The role of a new Cephalosporin with a beta …...The role of a new Cephalosporin with a...
32
The role of a new Cephalosporin with a beta-lactamase inhibitor in complicated Intra-Abdominal (cIAI) and complicated Urinary Tract Infections (cUTI) Nikolaos V. Sipsas, MD, FIDSA Associate Professor Internal Medicine – Infectious Diseases General Hospital of Athens “Laiko”, Medical School, National and kapodistrian University of Athens
Transcript of The role of a new Cephalosporin with a beta …...The role of a new Cephalosporin with a...
The role of a new Cephalosporin with a beta-lactamase inhibitor in complicated Intra-Abdominal (cIAI) and
complicated Urinary Tract Infections (cUTI)
Nikolaos V. Sipsas, MD, FIDSA Associate Professor
Internal Medicine – Infectious Diseases General Hospital of Athens “Laiko”,
Medical School, National and kapodistrian University of Athens
Circular ΕΟΦ 81867/19.11.2012 Conflict of Interest (2012-2016)
• Speakershonoraria,researchandtravelgrantsfrom:• AbbVie• Astellas• Gilead• GSK• Janssen• MSD• Pfizer
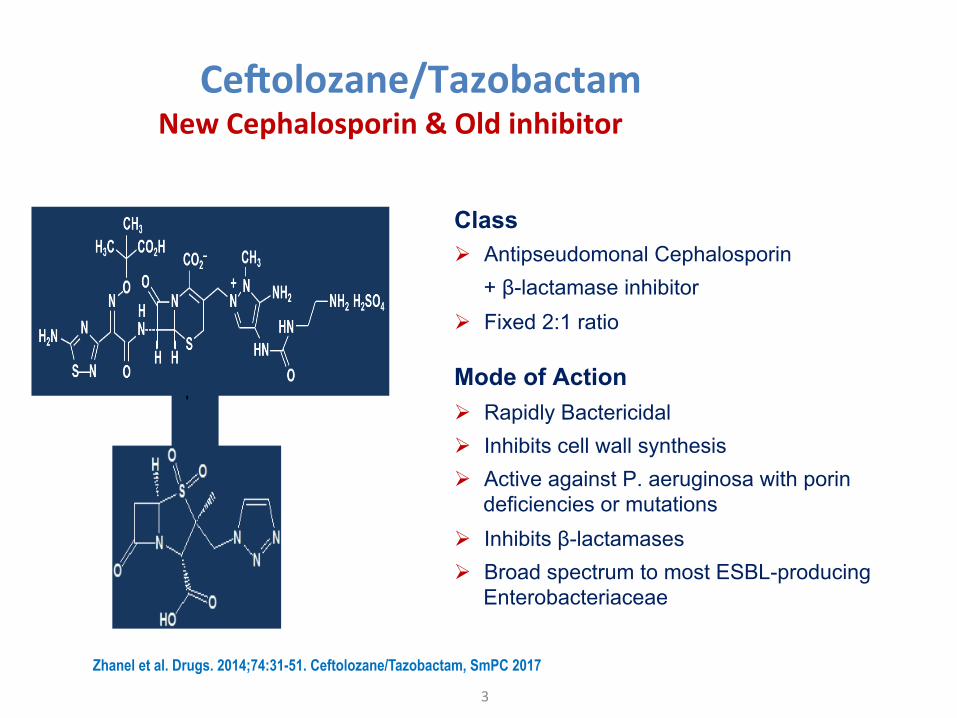
Ce#olozane/Tazobactam
3
NewCephalosporin&Oldinhibitor
Class Ø Antipseudomonal Cephalosporin + β-lactamase inhibitor Ø Fixed 2:1 ratio
Mode of Action Ø Rapidly Bactericidal Ø Inhibits cell wall synthesis Ø Active against P. aeruginosa with porin
deficiencies or mutations Ø Inhibits β-lactamases Ø Broad spectrum to most ESBL-producing
Enterobacteriaceae
Zhanel et al. Drugs. 2014;74:31-51. Ceftolozane/Tazobactam, SmPC 2017
+
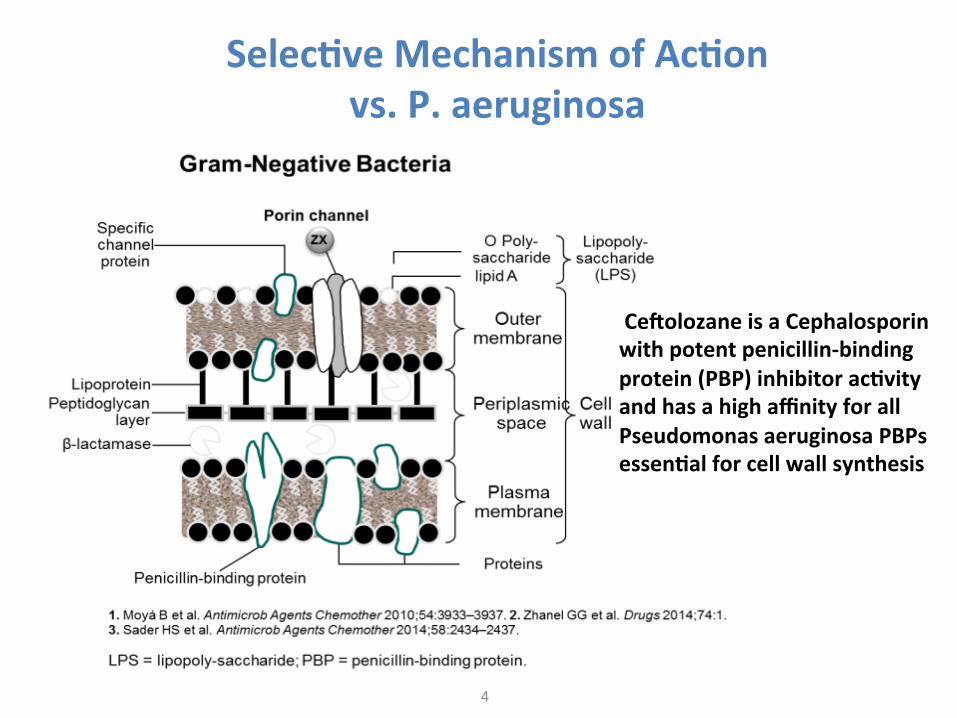
Selec;veMechanismofAc;onvs.P.aeruginosa
4
Ce#olozaneisaCephalosporinwithpotentpenicillin-bindingprotein(PBP)inhibitorac;vityandhasahighaffinityforallPseudomonasaeruginosaPBPsessen;alforcellwallsynthesis
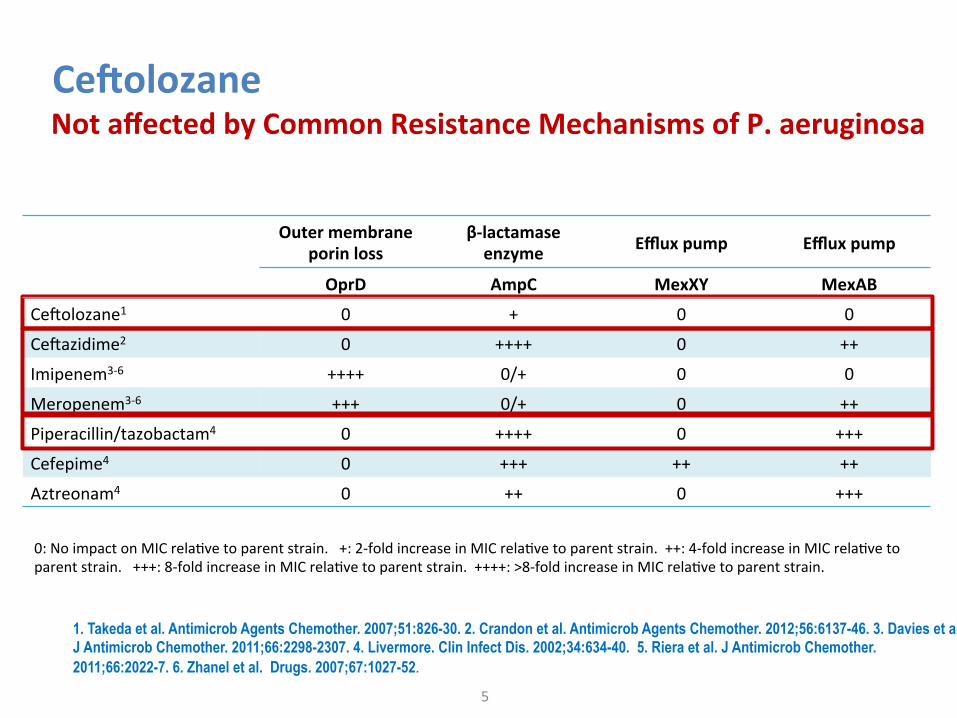
Ce#olozane
5
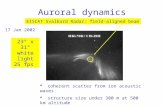
NotaffectedbyCommonResistanceMechanismsofP.aeruginosa
1. Takeda et al. Antimicrob Agents Chemother. 2007;51:826-30. 2. Crandon et al. Antimicrob Agents Chemother. 2012;56:6137-46. 3. Davies et al. J Antimicrob Chemother. 2011;66:2298-2307. 4. Livermore. Clin Infect Dis. 2002;34:634-40. 5. Riera et al. J Antimicrob Chemother. 2011;66:2022-7. 6. Zhanel et al. Drugs. 2007;67:1027-52.
Outermembrane
porinlossβ-lactamaseenzyme Effluxpump Effluxpump
OprD AmpC MexXY MexAB
CeGolozane1 0 + 0 0
CeGazidime2 0 ++++ 0 ++
Imipenem3-6 ++++ 0/+ 0 0
Meropenem3-6 +++ 0/+ 0 ++
Piperacillin/tazobactam4 0 ++++ 0 +++
Cefepime4 0 +++ ++ ++
Aztreonam4 0 ++ 0 +++
0:NoimpactonMICrelaPvetoparentstrain.+:2-foldincreaseinMICrelaPvetoparentstrain.++:4-foldincreaseinMICrelaPvetoparentstrain.+++:8-foldincreaseinMICrelaPvetoparentstrain.++++:>8-foldincreaseinMICrelaPvetoparentstrain.
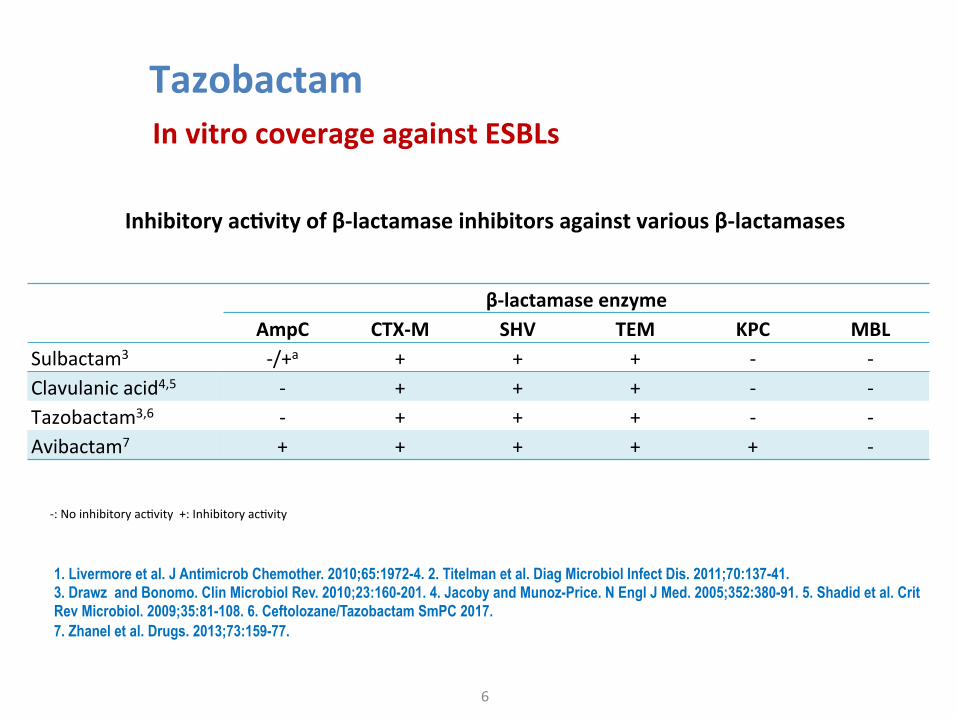
Tazobactam
6
InvitrocoverageagainstESBLs
Inhibitoryac;vityofβ-lactamaseinhibitorsagainstvariousβ-lactamases
1. Livermore et al. J Antimicrob Chemother. 2010;65:1972-4. 2. Titelman et al. Diag Microbiol Infect Dis. 2011;70:137-41. 3. Drawz and Bonomo. Clin Microbiol Rev. 2010;23:160-201. 4. Jacoby and Munoz-Price. N Engl J Med. 2005;352:380-91. 5. Shadid et al. Crit Rev Microbiol. 2009;35:81-108. 6. Ceftolozane/Tazobactam SmPC 2017. 7. Zhanel et al. Drugs. 2013;73:159-77.
-:NoinhibitoryacPvity+:InhibitoryacPvity
β-lactamaseenzyme
AmpC CTX-M SHV TEM KPC MBLSulbactam3 -/+a + + + - -Clavulanicacid4,5 - + + + - -Tazobactam3,6 - + + + - -Avibactam7 + + + + + -
Ce#olozane/Tazobactam
7
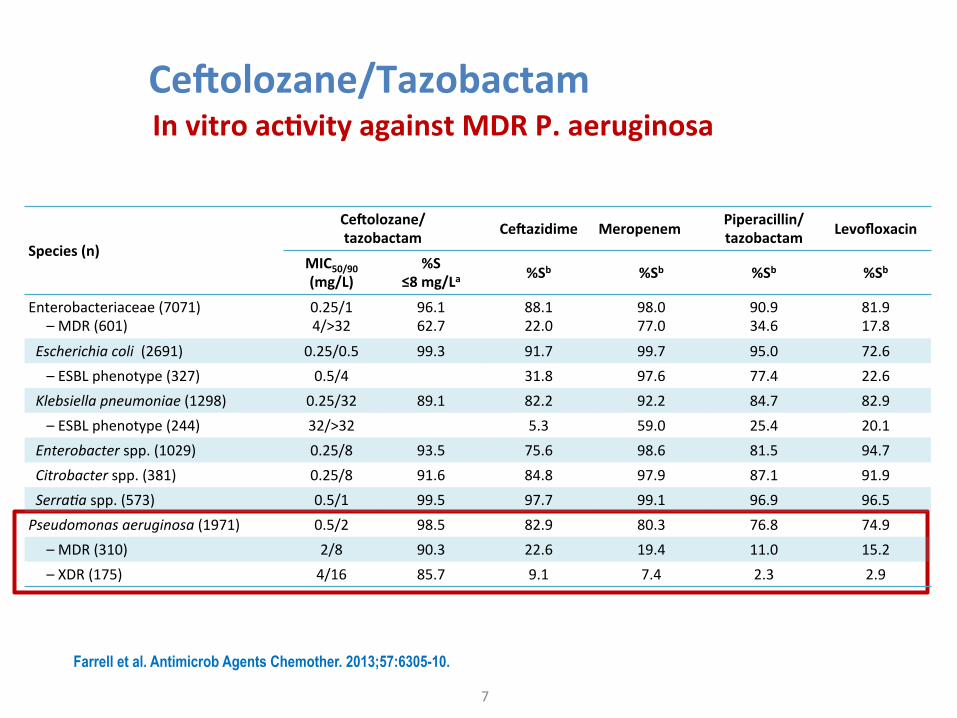
Invitroac;vityagainstMDRP.aeruginosa
Farrell et al. Antimicrob Agents Chemother. 2013;57:6305-10.
Species(n)
Ce#olozane/tazobactam Ce#azidime Meropenem Piperacillin/
tazobactam Levofloxacin
MIC50/90(mg/L)
%S≤8mg/La %Sb %Sb %Sb %Sb
Enterobacteriaceae(7071)–MDR(601)
0.25/14/>32
96.162.7
88.122.0
98.077.0
90.934.6
81.917.8
Escherichiacoli(2691) 0.25/0.5 99.3 91.7 99.7 95.0 72.6–ESBLphenotype(327) 0.5/4 31.8 97.6 77.4 22.6Klebsiellapneumoniae(1298) 0.25/32 89.1 82.2 92.2 84.7 82.9–ESBLphenotype(244) 32/>32 5.3 59.0 25.4 20.1Enterobacterspp.(1029) 0.25/8 93.5 75.6 98.6 81.5 94.7Citrobacterspp.(381) 0.25/8 91.6 84.8 97.9 87.1 91.9Serra5aspp.(573) 0.5/1 99.5 97.7 99.1 96.9 96.5Pseudomonasaeruginosa(1971) 0.5/2 98.5 82.9 80.3 76.8 74.9–MDR(310) 2/8 90.3 22.6 19.4 11.0 15.2–XDR(175) 4/16 85.7 9.1 7.4 2.3 2.9
Ce#olozane/Tazobactamvs.Pip/Tazo
8
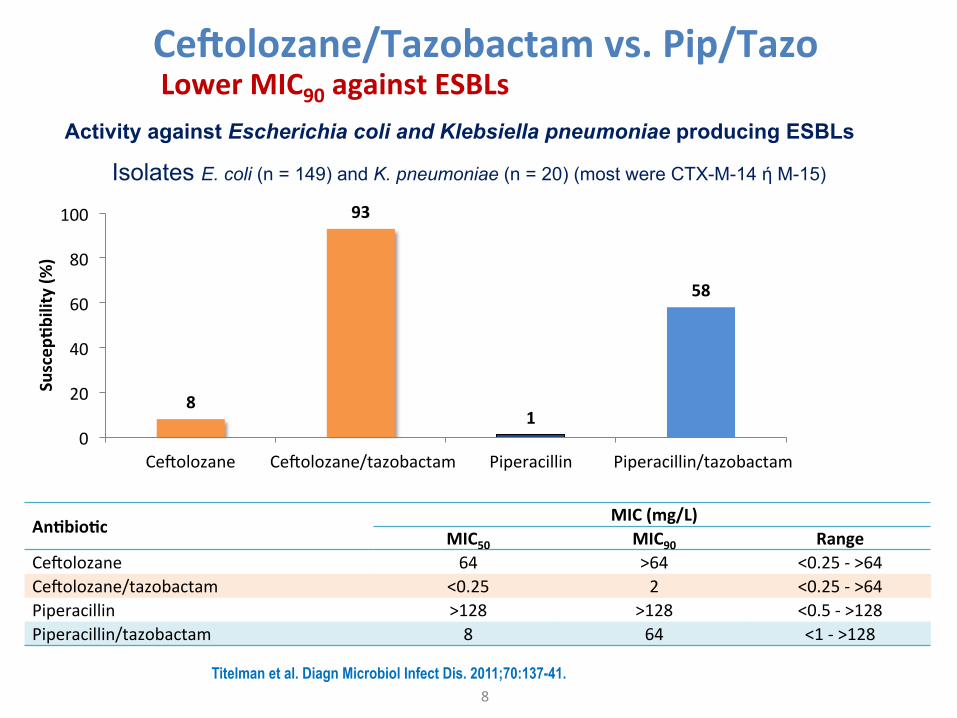
LowerMIC90againstESBLsActivity against Escherichia coli and Klebsiella pneumoniae producing ESBLs
Isolates E. coli (n = 149) and K. pneumoniae (n = 20) (most were CTX-M-14 ή M-15)
Titelman et al. Diagn Microbiol Infect Dis. 2011;70:137-41.
8
93
1
58
0
20
40
60
80
100
CeGolozane CeGolozane/tazobactam Piperacillin Piperacillin/tazobactam
Suscep
;bility(%
)
An;bio;c MIC(mg/L) MIC50 MIC90 Range
CeGolozane 64 >64 <0.25->64 CeGolozane/tazobactam <0.25 2 <0.25->64 Piperacillin >128 >128 <0.5->128 Piperacillin/tazobactam 8 64 <1->128
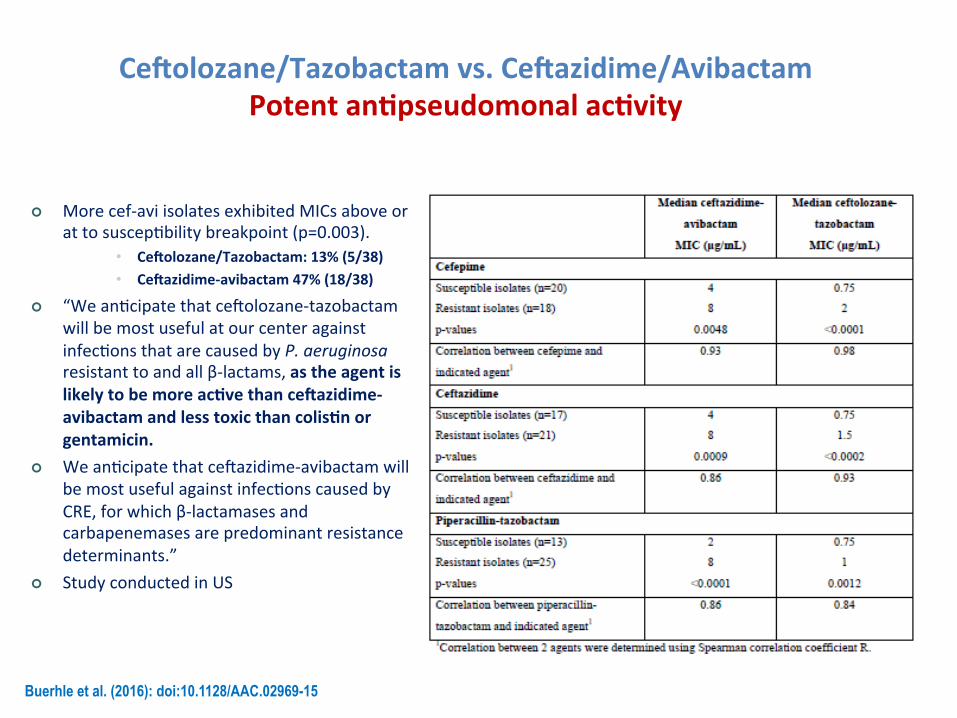
Ce#olozane/Tazobactamvs.Ce#azidime/AvibactamPotentan;pseudomonalac;vity
Buerhle et al. (2016): doi:10.1128/AAC.02969-15
¢ Morecef-aviisolatesexhibitedMICsaboveorattosuscepPbilitybreakpoint(p=0.003).
• Ce#olozane/Tazobactam:13%(5/38)• Ce#azidime-avibactam47%(18/38)
¢ “WeanPcipatethatceGolozane-tazobactamwillbemostusefulatourcenteragainstinfecPonsthatarecausedbyP.aeruginosaresistanttoandallβ-lactams,astheagentislikelytobemoreac;vethance#azidime-avibactamandlesstoxicthancolis;norgentamicin.
¢ WeanPcipatethatceGazidime-avibactamwillbemostusefulagainstinfecPonscausedbyCRE,forwhichβ-lactamasesandcarbapenemasesarepredominantresistancedeterminants.”
¢ StudyconductedinUS
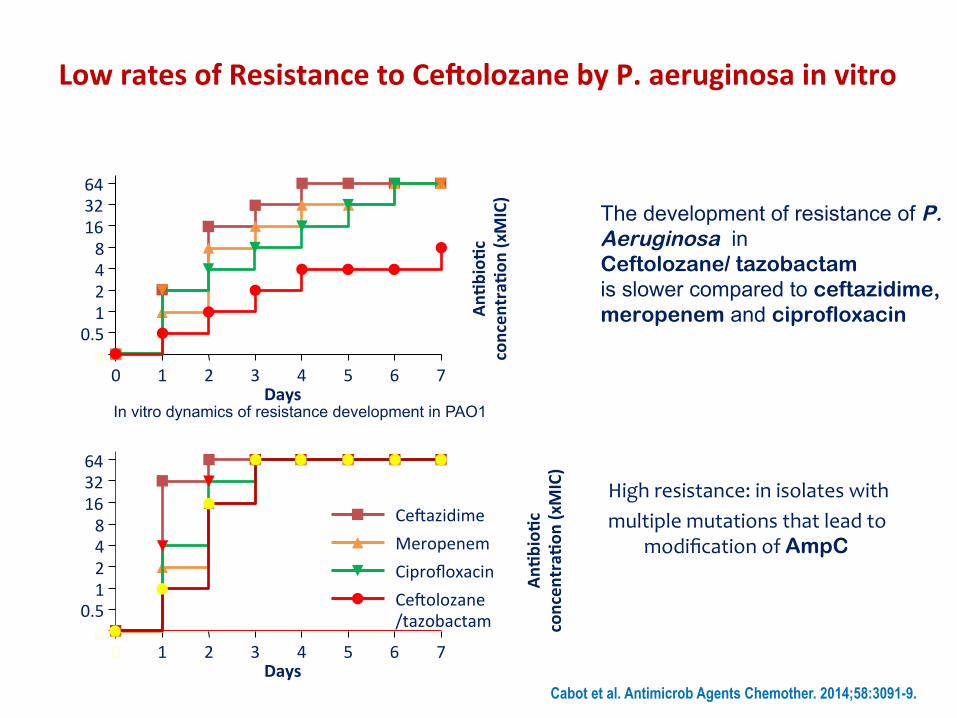
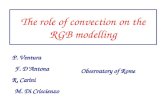
LowratesofResistancetoCe#olozanebyP.aeruginosainvitro
Highresistance:inisolateswithmultiplemutationsthatleadto
modificationofAmpC
Cabot et al. Antimicrob Agents Chemother. 2014;58:3091-9.
In vitro dynamics of resistance development in PAO1 In vitro dynamics of resistance development in PAOMS
0 1 2 3 40
64
Days
An;b
io;c
concen
tra;
on(xMIC)32
168421
0.55 6 7
CeGazidimeMeropenemCiprofloxacinCeGolozane/tazobactam
0 1 2 3 40
64
Days
An;b
io;c
concen
tra;
on(xMIC)
32168421
0.55 6 7
The development of resistance of P. Aeruginosa in Ceftolozane/ tazobactam is slower compared to ceftazidime, meropenem and ciprofloxacin
11
Ceftolozane/tazobactam dose (mg)
8
4
0
0 250 125
-4
500 250
750 375
1000 500
1250 625
1500 750
Δ L
og10
CFU
/mL
of th
e dr
ug-r
esis
tant
su
bpop
ulat
ion
at 1
0 da
ys
ESBL-producingEscherichiacoli1
Ceftolozane dose (mg)
Pseudomonasaeruginosa2
0 -1 -2
-4 -5
-3
0
5 4
2 1
3
62.5 31.25
125 62.5
250 125
500 250
750 375
1000 500
2000 1000
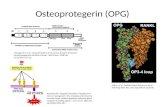
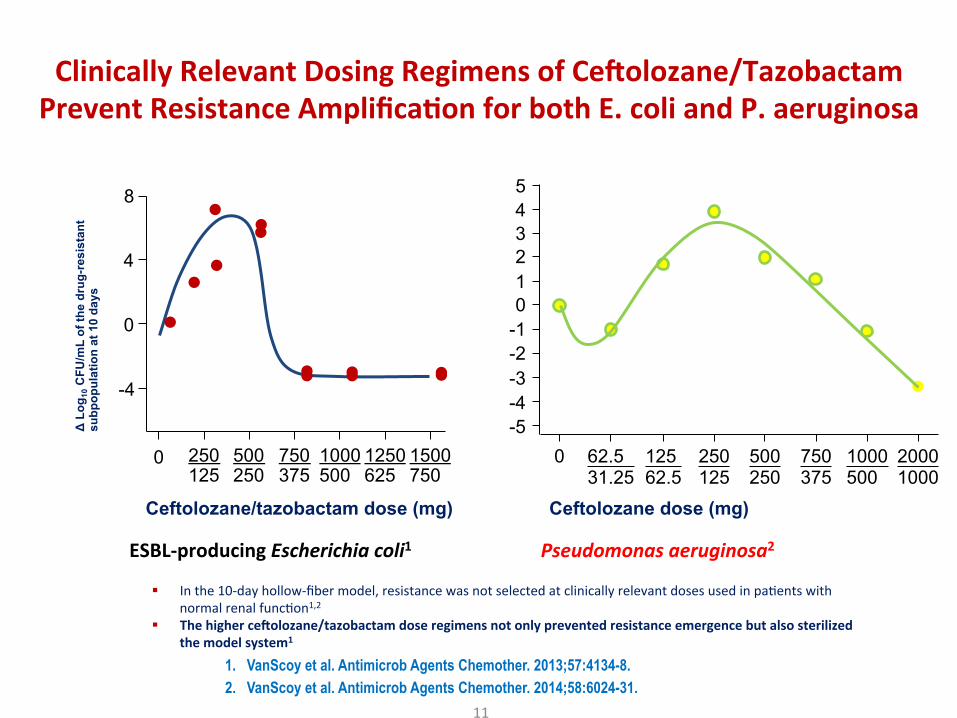
§ Inthe10-dayhollow-fibermodel,resistancewasnotselectedatclinicallyrelevantdosesusedinpaPentswithnormalrenalfuncPon1,2
§ Thehigherce#olozane/tazobactamdoseregimensnotonlypreventedresistanceemergencebutalsosterilizedthemodelsystem1
1. VanScoy et al. Antimicrob Agents Chemother. 2013;57:4134-8. 2. VanScoy et al. Antimicrob Agents Chemother. 2014;58:6024-31.
ClinicallyRelevantDosingRegimensofCe#olozane/TazobactamPreventResistanceAmplifica;onforbothE.coliandP.aeruginosa
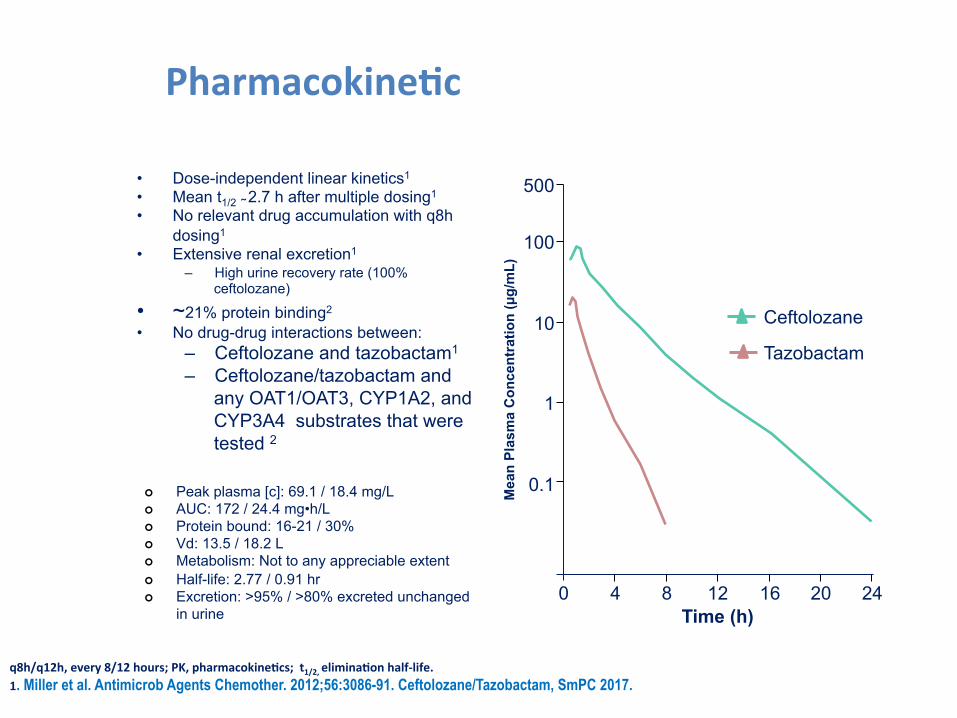
Pharmacokine;c
• Dose-independent linear kinetics1
• Mean t1/2 ̴ 2.7 h after multiple dosing1
• No relevant drug accumulation with q8h dosing1
• Extensive renal excretion1
– High urine recovery rate (100% ceftolozane)
• ~21% protein binding2
• No drug-drug interactions between: – Ceftolozane and tazobactam1
– Ceftolozane/tazobactam and any OAT1/OAT3, CYP1A2, and CYP3A4 substrates that were tested 2
Ceftolozane
Tazobactam
q8h/q12h,every8/12hours;PK,pharmacokine;cs;t1/2,elimina;onhalf-life.1. Miller et al. Antimicrob Agents Chemother. 2012;56:3086-91. Ceftolozane/Tazobactam, SmPC 2017.
Semilogconcentra;on-;meprofilea#ersingle-doseadministra;onof1.5gce#olozane/tazobactam1
0 4 8 12 16 20 24 Time (h)
0.1
1
10
100
500
Mea
n Pl
asm
a C
once
ntra
tion
(µg/
mL)
0.01
¢ Peak plasma [c]: 69.1 / 18.4 mg/L ¢ AUC: 172 / 24.4 mg•h/L ¢ Protein bound: 16-21 / 30% ¢ Vd: 13.5 / 18.2 L ¢ Metabolism: Not to any appreciable extent ¢ Half-life: 2.77 / 0.91 hr ¢ Excretion: >95% / >80% excreted unchanged
in urine
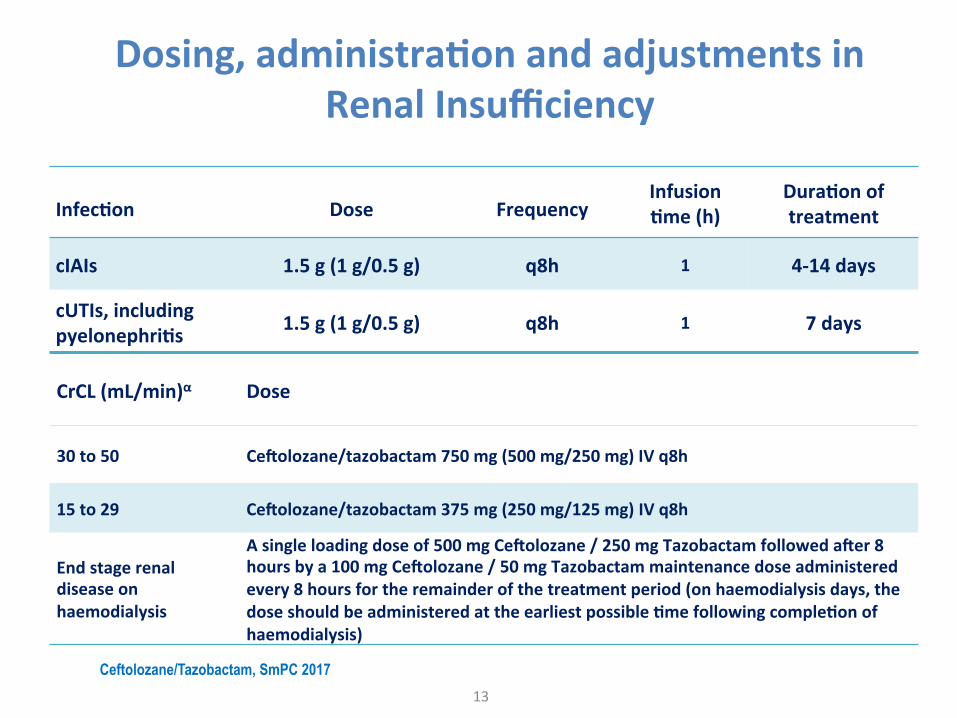
Dosing,administra;onandadjustmentsinRenalInsufficiency
13
Ceftolozane/Tazobactam, SmPC 2017
Infec;on Dose FrequencyInfusion;me(h)
Dura;onoftreatment
cIAIs 1.5g(1g/0.5g) q8h 1 4-14days
cUTIs,includingpyelonephri;s 1.5g(1g/0.5g) q8h 1 7days
CrCL(mL/min)α Dose
30to50 Ce#olozane/tazobactam750mg(500mg/250mg)IVq8h
15to29 Ce#olozane/tazobactam375mg(250mg/125mg)IVq8h
Endstagerenaldiseaseonhaemodialysis
Asingleloadingdoseof500mgCe#olozane/250mgTazobactamfolloweda#er8hoursbya100mgCe#olozane/50mgTazobactammaintenancedoseadministeredevery8hoursfortheremainderofthetreatmentperiod(onhaemodialysisdays,thedoseshouldbeadministeredattheearliestpossible;mefollowingcomple;onofhaemodialysis)
Registra;onTrials
14
ASPECTcIAI&cUTI
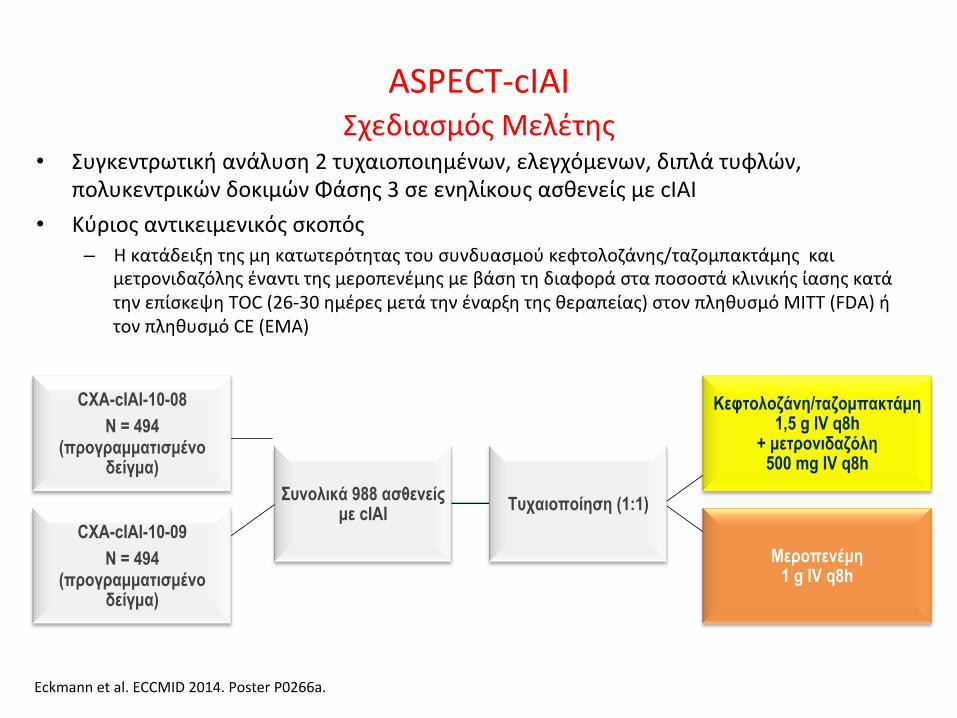
ASPECT-cIAIΣχεδιασμόςΜελέτης
• Συγκεντρωτικήανάλυση2τυχαιοποιημένων,ελεγχόμενων,διπλάτυφλών,πολυκεντρικώνδοκιμώνΦάσης3σεενηλίκουςασθενείςμεcIAI
• Κύριοςαντικειμενικόςσκοπός– Ηκατάδειξητηςμηκατωτερότηταςτουσυνδυασμούκεφτολοζάνης/ταζομπακτάμηςκαι
μετρονιδαζόληςέναντιτηςμεροπενέμηςμεβάσητηδιαφοράσταποσοστάκλινικήςίασηςκατάτηνεπίσκεψηTOC(26-30ημέρεςμετάτηνέναρξητηςθεραπείας)στονπληθυσμόMITT(FDA)ήτονπληθυσμόCE(EMA)
Eckmannetal.ECCMID2014.PosterP0266a.
Κεφτολοζάνη/ταζοµπακτάµη1,5 g IV q8h
+ µετρονιδαζόλη 500 mg IV q8h
Μεροπενέµη 1 g IV q8h
Συνολικά 988 ασθενείς µε cIAI Τυχαιοποίηση (1:1)
Διάρκειατηςθεραπείας:4-14ημέρεςενδοφλέβιουφαρμάκουτηςμελέτης(χωρίςαλλαγήσεαπότουστόματοςθεραπεία)
CXA-cIAI-10-08 N = 494
(προγραµµατισµένο δείγµα)
CXA-cIAI-10-09 N = 494
(προγραµµατισµένο δείγµα)
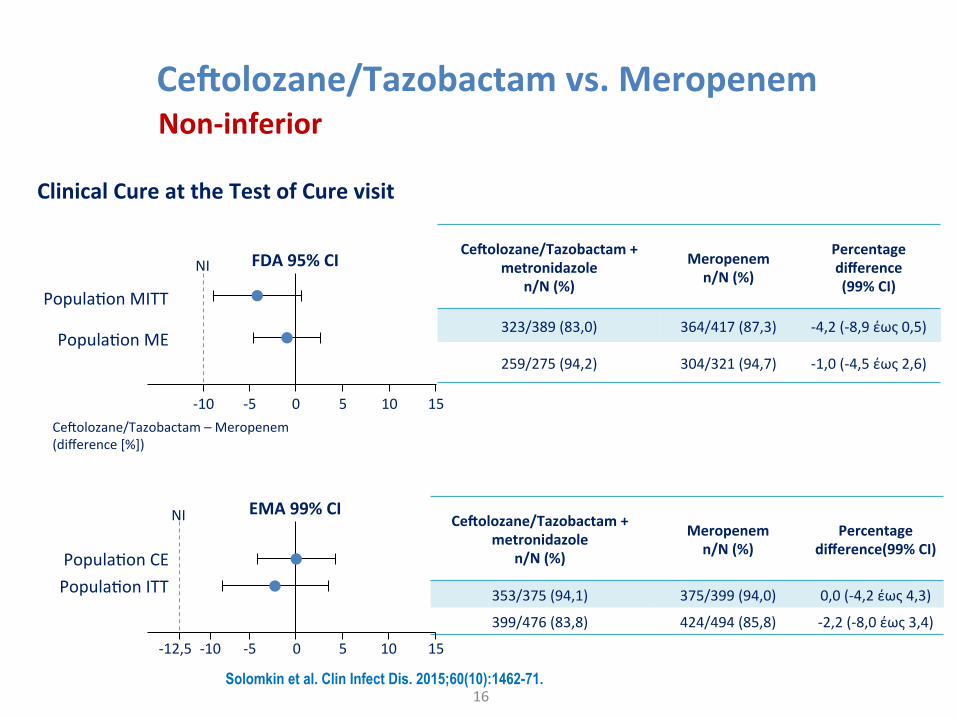
Ce#olozane/Tazobactamvs.Meropenem
16
Non-inferior
Ce#olozane/Tazobactam+metronidazole
n/N(%)
Meropenemn/N(%)
Percentagedifference(99%CI)
323/389(83,0) 364/417(87,3) -4,2(-8,9έως0,5)
259/275(94,2) 304/321(94,7) -1,0(-4,5έως2,6)
Ce#olozane/Tazobactam+metronidazole
n/N(%)
Meropenemn/N(%)
Percentagedifference(99%CI)
353/375(94,1) 375/399(94,0) 0,0(-4,2έως4,3)
399/476(83,8) 424/494(85,8) -2,2(-8,0έως3,4)
FDA95%CI
-10 -5 5 10 150
PopulaPonME
PopulaPonMITT
CeGolozane/Tazobactam–Meropenem (difference[%])
NI
EMA99%CI
-12,5 -5 5 15
PopulaPonCEPopulaPonITT
0
NI
-10 10
ClinicalCureattheTestofCurevisit
Solomkin et al. Clin Infect Dis. 2015;60(10):1462-71.
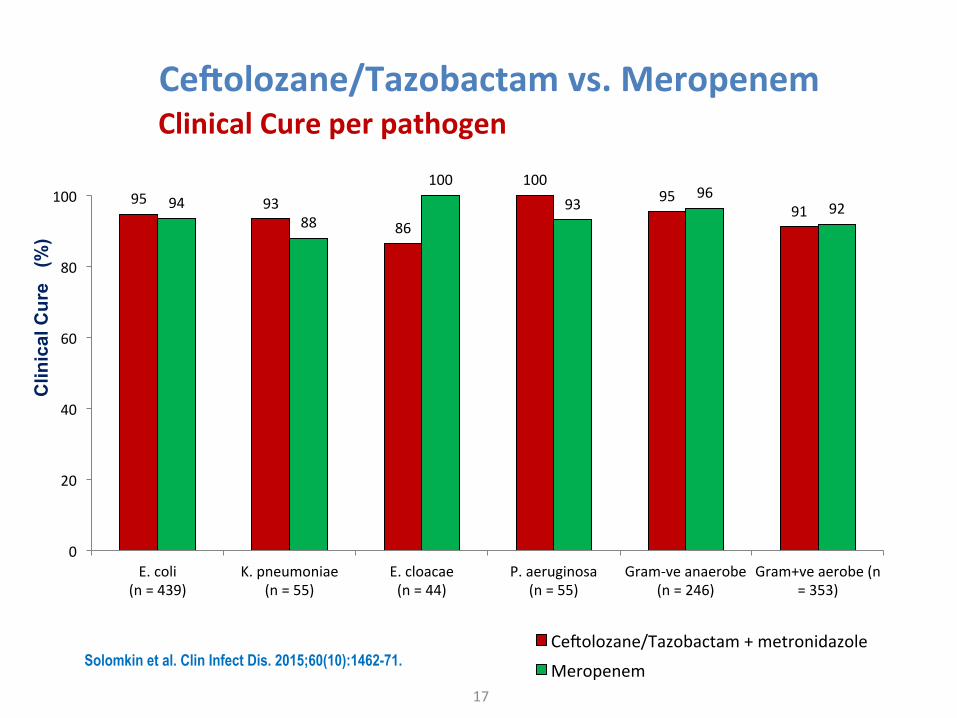
Ce#olozane/Tazobactamvs.Meropenem
17
ClinicalCureperpathogen
95 9386
10095
919488
10093
9692
0
20
40
60
80
100
E.coli(n=439)
K.pneumoniae(n=55)
E.cloacae(n=44)
P.aeruginosa(n=55)
Gram-veanaerobe(n=246)
Gram+veaerobe(n=353)
CeGolozane/Tazobactam+metronidazole
Meropenem
Clin
ical
Cur
e (
%)
Solomkin et al. Clin Infect Dis. 2015;60(10):1462-71.
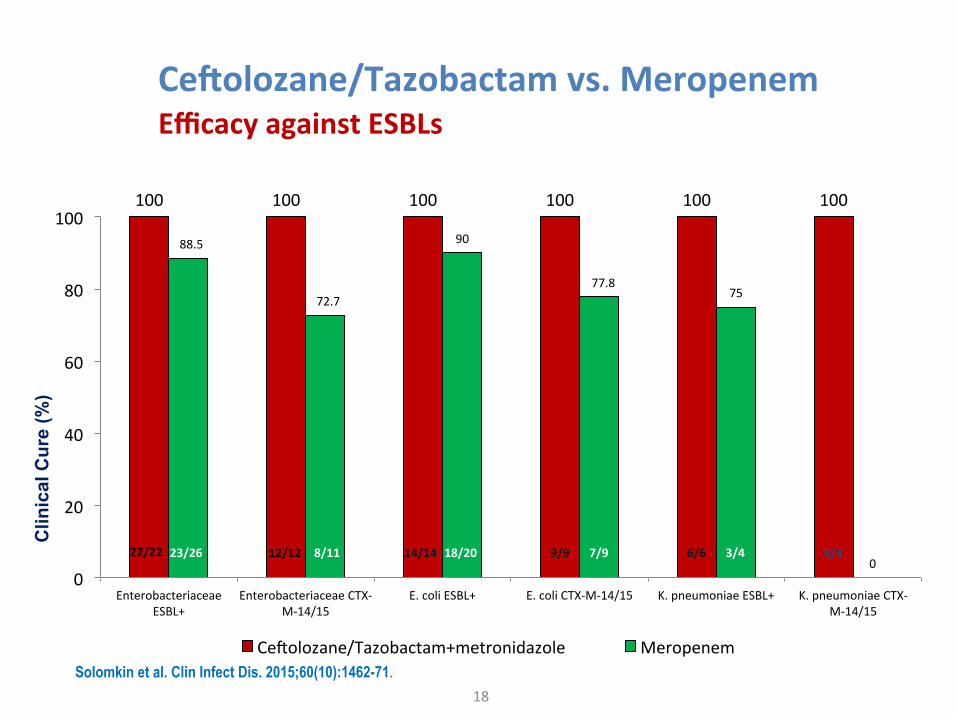
Ce#olozane/Tazobactamvs.Meropenem
18
EfficacyagainstESBLs
100 100 100 100 100 100
88.5
72.7
90
77.875
00
20
40
60
80
100
EnterobacteriaceaeESBL+
EnterobacteriaceaeCTX-M-14/15
E.coliESBL+ E.coliCTX-M-14/15 K.pneumoniaeESBL+ K.pneumoniaeCTX-M-14/15
CeGolozane/Tazobactam+metronidazole Meropenem
4/422/22 23/26 12/12 14/148/11 18/20 9/9 7/9 6/6 3/4
Clin
ical
Cur
e (%
)
Solomkin et al. Clin Infect Dis. 2015;60(10):1462-71.
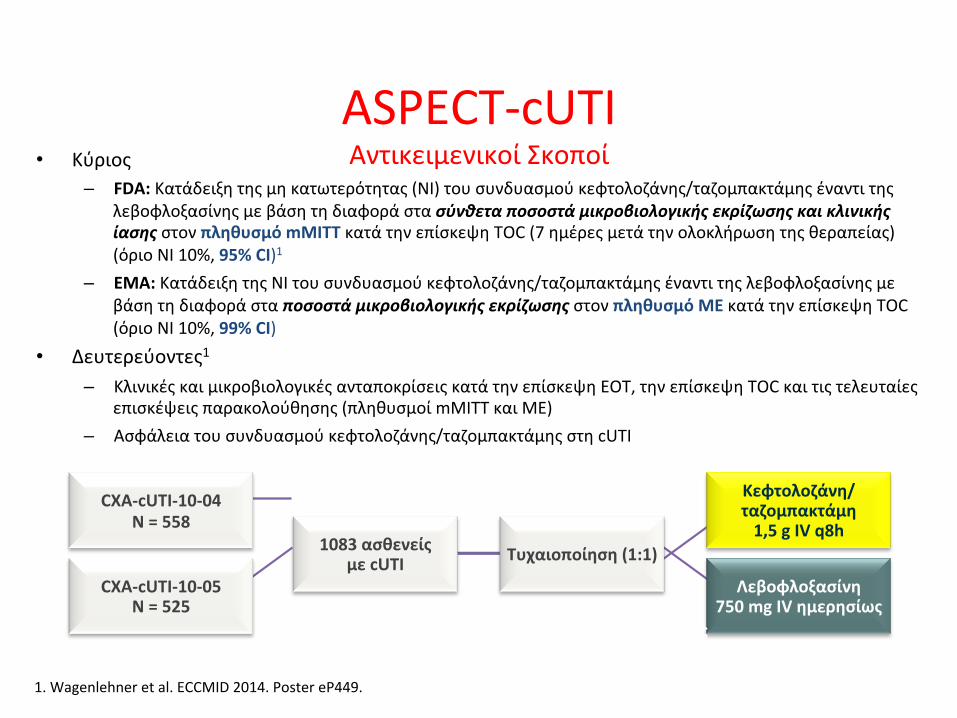
ASPECT-cUTIΑντικειμενικοίΣκοποί• Κύριος
– FDA:Κατάδειξητηςμηκατωτερότητας(NI)τουσυνδυασμούκεφτολοζάνης/ταζομπακτάμηςέναντιτηςλεβοφλοξασίνηςμεβάσητηδιαφοράστασύνθεταποσοστάμικροβιολογικήςεκρίζωσηςκαικλινικήςίασηςστονπληθυσμόmMITTκατάτηνεπίσκεψηTOC(7ημέρεςμετάτηνολοκλήρωσητηςθεραπείας)(όριοNI10%,95%CI)1
– EMA:ΚατάδειξητηςNIτουσυνδυασμούκεφτολοζάνης/ταζομπακτάμηςέναντιτηςλεβοφλοξασίνηςμεβάσητηδιαφοράσταποσοστάμικροβιολογικήςεκρίζωσηςστονπληθυσμόMEκατάτηνεπίσκεψηTOC(όριοNI10%,99%CI)
• Δευτερεύοντες1– ΚλινικέςκαιμικροβιολογικέςανταποκρίσειςκατάτηνεπίσκεψηEOT,τηνεπίσκεψηTOCκαιτιςτελευταίες
επισκέψειςπαρακολούθησης(πληθυσμοίmMITTκαιME)– Ασφάλειατουσυνδυασμούκεφτολοζάνης/ταζομπακτάμηςστηcUTI
1.Wagenlehneretal.ECCMID2014.PostereP449.
Κεφτολοζάνη/ταζομπακτάμη1,5gIVq8h
Λεβοφλοξασίνη750mgIVημερησίως
1083ασθενείςμεcUTI Τυχαιοποίηση(1:1)
CXA-cUTI-10-04N=558
CXA-cUTI-10-05N=525 Διάρκειατηςθεραπείας:
7ημέρεςενδοφλέβιουφαρμάκουτηςμελέτης(χωρίςαλλαγήσεαπότουστόματοςθεραπεία)
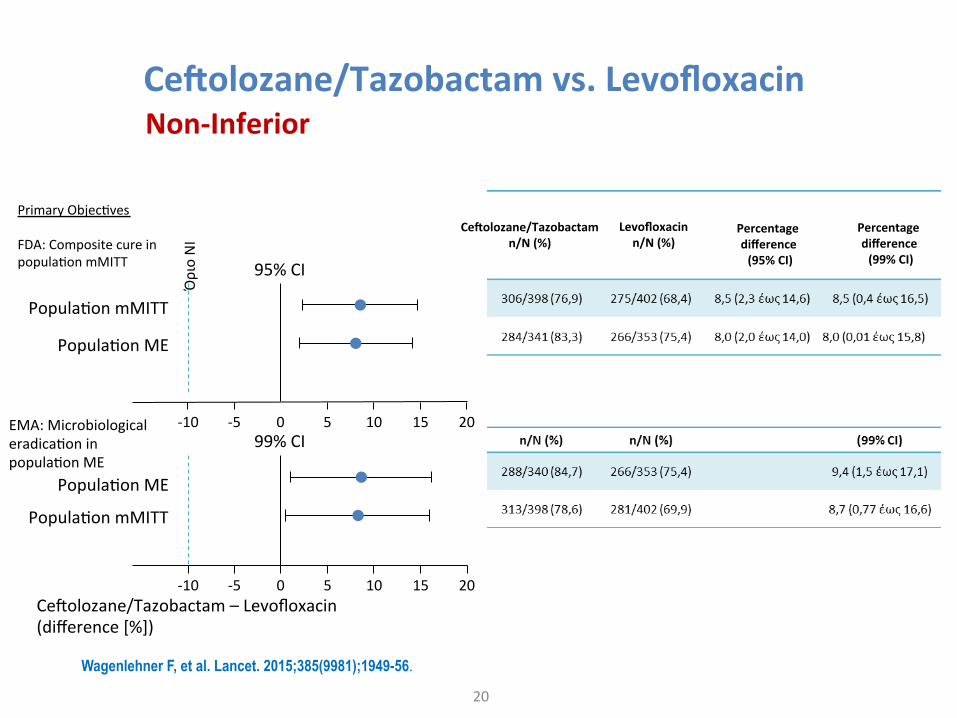
Ce#olozane/Tazobactamvs.Levofloxacin
20
Non-Inferior
ΌριοΝΙ
95%CI
PopulaPonME
PopulaPonmMITT
99%CI
CeGolozane/Tazobactam–Levofloxacin(difference[%])
-10 -5 5 10 150
PopulaPonmMITT
PopulaPonME
20
-10 -5 5 10 150 20
PrimaryObjecPvesFDA:CompositecureinpopulaPonmMITT
EMA:MicrobiologicaleradicaPoninpopulaPonME
Wagenlehner F, et al. Lancet. 2015;385(9981);1949-56.
Percentagedifference(99%CI)
Percentagedifference(95%CI)
Levofloxacinn/N(%)
Ce#olozane/Tazobactamn/N(%)
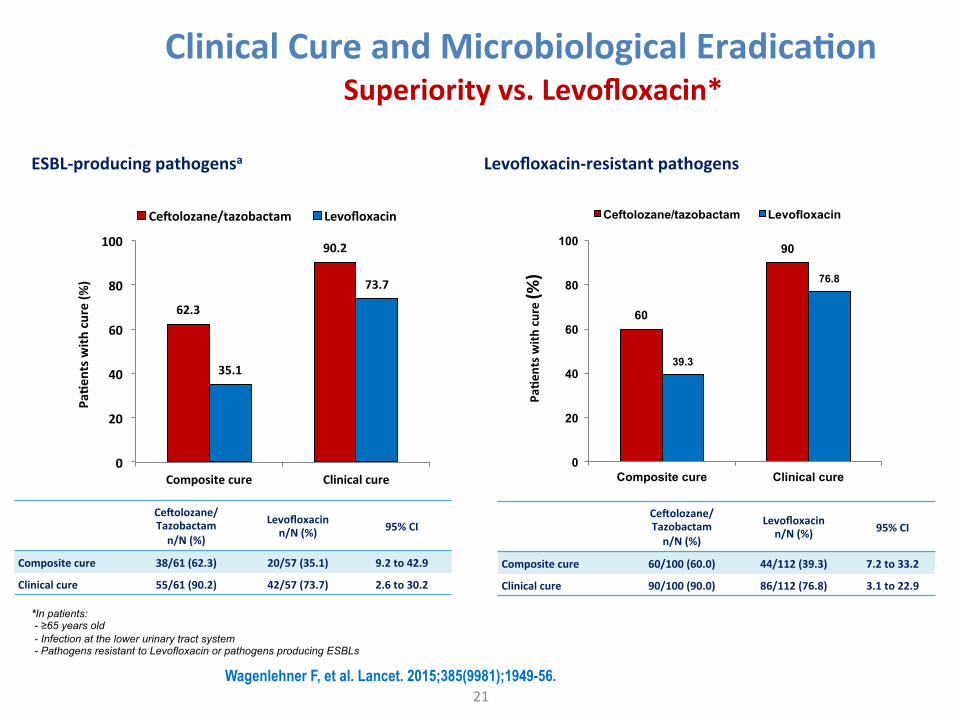
ClinicalCureandMicrobiologicalEradica;on
21
Superiorityvs.Levofloxacin*
Ce#olozane/Tazobactamn/N(%)
Levofloxacinn/N(%) 95%CI
Compositecure 38/61(62.3) 20/57(35.1) 9.2to42.9
Clinicalcure 55/61(90.2) 42/57(73.7) 2.6to30.2
62.3
90.2
35.1
73.7
0
20
40
60
80
100
Compositecure Clinicalcure
Ce#olozane/tazobactam Levofloxacin
Pa;e
ntsw
ithcure(%
)
60
90
39.3
76.8
0
20
40
60
80
100
Composite cure Clinical cure
Ceftolozane/tazobactam Levofloxacin
Pa;e
ntsw
ithcure(%
)
Levofloxacin-resistantpathogensESBL-producingpathogensa
Ce#olozane/Tazobactamn/N(%)
Levofloxacinn/N(%) 95%CI
Compositecure 60/100(60.0) 44/112(39.3) 7.2to33.2
Clinicalcure 90/100(90.0) 86/112(76.8) 3.1to22.9
*In patients: - ≥65 years old - Infection at the lower urinary tract system - Pathogens resistant to Levofloxacin or pathogens producing ESBLs
Wagenlehner F, et al. Lancet. 2015;385(9981);1949-56.
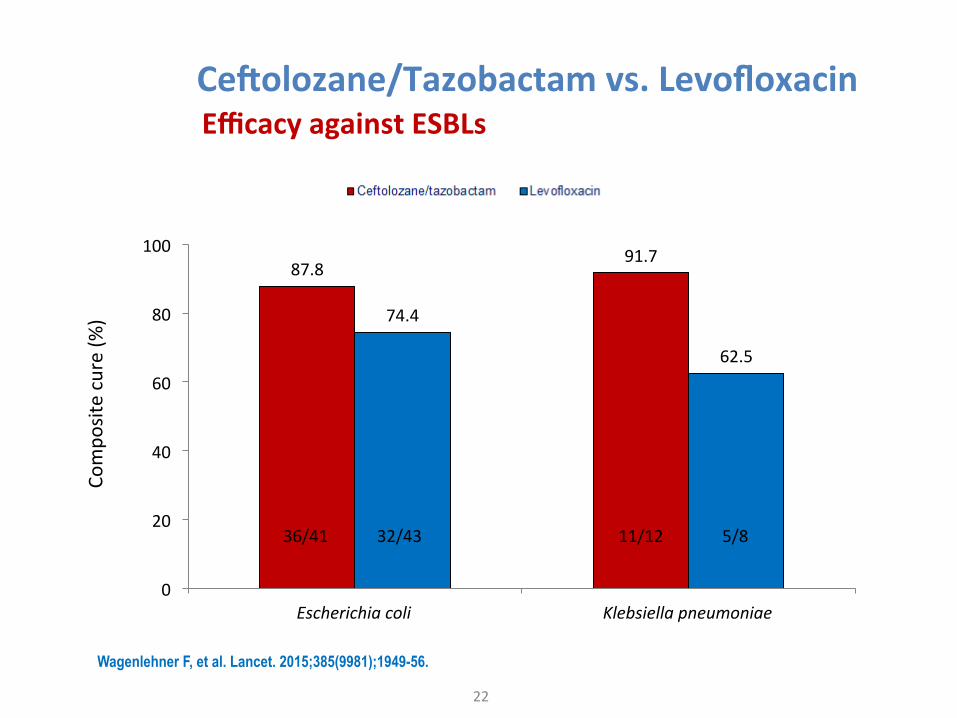
Ce#olozane/Tazobactamvs.Levofloxacin
22
EfficacyagainstESBLs
87.891.7
74.4
62.5
0
20
40
60
80
100
Escherichiacoli Klebsiellapneumoniae
Compo
sitecure(%
)
11/12 5/836/41 32/43
Wagenlehner F, et al. Lancet. 2015;385(9981);1949-56.
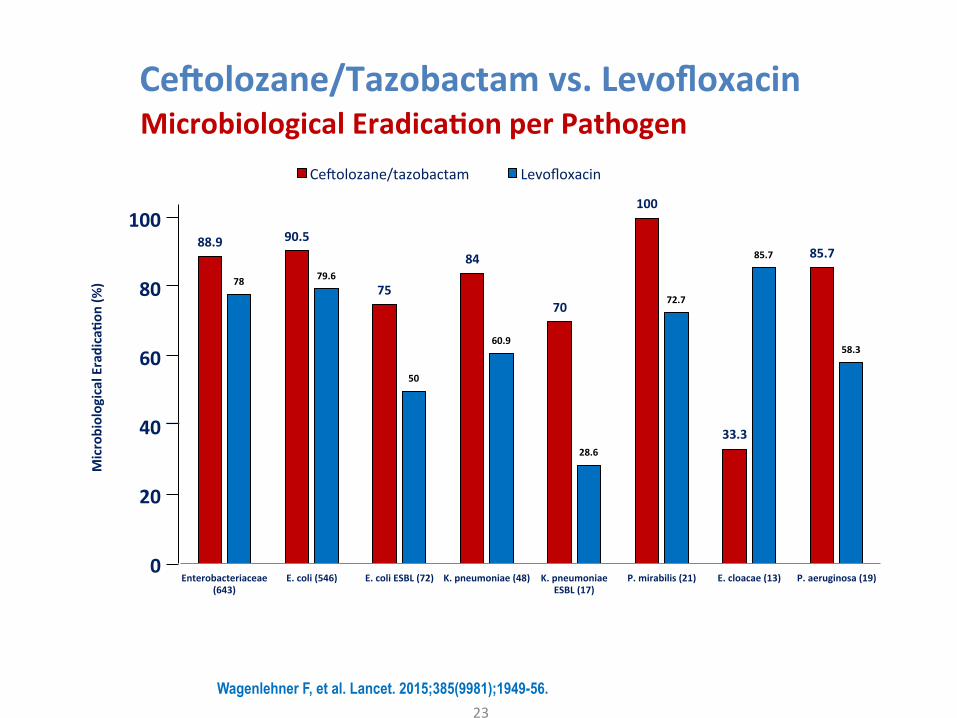
Ce#olozane/Tazobactamvs.Levofloxacin
23
MicrobiologicalEradica;onperPathogen
88.9 90.5
75
84
70
100
33.3
85.7
78 79.6
50
60.9
28.6
72.7
85.7
58.3
0
20
40
60
80
100
Enterobacteriaceae(643)
E.coli(546) E.coliESBL(72) K.pneumoniae(48) K.pneumoniaeESBL(17)
P.mirabilis(21) E.cloacae(13) P.aeruginosa(19)
MicrobiologicalEradica;o
n(%
)
Key Gram-negative PathogensCeGolozane/tazobactam Levofloxacin
Wagenlehner F, et al. Lancet. 2015;385(9981);1949-56.
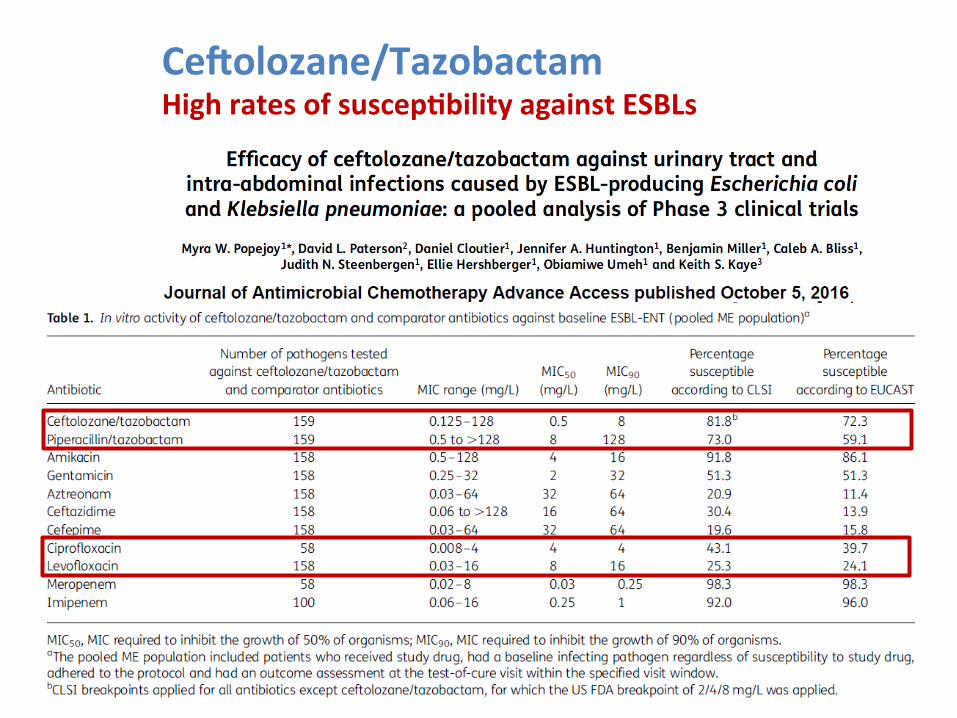
Ce#olozane/TazobactamHighratesofsuscep;bilityagainstESBLs
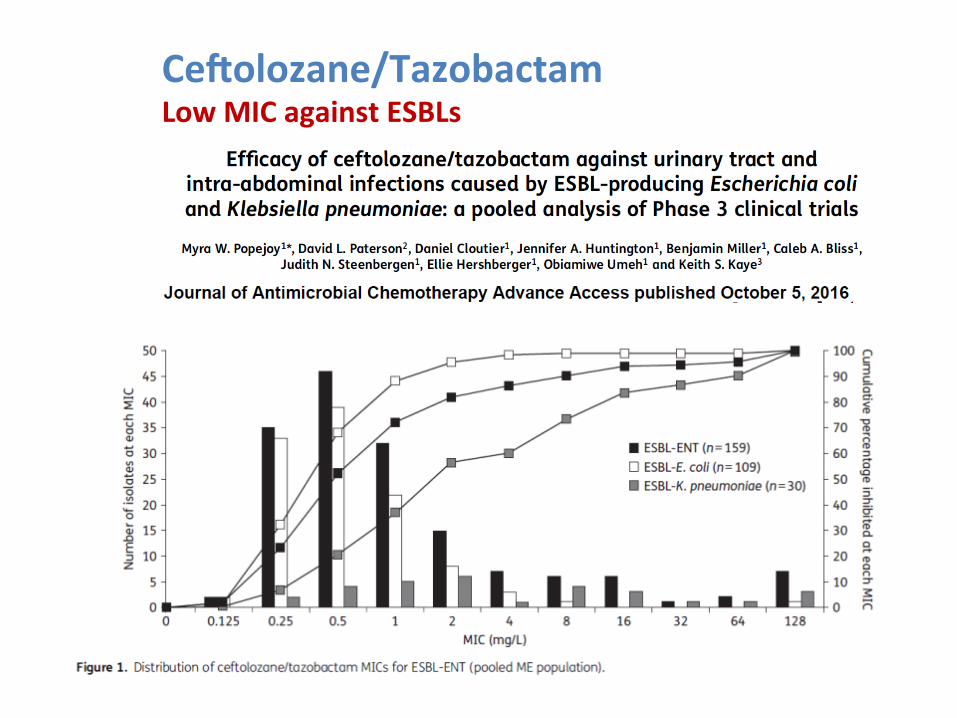
Ce#olozane/TazobactamLowMICagainstESBLs
Ce#olozane/Tazobactam
26
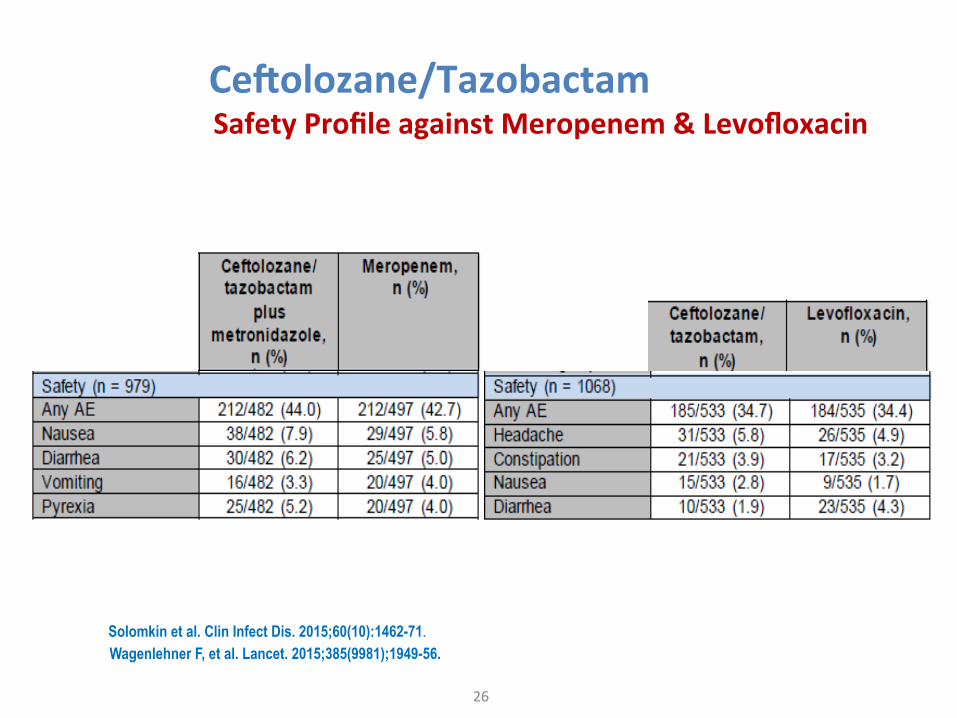
SafetyProfileagainstMeropenem&Levofloxacin
Solomkin et al. Clin Infect Dis. 2015;60(10):1462-71. Wagenlehner F, et al. Lancet. 2015;385(9981);1949-56.
Conclusion
27
Ø Invitroac;vityagainstESBLsandMDRP.aeruginosa3
Ø Non-InferiortoMeropenemincomplicatedIntra-AbdominalInfecPons2
Ø Non-InferiortoLevofloxacinincomplicatedUrinaryTractInfecPons1
Ø Superiorityvs.LevofloxacinininfecPonsoflowerUrinaryTractSystem1
1. Wagenlehner FM et al. Lancet. 2015;385:1949-1956. 2. Solomkin JS et al. Clin Infect Dis. 2015;60(10):1462-1471. 3. Ceftolozane/tazobactam, SmPC 2017 4. VanScoy B et al. Antimicrob Agents Chemother. 2013;57(8):4134-4138. 5. VanScoy B et al. Antimicrob Agents Chemother. 2014;58(10):6024-6031.
WhentoconsiderceGo/tazo• Asacarbapenem-sparingdefiniPvetherapyforthe
treatmentofinfecPonscausedby:– ESBL-producingEnterobacteriaceae– MDRP.aeruginosa.
• IncombinaPonwithmetronidazoleforempirictherapyof:– healthcare-associatedcIAIs– inpaPentswithriskfactorsforMDRs– inareaswheretheprevalenceofMDRpathogensishigh
• PhaseIIItrialforthetreatmentofvenPlatednosocomialpneumonia
28
PaPentProfile
§ History(last6mo)oftreatmentwithbroad-spectruman;bio;cs
§ Admissiontoahospitalfor>5days
§ PrioradmissiontoICU
§ Long-termhealth-carefacili;es
§ Hospitaliza;onclosetoknownMDRcarrier
§ Dialysis
§ Immunosuppression
§ Healthcareassociatedinfec;ons
Akovaetal.ClinMicrobiolInfect2012;18:439
Healthcare-associatedinfecPons,intheUSA,peryear
• ESBL-producingEnterobacteriaceae, ~26,000
• Carbapenem-resistantEnterobacteriaceae,
~9,000
• MDRP.aeruginosa ~6,700
• EspeciallyaffectedbyMDRsGram-ves
– cUTIs
– cIAIs30
HamptonT.JAMA.2013;310:1661–1663.ZilberbergMD,etal.InfectControlHospEpidemiol.2013;34:940–946.
CARBAPENEM–SPARINGREGIMENSINTHECONTEXTOFABSPROGRAMS
Thankyou