High resolution Fourier domain optical coherence tomography in the ...

Optics Communications 285 (2012) 5564–5569
Contents lists available at SciVerse ScienceDirect
Optics Communications
0030-40
http://d
n Corr
E-m
journal homepage: www.elsevier.com/locate/optcom
Ultrahigh resolution spectral-domain optical coherence tomographyat 1.3 mm using a broadband superluminescent diode light source
Masreshaw D. Bayleyegn a,n, Houssine Makhlouf a, Caroline Crotti b, Karsten Plamann b, Arnaud Dubois a
a Laboratoire Charles Fabry, Institut d’Optique Graduate School, CNRS UMR 8501, Universite Paris-Sud, 2 Avenue Augustin Fresnel, 91127 Palaiseau Cedex, Franceb Laboratoire d’Optique Appliquee, ENSTA ParisTech–Ecole Polytechnique–CNRS UMR 7639, Chemin de la Huni�ere, 91761 Palaiseau Cedex, France
a r t i c l e i n f o
Article history:
Received 17 February 2012
Received in revised form
21 July 2012
Accepted 23 July 2012Available online 8 August 2012
Keywords:
Biomedical imaging
Optical coherence tomography
Superluminescent diode
18/$ - see front matter & 2012 Elsevier B.V. A
x.doi.org/10.1016/j.optcom.2012.07.066
esponding author. Tel.: þ33 1 64 53 34 36.
ail address: masreshaw.bayleyegn@institutop
a b s t r a c t
We present an ultrahigh resolution spectral-domain optical coherence tomography imaging system
using a broadband superluminescent diode light source emitting at a center wavelength of 1.3 mm. The
light source consists of two spectrally shifted superluminescent diodes that are coupled together into a
single mode fiber. The effective emission power spectrum has a full width at half maximum of 200 nm
and the source output power is 10 mW. The imaging system has an axial resolution of 3.9 mm in air
(o3.0 mm in biological tissue), and a lateral resolution of 6.5 mm. The sensitivity and the maximum line
rate are 95 dB and 46 kHz, respectively. Images of an infrared viewing card and a cornea from human
eye suffering from glaucoma showing Schlemm’s canal are presented to illustrate the performance of
the system.
& 2012 Elsevier B.V. All rights reserved.
1. Introduction
Optical coherence tomography (OCT) is a modern opticalimaging technology that can perform cross-sectional imaging ofbiological tissues and semi-transparent materials in real-time atmicrometer-scale resolution [1,2]. OCT has been employed forin situ and in vivo biomedical imaging [3] as well as materialcharacterization [4]. The most significant impact of OCT occurs inophthalmology for retinal imaging [5,6] and measurement of thedimensions of the anterior segment of the eye [7,8].
To resolve fine sample structures at micrometer-scale, therehas been a growing interest towards improving the spatialresolution achieved by OCT systems. Since OCT is based on low-coherence interferometry, the axial image resolution depends onthe center emission wavelength and spectral bandwidth of thelight source. High resolution OCT imaging requires the use ofbroadband light sources (see Eq. (1)). Ultrahigh resolution time-domain OCT (TD-OCT) systems were demonstrated using femto-second solid-state lasers [9] and continuum generation-basedlight sources [10]. However, such light sources are bulky, expen-sive and sensitive to misalignment. In comparison, superlumi-nescent diode (SLD) sources are compact, robust, easy to operateand cost-effective. Since the emission spectrum of a single SLD isnot broad enough for ultrahigh resolution OCT imaging, wave-length-division multiplexing of several spectrally shifted SLDs can
ll rights reserved.
tique.fr (M.D. Bayleyegn).
be done to broaden the spectrum and provide higher axialresolution than currently possible with one SLD alone. A TD-OCT system with a measured axial resolution of 3.2 mm in theretina was demonstrated by multiplexing two SLDs to achieve anemission power spectrum with a full width at half maximum(FWHM) of 155 nm centered at a wavelength of 890 nm [11].However, dual-band experiments in scattering biological samplesdemonstrated the superiority of OCT systems operating at 1.3 mmcenter wavelength compared to those operating at 0.8 mm interms of imaging depth [12,13]. But since the axial resolution isproportional to the square of the center emission wavelength andinversely proportional to the spectral bandwidth (see Eq. (1)), thespectral bandwidth of emission at 1.3 mm center wavelengthneeds to be 2.6 times larger than the one at 0.8 mm to maintainthe axial resolution. Hence, getting a broadband light source anddealing with the subsequent dispersion issues are the challengesof ultrahigh resolution OCT at 1.3 mm center wavelength.
In addition to ultrahigh resolution, biomedical imaging appli-cations require high speed and high detection sensitivity toperform real-time imaging with large penetration depth. As aconsequence, Fourier-Domain OCT (FD-OCT) techniques areincreasingly employed compared to TD-OCT because they offersignificantly better sensitivity [14] and imaging speed [15]. InFD-OCT techniques, the depth information is retrieved by Fouriertransforming the power spectrum of the interferometric signal.Depending on the technical approach used for acquiring the OCTspectral interferogram, two types of FD-OCT techniques can bedistinguished: swept-source OCT (SS-OCT) and spectral-domain OCT(SD-OCT). In SS-OCT, a tunable light source and a single-element

M.D. Bayleyegn et al. / Optics Communications 285 (2012) 5564–5569 5565
detector are employed. The emission wavelength of the light sourceis rapidly swept and the interferometric signal is recorded as afunction of time [16]. In SD-OCT, a broadband light source and aspectrometer are used. The interferometric signal is obtained fromthe spectrometer directly as a function of spectral coordinate [17].
In this report, we present an ultrahigh resolution SD-OCTsystem operating at a center wavelength of 1.3 mm. The systemuses a broadband light source consisting of two spectrally shiftedSLDs that are coupled together into a single mode fiber. TheSD-OCT system is characterized in terms of performance andcompared to a commercial SS-OCT system operating at the samecenter wavelength of 1.3 mm. Images of an infrared viewing cardand a cornea from human eye suffering from glaucoma showingSchlemm’s canal are presented.
2. Principles and methods
2.1. Principles
The principle of SD-OCT relies on low-coherence light inter-ferometry and detection of spectral interferograms by a spectro-meter [17]. A beam emitted by a broadband light source is splitinto the sample arm and the reference arm of an interferometer.Light backscattered from different depths in a sample, whichcorrespond to various optical delays, interferes with lightreflected back from a reference mirror located at a fixed position.At the output of the interferometer, the interfering light isacquired by a grating-based spectrometer. Spectral componentsare detected by a linear array of photo-detectors. For a givenoptical path difference between the backscattering feature andthe reference mirror, destructive and constructive interferenceoccurs depending on the spectral component. This results in amodulated power spectrum at the output of the spectrometer.The modulation frequency is related to the optical path differenceassociated with the depth location of the backscattering featurewithin the sample. The modulation depth is proportional to theintensity of the backscattered light. The intensity-based depthprofile of the sample is then reconstructed by calculating the
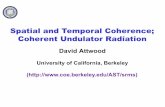
Fig. 1. Schematic diagram of the SD-OCT experimental setup. GR, grating; FL, focusing
lens; BS, beam splitter; GM, galvanometric-mounted mirror; DAQ, data acquisition boar
ND, neutral density filter and RM, reference mirror.
Fourier transform of the acquired spectral interferogram afterappropriate data re-sampling as explained in Section 2.2. Themain advantage of SD-OCT compared to TD-OCT is that the entiredepth information is obtained from a single spectral interfero-gram in one shot without any mechanical scanning. This explainswhy SD-OCT is inherently faster than TD-OCT because in TD-OCTthe depth reflectivity profile in the sample is sequentiallyacquired in time by mechanically scanning the optical path lengthin the reference arm.
The raw OCT data can be expressed as the sum of a strong DCterm, an autocorrelation term and a cross-correlation term [18].As the DC term is independent of optical path length difference, itcontains no useful information about the sample structure and itcan be easily removed by recording a background signal at thebeginning of the experiment, by blocking the sample arm andreference arm separately, and subtracting it from the interfero-metric signal. In the case of strongly backscattering samples, theautocorrelation term associated with the mutual interferencebetween all elementary waves scattered within the sample maysignificantly obscure the true sample structure that is given bythe cross-correlation term. For such samples, sophisticated phase-shifting methods can be used to remove the autocorrelation term[18,19]. However, such techniques increase the complexity of thesystem and data acquisition time. In practice, the autocorrelationterm shows as structures at shallow depths in OCT images. It iscustomary to displace the reference mirror so that the surface ofthe sample shows at a location beyond the autocorrelationstructures, and then the shallow depth range is numericallyzeroed in the image.
2.2. Methods
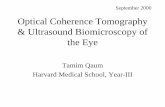
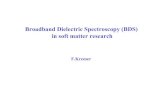
The experimental setup of our ultrahigh resolution SD-OCTsystem, based on a free-space Michelson interferometer, is shownin Fig. 1. The illuminating light source consists of a combination oftwo spectrally shifted broadband SLDs. The emission spectrum ofeach SLD was measured by the OCT spectrometer and is shown inFig. 2 (dotted curves). SLD 1 emits light at a center wavelength of1233 nm with a spectral bandwidth (FWHM) of 80 nm, while SLD
lens; LSC, InGaAs line scan camera; SLD, superluminescent diode; CL, collimating
d; PC, personal computer; DC, dispersion compensator; MO, microscope objective;

M.D. Bayleyegn et al. / Optics Communications 285 (2012) 5564–55695566
2 emits light at a center wavelength of 1335 nm with a spectralbandwidth of 110 nm. The combination of the two SLDs results ina broadband light source that has a spectral bandwidth of 200 nm(Fig. 2, solid curve). The combined broadband SLD light sourceprovides shorter coherence length and better axial resolutionthan we could get with one SLD alone. The emission spectrum ofthe combined SLD light source is centered at 1300 nm wave-length, and the maximum output power is 10 mW. The spectralbandwidth, the emission spectrum shape and the output power ofthe combined SLD light source can be controlled to a certainextent by independently changing the current drive and thetemperature control of each SLD. Light from the source is splitbetween the sample arm and the reference arm by a 50/50 cubebeam splitter. A telecentric scan lens (Thorlabs, LSM02) focuseslight onto the sample and collects the backscattered light. Agalvanometer-mounted mirror in the sample arm enables trans-verse beam scanning on the sample. In the reference arm, light isback-reflected by a silver mirror and interferes with the back-scattered light from the sample at the output of the interferom-eter. A dispersion compensator (Thorlabs, LSM02DC) in thereference arm introduces a similar magnitude of dispersion asthat of the scan lens placed in the sample arm to correct the
Fig. 2. Emission power spectrum of the light source (solid curve) for SD-OCT. SLD
1 and SLD 2 (dotted curves representing the emission spectra) are combined to
increase the spectral bandwidth of the illumination light source. The effective
spectral bandwidth of the light source is 200 nm at FWHM.
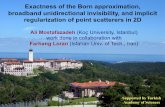
Fig. 3. Spectral interferogram and its axial PSF. (a) The spectral interferogram (left axis)
before correction (dotted curve) and after correction (solid curve) at 310 mm depth.
dispersion mismatch between the two arms. A variable attenuatoris placed in front of the reference mirror to attenuate lightreturning from the reference arm. The attenuator is adjusted tooptimize the modulation depth of the raw OCT interference term,and hence the OCT signal sensitivity [20]. A spectrometer, locatedat the output of the interferometer, consists of a diffractiongrating (600 lines/mm), an achromatic doublet (120 mm focallength) and an InGaAs linear array detector (Goodrich, SU-LDHDigital Line Scan Camera, 1024 pixels). The linear array cameraacquires the spectral interferogram and transfers the 14-bitdigital data to a personal computer equipped with an imageacquisition card (National Instruments, NI PCIe-1427). The max-imum line rate of the camera is 46 kHz.
The axial profile of the sample (A-scan) is reconstructed fromthe acquired spectral interferogram by fast Fourier transform(FFT) after data re-sampling. In FD-OCT, the structural informa-tion of the sample is encoded in the modulation frequencies ofwavenumber (k) dependent spectral fringes. However, a grating-based spectrometer in SD-OCT gives a spectral interferogram thatis almost evenly sampled with respect to wavelength (l), and as land k are inversely related, the dataset will be non-evenlysampled with respect to k. In order to apply the FFT andreconstruct the depth profile, the dataset needs to be first evenlysampled in k space. A spectral calibration method based on phaselinearization was employed to achieve this relevant re-sampling[21]. In this method, an attenuated single reflector is placed in thesample arm at a given location beyond the optical path matchcondition. Had the spectrum been evenly sampled in k space, thissingle reflector would yield a raw SD-OCT signal having a singlemodulation frequency. However, the acquired spectral interfero-gram that is plotted in Fig. 3(a) (intensity scale on the left axis) asa function of CCD pixel number shows a distorted modulationpattern. The FFT of this spectral interferogram gives a broadenedaxial point-spread function (PSF) as shown in Fig. 3(b) (dottedcurve). The phase associated with the distorted modulationpattern is extracted by a computer algorithm. It is plotted inFig. 3(a) (phase scale on the right axis) and shows a non-lineartrend. The phase is then linearized and the corresponding camerapixel indices are interpolated at those evenly spaced values of thephase. Finally, the spectral interferogram is interpolated at thenew pixel indices. The corresponding axial PSF obtained afterre-sampling (correction) is shown in Fig. 3(b) (solid curve). All thesubsequently acquired raw SD-OCT data are interpolated at thenew pixel index values determined by the above spectral calibra-tion to obtain properly sampled data in k space.
The image processing algorithm and user friendly control anddisplay software were developed using LabView. During lateralscanning of the illumination beam on the sample, multiple
and the associated non-linear phase (right axis) and (b) the corresponding axial PSF

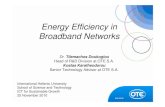
Fig. 4. Sensitivity measurement of SD-OCT. A single A-scan of a mirror with
neutral density filter of ND¼2 placed in the sample arm.
M.D. Bayleyegn et al. / Optics Communications 285 (2012) 5564–5569 5567
A-scans are acquired and processed. At the end of the scanningcycle, an intensity-based cross-sectional image (B-scan) of thesample is reconstructed and displayed on the computer screen.
3. System performance
3.1. Spatial resolutions
The transverse resolution of images obtained from OCTsystems, like other scanning imaging systems, is determined bythe size of the focused beam spot on the sample which dependson the focusing optics and the wavelength of the illuminatinglight. With a collimated Gaussian beam profile having a beamdiameter of 4.6 mm and a scan lens with an effective focal lengthof 18 mm, the transverse resolution of our SD-OCT is 6.5 mm.
The axial resolution of OCT is determined by the spectralbandwidth Dl and center wavelength lo of the light source thatilluminates the sample. For a light source with a Gaussian-shapedemission spectrum and with no dispersion mismatch betweenthe two arms of the interferometer, the axial resolution Dz isgiven by [22]
Dz¼2 ln2
pn
lo2
Dl, ð1Þ
where n is the refractive index of the sample. Eq. (1) indicates thata broader spectral bandwidth leads to a higher axial resolution. Inour system, the combination of the two SLDs with different centeremission wavelengths provides a larger spectral bandwidth andtherefore a higher axial resolution than what can be achievedusing one SLD alone. The reported SD-OCT system achieves atheoretical axial resolution of 3.7 mm in air, which corresponds to2.7 mm in biological tissue with a refractive index of n�1.4.Experimentally, the axial resolution in SD-OCT suffers not onlyfrom the constant dispersion mismatch between the two arms,which we have minimized by using a dispersion compensator, butalso from the uneven sampling of the spectral interferogram,which we have corrected as explained in Section 2.2. The experi-mental axial resolution of our system was determined by mea-suring the FWHM of the PSF obtained after correction as shown inFig. 3(b) (solid curve). At an arbitrary depth of 310 mm, the axialresolution was measured to be 3.9 mm in air (2.8 mm in tissue).
3.2. Dynamic range and sensitivity
Dynamic range (DR) refers to the ratio of the highest to thelowest measurable signals [6]. A camera with high DR is requiredin SD-OCT to be able to capture the modulating part of the rawOCT signal that is weak relative to the strong DC part. For shot-noise limited detection, the DR is proportional to the full-wellcapacity of the camera [6]. A DR of 70 dB can be reached with ourInGaAs line camera, depending on the gain capacitor setting. The14-bit digitization of the camera guarantees that the analog-to-digital convertor faithfully renders all the levels of the capturedanalog signal into a useable digital output for further digitalprocessing. A higher gain capacitor improves the dynamic rangeat the cost of increasing the readout noise.
Detection sensitivity S of OCT systems is a measure of thesmallest sample reflectivity Rs,minthat can be detected. It isdetermined by the signal level at which the signal-to-noise ratio(SNR) equals one. S is expressed as a function of Rs,min by [23]
XdB� �¼ 10log
1
Rs,min
� �ð2Þ
We have experimentally characterized the sensitivity of ourSD-OCT system by using a silver mirror as a sample and placing aneutral density (ND) filter with a density value D¼2 in front ofthe mirror. Considering a double pass through the ND filter, thecombination of the mirror and the ND filter corresponds to anequivalent sample reflectivity of 10�4. A typical PSF obtained inthis configuration after performing the required spectralre-sampling (see Section 2.2) and FFT is shown in Fig. 4. Thevertical axis in Fig. 4 gives the reflectivity expressed in decibels(�40 dB corresponds to a reflectivity of 10�4). The noise levelcorresponds to the minimal sample reflectivity that can bedetected by our SD-OCT system, defined as the sensitivity
P. It
was measured to be S¼95 dB. Inverting Eq. (2) enables one tocalculate the corresponding minimal detectable reflectivityRs,min¼3.16�10�10. A variable attenuator in the reference armhelps to match the experimental conditions during systemcharacterization and imaging of actual samples.
3.3. Imaging depth and sensitivity fall-off
The maximal imaging depth zmax of SD-OCT is determined bythe spectral sampling resolution dl of the spectrometer and isexpressed by [24]
zmax ¼1
4n
l2o
dlð3Þ
In the reported SD-OCT system, a total spectral bandwidth of245 nm was dispersed across the 1024 pixels of the lineardetector (see Fig. 2), resulting in a spectral sampling dl of0.24 nm. The theoretical imaging depth zmaxwas calculated to be1.8 mm in air (�1.3 mm in tissue), and is in agreement with theimaging depth observed experimentally by translating a singlereflector axially in the sample arm. Experimental studies of tissueabsorption and scattering have shown that the number of ballisticphotons used to image biological tissues using OCT decreasesexponentially as a function of depth [25]. The useful imagingdepth of SD-OCT in a biological specimen is in fact limited notonly by the attenuation of ballistic light but also by the depthdependent sensitivity fall-off of the imaging system.
In SD-OCT, the depth dependent sensitivity fall-off, evenwithout absorption or scattering from the sample, is due towashout of spectral fringe visibility primarily caused by thelimited spectral sampling resolution of the spectrometer toresolve high frequency spectral fringes that correspond to largedepths [24,26]. Another factor that contributes to the depth

Fig. 5. Comparison of two FD-OCT imaging systems. Cross-sectional image of an infra-red viewing card by SD-OCT (a) and SS-OCT (b). As can be seen, the ultrahigh
resolution SD-OCT image provides detailed internal structures of the viewing card better than with the SS-OCT system working at the same center wavelength.
M.D. Bayleyegn et al. / Optics Communications 285 (2012) 5564–55695568
dependent signal fall-off which becomes even worse for highresolution SD-OCT is partial aliasing [27] due to the non-uniformsampling of the spectrum in wavenumber. To characterize thesensitivity fall-off of the reported SD-OCT system as a function ofimaging depth, we repeated the sensitivity characterizationexperiment (see Section 3.2) for different axial positions of themirror used as a sample, while keeping the reflected sample armpower unchanged. Compared to the signal peak value in theproximity of zero path length difference, the sensitivity fall-off ata depth of 1 mm was found to be less than 6 dB. At the maximalimaging depth of our system (1.76 mm), the sensitivity fall-offwas measured to be �13 dB. Various hardware modifications[27–29] and advanced image reconstruction methods [26] havebeen reported to reduce the sensitivity fall-off, but at the cost ofmore hardware complexities and/or increased image acquisitionand processing time.
Fig. 6. Cross-sectional image of an excised corneosclera from glaucomatous eye
showing Schlemm’s canal. Schlemm’s canal is an annular channel situated at
nearly 0.8 mm depth from the external corneoscleral surface. It appears as two
holes (indicated by arrows) in the cross-sectional image of the cornea. The hole on
the right is wider than the hole on the left. This may be due to the collapse of one
side of the channel while working ex vivo.
4. Image results
The reported SD-OCT system was compared in terms of imagequality with a commercial SS-OCT system (Thorlabs, OCS1300SS)operating at the same center wavelength of emission and provid-ing images with a spatial resolution of 12 mm�25 mm (axial� -transverse). An infrared viewing card (Thorlabs, model VRC5) wasused as a test sample. The cross-sectional OCT images shown inFig. 5(a) and (b) were obtained using the SD-OCT system and thecommercial SS-OCT system, respectively. The images reveal theinternal structures of the card. Three distinct layers can bedistinguished. The upper layer corresponds to a plastic materialwith a thickness of 170 mm. A random distribution of scatteringstructures is revealed inside this polymer material. The bottomlayer is very inhomogeneous and corresponds to the photosensi-tive material. The middle layer, in contrast, is very homogeneoussince no scattered light is detected from this region. This layer isassumed to be the glue used for bonding the photosensitivematerial to the plastic layer. These OCT images demonstrate theimprovement of resolution when using the SD-OCT system.
As part of a collaborative project on glaucoma surgery, we alsoimaged samples of excised human corneas. Glaucoma is an eyedisorder that usually develops as a result of increased intraocularpressure (IOP) of the eye due to the accumulation of a fluid calledaqueous humor. It can permanently damage vision and lead toblindness if not treated. In a healthy eye, most of the outflow ofthe aqueous humor occurs through a circular channel calledSchlemm’s canal [30]. In glaucomatous eye, it is believed thatthe principal site of the fluid outflow resistance is related toSchlemm’s canal [31]. For the research project, human corneasnot suitable for transplantation because of low endothelial celldensity or small optical zone (o8 mm) were obtained from theBanque Franc-aise des Yeux (French Eye Bank, Paris, France). Thestudy was conducted according to the tenets of the Declaration ofHelsinki and the French legislation for scientific use of humancorneas.
Unlike the transparent fibers in healthy cornea, the sclera(white part of the eye) is made up of opaque fibers that stronglyscatter light. Moreover, glaucomatous cornea, cornea from a
person with glaucoma, scatters more light than a healthy cornea.This is partly because of the fact that glaucoma and cornealedema often co-exist [32]. It has been observed that there is ahigh incidence of endothelial dystrophies among patients withglaucoma [33], and one of the clinical manifestations of endothe-lial dystrophies is corneal edema [34]. Moreover, the persistentelevated IOP, which is often the case of glaucoma, creates highpressure gradient against stroma that drives the aqueous humorfrom the anterior chamber across endothelium into stroma,affecting corneal hydration and hence corneal edema [35,36]. Across-sectional image of excised cornea with a sclera rim of ahuman eye suffering from glaucoma is shown in Fig. 6. The twoarrows in the OCT image indicate Schlemm’s canal that is locatedat a depth of �0.8 mm inside the corneoscleral junction of humaneye suffering from glaucoma. This demonstrates that the choice ofthe wavelength region around 1.3 mm helps to maximize theimaging depth in a highly scattering biological tissue.
5. Conclusions
We have presented an ultrahigh resolution SD-OCT imagingsystem operating at a center emission wavelength of 1.3 mm usinga compact broadband light source consisting of two multiplexedSLDs with shifted spectral properties. The spectral region aroundthis center wavelength is optimal for its reduced absorption andlow tissue scattering. As a result, imaging depth in biologicalsamples is maximized. The SD-OCT imaging system has an axialresolution of 3.9 mm in air, which corresponds to 2.8 mm in typicalbiological tissues, and a lateral resolution of 6.5 mm. The sensi-tivity and the maximum line rate of the system are 95 dB and46 kHz, respectively. For ultrahigh resolution OCT, using compact,

M.D. Bayleyegn et al. / Optics Communications 285 (2012) 5564–5569 5569
robust and cost-effective SLD light sources is more convenientthan using bulky and expensive femtosecond lasers or super-continuum-generation based sources. Images of different sampleswere shown to illustrate the performance of the system. Inparticular, we have demonstrated the possibility of imagingSchlemm’s canal located at a relatively large depth inside a highlyscattering corneoscleral junction of a human eye suffering fromglaucoma. This paves the way to using ultrahigh resolutionSD-OCT imaging systems at 1.3 mm for guiding glaucoma lasersurgery. Currently, we are doing research on the development of anew tool for glaucoma surgery. A femtosecond laser will be usedto cut in the resistive region around Schlemm’s canal, which willfacilitate the drainage of the fluid. The ultrahigh resolutionSD-OCT reported here will be employed to guide the laser cutting.
Acknowledgments
This work was supported by the Agence Nationale de laRecherche under the Project NOUGAT, ANR-08-TECS-012,Program TecSan.
References
[1] D. Huang, E.A. Swanson, C.P. Lin, J.S. Schuman, W.G. Stinson, W. Chang,M.R. Hee, T. Flotte, K. Gregory, C.A. Puliafito, J.G. Fujimoto, Science 254 (1991)1178.
[2] A.F. Fercher, Journal of Biomedical Optics 1 (1996) 157.[3] J.G. Fujimoto, Biotechnology 21 (2003) 1361.[4] K. Wiesauer, M. Pircher, E. Gotzinger, S. Bauer, R. Engelke, G. Ahrens,
G. Grutzner, C Hitzenberger, D Stifter, Optics Express 13 (2005) 1015.[5] E.A. Swanson, J.A. Izatt, M.R. Hee, D. Huang, C.P. Lin, J.S. Schuman,
C.A. Puliafito, J.G. Fujimoto, Optics Letters 18 (1993) 1864.[6] M. Wojtkowski, R. Leitgeb, A. Kowalczyk, T. Bajraszewski, A.F. Fercher, Journal
of Biomedical Optics 7 (2002) 457.[7] J.A. Izatt, M.R. Hee, E.A. Swanson, C.P. Lin, D. Huang, J.S. Schuman,
C.A. Puliafito, J.G. Fujimoto, Archives of Ophthalmology 112 (1994) 1584.[8] S. Trefford, The Ocular Surface 6 (2008) 117.[9] W. Drexler, U. Morgner, F.X. Kartner, C. Pitris, S.A. Boppart, X.D. Li, E.P. Ippen,
J.G. Fujimoto, Optics Letters 24 (1999) 1221.
[10] I. Hartl, X.D. Li, C. Chudoba, R.K. Ghanta, T.H. Ko, J.G. Fujimoto, J.K. Ranka,R.S. Windeler, Optics Letters 26 (2001) 608.
[11] T. Ko, D. Adler, J. Fujimoto, D. Mamedov, V. Prokhorov, V. Shidlovski,
S. Yakubovich, Optics Express 12 (2004) 2112.[12] Y. Pan, D. Farkas, Journal of Biomedical Optics 3 (1998) 446.[13] D. Sacchet, J. Moreau, P. Georges, A. Dubois, Optics Express 16 (2008) 19434.[14] M. Choma, M. Sarunic, C. Yang, J. Izatt, Optics Express 11 (2003) 2183.[15] S. Yun, G. Tearney, B. Bouma, B. Park, J. de Boer, Optics Express 11 (2003)
3598.[16] S.R. Chinn, E.A. Swanson, J.G. Fujimoto, Optics Letters 22 (1997) 340.[17] A.F. Fercher, C.K. Hitzenberger, G. Kamp, S.Y. El-Zaiat, Optics Communications
117 (1995).[18] M. Wojtkowski, A. Kowalczyk, R. Leitgeb, A.F. Fercher, Optics Letters 27
(2002) 1415.[19] R.A. Leitgeb, C.K. Hitzenberger, A.F. Fercher, T. Bajraszewski, Optics Letters 28
(2003) 2201.[20] R. Leitgeb, W. Drexler, A. Unterhuber, B. Hermann, T. Bajraszewski, T. Le,
A. Stingl, A. Fercher, Optics Express 12 (2004) 2156.[21] H. Makhlouf, Integrated multimodal-spectral fluorescence confocal micro-
scope and spectral-domain optical coherence tomography imaging systemfor tissue screening, Thesis, Faculty of College of Optical Sciences,. The
University of Arizona (2011) 181.[22] E.A. Swanson, D. Huang, M.R. Hee, J.G. Fujimoto, C.P. Lin, C.A. Puliafito, Optics
Letters 17 (1992) 151.[23] R. Leitgeb, C. Hitzenberger, A. Fercher, Optics Express 11 (2003) 889–894.[24] G. Hausler, M.W. Lindner, Journal of Biomedical Optics 3 (1998) 21.[25] G. Popescu, A. Dogariu, Applied Optics 39 (2000) 4469.[26] K. Wang, Z. Ding, T. Wu, C. Wang, J. Meng, M. Chen, L. Xu, Optics Express 17
(2009) 12121.[27] T. Bajraszewski, M. Wojtkowski, M. Szkulmowski, A. Szkulmowska, R. Huber,
A. Kowalczyk, Optics Express 16 (2008) 4163.[28] Z. Wang, Z. Yuan, H. Wang, Y. Pan, Optics Express 14 (2006) 7014.[29] Z. Hu, A.M. Rollins, Optics Letters 32 (2007) 3525.[30] R. Avtar, R. Srivastava, Applied Mathematics and Computation 174 (2006)
316.[31] M.C. Johnson, R.D. Kamm, Investigative Ophthalmology and Visual Science 24
(3) (1983) 320.[32] R.S. Figueiredo, S.V. Araujo, E.J. Cohen, C.J. Rapuano, L.J. Katz, R.P. Wilson,
Ophthalmic Surgery and Lasers 27 (1996) 903.[33] F. Bigar, R. Witmer, Ophthalmology 89 (1982) 596.[34] G.O. 3rd. Waring, M.M. Rodrigues, P.R. Laibson, Survey of Ophthalmology 23
(1978) 147.[35] J. Ytteborg, C. Dohkman, Archives of Ophthalmology 74 (1965) 375.[36] W.S. Vanmeter, W.B Lee, D.G. Katz, Corneal Edema (Chapter 16A), Duane’s
Clinical Ophthalmology, Lippincott Williams and Wilkins (2006) http://www.
oculist.net/downaton502/prof/ebook/duanes/pages/v4/v4c016a.html#r115.