The pancreas and glucose homeostasis l4
68
The Pancreas and The Pancreas and Glucose Homeostasis Glucose Homeostasis
-
Upload
princesamera -
Category
Health & Medicine
-
view
1.441 -
download
2
Transcript of The pancreas and glucose homeostasis l4
The Pancreas and The Pancreas and Glucose HomeostasisGlucose Homeostasis
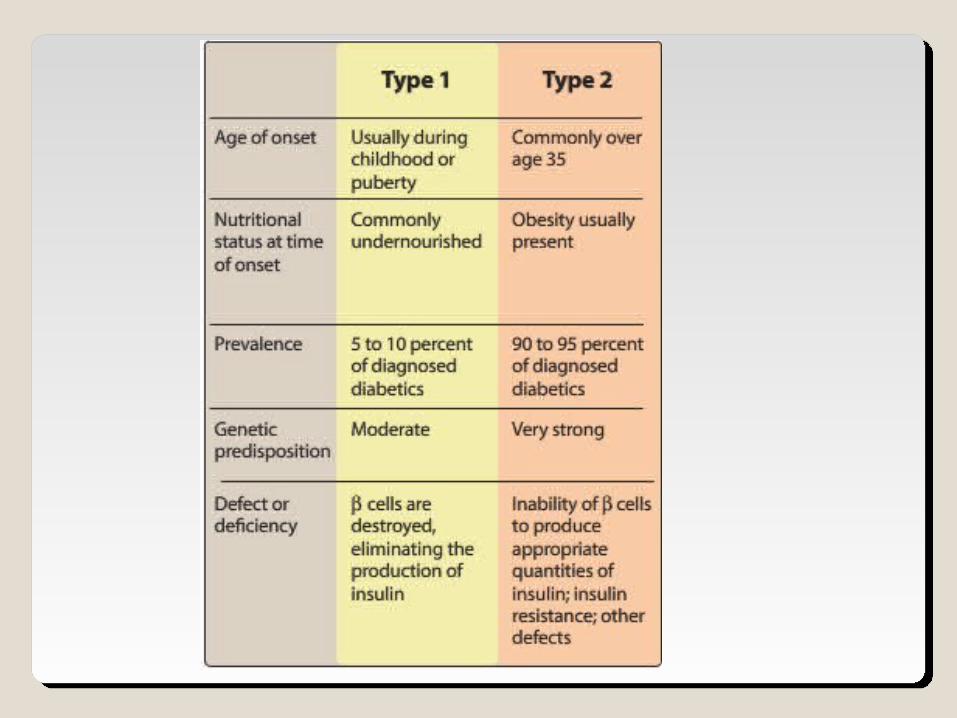
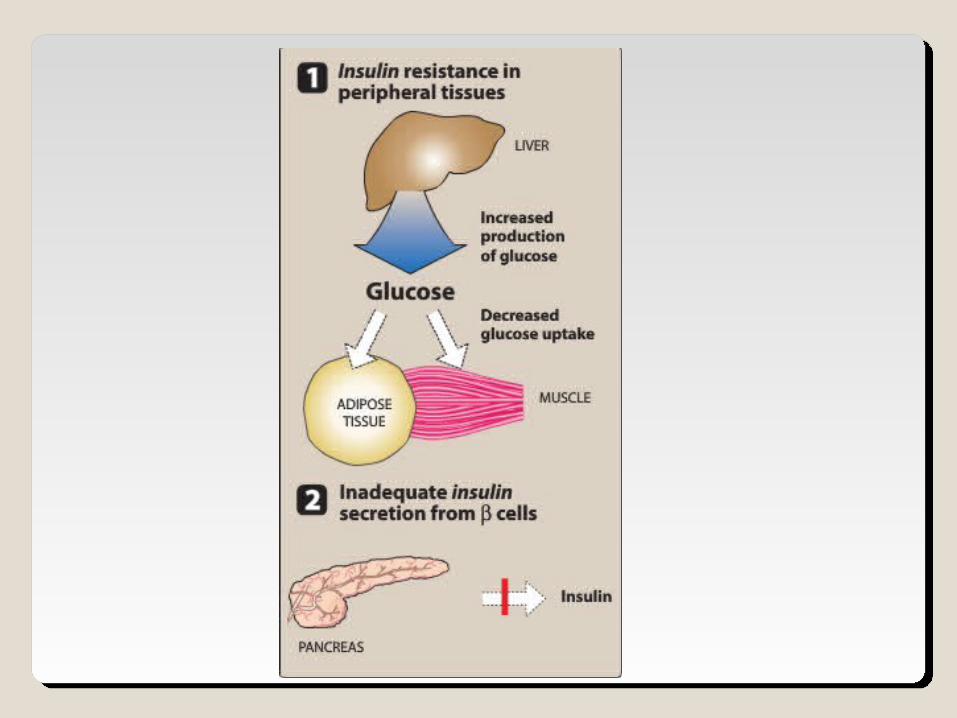
Diabetes mellitusDiabetes mellitusDM is characterized by elevated blood sugar
levels due to absolute or relative lack of insulin.
Type 1 diabetes - β-cell failure at outset◦ Insulin dependent
Type 2 diabetes - Gradual β-cell deterioration◦Early stages: Diet and Oral agents ◦Late-stage: Insulin therapy
Glycosylated hemoglobin Hb-A1c It is used to monitor the plasma glucose
concentration over prolonged periods of time (4-6 weeks).
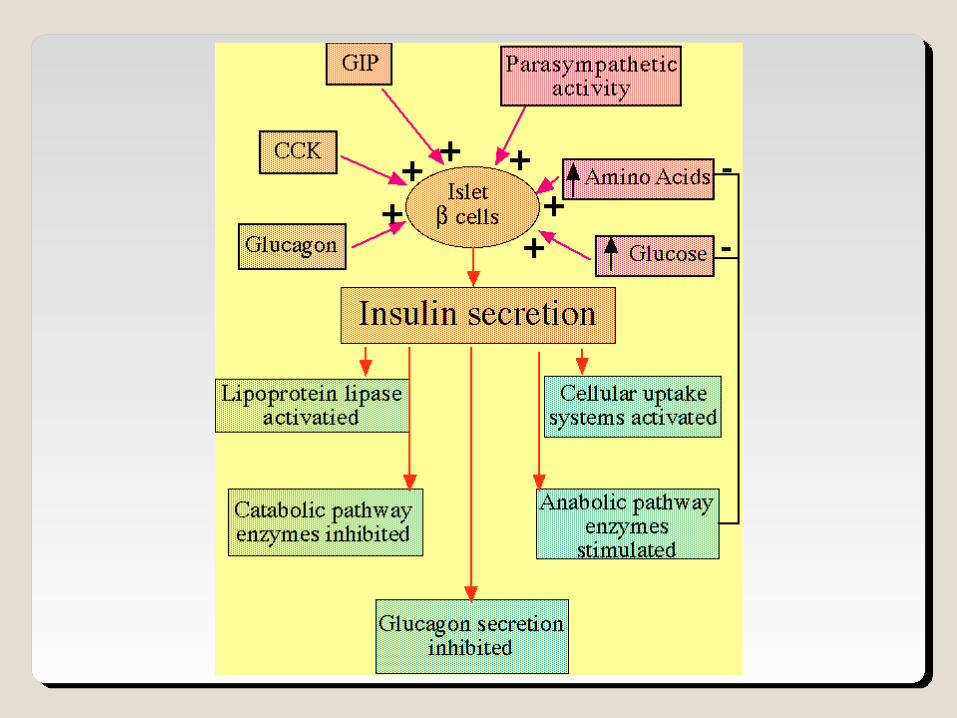
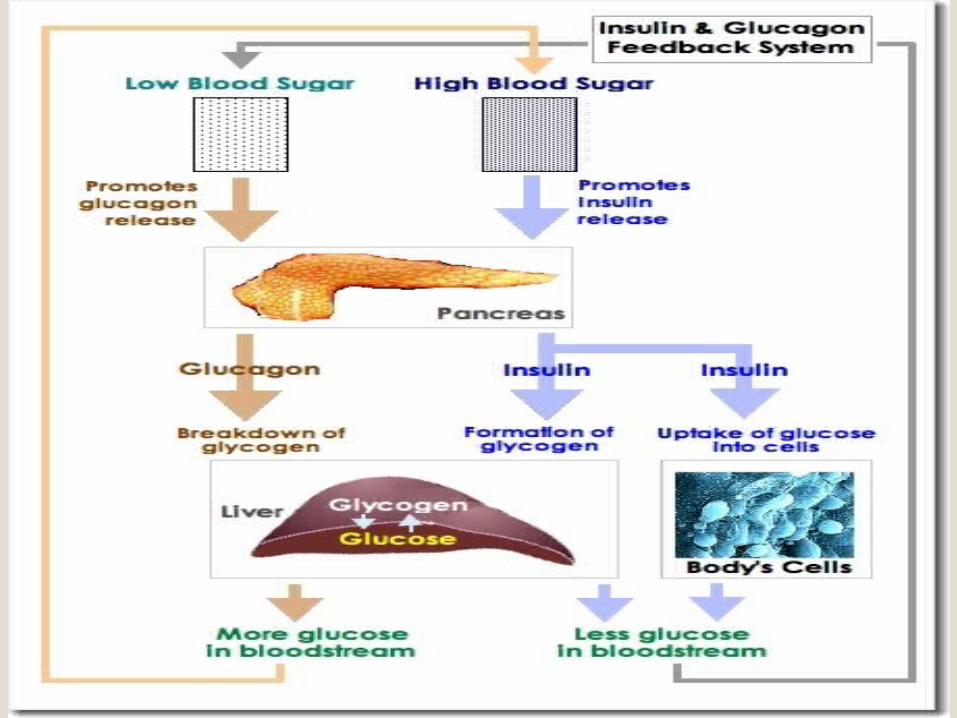
Insulin secretion is promoted by: ◦↑ blood glucose levels
◦↑ amino acids◦ GI hormones ◦ β-2 agonist: stimulates
glycogenolysis release of glucagon
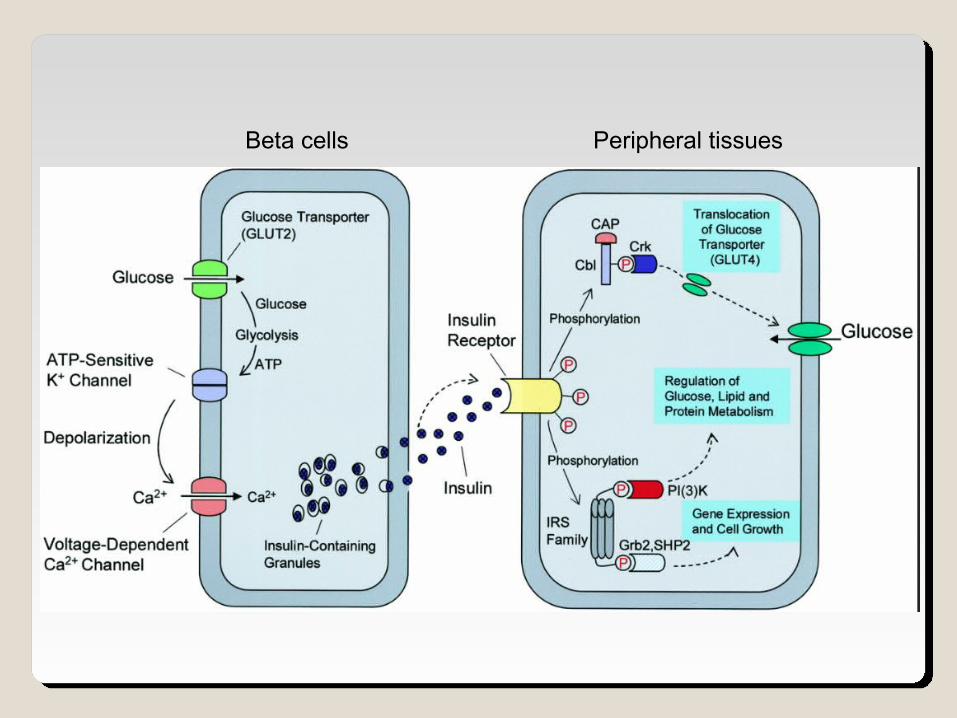
Beta cells Peripheral tissues
InsulinInsulin Insulin is a storage hormone:
i. it promotes anabolismii. inhibits catabolism of carbohydrates, fatty
acids and protein.
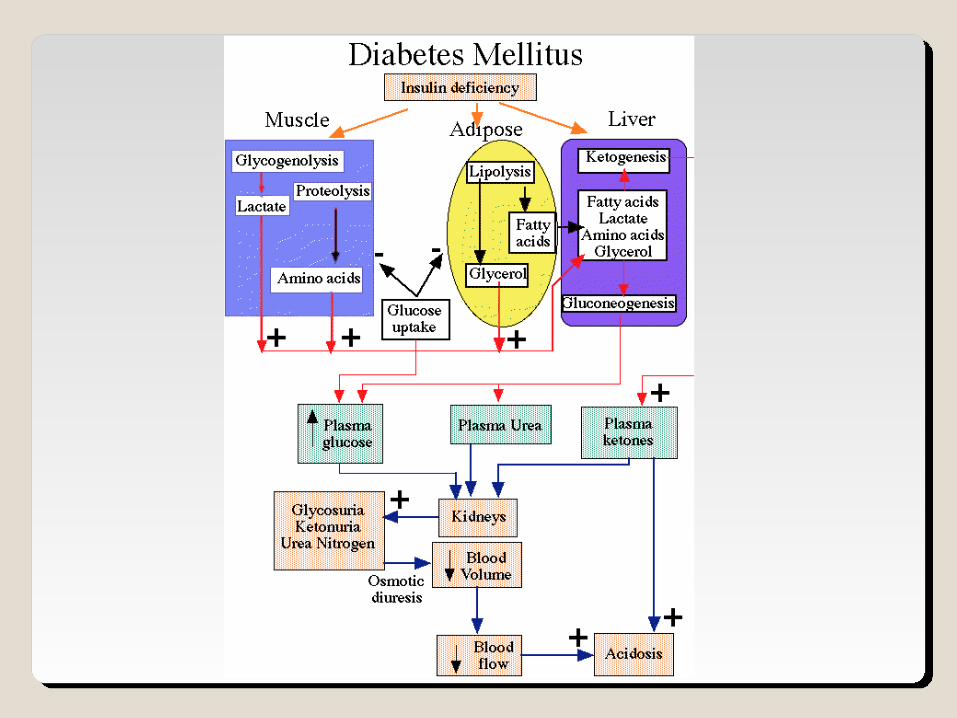
In the absence of insulin:i. most tissues cannot use glucose ii. fats/proteins are broken down to provide
energy.
Mechanism of action:
Insulin binds to insulin receptors on the plasma membrane and activates tyrosine kinase – primarily in adipose tissue, liver and skeletal muscle.
Liver: 1. Insulin increase the storage of glucose as
glycogen in the liver. ◦ It inserts the GLUT-2 glucose transport molecule in
the cell membrane. 1. It inhibits gluconeogenesis – thus significantly
↓ glucose output by the liver.2. It decrease the protein catabolism.
Muscle : 1. Insulin stimulates the glycogen synthesis
and protein synthesis.◦ Glucose transport into the cells is facilitated by
GLUT-4 into the cell membrane.1. It inhibits the protein catabolism.
Signs and symptomsThe classic symptoms of untreated diabetes are
loss of weight, polyuria (frequent urination), polydipsia (increased thirst) and polyphagia (increased hunger).[11] Symptoms may develop rapidly (weeks or months) in type 1 diabetes, while they usually develop much more slowly and may be subtle or absent in type 2 diabetes.
Prolonged high blood glucose can cause glucose absorption in the lens of the eye, which leads to changes in its shape, resulting in vision changes. Blurred vision is a common complaint leading to a diabetes diagnosis. A number of skin rashes that can occur in diabetes are collectively known as diabetic dermadromes.
Diabetic emergencies
People (usually with type 1 diabetes) may also present with diabetic ketoacidosis, a state of metabolic dysregulation characterized by the smell of acetone, a rapid, deep breathing known as Kussmaul breathing, nausea, vomiting and abdominal pain, and altered states of consciousness.
Complicationstypically develop after many years (10–
20). damage to blood vessels. Diabetes doubles the risk of
cardiovascular disease, ”macrovascular" diseases, (related to atherosclerosis of larger arteries) include ischemic heart disease (angina and myocardial infarction), stroke and peripheral vascular disease.
Diabetes also damages the capillaries (causes microangiopathy). Diabetic retinopathy, which affects blood vessel formation in the retina of the eye, can lead to visual symptoms, reduced vision, and potentially blindness.
Diabetic nephropathy, the impact of diabetes on the kidneys, can lead to scarring changes in the kidney tissue, loss of small or progressively larger amounts of protein in the urine, and eventually chronic kidney disease requiring dialysis.
Diabetic neuropathy is the impact of diabetes on the nervous system, most commonly causing numbness, tingling and pain in the feet and also increasing the risk of skin damage due to altered sensation. Together with vascular disease in the legs, neuropathy contributes to the risk of diabetes-related foot problems (such as diabetic foot ulcers) that can be difficult to treat and occasionally require amputation.
Insulin Insulin
Adipose tissue :1. Insulin facilitates the storage of
triglyceride by: i. activating plasma lipoprotein lipaseii. inhibiting intracellular lipolysis.
2. It increase the glucose uptake by GLUT-4 insertion into the cell membrane.
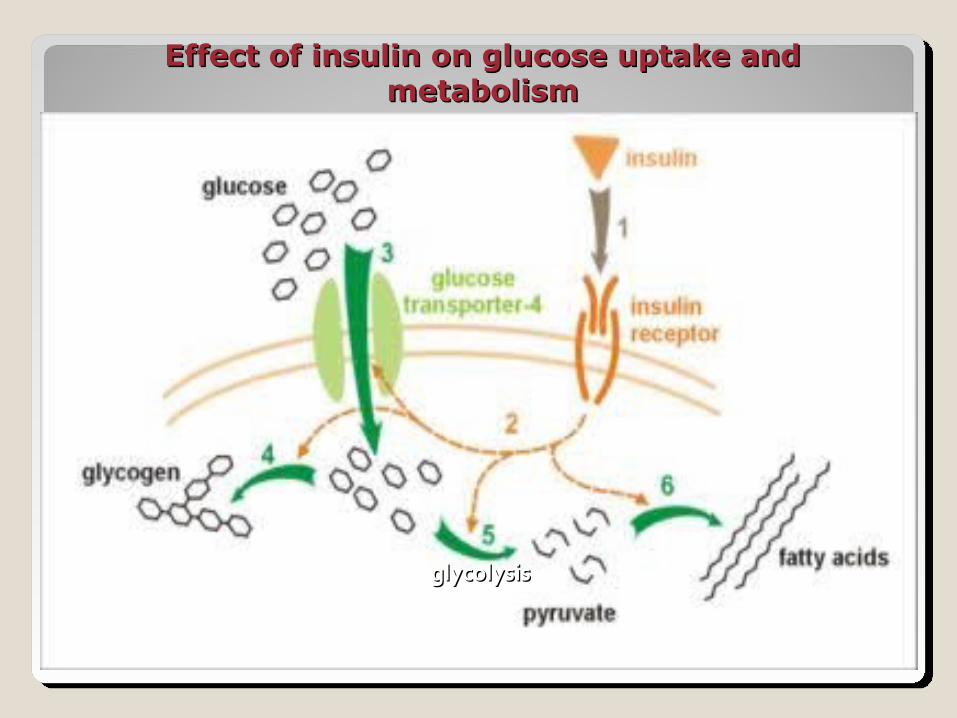
Effect of insulin on glucose uptake and Effect of insulin on glucose uptake and metabolismmetabolism
glycolysisglycolysis
Insulin is a 51 AA peptideNot active orally.Insulin is inactivated by insulinase (insulin
transhydrogenase ) found mainly in liver and kidney.
Dose reduced in renal insufficiencySources of Insulin :
◦ Beef pancreas / Pork pancreas ◦ Human insulin: recombinant DNA origin
Human Insulin: Do not contain measurable amounts of
proinsulin or contaminants.Diminished antibodyLess allergic reactionsLess lipodystrophyPreferred in gestational diabetes
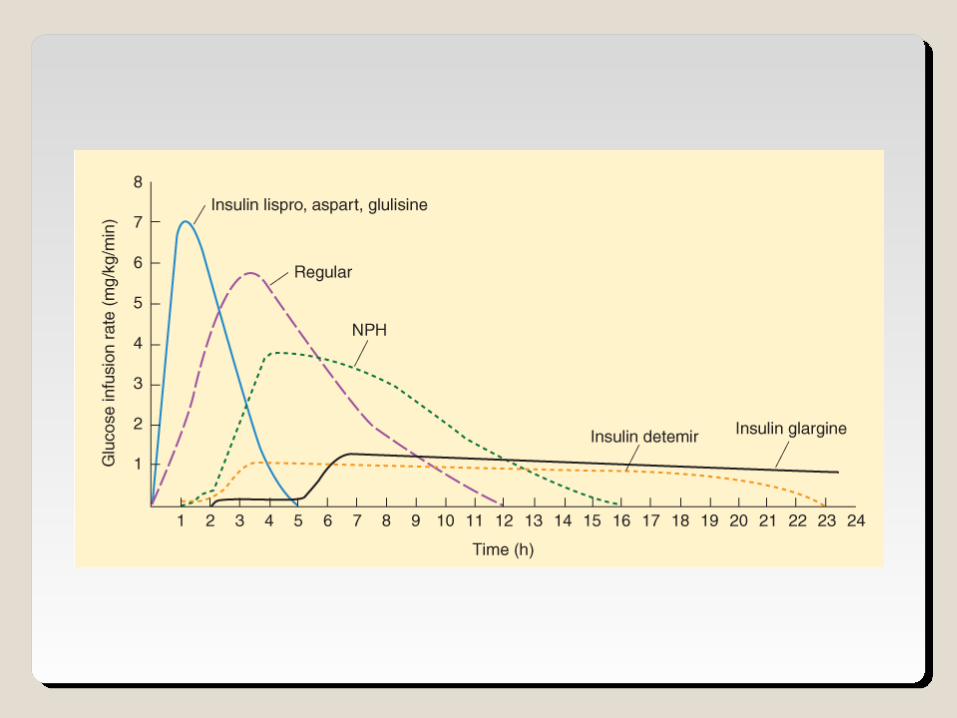
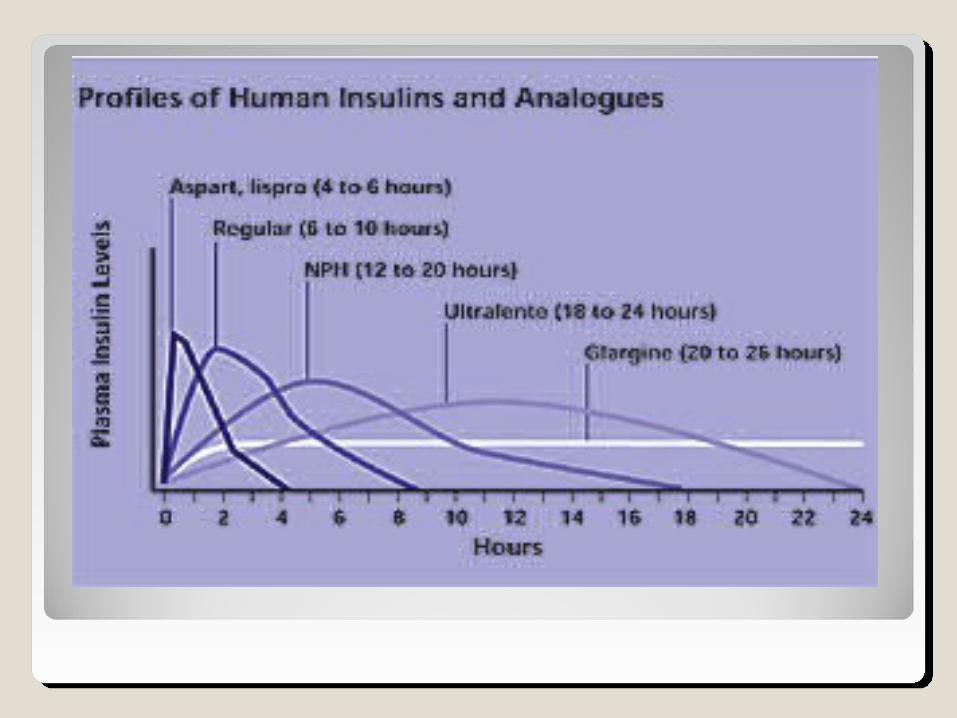
Insulin preparations:
A.Rapid acting insulin: Lispro, Aspart and Glulisine
B.Short acting insulin: Regular (crystalline)C. Intermediate acting insulin: NPH (isophane) and Lente (insulin zinc)
D. Long acting insulin: Protamine—zinc , Ultralente, Detimir and Glargine
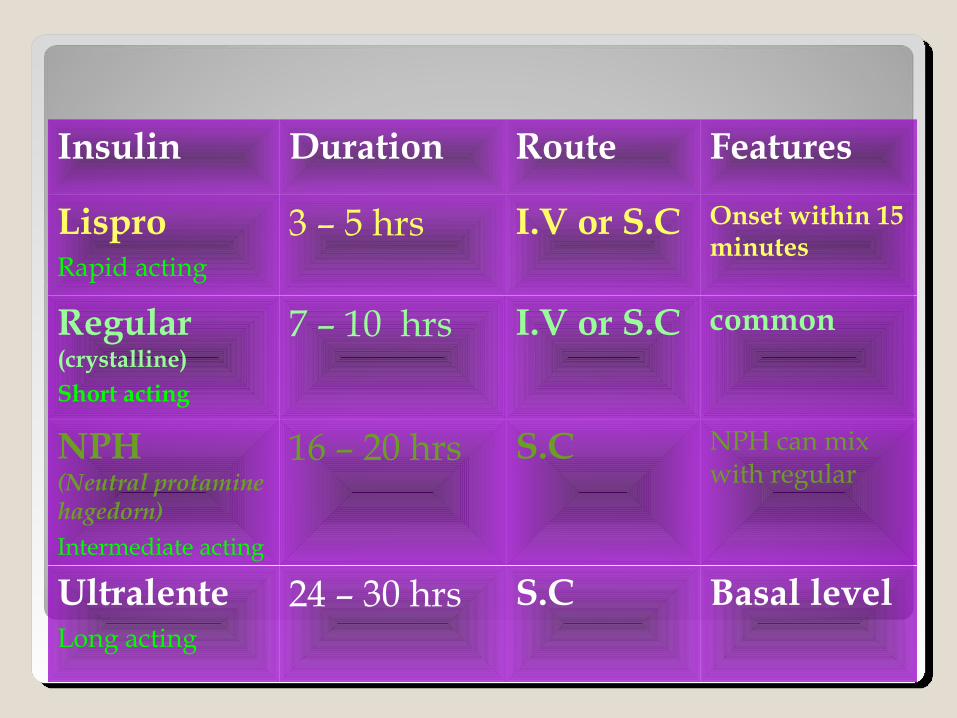
Insulin Duration Route Features
LisproRapid acting
3 – 5 hrs I.V or S.C Onset within 15 minutes
Regular (crystalline)Short acting
7 – 10 hrs I.V or S.C common
NPH (Neutral protamine hagedorn)Intermediate acting
16 – 20 hrs S.C NPH can mix with regular
UltralenteLong acting
24 – 30 hrs S.C Basal level
Adverse effects of Insulin Hypoglycemia Allergic reactionsLipodystrophyOthers includes
◦ Seizures◦ Coma
HypoglycemiaHypoglycemia
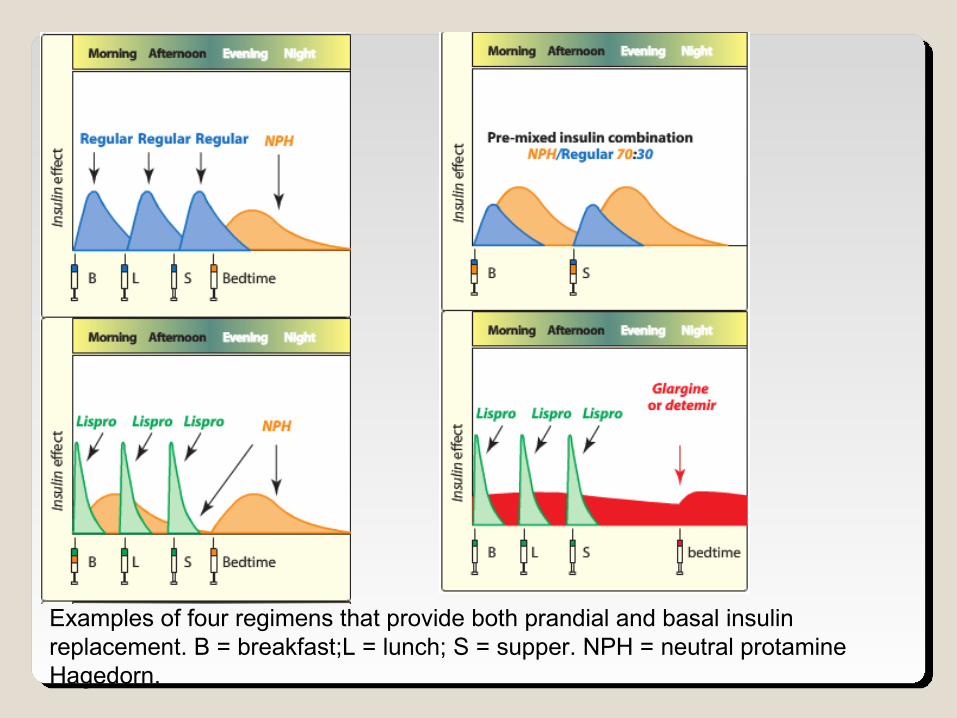
Examples of four regimens that provide both prandial and basal insulin replacement. B = breakfast;L = lunch; S = supper. NPH = neutral protamine Hagedorn.
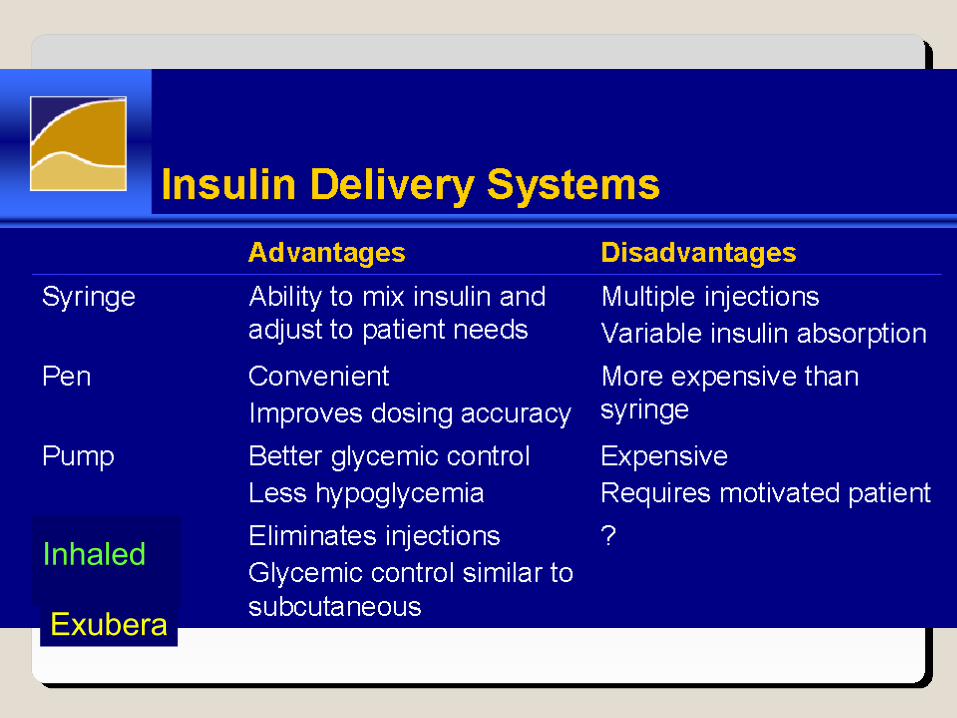
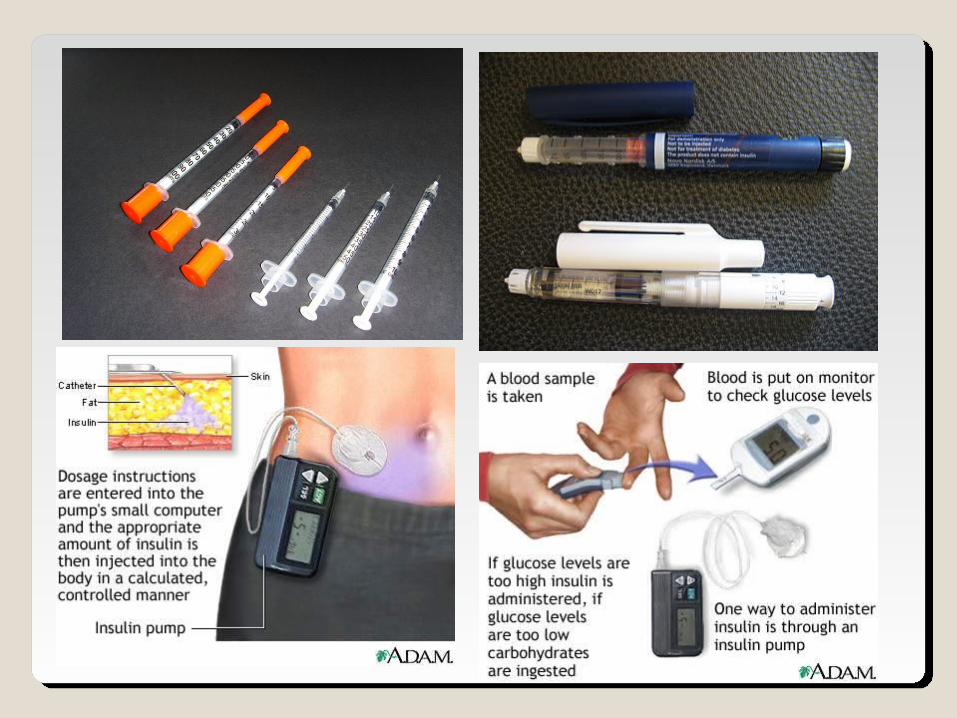
Insulin Delivery SystemsInsulin Delivery Systems
Exubera
Inhaled
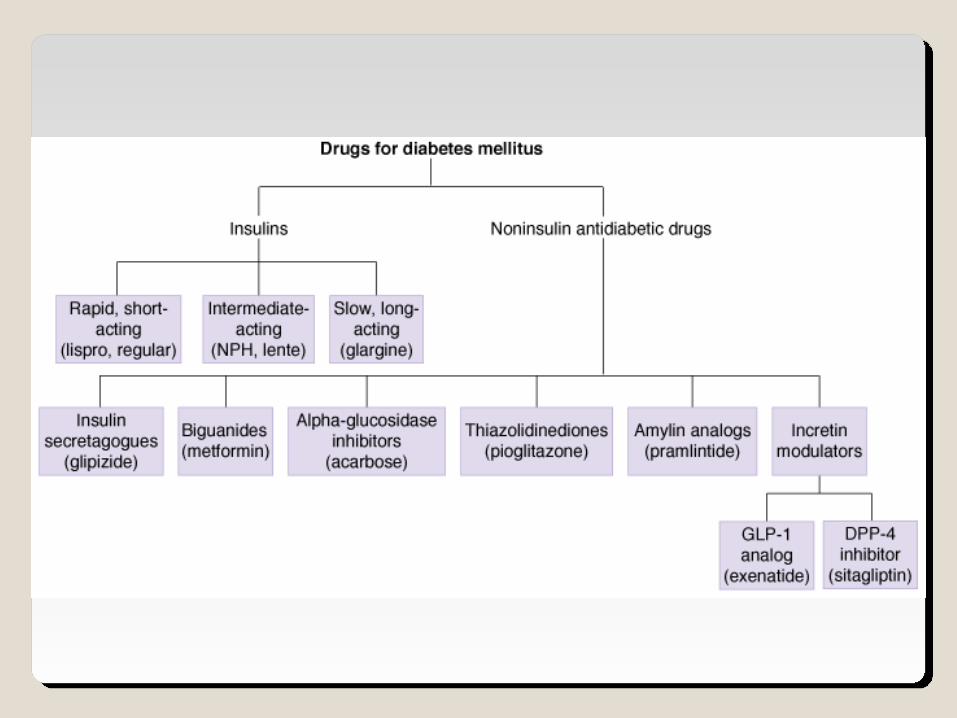
Oral Anti-diabetic drugsOral Anti-diabetic drugs
Mechanisms to reduce blood sugar 1.Stimulation of pancreatic insulin release –
Sulfonylureas, Meglitinide2.Reduce the bio-synthesis of glucose in liver –
Biguanides (Metformin)3.Increase the sensitivity of target cells to insulin
-- Thiazolidinediones4.Retard the absorption of sugars from the GI
tract – Acarbose, Miglitol
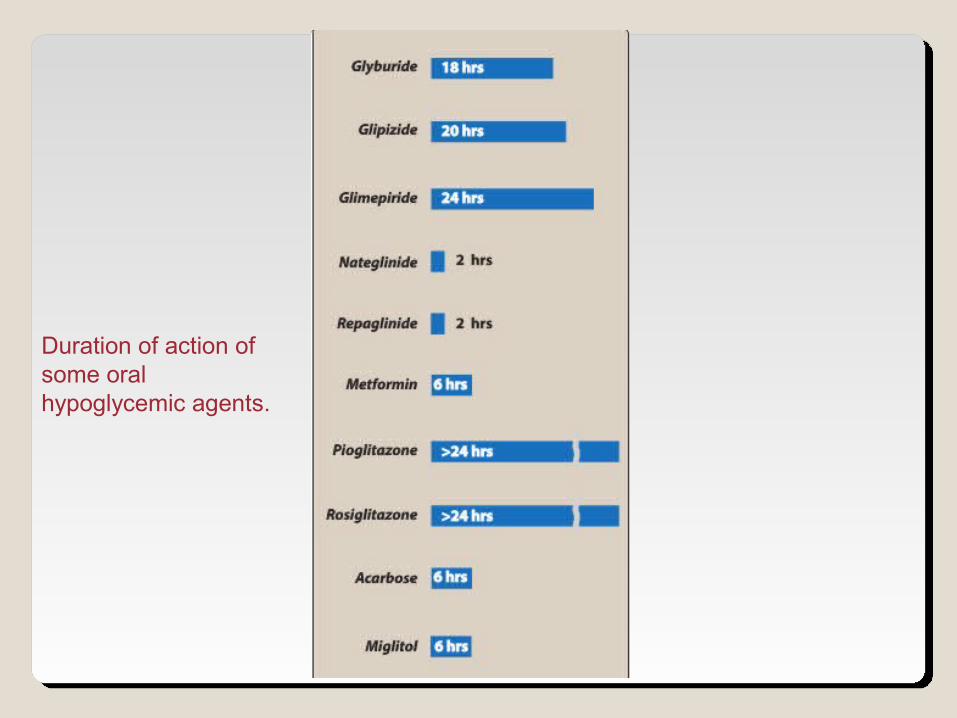
Duration of action of some oral hypoglycemic agents.
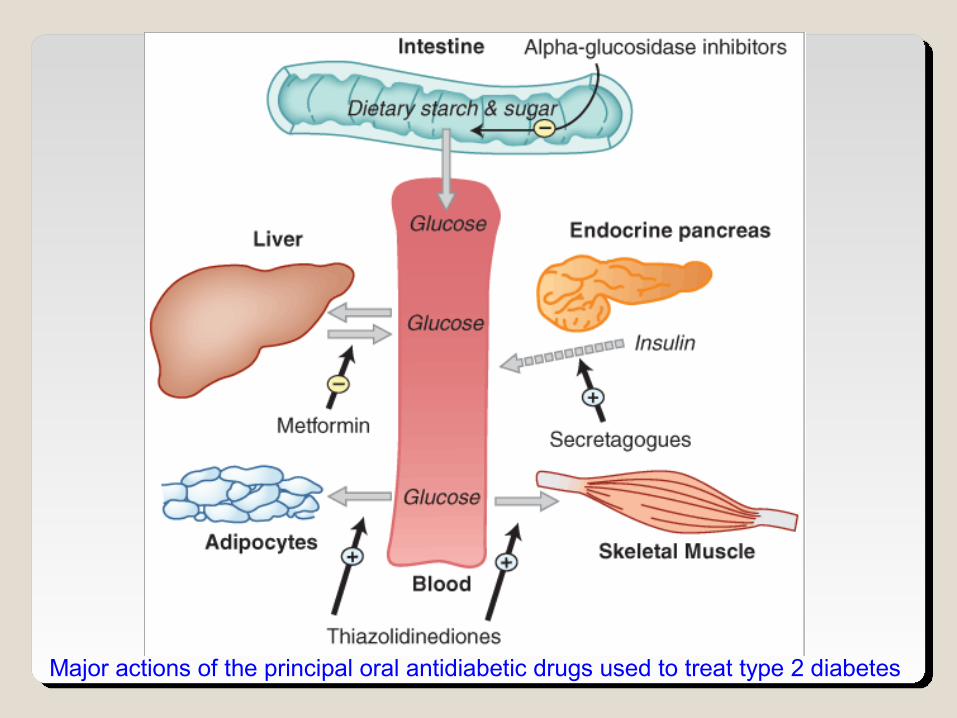
Major actions of the principal oral antidiabetic drugs used to treat type 2 diabetes
A.A. Alpha-Glucosidase Inhibitors:Alpha-Glucosidase Inhibitors:
Acarbose (Glucobay) , Miglitol (Glyset) 1. They inhibit α-glucosidase which converts
dietary starch and complex carbohydrates into simple sugars
2. It reduces absorption of glucose after meals.
The main side effects includes flatulence and diarrhea.
B.B. Insulin secretagoguesInsulin secretagogues
1.1. Sulfonylureas :Sulfonylureas :
First generation : ◦ Acetohexamide◦ Chlorpropamide◦ Tolbutamide◦ Tolazamide
Second generation : Glipizide, Glyburide more potent more efficacious fewer adverse effects.
Third generation : Glimiperide
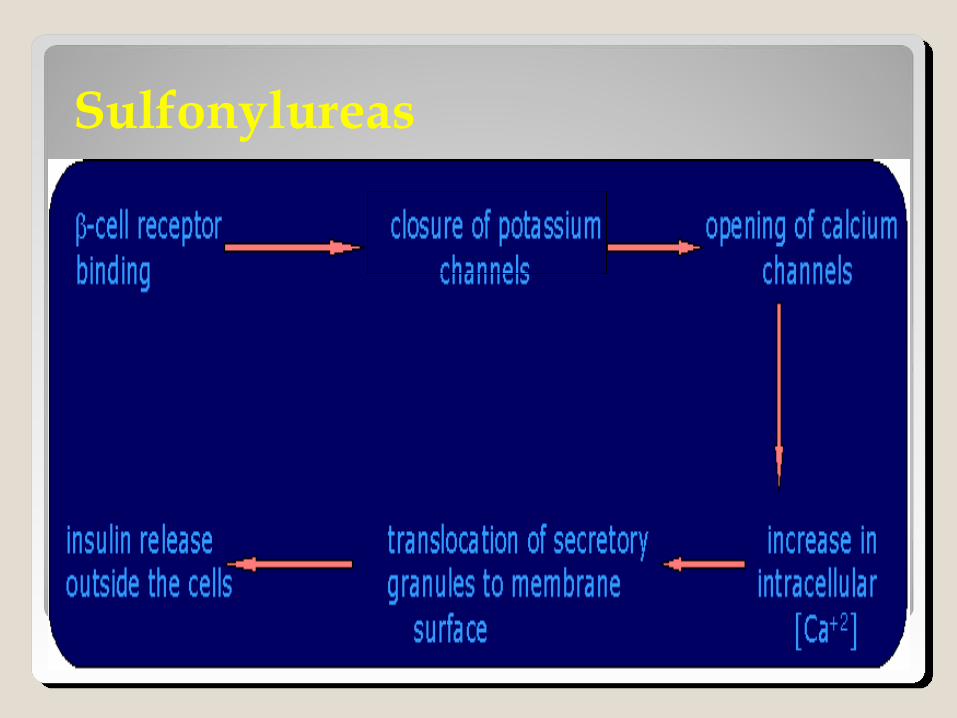
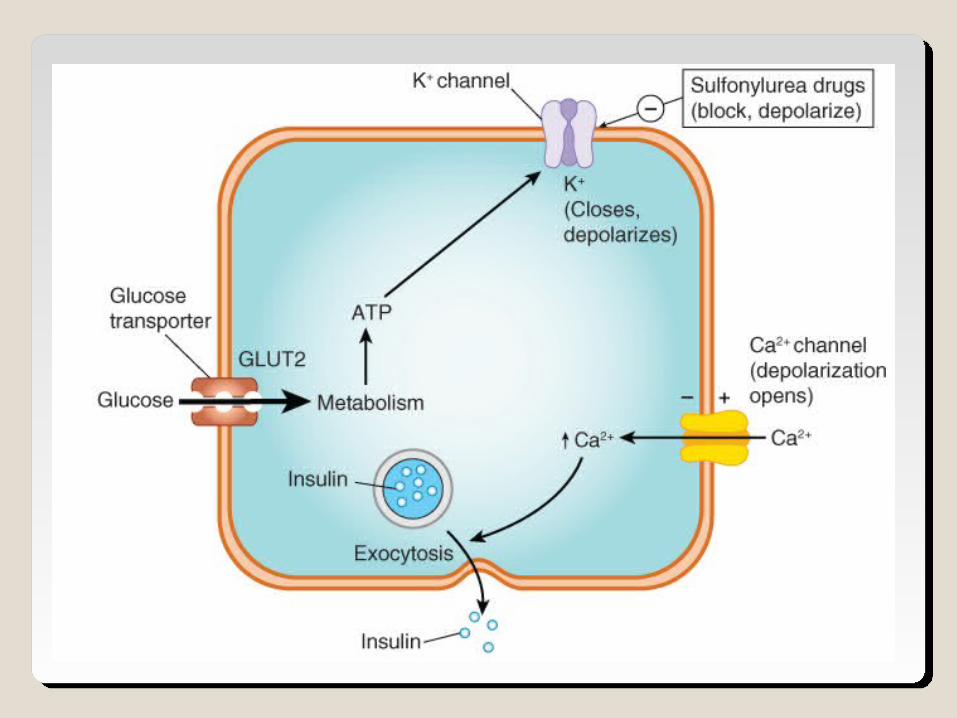
Mechanism of Action:
1)Stimulation of insulin release from the β cells of the pancreas by blocking the ATP-sensitive K+ channels, resulting in depolarization and Ca2+ influx
2)reduction in hepatic glucose production3)increase in peripheral insulin sensitivity.
Sulfonylureas
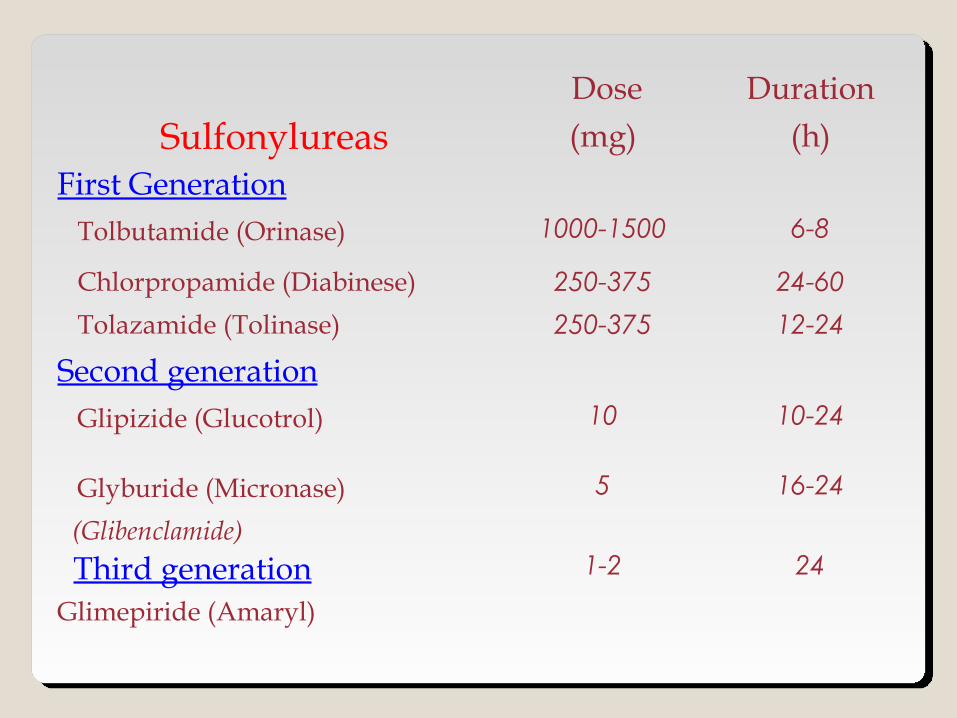
Sulfonylureas Dose(mg)
Duration(h)
First Generation Tolbutamide (Orinase) 1000-1500 6-8
Chlorpropamide (Diabinese) 250-375 24-60
Tolazamide (Tolinase) 250-375 12-24
Second generation Glipizide (Glucotrol) 10 10-24
Glyburide (Micronase) (Glibenclamide)
5 16-24
Third generationGlimepiride (Amaryl)
1-2 24
Sulfonylureas: Adverse effects :HypoglycemiaCholestatic jaundiceWeight gainCross placenta – fetal hypoglycemia.
Chlorpropamide : ◦ It can cause water retention by ↑ release of ADH
(SIADH)◦ Disulfiram-like reaction with alcohol.
2.2. Glinides: Glinides: Repaglinide, NateglinideRepaglinide, Nateglinide
More rapidly acting insulin enhancers and shorter duration than sulfonylurea.These are insulin secretagogues that act by
blocking ATP-dependent K+ channels.This leads to increased insulin secretion by
pancreatic β-cells.Hypoglycemia is the common adverse effect.Less weight gain
Repaglinide, Nateglinide
The drug has minimal renal excretion thus useful in patients with DM and impaired renal function.
It is designed to be taken with each meal to stimulate insulin release with meal. If a meal is skipped, so is the repaglinide.
C.C. Insulin sensitizersInsulin sensitizers
1. Biguanides (Metformin):
◦ Inhibits glucose output (gluconeogenesis).◦ It increase the sensitivity of liver and muscle to insulin.
(increase uptake of glucose)◦ Does not promote insulin secretion. ◦ It causes modest weight loss.
1. Biguanides2. Thiazolidinediones
Biguanides: Metformin (Glucophage) ◦ It does not cause hypoglycemia.
◦ It produces a significant ↓ TG and LDL, and ↑HDL.
There is a serious concern about lactic acidosis especially in patients with kidney disease.
2.2. Thiazolidinediones (glitazones) Thiazolidinediones (glitazones)
Enhance glucose and lipid metabolism through action on Peroxisome Proliferator Activated Receptor (PPAR–γ)
Enhance sensitivity to insulin in muscle and fat by increasing the GLUT 4 glucose transporters.
E.g. : Pioglitazone Actos, Rosiglitazone Avandia: EMA recommended in Sep
2010 to be suspended from the EU market due to elevated cardiovascular risks
Thiazolidinediones: Beneficial effects on serum lipid; ↓TG and
↑HDL.Troglitazone (Rezulin), was withdrawn in 1990s
from the market due to an increased incidence of drug-induced hepatitis.
The main side effect of all thiazolidinediones is water retention, leading to edema .
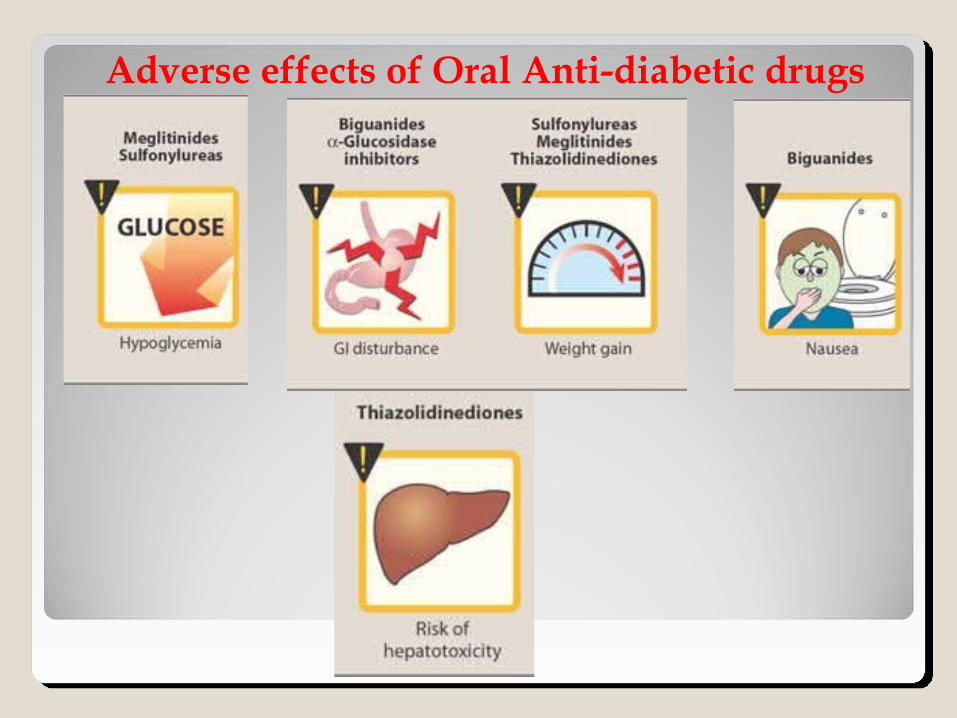
Adverse effects of Oral Anti-diabetic drugs
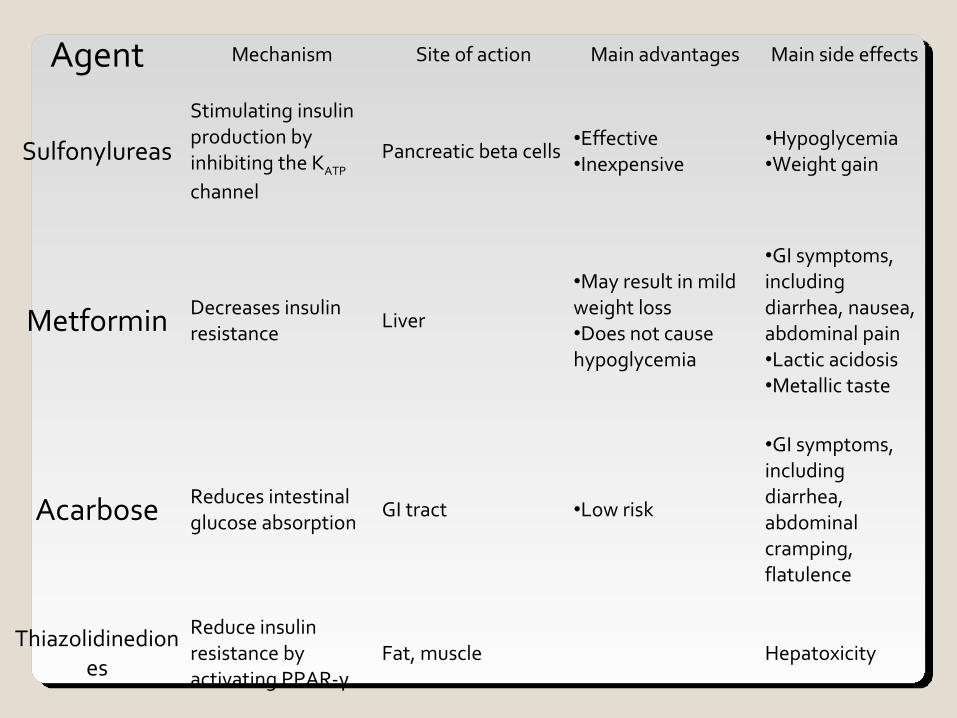
Agent Mechanism Site of action Main advantages Main side effects
Sulfonylureas
Stimulating insulin production by inhibiting the KATP channel
Pancreatic beta cells•Effective •Inexpensive
•Hypoglycemia •Weight gain
Metformin Decreases insulin resistance
Liver
•May result in mild weight loss •Does not cause hypoglycemia
•GI symptoms, including diarrhea, nausea, abdominal pain •Lactic acidosis •Metallic taste
Acarbose Reduces intestinal glucose absorption
GI tract •Low risk
•GI symptoms, including diarrhea, abdominal cramping, flatulence
Thiazolidinediones
Reduce insulin resistance by activating PPAR-γ
Fat, muscle Hepatoxicity
NEW CLASSES OF NEW CLASSES OF HYPOGLYCEMICSHYPOGLYCEMICS
• Glucagon-like peptide-1 (GLP-1)
• Gastric inhibitory peptide (GIP)
• Released from the gut
A. Incretins
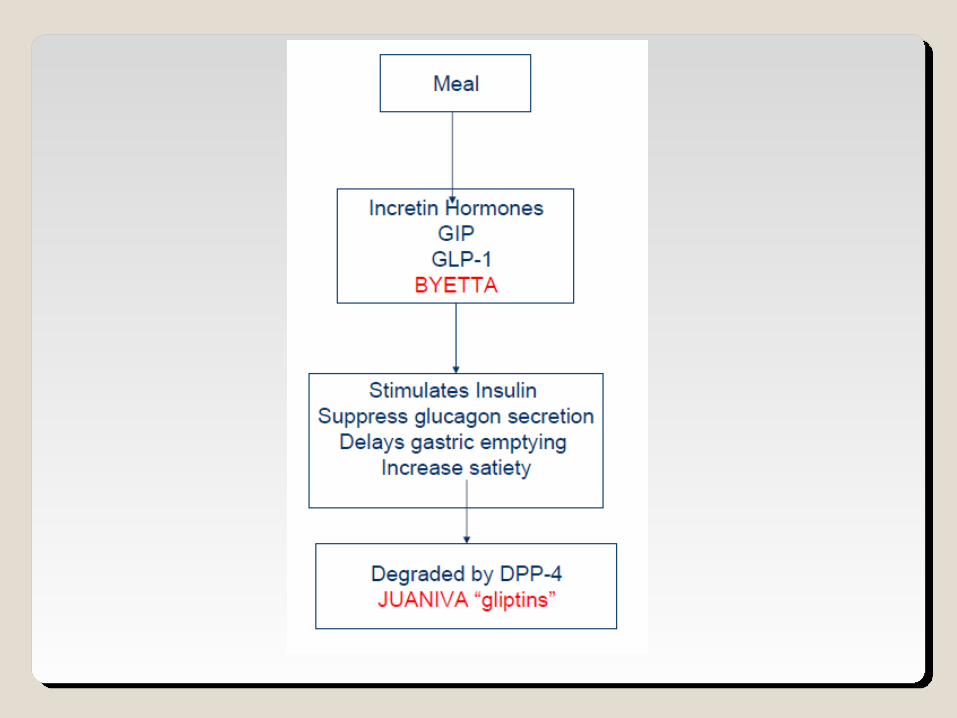
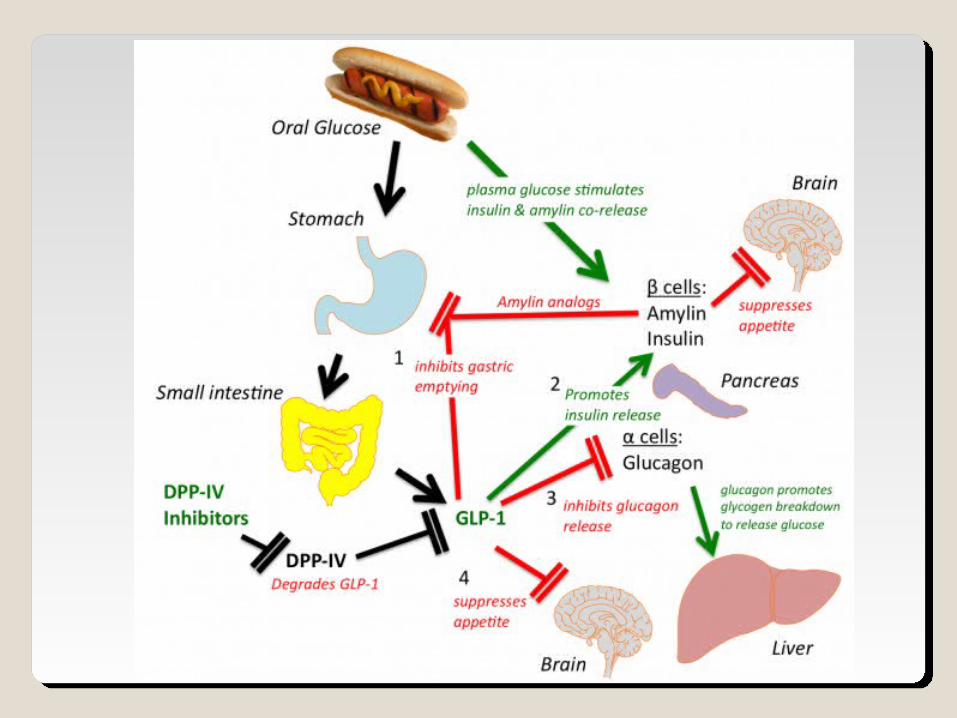
• Function of incretins:
1. augment glucose-dependent insulin secretion after a meal.
2. They also slow the rate of absorption of nutrients into the blood stream by:
1. reducing gastric emptying 2. may directly reduce food intake
3. They inhibit glucagon release from the alpha cells of the Islets of Langerhans.
Both GLP-1 and GIP are rapidly inactivated by the enzyme dipeptidyl peptidase 4 (DPP-4).
GIPGLP-1
DPP-4Inactive products
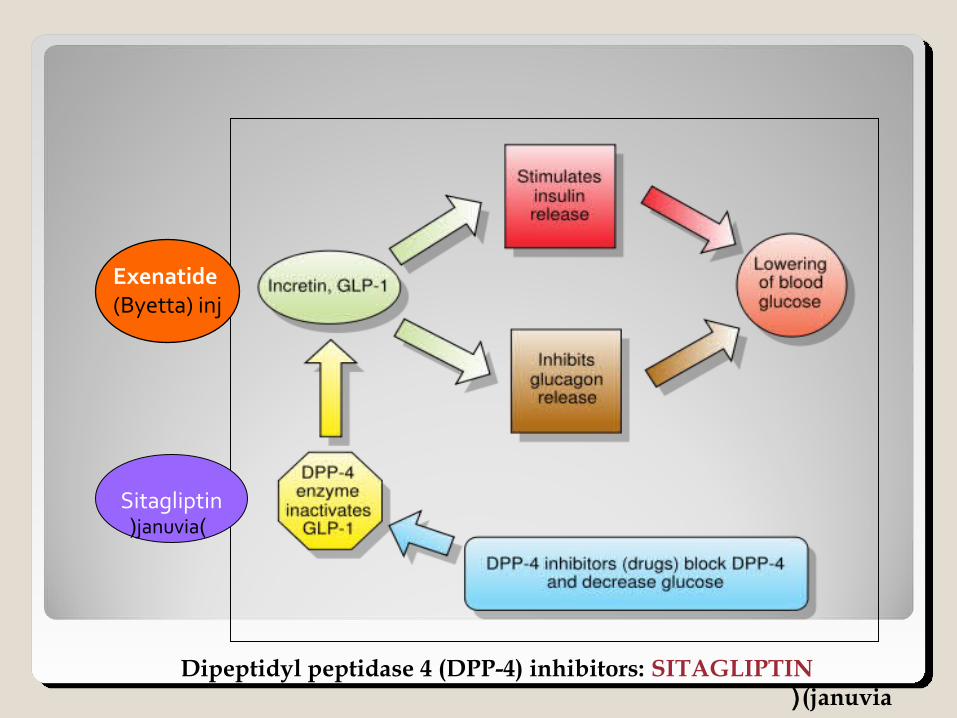
Dipeptidyl peptidase 4 (DPP-4) inhibitors: SITAGLIPTIN (januvia(
Exenatide (Byetta) inj
Sitagliptin)januvia(
• GLP-1 analogs. • improves glucose-dependent insulin secretion • slows gastric emptying time• decreases food intake • decreases postprandial glucagon secretion • promotes β-cell proliferation. • Consequently, weight gain and postprandial
hyperglycemia are reduced, and HbA1c levels decline. • Exenatide is administered subcutaneously.
A.Incretin Mimetics: • Exenatide Exenatide (Byetta) (Byetta)
• Liraglutide Liraglutide (Victosa): long duration of action approved in 2010(Victosa): long duration of action approved in 2010
Exenatide : Short duration of action.
Use: as an adjunct to therapy in patients with
Type 2 diabetes who have failed to achieve adequate glycemic control on a sulfonylurea, metformin, glitazone, or combination thereof.
Adverse effects: Nausea, vomiting, and diarrhea.
B. Dipeptidyl Peptidase-IV InhibitorsB. Dipeptidyl Peptidase-IV Inhibitors
Sitagliptin (Januvia) FDA approved Oct 2006Vildagliptin (Galvus) EU Approved 2008 Saxagliptin (Onglyza) FDA Approved July 2009 Linagliptin (Tradjenta) FDA Approved May 2, 2011
Sitagliptin (Januvia)
Mechanism of action•Sitagliptin inhibits the enzyme DPP-IV, which is
responsible for the inactivation of incretin hormones.
•Prolonging the activity of incretin hormones results in increased insulin release in response to meals and a reduction in inappropriate secretion of glucagon.
•Use: – as monotherapy or in combination with a
sulfonylurea, metformin or a glitazone.
Pharmacokinetics and fate
•Well absorbed after oral administration. •Food does not affect the extent of absorption. •The majority excreted unchanged in the urine. •Dosage adjustments are recommended for
patients with renal dysfunction.
Adverse effects•Nasopharyngitis and headache.
Synthetic Amylin Analog: Synthetic Amylin Analog: Pramlintide (SYMLIN): Pramlintide (SYMLIN):
Amylin: 37-aa peptide produced by beta cells
and co-secreted with insulin.Effects:
1. Inhibits glucagon secretion 2. delay gastric emptying3. suppress appetite
•indicated as an adjunct to mealtime insulin therapy in patients with Type 1 or Type 2 diabetes.
•Effects: - delays gastric emptying - decreases postprandial glucagon secretion- improves satiety
Pramlintide (SYMLIN):
•Administration of Pramlintide:
•subcutaneous injection
•injected immediately prior to meals.
•When pramlintide is initiated, the dose of rapid- or short-acting insulin should be decreased by 50% prior to meals to avoid a risk of severe hypoglycemia.
•Adverse effects are mainly gastrointestinal and consist of nausea, anorexia, and vomiting.
Agents that increase blood glucose Agents that increase blood glucose (hyperglycemics)(hyperglycemics)
Glucagon: UsesA.first aid in cases of severe hypoglycemia when the
victim is unconscious or for other reasons cannot take glucose orally.
B.treatment of overdose with beta blockers◦ It has positive inotropic action and chronotropic
action on the heart.◦ It acts by stimulation of glucagon receptors and not
through beta 1 receptors.
Diazoxide Diazoxide is a nondiuretic thiazide that promptly
increases blood glucose levels by direct inhibition of insulin secretion.
Diazoxide is useful in cases of insulinoma or leucine-sensitive hypoglycemia.
Diazoxide may cause sodium retention, gastrointestinal irritation, and changes in circulating white blood cells.