Unusual Occurrence of Dentoalveolar Manifestations in a...
4
425 Introduction Thalassemia is the most common type of hemoglubinopathies transmitted by hereditary. These disorders are characterized by decreased or absent synthesis of globin chains (Alpha (α) or Beta (β)). This results in a deficient hemoglobin structure with erythrocytes unable to carry adequate oxygen to cells causing insufficient tissue perfusion and delayed growth and development. In β thalassemia, β globin production can range from near normal to complete absent leading to wide range of symptoms. In the most severe form of the disease (β thalassemia major), severely reduced or absent synthesis of β globin chains from both genes (homozygous state) occurs, which results in splenomegally, growth retardation, irritability, pallor, skeletal abnormalities and maxillofacial complications. Thalassemia trait (minor), resulting from heterozygousity for β thalassemia, depending on the rate of β chain production presents as clinically asymptomatic or with very mild symptoms such as pale or shortness of breath which is more prominent during situations requiring more oxygen such as exercise and pregnancy [1,2]. These disorders may be diagnosed in laboratory investigations by elevated hemoglobin A2 and normal or elevated hemoglobin F. Also, hypochromic and microcytic Red Blood Cells (RBCs) with or without slight degree of anemia can be seen [3]. Thalassemia intermedia is a condition where the lack of β protein in hemoglobin is great enough to cause a moderately severe anemia and significant health problems including bone deformities and enlarged spleen. The severity of this condition is measured by the number of blood transfusions the patient requires in a period of time. Patients with thalassemia intermedia usually need blood transfusions to improve their quality of life but not in order to survive [4]. The incidence of thalassemia trait is 4.4 per 10000 live births and it is more common in people of Mediterranean origin and to a lesser degree, southern Asians and African Americans [5]. Iran as an Asian country is also affected with a large number of thalassemic patients. The highest rate (more than 10%) is seen in Caspian sea and the Persian gulf regions. The prevalence of the disease in other areas is 4-8 percent. Also, more than 2 million carriers of the β thalassemia mutant gene are living in this country [6]. Dentoalveolar abnormalities occur frequently in the course of β thalassemia major and to some extent in intermedia form [7], but tooth and bone changes in β thalassemia trait has not been previously reported in literature, however there is a report on clinical oral sign occurrence in a patient with minor α thalassemia trait [8]. The following is a first time case report of a β thalassemia minor patient with dentoalveolar manifestations. Case Description and Results A 22 years old male patient presented with a complaint of upper incisors mobility, which was exacerbated since 6 months before. There was no history of trauma, or any evidence of periodontal disease or caries of maxillary incisors. Oral examination revealed a class II division 1 malocclusion with no traumatic contacts. No other anomaly could be detected. Radiographic examination revealed enlarged medullary space, thin lamina dura, prominent antegonial notch (Figure 1), spiky and short roots of upper incisors (Figure 2) and a generalized root resorption (Figures 2-7). The marrow expansion within the anterior mandible resulted in a circular radiolucency consistent with over stimulation of bone marrow in thalassemia disorders (Figure 8). Laboratory examination showed microcytic, hypochromic RBCs with a compensatory increase in their numbers (Table 1). All other parameters were within normal limits. The patient was treated with 1 mg/day oral folic acid for 2 months. Within 3 weeks, the maxillary incisor mobility was fully resolved. The cyst-like radiolucency of mandibular anterior region decreased to about half its original size 2 month after therapy (Figure 9). Discussion Over the past decade the attitude toward clinical presentation of hereditary diseases has been changed. There are many hereditary transported disorders with a specific genetic Unusual Occurrence of Dentoalveolar Manifestations in a Case with Beta Thalassemia Trait Farhad Alireza, Allameh Maryam Department of Endodontics and Torabinejad Dental Research Center, Isfahan University of Medical Science, Isfahan, Iran.` Abstract A case of thalassemia minor with dentoalveolar manifestations in a 22-year-old Iranian male is presented. On the basis of patient complaint of upper incisors mobility, radiographic examination was performed which revealed enlarged medullary space, thin lamina dura, prominent antegonial notch, spiky and short roots of upper incisors and a generalized root resorption. This is the second report of dentoalveolar changes in regard to a minor hemoglubinopathy disorder. In this case treatment was carried out with 1 mg per day oral folic acid for 2 months which relived patient complaint as well as some radiographic changes. Key words: Beta thalassemia trait, Dentoalveolar manifestations, Hemoglubinopathy Corresponding author: Dr. Maryam Allameh, Postgraduate student, Department of Oral Medicine and Torabinejad Dental Research Center, Isfahan University of Medical Science, Isfahan, Iran, Tel: +983112736097; e-mail: [email protected]
Transcript of Unusual Occurrence of Dentoalveolar Manifestations in a...

425
IntroductionThalassemia is the most common type of hemoglubinopathies transmitted by hereditary. These disorders are characterized by decreased or absent synthesis of globin chains (Alpha (α) or Beta (β)). This results in a deficient hemoglobin structure with erythrocytes unable to carry adequate oxygen to cells causing insufficient tissue perfusion and delayed growth and development. In β thalassemia, β globin production can range from near normal to complete absent leading to wide range of symptoms. In the most severe form of the disease (β thalassemia major), severely reduced or absent synthesis of β globin chains from both genes (homozygous state) occurs, which results in splenomegally, growth retardation, irritability, pallor, skeletal abnormalities and maxillofacial complications. Thalassemia trait (minor), resulting from heterozygousity for β thalassemia, depending on the rate of β chain production presents as clinically asymptomatic or with very mild symptoms such as pale or shortness of breath which is more prominent during situations requiring more oxygen such as exercise and pregnancy [1,2]. These disorders may be diagnosed in laboratory investigations by elevated hemoglobin A2 and normal or elevated hemoglobin F. Also, hypochromic and microcytic Red Blood Cells (RBCs) with or without slight degree of anemia can be seen [3].
Thalassemia intermedia is a condition where the lack of β protein in hemoglobin is great enough to cause a moderately severe anemia and significant health problems including bone deformities and enlarged spleen. The severity of this condition is measured by the number of blood transfusions the patient requires in a period of time. Patients with thalassemia intermedia usually need blood transfusions to improve their quality of life but not in order to survive [4].
The incidence of thalassemia trait is 4.4 per 10000 live births and it is more common in people of Mediterranean origin and to a lesser degree, southern Asians and African Americans [5]. Iran as an Asian country is also affected with a large number of thalassemic patients. The highest rate (more than 10%) is seen in Caspian sea and the Persian gulf regions. The prevalence of the disease in other areas is 4-8 percent.
Also, more than 2 million carriers of the β thalassemia mutant gene are living in this country [6].
Dentoalveolar abnormalities occur frequently in the course of β thalassemia major and to some extent in intermedia form [7], but tooth and bone changes in β thalassemia trait has not been previously reported in literature, however there is a report on clinical oral sign occurrence in a patient with minor α thalassemia trait [8]. The following is a first time case report of a β thalassemia minor patient with dentoalveolar manifestations.
Case Description and ResultsA 22 years old male patient presented with a complaint of upper incisors mobility, which was exacerbated since 6 months before. There was no history of trauma, or any evidence of periodontal disease or caries of maxillary incisors. Oral examination revealed a class II division 1 malocclusion with no traumatic contacts. No other anomaly could be detected.
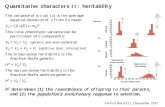
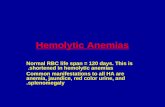
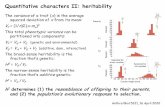
Radiographic examination revealed enlarged medullary space, thin lamina dura, prominent antegonial notch (Figure 1), spiky and short roots of upper incisors (Figure 2) and a generalized root resorption (Figures 2-7). The marrow expansion within the anterior mandible resulted in a circular radiolucency consistent with over stimulation of bone marrow in thalassemia disorders (Figure 8).
Laboratory examination showed microcytic, hypochromic RBCs with a compensatory increase in their numbers (Table 1). All other parameters were within normal limits.
The patient was treated with 1 mg/day oral folic acid for 2 months. Within 3 weeks, the maxillary incisor mobility was fully resolved. The cyst-like radiolucency of mandibular anterior region decreased to about half its original size 2 month after therapy (Figure 9).
DiscussionOver the past decade the attitude toward clinical presentation of hereditary diseases has been changed. There are many hereditary transported disorders with a specific genetic
Unusual Occurrence of Dentoalveolar Manifestations in a Case with Beta Thalassemia Trait
Farhad Alireza, Allameh Maryam
Department of Endodontics and Torabinejad Dental Research Center, Isfahan University of Medical Science, Isfahan, Iran.`
AbstractA case of thalassemia minor with dentoalveolar manifestations in a 22-year-old Iranian male is presented. On the basis of patient complaint of upper incisors mobility, radiographic examination was performed which revealed enlarged medullary space, thin lamina dura, prominent antegonial notch, spiky and short roots of upper incisors and a generalized root resorption. This is the second report of dentoalveolar changes in regard to a minor hemoglubinopathy disorder. In this case treatment was carried out with 1 mg per day oral folic acid for 2 months which relived patient complaint as well as some radiographic changes.
Key words: Beta thalassemia trait, Dentoalveolar manifestations, Hemoglubinopathy
Corresponding author: Dr. Maryam Allameh, Postgraduate student, Department of Oral Medicine and Torabinejad Dental Research Center, Isfahan University of Medical Science, Isfahan, Iran, Tel: +983112736097; e-mail: [email protected]

426
OHDM - Vol. 13 - No. 2 - June, 2014
etiology which show a vast range of manifestations. Today the classification of these diseases is preferably based on their clinical manifestations in spite of their genetic base. In β thalassemia, since 1990 the term intermedia was assigned for a group of thalassemia disorders with heterozygous compound which show a milder clinical picture than the homozygous form; however, these patients are also in need of transfusions. Furthermore, in contrast with the classical recessive forms of
β thalassemia which leads to a reduced production of normal β globin chains, some rare mutations result in the synthesis of extremely unstable β globin variants which precipitate in erythroid precursors causing ineffective erythropoiesis.
Figure 1. Class II malocclusion with the normal mandibular cortex thickening.
Figure 3. Root resorption in right maxillary canine and premolars.
Figure 4. Root resorption in left maxillary canine and premolars.
Figure 2. Resorption and spiky shape of upper incisors’ roots.
Figure 5. Root resorption in right maxillary molars.

427
OHDM - Vol. 13 - No. 2 - June, 2014
These mutations are associated with a clinically detectable thalassemia phenotype in the heterozygote and are therefore referred to as "dominant β thalassemias" [9].
Dento-alveolar manifestations in thalassemia major and to a lesser extent in the intermedia form include spiky shaped short roots, taurodontism, attenuated lamina dura, enlarged bone marrow spaces, small maxillary sinuses, absence of inferior alveolar canal and thin cortex of mandible. Craniofacial deformities include universal class II skeletal base relationship with a short mandible, a reduced posterior facial height and increased anterior facial proportions [10].
In a complete database search, only one case report of thalassemia trait with oral manifestations was found. Alexander et al reported a case of minor α thalassemia with clinical signs of pronounced anterior maxillary
protrusion, severe generalized alveolar bone loss, and an area of radiodensity usually seen in infarcted bone of other hemoglobinopathies [8].
In this case report a β thalassemia trait patient with dentoalveolar manifestations of class II malocclusion, bone marrow enlargement in jaws, attenuated lamina dura, and generalized root resorption is presented.
The coexistence of other diseases such as arthropathy [11], aseptic osteonecrosis of the femoral head [12], asthma [13], leg ulcer [14-17], hemochromatosis [18] and mood disorders [19] with minor β thalassemia trait has been shown in previous studies.
In thalassemia, reduced amount of β chains in the hemoglobin structure results in a relative excess of unbound alpha globin chains which precipitate in erythroid precursors in the bone marrow, leading to their premature death and thus causing ineffective erythropoisis. Peripheral hemolysis contributing to anemia, occurs when insoluble alpha globin include membrane damage to the peripheral erythrocytes. As a result, a compensatory mechanism in bone marrow to overcome chronic anemia leads to intensive and ineffective over stimulation of bone marrow [5,20], which in turn causes the bone marrow to expand (up to 25 to 30 times normal) [1]. Bone marrow expansion can result in the classical deformity (class II malocclusion) of facial bones [7].
There are several etiologic factors which may lead to root resorption. These include periapical or periodontal infection, orthodontic pressure, impacted tooth or tumor pressure [21]. In the present case report these stimulants were not detected. It can be postulated that over activation of osteoclasts, a major
Figure 6. Root resorption in right mandibular molars.
Figure 7. Root resorption in left mandibular molars. Figure 9. Decreased bone marrow space after therapy.
Figure 8. An enlarged bone marrow in left anterior region of mandible.
Marker Value UnitHematology
RBC 6.4 Mil/mm3Hemoglobin 13.1 g/dl
MCV 66.8 fLMCH 20.4 pg
MCHC 30.6 g/dlElectrophoresis
HbA 93.4 %HbA2 5.6 %HbF 1 %
Table 1. Laboratory results of patients.

428
OHDM - Vol. 13 - No. 2 - June, 2014
cause of osteopenia/osteoporosis in β thalassemia major [22], may be the contributing factor of root resorption.
Previous investigations have indicated that there is no significant correlation between mean serum levels of plasma folate and vitamin B12 levels in beta thalassemic carriers and in normal subjects [23,24]. However, the patient in this case report was treated with oral folic acid 1mg/day for 2
months and his chief complaint of incisor teeth mobility was completely resolved. In addition, widening of bone marrow in radiographic view decreased to about half its original size.
Considering the present case report, it seems that monitoring of patients with the thalassemia trait for possible clinical signs and symptoms is indicated, and the treatment of choice should be selected according to the patient’s symptoms.
References1. Galanello R, Origa R. Beta-thalassemia. Orphanet Journal
of Rare Diseases. 2010; 5: 11.2. Muncie HL Jr., Campbell J. Alpha and beta thalassemia.
American Family Physician. 2009; 80: 339-344.3. Handin RI, TP Stoesel, JB Lippincott. Blood: principles
and practice of hematology. Philadelphia: Lippincott Williams & Wilkins; 1997.
4. Borgna-Pignatti C. Modern treatment of thalassaemia intermedia. British Journal of Haematology. 2007; 138: 291-304.
5. Rund D, Rachmilewitz E. Beta-thalassemia. New England Journal of Medicine. 2005; 353: 1135-1146.
6. Amooeel S SA, Jahanbakhsh J, Karimi M. The pregnancy outcome in patients with minor β-thalassemia. Iranian Journal of Reproductive Medicine. 2011; 9: 9-14.
7. Perisano C, Marzetti E, Spinelli MS, Calla CA, Graci C, Maccauro G. Physiopathology of Bone Modifications in beta-Thalassemia. Anemia. 2012; 2012: 320737.
8. Alexander WN, Bechtold WA. alpha Thalassemia minor trait accompanied by clinical oral signs. Report of a case. Oral Surgery, Oral Medicine, Oral Pathology. 1977; 43: 892-897.
9. Thein SL. Dominant beta thalassaemia: molecular basis and pathophysiology. British Journal of Haematology. 1992; 80: 273-277.
10. Hazza'a AM, Al-Jamal G. Radiographic features of the jaws and teeth in thalassaemia major. Dentomaxillofacial Radiology. 2006; 35: 283-288.
11. Richter J, Specker C, Modder U, Schneider M. [Arthropathy in beta-thalassemia minor]. Medizinische Klinik (Munich). 2000; 95: 40-43.
12. Madhar M, Latifi M, Aziz S, Essadki B, Fikry T. [Aseptic osteonecrosis of the femoral head in thalassemia minor: a case report]. Revue De Chirurgie Orthopedique Et Reparatrice De L'appareil Moteur. 2005; 91: 170-172.
13. Palma-Carlos AG, Palma-Carlos ML, Costa AC. "Minor" hemoglobinopathies: a risk factor for asthma. Eur Ann Allergy Clin Immunol. 2005; 37: 177-182.
14. Vagaskar SR, Fernandez RJ, Mistry FP. Leg ulcer in a case of thalassemia minor (a case report). Journal of Postgraduate Medicine. 1989; 35: 120-121.
15. Estes JE, Farber EM, Stickney JM. Ulcers of the leg in Mediterranean disease. Blood. 1948; 3: 302-306.
16. Cooper CD, Wacker WE. The successful therapy with streptokinase-streptodornase of ankle ulcers associated with Mediterranean anemia. Blood. 1954; 9: 241-243.
17. March HW, Schlyen SM, Schwartz SE. Mediterranean hemopathic syndromes (Cooley's anemia) in adults; study of a family with unusual complications. American Journal of Medicine. 1952; 13: 46-57.
18. Lewis M, Lee GR, Haut A. The Association of Hemochromatosis with Thalassemia Minor. Annals of Internal Medicine. 1965; 63:122-128.
19. Harada H, Nakajima T, Inazawa J, Abe T. Bipolar affective disorder associated with beta-thalassemia minor. Biological Psychiatry. 1995; 37: 477-479.
20. Di Matteo R, Liuzza F, Pezzillo F, Gerardino L, Maccauro G. Subtrochanteric femoral fracture in a 26 year old woman affected by beta-thalassemia major due to minor trauma: analysis of bone modification causing the complication. Clinical Therapeutics. 2007; 158: 425-429.
21. Fuss Z, Tsesis I, Lin S. Root resorption--diagnosis, classification and treatment choices based on stimulation factors. Dental Traumatology. 2003; 19: 175-182.
22. Haidar R, Musallam KM, Taher AT. Bone disease and skeletal complications in patients with beta thalassemia major. Bone. 2011; 48: 425-432.
23. Gallerani M, Cicognani I, Ballardini P, Martinelli L, Ricci A, Dall'Ara G, et al. Analysis of folate and vitamin B12 in beta thalassemia minor. Rivista Europea Per Le Scienze Mediche E Farmacologiche. 1990; 12: 247-250.
24. Silva AE, Varella-Garcia M. Plasma folate and vitamin B12 levels in beta-thalassemia heterozygotes. Brazilian Journal of Medical and Biological Research. 1989; 22: 1225-1228.