, not much information regarding its interaction with persistent Na+ currents is available, and it is of interest to know whether such an interaction could potentially contribute to its anticonvulsant profile. For the relatively new AED TPM, it has been suggested that its anticonvulsant action relies on interactions with different neurotransmitter and/or ion channel systems, like inhibition of kainate-evoked currents (Gibbs et al., 2000), enhancement of GABA-evoked currents (White et al., 1997), inhibition of voltage-activated Ca2+ currents (Zhang et al., 2000), but also block of (persistent) Na+ currents (Zona et al., 1997, Taverna et al., 1999).
We first demonstrated that the observed sustained current is indeed a persistent Na+ current and not the window current of the fast transient Na+ current. The latter can generate a window current arising from overlap of the steady-state inactivation and activation functions in which the activated current is not completely inactivated (Patlak, 1991, Johnston, 1995, Ketelaars et al., 2001). The window current was found to be much smaller than the persistent current and reached maximal amplitude at more-negative potentials. We therefore conclude that the window current contributes marginally—and only in the voltage ranges negative to –20 mV—to the persistent Na+ current.
The persistent Na+ current, expressed as a percentage of the peak current at –10 mV, was 10.3 ± 3.8 % (n = 8), and its voltage dependence of activation was located 5 mV more positive than that of the transient Na+ current, even though the persistent and transient currents have similarly shaped I-V relations. In the same types of cells, (Chen et al., 2000) recorded a slightly larger proportion of persistent current ( 15% of the peak current) and also the same Vh values for the persistent and transient components (–29 mV); both are more negative than the Vh values we determined. These properties can differ, depending on the type of host cell (CHO cells vs. HEK293 cells), the method of transfection (transient vs. stable), and the details of the chemical conditions. In addition, it has been shown that phosphorylation of Na+ channels can affect the electrophysiologic properties of the transient and persistent current components (Astman et al., 1998, Franceschetti et al., 2000), so that differences in phosphorylation state will also affect the absolute value of the characteristic properties of the channels. Despite these considerations, the HEK293 cell line stably expressing the NaV1.3 Na+ channel proved an excellent preparation to compare the effects of CBZ and TPM with each other and on persistent and transient Na+ currents.

CBZ and TPM modulation of sodium current
91
We showed that CBZ shifted the steady-state inactivation function of the transient Na+ current to more-hyperpolarized potentials. CBZ and several other AEDs (e.g., PHT and LTG) have been reported to affect the inactivation properties of the transient Na+ current in this manner, and it has been demonstrated that this property is largely responsible for the frequency-dependent reduction in excitability. The molecular mechanism that underlies this effect is a more effective binding of CBZ to the inactivated state than to the non-inactivated state, which, even in the simple classic Hodgkin and Huxley formalism of current gating, leads to a shift in inactivation function and a slowing of recovery rate from inactivation; both facts will underlie the antiepileptic properties (Macdonald and Kelly, 1995, Meldrum, 1996, Ragsdale and Avoli, 1998, Wadman et al., 2005). In addition, we found that CBZ blocked the persistent Na+ current with a maximal effect of 40% block and with comparable affinity to the effect of CBZ on the steady-state inactivation properties of the transient Na+ channel; the EC50 values of 16 μM, respectively 14 μM were not different. So unlike other AEDs (see earlier), CBZ does not seem to have a preferential blocking effect on the persistent Na+ current carried by the NaV1.3 Na+ channel. The EC50 values we found are, however, in the range of therapeutic effective concentrations. The best anticonvulsant effect of CBZ in humans seems to be obtained at plasma concentrations of 10–40 μM, whereas in the brain, this range may be 3–15 μM (Bertilsson, 1978, Bertilsson and Tomson, 1986, Altafullah et al., 1989). The effect of CBZ on the persistent Na+ current may provide an additional mechanism that contributes to the anticonvulsant profile of CBZ in parallel with the effect on the inactivation properties. Whereas the interaction with the transient current will mainly interfere with potential high-frequency firing, the interaction with the persistent current will directly affect neuronal excitability.
We found that TPM blocked the persistent Na+ current at relatively low concentrations (EC50, 61 nM), albeit that the maximal block (30%) was slightly less than the one evoked by CBZ (40%). The TPM-evoked block of the persistent component of the Na+ current occurred at much lower concentrations as compared with the TPM effect on the shift of the steady-state inactivation curve (EC50, 3.2 μM). In addition, the maximal shift (2.9 mV) of the inactivation curve that can be induced by TPM was small compared with the one that can be evoked by CBZ. This suggests that this mechanism of action contributes only marginally to the antiepileptic properties of TPM. It seems likely that as far as the interaction with the Na+ channel is concerned, the effect on the persistent Na+ current is the dominant factor shaping the pharmacologic profile of TPM, but other mechanisms of action have to contribute to make it an effective AED (Shank et al., 2000). The fact that the therapeutic TPM concentrations in the brain are likely to be in the low micromolar range(Perucca, 1997, Shank et al., 2000) also indicates that the interaction with the persistent Na+ current contributes more to the antiepileptic property of TPM than the interaction with the transient Na+ current.
The persistent Na+ current is believed to play an important role in neuronal excitability via several routes, including modulation of rhythmic (Taddese and Bean, 2002) and repetitive (burst) firing (Azouz et al., 1996, Brumberg et al., 2000) and amplification of inhibitory and excitatory post-synaptic signaling (Stuart and Sakmann, 1995, Stuart, 1999). Furthermore, (aberrant) persistent Na+ currents are demonstrated to be present during epileptic activity (Kohling, 2002, Segal, 2002). It has also been shown that in subicular neurons of epileptic patients the persistent Na+ current is dramatically

Chapter 6
92
increased (Vreugdenhil et al., 2004). The NaV1.3 Na+ channel is able to carry a relatively large persistent Na+ current and since this channel was found to be upregulated in human and rat epileptic hippocampus (Bartolomei et al., 1997, Aronica et al., 2001, Whitaker et al., 2001a), it may be an important target for AEDs like CBZ and TPM. Conversely, the presence of several distinct subunits of the Na+ channel in most neurons will complicate the situation and could account for the large variation in effectiveness observed in patients.
In conclusion, this study, by using a HEK293 cell line that stably expresses the NaV1.3 Na+ channels, showed that block of the persistent Na+ current contributes to the antiepileptic properties of both CBZ and TPM. Although for CBZ, this effect comes in parallel with the effect on the inactivation properties of the transient Na+ current, the TPM-induced block of the Na+ current seems to be the dominant interaction with the Na+ channel. Acknowledgement
The support of the Dutch Epilepsy Society (grant 98-17): "The Power of the
Small" is gratefully acknowledged.

CHAPTER 7
General Discussion

Chapter 7
94
The functional role of sodium channels The main role of sodium channels in the excitable membrane of neurons is to
initiate the upstroke of the action potential. In this way they are the main determinants of neuronal excitability and they are involved in almost all processes that modulate neuronal excitability. In this thesis we concentrated on several aspects of the functional role of sodium channels in epilepsy and in particular, we dealt with the question whether subtle differences in the properties and the expression of the pore-forming α-subunit of the sodium channels have pharmacological consequences with potential impact on the treatment of pharmacoresistance.
The fundamental properties that enable sodium channels to carry out their physiological role consist of a rapid, voltage-dependent activation, which opens the channel, and a slower voltage dependent inactivation (Catterall, 2000, Hille, 2001, Goldin, 2003, Ulbricht, 2005). At relatively depolarized potentials inactivation will close the channel and more importantly it will prevent reopening until the membrane has cycled through a period of hyperpolarization that is deep enough in voltage and long enough in time to remove the inactivation. Inactivation makes the cell refractory to firing during longer depolarizations, thus limiting the maximal firing rate and preventing a breakdown of ionic gradients that could ultimately lead to cell death.
The sodium channel is a remarkable example of successful evolution; it is present in almost the same molecular form in all nervous systems, apparently optimized to generate the basic signal of neural signalling (Catterall, 2000, Catterall et al., 2005, Yu et al., 2005). Nevertheless it is important to point out several aspects of the current that create some diversity. The action potential is generated by the classical fast sodium current, whose kinetics were first described by Hodgkin and Huxley in their famous gating formalism that very successfully stood model for most of the other voltage dependent currents (mainly carried by calcium and potassium). However, in more recent years a fundamentally different type of sodium current (the “persistent” sodium current) was observed in many preparations (Crill, 1996). It has about the same activation characteristics as the fast current, but lacks inactivation. Although it is several orders of magnitude smaller in amplitude than the fast current, its permanent presence can have important consequences for membrane potential and will also strongly affect the excitability of the cell. Until a detailed molecular entity that represents this channel has been found, the question whether we are dealing with a new sodium channel or whether we are observing a special activity state of the classical channel will not be resolved.
In addition to the fast and persistent sodium current there is a phenomenon that we call the window current. It originates from the fact that there can be a small voltage window where the fast sodium current can (partly) activate while it does not completely inactivate (Johnston, 1995). The final result is that within this voltage window a permanent sodium current will flow through the fast sodium channel. It activates with identical kinetics of the fast current (because it flows through the fast sodium channel!) but it never inactivates. This window current is also small, but, as with the persistent current, its permanent presence can significantly contribute to membrane potential and excitability. Within the voltage window the window current and the persistent current are indistinguishable, but as soon as the membrane is further depolarized the persistent current will stay, while the window current will disappear due to complete inactivation.

General Discussion
95
In this thesis we have described and parameterized the fast sodium current using the classical gating formalism of Hodgkin and Huxley despite the fact that more advanced (and often more complex) models are available (Hille, 2001, Clay, 2005). The main reason is that the fits (see e.g. chapter 2) are so good that they fall within the error margins of the actual measurements. This implies that there is no statistical reason to incorporate more parameters as that will not increase the explanatory value of the description. Moreover the binding models that assume that binding of anti-epileptic drugs (AEDs) to the channels in their inactivated state, are conceptually the best we have to explain the effects of this class of AEDs. The results shown in chapter 2 thus validate the way we parameterize the sodium currents with only a few critical parameters: the voltage-dependent coefficients of the Boltzmann equations (Vh and Vc) that describe activation and inactivation. The maximal conductance of the current (gmax) is relevant but strongly related to the surface of the neuronal membrane, i.e. to cell size. We did not go in great length to determine cell size in most cases, for group comparisons mostly the mean value of cell capacitance as an indication was sufficient. For HEK293 cells the population size was constant; for quantifying drug effects we always used the cells as their own controls.
The relation between fast sodium current amplitude and spike generation is so well established that we did not try to quantify it for every drug effect that we encountered. In chapter 2 we have shown that carbamazepine (CBZ) application, under the right conditions, indeed affects maximal firing rate as predicted. It would however be illustrative to translate in particular the differences in α-subunit pharmacology also to their meaning for cell firing under more realistic conditions. Such a comparison would still not predict seizure-prone behaviour as that should incorporate the details of sodium channels in all neurons in the densely wired local circuit. As such information is certainly not available in terms of the subunit composition of the actual sodium channels in all participating neurons, it would be almost impossible to predict the likelihood of seizures based on current knowledge, let alone explain the detailed consequences of differences in subunit pharmacology. Sodium currents and epilepsy
The clearest disregulation of excitability in the brain is epilepsy. In the epileptic
state neurons get hyper-synchronized and then simultaneously generate reverberating activity in the form of an epileptic seizure. This thesis does not deal with the epileptogenesis, the interesting process that results in the (often very) slow transition from a normal brain into a brain that is in the epileptic state (Avanzini and Franceschetti, 2003). This irreversible transition (for as far as we know to date) leads to a large increase in the likelihood of the occurrence of a seizure. In the context of our study we need to emphasize that seizures (which we want to combat with AEDs) are not uniquely restricted to the epileptic brain, but they can occur in any brain, if certain conditions are fulfilled. The difference between normal and epileptic is a difference in the likelihood of seizure occurrence, an extremely rare event in the normal brain, but they can occur up to 100 times a day in the epileptic brain. This notion rules at least to some extent, that seizures are related to unique molecular components that are only present in the epileptic brain (Avoli et al., 2005).

Chapter 7
96
One of the many ways to combat seizures is reducing the chance of highly synchronized action potential generation, at least with high frequencies. That property is the common feature of many epileptic drugs and certainly of the ones that interact with the sodium channel (Rogawski and Loscher, 2004a). We need however, to realize that the cure is not necessarily identical to the cause of the enhanced state of excitability. In other words, the fact that we can effectively (at least in a large fraction of the patients) combat seizures with drugs that interfere with the sodium channel, does not imply that deviations in the sodium channel need to underlie the epileptic state. It could also explain why there is such a large range of efficacy differences of the same drug with various forms of epilepsy. It is clear that there is a large variety of epileptic syndromes that all lead to electromyographic seizures, but originate from very different molecular conditions (Riviello, 2003). The efficacy of a standard sodium channel blocker might vary tremendously in these situations.
The role of the sodium channel in epilepsy is strengthened however by the fact that mutations in the sodium channel very often lead to epileptic conditions and several of the genetic models of epilepsy (all linked to distinct clinical patient groups) are based on such well established mutations.
The SCN1A gene which encodes the NaV1.1 neuronal α-subunit is at present considered to be the most clinically relevant epilepsy gene (Mulley et al., 2005) and several mutations in this gene have been linked to different forms of generalized epilepsy with febrile seizures plus (GEFS+) and severe myoclonic epilepsy of infancy (SMEI) (Mulley et al., 2005, Vanoye et al., 2006). In addition, two other sodium channel genes where mutations lead to epilepsy syndromes are the SCN2A and SCN1B genes, encoding the NaV1.2 α-subunit and the β1-subunit, respectively (Armijo et al., 2005, Yamakawa, 2006). Finally, also for the SCN5A gene it has been suggested that mutations in that gene are linked to epilepsy (Hartmann et al., 1999). Several studies have indicated that NaV1.3 channels are re-expressed in adult neurons after some types of injury, such as axotomy (Waxman et al., 1994) and kainate-induced seizures (Bartolomei et al., 1997, Gastaldi et al., 1997). In animal models for SMEI (NaV1.1 mutant mice), it was demonstrated that NaV1.1 channels are present at higher levels in hippocampal inhibitory GABA-ergic interneurons than in pyramidal neurons (Yu et al., 2006, Ogiwara et al., 2007). In the (epileptic) mutant mice, it was found that specifically in the interneurons the sodium current density was reduced (but not in the pyramidal neurons), that the NaV1.3 channel subtype was upregulated and that the interneurons displayed a reduced excitability level (Yu et al., 2006). These findings indicate that (very) local changes in neuronal sodium channel compositions can be involved in epilepsy. Consequently, treating epilepsy successfully with AEDs that target sodium channels may need an accurate AED-channel subunit interaction that critically depends on the sodium channel composition of the epileptic tissue (and that may be quite different from that of healthy tissue).
Many AEDs are relatively effective against the genetic forms of epilepsy, but none of them precisely compensates for the deviations that result from the genetic aberration, which represents another example of a situation where cause and cure may deviate.

General Discussion
97
Sodium currents in experimental animal models of epilepsy The research in this thesis started out with an investigation of sodium currents in
the kainate-induced animal model of experimental epilepsy. The aim was to compare the properties of sodium current in the kainate model with data that we collected earlier on the classical kindling model (Vreugdenhil et al., 1998, Vreugdenhil and Wadman, 1999) and the status epilepticus (SE)-induced model of epilepsy (Ketelaars et al., 2001). The conclusion from the latter two studies was that all models demonstrated a small shift in the inactivation function of the sodium channel in depolarizing direction in the order of 3-5 mV; this looks like a negligible shift, but given the steepness of the inactivation curve it can imply a difference of up to 30% in available current at resting membrane potential. The analysis of the sodium currents in the SE model also revealed a shift of the activation in hyperpolarizing direction, which will directly increase excitability as it affects spike generating threshold. The main difference between the two models is that the SE model leads to spontaneous seizures while in the kindling model, at least the state that was tested, spontaneous seizures do not yet occur, in agreement with a smaller increase in excitability. This point was neither confirmed nor disproved by our experiments in the kainate model of epilepsy, as the shift in both activation and inactivation function in hyperpolarizing direction is very hard to interpret and lack of power in the experiments prevented a more detailed analysis. An observation that has been made in all models, be it to a different degree, is that the window current after epileptogenesis is considerably enhanced and that the voltage window where it occurs is shifted into a direction that strengthens its effect on excitability. When comparing our results in the three models with those reported in the literature, a similar partial match comes forward. In the pilocarpine-induced model of epilepsy, dentate granule cells acutely dissociated from chronic epileptic rats showed changes in sodium current that were comparable with our observations in the SE model: a positive shift of the voltage-dependent inactivation and a negative shift of the voltage-dependent activation resulting in an enhanced window current (Ellerkmann et al., 2003). Surprisingly the changes in inactivation and activation function were not accompanied by changes in the kinetics in recovery from inactivation, which result from the same rate constants in the classical Hodgkin and Huxley description of the current (Ellerkmann et al., 2003). In another study in pilocarpine treated rats CBZ completely lost its effects on slowing down the fast recovery from inactivation, and apparently failed to reduce the sodium current availability during high-frequency action potential series (Remy et al., 2003b). However, in that study the binding of CBZ to the inactivated state was not quantified, so that a final explanation of the reported phenomenon cannot be given yet. A comparable observation was made in the pilocarpine treated rats by Leite and Cavalheiro (Leite and Cavalheiro, 1995) who claim that the epileptic rats only responded to CBZ at very high concentrations, but these authors did not analyze CBZ binding to the sodium channel at the cellular/molecular level. Clearly differences in the specific experimental models of epileptogenesis could complicate these comparisons (Loscher, 2002). But also the fact that different neuron types were analysed may play a role. On the other hand, sodium channels and their response to AEDs seems to be fairly uniform, no striking differences in principal cell types from the central nervous system have been reported so far.

Chapter 7
98
We conclude that in many situations epileptogenesis can lead to subtle changes in sodium currents with potential consequences for excitability. This conclusion is supported by two additional facts: 1) Patients with refractory temporal lobe epilepsy (TLE), whose seizures cannot be controlled in any other way, can sometimes be operated in order to remove the seizure focus. Analysis of sodium current in neurons dissociated from surgical tissue from these patients, with all its shortcomings in finding perfectly matched controls, also showed different responses (Beck et al., 1997, Beck et al., 1998, Reckziegel et al., 1998). 2) The second argument comes from studies that employ in-situ hybridization and demonstrate that changes in molecular composition of the sodium channel seem to occur. None of these studies could, understandably, demonstrate that the observations were related to functioning ion channels. A shift in composition of sodium channel α-subunit (e.g. the expression of NaV1.3 mRNA was higher than NaV1.2 mRNA), was detected in the hippocampus of the (kainate-induced) epileptic rat (Bartolomei et al., 1997) as well as in epileptic patients (Whitaker et al., 2001a). The observation could be more generally linked to injury as was also seen in adult neurons after axotomy (Waxman et al., 1994, Cummins et al., 2001). Furthermore, neonatal isoforms of the NaV1.2 and NaV1.3 α-subunits were induced in adult rat hippocampus by epileptic seizures (Gastaldi et al., 1997, Aronica et al., 2001).
Reducing the problem of epilepsy to a problem of a single type of ion channel is probably a great oversimplification. There exist epilepsies that result from a single mutation in a channel or receptor, but they are very rare and more the exception than the rule. Reviewing the literature also makes clear that there is a wide range of molecules indicated to be involved in epilepsy and/or epileptogenesis (Avanzini and Franceschetti, 2003, Armijo et al., 2005, Avoli et al., 2005). There is certainly a role for several types of calcium and potassium channels; in various epilepsies GABA and glutamate receptors are implicated and there are many indications that peptides play a role. Often it is important to realize that information in the brain is processed in small local networks that consist of densely coupled excitatory and inhibitory neurons. Stability in these networks is a delicate balance between excitation and inhibition and e.g. the functional consequences of changes in a sodium channel or glutamate receptor are strongly dependent on where they are located in the circuit. In such situation predictions need careful modelling and they fall outside this discussion. We will concentrate on the sodium channel, because even though the complete stability problem of brain circuits is very complicated, changing sodium currents will certainly have an effect that can be analyzed.
Our conclusion that in many situations where we encounter epilepsy we also observe changes in sodium current leads to at least two follow-up questions: 1) How do these changes come about and what are the underlying molecular mechanisms? and 2) what are the pharmacological consequences of the changes in sodium current (or the underlying causes)?
ad 1) Sodium channels can be directly modulated by many intracellular mechanisms such as phosphorylation (Cantrell and Catterall, 2001), but for longer periods of time like weeks, months or in the human even years, that epileptogenesis can last, protein expression is probably a better and more stable alternative. As explained above, such changes not only happen normally during development, but also under many pathological conditions. The signals that regulate the level of expression of the various sodium channel subunits are to the best of our knowledge not known yet, just as we do

General Discussion
99
not know how the desired expression level is regulated. In well-defined acutely isolated neurons we measured complete sets of sodium current traces and determined voltage-dependent activation, inactivation, and recovery from inactivation by using the classical formalism of Hodgkin and Huxley. The differences in biophysical properties of the pore forming α-subunits NaV1.1, NaV1.2, NaV1.3, NaV1.6 were determined using specific HEK293 cell lines.
ad 2) The pharmacology of the interaction between AEDs (CBZ, phenytoin (DPH) and lamotrigine (LTG)) and the sodium channel were determined in either acutely isolated neurons or in HEK293 cell lines that specifically and stably express one of the α-subunits (NaV1.1, NaV1.2, NaV1.3, NaV1.6) of the sodium channel. The three drugs investigated in this thesis (CBZ, DPH and LTG) possess anticonvulsant properties through an interaction with voltage-gated sodium channels. The interaction between the drug and the channel can be incorporated in the H&H formalism that describes the kinetics of the sodium current, by adding one more inactivated state: the one that describes the binding to the AED (see chapter 2). CBZ, LTG and DPH all have a much higher affinity to the inactivated state than to the resting or open state of the channel (Macdonald and Kelly, 1993, Kuo et al., 1997) and they bind to the inactivated state via a simple bimolecular, one-to-one binding reaction (Macdonald and Kelly, 1993, Kuo et al., 1997, Kuo and Lu, 1997). Thus (seconds) long depolarizations will be needed for full binding (Matsuki et al., 1984, Lang et al., 1993, Kuo and Bean, 1994b, Kuo and Bean, 1994a, Xie et al., 1995). The interaction with the inactivated state is stronger at more depolarized potentials (Matsuki et al., 1984, Willow et al., 1985, Schwarz and Grigat, 1989, Kuo and Lu, 1997), resulting in the use- or frequency-dependent block of repetitive discharges which is viewed as the major mechanism for this class of AEDs (Macdonald and Kelly, 1993, Macdonald and Kelly, 1994, Macdonald and Kelly, 1995, Meldrum, 1996, Kuo et al., 1997, Rogawski and Loscher, 2004a, Perucca, 2005). The use- and frequency-dependent block readily explains why these nonsedative AEDs effectively inhibit seizure discharges, yet spare most normal activities (Kuo and Lu, 1997). Pharmacoresistance
The AEDs have the remarkable ability to protect against seizures while hardly
interfering with normal functioning of the nervous system. Besides drugs that affect voltage-gated sodium channels, the control of epilepsy is also obtained with drugs that interfere with voltage-gated calcium channels or with glutamate or GABAA (γ-aminobutyric acid, type A) receptors. We will not describe the pharmacology of the non-sodium channel AEDs but refer to the recent literature (Rogawski and Loscher, 2004a, Meldrum and Rogawski, 2007). AEDs provide satisfactory control of seizures for most patients with epilepsy, but a substantial fraction of patients (~ 30%) continues to have seizures despite carefully optimized drug treatment. Although the term “pharmacoresistant” or “medically refractory” that is used for this patient category lacks a precise definition, most clinicians would consider an epilepsy pharmacoresistant that had not been controlled by any of the two or three first-line AEDs that are normally prescribed for a given epilepsy syndrome (Loscher and Potschka, 2002). Consequently the most important characteristic of pharmacoresistant epilepsy is that patients with refractory epilepsy are resistant to most, and often all, AEDs (Regesta and Tanganelli,

Chapter 7
100
1999). Two concepts have been put forward to explain pharmacoresistance (Sisodiya,
2003, van Vliet et al., 2004, Remy and Beck, 2006). 1) The transporter hypothesis assumes that an impaired access of AEDs to the CNS targets is the cause of the pharmacoresistance. Such block could result from an enhanced expression or function of multidrug transporters in the brain. These transporters (especially the P-glycoproteins) are expressed in the blood-brain barrier to regulate the intraparenchymal concentrations of many substances and they are often good substrates for AEDs. The latter implies that upregulation of these transporter proteins and/or their function will lead to an effective extrusion of AEDs, reducing the brain concentration and thus the anti-epileptic efficacy (Tishler et al., 1995, Lazarowski et al., 1999, Schuetz et al., 1999, Zhang et al., 1999, Sisodiya et al., 2001, Abbott et al., 2002, Loscher and Potschka, 2002).
2) The target hypothesis holds that epilepsy-related genetic or functional modification are located in the drug targets themselves e.g. the receptor or ion channel, which results in a reduced drug sensitivity and efficacy (Heinemann et al., 1994, Vreugdenhil and Wadman, 1999). A changed sodium channel composition in epileptic tissue would fit with the target hypothesis (Vreugdenhil et al., 1998, Remy and Beck, 2006) and there is consistent evidence to support it, like e.g. the earlier discussed shift in composition of sodium channel subunit of both the epileptic model rat (Bartolomei et al., 1997) and epileptic patients (Whitaker et al., 2001a). The target hypothesis would force the search for new AEDs into a direction that tries to come up with drugs with a specific efficacy towards the “changed targets” (e.g. the re-expressed NaV1.3 channel subtype in epileptic tissue).
The two hypotheses expressed above are not mutually exclusive, both conditions may occur in parallel, not making the task for the neurologist more attractive. But it also implies that the search for new AEDs will aim at improving availability in the brain as well as focus on new (or modified) targets.
A highly relevant third aspect has also to be taken into account for both hypothesis and that is that most likely changes in target as well as blood brain barrier function could be quite inhomogeneously distributed over the brain and mostly be specifically located in certain brain regions. As discussed earlier the α- and β-subunits of the voltage-activated sodium channels have distinct expression patterns throughout the brain, in addition to a subcellular specialization (Trimmer and Rhodes, 2004). In combination with the observation that the four brain α-subunits possess different AED sensitivities (chapter 3) implies that uniform AED efficacy in all brain areas is rather unlikely. The larger such differences become the more difficult it will be to either control seizure activity without side effects; or alternatively, with the maximally tolerated side effects to control seizure activity. Development
Before embarking on the extensive attempt to quantify α-subunit specific sodium
channel pharmacology, we wanted to test its potential success on a preparation from which it is known that a clear difference in sodium channel subunit exists. Many studies in rat brain have shown that sodium channels have distinct expression patterns at different stages of development. The NaV1.2 subunit is abundant in the brain at all

General Discussion
101
developmental stages; NaV1.1 and NaV1.6 subunits display an increased expression pattern after birth, whereas the NaV1.3 subunit is barely detectable at P30 and it is mainly expressed at late embryonic and early postnatal time points (Brysch et al., 1991, Felts et al., 1997). However, more recent studies also indicate NaV1.3 channel expression in adult brain tissue (Chen et al., 2000, Whitaker et al., 2001b, Lindia and Abbadie, 2003, Candenas et al., 2006).
In this thesis voltage-activated sodium currents were studied in acutely dissociated CA1 hippocampal neurons of neonatal (P2-4) and adult rats (P36-41). In neonatal neurons voltage-activated sodium channels are present at a lower density than in adult neurons. Together with a shift of the steady-state inactivation function in hyperpolarizing direction and a slower recovery from inactivation, this will lead to a reduced excitability level in neonatal CA1 neurons compared to adult neurons. It has been suggested that a reduced excitability level (possibly due to the presence of NaV1.3 α-subunits) in neonatal neurons serves a protective mechanism for new-born mammals for dealing with hypoxic conditions (Park and Ahmed, 1991, Cummins et al., 2001).
Besides the lower excitability observed in neonatal neurons we also found that they have a higher sensitivity to CBZ. In neonatal CA1 neurons CBZ evoked a stronger slowing of the recovery from inactivation than it did in adult neurons.
The difference in CBZ response and the faster binding rate of CBZ to inactivated sodium channels of neonatal neurons could be a consequence of the higher expression level of the NaV1.3 channel subtype in neonatal neurons. This finding is partly in line with the HEK cell study (chapter 3) where NaV1.3 channels (compared to NaV1.1 channels) presented a more hyperpolarized Vh, a significantly slower recovery from inactivation, and a smaller EC50 of CBZ on sodium currents blocking. However, a faster CBZ binding rate to inactivated NaV1.3 currents (compared to the currents carried by the other α-subunits) was not observed (whereas the CBZ binding rate to inactivated neonatal currents was faster compared to that of adult currents). This illustrates that such comparisons remain awkward, and that the presence of more than one α-subunit and modifying molecules (like β-subunits) in native neurons may mask certain characteristics of channel-drug interactions (Isom, 2001, Waxman, 2007). The plasticity of sodium channel expression is not restricted to development, because NaV1.3 channels are re-expressed in adult neurons after kainate-induced seizures (Gastaldi et al., 1997) and after some types of injury, e.g. axotomy (Waxman et al., 1994). These observations predict that changes in the NaV1.3 channel expression pattern may play an important role in epilepsy and other pathological conditions, with potential pharmacological consequences. Pharmacology of the persistent sodium current
Sodium channels that inactivate rapidly carry the transient, inward currents
underlying fast action potentials, whereas non-inactivating or persistent sodium current may be responsible for spontaneous action potentials and plateau potentials, as was discussed in earlier sections (Llinas, 1988, Taylor, 1993, Crill, 1996). Persistent sodium currents are also thought to be involved in epileptic activity (Kohling, 2002, Segal, 2002).
The amplitude of the persistent sodium current was extremely large in subicular neurons isolated from tissue obtained from drug-resistant epileptic patients that underwent epilepsy surgery (Vreugdenhil et al., 2004). The NaV1.3 channel is able to

Chapter 7
102
carry a relatively large persistent sodium current and since this channel was found to be upregulated in human and rat epileptic brain, it may be important for the pharmaco-sensitivities of AEDs for sodium channels (Bartolomei et al., 1997, Whitaker et al., 2001a).
Persistent sodium current components are also targets of several first-line AEDs (CBZ, LTG and DPH) that affect the fast transient current (Ragsdale and Avoli, 1998, Kohling, 2002, Rogawski and Loscher, 2004a, Perucca, 2005). A persistent component of sodium currents can be produced by NaV1.1, NaV1.3 and NaV1.6 when expressed in HEK293 cells (Chen et al., 2000, Burbidge et al., 2002).
The HEK293 expression system provided an excellent tool to compare the effects of AEDs on the transient and persistent component generated by the same channel subtype. The persistent sodium current was evident in all cells that expressed the NaV1.3 α-subunit and its amplitude at –10 mV was ~10 % of the total current (chapter 6). Since the HEK cells only express one sodium channel subtype, it was easy to separate the persistent current from the window current. Both the transient and persistent NaV1.3 sodium currents were blocked by CBZ (at therapeutic concentrations, ~15 μM), and this property can therefore contribute to the anticonvulsant profile of CBZ. We also tested another AED whose mechanisms of action are slightly outside the standard sodium blocking profile. Topiramate (TPM) induced a block of the persistent sodium current that could well be the predominant action for the anticonvulsant profile of this drug as its effective concentration lies orders of magnitude below the one needed to affect the fast transient sodium channel (EC50 values were ~60 nM and ~3 μM, respectively).
The observation that the NaV1.3 channel can carry a relatively large persistent sodium current (Chen et al., 2000) suggests that its (re-)expression could underlie the increased persistent sodium currents isolated from epileptic tissues (Kohling, 2002, Segal, 2002, Vreugdenhil et al., 2004) and points to a crucial role for the NaV1.3 channel in epilepsy. In that respect the persistent sodium current is an interesting target for (new) AEDs. The confirmation that TPM indeed is a potent blocker of the persistent sodium current (chapter 6) and that this may be a dominant property of TPM as an anticonvulsant drug, indicates the usefulness of the sodium channel expression systems for screening new AEDs. Biophysical properties of sodium channel α-subunits investigated in HEK293 cells
The human brain voltage-gated sodium channel α-subunits Nav1.1, Nav1.2,
Nav1.3 and Nav1.6 have been cloned and stably expressed in HEK293 cells (Chen et al., 2000, Burbidge et al., 2002).
We have chosen these cell lines to study their biophysical properties and pharmacology in isolation, which enabled us to investigate the large set of pharmacological properties of the most commonly used AEDs. The precise role of each sodium channel α-subunits subtype is only poorly understood and different approaches have been used to address this problem including genetic analysis, mapping their cellular and sub-cellular distribution, and characterization of the cloned channels (Burbidge et al., 2002). The HEK cell lines have quick and easy reproduction and maintenance, high efficiency of protein production, small cell size with minimal processes appropriate for voltage-clamp experimentation (Thomas and Smart, 2005). Expression of the α-subunit

General Discussion
103
alone is sufficient for the formation of functional sodium channels (Catterall, 2000), and thus these cell lines provide a good vehicle to detect (subtle) channel differences between subtypes, a distinction level that cannot be reached in native tissues. However, one has to keep in mind that the HEK cell system lacks the contribution of sodium channel β-subunits, which are known to modify electrophysiological properties of sodium channels by hyperpolarizing shifts in the voltage-dependence of activation and inactivation, increasing the rate of inactivation as well as the rate of recovery from inactivation through changes in channel modal-gating behavior (Isom et al., 1994). Despite this shortcoming, studying the α-subunits in isolation can provide detailed information regarding the physiology of these channels and their interactions with modifying drugs.
So far the comparison of the electrophysiological properties of the four human brain sodium channel subtypes NaV1.1, NaV1.2, NaV1.3 and NaV1.6 expressed in the same mammalian cell line background, has not been reported in detail (Clare et al., 2000). By examining the functional properties of these sodium channel subtypes, we should gain a better understanding of how each subunit affects electrical excitability and how modifying drugs like AEDs influence neuronal excitability by interacting with the different sodium channel subtypes.
The sodium channel types NaV1.1, NaV1.2, NaV1.3 and NaV1.6 are very similar to each other in amino acid sequence (Catterall, 2000) and they all generate fast-activating and fast-inactivating currents (Smith and Goldin, 1998, Cummins et al., 2001, Burbidge et al., 2002).
In the present study, NaV1.1 currents showed distinguished properties with respect to activation, steady-state inactivation and recovery from inactivation when compared to NaV1.2, NaV1.3 and NaV1.6 currents. It activated at more negative potentials and inactivated at more positive potentials with 33 mV difference in half maximal voltage of activation and inactivation (ΔVh), whereas 40 mV of ΔVh was found for the other three channel subunits. Consistently, a ΔVh of ~40 mV was reported for sodium currents carried by the NaV1.2 and NaV1.3 channels (expressed in the same background of cells) (Cummins et al., 2001). For the same steepness of the activation and inactivation curves, the smaller ΔVh of NaV1.1 channel means a larger overlap of activation and steady-state inactivation and thus a larger window current that spans a wider voltage range, with all consequences for neuronal excitability as discussed in previous sections.
The recovery from inactivation for NaV1.1 currents was also faster compared with NaV1.2 and NaV1.3 currents, which could be consistent with an increase of sodium conductance, because it drives more inactivated channels to the resting state, making them available for a next pulse. All these characteristics of the NaV1.1 channel make it capable to underlie rapid firing of action potentials. In addition, the subcellular location of NaV1.1 channels in dendrites and cell bodies of neurons (Westenbroek et al., 1989) suggests a role in the facilitation of excitatory synaptic inputs. Such properties may also contribute to fast axonal action potential firing, since in a recent study it was reported that NaV1.1 channels also are present in axonal membranes (Ogiwara et al., 2007). The clustering of NaV1.6 channels in the nodes of Ranvier (Boiko et al., 2003) will accommodate rapid action potential propagation due to the fast recovery from inactivation kinetics of the NaV1.6 currents.

Chapter 7
104
The slowest recovery from inactivation was found for NaV1.3 currents (1.5-4 times larger time constants than those observed for the other three channel subunits) and are in line with previously reported values for NaV1.3 channels (Cummins et al., 2001). This property could make cells with relatively high levels of NaV1.3 α-subunits (compared to the other α-subunits) less excitable (see the section on development). Pharmacology of sodium channel α-subunits investigated in HEK293 cells
The findings presented in this thesis indicate that for the different brain α-subunits
the interactions of these channels with AEDs display subtle differences. Unfortunately we were not able to come to a complete comparison (e.g. determine all details regarding the drug-subunits interactions for the three AEDs with the four α-subunits), but nevertheless a relative good insight into AED-subunit interactions was obtained.
The maximal sodium conductance in neurons is huge, and blocking part of it may not completely affect cellular firing activity. However, during ictal discharges, prolonged depolarization may drive almost all sodium channels into the inactivated state. From the kinetic point of view, the length of interictal or ictal depolarization shift is crucial in discussing the antiepileptic action of DPH, CBZ and LTG (Kuo et al., 1997, Kuo and Lu, 1997). Therefore the interaction kinetics of the three AEDs with the four α-subunits provided some interesting information that may have important consequences for understanding AED efficacy in cases and/or conditions (in epileptic versus healthy tissues) with shifted α-subunit compositions.
The binding rates of CBZ, DPH and LTG that were determined for the different α-subunits (chapter 3) were in line of those described for sodium channels in native tissues (Kuo and Bean, 1994b, Kuo et al., 1997, Kuo and Lu, 1997). Moreover, it was for the first time described that AED binding rates can differ considerably between the four α-subunits, with possible consequences for AED efficacy.
An example is the different frequency-dependent block of NaV1.2 and NaV1.3 currents by CBZ and LTG (chapter 3), which could be explained by the differences in AED binding rates. The binding of CBZ to inactivated NaV1.2 and NaV1.3 channels (~75 mM-1s-1 and ~45 mM-1s-1, respectively) is fast enough to evoke a block of the sodium current where the applied stimulus frequencies (10 and 50 Hz) do not appear to be a rate-limiting factor. However, in the case of LTG, which has a much slower binding rate to the inactivated channels than CBZ, clear differences were found when activating NaV1.2 and NaV1.3 currents with 10 or 50 Hz stimulus trains. The LTG binding to the NaV1.2 subtype (~21 mM-1s-1) was fast enough to result in an acceleration of development of block when switching from a stimulus frequency from 10 Hz to 50 Hz but the LTG binding to the NaV1.3 subtype (~13 mM-1s-1) was apparently too slow to reveal such an acceleration. This illustrates that – depending on activity levels – the use- and frequency-dependent effects of AEDs could be different for neurons with diverse sodium channel compositions. Concluding remarks
Based on experimental work we have hypothesized that a shift in expression
patterns of the pore-forming α-subunit of the voltage-activated sodium channel could

General Discussion
105
affect the sensitivity of the sodium current to the commonly used AEDs and so be responsible for a change in sensitivity or worse, no response at all. If these differences occur at a different pace in different brain regions, it is clear that providing the epileptic patient with a dose effective for all brain regions becomes a mission impossible.
Therefore an AED screening strategy should be applied that considers that AED efficacy can be different in affected (i.e. epileptic) and normal tissues. Consequently, the use of the HEK293 cell lines expressing the different α-subunits could provide such a test system. Although such a strategy seems very promising, it has to be considered that targets studied in artificial expression systems may not exactly “behave” as the same targets in (epileptic) native tissues. In that respect the background of the tissue expressing the target (i.e. the voltage-gated sodium channel) may very likely influence its functioning (Waxman, 2007). Therefore in vivo testing systems should always play a dominant role in the search for new AEDs (Rogawski, 2006), but the in vitro expression systems may provide an additional exploration tool that can facilitate AED screening.
All together, the findings presented in this thesis support the view that the development of new AEDs may better rely on focusing on (affected) brain area-specific AED activity instead of studying “whole-brain” AED activity. In line with the efforts to optimise individual therapy of the epilepsies (Stefan and Feuerstein, 2007), such an approach may provide a novel and challenging strategy for finding new AEDs and possibly may help to solve the problem of pharmacorsistance in epilepsy.


REFERENCES
Abbott, N. J., Khan, E. U., Rollinson, C. M., Reichel, A., Janigro, D., Dombrowski, S. M.,
Dobbie, M. S. and Begley, D. J., 2002. Drug resistance in epilepsy: the role of the blood-brain barrier. Novartis Found Symp. 243, 38-47; discussion 47-53, 180-185.
Agrawal, N., Alonso, A. and Ragsdale, D. S., 2003. Increased persistent sodium currents in rat entorhinal cortex layer V neurons in a post-status epilepticus model of temporal lobe epilepsy. Epilepsia. 44, 1601-1604.
Altafullah, I., Talwar, D., Loewenson, R., Olson, K. and Lockman, L. A., 1989. Factors influencing serum levels of carbamazepine and carbamazepine-10,11-epoxide in children. Epilepsy Res. 4, 72-80.
Alzheimer, C., Schwindt, P. C. and Crill, W. E., 1993. Modal gating of Na+ channels as a mechanism of persistent Na+ current in pyramidal neurons from rat and cat sensorimotor cortex. J Neurosci. 13, 660-673.
Armijo, J. A., Shushtarian, M., Valdizan, E. M., Cuadrado, A., de las Cuevas, I. and Adin, J., 2005. Ion channels and epilepsy. Curr Pharm Des. 11, 1975-2003.
Armstrong, C. M., 1981. Sodium channels and gating currents. Physiol Rev. 61, 644-683. Aronica, E., Troost, D., Rozemuller, A. J., Yankaya, B., Jansen, G. H., Isom, L. L. and
Gorter, J. A., 2003. Expression and regulation of voltage-gated sodium channel beta1 subunit protein in human gliosis-associated pathologies. Acta Neuropathol (Berl). 105, 515-523.
Aronica, E., Yankaya, B., Troost, D., van Vliet, E. A., Lopes da Silva, F. H. and Gorter, J. A., 2001. Induction of neonatal sodium channel II and III alpha-isoform mRNAs in neurons and microglia after status epilepticus in the rat hippocampus. Eur J Neurosci. 13, 1261-1266.
Astman, N., Gutnick, M. J. and Fleidervish, I. A., 1998. Activation of protein kinase C increases neuronal excitability by regulating persistent Na+ current in mouse neocortical slices. J Neurophysiol. 80, 1547-1551.
Auld, V. J., Goldin, A. L., Krafte, D. S., Marshall, J., Dunn, J. M., Catterall, W. A., Lester, H. A., Davidson, N. and Dunn, R. J., 1988. A rat brain Na+ channel alpha subunit with novel gating properties. Neuron. 1, 449-461.
Avanzini, G. and Franceschetti, S., 2003. Cellular biology of epileptogenesis. Lancet Neurol. 2, 33-42.
Avanzini, G., Franceschetti, S. and Mantegazza, M., 2007. Epileptogenic channelopathies: experimental models of human pathologies. Epilepsia. 48 Suppl 2, 51-64.
Avoli, M., Louvel, J., Pumain, R. and Kohling, R., 2005. Cellular and molecular mechanisms of epilepsy in the human brain. Prog Neurobiol. 77, 166-200.
Azouz, R., Jensen, M. S. and Yaari, Y., 1996. Ionic basis of spike after-depolarization and burst generation in adult rat hippocampal CA1 pyramidal cells. J Physiol. 492 ( Pt 1), 211-223.
Bartolomei, F., Gastaldi, M., Massacrier, A., Planells, R., Nicolas, S. and Cau, P., 1997. Changes in the mRNAs encoding subtypes I, II and III sodium channel alpha subunits following kainate-induced seizures in rat brain. J Neurocytol. 26, 667-678.

References
108
Bear, M. F., Connors, B. W. and Paradiso, M. A., 2006. Neuroscience. Exploring the Brain. Lippincott Williams & Wilkins, Philadelphia, Baltimore, New York, London, Buenos Aires, Hong Kong, Sydney, Tokio.
Beck, H., Steffens, R., Elger, C. E. and Heinemann, U., 1998. Voltage-dependent Ca2+ currents in epilepsy. Epilepsy Res. 32, 321-332.
Beck, H., Steffens, R., Heinemann, U. and Elger, C. E., 1997. Properties of voltage-activated Ca2+ currents in acutely isolated human hippocampal granule cells. J Neurophysiol. 77, 1526-1537.
Ben-Ari, Y., 1985. Limbic seizure and brain damage produced by kainic acid: mechanisms and relevance to human temporal lobe epilepsy. Neuroscience. 14, 375-403.
Ben-Ari, Y. and Represa, A., 1990. Brief seizure episodes induce long-term potentiation and mossy fibre sprouting in the hippocampus. Trends Neurosci. 13, 312-318.
Bertilsson, L., 1978. Clinical pharmacokinetics of carbamazepine. Clin Pharmacokinet. 3, 128-143.
Bertilsson, L. and Tomson, T., 1986. Clinical pharmacokinetics and pharmacological effects of carbamazepine and carbamazepine-10,11-epoxide. An update. Clin Pharmacokinet. 11, 177-198.
Bertram, E., 2007. The relevance of kindling for human epilepsy. Epilepsia. 48 Suppl 2, 65-74.
Birch, P. J., Dekker, L. V., James, I. F., Southan, A. and Cronk, D., 2004. Strategies to identify ion channel modulators: current and novel approaches to target neuropathic pain. Drug Discov Today. 9, 410-418.
Black, J. A., Yokoyama, S., Higashida, H., Ransom, B. R. and Waxman, S. G., 1994. Sodium channel mRNAs I, II and III in the CNS: cell-specific expression. Brain Res Mol Brain Res. 22, 275-289.
Boiko, T., Rasband, M. N., Levinson, S. R., Caldwell, J. H., Mandel, G., Trimmer, J. S. and Matthews, G., 2001. Compact myelin dictates the differential targeting of two sodium channel isoforms in the same axon. Neuron. 30, 91-104.
Boiko, T., Van Wart, A., Caldwell, J. H., Levinson, S. R., Trimmer, J. S. and Matthews, G., 2003. Functional specialization of the axon initial segment by isoform-specific sodium channel targeting. J Neurosci. 23, 2306-2313.
Borges, K., McDermott, D., Irier, H., Smith, Y. and Dingledine, R., 2006. Degeneration and proliferation of astrocytes in the mouse dentate gyrus after pilocarpine-induced status epilepticus. Exp Neurol. 201, 416-427.
Borowicz, K. K., Kimber-Trojnar, Z., Ratnaraj, N., Patsalos, P. N., Luszczki, J. J. and Czuczwar, S. J., 2007. Isobolographic analysis of interactions between losigamone and conventional antiepileptic drugs in the mouse maximal electroshock model. Eur Neuropsychopharmacol. 17, 94-101.
Brodie, M. J., 2001. Do we need any more new antiepileptic drugs? Epilepsy Res. 45, 3-6. Brodie, M. J. and Porter, R. J., 1990. New and potential anticonvulsants. Lancet. 336,
425-426. Browne, T. R. and Holmes, G. L., 2001. Epilepsy. N Engl J Med. 344, 1145-1151. Brumberg, J. C., Nowak, L. G. and McCormick, D. A., 2000. Ionic mechanisms
underlying repetitive high-frequency burst firing in supragranular cortical neurons. J Neurosci. 20, 4829-4843.

References
109
Brysch, W., Creutzfeldt, O. D., Luno, K., Schlingensiepen, R. and Schlingensiepen, K. H., 1991. Regional and temporal expression of sodium channel messenger RNAs in the rat brain during development. Exp Brain Res. 86, 562-567.
Burbidge, S. A., Dale, T. J., Powell, A. J., Whitaker, W. R., Xie, X. M., Romanos, M. A. and Clare, J. J., 2002. Molecular cloning, distribution and functional analysis of the NA(V)1.6. Voltage-gated sodium channel from human brain. Brain Res Mol Brain Res. 103, 80-90.
Candenas, L., Seda, M., Noheda, P., Buschmann, H., Cintado, C. G., Martin, J. D. and Pinto, F. M., 2006. Molecular diversity of voltage-gated sodium channel alpha and beta subunit mRNAs in human tissues. Eur J Pharmacol. 541, 9-16.
Cantrell, A. R. and Catterall, W. A., 2001. Neuromodulation of Na+ channels: an unexpected form of cellular plasticity. Nat Rev Neurosci. 2, 397-407.
Catania, M. V., Giuffrida, R., Seminara, G., Barbagallo, G., Aronica, E., Gorter, J. A., Dell'Albani, P., Ravagna, A., Calabrese, V. and Giuffrida-Stella, A. M., 2003. Upregulation of neuronal nitric oxide synthase in in vitro stellate astrocytes and in vivo reactive astrocytes after electrically induced status epilepticus. Neurochem Res. 28, 607-615.
Catterall, W. A., 1984. The molecular basis of neuronal excitability. Science. 223, 653-661.
Catterall, W. A., 1992. Cellular and molecular biology of voltage-gated sodium channels. Physiol Rev. 72, S15-48.
Catterall, W. A., 1995. Structure and function of voltage-gated ion channels. Annu Rev Biochem. 64, 493-531.
Catterall, W. A., 1999. Molecular properties of brain sodium channels: an important target for anticonvulsant drugs. Adv Neurol. 79, 441-456.
Catterall, W. A., 2000. From ionic currents to molecular mechanisms: the structure and function of voltage-gated sodium channels. Neuron. 26, 13-25.
Catterall, W. A., Goldin, A. L. and Waxman, S. G., 2005. International Union of Pharmacology. XLVII. Nomenclature and structure-function relationships of voltage-gated sodium channels. Pharmacol Rev. 57, 397-409.
Celesia, G. G., 2001. Disorders of membrane channels or channelopathies. Clin Neurophysiol. 112, 2-18.
Ceulemans, B. P., Claes, L. R. and Lagae, L. G., 2004. Clinical correlations of mutations in the SCN1A gene: from febrile seizures to severe myoclonic epilepsy in infancy. Pediatr Neurol. 30, 236-243.
Chao, T. I. and Alzheimer, C., 1995. Effects of phenytoin on the persistent Na+ current of mammalian CNS neurones. Neuroreport. 6, 1778-1780.
Chen, Y. H., Dale, T. J., Romanos, M. A., Whitaker, W. R., Xie, X. M. and Clare, J. J., 2000. Cloning, distribution and functional analysis of the type III sodium channel from human brain. Eur J Neurosci. 12, 4281-4289.
Claes, L., Del-Favero, J., Ceulemans, B., Lagae, L., Van Broeckhoven, C. and De Jonghe, P., 2001. De novo mutations in the sodium-channel gene SCN1A cause severe myoclonic epilepsy of infancy. Am J Hum Genet. 68, 1327-1332.
Clare, J. J., 2006. Discovery of novel sodium channel inhibitors—A gene family-based approach. Comparative Biochemistry and Physiology. Part D 1, 309–318.

References
110
Clare, J. J., Tate, S. N., Nobbs, M. and Romanos, M. A., 2000. Voltage-gated sodium channels as therapeutic targets. Drug Discov Today. 5, 506-520.
Clay, J. R., 2005. Axonal excitability revisited. Prog Biophys Mol Biol. 88, 59-90. Crill, W. E., 1996. Persistent sodium current in mammalian central neurons. Annu Rev
Physiol. 58, 349-362. Crino, P. B., 2007. Gene expression, genetics, and genomics in epilepsy: some answers,
more questions. Epilepsia. 48 Suppl 2, 42-50. Cross, D. J. and Cavazos, J. E., 2007. Synaptic reorganization in subiculum and CA3
after early-life status epilepticus in the kainic acid rat model. Epilepsy Res. 73, 156-165.
Cummins, T. R., Aglieco, F., Renganathan, M., Herzog, R. I., Dib-Hajj, S. D. and Waxman, S. G., 2001. Nav1.3 sodium channels: rapid repriming and slow closed-state inactivation display quantitative differences after expression in a mammalian cell line and in spinal sensory neurons. J Neurosci. 21, 5952-5961.
Cummins, T. R., Xia, Y. and Haddad, G. G., 1994. Functional properties of rat and human neocortical voltage-sensitive sodium currents. J Neurophysiol. 71, 1052-1064.
DeLorenzo, R. J., Sombati, S. and Coulter, D. A., 2000. Effects of topiramate on sustained repetitive firing and spontaneous recurrent seizure discharges in cultured hippocampal neurons. Epilepsia. 41 Suppl 1, S40-44.
Destexhe, A. and Huguenard, J., 2000b. Which formalism to use for modeling voltage-dependent conductances? In: Computational Neuroscience: Realistic Modeling for Experimentalists
CRC Press., Boca Raton. Destexhe, A. and Huguenard, J. R., 2000. Nonlinear thermodynamic models of voltage-
dependent currents. J Comput Neurosci. 9, 259-270. Diss, J. K., Fraser, S. P. and Djamgoz, M. B., 2004. Voltage-gated Na+ channels:
multiplicity of expression, plasticity, functional implications and pathophysiological aspects. Eur Biophys J. 33, 180-193.
Ellerkmann, R. K., Remy, S., Chen, J., Sochivko, D., Elger, C. E., Urban, B. W., Becker, A. and Beck, H., 2003. Molecular and functional changes in voltage-dependent Na(+) channels following pilocarpine-induced status epilepticus in rat dentate granule cells. Neuroscience. 119, 323-333.
Engel, J., Jr., Babb, T. L. and Crandall, P. H., 1989. Surgical treatment of epilepsy: opportunities for research into basic mechanisms of human brain function. Acta Neurochir Suppl (Wien). 46, 3-8.
Escayg, A., MacDonald, B. T., Meisler, M. H., Baulac, S., Huberfeld, G., An-Gourfinkel, I., Brice, A., LeGuern, E., Moulard, B., Chaigne, D., Buresi, C. and Malafosse, A., 2000. Mutations of SCN1A, encoding a neuronal sodium channel, in two families with GEFS+2. Nat Genet. 24, 343-345.
Felts, P. A., Yokoyama, S., Dib-Hajj, S., Black, J. A. and Waxman, S. G., 1997. Sodium channel alpha-subunit mRNAs I, II, III, NaG, Na6 and hNE (PN1): different expression patterns in developing rat nervous system. Brain Res Mol Brain Res. 45, 71-82.

References
111
Franceschetti, S., Taverna, S., Sancini, G., Panzica, F., Lombardi, R. and Avanzini, G., 2000. Protein kinase C-dependent modulation of Na+ currents increases the excitability of rat neocortical pyramidal neurones. J Physiol. 528 Pt 2, 291-304.
French, C. R., Sah, P., Buckett, K. J. and Gage, P. W., 1990. A voltage-dependent persistent sodium current in mammalian hippocampal neurons. J Gen Physiol. 95, 1139-1157.
Fujiwara, T., Sugawara, T., Mazaki-Miyazaki, E., Takahashi, Y., Fukushima, K., Watanabe, M., Hara, K., Morikawa, T., Yagi, K., Yamakawa, K. and Inoue, Y., 2003. Mutations of sodium channel alpha subunit type 1 (SCN1A) in intractable childhood epilepsies with frequent generalized tonic-clonic seizures. Brain. 126, 531-546.
Gastaldi, M., Bartolomei, F., Massacrier, A., Planells, R., Robaglia-Schlupp, A. and Cau, P., 1997. Increase in mRNAs encoding neonatal II and III sodium channel alpha-isoforms during kainate-induced seizures in adult rat hippocampus. Brain Res Mol Brain Res. 44, 179-190.
Gastaldi, M., Robaglia-Schlupp, A., Massacrier, A., Planells, R. and Cau, P., 1998. mRNA coding for voltage-gated sodium channel beta2 subunit in rat central nervous system: cellular distribution and changes following kainate-induced seizures. Neurosci Lett. 249, 53-56.
George, A. L., Jr., 2005. Inherited disorders of voltage-gated sodium channels. J Clin Invest. 115, 1990-1999.
Gibbs, J. W., 3rd, Sombati, S., DeLorenzo, R. J. and Coulter, D. A., 2000. Cellular actions of topiramate: blockade of kainate-evoked inward currents in cultured hippocampal neurons. Epilepsia. 41 Suppl 1, S10-16.
Goddard, G. V., McIntyre, D. C. and Leech, C. K., 1969. A permanent change in brain function resulting from daily electrical stimulation. Exp Neurol. 25, 295-330.
Goldin, A. L., 2001. Resurgence of sodium channel research. Annu Rev Physiol. 63, 871-894.
Goldin, A. L., 2003. Mechanisms of sodium channel inactivation. Curr Opin Neurobiol. 13, 284-290.
Goldin, A. L., Barchi, R. L., Caldwell, J. H., Hofmann, F., Howe, J. R., Hunter, J. C., Kallen, R. G., Mandel, G., Meisler, M. H., Netter, Y. B., Noda, M., Tamkun, M. M., Waxman, S. G., Wood, J. N. and Catterall, W. A., 2000. Nomenclature of voltage-gated sodium channels. Neuron. 28, 365-368.
Goldin, A. L., Snutch, T., Lubbert, H., Dowsett, A., Marshall, J., Auld, V., Downey, W., Fritz, L. C., Lester, H. A., Dunn, R. and et al., 1986. Messenger RNA coding for only the alpha subunit of the rat brain Na channel is sufficient for expression of functional channels in Xenopus oocytes. Proc Natl Acad Sci U S A. 83, 7503-7507.
Gorter, J. A., Goncalves Pereira, P. M., van Vliet, E. A., Aronica, E., Lopes da Silva, F. H. and Lucassen, P. J., 2003. Neuronal cell death in a rat model for mesial temporal lobe epilepsy is induced by the initial status epilepticus and not by later repeated spontaneous seizures. Epilepsia. 44, 647-658.
Gorter, J. A., van Vliet, E. A., Aronica, E., Breit, T., Rauwerda, H., Lopes da Silva, F. H. and Wadman, W. J., 2006. Potential new antiepileptogenic targets indicated by

References
112
microarray analysis in a rat model for temporal lobe epilepsy. J Neurosci. 26, 11083-11110.
Gorter, J. A., van Vliet, E. A., Aronica, E. and Lopes da Silva, F. H., 2002. Long-lasting increased excitability differs in dentate gyrus vs. CA1 in freely moving chronic epileptic rats after electrically induced status epilepticus. Hippocampus. 12, 311-324.
Gulbis, J. M. and Doyle, D. A., 2004. Potassium channel structures: do they conform? Curr Opin Struct Biol. 14, 440-446.
Gustafson, T. A., Clevinger, E. C., O'Neill, T. J., Yarowsky, P. J. and Krueger, B. K., 1993. Mutually exclusive exon splicing of type III brain sodium channel alpha subunit RNA generates developmentally regulated isoforms in rat brain. J Biol Chem. 268, 18648-18653.
Hammarstrom, A. K. and Gage, P. W., 2002. Hypoxia and persistent sodium current. Eur Biophys J. 31, 323-330.
Hartmann, H. A., Colom, L. V., Sutherland, M. L. and Noebels, J. L., 1999. Selective localization of cardiac SCN5A sodium channels in limbic regions of rat brain. Nat Neurosci. 2, 593-595.
Heinemann, U., Draguhn, A., Ficker, E., Stabel, J. and Zhang, C. L., 1994. Strategies for the development of drugs for pharmacoresistant epilepsies. Epilepsia. 35 Suppl 5, S10-21.
Hellier, J. L. and Dudek, F. E., 1999. Spontaneous motor seizures of rats with kainate-induced epilepsy: effect of time of day and activity state. Epilepsy Res. 35, 47-57.
Hellier, J. L., Patrylo, P. R., Buckmaster, P. S. and Dudek, F. E., 1998. Recurrent spontaneous motor seizures after repeated low-dose systemic treatment with kainate: assessment of a rat model of temporal lobe epilepsy. Epilepsy Res. 31, 73-84.
Hille, B., 2001. Ionic channels of excitable membrane. Sinauer, Sunderland, MA, Washington, DC.
Hines, M. L. and Carnevale, N. T., 1997. The NEURON simulation environment. Neural Comput. 9, 1179-1209.
Hodgkin, A. L. and Huxley, A. F., 1952a. The components of membrane conductance in the giant axon of Loligo. J Physiol. 116, 473-496.
Hodgkin, A. L. and Huxley, A. F., 1952b. Currents carried by sodium and potassium ions through the membrane of the giant axon of Loligo. J Physiol. 116, 449-472.
Hodgkin, A. L. and Huxley, A. F., 1952c. The dual effect of membrane potential on sodium conductance in the giant axon of Loligo. J Physiol. 116, 497-506.
Hodgkin, A. L. and Huxley, A. F., 1952d. A quantitative description of membrane current and its application to conduction and excitation in nerve. J Physiol. 117, 500-544.
Hoffman, D. A., Magee, J. C., Colbert, C. M. and Johnston, D., 1997. K+ channel regulation of signal propagation in dendrites of hippocampal pyramidal neurons. Nature. 387, 869-875.
Ilyin, V. I., Hodges, D. D., Whittemore, E. R., Carter, R. B., Cai, S. X. and Woodward, R. M., 2005. V102862 (Co 102862): a potent, broad-spectrum state-dependent blocker of mammalian voltage-gated sodium channels. Br J Pharmacol. 144, 801-812.

References
113
Isom, L. L., 2001. Sodium channel beta subunits: anything but auxiliary. Neuroscientist. 7, 42-54.
Isom, L. L., De Jongh, K. S. and Catterall, W. A., 1994. Auxiliary subunits of voltage-gated ion channels. Neuron. 12, 1183-1194.
Isom, L. L., Ragsdale, D. S., De Jongh, K. S., Westenbroek, R. E., Reber, B. F., Scheuer, T. and Catterall, W. A., 1995. Structure and function of the beta 2 subunit of brain sodium channels, a transmembrane glycoprotein with a CAM motif. Cell. 83, 433-442.
Jeub, M., Beck, H., Siep, E., Ruschenschmidt, C., Speckmann, E. J., Ebert, U., Potschka, H., Freichel, C., Reissmuller, E. and Loscher, W., 2002. Effect of phenytoin on sodium and calcium currents in hippocampal CA1 neurons of phenytoin-resistant kindled rats. Neuropharmacology. 42, 107-116.
Johnston, D., Wu, S. M.S., 1995. Foundations of cellular neurophysiology. MIT Press, Cambridge, Massachusetts.
Kaplan, M. R., Cho, M. H., Ullian, E. M., Isom, L. L., Levinson, S. R. and Barres, B. A., 2001. Differential control of clustering of the sodium channels Na(v)1.2 and Na(v)1.6 at developing CNS nodes of Ranvier. Neuron. 30, 105-119.
Kayano, T., Noda, M., Flockerzi, V., Takahashi, H. and Numa, S., 1988. Primary structure of rat brain sodium channel III deduced from the cDNA sequence. FEBS Lett. 228, 187-194.
Kearney, J. A., Plummer, N. W., Smith, M. R., Kapur, J., Cummins, T. R., Waxman, S. G., Goldin, A. L. and Meisler, M. H., 2001. A gain-of-function mutation in the sodium channel gene Scn2a results in seizures and behavioral abnormalities. Neuroscience. 102, 307-317.
Ketelaars, S. O., Gorter, J. A., van Vliet, E. A., Lopes da Silva, F. H. and Wadman, W. J., 2001. Sodium currents in isolated rat CA1 pyramidal and dentate granule neurones in the post-status epilepticus model of epilepsy. Neuroscience. 105, 109-120.
Kohling, R., 2002. Voltage-gated sodium channels in epilepsy. Epilepsia. 43, 1278-1295. Koopmann, T. T., Bezzina, C. R. and Wilde, A. A., 2006. Voltage-gated sodium channels:
action players with many faces. Ann Med. 38, 472-482. Krzemien, D. M., Schaller, K. L., Levinson, S. R. and Caldwell, J. H., 2000.
Immunolocalization of sodium channel isoform NaCh6 in the nervous system. J Comp Neurol. 420, 70-83.
Kuo, C. C., 1997. Deactivation retards recovery from inactivation in Shaker K+ channels. J Neurosci. 17, 3436-3444.
Kuo, C. C., 1998. A common anticonvulsant binding site for phenytoin, carbamazepine, and lamotrigine in neuronal Na+ channels. Mol Pharmacol. 54, 712-721.
Kuo, C. C. and Bean, B. P., 1994a. Na+ channels must deactivate to recover from inactivation. Neuron. 12, 819-829.
Kuo, C. C. and Bean, B. P., 1994b. Slow binding of phenytoin to inactivated sodium channels in rat hippocampal neurons. Mol Pharmacol. 46, 716-725.
Kuo, C. C., Chen, R. S., Lu, L. and Chen, R. C., 1997. Carbamazepine inhibition of neuronal Na+ currents: quantitative distinction from phenytoin and possible therapeutic implications. Mol Pharmacol. 51, 1077-1083.

References
114
Kuo, C. C. and Lu, L., 1997. Characterization of lamotrigine inhibition of Na+ channels in rat hippocampal neurones. Br J Pharmacol. 121, 1231-1238.
Lampl, I., Schwindt, P. and Crill, W., 1998. Reduction of cortical pyramidal neuron excitability by the action of phenytoin on persistent Na+ current. J Pharmacol Exp Ther. 284, 228-237.
Lang, D. G., Wang, C. M. and Cooper, B. R., 1993. Lamotrigine, phenytoin and carbamazepine interactions on the sodium current present in N4TG1 mouse neuroblastoma cells. J Pharmacol Exp Ther. 266, 829-835.
Lazarowski, A., Sevlever, G., Taratuto, A., Massaro, M. and Rabinowicz, A., 1999. Tuberous sclerosis associated with MDR1 gene expression and drug-resistant epilepsy. Pediatr Neurol. 21, 731-734.
Leite, J. P. and Cavalheiro, E. A., 1995. Effects of conventional antiepileptic drugs in a model of spontaneous recurrent seizures in rats. Epilepsy Res. 20, 93-104.
Lenkowski, P. W., Shah, B. S., Dinn, A. E., Lee, K. and Patel, M. K., 2003. Lidocaine block of neonatal Nav1.3 is differentially modulated by co-expression of beta1 and beta3 subunits. Eur J Pharmacol. 467, 23-30.
Lerche, H., Jurkat-Rott, K. and Lehmann-Horn, F., 2001. Ion channels and epilepsy. Am J Med Genet. 106, 146-159.
Leresche, N., Parri, H. R., Erdemli, G., Guyon, A., Turner, J. P., Williams, S. R., Asprodini, E. and Crunelli, V., 1998. On the action of the anti-absence drug ethosuximide in the rat and cat thalamus. J Neurosci. 18, 4842-4853.
Lindia, J. A. and Abbadie, C., 2003. Distribution of the voltage gated sodium channel Na(v)1.3-like immunoreactivity in the adult rat central nervous system. Brain Res. 960, 132-141.
Liu, G., Yarov-Yarovoy, V., Nobbs, M., Clare, J. J., Scheuer, T. and Catterall, W. A., 2003. Differential interactions of lamotrigine and related drugs with transmembrane segment IVS6 of voltage-gated sodium channels. Neuropharmacology. 44, 413-422.
Llinas, R. R., 1988. The intrinsic electrophysiological properties of mammalian neurons: insights into central nervous system function. Science. 242, 1654-1664.
Lombardo, A. J., Kuzniecky, R., Powers, R. E. and Brown, G. B., 1996. Altered brain sodium channel transcript levels in human epilepsy. Brain Res Mol Brain Res. 35, 84-90.
Loscher, W., 2002. Animal models of epilepsy for the development of antiepileptogenic and disease-modifying drugs. A comparison of the pharmacology of kindling and post-status epilepticus models of temporal lobe epilepsy. Epilepsy Res. 50, 105-123.
Loscher, W. and Potschka, H., 2002. Role of multidrug transporters in pharmacoresistance to antiepileptic drugs. J Pharmacol Exp Ther. 301, 7-14.
Loscher, W. and Schmidt, D., 2002. New horizons in the development of antiepileptic drugs. Epilepsy Res. 50, 3-16.
Lossin, C., Rhodes, T. H., Desai, R. R., Vanoye, C. G., Wang, D., Carniciu, S., Devinsky, O. and George, A. L., Jr., 2003. Epilepsy-associated dysfunction in the voltage-gated neuronal sodium channel SCN1A. J Neurosci. 23, 11289-11295.
Lossin, C., Wang, D. W., Rhodes, T. H., Vanoye, C. G. and George, A. L., Jr., 2002. Molecular basis of an inherited epilepsy. Neuron. 34, 877-884.

References
115
Lothman, E. W., 1996. Basic mechanisms of seizure expression. Epilepsy Res Suppl. 11, 9-16.
Lothman, E. W., Rempe, D. A. and Mangan, P. S., 1995. Changes in excitatory neurotransmission in the CA1 region and dentate gyrus in a chronic model of temporal lobe epilepsy. J Neurophysiol. 74, 841-848.
Lupa, M. T., Krzemien, D. M., Schaller, K. L. and Caldwell, J. H., 1995. Expression and distribution of sodium channels in short- and long-term denervated rodent skeletal muscles. J Physiol. 483 ( Pt 1), 109-118.
Ma, J. Y., Catterall, W. A. and Scheuer, T., 1997. Persistent sodium currents through brain sodium channels induced by G protein betagamma subunits. Neuron. 19, 443-452.
Ma, J. Y., Li, M., Catterall, W. A. and Scheuer, T., 1994. Modulation of brain Na+ channels by a G-protein-coupled pathway. Proc Natl Acad Sci U S A. 91, 12351-12355.
Macdonald, R. L. and Kelly, K. M., 1993. Antiepileptic drug mechanisms of action. Epilepsia. 34 Suppl 5, S1-8.
Macdonald, R. L. and Kelly, K. M., 1994. Mechanisms of action of currently prescribed and newly developed antiepileptic drugs. Epilepsia. 35 Suppl 4, S41-50.
Macdonald, R. L. and Kelly, K. M., 1995. Antiepileptic drug mechanisms of action. Epilepsia. 36 Suppl 2, S2-12.
Magalhaes, L. H., Garcia-Cairasco, N., Massensini, A. R., Doretto, M. C. and Moraes, M. F., 2004. Evidence for augmented brainstem activated forebrain seizures in Wistar Audiogenic Rats subjected to transauricular electroshock. Neurosci Lett. 369, 19-23.
Mantegazza, M., Yu, F. H., Powell, A. J., Clare, J. J., Catterall, W. A. and Scheuer, T., 2005. Molecular determinants for modulation of persistent sodium current by G-protein betagamma subunits. J Neurosci. 25, 3341-3349.
Matsuki, N., Quandt, F. N., Ten Eick, R. E. and Yeh, J. Z., 1984. Characterization of the block of sodium channels by phenytoin in mouse neuroblastoma cells. J Pharmacol Exp Ther. 228, 523-530.
McNamara, J. O., 1999. Emerging insights into the genesis of epilepsy. Nature. 399, A15-22.
Meadows, L. S., Chen, Y. H., Powell, A. J., Clare, J. J. and Ragsdale, D. S., 2002. Functional modulation of human brain Nav1.3 sodium channels, expressed in mammalian cells, by auxiliary beta 1, beta 2 and beta 3 subunits. Neuroscience. 114, 745-753.
Meisler, M. H. and Kearney, J. A., 2005. Sodium channel mutations in epilepsy and other neurological disorders. J Clin Invest. 115, 2010-2017.
Meldrum, B. S., 1996. Update on the mechanism of action of antiepileptic drugs. Epilepsia. 37 Suppl 6, S4-11.
Meldrum, B. S. and Rogawski, M. A., 2007. Molecular targets for antiepileptic drug development. Neurotherapeutics. 4, 18-61.
Merritt, H. H. and Putnam, T. J., 1938. A new series of anticonvulsant drugs tested by experiments on animals. Arch Neurol Psychiatry. 39, 1003-1015.

References
116
Moody, W. J. and Bosma, M. M., 2005. Ion channel development, spontaneous activity, and activity-dependent development in nerve and muscle cells. Physiol Rev. 85, 883-941.
Morgan, K., Stevens, E. B., Shah, B., Cox, P. J., Dixon, A. K., Lee, K., Pinnock, R. D., Hughes, J., Richardson, P. J., Mizuguchi, K. and Jackson, A. P., 2000. beta 3: an additional auxiliary subunit of the voltage-sensitive sodium channel that modulates channel gating with distinct kinetics. Proc Natl Acad Sci U S A. 97, 2308-2313.
Moulard, B., Picard, F., le Hellard, S., Agulhon, C., Weiland, S., Favre, I., Bertrand, S., Malafosse, A. and Bertrand, D., 2001. Ion channel variation causes epilepsies. Brain Res Brain Res Rev. 36, 275-284.
Mulley, J. C., Scheffer, I. E., Petrou, S. and Berkovic, S. F., 2003. Channelopathies as a genetic cause of epilepsy. Curr Opin Neurol. 16, 171-176.
Mulley, J. C., Scheffer, I. E., Petrou, S., Dibbens, L. M., Berkovic, S. F. and Harkin, L. A., 2005. SCN1A mutations and epilepsy. Hum Mutat. 25, 535-542.
Niespodziany, I., Klitgaard, H. and Margineanu, D. G., 2004. Is the persistent sodium current a specific target of anti-absence drugs? Neuroreport. 15, 1049-1052.
Noda, M., Ikeda, T., Kayano, T., Suzuki, H., Takeshima, H., Kurasaki, M., Takahashi, H. and Numa, S., 1986a. Existence of distinct sodium channel messenger RNAs in rat brain. Nature. 320, 188-192.
Noda, M., Ikeda, T., Suzuki, H., Takeshima, H., Takahashi, T., Kuno, M. and Numa, S., 1986b. Expression of functional sodium channels from cloned cDNA. Nature. 322, 826-828.
Noda, M., Shimizu, S., Tanabe, T., Takai, T., Kayano, T., Ikeda, T., Takahashi, H., Nakayama, H., Kanaoka, Y., Minamino, N. and et al., 1984. Primary structure of Electrophorus electricus sodium channel deduced from cDNA sequence. Nature. 312, 121-127.
Noebels, J. L., 1999. Single-gene models of epilepsy. Adv Neurol. 79, 227-238. Numa, S. and Noda, M., 1986. Molecular structure of sodium channels. Ann N Y Acad
Sci. 479, 338-355. Ogata, N. and Ohishi, Y., 2002. Molecular diversity of structure and function of the
voltage-gated Na+ channels. Jpn J Pharmacol. 88, 365-377. Ogiwara, I., Miyamoto, H., Morita, N., Atapour, N., Mazaki, E., Inoue, I., Takeuchi, T.,
Itohara, S., Yanagawa, Y., Obata, K., Furuichi, T., Hensch, T. K. and Yamakawa, K., 2007. Na(v)1.1 localizes to axons of parvalbumin-positive inhibitory interneurons: a circuit basis for epileptic seizures in mice carrying an Scn1a gene mutation. J Neurosci. 27, 5903-5914.
Park, C. C. and Ahmed, Z., 1991. Characterization of sodium current in developing rat diencephalic neurons in serum-free culture. J Neurophysiol. 65, 1011-1021.
Patlak, J., 1991. Molecular kinetics of voltage-dependent Na+ channels. Physiol Rev. 71, 1047-1080.
Pereira, M. B., Freitas, R. L., Assis, M. A., Silva, R. F., Fonteles, M. M., Freitas, R. M. and Takahashi, R. N., 2007. Study pharmacologic of the GABAergic and glutamatergic drugs on seizures and status epilepticus induced by pilocarpine in adult Wistar rats. Neurosci Lett. 419, 253-257.

References
117
Perucca, E., 1997. A pharmacological and clinical review on topiramate, a new antiepileptic drug. Pharmacol Res. 35, 241-256.
Perucca, E., 2005. An introduction to antiepileptic drugs. Epilepsia. 46 Suppl 4, 31-37. Pitsch, J., Schoch, S., Gueler, N., Flor, P. J., van der Putten, H. and Becker, A. J., 2007.
Functional role of mGluR1 and mGluR4 in pilocarpine-induced temporal lobe epilepsy. Neurobiol Dis. 26, 623-633.
Plummer, N. W., Galt, J., Jones, J. M., Burgess, D. L., Sprunger, L. K., Kohrman, D. C. and Meisler, M. H., 1998. Exon organization, coding sequence, physical mapping, and polymorphic intragenic markers for the human neuronal sodium channel gene SCN8A. Genomics. 54, 287-296.
Prasad, A. N., Prasad, C. and Stafstrom, C. E., 1999. Recent advances in the genetics of epilepsy: insights from human and animal studies. Epilepsia. 40, 1329-1352.
Racine, R. J., 1972. Modification of seizure activity by electrical stimulation. II. Motor seizure. Electroencephalogr Clin Neurophysiol. 32, 281-294.
Ragsdale, D. S. and Avoli, M., 1998. Sodium channels as molecular targets for antiepileptic drugs. Brain Res Brain Res Rev. 26, 16-28.
Ragsdale, D. S., McPhee, J. C., Scheuer, T. and Catterall, W. A., 1996. Common molecular determinants of local anesthetic, antiarrhythmic, and anticonvulsant block of voltage-gated Na+ channels. Proc Natl Acad Sci U S A. 93, 9270-9275.
Ragsdale, D. S., Scheuer, T. and Catterall, W. A., 1991. Frequency and voltage-dependent inhibition of type IIA Na+ channels, expressed in a mammalian cell line, by local anesthetic, antiarrhythmic, and anticonvulsant drugs. Mol Pharmacol. 40, 756-765.
Reckziegel, G., Beck, H., Schramm, J., Elger, C. E. and Urban, B. W., 1998. Electrophysiological characterization of Na+ currents in acutely isolated human hippocampal dentate granule cells. J Physiol. 509 ( Pt 1), 139-150.
Regesta, G. and Tanganelli, P., 1999. Clinical aspects and biological bases of drug-resistant epilepsies. Epilepsy Res. 34, 109-122.
Remy, S. and Beck, H., 2006. Molecular and cellular mechanisms of pharmacoresistance in epilepsy. Brain. 129, 18-35.
Remy, S., Gabriel, S., Urban, B. W., Dietrich, D., Lehmann, T. N., Elger, C. E., Heinemann, U. and Beck, H., 2003a. A novel mechanism underlying drug resistance in chronic epilepsy. Ann Neurol. 53, 469-479.
Remy, S., Urban, B. W., Elger, C. E. and Beck, H., 2003b. Anticonvulsant pharmacology of voltage-gated Na+ channels in hippocampal neurons of control and chronically epileptic rats. Eur J Neurosci. 17, 2648-2658.
Ritchie, J. M. and Rogart, R. B., 1977. The binding of saxitoxin and tetrodotoxin to excitable tissue. Rev Physiol Biochem Pharmacol. 79, 1-50.
Riviello, J. J., 2003. Classification of seizures and epilepsy. Curr Neurol Neurosci Rep. 3, 325-331.
Rizzi, M., Caccia, S., Guiso, G., Richichi, C., Gorter, J. A., Aronica, E., Aliprandi, M., Bagnati, R., Fanelli, R., D'Incalci, M., Samanin, R. and Vezzani, A., 2002. Limbic seizures induce P-glycoprotein in rodent brain: functional implications for pharmacoresistance. J Neurosci. 22, 5833-5839.
Rogawski, M. A., 2006. Molecular targets versus models for new antiepileptic drug discovery. Epilepsy Res. 68, 22-28.

References
118
Rogawski, M. A. and Loscher, W., 2004a. The neurobiology of antiepileptic drugs. Nat Rev Neurosci. 5, 553-564.
Rogawski, M. A. and Loscher, W., 2004b. The neurobiology of antiepileptic drugs for the treatment of nonepileptic conditions. Nat Med. 10, 685-692.
Rogawski, M. A. and Porter, R. J., 1990. Antiepileptic drugs: pharmacological mechanisms and clinical efficacy with consideration of promising developmental stage compounds. Pharmacol Rev. 42, 223-286.
Sarao, R., Gupta, S. K., Auld, V. J. and Dunn, R. J., 1991. Developmentally regulated alternative RNA splicing of rat brain sodium channel mRNAs. Nucleic Acids Res. 19, 5673-5679.
Schaller, K. L., Krzemien, D. M., Yarowsky, P. J., Krueger, B. K. and Caldwell, J. H., 1995. A novel, abundant sodium channel expressed in neurons and glia. J Neurosci. 15, 3231-3242.
Scheuer, T., Auld, V. J., Boyd, S., Offord, J., Dunn, R. and Catterall, W. A., 1990. Functional properties of rat brain sodium channels expressed in a somatic cell line. Science. 247, 854-858.
Schuetz, J. D., Connelly, M. C., Sun, D., Paibir, S. G., Flynn, P. M., Srinivas, R. V., Kumar, A. and Fridland, A., 1999. MRP4: A previously unidentified factor in resistance to nucleoside-based antiviral drugs. Nat Med. 5, 1048-1051.
Schwarz, J. R. and Grigat, G., 1989. Phenytoin and carbamazepine: potential- and frequency-dependent block of Na currents in mammalian myelinated nerve fibers. Epilepsia. 30, 286-294.
Segal, M. M., 2002. Sodium channels and epilepsy electrophysiology. Novartis Found Symp. 241, 173-180; discussion 180-178, 226-132.
Segal, M. M. and Douglas, A. F., 1997. Late sodium channel openings underlying epileptiform activity are preferentially diminished by the anticonvulsant phenytoin. J Neurophysiol. 77, 3021-3034.
Shah, B. S., Stevens, E. B., Pinnock, R. D., Dixon, A. K. and Lee, K., 2001. Developmental expression of the novel voltage-gated sodium channel auxiliary subunit beta3, in rat CNS. J Physiol. 534, 763-776.
Shank, R. P., Gardocki, J. F., Streeter, A. J. and Maryanoff, B. E., 2000. An overview of the preclinical aspects of topiramate: pharmacology, pharmacokinetics, and mechanism of action. Epilepsia. 41 Suppl 1, S3-9.
Sisodiya, S. M., 2003. Mechanisms of antiepileptic drug resistance. Curr Opin Neurol. 16, 197-201.
Sisodiya, S. M., Lin, W. R., Squier, M. V. and Thom, M., 2001. Multidrug-resistance protein 1 in focal cortical dysplasia. Lancet. 357, 42-43.
Sloviter, R. S., 1994. The functional organization of the hippocampal dentate gyrus and its relevance to the pathogenesis of temporal lobe epilepsy. Ann Neurol. 35, 640-654.
Smith, R. D. and Goldin, A. L., 1998. Functional analysis of the rat I sodium channel in xenopus oocytes. J Neurosci. 18, 811-820.
Spadoni, F., Hainsworth, A. H., Mercuri, N. B., Caputi, L., Martella, G., Lavaroni, F., Bernardi, G. and Stefani, A., 2002. Lamotrigine derivatives and riluzole inhibit INa,P in cortical neurons. Neuroreport. 13, 1167-1170.

References
119
Spampanato, J., Kearney, J. A., de Haan, G., McEwen, D. P., Escayg, A., Aradi, I., Macdonald, B. T., Levin, S. I., Soltesz, I., Benna, P., Montalenti, E., Isom, L. L., Goldin, A. L. and Meisler, M. H., 2004. A Novel Epilepsy Mutation in the Sodium Channel SCN1A Identifies a Cytoplasmic Domain for beta Subunit Interaction. J Neurosci. 24, 10022-10034.
Stefan, H. and Feuerstein, T. J., 2007. Novel anticonvulsant drugs. Pharmacol Ther. 113, 165-183.
Steinlein, O. K., 2002. Channelopathies can cause epilepsy in man. Eur J Pain. 6 Suppl A, 27-34.
Stuart, G., 1999. Voltage-activated sodium channels amplify inhibition in neocortical pyramidal neurons. Nat Neurosci. 2, 144-150.
Stuart, G. and Sakmann, B., 1995. Amplification of EPSPs by axosomatic sodium channels in neocortical pyramidal neurons. Neuron. 15, 1065-1076.
Sugawara, T., Tsurubuchi, Y., Agarwala, K. L., Ito, M., Fukuma, G., Mazaki-Miyazaki, E., Nagafuji, H., Noda, M., Imoto, K., Wada, K., Mitsudome, A., Kaneko, S., Montal, M., Nagata, K., Hirose, S. and Yamakawa, K., 2001. A missense mutation of the Na+ channel alpha II subunit gene Na(v)1.2 in a patient with febrile and afebrile seizures causes channel dysfunction. Proc Natl Acad Sci U S A. 98, 6384-6389.
Sun, G. C., Werkman, T. R. and Wadman, W. J., 2006. Kinetic changes and modulation by carbamazepine on voltage-gated sodium channels in rat CA1 neurons after epilepsy. Acta Pharmacol Sin. 27, 1537-1546.
Taddese, A. and Bean, B. P., 2002. Subthreshold sodium current from rapidly inactivating sodium channels drives spontaneous firing of tuberomammillary neurons. Neuron. 33, 587-600.
Taverna, S., Mantegazza, M., Franceschetti, S. and Avanzini, G., 1998. Valproate selectively reduces the persistent fraction of Na+ current in neocortical neurons. Epilepsy Res. 32, 304-308.
Taverna, S., Sancini, G., Mantegazza, M., Franceschetti, S. and Avanzini, G., 1999. Inhibition of transient and persistent Na+ current fractions by the new anticonvulsant topiramate. J Pharmacol Exp Ther. 288, 960-968.
Taylor, C. P., 1993. Na+ currents that fail to inactivate. Trends Neurosci. 16, 455-460. Taylor, C. P. and Meldrum, B. S., 1995. Na+ channels as targets for neuroprotective
drugs. Trends Pharmacol Sci. 16, 309-316. Thimmapaya, R., Neelands, T., Niforatos, W., Davis-Taber, R. A., Choi, W., Putman, C.
B., Kroeger, P. E., Packer, J., Gopalakrishnan, M., Faltynek, C. R., Surowy, C. S. and Scott, V. E., 2005. Distribution and functional characterization of human Nav1.3 splice variants. Eur J Neurosci. 22, 1-9.
Thomas, P. and Smart, T. G., 2005. HEK293 cell line: a vehicle for the expression of recombinant proteins. J Pharmacol Toxicol Methods. 51, 187-200.
Tishler, D. M., Weinberg, K. I., Hinton, D. R., Barbaro, N., Annett, G. M. and Raffel, C., 1995. MDR1 gene expression in brain of patients with medically intractable epilepsy. Epilepsia. 36, 1-6.
Trimmer, J. S. and Rhodes, K. J., 2004. Localization of voltage-gated ion channels in mammalian brain. Annu Rev Physiol. 66, 477-519.

References
120
Ulbricht, W., 2005. Sodium channel inactivation: molecular determinants and modulation. Physiol Rev. 85, 1271-1301.
van Vliet, E. A., Aronica, E., Redeker, S. and Gorter, J. A., 2004. Expression and cellular distribution of major vault protein: a putative marker for pharmacoresistance in a rat model for temporal lobe epilepsy. Epilepsia. 45, 1506-1516.
Vanoye, C. G., Lossin, C., Rhodes, T. H. and George, A. L., Jr., 2006. Single-channel properties of human NaV1.1 and mechanism of channel dysfunction in SCN1A-associated epilepsy. J Gen Physiol. 127, 1-14.
Virginio, C. and Cherubini, E., 1995. Functional expression of voltage dependent sodium channels in Xenopus oocytes injected with mRNA from neonatal or adult rat brain. Brain Res Dev Brain Res. 87, 153-159.
Vreugdenhil, M., Faas, G. C. and Wadman, W. J., 1998. Sodium currents in isolated rat CA1 neurons after kindling epileptogenesis. Neuroscience. 86, 99-107.
Vreugdenhil, M., Hoogland, G., van Veelen, C. W. and Wadman, W. J., 2004. Persistent sodium current in subicular neurons isolated from patients with temporal lobe epilepsy. Eur J Neurosci. 19, 2769-2778.
Vreugdenhil, M. and Wadman, W. J., 1992. Enhancement of calcium currents in rat hippocampal CA1 neurons induced by kindling epileptogenesis. Neuroscience. 49, 373-381.
Vreugdenhil, M. and Wadman, W. J., 1999. Modulation of sodium currents in rat CA1 neurons by carbamazepine and valproate after kindling epileptogenesis. Epilepsia. 40, 1512-1522.
Wadman, W. J., Min, R. and Sun, G. C., 2005. Sodium current properties in different models of epilepsy. In: Corcoran M, Moshe L, eds. Kindling 6. Amsterdam: Springer, 61-70.
Wallace, R. H., Wang, D. W., Singh, R., Scheffer, I. E., George, A. L., Jr., Phillips, H. A., Saar, K., Reis, A., Johnson, E. W., Sutherland, G. R., Berkovic, S. F. and Mulley, J. C., 1998. Febrile seizures and generalized epilepsy associated with a mutation in the Na+-channel beta1 subunit gene SCN1B. Nat Genet. 19, 366-370.
Waxman, S. G., 2007. Channel, neuronal and clinical function in sodium channelopathies: from genotype to phenotype. Nat Neurosci. 10, 405-409.
Waxman, S. G., Kocsis, J. D. and Black, J. A., 1994. Type III sodium channel mRNA is expressed in embryonic but not adult spinal sensory neurons, and is reexpressed following axotomy. J Neurophysiol. 72, 466-470.
Weiss, J., Kerpen, C. J., Lindenmaier, H., Dormann, S. M. and Haefeli, W. E., 2003. Interaction of antiepileptic drugs with human P-glycoprotein in vitro. J Pharmacol Exp Ther. 307, 262-267.
Westenbroek, R. E., Merrick, D. K. and Catterall, W. A., 1989. Differential subcellular localization of the RI and RII Na+ channel subtypes in central neurons. Neuron. 3, 695-704.
Whitaker, W. R., Clare, J. J. and Emson, P. C., 1999. Differential distribution of voltage-gated sodium channel alpha- and beta-subunits in human brain. Ann N Y Acad Sci. 868, 88-92.
Whitaker, W. R., Clare, J. J., Powell, A. J., Chen, Y. H., Faull, R. L. and Emson, P. C., 2000. Distribution of voltage-gated sodium channel alpha-subunit and beta-

References
121
subunit mRNAs in human hippocampal formation, cortex, and cerebellum. J Comp Neurol. 422, 123-139.
Whitaker, W. R., Faull, R. L., Dragunow, M., Mee, E. W., Emson, P. C. and Clare, J. J., 2001a. Changes in the mRNAs encoding voltage-gated sodium channel types II and III in human epileptic hippocampus. Neuroscience. 106, 275-285.
Whitaker, W. R., Faull, R. L., Waldvogel, H. J., Plumpton, C. J., Emson, P. C. and Clare, J. J., 2001b. Comparative distribution of voltage-gated sodium channel proteins in human brain. Brain Res Mol Brain Res. 88, 37-53.
White, H. S., Brown, S. D., Woodhead, J. H., Skeen, G. A. and Wolf, H. H., 1997. Topiramate enhances GABA-mediated chloride flux and GABA-evoked chloride currents in murine brain neurons and increases seizure threshold. Epilepsy Res. 28, 167-179.
Willow, M., Gonoi, T. and Catterall, W. A., 1985. Voltage clamp analysis of the inhibitory actions of diphenylhydantoin and carbamazepine on voltage-sensitive sodium channels in neuroblastoma cells. Mol Pharmacol. 27, 549-558.
Wu, L., Nishiyama, K., Hollyfield, J. G. and Wang, Q., 2002. Localization of Nav1.5 sodium channel protein in the mouse brain. Neuroreport. 13, 2547-2551.
Wuarin, J. P. and Dudek, F. E., 1996. Electrographic seizures and new recurrent excitatory circuits in the dentate gyrus of hippocampal slices from kainate-treated epileptic rats. J Neurosci. 16, 4438-4448.
Xie, X., Dale, T. J., John, V. H., Cater, H. L., Peakman, T. C. and Clare, J. J., 2001. Electrophysiological and pharmacological properties of the human brain type IIA Na+ channel expressed in a stable mammalian cell line. Pflugers Arch. 441, 425-433.
Xie, X., Lancaster, B., Peakman, T. and Garthwaite, J., 1995. Interaction of the antiepileptic drug lamotrigine with recombinant rat brain type IIA Na+ channels and with native Na+ channels in rat hippocampal neurones. Pflugers Arch. 430, 437-446.
Yamakawa, K., 2006. Na channel gene mutations in epilepsy--the functional consequences. Epilepsy Res. 70 Suppl 1, S218-222.
Yang, Y. C. and Kuo, C. C., 2002. Inhibition of Na(+) current by imipramine and related compounds: different binding kinetics as an inactivation stabilizer and as an open channel blocker. Mol Pharmacol. 62, 1228-1237.
Yu, F. H. and Catterall, W. A., 2003. Overview of the voltage-gated sodium channel family. Genome Biol. 4, 207.
Yu, F. H., Mantegazza, M., Westenbroek, R. E., Robbins, C. A., Kalume, F., Burton, K. A., Spain, W. J., McKnight, G. S., Scheuer, T. and Catterall, W. A., 2006. Reduced sodium current in GABAergic interneurons in a mouse model of severe myoclonic epilepsy in infancy. Nat Neurosci. 9, 1142-1149.
Yu, F. H., Westenbroek, R. E., Silos-Santiago, I., McCormick, K. A., Lawson, D., Ge, P., Ferriera, H., Lilly, J., DiStefano, P. S., Catterall, W. A., Scheuer, T. and Curtis, R., 2003. Sodium channel beta4, a new disulfide-linked auxiliary subunit with similarity to beta2. J Neurosci. 23, 7577-7585.
Yu, F. H., Yarov-Yarovoy, V., Gutman, G. A. and Catterall, W. A., 2005. Overview of molecular relationships in the voltage-gated ion channel superfamily. Pharmacol Rev. 57, 387-395.

References
122
Yuen, A. W., 1994. Lamotrigine: a review of antiepileptic efficacy. Epilepsia. 35 Suppl 5, S33-36.
Zhang, L., Ong, W. Y. and Lee, T., 1999. Induction of P-glycoprotein expression in astrocytes following intracerebroventricular kainate injections. Exp Brain Res. 126, 509-516.
Zhang, X., Velumian, A. A., Jones, O. T. and Carlen, P. L., 2000. Modulation of high-voltage-activated calcium channels in dentate granule cells by topiramate. Epilepsia. 41 Suppl 1, S52-60.
Zhao, P., Xue, J., Gu, X. Q., Haddad, G. G. and Xia, Y., 2005. Intermittent hypoxia modulates Na+ channel expression in developing mouse brain. Int J Dev Neurosci. 23, 327-333.
Zona, C., Ciotti, M. T. and Avoli, M., 1997. Topiramate attenuates voltage-gated sodium currents in rat cerebellar granule cells. Neurosci Lett. 231, 123-126.

NEDERLANDSE SAMENVATTING
Spanningsafhankelijk ionkanalen zijn eiwitmoleculen die aanwezig zijn in de membraan van “exciteerbare” cellen, zoals b.v. zenuwcellen (neuronen) en spiercellen. Deze ionkanalen zijn selectief doorlaatbaar voor specifieke ionen zoals Na+ (natrium), K+ (kalium), Ca2+ (calcium) of Cl- (chloride). De toestand van deze ionkanalen (open of dicht) wordt geregeld door de spanning over de membraan, terwijl de geleidbaarheid van de ionkanalen ook weer die spanning bepaalt. Dankzij deze wederzijdse afhankelijkheid kunnen exciteerbare cellen zogenaamde actiepotentialen genereren. Actiepotentialen zijn kortstondige potentiaalveranderingen (~1 ms) die zich razendsnel over de membraan kunnen verplaatsen (tot wel 100 m/s). Zij coderen de informatie in het zenuwstelsel. Vooral de spanningsafhankelijke natrium- en kaliumkanalen zijn betrokken bij het genereren van deze “alles-of-niets” actiepotentialen (zie Fig. 1 van de Algemene Inleiding). De rol van de spanningsafhankelijke natriumkanalen in de exciteerbare membraan van neuronen is het op gang brengen van de actiepotentiaal. Een verlaging van de membraanspanning opent de natriumkanalen, maar de opening van natrium kanalen verlaagt op zijn beurt ook weer de membraanspanning. Dit leidt tot een sneeuwbal effect, waarbij de actiepotentiaal razendsnel zijn maximale waarde bereikt. Gelukkig zal het natriumkanaal bij deze potentiaal snel inactiveren, terwijl de gedepolariseerde potentiaal tevens de kaliumkanalen (langzaam) opent: twee effecten die ervoor zorgen dat de potentiaal uiteindelijk weer zijn oorspronkelijke waarde bereikt (repolariseert). Deze eigenschappen van het natriumkanaal zorgen ervoor dat zij hoofdrolspelers van neuronale exciteerbaarheid zijn en daardoor betrokken zijn bij bijna alle processen die neuronale exciteerbaarheid beïnvloeden. Het natriumkanaal is een opmerkelijk voorbeeld van succesvolle evolutie: aanwezig in een nauwelijks variërende moleculaire vorm (Kader 1) in alle zenuwstelsels (maar ook in perifere weefsels als b.v. spieren), blijkbaar geperfectioneerd om het basale signaal voor neuronale communicatie te genereren. In dit proefschrift hebben we ons geconcentreerd op verschillende aspecten van de functionele rol van natriumkanalen bij epilepsie, en in het bijzonder op de vraag of subtiele verschillen in de eigenschappen en expressie van de porievormende α-subunit van het natriumkanaal farmacologische consequenties hebben voor de potentiële behandeling van farmacoresistente vormen van epilepsie. Natriumstromen en epilepsie Epilepsie is een manifestatie van ontregelde prikkelbaarheid in de hersenen. Tijdens een epileptische aanval zijn grote groepen neuronen gelijktijdig actief waarbij ze met een hoge frequentie actiepotentialen genereren. Dit proefschrift gaat niet in op epileptogenese, het proces dat leidt tot de (vaak erg langzame) overgang van “normale” hersenen naar “epileptische” hersenen. Deze (voor zover bekend) onomkeerbare overgang wordt gekenmerkt door een sterke kans op het ontstaan van epileptische aanvallen. In het kader van ons onderzoek moeten we benadrukken dat aanvallen niet een unieke eigenschap zijn van epileptische hersenen, maar dat ze in alle hersenen kunnen ontstaan onder “geschikt” gekozen condities. Het verschil tussen normale hersenen en epileptische hersenen zit in de kans dat een epileptische aanval optreedt: een extreem

Nederlandse Samenvatting
124
Kader 1 Moleculaire eigenschappen van het natriumkanaal De neuronale natriumkanaaleiwitten bestaan uit een porievormende α-subunit geassocieerd met β-subunits. Hoewel β subunits (tot op heden zijn vier typen geïdentificeerd: β1 tot en met β4) de (inactivatie-) eigenschappen van het kanaal kunnen beïnvloeden, is expressie van alleen de α-subunit voldoende voor de vorming van functionele natriumkanalen. Van de tien tot op heden bekende natriumkanaal α-subunits vormen de NaV1.1, NaV1.2, NaV1.3 en NaV1.6 α-subunits de meest prominente natriumkanalen in de hersenen. Daarnaast coderen de NaV1.2 en NaV1.3 genen voor twee isovormen: A (voor “adult”) en N (voor “neonatal”), resultaat van de exlusieve splitsing van één enkel exon. Deze splitsing wordt gereguleerd gedurende de ontwikkeling.
Kinetische eigenschappen van het natriumkanaal
Na+Na+
Na+
Na+
Na+
Na+
Na+
Na+
Na+
Na+
Na+
a b c
Na+Na+Na+Na+
Na+Na+
Na+Na+
Na+Na+
Na+Na+
Na+Na+
Na+Na+
Na+Na+
Na+Na+
Na+Na+
a b c
Een kleine membraandepolarisatie (positiever worden van de membraan) zorgt voor een snelle activatie van het kanaal (a), waarna de inwaartse natriuminstroom het membraan verder depolariseert. Bij een redelijk gedepolariseerde membraanpotentiaal sluit inactivatie (b) het kanaal en, nog belangrijker, voorkomt heropening . Een voldoende lange en negatieve membraanhyperpolarisatie (negatiever worden van de membraan) heft de inactivatie op (c) waarna het kanaal weer beschikbaar komt voor activatie. Inactivatie zorgt ervoor dat de cel refractair wordt tijdens langere depolarisaties, wat de maximale vuurfrequentie beperkt. Dit voorkomt het wegvallen van iongradiënten, een proces dat kan leiden tot celdood. Er zijn twee typen natriumstromen: • De klassieke snelle natriumstroom, waarvan de kinetiek als eerste werd beschreven door Hodgkin
en Huxley in hun beroemde ionkanaalmodel, een theorie die succesvolle toepassingen heeft voor de beschrijving van de meeste andere voltage-afhankelijke ionstromen (voornamelijk calcium en kalium).
• de “persistente” natriumstroom, die vergelijkbare activatie-eigenschappen heeft als de snelle stroom, maar geen inactivatie ondergaat. Ondanks dat deze stroom in amplitude vele malen kleiner is dan de snelle natriumstroom, zorgt de permanente activatie ervoor dat deze stroom toch belangrijke consequenties kan hebben voor de membraanpotentiaal en prikkelbaarheid van de cel. Het is niet duidelijk of deze persistente stroom een uniek natriumkanaal is of een speciale activiteitstoestand van het klassieke natriumkanaal.
zeldzaam fenomeen in normale hersenen, maar welke tot wel 100 keer per dag in epileptische hersenen kan optreden. Dit suggereert dat, tot op zekere hoogte, aanvallen gerelateerd zijn aan unieke moleculaire componenten die alleen in epileptische hersenen aanwezig zijn. Eén van de manieren om epileptische aanvallen te bestrijden is het verkleinen van de kans op het sterk gesynchroniseerde vuren van actiepotentialen, althans met hoge frequenties. Dit is een belangrijke eigenschap van veel anti-epileptische medicijnen (AEM), in ieder geval van die AEM die aangrijpen op het natriumkanaal. Dergelijke AEM blokkeren voltage-afhankelijke natriumkanalen door met relatieve hoge affiniteit te binden aan geïnactiveerde kanalen (t.o.v. de affiniteit voor geopenden of gesloten kanalen). Het AEM “stabiliseert” als het ware het kanaal in de geïnactiveerde toestand, waarin het kanaal niet in staat is stroom te geleiden. De geïnactiveerde toestand

Nederlandse Samenvatting
125
van het kanaal (zie Kader 1) ontstaat vooral gedurende periodes van hoog-frequente activiteit, zoals tijdens epileptische aanvallen. Deze “activiteitsafhankelijke” blokkering van de natriumkanalen beperkt het optreden van synchrone en hoogfrequente ontladingen, zonder daarbij de “normale” activiteit te onderdrukken. Natuurlijk is het belangrijk te realiseren dat een succesvolle behandeling met een AEM niet per se ingrijpt op de daadwerkelijke oorzaak van de verhoogde prikkelbaarheid. Met andere woorden, het feit dat we effectief (althans bij een groot aantal van de patiënten) epileptische aanvallen kunnen bestrijden door een modulatie van natriumkanalen, betekent niet dat natriumkanaalafwijkingen epilepsie veroorzaken. Dit verklaart misschien ook de grote variabiliteit in de behandelings-effectiviteit van een AEM voor verschillende epilepsiesyndromen. Er bestaan een groot aantal verschillende epilepsiesyndromen, allemaal leidend tot electromyografische aanvallen, maar ze kunnen ontstaan vanuit andere moleculaire condities. De effectiviteit van een AEM kan sterk variëren in zulke situaties. Toch wordt de mogelijke rol van het natriumkanaal in epilepsie aannemelijker door het feit dat natriumkanaalmutaties vaak leiden tot epileptische condities en een aantal van de genetische epilepsiemodellen (allemaal gekoppeld aan aparte klinische patiënt-groepen) zijn gebaseerd op zulke vastgestelde mutaties (Tabel 1). Tabel 1. Genen en natriumkanalen geassocieerd met epilepsiesyndromen of diermodellen voor epilepsie. Gen Natriumkanaal subunit Epilepsievorm SCN1A NaV1.1α Gegeneraliseerde epilepsie met koorts aanvallen
Zware juveniele myoclonische epilepsie SCN2A NaV1.2α Diverse epilepsiesyndromen SCN1B NaV β1 Diverse epilepsiesyndromen SCN5A NaV1.5α Kainaat-geinduceerde aanvallen (diermodel)
Belangrijk zijn de aanwijzingen dat (zeer) lokale veranderingen in neuronale natriumkanaalsamenstellingen betrokken kunnen zijn bij epilepsie. De α- en β-subunits van de voltage-afhankelijke natriumkanalen hebben specifieke expressiepatronen in de hersenen, welke kunnen veranderen in reactie op beschadigende invloeden of andere signalen. Hierdoor kan het voor effectieve epilepsiebehandeling nodig zijn om een specifieke AEM-kanaalsubunit interactie te hebben, die sterk afhankelijk is van de natriumkanaalsamenstelling in het epileptische weefsel (wat kan afwijken van het gezonde weefsel). Veel van de AEM behandelen relatief effectief de genetische epilepsiesyndromen, maar geen van hen compenseert volledig voor de veranderingen die het gevolg zijn van de genetische afwijking, opnieuw een voorbeeld dat oorzaak en behandelpunt kunnen verschillen. Farmacoresistentie De AEM hebben de opmerkelijke eigenschap te beschermen tegen epileptische aanvallen, met amper een verstorend effect op het normaal functioneren van het zenuwstelsel. Naast medicijnen die aangrijpen op natriumkanalen, zijn er ook medicijnen die epilepsie bestrijden door een interactie met voltage-afhankelijke calciumkanalen of glutamaat- of GABAA (γ-aminobutyric acid, type A) receptoren. We zullen niet ingaan op deze stoffen, maar ons beperken tot AEM die aangrijpen op het natriumkanaal. Voor de meeste epilepsiepatiënten kan een bevredigende controle over de aanvallen worden verkregen

Nederlandse Samenvatting
126
met AEM, maar een flink aantal patiënten (~ 30%) blijft aanvallen houden na zorgvuldig geoptimaliseerde medicatie. Er zijn momenteel twee hypotheses die trachten te verklaren welke mechanismen ten grondslag liggen aan het fenomeen farmacoresistentie: de “transporter” en “target” hypotheses (zie Kader 2). Ondanks een gebrekkige definitie voor de termen “farmacoresistent” of “medisch refractair” die voor deze patiëntcategorie wordt gebruikt, beschouwen de meeste artsen een epilepsie farmacoresistent als geen van de twee à drie meestgebruikte AEM voor een epilepsiesyndroom effectief zijn. Dus de belangrijkste karakteristiek van patiënten met farmacoresistente epilepsie is onbehandelbaarheid met de meeste, en vaak alle, AEM.
Het onderwerp van dit proefschrift Het epilepsieprobleem proberen te reduceren tot een enkel probleem met één bepaald ionkanaal is zeer waarschijnlijk een veel te simpele benadering. Een paar epilepsievormen ontstaan door een enkele mutatie in een ionkanaal of receptor, maar deze zijn zeer zeldzaam en eerder uitzondering dan regel. De beschikbare literatuur maakt ook duidelijk dat er een groot aantal verschillende moleculen in verband kan worden gebracht met epilepsie en/of epileptogenese. Er zal zeker een rol zijn voor verschillende typen calcium- en kaliumkanalen. GABA- en glutamaatreceptoren worden in verband gebracht met verscheidene epilepsiesyndromen en er zijn tevens aanwijzingen dat neuropeptiden een rol spelen. Desalniettemin, in veel gevallen van epilepsie vinden we veranderingen in natriumstromen. Dit leidt tot minimaal twee vervolgvragen, welke onderwerp zijn geweest van het hier beschreven promotie-onderzoek: 1) Hoe ontstaan deze natriumstroomveranderingen en wat zijn de onderliggende
moleculaire mechanismen? 2) Wat zijn de farmacologische consequenties van de veranderingen in natriumstromen
(en/of de onderliggende mechanismen)?
Kader 2 Verklarende hypothesen voor farmacoresistentie 1) De “transporter” hypothese Een verminderde toegang voor AEM tot het centrale zenuwstelsel veroorzaakt farmacoresistentie. De verminderde toegang kan het resultaat zijn van een verhoogde expressie of versterkt functioneren van zogenaamde multidrugtransporters in de hersenen. Deze transporters (in het bijzonder de P-glycoeiwitten) zijn aanwezig in de bloed-hersen barriëre en reguleren de intraparenchymale concentraties van veel stoffen, waaronder AEM. Dit laatste impliceert dat een verhoogd aantal/functioneren van deze transportereiwitten effectief AEM weghaalt uit de hersenen, wat de hersenconcentratie van deze stoffen en dus anti-epileptische effectiviteit, verlaagt. 2) De “target” hypothese Epilepsie-gerelateerde genetische of functionele aanpassingen van de aangrijpingspunten (target) voor AEM, b.v. de receptor of het ionkanaal, verlagen de gevoeligheid voor en effectiviteit van AEM. Een veranderde natriumkanaalsamenstelling in epileptisch weefsel is in overeenstemming met deze hypothese. N.B. De twee hypothesen sluiten elkaar niet uit, beide situaties kunnen parallel optreden.

Nederlandse Samenvatting
127
Natriumstromen in experimentele diermodellen voor epilepsie Het onderzoek beschreven in dit proefschrift bekeek o.m. de natriumkanalen in het experimentele epilepsie kainaat diermodel (Hoofdstukken 2 en 5). In hippocampus CA1 neuronen in dit diermodel (rat) werd een verschuiving in hyperpolariserende richting van zowel de activatie- als de inactivatiefunctie van het natriumkanaal gevonden. Een kleine verschuiving (weliswaar van variabele grootte) van de inactivatiefunctie in depolariserende richting is gevonden in verschillende experimentele epilepsiemodellen, een indicatie dat de zogenaamde ‘window’stroom substantieel is toegenomen na epileptogenese en dat het voltagebereik ervan is verschoven in een richting die het effect op prikkelbaarheid versterkt. We concluderen dat in veel situaties epileptogenese kan leiden tot subtiele (en variabele) veranderingen in eigenschappen van natriumstromen met mogelijk consequenties voor de prikkelbaarheid. Deze conclusie wordt ondersteund door twee feiten: i. Patiënten met refractaire temporale kwab-epilepsie, wiens aanvallen niet beheerst kunnen worden met AEM, ondergaan soms een operatie, waarbij het weefsel met de focus van de aanvallen wordt verwijderd. Analyse van de natriumstromen in neuronen uit dit weefsel, met alle beperkingen voor het vinden van adequate controles, laat ook variabele responsen zien. ii. Het tweede argument wordt geleverd door in-situ hybrydisatiestudies, welke suggereren dat er veranderingen optreden in de moleculaire natriumkanaalsamenstelling in epileptisch hersenweefsel. Een verandering in de natriumkanaal α-subunitsamenstelling (de expressie van NaV1.3 mRNA was hoger dan NaV1.2 mRNA) werd gevonden in de hippocampus van de (kainaat-geïnduceerde) epileptische rat, evenals in epileptische patiënten. Daarnaast is beschreven dat expressie van neonatale isovormen van de NaV1.2 en NaV1.3 α-subunits geïnduceerd werd in de hippocampus van volwassen ratten door epileptische aanvallen. Deze resultaten duiden er op dat een verandering in α-subunitsamenstelling van voltage-afhankelijk natriumkanalen een belangrijke rol kan spelen bij epilepsie en epileptogenese. Ontwikkeling Voordat een uitgebreide kwantificatie van α-subunitfarmacologie werd gedaan, wilden we het mogelijke succes hiervan testen in een preparaat waarvan bekend is dat er grote verschillen in natriumkanaalsubunits bestaan. De vele studies in rattenhersenen hebben aangetoond dat natriumkanalen specifieke expressiepatronen hebben tijdens verschillende ontwikkelingsstadia. De NaV1.2 subunit is overvloedig aanwezig tijdens alle ontwikkelingsstadia; NaV1.1 en NaV1.6 subunitexpressie neemt toe na de geboorte, terwijl de NaV1.3 subunit voornamelijk tot expressie komt tussen laat-embryonale en vroeg-postnatale tijdspunten. Maar recentere studies toonden echter ook NaV1.3 expressie aan in volwassen hersenweefsel. In Hoofdstuk 4 werden voltage-afhankelijke natriumstromen gemeten in acuut gedissocieerde CA1 hippocampus neuronen van neonatale (P2-4) en volwassen ratten (P36-41). In neonatale neuronen is er een lagere dichtheid van voltage-afhankelijke natriumkanalen aanwezig in de membraan dan in volwassen neuronen. Samen met een verschoven steady-state inactivatiefunctie in hyperpolariserende richting en een langzamer herstel van inactivatie, resulteert dit een verminderde prikkelbaarheid van neonatale CA1 neuronen in vergelijking met volwassen neuronen. Een eventuele verklaring hiervoor is dat een verminderde prikkelbaarheid (mogelijk door de

Nederlandse Samenvatting
128
aanwezigheid van NaV1.3 α-subunits) van neonatale neuronen kan helpen om hersenweefsel van pasgeboren zoogdieren te beschermen tijdens periodes van zuurstofgebrek (hypoxia). Naast de verminderde prikkelbaarheid van neonatale neuronen bleken deze neuronen ook gevoeliger voor Carbamazepine (CBZ), een natriumkanaalblokker en veelgebruikt AEM. CBZ vertraagde het herstel van inactivatie sterker in neonatale CA1 neuronen dan in volwassen neuronen. Het verschil in CBZ respons en een snellere CBZ-binding aan geïnactiveerde natriumkanalen in neonatale neuronen kan een consequentie zijn van de hogere NaV1.3 subtype expressie in neonatale neuronen. Deze bevinding is gedeeltelijk in overeenstemming met de HEK-cel studies (Hoofdstukken 3 en 6), waar voor de NaV1.3 kanalen (in vergelijking met NaV1.1 kanalen) een meer gehyperpolariseerde Vh waarde voor steady-state inactivatie, een significant langzamer herstel van inactivatie en een lagere EC50 waarde voor natriumkanaalblokkade door CBZ werd gevonden. Daarentegen werd er geen snellere CBZ-binding aan geïnactiveerde NaV1.3 kanalen (in vergelijking met de andere α-subunits) gevonden, terwijl de CBZ-binding aan geïnactiveerde neonatale natriumkanalen sneller was in vergelijking met volwassen kanalen. Dit maakt duidelijk dat het maken van zulke vergelijkingen lastig blijft en dat de aanwezigheid van meer dan één α-subunit en modulerende moleculen (zoals β-subunits) in neuronen bepaalde eigenschappen van kanaal-AEM interacties kunnen maskeren. De plasticiteit van natriumkanaalexpressie is niet beperkt tot het ontwikkelende zenuwstelsel, aangezien NaV1.3 kanalen opnieuw tot expressie komen in volwassen neuronen na kainaat-geinduceerde epileptische aanvallen en na bepaalde typen beschadigingen, zoals beschadigingen aan het axon. Deze waarnemingen voorspellen dat veranderingen in het expressiepatroon van het NaV1.3 kanaal een belangrijke rol kunnen spelen bij epilepsie en andere pathologische aandoeningen, met mogelijk vergaande consequenties voor de farmacologie van AEM. Farmacologie van de persistente natriumstroom Snelactiverende en inactiverende natriumkanalen geleiden de transiente, inwaartse natriumstromen voor snelle actiepotentialen, terwijl niet-inactiverende, of persistente, natriumstromen verantwoordelijk kunnen zijn voor het genereren van spontane actiepotentialen en plateaupotentialen. Persistente natriumstromen worden gedacht ook betrokken te zijn bij epileptische activiteit. De NaV1.3 α-subunit kan een relatief grote persistente natriumstroom geleiden en aangezien expressie van dit kanaal toegenomen lijkt in neuronen van epileptische hersenen (van mens of rat), kan deze subunit belangrijk zijn voor de AEM-gevoeligheid van natriumkanalen. AEM als CBZ, Lamotrigine (LTG) en Fenytoine (DPH) kunnen de transiente natriumstroom “activititeitsafhankelijk” blokkeren, maar ze kunnen ook de persistente natriumstroom (gedeeltelijk) blokkeren. Een persistente component van natriumstromen kan worden aangetroffen in HEK293 cellen die NaV1.1, NaV1.3 of NaV1.6 tot expressie brengen. Het HEK293 expressie systeem bleek een ideaal preparaat om de AEM-effecten op de transiente en persistente componenten van hetzelfde kanaalsubtype te vergelijken. In hoofdstuk 6 beschrijven we de interacties van CBZ en topiramaat (TPM) met de transiente en persistente natriumstromen in HEK293 cellen die de NaV1.3 α-subunit tot expressie brengen. De persistente natriumstroom was aanwezig in alle cellen met NaV1.3 α-subunitexpressie en de amplitude bedroeg ~10 % van de totale stroom bij -10 mV. Aangezien deze HEK

Nederlandse Samenvatting
129
cellen slechts één natriumkanaalsubtype tot expressie brengen, was het eenvoudig de persistente stroom te scheiden van de ‘window’stroom. Tevens is dit een overtuigend bewijs dat één natriumkanaalsubunit zowel transiente als persistente natriumstromen kan geleiden. Zowel de transiente als de persistente NaV1.3 natriumstromen werden geblokkeerd door CBZ (met therapeutische concentraties, ~15 μM), en deze eigenschap kan dus bijdragen aan de anti-convulsieve werking van CBZ. We testten ook TPM, een AEM waarvan het werkingsmechanisme iets buiten het standaard natriumkanaalblokkerende profiel valt. TPM blokkeerde (gedeeltelijk) de persistente natriumstroom, waarschijnlijk een belangrijk mechanisme voor het anti-convulsieve effect van dit AEM, aangezien de effectieve concentratie een aantal malen lager is dan de effectieve concentratie voor beïnvloeding van de transiente natriumstroom (EC50 waarden van respectievelijk ~60 nM and ~3 μM). De observatie dat het NaV1.3 kanaal een relatief grote persistente natriumstroom geleidt, suggereert dat NaV1.3 (her)expressie de onderliggende oorzaak kan zijn van de toegenomen persistente natriumstromen in epileptisch weefsel en duidt op een cruciale rol voor het NaV1.3 kanaal in epilepsie. Dit maakt de persistente natriumstroom een interessant aangrijpingspunt voor (nieuwe) AEM. De bevestiging dat een relatief lage TPM concentratie inderdaad een blokkerend effect heeft op de persistente natriumstroom (wat het dominante mechanisme van TPM als een AEM lijkt te zijn) wijst op de bruikbaarheid van natriumkanaalsubunit expressiesystemen voor het testen van nieuwe AEM. Biofysische eigenschappen van natriumkanaal α-subunits in HEK293 cellen De humane neuronale voltage-afhankelijke natriumkanaal α-subunits NaV1.1, NaV1.2, NaV1.3 en NaV1.6 zijn gekloneerd en stabiel tot expressie gebracht in HEK293 cellen, ons in staat stellend hun biofysische en farmacologische eigenschappen in isolatie te bestuderen (Hoofdstukken 3 en 6). De precieze rol van deze verschillende natriumkanaal α-subunits is slechts marginaal begrepen en via verschillende technieken, waaronder genetische analyse, (sub)cellulaire distributiepatronen en karakterisatie van de gekloneerde kanalen, is geprobeerd dit te verbeteren. Expressie van de α-subunit alleen is voldoende voor de vorming van functionele natriumkanalen en hierdoor zijn deze cellijnen een goede manier om (subtiele) verschillen tussen de α-subunits te ontdekken, iets wat niet kan worden bereikt in hersenweefsel waar in neuronen bijna altijd meerdere α-subunits tot expressie komen. De natriumkanaaltypen NaV1.1, NaV1.2, NaV1.3 and NaV1.6 lijken sterk op elkaar wat betreft aminozuursequentie en genereren allemaal snel-activerende en snel-inactiverende stromen. In onze handen onderscheidde de NaV1.1 stroom zich van de NaV1.2, NaV1.3 en NaV1.6 stromen wat betreft activatie, steady-state inactivatie en herstel van inactivatie. Deze stroom activeerde bij negatievere potentialen en inactiveerde bij positievere potentialen met 33 mV verschil in halfmaximaal voltage van activatie en inactivatie (ΔVh), terwijl 40 mV voor ΔVh werd gevonden voor de andere drie subunits. Bij eenzelfde steilheid van de activatie- en inactivatiecurves betekent de kleinere ΔVh van het NaV1.1 kanaal een grotere overlap tussen activatie en steady-state inactivatie en dus een grotere ‘window’ stroom over een breder voltagebereik, wat neuronale prikkelbaarheid beïnvloedt. Het herstel van inactivatie voor NaV1.1 stromen was ook sneller in vergelijking met NaV1.2 en NaV1.3 stromen, wat kan leiden tot een toegenomen natriumconductantie doordat ze sneller beschikbaar komen voor activatie. Al deze

Nederlandse Samenvatting
130
eigenschappen van het NaV1.1 kanaal maken het snel vuren van actiepotentialen mogelijk. De subcellulaire locatie van NaV1.1 kanalen in dendrieten en cellichamen van neuronen, suggereert dat deze eigenschappen een rol spelen bij de facilitatie van exciterende synaptische input. Zulke eigenschappen dragen mogelijk ook bij aan snel axonaal actiepotentiaalvuren, aangezien NaV1.1 kanalen ook aanwezig zijn in axonale membranen. NaV1.6 α-subunits zijn in hoge dichtheid aanwezig in de knopen van Ranvier van axonen. Met name het snelle herstel na inactivatie van NaV1.6 natriumstromen faciliteert een snelle voortgeleiding van actiepotentialen door axonen. Het langzaamste herstel van inactivatie werd gevonden voor NaV1.3 stromen (1.5-4 keer grotere tijdsconstante dan gevonden voor de andere drie kanaalsubunits). Deze eigenschap kan cellen met een relatief hoog aantal NaV1.3 α-subunits (in vergelijking met de andere α-subunits) mogelijk minder prikkelbaar maken (zie de sectie over ontwikkeling). Farmacologie van natriumkanaal α-subunits in HEK293 cellen De bevindingen van Hoofdstuk 3 wijzen erop dat er subtiele verschillen bestaan voor de verschillende α-subunits wat betreft de interactie van AEM met deze natriumkanalen. Helaas konden we niet een volledige vergelijking maken, zoals b.v. het bepalen van alle details aangaande AEM-subunit interacties voor de drie gebruikte AEM. De maximale natriumconductantie in neuronen is erg groot en het blokkeren van een deel hiervan hoeft de vuuractiviteit niet volledig te beïnvloeden. Maar tijdens epileptische activiteit waarbij neuronen met hoge frequenties actiepotentialen vuren, kan aanhoudende depolarisatie een substantieel deel van de natriumkanalen in de geïnactiveerde toestand brengen. Door de relatief hoge affiniteit die AEM hebben voor geïnactiveerde natriumkanalen worden juist dan de kanalen geblokkeerd (of beter gezegd, ze worden gestabiliseerd in de niet-geleidende geïnactiveerde toestand). Dit resulteert in een sterk gereduceerde natriumstroom en een onderdrukking van het hoog-frequente vuurpatroon van de neuronen. Vanuit een kinetisch standpunt is de mate van een dergelijke depolarisatieverschuiving cruciaal voor het bespreken van de anti-epileptische werking van DPH, CBZ en LTG. Daarom leverde de interactiekinetiek van de drie AEM met de vier α-subunits interessante informatie op met mogelijk belangrijke consequenties voor het begrijpen van AEM-efficiëntie in gevallen en/of situaties (epileptisch versus gezond weefsel) met veranderde α-subunit samenstellingen. De bindingswaarden voor DPH, CBZ en LTG die werden bepaald voor de verschillende α-subunits (Hoofdstuk 3) waren in overeenstemming met waarden beschreven in de literatuur voor neuronale natriumkanalen. Daarnaast was het de eerste keer dat beschreven werd dat AEM bindingswaarden aanzienlijk kunnen verschillen voor de vier α-subunits, wat consequenties kan hebben voor AEM effectiviteit. Een voorbeeld is de verschillende frequentie-afhankelijke blokkade van NaV1.2 en NaV1.3 stromen door CBZ en LTG (Hoofdstuk 3), wat verklaard kon worden aan de hand van de verschillen in AEM bindingswaarden. De binding van CBZ aan geïnactiveerde NaV1.2 en NaV1.3 kanalen (respectievelijk ~75 mM-1s-1 en ~45 mM-1s-1) is snel genoeg om de natriumstroom te blokkeren als de opgelegde stimulusfrequentie (10 en 50 Hz) geen beperkende factor is. Opvallend was dat, in het geval van LTG (met een veel langzamere binding aan geïnactiveerde natriumkanalen dan CBZ), duidelijke verschillen werden gevonden wanneer NaV1.2 en NaV1.3 stromen werden geactiveerd met 10 of 50 Hz

Nederlandse Samenvatting
131
stimulatiereeksen. Een snelle bindingswaarde (zoals die van CBZ, vergeleken met die van DPH en LTG) duidt er op dat het AEM effectief kan zijn bij relatief kortdurende epileptische episodes. De aanwezigheid van afwijkende typen α-subunits in het epileptisch weefsel waaraan het AEM met verschillende snelheid bindt, kan dan van invloed zijn op de effectiviteit van het AEM in dat weefsel. Dit illustreert dat, afhankelijk van het activiteitsniveau, de gebruiks- en frequentie-afhankelijke effecten van AEM verschillend kunnen zijn voor neuronen met verschillende natriumkanaalsamenstellingen. Tot slot Aan de hand van de resultaten van de experimenten beschreven in dit proefschrift hebben we voorgesteld dat een verschuiving in expressiepatronen van de porievormende α-subunit van het voltage-afhankelijke natriumkanaal de gevoeligheid van natriumkanalen voor de gewoonlijk gebruikte AEM beïnvloedt en zo verantwoordelijk is voor een veranderde gevoeligheid of, in het ergste geval, volledige ongevoeligheid. Als deze veranderingen optreden op verschillende momenten in verschillende hersengebieden mag het duidelijk zijn dat het vinden van een optimale en volledig effectieve AEM dosis voor een epileptische patiënt een onmogelijke opdracht wordt. Het is daarom aan te bevelen om een AEM toetsingsstrategie toe te passen waarbij rekening wordt gehouden met het bestaan van een verschillende AEM effectiviteit in aangetast (b.v. epileptisch) versus gezond weefsel. Het HEK293 expressiesysteem waarin de verschillende α-subunits tot expressie worden gebracht kan een belangrijk middel zijn bij een dergelijke strategie. Er moet echter niet vergeten worden dat de componenten bestudeerd in kunstmatige expressiesystemen zich niet altijd hetzelfde hoeven te ‘gedragen’ als in intact (epileptisch) hersenweefsel. Waarschijnlijk beïnvloedt ook de achtergrond van het weefsel (w.o. modulerende moleculen als b.v. kinases en andere subunits) waarin deze componenten (in dit geval de natriumkanaalsubunits) zich bevinden hun functioneren. Daarom zullen in vivo testsystemen altijd een dominante rol moeten spelen bij het vinden van nieuwe AEM, maar kunnen in vitro testsystemen een aanvullende manier zijn om het testen van (nieuwe) AEM te faciliteren. De bevindingen in dit proefschrift ondersteunen het beeld dat de ontwikkeling van nieuwe AEM beter toegespitst kan worden op hersengebied-specifieke AEM-effectiviteit, dan op het bestuderen van AEM effecten op het volledige brein. Zo’n aanpak kan leiden tot een nieuwe en uitdagende strategie voor het vinden van nieuwe AEM en mogelijk helpen bij het vinden van een oplossing voor het probleem van farmacoresistentie.


中文摘要
中文摘要 (Chinese Summary)
电压依赖性钠通道在神经元动作电位的产生过程中起重要作用。癫痫是最常
见的神经紊乱性疾病之一,以神经元局限性或弥漫性异常放电为特征。因此可通过
抑制钠通道活性,降低神经元兴奋性,从而抑制癫痫发放,因此钠通道成为了目前
常用抗癫痫药物的作用靶点之一。钠通道蛋白由一个α亚单位及其辅助β亚单位所
构成,单独的α亚单位已足以构成功能性的钠通道,而β亚单位可对通道动力学进
行调节。迄今为止在大脑中已有四个钠通道的亚型被确认,NaV1.1, NaV1.2, NaV1.3 和 NaV1.6。
本论文旨在研究癫痫状态下的钠通道功能及其与抗癫痫药物的相互作用。以
往的研究工作已经表明癫痫发生后钠通道亚型的构成发生了改变,因此在癫痫的治
疗过程中,不同钠通道亚型对抗癫痫药物敏感性的差异是否会导致药物耐药性的产
生?为了验证此假设,我们以稳定表达了各种人脑型钠通道亚型NaV1.1、NaV1.2、 NaV1.3 和 NaV1.6α亚单位 的HEK细胞系作为研究对象,来研究各α亚单位的生物物
理特点以及它们与常用抗癫痫药物 Carbamazepine (CBZ)、Lamotrigine (LTG) 和 Phenytoin (DPH)的相互作用。此HEK细胞系为我们提供了稳定的、标准化的表达
系统,成为研究钠通道α亚单位的有用工具。进一步我们在急性分离的大鼠海马
CA1区神经元(如生长发育期及癫痫发生后神经元)上研究了具有不同亚单位组成
的钠通道的功能。
在HEK细胞系上研究表明,各钠通道亚型之间的生物物理特点具有差异
性。与 NaV1.2、NaV1.3和NaV1.6型钠通道电流相比,NaV1.1型钠通道电流在激活、
失活以及恢复的电压依赖性方面均表现出了独特的特点,而正是这些特点使得
NaV1.1型钠通道更容易介导快速发生的动作电位的产生,有可能在癫痫的发生中起
了重要作用;而NaV1.3 型钠通道电流失活后的缓慢恢复使得高表达这类亚型的细
胞具有较低的可兴奋性,可能参与了癫痫发生后维持正常脑功能的代偿机制。
CBZ、LTG和DPH浓度-依赖地抑制钠通道活性,并且这种抑制具有使用和频率依
赖性,从而维持正常的脑功能。基于上述各钠通道亚型所表现出的不同的生物物理
特点,抗癫痫药物在与它们的相互作用中也表现出了不同的药理学特点,例如
NaV1.1和NaV1.6型对CBZ表现出了较低的敏感性;尤其是在本论文研究中首次描述
了不同药物与不同钠通道亚型结合速率的差异性,如与其它两个药物相比,CBZ表现出了较快的结合速率,并且这些药物与NaV1.3型的结合速率相对较慢,这些差异
性与药物的作用强度密切相关。抗癫痫药物与各钠通道亚型相互作用的药理学特点
为我们理解在钠通道亚型构成发生改变情况下的药物作用强度提供了重要实验基
础。
与成年大鼠相比,新生大鼠神经元具有不同的钠通道亚型构成,尤其表现为

中文摘要
134
NaV1.3型的高表达,为了进一步验证差异性的存在,我们对新生及成年大鼠海马
CA1区神经元的钠通道特点及其CBZ的作用进行了研究。结果表明新生神经元上钠
通道表现出了可兴奋性的降低以及对CBZ的敏感性升高,进一步表明增加表达的
NaV1.3型钠通道在癫痫及其它病理情况下的重要作用及其相关的药物治疗效果。 癫痫发生后钠通道亚型构成也会发生改变,因此我们对kainate所诱导的癫痫模型大
鼠神经元钠通道进行了研究,结果表明通道失活的电压依赖性特点发生了微小改
变。我们认为在各种癫痫的发生发展过程中钠通道电流的微小变化也可导致神经元
兴奋性的改变。
NaV1.3型钠通道还介导了相对较大比例的持续性钠通道电流,由于在癫痫组
织中NaV1.3型钠通道的表达增高,使得相应增大的持续性钠通道电流成为了令人感
兴趣的(新的)抗癫痫药物的作用靶点。在我们的实验研究中确认了TPM的确是
持续性钠通道电流的强有力的阻滞剂,并且这种作用可能是其抗癫痫作用的主要机
制,因此这种钠通道表达系统可能成为筛选新型抗癫痫药物的有用工具。
本论文研究结果提示,对新型抗癫痫药物的研究最好强调它们的脑区特异性
而不是全脑的活性,从而达到优化癫痫病人个体治疗方案的目的;该理论也为新型
抗癫痫药物的研发提供了新颖的、具有挑战性的方向,并为解决癫痫治疗中的药物
依赖性问题提出了可能。

Curriculum Vitae
CURRICULUM VITAE
Guangchun Sun was born in September 5, 1967, Guizhou, P. R. China. After finishing the undergraduate course at the Guiyang Medical University, Guizhou in 1990, she started the Master Course in Pharmacology at the same university. In 2001 she was financed to study electrophysiology in the group of prof. dr. Wytse Wadman, University of Amsterdam, by the China-Netherlands exchange program. She liked this type of research, reason to start a PhD program after one year sponsored by the Dutch National Epilepsy Foundation, working on sodium channel and antiepileptic drugs, of which this thesis is the result. As of August 2006 she is a postdoc working on ion channels in the group of prof. dr. Tian-le Xu, Institute of Neuroscience, Chinese Academy of Sciences, Shanghai.


Dankwoord
DANKWOORD/ ACKNOWLEDGEMENTS
It is my great pleasure to express my thanks to many people who made this thesis possible. First, I would very much like to thank my supervisor prof. dr. Wytse Wadman for his enthusiasm, inspiration, preciseness and humor. Also for all his energy to teach me what I was lacking in background. He led me into the electrophysiology field and from him I have learned how a scientist should be. It is difficult to overstate my gratitude to my co-supervisor dr. Taco Werkman. Without him I would have been lost. He provided me with encouragement, sound advice, good teaching, and great efforts to explain things clearly, simply and with remarkable patience and he put in much effort to get this thesis done. Thanks to Dr. Jeff Clare from GlaxoSmithKline, UK for providing the nice cell lines, drugs and important advice. Twan, you are such a kind person, I cannot thank you enough. You gave me wonderful experimental support, like the HEK-cell culturing, which made this thesis possible. After work, you did your utmost to make my life easier in The Netherlands. We had a lot of fun together. How can I forget you, Hannah, a very kind person? I had a wonderful time when I stayed at your place. You took care of me more than I can thank you for. You also contributed to my thesis. Importantly, you showed me how to be a good wife and mother. Margreet, you kept caring for me, especially helping me those many times when I had yet another emergency. Lucie, it is not easy to thank you in a few words here. We had so much fun together and it is not over. You really cared about me with your kind heart. All a friend can ask for! I am grateful for prof. dr. Fernando H. Lopes da Silva’s kind help. Annelies, you put so much effort in my thesis. I am honored to have you as my paranimph. Of course we will see each other in China! Susan, it was very nice to patch and talk with you in the lab. Natalie, you were my good advisor on everything. It was nice to share the office. I would also very much like to thank my colleagues in the lab of the UvA: Hans, Dave, Elmar, Hans (K), Jeroen, Remco, Pascal, Chunyu Cao, Michiel, Oscar and Aly for providing a stimulating and fun environment in which to learn and grow. Furthermore, thanks to the China-Netherlands Exchange program, Dutch Epilepsy Committee for supporting my life in The Netherlands, and Guizhou Medical University for keeping the nice position for me. I cannot end without thanking my family, especially my husband Daiwei Zhao and my super parents in China. They took over my responsibilities at home, which made my studying abroad possible. Saisai, my son, I had left you for a couple of years. You deserve all the love I give to you. You must be very proud of your mum! To them I dedicate this thesis.
Guangchun Sun