Treatment options for mCRPC in 2015 Guidelines? Treatment...
87
Treatment options for mCRPC in 2015 Guidelines? Treatment Algorithm? Christos N. Papandreou, M.D., Ph.D. University of Thessaly School of Μedicine March 2015
Transcript of Treatment options for mCRPC in 2015 Guidelines? Treatment...

Treatment options for
mCRPC in 2015
Guidelines?
Treatment Algorithm?
Christos N. Papandreou, M.D., Ph.D.University of Thessaly
School of Μedicine
March 2015

DISCLOSURES
• Invited speaker / Advisory boards / Grants
– Amgen
– Astellas
– Bayer
– Bristol
– Janssen
– Novartis
– Roche
– Sanofi

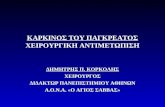
Prostate cancer disease continuum
Tumourvolume
Time
Castration
Docetaxel/chemotherapy
Localtherapy*
Metastatic
Symptoms
Castration-resistant
Non-metastatic
Asymptomatic
Hormone-sensitive
2nd-line hormonal therapies
BicalutamideFlutamideNilutamide
Death
AbirateroneCabazitaxelEnzalutamideAlpharadine
*e.g. Radiotherapy
Continued AR signalling
Kohli & Tindall. Mayo Clin Proc 2010;85:77–86.AR, androgen receptor
Abiraterone

CRPC – Definition
European Association of Urology (EAU)
Castrate-resistant prostate cancer
Serum castration levels of testosterone <50 ng/dL or <1.7 nmol/L
Three consecutive rises of PSA, 1 week apart, resulting in two 50% increases over
the nadir, with a PSA >2 ng/mL
Anti-androgen withdrawal for at least 4 weeksa
PSA progression despite secondary hormonal manipulations
or
Progression of osseous lesions: progression or appearance of two or more lesions
on bone scan or soft tissue lesions using the Response Evaluation Criteria In Solid
Tumours (RECIST) criteria and with nodes ≥2 cm in diameter
aEither anti-androgen withdrawal or one secondary hormonal manipulation completed


Cytokines, RTKs,
Microtubule bindingSteroids
AR gene located on
X chromosome
AR protein has 3 main
regions:
N-terminal domain
(NTD) which contains
the activation function
Central DNA binding
domain (DBD)
C-terminal ligand binding
domain (LBD) where
testosterone and DHT
bind
The human AR gene, transcript and protein
Hu R et al. Expert Rev Endocrinol Metab. 2010 Sep;5(5):753-76
(CAG repeats)



Pienta KJ et al. Clin Cancer Res 2006;12:1665-1671; Debes JD NEJM 2004; 351: 1488-90
1. T prod - Amplification AR
2. Mutations AR – AR SVR
3. Outlow pathway
4. Bypass pathway
5. Co-activiators
6. Stem cell regeneration
Mechanisms of disease progression in CRPC
Bcl
Bcl BclBcl
Bcl
Bcl
4
Bcl-2 overexpression
Androgen
production
ARSV
bicalutamide resistance

High concentrationsof androgens in tumour(both primary1-2 & mets3) microenvironment
Origin: adrenal gland & prostate cancer cells1-3
Genetic polymorphismsin androgen conversionand transportation4
DHT synthesis maybypass testosteronein driving CRPC5
1Nishiyama et al. Clin Cancer Res 2004; 10: 7121-262Titus MA et al. Clin Cancer Res 2005; 11: 4653-57
3Montgomery RB et al. Cancer Res 2008;68:4447-544Yang M et al.J Clin Oncol 2011; 29:2565-73
5Chang K-H et al. PNAS 2011;108: 13728–33
Persistent androgens in tumours (1)

AR splice variants (ARv)
Ligand bindingdomain is lacking
Not expected to associatewith cytoplasmicchaperones
May contribute to development of CRPC
ARv isoforms are constitutively active, promoting tumor cellgrowth independent of ligand
May contribute to resistance to Enz and Abi
Dehm SM et al. Cancer Res 2008; 68: 5469–77Hu R et al. Cancer Res 2009; 69:16-22
Watson et al. PNAS 2010; 107: 16759-65Ryan CJ & Tindall DJ; J Clin Oncol 2011; 29: 3651-58

Therapeutic strategies targeting
AR signaling pathway



Docetaxel inhibits PSA expression inhuman prostate tumors
Control Docetaxel treatment
Control Docetaxel
Significant reduction
in PSA expression
in prostate tumors
of patients treated
with docetaxel0
20
40
60
80
100
120
140
PSA
Exp
ress
ion
*
*p < 0.01
Zhu et al. Cancer Res, 70:7992,2010


Abiraterone: CYP17 blockade inhibits
androgen synthesis
Fizazi. ECCO-ESMO 2009; Teaching Lecture
abiraterone

Abiraterone acetate
Phase III post-chemo study design
Phase 3 multicenter, randomized, double-blind, placebo-controlled study (147 sites in 13 countries; USA, Europe, Australia, Canada)
Abiraterone 1000mg daily
Prednisone 5mg BID
n=797
Primary end point:
• OS (25% improvement;
HR 0.8)
Secondary end points:
• TTPP
• rPFS
• PSA response
Efficacy end points (ITT)
Placebo daily
Prednisone 5mg BID
n=398
RANDOMIZED
2:1
• 1195 patients with
progressive mCRPC
• Failed 1 or 2
chemotherapy regimens,
1 of which contained
docetaxel
de Bono et al. N Engl J Med 2011; 346(21): 1995-2005
COU-AA-301

14.8 months vs 10.9 months
Hazard ratio, 0.65;
95% CI, 0.54 to 0.77; P<0.001
N Engl J Med 2011;364:1995-2005
Median follow-up of 12.8 months
3.9-month benefit in OS
15.8 months vs 11.2 months
Final analysis
Survival benefit 4.6 months
The Lancet 13, Issue 10, 2012, 958–95
Abiraterone Acetate: OS Benefit Post-Chemotherapy

N Engl J Med 2011;364:1995-2005

N Engl J Med 2011;364:1995-2005

French ATU: Poor response to abiraterone
in patients with high Gleason score
Abiraterone French ATU program
(post-docetaxel setting)
408 mCRPC patients enrolled in 19 centers
Gleason 8-10: 51.2% at diagnosis
Independent predictive factors of poor
response to Abiraterone:
Gleason score 8-10
Number of chemotherapy lines (>1)
Azria D et al. J Clin Oncol 2012;30 (Suppl 5):abstract 149

Ph III trial of Abiraterone in asymptomatic or mildly
symptomatic mCRPC Pre-chemotherapy
Abiraterone acetate
1000 mg daily
Placebo daily
50% improvement in radiologic progression-free survival and 25%
improvement in overall survivalPrimary endpoint:
• 1000 patients with
asymptomatic or
mildly symptomatic
metastatic CRPC
• Chemotherapy naïve
• Randomized 1:1
• Stratified by: ECOG
performance status
(0 vs. 1)
T
R
E
A
T
U
N
T
I
L
P
R
O
G
R
E
S
S
I
O
N
Prednisone 5mg twice daily
Prednisone 5mg twice daily
COU-AA-302
No visceral mets





EPI-001
Inhibits transactivationof the N-terminal domain
Differs from anti-androgens which targetC-terminal ligand bindingdomain
Can potentially escape several mechanismsof castration resistance
Not yet clinically tested
Andersen RJ. Cancer cell 2010; Cancer Cell 17, 535–546
DHT
NUCLEUSCYTOPLASM
TDHEA
AR
EPI-001

MDV3100 (Enzalutamide)
Affects multiple steps in androgen signaling Inhibits binding of androgens to AR C-terminal
domain
Inhibits nuclear translocation of AR
Inhibits association of AR with DNA
Chen, et al. Lancet 2009, 10: 981–91
Scher H et al. ASCO GU 2012: J Clin Oncol 2012, 30;(suppl 5): abstr LBA1

Eplerenone activates mutant AR
Exogenous corticoids activate mutant AR in CRPC patients treated with abiraterone
Spironolactone binds and activates wild-type and mutant AR
Mutant AR activation by eplerenone inhibitedby abiraterone or bicalutamide, but most effectively by Enzalutamide (MDV3100)
Richards J et al. Cancer Res 2012; 72; 2176–82

31
Study design AFFIRM is a Phase 3, randomised, double-blind, placebo-controlled trial
Recruitment in 156 centres from 15 countries between September 2009 and November 2010
The AFFIRM trial design incorporated the recommendations of the Prostate Cancer Clinical Trials Working Group 2
Exclusion criteria included: Severe concurrent disease, infection or comorbidity, brain metastases, history of another malignancy
within previous 5 years, treatment with androgen receptor antagonists, 5-alpha reductase inhibitors, oestrogens or
chemotherapy, within 4 weeks of enrolment. Corticosteroids were not required but allowed.
CRPC=castration-resistant prostate cancer; OS=overall survival.
Scher HI, et al. N Eng J Med 2012;367:1187–97.
RANDOMISED
2:1
Patients:
• 1199 patients with
progressive CRPC
• 1–2 prior chemotherapy
regimens (≥1 docetaxel)
Primary endpoint:
• OS
Enzalutamide
160 mg daily
n=800
Placebo
n=399

Scher et al. NEJM Aug 15. [Epub ahead of print] (2012).
AFFIRM: Overall survival
3 6 9 18 21 2415
100
80
60
40
20
0
0
Surv
ival
(%
)
Duration of overall survival (months)
12
775 701 627 72 7 0211800 400Enzalutamide, n =
376 317 263 33 3 081399 167Placebo, n =
Placebo: 13.6 months(95% CI: 11.3–15.8)
Enzalutamide: 18.4 months(95% CI: 17.3–NYR)
HR = 0.63 (95%CI: 0.53–0.75); p<0.00137% reduction in risk of death
4.8 month difference in median overall survival
CI, confidence interval; HR, hazard ratio; NYR, not yet reached
No at risk:

{27%}

AFFIRM: Enzalutamide improved outcomes in patients with liver and
lung metastases compared with placebo
Efficacy outcome
Liver mCRPC Lung mCRPC
Enzalutamide
(n=92)
Placebo
(n=34)
Enzalutamide
(n=122)
Placebo
(n=59)
OS, months (95% CI) 9.0 (6.4–10.7) 5.7 (4.2–9.5) 16.5 (12.5–NM) 10.4 (8.1–NM)
HR0.697
(95% CI: 0.436–1.114)
0.760
(95% CI: 0.493–1.172)
rPFS, months (95% CI) 2.9 (2.8–4.9) 2.8 (2.7–3.2) 5.6 (5.3–8.2) 2.8 (2.7–2.9)
HR0.645
(95% CI: 0.413–1.008)
0.427
(95% CI: 0.298–0.612)
Confirmed PSA
response,* % (95% CI)
35.1
(24.4–47.1)
4.8
(0.1–23.8)
52.8
(42.9–62.5)
4.3
(0.5–14.5)
Objective response,† %
(95% CI)
14.9
(8.2–24.2)
3.3
(0.1–17.2)
29.3
(20.6–39.3)
4.9
(0.6–16.5)
*A confirmed PSA response reflected a 50% decline from baseline.
†Objective response defined as complete or partial soft tissue response per RECIST 1.1 (Response Evaluation Criteria In
Solid Tumors).
CI=confidence interval; HR=hazard ratio; mCRPC=metastatic castration-resistant prostate cancer; NM=not met; OS=overall survival;
PSA=prostate-specific antigen; rPFS=radiographic progression-free survival.
Loriot Y, et al. Presented at ASCO 2013; Poster presentation 5065.

35
AFFIRM: Significantly fewer patients experienced pain progression
with enzalutamide than with placebo
Enzalutamide Placebo
Number of evaluable patients 625 259
n (%) with pain progression 174 (28%) 101 (39%)
95% CI 24.4–31.5% 33.0–45.2%
p value 0.0018
CI=confidence interval.
Fizazi K, et al. Presented at ESMO 2012; Oral presentation 896O.
Definition: Any increase in the mean pain score at Week 13 compared with baseline
as assessed by pain diaries
To be evaluable: Valid pain diary entries for ≥4 out of 7 days at baseline run-in period
and 7 days preceding Week 13 visit

AEs, n (%)
Total events (all grades) Grade ≥3 events
Enzalutamide
(n=800)
Placebo
(n=399)
Enzalutamide
(n=800)
Placebo
(n=399)
Fatigue 269 (34) 116 (29) 50 (6) 29 (7)
Diarrhoea 171 (21) 70 (18) 9 (1) 1 (<1)
Hot flush 162 (20) 41 (10) 0 0
Musculoskeletal pain 109 (14) 40 (10) 8 (1) 1 (<1)
Headache 93 (12) 22 (6) 6 (<1) 0
36
AFFIRM: Most common AEs with enzalutamide*
*Included in this category are adverse events that occurred in >10% of patients in the enzalutamide group and that
occurred
in the enzalutamide group at a rate that was at least 2% higher than that in the placebo group.
AE=adverse event.
Scher HI, et al. N Engl J Med 2012;367:1187–97.

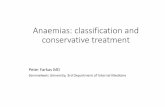
Enzalutamide substantially displaced FDHT binding at all
doses, with a maximum effect at 150 mg
Finding suggests androgen receptor binding by
enzalutamide might be saturated at plasma
concentrations of 5-15 mcg/ml
At baseline and 4 weeks post-enzalutamide
treatment, PET scans showed a reduction in
FDHT* accumulation in tumour within the
vertebrae
*FDHT: 16-18F-fluoro-5-dihydrotestosterone
Scher HI, et al. Lancet. 375:1437, 2010.
4 weeks post-enzalutamide therapy
Baseline
Phase I/II study: Androgen receptor inhibition by FDHT PET imaging
CTCs
Discordant FDG-PET / FDHT-PET
FDHT response does not predict
FDG response !

38
Enzalutamide in chemotherapy-naïve
mCRPC patients: Study design PREVAIL is a Phase 3 randomised, double-blind, placebo-controlled trial
evaluating the safety and efficacy of enzalutamide in chemotherapy-naïve patients with mCRPC
*Patient scored less than four on BPI-SF-Q3.
Recruitment in 207 centres from 22 countries across four continents between September 2010 and September 2012.
ADT=androgen-deprivation therapy; BPI-SF=Brief Pain Inventory-Short Form; ECOG PS=Eastern Cooperative Oncology Group
performance status; mCRPC=metastatic castration-resistant prostate cancer; OS=overall survival; QD=once daily;
rPFS=radiographic progression-free survival; T=testosterone.
Beer TM, et al. N Engl J Med 2014;371:424–33.
RANDOMISED
1:1
Patients:
•1717 patients with
mCRPC
•Chemotherapy-naïve
•Asymptomatic/
mildly symptomatic*
•ECOG PS 0–1
•PSA progression,
rPFS progression or
both in bone or soft
tissue on ADT
•Serum T ≤50 ng/dL
•Steroids allowed but
not required
•Ongoing ADT
Co-primary endpoints:
• OS
• rPFS
Secondary endpoints:
• PSA response
• Soft-tissue response
• Time to:
– Initiation of
chemotherapy
– First SRE
– PSA progression
Enzalutamide
160 mg QD
n=872
Placebo QD
n=845
4% of men were on steroids in
each treatment arm prior to
study entry


100
80
60
40
20
0
40
Enzalutamide significantly reduced the risk of radio-graphic
progression or death in both patient groups
*Non-visceral subgroup patients presented with only bone or nodal disease at screening; †Visceral subgroup patients
presented with lung and/or liver disease at screening.
CI=confidence interval; HR=hazard ratio; NYR=not yet reached; rPFS=radiographic progression-free survival.
Evans CP, et al. AUA 2014; Oral presentation PI-05.
rPF
S (
%)
0 3 6 9 12 15 18 21
Time to event (months)
Non-visceral Subgroup
HR=0.175
(95% CI: 0.14–0.22)
P<0.0001
Enzalutamide 735 465 235 114 29 3 1 0
Placebo 700 269 71 17 4 0 0 0
Placebo:
4.0 months
(95% CI: 3.7–5.4)
Enzalutamide: 14.1 months
(95% CI: 13.8–NYR)
0 3 6 9 12 15 18
100
80
60
40
20
0
97 49 21 14 5 2 0
101 36 8 3 1 0 0
Visceral Subgroup
rPF
S (
%)
Time to event (months)
Placebo:
3.6 months
(95% CI: 3.3–5.5)
Enzalutamide: NYR
(95% CI: 10.9–NYR)
HR=0.283
(95% CI: 0.16–0.49)
P<0.0001

41
Enzalutamide significantly improved the risk of death in patients
without visceral metastases
*Non-visceral subgroup patients presented with only bone or nodal disease at screening; †Visceral subgroup patients
presented with lung and/or liver disease at screening.
CI=confidence interval; HR=hazard ratio; NYR=not yet reached.
Evans CP, et al. AUA 2014; Oral presentation PI-05.
100
80
60
40
20
0
Ove
rall
su
rviv
al
(%)
0 3 6 9 12 15 18 21 24 27 30 33 36
Time to event (months)
HR=0.692
(95% CI: 0.57–0.83)
P=0.0001
Enzalutamide 774 771 763 741 714 669 510 360 219 112 27 2 0
Placebo 739 731 690 661 624 577 430 287 186 87 22 1 0
Placebo:
30.2 months
(95% CI: 28.0–NYR)
Enzalutamide: NYR
(95% CI: 31.5–NYR)
Non-visceral Subgroup
98 92 87 83 83 76 56 35 25 16 6 0 0
106 104 91 83 77 67 54 41 27 15 5 1 0
0 3 6 9 12 15 18 21 24 27 30 33 36
100
80
60
40
20
0
Ove
rall
su
rviv
al
(%)
Visceral Subgroup
Placebo:
22.8 months
(95% CI: 16.9–NYR)
Enzalutamide: 27.8
(95% CI: 20.9–NYR)
HR=0.822
(95% CI: 0.55–1.23)
P=0.343
Time to event (months)

42
Survival benefit was observed across all
patient subgroups analysed
Date of analysis: 16 September 2013.
CI=confidence interval; ECOG=European Cooperative Oncology Group; HR=hazard ratio.
Beer TM, et al. N Engl J Med 2014;371:424–33. Suppl appendix.
Subgroup
Number of patientsenzalutamide/
placebo
HRfor death(95% CI)
All patients 872/845 0.71 (0.60–0.84)
ECOG performance status=0 584/585 0.70 (0.56–0.87)
ECOG performance status=1 288/260 0.69 (0.53–0.90)
Age <75 555/553 0.77 (0.62–0.96)
Age ≥75 317/292 0.60 (0.47–0.79)
Geographic region – North America 218/208 0.83 (0.60–1.16)
Geographic region – Europe 465/446 0.68 (0.54–0.86)
Geographic region – Rest of world 189/191 0.62 (0.42–0.92)
Visceral disease (lung and/or liver) –Yes 98/106 0.82 (0.55–1.23)
Visceral disease (lung and/or liver) – No 774/739 0.69 (0.57–0.83)
0 0.5 1.0 1.5
Favours
enzalutamide
Favours
placebo


CHEMOTHERAPY IN mCRPC

Prednisone +/- Mitoxantrone
Ανακούφιση
από πόνο
Διάρκεια
ανακούφισης
Απάντηση
PSA
Διάμεση
επιβίωση
(μήνες)
M+P 29% 43 εβδομάδες 33% 12
P 12% 18 εβδομάδες 22% 11.3
P=.01 P<.001 NS NS
Tannock IF, et al., J Clin Oncol 14(6): 1756-64, 1996

Docetaxel / Estramustine vs Mitoxantrone / Prednisone
Petrylak DP, et al: NEJM 351:1513-20, 2004
Tannock IF, et al: NEJM 351:1502-12, 2004
Docetaxel / Prednisone vs Mitoxantrone / Prednisone
TAX 327

Median OS Δ: 2.9 mo
30% crossover
only 3% NF
TAX 327 OS
Tannock et al, N Engl J Med 2004; 351: 1502-1512

Impact of pain on OS in TAX 327
Docetaxel q3w
(n = 335)
Docetaxel qw
(n = 334)
Mitoxantrone
(n = 337)
No pain
n 183 183 184
Median survival 23.0 21.1 19.8
Hazard ratio 0.73 0.95
p value 0.009 0.65
Pain
n 152 151 153
Median survival 14.9 15.1 12.8
Hazard ratio 0.85 0.8
p value 0.17 0.068
Berthold DR, et al. J Clin Oncol 2008;26:242–45
However, asymptomatic Pts with adverse prognostic factors
may require prompt initiation of chemotherapy

Variable
Multivariate HR
95% CI P-Value
Liver metastases 1.63 1.07-2.50 0.023 Number of metastatic sites (>2 vs <2) 1.58 1.19-2.09 0.001
Pain at Baseline 1.46 1.21-1.76 <0.0001 Performance Status
(<70 vs >80)
1.42
1.08-1.85
0.011 Progression Type: Measurable disease
Bone scan progression
1.40 1.28
1.13-1.76 1.05-1.55
0.002 0.014
Baseline PSA Doubling Time (<55 days vs. >55 days)
1.20
1.001-1.44
0.048
Baseline log PSA (for every unit rise in log(PSA) in ng/dl)
1.17
1.10-1.24
<0.0001
Tumor Grade: (Gleason >8 or WHO 3-4 vs Gleason <7 or WHO 2-3)
1.18
0.98-1.41
0.076
Alkaline phosphatase (log scale) (per log unit rise, IU/L)
1.26
1.14-1.38
<0.001
Hemoglobin (per unit rise, g/dl)
0.91
0.85-0.97
0.006
Multivariate analysis (N= 635)



2nd line Chemo in mCRPC?
Symptomatic patients
Asymptomatic with Rapid Progression
Neuroendocrine / anaplastic phenotypre

Docetaxel Cabazitaxel
O OO
O
OCOCH3
OCOC6H
5
HOH
O
O
OH
NH
O
O
CH3
CH3
OH OOH
O
OCOCH3
OCOC6H
5
HOH
O
O
OH
NH
O
OO
Semisynthetic taxane selected to overcome emergence of taxane resistance1
Preclinical data1
As potent as docetaxel against sensitive cell lines and tumor models
Active against tumor cells/models resistant to currently available taxanes
Poor mdr substrate -- BBB penetration
Clinical data2
Neutropenia was the DLT in phase I trials
Antitumor activity in mCRPC, including docetaxel-resistant disease1. Attard G et al. Pathol Biol (Paris). 2006;54(2):72-84; Pivot X et al. Ann Oncol. 2008;19(9):1547-1552.
2. Mita AC et al. Clin Can Res. 2009;15(2):723-730.
(C45H57NO14)
7,10 dimethoxy analogue of docetaxel
(C43H53NO14)
Docetaxel : esterified product of 10-deacetyl baccatin III

1o Endpoint: Overall Survival (ITT analysis)
Mitoxantrone 377 300 188 67 11 1Cabazitaxel 378 321 231 90 28 4
De Bono JS et al. Lancet. 2010;376:1147-154.
100
90
0 6 12 18 24 30
Months
Probability of
Overall
Survival (%)
80
70
60
50
40
30
20
10Mitoxantrone
0
Number at risk
Cabazitaxel Mitoxantrone
Median OS (months) 15.1 12.7
Hazard ratio 0.70
95% CI 0.59-0.83
P value 0.0001
Cabazitaxel
(ITT analysis)

Factor
Patient
NumberHazard Ratio
(95%CI)
ITT population; all patients 755 0.70 (0.59-0.83)
ECOG status 0, 1 694 0.68 (0.57-0.82)
ECOG status 2 61 0.81 (0.48-1.38)
Measurable disease: no 350 0.72 (0.55-0.93)
Measurable disease: yes 405 0.68 (0.54-0.85)
No. of prior chemo: 1 528 0.67 (0.55-0.83)
No. of prior chemo: ≥2 227 0.75 (0.55-1.02)
Age <65 y 295 0.81 (0.61-1.08)
Age ≥65 y 460 0.62 (0.50-0.78)
Pain at baseline: no 314 0.57 (0.43-0.77)
Pain at baseline: yes 310 0.76 (0.59-0.98)
TROPIC: Overall Survival Subgroup Analysis
De Bono JS et al. Lancet. 2010;376:1147-1154.
0 0.5 1 1.5 2
Favors CBZ Favors M

TROPIC: Progression-Free Survival
De Bono JS et al. Lancet. 2010;376:1147-1154.
Cabazitaxel
100
90
0 6 9 1815 21
Months
Probability of
Progression-Free
Survival (%)
80
70
60
50
40
30
20
10
Cabazitaxel
0
Number at risk
Mitoxantrone 377 115 27 9 6 2452378 168 52 15 4 0090
3 12
Cabazitaxel Mitoxantrone
Median PFS (months) 2.8 1.4
Hazard ratio 0.74
95% CI 0.64-0.86
P value 0.0001
Mitoxantrone

TROPIC: Hematologic Adverse Events
Cabazitaxel (n=371)
Mitoxantrone (n=371)
All Grades
n (%)
Grade 3
n (%)
All Grades
n (%)
Grade 3
n (%)
Neutropenia 347 (94) 303 (82) 325 (88) 215(58)
Febrile neutropenia – 28 (8) – 5 (1)
Leukopenia 355 (96) 253 (68) 34 (92) 157 (42)
Anemia 361 (97) 39 (11) 30 (281) 18 (5)
Thrombocytopenia 176 (47) 15 (4) 160 (43) 6 (2)
58% grade ≥3 neutropenia in mitoxantrone arm of the TROPIC study vs 22% in mitoxantrone arm of TAX 327
Prophylactic use of G-CSF was permitted except for Cycle 1 of treatment at the discretion of the investigator
Data for hematologic adverse events were based on laboratory assessments
De Bono JS et al. Lancet. 2010;376:1147-1154.
Tannock IF et al, on behalf of the TAX 327 Investigators. N Engl J Med. 2004;351:1502-1512.

Chemo-tx in Hormone-naïve
high risk mPCa ?

Presented by: Christopher J. Sweeney, MBBS, ASCO 2014
E3805 – CHAARTED Treatment
STRATIFICATION
Extent of Mets
-High vs Low
Age
≥70 vs < 70yo
ECOG PS
- 0-1 vs 2
CAB> 30 days
-Yes vs No
SRE Prevention
-Yes vs No
Prior Adjuvant ADT
≤12 vs > 12 months
R
A
N
D
O
M
I
Z
E
ARM A:
ADT + Docetaxel
75mg/m2 every 21
days for up to 6
cycles
ARM B:
ADT (androgen
deprivation therapy
alone)
Evaluate
every 3 weeks
while
receiving
docetaxel and
at week 24
then every 12
weeks
Evaluate
every 12
weeks
Follow for time
to progression
and overall
survival
Chemotherapy
at investigator’s
discretion at
progression
ADT allowed up to 120 days prior to randomization.
Intermittent ADT dosing was not allowed
Standard dexamethasone premedication but no daily
prednisone
High volume: visceral metastases and/or >4 bone metastases
(at least 1 beyond pelvis and vertebral column)

Presented by: Christopher J. Sweeney, MBBS, ASCO 2014
Primary endpoint: Overall survival
0.0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1.0
OS (Months)
0 12 24 36 48 60 72 84
Arm ALIVEDEAD MEDIANTOTAL
A 397 101 296 57.6B 393 136 257 44.0
Pro
bability
HR=0.61 (0.47-0.80) p=0.0003
Median OS:
ADT + D: 57.6 months
ADT alone: 44.0 months
N=790
PS: 0-2
f/up: 29mos

0.0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1.0
OS (Months)
0 12 24 36 48 60 72 84
Arm ALIVEDEAD MEDIANTOTAL
A 134 19 115 .B 142 26 116 .
Pro
bability
Presented by: Christopher J. Sweeney, MBBS, ASCO 2014
0.0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1.0
OS (Months)
0 12 24 36 48 60 72 84
Arm ALIVEDEAD MEDIANTOTAL
A 263 82 181 49.2B 251 110 141 32.2
Pro
ba
bility
OS by extent of metastatic disease at start of ADT
In patients with high volume metastatic disease, there is a 17 month improvement in median
overall survival from 32.2 months to 49.2 months
We projected 33 months in ADT alone arm with collaboration of SWOG9346 team
High volume Low volume
p=0.0006
HR=0.60 (0.45-0.81)
Median OS:
ADT + D: 49.2 months
ADT alone: 32.2 months
p=0.1398
HR=0.63 (0.34-1.17)
Median OS:
ADT + D: Not reached
ADT alone: Not reached
f/up: 29mos

Presented by: Christopher J. Sweeney, MBBS, ASCO 2014
ADT + Docetaxel benefited all
subgroups
25% of High Volume : visceral

Comments
Strength: number of High Volume pts (514, 65%)
too selected? 125/514 (24%) HV pts with visceral
Insufficient evidence to recommend that low-volume patients with
castration-sensitive disease undergo early docetaxel therapy
f/up: 29 mos
There is a need to optimize the distinction between those who benefit from
chemotherapy and those who do not.
High volume: liver, lung, extensive / lytic bone, other, early non-
responders ?

OSTEOTROPIC
RADIOPHARMACEUTICALS

Radium-223 Targets Bone Metastases
Radium-223 acts
as a calcium
mimic
Naturally targets
new bone growth
in and around
bone metastases
Radium-223 is
excreted by the
small intestine
Ca
Sr
Ba
Ra

ALSYMPCA (ALpharadin in SYMptomatic
Prostate CAncer) Phase III Study Design
TREATMENT
6 injections at 4-week intervals
Radium-223 (50 kBq/kg)
+ Best standard of care
Placebo (saline)
+ Best standard of care
R
A
N
D
O
M
I
S
E
D
2:1
N = 921
PATIENTS
• Confirmed
symptomatic
CRPC
• ≥ 2 bone
metastases
• No known
visceral
metastases
• Post-
docetaxel or
unfit for
docetaxel
Planned follow-up is 3 years
• Total ALP:
< 220 U/L vs ≥ 220 U/L
• Bisphosphonate use:
Yes vs No
• Prior docetaxel:
Yes vs No
STRATIFICATION
Clinicaltrials.gov identifier: NCT00699751

Month 0 3 6 9 12 15 18 21 24 27 30
Radium-
223
614 487 332 193 125 62 31 8 8 1 0
Placebo 307 207 108 51 33 17 8 6 3 1 0
ALSYMPCA Updated Analysis
Time To First SRE*
HR = 0.64 95% CI, 0.52, 0.78
P < 0.0001
Radium-223, n = 614
Median: 12.2 months
Placebo, n = 307
Median: 6.7 months
0
10
20
30
40
50
60
70
80
90
100
%
*Provisional data

ALSYMPCA Updated Analysis
Overall Survival
Radium-223, n = 614
Median OS: 14.9 months
Placebo, n = 307
Median OS: 11.3 months
HR = 0.69595% CI, 0.581, 0.832
P = 0.00007
Month 0 3 6 9 12 15 18 21 24 27 30 33 36 39
Radium-
223614 578 504 369 274 178 105 60 41 18 7 1 0 0
Placebo307 288 228 157 103 67 39 24 14 7 4 2 1 0
0
10
20
30
40
50
60
70
80
90
100
%

ALSYMPCA Updated Analysis
Survival Benefit Across Patient Subgroups

2015

Abiraterone
Enzalutamide
in 2015

GUIDELINES ???
Guidelines are only relevant
to diseases and NOT to
patients; especially to A
particular patient



Short response (<1 year) to 1st-line ADT
Lack of undetectable PSA with 1st ADT
High Gleason score (8-10)
Short PSA doubling time (< 4-6 mo)
Visceral metastases
Predominantly lytic bone mets
Disproportionally low PSA to tumor burden
Presence of B symptoms (PS: co-morb vs dz!!)
PD on chemo-tx CEA or NSE (in the absence of other causes)
Decision tree
75
Indication for immediate chemotherapy
(Docetaxel Cabazitaxel or Pt-based)
There might be only one chance !!!
Predictors of very poor or No response to hormonal therapy
(including abiraterone/enzalutamide)
Think of
ANAPLASTIC
PCa

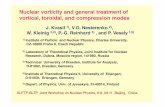
SUGGESTIONS...

mCSPC or mCRPC
Anaplastic Features
Yes (20%)
Docetaxel
Cabazitaxel
Paclitaxel ±Carboplatin
Mitoxantrone
Vinorelbine
EP
No (80%)
GoodPS
Chemo naïve
Indolent PD
Enzalutamide
Abiraterone*
Alpharadine*
Rapid PD
Docetaxel
Enzalutamide
Abiraterone
Post 1st line chemo
Indolent PD
Enzalutamide
Abiraterone
Alpharadine*
Rapid PD
Cabazitaxel
Enzalutamide
Abiraterone
Poor PS
Disease related
Chemo naïve
Docetaxel
Enzalutamide
Abiraterone*
Post 1st line chemo
Cabazitaxel(mitoxantrone
vinorelbine) Enzalutamide
Abiraterone
Alpharadine*
Comorbidity related
Chemo naïve
Enzalutamide
Abiraterone*
Alpharadine*
Post 1st line chemo
Enzalutamide
Abiraterone
(2nd line chemo)
Alpharadine*
* without visceral mets

mCSPC or mCRPC
Anaplastic Features
Yes (20%)
Docetaxel
Cabazitaxel
Paclitaxel ±Carboplatin
Mitoxantrone
Vinorelbine
EP
No (80%)
GoodPS
Chemo naïve
Indolent PD
Enzalutamide
Abiraterone*
Alpharadine*
Rapid PD
Docetaxel
Enzalutamide
Abiraterone
Post 1st line chemo
Indolent PD
Enzalutamide
Abiraterone
Alpharadine*
Rapid PD
Cabazitaxel
Enzalutamide
Abiraterone
Poor PS
Disease related
Chemo naïve
Docetaxel
Enzalutamide
Abiraterone*
Post 1st line chemo
Cabazitaxel(mitoxantrone
vinorelbine) Enzalutamide
Abiraterone
Alpharadine*
Comorbidity related
Chemo naïve
Enzalutamide
Abiraterone*
Alpharadine*
Post 1st line chemo
Enzalutamide
Abiraterone
(2nd line chemo)
Alpharadine*
* without visceral mets

FUTURE…


F-DHT scan
vs
Choline scan

Hypothesis
Detection of AR-V7 in CTC samples
from patients with mCRPC may predict
resistance to enzalutamide and abiraterone.
Antonarakis ES, ASCO 2014, A 5001

Design: Prospective Biomarker Study
30 men (in each group) with CRPC who were about to
begin treatment w/ enzalutamide or abiraterone
85% Power to detect a difference in PSA response
rates from 10% (in AR-V7[+] men) to 60% (in AR-V7[–]
men), using a 2-sided a=0.10
CTC samples were collected at 3 time points: Baseline/pretreatment
At time of Response to enzalutamide/abiraterone
At time of Resistance to enzalutamide/abiraterone
Antonarakis ES, ASCO 2014, A 5001

Outcome Measures
PSA response rate (≥50% PSA decline)
PSA progression-free survival (modified PCWG2)
Progression-free survival (modified PCWG2)
Overall survival (premature)
Antonarakis ES, ASCO 2014, A 5001

Outcomes: AR-V7 “conversions”
Outcome AR-V7[–] → AR-
V7[–] (n=36)
AR-V7[–] → AR-
V7[+] (n=6)
AR-V7[+] → AR-
V7[+] (n=16)
PSA Response68%
(95%CI, 52 –
81%)
17%
(95%CI, 4 – 58%)
0%
(95%CI, 0 – 19%)
PSA Progression-Free
Survival
6.1 months
(95%CI, 5.9 mo –
NR)
3.0 months
(95%CI, 2.3 mo –
NR)
1.4 months
(95%CI, 0.9 – 2.6
mo)
Progression-Free
Survival
6.5 months
(95%CI, 6.1 mo –
NR)
3.2 months
(95%CI, 3.1 mo –
NR)
2.1 months
(95%CI, 1.9 – 3.1
mo)Antonarakis ES, ASCO 2014, A 5001

Clinical Phenotypes
Scintigraphic Phenotypes (PET-CTs: FDG vs FDHT vs Choline)
IHC Phenotypes
CTCs Phenotype/Genotype
Molecular Pheno-/Geno-type ???