Detection of hepatitis Β virus DNA and mutations in K-ras ...

JOURNAL OF INTERFERON AND CYTOKINE RESEARCH 17:65-67 (1997) „T,^^ ^^. .. ,TT^TT^ . ^T^T
Mary Ann Lieber!, Inc. SHORT COMMUNICATION
Tolerance and Efficacy of Subcutaneous Interferon-/3Administered for Treatment of Chronic Hepatitis C
ANGELES CASTRO,1 ESTHER CARBALLO,2 AGUSTÍN DOMÍNGUEZ,3 MOISÉS DIAGO,4DOLORES SUÁREZ,5 JUAN ANTONIO QUIROGA,6 and VICENTE CARREÑO6
ABSTRACT
We studied tolerance to subcutaneous (s.c.) administration of 6 million units of interferon-/8 (IFN-/3), giventhree times per week for 6 months, and its efficacy in the treatment of 15 patients with chronic hepatitis C.At the end of the treatment, alanine aminotransferase (ALT) levels were significantly reduced (p = 0.024) inall patients, and 4 (27%) had a normal ALT value. However, at the end of the study (12 months), only 1 ofthese 4 had a sustained response. No patient cleared hepatitis C virus (HCV) RNA completely, but the RNAcould be detected only by polymerase chain reaction (PCR) in the sustained responder. Adverse side effectsto the S.C. IFN-/3 were infrequent. Leukocyte (p = 0.012) and platelet (p = 0.013) counts decreased signifi-cantly during treatment but did not necessitate dose modifications. Thus, although s.c. IFN-/3 at the dosageused had little efficacy in the treatment of chronic hepatitis C, the excellent tolerance to the treatment sug-gests that the effects of higher doses should be explored.
INTERFERON-a (IFN-a) therapy of chronic hepatitis C in- patients remained untreated for 12 months (the end of theduces alanine aminotransferase (ALT) normalization in ap- study). Fifteen of these 39 patients were selected for this study,
proximately 50% of the patients treated, but as many as 50% Their pretreatment characteristics are shown in Table 1. Criteriaof those responding relapse after therapy is discontinued.'" for inclusion were abnormal ALT values for at least 1 year be-IFN-a administration often induces a mild to severe myelo- fore study entry, a positive test for serum anti-hepatitis C virussuppression that may require dose reduction or even drug with- (HCV) and HCV RNA, chronic hepatitis histologically proveddrawal.(1-2) Interferon-/? (IFN-/3) has been used for the treat- in a liver biopsy obtained within the year before study entry/6-7'ment of chronic hepatitis C, usually given in low doses (1 or 3 and patient age between 18 and 65 years. Exclusion criteriamillion units), administered daily for short periods (4-12 were a positive test for HB sAg, HIV infection, other causes ofweeks) by i.v. infusion.'3-5' As this route is inconvenient and liver disease (e.g., alcohol abuse, autoantibody titer higher thantroublesome for patients, we have assessed the benefits of treat- 1/80), and active intravenous drug use, previous antiviral or im-ing chronic hepatitis C with IFN-/3 given s.c. munomodulatory treatment, or pregnancy.
Between December 1992 and January 1995, 90 patients with The patients received 6 MU of human fibroblast-derivedchronic hepatitis C were enrolled in a multicenter, randomized, IFN-/3 s.c. three times per week for 6 months. We used fi-controlled study (A. Castro et al., unpublished observations), broblast-derived IFN-ß because no recombinant IFN-/3 was
Of these, 51 were treated with 6 million units (MU) of human available to us at the time of the study design. Both prepara-fibroblast-derived IFN-/3 (Frone, Serono, Madrid, Spain) ad- tions seem to behave similarly in the clinic.(8) All patients were
ministered i.m. three times per week for 6 months. Thirty-nine examined every 3 months before study entry and monthly dur-
1Hospital luán Canalejo, A Coruña, Spain.2Complejo Hospitalario Universitario, Santiago de Compostela, Spain.3Hospital luán Ramón liménez, Huelva, Spain.4Hospital General Universitario, Valencia, Spain.5Hospital Arquitecto Marcide, Ferrol, Spain.department of Hepatology, Fundación Jiménez Díaz, and Fundación para el Estudio de las Hepatitis Virales, Madrid, Spain.The following investigators participated in this study: A Coruña: A. Castro, J. Pedreira, S. López-Calvo, M. Hermida, P. Vega; Santiago de
Compostela: E. Carballo, E. Losada; Huelva: A. Domínguez, J. Ponzone-Riera; Valencia (Hospital General): M. Diago, R. Zapater, P. Carbonell,C. González, R. Cors; Ferrol: D. Suárez, F. Carrasco-Sanz, E. Pastor-Rubin de Celis; Las Palmas de Gran Canaria: L. Inglada; Alicante: J.Such, J. Vázquez, M.F. Garcia; Valencia (Hospital Clínico): J.A. del Olmo, M.A. Serra-Desfilis, M.S. Gilabert-Fos, F. Rodríguez-Almendros;Madrid (Hospital Virgen de la Torre): A. Pérez-Mota; Madrid (Fundación Jiménez Díaz): V. Carreño, J.A. Quiroga, M. Pardo, V. Vaquero.
65

66 CASTRO ET AL.
Table 1. Characteristics of Patients at Study Entry ALT (IU/I)
Sex (M/F)Age (years)3Known duration of disease (years)3Body weight (kg)aALT in IU/liter3No. of transfusions (%)No. with intravenous drug use (%)No. by other route (%)Histologie activity (grading)bMinimalMildModerate
Histologie staging0No fibrosisMild fibrosisModerate fibrosisSevere fibrosis
385.169158
12/311 (23-56)6.4 (1-26)12 (51-93)102 (52^178)4(27)5 (33)6(40)
1 (7)9(60)5(33)
1 (7)5(33)5 (33)4(27)
aMean value ± SD (range).bAccording to Desmet et al.6 These are expressed as number
of cases (%).
ing and after treatment, for a total period of 12 months (end ofstudy). At each visit, blood samples were drawn for laboratoryassessment. This study was approved by the respective hospi-tal ethics committee and was conducted in accordance with theDeclaration of Helsinki on human experimentation. Informedconsent was obtained from each patient.
Anti-HCV was detected by second-generation HCV ELISA(Ortho Diagnostic Systems, Raritan, NJ) and confirmed by re-combinant immunoblot assay (RIBA-2). Serum HCV RNA was
tested by reverse transcription (RT) and nested polymerasechain reaction (PCR), using primer pairs derived from the 5'noncoding region of the HCV genome.(9) HCV RNA was quan-tified by the Amplicor HCV-Monitor test (Roche DiagnosticSystems, F. Hoffmann-La Roche, Basle, Switzerland), used ac-
cording to supplier's instructions. Paired samples (basal and fi-nal) were assayed in the same run. The assay is based on a sin-gle combined RT and amplification reaction of the target HCVRNA present in samples (100 pi), by means of the enzyme rTthDNA polymerase in the presence of Mn2+.
The results of the assay were expressed as HCV RNA copiesper milliliter (linear range lOMO6 copies per milliliter; the accu-rate limit of detection is 103 copies per milliliter). IFN-jS levelswere measured by an ELISA specific for biologically active hu-man IFN-ß according to supplier's instructions (Toray-FujiBionics, Inc., Tokyo, Japan), with the inclusion of standards (from0 to 200 UJ/ml). Serum samples from storage at -20°C were as-
sayed in duplicate. Patients were monitored for serum IFN-/3 lev-els at the beginning of the study, at 1-month intervals during thefirst 3 months of treatment, on the day of the last WN-ß injec-tion, and 1 month after the end of therapy. Hématologie parame-ters and liver function tests were performed by standard methods.For statistical analysis, repeated measurements were compared bynonparametric analysis of variance (Friedman's test).After 1 month of s.c. IFN-/3 administration, the ALT levels
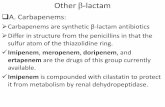
had decreased significantly from the pretreatment values (Fig.1), and they remained at similar low levels until the end of treat-ment (p = 0.024). Three of fifteen (20%) patients had normalALT values 1 month after therapy initiation, and 4 of 15 pa-
2 3 4TIME (MONTHS)
FIG. I. Changes in the mean transaminase levels in IFN-jß-treated patients. Vertical bars indicate the standard error of themean.
tients (27%) had normal ALT values after 2 months of treat-ment. Later, the proportion of patients with ALT normalizationfluctuated slightly, but 4 patients (27%) had normal values at
therapy end. During the posttreatment follow-up, 3 of these 4had relapsed in terms of serum ALT levels (2 within the first3 months and 1 later), and only 1 still had a normal ALT levelat the end of the study.All patients had HCV RNA in their serum at study entry. At
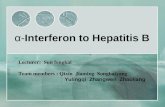
therapy end, the HCV RNA concentration had decreased in 4 pa-tients, including 2 patients who had a biochemical response (Fig.2). The HCV RNA concentration was below the limit of detec-tion in the quantitation assay in the patient who had a sustainedALT normalization, but HCV RNA was still detectable by PCR.
No serum IFN-/3 could be detected by ELISA in .any patientbefore, during, or after therapy.
Adverse side effects were, in general, absent. One patient de-veloped a mild flu-like syndrome (fever < 38°C). Two patientscomplained of headache, and 3 had asthenia. Local reaction atthe site of injection was uncommon (7%). One month after thebeginning of IFN-/3 administration, leukocyte counts had de-creased in all patients but were only significantly below pre-treatment levels at the fifth month (p = 0.012) and thereafter re-turned to their pretherapy values. Platelet counts decreasedsignificantly after 1 month of treatment (p = 0.013) and remainedthe same until therapy end. Thereafter, the counts returned to pre-treatment values. No dose modifications were necessary as a re-sult of these decreases in leukocyte and platelet counts.
HCV RNA COPIES/ml
THERAPY START THERAPY END
FIG. 2. HCV RNA concentration (copies per milliliter) in in-dividual patients before and after therapy. (•) biochemical re-sponders; (O) nonresponders.

SUBCUTANEOUS IFN-ß IN CHRONIC HEPATITIS C 67
IFN-ß has been used previously in the treatment of chronichepatitis C. Kiyosawa et al.,(4) in a small controlled trial, foundthat 3 of 12 patients had a sustained ALT normalization whengiven IFN-ß i.v. These included 1 of 5 patients who received3 MU daily for 28 days and 2 of 7 treated with 1 MU threetimes per week for 12 weeks. Other authors have reported bet-ter results with a dose of 6 MU given daily for up to 8 weeks'5'or 3 MU given three times a week for 6 months.'10* As the i.v.route was used in all these studies, we tried giving IFN-ß bythe s.c. route at a dosage of 6 MU three times a week for 6months. After the first month of treatment and thereafter untilcompletion of treatment (6 months), we observed a significantdecrease in ALT levels in the treated patients. Moreover, 4 pa-tients had a complete response at therapy end, although only 1of these had a sustained response. Interestingly, in the only sus-tained responder, HCV RNA was finally only detectable byPCR. Taken together, these results suggest that IFN-ß admin-istered by the s.c. route might be beneficial for some patientswith chronic hepatitis C.
The efficacy we obtained with an IFN-ß dosage of 6 MU islower than that achievable with IFN-a.'1,2' However, in vitroIFN-ß and IFN-a have comparable effects in the suppression ofHCV replication in human T cell lines.'1 •' Several authors'8,12,13'have reported that IFN-ß given s.c. can produce biologic effectseven though no IFN is detectable in the plasma. Our results arein agreement with this observation, as IFN-ß was never de-tectable in the serum during s.c. treatment, even when patientshad received a total dose of 468 MU at the end of therapy.
Some of our clinical findings might be due to the develop-ment of neutralizing antibodies to IFN-ß, which might blockits biologic effects."4' We did not look for these, but we ob-served a biochemical response and a slight virologie effect inour IFN-ß-treated patients, which suggests that it would beworth trying an s.c. dose higher than 6 MU in future trials.Indeed, recent preliminary results showed that when recombi-nant IFN-ß was administered s.c. at dosages of 9 or 12 MU for24 weeks, a response of as high as 43% was achieved in chronichepatitis C treatment.'15'
The excellent tolerance for IFN-ß should also be noted.Clinical symptoms were much less frequent and much milderthan those usually observed with IFN-a, where even at a lowdosage, almost all treated patients experience a flu-like syn-drome.'1,2' The dose did not need to be modified due to de-creases in leukocyte or platelet counts. This suggests thatdosages higher than 6 MU might be used safely.
REFERENCES
1. HOOFNAGLE, J.H. (1992). Interferon therapy of viral hepatitis.In: Interferon: Principles andMedicalApplications. S. Baron, D.H.Coppenhaver, F. Dianzani, W.R. Fleischmann, T.K. Hughes, G.R.Kumpel, D.W. Niesei, G.J. Stanton, and S.K Tyring (eds.)Galveston: The University of Texas Medical Branch at Galveston,pp. 431^162.
2. PARDO, M., MARRIOTT, E., MOLINER, M.C., QUIROGA,J.A., and CARREÑO, V. (1995). A risk-benefit assessment of in-terferon-alpha in the treatment of hepatitis. Drug Safety 13,304-316.
3. OHNISHI, K., NOMURA, F., and ITDA, S. (1989). Treatment ofposttransfusion non-A, non-B acute and chronic hepatitis with hu-
man fibroblast /3-interferon: A preliminary report. Am. J.Gastroenterol. 84, 596-600.
4. KIYOSAWA, K, SODEYAMA, T., NAKANO, Y., YODA, H.,TANAKA, E., HAYATA, T., TSUCHIYA, K, YOUSUF, M., andFURUTA, S. (1989). Treatment of chronic non-A, non-B hepati-tis with human interferon ß: A preliminary study. Antiviral Res.12, 151-162.
5. FUJIOKA, S., HINO, K, FUKUHARA, A., NASHIDA, Y., YA-SUDA, K, KONDO, T., NTWA, H., UNO, S., and SUZUKI, H.(1989). Treatment of chronic non-A, non-B hepatitis: Comparativestudy of dosage of human interferon-/3. Acta Hepatol. Jpn. 30,516-521.
6. DESMET, V.J., GERBER, M., HOOFNAGLE, J.H., MANNS, M.,and SCHEUER, P.J. (1994). Classification of chronic hepatitis:Diagnosis, grading and staging. Hepatology 19, 1513-1520.
7. KNODELL, R.G., ISHAK, KG, BLACK, W.C., CHEN, T.S.,CRAIG, R., KAPLOWITZ, N., and KIERNAN, T.W. (1981).Formulation and application of a numerical scoring system for as-sessing histological activity in asymptomatic chronic active he-patitis. Hepatology 1, 431-435.
8. LIBERATI, A.M., HORISBERGER, M.A., PALMISANO, L., AS-TOLFI, S., NASTARI, A., MECHATI, S., VILLA, A., MANCINI,S., ARZANO, S., and GRIGNANI, F. (1992). Double-blind random-ized phase I study on the clinical tolerance and biological effects ofnatural and recombinant interferon-ß. J. Interferon Res. 12, 329-336.
9. CASTILLO, I., BARTOLOMÉ, J., NAVAS, S., GONZALEZ, S.,HERRERO, M., and CARREÑO, V. (1994). Virological and bio-chemical long-term follow-up of patients with chronic hepatitis Ctreated with interferon. Hepatology 19, 1342-1346.
10. "KAKUMU, S., YOSHIOKA, K, WAKITA, T., ISHIKAWA, T.,TAKAYANAGI, M., and HIGASHI, Y. (1993). A pilot study ofribavirin and interferon beta for the treatment of chronic hepatitisC. Gastroenterology 105, 507-512.
11. SHIMIZU, Y.K., and YOSHIKURA, H. (1994). Multicycle infec-tion of hepatitis C virus in cell culture and inhibition by interfer-ons alpha and beta. J. Virol. 68, 8406-8408.
12. GOLDSTEIN, D., SIELAFF, K.M., STORER, B.E., BROWN,R.R., DATTA, S.P., WITT, P.L., TEITELBAUM, A.P., SMAL-LEY, R.V., and BORDEN, CE. (1989). Human biologic responsemodification by interferon in the absence of measurable serum con-
centrations: A comparative trial of subcutaneous and intravenousinterferon-/3 serine. J. Nati. Cancer Inst. 81, 1061-1068.
13. BOCCI, V. (1992). Pharmacokinetics of interferons and routes ofadministration. In: Interferon: Principles and MedicalApplications.S. Baron, D.H. Coppenhaver, F. Dianzani, W.R. Fleischmann, T.K.Hughes, G.R. Klimpel, D.W. Niesel, G.J. Stanton, and S.K. Tyring(eds.) Galveston: The University of Texas Medical Branch atGalveston, pp. 417^125.
14. FIERLBECK, G, and SCHREINER, T. (1994). Incidence and clin-ical significance of therapy-induced neutralizing antibodies againstinterferon-0. J. Interferon Res. 14, 205-206.
15. HALBERSETZER, F., MARCELLIN, P., BOYER, N., ZOULIM,F., CHOSSEGROS, P., ERLINGER, S., ALAM, J., and TREPOC. ( 1995). Recombinant interferon beta for the treatment of chronichepatitis C. Hepatology 22, 119A [Abstract].
Address reprint requests to:Dr. Vicente Carreño
Hepatology UnitFundación Jiménez DíazAvda. Reyes Católicos, 2
28040 MadridSpain
Received 2 April 1996/Accepted 1 October 1996