Utilization of a Chromatographic Internal Standard in the ...€¦ · An addition observation shows...
1
© 2013 Mayo Foundation for Medical Education and Research Utilization of a Chromatographic Internal Standard in the Rapid Quantification of Arsenic Species in Urine by HPLC-ICP-MS Peter Wegwerth, Curtis Rykal, Nathan Hines, Timothy McNeal, Matthew Hanley, Thomas Moyer Mayo Clinic, Rochester, MN Sensitivity and Precision The limit of blank (LOB) was determined using the equation LOB = |μ Blank | + 1.645 * σ Blank where the mean and standard deviation are from analyzing 60 blank samples. The limit of detection (LOD) was determined using the equation LOD = LOB + 1.645 * σ Sample where the standard deviation of the sample was obtained from 60 matrix blanks. Inter-assay (between run or run to run) precision data was obtained for four levels, over 20 separate runs, by four technologists. The guard column was changed every 5 runs and the analytical column was changed at 10 runs. Image 1, is the chromatographic overlay is of precision level 3 at ~ 10 mcg/L for each species. Table 2 Precision and Sensitivity Units = mcg/L Precision Level 1 Precision Level 2 Precision Level 3 Precision Level 4 Analyte: AsC Mean 0.000 0.652 10.353 31.787 LOB 0.013 SD 0.000 0.064 0.668 2.324 LOD 0.023 % CV NA 10% 6% 7% LLOQ 1.000 Analyte: AsB Mean 0.055 0.754 10.152 31.106 LOB 0.007 SD 0.021 0.056 0.537 1.736 LOD 0.043 % CV 39% 7% 5% 6% LLOQ 1.000 Analyte: As 3+ Mean 0.421 1.017 10.179 31.356 LOB 0.182 SD 0.223 0.167 0.648 1.385 LOD 0.259 % CV 53% 16% 6% 4% LLOQ 1.000 Analyte: DMA Mean 0.920 2.322 11.576 32.406 LOB 0.048 SD 0.063 0.150 0.703 1.907 LOD 0.278 % CV 7% 6% 6% 6% LLOQ 1.000 Analyte: MMA Mean 0.260 1.064 10.309 30.993 LOB 0.050 SD 0.061 0.087 0.623 1.890 LOD 0.123 % CV 24% 8% 6% 6% LLOQ 1.000 Analyte: As 5+ Mean 0.332 1.031 10.485 31.671 LOB 0.159 SD 0.104 0.108 0.492 1.561 LOD 0.214 % CV 31% 10% 5% 5% LLOQ 1.000 Acceptance Criteria %CV of 20% Instrument Parameters The HPLC system consisted of a PerkinElmer Series 200 peltier oven, pump, vacuum degasser and autosampler. The autosampler utilized a Rheodyne 7725 valve equipped with a tefzel rotor seal (for ph > 10) and a 100 uL sample loop. 2.5 mL syringes were used for sample injection. A PRP-X100 (Hamilton, Reno NV, USA) anion-exchange column (150 x 4.6 mm, 7 um, exchange capacity 0.19meq/gm o.228meq/column) was used for separation. A PRP-X100 guard column was used as a precolumn. 75 cm of PEEK capillary tubing (0.1778 mm I.D.) was used to connect the system from the pump to the PerkinElmer Elan DRC II ICP-MS detector equipped with an ESI PFA ST nebulizer (ES-2040), cyclonic quartz spray chamber (ES-3154-1018-13), quartz injector, and platinum cones. The operation conditions for both the HPLC and the ICP-MS can be found in Table 1. Table 1 Instrument Parameters HPLC Mobile phase A: 20mmol L -1 ammonium bicarbonate in 2% Methanol pH 8.1 B: 20mmol L -1 ammonium bicarbonate, 80 mL ~20% NH3OH 10mL ~70% HNO 3 in 2% HPLC grade Methanol pH 10.0 Flow Rate 3.5 mL min-1 Column Temperature 25°C Pump Pressure 2500-3500 (column dependent) Pump Program Step Type Step Time (min) % Mobile Phase A %Mobile Phase B Equilibration 0.7 100 Run 0.4 60 40 Run 0.9 100 Run 0.5 100 ICP-MS Rf power 1400 – 1600 optimized daily Data Acquisition Nebulizer Gas Flow 0.8 – 1.2 optimized daily Scanning Mode Peak Hopping Lens Voltage for AsO 4 - 7 optimized daily Dwell Time 150 ms N 2 O DRC gas flow 0.4 mL min -1 Integration mode Peak area RPq 0.5 Analyte AsO Arsenic is a toxic element with wide natural distribution; its toxicity is largely dependent on molecular species. Six species are of primary importance for clinical evaluation of patients. They are, in order of decreasing toxicity: As 3+ , As 5+ , monomethylarsine (MMA), dimethylarsine (DMA), and the non-toxic species arsenocholine (AsC), and arsenobetaine (AsB). Current methods for quantifying these species have two significant deficiencies: long elution times (greater than eight minutes) and lack of a chromatographic internal standard. We report a method which corrects these deficiencies by including phenylarsonic acid (PAA) as a seventh reference peak, and refining the separation to elute all seven peaks in less than two minutes. Abstract Image 1 Precision Level 3 overlay Linear Range Linear range was determined by linearity by dilution and spiked recovery. In both studies three pools of urine were collected, analyzed neat, aliquoted and spiked to the levels shown in the table and analyzed. Linearity by dilution samples were diluted with the appropriate amount of the original pre-spiked urine pool. Table 3 Linearity Studies Standard Addition Expected Analyte: AsC Analyte: AsB Analyte: As 3+ Analyte: DMA Analyte: MMA Analyte: As 5+ Spike 1000 S S S S S S x10 100 110% 99% 101% 97% 95% 95% x50 20 101% 90% 92% 93% 88% 89% x100 10 102% 93% 103% 101% 93% 97% The 1000 mcg/L spike saturated the detector Recovery values are an average of N=3 results Acceptance Criteria 20% Standard Addition Analyte: AsC Analyte: AsB Analyte: As 3+ Analyte: DMA Analyte: MMA Analyte: As 5+ 1 100% 94% 37% 91% 94% 125% 2 104% 97% 61% 97% 96% 115% 10 103% 95% 83% 95% 94% 101% 20 103% 95% 91% 94% 94% 96% 100 105% 96% 96% 95% 96% 97% Patient Data Under the current practice urine samples with a total arsenic > 50 mcg/L are considered positive and fractionated to separate and quantify organic and inorganic arsenic. Using this criteria patient method comparison results were split into positive and negative groups and compiled to give an expectation of typical results. This will be part of an ongoing study to illustrate the importance of speciation and establish a normal phenotype. Negative Total <50mcg/L N = 28 Total Analyte: AsC Analyte: AsB Analyte: As 3+ Analyte: DMA Analyte: MMA Analyte: As5+ Average 30.1 0.3 15.7 0.6 7.4 0.7 0.8 High 47.7 5.7 46.3 1.8 19.6 1.8 7.0 Low 15.4 0.0 0.2 0.0 1.2 0.2 0.2 SD 11.2 1.1 12.9 0.3 5.2 0.4 1.5 Positive Total >50mcg/L N = 23 Total Analyte: AsC Analyte: AsB Analyte: As 3+ Analyte: DMA Analyte: MMA Analyte: As5+ Average 130.3 0.7 81.3 1.0 14.8 1.0 0.5 High 883.0 4.6 439.5 3.7 147.9 3.0 1.8 Low 51.0 0.0 18.0 0.0 1.8 0.2 0.2 SD 170.0 1.2 84.1 0.8 29.7 0.8 0.5 Figure 2 Total (Sum of AsC, ASB, DMA, MMA, As 3+ , As 5+ ) Because this clinical analysis is to used determine the extent of arsenic exposure, sensitivity and accuracy are the most important aspects to explore. The sensitivity and precision studies show this method capable of producing consistent results at the 1 mcg/L level allowing us to set our lowest reportable at 1mcg/L. In image 1, very little variation is seen over the 20 days of analysis. This is especially impressive considering the data includes added variability from the column changes and multiple technologists. The NIST, and PT results show that the method is highly accurate throughout the calibration range of 1 – 100 mcg/L. Interspecies conversion from As 3+ to As 5+ can be seen in the low levels of the standard addition study. There is no known toxicity for these species at this concentration level and values in this range would be inconsequential for current clinical treatment. Additionally, this issue is resolved at increased concentrations because of the stabilizing effect of lower pH from the arseno acids. All other values for standard addition and linearity by dilution are within acceptance limits Patient data shows the two most frequently elevated species to be AsB and DMA. An addition observation shows the importance of speciation, as two patients from the 28 negative had As 5+ values >5 mcg/L. Under our previous method these samples would not be fractionated and these values would not be known. Discussion Validation of this method is near completion and the method will soon be offered routinely for the clinical determination of arsenic levels in patients. The speed of the analysis will allow us to perform our current patient volume (~30 samples per day) in a third of the time of our previous method which will also allow for increased capacity in the future. The inclusion of PAA as a chromatographic internal standard allows for greater troubleshooting information and accurate analysis despite the matrix variability of human urine. Complete method details, study results and clinical relevance will be included in a peer reviewed publication later this year. Conclusion and Future plans 1. Komorowicz, I. and D. Baralkiewicz (2011). "Arsenic and its speciation in water samples by high performance liquid chromatography inductively coupled plasma mass spectrometry—Last decade review." Talanta 84(2): 247-261. References Accuracy No reference test was available that offered the analysis of all six arsenic species so QME-QAS PCI urines and NIST 2669 were used to independently verify accuracy. QME-QAS PCI urines only provide values for non-diet “inorganic” arsenic (DMA, MMA, As 3+ , As 5+ ) and total (all species). No information is provided about the methods used to determine values for PCI urines. Table 4 NIST 2669 Results Level 1 Target Low High Mean Difference from Target % Difference AsB 12.4 10.5 14.3 10.41 -1.99 -16% As 3+ 1.47 1.37 1.57 1.40 -0.07 -5% DMA 3.47 3.06 3.88 3.78 0.31 9% MMA 1.87 1.48 2.26 1.66 -0.21 -11% As5+ 2.41 2.11 2.71 2.21 -0.20 -8% Total 22.20 18.52 24.72 19.46 -2.74 -12% Level 2 Target Low High Mean Difference from Target % Difference TMAO 1.94 1.7 2.21 0 1.94 AsC 3.74 3.39 4.09 2.56 -3.12 -55% AsB 1.43 1.35 1.51 4.69 3.26 228% As 3+ 5.03 4.72 5.34 5.02 -0.01 0% DMA 25.3 24.6 26 26.36 1.06 4% MMA 7.18 6.62 7.74 6.20 -0.98 -14% As5+ 6.16 5.21 7.11 6.28 0.12 2% Total 50.78 47.59 54.00 51.10 0.40 1% TMAO elutes within the co-elution of AsC and AsB Values are in mcg/L, the mean is an average of N=9 runs Figure 1 Non-diet (Sum of DMA, MMA, As 3+ , As 5+ )
Transcript of Utilization of a Chromatographic Internal Standard in the ...€¦ · An addition observation shows...

© 2013 Mayo Foundation for Medical Education and Research
Utilization of a Chromatographic Internal Standard in the Rapid Quantifi cation of Arsenic Species in Urine by HPLC-ICP-MS
Peter Wegwerth, Curtis Rykal, Nathan Hines, Timothy McNeal, Matthew Hanley, Thomas MoyerMayo Clinic, Rochester, MN
Sensitivity and Precision
The limit of blank (LOB) was determined using the equation LOB = |μBlank| + 1.645 * σBlank where the mean and standard deviation are from analyzing 60 blank samples. The limit of detection (LOD) was determined using the equation LOD = LOB + 1.645 * σSample where the standard deviation of the sample was obtained from 60 matrix blanks.
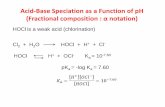
Inter-assay (between run or run to run) precision data was obtained for four levels, over 20 separate runs, by four technologists. The guard column was changed every 5 runs and the analytical column was changed at 10 runs. Image 1, is the chromatographic overlay is of precision level 3 at ~ 10 mcg/L for each species.
Table 2
Precision and Sensitivity
Units = mcg/L Precision Level 1
Precision Level 2
Precision Level 3
Precision Level 4
Analyte: AsC
Mean 0.000 0.652 10.353 31.787 LOB 0.013
SD 0.000 0.064 0.668 2.324 LOD 0.023
% CV NA 10% 6% 7% LLOQ 1.000
Analyte: AsB
Mean 0.055 0.754 10.152 31.106 LOB 0.007
SD 0.021 0.056 0.537 1.736 LOD 0.043
% CV 39% 7% 5% 6% LLOQ 1.000
Analyte: As3+
Mean 0.421 1.017 10.179 31.356 LOB 0.182
SD 0.223 0.167 0.648 1.385 LOD 0.259
% CV 53% 16% 6% 4% LLOQ 1.000
Analyte: DMA
Mean 0.920 2.322 11.576 32.406 LOB 0.048
SD 0.063 0.150 0.703 1.907 LOD 0.278
% CV 7% 6% 6% 6% LLOQ 1.000
Analyte: MMA
Mean 0.260 1.064 10.309 30.993 LOB 0.050
SD 0.061 0.087 0.623 1.890 LOD 0.123
% CV 24% 8% 6% 6% LLOQ 1.000
Analyte: As5+
Mean 0.332 1.031 10.485 31.671 LOB 0.159
SD 0.104 0.108 0.492 1.561 LOD 0.214
% CV 31% 10% 5% 5% LLOQ 1.000
Acceptance Criteria %CV of 20%
Instrument Parameters
The HPLC system consisted of a PerkinElmer Series 200 peltier oven, pump, vacuum degasser and autosampler. The autosampler utilized a Rheodyne 7725 valve equipped with a tefzel rotor seal (for ph > 10) and a 100 uL sample loop. 2.5 mL syringes were used for sample injection.
A PRP-X100 (Hamilton, Reno NV, USA) anion-exchange column (150 x 4.6 mm, 7 um, exchange capacity 0.19meq/gm o.228meq/column) was used for separation. A PRP-X100 guard column was used as a precolumn. 75 cm of PEEK capillary tubing (0.1778 mm I.D.) was used to connect the system from the pump to the PerkinElmer Elan DRC II ICP-MS detector equipped with an ESI PFA ST nebulizer (ES-2040), cyclonic quartz spray chamber (ES-3154-1018-13), quartz injector, and platinum cones. The operation conditions for both the HPLC and the ICP-MS can be found in Table 1.
Table 1
Instrument Parameters HPLC
Mobile phaseA: 20mmol L-1 ammonium bicarbonate in 2% Methanol pH 8.1
B: 20mmol L-1 ammonium bicarbonate, 80 mL ~20% NH3OH 10mL ~70% HNO3 in 2% HPLC grade Methanol pH 10.0
Flow Rate 3.5 mL min-1 Column Temperature 25°C
Pump Pressure 2500-3500 (column dependent)
Pump Program
Step Type Step Time (min) % Mobile Phase A %Mobile Phase B
Equilibration 0.7 100
Run 0.4 60 40
Run 0.9 100
Run 0.5 100
ICP-MS
Rf power 1400 – 1600 optimized daily Data Acquisition
Nebulizer Gas Flow 0.8 – 1.2 optimized daily Scanning Mode Peak Hopping
Lens Voltage for AsO 4 - 7 optimized daily Dwell Time 150 ms
N2O DRC gas fl ow 0.4 mL min-1 Integration mode Peak area
RPq 0.5 Analyte AsO
Arsenic is a toxic element with wide natural distribution; its toxicity is largely dependent on molecular species. Six species are of primary importance for clinical evaluation of patients. They are, in order of decreasing toxicity: As3+, As5+, monomethylarsine (MMA), dimethylarsine (DMA), and the non-toxic species arsenocholine (AsC), and arsenobetaine (AsB). Current methods for quantifying these species have two signifi cant defi ciencies: long elution times (greater than eight minutes) and lack of a chromatographic internal standard. We report a method which corrects these defi ciencies by including phenylarsonic acid (PAA) as a seventh reference peak, and refi ning the separation to elute all seven peaks in less than two minutes.
Abstract Image 1 Precision Level 3 overlay
Linear RangeLinear range was determined by linearity by dilution and spiked recovery. In both studies three pools of urine were collected, analyzed neat, aliquoted and spiked to the levels shown in the table and analyzed.
Linearity by dilution samples were diluted with the appropriate amount of the original pre-spiked urine pool.
Table 3
Linearity Studies
Standard Addition Expected Analyte:
AsCAnalyte:
AsBAnalyte:
As3+Analyte:
DMAAnalyte:
MMAAnalyte:
As5+
Spike 1000 S S S S S S
x10 100 110% 99% 101% 97% 95% 95%
x50 20 101% 90% 92% 93% 88% 89%
x100 10 102% 93% 103% 101% 93% 97%
The 1000 mcg/L spike saturated the detectorRecovery values are an average of N=3 resultsAcceptance Criteria 20%
Standard Addition
Analyte: AsC
Analyte: AsB
Analyte: As3+
Analyte: DMA
Analyte: MMA
Analyte: As5+
1 100% 94% 37% 91% 94% 125%
2 104% 97% 61% 97% 96% 115%
10 103% 95% 83% 95% 94% 101%
20 103% 95% 91% 94% 94% 96%
100 105% 96% 96% 95% 96% 97%
Patient DataUnder the current practice urine samples with a total arsenic > 50 mcg/L are considered positive and fractionated to separate and quantify organic and inorganic arsenic. Using this criteria patient method comparison results were split into positive and negative groups and compiled to give an expectation of typical results. This will be part of an ongoing study to illustrate the importance of speciation and establish a normal phenotype.
Negative Total <50mcg/L
N = 28 Total Analyte: AsC
Analyte: AsB
Analyte: As3+
Analyte: DMA
Analyte: MMA
Analyte: As5+
Average 30.1 0.3 15.7 0.6 7.4 0.7 0.8
High 47.7 5.7 46.3 1.8 19.6 1.8 7.0
Low 15.4 0.0 0.2 0.0 1.2 0.2 0.2
SD 11.2 1.1 12.9 0.3 5.2 0.4 1.5
Positive Total >50mcg/L
N = 23 Total Analyte: AsC
Analyte: AsB
Analyte: As3+
Analyte: DMA
Analyte: MMA
Analyte: As5+
Average 130.3 0.7 81.3 1.0 14.8 1.0 0.5
High 883.0 4.6 439.5 3.7 147.9 3.0 1.8
Low 51.0 0.0 18.0 0.0 1.8 0.2 0.2
SD 170.0 1.2 84.1 0.8 29.7 0.8 0.5
Figure 2 Total (Sum of AsC, ASB, DMA, MMA, As3+, As5+)
Because this clinical analysis is to used determine the extent of arsenic exposure, sensitivity and accuracy are the most important aspects to explore. The sensitivity and precision studies show this method capable of producing consistent results at the 1 mcg/L level allowing us to set our lowest reportable at 1mcg/L. In image 1, very little variation is seen over the 20 days of analysis. This is especially impressive considering the data includes added variability from the column changes and multiple technologists. The NIST, and PT results show that the method is highly accurate throughout the calibration range of 1 – 100 mcg/L.
Interspecies conversion from As3+ to As5+ can be seen in the low levels of the standard addition study. There is no known toxicity for these species at this concentration level and values in this range would be inconsequential for current clinical treatment. Additionally, this issue is resolved at increased concentrations because of the stabilizing effect of lower pH from the arseno acids. All other values for standard addition and linearity by dilution are within acceptance limits
Patient data shows the two most frequently elevated species to be AsB and DMA. An addition observation shows the importance of speciation, as two patients from the 28 negative had As5+ values >5 mcg/L. Under our previous method these samples would not be fractionated and these values would not be known.
Discussion
Validation of this method is near completion and the method will soon be offered routinely for the clinical determination of arsenic levels in patients. The speed of the analysis will allow us to perform our current patient volume (~30 samples per day) in a third of the time of our previous method which will also allow for increased capacity in the future. The inclusion of PAA as a chromatographic internal standard allows for greater troubleshooting information and accurate analysis despite the matrix variability of human urine. Complete method details, study results and clinical relevance will be included in a peer reviewed publication later this year.
Conclusion and Future plans
1. Komorowicz, I. and D. Barałkiewicz (2011). "Arsenic and its speciation in water samples by high performance liquid chromatography inductively coupled plasma mass spectrometry—Last decade review." Talanta 84(2): 247-261.
References
Accuracy
No reference test was available that offered the analysis of all six arsenic species so QME-QAS PCI urines and NIST 2669 were used to independently verify accuracy. QME-QAS PCI urines only provide values for non-diet “inorganic” arsenic (DMA, MMA, As3+, As5+) and total (all species). No information is provided about the methods used to determine values for PCI urines.
Table 4
NIST 2669 ResultsLevel 1 Target Low High Mean Difference from Target % Difference
AsB 12.4 10.5 14.3 10.41 -1.99 -16%As3+ 1.47 1.37 1.57 1.40 -0.07 -5%DMA 3.47 3.06 3.88 3.78 0.31 9%MMA 1.87 1.48 2.26 1.66 -0.21 -11%As5+ 2.41 2.11 2.71 2.21 -0.20 -8%Total 22.20 18.52 24.72 19.46 -2.74 -12%
Level 2 Target Low High Mean Difference from Target % Difference
TMAO 1.94 1.7 2.21 0 1.94AsC 3.74 3.39 4.09 2.56 -3.12 -55%AsB 1.43 1.35 1.51 4.69 3.26 228%As3+ 5.03 4.72 5.34 5.02 -0.01 0%DMA 25.3 24.6 26 26.36 1.06 4%MMA 7.18 6.62 7.74 6.20 -0.98 -14%As5+ 6.16 5.21 7.11 6.28 0.12 2%Total 50.78 47.59 54.00 51.10 0.40 1%
TMAO elutes within the co-elution of AsC and AsBValues are in mcg/L, the mean is an average of N=9 runs
Figure 1 Non-diet (Sum of DMA, MMA, As3+, As5+)