Thai Journal of Tuberculosis Chest Diseases and Critical CareAubertin J, Dabis F, Fleurette J, et...
44
“√∫—≠ «“√ “√«—≥‚√§ ‚√§∑√«ßÕ°·≈–‡«™∫”∫—¥«‘°ƒμ ªï∑’Ë 25 ©∫—∫∑’Ë 3 °√°Æ“§¡ - °—𬓬π 2547 ● ∫∑∫√√≥“∏‘°“√ : Atypical Does Not Mean Uncommon «—π™—¬ ‡¥™ ¡ƒ∑∏‘σ∑—¬ 127 ● Weaning : an Evidence-Based Approach Õ¥‘»√ «ß…“ 131 ● Can Overnight Pulse Oximetry Recording Be Used as a Manapol Kulpraneet 139 Screening Measure for Obstructive Sleep Apnea Nitipatana Chierakul Arth Nana ● The Retinoic Acid Syndrome : A Steroid-Responsive Acute ‡©≈‘¡ ≈‘Ë«»√’ °ÿ≈ 147 Respiratory Distress Syndrome (ARDS). The First Case ∫ÿ≠ ¡ ™—¬¡ß§≈ Report of Thailand ● °“√»÷°…“ “‡Àμÿ¢Õ߇™◊ÈÕ‚√§™π‘¥º‘¥√Ÿª·∫∫∑’Ë∑”„À⇰‘¥ªÕ¥Õ—°‡ ∫ ¡§‘¥ Õÿàπ‡ ¡“∏√√¡ 155 ™ÿ¡™π„π‚√ß欓∫“≈√“™«‘∂’ ª«‘≥ ¥ÿ√ߧ‡«‚√®πå ● ª√– ‘∑∏‘¿“æ·≈–§«“¡ª≈Õ¥¿—¬¢Õ߬“´“‡øÕ≈Ÿ§“ ∑—»π’¬“ ÿ∏√√¡ ¡—¬ 163 „π°“√√—°…“ºŸâªÉ«¬‚√§À◊¥ ª√–æ“à ¬ß„®¬ÿ∑∏ «—™√“ ∫ÿ≠ «— ¥‘Ï √—μπ“¿√≥å ‡øóòÕß∑Õß ‡©≈‘¡ ≈‘Ë«»√’ °ÿ≈ «“√ “√«—≥‚√§ ‚√§∑√«ßÕ°·≈–‡«™∫”∫—¥«‘°ƒμ Thai Journal of Tuberculosis Chest Diseases and Critical Care
Transcript of Thai Journal of Tuberculosis Chest Diseases and Critical CareAubertin J, Dabis F, Fleurette J, et...

“√∫—≠
«“√ “√«—≥‚√§ ‚√§∑√«ßÕ°·≈–‡«™∫”∫—¥«‘°ƒµ ªï∑ ’Ë 25 ©∫ —∫∑ ’Ë 3 °√°Æ“§¡ - °—𬓬π 2547
● ∫∑∫√√≥“∏‘°“√ : Atypical Does Not Mean Uncommon «—π™—¬ ‡¥™ ¡ƒ∑∏ ‘σ∑ —¬ 127
● Weaning : an Evidence-Based Approach Õ¥‘»√ «ß…“ 131
● Can Overnight Pulse Oximetry Recording Be Used as a Manapol Kulpraneet 139Screening Measure for Obstructive Sleep Apnea Nitipatana Chierakul
Arth Nana
● The Retinoic Acid Syndrome : A Steroid-Responsive Acute ‡©≈‘¡ ≈ ‘Ë«»√’ °ÿ≈ 147Respiratory Distress Syndrome (ARDS). The First Case ∫ÿ≠ ¡ ™—¬¡ß§≈Report of Thailand
● °“√»÷°…“ “‡Àµÿ¢Õ߇™◊ÈÕ‚√§™π ‘¥º‘¥√Ÿª·∫∫∑ ’Ë∑”„À⇰‘¥ªÕ¥Õ—°‡ ∫ ¡§‘¥ Õÿàπ‡ ¡“∏√√¡ 155™ÿ¡™π„π‚√ß欓∫“≈√“™«‘∂ ’ ª«‘≥ ¥ÿ√ߧ‡«‚√®πå
● ª√– ‘∑∏‘¿“æ·≈–§«“¡ª≈Õ¥¿—¬¢Õ߬“´“‡øÕ≈Ÿ§“ ∑—»π’¬“ ÿ∏√√¡ ¡—¬ 163„π°“√√—°…“ºŸâªÉ«¬‚√§À◊¥ ª√–æ“à ¬ß„®¬ÿ∑∏
«—™√“ ∫ÿ≠ «— ¥‘Ï√—µπ“¿√≥å ‡øóòÕß∑Õ߇©≈‘¡ ≈ ‘Ë«»√’ °ÿ≈
«“√ “√«—≥‚√§ ‚√§∑√«ßÕ°·≈–‡«™∫”∫ —¥«‘°ƒµThai Journal of Tuberculosis
Chest Diseases and Critical Care

ªï∑’Ë 25 ©∫ —∫∑’Ë 3 °√°Æ“§¡-°—𬓬π 2547 ∫∑∫√√≥“∏ ‘°“√œ 127
ªí®®ÿ∫—π °“√√ —°…“‚√§ªÕ¥Õ—°‡ ∫™ÿ¡™π ‚¥¬‡©æ“–Õ¬à“߬‘Ëß°“√‡≈◊Õ°„™â¬“µâ“π®ÿ≈™’æ ®–‡ªìπ‰ª„π≈—°…≥–¢Õß°“√√—°…“·∫∫ empiric ‡ªìπ à«π„À≠ à ∑—Èßπ’ȇπ◊ËÕß®“°·æ∑¬åºŸâ√—°…“‰¡à “¡“√∂„™â≈—°…≥–∑“ߧ≈ ‘π ‘°„π°“√„Àâ°“√«‘π‘®©—¬‡™ ◊ÈÕ°àÕ‚√§‰¥â™—¥‡®π µ≈Õ¥®π¢âÕ®”°—¥„π°“√‡°Á∫ ‘Ëß àßµ√«® ·≈–√–¬–‡«≈“∑ ’Ë„™â„π°“√µ√«®∑“ßÀâÕߪؑ∫—µ‘°“√ ¥—ßπ —Èπ ¢âÕ¡Ÿ≈‡°’ˬ«°—∫√–∫“¥«‘∑¬“¢Õ߇™ ◊ÈÕ°àÕ‚√§ªÕ¥Õ—°‡ ∫™ÿ¡™π®÷ß¡’§«“¡ ”§—≠Õ¬à“߬‘Ëß„π°“√‡≈◊Õ°¬“µâ“π®ÿ≈™’æ∑’ˇÀ¡“– ¡ ‚¥¬‡©æ“–„π√–¬–·√°¢Õß°“√√—°…“ ªí≠À“∑’Ë ”§—≠ª√–°“√Àπ÷ËߢÕß°“√»÷°…“‡™◊ÈÕ
ATYPICAL DOES NOT MEAN UNCOMMON∫∑∫√√≥“∏‘°“√
°àÕ‚√§ªÕ¥Õ—°‡ ∫™ÿ¡™π°Á§◊Õ °“√∑’Ë ‰¡à “¡“√∂√–∫ ÿ‡™◊ÈÕ°àÕ‚√§‰¥â„πºŸâªÉ«¬®”π«πÀπ÷Ëß´÷ËßÕ“®¡“°∂÷ß√âÕ¬≈– 50πÕ°®“°π—Èπ ¬—ß¡’ºŸâªÉ«¬®”π«πÀπ÷Ëß∑ ’Ë¡’°“√µ‘¥‡™◊ÈÕ¡“°°«à“Àπ÷Ëß™π‘¥ Õ¬à“߉√°Áµ“¡ „π√–¬–À≈ —ß ¡’§«“¡°â“«Àπâ“¢Õß°“√µ√«®∑“ßÀâÕߪؑ∫ —µ‘°“√¡“°¢÷Èπ ‰¥â¡’°“√»÷°…“∂÷߇™◊ÈÕ°àÕ‚√§ªÕ¥Õ—°‡ ∫„π·µà≈–¿Ÿ¡‘¿“§ÕÕ°¡“¡“°¡“¬ º≈°“√»÷°…“™’È„Àâ‡ÀÁπ∂÷ߧ«“¡ ”§—≠¢Õ߇™◊ÈÕ°àÕ‚√§„π°≈ ÿà¡ atypical pathogen ´÷Ëߪ√–°Õ∫¥â«¬Mycoplasma pneumoniae, Chlamydia pneumoniae·≈– Legionella spp ‚¥¬æ∫«à“§«“¡™ÿ°¢Õ߇™◊ÈÕ°àÕ‚√§°≈ÿà¡π’È¡’·π«‚πâ¡ Ÿß¢÷Èπ (µ“√“ß∑’Ë 1)
µ“√“ß∑’Ë 1 §«“¡™ÿ°¢Õ߇™ ◊ÈÕ°àÕ‚√§„π°≈ÿà¡ atypical pathogen „π‚√§ªÕ¥Õ—°‡ ∫™ÿ¡™π(¥—¥·ª≈ß®“° Blasi F. Eur Respir J 2004; 24:171-181)1
√—∫‰«âµ’æ‘¡æ凡◊ËÕ«—π∑’Ë 22 °—𬓬π 2547
«“√ “√«—≥‚√§ ‚√§∑√«ßÕ°·≈–‡«™∫”∫—¥«‘°ƒµThai Journal of TuberculosisChest Diseases and Critical Care

128 «—π™—¬ ‡¥™ ¡ƒ∑∏ ‘σ∑—¬ «“√ “√«—≥‚√§ ‚√§∑√«ßÕ°·≈–‡«™∫”∫ —¥«‘°ƒµ
®–‡ÀÁπ‰¥â«à“ §«“¡™ÿ°¢Õ߇™ ◊ÈÕ°≈ ÿà¡π’È¡’§«“¡À≈“°À≈“¬ ¢÷Èπ°—∫¿Ÿ¡‘¿“§∑’Ë∑”°“√»÷°…“ √«¡∑ —Èß«‘∏’°“√µ√«®∑“ßÀâÕߪؑ∫—µ‘°“√∑’Ë„™â„π°“√ ”√«® „πª√–‡∑»‰∑¬Õπ—πµå «—≤π∏√√¡ ·≈–§≥–12 ‰¥â‡§¬∑”°“√»÷°…“„πºŸâªÉ«¬‚√§ªÕ¥Õ—°‡ ∫™ÿ¡™π®”π«π 245 √“¬ ∑ —ÈߺŸâªÉ«¬πÕ°(98) ·≈–ºŸâªÉ«¬„π (147) æ∫«à“‡™ ◊ÈÕ„π°≈ÿà¡ atypicalpathogen ‡ªìπ‡™ ◊ÈÕ°àÕ‚√§∑ ’Ëæ∫¡“°‡ªìπÕ—π¥—∫µâπÊ„πºŸâªÉ«¬πÕ° §◊Õ Chlamydia pneumoniae (36.7%)·≈– Mycoplasma pneumoniae (29.6%) ·≈–∂÷ß·¡â Streptococcus pneumoniae ¬—ߧ߇ªìπ‡™◊ÈÕ°àÕ‚√§Õ—π¥—∫·√° (22.4%) „πºŸâªÉ«¬∑’ˉ¥â√ —∫°“√√—°…“„π‚√ß欓∫“≈ ·µà°Áæ∫‡™◊ÈÕ„π°≈ÿà¡ atypical pathogen‡ªìπ‡™◊ÈÕ°àÕ‚√§√«¡°—π·≈â«∂÷ß 28%
„π«“√ “√«—≥‚√§ ‚√§∑√«ßÕ°·≈–‡«™∫”∫—¥«‘°ƒµ©∫—∫π’È ¡§‘¥ Õÿàπ‡ ¡“∏√√¡ ·≈–§≥–13 ‰¥â√“¬ß“πº≈°“√»÷°…“∂ ÷߇™◊ÈÕ°àÕ‚√§„πºŸâªÉ«¬‚√§ªÕ¥Õ—°‡ ∫™ÿ¡™π®”π«π 22 √“¬ ‚¥¬„™â«‘∏’°“√µ√«®∑“ß serology√à«¡°—∫ polymerase chain reaction (PCR) æ∫«à“§«“¡™ÿ°¢Õ߇™◊ÈÕ°àÕ‚√§„π°≈ÿà¡ atypical pathogen7 √“¬ §‘¥‡ªìπ 31.8% ‚¥¬æ∫ M pneumoniae 2 √“¬,C pneumoniae 2 √“¬, C psittaci 1 √“¬·≈– mixedinfection 2 √“¬
º≈°“√»÷°…“¥—ß°≈à“« ™’È „Àâ‡ÀÁ𧫓¡ ”§—≠¢Õßatypical pathogen „π°“√‡ªìπ‡™ ◊ÈÕ°àÕ‚√§ªÕ¥Õ—°‡ ∫™ÿ¡™π„πª√–‡∑»‰∑¬ ¥—ßπ—È𠬓µâ“π®ÿ≈™’æ∑’ˇÀ¡“– ¡®÷ߧ«√‡ªìπ¬“∑ ’˧√Õ∫§≈ÿ¡∂÷߇™◊ÈÕ°≈ÿà¡π’ȥ⫬ Õ¬à“߉√°Áµ“¡°“√»÷°…“¥—ß°≈ à “«∑”„πª√–™“°√∑ ’ËÕ¬Ÿà „π°√ÿ߇∑æ-¡À“π§√·≈–ª√‘¡≥±≈ ®÷߉¡à “¡“√∂𔉪„™âÕâ“ßÕ‘ß„π¿Ÿ¡‘¿“§Õ◊Ëπ¢Õߪ√–‡∑»‰¥â ‚¥¬‡©æ“–Õ¬à“߬‘Ëß„π¿“§µ–«—πÕÕ°‡©’¬ß‡Àπ◊Õ∑’Ëæ∫‡™ ◊ÈÕª√–®”∂ ‘Ëπ ‰¥â·°àBurkholderia pseudomallei ¡“° ¥—ßπ —Èπ°“√‡≈◊Õ°¬“µâ“π®ÿ≈™’æ®÷ßµâÕߪ√—∫‡ª≈’Ë¬π‰ªµ“¡¢âÕ¡Ÿ≈√–∫“¥«‘∑¬“„π·µà≈–æ◊Èπ∑ ’ ˥⫬
«—π™—¬ ‡¥™ ¡ƒ∑∏‘σ∑—¬ æ.∫., M.Sc. “¢“«‘™“‚√§√–∫∫°“√À“¬„®·≈–«—≥‚√§
¿“§«‘™“Õ“¬ÿ√»“ µ√å §≥–·æ∑¬»“ µ√廑√‘√“™æ¬“∫“≈
‡Õ° “√Õâ“ßÕ‘ß1. Blasi F. Atypical pathogens and respiratory tract
infections. Eur Respir J 2004; 24:171-181.2. Almirall J, Morato I, Riera F, et al. Incidence of
community-acquired pneumonia and Chlamydiapneumoniae infection: a prospective multicentre study.Eur Respir J 1993; 6:14-18.
3. Marrie TJ, Peeling RW, Fine MJ, Singer DE, ColeyCM and Kapoor WN. Ambulatory patients withcommunity-acquired pneumonia: the frequency ofatypical agents and clinical course. Am J Med 1996;101:508-515.
4. File TM Jr, Segreti J, Dunbar L, et al. A multicenter,randomized study comparing the efficacy and safetyof intravenous and/or oral levofloxacin versusceftriaxone and/or cefuroxime axetil in treatment ofadults with community-acquired pneumonia. AntimicrobAgents Chemother 1997; 41:1965-1972.
5. Sopena N, Sabria-Leal M, Pedro-Botet ML, et al.Comparative study of the clinical presentation ofLegionella pneumonia and other community-acquiredpneumonias. Chest 1998; 113:1195-1200.
6. Aubertin J, Dabis F, Fleurette J, et al. Prevalence oflegionellosis among adults: a study of community-acquired pneumonia in France. Infection 1987; 15:328-331.
7. Steinhoff D, Lode H, Ruckdeschel G, et al. Chlamydiapneumoniae as a cause of community-acquiredpneumonia in hospitalized patients in Berlin. ClinInfect Dis 1996; 22:958-964.
8. Lieberman D, Lieberman D and Porath A. Seasonalvariation in community-acquired pneumonia. Eur RespirJ 1996; 22:958-964.
9. Neill AM, Martin IR, Weir R, et al. Communityacquired pneumonia: aetiology and usefulness ofseverity criteria on admission. Thorax 1996; 51:1010-1016.
10. Bohte R, van Furth R, van den Broek PJ. Aetiology ofcommunity-acquired pneumonia: a prospective studyamong adults requiring admission to hospital. Thorax1995; 50: 543-547.

ªï∑’Ë 25 ©∫ —∫∑’Ë 3 °√°Æ“§¡-°—𬓬π 2547 ∫∑∫√√≥“∏ ‘°“√œ 129
11. Bochud PY, Moser F, Erard P, et al. Community-acquired pneumonia. A prospective outpatient study.Medicine (Baltimore) 2001; 80:75-87.
12. Wattanathum A, Chaoprasong C, Nunthapisud P, etal. Community-acquired pneumonia in Southeast Asia.The microbial differences between ambulatory andhospitalized patients. Chest 2003; 123:1512-1519.
13. ¡§‘¥ Õÿàπ‡ ¡“∏√√¡, ª«‘≥ ¥ÿ√ߧ‡«‚√®πå. °“√»÷°…“À“ “‡Àµÿ¢Õ߇™ ◊ÈÕ‚√§™π ‘¥º‘¥√ Ÿª·∫∫∑’Ë∑”„À⇰‘¥‚√§ªÕ¥Õ—°‡ ∫™ÿ¡™π„π‚√ß欓∫“≈√“™«‘∂’. «“√ “√«—≥‚√§ ‚√§∑√«ßÕ°·≈–‡«™∫”∫ —¥«‘°ƒµ 2547; 25:155-163.

ªï∑’Ë 25 ©∫ —∫∑’Ë 3 °√°Æ“§¡-°—𬓬π 2547 Weaning : an evidence-based approach 131
Õ¥‘»√ «ß…“ æ.∫.
Àπ૬‚√§ªÕ¥ °ÕßÕ“¬ÿ√°√√¡ ‚√ß欓∫“≈æ√–¡ß°ÿƇ°≈â“
WEANING: AN EVIDENCE-BASED APPROACH
ºŸâªÉ«¬∑’Ë„™â‡§√◊ËÕߙ૬À“¬„®π —Èπ ‡¡◊ËÕ “‡Àµÿ·≈–ªí≠À“∑’Ë∑”„ÀâµâÕß„™â‡§√◊ËÕ߉¥â√—∫°“√·°â ‰¢·≈– ¿“æ¢Õß ºŸâªÉ«¬¥’¢÷Èπ°Á§«√æ‘®“√≥“À¬à“/À¬ÿ¥À√◊Õ‡≈ ‘°„™â‡§√◊ËÕߙ૬À“¬„®ºŸâªÉ«¬ à«π„À≠à “¡“√∂‡≈ ‘°„™â‡§√◊ËÕ߉¥â·µà∫“ß à«πµâÕß°≈—∫¡“„™â‡§√◊ËÕßÕ’° ºŸâªÉ«¬∑’Ë„™â‡§√◊ËÕߙ૬À“¬„®π“π (∑—Èß∑’ËÕ“®À¬ÿ¥„™â‡§√◊ËÕ߉¥â) À√◊ÕºŸâªÉ«¬∑ ’Ë∂Õ¥∑ àՙ૬À“¬„®·≈–‡Õ“‡§√◊ËÕߙ૬À“¬„®ÕÕ°°àÕπ‡«≈“Õ—π ¡§«√ æ∫«à“¡’ªí≠À“·∑√° âÕπ·≈–¡’Õ—µ√“°“√‡ ’¬™’«‘µ‡æ‘Ë¡ ¥—ßπ—Èπ·æ∑¬åºŸâ¥Ÿ·≈®÷ߧ«√¡’°“√ª√–‡¡‘πºŸâªÉ«¬∑’Ë “¡“√∂À¬ÿ¥„™â‡§√◊ËÕ߉¥â·≈– “¡“√∂‡≈◊Õ°«‘∏’°“√‡≈ ‘°„™â‡§√◊ËÕ߉¥âÕ¬à“߇À¡“– ¡ ‡æ ◊ËÕ≈¥ªí≠À“·≈–º≈·∑√°´âÕπ∑ ’˵“¡¡“ ‡π◊ËÕß®“°§«“¡√ Ÿâ·≈–°“√»÷°…“«‘®—¬∑“ß°“√·æ∑¬å„πªí®®ÿ∫—π‰¥â°â“«Àπ â“¡“°√«¡∂÷߇∑§π ‘§„π°“√ wean ºŸâªÉ«¬ÕÕ°®“°‡§√◊ËÕߙ૬À“¬„®‰¥â¡’°“√»÷°…“Õ¬à“ß°«â“ߢ«“ß ∫∑§«“¡π ’È®–‰¥â √ ÿª∂÷ßevidence-based ¢Õß°“√ wean „πªí®®ÿ∫—π ´÷Ëß·∫àß√–¥—∫¢ÕßÀ≈—°∞“πÕÕ°‡ªìπ
√–¥—∫ 1 : ¡’°“√»÷°…“∑’Ë¡’°“√ÕÕ°·∫∫Õ¬à“ߥ’‚¥¬‡ªìπ control trial ·≈–º≈°“√»÷°…“¡’§à“π—¬ ”§—≠∑“ß ∂‘µ‘
√–¥—∫ 2 : ¡’°“√»÷°…“·∫∫°“√ —߇°µ (observationstudy) À√◊Õ control trial ·µàº≈°“√»÷°…“¬—߉¡à™—¥‡®π¡“°
√–¥—∫ 3 : ‡ªì𧫓¡‡ÀÁπ¢ÕߺŸâ‡™’ˬ«™“≠‡π◊ËÕß®“°º≈°“√»÷°…“¢—¥·¬âß°—π‡ÕßÀ√◊Õ‰¡à¡’°“√»÷°…“„πªí≠À“π—Èπ
‚¥¬ √ ÿª®“°º≈°“√«‘®—¬¢Õß¡À“«‘∑¬“≈—¬ McMaster(The Agency for Health Care Policy and Research =AHCPR) „πªï 25421 ·≈–°“√ª√–™ÿ¡√ à«¡°—π√–À«à“ßAmerican College of Chest Physicians, AmericanAssociation for Respiratory Care ·≈– American Col-lege of Critical Care Medicine „πªï 25442 À—«¢âÕ´÷Ë߇ªìπ§”∂“¡„π°“√ wean ºŸâªÉ«¬ÕÕ°®“°‡§√◊ËÕߙ૬À“¬„® “¡“√∂·∫àßÕÕ°‰¥â‡ªìπ
● ‡¡ ◊ËÕ‰√§«√‡√‘Ë¡ wean ºŸâªÉ«¬ÕÕ°®“°‡§√◊ËÕߙ૬À“¬„®
● ¥—™π’™’È«—¥ (weaning parameter) ∑ ’Ë∫Õ°∂÷ß‚Õ°“ ∑ ’Ë®– wean ‰¥â ”‡√Á®
● ‡∑§π‘§°“√ wean ∑ ’ˉ¥âº≈● °“√ª√–‡¡‘π·≈–·°â ‰¢ “¬‡ ’¬ß∫«¡„πºŸâªÉ«¬∑ ’Ë
„ à∑àՙ૬À“¬„®
‡¡◊ËÕ‰√§«√‡√‘Ë¡ wean (À≈—°∞“π„π√–¥—∫ 2)‚¥¬æ∫«à“°“√ wean „πºŸâªÉ«¬∑’Ë¿“«–°“√À“¬„®≈ ⡇À≈«
¬—߉¡à‰¥â√—∫°“√·°â ‰¢·≈–¬—ßµâÕß°“√°“√™à«¬®“°‡§√◊ËÕßÕ¬Ÿà„π√–¥—∫ Ÿßπ—Èπ ®–∑”„Àâ°≈â“¡‡π◊ÈÕÀ“¬„®≈â“·≈–Õ“®∑”„À⺟âªÉ«¬µâÕß„™â‡§√◊ËÕߙ૬À“¬„®π“π¢÷Èπ3-5 ¥—ßπ—ÈπºŸâªÉ«¬§«√‡√‘Ë¡wean ‡¡◊ËÕ “‡Àµÿ∑ ’Ë∑”„Àâ respiratory failure À√◊Õ “‡Àµÿ∑ ’˵âÕß„™â‡§√◊ËÕߙ૬À“¬„®‰¥â√—∫°“√·°â ‰¢·≈â« ·≈–æ∫«à“°“√„™âÕ“°“√∑“ߧ≈‘π‘°‡æ’¬ßÕ¬à“߇¥’¬«¡“µ—¥ ‘π°“√ wean°Á¡’‚Õ°“ º‘¥æ≈“¥ Ÿß6 ·≈–‡¡◊ËÕªí≠À“¢Õß°“√À“¬„®‰¥â√—∫
√—∫‰«âµ’æ‘¡æ凡 ◊ËÕ«âπ∑’Ë 18 ∏ —𫓧¡ 2545
«“√ “√«—≥‚√§ ‚√§∑√«ßÕ°·≈–‡«™∫”∫—¥«‘°ƒµThai Journal of TuberculosisChest Diseases and Critical Care

132 Õ¥‘»√ «ß…“ æ.∫. «“√ “√«—≥‚√§ ‚√§∑√«ßÕ°·≈–‡«™∫”∫ —¥«‘°ƒµ
°“√∑¥ Õ∫«à“ºŸâªÉ«¬ “¡“√∂À“¬„®‡Õ߉¥â (À≈—°∞“π„π√–¥—∫ 1)
∂÷ß·¡âºŸâªÉ«¬∑’Ë¡’¢âÕ∫àß™’È„π°“√ wean µ“¡µ“√“ß∑ ’Ë 1π—Èπ°Áæ∫«à“‡¡ ◊ËÕ wean ·≈â«Õ“®‰¡à ”‡√ Á®À√◊ÕºŸâªÉ«¬µâÕß°≈—∫¡“„™â‡§√◊ËÕßÕ’° ¥—ßπ—Èπ®÷ߧ«√∑”°“√∑¥ Õ∫°“√À“¬„® ¢ÕߺŸâªÉ«¬°àÕπ®–À¬ÿ¥„™â‡§√◊ËÕߙ૬À“¬„®∑ ÿ°§√ —Èß °“√»÷°…“æ∫«à“°“√∑¥ Õ∫‚¥¬„™â spontaneous breathing trial(SBT) ®–∫Õ°∂÷ߧ«“¡ “¡“√∂„π°“√À“¬„®‰¥â‡ÕߢÕߺŸâªÉ«¬‰¥â¥’°«à“°“√∑¥ Õ∫‚¥¬„À⺟âªÉ«¬À“¬„®ºà“π‡§√◊ËÕß (∂÷ß®–™à«¬„π¢π“¥π âÕ¬) ‚¥¬‡©æ“–„π√–¬–·√°¢Õß SBT (3-5π“∑ ’·√°) ‡ªìπ™à«ß∑’Ë¡’§«“¡ ”§—≠∑’Ë®–∫Õ°‰¥â«à“ºŸâªÉ«¬®– “¡“√∂ºà“π°“√∑¥ Õ∫‰¥â¥’À√◊Õ‰¡à ºŸâªÉ«¬®–µâÕß¡’·∫∫
°“√À“¬„® (respiratory pattern) ∑ ’ˇÀ¡“– ¡, °“√·≈°‡ª≈ ’ˬπ·°ä ∑ ’Ë¥’, √–¥—∫°“√‰À≈‡«’¬π¢Õ߇≈◊Õ¥ (hemodynamic) ∑ ’˧ß∑’Ë ·≈–ºŸâªÉ«¬¥Ÿ ÿ¢ ∫“¬ ¢≥–∑’Ë∑”°“√∑¥ Õ∫‚¥¬ SBT·≈–À“°ºŸâªÉ«¬ “¡“√∂ºà“π°“√∑¥ Õ∫‰¥â 30-120 π“∑ ’°Á§«√æ‘®“√≥“π”ºŸâªÉ«¬ÕÕ°®“°‡§√◊ËÕߙ૬À“¬„®
°“√„™â¥—™π’ (weaning index) ‡æ ◊ËÕª√–‡¡‘π‚Õ°“ ∑’Ë®– wean ‰¥â ”‡√Á®π—Èπ ¡’°“√»÷°…“Õ¬Ÿà¡“°·µà∑’Ë¡’π—¬ ”§—≠∑“ß ∂ ‘µ‘π—Èπ¡’‰¡à¡“° §à“∑’Ë∫àß«à“®– wean ‰¥â¥’π—Èπ¡À“«‘∑¬“≈—¬McMaster AHCPR ·π–π”„Àâ„™â§à“ Likelihood ratios(LRs) §◊Õ§à“∑’Ë¡“°°«à“ 1 ·≈–À“°§à“ LRs Ÿß¡“°‚Õ°“ ∑’Ë®–„™â欓°√≥ å«à“ “¡“√∂ wean ‰¥âº≈¬‘Ëß¡“°¢÷Èπ ¥—ßµ“√“ß∑ ’Ë 2
°“√·°â ‰¢·≈â«°Á§«√ª√–‡¡‘π°“√∑”ß“π ¢Õß√–∫∫°“√À“¬„®·≈– à«π∑’ˇ°’ˬ«¢âÕß ´÷Ë߉¥â·°à hemodynamic
·≈–°“√∑”ß“π¢Õß ¡Õß √«¡∑ —Èß electrolytes ·≈– acid-base disturbance ¥—ßµ“√“ß∑ ’Ë 1
µ“√“ß∑ ’Ë 1 · ¥ß¢âÕ∫àß™’È∑’˧«√‡æ‘Ë¡ wean 7-12
GCS* = Glasgow Coma Scale@Minimal vasopressor ‡™àπ Dopamine „π¢π“¥ renal dose À√◊Õ Dobutamine 5µg/kg/min
°“√·≈°‡ª≈ ’ˬπ·°ä ¥’ PaO2 > 60 mmHg ¢≥–‰¥â FiO2 0.40, PEEP 5 cmH2O À√◊ÕPaO2/ FiO2 ratio 150-300
HR 140, stable BP, minimal vasopressor@
General ¥’¢÷Èπ Afebrile (T < 38 C)‰¡à¡’ respiratory acidosis ·≈– electrolyte ∑ ’ËÕ¬Ÿà „π‡°≥±åª°µ‘√–¥—∫ Hemoglobin ∑ ’ˇÀ¡“– ¡ ( 8-19 g/dL)Adequate mentation (GCS* 13) ·≈–‰¡à‰¥â√—∫ continuous IVsedation
Subjective clinical assessments ‚√§‰¥â√—∫°“√·°â ‰¢„À⥒¢÷Èπ ·≈–·æ∑¬åª√–‡¡‘π·≈⫺ŸâªÉ«¬‡√‘Ë¡ wean ‰¥â·≈– “¡“√∂‰Õ‰¥â·√ß
Hemodynamic stable
Objective Measurement

ªï∑’Ë 25 ©∫ —∫∑’Ë 3 °√°Æ“§¡-°—𬓬π 2547 Weaning : an evidence-based approach 133
µ“√“ß∑ ’Ë 2 °“√ª√–‡¡‘𧫓¡ “¡“√∂„π°“√À“¬„®‡Õß‚¥¬ weaning parameter1
Parameter
«—¥¢≥–ºŸâªÉ«¬„™â‡§√◊ËÕߙ૬À“¬„®
VE
NIF
PImax
CROP score
«—¥„π™à«ßµâπ¢≥–ºŸâªÉ«¬‡√‘Ë¡∑¥ Õ∫‚¥¬ spontaneous breathing
RR
Vt
f/Vt ratio
§à“∑’Ë∫àß«à“ wean ‰¥â
10 - 15 L/min
-20_ - 30 cmH2O
-15_ - 30 cmH2O
13
30 - 38 breaths/min
325 - 408 ml (4-6 ml/kg)
60 - 105
§à“ LRs
0.81 - 2.37
0.23 - 2.45
0.98 - 3.01
2.14 - 25.3
1.00 - 3.89
0.71 - 3.83
0.84 - 4.67
VE = minute ventilation, NIF = negativ e inspiratory force, P Imax = maximum inspiratory pressure, RR = respiratory rate, Vt = tidalvolume, f/Vt = respiratory rate/tidal v olume ratio, CROP = index ´÷Ëߪ√–°Õ∫¥â«¬ compliance, rate, oxygenation ·≈– pressure
°“√»÷°…“„πªí®®ÿ∫—πæ∫«à“«‘∏’°“√ wean ∑ ’Ë ‰¥âº≈·≈–„™â√–¬–‡«≈“∑’Ëπ âÕ¬∑’Ë ÿ¥§◊Õ SBT ∑ ’Ë√Õß≈߉ª§◊Õ pres-sure support technique ·≈–∑ ’Ë„™â√–¬–‡«≈“„π°“√ weanπ“π∑ ’Ë ÿ¥ §◊Õ IMV9,11 ¥—ßπ —Èπ„πªí®®ÿ∫—π®÷ß·π–π”„Àâ‡√‘Ë¡
wean ¥â«¬ SBT ·≈–¢≥–∑¥ Õ∫¥â«¬ SBT π —ÈπµâÕßµ‘¥µ“¡¥ŸºŸâªÉ«¬Õ¬à“ß„°≈♑¥ ‡æ◊ËÕæ‘®“√≥“«à“ºŸâªÉ«¬ “¡“√∂wean ‰¥âÀ√◊Õ‰¡à ·≈–µ√«®À“„π°√≥ ’∑’˺ŸâªÉ«¬‰¡à ¡§«√wean µàÕ (weaning failure) ¥—ßµ“√“ß∑’Ë 3
µ“√“ß∑ ’Ë 3 · ¥ß∂÷ߢâÕ∫àß™’È∑’˺ŸâªÉ«¬§«√À¬ÿ¥ wean7-12
Objective measurement √«¡∂÷ߺŸâªÉ«¬∑’Ë “¡“√∂∑”°“√∑¥ Õ∫µàÕ‰¥â
°“√·≈°‡ª≈ ’Ë¬π·° ¥’
Hemodynamic stable
√Ÿª·∫∫°“√À“¬„®ª°µ‘
Subjective clinical assessment √«¡∂ ÷ߺŸâªÉ«¬∑’˧«√À¬ÿ¥ wean
¢âÕ∫àß™’È
SpO2 85 - 90%, PaO2 > 60 mmHg, pH 7.32, PaCO2‡æ‘Ë¡ 10 mmHg
HR < 120 - 140 §√ —Èß/π“∑ ’ À√◊Õ‡ª≈ ’ˬπ < 20%,SBP < 180 - 200 ·≈– > 90 mmHg, BP ‡ª≈ ’ˬπ < 20%
RR 30 - 35/min À√◊Õ RR ‡ª≈’ˬπ < 50%
√–¥—∫§«“¡√ Ÿâ ÷°µ—«∑’Ë·¬à≈ß ‡™àπ somnolence, coma,agitation, anxietyDiaphoresis‡æ‘Ë¡ work of breathing ‡™àπ °“√„™â°≈â“¡‡π◊Èՙ૬À“¬„®,thoracoabdominal paradox

134 Õ¥‘»√ «ß…“ æ.∫. «“√ “√«—≥‚√§ ‚√§∑√«ßÕ°·≈–‡«™∫”∫ —¥«‘°ƒµ
°“√‡Õ“∑àՙ૬À“¬„®ÕÕ°®“°ºŸâªÉ«¬ (À≈—°∞“π„π√–¥—∫ 3)
ºŸâªÉ«¬∑ ’Ë “¡“√∂‡≈ ‘°„™â‡§√◊ËÕߙ૬À“¬„®‰¥â§«√æ‘®“√≥“∂Õ¥∑ àՙ૬À“¬„®ÕÕ° ‚¥¬ª√–‡¡‘π®“° airwaypatency ·≈– airway protection
ºŸâªÉ«¬∫“ß°≈ÿà¡¡’‚Õ°“ ‡°‘¥ upper airway obstruc-tion ‰¥â∫àÕ¬¿“¬À≈—ß°“√∂Õ¥∑àՙ૬À“¬„®ÕÕ° ´÷Ëßæ∫„πºŸâªÉ«¬∑ ’˵âÕß„™â‡§√◊ËÕߙ૬À“¬„®„π√–¬–‡«≈“π“π, „ à∑àՙ૬À“¬„®À≈“¬§√ —ÈßÀ√◊Õ„ à∑àÕ¬“° ·≈–æ∫„π‡æ»À≠ ‘ß¡“°°«à“™“¬13 ¥—ßπ—Èπ®÷ß·π–π”„Àâµ√«® cuff-leak ¿“¬„π24 ™—Ë«‚¡ß14-17 °àÕπ∑’Ë®–‡Õ“∑àՙ૬À“¬„®ÕÕ°
Cuff-leak test “¡“√∂µ√«®‰¥â‚¥¬ª≈àÕ¬ cuff ·≈ â«„À⺟âªÉ«¬À“¬„®¢≥–Õÿ¥∑àՙ૬À“¬„® øí߇ ’¬ß≈¡∑’Ë ‰À≈ºà“π¢â“ß∑àե⫬ stethoscope ∂Ⓣ¥â¬‘π‡ ’¬ß≈¡· ¥ß«à“∑“߇¥‘πÀ“¬„®µÕπ∫π°«â“ßæÕ‰¡à§«√‡°‘¥ªí≠À“ post-extubation stridor.
Cuff-leak volume µ√«®‰¥â‚¥¬„À⺟âªÉ«¬À“¬„®¥â«¬‡§√◊ËÕߙ૬À“¬„®·∫∫ª√‘¡“µ√ ·≈ ⫪≈àÕ¬ cuff ∫ —π∑÷°§à“exhaled tidal volume „π°“√À“¬„® 6 §√—Èß∂—¥¡“ π”§à“∑ ’˵˔∑’Ë ÿ¥ 3 „π 6 §à“¡“‡©≈’ˬ ∂ â“§à“ exhaled volume‡©≈’ˬ∑ ’ˉ¥âµà“ß®“°§à“ tidal volume ∑ ’˵—È߉«â¡“°°«à“ 110 ¡≈.· ¥ß«à“¢π“¥¢Õß∑“߇¥‘πÀ“¬„®‰¡àµ’∫ „π°√≥ ’∑’˺ŸâªÉ«¬∑”cuff leak test ·≈ ⫉¡àºà“π°“√∑¥ Õ∫·π–π”„Àâ„™â ste-roid À√◊Õ epinephrine πÕ°®“°π’ȧ«√µ√«®§«“¡ “¡“√∂„π°“√‰Õ §«“¡∂’Ë„π°“√¥Ÿ¥‡ ¡À–¢ÕߺŸâªÉ«¬¥â«¬ ‡æ ◊ËÕæ‘®“√≥“§«“¡æ√ âÕ¡¢Õß°“√ªÑÕß°—πµπ‡Õß·≈–°“√°”®—¥‡ ¡À–¢ÕߺŸâªÉ«¬°àÕπ∑’Ë®–‡Õ“∑ àՙ૬À“¬„®ÕÕ°18
°“√¥Ÿ·≈ºŸâªÉ«¬∑ ’ˉ¡àºà“π°“√∑¥ Õ∫¥â«¬ SBT(À≈—°∞“π„π√–¥—∫ 1)
ºŸâªÉ«¬∑’Ë ‰¡à “¡“√∂ºà“π°“√∑¥ Õ∫ SBT ‰¥â §«√æ—°°≈â“¡‡π◊ÈÕÀ“¬„® 24 ™—Ë«‚¡ß ·≈–‰¥â√—∫°“√µ√«®§âπ‡æ ◊ËÕÀ“ “‡Àµÿ ·≈–À≈—ß®“°∑ ’ˉ¥â√ —∫°“√·°â ‰¢·≈â« ‡¡◊ËÕºŸâªÉ«¬ ¡’¢âÕ∫ àß™’È∑ ’ˇ¢â“‰¥â°—∫°“√‡√ ‘Ë¡ wean µ“√“ß∑ ’Ë 1 °Á§«√‰¥â√—∫°“√∑¥ Õ∫‚¥¬ SBT ∑ÿ° 24 ™—Ë«‚¡ß9 ºŸâªÉ«¬∑’ˉ¡à “¡“√∂ºà“π°“√∑¥ Õ∫·≈–µâÕß„™â‡§√◊ËÕߙ૬À“¬„®µàÕπ—È𠧫√‰¥â√—∫°“√µ—È߇§√◊ËÕß∑ ’Ë∑”„À⺟âªÉ«¬‰¥â√—∫°“√æ—°ºàÕπ¡“°∑ ’Ë ÿ¥·≈–‰¡à∑”„À⇰‘¥°“√≈â“¢Õß°≈â“¡‡π◊ÈÕÀ“¬„®·≈–√à“ß°“¬3,5,19
°“√ª√–‡¡‘π„π°√≥’∑ ’˺ŸâªÉ«¬‰¡à “¡“√∂ºà“π SBT
ºŸâªÉ«¬∑’Ë wean ‰¡à‰¥â¡—°‡ªìπ®“° (µ“√“ß∑’Ë 4)
1. respiratory load ¬—ß¡“°Õ¬Ÿà (∑—Èß mechanicalloads ‡™àπ ‡ ¡À–¡“° pulmonary congestion À√◊Õmetabolic loads ‡™àπ CO2 §—Ëß, severe metabolic aci-dosis)
2. respiratory drive ¬—ß∑”ß“π‰¡à‰¥â µâÕߧ”π÷ß∂÷߬“∑’Ë„À⺟âªÉ«¬¥â«¬ ‡™àπ sedative ·≈– metabolic causes¥â«¬ ‡™àπ hypothyroid
3. respiratory strength ¬—ßÕàÕπ·√ßÕ¬Ÿà µâÕߧ”π ÷ß∂÷ß¿“«– malnutrition, electrolyte imbalance ‚¥¬‡©æ“–magnesium ·≈– phosphate
4. ¡’§«“¡º‘¥ª°µ‘∑“ß√–∫∫ cardiovascular √ à«¡¥â«¬·≈–¬—߉¡à‰¥â√—∫°“√·°â ‰¢ ‡™àπ congestive heart failure‡¡◊ËÕ‡ª≈’Ë¬π®“° positive ➟ negative pressure ventila-tion (®“°‡§√◊ËÕߙ૬À“¬„® ➟ ‰ª‡ªìπ T-piece) ∑”„Àâvenous return ‡æ‘Ë¡¡“°

ªï∑’Ë 25 ©∫ —∫∑’Ë 3 °√°Æ“§¡-°—𬓬π 2547 Weaning : an evidence-based approach 135
µ“√“ß∑ ’Ë 4 “‡ÀµÿÀ√◊Õªí®®—¬‡ √ ‘¡∑ ’Ë∑”„À⺟âªÉ«¬‰¡à “¡“√∂À“¬„®‰¥â‡Õß20
Increase Ventil atory LoadIncrease minute ventilation requirement
- Increase CO2 production : high calorie intake, fev er, sepsis, burn, trauma, increase muscle activity- Hyperventilation : pain, anxiety, restlessness, metabolic acidosis, sepsis- Increase physiologic dead-space (V D/VT) : pulmonary embolism, pulmonary hypoper fusion, late ARDS
Increase mechanical load- low thoracic and lung compliance : ARDS, kyphoscoliosis, auto PEEP, abdominal distention, pneumonia,
pulmonary edema, marked obesity- Increase resistive load : bronchospasm, secretion, small endotracheal tube, v entilator circuit and demand
valve
Inadequate Ventilatory CapacityInadequate central respiratory driv e
- Impaired consciousness / CNS suppressant drug- abnormal respiratory center : sev ere metabolic alkalosis, hypothyroidism
Respiratory pump failureThoracic wall abnormality : flail chestImpaired neural transmission- Cervical spine damage- Phrenic nerve injury- Peripheral neuropathy : Guillain-Barre syndrome, critical illness polyneuropathy- Neuromuscular disorder : Myasthenia gravis
Muscular dysfunction- Malnutrition- Severe electrolyte imbalance & metabolic disorder : potassium magnesium phosphate calcium hypothyroidism- Respiratory muscle ov erloading or fatigue- Myopathy, postneuromuscular blockage w eakness- Hyperinflation
Cardiovascular Disease- Left ventricular dysfunction, coronary ar tery disease, cardiac arrhythmia
Arterial Hypoxemia
Psychogenic Dependence

136 Õ¥‘»√ «ß…“ æ.∫. «“√ “√«—≥‚√§ ‚√§∑√«ßÕ°·≈–‡«™∫”∫ —¥«‘°ƒµ
°“√‡®“–§Õ (À≈—°∞“π„π√–¥—∫ 2) 21
§«√æ‘®“√≥“‡¡◊ËÕºŸâªÉ«¬Õ“°“√§ß∑ ’Ë·≈â« ·≈–¡’·π«‚πâ¡∑’˵âÕß„™â‡§√◊ËÕߙ૬À“¬„®„π√–¬–¬“« ‚¥¬ºŸâªÉ«¬∑’Ë®–‡®“–§Õπ—Èπ§«√‰¥âª√–‚¬™πå ¥—ßµàÕ‰ªπ ’È
● µâÕß°“√¬“ sedation „π¢π“¥∑ ’Ë Ÿß¡“°‡æ ◊ËÕ„Àâ∑πµàÕ°“√„ à∑àՙ૬À“¬„®ºà“π°≈àÕ߇ ’¬ß (trans-laryngeal tube)
● ºŸâªÉ«¬∑’Ë¡’°≈»“ µ√å°“√À“¬„® (respiratorymechanic) ∑’Ë®”°—¥ ( ÷Ëß¡—°· ¥ßÕÕ°‚¥¬°“√À“¬„® ‡√Á«) °“√‡®“–§Õ®–™à«¬≈¥·√ßµâ“π°“√À“¬„® ·≈–Õ“®≈¥°“√∑”ß“π¢Õß°≈ â“¡‡π◊ÈÕÀ“¬„®≈߉¥â
● ºŸâªÉ«¬∑ ’ËÕ“®‰¥âª√–‚¬™π å„π‡™‘ß®‘µ«‘∑¬“∑ ’Ë “¡“√∂°‘πÕ“À“√∑“ߪ“°‰¥â À√◊ÕÕÕ°‡ ’¬ßºà“π∑àÕ™π‘¥æ‘‡»… ´÷Ëß∑”„ÀâÕ“√¡≥ å¢ÕߺŸâªÉ«¬¥’¢÷Èπ
● ºŸâªÉ«¬∑’ˇ®“–§Õ·≈⫙૬„Àâ°“√‡§≈◊ËÕπ‰À«¥’¢÷ÈπÕ“®™à«¬„π¥â“𰓬¿“æ∫”∫—¥‰¥â¥’¢÷Èπ
√ÿª®“°À≈ —°∞“π°“√»÷°…“„πªí®®ÿ∫—π °“√ wean ºŸâªÉ«¬
ÕÕ°®“°‡§√◊ËÕߙ૬À“¬„®¡’¢âÕ¡Ÿ≈∑’Ë¡“°æÕ∑ ’Ë®–‡ªìπ·π«∑“ß„π°“√ wean ‰¥â §◊Õ
● µ√«®À“ºŸâªÉ«¬∑’Ëæ√ âÕ¡®– wean (µ“√“ß∑ ’Ë 1) ·≈–∑¥ Õ∫ weaning parameter (µ“√“ß∑’Ë 2)
● ∑”°“√ wean ‚¥¬ SBT 30 - 120 π“∑ ’ ‚¥¬µâÕߪ√–‡¡‘πºŸâªÉ«¬Õ¬à“ß„°≈♑¥‡ªìπ√–¬– ‚¥¬‡©æ“–„π 3 - 5 π“∑ ’·√° ·≈–À¬ÿ¥ wean ‡¡◊ËÕ¡’¢âÕ∫àß™’È (µ“√“ß∑ ’Ë 3)
● ºŸâªÉ«¬∑’ˉ¡àºà“π°“√∑¥ Õ∫µâÕßæ—°‡µÁ¡∑’ËÕ¬à“ßπâÕ¬24 ™—Ë«‚¡ß æ√ âÕ¡À“ “‡Àµÿ (µ“√“ß∑ ’Ë 4) ·≈–‡√ ‘Ë¡SBT ∑ ÿ° 24 ™—Ë«‚¡ß ‡¡ ◊ËÕºà“πµ“√“ß∑ ’Ë 1
‡Õ° “√Õâ“ßÕ‘ß1. Cook D, Meade M, Guyatt G, et al. Evidence repor t on
criteria for weaning from mechanical v entilation, Rockville,MD: Agency for Health care P olicy and Research, 1999.
2. Evidence-Based Guidelines for W eaning and discon-tinuing Ventilatory suppor t. Chest 2001:120: 357S-395S.
3. Cohen CA, Zagelbaum G, Gross D, et al. Clinical mani-festations of inspiratory muscle fatigue. Am J Med1982;73:308-316.
4. Jubran A and Tobin MJ. Pathophysiological basis ofacute respiratory distress in patients who fail a trial ofweaning from mechanical v entilation. Am J Respir CritCare Med 1997;155:906-915.
5. Vassilakopoulos T, Zakynthinos S and Roussos C. Thetension time index and the frequency/tidal v olume ratioare the major pathophysiologic determinants of w ean-ing failure and success. Am J Respir Crit Care Med1998;158:378-385.
6. Stroetz RW and Hubmayr RD. Tidal v olume mainte-nance during weaning with pressure suppor t. Am J RespirCrit Care Med 1995;152:1034-1040.
7. Esteban A, Alia I, Tobin MJ, et al. Ef fort of spontaneousbreathing trial duration on outcome of attempts todiscontinue mechanical v entilation: the Spanish LungFailure Collaborative Group. Am J Respir Crit CareMed 1999;159:512-518.
8. Vallverdu I, Calaf N, Subirana M, et al. Clinical charac-teristics, respiratory functional parameters, and outcomeof a two-hour T-piece trial in patients w eaning frommechanical ventilation. Am J Respir Crit Care Med1998;158:1855-1862.
9. Esteban A, Frutos F, Tobin MJ, et al. A comparisonof four methods of weaning patients from mechanicalventilation the Spanish Lung F ailure Collaborative Group.N Engl J Med 1995;332: 345-350.
10. Ely EW, Baker AM, Dunagan DP, et al. Ef fect on theduration of mechanical v entilation of identifying patientscapable of breathing spontaneously. N Engl J Med1996;335:1864-1869.
11. Brochard L, Rauss A, Benito S, Conti G, et al. Compari-son of three methods of gradual withdraw al fromventilatory suppor t during weaning from mechanicalventilation. Am J Respir Crit Care Med 1994;150:896-903.

ªï∑’Ë 25 ©∫ —∫∑’Ë 3 °√°Æ“§¡-°—𬓬π 2547 Weaning : an evidence-based approach 137
12. Kollef MH, Shapiro SD, Sliv er P, et al. A randomizedcontrolled trial of protocol-directed v ersus physician-directed weaning from mechanical v entilation. Crit CareMed 1997;25:567-574.
13. Epstein SK and Ciubotaru RL. Independence ef fectsof etiology of failure and time to reintubation onoutcome for patients failing extubation. Am J RespirCrit Care Med 1998;158:489-493.
14. Fisher MM and Raper RF. The çcuf f leaké test forextubation. Anaesthesis 1992;47:10-12.
15. Marik PE. The cuf f-leak test as a predictor of postex-tubation stridor: a prospectiv e study. Respir Care1996;41:509-511.
16. Miller RL and Cole RP. Association betw een reducedcuff leak volume and postextubation stridor. Chest 1996,110; 1035-1040.
17. Engoren M. Evaluation of the cuf f leak test in cardiacsurgery patients. Chest 1999;116:1029-1031.
18. Coplin WM, Pierson DJ, Cooley KD, et al. Implication ofextubation delay in brain injured patients meeting stan-dard weaning criteria. Am J Respir Crit Care Med2000;161:1530-1536.
19. Capdeviala X, Perrigault PF, Ramonatxo M, et al. Changesin breathing pattern and respiratory muscle per formanceparameters during dif ficulty weaning. Crit Care Med1998;26:79-87.
20. Mantous CA, Schmidt GA and Hall JB. Liberation frommechanical ventilation, a decade of progress. Chest1998;114:886-901.
21. Maziak DE, Meade MO and Todd TRJ. The timing oftracheostomy : a systemic review. Chest 1998;114:605-609.

ªï∑’Ë 25 ©∫ —∫∑’Ë 3 °√°Æ“§¡-°—𬓬π 2547 Can overnight pulse oximetry recording 139
Division of Respiratory Disease and Tuberculosis, Department of Medicine,Faculty of Medicine Siriraj Hospital, Mahidol University
CAN OVERNIGHT PULSE OXIMETRYRECORDING BE USED AS A SCREENING
MEASURE FOR OBSTRUCTIVE SLEEP APNEAManapol Kulpraneet M.D.Nitipatana Chierakul M.D.
Arth Nana MB., M.D.
Received for publication 25 December, 2003
∫∑§—¥¬àÕ: ¡π–æ≈ °ÿ≈ª√“≥’µ, π‘∏ ‘æ—≤πå ‡®’¬√°ÿ≈ ·≈–Õ√√∂ π“π“. °“√µ√«®§—¥°√Õß¿“«–À¬ÿ¥À“¬„®√–À«à“ßπÕπÀ≈—∫¥â«¬‡§√◊ËÕß pulse oximetry. «“√ “√«—≥‚√§ ‚√§∑√«ßÕ°·≈–‡«™∫”∫—¥«‘°ƒµ 2547;25:139-145 “¢“«‘™“‚√§√–∫∫°“√À“¬„®·≈–«—≥‚√§ ¿“§«‘™“Õ“¬ÿ√»“ µ√ å §≥–·æ∑¬»“ µ√廑√‘√“™æ¬“∫“≈ ¡À“«‘∑¬“≈ —¬¡À‘¥≈
¿“«–°“√À¬ÿ¥À“¬„®√–À«à“ßπÕπÀ≈ —∫°”≈—߇ªìπ∑’Ë π„®°—πÕ¬à“ß¡“° ‡π◊ËÕß®“°‡ªìπªí®®—¬ à߇ √ ‘¡„À⇰‘¥‚√§¢ÕßÀ≈Õ¥‡≈◊Õ¥ ¡Õß·≈–À—«„® °“√«‘π‘®©—¬µâÕß„™â°“√µ√«®°“√πÕπÀ≈—∫¡“µ√∞“π ÷Ë߉¡à “¡“√∂∑”‰¥â·æ√àÀ≈“¬„πª√–‡∑»‰∑¬ °“√»÷°…“π ’ȵâÕß°“√‡ª√ ’¬∫‡∑ ’¬∫º≈°“√µ√«®§—¥°√Õߥ⫬‡§√◊ËÕß pulse oximetry °—∫°“√µ√«®°“√πÕπÀ≈—∫¡“µ√∞“π „πºŸâªÉ«¬∑’Ë ß —¬®”π«π 51 √“¬ ‚¥¬„™â‡°≥±å°“√«‘π‘®©—¬∑’Ë√–¥—∫§«“¡º‘¥ª°µ‘µà“ßÊ°—πæ∫«à“¡’ºŸâªÉ«¬ 40 √“¬¡’¿“«–°“√À¬ÿ¥À“¬„®√–À«à“ßπÕπÀ≈—∫ ‚¥¬„™â‡°≥±å oxygen desaturation ‡°‘π√âÕ¬≈– 3,π“π°«à“ 10 «‘π“∑’, ¡“°°«à“ 5 §√ —ÈßµàÕ™—Ë«‚¡ß ¡’§«“¡‰«, §«“¡®”‡æ“–, º≈∫«°„π°“√«‘π‘®©—¬ ·≈–º≈≈∫„π°“√«‘π‘®©—¬ ‡∑à“°—∫√âÕ¬≈– 82, 100, 100 ·≈– 60 µ“¡≈”¥—∫ º≈≈∫≈«ß®–æ∫„πºŸâªÉ«¬∑’Ë¡’¿“«–°“√À¬ÿ¥À“¬„®√–À«à“ßπÕπÀ≈ —∫√–¥—∫§«“¡√ ÿπ·√ßπ âÕ¬ ¥—ßπ—Èπ°“√µ√«®¥â«¬‡§√◊ËÕß pulse oximetry “¡“√∂„™â§—¥°√ÕߺŸâªÉ«¬∑’Ë ß —¬¿“«–°“√À¬ÿ¥À“¬„®√–À«à“ßπÕπÀ≈—∫∑ ’Ë¡’§«“¡√ÿπ·√ß√–¥—∫ª“π°≈“ߢ÷Èπ‰ª‰¥â¥’
«“√ “√«—≥‚√§ ‚√§∑√«ßÕ°·≈–‡«™∫”∫—¥«‘°ƒµThai Journal of TuberculosisChest Diseases and Critical Care

140 Manapol Kulpraneet et al. «“√ “√«—≥‚√§ ‚√§∑√«ßÕ°·≈–‡«™∫”∫ —¥«‘°ƒµ
Abstract :Background: Although the prevalence of obstructive sleep apnea (OSA) in Thailand is uncertain,it is being increasingly recognized because of its adverse sequelae, especially cardiovascular andcerebrovascular events. Conventional diagnosis of OSA requires sophisticated polysomnography(PSG) which is not widely available. The purpose of this study is to verify the validity of overnightpulse oximetry (PO) recording for the diagnosis of OSA and to determine the optimum cutoff level.Materials and Methods: Fifty-one patients with clinical suspicion of OSA underwent PSG andseparate PO recording in the same night. The oxygen desaturation index (ODI) as measured by POas events/h of ≥ 3 % and ≥ 4% decrease from baseline which persisted ≥ 10, ≥ 15, and ≥ 20 secwere evaluated, and different cut off points at > 5, > 10, and > 15 events/h were also determined.A comparison between each ODI and apnea-hypopnea index (AHI) from PSG was finally explored.Results : Forty patients were diagnosed as having OSA according to the criteria of having AHI > 5events/h. Patients with ODI ≥ 3% for ≥ 10 sec for > 5 events/h had the highest diagnostic yield forthe sensitivity, specificity, positive predictive value, and negative predictive value of 82, 100, 100,and 60% respectively. False negative results were frequently observed among those with mild OSA(AHI < 15 events/h).Conclusion : Overnight pulse oximetry recording was useful for the screening of moderate to severeobstructive sleep apnea in clinically suspected patients.
IntroductionObstructive sleep apnea (OSA) is a common
syndrome, the prevalence varying from 2 - 4% inone report.1 Although the prevalence of OSA inThailand is not known, it is now increasinglyrecognized by physicians and there is increasedpublic awareness about it as well.2 This syndromecan lead to many adverse sequelae includingcardiovascular and cerebrovascular events, lossof efficiency at work, and an increased incidenceof car accidents due to sleepiness.3-4
Polysomnography (PSG) is the standard toolused for the diagnosis of OSA. It is a technically
complicated and costly investigation. Alternativemethods for diagnosing OSA have been introduced,and overnight pulse oximetry (PO) recording is oneof the most widely used. Conflicting data concern-ing the reliability of this screening tool have beenreported in the literature.5-14
Because OSA has been linked to co-morbid-ity and mortality as described above, early diagno-sis should be made to prevent its costly adverseconsequences. The introduction of a diagnosticmethod that is cost-saving with good accuracywould be suitable for limited resource country.This study aims to determine the validity of PO as

ªï∑’Ë 25 ©∫ —∫∑’Ë 3 °√°Æ“§¡-°—𬓬π 2547 Can overnight pulse oximetry recording 141
a screening method for OSA in Thailand, and alsoto determine the optimum cut-off level.
Materials and MethodsSubjects
All patients referred to the Sleep Laboratory,Division of Respiratory Disease and Tuberculosisat Siriraj Hospital for overnight PSG study duringJanuary 2001 to January 2002 were recruited.The medical histories of these patients were takenand they also responded to sleep questionnaires.General physical examination was performedwith special attention given to the presence ofany underlying diseases which affect oxygenationstatus such as obstructive lung or structural heartdiseases. Those in whom the finger probe of POcould not be applied due to peripheral limbischemia or who declined participation in the studywere excluded. All participants gave informedconsents, and the study was approved by thelocal Ethical Committee.
ProceduresPatients underwent standard overnight PSG
using diagnostic criteria of the Association of SleepDisorder Centers (ASDC) guidelines. At least 3 hoursof sleep must be obtained for evaluation. Apneawas defined as cessation of airflow for 10 sec.Hypopnea was defined as a decrease of airflow to1/3 of baseline associated with 3% oxygendesaturation. The apnea-hypopnea events/hour(apnea-hypopnea index = AHI) were scored auto-matically. OSA was defined as an apnea-hypopneaindex (AHI) of > 5. The severity of OSA was definedas severe if AHI > 30, moderate > 15-30, and mild> 5-15.15 The scoring was performed automatically.
During the PSG study, patients underwentsimultaneous PO recording with INVIVO 4500 plus
4 (Sensor Medics, CA, USA) in the opposite handof PO in the system of PSG. This instrument wasable to record oxygen saturation every 6 sec con-tinuously and store it for later analyses usingdefault criteria by EPOCH programme. The criteriadetermining that the was to be analyzed washaving oxygen desaturation of 3% and 4%from baseline. Such an event was analyzed if itpersisted for 10 sec, 15 sec, and 20 sec.The cut-off points for abnormality were those ofoxygen desaturation events (oxygen desaturationindex-ODI) of >5, >10 and >15 events per hour(ODI -5, ODI-10, and ODI-15 respectively).
Data AnalysisData was analyzed using PO as the test and
PSG as the gold standard. Each event with an ODIof ≥3% or 4% which persisted for >10, >15 and>20 sec was determined for sensitivity, specificity,positive predictive value (PPV), negative predictivevalue (NPV), and accuracy using 2 x 2 contingencytable. Subgroup analysis of OSA severity levelsaccording to the AHI was also evaluated.
ResultsA total of 55 patients were recruited to the
study. Fifty-one of these had qualified PO tracingfor evaluation, 39 were male and 12 were female.Forty patients were diagnosed with OSA, 34 weremale and 6 were female, with the mean age of48.5 years and mean AHI of 48.7. There were 28patients with severe OSA, 1 patient with moderateOSA, and 11 patients with mild OSA.
When a diagnosis of OSA was establishedby PSG the results of simultaneous PO recordingat different cut-off points were analyzed. For 3%desaturation persisting >10 sec at ODI >5 (10 sec,

142 Manapol Kulpraneet et al. «“√ “√«—≥‚√§ ‚√§∑√«ßÕ°·≈–‡«™∫”∫ —¥«‘°ƒµ
3%, ODI-5) there were 32 patients with a positivePO test, at ODI >10 (10 sec, 3%, ODI-10) therewere 27 patients with a positive PO test, and atODI >15 (10 sec, 3%, ODI-15) there were 26
patients with a positive PO test. There was nonewith false positive test result. The sensitivity,specificity, PPV, and NPV for each cut-off pointare present in Table 1.
Table 2 A comparison of accuracy at each criteria and cut-off point between each severity accordingto AHI.
Criteria and cut-off point Mild (n=11) Moderate (n=1) Severe (n=28)
10 sec, 3%, ODI - 5ODI - 10ODI - 15ODI - 5ODI - 10ODI - 15ODI - 5ODI - 10ODI - 15
0.70.20.1
0.40.10
0.270.090
0
0
0
0.890.890.89
0.890.860.71
0.860.710.57
Table 1 Sensitivity, specificity, positive predictive value (PPV) and negative predictive value (NPV) ofpulse oximetry at each criteria and cut-off point. Numbers in parentheses are related to thedesaturation of 4%.
10 sec, 3% (4%)
15 sec, 3% (4%)
20 sec, 3% (4%)
Cut-off pointCriteria Sensitivity (%) Specificity (%) PPV (%) NPV (%)
ODI - 5ODI - 10ODI - 15
ODI - 5ODI - 10ODI - 15ODI - 5ODI - 10ODI - 15
100 (100)
100 (100)
100 (100)
100 (100)
100 (100)
100 (100)
82 (74)69 (69)67 (51)74 (69)64 (49)51 (44)68 (63)53 (45)40 (33)
61 (52)48 (48)46 (37)52 (48)44 (35)37 (33)46 (42)37 (33)32 (29)
15 sec, 3%,
20 sec, 3%,

ªï∑’Ë 25 ©∫ —∫∑’Ë 3 °√°Æ“§¡-°—𬓬π 2547 Can overnight pulse oximetry recording 143
For each severity level of OSA, the authorsfound that PO had positive results more frequentlyin severe OSA than in mild OSA. At 10 sec, 3%,ODI-5 the test was positive in 25 of 28 patientswith severe OSA and 7 of 10 patients with mildOSA. The accuracy of PO at each cut-off pointfor each severity level of OSA is present in Table2; the 10 sec, 3%, ODI-5 was found to yield thehighest accuracy.
DiscussionIt was demonstrated in this study that over-
night PO recording has very high specificity andpositive predictive value for the diagnosis of OSA.The sensitivity of this measurement at differentcriteria and cut-off points ranged between 33%(20 sec, 4%, ODI-5) and 82% (10 sec, 3%, ODI-5).The authors recommend the 10 sec, 3%, ODI-5,which has the highest sensitivity for screening ofOSA.
The high specificity with modest sensitivityof PO measured in this study was comparable tothat of previous studies.6,7,10-13 Those reports oflow sensitivity with high specificity or high sensi-tivity but low specificity were from studies usingdifferent diagnostic criteria and cut-off points bothfor PO and PSG. In 3 studies using AHI of >15 asstandard diagnostic criteria for OSA, the sensitivitywas about 40% with a specificity of 98%.7,10,12
The criteria for the diagnosis of OSA defined bythe American Academy of Sleep Medicine TaskForce is AHI of more than 515. This cut-off levelhas high correlation with increasing prevalence ofhypertension, excessive daytime sleepiness, andcar accidents.15,16 So the authors used this lessrigid criteria, different from previous studies, to
determine the abnormal threshold defining theclinical significance of this syndrome.7,10,12
There are other differences for considerationbetween our study and other ones. First, otherstudies did not compare overnight PO recordingand PSG in the same night as was done in thisstudy. Swieca et al reported the discrepancy ofAHI between each night of the studies.17 Second,signal averaging time also had an effect on theestimation of desaturation events. The averagingtime of 12 sec used by Gyulay et al may result inan underestimation of desaturation events.18 Weused 6 sec as the signal averaging time to over-come this limitation and improve the sensitivity.Lastly, the modest sensitivity of PO may resultfrom apnea episodes with unaccompanieddesaturation. By using the lower threshold at 10sec, 3%, ODI-5 as in our study, the sensitivity ofPO recording was increased.
The specificity and positive predictive valueof overnight PO were very high, so the furthermanagement of OSA can be done with high con-fidence to the patient who has positive result. Butbecause of its low negative predictive value, stan-dard PSG should be performed in patients whoare highly suspected of having OSA and negativePO recording. The higher accuracy for detection ofsevere OSA with PO may be due to the fact thatthe less severe patient might have hypopnea whichdoes not result in significant desaturation in POrecording. In addition, the duration of apnea maybe too short to affect the desaturation episode.
Potential limitations in this study should bementioned. First, the small sample size of 51patients may not be enough to determine a deci-

144 Manapol Kulpraneet et al. «“√ “√«—≥‚√§ ‚√§∑√«ßÕ°·≈–‡«™∫”∫ —¥«‘°ƒµ
AcknowledgementThe PO recording machine was kindly
provided by E for L International Co., Ltd.
References1. Young T, Palta M, Dempsey J, Skatrud J, W eber S
and Badr S. The occurrence of sleep-disorderedbreathing among middle-aged adults. N Eng J Med1993; 328:1230-1235.
2. Charoenpan P, Thanakitcharu S, Muntarbhorn K,et al. Sleep apnoea syndrome in RamathibodiHospital: clinical and polysomnographic baselinedata. Respirology 1999; 4:371-374.
3. He J, Kryger MH, Zorick FJ, Conw ay W and Roth T.Mortality and apnea index in obstructiv e sleep apnea:experience in 385 male patients. Chest 1998; 94:9-14.
4. Findley LJ, Unverzagt ME and Suratt PM. Automobileaccidents involving patients with obstructiv e sleepapnea. Am Rev Respir Dis 1988; 138:337-340.
5. Svanborg E, Larsson H, Carlsson-Nordlander B andPirskanen R. A limited diagnostic inv estigation for
obstructive sleep apnea syndrome. Chest 1990;98:1341-1345.
6. William AJ, Yu G, Santiago S and Stein M. Screeningfor sleep apnea using pulse oximetry and a clinicalscore. Chest 1991; 100:631-635.
7. Gyulay S, Olson LG, Hensley MJ, King MT, Allen Mand Saunders NA. A comparison of clinical assess-ment and home oximetry in the diagnosis of obstruc-tive sleep apnea. Am Rev Respir Dis 1993; 147:50-53.
8. Series F, Marc I, Cormier Y and La F orge J. Utility ofnocturnal home oximetry for case finding in patientswith suspected sleep apnea hypopnea syndrome.Ann Intern Med 1993; 119:449-453.
9. Rauscher H, Popp W and Zwick H. Model for inv esti-gating snorers with suspected sleep apnoea. Thorax1993; 48:275-279.
10. Ryan PJ, Hilton MF, Boldy DAR, et al. V alidation ofBritish Thoracic Society guidelines for the diagnosisof the sleep apnoea/hypopnoea syndrome: canpolysomnography be av oided? Thorax 1995; 50:972-975.
11. Chiner E, Signes-Costa J, Arriero JM, Marco J, FluenteI and Sergado A. Nocturnal oximetry for the diagnosisof the sleep apnoea hypopnoea syndrome: a methodto reduce the number of polysomnographies. Thorax1999; 54:968-971.
12. Golpe R, Jimenez A, Carpizo R and Cifrian JM. Utilityof home oximetry as a screening test for patientswith moderate to severe symptoms of obstructiv e sleepapnea. Sleep 1999; 22:932-937.
13. Vazquez JC, Tsai WH, Flemons WW, et al. Automatedanalysis of digital oximetry in the diagnosis ofobstructive sleep apnoea. Thorax 2000; 55:302-307.
14. Wiltshire N, Kendrick AH and Catterall JR. Home oxim-etry studies for diagnosis of sleep apnea/hypopneasyndrome. Chest 2001; 120:384-389.
15. American Academy of Sleep Medicine T ask Force.Sleep-related breathing disorders in adults: recom-mendations for syndrome definition and measurementtechniques in clinical research. Sleep 1999; 22:667-689.
sive conclusion. Second, the authors could notcompletely exclude the patients with some dis-eases known to affect the nocturnal oxygenationstatus by mean of routine physical examination.Lastly, this study had only one subject with mod-erately severe OSA, so the result in this subgroupmay not have conclusive implications.
In conclusion, overnight PO is useful for thescreening of OSA. This will enhance the reductionin number of standard PSG, which is unavailablenationwide in Thailand, that need to be performed.To increase the sensitivity of overnight PO record-ing, 10 sec, 3%, ODI-5 should be used as thecriteria and cut-off point for detecting anyabnormality. In cases strongly suspected of hav-ing OSA, PSG should be further performed when-ever an unanticipated negative PO result is found.

ªï∑’Ë 25 ©∫ —∫∑’Ë 3 °√°Æ“§¡-°—𬓬π 2547 Can overnight pulse oximetry recording 145
16. Young T, Blustein J, F inn L and Palta M. Sleep-disordered breathing and motor v ehicle accidents ina population-based sample of employed adults. Sleep1997; 20:608-613.
17. Swieca J and Westbrool PR. Relationship betw eenbody position dependence of apnea and hypopnea
and overall severity of sleep-disordered breathing.Am J Respir Crit Care Med 1994; 49:54-58.
18. Farre R, Montserrat JM, Ballester E, et al. Impor tanceof the pulse oximeter av eraging time when measuringoxygen desaturation in sleep apnea. Sleep 1998;21:386-390.

ªï∑’Ë 25 ©∫ —∫∑’Ë 3 °√°Æ“§¡-°—𬓬π 2547 The Retinoic Acid Syndrome : 147
THE RETINOIC ACID SYNDROME:A STEROID-RESPONSIVE ACUTE
RESPIRATORY DISTRESS SYNDROME (ARDS).THE FIRST CASE REPORT OF THAILAND
‡©≈‘¡ ≈ ‘Ë«»√ ’ °ÿ≈ æ.∫.∫ÿ≠ ¡ ™—¬¡ß§≈ æ.∫.
¿“§«‘™“Õ“¬ÿ√»“ µ√å §≥–·æ∑¬»“ µ√ å ¡À“«‘∑¬“≈—¬‡™’¬ß„À¡à
Abstract: Retinoic acid syndrome (RAS) is a major cause of death in acute promyelocytic leukemia(APL) patients, who have been treated with all-trans retinoic acid (ATRA). This report describes a 49-year-old woman, who developed fever and acute hypoxemic respiratory failure following 8 days oftreatment with ATRA for APL. Her condition, including clinical manifestations, diffuse infiltration on achest radiograph and gas exchange (PaO2/FiO2), fulfilled the criteria of acute respiratory distresssyndrome (ARDS). She had been treated with mechanical ventilation with high fractional inspired oxygentension and positive end-expiratory pressure (PEEP) for 2 days without response, but she respondeddramatically to intravenous dexamethasone. To the best of our knowledge, this is the first case report ofRAS in Thailand.
∫∑§—¥¬àÕ: ‡©≈‘¡ ≈ ‘Ë«»√’ °ÿ≈ ·≈–∫ÿ≠ ¡ ™—¬¡ß§≈. The Retinoic Acid Syndrome: A Steroid-Responsive AcuteRespiratory Distress Syndrome (ARDS). The First Case Report of Thailand. «“√ “√«—≥‚√§ ‚√§∑√«ßÕ°·≈–‡«™∫”∫—¥«‘°ƒµ;25:147-153¿“§«‘™“Õ“¬ÿ√»“ µ√å §≥–·æ∑¬»“ µ√ å ¡À“«‘∑¬“≈—¬‡™’¬ß„À¡à
Retinoic acid syndrome (RAS) ‡ªìπµâπ‡Àµÿ ”§—≠¢Õß°“√‡ ’¬™’«‘µ„πºŸâªÉ«¬ acute promyelocytic leuke-mia (APL) ´÷Ë߉¥â√—∫°“√√ —°…“¥â«¬ all-trans retinoic acid (ATRA) ∫∑§«“¡©∫ —∫π’È√“¬ß“πºŸâªÉ«¬À≠‘ßÕ“¬ÿ 49 ªï ´÷Ëߪɫ¬‡ªìπ APL ·≈–¡’‰¢â√à«¡°—∫√–∫∫°“√À“¬„®≈ ⡇À≈«‡©’¬∫æ≈—π™π‘¥¢“¥ÕÕ° ‘‡®π (acute hypoxemic respira-tory failure) À≈ —ß®“°√—°…“¥â«¬ ATRA ‡ªìπ‡«≈“ 8 «—π ≈—°…≥–∑“ߧ≈‘π‘°¢ÕߺŸâªÉ«¬√à«¡°—∫ infiltrations „πªÕ¥∑—Èß 2 ¢â“ß∑ —Ë«Ê ‰ª®“°¿“æ√ —ß ’∑√«ßÕ°·≈–§«“¡º‘¥ª°µ‘¢Õß°“√·≈°‡ª≈’ˬπ°ä“´ (PaO2/FiO2) ‡¢â“‰¥â°—∫‡°≥±å°“√
Received for publication 3 February, 2004
«“√ “√«—≥‚√§ ‚√§∑√«ßÕ°·≈–‡«™∫”∫—¥«‘°ƒµThai Journal of TuberculosisChest Diseases and Critical Care

148 ‡©≈ ‘¡ ≈ ‘Ë«»√ ’ °ÿ≈ ·≈–∫ ÿ≠ ¡ ™—¬¡ß§≈ «“√ “√«—≥‚√§ ‚√§∑√«ßÕ°·≈–‡«™∫”∫ —¥«‘°ƒµ
«‘π‘®©—¬¢Õß°≈ ÿà¡‚√§√–∫∫°“√À“¬„®≈”∫“°‡©’¬∫æ≈ —π (acute respiratory distress syndrome, ARDS)ºŸâªÉ«¬‰¥â√—∫°“√√ —°…“¥â«¬°“√„ à‡§√◊ËÕߙ૬À“¬„® √ à«¡°—∫„ÀâÕÕ°´‘‡®π„π√–¥—∫ Ÿß·≈–·√ߥ—π∫«°‡¡ ◊ËÕ ‘Èπ ÿ¥°“√À“¬„®ÕÕ° (positive end-expiratory pressure, PEEP) ‡ªìπ‡«≈“ 48 ™—Ë«‚¡ß ·µà‰¡àµÕ∫ πÕßµàÕ°“√√—°…“„π¢≥–∑’Ë≈ —°…≥–∑“ߧ≈‘π‘°¢ÕߺŸâªÉ«¬¥’¢÷ÈπÕ¬à“ß√«¥‡√Á«¿“¬À≈—߉¥â√ —∫°“√√—°…“¥â«¬°“√©’¥¬“ dexamethasone‡¢â“∑“ßÀ≈Õ¥‡≈◊Õ¥¥” √“¬ß“πºŸâªÉ«¬√“¬π ’ȇªìπ√“¬ß“π‚√§ RAS ‡ªìπ§√—Èß·√°„πª√–‡∑»‰∑¬
IntroductionThe value of all-trans retinoic acid (ATRA) in
the treatment of acute promyelocytic leukemia (APL,M3) is well established. ATRA yields a completeremission rate of around 90%1 and has made APLthe most curable acute myeloid leukemia (AML) inadults.2 Although ATRA improves disease-freesurvival and overall survival rate, as compared withconventional chemotherapy for the treatment of APL,it does not decrease the early mortality rate.2
The early death following treatment with ATRA wasprimarily caused by the serious pulmonary compli-cation, retinoic acid syndrome (RAS).2
Case reportA 49-year-old woman presented with a 10-day
history of high-grade fever, malaise and multipleareas of subcutaneous ecchymosis at all extremi-ties. She went to a community hospital beforereferred to our center for evaluation of pancytopenia[initial complete blood counts (CBC) revealedhemoglobin of 9.5 gm%, hematocrit of 27.7%, awhite blood cell (WBC) count of 1,100/mm3 with78% neutrophils, 20% lymphocytes, and 1% mono-cytes and a platelet count of 23,000/mm3]. Her vital
signs on admission were a temperature of 38.8OC,respiratory rate of 20/min, pulse rate of 130/min andblood pressure of 150/70 mmHg. Other positivefindings on physical examination included mildly paleconjunctivae, mild icterus, and multiple areas ofecchymosis at all extremities. Neither gum hypertro-phy nor hepatosplenomegaly was observed. Bonemarrow aspiration showed 83% of promyelocytesand a decreased number of megakaryocytes, whichwere typical findings in APL. Other laboratoryfindings included mild indirect hyperbilirubinemia(direct bilirubin/total bilirubin = 1.02/2.72 mg/dl) andprolonged prothrombin and partial thromboplastintime, which might be caused by disseminated intra-vascular coagulation (DIC). The chest radiographywas normal (fig. 1). All-trans retinoic acid (ATRA)was started at a dose of 45 mg/m2/day. CBC on thefirst day of ATRA treatment showed hemoglobin of5.4 gm%, hematocrit of 16.1%, a WBC count of14,800/mm3 with 70% promyelocytes, 4% bandforms, 4% neutrophils, 20% lymphocytes, and 2%monocytes and a platelet count of 19,800/mm3.
During treatment with ATRA, she still had fever.On the eighth day of ATRA therapy, she developed
Abbreviations: AML = acute myeloid leukemia, APL = acute promyelocytic leukemia, ARDS = acute respiratory distresssyndrome, ATRA = all-trans retinoic acid, DIC = disseminated intrav ascular coagulation, PEEP = positiv e end-expiratorypressure, RAS = retinoic acid syndrome.

ªï∑’Ë 25 ©∫ —∫∑’Ë 3 °√°Æ“§¡-°—𬓬π 2547 The Retinoic Acid Syndrome : 149
tachypnea. Her vital signs were a temperature of40.4oC, pulse rate of 120/min, respiratory rate of 40/min, and blood pressure of 140/90 mmHg. General-ized crepitations were heard on chest physical ex-amination. Chest roentgenography showed normalheart size with diffuse alveolar infiltrations of bothlungs (fig. 2), without a drop in hematocrit or imbal-ance of fluid intake and output. CBC, performed oneday earlier, demonstrated hemoglobin of 6.0 gm/dl,hematocrit of 17%, rising WBC count to 15,800/mm3 with 57% promyelocytes, 14% neutrophils, 24%lymphocytes, and 5% monocytes, and a platelet countof 20,500/mm3. Her condition rapidly deterioratedto acute hypoxemic respiratory failure requiring tra-cheal intubation and mechanical ventilation (MV).Mechanical ventilatory settings included assist/con-trol mode, positive end-expiratory pressure (PEEP)of 5 cm H2O, fractional inspired oxygen (FiO2) of1.0 and tidal volume of 500 ml. Arterial blood gasanalysis after 30 minutes of MV showed a pH of
7.225, PaO2 of 72.4 mmHg and PaCO2 of 51.0 mmHg.Her conditions did not respond to broad-spectrumantibiotics and diuretics. Forty-eight hours later, af-ter the results of sepsis work-up turned out to benegative and CBC displayed a peak WBC of 57,800/mm3, a diagnosis of retinoic acid syndrome (RAS)was made. Twenty mg/day of intravenous dexam-ethasone was prescribed and ATRA was discontin-ued. Her condition comprising temperature, respira-tory rate, lung signs, requirement of high FiO2 andlung mechanics (airway pressure) dramatically im-proved within 24 hours. Her chest radiography, taken48 hours after administration of dexamethasone,showed much clearing of alveolar infiltrations (fig.3), and a full-dose of cytosine arabinoside andidarubicin for the first induction to remission of APLwere administered on that day. Her conditionremained stable until febrile neutropenia developedone week later. Eventually, she died from sepsis onthe 17th day after chemotherapy.
Fig 1: Chest radiograph that was taken on admission. Fig 2: Chest radiograph that was taken on 8th dayof ATRA therapy

150 ‡©≈ ‘¡ ≈ ‘Ë«»√ ’ °ÿ≈ ·≈–∫ ÿ≠ ¡ ™—¬¡ß§≈ «“√ “√«—≥‚√§ ‚√§∑√«ßÕ°·≈–‡«™∫”∫ —¥«‘°ƒµ
DiscussionThe mechanism of ATRA action for the treat-
ment of APL is through terminal differentiation ofmalignant cells into phenotypically mature myeloidcells, instead of rapid cell lysis induced by conven-tional chemotherapy.1 Therefore, unlike cytotoxicmedications, ATRA does not initiate disseminatedintravascular coagulation (DIC). Actually, the earliestsign of response to ATRA treatment is normalizationof DIC.3 In addition, ATRA induces complete remis-sion of APL without causing bone marrow hypopla-sia and its consequent pancytopenia.3 Therefore,ATRA does not increase the incidence of infection,that is the major cause of high morbidity and mor-tality in leukemic patients.1 Although it appears tobe safer than conventional chemotherapy, many sideeffects from ATRA have been reported. Most of themare usually moderate in severity such as dryness of
skin and mucosa, headache, bone pain, hyperbiliru-binemia, hypertransaminasemia, hypertriglyceridemiaand intracranial hypertension with pseudotumorcerebri.1 Two other major side effects, which may beassociated with poor outcome, are hyperleukocytosisand RAS.15
The occurrence of hyperleukocytosis (peakWBC 10,000-15,000/mm3) around day 7-15 of treat-ment is common.3,4 Some patients may have rap-idly-developed hyperleukocytosis leading to clinicalsigns of leukostasis (stroke, myocardial infarction,respiratory failure and renal failure).1 Treatment ofthese patients requires leukapheresis and intensivechemotherapy to achieve a rapid reduction in leuko-cyte count for the prevention of clinical complica-tions.1 Our patient developed hyperleukocytosis (WBC> 15,000/mm3) on day 7 of ATRA therapy. Althoughshe had no signs of leukostasis, this high WBC mightbe associated with the RAS that developed one daylater.
RAS is the most serious toxicity of ATRA. Theincidence ranges from 5% to 27%.5 There is no sexor age predominance.6,7 The overall incidence of RASdoes not differ between new and retreatment cases.8
Although patients with RAS experience a higher peakleukocyte count compared to patients without it, anelevated WBC count is not uniformly associated withRAS.8 Only 32% to 42% of patients who have apeak leukocyte count over 20,000/mm3 develop thissyndrome.7,8 It had been suggested that patientswho had a WBC count higher than 5,000/mm3 onday 1, or higher than 6,000/mm3 on day 5, or higherthan 10,000/mm3 on day 10, or higher than 15,000/mm3 on day 15 were at increased risk of RAS devel-opment.9 Our case had a WBC count of 15,800/mm3
Fig 3: Chest radiograph that was taken 48 hoursafter dexamethasone administration

ªï∑’Ë 25 ©∫ —∫∑’Ë 3 °√°Æ“§¡-°—𬓬π 2547 The Retinoic Acid Syndrome : 151
on day 7, just before the onset of RAS, and it in-creased to 57,800/mm3 48 hours later. This sug-gested that the rate of a rising WBC count might bea better predictor of RAS than a WBC count per se.However, it has been proven that an initial WBCcount and rate of rising WBC does not statisticallycorrelate with the development of the syndrome.5,8Besides, it is not necessary for RAS to be associ-ated with hyperleukocytosis. Only one-third of pa-tients with RAS have a WBC count of over 20,000/mm.3,7
The onset of RAS is 2-47 days after startingtreatment with ATRA, with a median of 11-12days. 2-5-7 Our patient developed RAS on the 8th dayof treatment. In general, clinical manifestationsinclude fever, respiratory distress, pleural effusion,pericarditis with pericardial effusion, lower-extremityor generalized edema, weight gain, episodic hypoten-sion, hyperbilirubinemia and acute renal failure.7 Chestradiographis show interstitial infiltrates and pleuraleffusions in all cases.7 Arterial blood gas analysisalways reveals hypoxemia that is typical of intrapul-monary right-to-left shunting.7 All characteristics ofthis syndrome meet the criteria of acute respiratorydistress syndrome (ARDS) that consist of acute on-set, bilateral infiltrates on chest radiography, pulmo-nary artery wedge pressure 18 mmHg or absenceof clinical evidence of left atrial hypertension, andPaO2: FiO2 200.10 Treatment of ARDS includes propersupportive care, particularly mechanical ventilation,and management of treatable causes such assepsis or pneumonia.10 The role of corticosteroids inthe treatment of ARDS is limited to only the latefibrosing-alveolitis phase of the disease.10
In contrast, ARDS caused by RAS is highlyresponsive to steroids and the outcome of the
disease depends on how quickly systemic steroidsare prescribed for the patient. The benefits of earlyintervention with steroids in symptomatic patients,irrespective of WBC count, clearly outweigh the risksassociated with pneumonia or congestive heartfailure.7 The medication commonly used for thetreatment of RAS is intravenous dexamethasoneat a dose of 10 mg every 12 hours for a least 3 days.7
Seventy-five per cent of patients respond promptlyto the treatment. Temporary discontinuation of ATRAmay not be necessary if the disease has not reacheda moderate to severe degree and dexamethasone isinstituted early. In the case of ATRA being stopped,it can be successfully reintroduced following the reso-lution of RAS without concomittent steroids, but closeobservation is recommended.5 Leukapheresis orcytotoxic therapy in a moderate dose is not usefulafter respiratory distress is established.7
The major histopathologic findings, mostlyobtained from postmortem studies, include pulmo-nary interstitial and intraalveolar infiltration with ma-turing myeloid cells.7 In the case of prominent intra-alveolar myeloid infiltrates, additional findings indica-tive of endothelial cell damage are present andinclude intra-alveolar edema, intra-alveolar hemor-rhage and fibrinous exudates.5 These histologic find-ings suggest that endothelial damage and capillaryleakage play the major role in the pathogenesis ofRAS.5 In addition, there is evidence that ATRAincreases expression of the intercellular adhesionmolecule (ICAM) -1 and -3, and integrins (leukocyteadhesion receptor) expression on the leukemic cellsurface, which enhances cell adherence to the cap-illary endothelium (heterotypic adhesion) and extrava-sation from the blood.11

152 ‡©≈ ‘¡ ≈ ‘Ë«»√ ’ °ÿ≈ ·≈–∫ ÿ≠ ¡ ™—¬¡ß§≈ «“√ “√«—≥‚√§ ‚√§∑√«ßÕ°·≈–‡«™∫”∫ —¥«‘°ƒµ
Besides leukemic cells-endothelium interaction,ATRA also induces LFA-1 (lymphocyte functionassociated antigen-1) expression that makes leuke-mic cells adhere easily to each other (homotypicadhesion).11 This mechanism leads to mechanicalobstruction of the pulmonary capillary by poorlydeformable, aggregated leukocytes that are typicalof the pulmonary leukostasis found in acute myeloidleukemia (AML).12,13 Although circulating myeloidprecursors at various stages of differentiation canbe found in RAS, they are not as prominent whencompared to non-M3 AML with hyperleukocytosis.Therefore, the concept of capillary leakage syndromesbeing the major mechanism of RAS is supported.Other clinical evidence that supports this concept isthe response of RAS to dexamethasone rather thanleukapheresis or chemotherapy. Dexamethasone actsby blocking interleukin 2-included synthesis of thetumor necrosis factor-alpha (TNF-α.14 TNF-α is themediator that induces capillary-leak syndrome, whichhas the same clinical manifestations as RAS.14 Dex-amethasone also inhibits generation of nitric oxide,that is a principal mediator of cytokine-inducedvasodilation.7 Not only the response to dexametha-sone, but also the clinical manifestations thatinclude edema, weight gain, pleural effusion, peri-cardial effusion and episodic hypotension make therole of vasoactive cytokines likely.7 Although we didnot perform histopathologic diagnosis for our pa-tient, the typical clinical manifestations without otherpossible causes, particularly infections, and the dra-matic response to dexamethasone made RAS themost likely diagnosis.
Because of the relatively high mortality in un-treated RAS (5% to 33%),5,7,8,15 prevention would bethe appropriate approach, but unfortunately, there isno effective way to prevent the development of this
syndrome. The use of ATRA at a lower dose (25mg/m2/day) is not useful in lowering the incidenceof RAS, although it has the same efficacy as theconventional dose (45 mg/m2/day).9,16 Prophylaxishigh dose prednisolone (75 mg/day) in patients whohave a WBC count of more than 10,000/mm3 dur-ing ATRA therapy was reported as beneficial indecreasing the incidence of this syndrome. How-ever, this study compared the incidence of RASwith the previous study, which was not a random-ized controlled trail.17 Actually, RAS could developdespite taking a moderately high dose of dexam-ethasone.6 Neither low-dose chemotherapy norleukapheresis can prevent its occurrence or ame-liorate its effects.8 Although concurrent administra-tion of chemotherapy for the prevention of leukocy-tosis in patients receiving ATRA has been reportedto lower the incidence of this syndrome, again, norandomized controlled trial has ever been done.5Therefore, the recommended approach to patientsbeing treated with ATRA is close observation andmonitoring for clinical manifestations of RAS, par-ticularly in those who have leukocytosis, and aprompt institution of dexamethasone should becarried out whenever the clinical syndrome hasdeveloped. At present, this approach would be thebest way to decrease the mortality of RAS. Havingdeveloped a severe form of RAS, our patient sur-vived from this syndrome, but died later of septiccomplication from chemotherapy.
ConclusionRAS is the most serious pulmonary complica-
tion of ATRA therapy. The patients present with aclinical syndrome consistent with ARDS as well asother signs of capillary leak syndrome such as weightgain, pleural effusion, pericardial effusion, edema orepisodic hypotension. The role of histopathology forthe diagnosis of RAS is limited because of a bleed-

ªï∑’Ë 25 ©∫ —∫∑’Ë 3 °√°Æ“§¡-°—𬓬π 2547 The Retinoic Acid Syndrome : 153
ing tendency in APL. Therefore, diagnosis can bemade by typical manifestations of this syndrome,no other explainable causes especially from infec-tions and bleeding, and a dramatic response todexamethasone. There is no preventive therapy thatis effective for RAS. The best ways to lower themortality of this syndrome are early recognition,best supportive therapy including mechanical ven-tilation, and early administration of dexamethasone.
Reference1. Fenaux P. The role of all-trans-retinoic acid in the treat-
ment of acute promyelocytic leukemia. Acta Haematol1993; 89 (Suppl 1): 22-27.
2. Tallman MS, Anderson JW, Schif fer CA, et al. All-transretinoic acid in acute promyelocytic leukemia. N Engl JMed 1997; 337:1021-1028.
3. Castaigne S, Chomienne C, Daniel MT, et al. All-transretinoic acid as a dif ferentiation therapy for acutepromyelocytic leukemia. I: clinical results. Blood 1990;76:1704-1709.
4. Meng-er H, Yu-Chen Y, Shu-Rong C, et al. Use ofall-trans retinoic acid in the treatment of acutepromyelocytic leukemia. Blood 1998; 72:567-572.
5. Tallman MS, Anderson JW, Schif fer CA, et al. Clinicaldescription of 44 patients with acute promyelocytic leu-kemia who developed the retinoic acid syndrome. Blood2000; 95:90-95.
6. Smith-Whitley K and Lange B. F atal all-trans retinoicacid pneumonitis. Ann Intern Med 1993; 118:472-473.
7. Frankel SR, Eardley A, Lauw ers G, Weiss M andWarrell RP Jr. The çretinoic acid syndromeé in acutepromyelocytic leukemia. Ann Intern Med 1992; 117:292-296.
8. Vahdat L, Maslak P, Miller WH Jr, et al. Early mor talityand the retinoic acid syndrome in acute promyelocyticleukemia: impact of leukocytosis, low dose chemo-
therapy, PMN-RAR α isoform, and CD13 expression inpatients with all-trans retinoic acid. Blood 1994; 84:3843-3849.
9. Fenaux P, Le Delcy MC, Castaignes, et al. Ef fects ofall-trans retinoic acid in newly diagnosed acute promy-elocytic leukemia. Results of a multicentre randomizedtrial. Blood 1993; 82:3241-3249.
10. Ware LB and Matthay MA. The acute respiratorydistress syndrome. N Engl J Med 2000; 342:1334-1349.
11. Larson RS, Brown DC and Sklar LA. Retinoic acidinduces aggregation of the acute promyelocytic leuke-mia cell line NB4 by utilization of LFA-1 and ICAM-2.Blood 1997; 90:2747-2756.
12. Vernant JP, Brun B, Mannoni P and Dreyfus B.Respiratory distress of hyperleukocytic granulocyticleukemias. Cancer 1979; 44:264-268.
13. Lester TJ, Johnson JW and Cuttner J. P ulmonaryleukostasis as the single w orst prognostic factorin patients with acute myelocytic leukemia andhyperleukocytosis. Am J Med 1985; 79:43-48.
14. Mier JW, Vachino G, Klempner MS, et al. Inhibition ofinterleukin-2-induced tumor necrosis factor release bydexamethasone: prev ention of an acquired neutrophilchemotaxis defect and dif ferential suppression ofinterleukin-2-associated side ef fects. Blood 1990;76:1933-1940.
15. Frankel SR, Eardley A, Heller G, et al. All-trans retinoicacid for acute promyelocytic leukemia: results of theNew York Study. Ann Intern Med 1994; 120:278-286.
16. Castaigne S, Lefebvre P, Chomienne C, et at. Ef fective-ness and pharmacokinetics of low-dose all-trans retinoicacid (25 mg/m2) in acute promyelocytic leukemia. Blood1993; 82:3560-3563.
17. Wiley JS, Firkin FC. Reduction of Pulmonary toxicity byprednisolone prophylaxis during all-trans retinoic acidtreatment of acute promyelocytic leukemia. AustralianLeukemia Study Group. Leukemia 1995; 9:774-778.

ªï∑’Ë 25 ©∫ —∫∑’Ë 3 °√°Æ“§¡-°—𬓬π 2547 °“√»÷°…“À“ “‡Àµÿ¢Õ߇™ ◊ÈÕ‚√§™π ‘¥º‘¥√Ÿª·∫∫œ 155
¡§‘¥ Õÿàπ‡ ¡“∏√√¡ æ.∫.ª«‘≥ ¥ÿ√ߧ‡«‚√®π å æ.∫.
ß“π‚√§ªÕ¥ °≈ ÿà¡ß“πÕ“¬ÿ√°√√¡ ‚√ß欓∫“≈√“™«‘∂’
°“√»÷°…“À“ “‡Àµÿ¢Õ߇™◊ÈÕ‚√§™π‘¥º‘¥√Ÿª·∫∫∑’Ë∑”„À⇰‘¥‚√§ªÕ¥Õ—°‡ ∫™ÿ¡™π„π‚√ß欓∫“≈√“™«‘∂’
∫∑§—¥¬àÕ: °“√µ√«®‡æ ◊ËÕ°“√«‘π ‘®©—¬‚√§ªÕ¥Õ—°‡ ∫™ÿ¡™π (community acquired pneumonia) ∑ ’ˇ°‘¥®“°°“√µ‘¥‡™◊ÈÕ·∫§∑ ’‡√ ’¬™π‘¥º‘¥√Ÿª·∫∫ (atypical pathogens) µâÕßÕ“»—¬°“√µ√«®æ‘‡»… ÷Ëß¡’§à“„™â®à“¬ Ÿß·≈–„™â‡«≈“π“π°«à“®–∑√“∫º≈ ®÷߉¡à‰¥â àßµ√«®„π‚√ß欓∫“≈∑—Ë«‰ª °“√»÷°…“§√—Èßπ’ȇæ ◊ËÕÀ“ “‡Àµÿ¢Õ߇™◊ÈÕ¥—ß°≈à“« ‰¥â·°àMycoplasma pneumoniae, Chlamydia pneumoniae, Legionella pneumophila ‚¥¬„™â serology ·≈–polymerase chain reaction (PCR) method ‚¥¬»÷°…“·∫∫ prospective study √–¬–‡«≈“µ—Èß·µà °ÿ¡¿“æ—π∏å -惻®‘°“¬π 2545 ¡’®”π«πºŸâªÉ«¬ 22 √“¬∑ ’ ˇ¢â“‰¥â°—∫‡°≥±å°“√»÷°…“∑’Ë¡“‚√ß欓∫“≈√“™«‘∂’ º≈°“√»÷°…“æ∫«à“¡’ºŸâªÉ«¬ 7 √“¬§‘¥‡ªìπ√âÕ¬≈– 31.8 ‰¥â√ —∫°“√«‘π‘®©—¬«à“‡ªìπ‚√§ªÕ¥Õ—°‡ ∫™π‘¥º‘¥√Ÿª·∫∫ (atypical pneumonia)·¬°‡ªìπ Mycoplasma pneumoniae 2 √“¬ Chlamydia pneumoniae 2 √“¬ Chlamydia psittaci 1 √“¬Mycoplasma pneumoniae & Chlamydia pneumoniae mixed infection 2 √“¬ ºŸâªÉ«¬∑ÿ°√“¬¡’√–¥—∫ ’√—Ë¡‰µ‡µÕ√å Ÿß¢÷Èπµ—Èß·µà 4 ‡∑ à“¢÷Èπ‰ª‡¡ ◊ËÕ‡∑’¬∫√–À«à“ß´’√—Ë¡§√—Èß·√°°—∫´’√ —Ë¡∑’Ë√–¬– 2-3 —ª¥“Àå∂—¥‰ª ‰¡àæ∫ Legionellapneumophila ∑—Èß®“°°“√µ√«® serology ·≈– urine antigen ≈ —°…≥–¿“æ√—ß ’∑√«ßÕ° à«π„À≠à‡ªìπ„πªÕ¥°≈’∫‡¥’¬« (72%) ·≈–‡ªìπ·∫∫ alveolar infiltration (68%)
®“°¢âÕ¡Ÿ≈ªí®®ÿ∫—πæ∫«à“‡™◊ÈÕ·∫§∑’‡√ ’¬™π‘¥º‘¥√ Ÿª·∫∫ ¡’Õÿ∫—µ‘°“√≥å Ÿß¢÷Èπ„πºŸâªÉ«¬‚√§ªÕ¥Õ—°‡ ∫™ÿ¡™π ¥—ßπ—Èπ°“√√—°…“®÷ߧ«√æ‘®“√≥“„À⬓ªØ‘™’«π–§√Õ∫§≈ÿ¡‡™◊ÈÕ¥—ß°≈à“«‚¥¬Õ“»—¬¢âÕ¡Ÿ≈∑“ß√–∫“¥«‘∑¬“¢Õß∑âÕß∂‘Ëπ·≈–≈—°…≥–∑“ߧ≈‘π ‘°‡æ◊ËÕ„Àâ ‰¥âº≈°“√√ —°…“∑’Ë¥’∑’Ë ÿ¥
√—∫‰«âµ’æ‘¡æ凡◊ËÕ«—π∑’Ë 7 ¡‘∂ÿπ“¬π 2547
«“√ “√«—≥‚√§ ‚√§∑√«ßÕ°·≈–‡«™∫”∫—¥«‘°ƒµThai Journal of TuberculosisChest Diseases and Critical Care

156 ¡§‘¥ Õÿàπ‡ ¡“∏√√¡ ·≈–ª«‘≥ ¥ÿ√ߧ‡«‚√®π å «“√ “√«—≥‚√§ ‚√§∑√«ßÕ°·≈–‡«™∫”∫ —¥«‘°ƒµ
∫∑π”‚√§ªÕ¥Õ—°‡ ∫„π™ÿ¡™πÕ“®‡°‘¥®“°‡™ ◊ÈÕ‚√§‰¥â
À≈“¬™π‘¥ ‡™àπ ·∫§∑’‡√ ’¬ ‰«√ — À√◊Õ‡™◊ÈÕ·∫§∑’‡√’¬™π‘¥º‘¥√Ÿª·∫∫ (atypical pathogens)1,2 ‡™◊ÈÕ·µà≈–™π ‘¥µâÕßÕ“»—¬°“√µ√«®‡æ◊ËÕÀ“ “‡Àµÿ ´÷Ëß‚¥¬ª°µ‘°Á®–µ√«®‰¥â‡©æ“–‡™ ◊ÈÕ·∫§∑ ’‡√’¬∫“ßµ—«‡∑ à“π —È𠇙 ◊ÈÕ·∫§∑ ’‡√’¬™π ‘¥º‘¥√Ÿª·∫∫Õ ◊ËπÊ ∑ ’Ëæ∫‡ªì𠓇Àµÿ¢Õߪե՗°‡ ∫µâÕßÕ“»—¬°“√µ√«®«‘∏ ’摇»…πÕ°‡Àπ◊Õ®“°°“√µ√«®µ“¡ª°µ‘ ‰¥â·°à°“√‡æ“–‡™ ◊ÈÕ µ√«®À“·Õ𵑇®π·≈–·Õπµ‘∫Õ¥’ ´÷Ëß¡’§à“„™â®à“¬·≈–„™â‡«≈“π“π°«à“®–∑√“∫º≈ ∑”„ÀâµâÕßµ—¥ ‘π„®„Àâ°“√√—°…“°àÕπ °“√»÷°…“§√—Èßπ’ȇæ◊ËÕÀ“Õÿ∫—µ‘°“√≥å¢Õ߇™◊ÈÕ·∫§∑’‡√’¬™π‘¥º‘¥√Ÿª·∫∫∑’Ëæ∫∫àÕ¬ ‰¥â·°à Mycoplasmapneumoniae, Chlamydia pneumoniae ·≈– Legionellapneumophila ∑’Ë∑”„À⇰‘¥‚√§ªÕ¥Õ—°‡ ∫„π™ÿ¡™π ‡æ ◊ËÕ®–‡ªìπ·π«∑“ß∑’Ë®–‡≈◊Õ°„™â¬“ªØ‘™’«π–µà“ßÊ ‡æ◊ËÕ°“√√—°…“‰¥â∂ Ÿ°µâÕß„π‚√ß欓∫“≈√“™«‘∂’ ‚¥¬„™â°“√µ√«®∑“ß
Abstract: Oonsaemathum S and Durongkaveroj P. Role of atypical pathogens in community ac-quired pneumonia at Rajavithi Hospital. Thai J Tuberc Chest Dis and Crit Care 2004;25: 155-163
Department of Medicine, Rajavithi Hospital, Ministry of Public Health
Establishing an etiological diagnosis of atypical respiratory pathogens in community acquiredpneumonia has been handicapped by a general lack of diagnostic facilities and expense. This prospec-tive study was done to determine atypical pathogens causing community-acquired pneumonia (CAP) atRajavithi Hospital by serology and PCR method. There were twenty-two adult patients fulfilling theclinical of CAP from February 2002 to November 2002. Etiological diagnosis was based on seroconversionor significant changes in antibody titer of the patients with paired sera. Seven patients (31.8%) hadpneumonia due to atypical pathogens, with Mycophasma pneumoniae, Chlamydia pneumoniae, Chlamydiapsittaci, and Mycoplasma pneumoniae & Chlamydia pneumoniae mixed infection responsible for 2, 2,1 and 2 patients, respectively. The majority of chest x-ray showed one lobe lesion (72%) and alveolarinfiltration (68%).
The data indicate that the incidence of atypical pathogens causing CAP is increasing. Thetreatment of CAP should cover atypical pathogens. To achieve the best outcome of therapy, however,physicians must be aware of local epidemiologic study and clinical features.
serology, polymerase-chain reaction (PCR) method·≈– urine for Legionella antigen test
«‘∏’°“√‡ªìπ°“√»÷°…“·∫∫ prospective study √–¬–‡«≈“
°“√»÷°…“µ—Èß·µà °ÿ¡¿“æ—π∏å 2545 ∂ ÷ß æƒ»®‘°“¬π 2545√«¡√–¬–‡«≈“ 10 ‡¥ ◊Õπ
‡°≥±å°“√§—¥‡≈◊Õ° (Inclusion criteria)1. ¡’ new infiltration „π¿“æ√ —ß ’∑√«ßÕ°∑’ˉ¡à “¡“√∂
Õ∏‘∫“¬‰¥â®“° “‡ÀµÿÕ◊Ëπ2. ¡’Õ“°“√·≈–Õ“°“√· ¥ßÕ¬à“ßπâÕ¬ 3 Õ¬à“ß ®“°
¢âÕµàÕ‰ªπ’È- ¡’°“√‡ª≈’ˬπ·ª≈ߢÕߪ√‘¡“≥‡ ¡À–Õ¬à“ß
‡©’¬∫æ≈—π- ¡’Õ“°“√‰Õ- ¡’‰¢â¿“¬„π 24 ™—Ë«‚¡ß ∑ ’˺à“π¡“‡°‘π°«à“ 38OC

ªï∑’Ë 25 ©∫ —∫∑’Ë 3 °√°Æ“§¡-°—𬓬π 2547 °“√»÷°…“À“ “‡Àµÿ¢Õ߇™ ◊ÈÕ‚√§™π ‘¥º‘¥√Ÿª·∫∫œ 157
- rales or evidence of pulmonary consoli-dation
- leukocytosis or malaise (WBC > 10,000/mm3 or > 15% bands)
- myalgia or gastrointestinal symptoms ormalaise
3. ºŸâªÉ«¬∑ ÿ°√“¬µâÕ߉¥â√ —∫§”Õ∏ ‘∫“¬·≈–‡´Áπ„∫¬‘π¬Õ¡√ à«¡°“√»÷°…“
‡°≥±å°“√§—¥ÕÕ° (Exclusion criteria)1. ‡ªìπ tuberculosis, nosocomial pneumonia,
lung cancer, aspiration pneumonia, bronchiectasis,HIV infection, systemic immunosuppressant
2. ‡§¬πÕπ‚√ß欓∫“≈„π™à«ß 2 —ª¥“Àå∑’˺à“π¡“
ºŸâªÉ«¬∑’ˇ¢â“‡°≥±å¥—ß°≈à“«∑ÿ°√“¬®–‰¥â√—∫°“√´—°ª√–«—µ‘·≈–µ√«®√à“ß°“¬ µ√«®‡≈◊Õ¥ ‡ ¡À– ªí “«– ·≈–∂à“¬¿“æ√ —ß ’∑√«ßÕ°„π«—π·√°∑ ’Ë¡“ ·≈–®–‰¥â√ —∫°“√√—°…“µ“¡¢—ÈπµÕπª°µ‘ ®“°π—Èπ®–π —¥ºŸâªÉ«¬¡“µ√«®´È”Õ’° 2-3 —ª¥“Àå ‡æ ◊ËÕ¥ŸÕ“°“√·≈–µ√«®‡≈◊Õ¥´È”
°“√µ√«®∑“ßÀâÕߪؑ∫—µ‘°“√·≈–°“√·ª≈º≈‚¥¬„™â‡°≥±å°“√«‘π‘®©—¬¥—ßµàÕ‰ªπ’È
1. Mycoplasma pneumoniae µ√«®À“ Myco-plasma antibody ¥â«¬«‘∏ ’ particle agglutination °—∫serum ‚¥¬„™â Serodia Mycoll, manufactured byFujirebio, Japan °“√·ª≈º≈§◊Õº≈∫«°‡¡ ◊ËÕ¡’‰µ‡µÕ√å‡æ‘Ë¡¢÷ÈπÀ√◊Õ≈¥≈ßµ—Èß·µà 4 ‡∑à“¢Õß serum √–À«à“ߧ√ —Èß∑ ’Ë 1 ·≈–2 À√◊Õ‰µ‡µÕ√ åµ—Èß·µà 1:160 ∑ —Èß 2 §√—Èß√ à«¡°—∫º≈ PCRpositive3
2. Chlamydia pneumoniae ·≈– Chlamydiapsittaci µ√«®À“ Chlamydia antibody ¥â«¬«‘∏’ micro-immunofluorescence test for IgM, IgG, IgA; manu-factured by MRL, USA4,5 °“√·ª≈º≈§◊Õ º≈∫«°‡¡◊ËÕ¡’‰µ‡µÕ√å‡æ‘Ë¡¢÷ÈπÀ√◊Õ≈¥≈ßµ—Èß·µà 4 ‡∑ à“¢Õß serum √–À«à“ߧ√—Èß∑’Ë 1 ·≈– 2 À√◊Õ‰µ‡µÕ√åµ—Èß·µà 1:512 ∑—Èß 2 §√ —Èß √ à«¡°—∫º≈ PCR positive
3. Legionella pneumophila µ√«®À“ Legionellaantibody ¥â«¬«‘∏’ immunofluorescence test;manufactured by MARDX, USA °“√·ª≈º≈§◊Õº≈∫«°‡¡◊ËÕ¡’‰µ‡µÕ√å‡æ‘Ë¡¢÷ÈπÀ√◊Õ≈¥≈ßµ—Èß·µà 4 ‡∑ à“¢Õßserum √–À«à“ߧ√—Èß∑ ’Ë 1 ·≈– 2 À√◊Õ‰µ‡µÕ√åµ—Èß·µà 1:256∑—Èß 2 §√—Èß√à«¡°—∫µ√«®À“ urinary antigen ‚¥¬«‘∏ ’ ELISA¡’º≈ positive6
º≈°“√»÷°…“¡’ºŸâªÉ«¬‚√§ªÕ¥∫«¡™ÿ¡™π∑ ’Ë ‡¢â“√ —∫°“√√ —°…“„π
‚√ß欓∫“≈√“™«‘∂’·≈– ¡—§√„®‡¢â“√à«¡°“√«‘®—¬ µ—Èß·µà°ÿ¡¿“æ—π∏å ∂÷ß æƒ»®‘°“¬π 2545 ‡ªìπ√–¬–‡«≈“ 10 ‡¥◊Õπ®”π«πºŸâªÉ«¬ 27 §π µ—¥ÕÕ°®“°°“√»÷°…“‡π◊ËÕß®“°‰¡à¡“µ“¡·æ∑¬åπ—¥ 4 √“¬ ·≈–‡ªìπ«—≥‚√§ªÕ¥ 1 √“¬√“¬≈–‡Õ’¬¥¢ÕߺŸâªÉ«¬¥—ß· ¥ßµ“¡µ“√“ß∑ ’Ë 1
º≈°“√µ√«®∑“ßÀâÕߪؑ∫—µ‘°“√‚¥¬„™â PCR ·≈–serology æ∫«à“ ¡’ºŸâªÉ«¬ 7 √“¬„π 22 √“¬§‘¥‡ªìπ√âÕ¬≈–31.8 ‰¥â√—∫°“√«‘π‘®©—¬«à“‡ªìπ atypical pneumonia ·¬°ÕÕ°‡ªìπ Mycoplasma pneumoniae 2 √“¬ Chlamydiapneumoniae 2 √“¬ Chlamydia psittaci 1 √“¬·≈–‡ªìπMycoplasma pneumoniae & Chlamydia pneumoniaemixed infection 2 √“¬ ºŸâªÉ«¬∑ÿ°√“¬∑’ˉ¥â√—∫°“√«‘π‘®©—¬«à“‡ªìπ Mycoplasma pneumoniae ¡’√–¥—∫¿Ÿ¡‘§ÿâ¡°—π„π´’√ —Ë¡√–¥—∫‰µ‡µÕ√å Ÿß¢÷Èπµ—Èß·µà 4 ‡∑à“¢÷Èπ‰ª‡¡◊ËÕ‡∑’¬∫√–À«à“ß´’√—Ë¡∑ ’Ë·√°√ —∫°—∫´’√—Ë¡∑ ’Ë√–¬– 2-3 —ª¥“Àå∂—¥‰ª·≈–µ√«®æ∫«à“ PCR positive 3 „π 4 √“¬ à«πºŸâªÉ«¬∑’ˉ¥â√—∫°“√«‘π‘®©—¬«à“‡ªìπ Chlamydia pneumoniae ºŸâªÉ«¬∑—Èß 4 √“¬¡’√–¥—∫¿Ÿ¡‘§ÿâ¡°—π (IgA) „π´’√—Ë¡√–¥—∫‰µ‡µÕ√å Ÿß¢÷Èπµ—Èß·µà4 ‡∑ à“√–À«à“ß´’√—Ë¡§√ —Èß∑ ’Ë 1 ·≈– 2 ‚¥¬ºŸâªÉ«¬∑ÿ°√“¬¡’º≈PCR negative ¡’ºŸâªÉ«¬ 2 √“¬‰¥â√—∫°“√«‘π‘®©—¬«à“‡ªìπmixed Mycoplasma pneumoniae ·≈– Chlamydiapneumoniae ‡π◊ËÕß®“°¡’√–¥—∫¿Ÿ¡‘§ÿâ¡°—π (IgG) ‰µ‡µÕ√å Ÿß¢÷Èπµ—Èß·µà 4 ‡∑ à“¢Õ߇™◊ÈÕ∑ —Èß 2 µ—« πÕ°®“°π’Ȭ—ß¡’ºŸâªÉ«¬1 √“¬∑ ’Ë¡’√–¥—∫¿Ÿ¡‘§ÿâ¡°—π (IgA & IgG) µàÕ Chlamydiapsittaci „π ’√—Ë¡√–¥—∫‰µ‡µÕ√å Ÿß¢÷Èπ 4 ‡∑ à“√–À«à“ß ’√—Ë¡§√—Èß∑’Ë 1 ·≈– 2 °“√»÷°…“π’È ‰¡àæ∫ Legionella pneumophila∑—Èß®“°°“√µ√«®‚¥¬ serology ·≈– urinary antigen¥—ß· ¥ßµ“¡µ“√“ß∑ ’Ë 2 ·≈– 3

158 ¡§‘¥ Õÿàπ‡ ¡“∏√√¡ ·≈–ª«‘≥ ¥ÿ√ߧ‡«‚√®π å «“√ “√«—≥‚√§ ‚√§∑√«ßÕ°·≈–‡«™∫”∫ —¥«‘°ƒµ
≈—°…≥–¿“æ√—ß ’∑√«ßÕ°¢ÕߺŸâªÉ«¬‚√§ªÕ¥Õ—°‡ ∫ à«π„À≠ à‡ªìπ„πªÕ¥°≈ ’∫‡¥’¬« (72%) ·≈–‡ªìπ·∫∫ alveo-lar infiltration (63%) æ∫«à“¡’ pleural effusion ‡æ’¬ß 1√“¬ (4.5%) ¥—ß· ¥ßµ“¡µ“√“ß∑’Ë 4 à«πº≈°“√«‘π‘®©—¬ºŸâªÉ«¬‚√§ªÕ¥Õ—°‡ ∫™ÿ¡™π∑’Ë¡“√—∫°“√√—°…“∑’Ë ‚√ß欓∫“≈
√“™«‘∂’ „π™à«ß‡«≈“∑’Ë»÷°…“ “¡“√∂„Àâ°“√«‘π‘®©—¬‰¥â®“°serology, PCR ·≈– sputum culture ®”π«π 12 §π®“° 22 §π §‘¥‡ªìπ√âÕ¬≈– 54.5 ¥—ß· ¥ß µ“¡µ“√“ß∑’Ë 4·≈– 5
µ“√“ß∑’Ë 1 · ¥ß¢âÕ¡Ÿ≈§ÿ≥≈—°…≥–ª√–™“°√·≈–≈—°…≥–∑“ߧ≈‘π‘°¢ÕߺŸâªÉ«¬¢≥–·√°√—∫
µ“√“ß∑’Ë 2 · ¥ßº≈°“√µ√«® PCR ·≈– Serology
Mycoplasma pneumoniae PCR + serology 3Total positive 4
PCR + serology 3Total positive 4
PCR positive 0Serology only 5
PCR positive 0Serology positive 5
PCR only 0Serology only 1
PCR + serology 0Total positive 5
Total 4
Chlamydia serologyChlamydia pneumoniae Chlamydia psittaci
IgG1
IgA4
IgG1
IgA1
Total 1
Chlamydia spp.
Total positive 7 case (Mycoplasma & Chlamydia mixed infection 2 case)Positive for Mycoplasma pneumoniae 4 case Positive for Chlamydia pneumoniae 4 casePositive for Chlamydia psittaci 1 case
®”π«πºŸâªÉ«¬ (n = 22)¢âÕ¡Ÿ≈
™“¬/À≠‘ßÕ“¬ÿ (ªï)√—∫√—°…“‰«â„π‚√ß欓∫“≈ (% ºŸâªÉ«¬)Õ“°“√·≈–Õ“°“√· ¥ß (% ºŸâªÉ«¬)
‰ÕÀÕ∫‡Àπ◊ËÕ¬‰¢â (¢≥–·√°√ —∫)3ÕàÕπ‡æ≈ ’¬‡®Á∫Àπâ“Õ°ª«¥°≈ â“¡‡π◊ÈÕÀπ“« —Ëπ∑âÕ߇ ’¬Rales/crepitationsRhonchiWheezing
13/946 (19-90)12 (54)
1009068685045401386229

ªï∑’Ë 25 ©∫ —∫∑’Ë 3 °√°Æ“§¡-°—𬓬π 2547 °“√»÷°…“À“ “‡Àµÿ¢Õ߇™ ◊ÈÕ‚√§™π ‘¥º‘¥√Ÿª·∫∫œ 159
µ“√“ß∑ ’Ë 3 · ¥ßº≈ PCR ·≈– Serology ¢ÕߺŸâªÉ«¬∑’ˉ¥â√ —∫°“√«‘π‘®©—¬«à“‡ªìπ atypical pneumonia
C.pneumoniae C.psittaci
SerologyIgA IgG
ºŸâªÉ«¬√“¬∑ ’Ë Õ“¬ÿ PCR result M.pneumoniae C.pneumoniae C.psittaci
MP CP 1st 2nd 1st 2nd 1st 2nd 1st 2nd 1st 2nd
19476930273225
1234*567*
+---+-+
-------
1280 10240<40<40
<40 10240640 2560
<40<40 10240
256 128512 1024<16 6432 128
<1616 6432 128
<16256 1024
<16<16<16<16<16
10242048 4096
1024128 512
<16512512
<16256 1024
<16<16<16
<16 1616
* Mixed M. pneunoniae and C. pneumoniae infection
®”π«πºŸâªÉ«¬ (n=22)
2221211112 (54.5%)
µ“√“ß∑’Ë 5 · ¥ßº≈°“√«‘π‘®©—¬ºŸâªÉ«¬‚√§ªÕ¥Õ—°‡ ∫5 ™ÿ¡™π®“° serology, PCR, sputum culture
‡™ ◊ÈÕ∑ ’˵√«®æ∫
Mycoplasma pneumoniaeChlamydia pneumoniaeMycoplasma & Chlamydia pneumoniae mixed infectionChlamydia psittaciHaemophilus influenzaeStreptococcus pneumoniaeKlebsiella pneumoniae and Haemophilus influenzaeEscherichia coli√«¡
µ“√“ß∑’Ë 4 · ¥ß≈ —°…≥–¿“æ√—ß ’∑√«ßÕ°¢ÕߺŸâªÉ«¬‚√§ªÕ¥Õ—°‡ ∫™ÿ¡™π4
≈ —°…≥–¿“æ√—ß ’
One lobeMore than 1 lobeInterstitial shadowingAlveolar shadowingLobar consolidationMixed alveolar and interstitial shadowingPleural effusion
®”π«πºŸâªÉ«¬ (%)
16/22 (72.7%) 6/22 (27.2%) 7/22 (31.8%)14/22 (63.6%) 2/22 (9.0%) 1/22 (4.5%) 1/22 (4.5%)

160 ¡§‘¥ Õÿàπ‡ ¡“∏√√¡ ·≈–ª«‘≥ ¥ÿ√ߧ‡«‚√®π å «“√ “√«—≥‚√§ ‚√§∑√«ßÕ°·≈–‡«™∫”∫ —¥«‘°ƒµ
«‘®“√≥å‡π◊ËÕß®“°°“√À“ “‡Àµÿ¢Õ߇™◊ÈÕ‚√§™π ‘¥º‘¥√Ÿª·∫∫∑’Ë
∑”„À⇰‘¥‚√§ªÕ¥Õ—°‡ ∫™ÿ¡™π∑ ’ˇ°‘¥®“°‡™ ◊ÈÕ atypicalpathogens ‰¥â·°à Mycoplasma pneumoniae, Chlamy-dia pneumoniae, Legionella pneumophila ∑”‰¥â¬“°‡æ√“–‰¡à “¡“√∂µ√«®æ∫®“°°“√¬âÕ¡·°√¡‡ ¡À–·≈–°“√‡æ“–‡™ ◊ÈÕµâÕßÕ“»—¬Õ“À“√‡≈ ’Ȭ߇™ ◊ÈÕ‚¥¬‡©æ“–´÷Ë߉¡à “¡“√∂∑”‰¥âµ“¡‚√ß欓∫“≈∑—Ë«‰ª „πªí®®ÿ∫—π¡’√“¬ß“π∑—Èß®“°µà“ߪ√–‡∑»·≈–„πª√–‡∑»«à“¡’Õÿ∫—µ‘°“√≥å¢Õ߇™◊ÈÕ¥—ß°≈à“«¡“°¢÷Èπ7-9 ≈—°…≥–∑“ߧ≈‘π‘°¢Õß atypical pneu-monia ·≈– bacteria pneumonia ∑ ’ˇ°‘¥®“°·∫§∑ ’‡√’¬Õ◊ËπÊ ∑ ’Ëæ∫∫ àÕ¬ ‡™àπ Streptococcus pneumoniae,Haemophilus influenzae ·≈– Klebsiella pneumoniae√«¡∑—Èß¿“æ√—ß ’∑√«ßÕ°‰¡à “¡“√∂·¬°«‘π‘®©—¬‚√§¥—ß°≈à“«‰¥â1,10 ¥—ßπ—Èπ°“√«‘π ‘®©—¬‚√§∑’Ë·πàπÕπµâÕßÕ“»—¬°“√µ√«®∑“ßserology, PCR ·≈– urinary antigen µ“¡‡°≥±å«‘π‘®©—¬¥—ß°≈à“«¡“·≈â«
°“√»÷°…“§√—Èßπ ’Èæ∫«à“ “¡“√∂„Àâ°“√«‘π‘®©—¬‚√§ªÕ¥Õ—°‡ ∫™π ‘¥º‘¥√Ÿª·∫∫®”π«π 7 √“¬®“°ºŸâªÉ«¬ 22 √“¬§‘¥‡ªìπ√âÕ¬≈– 31.8 ·∫ à߇ªìπ Mycoplasma pneumoniae,Chlamydia pneumoniae, Mycoplasma & Chlamydiapneumoniae mixed infection ·≈– Chlamydia psittaci‡∑à“°—∫√âÕ¬≈– 9.0, 9.0, 9.0 ·≈– 4.5 µ“¡≈”¥—∫ ´÷Ë߇ªìπ®”π«π∑ ’Ë Ÿß°«à“‡¡◊ËÕ‡∑’¬∫°—∫°“√»÷°…“„πÕ¥’µ ‡Àµÿº≈ª√–°“√ ”§—≠‰¥â·°à §«“¡ “¡“√∂„π°“√«‘π‘®©—¬∑’Ë¥’¢÷Èπ‚¥¬„™â serology ∑—Èß®“°ºŸâªÉ«¬∑’˵âÕßπÕπ‚√ß欓∫“≈·≈–®“°ºŸâªÉ«¬∑’Ë√—°…“·∫∫ºŸâªÉ«¬πÕ° à«π°“√µ‘¥‡™◊ÈÕ√à«¡√–À«à“ßMycoplasma pneumoniae ·≈– Chlamydia pneu-moniae 2 √“¬´÷Ë߇§¬¡’„π√“¬ß“πÕ ◊ËπÊ ¡“°àÕπ7,11 ¡—°‡ªìπ°“√µ‘¥‡™ ◊ÈÕ®“° Chlamydia pneumoniae ‡æ√“–«à“‡™◊ÈÕ “¡“√∂∑”≈“¬‡¬◊ËÕ∫ÿÀ≈Õ¥≈¡ (ciliostasis) ∑”„Àâ¡’‚Õ°“ µ‘¥‡™◊ÈÕ√ à«¡°—∫µ—«Õ◊Ëπ‰¥â¡“°¢÷Èπ12,13 °“√»÷°…“π’Ȭ—ßæ∫«à“¡’°“√µ‘¥‡™ ◊ÈÕ Chlamydia psittaci 1 √“¬ ´÷Ë߇§¬√“¬ß“π‚¥¬ª√–∑ ’ª·≈–§≥–14 ·µà‡π◊ËÕß®“°ºŸâªÉ«¬√“¬π ’È¡’PCR ‡ªìπ≈∫·≈–‰¡à‰¥â à߇擖‡™◊ÈÕ (cell culture) ®÷߉¥â·§à —ππ‘…∞“π«à“‡ªìπ C. psittaci pneumonia15,16 ®“°°“√
»÷°…“¢ÕßÕπ —πµå·≈–§≥–7 æ∫«à“‚√§ªÕ¥Õ—°‡ ∫™ÿ¡™π·∫∫ºŸâªÉ«¬πÕ°‡ªìπ‡™◊ÈÕ Chlamydia pneumoniae, Myco-plasma pneumoniae ·≈– Legionella pneumophila§‘¥‡ªìπ√âÕ¬≈– 36.7, 29.6 ·≈– 8.2 ·≈–·∫∫ºŸâªÉ«¬„𧑥‡ªìπ√âÕ¬≈– 16.3, 6.8 ·≈– 5.4 µ“¡≈”¥—∫ ‚√§ªÕ¥∫«¡™ÿ¡™π∑’˵‘¥‡™◊ÈÕ√ à«¡√–À«à“ß Mycoplasma pneumoniae °—∫Chlamydia pneumoniae ·∫∫ºŸâªÉ«¬πÕ°·≈–„𠧑¥‡ªìπ√âÕ¬≈– 9.1 ·≈– 1.3 µ“¡≈”¥—∫ πÕ°®“°π’È®“°°“√»÷°…“√à«¡°—π¢Õß 12 ‚√ß欓∫“≈„π 8 ª√–‡∑»¢Õ߇Շ™’¬‡æ◊ËÕÀ“Õÿ∫—µ‘°“√≥ å¢Õß‚√§ªÕ¥Õ—°‡ ∫™ÿ¡™π∑ ’ˇ°‘¥®“°‡™ ◊ÈÕ·∫§∑’‡√’¬™π‘¥º‘¥√Ÿª·∫∫ (atypical pathogens) §‘¥‡ªìπ√ âÕ¬≈– 19.9 ·∫à߇ªìπ Mycoplasma pneumoniae √âÕ¬≈–9.4, Chlamydia pneumoniae √âÕ¬≈– 4.3 ·≈– Legionellapneumophila √ âÕ¬≈– 6.28 ¥—ßπ—Èπ®–‡ÀÁπ«à“‚√§ªÕ¥Õ—°‡ ∫™ÿ¡™π™π ‘¥º‘¥√ Ÿª·∫∫ (atypical pneumonia) ¡’§«“¡ ”§—≠¡“°¢÷Èπ„πªí®®ÿ∫ —π‡π◊ËÕß®“°¡’Õÿ∫ —µ‘°“√≥å¡“°¢÷Èπ·≈–‡°‘¥‰¥âµ≈Õ¥ªï ´÷Ë߉¡à “¡“√∂„Àâ°“√«‘π‘®©—¬®“°°“√µ√«®·≈–‡æ“–‡™ ◊ÈÕ®“°‡ ¡À–®“°‚√ß欓∫“≈∑ —Ë«‰ª µâÕßÕ“»—¬°“√µ√«®∑“ß ’ ‚√‚≈¬’∑ ’Ë¡’‰µ‡µÕ√å Ÿß¢÷Èπµ—Èß·µà 4 ‡∑ à“¢÷Èπ‰ªÀ√◊Õ¡’‰µ‡µÕ√å Ÿß°«à“‡°≥±å°”Àπ¥√à«¡°—∫¡’º≈ PCR‡ªìπ∫«°¢Õ߇™ ◊ÈÕ Chlamydia pneumoniae, Mycoplasmapneumoniae À√◊Õ¡’·Õ𵑇®π„πªí “«–‡ªìπ∫«°¢Õ߇™◊ÈÕLegionella pneumophila serogroup1 à«π‡™◊ÈÕ·∫§∑’‡√’¬™π‘¥·°√¡∫«°·≈–·°√¡≈∫Õ◊ËπÊ ¡’‚Õ°“ ‡°‘¥¡“°¢÷Èπ„πºŸâªÉ«¬‚√§ªÕ¥Õ—°‡ ∫™ÿ¡™π∑ ’˵âÕßπÕπ‚√ß欓∫“≈Õ“¬ÿ¡“°À√◊Õ¡’‚√§ª√–®”µ—«‡√◊ÈÕ√ —ßµà“ßÊ ‡™àπ ‚√§ªÕ¥Õÿ¥°—Èπ‡√◊ÈÕ√—ß ‡∫“À«“π ¿Ÿ¡‘§ÿâ¡°—π∫°æ√àÕß ‡ªìπµâπ °“√»÷°…“π’ȉ¡à “¡“√∂„Àâ°“√«‘π‘®©—¬À“‡™◊ÈÕ∑’Ë°àÕ‚√§§‘¥‡ªìπ√âÕ¬≈– 45.5‡π◊ËÕß®“°¢âÕ®”°—¥„π°“√ àßµ√«®‰«√ — «‘∏’°“√‡°Á∫ ‘Ëß àßµ√«®‡ ¡À–°“√ à߇擖‡™◊ÈÕ®“°‡ ¡À–·≈–‡≈◊Õ¥‰¡àæ∫‡™◊ÈÕÀ√◊Õ‰¡à§√∫∂ â«π
√ÿª®“°¢âÕ¡Ÿ≈°“√»÷°…“„πªí®®ÿ∫ —πæ∫«à“ ‡™◊ÈÕ·∫§∑ ’‡√’¬
™π‘¥º‘¥√ Ÿª·∫∫ ¡’Õÿ∫ —µ‘°“√≥å Ÿß¢÷Èπ¡“°„πºŸâªÉ«¬‚√§ªÕ¥Õ—°‡ ∫™ÿ¡™π‚¥¬‡©æ“–„πºŸâªÉ«¬Õ“¬ÿπâÕ¬À√◊ÕÕ“°“√‰¡à

ªï∑’Ë 25 ©∫ —∫∑’Ë 3 °√°Æ“§¡-°—𬓬π 2547 °“√»÷°…“À“ “‡Àµÿ¢Õ߇™ ◊ÈÕ‚√§™π ‘¥º‘¥√Ÿª·∫∫œ 161
√ÿπ·√ß1,9,17 ≈—°…≥–∑“ߧ≈ ‘π‘°·≈–¿“æ√ —ß ’∑√«ßÕ°‰¡à “¡“√∂„™â„π°“√«‘π‘®©—¬·¬°‚√§®“°‡™◊ÈÕ·∫§∑’‡√ ’¬Õ◊Ëπʉ¥âÕ¬à“ß™—¥‡®π ‰¡à “¡“√∂¬âÕ¡‡ ¡À–·≈– à߇擖‡™◊ÈÕ·∫§-∑’‡√’¬™π‘¥º‘¥√Ÿª·∫∫‰¥â °“√ àßµ√«®∑“ß´’‚√‚≈¬’‰¥âº≈™â“‰¡à∑—πµàÕ°“√„Àâ°“√√—°…“·≈–§à“„™â®à“¬·æß ®÷ßµâÕßÕ“»—¬¢âÕ¡Ÿ≈∑“ß√–∫“¥«‘∑¬“¢Õ߇™◊ÈÕ·∫§∑’‡√’¬™π‘¥º‘¥√ Ÿª·∫∫‰¥â·°à Mycoplasma pneumoniae, Chlamydia pneu-moniae ·≈– Legionella pneumophila ¢Õß∑ âÕß∂‘Ëππ—ÈπÊ„π°“√æ‘®“√≥“„Àâ°“√√—°…“ ¥—ßπ—Èπ¬“ªØ‘™’«π–°≈ÿà¡ macro-lides ∑’˧√Õ∫§≈ ÿ¡‡™ ◊ÈÕ·∫§∑ ’‡√’¬™π ‘¥º‘¥√Ÿª·∫∫ ®÷ß¡’∑’Ë„™âÕ¬à“ß°«â“ߢ«“ß18,19 Õ¬à“߉√°Áµ“¡°“√√ —°…“ºŸâªÉ«¬‚√§ªÕ¥∫«¡™ÿ¡™πµâÕߧ√Õ∫§≈ÿ¡‡™◊ÈÕ·∫§∑’‡√’¬·°√¡∫«°·≈–·°√¡≈∫Õ◊ËπÊ µ“¡≈—°…≥–∑“ߧ≈‘π‘°√ à«¡°—∫Õߧåª√–°Õ∫Õ◊Ëπʉ¥â·°à §«“¡√ÿπ·√ߢÕß‚√§ ¡’‚√§ªÕ¥‡√◊ÈÕ√ —ß À√◊Õ‚√§À—«„®√à«¡¥â«¬ §«“¡‡ ’ˬߵàÕ°“√‡°‘¥ªÕ¥µ‘¥‡™◊ÈÕ ‡©æ“–∫“ß™π‘¥µ“¡·π«∑“ß°“√√ —°…“‚√§ªÕ¥Õ—°‡ ∫™ÿ¡™π„πª√–‡∑»‰∑¬20
°‘µµ‘°√√¡ª√–°“»¢Õ¢Õ∫§ÿ≥∫√‘…—∑ ‰ø‡´Õ√ å ∑’Ë „Àâ°“√ π —∫ πÿπ∑ÿπ
«‘®—¬ §ÿ≥‡æÁ≠æ√√≥ ÿ∏√√¡ ·≈–§ÿ≥¬ÿæ“ √—°‡À≈◊Õß“π‚√§ªÕ¥ ‚√ß欓∫“≈√“™«‘∂’ ∑ ’˙૬∑”°“√»÷°…“§√ —Èßπ’È
‡Õ° “√Õâ“ßÕ‘ß1. Ruiz M, Ewig S, Marcos MA, et al. Etiology of commu-
nity-acquired pneumonia: impact of age, comorbidity,and severity. Am J Respir Crit Care Med 1999;160:397-405.
2. Macfarlane J, Holmes W, Gard P, Macfalane R, et at.Prospective study of the incidence, aetiology and out-come of adult lower respiratory tract illness in commu-nity. Thorax 2001;56:109-114.
3. Echevarria JM, Leon P, Balfagon P, et al. Diagnosis ofMycoplasma pneumoniae infection by microparticleagglutination and antibody-capture enzyme-immunoas-say. Eur J Clin Microbiol Infect Dis 1990;9:217-220.
4. Bennedsen M, Berthelsen L and Lind I. Performance ofthree microimmunofluorescence assays for detection ofChlamydia pneumoniae immunoglobulin M, G, and Aantibodies. Clin Diagn Lab Immunol 2002;9:833-839.
5. Freidank HM, Vogele H and Eckert K. Evaluation ofnew commercial microimmunofluorescence test fordetection of antibodies to Chlamydia pneumoniae,Chlamydia trachomatis, and Chlamydia psittaci. Eur JClin Microbiol Infect Dis 1997 16:685-688.
6. Dominguez JA, Gali N, Pedroso P, et al. Comparison ofthe Binax Legionella urinary antigen enzyme immu-noassay (EIA) with the biotest Legionella urine antigenEIA for detection of Legionella antigen in both concen-trated and nonconcentrated urine samples. J ClinMicrobiol 1998;36:2718-2722.
7. Wattanathum A, Chutima C and Nunthapisud P, et al.Community-acquired pneumonia in southeast Asia.The microbial differences between ambulatory andhospitalized patients. Chest. 2003;123:1512-1519.
8. Yun-Fong Ngeow, et al. Asian study on the role ofatypical pathogens in community acquired pneumonia.Concurrent poster presentations in 8th Asian PacificSociety of Respirology Congress. Malaysia, December2003.
9. Lim WS, Macfarlane JT, Boswell TC, Harrison TG, RoseD, Leinonen M and Saiku P. Study of communityacquired pneumonia Bennedsen M, Berthelsen L,Lind I. Performance of three microimmunofluorescenceassays for detection of Chlamydia pneumoniae immu-noglobulin M, G and A antibodies. Clin Diagn LabImmunol 2002;9:833-839.
10. Marrie TJ, Peeling RW, Fine MJ, Singer DE, Coley CMand Kapoor WN. Ambulatory patients with communityacquired pneumonia: the frequency of atypical agentsand clinical cause. Am J Med. 1996;101:508-515.
11. Niederman MS, Mandell LA, Anzueto A, et al. Guide-lines for the management of adults with community-acquired pneumonia: diagnosis, assessment of severity,antimicrobial therapy, and prevention. Am J Respir CritCare Med 2001;163:1730-1754.
12. Collier AM and Clyde WA Jr. Relationships betweenMycoplasma pneumoniae and human respiratoryepithelium. Infect Immun 1977;3:694-701.

162 ¡§‘¥ Õÿàπ‡ ¡“∏√√¡ ·≈–ª«‘≥ ¥ÿ√ߧ‡«‚√®π å «“√ “√«—≥‚√§ ‚√§∑√«ßÕ°·≈–‡«™∫”∫ —¥«‘°ƒµ
13. Shemer-Avni Y and Lieberman D. Chlamydia pneumoniaeinduced ciliostasis in ciliated bronchial epithelial cells. JInfect Dis 1995;171:1274-1278.
14. Riantawan P and Nunthapisud P. Psittacosis pneumo-nia: a case report and review of the literature. J MedAssoc Thai 1996;79:55-59.
15. Essig A, Zucs P and Susa M, et al. Diagnosis ofornithosis by cell culture and polymerase chain reactionin a patient with chronic pneumonia. Clin Infect Dis1995;21:1495-1497.
16. Heddema ER, Kraan MC, Buys-Bergen HE, Smith HE,Wertheim-van Dillen PM. A woman with a lobar infiltra-
tion due to psittacosis detected by polymerase chainreaction. Scan J Infect Dis 2003;35:422-424.
17. Bochud PY, Moser F, Erard P, et al. Community-acquired pneumonia: a prospective outptient study.Medicine (Baltimore) 2001;80:75-87.
18. Vergis EN, Yu VI. Marcrolides are ideal for empiricaltherapy of community-acquired pneumonia in the immu-nocompetent host. Seminar Respir Infect. 1997;12:322-328.
19. Lieberman D. Atypical pathogen pneumonia. Curr OpinPul Med. 1997;3:111-115.
20. ¡“§¡Õÿ√‡«™™å·Ààߪ√–‡∑»‰∑¬. ·π«∑“ß°“√√—°…“‚√§ªÕ¥Õ—°‡ ∫™ÿ¡™π„πª√–‡∑»‰∑¬ ( ”À√ —∫ºŸâ„À≠ à) °√ÿ߇∑æœ: ‡Õ æ’°“√æ‘¡æå µÿ≈“§¡ 2544.

ªï∑’Ë 25 ©∫—∫∑’Ë 3 °√°Æ“§¡-°—𬓬π 2547 ª√– ‘∑∏ ‘¿“æ·≈–§«“¡ª≈Õ¥¿—¬¢Õ߬“´“‡øÕ≈ Ÿ§“ œ 163
*¿“§«‘™“Õ“¬ÿ√»“ µ√å §≥–·æ∑¬»“ µ√ 廑√‘√“™æ¬“∫“≈ ¡À“«‘∑¬“≈—¬¡À‘¥≈**¿“§«‘™“Õ“¬ÿ√»“ µ√å §≥–·æ∑¬»“ µ√ å ¡À“«‘∑¬“≈—¬¢Õπ·°àπ
***Àπ૬‚√§¿Ÿ¡‘·æâ °ÕßÕ“¬ÿ√°√√¡ ‚√ß欓∫“≈æ√–¡ß°ÿƇ°≈â“****‚√ß欓∫“≈¡À“√“™π§√‡™’¬ß„À¡à
ª√– ‘∑∏ ‘¿“æ·≈–§«“¡ª≈Õ¥¿—¬¢Õ߬“´“‡øÕ≈Ÿ§“ „π°“√√—°…“ºŸâªÉ«¬‚√§À◊¥
∑—»π ’¬“ ÿ∏√√¡ ¡—¬ «∑¡.*ª√–æ“à ¬ß„®¬ÿ∑∏ æ∫. *
«—™√“ ∫ ÿ≠ «— ¥‘Ï æ∫. **√ —µπ“¿√≥ å ‡øóòÕß∑Õß æ∫. ***
‡©≈‘¡ ≈ ‘Ë«»√ ’ °ÿ≈ æ∫. ****
∫∑§—¥¬àÕ : ª√– ‘∑∏‘¿“æ·≈–§«“¡ª≈Õ¥¿—¬¢Õ߬“´“‡øÕ≈Ÿ§“ „π°“√√—°…“ºŸâªÉ«¬‚√§À◊¥∑’Ë¡’Õ“°“√„π¢π“¥πâÕ¬∂÷ߪ“π°≈“ß ®”π«π 112 √“¬ „π°“√»÷°…“·∫∫‡ªî¥‚¥¬„™â¬“´“‡øÕ≈Ÿ§“ ¢π“¥ 20 ¡°. «—π≈– 2 §√—Èß √ à«¡°—∫¬“‡¥‘¡∑’˺ŸâªÉ«¬„™âµ‘¥µàÕ°—π‡ªìπ‡«≈“ 8 —ª¥“Àå „π√–À«à“ß°“√»÷°…“ ºŸâªÉ«¬®–µâÕß∫ —π∑÷°§à“ PEFR Õ“°“√ÀÕ∫„π·µà≈–«—π ·≈–®”π«π¬“ β2-agonist ™π‘¥ Ÿ¥¥¡∑’Ë„™â‡æ◊ËÕ∫√√‡∑“Õ“°“√ √«¡∑—ÈßÕ“°“√·∑√° âÕπ‡π◊ËÕß®“°¬“∑’ˇ°‘¥¢÷ÈππÕ°®“°π’È ºŸâªÉ«¬®–‰¥â√ —∫°“√µ√«® ¡√√∂¿“æ°“√∑”ß“π¢Õߪե·≈– ¡√√∂¿“æ°“√∑”ß“π¢Õßµ—∫∑’˧≈‘π‘°„π√–¬–°àÕπ·≈–À≈—߉¥â√—∫°“√√—°…“ ª√– ‘∑∏ ‘¿“æ·≈–§«“¡ª≈Õ¥¿—¬¢Õ߬“´“‡øÕ≈Ÿ§“ «—¥®“°°“√‡ª≈’ˬπ·ª≈ߢÕßÕ“°“√®”π«π¬“¢¬“¬À≈Õ¥≈¡∑’Ë„™â ¡√√∂¿“æ°“√∑”ß“π¢Õߪե·≈–Õ“°“√·∑√° âÕπ∑’ˇ°‘¥¢÷Èπ√«¡∑—Èߺ≈°“√µ√«®∑“ßÀâÕߪؑ∫—µ‘°“√ °“√»÷°…“π ’Èæ∫«à“ºŸâªÉ«¬¡’§à“ FEV1 ‡æ‘Ë¡¢÷Èπ®“° 1.62 ‡ªìπ 1.71 ·≈– 1.74 ≈‘µ√ æ√ âÕ¡°—∫¡’ PEFR‡æ‘Ë¡¢÷Èπ®“° 278.19 ‡ªìπ 299.17 ·≈– 313.31 ≈ ‘µ√/π“∑’ „π —ª¥“Àå∑’Ë 4 ·≈– 8 µ“¡≈”¥—∫ „π¢≥–∑ ’Ë§à“‡©≈’ˬ¢Õß PEFR „πµÕπ‡™â“®“°∫ —π∑÷°ª√–®”«—π¢ÕߺŸâªÉ«¬‡æ‘Ë¡¢÷Èπ®“° 294.11 ‡ªìπ 314.7 ·≈– 316.27 ≈ ‘µ√/π“∑ ’ ”À√—∫ PEFR °àÕπ‡¢â“πÕπ‡æ‘Ë¡¢÷Èπ®“° 295.93 ‡ªìπ 316.38 ·≈– 320.66 ≈‘µ√/π“∑’ √«¡∑ —Èß¡’§à“‡©≈’ˬ¢ÕßÕ“°“√ÀÕ∫À◊¥„π‡«≈“°≈“ß«—π·≈–°≈“ߧ◊π≈¥≈ß®“° 0.53 ‡ªìπ 0.42, 0.29 ·≈– ®“° 1.41 ‡ªìπ 1.02, 0.84 „π —ª¥“Àå∑’Ë 4·≈– 8 À≈ —ß„À⬓‡™àπ°—π πÕ°®“°π ’Ȭ—ßæ∫«à“§à“‡©≈’ˬ¢Õß°“√„™â¬“¢¬“¬À≈Õ¥≈¡ β2-agonist ™π‘¥ Ÿ¥¥¡ ≈¥≈ß®“°2.25 ‡ªìπ 1.54 ·≈– 1.13 µ“¡≈”¥—∫ °“√»÷°…“π’È¡’ºŸâªÉ«¬ 2 √“¬ (√âÕ¬≈– 1.8) ‡°‘¥Õ“°“√·∑√° âÕπ‡π◊ËÕß®“°¬“‰¥â·°à ª«¥»’√…–À√◊Õ„® —Ëπ ·≈–ºŸâªÉ«¬ 3 √“¬ (√âÕ¬≈– 2.6) ¡’√–¥—∫ aminotransferase „π‡≈◊Õ¥ Ÿß°«à“§à“ª°µ‘3 ‡∑à“‚¥¬‰¡à¡’Õ“°“√· ¥ß¢Õßµ—∫Õ—°‡ ∫‡°‘¥¢÷Èπ ·≈–°≈—∫§◊π‡ªìπª°µ‘‰¥âÀ≈—ßÀ¬ÿ¥¬“ ´“‡øÕ≈Ÿ§“ ®÷߇ªìπ¬“√ —°…“‚√§À◊¥Õ’°¢π“πÀπ÷Ëß∑’Ë “¡“√∂π”¡“„™â„π°“√√—°…“‡æ◊ËÕ§«∫§ÿ¡Õ“°“√¢ÕߺŸâªÉ«¬‚√§À◊¥‰¥âÕ¬à“ß¡’ª√– ‘∑∏‘¿“æ·≈–ª≈Õ¥¿—¬
√—∫‰«âµ’æ‘¡æ凡 ◊ËÕ«—π∑’Ë 12 ¡‘∂ÿπ“¬π 2547
«“√ “√«—≥‚√§ ‚√§∑√«ßÕ°·≈–‡«™∫”∫—¥«‘°ƒµThai Journal of TuberculosisChest Diseases and Critical Care

164 ∑ —»π’¬“ ÿ∏√√¡ ¡—¬ ·≈–§≥– «“√ “√«—≥‚√§ ‚√§∑√«ßÕ°·≈–‡«™∫”∫ —¥«‘°ƒµ
Abstract: T. Suthamsmai*, P. Youngchaiyud*, W. Boonsawat**, R. Fuengthong*** and C. Liwsrisakun.Efficacy and safety of Zafirlukast in the treatment of Thai asthmatic patients. Thai J Tuberc Chest Disand Crit Care 2004;25:163-172* Department of Medicine, Faculty of Medicine, Siriraj Hospital, Mahidol University ** Department ofMedicine, Faculty of Medicine, Khon Kaen *** Phar Mongkut Klao Hospital **** Maharaj NakornChiang Mai Hospital
The efficacy and safety of Zafirlukast was assessed as maintainance therapy for patient withmild to moderate asthma. A total of 112 patients were enrolled in a 8 week, non-radomized, open-labelextension multicentre trial in Thailand using Zafirlukast at the dosage of 20 mg twice daily for 8 weeks.Efficacy assessed by clinical evaluation, number of β2-agonist used, spriometry and daily Peak Expira-tory Flow Rate (PEFR) measurement. Safety evaluated by adverse events and laboratory tests. Zafirlukasthas demonstrated satistically significance improved in pulmonary function both FEV1 and PEFR. Themean FEV1, was 1.62 L. at baseline and was increase to 1.71 L. at week 4 and to 1.74 L. at week 8. Themean PEFR was 278.17 L/min at baseline and increased to 299.17 L/min at week 4 and to 313.31 L/minat week 8. The results of morning and evening PEFR from the dairy card data show inprovements afterthe treatment of Zafirlukast. The mean morning PEFR was 294.11 L/min before treatment and wasincreased to 314.7 L/min at week 4 and 316.27 L/min at week 8 after treatment while the mean eveningPEFR was 295.93 L/min before treatment and was increased to 316.38 L/min at week 4 and 320.66 L/min at week 8 after treatment. Zafirlukast also decreased daytime asthma symptom score from 0.53before treatment to 0.42 at week 4 and 0.29 at week 8; and night-time asthma symptom from 1.41before treatment to 1.02 and 0.84 at week 8 while the mean used of β2-agonist was decreased from 2.25to 1.54 at week 4 and 1.13 at week 8 of treatment. Two patients (1.8%) had adverse events, (headacheor palpitation) during the trial. Asymptomatic increases in serum aminotransferase levels of three timesthe upper limit of normal values were seen in 3 patients (2.6%). These adverse events and abnormalincrease in serum aminotransferase retumed to normal after discontinue of Zafirlukast. The result of thistrial demonstrate that Zafirlukast is safe and effective for the prophylactic treatment of asthma.
∫∑π”‚√§À◊¥‡ªÁπ‚√§¢Õß√–∫∫∑“߇¥‘πÀ“¬„®∑ ’Ëæ∫∫ àÕ¬
·≈–‡ªìπ‚√§Àπ÷Ëß∑’Ë¡’Õÿ∫—µ‘°“√≥å¢Õß°“√‡®Á∫ªÉ«¬‡æ‘Ë¡¢÷ÈπÕ¬à“ß√«¥‡√ Á«∑ —Èß„πª√–‡∑»∑ ’Ëæ—≤π“·≈â« ·≈–ª√–‡∑»∑’Ë°”≈—ßæ—≤π“ 欓∏ ‘ √ ’√«‘∑¬“ ”§—≠¢Õß‚√§π ’Ȫ√–°Õ∫¥â«¬°“√Õ—°‡ ∫‡√◊ÈÕ√ —ߢÕßÀ≈Õ¥≈¡‚¥¬¡’‡´≈À≈“¬™π ‘¥
·∑√°µ—«Õ¬Ÿà„π™—Èπ‡¬ ◊ËÕ∫ÿÀ≈Õ¥≈¡ √ à«¡°—∫°“√∑ ’ËÀ≈Õ¥≈¡¡’ªØ‘°‘√‘ ¬“µÕ∫ πÕßµàÕµ—«°√–µÿâπ‰¥â ‰«°«à“§πª°µ‘°≈‰°„π°“√ ‡°‘¥°“√À¥‡°√Á ߢÕßÀ≈Õ¥≈¡‡°‘¥®“°°“√ª≈¥ª≈àÕ¬ “√µà“ßÊ ‡™àπ histamine, cysteinylleukotrienes (CysLTs), prostaglandin, thromboxane œ≈œ

ªï∑’Ë 25 ©∫—∫∑’Ë 3 °√°Æ“§¡-°—𬓬π 2547 ª√– ‘∑∏ ‘¿“æ·≈–§«“¡ª≈Õ¥¿—¬¢Õ߬“´“‡øÕ≈ Ÿ§“ œ 165
„πªí®®ÿ∫—πæ∫«à“ cysteinyl leukotrienes ‡ªìπ mediators ”§—≠„π°“√‡°‘¥°“√Õ—°‡ ∫·≈–À¥‡°√ ÁߢÕßÀ≈Õ¥≈¡ ‚¥¬CysLTs ÕÕ°ƒ∑∏‘Ï°√–µÿâπ„À⇴≈À≈“¬™π ‘¥ ‡™àπ mast cell,eosinophil ‡§≈◊ËÕπµ—«‡¢â“‰ªÕ¬Ÿà „πºπ—ßÀ≈Õ¥≈¡ ·≈–CysLTs ¬—ß°√–µÿâπ cationic protein ∑”„À⇰‘¥°“√≈Õ°µ—«¢Õ߇¬ ◊ËÕ∫ÿÀ≈Õ¥≈¡∫«¡ ¡’º≈∑”„À⇬◊ËÕ∫ÿÀ≈Õ¥≈¡¡’ªØ‘°‘√‘¬“µÕ∫ πÕßµàÕµ—«°√–µÿâπ¡“°¢÷Èπ √ à«¡°—∫°“√°√–µÿâπmucous gland ∑”„Àâ¡’®”π«π‡ ¡À–·≈–‡¬◊ËÕ∫ÿÀ≈Õ¥≈¡∫«¡¡“°¢÷Èπ „π√–¬– 20 ªï∑ ’˺à“π¡“‰¥â¡’°“√§âπ§«â“À“¬“„À¡à∑’ËÕÕ°ƒ∑∏‘Ï¢—¥¢«“ß°“√∑”ß“π¢Õß CysLTs ‡æ◊ËÕπ”¡“„™â√—°…“ºŸâªÉ«¬‚√§À◊¥ ¬“¥—ß°≈à“«ª√–°Õ∫¥â«¬¬“°≈ÿà¡·√°∑’ËÕÕ°ƒ∑∏ ‘Ï¢—¥¢«“ß°“√∑”ß“π¢Õß 5 - lipoxygenase∑’ˇ√’¬°«à“ leukotriene synthesis inhibitor µ—«Õ¬à“߇™àπZileuton à«π¬“ °≈ ÿà¡∑’Ë 2 ‡ªìπ¬“∑’ËÕÕ°ƒ∑∏‘Ï‚¥¬µ√ßµàÕreceptor ∑’ˇ√’¬°«à“ leukotriene receptor antagonist(LTRA) ‡™àπ Pranlukast, Zafirlukast ·≈– Montelukast
«—µ∂ÿª√– ߧ嫗µ∂ÿª√– ߧå¢Õß°“√»÷°…“π ’ȇæ◊ËÕ∑¥ Õ∫ª√– ‘∑∏‘-
¿“æ·≈–§«“¡ª≈Õ¥¿—¬¢Õ߬“´“‡øÕ≈Ÿ§“ (Zafirlukast)„π°“√√—°…“ºŸâªÉ«¬‚√§À◊¥∑’Ë¡’Õ“°“√∑“ߧ≈‘π‘°„π¢π“¥πâÕ¬∂÷ߪ“π°≈“ß ‚¥¬„À⬓π’È√—∫ª√–∑“𵑥µàÕ°—π‡ªìπ‡«≈“ 8 —ª¥“Àå √à«¡°—∫¬“√ —°…“‚√§À ◊¥∑ ’˺ŸâªÉ«¬°”≈—ß„™âÕ¬Ÿàª√– ‘∑∏‘¿“æ·≈–§«“¡ª≈Õ¥¿—¬¢Õ߬“´“‡øÕ≈Ÿ§“ „π°“√√—°…“ºŸâªÉ«¬‚√§À◊¥ «—¥®“°°“√‡ª≈ ’ˬπ·ª≈ߢÕßÕ“°“√ºŸâªÉ«¬®”π«π¬“¢¬“¬À≈Õ¥≈¡∑’˺ŸâªÉ«¬„™â °“√‡ª≈’ˬπ·ª≈ߢÕß ¡√√∂¿“æ°“√∑”ß“π¢Õߪե ·≈–Õ“°“√·∑√° âÕπ∑’ˇ°‘¥¢÷Èπ √«¡∑—Èߺ≈°“√µ√«®∑“ßÀâÕߪؑ∫—µ‘°“√
«—µ∂ÿ·≈–«‘∏’°“√ºŸâªÉ«¬: ºŸâªÉ«¬‚√§À◊¥∑’Ë¡’Õ“°“√ÀÕ∫„π¢π“¥πâÕ¬∂÷ß
ª“π°≈“ß ∑ —ÈßÀ≠‘ß·≈–™“¬ Õ“¬ÿ√–À«à“ß 12-60 ªï ”À√—∫ºŸâªÉ«¬À≠‘ß®–µâÕ߉¡àÕ¬Ÿà„π√–À«à“ß°“√µ—Èߧ√√¿å À√◊Õ„Àâπ¡∫ÿµ√ ·≈–µâÕßÀ≈’°‡≈’ˬ߰“√µ—Èߧ√√¿å„π√–À«à“ß∑’Ë∑”°“√»÷°…“ ºŸâªÉ«¬∑ ’Ë ‰¥â√—∫°“√§—¥‡≈◊Õ°‡¢â“„π°“√»÷°…“π ’È®–µâÕߺà“π¢âÕ°”Àπ¥µà“ß Ê „π°“√»÷°…“¥—ßµàÕ‰ªπ ’È
1. “¡“√∂∫—π∑÷°§à“ Peak Expiratory Flow Rate
(PEFR) ¥â«¬‡§√◊ËÕß Peak Flow Meter ·≈–Õ“°“√ÀÕ∫À◊¥„π·µà≈–«—π‰¥âÕ¬à“ß∂Ÿ°µâÕß
2. ¡’§à“ Forced Expiratory Volume at onesecond (FEV1) µË”°«à“À√◊Õ‡∑ à“°—∫√âÕ¬≈– 80 ¢Õß§à“§“¥§–‡π„π§πª°µ‘
3. ¡√√∂¿“æ°“√∑”ß“π¢Õߪե„π√Õ∫ªï∑’˺à“π¡“ª√–°Õ∫¥â«¬
3.1 ¡’°“√‡ª≈’ˬπ·ª≈ߢÕß§à“ FEV1 ¡“°°«à“√âÕ¬≈– 15 À√◊Õ
3.2 ¡’°“√‡æ‘Ë¡¢Õß§à“ FEV1 À≈—ß®“°‰¥â√—∫¬“¢¬“¬À≈Õ¥≈¡ Salbutamol „π¢π“¥ 400 µg ‡°‘π°«à“√âÕ¬≈–15 À√◊Õ
3.3 ¡’°“√‡æ‘Ë¡¢Õß§à“ FVC À√◊Õ FEV1 À≈ —߉¥â√ —∫¬“¢¬“¬À≈Õ¥≈¡ ‡°‘π°«à“√âÕ¬≈– 12 À√◊Õ 200 ¡≈.
4. ‰¥â√—∫°“√√—°…“¥â«¬¬“§Õ√嵑‚§ ‡µ’¬√Õ¬¥å™π‘¥ Ÿ¥¥¡„π¢π“¥§ß∑ ’Ë Õ¬à“ßπâÕ¬ 4 —ª¥“Àå °àÕπ‡¢â“√à«¡„π°“√»÷°…“ ·≈–¡’°“√„™â β2- agonist ™π‘¥ Ÿ¥¥¡‡ªìπ§√ —Èߧ√“« ‡æ◊ËÕ∫√√‡∑“Õ“°“√ÀÕ∫À◊¥
5. ¡’Õ“°“√ÀÕ∫À◊¥‡¢â“‰¥â°—∫¢âÕ„¥¢âÕÀπ÷Ëß ¥—ßµàÕ‰ªπ’È5.1 ¡’Õ“°“√ÀÕ∫„π·µà≈–«—π (symptom score)
‡∑à“°—∫ 2 À√◊Õ¡“°°«à“ „π™à«ß 4 - 7 «—π°àÕπ∑”°“√»÷°…“À√◊Õ
5.2 ¡’Õ“°“√ÀÕ∫®πµâÕß„™â¬“ β2- agonist‡æ◊ËÕ§«∫§ÿ¡Õ“°“√Õ¬à“ßπâÕ¬ 4 «—π „π™à«ß 7 «—π ÿ¥∑ ⓬°àÕπ∑”°“√»÷°…“ À√◊Õ
5.3 ¡’Õ“°“√ÀÕ∫„π™à«ß°≈“ߧ ◊π‡°‘¥¢÷ÈπÕ¬à“ßπâÕ¬4 „π 7 «—π °àÕπ∑”°“√»÷°…“ ®π√∫°«π°“√πÕπÀ≈—∫
πÕ°®“°π ’ȺŸâªÉ«¬®–µâÕ߉¡à¡’Õ“°“√®—∫À◊¥√ ÿπ·√ß®πµâÕ߇¢â“√—∫°“√√ —°…“„π‚√ß欓∫“≈„π√–¬– 6 ‡¥◊Õπ°àÕπ‡¢â“√ à«¡„π°“√»÷°…“ À√◊ÕµâÕ߉¡à‡ªìπºŸâªÉ«¬‚√§À◊¥∑’Ë¡’Õ“°“√ÀÕ∫‡ªìπ§√ —Èߧ√“« ·≈–‰¡à¡’°“√µ‘¥‡™◊ÈÕ¢Õß√–∫∫°“√À“¬„® à«πµâπ „π™à«ß 6 —ª¥“Àå °àÕπ‡¢â“√ à«¡„π°“√»÷°…“ºŸâªÉ«¬®–µâÕ߉¡à‰¥â√—∫°“√√ —°…“¥â«¬¬“§Õ√ 嵑‚§ ‡µ’¬√Õ¬¥å ∑—Èß™π‘¥√ —∫ª√–∑“π À√◊Õ©’¥„π™à«ß 3 ‡¥ ◊Õπ°àÕπ‡¢â“√à«¡„π°“√»÷°…“ ·≈–µâÕßÀ≈ ’°‡≈ ’ˬ߰“√„™â¬“ anti-histamine,

166 ∑ —»π’¬“ ÿ∏√√¡ ¡—¬ ·≈–§≥– «“√ “√«—≥‚√§ ‚√§∑√«ßÕ°·≈–‡«™∫”∫ —¥«‘°ƒµ
ketotifen, long-acting β2- agonist ·≈– theophylline√«¡∑ —È߬“„π°≈ ÿà¡ anticholinergics ·≈–¬“¢¬“¬À≈Õ¥≈¡™π‘¥√—∫ª√–∑“π„π√–¬– Õß —ª¥“Àå°àÕπ°“√»÷°…“ ·≈–µ≈Õ¥‡«≈“∑ ’Ë∑”°“√»÷°…“
¬“∑’Ë„™â„π°“√»÷°…“ : ´“‡øÕ≈ Ÿ§“ ¢π“¥ 20 ¡°.√—∫ª√–∑“π«—π≈– 2 §√ —Èß „πµÕπ‡™â“ ·≈–‡¬Áπ ”À√ —∫¬“√—°…“‚√§À◊¥∑ ’˺ŸâªÉ«¬„™âÕ¬Ÿà‡¥‘¡ ‡™àπ §Õ√ 嵑‚§ ‡µ’¬√Õ¬¥å™π ‘¥ Ÿ¥¥¡ „Àâ§ß¢π“¥‡¥‘¡‰«âµ≈Õ¥°“√»÷°…“ à«π¬“¢¬“¬À≈Õ¥≈¡ β2- agonist ™π ‘¥ Ÿ¥¥¡ „Àâ„™â‡æ◊ËÕ∫√√‡∑“Õ“°“√∑ ’ˇ°‘¥¢÷Èπ‡ªìπ§√—Èߧ√“«‡∑ à“π —Èπ
°“√»÷°…“π’ȇªìπ°“√»÷°…“·∫∫‡ªî¥ ‚¥¬„™âºŸâªÉ«¬πÕ°¢Õß‚√ß欓∫“≈»‘√‘√“™, ‚√ß欓∫“≈»√ ’π§√‘π∑√å ,‚√ß欓∫“≈¡À“√“™π§√‡™’¬ß„À¡à ·≈–‚√ß欓∫“≈æ√–¡ß°ÿƇ°≈â“œ ºŸâªÉ«¬∑’Ë¡’§ÿ≥ ¡∫—µ‘§√∫∂â«πµ“¡∑’Ë°”Àπ¥‰«â ®–‰¥â√—∫°“√µ√«®«—¥ ¡√√∂¿“æ°“√∑”ß“π¢Õߪե„π™à«ß 2 —ª¥“Àå·√° ´÷Ë߇ªìπ™à«ß§—¥‡≈◊Õ°ºŸâªÉÉ«¬‡¢â“„π°“√»÷°…“ ·≈–®–¡’°“√ª√–‡¡‘πÕ“°“√∑“ߧ≈ ‘π‘°√à«¡°—∫°“√µ√«® ¡√√∂¿“æ°“√∑”ß“π¢Õߪե‡°’ˬ«°—∫ FEV1·≈– PEFR È”„π —ª¥“Àå∑’Ë 4 ·≈– 8 À≈ —ß„Àâ⬓ √«¡∑ —Èß¡’°“√µ√«® ¡√√∂¿“æ°“√∑”ß“π¢Õßµ—∫„π√–¬–°àÕπ ·≈–À≈—ß„À⬓´“‡øÕ≈ Ÿ§“ „π —ª¥“Àå∑’Ë 8 ¢Õß°“√√ —°…“ µ≈Õ¥°“√»÷°…“ºŸâªÉ«¬®–µâÕß∫—π∑÷°§à“µà“ßÊ ¥—ßµàÕ‰ªπ ’È
1. Peak Expiratory Flow Rate (PEFR): ºŸâªÉ«¬®–µâÕß∫ —π∑ ÷°§à“ PEFR «—π≈– Õߧ√ —Èß„πµÕπ‡™â“ ·≈–°àÕπ‡¢â“πÕπ ‚¥¬«—¥¥â«¬‡§√◊ËÕß Mini-Wright Peak FlowMeter °“√«—¥§à“ PEFR ®–µâÕß∑”°àÕπ°“√„™â¬“¢¬“¬À≈Õ¥≈¡ β2- agonist Õ¬à“ßπ âÕ¬ 3 ™—Ë«‚¡ß
2. Õ“°“√ÀÕ∫∑’Ë ‡°‘¥¢÷Èπ„π·µà≈–«—π ∑—Èß„π‡«≈“°≈“ß«—π ·≈–°≈“ߧ◊π „™â«‘∏’°“√„Àâ⧖·ππ¥—ßµàÕ‰ªπ’È0 §–·ππ = ‰¡à¡’Õ“°“√ÀÕ∫À◊¥1 §–·ππ = ¡’Õ“°“√ÀÕ∫À◊¥·µà “¡“√∂∑π‰¥â ‚¥¬‰¡à
√∫°«π°‘®«—µ√ª√–®”«—π2 §–·ππ = Õ“°“√ÀÕ∫À ◊¥∑”„Àâ√Ÿâ ÷°‰¡à ∫“¬„π°“√
∑”°‘®«—µ√ª√–®”«—π À√◊Õ√∫°«π°“√πÕπÀ≈—∫
3 §–·ππ = Õ“°“√ÀÕ∫À ◊¥∑”„Àâ ‰¡à “¡“√∂∑”°‘®«—µ√ª√–®”«—π À√◊ÕπÕπÀ≈—∫
3. ª√ ‘¡“≥¢Õ߬“¢¬“¬À≈Õ¥≈¡™π ‘¥ Ÿ¥¥¡∑ ’Ë„™â„π·µà≈–«—π: ‚¥¬·∫ à߇ªìπ®”π«π§√—ÈߢÕ߬“∑’Ë„™â „π™à«ß‡«≈“°≈“ß«—π ·≈–°≈“ߧ◊π
4. Õ“°“√·∑√° âÕπ·≈–§«“¡º‘¥ª°µ‘µà“ßÊ ∑ ’ˇ°‘¥¢÷Èπ„π√–À«à“ß∑”°“√»÷°…“
°“√ª√–‡¡‘πº≈°“√»÷°…“°“√«‘‡§√“–Àå°“√‡ª≈’ˬπ·ª≈ߢÕßÕ“°“√ ·≈–®”π«π
¢Õ߬“¢¬“¬À≈Õ¥≈¡ β2- agonist ™π ‘¥ Ÿ¥¥¡∑ ’Ë„™âÀ≈—ß„À⬓´“‡øÕ≈ Ÿ§“ ‡ª√ ’¬∫‡∑ ’¬∫°—∫™à«ß°àÕπ„À⬓ „™â«‘∏’ANOVA à«π°“√«‘‡§√“–Àå°“√‡ª≈’ˬπ·ª≈ߢÕß ¡√√∂-¿“æ°“√∑”ß“π¢Õߪե∑’ˇ°‘¥¢÷Èπ „™â«‘∏’ pair t-test
º≈°“√»÷°…“ºŸâªÉ«¬‚√§ÀÕ∫À◊¥∑ —ÈßÀ¡¥ 124 √“¬ ∑ ’ˇ≈◊Õ°‡¢â“¡“„π
°“√»÷°…“π’È ¡’ºŸâªÉ«¬®”π«π 112 √“¬∑ ’˺à“π°“√§—¥°√Õß‚¥¬·∫à߇ªì𙓬 36 √“¬ À≠‘ß 76 √“¬ Õ“¬ÿ√–À«à“ß13-59 ªï Õ“¬ÿ‡©≈’ˬ 43.2 ªï „π√–À«à“ß°“√»÷°…“ ¡’ºŸâªÉ«¬®”π«π 11 √“¬ ∂Ÿ°§—¥ÕÕ°®“°°“√»÷°…“‡π◊ËÕß®“°„™â¬“√—°…“‚√§ÀÕ∫™π ‘¥Õ◊Ëπ∑’Ë ‰¡à ‰¥â°”Àπ¥‰«â „π°“√»÷°…“„π®”π«ππ ’È¡’ºŸâªÉÉ«¬ 2 √“¬ ∑ ’Ë¡’Õ“°“√°”‡√ ‘∫¢Õß‚√§®πµâÕß„Àââ°“√√—°…“¥â«¬¬“§Õ√嵑‚§ ‡µ’¬√Õ¬¥å ™π ‘¥√ —∫ª√–∑“πÀ√◊Õ©’¥ ·≈–¬—ß¡’ºŸâªÉ«¬Õ’° 2 √“¬ ∑ ’Ë¡’Õ“°“√·∑√° âÕπ(ª«¥»’√…–√à«¡°—∫™“∫√‘‡«≥µâπ§Õ 1 √“¬ À≈—߉¥â√—∫¬“´“‡øÕ≈Ÿ§“ 3 «—π ·≈–„® —ËπÀ≈—ß√ —∫ª√–∑“π¬“´“‡øÕ-≈Ÿ§“ 4 «—π Õ’° 1 √“¬) ®π∑”„Àâ‰¡à “¡“√∂√à«¡„π°“√»÷°…“®π®∫‰¥ââ ∑”„Àââ®”π«πºŸâªÉ«¬∑ ’ˇ¢â“√à«¡„π°“√»÷°…“®π®∫‚§√ß°“√»÷°…“π’È≈¥≈߇À≈◊Õ 99 √“¬
¡√√∂¿“æ°“√∑”ß“π¢Õߪե‡°’ˬ«°—∫ FEV1 ·≈–PEFR „π§≈ ‘π‘°¢Õß‚√ß欓∫“≈ µ—Èß·µà‡√ ‘Ë¡µâπ°“√»÷°…“, —ª¥“Àå∑ ’Ë 4 ·≈– 8 ¢Õß°“√»÷°…“ ‰¥â· ¥ß‰«â„πµ“√“ß∑’Ë 1

ªï∑’Ë 25 ©∫—∫∑’Ë 3 °√°Æ“§¡-°—𬓬π 2547 ª√– ‘∑∏ ‘¿“æ·≈–§«“¡ª≈Õ¥¿—¬¢Õ߬“´“‡øÕ≈ Ÿ§“ œ 167
®–‡ÀÁπ‰¥â«à“§à“‡©≈ ’ˬ¢Õߪ√ ‘¡“µ√ Ÿß ÿ¥¢Õß≈¡À“¬„®ÕÕ°„π 1 «‘π“∑’·√° (FEV1) ‡æ‘Ë¡¢÷Èπ®“° 1.62 ± 0.51 ≈‘µ√‡ªìπ1.71 ± 0.58 ·≈–1.74 ± 0.56 ≈‘µ√ „π¢≥–∑ ’Ë§à“‡©≈ ’ˬ¢ÕßÕ—µ√“‡√ Á« Ÿß ÿ¥¢Õß°“√À“¬„® (PEFR) ‡æ‘Ë¡¢÷Èπ®“°
µ“√“ß∑ ’Ë 1 °“√‡ª≈’ˬπ·ª≈ߢÕß§à“ FEV1 ·≈– PEFR „π§≈‘π‘° ‡ª√’¬∫‡∑ ’¬∫™à«ßæ◊Èπ∞“π°àÕπ°“√»÷°…“ °—∫ —ª¥“Àå∑’Ë 4·≈– 8 À≈ —߉¥â√—∫°“√√ —°…“¥â«¬¬“´“‡øÕ≈Ÿ§“
FEV1Week 0 (Baseline)Week 4Week 8
PEFRWeek 0 (Baseline)Week 4Week 8
Actual meausrement(L.) ±±±±± SD
% PredictedValues
Percent changesMeans SD P Value
1.62 ± 0.511.71 ± 0.581.74 ± 0.56
62.06 ± 13.265.28 ± 15.766.65 ± 14.3
6.78 ± 20.029.14 ± 20.23
L/min.278.19 ± 94.07299.17 ± 99.62313.31 ± 100.33
11.49 ± 29.4115.98 ± 28.8
0.003< 0.001
<0.001<0.001
°“√‡ª≈’ˬπ·ª≈ߢÕßÕ—µ√“‡√Á« Ÿß ÿ¥¢Õß°“√À“¬„®(PEFR) „πµÕπ‡™â“·≈–°àÕππÕπ ®“°∫—π∑÷°ª√–®”«—π¢ÕߺŸâªÉ«¬ ‡ª√’¬∫‡∑’¬∫„π™à«ß°àÕπ„À⬓°—∫ —ª¥“Àå∑’Ë 4 ·≈–8 À≈—߉¥â√—∫°“√√—°…“¥â«¬¬“´“‡øÕ≈Ÿ§“ ‰¥â· ¥ß‰«â„πµ“√“ß∑ ’Ë 2 ·≈–√Ÿª∑’Ë 1 ´÷Ëßæ∫«à“§à“‡©≈’ˬ¢Õß PEFR „πµÕπ‡™â“ Ÿß¢÷Èπ®“° 294.11 ± 2.81 ‡ªìπ 314.7 ± 19.35
·≈– 316.27 ± 5.68 ≈ ‘µ√/π“∑’ ·≈–§à“‡©≈’ˬ¢Õß PEFR°àÕπ‡¢â“πÕπ Ÿß¢÷Èπ ®“° 295.93 ± 19.47 ‡ªìπ 316.38 ±3.45 ·≈– 320.66 ± 2.63 ≈‘µ√/π“∑’ „π —ª¥“Àå∑’Ë 4 ·≈– 8À≈—ß„À⬓µ“¡≈”¥—∫ ‚¥¬°“√‡ª≈’ˬπ·ª≈ßπ’Èæ∫«à“¡’§«“¡·µ°µà“ß ®“°§à“æ◊Èπ∞“π∑’Ë¡’π—¬ ”§—≠„π∑“ß ∂‘µ‘
µ“√“ß∑’Ë 2 °“√‡ª≈’ˬπ·ª≈ߢÕßÕ—µ√“‡√Á« Ÿß ÿ¥¢Õß°“√À“¬„®„πµÕπ‡™â“·≈–°àÕππÕπ ®“° ¡ÿ¥∫—π∑÷°ª√–®”«—π¢ÕߺŸâªÉ«¬‡ª√’¬∫‡∑’¬∫™à«ßæ◊Èπ∞“π°àÕπ°“√»÷°…“ °—∫ —ª¥“Àå∑ ’Ë 4 ·≈– 8 À≈—߉¥â√—∫°“√√—°…“¥â«¬¬“´“‡øÕ≈Ÿ§“
µÕπ‡™â“°àÕπ‰¥â√—∫¬“À≈—߉¥â√—∫¬“ 4 —ª¥“ÀåÀ≈—߉¥â√—∫¬“ 8 —ª¥“Àå°àÕπ‡¢â“πÕπ°àÕπ‰¥â√—∫¬“À≈—߉¥â√—∫¬“ 4 —ª¥“ÀåÀ≈—߉¥â√—∫¬“ 8 —ª¥“Àå
Mean(L/min)
Standard deviation P Value
294.11314.70316.27
295.93316.38320.66
0.002< 0.001
0.001<0.001
± 2.81 ± 19.35± 5.68
± 19.47± 3.45± 2.63
278.19 ± 94.07 ‡ªìπ 299.17± 99.6 ·≈– 313.31 ± 100.3≈‘µ√/π“∑ ’ „π —ª¥“Àå∑’Ë 4 ·≈– 8 ¢Õß°“√√—°…“¥â«¬´“‡øÕ≈Ÿ§“ µ“¡≈”¥—∫ °“√‡ª≈ ’ˬπ·ª≈ߥ—ß°≈à“«æ∫«à“¡’§«“¡·µ°µà“ß®“°§à“æ◊Èπ∞“π∑ ’Ë¡’π—¬ ”§—≠„π∑“ß ∂ ‘µ‘

168 ∑ —»π’¬“ ÿ∏√√¡ ¡—¬ ·≈–§≥– «“√ “√«—≥‚√§ ‚√§∑√«ßÕ°·≈–‡«™∫”∫ —¥«‘°ƒµ
* ·≈– t = ¡’§«“¡·µ°µà“ß®“°æ◊Èπ∞“π∑’Ë¡’π—¬ ”§—≠∑“ß ∂‘µ‘
§à“‡©≈’ˬ¢ÕßÕ“°“√ÀÕ∫À◊¥∑’ˇ°‘¥¢÷Èπ ∑—Èß„π‡«≈“°≈“ß«—π ·≈–°≈“ߧ◊π „π√–¬–°àÕπ·≈–À≈—ß„Àâ°“√√—°…“¥â«¬¬“´“‡øÕ≈ Ÿ§“ ‰¥â· ¥ß‰«â„πµ“√“ß∑ ’Ë 3 ®–‡ÀÁπ‰¥â«à“À≈—ß®“°°“√√ —°…“¥â«¬¬“´“‡øÕ≈ Ÿ§“ ºŸâªÉ«¬¡’§à“‡©≈ ’ˬ¢ÕßÕ“°“√ÀÕ∫‡Àπ◊ËÕ¬„π™à«ß°≈“ß«—π≈¥≈ß®“° 0.53 ± 0.06‡ªìπ 0.42 ± 0.03 ·≈– 0.29 ± 0.07 à«π§à“‡©≈’ˬ¢ÕßÕ“°“√ÀÕ∫‡Àπ◊ËÕ¬„π‡«≈“°≈“ߧ ◊π≈¥≈ß®“° 1.41 ± 0.12‰ª‡ªìπ 1.02 ± 0.06 ·≈– 0.84 ± 0.04 „π —ª¥“Àå∑ ’Ë 4·≈– 8 ¢Õß°“√√—°…“¥â«¬¬“´“‡øÕ≈ Ÿ§“ µ“¡≈”¥—∫
”À√—∫Õ“°“√ÀÕ∫®π∑”„ÀâµâÕßµ◊Ëπ¢÷Èπ®“°°“√πÕπÀ≈ —∫π—Èπ¡’°“√≈¥≈ß®“° 0.59 ± 0.14 §√ —Èß/§◊𠇪ìπ0.38 ± 0.05 ·≈– 0.24 ± 0.04 §√—Èß/§◊π „π —ª¥“Àå∑ ’Ë 4
·≈– 8 À≈—ß„À⬓ µ“¡≈”¥—∫ ·≈–°“√≈¥≈ßπ’Èæ∫¡’§«“¡·µ°µà“ß®“°æ ◊Èπ∞“π∑ ’Ë¡’π—¬ ”§—≠∑“ß ∂‘µ‘∑—Èß„π —ª¥“Àå∑ ’Ë 4 ·≈– 8 à«π§à“‡©≈ ’ˬ¢Õß°“√„™â¬“¢¬“¬À≈Õ¥≈¡β2- agonist „π√–¬–°àÕπ·≈–À≈ —ß„À⬓´“‡øÕ≈ Ÿ§“ ‰¥â· ¥ß‰«â„πµ“√“ß∑ ’Ë 4 ÷Ëß®–æ∫«à“®”π«π§√ —ÈߢÕß°“√„™â¬“¢¬“¬À≈Õ¥≈¡ β2-agnoist „π°“√√—°…“Õ“°“√ÀÕ∫À ◊¥∑’ˇ°‘¥¢÷È𠉥â≈¥≈ß®“° 2.25 ± 0.16 §√—Èß/«—π‡ªìπ 1.54 ± 0.09 ·≈– 1.13 ± 0.09 §√—Èß/«—π À≈—߉¥â√—∫¬“„π —ª¥“Àå∑’Ë 4 ·≈– 8 µ“¡≈”¥—∫ ·≈–æ∫¡’§«“¡·µ°µà“ß∑’Ë¡’π—¬ ”§—≠∑“ß ∂‘µ‘
√Ÿª∑’Ë 1 · ¥ß§à“‡©≈’ˬ¢Õß PEFR ®“° ¡ÿ¥∫—π∑÷°ª√–®”«—π¢ÕߺŸâªÉ«¬ ‡ª√’¬∫‡∑ ’¬∫™à«ßæ◊Èπ∞“π°àÕπ°“√»÷°…“°—∫ —ª¥“Àå∑’Ë 4 ·≈– 8 À≈ —߉¥â√—∫°“√√ —°…“¥â«¬¬“´“‡øÕ≈Ÿ§“

ªï∑’Ë 25 ©∫—∫∑’Ë 3 °√°Æ“§¡-°—𬓬π 2547 ª√– ‘∑∏ ‘¿“æ·≈–§«“¡ª≈Õ¥¿—¬¢Õ߬“´“‡øÕ≈ Ÿ§“ œ 169
µ“√“ß∑ ’Ë 3 §à“‡©≈ ’ˬ¢ÕßÕ“°“√ÀÕ∫À ◊¥ ∑’ˇ°‘¥¢÷Èπ„π‡«≈“°≈“ß«—π·≈–°≈“ߧ ◊π ®“° ¡ÿ¥∫—π∑ ÷°ª√–®”«—π¢ÕߺŸâªÉ«¬‡ª√’¬∫‡∑’¬∫™à«ßæ ◊Èπ∞“π°àÕπ°“√»÷°…“°—∫ —ª¥“Àå∑’Ë 4 ·≈– 8 À≈—߉¥â√—∫°“√√—°…“¥â«¬¬“´“‡øÕ≈Ÿ§“
µ“√“ß∑’Ë 4 §à“‡©≈’ˬ¢Õß°“√„™â¬“¢¬“¬À≈Õ¥≈¡ β2-agonist ™π ‘¥ Ÿ¥¥¡ ‡æ ◊ËÕ∫√√‡∑“Õ“°“√ ®“° ¡ÿ¥∫—π∑÷°ª√–®”«—π¢ÕߺŸâªÉ«¬ ‡ª√ ’¬∫‡∑’¬∫™à«ßæ ◊Èπ∞“π°àÕπ°“√√ —°…“°—∫ —ª¥“Àå∑’Ë 4 ·≈– 8 À≈—߉¥â√—∫°“√√—°…“¥â«¬¬“´“‡øÕ≈Ÿ§“
Mean Standard deviation P Value
°àÕπ‰¥â√—∫¬“À≈—߉¥â√—∫¬“ 4 —ª¥“ÀåÀ≈—߉¥â√—∫¬“ 8 —ª¥“Àå
± 0.16± 0.09± 0.09
2.251.541.13
0.001< 0.001
Mean Standard deviation P Value (symptom scores)
°≈“ß«—π°àÕπ‰¥â√—∫¬“À≈—߉¥â√—∫¬“ 4 —ª¥“ÀåÀ≈—߉¥â√—∫¬“ 8 —ª¥“Àå
°≈“ߧ◊π°àÕπ‰¥â√—∫¬“À≈—߉¥â√—∫¬“ 4 —ª¥“ÀåÀ≈—߉¥â√—∫¬“ 8 —ª¥“Àå
Õ“°“√ÀÕ∫∑ ’Ë∑”„ÀâµâÕßµ◊Ëπ„π°≈“ߧ ◊π°àÕπ‰¥â√—∫¬“À≈—߉¥â√—∫¬“ 4 —ª¥“ÀåÀ≈—߉¥â√—∫¬“ 8 —ª¥“Àå
± 0.06± 0.03± 0.07
± 0.12± 0.06± 0.04
±0.14±0.05±0.04
0.530.420.29
1.411.020.84
0.590.380.24
< 0.001< 0.001
< 0.001< 0.001
< 0.001< 0.001
Õ“°“√¢â“߇§’¬ß‡π◊ËÕß®“°¬“ : ºŸâªÉ«¬ à«π„À≠à∑πµàÕ¬“´“‡øÕ≈Ÿ§“ ‰¥â¥’‚¥¬„π™à«ß·√°µ—Èß·µà‡√‘Ë¡µâπ°“√»÷°…“®π∂ ÷ß —ª¥“Àå∑ ’Ë 4 ºŸâªÉ«¬„À⧫“¡√ à«¡¡ ◊Õ„π°“√√ —∫ª√–∑“π¬“´“‡øÕ≈Ÿ§“ §‘¥‡ªìπ√âÕ¬≈– 92.3 „π¢≥–∑’Ë°“√„™â¬“„π™à«ß —ª¥“Àå∑’Ë 4 ∂ ÷ß 8 ºŸâªÉ«¬„À⧫“¡√à«¡¡◊Õ„π°“√„™â¬“‡æ‘Ë¡¢÷Èπ√âÕ¬≈– 97.7 ”À√—∫ºŸâªÉ«¬ Õß√“¬ (√âÕ¬≈– 1.8)∑’Ë¡’Õ“°“√·∑√° âÕπ ™π ‘¥ª«¥»√’…– √à«¡°—∫Õ“°“√™“∫√‘‡«≥µâπ§Õ À√◊Õ„® —Ëπ À≈—ß√—∫ª√–∑“π¬“´“‡øÕ≈ Ÿ§“
‰¡à “¡“√∂√ à«¡„π°“√»÷°…“®π®∫‰¥â ‡¡ ◊ËÕÀ¬ÿ¥¬“´“‡øÕ≈ Ÿ§“ æ∫«à“Õ“°“√¥—ß°≈à“«À“¬‡ªìπª°µ‘¿“¬„π 2-3 «—ππÕ°®“°π’ȺŸâªÉ«¬Õ’° 3 √“¬ (√âÕ¬≈– 2.6) ∑’Ë¡’√–¥—∫ ami-notransferase „π‡≈◊Õ¥ Ÿß‡°‘π°«à“ 3 ‡∑ à“¢Õß§à“ª°µ‘ ·µà‰¡àæ∫Õ“°“√ µ—∫Õ—°‡ ∫ ‡™àπ µ—«‡À≈◊Õß µ“‡À≈◊Õß ‡°‘¥¢÷Èπ„π —ª¥“Àå∑ ’Ë 8 ¢Õß°“√√—°…“ °“√µ‘¥µ“¡ºŸâªÉ«¬„π√–¬–µàÕ¡“æ∫«à“√–¥—∫ aminotransferase ¢ÕߺŸâªÉ«¬∑—Èß 3 √“¬π’È°≈—∫§ ◊π‡ªìπª°µ‘À≈—ßÀ¬ÿ¥¬“´“‡øÕ≈ Ÿ§“

170 ∑ —»π’¬“ ÿ∏√√¡ ¡—¬ ·≈–§≥– «“√ “√«—≥‚√§ ‚√§∑√«ßÕ°·≈–‡«™∫”∫ —¥«‘°ƒµ
«‘®“√≥åCysteinyl leukotrienes ‡ªìπ “√∑ ’ˇ°‘¥®“°°“√‡ª≈ ’ˬπ
·ª≈ߢÕß arachidonic acid „π¢∫«π°“√µÕ∫ πÕßµàժؑ°‘√‘¬“∑“ß immune “√ ”§—≠„π°≈ ÿà¡π’È ‰¥â·°à LTC4, LTD4·≈– LTE4 ‡ªìπµ—«°“√ ”§—≠∑’Ë∑”„À⇰‘¥°“√Õ—°‡ ∫ ·≈–À≈Õ¥≈¡À¥‡°√ Áß ¬“∑’ËÕÕ°ƒ∑∏ ‘Ï¢—¥¢«“ß°“√∑”ß“π¢Õßcysteinyl leukotrienes ‡™àπ Pranlukast, Montelukast·≈– Zafirlukast ®–ÕÕ°ƒ∑∏‘Ï¢—¥¢«“ß°“√∑”ß“π¢Õßcysteinyl leukotrienes ∑’Ë receptor ∑”„Àâ¡’Õÿ∫—µ‘°“√≥å¢ÕßÕ“°“√·∑√° âÕπ‡π◊ËÕß®“°¬“‡°‘¥¢÷Èππ âÕ¬¡“° º≈°“√»÷°…“π’È· ¥ß„Àâ‡ÀÁπ«à“¬“´“‡øÕ≈Ÿ§“ ¡’ª√– ‘∑∏ ‘“æ„π°“√§«∫§ÿ¡Õ“°“√‚√§À◊¥‰¥â¥’ ‚¥¬¡’Õ“°“√·≈–°“√„™â¬“¢¬“¬À≈Õ¥≈¡™π ‘¥ β2-agonist ‡æ ◊ËÕ∫√√‡∑“Õ“°“√≈¥≈ßæ√âÕ¡ Ê°—π¡’ ¡√√∂¿“æ°“√∑”ß“π¢Õߪե‡æ‘Ë¡¢÷Èπµ≈Õ¥√–¬–‡«≈“8 —ª¥“Àå∑’Ë ‰¥â√—∫°“√√ —°…“ Fish JE ·≈–§≥–1 æ∫«à“°“√„™â¬“‡øÕ≈Ÿ§“ √à«¡°—∫¬“‡¥‘¡∑’˺ŸâªÉ«¬‰¥â√—∫Õ¬Ÿà®–∑”„ÀâÕ“°“√·≈– ¡√√∂¿“æ°“√∑”ß“π¢Õߪե¥’¢÷Èπ„π¢≥–∑’Ë¡’°“√„™â¬“¢¬“¬À≈Õ¥≈¡‡æ ◊ËÕ∫√√‡∑“Õ“°“√≈¥≈ßµ—Èß·µà«—π∑’Ë ÕߢÕß°“√√—°…“ ·≈–°“√‡ª≈’ˬπ·ª≈ߥ—ß°≈à“« ®–¡’Õ¬Ÿàµ≈Õ¥‡«≈“∑’˺ŸâªÉ«¬‰¥â√ —∫°“√√—°…“¥â«¬¬“π’È ‡π◊ËÕß®“°°“√»÷°…“π ’ȇªìπ°“√»÷°…“„π√–¬–‡«≈“‡æ’¬ß 8 —ª¥“Àå®÷߉¡à “¡“√∂· ¥ß„Àâ‡ÀÁπª√– ‘∑∏ ‘¿“æ¢Õ߬“„π°“√§«∫§ÿ¡Õ“°“√¢Õß‚√§„π√–¬–¬“«‰¥â Õ¬à“߉√°Á¥’¡’º≈°“√»÷°…“„π√–¬–¬“«À≈“¬°“√»÷°…“∑’Ë· ¥ßª√– ‘∑∏‘¿“æ¢Õ߬“„π°“√§«∫§ÿ¡Õ“°“√®–§ßÕ¬Ÿàµ≈Õ¥√–¬–‡«≈“∑ ’˺ŸâªÉ«¬‰¥â√—∫°“√√ —°…“¥â«¬¬“π ’È1-3 ·≈–º≈°“√»÷°…“π ’Ȭ—ßµ√ß°—∫°“√»÷°…“Õ ◊ËπÕ’°À≈“¬°“√»÷°…“ ∑ ’Ë· ¥ß„Àâ‡ÀÁπ«à“ Anti-leukotriene ¡’ª√– ‘∑∏‘¿“æ„π°“√§«∫§ÿ¡Õ“°“√¢Õß‚√§À◊¥‰¥â‡ªìπÕ¬à“ߥ’ 4-11 °“√‡ª√ ’¬∫‡∑’¬∫ª√– ‘∑∏‘¿“æ¢Õß´“‡øÕ≈ Ÿ§“ °—∫§Õ√ 嵑‚§ ‡µ’¬√Õ¬¥å™π‘¥ Ÿ¥¥¡ „π°“√»÷°…“¢Õß Knorr B ·≈–§≥–12 æ∫«à“„π√–¬–·√°¢Õß°“√√—°…“ºŸâªÉ«¬‚√§À◊¥∑ ’Ë¡’§«“¡√ÿπ·√ߢÕß‚√§„π¢π“¥ª“π°≈“ߧÕ√嵑‚§ ‡µ’¬√Õ¬¥å™π‘¥ Ÿ¥¥¡®–∑”„À⺟âªÉ«¬¡’ ¡√√∂¿“æ°“√∑”ß“π¢Õߪե‡°’ˬ«°—∫ FEV1 Ÿß¢÷Èπ·≈–¥’°«à“°≈ÿࡺŸâªÉ«¬∑’ˉ¥â√—∫°“√√ —°…“¥â«¬¬“ Montelukast Õ¬à“߉√-
°Áµ“¡°“√„™â¬“∑—Èß Õßπ’ȵ‘¥µàÕ°—π‡ªìπ‡«≈“π“π∂÷ß 12 ‡¥ ◊Õπ®–‰¡àæ∫§«“¡·µ°µà“ß√–À«à“ߪ√– ‘∑∏‘¿“æ„π°“√§«∫§ÿ¡Õ“°“√ ·≈– ¡√√∂¿“æ°“√∑”ß“π¢Õߪե„πºŸâªÉ«¬∑ —Èß Õß°≈ÿà¡ „π°“√»÷°…“‡ª√ ’¬∫‡∑ ’¬∫ª√– ‘∑∏‘¿“æ¢Õ߬“∑ —Èß Õß„πºŸâªÉ«¬‚√§À ◊¥‡√◊ÈÕ√—ß∑’Ë¡’§«“¡√ ÿπ·√ߢÕß‚√§„π¢π“¥ª“π°≈“ß Busse W ·≈–§≥–13 æ∫«à“ Fluticasone ¡’ª√– ‘∑∏‘¿“æ„π°“√§«∫§ÿ¡Õ“°“√‰¥â¥’°«à“´“‡øÕ≈Ÿ§“ Calhoun W 14 æ∫«à“°“√„™â¬“‡øÕ≈Ÿ§“ „π¢π“¥ 80 ¡°.√—∫ª√–∑“π«—π≈– 2 §√—Èß ®–∑”„Àâ√–¥—∫ aminotransferase„π‡≈◊Õ¥¢ÕߺŸâªÉ«¬∫“ß√“¬ Ÿß‚¥¬‰¡à¡’Õ“°“√· ¥ß¢Õßµ—∫Õ—°‡ ∫ „π¢≥–∑’Ë Fish JE ·≈–§≥–1 æ∫«à“ºŸâªÉ«¬‚√§À◊¥∑ ’ˉ¥â√—∫´“‡øÕ≈Ÿ§“ „π¢π“¥ 20 ¡°. √—∫ª√–∑“π«—π≈– 2 §√ —Èß ¡’Õÿ∫ —µ‘°“√≥å¢Õß√–¥—∫ aminotransferase„π‡≈◊Õ¥ Ÿß¢÷Èπ‡°‘π°«à“ 2 ‡∑ à“¢Õß§à“ª°µ‘ „π°≈ÿࡺŸâªÉ«¬∑’ˉ¥â√—∫´“‡øÕ≈ Ÿ§“ ·≈–¬“À≈Õ°‡ªìπ√âÕ¬≈– 3.1 ·≈– 2.8µ“¡≈”¥—∫ ´÷Ë߉¡àæ∫«à“¡’§«“¡·µ°µà“ß∑’Ë¡’π—¬ ”§—≠∑“ß ∂‘µ‘ ·≈–ºŸâªÉ«¬∑ ’Ë¡’√–¥—∫ aminotransferase Ÿß‡À≈à“π’ȉ¡àæ∫«à“¡’Õ“°“√∑“ߧ≈ ‘π‘°¢Õßµ—∫Õ—°‡ ∫‡°‘¥¢÷Èπ·µàÕ¬à“߉√√«¡∑—Èß√–¥—∫ aminotransferase ∑’Ë Ÿß¢÷Èππ’È®–≈¥≈߇¢â“ Ÿà¿“«–ª°µ‘„π√–¬–‡«≈“‰¡à‡°‘π 3 ‡¥◊ÕπÀ≈—ßÀ¬ÿ¥¬“Õ¬à“߉√°Á¥’¡’√“¬ß“πºŸâªÉ«¬∑’Ë¡’Õ“°“√µ—∫Õ—°‡ ∫√ ÿπ·√ßÀ≈ —߉¥â√—∫¬“´“‡øÕ≈ Ÿ§“ 3 √“¬15 √“¬·√°¡’ aminotransferase„π‡≈◊Õ¥ Ÿ¥¢÷ÈπÀ≈—ß„™â¬“ “‡øÕ≈ Ÿ§“ ¡“ 9 ‡¥ ◊Õπ ·≈–√–¥—∫aminotransferase „π‡≈◊Õ¥∑ ’Ë≈¥≈߇ªìπª°µ‘À≈—ßÀ¬ÿ¥¬“°≈—∫ Ÿß¢÷ÈπÕ’°‡¡◊ËÕ∑¥≈Õß„À⬓´“‡øÕ≈Ÿ§“ „À¡àÕ’°§√—Èß√“¬∑’Ë Õß¡’√–¥—∫ amonotransferase ·≈– bilirubin Ÿß¢÷ÈπÀ≈—ß√ —∫ª√–∑“π¬“´“‡øÕ≈Ÿ§“ ¡“ 5 ‡¥ ◊Õπ ‡π◊ËÕß®“°ºŸâªÉ«¬¡’Õ“°“√µ—∫Õ—°‡ ∫√ÿπ·√ß¡“°¢÷Èπ ®÷߉¥â√ —∫°“√√—°…“‚¥¬°“√ºà“µ—¥‡ª≈’ˬπµ—∫ À≈—ßºà“µ—¥ºŸâªÉ«¬À“¬‡ªìπª°µ‘√“¬ ÿ¥∑⓬ºŸâªÉ«¬¡’Õ“°“√µ—∫Õ—°‡ ∫‡°‘¥¢÷ÈπÀ≈—߉¥â√—∫¬“´“‡øÕ≈ Ÿ§“ 6 ‡¥◊Õπ ºŸâªÉ«¬√“¬π ’È ‰¥â√ —∫°“√√—°…“¥â«¬¬“§Õ√ 嵑‚§ ‡µ’¬√Õ¬¥å ®πÀ“¬‡ªìπª°µ‘ „π°“√»÷°…“π’Èæ∫«à“¡’ºŸâªÉ«¬ 3 √“¬ (√âÕ¬≈– 2.6) ∑’Ë¡’√–¥—∫ aminotrans-ferase „π‡≈◊Õ¥ Ÿß°«à“§πª°µ‘ 3 ‡∑ à“ ‚¥¬‰¡à¡’Õ“°“√· ¥ß¢Õßµ—∫Õ—°‡ ∫ ‡™àπ µ—«‡À≈◊Õß µ“‡À≈◊Õß „π —ª¥“Àå

ªï∑’Ë 25 ©∫—∫∑’Ë 3 °√°Æ“§¡-°—𬓬π 2547 ª√– ‘∑∏ ‘¿“æ·≈–§«“¡ª≈Õ¥¿—¬¢Õ߬“´“‡øÕ≈ Ÿ§“ œ 171
∑’Ë 8 ¢Õß°“√√—°…“ ·≈–„π°“√µ‘¥µ“¡µàÕ¡“æ∫«à“√–¥—∫aminotransferase ∑’Ë Ÿß¢÷Èππ ’È °≈—∫§◊π Ÿà ¿“«–ª°µ‘‰¥âÀ≈—ßÀ¬ÿ¥¬“ ”À√—∫Õ“°“√·∑√° âÕπ‡π◊ËÕß®“°¬“∑’Ëæ∫„π°“√»÷°…“π ’È ‰¥â·°àª«¥»’√…– À√◊Õ„® —Ëπ´÷Ëßæ∫„πºŸâªÉ«¬ 2 √“¬(√âÕ¬≈– 1.8) lge OM ·≈–§≥–16 æ∫Õÿ∫—µ‘°“√≥ å¢Õß°“√ª«¥»√’…– ‡π◊ËÕß®“°¬“´“‡øÕ≈Ÿ§“ Ÿß∂÷ß√âÕ¬≈– 6.7 ·µà¬—߉¡àà¡’§”Õ∏ ‘∫“¬∑ ’Ë™—¥‡®π„π‡√◊ËÕßπ ’È °“√∑ ’ˬ“´“‡øÕ≈ Ÿ§“ ¡’ª√– ‘∑∏‘¿“æ„π°“√§«∫§ÿ¡Õ“°“√‰¥â¥’ ¡’Õ“°“√·∑√°´âÕπ‡π◊ËÕß®“°¬“‡°‘¥¢÷Èππ âÕ¬¡“° ·≈–‰¡à√ÿπ·√ß √«¡∑—ÈßÕ“°“√·∑√°´âÕπ¥—ß°≈à“«®–À“¬‰ª‡¡ ◊ËÕÀ¬ÿ¥¬“ ®÷ßÕ“®°≈à“«‰¥â«à“´“‡øÕ≈ Ÿ§“ ‡ªìπ¬“Õ’°¢π“πÀπ ÷Ëß ∑ ’Ë¡’ª√– ‘∑∏‘¿“æ·≈–§«“¡ª≈Õ¥¿—¬„π°“√„™â√—°…“‚√§À ◊¥‰¥â¥’Õ’°¢π“πÀπ ÷Ëß
√ÿª´“‡øÕ≈Ÿ§“ ‡ªìπ¬“√—°…“‚√§À◊¥™π‘¥√ —∫ª√–∑“π∑’Ë
ÕÕ°ƒ∑∏‘Ï¢—¥¢«“ß°“√∑”ß“π¢Õß cysteinyl leukotrienes°“√„™â¬“π ’È√—°…“ºŸâªÉ«¬‚√§À◊¥∑’Ë¡’§«“¡√ÿπ·√ߢÕß‚√§„π¢π“¥πâÕ¬∂ ÷ߪ“π°≈“ß‚¥¬„™â¬“ 20 ¡°.√ —∫ª√–∑“π«—π≈–2 §√ —Èß ‡ªìπ‡«≈“ 8 —ª¥“Àå æ∫«à“¬“ “¡“√∂§«∫§ÿ¡Õ“°“√¢Õß‚√§À◊¥‰¥â‡ªìπÕ¬à“ߥ’ ·≈–ºŸâªÉ«¬¡’ ¡√√∂¿“æ°“√∑”ß“π¢Õߪե‡æ‘Ë¡¢÷Èπµ≈Õ¥√–¬–‡«≈“∑ ’Ë∑”°“√»÷°…“ „π¢≥–∑ ’ËÕ“°“√·∑√°´âÕπ‡π◊ËÕß®“°¬“‡°‘¥¢÷ÈππâÕ¬¡“° ·≈–Õ“°“√¥—ß°≈à“«°≈—∫§◊π‡ªìπª°µ‘‰¥âÀ≈—ßÀ¬ÿ¥¬“ ´“‡øÕ≈Ÿ§“ ®÷߇ªìπ¬“√—°…“‚√§À ◊¥Õ’°¢π“πÀπ ÷Ëß∑’Ë “¡“√∂π”¡“„™â„π°“√√— °…“‡æ◊Ë Õ§«∫§ÿ¡Õ“°“√¢ÕߺŸâªÉ«¬‚√§À◊¥‰¥âÕ¬à“ß¡’ª√– ‘∑∏ ‘¿“æ·≈–ª≈Õ¥¿—¬
‡Õ° “√Õâ“ßÕ‘ß1. Fish JE, Kemp JP, Lockey RF et al. Zafirlukast for symp-
tomatic mild-to-moderate asthma: a 13-w eek multicenterstudy. Clin Therap 1997;19(4):675-690.
2. Kelloway JS. Zafirlukast: The first leukotriene-receptorantagonist approved for the treatment of asthma. AnnPharmacother 1997; 31:1012-1021.
3. Grossman J, Smith LJ., Wilson AM, et al. Long-termsafety and efficacy of Zafirlukast in the treatment ofasthma: interim results of an open-label-extension trial.Ann Allergy Asthma Immunol 1999;82:361-369 .
4. Holgate ST. What is the place of leukotriene receptorantagonist in clinical practice ? Eur Respir J 2001;11:74, 41-46.
5. Bjermer L. History and future perspective of treatngasthma as systemic and small airways disease. RespirMed 2001; 95: 703-719.
6. Knorr B, Franchi LM, Bisgaard H, et al. Montelukast,a Leukotriene receptor antagonist, for the treatmentof persistant asthma in children age 2 to 5 years.Pediatrics 2001; 108 (3):E48.
7. Bisgaard H. Leukotriene modifiers in pediatric asthmamanagement. Pediatrics 2001; 107:2. 381-390.
8. Donald P, Tashkin MD, Robert A, et al. An evaluationof Zufirlukast in the treatment of asthma with explor-atory subset analyses. J Allergy Clin Lmmunol 1999;103;2: 246-254.
9. Suissa S, Dennis R, Ernst P, et al. Effectiveness of theleukotriene receptor antagonist Zafirlukast for mild-tomoderate asthma. A randomized, double-blind,placebo-controlled trial. Ann Intern Med 1997: 126:177-183.
10. Tsai JJ, Chan SC, Ho CK, et al. Efficacy of Zafirlukastin the treatment of patients with bronchial asthma. JMicrob Immunol infec 2001; 34:63-70.
11. Barnes NC, Black B, Syrett N, et al. Reduction ofexacerbations of asthma in multinational clinical trialwith Zafirlukast (Accolate TM). Allergy 1996; 51 (Suppl30): 84.
12. Knorr B, Noonan G, McBurpey J, et al. Evaluation ofthe long-term effect of montelukast in adult ( 15 years)and pediatric (6 to 14 years) patients. Eur Respir J1999; 14 (suppl. 30):29s Abstract.
13. Busse W, Wolfe J, Storms W, et al. Fluticasonepropionate compared with Zafirlukast in controllingpersistent asthma: a randomized double-blind,placebo-controlled trial. J Family Practics 2001;50:595-602.

172 ∑ —»π’¬“ ÿ∏√√¡ ¡—¬ ·≈–§≥– «“√ “√«—≥‚√§ ‚√§∑√«ßÕ°·≈–‡«™∫”∫ —¥«‘°ƒµ
14. Calhoun WJ. Summary of clinical trials with Zafirlukast.Am J Respir Crit Care Med. 1998; 157:S238-46.
15. Reinus JF, Presky S, Burkiewicz JS, et al. Severe liverinjury after treatment with the leukitriene receptor an-tagonist Zafirlukast. Ann Intern Med. 2000 ;133:964-968.
16. Ige OM and Onadeko BO. An open study to evaluatethe safety and efficacy of Zafirlukast (Accolate) inpatients with mild to moderate asthma in lbadan,Nigeria, West African J Med 2001 ;20:220-226.

130 «—π™—¬ ‡¥™ ¡ƒ∑∏ ‘σ∑—¬ «“√ “√«—≥‚√§ ‚√§∑√«ßÕ°·≈–‡«™∫”∫ —¥«‘°ƒµ
æ‘∏’«“ßæ«ß¡“≈“ ç«—π¡À‘¥≈é
«—π∑’Ë 24 °—𬓬π 2547 𓬷æ∑¬åπ—¥¥“ »√ ’¬“¿—¬ 𓬰 ¡“§¡ª√“∫«—≥‚√§·Ààߪ√–‡∑»‰∑¬ „πæ√–∫√¡√“™Ÿª∂—¡¿å æ√âÕ¡¥â«¬§≥–欓∫“≈·≈–‡®â“Àπâ“∑ ’Ë ‰¥â‡¢â“√à«¡æ‘∏’«“ßæ«ß¡“≈“∂«“¬ —°°“√–·¥à ¡‡¥Á®æ√–¡À‘µ≈“∏‘‡∫»√ Õ¥ÿ≈¬‡¥™«‘°√¡æ√–∫√¡√“™™π° ≥ Õπ ÿ “«√’¬å ¡‡¥Á®æ√–√“™∫‘¥“ ·Ààß°“√·æ∑¬å‰∑¬ „π∫√‘‡«≥‚√ß欓∫“≈»‘√‘√“™
❄




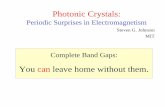


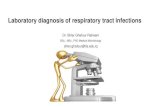





![Ba^QdPc E RPW lPMcW^] - Farnell element145 P^\_McWOWZWch 5 § 5 @^ §@^ BVhbWPMZ EWjR HI g : g 5 I \\ ?MW] J J 7a^]c E_RMYRa J J 4R]cRa E_RMYRa J J DRMa E_RMYRa J J EdOf^^SRa g g 5WbP](https://static.fdocument.org/doc/165x107/5f62e0104f48cc34e33e05f9/baqdpc-e-rpw-lpmcw-farnell-5-pmcwowzwch-5-5-bvhbwpmz-ewjr-hi.jpg)