Treatment of HCV infection among active IDUs Jason Grebely, PhD Lecturer Viral Hepatitis Clinical...
26
Treatment of HCV infection among active IDUs Jason Grebely, PhD Lecturer Viral Hepatitis Clinical Research Program National Centre in HIV Epidemiology and Clinical Research University of New South Wales
-
Upload
phillip-lamb -
Category
Documents
-
view
221 -
download
2
Transcript of Treatment of HCV infection among active IDUs Jason Grebely, PhD Lecturer Viral Hepatitis Clinical...

Treatment of HCV infection among active IDUs
Jason Grebely, PhDLecturer
Viral Hepatitis Clinical Research Program
National Centre in HIV Epidemiology and Clinical Research
University of New South Wales

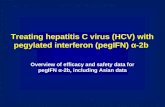
Hepatitis C treatment
IFN-α2b24 weeks
8%-12%
PEG-IFN48 weeks
25%-29%IFN-α2b 48 weeks
15%-22%
IFN-α2b+RBV 48 weeks
41%
PEG-IFN+RBV 24-48 weeks 61%-65%
10 years
?
Sustained virologic response

Management of Hepatitis C
• 1997 NIH Consensus Development Conference Statement:
“treatment of patients who are drinking significant amounts of alcohol or who are actively using illicit drugs should be delayed until these habits are discontinued for at least 6 months”
3
National Institutes Of Health Consensus Development Conference Statement. March 24-26, 1997. Available at: http://consensus.nih.gov/1997/1997HepatitisC105html.htm Accessed September 19, 2009.

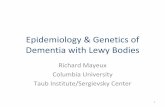
Treatment of HCV in IDUs
• Treatment initiated during opiate detoxification treatment (n=50)– IFN alfa-2a (n=34) – IFN alfa-2a + RBV (n=16)
• Drug use:– ICD-10 opiate dependency– 36% cocaine (>weekly)
• Treatment completion: 46%• Overall SVR: 36%
• 80% relapsed to drug use– SVR: 24% vs 53%
4Backmund et al. Hepatology 2001.
0
10
20
45%
6%S
VR
(%
)
30
40
50
60
70
80
90
100
>2/3 Appointments
<2/3 Appointments
P<0.05

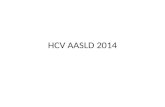
Treatment of HCV in IDUs
• Treatment of HCV during methadone maintenance therapy (interim analysis)
• IFN alfa-2b + RBV (n=50)• Mean age 50, 62% psych history, 62% markers of
advanced disease, 52% genotype 1• 78% completed HCV treatment
5
Sylvestre D, et al. Drug and Alcohol Dependence 2002.
54%
Poynard 1998McHutchison 1998
Overall
ET
R (
%)
0
20
40
60
80
100
G1 Non-G1
36%
70%
51%
P>0.05

NIH Revises Recommendations
• 2002 NIH Consensus Statement:– Management of HCV is enhanced by linking to drug-
treatment programs– Methadone is not a contraindication to HCV treatment– HCV treatment of active IDUs should be considered on
a case-by-case basis– Active IDU in and of itself should not exclude such
patients from antiviral therapy
6
NIH Management of Hepatitis C Consensus Conference Statement. June 10-12, 2002. Available at: http://consensus.nih.gov/2002/2002HepatitisC2002116html. Accessed September 19, 2009.

Treatment uptake among IDUs is still low
7
n Cohort HCV Treatment
Uptake/Year
Canada (Vancouver) 1,360 Community-based inner city residents
<1%
United States (Baltimore) 597 Community-based IDUs <1%
Australia 2,500 Needle exchange participants
1%
Grebely J, et al. J Viral Hepatitis 2009. Mehta S, et al J Community Health 2008. National Centre in HIV Epidemiology and Clinical Research 2008.

IDUs demonstrate high HCV treatment willingness
8
Stein MD, et al. Drug and Alcohol Dependence 2001. Walley AY, et al. J Substance Abuse Treatment 2005. Doab A, et al. Clinical Infectious Diseases 2005. Fischer B, et al. Presse Med 2005. Strathdee S, et al Clinical Infectious Diseases 2005. Grebely J, et al. Drug and Alcohol Dependence 2008.

Barriers to seeking treatment for HCV infection
• The major reasons for not having sought treatment were:– Lack of information/did not know that treatment was available
(23%)– Absence of symptoms (20%)– Perceived side effects of treatment (14%)– Mild liver disease (10%)– Other medical co-morbidities (8%) – Lack of interest in treatment (3%)
9
Self-reported current HCV positive status (n=188)
Never sought treatment for HCV infection (n=107, 57%)
Grebely J, et al. Drug and Alcohol Dependence 2008.

Barriers to HCV treatment uptake are multi-factorial
• Barriers to HCV treatment access may relate to:– lack of knowledge and low prioritisation among
patients– limited HCV treatment infrastructure, particularly in
settings of drug dependency treatment– lack of treatment consideration or active
discrimination by clinicians
10

Remains a reluctance to treat IDUs for HCV
• Concerns of:– Adherence– Ongoing drug use – Relapse to substance use– Risk of exacerbation of co-morbid psychiatric disease– Perceived risk of HCV reinfection following successful
treatment
11

Treatment of HCV in IDUs
12Hellard M, et al. Clinical Infectious Diseases 2009.
• Median SVR– Regardless of treatment regimen: 40.6%– Peg-IFN alfa + RBV: 54.3%

Impact of adherence on SVR
• Methadone maintenance (n=71)• IFN alfa-2b+RBV• Adherence: 80/80/80
• 59% used illicit drugs during treatment – 35% used heroin, cocaine, or
methamphetamine
• 68% (n=48) were adherent
13
0
10
20
42%
4%S
VR
(%
)
30
40
50
60
70
80
90
100
Adherent Nonadherent
P=0.001
Sylvestre D, et al. European Journal of Gastroenterology and Hepatology 2007.

Impact of ongoing drug use on adherence
14Sylvestre D, et al. European Journal of Gastroenterology and Hepatology 2007.

Discontinuation occurs early in therapy
15
• Observational study of MMT (n=50) vs. controls (n=50)• SVR was 42% in MMT vs. 56% in controls• No significant increase in methadone dose during therapy
Methadone - All
Methadone - Noncompliance
Controls - All
Controls - Noncompliance
Mauss S, et al. Hepatology 2004.

Treatment completion
16Hellard M, et al. Clinical Infectious Diseases 2009.
• Median completion overall: 70.7%• Only 1 of 5 evaluable studies demonstrated a difference in
treatment completion rates in IDUs vs. non-IDUs

Adherence
• Poor data on adherence• Varying definitions of adherence makes it difficult
to compare studies
17Hellard M, et al. Clinical Infectious Diseases 2009.

Adherence failure….
18
A “bad patient?” or …
... our failure to design a treatment program which works for that individual

Directly observed therapy for HCV
19
Grebely J, et al. Journal of Gastroenterology and Hepatology 2007.
Study Design:• Open label, prospective, observational trial
Primary Endpoint:• Proportion with undetectable HCV RNA 6 months after treatment (SVR)
N = 40
Week 48 forgenotype 1;Week 24 for genotypes 2/3
Interferon alfa-2b 3 MIU 3x/week
+ Ribavirin 800-1200 mg/day
(n = 12)
Peginterferon alfa-2b 1.5 µg/kg/week
+ Ribavirin 800-1200 mg/day
(n = 28)
Medication administration:
• IFN (3x week) and PEG-IFN (1x week) were administered as DOT
• RBV self-administered

Directly observed therapy for HCV
20
Grebely J, et al. Journal of Gastroenterology and Hepatology 2007.
• Mean age 43, 83% male, 55% genotype 2/3• Early discontinuation - 11 patients (28%)• 35% used illicit drugs in the last 6 months• 48% used illicit drugs during treatment

Impact of prior and ongoing IDU on SVR
Grebely J, et al. Journal of Gastroenterology and Hepatology 2007.
• 35% used illicit drugs in the last 6 months• 48% used illicit drugs during treatment• “frequent” – greater than weekly
21

Impact of prior and ongoing IDU on SVR
22
Sylvestre D, et al. Journal of Substance Abuse Treatment 2005.
• IFN alfa-2b + RBV during methadone maintenance (n=76)• 36% used illicit drugs during treatment• “frequent” - everyday or every other day for a min of 1 month

Impact of IDU and adherence on SVR
23
• Australian Trial in Acute Hepatitis C Study (n=109), 74 HCV
Dore G, et al. Gastroenterology 2010.

Enhancing HCV treatment through peer support
• From March 2005 to 2008, HCV-infected individuals were referred to a weekly peer-support group and assessed for HCV infection (n=204 accepted referral).
• Assessment for HCV in 53%• The first 4 weeks of support group attendance predicted
successful HCV assessment (OR: 6.03, 95% CI:3.27–11.12, P<0.001)
• Treatment for HCV was initiated in 28% (n=57)
24Grebely J, et al. J European Gastroenterology and Hepatology 2009 (In Press).

Conclusions
• Treatment of HCV among current and former IDUs is effective– Studies to date are limited by small sample size and absence of
prospective, longitudinal data collection
• Treatment completion/adherence– Comparable rates of treatment completion between IDUs and non-IDUs– Adherence has an impact on SVR
• Drug use during treatment – Drug use prior to treatment is not associated with reduced SVR – Frequent drug use may be associated with reduced response to therapy– Cannot predetermine who will discontinue due to drug use prior to initiation
of treatment – Must evaluate patients on a case by case basis
25

There is still much to learn....
• Current uptake of assessment and treatment among IDUs is still unacceptably low– Why are IDUs assessed for HCV infection not receiving treatment?
• Treatment is effective– What factors are associated with response?
• Treatment completion/adherence– Evaluation of strategies to enhance adherence (e.g. Individualized
treatment, DOT)
• Drug use prior to and during treatment– What is the impact of drug use on treatment for HCV infection?
• There is still concern about HCV reinfection following HCV treatment– Factors associated with reinfection?
26