İNHALER STEROİD/ UZUN ETKİLİ b 2 AGONİST KOMBİNASYONUN OSTEOPOROZA ETKİSİ

Utah Medicaid Pharmacy and Therapeutics Committee
Drug Class Review
Long-Acting β2-Agonist and Long-Acting Muscarinic Antagonist Combination Products
AFHS classifications: Antimuscarinics/Antispasmodics 12:08.08, Selective Beta2-Adrenergic
Agonists 12:12.08.12
Glycopyrrolate and formoterol fumarate (Bevespi Aerosphere)
Glycopyrrolate and indacaterol (Utibron Neohaler)
Tiotropium bromide and olodaterol (Stiolto Respimat)
Umeclidinium and vilanterol (Anoro Ellipta)
Final Report August 2017
Review prepared by: Elena Martinez Alonso, B.Pharm., MSc MTSI, Medical Writer Joanita Lake, B.Pharm., MSc EBHC (Oxon), Clinical Pharmacist Vicki Frydrych, B.Pharm., Pharm.D., Clinical Pharmacist Valerie Gonzales, Pharm.D., Clinical Pharmacist Michelle Fiander, MA, MLIS, Systematic Review/Evidence Synthesis Librarian Joanne LaFleur, Pharm.D., MSPH, Associate Professor University of Utah College of Pharmacy University of Utah College of Pharmacy, Drug Regimen Review Center Copyright © 2017 by University of Utah College of Pharmacy Salt Lake City, Utah. All rights reserved

1
Table of Contents Executive Summary ...................................................................................................................................... 2 Introduction ................................................................................................................................................... 4
Table 1. FDA Approved LABA/LAMA Combination Products for COPD .................................... 5
Utah Medicaid Utilization Data 6
Table 2. Utah Medicaid FFS Patients diagnosed with COPD, Asthma or COPD/Asthma overlap . 7
Table 3. LABA/LAMA or ICS/LABA treatment in Utah Medicaid FFS patients for 2013-2017 period ................................................................................................................................................ 8
Disease Overview and Clinical Guidelines 9
A) Chronic Obstructive Pulmonary Disease 9
Table 4. Pharmacologic treatment algorithms for the management of COPD (GOLD Guidelines) ........................................................................................................................................................ 14
B) COPD and Asthma 18
Table 5. Recommendations for Initial Treatment in Patients with Asthma-COPD Overlap .......... 18
Pharmacology ............................................................................................................................................. 19
Table 6. Pharmacokinetics of LABA/LAMA Combination Products for COPD .......................... 20
Special Populations ..................................................................................................................................... 22
Table 7. Recommendations for Special Populations of LABA/LAMA Combination Products for COPD .............................................................................................................................................. 23
Methods ...................................................................................................................................................... 24
Clinical Efficacy ......................................................................................................................................... 26
Safety .......................................................................................................................................................... 28
Table 8. Adverse Effects and Warnings of LABA/LAMA Combination Products for COPD ...... 29
Summary ..................................................................................................................................................... 31
References ................................................................................................................................................... 32
Appendix A. Medications Commonly Used in COPD ............................................................................... 37
Appendix B. MEDLINE and EMBASE Literature Search Strategies of LABA/LAMA Combination Products for COPD ..................................................................................................................................... 40
Table 1. Medline Literature Search Strategy (via Ovid) for systematic reviews and randomized controlled trials ............................................................................................................................... 40
Table 2. EMBASE Literature Search Strategy (via EMBASE.com) ............................................. 41
Appendix C. Network Meta-analyses Comparing LABA/LAMA Combination Products for COPD ....... 41
Appendix D. Summary of Evidence of LABA/LAMA Combination Products for COPD ........................ 42
Appendix E. List of Excluded References .................................................................................................. 45

2
Executive Summary Introduction: Chronic Obstructive Pulmonary Disease (COPD) is a respiratory disease characterized by a progressive lung function impairment that causes disabilities and impacts the patient’s quality of life. COPD is associated with elevated morbidity and mortality rates and high social and economic burden. The prevalence of COPD is increasing worldwide and the major risk factor is the inhalation of tobacco smoke.
This report evaluates the clinical efficacy and safety of long-acting β2-agonist (LABA) plus long-acting muscarinic antagonist (LAMA) combination products based on systematic reviews, meta-analyses and randomized controlled trials (RCTs) assessing head-to-head comparisons between these combination products. Currently, four LABA/LAMA fixed dose combination (FDCs) products available in a single inhaler are approved by the Federal Drug Administration (FDA) in the United States: formoterol fumarate/glycopyrrolate (Bevespi Aerosphere), indacaterol maleate/glycopyrrolate (Utibron Neohaler), olodaterol/tiotropium bromide (Stiolto Respimat) and vilanterol/umeclidinium (Anoro Ellipta).
Combinations of LABA/LAMA bronchodilators with differing mechanisms of action produce a synergic increase in bronchodilation. Therefore, these combinations are recommended in patients with COPD not adequately controlled with monotherapy or when airflow obstruction is very severe and cannot be adequately treated with monotherapy.
According to fee-for-service (FFS) utilization data, combination products containing LABA and inhaled corticosteroids (ICS) are more frequently prescribed for the treatment of moderate to severe COPD than LABA and LAMA combination products. This prescription pattern may reflect the old 2011 Global Initiative for Chronic Obstructive Lung Disease (GOLD) guideline recommendations. However, the updated 2017 GOLD guidelines include new strategies for the management of COPD reflecting the available published literature. Current treatment recommendations for moderate to severe COPD places LABA/LAMA combination products as preferred treatment options over LABA/ICS combination products. LABA/LAMA provides superior efficacy versus LABA/ICS in terms of improvement in lung function and reduction in exacerbation risk in several recent clinical trials. However, there are some study limitations and unclear effects such as the benefit of LABA/LAMA on COPD-related mortality and comorbidities (e.g. cardiovascular disease). Evidence shows that further research is required to better characterize the comparative efficacy and safety among the current available combinations for COPD management. It is currently unclear which group of patients will benefit most from LABA/LAMA or LABA/ICS considering comorbidities (e.g. cardiovascular disease, osteoporosis, anxiety, depression, etc.) and the safety profile of each FDC (e.g. cardiovascular events associated with the use of LABA/LAMA or risk of pneumonia and other adverse events related to the long-term use of an inhaled corticosteroid).
Clinical efficacy: The search strategy performed identified no head-to-head comparisons evaluating the efficacy and safety between LABA/LAMA fixed-dose combination products. A single network meta-analysis indirectly assessing the clinical benefits of four LABA/LAMA FDCs was identified for this review. Results from one comparison of interest involving two

3
FDCs approved in the U.S. (i.e. umeclidinium/vilanterol versus titropium/olodaterol) showed no significant differences between groups with respect to lung function (i.e. change in forced expiratory volume in one second or FEV1 from baseline), exacerbation rates and incidence of discontinuations due to adverse events. Nonetheless, inter-study heterogeneity including different patient’s disease severity and patient’s exacerbation history may have influenced the final results. Direct head-to-head comparisons are needed to better assess the comparative efficacy and safety between the four LABA/LAMA FDCs. Available clinical data regarding LABA/LAMA combination products is outlined in this review. Overall, clinical trials indicated that LABA/LAMA combination products improve lung function, symptoms and health-related quality of life compared to placebo and the mono-components alone. Moreover, trials demonstrated that these FDCs afforded significant benefits in lung function, dyspnea, symptoms, health status, exacerbation rate, rescue medication use, and incidence of pneumonia in comparison to LABA/ICS combinations. No studies compared LABA/LAMA FDCs in a single inhaler with the same drugs administered in separate inhalers.
Clinical safety: Overall, LABA/LAMA FDCs are well-tolerated and adverse events (AEs) reported in clinical trials were typically mild to moderate in severity. The safety profile of FDCs reflects the combination of the AEs specific to each component. An increase in the incidence of AEs has not been observed when both bronchodilators are combined in the same inhaler device. However, both bronchodilators are associated with a risk of cardiovascular events and further investigation is needed in COPD patients with co-morbidities, especially in those with cardiovascular diseases. The most commonly reported AEs with LABA/LAMA FDCs are urinary retention, urinary tract infection, cough, pneumonia, headache, dizziness, chest pain, arthralgia, muscle spasms, glaucoma, increased intraocular pressure, hypersensitivity and cardiovascular effects including tachycardia, palpitations, atrial fibrillation and hypertension. A main LABA class effect Black Box Warning is the increased risk of asthma-related death.
Summary: LABA/LAMA FDCs available in a single inhaler are effective and well-tolerated for the treatment of patients with moderate to severe COPD not responding to monotherapy. Although an indirect comparison performed through a network meta-analysis demonstrated no clinical differences between two of the FDCs available in the U.S, direct head-to-head comparisons are necessary to confirm the comparative efficacy and safety between the different combination products. Cardiovascular events and the risk of asthma-related death are the main safety concerns associated with LABA/LAMA FDCs. Patient adherence to inhalation therapy is important in the management of COPD. The use of a single inhaler providing a simple and intuitive technique, a low dosing-frequency allowing for fewer administrations daily, and educating patients concerning the appropriate inhaler technique may improve adherence to inhalation therapy and symptom control in COPD.

4
Introduction
Chronic Obstructive Pulmonary Disease (COPD) is a preventable, treatable and life-threatening lung disease clinically manifested by dyspnea, chronic cough and/or sputum production due to airway damage and alveolar wall dysfunction.1-3 Tobacco smoke exposure is the foremost risk factor for COPD and the main cause of COPD increase in high and middle income countries.2,4
Management of COPD includes a wide variety of preventive and maintenance interventions including smoking cessation, vaccinations, pharmacological therapy (for stable COPD and management of exacerbations), education and pulmonary rehabilitation.2 The goals of pharmacological treatment for stable COPD are to reduce symptoms, decrease the frequency of acute exacerbations, prevent disease progression, and improve quality of life and exercise tolerance.2 Medications commonly used in stable COPD include short and long-acting β2-agonists (SABA and LABA), short and long-acting muscarinic antagonists (SAMA and LAMA), methylxanthines, phosphodiesterase-4 (PDE4) inhibitors and single device combinations of SABA plus SAMA, LABA plus LAMA, or LABA plus inhaled corticosteroids (ICS). Three drug combination therapy may be used when dual combinations are not effective. The first once daily, triple, fixed-dose combination of LABA, LAMA and ICS for COPD was approved in Europe in May 20175 and another triple FDC is currently under evaluation by the FDA.
This report evaluates the clinical efficacy and safety of LABA plus LAMA combination products based on systematic reviews, meta-analyses and randomized controlled trials (RCTs) assessing head-to-head comparisons between these combination products. Currently, four LABA/LAMA fixed dose combination (FDC) products available in a single inhaler are approved by the Federal Drug Administration (FDA) in the United States: formoterol fumarate/glycopyrrolate (Bevespi Aerosphere),6 indacaterol maleate/ glycopyrrolate (Utibron Neohaler),7 olodaterol/tiotropium bromide (Stiolto Respimat)8 and vilanterol/umeclidinium (Anoro Ellipta).9 Nomenclature used in this report includes a slash ('/') to separate the different active substances contained in a fixed-dose combination (FDC) product. The recently approved 2017 GOLD guidelines2 recommend one of the above LABA/LAMA bronchodilator combinations in COPD patients with persistence of symptoms and further exacerbations receiving monotherapy treatment with a short or long-acting bronchodilator (i.e. groups B, C and D according to the ABCD assessment tool defined by GOLD Guideline for patient classification).1,2 See further information in the clinical guideline section.
Appendix A compares the available COPD medications in terms of therapeutic classes, agents in classes, routes of administration, mechanism of action, labeled indications, and notable adverse effects. Table 1 outlines FDA approved formulations, labeled indications and recommended dosages for LABA/LAMA combinations. Each of the four LABA/LAMA FDC products are administered by oral inhalation and are all indicated for the long-term maintenance

5
therapy of COPD. No generic products are available. An advantage of olodaterol/tiotropium and vilanterol/umeclidinium is once-daily administration compared to formoterol fumarate/glycopyrrolate and indacaterol/glycopyrrolate, which require twice daily administration. A reduction in dosing frequency has been shown to improve patient’s adherence to COPD treatment.10,11 Of note, the indacaterol maleate/glycopyrrolate combination product is approved in the U.S. at lower doses (indacaterol 27.5 mcg/glycopyrrolate 15.6 mcg twice daily) than in Europe and Canada (indacaterol 110 mcg/glycopyrrolate 50 mcg once daily). Most of the evidence available includes the high dose combination product.
Table 1. FDA Approved LABA/LAMA Combination Products for COPD6-9
Active Substances (Brand Name)
Dosage Form(s) and Strengths
Mechanism of Action
Indication Recommended dose
Formoterol fumarate/ Glycopyrrolate (MDI) (Bevespi Aerosphere) Approved:4/2016
Inhalation aerosol: glycopyrrolate 9mcg and formoterol 4.8mcg per inhalation
Formoterol: LABA Glycopyrrolate: LAMA
Long-term maintenance treatment of airflow obstruction in patients with COPD, including chronic bronchitis and/or emphysema Limitations of use: NOT indicated for the relief of acute bronchospasm or for the treatment of asthma
Two inhalations twice daily in the morning and in the evening MAX: 2 inhalations twice daily
Indacaterol maleate/ glycopyrrolate (DPI) (Utibron Neohaler)
Approved: 10/2015
Inhalation powder: indacaterol 27.5mcg and glycopyrrolate 15.6mcg inhalation powder per capsule
Indacaterol: LABA Glycopyrrolate: LAMA
Long-term maintenance treatment of airflow obstruction in patients with COPD, including chronic bronchitis and/or emphysema Limitations of use: NOT indicated for the relief of acute bronchospasm or for the treatment of asthma
Inhalation powder of one capsule twice daily using the NEOHALER device MAX: 2 capsules for inhalation per day

6
Table 1. FDA Approved LABA/LAMA Combination Products for COPD6-9
Active Substances (Brand Name)
Dosage Form(s) and Strengths
Mechanism of Action
Indication Recommended dose
Olodaterol/ tiotropium bromide (SMI) (Stiolto Respimat) Approved: 5/2015
Inhalation spray: olodaterol 2.5mcg and tiotropium 2.5mcg per actuation
Olodaterol: LABA Tiotropium: LAMA
Long-term, once-daily maintenance treatment of airflow obstruction in patients with COPD, including chronic bronchitis and/or emphysema Limitations of use: NOT indicated to treat acute deteriorations of COPD. NOT indicated to treat asthma
Two inhalations once daily at the same time of the day MAX: 2 inhalations in 24 hours
Vilanterol/ umeclidinium (DPI) (Anoro Ellipta)
Approved: 12/2013
Inhalation powder: delivered dose of umeclidinium 62.5mcg and vilanterol 25mcg per inhalation. Inhaler containing 2 foil blister strips of inhalation powder. One strip contains umeclidinium 62.5mcg per blister and the other strip contains vilanterol 25mcg per blister.
Vilanterol: LABA Umeclidinium: LAMA
Long-term, once-daily, maintenance treatment of airflow obstruction in patients with COPD, including chronic bronchitis and/or emphysema Limitations of use: NOT indicated for the relief of acute bronchospasm or for the treatment of asthma
One inhalation once daily MAX: 1 inhalation in 24 hours
Abbreviations: COPD, chronic obstructive pulmonary disease; DPI, dry powder inhaler; LABA, long-acting β2-adrenergic agonist; LAMA, long-acting muscarinic antagonist; MAX: maximum dose; MDI, metered-dose inhaler; SMI, soft mist inhaler
Utah Medicaid Utilization Data
According to Utah Medicaid fee-for-service (FFS) data, the number of unique FFS patients diagnosed with COPD from 2013 to 2017 was 8,824 with only five unique patients (aged 40-64 years old) on treatment with a LABA/LAMA combination product. Table 2 contains the total number of unique patients with COPD, asthma or asthma/COPD diagnosis coding. Table 3 contains the number of patients with these diagnosis codes and on treatment with a FDC or separate inhalers for 2013-2017 period. There was limited utilization for umeclidinium/ vilanterol (13 claims, 4 unique patients) and olodaterol/tiotropium (2 claims, 1 unique patient) during 2013-2017 period. No utilization data for formoterol fumarate/glycopyrrolate or indacaterol maleate/glycopyrrolate was reported during this period. Notably, 16 out of 8,824 patients with COPD diagnosis coding were on treatment with at least two separate inhalers at the

7
same time (i.e. with LABA+LAMA products) instead of using fixed-dose combination products. Concomitant, separate LABA+LAMA inhaler use included salmeterol plus tiotropium (7 patients), formoterol plus tiotropium (6 patient), formoterol plus aclidinium (2 patients) and salmeterol plus aclidinium (1 patient). Although 2017 GOLD guidelines2 identify LABA/LAMA combination products as the preferred option over ICS/LABA combination products, the treatment mainstay for Medicaid FFS patients with COPD not responding to monotherapy is combination therapy containing ICS and LABA. During 2013-2017 period, utilization data show that 502 patients with COPD diagnosis codes submitted were treated with ICS/LABA FDCs and 19 patients were using ICS plus LABA via separate inhalers. In addition, 902 patients with COPD and asthma diagnosis codes submitted were using ICS/LABA FDCs. Currently, ICS/LABA combinations are preferred and LABA/LAMA combinations are non-preferred in the Utah Medicaid Preferred Drug List.
Table 2. Utah Medicaid FFS Patients diagnosed with COPD, Asthma or COPD/Asthma overlap
DIAGNOSIS ICD 2016 2013-2017 period
COPD 491-4928 or 496 3,549 8,824
Asthma without COPD 493 without 4932 5,117 19,449
Asthma and COPD overlap 491-4928 or 493 or 4932 or 496 733 2,955
Abbreviations: COPD, chronic obstructive pulmonary disease, ICD, International Classification of Diseases

8
Table 3. LABA/LAMA or ICS/LABA treatment in Utah Medicaid FFS patients for 2013-2017 period
Combination Products*
Total Unique Patients with Medication
Fills
Total Unique Patients with Either COPD
or Asthma Dx Coding**
Only COPD Dx Coding**
(n= 8,824)
Only Asthma Dx Coding**
(n= 19,449)
Asthma AND COPD Dx Coding** (n=2,955)
No COPD/Asthma
Dx Coding
LABA and LAMA Fixed-dose combinations (LABA/LAMA)
Umeclidinium/vilanterol 4 3 1 0 2 1 Olodaterol/tiotropium 1 1 1 0 0 0 Indacaterol/glycopyrrolate 0 0 0 0 0 0 Formoterol/glycopyrrolate 0 0 0 0 0 0
Separate inhalers in combination*** (LABA+LAMA) Salmeterol + tiotropium 22 12 7 1 4 10 Salmeterol + aclidinium 6 3 1 0 2 3 Formoterol + aclidinium 3 3 2 0 1 0 Formoterol + tiotropium 12 8 6 0 2 4
ICS and LABA Fixed-dose combinations (ICS/LABA)
Budesonide/formoterol 1154 1018 158 602 258 136 Fluticasone/salmeterol 2311 2073 291 1256 526 238 Fluticasone/vilanterol 65 50 9 24 17 15 Mometasone/formoterol 519 447 44 302 101 72
Separate inhalers in combination*** (ICS+LABA) Beclomethasone + formoterol
1 1 1 0 0 0
Beclomethasone + salmeterol 5 4 1 2 1 1 Budesonide + formoterol 17 16 9 1 6 1 Budesonide + salmeterol 1 1 1 0 0 0 Fluticasone + formoterol 8 8 5 0 3 0 Fluticasone + salmeterol 16 14 1 9 4 2 Mometasone + formoterol 1 1 1 0 0 0 Mometasone + salmeterol 3 3 0 2 1 0
Abbreviations: COPD, chronic obstructive pulmonary disease; Dx, diagnosis; FDC, fixed-dose combination; FFS, fee-for-service; ICS, inhaled corticosteroid; LABA, long-acting beta-2 agonist; LAMA, long-acting muscarinic antagonist * Via FDCs or via separate inhalers ** Total unique patients with COPD, asthma or asthma AND COPD diagnosis codes submitted (see table 2) for 2013-2017 period *** Separate single inhalers filled within 30 days

Disease Overview and Clinical Guidelines
A) Chronic Obstructive Pulmonary Disease
Disease Overview:
“Chronic Obstructive Pulmonary Disease (COPD) represents an important public health challenge and is a major cause of chronic morbidity and mortality throughout the world.”12 Around 16 million Americans have been diagnosed with COPD13 and the mortality rate due to COPD has doubled since 1969.13 COPD was the third leading cause of death in the United States in 201414 and the World Health Organization (WHO) has estimated that COPD will rise from the fourth to the third leading cause of mortality worldwide by 2030.2,15 According to the National Heart, Lung and Blood Institute and COPD National Action Plan, COPD kills more than 135,000 Americans each year16. Smoking accounts for 80% of COPD-related deaths although13 25% of cases were not related to cigarette smoking.13 Between 2000 and 2014, the overall incidence of COPD-related deaths declined for both men and women ≥25 years, but increased for the population subsets of men and women aged 45-64 and women aged ≥85.17 The number of people with COPD is increasing “because of continued exposure to risk factors and aging of the population”. Several million people are likely to have undiagnosed COPD due to patient underreporting of symptoms and under-diagnosis by practitioners. 2,16 According to estimates based on the Behavioral Risk Factor Surveillance System (BRFSS, 2015), 79,200 (3.8%) people ≥ 18 years old have COPD in Utah.13 Data provided by the Bureau of Epidemiology of the Utah Department of Health showed “a slow but steady increase in the rate of emergency department visits due to COPD, asthma, and hypersensitivity pneumonitis” from 2000 to 2011, with a monthly rate (higher during winter months) between 3 to 14 people per 100,000 Utahn’s. Monthly hospitalizations rates (4 to 15 people/100,000/month) and death rates (1 to 4 people/100,000/month) due to the above three respiratory diseases remained constant from 2000 to 2011.18
COPD is a progressive disease which includes emphysema, chronic bronchitis, and in some cases asthma.14 It is characterized by chronic coughing (most commonly daily and productive, but also intermittent and unproductive), breathlessness on exertion (initially intermittent and becoming persistent), sputum production (any pattern of sputum production may indicate COPD), and frequent exacerbations of bronchitis.2,19 In the United States, the Centers for Disease Control and Prevention (CDC) reports that tobacco smoke is a key factor in the development and progression of COPD, but other factors such as air pollutants in the home and workplace (e.g. occupational dusts, home cooking and biomass fuels), genetic factors, and respiratory infections also contribute to disease progression.14 Besides genetic factors, abnormal lung development and accelerated aging are also host factors that predispose individuals to develop COPD.2 In relation to COPD and air pollution, the Utah Department of Health recommends checking the air quality before doing any outdoor activity in order to modify the

10
level of exertion, accordingly.18 According to the National Heart, Lung and Blood Institute, COPD most often occurs in people age 40 and over with a history of smoking (either current or former smokers), and several relevant sources report that tobacco smoke is the main risk factor for COPD.1,2,4,13,14 According to the CDC, groups more likely to report COPD include people aged 65–74 years, American Indians/Alaska natives and multiracial non-Hispanics, women, individuals who were unemployed, retired, or unable to work, individuals with less than a high school education, people with lower incomes, individuals who were divorced, widowed, or separated, current or former smokers, and those with a history of asthma.14 In 2010, the annual costs related to COPD for the American health care system were estimated to be more than $32 billion with additional absenteeism costs of $3.9 billion.13,20 Medical costs are projected to increase to $49 billion by 2020.20 The implementation of programs and strategies to prevent COPD are intended to reduce the economic burden of COPD and improve the quality of life of people with COPD.20
Spirometry is considered the gold standard for accurate, reproducible, and objective measurement of lung function and it is the best way of making a definitive diagnosis of asthma and COPD.2,19 However, the GOLD guidelines state that “Despite its good sensitivity, peak expiratory flow measurement alone cannot be reliably used as the only diagnostic test because of its week specificity.”2 Spirometry measures the volume of air that the patient forcibly expels from the lungs after a maximal inspiration (forced vital capacity or FVC) and the air volume exhaled during the first second (forced expiratory volume in one second or FEV1).2,19 Values are compared with predicted normal values (for age, height, sex, and ethnicity) to determine the severity of airway obstruction (e.g. mild, moderate, or severe disease levels).2 A post-bronchodilator FEV1/FVC ratio < 70% confirms the presence of airflow limitation that is not fully reversible.2 Some other measures such as the Modified Medical Research Council (mMRC) dyspnea scale for measuring breathlessness, exacerbation frequency, body mass index, quality of life assessment, and exercise capacity are used to better understand patient’s airflow status. Jones et al (2014) outlined the validated minimal clinically important differences (MCID) for the most frequently used COPD outcomes in placebo-controlled clinical trials. For the lung function outcome, a MCID of 100 ml for FEV1 was established for a COPD treatment to be considered effective. An improvement of 1 unit in the Transition Dyspnea Index (TDI) and a reduction of 4 units in the St George’s Respiratory Questionnaire were defined as MCID. No validated MCID is available for the exacerbation rate.21
COPD is a preventable disease, but once a patient has developed COPD, it is a chronic disease that is largely incurable. The goal of management is to improve a patient’s functional status and quality of life (reducing symptoms and future risk of exacerbations).2 Initially, smoking cessation or avoidance of smoke and other air pollutants is fundamental to prevent or slow disease progression.14,22 According to the WHO, smoking cessation is the single most effective and cost-effective way to reduce the risk of developing COPD and stop its

11
progression.23 The WHO states that brief tobacco dependence treatment is effective and recommends that every tobacco user should be offered this treatment at every health care provider visit.23 The 2017 GOLD guideline includes several smoking cessation pharmacological strategies, such as nicotine replacement products, varenicline and bupropion, and highlights the utility of behavioral support programs.22 COPD pharmacotherapy can alleviate symptoms such as wheezing and coughing, decrease the frequency and severity of exacerbations, and increase exercise tolerance (by acting on bronchial smooth muscle contraction, bronchial mucosal congestion and edema, airway inflammation, and increased airway secretions). Currently, no treatment (aside from lung transplantation) has been shown to significantly improve long-term lung function or decrease mortality.2,14 Reduction of therapy once symptom control has been achieved is not normally possible in COPD and further worsening of lung function usually requires the introduction of additional treatments.23 Medications for the management of COPD include oral inhalation β2-agonists (SABA and LABA), oral inhalation anticholinergics (SAMA and LAMA), corticosteroids (inhaled and systemic), methylxanthines, phosphodiesterase-4 inhibitors, and combinations of short-acting bronchodilators (SABA/SAMA), long-acting bronchodilators (LABA/LAMA), and long-acting β2-agonists with inhaled corticosteroids (LABA/ICS). Bronchodilators on an as-needed basis or on a regular basis provide symptomatic relief but do not reduce disease progression.23,24 The long-term decline in lung function is one of the hallmarks of the disease.2,23 The GOLD pharmacologic treatment algorithm based on group A through D classification (using symptoms and exacerbation history) is discussed in the guideline section.
Patients with COPD often experience acute exacerbations of signs and symptoms which the WHO describes as another hallmark of COPD, and exacerbations and co-morbidities contribute to the overall severity of COPD.23 An exacerbation can be caused by several factors, but most commonly by respiratory tract infections.2 Initial recommendations for pharmacological treatment of an exacerbation include short-acting β2-agonists, with or without short-acting anticholinergics, and short courses (5-7 days) of systemic corticosteroids. Antibiotics are also considered for those with clinical signs of airway infection (e.g., increased volume and change of color of sputum, or fever).2,23 Methylxanthines, which have a narrow therapeutic index, are not recommended due to their unfavorable safety profiles.2,25 GOLD guidelines state that adequate interventions for the prevention of exacerbations should be initiated following an exacerbation, and include bronchodilators (LABAs, LAMAs, LABA+LAMA), corticosteroid-containing regimens (LABA+ICS, LABA+LAMA+ICS), non-steroid anti-inflammatory (roflumilast), anti-infectives (vaccines, long-term macrolides), mucoregulators (N-acetlcysteine, carbocysteine), and others (smoking cessation, rehabilitation, lung volume reduction).2 Selective inhibitors of isoenzyme phosphodiesterase-4 (PDE-4 inhibitors) increase cyclic adenosine monophosphate (cAMP) in inflammatory and immunomodulatory cells reducing airway inflammation.26 The only PDE-4 inhibitor currently available in the U.S. is roflumilast (Daliresp), administered orally

12
and once-daily, to reduce the risk of exacerbations in patients with severe COPD associated with chronic bronchitis and a history of exacerbations (not for the relief of acute bronchospasm).27,28 Azithromycin or erythromycin can also be used to reduce exacerbation risk. GOLD guidelines report that a reduction in the exacerbation risk has been demonstrated with the long-term use over 1 year of azithromycin or erythromycin. However, azithromycin may be linked with an increased risk of bacterial resistance and hearing impairment.22
Patient adherence to COPD treatment is a key component to achieve treatment success, improve health-related quality of life, reduce the risk of hospitalizations and diminish health system costs.10,11,29 Treatment adherence may increase by simplifying dosing regimens (i.e. using medications allowing for lower dosing frequencies such as once daily instead of twice daily), employing an easy-to-use30 and intuitive inhalation device, and using a single inhaler instead of multiple separate inhalers when dual- or triple-combination therapy is necessary.11,29,31
Patients with COPD may also benefit from supplemental oxygen (if blood oxygen levels are low), nonpharmacological interventions such as exercise,14,22,23 and administration of influenza and pneumococcal vaccines to decrease the impact of lower respiratory infections (infections often trigger exacerbations).14,22 Treatment programs such as pulmonary rehabilitation teach COPD management strategies on an individualized basis (e.g. breathing strategies, energy-conserving techniques, and nutritional counseling) to increase quality of life.2,14 It has been reported that COPD patients with poor nutritional status and low body weight have decreased pulmonary status, reduced diaphragmatic mass, poorer exercise capacity, increased mortality rates and reduced quality of life.32
Clinical Guidelines for the Management of COPD
Diagnosis
The Global Initiative for Chronic Obstructive Lung Disease (GOLD) assessment guideline for guiding pharmacotherapy in COPD has progressed from a simple spirometric grading system (classified COPD severity into GOLD 1 to 4 groups according to the predicted FEV1) to the “ABCD” assessment tool in 2011 which combined spirometry, clinical symptoms, and frequency of exacerbations per year,2,33 and currently to the 2017 guideline in which some refinements were included to address concerns with the 2011 tool while “maintaining consistency and simplicity for the practicing clinician.”2,22 In the new guideline, spirometric grades are separated from symptoms and exacerbation history so that patients are first classified as GOLD grades 1-4 (disease severity based on FEV1), and then as Group A-D based on exacerbation history, assessment of symptoms, and risk of future exacerbations.1,2,22
In the current guideline, the GOLD committee recommends, after a confirmed diagnosis by spirometry (post-bronchodilator FEV1/FVC <0.7), further assessment of the patients’ condition by:

13
1. Spirometry to determine the severity of airflow limitation which is graded as GOLD 1=mild (FEV1 ≥80), GOLD 2=moderate (FEV1 50-79), GOLD 3=severe (FEV1 30-49), or GOLD 4=very severe (FEV1 <30)
2. Assessment of symptoms using different questionnaires: a. the Modified Medical Research Council (mMRC) questionnaire for assessment of
dyspnea, i.e. ranging from Grade 0= “I only get breathless with strenuous exercise” to Grade 4= “I am too breathless to leave the house or I am breathless when dressing and undressing.”2
b. the COPD Assessment Test (CAT) for assessment of symptoms. 3. Recording their history of exacerbations in the previous year (0-1 or ≥2 exacerbations)
and prior hospitalizations
Labelling a patient’s COPD condition includes both a grade and a group e.g. GOLD Grade 4, group B.
As stated in the guideline: “This classification scheme may facilitate consideration of individual therapies (exacerbation prevention versus symptom relief)” and “also help guide escalation and de-escalation therapeutic strategies for a specific patient.”2
Smoking Cessation
Current Global Initiative for GOLD guidelines stress the importance of smoking cessation, and include a Cochrane systematic review reference of long-term quit success rates of up to 25% if effective resources and time are dedicated.2,34 The guideline includes a strategic framework for health care providers to help patients stop smoking. The benefit of vaccinations (influenza and pneumococcal), other non-pharmacological treatments, and recommendations for prescription of supplemental oxygen are also included as pharmacological treatments “should be complemented by appropriate non-pharmacological interventions.”2
Pharmacotherapy
The GOLD committee recommends that treatment should “be individualized and guided by severity of symptoms, risk of exacerbations, side-effects, comorbidities, drug availability and cost, and the patient’s response, preference and ability to use various drug delivery devices.”2
Pharmacologic therapy used in COPD includes β2-agonists, anticholinergics, methylxanthines, phosphodiesterase-4 inhibitors, and combinations (including corticosteroids).2 In the past, GOLD recommendations were given for initial therapy according to airflow obstruction (FEV1), symptoms and exacerbations. Currently, the 2017 GOLD guidelines include proposed pharmacologic algorithms based on patients’ symptoms and exacerbation rate (i.e. by ABCD group classification) without considering FEV1 measurement.2,35 Moreover, recommendations are proposed for initiation of therapy and for subsequent escalation and/or de-

14
escalation (considering symptoms and exacerbation risk).2 It is important to note that treatment escalation has not been systematically evaluated and de-escalation strategies only include ICS. The recommendations will be re-evaluated as additional evidence becomes available.2
GOLD guideline recommends the following pharmacologic treatment algorithms for each group (A-D):
Table 4. Pharmacologic treatment algorithms for the management of COPD (GOLD Guidelines)2
GOLD Groups
Symptom Burden
Exacerbation/previous year
Initial, escalation and de-escalation pharmacological strategiesa
A Low (mMRC 0-1,
CAT <10)
0-1 (no hospital admission)
1. Single bronchodilator (short or long-acting bronchodilator)
2. Evaluate and switch to another if necessary;
B High (mMRC ≥2, CAT ≥10)
0-1 (no hospital admission)
1. LAMA or LABA 2. If symptoms persist: LAMA+LABA
Cb Low (mMRC 0-1,
CAT <10)
≥2 or ≥1 leading to hospitalization
1. LAMA 2. If further exacerbations, switch to:
LAMA+LABA (preferred) or LABA+ICS (alternative)
Db High (mMRC ≥2, CAT ≥10)
≥2 or ≥1 leading to hospitalization
1. LABA+LAMA (preferred); some patients may start with LAMA or LABA/ICS
2. If further exacerbations and symptoms persist: TT (LABA+LAMA+ICS)
3. If further exacerbations occurs: Roflumilast (if FEV1<50 and chronic
bronchitis) Macrolide (in former smokers)c Stop ICS
Abbreviations: CAT, COPD assessment test; COPD, chronic obstructive pulmonary disease; GOLD, Global Initiative for Chronic Obstructive Lung Disease; ICS, inhaled corticosteroids; LABA, long-acting β2-adrenergic agonist; LAMA, long-acting antimuscarinic agent; mMRC, modified Medical Research Council; TT, triple therapy; a Based on efficacy and safety data available. GOLD guidelines note that escalation and de-escalation have not been “systematically tested” b Treatment recommendations with lack of supporting direct evidence c Azithromycin is preferred2
The 2017 GOLD guidelines recommend a single bronchodilator for initial therapy in those
groups with lower risk of exacerbations (i.e. groups A and B). LABA/LAMA combination products are recommended as the preferred option in patients with moderate to severe COPD, when symptoms persist or further exacerbations occur on monotherapy treatment with LAMA or

15
LABA (i.e. group B and C). For group D patients, initiate therapy with a LABA/LAMA combination product (preferred treatment) and escalate to triple therapy (LABA+LAMA+inhaled corticosteroids) if further exacerbations occur. Roflumilast or a macrolide may be considered, in certain severe patients if appropriate, and require evaluations and individual management.1,2,22
Comparison data LABA/LAMA vs. Monotherapy or vs. LABA/ICS
Recent evidence from a study published in the New England Journal of Medicine indicates that LABA/LAMA treatment is more effective at reducing exacerbations than LABA/ICS combinations.22,36 The 2017 GOLD guideline reflects this evidence in recommending LABA/LAMA combination as preferred over LABA/ICS combinations (but still keeping it as an alternative).2 The LABA/LAMA combinations in Table 1 reflect the agents listed in the GOLD guideline with the exception of formoterol/aclidinium, currently unavailable in the U.S. Based on RCT evidence (FLIGHT1 and FLIGHT2 trials), the 2017 GOLD guideline states that “a lower dose, twice daily regimen for a LABA/LAMA has also been shown to improve symptoms and health status in COPD patients.”2,37
In stable COPD, the guidelines state the following evidence regarding combination treatment with a LABA plus LAMA:
• “Increases FEV1 and reduces symptoms compared to monotherapy (Evidence A)”2,38
Farne et al. conducted a review to determine the benefits and risks of LABA and LAMA combinations compared to individual components (RCTs of 3 months or longer) and included 10 trials (10,894 participants):
“All of the trials compared tiotropium plus LABA to tiotropium alone, and four trials compared LABA plus LAMA with LABA alone.”38
“Four studies used the LABA olodaterol, three used indacaterol, two used formoterol, and one used salmeterol.” “The results were largely from studies of olodaterol and there was insufficient information to assess whether the other LABAs were equivalent to olodaterol or each other.”38
Salmeterol and formoterol are administered twice daily, indacaterol and olodaterol are administered once daily.38
The authors reported, “a small mean improvement in health-related quality of life and FEV1 for participants on a combination of tiotropium and LABA compared to either agent alone, and this translated into a small increase in the number of responders on combination treatment. In addition, adding tiotropium to LABA reduced exacerbations, although adding LABA to tiotropium did not. Hospital admission and mortality were not altered by adding LABA to tiotropium, although there may not be enough data.”38

16
• “Reduces exacerbations compared to monotherapy (Evidence B) or LABA/ICS (Evidence B)”2
Compared to monotherapy: Wedzicha et al. (2013) evaluated the effect of LABA/LAMA combination (once-daily QVA149: fixed-dose combination of indacaterol 110 mcg and glycopyrronium 50 mcg), to monotherapy (glycopyrronium 50 mcg or tiotropium 18 mcg) for 64 weeks. Results found “superiority of QVA149 versus glycopyrronium for rate of moderate to severe COPD exacerbations (defined by worsening symptoms and categorized by treatment requirements) during treatment.”39 The QVA149 and glycopyrronium arm was double-blind while tiotropium arm was open-label. The authors found that the combination was more effective in preventing moderate to severe exacerbations versus glycopyrronium.39
Compared to LABA/ICS: Wedzicha et al. (2016) in a 52-week non-inferiority trial evaluated LABA/LAMA vs LABA/ICS (LABA indacaterol 110 mcg plus the LAMA glycopyrronium 50 mcg once daily or the LABA salmeterol 50 mcg plus the inhaled glucocorticoid fluticasone 500 mcg twice daily). The primary outcome was the annual rate of COPD exacerbations.36 This non-inferiority trial found that indacaterol/glycopyrronium was not only non-inferior, but more effective than salmeterol/fluticasone in decreasing COPD exacerbations in patients with a history of exacerbation during the previous year.36
Triple Therapy
Evidence presented by the GOLD guidelines supporting stepping up to triple therapy, includes (details of evidence referenced by the GOLD guidance was included to improve understanding):
• “The step up in inhaled treatment to LABA plus LAMA plus ICS (triple therapy) can occur by various approaches.”2,40
o According to Bruselle et al. (2015) “Real-world prescription pathways leading to triple therapy (TT) (inhaled corticosteroid [ICS] plus long-acting beta2-agonist bronchodilator [LABA] plus long-acting muscarinic antagonist) differ from Global initiative for chronic Obstructive Lung Disease [GOLD] and National Institute for Health and Care Excellence treatment recommendations” and they therefore conducted a historical analysis of prescribing pathways in the UK (2002 to 2010). COPD patients without asthma that were receiving TT were identified and pathways from diagnosis to TT were then identified, and LABA plus ICS was identified as the most common prescription pathway to TT. The authors concluded that “Real life UK prescription data demonstrates the inappropriate prescribing of TT and confirms that starting patients on ICS plus LABA results in the inevitable drift to overuse of TT. This study highlights the need for

17
dissemination and implementation of COPD guidelines to physicians, ensuring that patients receive the recommended therapy.”40
• “This may improve lung function and patient reported outcomes.”2,41 o Welte et al (2009): “budesonide/formoterol added to tiotropium versus tiotropium
alone provides rapid and sustained improvements in lung function, health status, morning symptoms and activities, and reduces severe exacerbations.”41
o Singh et al (2008) states that there is little data on triple therapy with salmeterol, fluticasone propionate (SFC) and tiotropium bromide (TIO). They compared the effects of SFC 50/500 mcg twice daily in addition to TIO 18 mcg once daily versus the individual treatments alone, and found greater improvements with triple therapy in terms bronchodilation, as well as advantages in airway conductance, lung volumes, and patient related benefits (improving Transition Dyspnoea Index and use of rescue medication).”42
o Jung et al (2012) states that triple therapy with tiotropium and fluticasone propionate/salmeterol (FSC) is commonly used in COPD, “but no study had evaluated the effectiveness of tiotropium plus FSC with 250 mug of fluticasone propionate.” They therefore evaluated “whether tiotropium (18 mug once daily) plus FSC (250/50 mug twice daily) provides better clinical outcomes compared to tiotropium monotherapy” and found that “Over the course of 24 weeks, FSC (250/50 mug twice daily) added to tiotropium provided greater improvement in lung function and quality of life in patients with COPD (FEV(1) </= 65%) than tiotropium alone.”43
o Hanania et al (2012) evaluated the efficacy and safety of triple therapy: “fluticasone/salmeterol (FSC) (250/50 mcg twice daily) when added to tiotropium (18 mcg once daily) (TIO)” and found that it “significantly improves lung function without increasing the risk of adverse events.”44
• “Adding a LAMA to existing LABA/ICS improves lung function and patient reported outcomes, in particular exacerbation risk.”2 42,45-47
• “A RCT did not demonstrate any benefit of adding ICS to LABA plus LAMA on exacerbations.”2,48
• “Altogether, more evidence is needed to draw conclusions on the benefits of triple therapy LABA/LAMA/ICS compared to LABA/LAMA.”2

18
B) COPD and Asthma
Disease overview
According to the updated Joint Project of GINA and GOLD (April 2017),49 “asthma-COPD overlap is characterized by persistent airflow limitation with several features usually associated with asthma and several features usually associated with COPD. Asthma-COPD overlap is therefore identified in clinical practice by the features that it shares with both asthma and COPD”. This project includes new recommendations for patients with both COPD and asthma. The correct identification of these patients and adequate treatment decisions remain a challenge. Some patients are borderline between asthma and COPD because they share asthma and COPD symptoms. This is especially common in smokers and the elderly. Given that this condition is considered a combination of asthma and COPD characteristics, the usual term used in previous guideline versions (i.e “Asthma COPD Overlap Syndrome (ACOS)”) is no longer recommended. Currently, the Joint Project of GINA and GOLD considers that “asthma-COPD overlap” is the most appropriate term.49
Diagnosis of patients with respiratory symptoms is based on a stepwise process including: a) identification of patients with chronic airway disease by clinical history evaluation, physical examination and other investigations, b) differentiation between typical asthma, typical COPD and asthma-COPD overlap by exploring the usual features, c) assessment of airflow limitation by spirometry, and d) referral to a specialist in special situations.49
Clinical Guidelines for the Management of Asthma-COPD Overlap
The treatment recommendations outlined in table 5 are based on limited clinical evidence since studies conducted in this type of population are lacking.49
Table 5. Recommendations for Initial Treatment in Patients with Asthma-COPD Overlap49* Diagnosis Symptoms Initial Treatment
Asthma Features of asthma - Asthma drugs (adequate ICS as controller therapy)
- NO LABA monotherapy Possible Asthma Some features of asthma
Asthma-COPD Overlap Features of both asthma and COPD - Low/moderate dose ICS and consider LABA +/or LAMA
COPD Features of COPD - COPD drugs (bronchodilators or ICS/bronchodilator)
- NO ICS alone Possible COPD Some features of COPD
Abbreviations: COPD, chronic obstructive pulmonary disease; GINA, global initiative for asthma; GOLD, global initiative for chronic obstructive lung disease; ICS, inhaled corticosteroids; LABA, long-acting beta2 agonists; LAMA, long-acting muscarinic antagonist * See GINA and GOLD guidelines for further information about recommended treatments

19
Pharmacology The mechanism of action of long-acting beta2 agonists (LABAs) such as formoterol, indacaterol, olodaterol and vilaterol is characterized by the relaxation of bronchial smooth muscle due to the selective activation of beta2 receptors.50 Long-acting muscarinic antagonists (LAMAs) include tiotropium, umeclidinium, glycopyrrolate and aclidinium, which act by producing a bronchodilation effect via blocking muscarinic receptors located on bronchial smooth muscle cells.51 Evidence indicates that the combination of two bronchodilator agents with different mechanisms of action provides synergic benefits in patients with moderate COPD, without increasing the incidence of cardiovascular and severe adverse events compared to monotherapy or placebo.50,52 In addition, several animal studies suggest a positive interaction between LABA and LAMA, with both agents decreasing the release of acetylcholine and reducing bronchoconstriction.50
Products combining both LABA and LAMA in one device provide a rapid onset of action that ranges from 5 to 20 minutes and a bronchodilation effect that lasts from 12 to 24 hours.6-9,53 The long duration of action allows once or twice daily administration, which may improve treatment adherence.10,11,29,31
LABA and LAMA are administered by inhalation route, primarily metabolized by the liver via the cytochrome P450 system, excreted through urine or feces and eliminated with a half-life of 7.5 to 56 hours.25 Table 6 outlines the main pharmacokinetic characteristics of LABA/LAMA combination products. Drug-drug interactions may occur, especially with formoterol, indacaterol, olodaterol, vilanterol and umeclidinium, which undergo extensive hepatic metabolism. For instance, vilanterol is a substrate of CYP3A49 and indacaterol hydroxylation is mainly metabolized by the isoenzyme CYP3A4.7 Olodaterol is primarily metabolized by CYP2C9 and marginally by CYP3A4. Systemic exposure to vilanterol, indacaterol and olodaterol may be amplified when they are concomitantly administered with inhibitors of cytochrome P450 3A4 such as ketoconazole, verapamil, erythromycin and ritonavir or CYP2C9 inhibitors like fluconazole.54 However, studies have shown that no dosage adjustment of LABA/LAMA combinations is required. LABA/LAMA combination products should be used with caution when administered concurrently with other adrenergic drugs (LABAs’ effects may be increased), xanthine derivatives, steroids, diuretics or non-potassium sparing diuretics (hypokalemia and electrocardiograph changes produced by LABA may be worsened), monoamine oxidase inhibitors, tricyclic antidepressants, QTc-prolonging drugs (LABAs’ cardiovascular events may increase), beta blockers (the effect of beta-agonists may be reduced and the risk of severe bronchospasm may increase) and anticholinergics (anticholinergic adverse events may increase).6-9

20
Table 6. Pharmacokinetics of LABA/LAMA Combination Products for COPD25,53
Active Substance (Combination
Products) Absorption Protein
binding Metabolism Excretion Elimination (half-life)
Onset of action
(Time to peak concentration)
Duration of action
Formoterol
(Formoterol fumarate/
glycopyrrolate)
Rapidly into plasma 61% to 64%
Hepatic; CYP2D6,CYP2C19,CYP2C9 and
CYP2A6; direct glucuronidation (primary pathway), O-
demethylation and glucuronide conjugation
Children 5-12 years: Urine (7% to 9% as direct glucuronide metabolites, 6% as unchanged drug)
Adults: Urine (15%
to 18% as direct glucuronide
metabolites, 2% to 10% as unchanged
drug)
10-14 hr Powder for inhalation:
3 min Peak effect:
15 min
12 hr
Glycopyrrolatea
(Formoterol fumarate/
glycopyrrolate)
BA: Inhalation (40%) 38% to 41%
Hepatic: minimal, via oxidation and hydrolysis
Urine: 60% to 85% Bile: < 5% (> 80%
unchanged)
33 to 53 hr 5 min 12 hr
Indacaterol
(Indacaterol maleate/
glycopyrrolate)
BA: Inhalation (43 to 45%)
~95% Hepatic: hydroxylated via CYP3A4, CYP2D6, and CYP1A1
Feces (>90%; 54% as unchanged drug
after oral administration);
urine (<2% as unchanged drug)
40 to 56 hr 15 min 24 hr
Olodaterol
(Olodaterol/ tiotropium bromide)
BA: Inhalation (30% to 49.4%)
60% Hepatic: extensive direct glucuronidation (UGT2B7,
UGT1A1, 1A7, and 1A9) and O-demethylation (primarily
CYP2C9 and 2C8)
Urine (5% to 7% unchanged)
Feces
7.5 hr 10-20 min 24 hr
Tiotropium
(olodaterol/ tiotropium bromide)
• Systemic absorption from lungs
• BA: Inhalation (spray), 33%
72% Hepatic: minimal, via CYP2D6 and CYP3A4
Urine: 18.6% of an inhaled dose
(COPD). Remainder eliminated via feces
25 hr 5 to 7 min 24 hr

21
Active Substance (Combination
Products) Absorption Protein
binding Metabolism Excretion Elimination (half-life)
Onset of action
(Time to peak concentration)
Duration of action
Vilanterol
(Vilanterol/ umeclidinium)b
Systemic, primarily via lungs
94% Hepatic: extensive; via CYP3A4 Urine (70% vilanterol); Feces (30% vilanterol)
11 hr
UMEC/VI: 5 to 15 min
24 hr
Umeclidinium
(Vilanterol/ umeclidinium)b
Systemic, primarily via lungs
89% Hepatic: extensive; via CYP2D6 Urine (<1%); Feces (92%)
11 hr 24 hr
Abbreviations: BA, bioavailability; COPD, chronic obstructive pulmonary disease; min, minute; hr, hour; LABA, long-acting β2-adrenergic agonist; LAMA, long-acting antimuscarinic agent; UMEC, umeclidinium; VI, vilanterol a Different doses available for glycopyrrolate (Europe: 50 mcg of glycopyrrolate;55 United States: 15.6 mcg of glycopyrrolate).6 In this report, only data for the U.S. formulation is outlined. b Vilanterol is only available taking part of dual combinations

22
Special Populations
Table 7 describes the recommendations for LABA/LAMA combination product use in special populations.
In general, no dosage adjustment is required in patients with mild to moderate renal impairment. In patients with severe renal impairment or end-stage renal disease, package inserts of formoterol/glycopyrrolate, indacaterol/glycopyrrolate and olodaterol/tiotropium bromide indicate that these combinations should be used with caution or if benefits outweigh the potential risks.6-9
In patients with mild to moderate hepatic impairment, no dose adjustments are required. Overall, no recommendations are provided for patients with severe hepatic impairment since no studies have been performed. However, the package insert of formoterol/glycopyrrolate states that caution should be exercised in those patients with severe hepatic impairment since systemic exposure to formoterol may increase.6-9
The four available LABA/LAMA combination products are not indicated for pediatric patients since safety and efficacy in this population has not been established. In the geriatric population, studies involving patients 65 years and older demonstrated no differences in efficacy or safety between age groups. No dosage adjustments are required in geriatric patients.6-9
In pregnancy and lactation, no adequate and well-controlled studies of LABA/LAMA FDCs are available and the use of these products during pregnancy and lactation should be assessed in relation to the benefit for the mother and the risk for the fetus. Beta-agonists may affect uterine contractility. Careful use is advised when these combinations are administered during labor and delivery.6-9
Comorbidities associated with COPD may include lung cancer, cardiovascular disease (heart failure, arrhythmias, peripheral vascular disease and hypertension), osteoporosis, depression/anxiety and gastroesophageal reflux. These may worsen COPD or increase respiratory symptoms. Treatment for the management of COPD should not be modified. In addition, each comorbid disease should be appropriately treated.1,2

23
Table 7. Recommendations for Special Populations of LABA/LAMA Combination Products for COPD6-9,25,53 Active
Substance (Combination
Products)
Renal Impairment Hepatic Impairment Pregnancy and lactation Pediatric Geriatric
Formoterol fumarate/
glycopyrrolate
• CrCl >30 mL/min/1.73 m2: studies not performed
• CrCl ≤30 mL/min/1.73 m2 or ESRD requiring dialysis: studies not performed, use with caution. Use if benefits outweigh potential risks
• Studies not performed
• No dosage adjustment
• Use with caution in patients with hepatic impairment since formoterol levels may increase
Pregnancy: U.S. FDA pregnancy Category: C. It should be used during pregnancy only if the potential benefit justifies the potential risk to the fetus Lactation: Not known whether this combination is excreted in human milk. A decision should be made whether to discontinue nursing or discontinue glycopyrrolate/formoterol, considering the mother's clinical need for therapy Labor and delivery: potential for β-agonist interference with uterine contractility. Use restricted to those patients in whom the benefits clearly outweigh the risks
Safety and efficacy
not established in children
No adjustment
required
Indacaterol maleate/
glycopyrrolate
• Mild to moderate renal impairment: No dosage adjustment
• Severe renal impairment or ESRD: Use if benefits outweigh potential risks
• No dosage adjustment. Use with caution in patients with severe hepatic impairment
Pregnancy: U.S. FDA pregnancy Category: C. It should be used during pregnancy only if the potential benefit justifies the potential risk to the fetus Lactation: Not known whether this combination is excreted in human milk. A decision should be made whether to discontinue nursing or discontinue indacaterol/glycopyrrolate, considering the mother's clinical need for therapy Labor and delivery: potential for β-agonist interference with uterine contractility. Use restricted to those patients in whom the benefits clearly outweigh the risks
Safety and efficacy
not established in children
No adjustment
required
Olodaterol/ tiotropium
bromide
• CrCl >60 mL/min: No dosage adjustment necessary
• CrCl ≤60 mL/min: No dosage adjustment necessary; monitor closely for anticholinergic adverse effects
• No adjustment required
• No studies performed in severe hepatic impairment
Pregnancy: U.S. FDA pregnancy Category: C. It should be used during pregnancy only if the potential benefit justifies the potential risk to the fetus Lactation: Not known whether this combination is excreted in human milk, but caution should be exercised Labor and delivery: potential for β-agonist interference with uterine contractility. Use restricted to those patients in whom the benefits clearly outweigh the risks
Safety and efficacy
not established in children
No adjustment
required
Vilanterol/ Umeclidiniuma
No adjustment required • No adjustment required
• No studies performed in severe hepatic impairment
Pregnancy: U.S. FDA pregnancy Category: C. It should be used during pregnancy only if the potential benefit justifies the potential risk to the fetus Lactation: Not known whether this combination is excreted in human milk. A decision should be made whether to discontinue nursing or discontinue vilanterol/umeclidinium, considering the mother's clinical need for therapy Labor and delivery: potential for β-agonist interference with uterine contractility. Use restricted to those patients in whom the benefits clearly outweigh the risks
Safety and efficacy
not established in children
No adjustment
required
Abbreviations: CrCl, creatinine clearance; ESRD, end-stage renal disease; COPD, chronic obstructive pulmonary disease; LABA, long-acting β2-adrenergic agonist; LAMA, long-acting anti-muscarinic agent a Vilanterol is only available taking part of dual combinations

24
Methods Literature Search
Search strategies were developed by an Informational Scientist for OVID Medline and EMBASE. Strategies consisted of controlled vocabulary, such as MeSH, and keyword phrases. Two methodological filters were used, one for systematic reviews and another for randomized controlled trials (RCT). Results were limited to English language. Databases were searched from date of inception forward. In EMBASE we excluded conference abstracts. Searches were conducted in May 2017. The complete search strategies and terms are available in Appendix B.
We also screened the reference lists of related systematic reviews. Likewise, we searched other websites for further information:
1. The National Institute of Health (NIH), The National Heart, Lung, and Blood Institute (NHLBI), the World Health Organization (WHO), the Centers for Disease and Control (CDC) and the Global Initiative for Chronic Obstructive Lung Disease (GOLD) websites for the most recent COPD treatment guidelines.
2. Food and Drug Administration (Drugs@FDA: FDA Approved Drug Products: https://www.accessdata.fda.gov/scripts/cder/daf/) for prescribing information package inserts
3. Evidence based drug information databases (Micromedex, Lexicomp, and UpToDate)
Screening
At least two review authors screened titles and abstracts. The full text for all citations receiving two inclusion votes was retrieved; screening and inclusion were determined by the lead author. Conflicts were resolved via discussion between reviewers or a third person. Figure 1 shows the PRISMA flow chart56 for the review process.
Inclusion and Exclusion Criteria
Systematic reviews and RCTs providing head-to-head efficacy comparisons between the LABA/LAMA combination products were included. For product comparisons where a systematic review provided robust data, we examined only those trials or systematic reviews published after the search date of the robust systematic reviews. The GOLD guidelines, published in 2017, contain the most recent and relevant evidence available for the four fixed dose combination products. We searched for RCTs along the last year (from May 2016 to May 2017).
A list containing the excluded references is provided in Appendix E.
References were excluded if they met the following exclusion criteria:
• Studies evaluating non-FDA-approved doses

25
• Other types of studies (e.g. non-comparative or non-randomized trials, placebo-controlled studies, phase 2 studies, observational studies, in vitro studies, animal studies, cost-effectiveness studies, etc.)
• Reviews not using a systematic review methodology
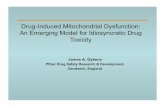
Figure 1. PRISMA Flow Diagram of the selection process
Records identified through database searching
(n = 247)
Scre
enin
g In
clud
ed
Elig
ibili
ty
Iden
tific
atio
n
Additional records identified through other sources
(n = 1)
Records after duplicates removed (n = 246)
Records screened (n = 246)
Records excluded (n = 233)
Full-text articles assessed for eligibility
(n = 13)
Full-text articles excluded, with reasons
(n = 12) • Wrong comparator (9) • Only abstract available (3)
Studies included in qualitative synthesis
(n = 1 network meta-analysis)

26
Clinical Efficacy
Clinical evidence involving head-to-head comparisons among LABA/LAMA combination products is presented for the products currently available in the United States. Overall, from 248 references identified using the developed search strategy (133 systematic reviews and 115 randomized controlled trials), one network meta-analysis57 was identified. No direct head-to-head trials comparing LABA/LAMA FDC products were identified, limiting the assessment of efficacy and safety differences of the various LABA/LAMA FDCs. Likewise, no studies were found comparing the LABA/LAMA FDCs in a single inhaler with the same drugs administered concurrently in separate inhalers.
LABA/LAMA vs. LABA/LAMA
One network meta-analysis including indirect comparisons among the available LABA/LAMA FDCs at that time was identified. Four FDCs including tiotropium/olodaterol, umeclidinium/vilanterol, glycopyrronium/indacaterol and aclidinium/formoterol were evaluated. For FDA approved combinations, results indicated similar clinical benefits in terms of lung function (i.e. FEV1 improvement), exacerbation rate and incidence of discontinuations due to adverse events with tiotropium/olodaterol compared to umeclidinium/vilanterol in the maintenance of COPD. Nonetheless, the differences between studies on disease severity at baseline and the inclusion of patients with different exacerbation histories limit this network meta-analysis. In order to avoid the challenges associated with indirect comparison, direct head-to-head comparison is needed to determine clinical differences among LABA/LAMA fixed-dose combinations. Results from the network meta-analysis included in this review are outlined in Appendix C.
Evidence currently available from RCTs leading to FDA approval and relevant guidelines was extracted for informational purposes. Key randomized controlled trials leading to the FDA approval of the four LABA/LAMA FDCs, and additional evidence is provided in Appendix D. Overall, studies including LABA/LAMA combinations were performed in patients with moderate to severe COPD. The most common primary endpoints recommended by the FDA24 and measured throughout the clinical trials were: a) change in trough post-dose FEV1 from baseline, b) assessment of symptoms (dyspnea, cough, etc), c) exacerbation risk (e.g. duration, severity, reduction in frequency and delay in the occurrence of exacerbations), and d) disease progression.
LABA/LAMA vs. monotherapy, placebo or tiotropium
Several randomized clinical trials, systematic reviews and meta-analyses have demonstrated a greater bronchodilator effect (i.e. increase in FEV1) and improvements in symptoms and health-related quality of life when LABA/LAMA combinations were compared to

27
monotherapies37,38,58-61 or placebo62,63 in patients with moderate to severe COPD not responding to single bronchodilators (LABA or LAMA). Evidence demonstrated that LABA/LAMA FDCs are more effective in terms of change in lung function from baseline, dyspnea and quality of life than tiotropium alone38,58,61. However, no differences in the risk of exacerbations were reported between LABA/LAMA and LAMA groups.38,64
LABA/LAMA vs. LABA/ICS
Studies comparing LABA/LAMA FDCs versus LABA/ICS combinations (e.g. salmeterol/fluticasone) in patients with COPD showed improvements in trough FEV1, lower moderate and/or severe exacerbation rate, reduced use of rescue medications and lower incidence of pneumonia with the LABA/LAMA group compared to LABA/ICS group.36,58,61,65 No differences were observed with respect to dyspnea and St George’s Respiratory Questionnaire scores between LABA/LAMA and ICS/LABA treatment groups.58 These consistent results have led to the inclusion of LABA/LAMA FDCs as preferred treatment options in patients with moderate to severe COPD not responding to monotherapy, with LABA/ICS FDCs being the alternative therapies.2

28
Safety
Overall, LABA/LAMA FDCs are well-tolerated and the adverse events (AEs) reported in clinical trials were usually of mild to moderate severity. The safety profile of FDCs is characterized by the combination of the AEs specific to each component. LAMAs usually present a better safety profile than LABAs, but both components are associated with a risk of cardiovascular events.66 The most commonly AEs reported with LABA/LAMA FDCs and occurring with an incidence of 1 to 10% are urinary retention, urinary tract infection, cough, pneumonia, headache, dizziness, chest pain, arthralgia, muscle spasms, glaucoma, increased intraocular pressure, hypersensitivity and cardiovascular effects including tachycardia, palpitations, atrial fibrillation and hypertension.6-9,66 Clinical trials comparing LABA/LAMA FDCs versus monotherapies have not demonstrated an increase in the incidence of AEs.66 Further investigation is needed in COPD patients with co-morbidities, especially in those with cardiovascular diseases.66 Several safety warnings and precautions included in the LABA/LAMA package inserts are associated with the LABA component of the combination. . A class effect of all LABAs is the increased risk of asthma-related death. This information comes from the results of a trial comparing salmeterol (LABA) versus placebo (each combined with usual asthma therapy), which showed an increased risk in death associated with asthma in the salmeterol group (relative risk: 4.37 [95% CI: 1.25, 15.34]). Other important warnings include paradoxical bronchospasm, a rare but life-threatening, cardiovascular effect and the restriction of use in patients with acute deterioration of COPD or acute bronchospasm due to limited clinical data. Table 8 includes further safety information on LABA/LAMA combinations.
One network meta-analysis performed by Oba et al evaluated the efficacy and safety of LABA/LAMA FDCs versus monotherapies and showed no significant differences between groups in terms of mortality, total serious adverse events (SAEs) and discontinuations due to AEs.67 Glycopyrronium/indacaterol 27.5/15.6 mcg administered twice daily was the first FDA approved LABA/LAMA FDC. Results from FLIGHT1 and FLIGHT2 trials37 indicated a similar safety profile (incidence of AEs, SAEs and cardiovascular events) between the FDC and the monocomponents or placebo, with COPD worsening being the most frequently reported AEs in all treatment arms. In addition, the safety profile of the higher dose of glycopyrronium/indacaterol (110/50 mcg administered once daily; dose not approved in the U.S.) is well-characterized since it has been extensively studied in trials over 64 weeks.68 A pooled safety analysis of 14 trials,69 and several studies such as those conducted by Van de Maele et al70, Bateman71 and Dahl et al72 showed comparable safety outcomes (incidence of AEs, SAEs and cardiovascular events) between glycopyrronium/indacaterol 110/50 mcg and the monocomponents, placebo, tiotropium or salmeterol/fluticasone propionate.36,66,68,73 Cardiovascular safety was demonstrated for this FDC with respect to heart rate, corrected QT interval and electrocardiogram parameters.66,73 Regarding the umeclidinium/vilanterol

29
combination, some studies reported a higher incidence of cardiovascular effects (e.g. atrial fibrillation, ventricular extrasystoles and sustained supraventricular tachycardia) in the FDC compared to placebo.66 For tiotropium/ olodaterol, the two, 52-week, TONADO studies 74 and a safety analysis75 showed similar safety results (including major cardiac events) between the FDC and the monocomponents.66 Glycopyrronium/formoterol was evaluated in a long-term safety trial (52-week duration). Results showed no differences between the FDC and the monocomponents or tiotropium in the incidence of AEs and major adverse cardiovascular events.76
Table 8. Adverse Effects and Warnings of LABA/LAMA Combination Products for COPD6-9,25,53
Combination Product Adverse Effects Black Box, warnings and precautions
Formoterol fumarate/
glycopyrrolate
>2%: Renal: Urinary tract infectious disease (2.6%) Resp: Cough (4%) 1% to <2%: CNS: headache, dizziness, anxiety CV: chest pain GI: vomiting NMS: Arthralgia, muscle spasms, pain in extremity Others: tooth abscess, oropharyngeal pain, dry mouth, fall, influenza, fatigue, acute sinusitis, and contusion AE associated with formoterol: hypersensitivity reactions, hyperglycemia, sleep disturbance, agitation, restlessness, tremor, nausea, tachycardia, palpitations, cardiac arrhythmias (atrial fibrillation, supraventricular tachycardia, and extrasystoles)
• Black Box: ASTHMA-RELATED DEATH associated to LABA component. This is considered a class effect among all LABAs. Safety and efficacy of these FDCs have not been established in patients with asthma
• Not indicated in patients with acute deterioration of COPD or acute bronchospasm
• Excessive use of the FDC or use with other LABAs may cause overdose and produce life-threatening CV effects
• Paradoxical bronchospasm: rare but life-threatening
• CNS depression: drowsiness, dizziness, and/or blurred vision
• Immediate hypersensitivity reactions: angioedema, urticarial or skin rash (discontinue therapy immediately)
• CV effects: LABA may increase pulse rate, blood pressure, ECG changes, prolongation of QTc interval
• Be alert to hypokalemia, and hyperglycemia
• Use with caution in patients with: CV disease, diabetes, hepatic impairment, hyperthyroidism, hypokalemia, narrow angle glaucoma, renal impairment, seizure disorders, urinary retention
Indacaterol maleate/
glycopyrrolate
1% to 10%: CV: Hypertension (2%) GI: Diarrhea (2% or more), Gastroesophageal reflux disease (2% or more) Neuro: Headache (2% or more) Resp: Nasopharyngitis (4.1%), Rhinitis (2% or more), Pneumonia (2% or more) <1%: CV: Atrial fibrillation, Chest pain, Tachycardia, palpitations Immuno: Hypersensitivity reaction GI: dyspepsia, gastroenteritis Renal: bladder obstruction/urinary retention General: fatigue, peripheral edema
Olodaterol/ tiotropium
bromide
>3%: NMS: Backache (3.6%) Resp: Nasopharyngitis (12.4%), Cough (4%) ≤3%: Metab: dehydration CNS: dizziness, insomnia Ophth: glaucoma, intraocular pressure increased, vision blurred CV: atrial fibrillation, palpitations, supraventricular tachycardia, tachycardia, hypertension

30
Combination Product Adverse Effects Black Box, warnings and precautions
Resp: epistaxis, pharyngitis, dysphonia, bronchospasm, laryngitis, sinusitis GI: dry mouth, constipation, oropharyngeal candidiasis, dysphagia, gastroesophageal reflux disease, gingivitis, glossitis, stomatitis, intestinal obstruction including ileus paralytic Skin: rash, pruritus, angioneurotic edema, urticaria, skin infection, and skin ulcer, dry skin, hypersensitivity NMS: arthralgia, joint swelling Renal: urinary retention, dysuria, and urinary tract infection
Vilanterol/ umeclidinium
1% to 10%: CV: Chest pain (1%) GI: Constipation (1%), Diarrhea (2%) NMS: Neck pain (1%), Pain in limb (2%), Spasm (1%) Resp: Lower respiratory tract infection (1%), Pharyngitis (2%), Sinusitis (1% or greater) Postmarketing experience (frequency not defined) CNS: Dysgeusia, tremor CV: Palpitations Ophth: Blurred vision, glaucoma, increased intraocular pressure Immuno: Hypersensitivity reaction Psy: Anxiety Renal: Dysuria, urinary retention Resp: Paradoxical bronchospasm
Abbreviations: CNS, central nervous system; COPD, chronic obstructive pulmonary disease; CV, cardiovascular; Derm, dermatologic; ECG, electrocardiogram; Endo, Endocrine; FDC, fixed-dose combinations; GI, gastrointestinal; GU, genitourinary; Hema&onco, hematologic and oncologic; HSR, hypersensitivity reaction; ICP, intracranial pressure; Immuno, Immunologic; LABA, long-acting β2-adrenergic agonist; LAMA, long-acting antimuscarinic agent; Metab, metabolic; Misc, miscellaneous; Neuro, Neurologic; NMS, neuromuscular system; Onc, oncologic; Ophth, Opthamologic; Psy, Psychiatric; Resp, respiratory

31
Summary
LABA/LAMA combination products are indicated for patients with moderate to severe COPD that is not well-managed with monotherapy (i.e. LABA or LAMA). According to the updated 2017 GOLD guidelines, LABA/LAMA FDCs are the preferred treatment option, with LABA/ICS FDCs being appropriate alternative therapies. Clinical trials demonstrated superior efficacy with LABA/LAMA versus LABA/ICS in terms of lung function and exacerbation risk. These treatment recommendations are not yet reflected in the Medicaid FFS prescription usage patterns, where FFS utilization data show that LABA/ICS combinations are prescribed more frequently than LABA/LAMA combinations for moderate to severe COPD. GOLD guidelines also highlight that none of the existing medications for COPD have been conclusively shown to modify the long-term decline in lung function.
No direct head-to-head comparisons of LABA/LAMA combinations were identified. One network meta-analysis with important inter-study heterogeneity (e.g. different patients’ disease severities and patients’ exacerbation histories) showed no statistically significant differences with respect to lung function, exacerbation rates and incidence of discontinuations due to adverse events between umeclidinium/vilanterol and titropium/olodaterol (two of the four U.S. available LABA/LAMA FDCs). Clinical evidence confirms that combination products containing LABA/LAMA are more effective than monotherapy (increases FEV1, reduces symptoms and improves exacerbations), tiotropium (improves lung function, dyspnea and quality of life) and ICS/LABA (increases FEV1, reduces exacerbations and diminish pneumonia incidence rate).
Direct head-to-head comparisons involving LABA/LAMA combinations are required to enhance the understanding of the potential benefits of one fixed-dose combination over another in patients with moderate to severe COPD. Further research is necessary to identify the groups of patients that will benefit most from LABA/LAMA or LABA/ICS, considering comorbidities (e.g. cardiovascular disease) and the safety profile of each FDC (e.g. cardiovascular events are associated with the use of a LABA/LAMA and the risk of pneumonia and several adverse events are related to the long-term use of an inhaled corticosteroid).
The most common AEs reported with LABA/LAMA FDCs are urinary retention, urinary tract infection, cough, pneumonia, headache, dizziness, chest pain, arthralgia, muscle spasms, glaucoma, increased intraocular pressure, hypersensitivity and cardiovascular effects including tachycardia, palpitations, atrial fibrillation and hypertension. One of the main safety warnings and a class effect of all LABAs is the increased risk of asthma-related death.
The available four LABA/LAMA combinations have differing frequencies of administration (once daily and twice daily). Olodaterol/tiotropium and umeclidinium/vilanterol are administered once daily whereas formoterol fumarate/glycopyrrolate and indacaterol maleate/glycopyrrolate are administered twice daily.25,53 Device characteristics and inhalation techniques differ between products, and patients should be adequately trained by health professionals to assure the correct use of inhalers. Patient adherence to inhalation therapy is important in the management of COPD. The use of a single inhaler providing a simple and intuitive technique, a low-dosing frequency allowing for fewer administrations daily, and educating patients concerning the appropriate inhaler technique may improve adherence to inhalation therapy, treatment efficacy, and health-related quality of life. This may also reduce the risk of hospitalizations and health system costs.

32
References 1. Vogelmeier CF, Criner GJ, Martinez FJ, et al. Global Strategy for the Diagnosis, Management,
and Prevention of Chronic Obstructive Lung Disease 2017 Report: GOLD Executive Summary. Archivos de bronconeumologia. 2017;53(3):128-149.
2. Global Strategy for the Diagnosis, Management and Prevention of COPD, Global Initiative for Chronic Obstructive Lung Disease (GOLD) 2017. http://goldcopd.org.
3. Reilly JJ, Silverman EK, Shapiro SD. Chapter 260. Chronic Obstructive Pulmonary Disease. In: Longo DL, Fauci AS, Kasper DL, Hauser SL, Jameson JL, Loscalzo J, eds. Harrison's Principles of Internal Medicine, 18e. New York, NY: The McGraw-Hill Companies; 2012.
4. Chronic respiratory diseases. Chronic obstructive pulmonary disease (COPD). Causes of COPD. World Health Organization (WHO). http://www.who.int/respiratory/copd/causes/en/. Accessed May 24, 2017.
5. Trimbow. European Medicines Agency. http://www.ema.europa.eu/ema/index.jsp?curl=pages/medicines/human/medicines/004257/smops/Positive/human_smop_001142.jsp&mid=WC0b01ac058001d127&source=homeMedSearch&category=human. Accessed 06 June, 2017.
6. Bevespi Aerosphere® (formoterol fumarate/glycopyrrolate) inhalation aerosol [package insert]. Wilmington, DE: AstraZeneca Pharmaceuticals LP; revised April 2016.
7. Utibron® Neohaler® (indacaterol and glycopyrrolate) inhalation powder [package insert]. East Hanover, New Jersey: Novartis Pharmaceuticals Corporation; revised January 2017.
8. Stiolto® Respimat® (tiotropium bromide and olodaterol) inhalation spray [package insert]. Ridgefield, CT: Boehringer Ingelheim Pharmaceuticals, Inc.; revised June 2016.
9. Anoro® Ellipta® (umeclidinium and vilanterol) inhalation powder [package insert]. Research Triangle Park, NC: GlaxoSmithKline; revised March 2017.
10. Toy EL, Beaulieu NU, McHale JM, et al. Treatment of COPD: relationships between daily dosing frequency, adherence, resource use, and costs. Respiratory medicine. 2011;105(3):435-441.
11. Bourbeau J, Bartlett SJ. Patient adherence in COPD. Thorax. 2008;63(9):831-838. 12. Global initiative for chronic obstructive lung disease (GOLD). Pocket guide to COPD diagnosis,
management, and prevention. A Guide for Health Care Professionals 2017 http://goldcopd.org/wp-content/uploads/2016/12/wms-GOLD-2017-Pocket-Guide.pdf.
13. COPD National Action Plan. National Heart, Lung and Blood Institute. National Institutes of Health. U.S. Health Department and Human Services. Publication No. 17-HL-8031. May 2017. https://www.nhlbi.nih.gov/sites/www.nhlbi.nih.gov/files/COPD_NationalActionPlan_05222017.pdf
14. Chronic Obstructive Pulmonary Disease (COPD). Centers for Disease Control and Prevention (CDC). http://www.cdc.gov/copd/. Accessed May 24, 2017.
15. Chronic respiratory diseases. Chronic obstructive pulmonary disease (COPD). Burden of COPD. World Health Organization (WHO). http://www.who.int/respiratory/copd/burden/en/. Accessed May 24, 2017.
16. Learn More About COPD. National Heart, Lung and Blood Institute. National Institutes of Health. U.S. Health Department and Human Services. https://www.nhlbi.nih.gov/health/educational/copd/what-is-copd/. Accessed May 25, 2017.
17. Ni H, Xu JQ. COPD-related mortality by sex and race among adults aged 25 and over: United States, 2000–2014. NCHS data brief, no 256. Hyattsville, MD: National Center for Health Statistics. 2016.
18. Respiratory Diseases. Air Pollution and Public Health in Utah. Bureau of Epidemiology. Utah Department of Health. http://www.health.utah.gov/utahair/respiratory/. Accessed May 25, 2017.
19. Spirometry for Health care Providers. Global Initiative for Chronic Obstructive Lung Disease (GOLD); 2010.

33
20. Ford ES, Murphy LB, Khavjou O, Giles WH, Holt JB, Croft JB. Total and state-specific medical and absenteeism costs of COPD among adults aged >/= 18 years in the United States for 2010 and projections through 2020. Chest. 2015;147(1):31-45.
21. Jones PW, Beeh KM, Chapman KR, Decramer M, Mahler DA, Wedzicha JA. Minimal clinically important differences in pharmacological trials. Am J Respir Crit Care Med. 2014;189(3):250-255.
22. APhA DrugInfoLine. Revised guideline for COPD released. May 15, 2017. http://www.aphadruginfoline.com/respiratory/revised-guideline-copd-released.
23. Chronic respiratory diseases. COPD management. http://www.who.int/respiratory/copd/management/en/. Accessed May 26, 2017.
24. Chronic Obstructive Pulmonary Disease: Developing Drugs for Treatment Guidance for Industry. Draft Guidance. U.S. Department of Health and Human Services, Food and Drug Administration, Center for Drug Evaluation and Research (CDER). May 2016. https://www.fda.gov/downloads/drugs/guidances/ucm071575.pdf.
25. Lexicomp. Wolters Kluwer; 2017. http://online.lexi.com/action/home. Accessed May 15, 2017. 26. Chong J, Poole P, Leung B, Black PN. Phosphodiesterase 4 inhibitors for chronic obstructive
pulmonary disease. The Cochrane database of systematic reviews. 2011(5):Cd002309. 27. DALIRESP® (roflumilast) tablets [package insert]. Wilmington, DE: AstraZeneca
Pharmaceuticals LP. Revised November 2015. 28. Taegtmeyer AB, Leuppi JD, Kullak-Ublick GA. Roflumilast--a phosphodiesterase-4 inhibitor
licensed for add-on therapy in severe COPD. Swiss medical weekly. 2012;142:w13628. 29. Chrischilles E, Gilden D, Kubisiak J, Rubenstein L, Shah H. Delivery of ipratropium and
albuterol combination therapy for chronic obstructive pulmonary disease: effectiveness of a two-in-one inhaler versus separate inhalers. The American journal of managed care. 2002;8(10):902-911.
30. Riley JH, Tabberer M, Richard N, Donald A, Church A, Harris SS. Correct usage, ease of use, and preference of two dry powder inhalers in patients with COPD: analysis of five phase III, randomized trials. Int J Chron Obstruct Pulmon Dis. 2016;11:1873-1880.
31. Svedsater H, Roberts J, Patel C, Macey J, Hilton E, Bradshaw L. Life Impact and Treatment Preferences of Individuals with Asthma and Chronic Obstructive Pulmonary Disease: Results from Qualitative Interviews and Focus Groups. Advances in therapy. 2017.
32. Ferreira IM, Brooks D, White J, Goldstein R. Nutritional supplementation for stable chronic obstructive pulmonary disease. The Cochrane database of systematic reviews. 2012;12:Cd000998.
33. Gruffydd-Jones K. GOLD guidelines 2011: what are the implications for primary care? Primary care respiratory journal : journal of the General Practice Airways Group. 2012;21(4):437-441.
34. van Eerd EA, van der Meer RM, van Schayck OC, Kotz D. Smoking cessation for people with chronic obstructive pulmonary disease. The Cochrane database of systematic reviews. 2016(8):Cd010744.
35. Singh D. Pharmacological treatment for COPD; GOLD 2017 changes direction. British journal of clinical pharmacology. 2017;83(5):935-937.
36. Wedzicha JA, Banerji D, Chapman KR, et al. Indacaterol-Glycopyrronium versus Salmeterol-Fluticasone for COPD. The New England journal of medicine. 2016;374(23):2222-2234.
37. Mahler DA, Kerwin E, Ayers T, et al. FLIGHT1 and FLIGHT2: Efficacy and Safety of QVA149 (Indacaterol/Glycopyrrolate) versus Its Monocomponents and Placebo in Patients with Chronic Obstructive Pulmonary Disease. Am J Respir Crit Care Med. 2015;192(9):1068-1079.
38. Farne HA, Cates CJ. Long-acting beta2-agonist in addition to tiotropium versus either tiotropium or long-acting beta2-agonist alone for chronic obstructive pulmonary disease. The Cochrane database of systematic reviews. 2015(10):Cd008989.
39. Wedzicha JA, Decramer M, Ficker JH, et al. Analysis of chronic obstructive pulmonary disease exacerbations with the dual bronchodilator QVA149 compared with glycopyrronium and

34
tiotropium (SPARK): a randomised, double-blind, parallel-group study. The Lancet Respiratory medicine. 2013;1(3):199-209.
40. Brusselle G, Price D, Gruffydd-Jones K, et al. The inevitable drift to triple therapy in COPD: an analysis of prescribing pathways in the UK. Int J Chron Obstruct Pulmon Dis. 2015;10:2207-2217.
41. Welte T, Miravitlles M, Hernandez P, et al. Efficacy and tolerability of budesonide/formoterol added to tiotropium in patients with chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2009;180(8):741-750.
42. Singh D, Brooks J, Hagan G, Cahn A, O'Connor BJ. Superiority of "triple" therapy with salmeterol/fluticasone propionate and tiotropium bromide versus individual components in moderate to severe COPD. Thorax. 2008;63(7):592-598.
43. Jung KS, Park HY, Park SY, et al. Comparison of tiotropium plus fluticasone propionate/salmeterol with tiotropium in COPD: a randomized controlled study. Respiratory medicine. 2012;106(3):382-389.
44. Hanania NA, Crater GD, Morris AN, Emmett AH, O'Dell DM, Niewoehner DE. Benefits of adding fluticasone propionate/salmeterol to tiotropium in moderate to severe COPD. Respiratory medicine. 2012;106(1):91-101.
45. Frith PA, Thompson PJ, Ratnavadivel R, et al. Glycopyrronium once-daily significantly improves lung function and health status when combined with salmeterol/fluticasone in patients with COPD: the GLISTEN study, a randomised controlled trial. Thorax. 2015;70(6):519-527.
46. Siler TM, Kerwin E, Singletary K, Brooks J, Church A. Efficacy and Safety of Umeclidinium Added to Fluticasone Propionate/Salmeterol in Patients with COPD: Results of Two Randomized, Double-Blind Studies. Copd. 2016;13(1):1-10.
47. Singh D, Papi A, Corradi M, et al. Single inhaler triple therapy versus inhaled corticosteroid plus long-acting beta2-agonist therapy for chronic obstructive pulmonary disease (TRILOGY): a double-blind, parallel group, randomised controlled trial. Lancet. 2016;388(10048):963-973.
48. Aaron SD, Vandemheen KL, Fergusson D, et al. Tiotropium in combination with placebo, salmeterol, or fluticasone-salmeterol for treatment of chronic obstructive pulmonary disease: a randomized trial. Ann Intern Med. 2007;146(8):545-555.
49. Diagnosis and Initial Treatment of Asthma, COPD and Asthma-COPD Overlap. A Joint Project of GINA and GOLD. Updated April 2017. http://goldcopd.org/asthma-copd-asthma-copd-overlap-syndrome/. Accessed July 14, 2017.
50. Cazzola M, Molimard M. The scientific rationale for combining long-acting beta2-agonists and muscarinic antagonists in COPD. Pulmonary pharmacology & therapeutics. 2010;23(4):257-267.
51. UpToDate, Inc. Wolters Kluwer; 2017. https://www.uptodate.com/. Accessed May 18, 2017. 52. Calzetta L, Matera MG, Cazzola M. Pharmacological interaction between LABAs and LAMAs in
the airways: optimizing synergy. European journal of pharmacology. 2015;761:168-173. 53. Micromedex (electronic version). Truven Health Analytics; 2017.
http://www.micromedexsolutions.com/. Accessed May 15, 2017. 54. Ramadan WH, Kabbara WK, Abilmona RM. Olodaterol for the treatment of chronic obstructive
pulmonary disease. Am J Health-Syst Pharm. 2016;73(15):1135-1143. 55. Ultibro Breezhaler 85 micrograms/43 micrograms, inhalation powder hard capsules [packege
insert]. European Medicines Agency. 56. Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred reporting items for systematic reviews and
meta-analyses: the PRISMA statement. PLoS medicine. 2009;6(7):e1000097. 57. Schlueter M, Gonzalez-Rojas N, Baldwin M, Groenke L, Voss F, Reason T. Comparative
efficacy of fixed-dose combinations of long-acting muscarinic antagonists and long-acting beta2-agonists: a systematic review and network meta-analysis. Therap. 2016;10(2):89-104.
58. Rodrigo GJ, Price D, Anzueto A, et al. LABA/LAMA combinations versus LAMA monotherapy or LABA/ICS in COPD: a systematic review and meta-analysis. Int J Chron Obstruct Pulmon Dis. 2017;12:907-922.

35
59. Buhl R, Maltais F, Abrahams R, et al. Tiotropium and olodaterol fixed-dose combination versus mono-components in COPD (GOLD 2-4). The European respiratory journal. 2015;45(4):969-979.
60. Decramer M, Anzueto A, Kerwin E, et al. Efficacy and safety of umeclidinium plus vilanterol versus tiotropium, vilanterol, or umeclidinium monotherapies over 24 weeks in patients with chronic obstructive pulmonary disease: results from two multicentre, blinded, randomised controlled trials. The Lancet Respiratory Medicine. 2014;2(6):472-486.
61. Rodrigo GJ, Neffen H. A Systematic Review of the Efficacy and Safety of a Fixed-Dose Combination of Umeclidinium and Vilanterol for the Treatment of COPD. Chest. 2015;148(2):397-407.
62. Martinez FJ, Rabe KF, Ferguson GT, et al. Efficacy and Safety of Glycopyrrolate/Formoterol Metered Dose Inhaler Formulated Using Co-Suspension Delivery Technology in Patients With COPD. Chest. 2017;151(2):340-357.
63. Singh D, Ferguson GT, Bolitschek J, et al. Tiotropium + olodaterol shows clinically meaningful improvements in quality of life. Respiratory medicine. 2015;109(10):1312-1319.
64. Decramer M, Anzueto A, Kerwin E, et al. Efficacy and safety of umeclidinium plus vilanterol versus tiotropium, vilanterol, or umeclidinium monotherapies over 24 weeks in patients with chronic obstructive pulmonary disease: results from two multicentre, blinded, randomised controlled trials. The Lancet Respiratory medicine. 2014;2(6):472-486.
65. Horita N, Miyazawa N, Tomaru K, Inoue M, Kaneko T. Long-acting muscarinic antagonist + long-acting beta agonist versus long-acting beta agonist + inhaled corticosteroid for COPD: A systematic review and meta-analysis. Respirology (Carlton, Vic). 2015;20(8):1153-1159.
66. Matera MG, Rogliani P, Calzetta L, Cazzola M. Safety Considerations with Dual Bronchodilator Therapy in COPD: An Update. Drug safety. 2016;39(6):501-508.
67. Oba Y, Sarva ST, Dias S. Efficacy and safety of long-acting beta-agonist/long-acting muscarinic antagonist combinations in COPD: a network meta-analysis. Thorax. 2016;71(1):15-25.
68. Ficker JH, Rabe KF, Welte T. Role of dual bronchodilators in COPD: A review of the current evidence for indacaterol/glycopyrronium. Pulmonary pharmacology & therapeutics. 2017.
69. Wedzicha JA, Dahl R, Buhl R, et al. Pooled safety analysis of the fixed-dose combination of indacaterol and glycopyrronium (QVA149), its monocomponents, and tiotropium versus placebo in COPD patients. Respiratory medicine. 2014;108(10):1498-1507.
70. Van de Maele B, Fabbri LM, Martin C, Horton R, Dolker M, Overend T. Cardiovascular safety of QVA149, a combination of Indacaterol and NVA237, in COPD patients. Copd. 2010;7(6):418-427.
71. Bateman ED, Ferguson GT, Barnes N, et al. Dual bronchodilation with QVA149 versus single bronchodilator therapy: the SHINE study. The European respiratory journal. 2013;42(6):1484-1494.
72. Dahl R, Chapman KR, Rudolf M, et al. Safety and efficacy of dual bronchodilation with QVA149 in COPD patients: the ENLIGHTEN study. Respiratory medicine. 2013;107(10):1558-1567.
73. Ulrik CS. Clinical benefit of fixed-dose dual bronchodilation with glycopyrronium and indacaterol once daily in patients with chronic obstructive pulmonary disease: a systematic review. Int J Chron Obstruct Pulmon Dis. 2014;9:331-338.
74. Ferguson GT, Karpel J, Bennett N, et al. Effect of tiotropium and olodaterol on symptoms and patient-reported outcomes in patients with COPD: results from four randomised, double-blind studies. NPJ primary care respiratory medicine. 2017;27(1):7.
75. Buhl R, Magder S, Bothner U, et al. Long-term general and cardiovascular safety of tiotropium/olodaterol in patients with moderate to very severe chronic obstructive pulmonary disease. Respiratory medicine. 2017;122:58-66.
76. Hanania NA, Tashkin DP, Kerwin EM, et al. Long-term safety and efficacy of glycopyrrolate/formoterol metered dose inhaler using novel Co-Suspension Delivery Technology in patients with chronic obstructive pulmonary disease. Respiratory medicine. 2017;126:105-115.

36
77. Rabe KF. GFF MDI for the improvement of lung function in COPD - A look at the PINNACLE-1 and PINNACLE-2 data and beyond. Expert review of clinical pharmacology. 2017:1-14.
78. Huisman EL, Cockle SM, Ismaila AS, Karabis A, Punekar YS. Comparative efficacy of combination bronchodilator therapies in COPD: a network meta-analysis. Int J Chron Obstruct Pulmon Dis. 2015;10:1863-1881.
79. Wang L, Zhai CJ, Liu Y, Liu Y, Jiang SJ. Umeclidinium Plus Vilanterol Versus Placebo, Umeclidinium, or Vilanterol Monotherapies for Chronic Obstructive Pulmonary Disease: A Meta-Analysis of Randomized Controlled Trials. Clin Drug Invest. 2016;36(11):865-875.
80. Price D, Ostrem A, Thomas M, Welte T. Dual bronchodilation in COPD: lung function and patient-reported outcomes - a review. Int J Chron Obstruct Pulmon Dis. 2017;12:141-168.
81. Donohue JF, Maleki-Yazdi MR, Kilbride S, Mehta R, Kalberg C, Church A. Efficacy and safety of once-daily umeclidinium/vilanterol 62.5/25 mcg in COPD. Respiratory medicine. 2013;107(10):1538-1546.
82. Beeh KM, Westerman J, Kirsten AM, et al. The 24-h lung-function profile of once-daily tiotropium and olodaterol fixed-dose combination in chronic obstructive pulmonary disease. Pulmonary pharmacology & therapeutics. 2015;32:53-59.
83. Dahl R, Jadayel D, Alagappan VK, Chen H, Banerji D. Efficacy and safety of QVA149 compared to the concurrent administration of its monocomponents indacaterol and glycopyrronium: the BEACON study. Int J Chron Obstruct Pulmon Dis. 2013;8:501-508.
84. Vogelmeier CF, Bateman ED, Pallante J, et al. Efficacy and safety of once-daily QVA149 compared with twice-daily salmeterol-fluticasone in patients with chronic obstructive pulmonary disease (ILLUMINATE): a randomised, double-blind, parallel group study. The Lancet Respiratory medicine. 2013;1(1):51-60.
85. Zhong N, Wang C, Zhou X, et al. LANTERN: a randomized study of QVA149 versus salmeterol/fluticasone combination in patients with COPD. Int J Chron Obstruct Pulmon Dis. 2015;10:1015-1026.
86. Buhl R, Gessner C, Schuermann W, et al. Efficacy and safety of once-daily QVA149 compared with the free combination of once-daily tiotropium plus twice-daily formoterol in patients with moderate-to-severe COPD (QUANTIFY): a randomised, non-inferiority study. Thorax. 2015;70(4):311-319.

37
Appendix A. Medications Commonly Used in COPD Class Agents in Class Route of
Administration Mechanism of Action Labeled
Indications Notable Side Effects
Anticholinergics (Short Acting)
Ipratropium
Inhalation Antagonist of acetylcholine at cholinergic receptors, preventing the increase of cyclic GMP. This relaxes smooth muscle, causes bronchodilation, and reduces secretions.
COPD, nasal discharge
Xerostomia, constipation, sinusitis
Anticholinergics (Long Acting)
Aclidinium Glycopyrronium/Glycopyrrolate Tiotropium Umeclidinium
Inhalation Antagonist of acetylcholine at M3-receptors cholinergic receptors in smooth muscle causing bronchodilation.
COPD Xerostomia, upper respiratory infection, constipation, sinusitis
Beta-Agonists (Short Acting)
Albuterol Levalbuterol Terbutaline
Inhalation Oral tablets Injection
Beta-adrenergic agonist selective for beta (2) receptors, causing smooth muscle relaxation and decreases release of hypersensitivity mediators from mast cells.
Asthma, Exercise-induced asthma, bronchospasm
Tachycardia, hypokalemia, pharyngitis, palpitations, tremor
Beta-Agonists (Long Acting)
Arformoterol Formoterol Indacaterol Olodatrol Salmeterol
Inhalation Beta-adrenergic agonist selective for beta (2) receptors, causing smooth muscle relaxation and bronchodilation.
Asthma, Exercise-induced asthma, Nocturnal asthma, COPD
Musculoskeletal pain, headache, tremor, insomnia
Inhaled Corticosteroids
Beclomethasone Budesonide Fluticasone
Inhalation Inhibits inflammatory cells and the release of inflammatory mediators to exert potent anti-inflammatory effects.
Asthma, COPD Headache, respiratory tract infections, pharyngitis
Methylxanthines Aminophylline Theophylline
IV infusion Oral tablets Capsules Solution IV solution
Bronchodilation through smooth muscle relaxation and suppression of airway stimuli. The exact MOA is not fully known, but is thought to be associated with inhibition of two isoenzymes, phosphodiesterase 3 (PDE III) and 4 (PDE IV). Methylxanthines may also increase the force of contraction of the diaphragm through
Acute exacerbations of Asthma, COPD
Common: Nausea, vomiting, Headache, insomnia, tremor, irritability, restlessness. Serious: Atrial fibrillation, tachyarrhythmia, Stevens-Johnson syndrome, seizure,

38
Class Agents in Class Route of Administration
Mechanism of Action Labeled Indications
Notable Side Effects
enhanced calcium uptake through adenosine-mediated channels.
intracranial hemorrhage
Systemic Corticosteroids
Dexamethasone Methylprednisolone Prednisone
Oral Tablets/ Injection
Corticosteroids exert potent anti-inflammatory effects in many organ systems by inhibiting inflammatory cells and the release of inflammatory mediators.
Allergic disorder, asthma, inflammatory disorders, exacerbation of multiple sclerosis, etc.
short term use: Hypertension, fluid retention, hypokalemia, weight gain, disturbance in mood, impaired glucose tolerance Long term use: Adrenal insufficiency, osteoporosis, hyperlipidemia, growth suppression
Phosphodiesterase-4 Inhibitors
Roflumilast Oral Tablets Inhibit phosphodiesterase 4 (PDE 4). Exact MOA is not known but is thought to be associated with increased levels of intracellular cyclic AMP in lung cells and reduced neutrophil and eosinophil cell counts in the lungs.
COPD
Weight loss, decrease in appetite, diarrhea, nausea, backache, headache, insomnia, suicidal thoughts
Combinations available in one device Short-acting beta2-agonist plus anticholinergic
Albuterol/Ipratropium
Inhalation See individual products COPD Upper respiratory infection, nasopharyngitis, cough, bronchitis, headache, and dyspnea
Long-acting beta2-agonist plus long-acting anticholinergic
Formoterol/glycopyrrolate Indacaterol/glycopyrrolate Olodaterol/tiotropium Vilanterol/umeclidinium
Inhalation See individual products COPD Central nervous system depression, cardiovascular effects, neuromuscular pain, pneumonia, urinary retention, bronchospasm

39
Class Agents in Class Route of Administration
Mechanism of Action Labeled Indications
Notable Side Effects
Long-acting beta2-agonist plus corticosteroid
Formoterol/Budesonide Formoterol/Mometasone Salmeterol/Fluticasone Vilanterol/Fluticasone
Inhalation See individual products COPD, asthma Headache, respiratory tract infections, pharyngitis, throat irritation, oropharyngeal candidiasis, voice disorder gastrointestinal disorders, musculoskeletal pain
Abbreviations: COPD, chronic obstructive pulmonary disease; LABA, long-acting β2-adrenergic agonist; LAMA, long-acting antimuscarinic agent

40
Appendix B. MEDLINE and EMBASE Literature Search Strategies of LABA/LAMA Combination Products for COPD Table 1. Medline Literature Search Strategy (via Ovid) for systematic reviews and randomized controlled trials
Ovid MEDLINE(R) Epub Ahead of Print, In-Process & Other Non-Indexed Citations, Ovid MEDLINE(R) Daily, Ovid MEDLINE and Versions(R). Search Date: May 2017 1 adrenergic beta-agonists/ or adrenergic beta-2 receptor agonists/ or formoterol fumarate/ (19862) 2 ((glycopyr?olat$ adj3 indacaterol$) or qva 149 or qva 149a or qva149 or qva149a or ultibro$ or ulunar breezhaler? or utibron$ or xoterna$).ti,ab,kw,kf,rn. (87) 3 (bevespi? or anoroel?ipta? or anoro el?ipta? or stiolto respimat? or utibron?).ti,ab,kw,kf,rn. (12) 4 (formoterol fumarate adj3 glycopyrr$).ti,ab,kw,kf,rn. (19) 5 (anoro or laventair* or (umeclidinium* adj4 vilanterol*)).ti,ab,kw,kf,rn. (92) 6 (tiotropium* adj3 olodaterol*).ti,ab,kw,kf,rn. (66) 7 (glycopyrrolat* adj3 formoterol*).ti,ab,kw,kf,rn. (16) 8 or/2-7 [Specific Drugs-Anticholinergics-COPD] (241) 9 adrenergic beta-agonists/ or adrenergic beta-2 receptor agonists/ or formoterol fumarate/ (19862) 10 cholinergic antagonists/ or ipratropium/ or scopolamine hydrobromide/ or tiotropium bromide/ (13565) 11 (((acetylcholin$ or cholinergic-blocking or cholinergic? or cholinergic receptor?) adj3 (agent? or antagonist? or inhibitor? or receptor? block$)) or (anti cholinergic? or anticholinergic? or cholinolytic?) or (achr inhibitor? or parasympatholytic? or (atropinic? adj2 (agent? or drug?)) or ((parasympathetic? or parasympathicolytic$) adj2 (agent? or blocker? or blocking agent? or drug?)))).ti,ab,kw,kf,rn. (34032) 12 Receptors, Adrenergic, beta-2/ (4039) 13 (((adrenergic beta or adrenergic beta2 or beta2 adrenergic receptor? or beta 2 adrenergic receptor? or beta 2 adrenoceptor? or beta adrenocept$) and (agonists* or agent* or stimulant* or stimulating or stimulator*)) or beta 2 agonist* or beta2 agonist?).ti,ab,kw,kf,rn. (12487) 14 (or/9-11) and (or/12-13) [Anticholinergics & Beta 2 Agonists] (6096) 15 Pulmonary Disease, Chronic Obstructive/ (31316) 16 copd.ti,ab,kw,kf. (37001) 17 (chronic* adj2 obstruct$ adj4 (airflow or pulmonar$ or lung or respirator$)).ti,ab,kw,kf. (43595) 18 or/15-17 [COPD] (59671) 19 (systematic adj2 review).ti. or (metaanaly$ or meta-analy$).ti,ab,pt. (176632) 20 ((systematic adj2 review) or (metaanaly$ or meta-analy$)).kw,kf. (20516) 21 or/19-20 [SRFilter] (178105) 22 (randomized controlled trial or controlled clinical trial).pt. or randomized.ab. or placebo.ab. or clinical trials as topic.sh. or randomly.ab. or trial.ti. (1144456) 23 exp animals/ not humans.sh. (4414736) 24 22 not 23 [Cochrane RCT Filter 6.4.d Sens/Precision Maximizing] (1055699) 25 (animal? or beaver? or beef or bovine or breeding or bull or canine or castoris or cat or cattle or cats or chicken? or chimp$ or cow or dog or dogs or equine or foal or foals or fish or insect? horse or horses or livestock or mice or monkey? or mouse or murine or plant or plants or pork or porcine or protozoa? or purebred or rat or rats or rodent? or sheep or thoroughbred).ti. or veterinar$.ti,ab,kw,kf,hw. (2157622) 26 english.lg. (23280670) 27 ((8 or (and/14,18)) and 21 and 26) not (or/23,25) [SR Results] (94) 28 (8 or ((and/14,18) and 24 and 26)) not (or/25,27) [RCT Results] (572) 29 remove duplicates from 27 [SR to export] (82) 30 limit 28 to yr="2016 -Current" [RCTs to export] (100) 31 remove duplicates from 30 (86)

41
Table 2. EMBASE Literature Search Strategy (via EMBASE.com) EMBASE.com. Search Date: May 2017 (('formoterol fumarate plus glycopyrronium bromide'/de or 'umeclidinium plus vilanterol'/de or 'olodaterol plus tiotropium bromide'/de or 'glycopyrronium bromide plus indacaterol'/de) or ((glycopyr* near/3 indacaterol*):ti,ab,rn,mn,tn or 'qva 149':ab,ti or 'qva 149a':ab,ti or 'qva149':ab,ti or 'qva149a':ab,ti or 'ultibro':ab,ti,rn,tn,mn or 'ulunar breezhaler':ab,ti,rn,tn,mn or 'utibron':ab,ti or 'xoterna':ab,ti,rn,tn,mn) or ('bevespi':ab,ti,tn,mn,rn or (formoterol* near/3 glycopyr*):ti,ab,rn,mn,tn) or ('anoro':ab,ti or 'laventair':ab,ti or (umeclidinium* near/3 vilanterol*):ti,ab,rn,tn,mn) or (tiotropium* near/3 olodaterol*):ab,ti,mn,dn,rn) or (('cholinergic receptor blocking agent'/de or ((('acetylcholin*' or 'cholinergic-blocking' or 'cholinergic*' or 'cholinergic receptor*') near/3 (agent* or antagonist* or inhibitor* or 'receptor* block*')):ti,ab,rn or 'anti cholinergic*':ti,ab,rn or anticholinergic*:ti,ab,rn or cholinolytic*:ti,ab,rn or 'achr inhibitor*':ti,ab,rn or parasympatholytic*:ti,ab,rn or (atropinic* near/2 (agent* or drug*)):ti,ab,rn or ((parasympathetic* or parasympathicolytic*) near/2 (agent* or blocker* or 'blocking agent*' or drug*)):ti,ab,rn) or 'beta 2 adrenergic receptor stimulating agent'/de or ((('adrenergic beta 2' or 'adrenergic beta2' or 'beta2 adrenergic' or 'beta 2 adrenergic' or 'beta 2 adrenoceptor*' or 'beta2 adrenoceptor*') near/3 (agonist* or stimulant* or stimulator* or stimulating)):ti,ab,rn or 'beta 2 agonist*':ti,ab or 'beta2 agonist*':ti,ab)) and ('chronic obstructive lung disease'/mj or copd:ti,ab or (chronic near/2 obstructi* near/2 (lung or lungs or pulmonar* or airway or respirator*)):ti,ab)) and ('clinical study'/mj or 'clinical trial'/mj or 'controlled clinical trial'/mj or 'controlled study'/mj or 'major clinical study'/mj or 'randomized controlled trial'/mj or 'control group'/mj or ((clinical or randomi* or controlled or multicentre or multicenter or 'multi centre' or 'multi center') near/3 (study or trial)):ti,ab or placebo:ab,ti or 'head to head':ti,ab) not ((('animal'/exp or 'invertebrate'/exp or 'animal experiment'/exp or 'animal model'/exp or 'animal tissue'/exp or 'animal cell'/exp or 'nonhuman'/de not ('animal'/exp or 'invertebrate'/exp or 'animal experiment'/exp or 'animal model'/exp or 'animal tissue'/exp or 'animal cell'/exp or 'nonhuman'/de and ('human'/exp or 'human cell'/de))) or (animal*:ti or beaver*:ti or beef:ti or bovine:ti or breeding:ti or bull:ti or canine:ti or castoris:ti or cat:ti or cattle:ti or cats:ti or chicken*:ti or chimp*:ti or cow:ti or dog:ti or dogs:ti or equine:ti or foal:ti or foals:ti or fish:ti or insect*:ti and horse:ti or horses:ti or livestock:ti or mice:ti or monkey*:ti or mouse:ti or murine:ti or plant:ti or plants:ti or pork:ti or porcine:ti or protozoa*:ti or purebred:ti or rat:ti or rats:ti or rodent*:ti or sheep:ti or thoroughbred:ti or veterinar*:ti,ab)) or ((('formoterol fumarate plus glycopyrronium bromide'/de or 'umeclidinium plus vilanterol'/de or 'olodaterol plus tiotropium bromide'/de or 'glycopyrronium bromide plus indacaterol'/de) or ((glycopyr* near/3 indacaterol*):ti,ab,rn,mn,tn or 'qva 149':ab,ti or 'qva 149a':ab,ti or 'qva149':ab,ti or 'qva149a':ab,ti or 'ultibro':ab,ti,rn,tn,mn or 'ulunar breezhaler':ab,ti,rn,tn,mn or 'utibron':ab,ti or 'xoterna':ab,ti,rn,tn,mn) or ('bevespi':ab,ti,tn,mn,rn or (formoterol* near/3 glycopyr*):ti,ab,rn,mn,tn) or ('anoro':ab,ti or 'laventair':ab,ti or (umeclidinium* near/3 vilanterol*):ti,ab,rn,tn,mn) or (tiotropium* near/3 olodaterol*):ab,ti,mn,dn,rn) or (('cholinergic receptor blocking agent'/de or ((('acetylcholin*' or 'cholinergic-blocking' or 'cholinergic*' or 'cholinergic receptor*') near/3 (agent* or antagonist* or inhibitor* or 'receptor* block*')):ti,ab,rn or 'anti cholinergic*':ti,ab,rn or anticholinergic*:ti,ab,rn or cholinolytic*:ti,ab,rn or 'achr inhibitor*':ti,ab,rn or parasympatholytic*:ti,ab,rn or (atropinic* near/2 (agent* or drug*)):ti,ab,rn or ((parasympathetic* or parasympathicolytic*) near/2 (agent* or blocker* or 'blocking agent*' or drug*)):ti,ab,rn) or 'beta 2 adrenergic receptor stimulating agent'/de or ((('adrenergic beta 2' or 'adrenergic beta2' or 'beta2 adrenergic' or 'beta 2 adrenergic' or 'beta 2 adrenoceptor*' or 'beta2 adrenoceptor*') near/3 (agonist* or stimulant* or stimulator* or stimulating)):ti,ab,rn or 'beta 2 agonist*':ti,ab or 'beta2 agonist*':ti,ab)) and ('chronic obstructive lung disease'/mj or copd:ti,ab or (chronic near/2 obstructi* near/2 (lung or lungs or pulmonar* or airway or respirator*)):ti,ab)) and ((metaanaly*:ti,ab or 'meta analy*':ti,ab or (systematic near/2 review):ti) or ('systematic review'/mj or 'meta analysis'/mj)) not (('animal'/exp or 'invertebrate'/exp or 'animal experiment'/exp or 'animal model'/exp or 'animal tissue'/exp or 'animal cell'/exp or 'nonhuman'/de not ('animal'/exp or 'invertebrate'/exp or 'animal experiment'/exp or 'animal model'/exp or 'animal tissue'/exp or 'animal cell'/exp or 'nonhuman'/de and ('human'/exp or 'human cell'/de))) or (animal*:ti or beaver*:ti or beef:ti or bovine:ti or breeding:ti or bull:ti or canine:ti or castoris:ti or cat:ti or cattle:ti or cats:ti or chicken*:ti or chimp*:ti or cow:ti or dog:ti or dogs:ti or equine:ti or foal:ti or foals:ti or fish:ti or insect*:ti and horse:ti or horses:ti or livestock:ti or mice:ti or monkey*:ti or mouse:ti or murine:ti or plant:ti or plants:ti or pork:ti or porcine:ti or protozoa*:ti or purebred:ti or rat:ti or rats:ti or rodent*:ti or sheep:ti or thoroughbred:ti or veterinar*:ti,ab)) not 'conference abstract'/it)) not 'conference abstract'/it and [2016-2017]/py and [english]/lim; no conference abstracts)

41
Appendix C. Network Meta-analyses Comparing LABA/LAMA Combination Products for COPD
Study Reference and Search Date Objective(s) Studies Characteristics Interventions Clinical Efficacy and Safety Resultsa Limitations
Schlueter et al57 (2016) • Literature search
up to September 2014: 27 trials from 26 publications with 30,361 subjects were included in the NMA
To assess the relative clinical benefit of all currently available LAMA/LABA FDCs using a Bayesian network meta-analysis (NMA)
• 40% of studies were excluded since they do not followed the modified Anthonisen definition of COPD exacerbations
• Mean %FEV1: 50.9% (37.2% to 65.7%)
• Average distribution of patients by GOLD stages: GOLD II (51%), GOLD III (41.9%), GOLD IV (6.8%)
• Variations in the distribution of use of concomitant ICS at BL
• Meta-regression controlling for % of tFEV1 predicted at BL and meta-regression adjusting for concomitant use of ICS at BL was performed
TIO/OLO 5/5 mcg UMEC/VI 62.5/25 mcg GLY/IND 110/50 mcg* ACLI/FM 400/12 mcg*
Change in through tFEV1 from BL at 24/26 wks: TIO/OLO vs UMEC/VI: 0.025 [-0.002, 0.052] UMEC/VI vs TIO/OLO: -0.025 [-0.052, 0.002] (No statistically significant differences between groups)
SGRQ percentage of responders at 24/26 wks No significant differences between the FDCs Exacerbation rate No significant differences between the FDCs Discontinuation rates due to AEs: No significant differences between the FDCs Conclusion: “All LAMA/LABA FDCs were found to have similar efficacy and safety. Definitive assessment of the relative efficacy of different treatments can only be performed through direct comparison in head-to-head RCTs. In the absence of such data, this indirect comparison may be of value in clinical and health economic decision-making.”
• Indirect comparisons • GLY/IND 110/50 mcg
and ACLI/FM not approved in the U.S.
• Studies reporting results at different time points
• Patients with different disease severity (from GOLD grade II to IV)
• Concomitant use of ICS that may increase treatment effects
• Patients with different exacerbation history
• No baseline SGRQ values for UMEC/VI studies
* Not approved in the U.S. a Only information of interest related to the products and doses approved in the U.S. was included (i.e. data for UMEC/VI vs TIO/OLO) Abbreviations: ACLI, aclidinium; AE, adverse events; BL, baseline; COPD, Chronic Obstructive Pulmonary Disease; FM, formoterol; GLY, glycopyrrolate or glycopyrronium; IND, indacaterol; LABA, long-acting β2-adrenergic agonist; LAMA, long-acting antimuscarinic agent; MDI, metered dose inhaler; NMA, netwotk meta-analysis; OLO, olodaterol; PLB, placebo; RCT, randomized controlled trial; tFEV1, trough forced expiratory volume in 1 second; TIO, tiotropium; UMEC, umeclidinium, VI, vilanterol; wks, weeks

42
Appendix D. Summary of Evidence of LABA/LAMA Combination Products for COPD
Combination Product (Brand
name)
RCTs leading to FDA Approval
Treatment Comparisons Clinical Results from the Main RCTsa and Additional Evidenceb
Glycopyrrolate 9mcg/ formoterol fumarate 4.8mcg per actuation
(Bevespi Aerosphere, 2 inhalations twice daily)
• PINNACLE 1 and 2 (24 wks): Two placebo-controlled confirmatory trials (24 weeks) in 3274 patients with moderate to severe COPD: 7.2%, 41.6%, 5.1%, and 45.6% of patients were in GOLD categories A, B, C, and D, respectively. 87.2% of patients with CAT score ≥10, and 57.1% had an MMRC grade ≥2.0)
• GLY/FM 18/9.6 mcg MDI BID
• GLY 18 mcg MDI BID • FM 9.6 mcg MDI BID • PLB MDI BID • TIO 18 mcg dry powder
inhaler (open label) QD (PINNACLE 1)
Main efficacy and safety results 1. Martinez et al 201762 - PINNACLE 1 and 2 (24 wks): Results: “At week 24, differences in change from baseline in the morning predose trough FEV1 for GFF MDI vs placebo MDI, GP MDI, and FF MDI were 150 mL, 59 mL, and 64 mL in PINNACLE-1 (all P < .0001) and 103 mL, 54 mL, and 56 mL in PINNACLE-2 (all P < .001), respectively. There were no significant safety findings (incidence of adverse events was similar between treatment arms).” Conclusions: “We conclude that glycopyrrolate [GP]/formoterol [FF] 18/9.6 mcg metered dose inhaler (MDI) demonstrated superiority over placebo and monocomponent MDIs and was well tolerated, thus providing an additional treatment option for patients with moderate-to-very severe COPD.”
Additional evidence • Hanania et al 201776: long-term safety and efficacy (PINNACLE 3) Conclusions: “Results confirmed the long-term safety and tolerability of GFF MDI 18/9.6 mg twice-daily in
subjects with moderate-to-very severe COPD. Improvements in efficacy endpoints were also sustained over 52 weeks.”
• Rabe 201777: Review of PINNACLE 1 and 2 • Oba et al 201667: Network meta-analysis of LABA/LAMA combinations versus monotherapies
Umeclidinium 62.5mcg/vilanterol 25mcg per actuation
(Anoro Ellipta, 1 inhalation once daily)
• Two placebo-controlled confirmatory trials (24 wks) in 1141 (study 1) and 1191 (study 2) patients with moderate to severe COPD
• Additional support from 2 active-controlled and 2 crossover trials in subjects with COPD
• One 12-month long term safety trial
Study 1: UMEC/VI 62.5/25 mcg QD UMEC/VI 125/25 mcg QD VI 25 mcg QD TIO 18 mcg QD PLB Study 2: UMEC/VI 62.5/25 mcg QD UMEC/VI 125/25 mcg QD UMEC 125 mcg QD TIO 18 mcg QD PLB
Main efficacy and safety results 1. Decramer et al 201464: Results: “In both studies, we noted improvements in trough FEV1 on day 169 for both doses of UMEC plus VI compared with TIO monotherapy (study 1, UMEC 125 μg plus VI 25 μg: 0·088 L [95% CI 0·036 to 0·140; p=0·0010]; study 1, UMEC 62·5 μg plus VI 25 μg: 0·090 L [0·039 to 0·141; p=0·0006]; study 2, UMEC 125 μg plus VI 25 μg: 0·074 L [0·025 to 0·123; p=0·0031]; study 2, UMEC 62·5 μg plus VI 25 μg: 0·060 L [0·010 to 0·109; nominal p=0·0182]). Both doses of UMEC plus VI also improved trough FEV1 compared with VI monotherapy (UMEC 62·5 μg plus VI 25 μg: 0·090 L [0·039 to 0·142; p=0·0006] but not compared with UMEC 125 μg monotherapy. All treatments produced improvements in dyspnoea and health-related quality of life; we noted no significant differences in symptoms, health status, or risk of exacerbation between UMEC plus VI and TIO. The most common on-treatment, severe-intensity adverse event in both studies was acute exacerbation of COPD (1-4 [<1-2%] patients across treatment groups in study 1 and 1-6 [<1-3%] patients in study 2). We recorded five to 15 (2-7%) on-treatment serious adverse events across treatment groups in study 1, and nine to 22 (4-10%) in study 2. We noted no substantial changes from baseline in vital signs, clinical laboratory findings, or electrocardiography findings in any of the treatment groups.” Conclusions: “Combination treatment with once-daily UMEC plus VI improved lung function compared with VI monotherapy and TIO monotherapy in patients with COPD. Overall our results suggest that the combination of UMEC plus VI could be beneficial for the treatment of moderate to very severe COPD.”
Additional evidence • Schlueter et al 201657: Network meta-analysis (TIO/OLO vs UMEC/VI) • Oba et al 201667: Network meta-analysis of LABA/LAMA combinations versus monotherapies • Huisman et al 201578: Network meta-analysis (UMEC/VI vs IND/GLY 110/50 mcg)

43
Combination Product (Brand
name)
RCTs leading to FDA Approval
Treatment Comparisons Clinical Results from the Main RCTsa and Additional Evidenceb
• Rodrigo et al 201561: Systematic review of UMEC/VI vs monocomponents, TIO or SFC • Wang et al 201679: Meta-analysis of UMEC/VI vs PLB or monocomponents • Price 201780: Review of dual bronchodilators in COPD • Donohue et al 201381: UMEC/VI vs monocomponents
Tiotropium 2.5mcg/olodaterol 2.5mcg per actuation
(Stiolto Respimat, 2 inhalations once daily)
• TONADO 1 and 2 (52 wks): two replicate, randomized, double-blind, active controlled, parallel phase III trials (52-week) in 5162 patients with moderate to very severe COPD (post-bronchodilator FEV1<80% predicted normal [GOLD Stage 2-4]; post-bronchodilator FEV1 to FVC ratio <70%)
• OTEMTO 1 and 2 (12 wks):
two replicate, multinational, double-blind, parallel group, placebo-controlled studies in patients with moderate to severe COPD (GOLD 2-3)
TONADO 1 and 2: • TIO/OLO 2.5/5 mcg QD • TIO/OLO 5/5 mcg QD • TIO 2.5 mcg QD • TIO 5 mcg QD • OLO 5 mcg QD OTEMTO 1 and 2: • TIO/OLO 2.5/5 mcg QD • TIO/OLO 5/5 mcg QD • TIO 5 mcg QD • PLB QD
Main efficacy and safety results • Buhl et al 201559 - TONADO 1 and 2 (52 wks): “Patients received tiotropium+olodaterol FDC 2.5/5 μg or 5/5 μg, tiotropium 2.5 μg or 5 μg, or olodaterol 5 μg delivered once-daily via Respimat inhaler over 52 weeks. Primary end points were forced expiratory volume in 1 s (FEV1) area under the curve from 0 to 3 h (AUC0–3) response, trough FEV1 response and St George’s Respiratory Questionnaire (SGRQ) total score at 24 weeks. Both FDCs significantly improved FEV1 AUC0–3 and trough FEV1 response versus the mono-components in both studies. Statistically significant improvements in SGRQ total score versus the mono-components were only seen for tiotropium+olodaterol FDC 5/5 μg. Incidence of adverse events was comparable between the FDCs and the mono-components. These studies demonstrated significant improvements in lung function and health-related quality of life with once-daily tiotropium+olodaterol FDC versus mono-components over 1 year in patients with moderate to very severe COPD.” • Singh et al 201563 - OTEMTO 1 and 2 (12 wks): Results: “In OTEMTO 1 and 2, tiotropium + olodaterol 5/5 µg improved SGRQ total score by 4.89 (95% confidence interval [CI] -6.90, -2.88) and 4.56 (95% CI -6.50, -2.63) units versus placebo (both p < 0.0001), and 2.49 (95% CI -4.47, -0.51; p < 0.05) and 1.72 (95% CI -3.63, 0.19) units versus tiotropium 5 µg. Tiotropium + olodaterol 2.5/5 µg significantly improved SGRQ score compared to placebo. Both doses significantly improved FEV1 AUC0-3 response compared to placebo and tiotropium 5 µg. Tiotropium + olodaterol 5/5 and 2.5/5 µg also significantly improved trough FEV1 response compared to placebo (both studies) and separated from tiotropium 5 µg in OTEMTO 2. Adverse-event incidence was similar between treatment groups.” Conclusion: “Tiotropium + olodaterol improved lung function and quality of life compared to placebo and tiotropium 5 µg.”
Additional evidence • Schlueter et al 201657: Network meta-analysis (TIO/OLO vs UMEC/VI) • Oba et al 201667: Network meta-analysis of LABA/LAMA combinations versus monotherapies • Beeh et al 201582: TIO/OLO 2.5/5 mcg or 5/5 mcg QD, TIO 2.5 mcg or 5 mcg QD, OLO 5 mcg QD or PLB
(6 wks) • Ferguson et al 201774: Review of Otemto 1 and 2 and Tonado 1 and 2

44
Combination Product (Brand
name)
RCTs leading to FDA Approval
Treatment Comparisons Clinical Results from the Main RCTsa and Additional Evidenceb
Indacaterol 27.5mcg/ glycopyrrolate 15.6mcg per capsule
(Utibron Neohaler, 1 capsule twice daily)
1. FLIGHT 1 and 2: 12-week, identical, multicenter, randomized, double-blind, parallel-group, placebo and active-controlled studies in 2038 subjects with moderate to severe COPD
• Primary objective: to demonstrate superiority of IND/GLY versus its monocomponents for FEV1 at week 12
2. One active-controlled 12-month trial in 615 patients with COPD
IND 27.5 mcg/ GLY 15.6 mcg BID IND 27.5 mcg BID GLY 15.6 mcg BID PLB BID
Main efficacy and safety results 1. Mahler et al 2015 - FLIGHT 1 and 237: Results: “Indacaterol/glycopyrrolate was statistically superior in terms of FEV1 area under the curve from 0–12 hours compared with its monocomponents (P<0.001). Statistically and clinically meaningful improvements in St. George’s Respiratory Questionnaire total score, transition dyspnea index total score, and reduction in rescue medication use were observed with indacaterol/glycopyrrolate compared with placebo (P<0.001). The safety profile was comparable across the treatment groups.” Conclusions: “Indacaterol/glycopyrrolate twice daily can be an alternative treatment option for the management of symptomatic patients with moderate-to-severe COPD.”
Additional evidence with higher doses of IND/GLY (110 mcg/50 mcg once daily)c • Huisman et al 201578: Network meta-analysis (UMEC/VI vs IND/GLY 110/50 mcg) • Oba et al 201667: Network meta-analysis of LABA/LAMA combinations versus monotherapies • Ulrik 201473: systematic review (IND/GLY vs IND, GLY or TIO) • Mahler et al 2014 (BLAZE study): IND/GLY vs TIO (6 wks) • Bateman et al 2013 (SHINE study)71: IND/GLY vs monocomponents or TIO (26 wks) • Wedzicha et al 2013 (SPARK study)39: IND/GLY vs GLY or TIO (64-76 wks) • Beeh et al 2012 (BRIGTH study): IND/GLY vs TIO (15 wks) • Dahl et al 2013 (BEACON study)83: IND/GLY vs IND+GLY (4 wks) • Vogelmeier et al 2013 (ILLUMINATE study)84: IND/GLY vs SFC (26 wks) • Dahl et al 2013 (ENLIGHTEN study)72: IND/GLY vs PLB (52 wks) • Zhong et al 2015 (LANTERN study)85: IND/GLY vs SFC (26 wks) • Buhl et al 2015 (QUANTIFY study)86: IND/GLY vs TIO+FM (26 wks) • Wedzicha et al 2016 (FLAME study)36: IND/GLY vs SFC (52 wks)
a Efficacy and safety results and conclusions outlined in this table were extracted from the abstracts of the articles related to the RCTs leading to FDA approval b Other key evidence may include additional RCTs (different from those leading to FDA approval), systematic reviews, meta-analysis and network meta-analyses c Dose not approved in the U.S. Abbreviations: BID, twice daily; COPD, chronic obstructive pulmonary disease; FDA, Food and Drug Administration; FM, formoterol; GLY, glycopyrrolate or glycopyrronium; GOLD, Global Initiative for Chronic Obstructive Lung Disease; IND, indacaterol; LABA, long-acting β2-adrenergic agonist; LAMA, long-acting antimuscarinic agent; MDI, metered dose inhaler; OLO, olodaterol; PLB, placebo; QD, once daily; RCT, randomized controlled trial; SFC, salmeterol/fluticasone propionate 50/500 mcg BID; TIO, tiotropium; UMEC, umeclidinium, VI, vilanterol; wks, weeks

45
Appendix E. List of Excluded References
Wrong comparator (LABA/LAMA versus monotherapies, placebo, salmeterol/fluticasone, other)
1. Horita N, Kaneko T. Role of combined indacaterol and glycopyrronium bromide (QVA149) for the
treatment of COPD in Japan. Int J Chron Obstruct Pulmon Dis. 2015;10:813-822. (QVA149* vs. salmeterol/fluticasone)
2. Huisman EL, Cockle SM, Ismaila AS, Karabis A, Punekar YS. Comparative efficacy of combination bronchodilator therapies in COPD: a network meta-analysis. Int J Chron Obstruct Pulmon Dis. 2015;10:1863-1881. (Umeclidinium/vilanterol vs. QVA149* or formoterol plus tiotropium)
3. Ismaila AS, Huisman E, Punekar YS, et al. Comparative efficacy of umeclidinium/vilanterol versus other LAMA/LABA as maintenance treatments for COPD: A systematic review and network meta-analysis. American Journal of Respiratory and Critical Care Medicine. 2015;191 Meeting Abstracts. (Umeclidinium/vilanterol vs. QVA149*, indacaterol+tiotropium, tiotropium+formoterol, salmeterol+tiotropium, placebo or tiotropium)
4. Oba Y, Sarva ST, Dias S. Efficacy and safety of long-acting beta-agonist/long-acting muscarinic antagonist combinations in COPD: a network meta-analysis. Thorax. 2016;71(1):15-25. (LABA/LAMA vs. monotherapy or placebo)
5. Puhan MA, Bachmann LM, Kleijnen J, Ter Riet G, Kessels AG. Inhaled drugs to reduce exacerbations in patients with chronic obstructive pulmonary disease: a network meta-analysis. BMC Med. 2009;7:2. (LABA vs. LAMA or ICS/LABA)
6. Ramadan WH, Kabbara WK, Abilmona RM. Olodaterol for the treatment of chronic obstructive pulmonary disease. Am J Health-Syst Pharm. 2016;73(15):1135-1143. (Olodaterol/tiotropium vs. tiotropium)
7. Rodrigo GJ, Neffen H. A Systematic Review of the Efficacy and Safety of a Fixed-Dose Combination of Umeclidinium and Vilanterol for the Treatment of COPD. Chest. 2015;148(2):397-407. (Umeclidinium/vilanterol vs. monocomponents, tiotropium, or fluticasone/salmeterol)
8. Rodrigo GJ, Plaza V. Efficacy and safety of a fixed-dose combination of indacaterol and Glycopyrronium for the treatment of COPD: a systematic review. Chest. 2014;146(2):309-317. (QVA149* vs. glycopyrronium or tiotropium)
9. Ulrik CS. Clinical benefit of fixed-dose dual bronchodilation with glycopyrronium and indacaterol once daily in patients with chronic obstructive pulmonary disease: a systematic review. Int J Chron Obstruct Pulmon Dis. 2014;9:331-338. (QVA149* vs. monocomponents or placebo)
10. Villalobos RE, David-Wang A, Magallanes J, et al. Efficacy and safety of long-acting beta agonists + long acting muscarinic antagonists vs. long-acting beta agonists + inhaled corticosteroids in COPD: A metaanalysis. Thorax. 2016;71 Supplement 3:A113-A114. (LABA/LAMA vs. ICS/LABA)
11. Wang L, Zhai CJ, Liu Y, Liu Y, Jiang SJ. Umeclidinium Plus Vilanterol Versus Placebo, Umeclidinium, or Vilanterol Monotherapies for Chronic Obstructive Pulmonary Disease: A Meta-Analysis of Randomized Controlled Trials. Clin Drug Invest. 2016;36(11):865-875. (Umeclidinium/vilanterol vs. placebo, umeclidinium, or vilanterol)
Full text not available
12. Huisman E, Sion K, Punekar Y, et al. Comparative efficacy of umeclidinium/vilanterol versus
LABA/LAMA therapies in COPD: A network meta-analysis. European Respiratory Journal. 2016;48 Supplement 60.
* QVA149= indacaterol/glycopyrronium 110/50 mcg (dose not approved in the U.S.)

![Enhancing the Solubility of Curcumin Using a Solid ......drug solubility owing to its ability to reduce the drug particle size [11], increase the drug wettability [12], develop porous](https://static.fdocument.org/doc/165x107/613fcff7b44ffa75b8047733/enhancing-the-solubility-of-curcumin-using-a-solid-drug-solubility-owing.jpg)