Thalassaemia - WordPress.com · clinical management of these diseases. As will become evident, this...
13
Seminar www.thelancet.com Published online July 31, 2017 http://dx.doi.org/10.1016/S0140-6736(17)31822-6 1 Thalassaemia Ali T Taher, David J Weatherall, Maria Domenica Cappellini Inherited haemoglobin disorders, including thalassaemia and sickle-cell disease, are the most common monogenic diseases worldwide. Several clinical forms of α-thalassaemia and β-thalassaemia, including the co-inheritance of β-thalassaemia with haemoglobin E resulting in haemoglobin E/β-thalassaemia, have been described. The disease hallmarks include imbalance in the α/β-globin chain ratio, ineffective erythropoiesis, chronic haemolytic anaemia, compensatory haemopoietic expansion, hypercoagulability, and increased intestinal iron absorption. The complications of iron overload, arising from transfusions that represent the basis of disease management in most patients with severe thalassaemia, might further complicate the clinical phenotype. These pathophysiological mechanisms lead to an array of clinical manifestations involving numerous organ systems. Conventional management primarily relies on transfusion and iron-chelation therapy, as well as splenectomy in specific cases. An increased understanding of the molecular and pathogenic factors that govern the disease process have suggested routes for the development of new therapeutic approaches that address the underlying chain imbalance, ineffective erythropoiesis, and iron dysregulation, with several agents being evaluated in preclinical models and clinical trials. Introduction Since the first published description of severe thalass- aemia over 90 years ago by Cooley and Lee, 1 several accounts of the disease have been described and an extensive amount has been learnt. 2–4 Although the cellular and molecular basis of this group of diseases was initially unknown, in the past 50 years a considerable amount has been discovered to create a substantial body of work. 5 Using these resources we now have a refined under- standing of the pathophysiology of the thalassaemia syndromes. However, despite our understanding of the pathophysiology, management of these diseases has been complex and is progressing gradually. 3,4 Additionally, the available therapeutic routes for thalassaemias and the complications that result from current treatments are few. Although a great deal of excitement has developed around newer therapeutic approaches and potential curative strategies, 6 much remains to be understood about the clinical variability of these disorders, the natural history of the thalassaemia syndromes, and the optimal use of the currently available treatments. In this Seminar, we aim to provide an overview of the thalassaemia syndromes and comprehensively discuss our current approach to the clinical management of these diseases. As will become evident, this understanding is crucial to ensuring that new therapies can be effectively integrated into the repertoire of existing management strategies. Thalassaemia, sickle-cell disease, and other inherited haemoglobin disorders are the most pervasive mono- genic diseases worldwide. The high frequency of in- herited haemoglobin variants in certain regions reflects their heterozygote resistance to Plasmodium falciparum malaria, and extensive studies 7 have shown that this resistance is certainly the case for α-thalassaemia, β-thalassaemia, and haemoglobin E. An estimated 1–5% of the global population are carriers for a genetic thalassaemia mutation. 8–14 Although the epidemiology of the various clinical forms remains poorly recognised, the disease is known to be highly prevalent in the area extending from sub-Saharan Africa, through the Mediterranean region and Middle East, to the Indian subcontinent and east and southeast Asia. 8–14 Thus, over 90% of patients with these disorders live in low-income and middle-income countries. The number of patients with these diseases is expected to increase in the coming years as infant mortality from infectious and nutritional causes declines in many regions of the world. As a result, when discussing management strategies, we will often focus on the current best practices, but it is important for clinicians to be aware of the substantial limitations in implementing even these stan- dard therapies to many patients around the world. Therefore we will focus our discussion on the need for improved therapies, as well as on more standardised and easy-to- implement strategies for use in resource-poor countries. It should also be noted that because of continued migration, these diseases are now becoming increasingly common in large multiethnic cities in Europe and North America, making it a global health concern. 15–18 Molecular and clinical forms At the molecular level, haemoglobin synthesis is controlled by two multigene clusters on chromosome 16 (encoding Published Online July 31, 2017 http://dx.doi.org/10.1016/ S0140-6736(17)31822-6 Department of Internal Medicine, American University of Beirut Medical Centre, Beirut, Lebanon (Prof A T Taher MD); MRC Weatherall Institute of Molecular Medicine, University of Oxford, Oxford, UK (Sir D J Weatherall MD); and Department of Clinical Sciences and Community, University of Milan, IRCCS Ca’Granda Foundation Maggiore Policlinico Hospital, Milan, Italy (Prof M D Cappellini MD) Correspondence to: Prof Ali T Taher, Department of Internal Medicine, American University of Beirut Medical Center, PO Box 11–0236, Beirut 11072020, Lebanon [email protected] Search strategy and selection criteria We searched PubMed using the terms “thalassaemia OR thalassemia” in combination with “molecular” or “epidemiology” or “diagnosis” or “pathophysiology” or “clinical complications” or “treatment OR management”. We limited our search to publications in English. We mostly selected publications from January, 2006, to May, 2017, but did not exclude frequently referenced and highly regarded older publications. We also searched the reference lists of articles identified by this search strategy and selected the most relevant ones. Review articles and book chapters are cited to provide readers with more details and more references than can be addressed in this Seminar.
Transcript of Thalassaemia - WordPress.com · clinical management of these diseases. As will become evident, this...

Seminar
www.thelancet.com Published online July 31, 2017 http://dx.doi.org/10.1016/S0140-6736(17)31822-6 1
ThalassaemiaAli T Taher, David J Weatherall, Maria Domenica Cappellini
Inherited haemoglobin disorders, including thalassaemia and sickle-cell disease, are the most common monogenic diseases worldwide. Several clinical forms of α-thalassaemia and β-thalassaemia, including the co-inheritance of β-thalassaemia with haemoglobin E resulting in haemoglobin E/β-thalassaemia, have been described. The disease hallmarks include imbalance in the α/β-globin chain ratio, ineffective erythropoiesis, chronic haemolytic anaemia, compensatory haemopoietic expansion, hypercoagulability, and increased intestinal iron absorption. The complications of iron overload, arising from transfusions that represent the basis of disease management in most patients with severe thalassaemia, might further complicate the clinical phenotype. These pathophysiological mechanisms lead to an array of clinical manifestations involving numerous organ systems. Conventional management primarily relies on transfusion and iron-chelation therapy, as well as splenectomy in specific cases. An increased understanding of the molecular and pathogenic factors that govern the disease process have suggested routes for the development of new therapeutic approaches that address the underlying chain imbalance, ineffective erythropoiesis, and iron dysregulation, with several agents being evaluated in preclinical models and clinical trials.
IntroductionSince the first published description of severe thalassaemia over 90 years ago by Cooley and Lee,1 several accounts of the disease have been described and an extensive amount has been learnt.2–4 Although the cellular and molecular basis of this group of diseases was initially unknown, in the past 50 years a considerable amount has been discovered to create a substantial body of work.5 Using these resources we now have a refined understanding of the pathophysiology of the thalassaemia syndromes. However, despite our understanding of the pathophysiology, management of these diseases has been complex and is progressing gradually.3,4 Additionally, the available therapeutic routes for thalassaemias and the complications that result from current treatments are few. Although a great deal of excitement has developed around newer therapeutic approaches and potential curative strategies,6 much remains to be understood about the clinical variability of these disorders, the natural history of the thalassaemia syndromes, and the optimal use of the currently available treatments. In this Seminar, we aim to provide an overview of the thalass aemia syndromes and comprehensively discuss our current approach to the clinical management of these diseases. As will become evident, this under standing is crucial to ensuring that new therapies can be effectively integrated into the repertoire of existing management strategies.
Thalassaemia, sicklecell disease, and other inherited haemoglobin disorders are the most pervasive mono genic diseases worldwide. The high frequency of inherited haemoglobin variants in certain regions reflects their heterozygote resistance to Plasmodium falciparum malaria, and extensive studies7 have shown that this resis tance is certainly the case for αthalassaemia, β thalassaemia, and haemoglobin E. An estimated 1–5% of the global population are carriers for a genetic thalassaemia mutation.8–14 Although the epidemiology of the various clinical forms remains poorly recognised, the disease is known to be highly prevalent in the area extending from
subSaharan Africa, through the Mediterranean region and Middle East, to the Indian subcontinent and east and southeast Asia.8–14 Thus, over 90% of patients with these disorders live in lowincome and middleincome countries. The number of patients with these diseases is expected to increase in the coming years as infant mortality from infectious and nutritional causes declines in many regions of the world. As a result, when discussing management strategies, we will often focus on the current best practices, but it is important for clinicians to be aware of the substantial limitations in implementing even these standard therapies to many patients around the world. Therefore we will focus our discussion on the need for improved therapies, as well as on more standardised and easytoimplement strategies for use in resourcepoor countries. It should also be noted that because of continued migration, these diseases are now becoming increasingly common in large multiethnic cities in Europe and North America, making it a global health concern.15–18
Molecular and clinical formsAt the molecular level, haemoglobin synthesis is controlled by two multigene clusters on chromosome 16 (encoding
Published Online July 31, 2017 http://dx.doi.org/10.1016/S0140-6736(17)31822-6
Department of Internal Medicine, American University of Beirut Medical Centre, Beirut, Lebanon (Prof A T Taher MD); MRC Weatherall Institute of Molecular Medicine, University of Oxford, Oxford, UK (Sir D J Weatherall MD); and Department of Clinical Sciences and Community, University of Milan, IRCCS Ca’Granda Foundation Maggiore Policlinico Hospital, Milan, Italy (Prof M D Cappellini MD)
Correspondence to: Prof Ali T Taher, Department of Internal Medicine, American University of Beirut Medical Center, PO Box 11–0236, Beirut 11072020, Lebanon [email protected]
Search strategy and selection criteria
We searched PubMed using the terms “thalassaemia OR thalassemia” in combination with “molecular” or “epidemiology” or “diagnosis” or “pathophysiology” or “clinical complications” or “treatment OR management”. We limited our search to publications in English. We mostly selected publications from January, 2006, to May, 2017, but did not exclude frequently referenced and highly regarded older publications. We also searched the reference lists of articles identified by this search strategy and selected the most relevant ones. Review articles and book chapters are cited to provide readers with more details and more references than can be addressed in this Seminar.

Seminar
2 www.thelancet.com Published online July 31, 2017 http://dx.doi.org/10.1016/S0140-6736(17)31822-6
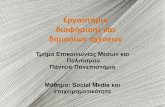
the αlike globins) and on chromosome 11 (encoding the βlike globins; figure 1).19,20 The genes in such clusters are arranged along the chromosome in the order that they are expressed during development to produce different haemoglobin tetramers during embryonic, fetal, and adult life. The high homology of the αglobin genes can result in unequalmeiotic cross over, which is the basis for the deletions that cause the αthalassaemias discussed later in this section. Within the βglobin gene cluster, the εgene is expressed only in early embryos, and downstream from this gene are two γgenes, the product of which is found in fetal haemoglobin (Hb F, α2γ2)—the haemoglobin form that predominates throughout most of gestation. The δgene product forms a minor haemoglobin component, Hb A2 (α2δ2), which is useful in the diagnosis of the thalassaemias. The βgene product combines with
αglobin to form Hb A (α2β2), the major haemoglobin component of adult red blood cells. During the first month of gestation, embryonic haemoglobins β2ε2, α2ε2, and β2γ2 are formed in erythroid cells located primarily in the yolk sac. During the remainder of fetal life, the sites of erythropoiesis gradually shift from the liver and spleen to the bone marrow, with red blood cells mainly containing Hb F (α2γ2). A switch from γglobin to βglobin expression begins before birth and completes by the time the baby reaches 6 months of age. After this time over 95% of the haemoglobin in normal red blood cells is adult Hb A (α2β2), with the remaining haemoglobin consisting of two minor components, Hb A2 and Hb F.19,20 Hb F is usually confined to a small number of red blood cells known as F cells. Underlying molecular defects in the αglobin or βglobin gene clusters form the basis of defective haemoglobin synthesis and the various inherited forms of αthalassaemias or βthalassaemias. The type and severity of these clinical forms can also rely on additional and independent intrinsic and extrinsic factors, which will be explained in this section. The thalassaemias can also manifest from coinheritance of βthalassaemia and structural haemoglobin variants like haemoglobin S, C, and E.11,21 Several clinically recognisable forms of haemoglobin S/βthalassaemia and haemoglobin C/βthalassaemia exist, each of which have unique character istics and management peculiarities;20 however, these will not be covered in this seminar.
β-ThalassaemiaPatients with βthalassaemia have been typically categorised as minor, major, or intermedia on the basis of their αglobin or βglobin chain imbalance, severity of anaemia, and clinical picture at presentation. Over 200 mutations in the βglobin gene that cause disease have been recognised, ranging from silent mutations (silent β), to mild mutations that cause a relative reduction in βglobin chain production (β+), to severe mutations that result in complete absence of βglobin chain synthesis (β0), with deletions of the gene being uncommon.22 βThalassaemia minor (trait or carrier) represents the heterozygous inheritance of a βthalassaemia mutation, with patients often having clinicallyasymptomaticmicrocytic anaemia, although others can have no identified haematological abnormalities—socalled silent carriers. Patients with βthalassaemia major usually present with severe anaemia in infancy and become transfusion dependent for life, whereas patients with βthalassaemia intermedia can present later in life with mildtomoderate anaemia and variable transfusion requirements.23–25 Both βthalassaemia major and intermedia can result from the homozygous or compoundheterozygous inheritance of mutations in the βglobin gene.
Several modifications can result in patients having βthalassaemia intermedia rather than major, including the extent of the αglobin to βglobin chain imbalance, ineffectiveness of erythropoiesis, and the resulting
Figure 1: Globin synthesis at the molecular level(A) Organisation of the α-globin family on chromosome 16 and the β-globin family on chromosome 11. (B) The sites of erythropoiesis and the pattern of globin synthesis during development. ψ designates non-expressing pseudogenes. The three exons of the globin genes are shown in pale blue. Reproduced from Bunn and colleagues19 with permission from McGraw-Hill Education. IVS=intervening segments (or introns).
50B
A
40
30
20
10
Site of erythropoiesis
Bone marrowLiver
Yolk sac
Spleen
Birth
α
γ
β
ε
ξ
β
γ
6 12 302418 636 121 18 24 30 36 4842
Postconceptual age (weeks) Postnatal age (weeks)
Tota
l glo
bin
synt
hesis
(%)
5’
5’ 3’
5 kb
α1 α1α2ψξξ
5’
11
16
3’Gγε ψβ
ψ
1ψβ2 βδΑγ
3’
5’ IVS-I IVS-II 3’
IVS-I IVS-II

Seminar
www.thelancet.com Published online July 31, 2017 http://dx.doi.org/10.1016/S0140-6736(17)31822-6 3
anaemia. The primary modifier is the severity of the mutation or mutations in the βglobin gene. Secondary modifiers include coinheritance of αthalas saemia, and increased synthesis of γchains and fetal haemoglobin production after infancy.22–26 Some rare forms of β thalassaemia intermedia result from deletions removing the upstreamregulatory elements, but leaving the globin genes intact. Other rare mutations linked on the same chromosome have been important in developing our understanding of how the switch from γglobin to βglobin gene expression is regulated. All these mutations result in variable concentrations of increased γglobin expression and increased concentrations of fetal haemoglobin, leading to what is known as hereditary persistence of fetal haemoglobin. Other forms of hereditary persistence of fetal haemoglobin result from deletions removing the adult δglobin and βglobin genes, but leaving at least one γglobin gene intact (δβthalassaemia).19,20 Tertiary modifiers include genetic and environmental factors that alter specific complication rates.23–25,27 βThalassaemia intermedia might also result from the increased production of αglobin chains by a triplicated or quadruplicated αgenotype associated with βheterozygosity, or when a single βglobin locus is affected and the other is completely normal (dominant inclusion body βthalassaemia).23–25 When βthalassaemia is coinherited with the structural variant haemoglobin E (haemoglobin E/βthalassaemia), which results in βglobin chain synthesis similar to a mild βgene mutation, the resulting clinical forms can also be of varying severity depending on age and the degree of anaemia at presentation. The clinical forms of haemoglobin E/βthalassaemia are commonly classified as mild, moderate, and severe, with the severe form being similar to βthalassaemia major, and the mild and moderate forms being similar to βthalassaemia intermedia.28,29 The same primary, secondary, and tertiary genetic and environmental modifiers are also relevant in the case of haemoglobin E/βthalassaemia, and influence the clinical severity of the disease.30,31
α-ThalassaemiaαThalassaemia has two main forms, α+thalassaemia and α⁰thalassaemia, and their classifications depend on whether one or both of the linked αglobin genes are deleted or reduced in activity by mutation. The two common forms of α+thalassaemia are designated –α³·⁷ and –α⁴·² to describe the lengths of the underlying deletions. α+Thalassaemia has several forms that result from point mutations, the most common being caused by the chaintermination mutant haemoglobin Constant Spring, designated αCSα. In their heterozygous state these conditions are silent and in their homozygous state they are characterised by mildhypochromic anaemia. α⁰Thalassaemias are usually caused by the deletion of both the linked αglobin genes and are designated by the place of discovery of the first case (eg, –Med and –SEA, reflecting the first cases to have been found in the
Mediterranean region and southeast Asia). The compound heterozygous states for α+thalassaemia and α⁰thalassaemia, –α/— or αCSα/—, result in a large excess of βchain production with the formation of β4 tetramers, designated as haemoglobin H. These β4 tetramers are a highly unstable variant of the βchain and they precipitate in red blood cells causing haemoglobin H disease, which is characterised by variably severe haemolysis and consequent anaemia. The homozygous state for α⁰thalassaemia, —/—, results in the production of tetramers of γchains (γ4) known as haemoglobin Bart’s, named after the hospital in London, UK, where it was first discovered. This homozygous state of α⁰thalassaemia is associated with a condition called haemoglobin Bart’s Hydrops fetalis, which is usually characterised by death in utero or just after birth. Rarer causes of αthalassaemias include deletions or mutations of regulatory mutations involving the αglobin gene cluster.4,17
There is another group of αthalassaemias that, unlike those described above, occur in no particular ethnic groups. They are described under the general title of αthalassaemia and mental retardation. One thalassaemia in this group is known as ATR16 syndrome. This syndrome involves the whole αglobin gene complex on chromosome 16 and is associated with mildtomoderate mental retardation. Another member of this group is known as αthalassaemia Xlinked intellectual disability (ATRX) syndrome and results from mutations of the ATRX gene leading to severe developmental abnormalities, facial dysmorphism, and other disorders in addition to its αthalassaemia phenotype. Finally, there is another form of mild hemoglobin H disease that occurs predominantly in men and is associated with a form of myelodysplastic syndrome and preleukaemia, which has also been found to be associated with mutations involving ATRX.17
Screening and diagnosisScreening and prevention programmes for thalassaemia are now widespread, with their adoption being dependent on regional distribution and cultural factors. Programmes of nationwide screening, and premarital and neonatal screenings have been implemented. Confirmation of a thalassaemia diagnosis requires analysis of red blood cells combined with haemoglobin electrophoresis, with DNA analysis required to confirm the diagnosis of αthalassaemia and haemoglobin E. Specific guidance on the pathway to establish a thalassaemia diagnosis has been reviewed elsewhere and is available from recent clinical management guidelines.23,32,33
Clinical classificationOver the past decade, a gradual transition in the labelling of the thalassaemias has occurred, moving away from the molecular forms to a more simplified categorisation largely based on clinicalmanagement criteria. Transfusion therapy remains the basis of management for these disorders, and the frequency and magnitude of transfusion

Seminar
4 www.thelancet.com Published online July 31, 2017 http://dx.doi.org/10.1016/S0140-6736(17)31822-6
requirements indirectly reflects the underlying severity of the disease. Moreover, transfusion therapy is not only able to control most of the underlying pathophysiological mechanisms but it also contributes a great deal to secondary morbidity.23,33 Thus, patients today are commonly categorised as having transfusiondependent thalassaemia (TDT)—patients who are not capable of producing sufficient haemoglobin to survive without blood transfusions—or nontransfusiondependent thalassaemia (NTDT).23,33 However, several points of caution should be highlighted when using such categorisations. For instance, patients with NTDT can still require transfusion therapy sporadically, or even regularly, but not for their entire lifetime. This treatment would be for the prevention or management of certain disease manifestations—and will be illustrated in subsequent sections—whereas patients with TDT require lifelong transfusion treatment for survival. Patients with βthalassaemia intermedia, haemoglobin H disease, and mildtomoderate forms of haemoglobin E/βthalassaemia often fall under the classification of NTDT; whereas patients with βthalassaemia major and severe forms of haemoglobin E/βthalassaemia are classified as having TDT.23,24,33 Additionally, it should be noted that some patients categorised as having TDT might have been misclassified. For instance, if transfusions had been started to treat low haemoglobin concentrations as a result of an acute complication (eg, an infection) in childhood, and the patient’s transfusion requirements had not been revisited and the transfusions thus never halted.34 Also, it should be highlighted that TDT and NTDT are fluid categories based on clinical variables and a patient might move from one group to another as a result of variations and advances in clinical management, or because of changes in other disease modifiers—thus these designations should primarily represent a patient’s current clinical status with the understanding that the categories are interchangeable.23,24,33,34
Pathophysiology and associated morbidityThe underlying disease process in patients with thalassaemia remains similar for those patients categorised as
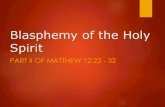
having NTDT or TDT, and the role of transfusion therapy in ameliorating much of these pathogenic mechanisms (while introducing other secondary complications) is best illustrated in studies showing the different morbidity profile between the two catagories.24,35 The hallmarks of the disease—with or without treatment—are the αglobin or βglobin chain imbalance leading to ineffective erythropoiesis, an array of subsequent pathophysiological mechanisms, and a multimorbidity profile (figure 2).24,36 In βthalassaemia, accumulation of unstable αglobin chain tetramers in erythroid cells leads to premature cell death inside (ineffective erythropoiesis) and outside (peripheral haemolysis) the bone marrow, facilitated by reactiveoxygenspecies formation and structuralmembrane deformities leading to senescenceantigen exposure.37,38 The immediate resulting manifestation is chronichaemolytic anaemia that can result in acute compli cations such as cholelithiasis and shortterm and longterm detrimental effects on growth, organ, and vascular function.39 Increased proliferation of erythroid precursors in the bone marrow leads to medullary expansion and subsequent bone deformities and low bone mass.37 Compensatory haemo poietic points out side the bone marrow are also activated, primarily in the spleen (splenomegaly) and liver (hepatomegaly), but can also be activated in any body tissues with haemopoietic potential, leading to the formation of extramedullary pseudotumours in highrisk anatomic locations such as the spinal canal.40 The exposure of erythroid cells to senescence antigens, such as phosphatidylserine, during ineffective erythro poiesis gives them prothrombotic potential. Alongside other abnor malities in platelets and the coagulation system, hyper coagulability and associated vascular mani festations like venous thrombosis and pulmonary hypertension are commonly seen in patients with thalassaemia, especially in patients who have been splenectomised and in whom such markers are further elevated.41 Finally, ineffective erythropoiesis results in increased iron absorption and primary iron overload mediated by the hepatic hormone hepcidin. An erythroid factor has been postulated as communicating to the liver the need of iron for the incoming red blood cells. This factor would be produced
Figure 2: Pathophysiology of patients with thalassaemia syndromes
Marrow expansion and bone disease
Extramedullary haemopoiesis and organomegaly
Peripheral haemolysis and gall stones
Organ damage (heart, liver, endocrine)
Hypercoagulability and vascular disease
α/β-Chain imbalance Ineffective erythropoiesis
Iron overload
Anaemia

Seminar
www.thelancet.com Published online July 31, 2017 http://dx.doi.org/10.1016/S0140-6736(17)31822-6 5
by erythroid cells, especially under the condition of ineffective erythro poiesis, and acts to suppress hepcidin synthesis in the liver, leading to increased intestinal iron absorption and increased release of recycled iron from the reticulo endothelial system. Various erythroid factors have been investigated, including growth differentiation factor 15 (GDF15), twistedgastrulation 1 (TWSG1), and erythroferrone (ERFE); although only ERFE was shown to be increased in animals with βthalassaemia compared with those without βthalassaemia.42,43 Such iron overload concen trations can reach clinically significant thresholds and lead to morbidities in various organ systems, especially the liver.44 Notably, both anaemia and iron overload can also further worsen ineffective erythropoiesis and complicate patho physiology.42,43 In patients with αthalassaemia, the concepts of αchain to βchain imbalance and ineffective erythropoiesis is similar to βthalassaemia. βGlobin chains can form soluble tetramers—β4, or haemoglobin H—that precipitate within the cell forming insoluble inclusions (Heinz bodies) that damage the red blood cell’s membrane. Although downstream manifestations like primary iron overload and hypercoagulability exist, they tend to be milder in patients with αthalassaemia than in patients with βthalassaemia, and the key pathological mechanism is peripheral haemolysis and chronic anaemia, rather than ineffective erythropoiesis, as is seen in patients with βthalassaemia.24,36
Since adequate and regular transfusion therapy can be considered part of the disease profile of patients with TDT, it is fair to say that the majority of these patho genic mechanisms and associated morbidities are more commonly encountered in patients with NTDT.24,35 Whereas adverse transfusionrelated complications, including secondaryiron overload and subsequent organ dysfunction, have become hallmarks of clinical morbidity in well transfused patients with TDT.45 Clinical aspects of all such morbidities in patients with thalassaemia are further highlighted in the relevant management sections below.
Conventional managementWithout intervention, any form of thalassaemia (excluding carrier status) is a progressive disease with increased morbidity as the patient advances in age.46 Moreover, the availability of effective therapeutic options and improved patient survival could allow multiple morbidities to manifest with age and the quality of life of the patient to deteriorate.47,48 Adult and elderly patients (older than 40 years) with thalassaemia should also be considered at risk of diseases that are common in nonthalassaemic populations, such as cancer and cardiovascular disease. Management guidelines for both patients with TDT and, more recently, NTDT, are available as part of the global efforts of the Thalassaemia International Federation to improve the outcomes of patients affected by these disorders.23,33
TransfusionTransfusion therapy works by supplying normal erythrocytes and suppressing ineffective erythropoiesis, essentially controlling all downstream pathophysiological mechanisms in thalassaemia.49–51 Advances in transfusion and ironchelation therapy were associated with improvements in survival in longterm followup studies evaluating different birth cohorts of patients with βthalassaemia major.52,53 Blood product screening, preparation, and administration practices have largely improved over the past 3 decades,53,54 and nowadays most patients with TDT can successfully achieve target haemoglobin concentrations of 90–105 g/L (110–120 g/L in those with heart disease); although access to blood for transfusion therapy remains a challenge in resourcepoor countries and poses a substantial public health burden.33 In patients with NTDT, however, the indicators for when blood transfusion is necessary are not as well established, although increased morbidity has been identified in patients with βthalassaemia intermedia who have haemoglobin concentrations of less than 100 g/L.39 Transfusions are sporadically given to patients when under acute stress or experiencing a drop in haemoglobin concentration, such as during infections, pregnancy, or surgery. Some patients are maintained on a regular transfusion programme following these incidents—a practice that in many cases might not be clinically indicated. Haemoglobin concentrations in isolation should not be an indication for lifelong, regular transfusions in patients with NTDT, especially given that many patients can adapt to their chronic anaemia without substantial bone marrow stress.55,56 Nonetheless, a role for regular transfusion therapy for a period of months or years has been established in patients with NTDT. Although data have emerged from observational studies reporting improved growth variables in children, and a lower proportion of morbidities in regularly transfused adults than in those not regularly transfused, especially in patients with βthalassaemia intermedia patients, including leg ulcers, thrombotic events, pulmonary hypertension, silent strokes, and extramedullary haemopoietic pseudo tumours.23,34,55–61 Collectively, these data might explain the differential clinical picture and increased proportion of such morbidities in patients with NTDT than in those with TDT.24,25,35 Transfusion therapy, however, does not come without its own sideeffects. Although the risks of alloimmunisation and bloodborne infection remain a concern in transfused patients, the greatest challenge with regular transfusion therapy is secondaryiron overload.23,33
The human body has no means to excrete iron. Transfused blood contains around 200–250 mg of iron per unit. Patients receiving 2–4 units of blood per month will have an annual accumulation of 5000–10 000 mg of iron or 0·3–0·6 mg/kg per day.33,62 With continued transfusions, the reticuloendothelial system—primarily in the liver—

Seminar
6 www.thelancet.com Published online July 31, 2017 http://dx.doi.org/10.1016/S0140-6736(17)31822-6
can no longer retain all the extra iron. Iron then enters the plasma in amounts that exceed the transport capacity of circulating transferrin. Consequentially, nontransferrinbound iron exists in the plasma as a heterogeneous mixture of iron complexes that appear to be the major mediators of hepatic and extrahepatic tissue damage in transfusional iron overload.63 Nontransferrinbound iron enters specific cells, particularly hepatocytes, cardiomyocytes, anterior pituitary cells, and pancreatic β cells. In these cells iron accumulation leads to the generation of reactiveoxygen species, resulting in damage to lipids, proteins, DNA, and subcellular organelles, including lysosomes and mitochondria. This injury can result in cellular dysfunction, apoptosis, and necrosis that translates into target organ toxicity and dysfunction.63 The clinical burden of iron overload and its management are further illustrated in the following section.
Iron chelationWhether iron overload develops from increased intestinal absorption—such as in patients with NTDT—or is secondary to regular transfusions, it can cause substantial morbidity and mortality, and so warrants prompt diagnosis and effective management. In patients with TDT, iron accumulation in organ tissues is evident in children aged as young as 2–6 years,64–67 with cumulative iron overload subsequently leading to organ toxiceffects and dysfunction, for instance in the heart, liver, or endocrine glands.33 Cardiomyopathy has been the leading cause of death in patients with TDT,33,52 although more recently large cohort studies68 have also highlighted the high incidence of mortality from hepatic causes in patients with TDT. Iron overload in patients with NTDT is a cumulative process with advancing age, and concerns over secondary morbidities start beyond the ages of 10–15 years.24,46,69,70 Although cardiac iron overload is commonly absent in patients with NTDT,71–74 an association between iron overload and hepatic fibrosis has been observed in patients with βthalassaemia intermedia,75 and the occurrence of hepatocellular carcinoma is increasingly being reported.76 Cumulative iron overload in patients with NTDT also increases their risk of developing thrombosis, pulmonary hypertension, silent strokes, hypo thyroidism, hypogonadism, osteo porosis, and renal disease, as is evident from studies in patients with βthalassaemia intermedia.61,69,77–81
Several methods are currently available for the diagnosis and monitoring of iron overload in patients with TDT and NTDT. Serum ferritin assessment is widely available and might be the only assessment that is affordable in resourcepoor countries. The assessment of serial serum ferritin concentrations can be a good indicator of iron chelator effectiveness,33 and available guidelines recommend measurement of serum ferritin concen trations every 3 months.23,33,82 Serum ferritin thresholds are commonly used to indicate the need for initiation or modification of ironchelation therapy. In patients with
TDT, maintaining concentrations lower than 1000 μg/L of ferritin is associated with lower morbidity and mortality, and this threshold is most commonly used to indicate the need for initiation of ironchelation therapy.33,52,83,84 Serum ferritin concentrations consistently higher than 2500 μg/L are associated with an increased risk of cardiac and endocrine disease, and thus are commonly used to flag the need for dose optimisation or a change in ironchelation therapy.33,83,84 However, although the association of high serum ferritin concentrations with hepatic siderosis is usually clear, a study85 using imaging techniques to evaluate organspecific iron overload failed to establish an association between serum ferritin concentrations and cardiac siderosis. Moreover, single measurements of serum ferritin concentration are prone to mis interpretation or not being representative of a patient’s condition, considering their high variability when a patient is experiencing inflammation, infection, vitamin C deficiency, hepatic dysfunction, and severe iron overload with values higher than 4000 μg/L.33,86 This high variability suggests that, when available and affordable, the use of imaging to evaluate organspecific siderosis should be recommended.33 Worth mentioning is that several case reports on patients with NTDT have confirmed that serum ferritin concentrations are commonly lower than in patients with TDT with the same hepatic iron concentration.87 In patients with NTDT (patients with β thalassaemia intermedia), concentrations of greater than 800 μg/L are associated with an increased risk of morbidity, and concentrations of less than 300 μg/L are associated with an absence of risk of morbidity. These thresholds are thus used to indicate the need for iron chelation initiation or interruption.23,69
Measurement of liver iron concentration has become common practice since the early 2000s, considering the strong correlation with totalbody iron stores.88 Initial reports relied primarily on the use of liver biopsy, although the technique is now used less frequently and only reserved for those situations when assessment of hepatic histology is needed.89 The use of a Superconducting Quantum Interference Device (SQUID) is also still practised, but the technology is only available in few centres worldwide.33,90 The introduction of MRI for the noninvasive assessment of liver iron concentration, and later myocardial iron concentration, is considered one of the most important advances in thalassaemia care over the past decade. The use of MRI in clinical practice can allow better tailoring of ironchelation therapy. For measurement of liver iron concentration, both the R2 and T2* techniques are used as they have been validated against liver biopsy measurements of iron.91,92 They are internationally reproducible and accurately measure liver iron concentration throughout the clinically relevant range with appropriate calibration and MRI acquisition techniques, and give a measurement of liver iron concentration in mg of iron per g of dry liver weight.93,94 They are also equally effective in evaluating chronic

Seminar
www.thelancet.com Published online July 31, 2017 http://dx.doi.org/10.1016/S0140-6736(17)31822-6 7
response to iron chelation.95,96 R2 MRI has also been validated in patients at different stages of liver fibrosis and grades of liver inflammation and the technique (FerriScan®, Resonance Health, Burswood, WA, Australia) is approved by the US Food and Drug Administration.94 Cardiac T2* MRI is used for the assessment of cardiac iron (values in ms), with recent validation against myocardial iron concentration in mg of iron per g of dry heart weight from postmortem cardiac biopsies.97 The use of both techniques to evaluate iron content in other organs—such as the endocrine gland—has also been investigated, although they are less commonly used in routine practice.98–100 Certain liver iron concentrations and cardiac T2* thresholds have been linked to morbidity in patients with thalassaemia. In patients with TDT, liver iron concentrations greater than 7 mg/g are usually used to indicate increased risks of complication, and lower target concentrations are used to prevent ironrelated complications, although this evidence has mainly been extrapolated from patients with hereditary haemochromatosis.101–103 Concentrations greater than 15 mg/g are associated with progressive liver fibrosis and cardiac mortality. Cardiac T2* values of less than 20 ms are indicative of a declining left ventricular ejection
fraction and associated with arrhythmias, whereas values of less than 10 ms are associated with clinical heart failure and mortality.104–106 Thus, these thresholds are commonly used to determine a patient’s ironoverload profile, to evaluate their response to ironchelation therapy in clinical trials, and to tailor their chelator type and dose in routine practice.33,107 In patients with NTDT (βthalassaemia intermedia), liver iron concentration values higher than 5 mg/g are associated with increased morbidity,78 supporting the recommendation of ironchelation initiation in patients showing liver iron concentrations greater than 5 mg/g.23 It should be noted that patients with αthalassaemia do tend to show slower rates of iron overload than patients with other NTDT forms, and lowerintensity iron chelation standards are usually considered. Most available guidelines recommend assessment every 6, 12, or 24 months depending on ironoverload severity and ironchelation adjustment needs.23,33,82
Three iron chelators are currently available for the treatment of iron overload in patients with thalassaemia: deferoxamine in subcutaneous or intravenous injection, oral deferiprone in tablet or solution form, and oral deferasirox in dispersible tablet and, more recently, filmcoated tablet forms (table 1), and guidelines for their use
Deferoxamine Deferiprone Deferasirox
Administration33
Method Subcutaneous or intravenous Oral Oral
Frequency 8–12 h, 5–7 days per week 3 times daily Once daily
Half-life of iron-free drug33 20–30 min 3–4 h 12–16 h
Lipid solubility33 Low Intermediate High
Route of iron excretion33 Urinary and faecal Urinary Faecal
Recommended dose23,33 30–60 mg/kg per day 75–100 mg/kg per day TDT: 20–40 mg/kg per day; NTDT: 5–20 mg/kg per day
TIF guidelines indication
TDT33 >2 years: first-line 2–6 years: no sufficient data; >6 years: second-line† 2–6 years: first-line (USA), second-line (EU); >6 years: first-line
NTDT23 No sufficient data No sufficient data >10 years: first-line
Most relevant clinical data
TDT33 Reduction in serum ferritin and liver iron concentration;108 improvement in cardiac T2*;108 improvement in cardiac dysfunction with continuous infusion109
Improvement of cardiac T2* in monotherapy or in combination with deferoxamine (higher doses than commonly used in clinical practice)‡;110,111 improvement in cardiac dysfunction in combination with deferoxamine†‡;112 improvement in endocrine dysfunction in combination with deferoxamine or deferasirox113,114
Reduction in serum ferritin and liver iron concentration after up to 5 years, and cardiac T2* after up to 3 years of therapy, even in patients with severe iron overload;115–118 not inferior to deferoxamine for improving cardiac T2*;108 improvements in hepatic fibrosis and inflammation;119 stabilisation of heart function;108,115 stabilisation of endocrine function120
NTDT23 Data restricted to case series and small studies
Data restricted to case series and small studies Significant reduction in serum ferritin and liver iron concentration after up to 2 years of therapy121
Main adverse events33 Ocular and auditory symptoms, bone-growth retardation, local reactions, allergy
Gastrointestinal symptoms, arthralgia, agranulocytosis or neutropenia
Gastrointestinal symptoms, increased creatinine, increased hepatic enzymes
Pregnancy33 Contraindicated (but has been used in third trimester)
Contraindicated Contraindicated
TDT=transfusion-dependent thalassaemia. NTDT=non-transfusion-dependent thalassaemia. TIF=Thalassaemia International Federation. †In a recent Cochrane review122 it was concluded that in the absence of data from randomised controlled trials, there is no evidence to suggest the need for a change in the current treatment recommendations. Specifically, deferiprone is indicated for treating iron overload in patients with thalassaemia major when deferoxamine is contraindicated or inadequate. Intensified deferoxamine treatment, use of other oral iron chelators, or both, remains the established treatment to reverse cardiac dysfunction due to iron overload. ‡Despite results of some trials110,111 indicating the superiority of deferiprone, or its combination with deferoxamine, compared with deferoxamine monotherapy in improving cardiac T2*, a meta-analysis123 concluded that deferoxamine and deferiprone monotherapy appeared to reduce myocardial iron by similar amounts. Moreover, the addition of deferiprone to deferoxamine in a recent study124 did not enhance its ability to improve cardiac dysfunction compared to monotherapy. There is an urgent need for high-quality trials to compare the overall clinical efficacy and long-term outcome of treatment with deferiprone combined with deferoxamine.122
Table 1: Characteristics and evidence on iron chelators for the management of iron overload in thalassaemia

Seminar
8 www.thelancet.com Published online July 31, 2017 http://dx.doi.org/10.1016/S0140-6736(17)31822-6
are now widely available.23,33,82 Data from several large, randomised trials since the development of MRI technology showed the efficacy and safety of oralironchelation therapy in removing iron from the liver and heart, which represents a considerable advance in patient management owing to the greater convenience compared to parenteral deferoxamine. However, parenteral deferoxamine remains the treatment of choice in patients with decompensated heart disease, and might be the only affordable option in resourcepoor countries.33 Nonetheless, the search for other novel iron chelators that can address the specific efficacy or safety shortcomings of these chelators continues.33 Moreover, successful manage ment of iron overload extends beyond chelator efficacy and safety. Ensuring adherence to treatment is essential, and applicable to most chelators irrespective of their administrative form. Adherence to ironchelation therapy correlates with both effective management and patient survival, as is evident from several studies.125,126 Moreover, appropriate dose determination and adjustment of the iron chelator according to baseline and ongoing iron intake is essential to ensure adequate response and avoid overchelation.33
SplenectomySplenectomies have traditionally been performed as an alternate or adjunct to transfusion therapy. Although some studies have found that splenectomies have resulted in improvements in growth, quality of life, and haemoglobin concentration for some patients with haemoglobin E/βthalassaemia.127 The procedure has now become almost obsolete in patients with TDT, especially in the context of improved access to and safety of blood transfusions with regards to bloodborne infections. The procedure is still more commonly used in patients with NTDT, because it might be enough to improve mildtomoderate anaemia and avoid the need for transfusions.25,31,34,57,58 However, data for serious adverse events caused by splenectomies continue to accumulate in the thalassaemia patient population, alongside the known risk of infection and sepsis. Removal of the spleen promotes a hypercoagulable state in thalassaemia because of the decreased ability to scavenge procoagulant red blood cells and activated platelets. Observational studies have further established that splenectomised NTDT patients are at a 4–5 fold increased risk of overt venous thrombosis and other vascular manifestations like pulmonary hypertension, leg ulcers, and silent strokes than nonsplenectomised patients.60,61 In patients with βthalassaemia intermedia, the longterm risk of thrombosis is further increased in those with concomitant high counts of nucleated red blood cells (≥300 × 10⁶ cells per L) and platelets (≥500 × 10⁹ platelets per L), and those patients who never received any transfusions.128 The spleen also usually acts as a reservoir for scavengers of toxic iron in the body, and so removal of the spleen could also decrease the ability of these scavengers, thus putting patients at increased risk of endorgan damage.60 The current recommendations for splenectomy are restricted to those patients with an inability to receive transfusion and ironchelation therapy, as well as those with clinically symptomatic splenomegaly or hyper splenism.23,33 When indicated, appropriate treatment with vaccination and antibiotics is recommended, and prophylaxis with aspirin or lowmolecular weight heparins for highrisk patients.23,33
Management of specific morbiditiesPrevention of morbidity in patients with thalassaemia starts with appropriate and adequate application of conventional therapies including transfusion or iron chelation, or both.23,33 Special clinical considerations and management options beyond conventional therapy are summarised in table 2 for key clinical complications.
Haemopoietic stem-cell transplantationReplacement of mutant haemopoietic cells using haemopoietic stemcell transplantation is the only existing curative therapy for thalassaemia and is now an established approach to correct defective erythropoiesis, particularly when matched sibling donors are available.
Assessment considerations (indication) Management considerations
Cardiac dysfunction and arrhythmia
Echocardiography (routine), electrocardiogram (routine)
As per standard care
Pulmonary hypertension
Tricuspid regurgitant jet velocity (routine), right-heart catheterisation (high risk)
As per standard care, sildenafil citrate, bosentan
Cerebrovascular events
MRI and MRA (high risk) As per standard care, antiplatelet prophylaxis
Venous thrombosis Standard imaging (suggestive of signs and symptoms)
Anticoagulant therapy, medical and surgical prophylaxis
Leg ulcers Physical examination (routine) Topical measures, pentoxifylline, hydroxycarbamide, hyperoxygenation
Viral hepatitis Viral serology (routine in transfused patients), viral RNA-PCR (if positive serology)
Hepatitis B vaccination, antiviral therapy
Hepatic fibrosis, cirrhosis, and cancer
Live function tests (routine), ultrasound (high risk), α-fetoprotein (high risk), transient elastography (investigational)
As per standard care
Endocrine disease Growth retardation (routine), sexual development (routine), endocrine-function tests (routine), bone-mineral density (routine)
As per standard care
Bone disease Bone-mineral density (routine) As per standard care, bisphosphonates
Pregnancy As per high-risk pregnancy Revisit iron chelation, anticoagulation prophylaxis, maintenance of haemoglobin concentration and heart function
Extramedullary haematopoietic pseudotumours
Physical exam and imaging to rule out compression (suggestive signs and symptoms)
Hypertransfusion, radiation, surgery
Haemolytic crisis (haemoglobin H disease)
Infection screening, electrolytes Adequate hydration, correction of blood electrolytes, control body temperature, antibiotics or antivirals
The frequency and age at the start of assessment should rely on the underlying diagnosis and individual patient’s needs. Further management details are available in the respective Thalassaemia International Federation guidelines.23,33 MRA=magnetic resonance angiography.
Table 2: Management considerations for specific morbidities in thalassaemia patients beyond transfusion and iron chelation

Seminar
www.thelancet.com Published online July 31, 2017 http://dx.doi.org/10.1016/S0140-6736(17)31822-6 9
Haemopoietic stemcell transplantation is now widely applied with a diseasefree survival exceeding 80% with transplants from HLAmatchedsibling donors.129 Moreover, improvements in the management of graftversushost disease and inducing graft tolerance have encouraged the use of unrelated donors and umbilicalcord blood as the haemopoietic stemcell source for patients who do not have a matchedsibling donor. Nevertheless, matchedunrelated transplants for highrisk patients with thalassaemia have an overall survival of 65%. However, a 5–10% mortality from transplant conditioning, graftversushost disease, and graft failure continues to limit the acceptability of this treatment method. The need for complete myeloablation, which can result in infertility and other toxiceffects, is also a concern, although improved approaches with reducedintensity conditioning are being developed.130 Clinical guidelines specific to patients with thalassaemia are now available.129
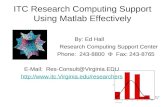
Future outlookIn the past decade several promising targets and associated therapeutic options have emerged for patients with thalassaemia, though primarily for those with βthalassaemia, which is reasonable considering the patient’s more complex and advanced management needs (figure 3).6,42,43 These therapeutic options can be classified into three major categories on the basis of their attempts to address different aspects of the underlying pathophysiology of thalassaemia: correction of globinchain imbalance, addressing ineffective erythro poiesis, and improving how the body handles iron. In this section, we will shortly discuss some of the emerging approaches in each of these areas.
Gene therapy is based on the idea that if there is a defect in the production of βglobin in βthalassaemia, exogenous production of βlike globins could correct the disorder. The haemopoietic system is convenient for such approaches, since haemopoietic stem cells from an individual with βthalassaemia can be isolated and transduced with viruses to introduce exogenous genetic
material, such as βlike globin transgenes that can allow for such exogenous gene expression. Following successful application in a few patients with thalassaemia,131 clinical trials have been initiated.
Several approaches are also being developed to address the αglobin or βglobin chain imbalance in patients with thalassaemia by stimulation of γglobin production.26 Although many small trials have examined the use of currently available cytotoxic agents, such as hydroxycarbamide, there is a scarcity of published results and studies.132 The limitations of the currently available approaches to address the αglobin or βglobin chain imbalance have motivated a considerable amount of research into better understanding the molecular regulation of γglobin. In recent years, humangenetic studies have provided important insights into this area and have suggested several promising molecular targets, such as BCL11A, which is a transcription factor capable of silencing the γglobin genes specifically without affecting production of red blood cells.26 Instead of gene therapy, recent approaches have been developed to directly correct genetic mutations in the endogenous DNA of the cell or to disrupt specific DNA sequences in the genome. This approach is known as genome editing and has been facilitated through the identification of several enzymes, including CRISPR/Cas9, that can introduce DNA breaks in specific regions of the genome. Although it is challenging to envision correcting every one of the hundreds–thousands of mutations that cause βthalassaemia, disruption of factors that silence the γglobin genes, such as BCL11A, might allow more immediate treatment of βthalassaemia with current genome editing approaches.6
Ineffective erythropoiesis is the major contributor to the anaemia observed in patients with βthalassaemia. In the past few years, a group of ligand traps (which include sotatercept and luspatercept) have been developed that have shown potent stimulation of latestage erythropoiesis and improved ineffective erythropoiesis in patients with βthalassaemia.6,133,134 Ongoing clinical studies of these drugs are evaluating their role in reducing transfusion
Figure 3: Novel targets and therapies for patients with β-thalassaemiaEPO=erythropoietin. ROS=reactive-oxygen species.
α/β-Chain imbalance Ineffective erythropoiesis
Minihepcidins
JAK2 inhibitors
SotaterceptLuspatercept
Gene therapyGene editing
TMPRSS inhibitors
TMPRSS6↓ Differentiation ↓ Hepcidin
↑ Proliferation
↑ ROS
↑ EPO
↑ GDF11
Anaemia
Iron overload
Erythroferrone

Seminar
10 www.thelancet.com Published online July 31, 2017 http://dx.doi.org/10.1016/S0140-6736(17)31822-6
requirements and raising haemoglobin concentrations in patients with TDT and NTDT, respectively. JAK2 inhibition, an established therapy in patients with myeloproliferative disorders, can also ameliorate ineffective erythropoiesis and decrease spleen size in mice with thalassaemia, which has motivated ongoing clinical trials in this area to evaluate the role of JAK2 in patients with TDT.43
In NTDT mouse models, moderate transgenic hepcidin expression decreased iron loading in the liver, and resulted in an extended red blood cell lifespan, increased haemoglobin concentrations and amelioration of splenomegaly.43,135 Recent preclinical studies43,136 have suggested that longacting hepcidin analogues (minihepcidins) could be beneficial to restrict iron absorption and use in the setting of iron overload, with beneficial effects on ineffective erythropoiesis. If such molecules are developed for clinical use, these could help to further restrict iron overload either alone or in combination with currently available iron chelators. An alternative approach is to stimulate endogenous hepcidin prod uction through the downregulation of a metallo protease, TMPRSS6, that plays a key role in hepcidin expression.137 Antisense oligonucleotides and siRNAs targeting TMPRSS6 have been effectively used to stimulate hepcidin, reduce the iron burden, and improve in effective erythropoiesis and red blood cell survival in preclinical ironoverload models138,139—clinical trials are expected soon.
Concluding remarksOur improved understanding of the pathophysiology and disease burden in patients with thalassaemia has helped optimise disease management and construct a plan for the development of novel therapeutics. With several treatment options available, the need for comparative and combinative clinical trials is essential to design the best management approach. Nonetheless, the complexity of thalassaemia as a disease might always imply the need for individualised therapy, and offering the right treatment approach to the right patient. The equal prioritisation of efforts to promote the prevention of thalassaemia births through nationwide screening programmes and premarital policy adaptations should also be addressed. Successful examples of a remarkable decline in disease incidence from the Mediterranean should aim to be reproduced in resourcepoor countries where the disease continues to pose public health concerns. This effort, however, will require challenges attributed to economic, cultural, and religious differences to be addressed with innovative approaches to premarital and prenatal counselling. Expandededucation pro grammes and healthcaresystem awareness are also needed nowadays in highincome communities where thalassaemias were, until recently, not commonly present. Lastly, collaborations and partnerships between centres for the exchange of expertise and resources could help improve the diagnosis and management of the thalassaemias, especially in lowincome countries where they are most common.
ContributorsATT, DJW, and MDC participated in the literature search, manuscript drafting, and review. All authors approved the final manuscript before submission.
Declaration of interestsATT and MDC report grants and personal fees from Novartis and Celgene, outside the submitted work. DJW declares no competing interests.
AcknowledgmentsWe thank Khaled Musallam and Vijay Sankaran for their constructive review of this manuscript. We apologise to those authors whose work could not be cited in this review because of space limitations.
References1 Cooley TB, Lee P. A series of cases of splenomegaly in children and
peculiar changes in bones; report of cases. Am J Dis Child 1927; 34: 347–63
2 Olivieri NF. The betathalassemias. N Engl J Med 1999; 341: 99–109.3 Rund D, Rachmilewitz E. Betathalassemia. N Engl J Med 2005;
353: 1135–46.4 Piel FB, Weatherall DJ. The αthalassemias. N Engl J Med 2014;
371: 1908–16.5 Sankaran VG, Nathan DG. Thalassemia: an overview of 50 years
of clinical research. Hematol Oncol Clin North Am 2010; 24: 1005–20.
6 Sankaran VG, Weiss MJ. Anemia: progress in molecular mechanisms and therapies. Nat Med 2015; 21: 221–30.
7 Weatherall DJ, Williams TN, Allen SJ, O’Donnell A. The population genetics and dynamics of the thalassemias. Hematol Oncol Clin North Am 2010; 24: 1021–31.
8 Weatherall DJ. The inherited diseases of hemoglobin are an emerging global health burden. Blood 2010; 115: 4331–36.
9 Christianson A, Howson CP, Modell B. March of dimes global report on birth defects. The hidden toll of dying and disabled children. White Plains, New York: March of Dimes Birth Defects Foundation, 2006.
10 Modell B, Darlison M. Global epidemiology of haemoglobin disorders and derived service indicators. Bull World Health Organ 2008; 86: 480–87.
11 Weatherall DJ, Clegg JB. The thalassaemia syndromes. 4th edn. Oxford: Blackwell Science, 2001.
12 Olivieri NF, Pakbaz Z, Vichinsky E. Hb E/betathalassaemia: a common & clinically diverse disorder. Indian J Med Res 2011; 134: 522–31.
13 Cohen AR, Galanello R, Pennell DJ, Cunningham MJ, Vichinsky E. Thalassemia. Hematology Am Soc Hematol Educ Program 2004: 14–34.
14 Vichinsky E. Complexity of alpha thalassemia: growing health problem with new approaches to screening, diagnosis, and therapy. Ann N Y Acad Sci 2010; 1202: 180–87.
15 Lorey F, Cunningham G, Vichinsky EP, et al. Universal newborn screening for Hb H disease in California. Genet Test 2001; 5: 93–100.
16 Lorey F. Asian immigration and public health in California: thalassemia in newborns in California. J Pediatr Hematol Oncol 2000; 22: 564–66.
17 Harteveld CL, Higgs DR. Alphathalassaemia. Orphanet J Rare Dis 2010; 5: 13.
18 Michlitsch J, Azimi M, Hoppe C, et al. Newborn screening for hemoglobinopathies in California. Pediatr Blood Cancer 2009; 52: 486–90.
19 Bunn HF, Nathan DG. Thalassemia. In: Bunn HF, Aster JC, eds. Pathophysiology of blood disorders. New York: McGrawHill, 2011; 93–104.
20 Higgs DR, Engel JD, Stamatoyannopoulos G. Thalassaemia. Lancet 2012; 379: 373–83.
21 Steinberg MH, Forget BG, Higgs DR, Weatherall DJ. Disorders of hemoglobin: genetics, pathophysiology, and clinical management. 2nd edn. New York: Cambridge University Press, 2009.
22 Danjou F, Anni F, Galanello R. Betathalassemia: from genotype to phenotype. Haematologica 2011; 96: 1573–75.
23 Taher A, Vichinsky E, Musallam K, Cappellini MD, Viprakasit V. Guidelines for the management of non transfusion dependent thalassaemia (NTDT). Nicosia, Cyprus: Thalassaemia International Federation, 2013.

Seminar
www.thelancet.com Published online July 31, 2017 http://dx.doi.org/10.1016/S0140-6736(17)31822-6 11
24 Musallam KM, Rivella S, Vichinsky E, Rachmilewitz EA. Nontransfusiondependent thalassemias. Haematologica 2013; 98: 833–44.
25 Musallam KM, Taher AT, Rachmilewitz EA. βthalassemia intermedia: a clinical perspective. Cold Spring Harb Perspect Med 2012; 2: a013482.
26 Sankaran VG, Orkin SH. The switch from fetal to adult hemoglobin. Cold Spring Harb Perspect Med 2013; 3: a011643.
27 Weatherall D. 2003 William Allan award address. The thalassemias: the role of molecular genetics in an evolving global health problem. Am J Hum Genet 2004; 74: 385–92.
28 Galanello R, Origa R. Betathalassemia. Orphanet J Rare Dis 2010; 5: 11.
29 Sripichai O, Makarasara W, Munkongdee T, et al. A scoring system for the classification of betathalassemia/Hb E disease severity. Am J Hematol 2008; 83: 482–84.
30 Fucharoen S, Weatherall DJ. The hemoglobin E thalassemias. Cold Spring Harb Perspect Med 2012; 2: a011734
31 Olivieri NF. Treatment strategies for hemoglobin E betathalassemia. Blood Rev 2012; 26 (suppl 1): S28–30.
32 Viprakasit V, Tyan P, Rodmai S, Taher AT. Identification and key management of nontransfusiondependent thalassaemia patients: not a rare but potentially underrecognised condition. Orphanet J Rare Dis 2014; 9: 131.
33 Cappellini MD, Cohen A, Porter J, Taher A, Viprakasit V. Guidelines for the management of transfusion dependent thalassaemia (TDT). 3rd edn. Nicosia, Cyprus: Thalassaemia International Federation, 2014.
34 Taher AT, Musallam KM, Cappellini MD, Weatherall DJ. Optimal management of β thalassaemia intermedia. Br J Haematol 2011; 152: 512–23.
35 Taher A, Isma’eel H, Cappellini MD. Thalassemia intermedia: revisited. Blood Cells Mol Dis 2006; 37: 12–20.
36 Musallam KM, Taher AT, Duca L, Cesaretti C, Halawi R, Cappellini MD. Levels of growth differentiation factor15 are high and correlate with clinical severity in transfusionindependent patients with β thalassemia intermedia. Blood Cells Mol Dis 2011; 47: 232–34.
37 Rivella S. The role of ineffective erythropoiesis in nontransfusiondependent thalassemia. Blood Rev 2012; 26 (suppl 1): S12–15.
38 Rivella S. Ineffective erythropoiesis and thalassemias. Curr Opin Hematol 2009; 16: 187–94.
39 Taher AT, Musallam KM, Saliba AN, Garziadei G, Cappellini MD. Hemoglobin level and morbidity in nontransfusiondependent thalassemia. Blood Cells Mol Dis 2015; 55: 108–09.
40 Haidar R, Mhaidli H, Taher AT. Paraspinal extramedullary hematopoiesis in patients with thalassemia intermedia. Eur Spine J 2010; 19: 871–78.
41 Cappellini MD, Poggiali E, Taher AT, Musallam KM. Hypercoagulability in βthalassemia: a status quo. Expert Rev Hematol 2012; 5: 505–11; quiz 12.
42 Camaschella C, Nai A. Ineffective erythropoiesis and regulation of iron status in iron loading anaemias. Br J Haematol 2016; 172: 512–23
43 Rivella S. βthalassemias: paradigmatic diseases for scientific discoveries and development of innovative therapies. Haematologica 2015; 100: 418–30.
44 Musallam KM, Cappellini MD, Wood JC, Taher AT. Iron overload in nontransfusiondependent thalassemia: a clinical perspective. Blood Rev 2012; 26 (suppl 1): S16–19.
45 Rund D. Thalassemia 2016: modern medicine battles an ancient disease. Am J Hematol 2016; 91: 15–21.
46 Taher AT, Musallam KM, ElBeshlawy A, et al. Agerelated complications in treatmentnaïve patients with thalassaemia intermedia. Br J Haematol 2010; 150: 486–89.
47 Musallam KM, Khoury B, AbiHabib R, et al. Healthrelated quality of life in adults with transfusionindependent thalassaemia intermedia compared to regularly transfused thalassaemia major: new insights. Eur J Haematol 2011; 87: 73–79.
48 Haines D, Martin M, Carson S, et al. Pain in thalassaemia: the effects of age on pain frequency and severity. Br J Haematol 2013; 160: 680–87.
49 Cazzola M, Finch CA. Evaluation of erythroid marrow function in anemic patients. Haematologica 1987; 72: 195–200.
50 Cazzola M, Pootrakul P, Huebers HA, Eng M, Eschbach J, Finch CA. Erythroid marrow function in anemic patients. Blood 1987; 69: 296–301.
51 Cazzola M, De Stefano P, Ponchio L, et al. Relationship between transfusion regimen and suppression of erythropoiesis in betathalassaemia major. Br J Haematol 1995; 89: 473–78.
52 BorgnaPignatti C, Rugolotto S, De Stefano P, et al. Survival and complications in patients with thalassemia major treated with transfusion and deferoxamine. Haematologica 2004; 89: 1187–93.
53 Modell B, Khan M, Darlison M. Survival in βthalassaemia major in the UK: data from the UK Thalassaemia Register. Lancet 2000; 355: 2051–52.
54 Cao A. Quality of life and survival of patients with betathalassemia major. Haematologica 2004; 89: 1157–59.
55 O’Donnell A, Premawardhena A, Arambepola M, et al. Agerelated changes in adaptation to severe anemia in childhood in developing countries. Proc Natl Acad Sci U S A 2007; 104: 9440–44.
56 Allen A, Fisher C, Premawardhena A, et al. Adaptation to anemia in hemoglobin Eβ thalassemia. Blood 2010; 116: 5368–70.
57 Olivieri NF, Muraca GM, O’Donnell A, Premawardhena A, Fisher C, Weatherall DJ. Studies in haemoglobin E betathalassaemia. Br J Haematol 2008; 141: 388–97.
58 Vichinsky E. Advances in the treatment of alphathalassemia. Blood Rev 2012; 26 (suppl 1): S31–34.
59 Taher A, Isma’eel H, Mehio G, et al. Prevalence of thromboembolic events among 8,860 patients with thalassaemia major and intermedia in the Mediterranean area and Iran. Thromb Haemost 2006; 96: 488–91.
60 Taher AT, Musallam KM, Karimi M, et al. Overview on practices in thalassemia intermedia management aiming for lowering complication rates across a region of endemicity: the OPTIMAL CARE study. Blood 2010; 115: 1886–92.
61 Musallam KM, Taher AT, Karimi M, Rachmilewitz EA. Cerebral infarction in βthalassemia intermedia: breaking the silence. Thromb Res 2012; 130: 695–702.
62 Porter JB. Practical management of iron overload. Br J Haematol 2001; 115: 239–52.
63 Brittenham GM. Ironchelating therapy for transfusional iron overload. N Engl J Med 2011; 364: 146–56.
64 Berdoukas V, Nord A, Carson S, et al. Tissue iron evaluation in chronically transfused children shows significant levels of iron loading at a very young age. Am J Hematol 2013; 88: E283–85.
65 BorgnaPignatti C, Meloni A, Guerrini G, et al. Myocardial iron overload in thalassaemia major. How early to check? Br J Haematol 2014; 164: 579–85.
66 Wood JC, Origa R, Agus A, Matta G, Coates TD, Galanello R. Onset of cardiac iron loading in pediatric patients with thalassemia major. Haematologica 2008; 93: 917–20.
67 Yang G, Liu R, Peng P, et al. How early can myocardial iron overload occur in beta thalassemia major? PLoS One 2014; 9: e85379.
68 Voskaridou E, Ladis V, Kattamis A, et al. A national registry of haemoglobinopathies in Greece: deducted demographics, trends in mortality and affected births. Ann Hematol 2012; 91: 1451–58.
69 Musallam KM, Cappellini MD, Daar S, et al. Serum ferritin level and morbidity risk in transfusionindependent patients with βthalassemia intermedia: the ORIENT study. Haematologica 2014; 99: e218–21
70 Lal A, Goldrich ML, Haines DA, Azimi M, Singer ST, Vichinsky EP. Heterogeneity of hemoglobin H disease in childhood. N Engl J Med 2011; 364: 710–18.
71 Origa R, Barella S, Argiolas GM, Bina P, Agus A, Galanello R. No evidence of cardiac iron in 20 never or minimallytransfused patients with thalassemia intermedia. Haematologica 2008; 93: 1095–96.
72 Taher AT, Musallam KM, Wood JC, Cappellini MD. Magnetic resonance evaluation of hepatic and myocardial iron deposition in transfusionindependent thalassemia intermedia compared to regularly transfused thalassemia major patients. Am J Hematol 2010; 85: 288–90.
73 Roghi A, Cappellini MD, Wood JC, et al. Absence of cardiac siderosis despite hepatic iron overload in Italian patients with thalassemia intermedia: an MRI T2* study. Ann Hematol 2010; 89: 585–89.

Seminar
12 www.thelancet.com Published online July 31, 2017 http://dx.doi.org/10.1016/S0140-6736(17)31822-6
74 Mavrogeni S, Gotsis E, Ladis V, et al. Magnetic resonance evaluation of liver and myocardial iron deposition in thalassemia intermedia and bthalassemia major. Int J Cardiovasc Imaging 2008; 24: 849–54.
75 Musallam KM, Motta I, Salvatori M, et al. Longitudinal changes in serum ferritin levels correlate with measures of hepatic stiffness in transfusionindependent patients with βthalassemia intermedia. Blood Cells Mol Dis 2012; 49: 136–39.
76 Maakaron JE, Cappellini MD, Graziadei G, Ayache JB, Taher AT. Hepatocellular carcinoma in hepatitisnegative patients with thalassemia intermedia: a closer look at the role of siderosis. Ann Hepatol 2013; 12: 142–46.
77 Musallam KM, Cappellini MD, Wood JC, et al. Elevated liver iron concentration is a marker of increased morbidity in patients with β thalassemia intermedia. Haematologica 2011; 96: 1605–12.
78 Musallam KM, Cappellini MD, Taher AT. Evaluation of the 5mg/g liver iron concentration threshold and its association with morbidity in patients with βthalassemia intermedia. Blood Cells Mol Dis 2013; 51: 35–38.
79 Ziyadeh FN, Musallam KM, Mallat NS, et al. Glomerular hyperfiltration and Pproteinuria in transfusionindependent patients with βthalassemia intermedia. Nephron Clin Pract 2012; 121: c136–43.
80 Musallam KM, Beydoun A, Hourani R, et al. Brain magnetic resonance angiography in splenectomized adults with βthalassemia intermedia. Eur J Haematol 2011; 87: 539–46.
81 Musallam KM, Nasreddine W, Beydoun A, et al. Brain positron emission tomography in splenectomized adults with βthalassemia intermedia: uncovering yet another covert abnormality. Ann Hematol 2012; 91: 235–41.
82 Musallam KM, Angastiniotis M, Eleftheriou A, Porter JB. Crosstalk between available guidelines for the management of patients with betathalassemia major. Acta Haematol 2013; 130: 64–73.
83 Belhoul KM, Bakir ML, Saned MS, Kadhim AM, Musallam KM, Taher AT. Serum ferritin levels and endocrinopathy in medically treated patients with β thalassemia major. Ann Hematol 2012; 91: 1107–14.
84 Olivieri NF, Nathan DG, MacMillan JH, et al. Survival in medically treated patients with homozygous betathalassemia. N Engl J Med 1994; 331: 574–78.
85 Aessopos A, Fragodimitri C, Karabatsos F, et al. Cardiac magnetic resonance imaging R2* assessments and analysis of historical parameters in patients with transfusiondependent thalassemia.Haematologica 2007; 92: 131–32.
86 Worwood M, Cragg SJ, Jacobs A, McLaren C, Ricketts C, Economidou J. Binding of serum ferritin to concanavalin A: patients with homozygous beta thalassaemia and transfusional iron overload. Br J Haematol 1980; 46: 409–16.
87 Taher A, El Rassi F, Isma’eel H, Koussa S, Inati A, Cappellini MD. Correlation of liver iron concentration determined by R2 magnetic resonance imaging with serum ferritin in patients with thalassemia intermedia. Haematologica 2008; 93: 1584–86.
88 Angelucci E, Brittenham GM, McLaren CE, et al. Hepatic iron concentration and total body iron stores in thalassemia major. N Engl J Med 2000; 343: 327–31.
89 Siegel CA, Silas AM, Suriawinata AA, van Leeuwen DJ. Liver biopsy 2005: when and how? Cleve Clin J Med 2005; 72: 199–201, 206, 208 passim.
90 Fischer R, Piga A, Harmatz P, Nielsen P. Monitoring longterm efficacy of iron chelation treatment with biomagnetic liver susceptometry. Ann N Y Acad Sci 2005; 1054: 350–57.
91 St Pierre TG, Clark PR, Chuaanusorn W, et al. Noninvasive measurement and imaging of liver iron concentrations using proton magnetic resonance. Blood 2005; 105: 855–61.
92 Hankins JS, McCarville MB, Loeffler RB, et al. R2* magnetic resonance imaging of the liver in patients with iron overload. Blood 2009; 113: 4853–55.
93 Kirk P, He T, Anderson LJ, et al. International reproducibility of single breathhold T2* MR for cardiac and liver iron assessment among five thalassemia centers. J Magn Reson Imaging 2010; 32: 315–19.
94 St Pierre TG, ElBeshlawy A, Elalfy M, et al. Multicenter validation of spindensity projectionassisted R2MRI for the noninvasive measurement of liver iron concentration. Magn Reson Med 2014; 71: 2215–23.
95 Wood JC, Enriquez C, Ghugre N, et al. MRI R2 and R2* mapping accurately estimates hepatic iron concentration in transfusiondependent thalassemia and sickle cell disease patients. Blood 2005; 106: 1460–65.
96 Wood JC, Zhang P, Rienhoff H, AbiSaab W, Neufeld E. R2 and R2* are equally effective in evaluating chronic response to iron chelation. Am J Hematol 2014; 89: 505–08.
97 Carpenter JP, He T, Kirk P, et al. On T2* magnetic resonance and cardiac iron. Circulation 2011; 123: 1519–28.
98 Wood JC. Impact of iron assessment by MRI. Hematology Am Soc Hematol Educ Program 2011; 2011: 443–50.
99 Noetzli LJ, Panigrahy A, Mittelman SD, et al. Pituitary iron and volume predict hypogonadism in transfusional iron overload. Am J Hematol 2012; 87: 167–71.
100 Noetzli LJ, Mittelman SD, Watanabe RM, Coates TD, Wood JC. Pancreatic iron and glucose dysregulation in thalassemia major. Am J Hematol 2012; 87: 155–60.
101 Olivieri NF, Brittenham GM. Ironchelating therapy and the treatment of thalassemia. Blood 1997; 89: 739–61.
102 Angelucci E, Muretto P, Nicolucci A, et al. Effects of iron overload and hepatitis C virus positivity in determining progression of liver fibrosis in thalassemia following bone marrow transplantation. Blood 2002; 100: 17–21.
103 Telfer PT, Prestcott E, Holden S, Walker M, Hoffbrand AV, Wonke B. Hepatic iron concentration combined with longterm monitoring of serum ferritin to predict complications of iron overload in thalassaemia major. Br J Haematol 2000; 110: 971–77.
104 Anderson LJ, Holden S, Davis B, et al. Cardiovascular T2star (T2*) magnetic resonance for the early diagnosis of myocardial iron overload. Eur Heart J 2001; 22: 2171–79.
105 Kirk P, Roughton M, Porter JB, et al. Cardiac T2* magnetic resonance for prediction of cardiac complications in thalassemia major. Circulation 2009; 120: 1961–68.
106 Carpenter JP, Roughton M, Pennell DJ, Myocardial Iron in Thalassemia Investigators. International survey of T2* cardiovascular magnetic resonance in βthalassemia major. Haematologica 2013; 98: 1368–74.
107 Aydinok Y, Porter JB, Piga A, et al. Prevalence and distribution of iron overload in patients with transfusiondependent anemias differs across geographic regions: results from the CORDELIA study. Eur J Haematol 2015; 95: 244–53.
108 Pennell DJ, Porter JB, Piga A, et al. A 1year randomized controlled trial of deferasirox vs deferoxamine for myocardial iron removal in βthalassemia major (CORDELIA). Blood 2014; 123: 1447–54.
109 Davis BA, Porter JB. Longterm outcome of continuous 24hour deferoxamine infusion via indwelling intravenous catheters in highrisk betathalassemia. Blood 2000; 95: 1229–36.
110 Pennell DJ, Berdoukas V, Karagiorga M, et al. Randomized controlled trial of deferiprone or deferoxamine in betathalassemia major patients with asymptomatic myocardial siderosis. Blood 2006; 107: 3738–44.
111 Tanner MA, Galanello R, Dessi C, et al. A randomized, placebocontrolled, doubleblind trial of the effect of combined therapy with deferoxamine and deferiprone on myocardial iron in thalassemia major using cardiovascular magnetic resonance. Circulation 2007; 115: 1876–84.
112 Tanner MA, Galanello R, Dessi C, et al. Combined chelation therapy in thalassemia major for the treatment of severe myocardial siderosis with left ventricular dysfunction. J Cardiovasc Magn Reson 2008; 10: 12.
113 Farmaki K, Tzoumari I, Pappa C, Chouliaras G, Berdoukas V. Normalisation of total body iron load with very intensive combined chelation reverses cardiac and endocrine complications of thalassaemia major. Br J Haematol 2010; 148: 466–75.
114 Farmaki K, Tzoumari I, Pappa C. Oral chelators in transfusiondependent thalassemia major patients may prevent or reverse iron overload complications. Blood Cells Mol Dis 2011; 47: 33–40.
115 Pennell DJ, Porter JB, Cappellini MD, et al. Deferasirox for up to 3 years leads to continued improvement of myocardial T2* in patients with βthalassemia major. Haematologica 2012; 97: 842–48.
116 Cappellini MD, Bejaoui M, Agaoglu L, et al. Iron chelation with deferasirox in adult and pediatric patients with thalassemia major: efficacy and safety during 5 years’ followup. Blood 2011; 118: 884–93.

Seminar
www.thelancet.com Published online July 31, 2017 http://dx.doi.org/10.1016/S0140-6736(17)31822-6 13
117 Pathare A, Taher A, Daar S. Deferasirox (exjade) significantly improves cardiac T2* in heavily ironoverloaded patients with betathalassemia major. Ann Hematol 2010; 89: 405–09.
118 Taher A, Cappellini MD, Vichinsky E, et al. Efficacy and safety of deferasirox doses of >30 mg/kg per d in patients with transfusiondependent anaemia and iron overload. Br J Haematol 2009; 147: 752–59.
119 Deugnier Y, Turlin B, Ropert M, et al. Improvement in liver pathology of patients with βthalassemia treated with deferasirox for at least 3 years. Gastroenterology 2011; 141: 1202–11.
120 Casale M, Citarella S, Filosa A, et al. Endocrine function and bone disease during longterm chelation therapy with deferasirox in patients with βthalassemia major. Am J Hematol 2014; 89: 1102–06.
121 Taher AT, Porter JB, Viprakasit V, et al. Deferasirox effectively reduces iron overload in nontransfusiondependent thalassemia (NTDT) patients: 1year extension results from the THALASSA study. Ann Hematol 2013; 92: 1485–93.
122 Fisher SA, Brunskill SJ, Doree C, Chowdhury O, Gooding S, Roberts DJ. Oral deferiprone for iron chelation in people with thalassaemia. Cochrane Database Syst Rev 2013; 8: CD004839.
123 Mamtani M, Kulkarni H. Influence of iron chelators on myocardial iron and cardiac function in transfusiondependent thalassaemia: a systematic review and metaanalysis. Br J Haematol 2008; 141: 882–90.
124 Porter JB, Wood J, Olivieri N, et al. Treatment of heart failure in adults with thalassemia major: response in patients randomised to deferoxamine with or without deferiprone. J Cardiovasc Magn Reson 2013; 15: 38.
125 Gabutti V, Piga A. Results of longterm ironchelating therapy. Acta Haematol 1996; 95: 26–36.
126 Delea TE, Edelsberg J, Sofrygin O, et al. Consequences and costs of noncompliance with iron chelation therapy in patients with transfusiondependent thalassemia: a literature review. Transfusion 2007; 47: 1919–29.
127 Premawardhena A, Fisher CA, Olivieri NF, et al. Haemoglobin E beta thalassaemia in Sri Lanka. Lancet 2005; 366: 1467–70.
128 Taher AT, Musallam KM, Karimi M, et al. Splenectomy and thrombosis: the case of thalassemia intermedia. J Thromb Haemost 2010; 8: 2152–58.
129 Angelucci E, MatthesMartin S, Baronciani D, et al. Hematopoietic stem cell transplantation in thalassemia major and sickle cell disease: indications and management recommendations from an international expert panel. Haematologica 2014; 99: 811–20.
130 Angelucci E. Hematopoietic stem cell transplantation in thalassemia. Hematology Am Soc Hematol Educ Program 2010; 2010: 456–62.
131 CavazzanaCalvo M, Payen E, Negre O, et al. Transfusion independence and HMGA2 activation after gene therapy of human βthalassaemia. Nature 2010; 467: 318–22.
132 Musallam KM, Taher AT, Cappellini MD, Sankaran VG. Clinical experience with fetal hemoglobin induction therapy in patients with βthalassemia. Blood 2013; 121: 2199–212; quiz 2372.
133 Dussiot M, Maciel TT, Fricot A, et al. An activin receptor IIA ligand trap corrects ineffective erythropoiesis in βthalassemia. Nat Med 2014; 20: 398–407.
134 Suragani RN, Cadena SM, Cawley SM, et al. Transforming growth factorβ superfamily ligand trap ACE536 corrects anemia by promoting latestage erythropoiesis. Nat Med 2014; 20: 408–14.
135 Gardenghi S, Ramos P, Marongiu MF, et al. Hepcidin as a therapeutic tool to limit iron overload and improve anemia in βthalassemic mice. J Clin Invest 2010; 120: 4466–77.
136 Preza GC, Ruchala P, Pinon R, et al. Minihepcidins are rationally designed small peptides that mimic hepcidin activity in mice and may be useful for the treatment of iron overload. J Clin Invest 2011; 121: 4880–88.
137 Nai A, Pagani A, Mandelli G, et al. Deletion of TMPRSS6 attenuates the phenotype in a mouse model of βthalassemia. Blood 2012; 119: 5021–29.
138 Guo S, Casu C, Gardenghi S, Booten S, Aghajan M, Peralta R, et al. Reducing TMPRSS6 ameliorates hemochromatosis and βthalassemia in mice. J Clin Invest 2013; 123: 1531–41.
139 Schmidt PJ, Toudjarska I, Sendamarai AK, et al. An RNAi therapeutic targeting TMPRSS6 decreases iron overload in Hfe(/) mice and ameliorates anemia and iron overload in murine βthalassemia intermedia. Blood 2013; 121: 1200–08.