Therapeutic effect of β-blockers in triple-negative breast cancer postmenopausal women
9
EPIDEMIOLOGY Therapeutic effect of b-blockers in triple-negative breast cancer postmenopausal women Edoardo Botteri • Elisabetta Munzone • Nicole Rotmensz • Carlo Cipolla • Vincenzo De Giorgi • Barbara Santillo • Arnaldo Zanelotti • Laura Adamoli • Marco Colleoni • Giuseppe Viale • Aron Goldhirsch • Sara Gandini Received: 1 July 2013 / Accepted: 26 July 2013 / Published online: 3 August 2013 Ó Springer Science+Business Media New York 2013 Abstract Beta-blockers (BB) drugs have been used for decades worldwide, mainly to treat hypertension. However, in recent epidemiological studies, BBs were suggested to improve cancer prognosis. In the wake of this evidence, we evaluated the possible therapeutic effect of BBs in triple- negative breast cancer (TNBC) patients. We identified 800 postmenopausal women operated between 1997 and 2008 for early primary TNBC. The effect of BB intake on the risk of breast cancer (BC) recurrence and death was evaluated through competing risk and Cox regression survival models. At cancer diagnosis, 74 (9.3 %) women out of 800 were BBs users. Median age was 62 years in BB users and 59 years in non-users (P = 0.02). BB users and non-users were similarly distributed by all tumor characteristics. The 5-year cumulative incidence of BC-related events was 13.6 % in BB users and 27.9 % in non-users (P = 0.02). The beneficial impact of BBs remained statistically significant at multivariable analysis (HR, 0.52; 95 % CI 0.28–0.97), after the adjustment for age, tumor stage, and treatment, peritumoral vascular invasion and use of other antihypertensive drugs, antithrombotics, and statins. Adjusted HRs for metastases and for BC deaths were 0.32 (95 % CI 0.12–0.90) and 0.42 (95 % CI 0.18–0.97), respectively, in favor of BBs. Hypertension, other antihyper- tensive drugs, antithrombotics, and statins did not impact prognosis. In this series of postmenopausal TNBC patients, BB intake was associated with a significantly decreased risk of BC-related recurrence, metastasis, and BC death. Innovative therapeutic strategies including BBs should be urgently explored in cancer patients. Keywords Beta-blockers Á Breast cancer Á Triple negative Á Prognosis Introduction Beta-blocker (BB) drugs have been used for decades worldwide, typically to treat hypertension, coronary artery Electronic supplementary material The online version of this article (doi:10.1007/s10549-013-2654-3) contains supplementary material, which is available to authorized users. E. Botteri (&) Á N. Rotmensz Á B. Santillo Á S. Gandini Division of Epidemiology and Biostatistics, European Institute of Oncology, Milan, Italy e-mail: [email protected] E. Munzone Á M. Colleoni Division of Medical Senology, European Institute of Oncology, Milan, Italy C. Cipolla Á A. Zanelotti Division of Cardiology, European Institute of Oncology, Milan, Italy V. De Giorgi Department of Dermatology, University of Florence, Florence, Italy L. Adamoli Á A. Goldhirsch Department of Medicine, European Institute of Oncology, Milan, Italy G. Viale Department of Pathology and Laboratory Medicine, European Institute of Oncology, Milan, Italy G. Viale University of Milan, Milan, Italy 123 Breast Cancer Res Treat (2013) 140:567–575 DOI 10.1007/s10549-013-2654-3
Transcript of Therapeutic effect of β-blockers in triple-negative breast cancer postmenopausal women

EPIDEMIOLOGY
Therapeutic effect of b-blockers in triple-negative breast cancerpostmenopausal women
Edoardo Botteri • Elisabetta Munzone • Nicole Rotmensz • Carlo Cipolla •
Vincenzo De Giorgi • Barbara Santillo • Arnaldo Zanelotti • Laura Adamoli •
Marco Colleoni • Giuseppe Viale • Aron Goldhirsch • Sara Gandini
Received: 1 July 2013 / Accepted: 26 July 2013 / Published online: 3 August 2013
� Springer Science+Business Media New York 2013
Abstract Beta-blockers (BB) drugs have been used for
decades worldwide, mainly to treat hypertension. However, in
recent epidemiological studies, BBs were suggested to
improve cancer prognosis. In the wake of this evidence, we
evaluated the possible therapeutic effect of BBs in triple-
negative breast cancer (TNBC) patients. We identified 800
postmenopausal women operated between 1997 and 2008 for
early primary TNBC. The effect of BB intake on the risk of
breast cancer (BC) recurrence and death was evaluated
through competing risk and Cox regression survival models.
At cancer diagnosis, 74 (9.3 %) women out of 800 were BBs
users. Median age was 62 years in BB users and 59 years in
non-users (P = 0.02). BB users and non-users were similarly
distributed by all tumor characteristics. The 5-year cumulative
incidence of BC-related events was 13.6 % in BB users and
27.9 % in non-users (P = 0.02). The beneficial impact of BBs
remained statistically significant at multivariable analysis
(HR, 0.52; 95 % CI 0.28–0.97), after the adjustment for age,
tumor stage, and treatment, peritumoral vascular invasion and
use of other antihypertensive drugs, antithrombotics, and
statins. Adjusted HRs for metastases and for BC deaths were
0.32 (95 % CI 0.12–0.90) and 0.42 (95 % CI 0.18–0.97),
respectively, in favor of BBs. Hypertension, other antihyper-
tensive drugs, antithrombotics, and statins did not impact
prognosis. In this series of postmenopausal TNBC patients,
BB intake was associated with a significantly decreased risk of
BC-related recurrence, metastasis, and BC death. Innovative
therapeutic strategies including BBs should be urgently
explored in cancer patients.
Keywords Beta-blockers � Breast cancer �Triple negative � Prognosis
Introduction
Beta-blocker (BB) drugs have been used for decades
worldwide, typically to treat hypertension, coronary artery
Electronic supplementary material The online version of thisarticle (doi:10.1007/s10549-013-2654-3) contains supplementarymaterial, which is available to authorized users.
E. Botteri (&) � N. Rotmensz � B. Santillo � S. Gandini
Division of Epidemiology and Biostatistics, European Institute
of Oncology, Milan, Italy
e-mail: [email protected]
E. Munzone � M. Colleoni
Division of Medical Senology, European Institute of Oncology,
Milan, Italy
C. Cipolla � A. Zanelotti
Division of Cardiology, European Institute of Oncology,
Milan, Italy
V. De Giorgi
Department of Dermatology, University of Florence, Florence,
Italy
L. Adamoli � A. Goldhirsch
Department of Medicine, European Institute of Oncology, Milan,
Italy
G. Viale
Department of Pathology and Laboratory Medicine, European
Institute of Oncology, Milan, Italy
G. Viale
University of Milan, Milan, Italy
123
Breast Cancer Res Treat (2013) 140:567–575
DOI 10.1007/s10549-013-2654-3

disease, and arrhythmias [1]. Despite the therapeutic indi-
cations, evidence from recent epidemiological studies
suggested that BB intake might potentially improve prog-
nosis in patients affected by prostate [2, 3], breast [4–7],
lung [8], and ovarian [9] cancer as well as cutaneous
melanoma [10, 11]. Moreover, BB intake was reported to
reduce overall cancer incidence [12] and specific prostate
cancer risk [13]. This observed association is supported by
data coming from preclinical in vivo and in vitro studies,
which showed how b-adrenergic receptors mediate the
effect of stress hormones norepinephrine and epinephrine
on the tumor microenvironment, and how antagonists of
Table 1 Characteristics at
baseline by beta-blocker intake
BB beta-blocker, ACEI
angiotensin-converting enzyme
inhibitor, ARB angiotensin
receptor blocker, CCB calcium
channel blocker, MAST
mastectomy, QUAD
quadrantectomya Clinical stage was used for
patients undergoing
neoadjuvant chemotherapyb Among patients not receiving
neoadjuvant chemotherapy.
Numbers might not sum up to
totals due to missing values
Variable Category No BB BB P value
No. (%) No. (%)
Total 726 (90.7) 74 (9.3)
Age Median (range) 59 (30–89) 62 (48–80) 0.02
\65 506 (69.7) 42 (56.8) 0.02
C65 220 (30.3) 32 (43.2)
BMI \25 364 (60.2) 35 (52.2) 0.15
25–30 187 (30.9) 23 (34.3)
[30 54 (8.9) 9 (13.4)
Ta 1 321 (45.5) 41 (56.2) 0.34
2 285 (40.4) 22 (30.1)
3 36 (5.1) 3 (4.1)
4 64 (9.1) 7 (9.6)
Na 0 374 (53.5) 42 (57.5) 0.43
1 206 (29.5) 21 (28.8)
2/3 119 (17.0) 10 (13.7)
Ki-67 Median (range) 42 (1–95) 38 (4–90) 0.37
B40 337 (48.6) 40 (54.8) 0.32
[40 356 (51.4) 33 (45.2)
Peritumoral vascular invasion Absent 539 (76.0) 61 (83.6) 0.14
Focal 90 (12.7) 7 (9.6)
Extensive 80 (11.3) 5 (6.9)
Neoadjuvant chemotherapy No 598 (82.4) 61 (82.4) 0.99
Yes 128 (17.6) 13 (17.6)
Type of surgery MAST 168 (23.1) 15 (20.3) 0.58
QUAD 558 (76.9) 59 (79.7)
Radiotherapy No 106 (14.6) 8 (10.8) 0.37
Yes 620 (85.4) 66 (89.2)
Adjuvant chemotherapy No 117 (16.1) 10 (13.5) 0.56
Yes 609 (83.9) 64 (86.5)
Hypertension No 533 (73.4) 1 (1.3) \0.01
Yes 193 (26.6) 73 (98.7)
ACEI No use 640 (88.2) 51 (68.9) \0.01
Use 86 (11.8) 23 (31.1)
ARB No use 686 (94.5) 63 (85.1) \0.01
Use 40 (5.5) 11 (14.9)
CCB No use 677 (93.3) 61 (82.4) \0.01
Use 49 (6.7) 13 (17.6)
Diuretic No use 654 (90.1) 49 (66.2) \0.01
Use 72 (9.9) 25 (33.8)
Antithrombotics No use 710 (97.8) 65 (87.8) \0.01
Use 16 (2.2) 9 (12.1)
Statins No use 680 (93.7) 63 (85.1) \0.01
Use 46 (6.3) 11 (14.9)
568 Breast Cancer Res Treat (2013) 140:567–575
123

b-adrenergic receptors, such as BBs, can interfere with
tumor cell proliferation and migration, as well as tumoral
angiogenesis [14–17]. The general pattern of transcrip-
tional responses induced by b-adrenergic signaling
includes upregulated expression of metastasis-associated
genes involved in inflammation, angiogenesis, tissue
invasion, and epithelial–mesenchymal transition, and
downregulated expression of genes facilitating antitumor
immune responses [16].
On the basis of all this evidence, we decided to examine
the potential benefit of BB use in the subset of women
affected by triple-negative breast cancer (TNBC), which
represents one of the most aggressive and difficult-to-treat
cancers. Should the beneficial impact of BBs on prognosis
be confirmed in this and other series of TNBC patients,
innovative therapeutic strategies involving the use of BBs
are to be urgently explored.
Patients and methods
We retrospectively analyzed data of all consecutive women
diagnosed and operated for early primary TNBC between
1997 and 2008 at the European Institute of Oncology in
Milan (n = 1,464). Patients with history of any previous
invasive cancer or with metastatic disease at diagnosis
(stage IV) were previously excluded. Given the low prev-
alence (1.1 %) of BB users in premenopausal patients, we
decided to limit the analysis to postmenopausal women
only (n = 800) in order to avoid high heterogeneity
between BB users and non-users. Patients were divided
into two groups: the BB users group, which included
patients who were using any BB at the moment of their
diagnosis of TNBC, and the BB non-users group, which
included all the other patients. The data sources were the
institutional Breast Cancer Database, which collects data
on patients’ characteristics, breast cancer (BC) features and
comorbidities such as hypertension and hypercholesterol-
emia, and the Cardiology Division Database, which col-
lects information on patients’ diseases of the circulatory
system and cardiovascular drugs. In addition to BBs, we
analyzed data on statins, antithrombotics, and other anti-
hypertensive drugs such as angiotensin-converting enzyme
inhibitors, angiotensin receptor blocker, calcium channel
blocker, and diuretics. If a patient took one single drug
containing two or more different antihypertensive agents
(e.g., angiotensin-converting enzyme inhibitor plus diure-
tic), she was considered as taking two or more different
antihypertensive drugs. Use of the data for the present
study was approved by the Institutional Review Board.
TNBC was defined as a BC with negative estrogen and
progesterone receptor expression (i.e., \1 % immunore-
active tumor cells) and without overexpression of HER2/
neu. Immunohistochemical expression of HER2/neu was
scored as follows: 0 (no staining or faint membrane
staining), 1? (faint membrane staining in[10 % of tumor
cells, incomplete membrane staining), 2? (weak to mod-
erate membrane staining in[10 % of tumor cells), and 3?
(intense circumferential membrane staining in [10 % of
tumor cells). For this analysis, we included patients with
negative estrogen and progesterone receptor tumors char-
acterized by HER2/neu scores of 0 and 1?, as well as 2?
resulting negative for gene amplification by fluorescence
in situ hybridization (FISH; Vysis PathVysion; Abbott,
Chicago, IL).
For all the patients receiving pre-surgical chemotherapy
(CT) we reported the clinical stage (T and N). When
pathological complete response was obtained, pathological
data such as ER, PgR, HER2/neu, and Ki-67 were retrieved
from the initial breast lesion biopsy. Responses to pre-
surgical CT were evaluated using the Response Evaluation
Criteria in Solid Tumors (RECIST) guidelines.
Statistical analysis
Association between categorical variables and BB use was
evaluated by the Chi square test, the Fisher exact test and
Table 2 Events and follow-up by beta-blocker intake
Event No BB BB P value
No. (%) No. (%)
At risk 726 74
First events
Locala 52 (7.2) 6 (8.1) 0.77
Regionala 28 (3.9) 1 (1.3) 0.51
Distanta,b 110 (15.2) 3 (4.1) \0.01
Contralateral breast tumor 21 (2.9) 3 (4.1) 0.48
Other non-breast primary
tumor
27 (3.7) 4 (5.4) 0.52
Death from breast cancera,b 9 (1.2) 1 (1.4) 1.00
Death from other cancer 0 (0.0) 0 (0.0) –
Death from other causes 8 (1.1) 3 (4.1) 0.07
Death from missing causes 16 (2.2) 2 (2.7) 0.68
Overall mortality
Death from breast cancerc 141 (19.4) 6 (8.1) 0.02
Death from other cancerd 8 (1.1) 4 (5.4) \0.01
Death from other causesd 9 (1.2) 3 (4.1) 0.09
Death from missing causesd 17 (2.3) 2 (2.7) 0.69
Follow-up
Months, median (Q1–Q3) 68 (43–98) 72 (52–100) 0.62
Events were used for the calculation of cumulative incidence of
(a) breast cancer related events; (b) metastases; (c) breast-related
deaths; (d) deaths from causes other than breast cancer. Association
between number of events and BB use was tested by the Chi square or
the Fisher exact test, and the corresponding P value was reported
BB beta-blocker, Q1 lower quartile, Q3 upper quartile
Breast Cancer Res Treat (2013) 140:567–575 569
123

the Chi square test for trend, as appropriate. Differences in
median age and Ki-67 were tested using the non-parametric
median two sample test. Ki-67 was also dichotomized
using the median value of 40 % as cutpoint. For the cal-
culation of cumulative incidences, only first events of
interest were considered. For the cumulative incidence of
BC-related events, BC-related recurrences, and deaths
from BC were counted as events, while contralateral
tumors, non-breast primary tumors, and deaths from other
causes were considered as competing events. For the
cumulative incidence of metastases, metastases and deaths
from BC were counted as events, while loco-regional
events, contralateral tumors, non-breast primary tumors,
and deaths from other causes were considered as compet-
ing events. For the cumulative incidence BC-related
deaths, we considered deaths from other causes as com-
peting events. For the cumulative incidence non-BC
deaths, we considered deaths from BC as competing
events. Cumulative incidences were compared across dif-
ferent subgroups by means of the Gray test. Multivariable
Cox proportional hazards models were applied to evaluate
BB intake as independent prognostic factor, adjusting the
YearsYears
Years
Cum
ulat
ive
Inci
denc
e
0.0
0.1
0.2
0.3
0.4
0.5
0 1 2 3 4 5 6 7
Gray test P-value: 0.017
HR* Beta-Blockers vs Beta-Blocker: 1.79 (95% CI 0.82-3.90; P-value 0.146)
* From multivariable analysis
At risk
BB 74 71 67 67 59 50 37 29
No BB 726 702 646 583 513 427 341 257
0.0
0.1
0.2
0.3
0.4
0.5
0 1 2 3 4 5 6 7
Gray test P-value: 0.017
HR* Beta-Blockers vs Beta-Blocker: 0.42 (95% CI 0.18-0.97; P-value 0.042)
* From multivariable analysis
At risk
BB 74 71 67 67 59 50 37 29
No BB 726 702 646 583 513 427 341 257
0.0
0.1
0.2
0.3
0.4
0.5
0 1 2 3 4 5 6 7
Gray test P-value: 0.011
HR* Beta-Blockers vs Beta-Blocker: 0.32 (95% CI 0.12-0.90; P-value 0.031)
* From multivariable analysis
At risk
BB 74 70 65 60 51 43 31 24
No BB 726 659 654 512 434 349 271 201
0.0
0.1
0.2
0.3
0.4
0.5
0 1 2 3 4 5 6 7
Beta-Blockers
Gray test P-value: 0.015
HR* Beta-Blockers vs Beta-Blocker: 0.52 (95% CI 0.28-0.97; P-value 0.041)
*From multivariable analysis
At risk
BB 74 70 65 60 51 43 31 24
No BB 726 659 654 512 434 349 271 201
No Beta-Blockers
Years
Cum
ulat
ive
Inci
denc
eC
umul
ativ
e In
cide
nce
Cum
ulat
ive
Inci
denc
e
Beta-BlockersNo Beta-Blockers
Beta-BlockersNo Beta-Blockers
Beta-BlockersNo Beta-Blockers
a b
c d
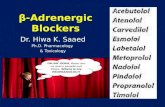
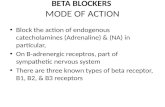
Fig. 1 a Cumulative incidence of breast cancer related events by use
of beta-blockers, b cumulative incidence of distant metastases by use
of beta-blockers, c cumulative incidence of deaths from breast cancer
by use of beta-blockers, d cumulative incidence of deaths from causes
other than breast cancer by use of beta-blockers
570 Breast Cancer Res Treat (2013) 140:567–575
123

effect of BB for all the variables that were associated in
univariate analysis with BB use or with the event of
interest. Hypertension was excluded from the multivariable
models in order to avoid multicollinearity with the use of
antihypertensive drugs. Adjusted hazard ratios (HR) with
95 % confidence intervals (CIs) were reported. All analy-
ses were carried out with SAS software (SAS Institute,
Cary, NC) and R software, version 2.12.2 (http://www.r-
project.org). Results associated with P values \0.05 were
considered statistical significant. All reported P values
were two-sided.
Results
At the time of cancer diagnosis, 74 women (9.3 %) out of
800 postmenopausal women were using BBs, while 726
(90.7 %) were not. Among the 74 users, 11 were taking
Carvedilol, 3 Sotalol, 27 Atenolol, 1 Betaxolol, 11 Biso-
prolol, 8 Metoprolol, and 13 Nebivolol. In Table 1 we
reported baseline characteristics in association with BB
use, as well as information on hypertension and use of
statins, antithrombotics and antihypertensive drugs other
than BBs. Median age was 62 years for the BB users and
59 years for the non-users (P = 0.015). BB users and non-
users were similarly distributed by body mass index, cancer
characteristics, and cancer treatments. Quadrantectomy
was performed in 617 (77.1 %) cases, 33 (5.3 %) of which
without radiotherapy. Details of adjuvant CT were as fol-
lows, respectively for BB users and non-users: 23 (31.1 %)
and 199 (27.4 %) received an anthracycline containing
regimen, 26 (35.1 %) and 283 (39.0 %) classical CMF, 15
(20.3 %) and 127 (17.5 %) another regimen, while 10
(13.5 %) and 117 (16.1 %) received no CT (P = 0.763).
As expected, the presence of hypertension and the use of
other antihypertensive drugs, antithrombotics and statins
were significantly more frequent in BBs users (P \ 0.01).
Median follow-up was 72 months (interquartile range
52–100) and 68 months (48–93) in BB users and non-users,
respectively (P = 0.62). Details on first events and
Table 3 Multivariable survival analysis
BC events Metastases BC deaths
HR (95 % CI) HR (95 % CI) HR (95 % CI)
Beta-blockers Use versus No use 0.52 (0.28–0.97) 0.32 (0.12–0.90) 0.42 (0.18–0.97)
Age 1-year increase 1.00 (0.99–1.02) 0.99 (0.97–1.02) 1.01 (0.99–1.03)
Primary tumor (T) 2 versus 1 1.37 (0.96–1.95) 1.28 (0.81–2.03) 1.26 (0.80–1.96)
3/4 versus 1 2.08 (1.11–3.91) 2.53 (1.13–5.63) 2.01 (0.95–4.23)
Positive lymph nodes 1–3 versus 0 1.20 (0.80–1.80) 1.47 (0.88–2.45) 1.77 (1.08–2.90)
[3 versus 0 2.49 (1.64–3.78) 2.33 (1.33–4.07) 2.91 (1.73–4.90)
Peritumoral vascular invasion Present versus absent 1.96 (1.41–2.73) 1.88 (1.22–2.89) 1.99 (1.35–2.94)
Antihypertensive drugs other than Beta-blockers Use versus No use 0.97 (0.69–1.38) 0.83 (0.51–1.35) 0.86 (0.56–1.32)
Antithrombotics Use versus No use 1.02 (0.46–2.28) 1.60 (0.60–4.22) 1.17 (0.45–3.05)
Statins Use versus No use 1.11 (0.66–1.88) 1.12 (0.55–2.24) 0.89 (0.43–1.85)
Response to neoadjuvant chemotherapy CR/PR versus No use 1.11 (0.65–1.90) 1.08 (0.56–2.1) 1.51 (0.81–2.83)
SD/PD versus No use 2.57 (1.49–4.45) 1.30 (0.61–2.76) 2.29 (1.21–4.34)
Loco-regional treatment QUAD versus QUART 3.29 (1.89–5.74) 3.34 (1.59–6.99) 2.99 (1.59–5.66)
MAST versus QUART 1.10 (0.75–1.61) 1.25 (0.76–2.05) 1.37 (0.87–2.14)
BC breast cancer, CR complete response after neoadjuvant chemotherapy, PR partial response after neoadjuvant chemotherapy, SD stable disease
after neoadjuvant chemotherapy, PD progressive disease after neoadjuvant chemotherapy, QUAD quadrantectomy, QUART quadrantectomy and
radiotherapy, MAST mastectomy
Cum
ulat
ive
Inci
denc
e
0.0
0.1
0.2
0.3
0.4
0.5
0 1 2 3 4 5 6 7
No hypertensionHypertension
Gray test P-value: 0.444
Hypertension 266 249 214 190 157 125 95 70
No Hypertension 534 480 415 382 328 267 207 155
YearsAtrisk
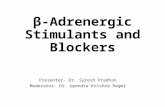
Fig. 2 Cumulative incidence of breast cancer related events by
hypertension
Breast Cancer Res Treat (2013) 140:567–575 571
123

No StatinsAny Statins
Gray test P-value: 0.923
At risk
Any Statins 57 55 49 45 38 29 24 21
No Statins 743 675 580 528 449 363 278 205
No Antithrombotics Any Antithrombotics
Gray test P-value: 0.864
At risk
Any Antithrombotics 25 21 21 16 14 10 7 3
No Antithrombotics 608 557 473 382 295 222
No Diuretics Any Diuretics
Gray test P-value: 0.629
At risk
Any Diuretics 97 94 80 68 58 48 40 29
No Diuretics 703 635 549 505 429 344 262 196
No CCB Any CCB
Gray test P-value: 0.342
At risk
Any CCB 62 58 51 44 38 24 18 16
No CCB 738 671 578 529 447 367 284 209
Years
Cum
ulat
ive
Inci
denc
e
0.0
0.1
0.2
0.3
0.4
0.5No ARBAny ARB
Gray test P-value: 0.812
At risk
Any ARB 51 49 40 36 26 21 15 9
No ARB 749 680 589 537 459 371 287 216
Years
Cum
ulat
ive
Inci
denc
e
0.0
0.1
0.2
0.3
0.4
0.5
0 1 2 3 4 5 6 70 1 2 3 4 5 6 7
No ACEIAny ACEI
Gray test P-value: 0.920
At risk
Any ACEI 109 101 89 80 66 56 48 37
No ACEI 691 628 540 493 419 336 254 188
0.0
0.1
0.2
0.3
0.4
0.5
0 1 2 3 4 5 6 7
0.0
0.1
0.2
0.3
0.4
0.5
0 1 2 3 4 5 6 7
0.0
0.1
0.2
0.3
0.4
0.5
0 1 2 3 4 5 6 7 0.0
0.1
0.2
0.3
0.4
0.5
0 1 2 3 4 5 6 7
Cum
ulat
ive
Inci
denc
e
Cum
ulat
ive
Inci
denc
eC
umul
ativ
e In
cide
nce
Cum
ulat
ive
Inci
denc
e
Years Years
YearsYears
775 708
a b
c d
e f
572 Breast Cancer Res Treat (2013) 140:567–575
123

mortality were reported in Table 2. Six (8.1 %) local
recurrences were observed in BB users and 52 (7.2 %) in
non-users (P = 0.77), while 1 (1.3 %) regional recurrence
in BB users and 28 (3.9 %) in non-users (P = 0.51). Three
(4.1 %) distant metastases were observed in BB users and
110 (15.2 %) non-users (P \ 0.01).
The 5-year cumulative incidence of BC-related events
was 13.6 % in BB users and 27.9 % in non-users
(P = 0.015; Fig. 1a). Multivariable analysis was reported
in Table 3. After adjusting for age, tumor stage, peritu-
moral vascular invasion, use of other antihypertensive
drugs, antithrombotics and statins, use of and response to
neoadjuvant chemotherapy, and loco-regional BC treat-
ment, the beneficial impact of BB use remained statistically
significant, with a HR of 0.52 (95 % CI 0.28–0.97;
P = 0.041). When analyzing the risk of distant metastases,
the HR adjusted for the same variables was 0.32 (95 % CI
0.12–0.90; P = 0.031; Fig. 1b) in favor of BBs. With
regard to mortality, 6 (8.1 %) BC-related deaths were
observed in BB users and 141 (19.4 %) in non-users, with a
corresponding adjusted HR of 0.42 (95 % CI 0.18–0.97;
P = 0.042; Fig. 1c). Causes of death other than cancer
were as follows: 2 circulatory system disease and 1
myelodysplastic syndrome in BB users; 2 circulatory sys-
tem disease, 1 pulmonary embolism, 1 head trauma, 1 old
age, 1 renal failure, and 3 causes different from BC not
better specified in BB non-users. At univariate analysis, the
risk of death from causes other than BC (other cancer,
other cause and missing cause) was higher in BB users
compared with non-users, but the difference was not sta-
tistically significant after the adjustment for age, antihy-
pertensive and antithrombotic drugs (HR: 1.79; 95 % CI
0.82–3.90; P value 0.146; Fig. 1d). Hypertension, antihy-
pertensive drugs other than BBs, antithrombotics, and
statins did not have any significant effect on the risk of BC-
related events (Figs. 2, 3).
In Supplementary Figure 1 we reported the effect of BB
use on BC-related events in various subgroups of patients.
BBs showed a protective effect in all subgroups (HR \ 1),
even if some HR estimates were not statistically significant,
possibly due to reduced numbers of events. No significant
interaction between BB use and any of the reported vari-
ables was identified. Finally, as shown in Supplementary
Table 1, in the subgroup of patients receiving neoadjuvant
CT, response to therapy was not statistically different by
BB intake.
Discussion
In this large series of postmenopausal women affected by
TNBC, we found that BB intake was associated with a
significantly decreased risk of BC recurrence and death.
Being the TNBC one of the most aggressive and difficult-
to-treat cancers, these findings might be of major clinical
relevance.
Mechanisms through which BB drugs could enhance
cancer patients’ prognosis were explained in preclinical
studies, through in vitro and in vivo models [18–22]. The
sympathetic nervous system mediates the acute stress
response by regulating levels of norepinephrine and epi-
nephrine in organ tissues and circulating blood. Those two
stress hormones interfere with the tumor microenvironment
by modulating the function of several cancer-relevant cell
types, such as epithelial, myocytes and pericytes, adipo-
cytes, fibroblasts, neural and glial cells, and most lym-
phoid, and myeloid immune cells [22]. Ligation of
b-receptors by norepinephrine and epinephrine leads to
activation of Protein kinase A (PKA) which in turn regu-
lates a wide variety of cellular processes by activating
transcription factors and downstream kinases with conse-
quent modulation of cell trafficking and motility as well as
cellular resistance to apoptosis. In a preclinical study on
BC, norepinephrine was shown to be a potent inducer of
migratory activity [21]. Also, b-adrenergic antagonists
have been found to block stress-induced enhancement of
tumor progression and metastasis, while b-adrenergic
agonists have also been found to accelerate in vivo tumor
progression and metastasis in the absence of stress [22].
Therefore, BB drugs might have a role in weakening the
pro-migratory and pro-metastatic effects induced by stress
hormones.
Our findings on BB use in TNBC patients are in
agreement with studies reporting a beneficial prognostic
role of BBs in patients with prostate [2, 3], breast [4–7],
lung [8], and ovarian [9] cancer as well as cutaneous
melanoma [10, 11]. One study reported a null association
between BB use and risk of developing colorectal cancer
[23]. A very recent large study [24] reporting data from the
Danish Breast Cancer Cooperative Group registry showed
a protective effect of BB use on BC recurrence in univar-
iate analysis and a detrimental effect in multivariable
analysis. The switch from protective to detrimental effect
was mainly due to the adjustments for use of simvastatin
and ARB in the multivariable model. That switch was not
observed in our analysis. Unfortunately, the authors did not
Fig. 3 a Cumulative incidence of breast cancer related events by use
of angiotensin-converting enzyme inhibitor, b cumulative incidence
of breast cancer related events by use of angiotensin receptor blocker,
c cumulative incidence of breast cancer related events by use of
calcium channel blocker, d cumulative incidence of breast cancer
related events by use of diuretics, e cumulative incidence of breast
cancer related events by use of antithrombotics, f cumulative
incidence of breast cancer related events by use of statins. ACEI
angiotensin-converting enzyme inhibitor, ARB angiotensin receptor
blocker, CCB calcium channel blocker
b
Breast Cancer Res Treat (2013) 140:567–575 573
123

report results for the subgroups of TNBC patients. Since
the effect of BB on BC prognosis was reported to vary
according to BC molecular subtypes [4], the stratification
according to ER/PgR status as well as HER/neu status
might have possibly led to different conclusions. Finally, of
particular interest, Melhem-Bertrandt et al. [4] showed a
significant protective effect of BB use on relapse-free
survival in a series of 377 TNCB patients, with an adjusted
HR of 0.30 in favor of BB use. That finding was obtained
from a subgroup analysis performed on patients with
TNBC treated with neoadjuvant CT. In accordance to that
finding, when we limited the analysis to TNBC patients
who underwent neoadjuvant CT, we obtained an adjusted
HR of 0.36 in favor of BB (Supplementary Fig. 1). The
authors did not find any potential beneficial effect of BB on
prognosis in estrogen receptor-positive breast cancer
patients. The observed null effect could be due to the
presence of the ER and the use of ER targeting drugs that
may modulate the response to BB.
Interestingly, we did not observe fewer loco-regional
recurrences in BB users in comparison with non-users,
while we found a protective effect of BBs on the risk of
distant metastases and breast-specific mortality. This dif-
ferential effect of BBs on different types of recurrence
could be due to the fact that stress hormone norepinephrine
was shown to be a potent inducer of migratory activity,
with no or little effect on primary tumor growth [21].
Hypothetically, this mechanism might also explain why we
did not find any significant difference between BB users
and non-users in the response to pre-surgical CT. Our
findings on response to pre-surgical CT are consistent with
those reported in the paper by Melhem-Bertrandt et al. [4].
The main strengths of our study are the large size of the
population and its homogeneity, given by the selection of
early primary TNBC diagnosed and operated in one single
institution. An additional strong point of the study was that
BB users and non-users were uniformly distributed by
tumor characteristics and cancer treatments. Also, the
inclusion of TNBC only prevented possible biases due to
interaction between BBs and hormone or anti-HER2/neu
therapies. Moreover, for the analyses of events, we used
competing risk models to take into account the different
types of recurrences as well as the different causes of
death, and these analyses allowed us to highlight the dif-
ferential effect of BBs on different types of recurrence and
the specific effect of BBs on deaths due to BC rather than
deaths due to other causes.
Despite these strengths, the present study has some clear
limitations, apart from the ones linked to the retrospective
design. First of all, we could not retrieve information on
BB use before and after the diagnosis of TNBC. Therefore,
patients that were using BBs at the time of diagnosis might
have quit the medication after BC diagnosis, possibly
switching to different antihypertensive drugs; on the other
hand, patients who were not currently using BB at TNBC
diagnosis, could have started after. Also, the association
between duration of BB use and prognosis could not be
determined. Moreover, possibly not all the patients
receiving BBs at BC diagnosis were correctly identified,
and this would likely have lead to a dilution of the risk
estimates. However, our proportion of BB users was sim-
ilar to the ones reported in other groups of postmenopausal
BC patients [4–6]. Another potential flaw is that BB users
were older than non-users. It is to say, though, that 3 years
difference in median age has no or little clinical relevance
and that all the reported analyses were adjusted for age.
In conclusion, in this series of women affected by
TNBC, BB intake was associated with a significantly
decreased risk of BC recurrence and death. On the basis of
all the extensive preclinical and clinical evidence, and
given the limited number of treatment options in TNBC
patients, we believe that innovative therapeutic strategies,
including BBs, should be urgently explored.
Conflict of interest None.
References
1. Ram CV (2010) Beta-blockers in hypertension. Am J Cardiol
106(12):1819–1825
2. Grytli HH, Fagerland MW, Fossa SD et al (2013) Association
between use of b-blockers and prostate cancer-specific survival: a
cohort study of 3561 prostate cancer patients with high-risk or
metastatic disease. Eur Urol 64(1):e11–e12
3. Grytli HH, Fagerland MW, Fossa SD et al (2013) Use of
b-blockers is associated with prostate cancer-specific survival in
prostate cancer patients on androgen deprivation therapy. Prostate
73(3):250–260
4. Melhem-Bertrandt A, Chavez-Macgregor M, Lei X et al (2011)
Beta-blocker use is associated with improved relapse-free sur-
vival in patients with triple-negative breast cancer. J Clin Oncol
29(19):2645–2652
5. Barron TI, Connolly RM, Sharp L et al (2011) Beta blockers and
breast cancer mortality: a population-based study. J Clin Oncol
29(19):2635–2644
6. Powe DG, Voss MJ, Zanker KS et al (2010) Beta-blocker drug
therapy reduces secondary cancer formation in breast cancer and
improves cancer specific survival. Oncotarget 1(7):628–638
7. Ganz PA, Habel LA, Weltzien EK et al (2011) Examining the
influence of beta blockers and ACE inhibitors on the risk for
breast cancer recurrence: results from the LACE cohort. Breast
Cancer Res Treat 129(2):549–556
8. Wang HM, Liao ZX, Komaki R et al (2013) Improved survival
outcomes with the incidental use of beta-blockers among patients
with non-small-cell lung cancer treated with definitive radiation
therapy. Ann Oncol 24(5):1312–1319
9. Diaz ES, Karlan BY, Li AJ (2012) Impact of beta blockers on
epithelial ovarian cancer survival. Gynecol Oncol 127(2):
375–378
10. De Giorgi V, Grazzini M, Gandini S et al (2011) Treatment with
b-blockers and reduced disease progression in patients with thick
melanoma. Arch Intern Med 171(8):779–781
574 Breast Cancer Res Treat (2013) 140:567–575
123

11. Lemeshow S, Sørensen HT, Phillips G et al (2011) b-Blockers
and survival among Danish patients with malignant melanoma: a
population-based cohort study. Cancer Epidemiol Biomarkers
Prev 20(10):2273–2279
12. Monami M, Filippi L, Ungar A et al (2013) Further data on beta-
blockers and cancer risk: observational study and meta-analysis
of randomized clinical trials. Curr Med Res Opin 29(4):369–378
13. Perron L, Bairati I, Harel F et al (2004) Antihypertensive drug
use and the risk of prostate cancer (Canada). Cancer Causes
Control 15(6):535–541
14. Powe DG, Entschladen F (2011) Targeted therapies: using b-
blockers to inhibit breast cancer progression. Nat Rev Clin Oncol
8(9):511–512
15. Antoni MH, Lutgendorf SK, Cole SW et al (2006) The influence
of bio-behavioural factors on tumour biology: pathways and
mechanisms. Nat Rev Cancer 6(3):240–248
16. Cole SW, Sood AK (2012) Molecular pathways: beta-adrenergic
signaling in cancer. Clin Cancer Res 18(5):1201–1206
17. Schuller HM (2010) Beta-adrenergic signaling, a novel target for
cancer therapy? Oncotarget 1(7):466–469
18. Campbell JP, Karolak MR, Ma Y et al (2012) Stimulation of host
bone marrow stromal cells by sympathetic nerves promotes breast
cancer bone metastasis in mice. PLoS Biol 10(7):e1001363
19. Benish M, Bartal I, Goldfarb Y et al (2008) Perioperative use of
beta-blockers and COX-2 inhibitors may improve immune
competence and reduce the risk of tumor metastasis. Ann Surg
Oncol 15(7):2042–2052
20. Drell TL 4th, Joseph J, Lang K et al (2003) Effects of neuro-
transmitters on the chemokinesis and chemotaxis of MDA-MB-
468 human breast carcinoma cells. Breast Cancer Res Treat
80(1):63–70
21. Sloan EK, Priceman SJ, Cox BF et al (2010) The sympathetic
nervous system induces a metastatic switch in primary breast
cancer. Cancer Res 70(18):7042–7052
22. Daly CJ, McGrath JC (2011) Previously unsuspected widespread
cellular and tissue distribution of b-adrenoceptors and its rele-
vance to drug action. Trends Pharmacol Sci 32:219–226
23. Jansen L, Below J, Chang-Claude J et al (2012) Beta blocker use
and colorectal cancer risk: population-based case–control study.
Cancer 118(16):3911–3919
24. Sørensen GV, Ganz PA, Cole SW et al (2013) Use of b-blockers,
angiotensin-converting enzyme inhibitors, angiotensin II receptor
blockers, and risk of breast cancer recurrence: a Danish nation-
wide prospective cohort study. J Clin Oncol 31(18):2265–2272
Breast Cancer Res Treat (2013) 140:567–575 575
123