Umbilical artery Doppler flow velocity waveforms and maternal prostaglandin E2 and F2α metabolite...
7
European Journal of Obstetrics & Gynecology and Reproductive Biology, 31 (1990) 7-13 Elsevier EUROBS 00971 Umbilical artery Doppler flow velocity waveforms and maternal prostaglandin E, and Fzn metabolite concentrations during cervical ripening with prostaglandin E, Fiona M. Fairlie ‘, Gordon D. Lang ‘, Ian A. Greer 3 and Margaret McLaren 4 I Giasgow Royal Maternity Hospital, 2 Department of Obstetrics & Gynaecology, Leicester Roya! injkrnaty, 3 Department of Obstetrics & Gynaecology, University of Edinburgh and 4 Department of Medicine, University of Dundee, U.K. Accepted for publication 2 November 1989 In 20 women, the umbilical artery flow velocity waveform (FVW) was recorded immediately before and 30-40 min after administering vaginal or extraamniotic prostaglandiu E, to ripen the cervix. Maternal plasma concentrations of pros- taglandin E, (PGE,) and prostaglandin Fzcr (PGF,,) metabolites (bicycle-PGEM and PGFM, respectively) were measured at the time of the Doppler recordings. The administration of prostaglandin E, was associated with a significant rise in maternal plasma PGFM and bicycle-PGEM concentrations, but there was no change in the umbilical artery FVW Pulsatility index (PI). These results suggest that cervical ripening with local prostaglandin E, has no effect on the umbilical artery FVW. Umbilical artery blood flow; F’rostaglandin metabolite Introduction Prostaglandin E, has been shown to be an effective method of inducing and augmenting labour with few side effects [l]. PGE, is also employed to ripen the cervix prior to induction [2]. For this purpose it may be administered either as a 3 mg vaginal pessary (Upjohn) or extraamniotically in Tylose gel [3]. Novy et al. [4] Correspondence; Dr. G.D. Lang, University of L&ester, Department of Obstetrics and Gynaecology, Clinical Sciences Building, L&ester Royal Infirmary, PO Box 65, LE27LX, U.K. 002%2243/90/$03.50 0 1990 Elsevier Science Publishers B.V. (Biomedical Division)
Transcript of Umbilical artery Doppler flow velocity waveforms and maternal prostaglandin E2 and F2α metabolite...
European Journal of Obstetrics & Gynecology and Reproductive Biology, 31 (1990) 7-13
Elsevier
EUROBS 00971
Umbilical artery Doppler flow velocity waveforms and maternal prostaglandin E, and Fzn metabolite
concentrations during cervical ripening with prostaglandin E,
Fiona M. Fairlie ‘, Gordon D. Lang ‘, Ian A. Greer 3 and Margaret McLaren 4
I Giasgow Royal Maternity Hospital, 2 Department of Obstetrics & Gynaecology, Leicester Roya! injkrnaty,
3 Department of Obstetrics & Gynaecology, University of Edinburgh
and 4 Department of Medicine, University of Dundee, U.K.
Accepted for publication 2 November 1989
In 20 women, the umbilical artery flow velocity waveform (FVW) was recorded immediately before and 30-40 min after administering vaginal or extraamniotic prostaglandiu E, to ripen the cervix. Maternal plasma concentrations of pros- taglandin E, (PGE,) and prostaglandin Fzcr (PGF,,) metabolites (bicycle-PGEM and PGFM, respectively) were measured at the time of the Doppler recordings. The administration of prostaglandin E, was associated with a significant rise in maternal plasma PGFM and bicycle-PGEM concentrations, but there was no change in the umbilical artery FVW Pulsatility index (PI). These results suggest that cervical ripening with local prostaglandin E, has no effect on the umbilical artery FVW.
Umbilical artery blood flow; F’rostaglandin metabolite
Introduction
Prostaglandin E, has been shown to be an effective method of inducing and augmenting labour with few side effects [l]. PGE, is also employed to ripen the cervix prior to induction [2]. For this purpose it may be administered either as a 3 mg vaginal pessary (Upjohn) or extraamniotically in Tylose gel [3]. Novy et al. [4]
Correspondence; Dr. G.D. Lang, University of L&ester, Department of Obstetrics and Gynaecology,
Clinical Sciences Building, L&ester Royal Infirmary, PO Box 65, LE27LX, U.K.
002%2243/90/$03.50 0 1990 Elsevier Science Publishers B.V. (Biomedical Division)
8
observed that PGE, injected into the fetal lamb circulation increased arterial pressure, decreased umbilical blood flow (measured as ml/mm per kg of fetus) and induced significant placental bed vasoconstriction. In vitro perfusion of human umbilical artery or umbilical vein preparations with a PGE,-rich solution, induces a dose-dependent vasoconstriction [5,6].
The results of in vitro studies are not necessarily applicable in vivo, but the possibility that prostaglandin administration may have significant and potentially harmful effects on human fetoplacental blood flow in vivo cannot be ignored. Furthermore, the development of reliable radioimmunoassays to measure pros- taglandin E, and Fza metabolite concentrations [7-91 provided an opportunity to study the relationship between in vivo concentrations of these vasoactive agents and the umbilical artery FVW before and after cervical ripening.
The aims of this study were to investigate whether the administration of pros- taglandin E, to ripen the cervix is associated with a change in the umbilical artery PI and to determine whether the PI is related to maternal plasma concentrations of maternal prostaglandin E, and F,, metabolites.
Methods
Twenty women admitted for induction of labour were studied. All were judged to require cervical ripening by the obstetrician responsible for their management. Fifteen women received a 3 mg PGE, vaginal pessary (Upjohn) and five women received extraamniotic PGE, (450 pg in tylose gel via a Foley catheter). The method of cervical ripening was determined by the Bishop score on admission, a low score being ‘an indication for extraamniotic PGE, [lo]. The fetal heart rate and uterine activity were monitored for 1 h after the administration of prostaglandin.
Doppler recordings Umbilical artery FVWs were recorded immediately before and 30-40 min after
PGE, administration, using a Sonicaid Vasoscan continuous wave system with a 200 Hz vessel wall filter. The PI was used to quantify waveforms [ll]. For each recording, five waveforms were measured and the mean PI value calculated. Dop- pler recordings were made in the absence of fetal breathing movements.
Measurement of prostaglandin metabolites Maternal PGE, and PGF,, metabolite concentrations (in pg per ml) were
measured at the time of the Doppler recordings. Tissue and plasma concentrations of the primary prostaglandins are difficult to measure since they are rapidly metabolised. However, in vivo studies have shown that the ‘concentrations of primary prostaglandins correlate closely with plasma concentrations of their metabolites [12,13]. It has therefore been recommended that methods of measuring prostaglandin concentrations in peripheral blood should be directed towards the more stable main metabolites rather than the primary prostaglandins [14]. The major PGF,, metabolite, 13,14-dihydro-15-ketoPGF,, (PGFM) is relatively stable and can be readily measured by radioimmunoassay [13,12]. In the case of PGE,, the major metabolite, 13,14-dihydro-15-keto-PGE, is unstable. However, if plasma is
9
incubated with sodium carbonate, a stable degradation product, bicycle-PGEM, (ll-deoxy-13,14-dihydro-15-keto-llp-16E-o-PGE~) [15] is generated which can be reliably measured by radioimmunoassay [7,16].
Maternal blood (5 ml) was obtained without venous occlusion. The blood was anticoagulated with 3.8% weight for volume trisodium citrate containing 3 . lop5 M indomethacin and 10m4 M adenosine (9 volumes of blood to 1 volume anticoagu- lant), immediately placed on ice and then centrifuged at 4” C for 20 min at 2500 x g
within 30 min of venapuncture. The plasma was separated and stored at -70 degrees C until the PGE, and PGF,, metabolite concentrations were measured by radioimmunoassay on the unextracted plasma as described above [7-91. The units of measurement were pg/ml. The antibody to PGFM was obtained from Sigma (U.K.) and the PGE, metabolite antibody was obtained from Amersham International.
Statistical analysis Wilcoxon matched-pairs signed-ranks test, Fisher’s test and Spearman’s rank
correlation coefficient were used for statistical analysis. A p value less than 0.05 was regarded as statistically significant.
Results
Table I shows pregnancy details of the 20 patients studied. Gestation ranged from 38-42 weeks. The indications for induction were: past estimated date of delivery (n = 16), social reasons (n = 2), pregnancy-induced hypertension (n = 1) and small for dates (n = 1). The Bishop score before ripening was lower in the patients treated with extraamniotic PGE,. There was no difference between the pessary and extraamniotic groups in terms of mode of delivery, parity, gestation or birthweigbt under the 10th centile (Fisher’s test).
None of the patients had detectable uterine activity (measured by an external tocodynometer) during Doppler recordings. There was no significant change in the
TABLE I
Pregnancy and delivery details of patients studied
PGE, pessary Extraamniotic PGE,
Priming method
Total Primiparous Prepriming
Bishop score mean (range)
Mode of delivery
Spontaneous vaginal Forceps Caesarean section Birthweight
< 10th centile
15 5 11 4
6.4 (4.0-8.0) 2.6 (1.0-4.0)
12 3 1 1 2 1
1 1
10
1.41 PI
1.1’
0.8’
Y.”
Pre PGE 2 Post PGE2
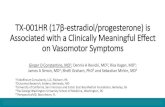
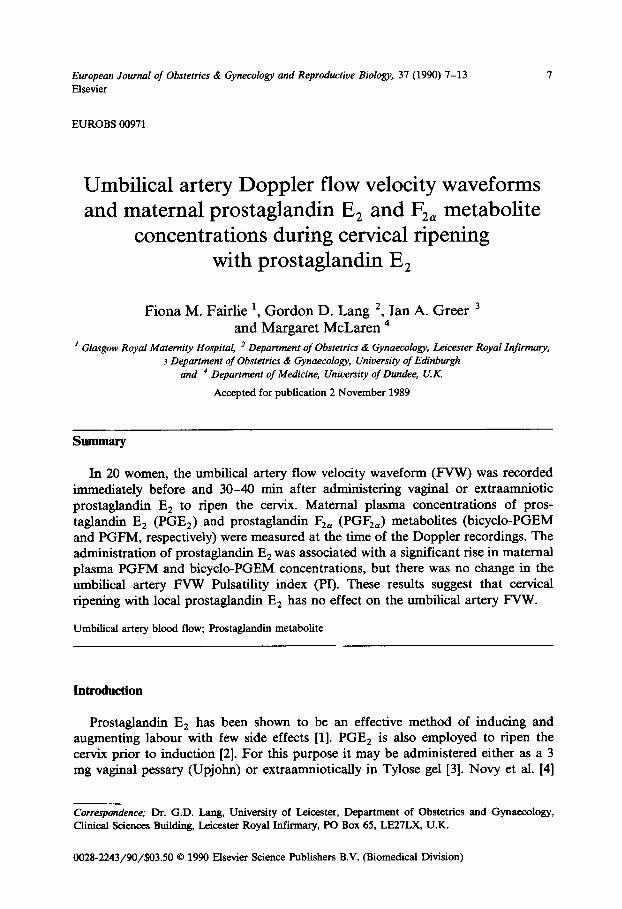
Fig. 1. Umbilical artery pulsatihty index pre and post cervical priming with a 3 mg PGE, pessary.
PI
1.3 I --.----* 0.4 ’
Pre PGE2 Post PGE2
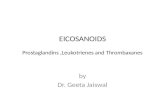
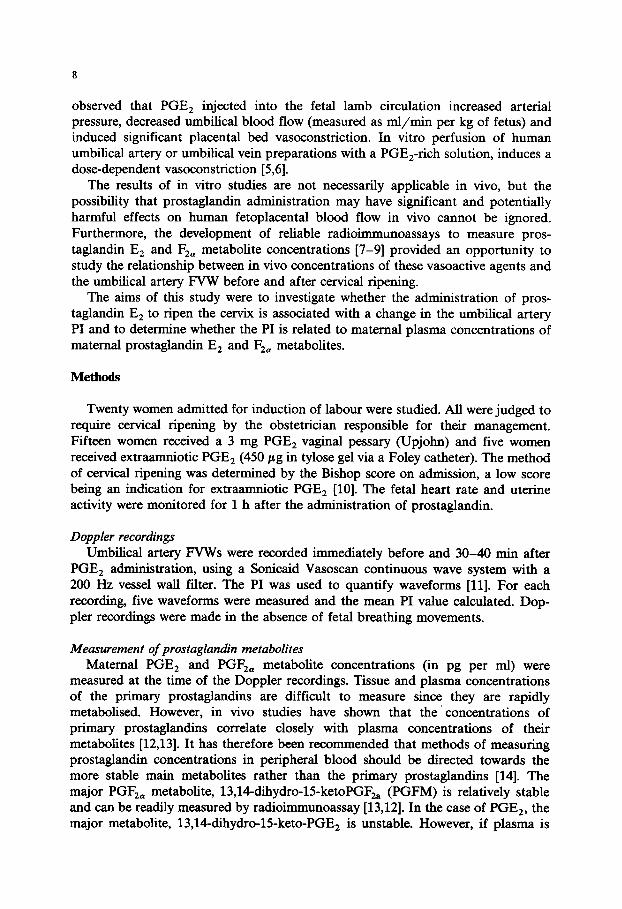
Fig. 2. Umbilical artery pulsatility index pre and post cervicaJ_primhg with extr aamniotic PGE,.
umbilical artery PI 30-40 min after administration of PGE, either as a vaginal pessary or extraamniotically (Figs. 1 and 2: p > 0.05). There was a significant rise in PGE, and PGF,, metabolite concentrations 30-40 min after PGE, administration
TABLE II
Mean (standard error of mean) for bicycle prostaglandin Ez and prostaglandin Fza metabolite concentra- tions pre and post cervical priming (pg/ml)
Concentration
Bicycloprostaghndin E,
Prostaghndin F&
Pre priming Post priming
172.2 384.7 * (20.0) (60.0)
101.5 171.4 (18.6) (34.0)
* p < 0.005 Wilcoxon test.
11
Prost@ndin Metabolite pg/mf
-1
00
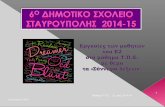
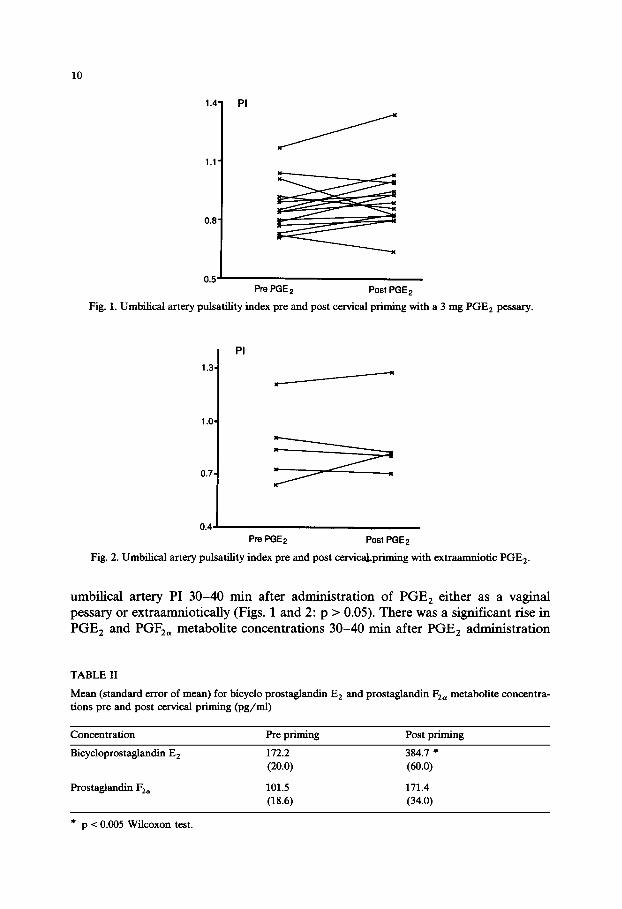
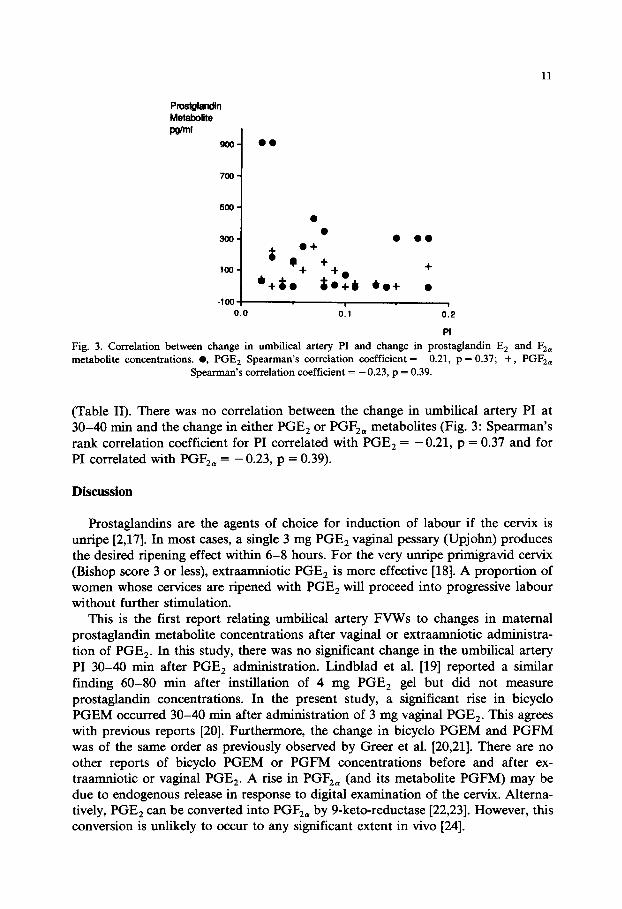
Fig. 3. Correlation between change in umbilical artery PI and change in prostaglandin E, and F,, metabolite concentrations. 0, PGE, Spearman’s correlation coefficient = - 0.21, p = 0.37; + , PGF,,
Spearman’s correlation coefficient = -0.23, p = 0.39.
(Table II). There was no correlation between the change in umbilical artery PI at 30-40 min and the change in either PGE, or PGF,, metabolites (Fig. 3: Spearman’s rank correlation coefficient for PI correlated with PGE, = -0.21, p = 0.37 and for PI correlated with PGF,, = - 0.23, p = 0.39).
Discussion
Prostaglandins are the agents of choice for induction of labour if the cervix is unripe [2,17]. In most cases, a single 3 mg PGE, vaginal pessary (Upjohn) produces the desired ripening effect within 6-8 hours. For the very unripe primigravid cervix (Bishop score 3 or less), extraamniotic PGE, is more effective [18]. A proportion of women whose cervices are ripened with PGE, will proceed into progressive labour without further stimulation.
This is the first report relating umbilical artery FVWs to changes in maternal prostaglandin metabolite concentrations after vaginal or extraamniotic administra- tion of PGE,. In this study, there was no significant change in the umbilical artery PI 30-40 min after PGE, administration. Lindblad et al. [19] reported a similar finding 60-80 min after instillation of 4 mg PGE, gel but did not measure prostaglandin concentrations. In the present study, a significant rise in bicycle PGEM occurred 30-40 min after administration of 3 mg vaginal PGE,. This agrees with previous reports [20]. Furthermore, the change in bicycle PGEM and PGFM was of the same order as previously observed by Greer et al. [20,21]. There are no other reports of bicycle PGEM or PGFM concentrations before and after ex- traamniotic or vaginal PGE,. A rise in PGF,, (and its metabolite PGFM) may be due to endogenous release in response to digital examination of the cervix. Altema- tively, PGE, can be converted into PGF,, by 9-keto-reductase [22,23]. However, this conversion is unlikely to occur to any significant extent in vivo [24].
12
Previous work has suggested that the transplacental passage of prostaglandins to the fetus is minimal owing to its metabolism by the fetus or trophoblast [25]. Prostaglandin administered vaginally or extraamniotically would be most likely to reach the umbilical vessels by direct absorption into the amniotic fluid. A significant rise in maternal plasma prostaglandin metabolite concentrations would not neces- sarily indicate a comparable concentration in the amniotic fluid or umbilical blood. Furthermore, Mak et al. [6] found that the concentration of PGE, and PGF,, required to induce vasoconstriction of the umbilical vein in vitro, was significantly greater than the concentration of these substances in umbilical blood in vivo [25,26]. Although in vitro and in vivo effects are not strictly comparable, it is possible that concentration of PGE, and PGF,, reaching the cord vessels after priming is too low to stimulate vasoconstriction.
In conclusion, this study shows that 30-40 minutes after administering PGE, vaginally or extraamniotically, there is a significant rise in maternal plasma PGE, and F,n metabolite concentrations but no change in the umbilical artery PI.
References
1 Kennedy JH, Stewart P, Barlow DH et al Induction of labour: a comparison of a single prostaglan- din Es vaginal tablet with amniotomy and intravenous oxytocin. Br J Obstet Gynaecol 1982;89:704- 707.
2 CaIder AA. Management of the unripe cervix. In Keirse MJNC., Anderson, ABM, Bennebroek Gravenhorst J, eds. Human parturition. Leiden: University Press, 1979;201-217.
3 Stewart P, Kennedy JH, Hihan E et al The unripe cervix: management with vaginal or extraamniotic prostagIandin E,. J Obstet Gynaecol 1983;4:90-93.
4 Novy MJ, Piasecki G, Jackson BT. Effect of prostagIandins E, and F2 on umbilical blood flow and fetal hemodynamics. ProstagIandins 1974;5:534-555.
5 Bjoro K, Stray-Pedersen S. In vitro perfusion studies on human umbilical arteries. Acta Obstet Gynecol Stand 1986;65:351-355.
6 Mak KKW, Gude NM, Walters WAW et al. Effects of vasoactive autacoids on the human umbilical-fetal placental vasculature 1984; Br J Obstet Gynaecol 1984;91:99-106.
7 Demers LM, Brennecke SP, Mountford LA et al Development and validation of a radioimmunoassay for prostaglandin E, metabohte levels in plasma. J Chn Endocrinol Metab 1983;57:101-106.
8 Mitchell MD, Fhnt APF, Bibby J et al Plasma concentrations of prostaglandins during late human pregnancy: the influence of normal and preterm labour. J Chn Endocrinol Metab 1978;46:947-951.
9 Mitchell MD, Flint APF, Bibby J et al. Prostaghmdins in the human umbilical circulation at birth. Br J Obstet Gynaecol 1978;85:114-118.
10 CaIder AA. Methods of induction of labour. In Studd J, ed. Progress in Obstetrics and Gynaecology, vol 3. Edinburgh: Churchill Livingstone, 1983;86-100.
11 Gosling RG, Dunbar G, King DH et al The quantitative analysis of occlusive peripheral arterial disease by a nonintrusive ultrasonic technique. Angiology 1971;22:52-55.
12 Granstrom E, KindahI H. Radioimmunoassay for prostaglandin metabolites. Adv Prostaglandin Thromboxane Res 1976;1:81-92.
13 Mitchell MD, Flint APF, Turnbull AC. Plasma concentrations of 13,14-dihydro-15-keto-prostaghm- din F during pregnancy in sheep. ProstagIandins 1976;11:319-329.
14 Granstrom E, Samuelson B. Quantitative measurement of prostaghmdins and thromboxanes: general considerations. Adv ProstagIandin Thromboxane Res 1978;5:1-13.
15 Granstrom E, Hamberg H, Hansson G et al Chemical instability of 15-keto-l-3,lCdihydro-PGE,. The reason for low assay reliability. Prostaglandins 1980;19:933-957.
16 Bothwell W, Verburg M, Wynalda M, et al A radioimmunoassay for the unstable pulmonary metabohtes of prostaglandin E, and E,: an indirect index of then in vivo disposition and pharmaco- kinetics. J Pharmacol Exp Ther 1982;220:229-235.
13
17 Mackenzie IZ. Clinical Studies on Cervical Ripening. In: Ellwood DA and Anderson ABM, eds. The
cervix in pregnancy and labour, Edinburgh: Churchill Livingstone, 1981;163-186.
18 Calder AA, Embrey MP, Tait T. Ripening of the cervix with extraamniotic prostaglandin E, in
viscous gel before induction of labour. Br J Obstet Gynaecol 1977;84:264-268.
19 Lindblad A, Ekman G, Marsal K et al. Fetal circulation 60 to 80 minutes after vagina1 prostaglandin
E, in pregnant women at term. Arch Gynecol 1985;237:31-36.
20 Greer IA, McLaren M, Godfree V et al. The effects of vaginal prostaglandin E, administration on
plasma concentrations of prostaglandin E, and prostaglandin F2 metabolites. (Abstract) 1st European
Congress on prostaglandins in Reproduction, Vienna, 1988; 108.
21 Greer IA, Fairhe FM, Calder AA. Prostaglandin E, and prostaglandin F2 metabolite concentrations
following priming of the prim&avid cervix with prostaglandin E,. (Abstract) 1st European Congress
on Prostaglandins in Reproduction, Vienna, 1988;39.
22 Flower RJ, Cheung HS, Cushman DW. Quantitative determination of prostaglandins and
malondialdehyde formed by the arachidonate oxygenase (prostaglandin synthetase) system of bovine
seminal vesicle. Prostaglandins 1973;4:325-341.
23 Jarabak J. Early steps in prostaglandin metabolism in the human placenta. Am J Obstet Gynecol
1980;138:534-540.
24 Niesert S, Christopherson W, Korte K et al. Prostaglandin E, 9-ketoreductase activity in human
decidua vera tissue. Am J Obstet Gynecol 1986;155:1348-1352.
25 Mackenzie IZ, MacLean DA, Mitchell MD. Prostaglandins in the human fetal circulation in
mid-trimester and term pregnancy. Prostaglandins 1980;20:649-654.
26 Craft IL, Scrivener R. and Dewhurst CJ. Prostaglandin Fza levels in the maternal and fetal
circulations in late pregnancy. J Obstet Gynaecol Br Commonw 1973;80:616-618.