Transforming Growth Factor β in Retinoblastoma … Growth Factor in Retinoblastoma-Related Cataract...
4
Click here to load reader
Transcript of Transforming Growth Factor β in Retinoblastoma … Growth Factor in Retinoblastoma-Related Cataract...

LABORATORY SCIENCES
Transforming Growth Factor �in Retinoblastoma-Related CataractSatoru Kase, MD; Jignesh G. Parikh, MD; Peter N. Youssef, MD;A. Linn Murphree, MD; Narsing A. Rao, MD
Objective: To analyze the histopathology and expres-sion of transforming growth factor � (TGF-�) in retino-blastoma with and without cataractous changes.
Methods:Twenty patients with unilateral retinoblastomaunderwentenucleation.Noneof thesepatientshadreceivedpreoperativechemotherapyorradiotherapy.Formalin-fixed,paraffin-embedded tissue sections were examined histo-logically for the presence of morgagnian globules or liq-uefactionof lens fibers;TGF-�was immunolocalizedusingan anti-TGF-� antibody.
Results: Two globes showed several morgagnian glob-ules and liquefaction of the lens fibers, representing cata-ractous changes. One patient had posterior subcapsularcataract; the other, anterior polar cataract. In both cases,
prominent cytoplasmic immunoreactivity for TGF-� wasdetected in retinoblastoma cells. In contrast, 3 patientsshowed histologic evidence of minor cataractous changes.The globes with either minor or no cataractous changesrevealed minimal to no expression of TGF-�.
Conclusions:These results suggest that TGF-� producedby retinoblastoma cells may induce cataract formation.
Clinical Relevance: The growth factors produced by reti-noblastoma cells may lead to associated pathologies, suchas cataracts, in the ocular structures. This study implies thatwhen a child presents with a unilateral cataract, retino-blastoma should be excluded as the primary diagnosis.
Arch Ophthalmol. 2008;126(11):1539-1542
R ETINOBLASTOMA IS A MALIG-nant ocular tumor that oc-curs in childhood. Radia-tion-induced cataract is 1complication of the treat-
ment of retinoblastoma.1 In contrast, thesimultaneous occurrence of cataract andretinoblastoma is rare,2 with a frequencyof less than 1%.3
The cytokine transforming growth fac-tor � (TGF-�) plays an important role inepithelial-mesenchymal transition of lensepithelial cells and in the accumulation ofthe extracellular matrix, which subse-quently induces cataract formation.4,5
Herein, we used immunohistochemicalmethods to examine the expression ofTGF-� in enucleated eyes with retinoblas-toma, with and without cataract.
METHODS
OPERATIVE SPECIMENS
The institutional review board of the Univer-sity of Southern California approved our useof human specimens. All procedures con-formed to the Declaration of Helsinki for re-
search involving human subjects. We col-lected 20 specimens of eyes with retinoblastomadetermined by enucleation using medical rec-ords at the Doheny Eye Institute from Janu-ary 2006 through October 2007. All eyeballshad been fixed in paraformaldehyde, 4%, soonafter enucleation. Formalin-fixed, paraffin-embedded tissue sections were processed forroutine hematoxylin-eosin and periodic acid–Schiff staining. Necrotic areas in retinoblas-toma specimens were measured using a SPOTRT-SE digital camera (Diagnostic Instru-ments Inc, Sterling Heights, Michigan).
IMMUNOHISTOCHEMISTRY
We examined 20 cases using immunohisto-chemistry to determine whether TGF-� ex-pression is characteristic in retinoblastoma ineyes with concomitant posterior subcapsularor anterior polar cataract. The slides were de-waxed, rehydrated, and rinsed twice in phos-phate-buffered saline for 10 minutes. As a pre-treatment, microwave-based antigen retrievalwas performed in 10mM citrate buffer (pH 6.0).These slides were incubated with hydrogen per-oxide, 3%, for 10 minutes and then with nor-mal goat serum for 30 minutes. Next, sec-tions were incubated with anti-mouse TGF-�monoclonal antibody (dilution 1:50; 1D11,
Author Affiliations: DohenyEye Institute (Drs Kase, Parikh,Youssef, Murphree, and Rao),Childrens Hospital Los Angeles(Drs Youssef and Murphree),and Department ofOphthalmology, Keck School ofMedicine, University ofSouthern California(Drs Youssef, Murphree, andRao), Los Angeles, California.
(REPRINTED) ARCH OPHTHALMOL / VOL 126 (NO. 11), NOV 2008 WWW.ARCHOPHTHALMOL.COM1539
©2008 American Medical Association. All rights reserved.
Downloaded From: on 06/07/2018

R&D Systems, Minneapolis, Minnesota) at room temperaturefor 2 hours. Binding of the primary antibody was localized withthe fluorescein isothiocyanate–conjugated anti-mouse second-ary antibody (Jackson ImmunoResearch Laboratories, WestGrove, Pennsylvania) for 30 minutes. Negative controls wereincubated with fluorescein isothiocyanate–conjugated mouseIgG without treatment of the primary antibody. Uveal mela-noma tissues served as positive controls for TGF-� immuno-histochemistry as previously reported.6 Sections were mountedin mounting medium, which included 46-diamidino-2-phenylindole (Vector Laboratories, Burlingame, California).Slides were examined using a Zeiss LSM510 confocal micro-scope (Zeiss, Thornwood, New York). In the non-necrotic vi-able tumor tissues, 300 tumor cells were counted from 3 or 4fields of the same slide for each specimen.
STATISTICAL ANALYSIS
Statistical evaluations were performed using the t test. Signifi-cance for all tests was P� .05.
RESULTS
DEFINITE CATARACT ASSOCIATEDWITH RETINOBLASTOMA IN 2 CASES
The Table summarizes the clinicopathologic profiles thatwere revealed in this study. Two retinoblastoma casesshowed histologic evidence of cataract (cases 1 and 2).One 2-year-old girl (case 1) and one 1-year-old girl (case2) with both diagnosed retinoblastoma and neovascularglaucoma in the left and right eyes, respectively, under-went enucleation. No systemic anomalies or metabolicdisorders were observed. Neither of the patients had cata-racts in the unaffected eyes. In each of the affected eyes,
the anterior chamber was shallow and the angle wasclosed. The iris revealed rubeosis iridis. Marked neovas-cularization of the iris was present with ectropion uvea.The vitreous cavity was partially obliterated by a grayish-white mass arising from the retina.
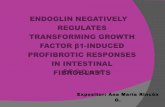
In case 1, the lens showed significant cataractouschanges, forming morgagnian globules within the en-tire cortex with the exception of the anterior portion(Figure 1A and B). Posteriorly, wide liquefaction of thelens fibers was seen (Figure 1B and C), while the nucleusremained intact. The posterior lens capsule was thick-ened where lens epithelial cells migrated (Figure 1C).
In case 2, liquefaction was present beneath the ante-rior lens capsule (Figure 1D). No cataractous changes wereobserved in the posterior side of the lens. Examinationof the tumors revealed undifferentiated retinoblastoma(Figure 2A) with a necrotic area and multiple foci ofcalcification in both cases. The retina adjacent to the tu-mor tissue was detached. Retinoblastoma cells invadedthe vitreous cavity and were present in the vicinity of theposterior capsule (Figure 1C). Microscopic rupture of thelens capsule was not detected in either case.
MINOR CATARACTOUS CHANGESIN 3 CASES OF RETINOBLASTOMA
Three cases showed histopathologic evidence that couldbe classified as minor cataractous changes (cases 3-5). Sev-eral morgagnian globules existed near the posterior cap-sule (Figure 1E). The number of morgagnian globules waslow,and theextentof the lenschangewas small in thisgroupcompared with that in the definite group. Liquefaction wasobserved beneath the posterior capsule (Figure 1F), but thearea of liquefied change was limited in this group.
Table. Clinicopathologic Characteristics of Retinoblastoma Cases
Case No./Sex/Age, y Eye Lens
MorgagnianGlobules Liquefaction
TumorDimension,
mm
Necrosis
Diff NVGChoroidalInvasion
ON HeadInvasion
TGF-�– PositiveCells, %
Eye,%
Size,mm2
1/F/2 L PSC �� �� 12�9 26 28 Un � � − 802/F/1 R APC � � 12�10 49 59 Un � − � 803/M/1 L Minor � − 16�11 54 95 Un � � � �104/M/2 L Minor � − 14�14 68 133 Un − � � �105/M/3 L Minor − � 14�13 57 104 Un − − � �106/F/1 R − − − 16�12 63 121 Un − − − �107/M/3 R − − − 7�5 75 26 Un − − − �108/F/1 L − − − 6�2 42 50 Well − − � �109/F/0.5 L − − − 12�9 58 63 Well − − − �10
10/F/2 L − − − 17�13 42 92 Un � − − 2011/F/1 L − − − 14�10 45 63 Well � � − �1012/M/2 R − − − 13�10 39 51 Well − − − �1013/F/1 L − − − 18�13 51 119 Un − − − �1014/M/0.4 R − − − 10�9 14 13 Well − − − �1015/F/3 L − − − 12�9 63 68 Well − − − �1016/M/4 L − − − 13�11 47 67 Un − − − �1017/M/1 R − − − 14�10 9 13 Well − − − �1018/M/1 R − − − 12�4 19 9 Un � − � �1019/F/1 L − − − 13�4 49 25 Un − − � �1020/F/2 R − − − 11�9 47 46 Un � − − �10
Abbreviations: APC, anterior polar cataract; Diff, differentiation; L, left; NVG, neovascular glaucoma; ON, optic nerve; PSC, posterior subcapsular cataract; R, right;TGF-�, transforming growth factor �; Well, well-differentiated; Un, undifferentiated; �, present focally; ��, prominently present; −, not found/identified.
(REPRINTED) ARCH OPHTHALMOL / VOL 126 (NO. 11), NOV 2008 WWW.ARCHOPHTHALMOL.COM1540
©2008 American Medical Association. All rights reserved.
Downloaded From: on 06/07/2018

IMMUNODETECTION FOR TGF-�IN RETINOBLASTOMA TISSUES
The number of TGF-�–immunopositive tumor cells wasmarkedly high (80%) in 2 cases (cases 1 and 2), show-ing association of cataract with the retinoblastoma. Im-munohistochemical analysis demonstrated cytoplasmicimmunoreactivity for TGF-� in most of the tumor cells,including those in the vitreous cavity (Figure 2A and B).In contrast, no TGF-� was expressed in the detachedretina adjacent to the tumor (Figure 2C and D). Com-pared with the findings seen in the definite cataract group,the rate of cases positive for TGF-� was low in those withretinoblastoma, representing minor cataractous changes,and in those with no cataractous changes (Table).
ASSOCIATION BETWEEN TUMOR SIZE,NECROSIS, AND CATARACTOUS CHANGE
In this study, statistical analysis was performed betweenretinoblastoma cases with (n=5, cases 1-5) and without(n=15, cases 6-20) cataractous changes. The mean tumorsize, calculated by multiplying the anterior-posterior andhorizontal dimensions, was 156.4 mm2 (standard devia-tion [SD], 39.6 mm2) in those with cataractous changes
and 116.8 mm2 (SD, 65.5 mm2) in those without catarac-tous changes (P=.22). The mean necrotic area was 83.8mm2 (SD, 40.9 mm2) (mean rate of immunopositive cells,50.8% [SD, 15.5%]) in cases with cataractous changes and55.1 mm2 (SD, 35.6 mm2) (mean rate of immunopositivecells, 44.2% [SD, 14.8%]) in those without cataractouschanges (P=.06 in size, P=.45 in percentage).
COMMENT
These 2 conditions, retinoblastoma and congenital cata-ract, are believed to be unrelated2; however, anterior po-lar cataract has been reported to occur in association withretinoblastoma.7 Because it is very unlikely that congen-ital cataracts of any type are related to retinoblastoma,2
the presence of the cataracts found in this series is un-usual. In the present study, 2 patients showed the pres-ence of definite cataracts (cases 1 and 2) in their eyes thatcontained retinoblastoma. Case 1 had a posterior sub-capsular cataract intermingled with morgagnian glob-ules in her left eye, implying that the histological find-ings of the cataract are typical.
It is likely that retinoblastoma cells upregulate vascu-lar endothelial growth factor, which causes neovascular-
A B C
D E F
Figure 1. Hematoxylin-eosin staining (A, B, and D-E) and periodic acid–Schiff staining (C) in the lenses of retinoblastoma cases. A, There are no apparent changesin the anterior capsule or cortex of the lens in case 1. B, The lens reveals significant cataractous changes forming morgagnian globules within the posterior cortex(arrows). Lens epithelial cells migrate beneath the posterior capsule. There is liquefaction of the lens fibers (arrowhead). C, The posterior lens capsule positive forperiodic acid–Schiff staining is thickened with wide liquefied necrosis. Retinoblastoma cells in the vitreous cavity exist in the vicinity of the posterior capsule(arrow). D, There is liquefaction beneath the anterior lens capsule (case 2). E, Several morgagnian globules exist near the posterior capsule (case 3). F, Focalliquefied necrosis is observed beneath the posterior capsule (case 5).
(REPRINTED) ARCH OPHTHALMOL / VOL 126 (NO. 11), NOV 2008 WWW.ARCHOPHTHALMOL.COM1541
©2008 American Medical Association. All rights reserved.
Downloaded From: on 06/07/2018

ization of the iris.8 This indicates that retinoblastoma cellscan produce bioactive growth factors. Hales et al4 dem-onstrated that an intravitreal TGF-� injection induced pos-terior and anterior subcapsular cataractous changes in vivo.In retinoblastoma cases with cataract (cases 1 and 2), im-munoreactivity for TGF-� was detected in tumor cells, in-cluding cells floating in the vitreous cavity, whereas thedetached retina in conjunction with the tumor tissueshowed no TGF-� expression. These results indicate thatTGF-� was upregulated in retinoblastoma tissue in thesecases. Moreover, the immunohistochemical results in theretinoblastoma cases we examined revealed that the num-ber of TGF-�–positive tumor cells was low in almost allcases without cataractous changes. Taken together, thesefindings indicate that TGF-� produced by retinoblas-toma cells may induce cataract formation, suggesting thatthe 2 conditions are related.
Seven of the 20 eyes had neovascular glaucoma, ofwhich 3 had increased expression of TGF-� with posi-tive neoplastic cells ranging from 20% to 80% (Table).It was demonstrated that TGF-� concentrations were highin the aqueous humor of patients with open-angle andneovascular glaucoma secondary to other patholo-gies.9,10 Indeed, TGF-� is a multifunctional growth fac-tor involved in various ocular changes.11 These resultssuggest that TGF-� produced by tumor cells may play arole not only in the pathogenesis of cataract develop-ment, but also in neovascular glaucoma associated withretinoblastoma.
As shown in the Table, the 3 patients with retinoblas-toma and only minimal cataractous changes (cases 3-5)demonstrated no upregulation of TGF-�. The pathogen-esis of minor cataractous changes in eyes containingretinoblastoma is unclear from the current study. Size ofthe tumor and extent of necrosis did not correlate withthe lens changes when comparing eyes with and withoutcataractous changes, as there was no statistically signifi-cant difference in size of the tumor (P=.22) and extentof necrosis (P=.06 in size, P=.45 in percentage). Theseresults suggest that the extent of tumor growth andnecrosis in retinoblastoma may not be associated withpathogenesis of cataractous changes. However, expres-sion of TGF-� may play a role in the development of thelens changes with typical histologic features of well-developed cataract.
Submitted for Publication: December 17, 2007; final re-vision received March 24, 2008; accepted April 25, 2008.Correspondence: Narsing A. Rao, MD, Doheny Eye In-stitute, 1450 San Pablo St, Room DRVC 211, Los Ange-les, CA 90033 ([email protected]).Financial Disclosure: None reported.Funding/Support: This study was supported by grantEY03040 from the National Institutes of Health.
REFERENCES
1. Brooks HL Jr, Meyer D, Shields JA, Balas AG, Nelson LB, Fontanesi J. Removalof radiation-induced cataracts in patients treated for retinoblastoma. ArchOphthalmol. 1990;108(12):1701-1708.
2. Brown GC, Shields JA, Oglesby RB. Anterior polar cataracts associated with bi-lateral retinoblastoma. Am J Ophthalmol. 1979;87(3):276.
3. Balasubramanya R, Pushker N, Bajaj MS, Ghose S, Kashyap S, Rani A. Atypicalpresentations of retinoblastoma. J Pediatr Ophthalmol Strabismus. 2004;41(1):18-24.
4. Hales AM, Chamberlain CG, Dreher B, McAvoy JW. Intravitreal injection ofTGF� induces cataract in rats. Invest Ophthalmol Vis Sci. 1999;40(13):3231-3236.
5. Schulz MW, Chamberlain CG, McAvoy JW. Inhibition of transforming growth factor-beta-induced cataractous changes in lens explants by ocular media and alpha2-macroglobulin. Invest Ophthalmol Vis Sci. 1996;37(8):1509-1519.
6. Esser P, Grisanti S, Bartz-Schmidt K. TGF-� in uveal melanoma. Microsc ResTech. 2001;52(4):396-400.
7. Amaya L, Taylor D, Russell-Eggitt I, Nischal KK, Lengyel D. The morphologyand natural history of childhood cataracts. Surv Ophthalmol. 2003;48(2):125-144.
8. Pe’er J, Neufeld M, Baras M, Gnessin H, Itin A, Keshet E. Rubeosis iridis in reti-noblastoma: histologic findings and the possible role of vascular endothelial growthfactor in its induction. Ophthalmology. 1997;104(8):1251-1258.
9. Yu XB, Sun XH, Dahan E, et al. Increased levels of transforming growth factor-beta1 and -beta2 in the aqueous humor of patients with neovascular glaucoma.Ophthalmic Surg Lasers Imaging. 2007;38(1):6-14.
10. Yamamoto N, Itonaga K, Marunouchi T, Majima K. Concentration of trans-forming growth factor �2 in aqueous humor. Ophthalmic Res. 2005;37(1):29-33.
11. Saika S. TGF� pathobiology in the eye. Lab Invest. 2006;86(2):106-115.
Hematoxylin-eosin
Deta
ched
Ret
ina
Retin
obla
stom
a
TGF-β
50 µm
50 µm
A B
C D
Figure 2. Hematoxylin-eosin staining and immunodetection for transforminggrowth factor � (TGF-�) in retinoblastoma and the detached retina adjacentto the tumor. A, Tumor cells diffusely proliferate without formingFlexner-Wintersteiner rosettes, representing undifferentiated retinoblastomain case 1. Cytoplasmic immunoreactivity for TGF-� is observed inretinoblastoma cells (B) but not in the detached retina (D). C, Inner nuclearlayer gets thin in the detached retina in conjunction with retinoblastomatissue.
(REPRINTED) ARCH OPHTHALMOL / VOL 126 (NO. 11), NOV 2008 WWW.ARCHOPHTHALMOL.COM1542
©2008 American Medical Association. All rights reserved.
Downloaded From: on 06/07/2018












![OPEN ACCESS International Journal of Molecular Sciences...hair growth [2].Platelet-derived growth factor (PDGF) isoforms reportedlyinduce and maintain theanagen phase of the murine](https://static.fdocument.org/doc/165x107/60f85444d7faee31306fdb0e/open-access-international-journal-of-molecular-sciences-hair-growth-2platelet-derived.jpg)



