Spring Issue
21
-
Upload
mostly-medicaid -
Category
Documents
-
view
235 -
download
2
description
Medicaid news
Transcript of Spring Issue

X
I S I T D E A D?
Jobs
X
T h e M e d i c a i d B i g P i c t u r e Y o u N e e d . I n U n d e r 5 M i n u t e s.
M o s t ly M e d i c a i d
HEALTH REFORM
SPECIAL ANALYSIS- MEDICAID FINANCIAL REALITY- A SCARY STORY TOLD WITH PICTURES P. 10
Fraud News P.15
Quality+ Innovaon News P.3 Rx Update
P. 13
Health Reform NewsPage 5
Spring 2010
Joblis ngsPAGE 18

4th Annual
Medicaid Medicaid Medicaid Medicare Medicare Medicare Medicare Medicare Medicare Medicare Medicare Medicare Medicare Medicare Medicare Medicare Medicare Medicare Medicare Medicare Medicare Medicare Medicare Medicare Medicare Medicare Medicare Medicare Medicare Medicare Medicare Medicare Medicare Medicare Medicare Medicare Medicare Medicare Medicare Marketing Marketing Marketing Marketing Marketing Marketing Marketing Marketing Marketing Marketing Marketing Marketing Marketing Marketing Marketing Marketing Marketing Marketing Marketing Marketing Marketing Marketing Marketing Marketing Marketing Marketing Marketing Marketing Marketing Marketing Marketing Marketing Marketing Marketing Marketing Marketing Marketing Marketing Marketing Marketing Marketing Marketing Marketing Marketing Marketing Marketing Marketing Marketing Marketing Marketing Marketing Marketing Marketing Marketing Marketing Marketing Marketing Marketing Marketing Marketing Marketing Marketing Marketing Marketing Marketing Marketing Marketing Marketing Marketing Marketing Marketing Marketing Marketing Marketing Marketing Marketing Marketing Marketing Marketing Marketing Marketing Marketing Marketing Marketing Marketing Marketing Marketing Marketing Marketing Marketing Marketing Marketing Marketing Medicare Medicare Medicare Marketing Marketing Marketing
Medicare Toolkit• Receive Key Updates on Healthcare Reform and its
Impact on Marketing to Increase Plan Compliance
• Integrate Marketing Across Diff erent Media Channels to Grow Age-In and Current Enrollee Market Share
• Create Compliant Customer Service Approaches to Identify and Respond to Today’s Senior Population
• Understand the Evolving Medicare Sales Strategy to Prepare for a Post-Reform Environment
• Explore Innovative Marketing and Retention Strategies for Medicare SNP Plan Growth
• Leverage Best Practices to Maintain Quality and Boost Enrollment During Peak Periods
Medicaid Toolkit• Drive Creative Partnerships with Advocacy Groups to
Expand Outreach Dollars under Limited Budgets
• Maximize ROI on Marketing Initiatives in Tight Budgets
• Master Meeting EPSDT Well Visit Goals Th rough Innovative Checkup Outreach Programs
• Improve Member Retention and Quality Outcomes For Better Regulatory and Financial Outcomes
• Grow Maternal Post-Partum Visit Rates through Overcoming Barriers to Improve HEDIS Scores
• Understand the changing demographics of your plan and community to provide culturally competent services and give providers to the tools to make necessary changes
Advanced strategies to optimize enrollment, maximize retention and ensure compliance in an era of change
&
Enrollment Congress&
March 22-23, 2010 • Hilton Baltimore • Baltimore, MDMention priority code XP1514MMad when registering
www.iirusa.com/mmo
Actionable Insights from the Plans & Thought Leaders You Admire MostAetna • Amerigroup • Amerihealth Mercy • Blue Cross Blue Shield of AL • Blue Cross Blue Shield of MN • Blue Cross Blue Shield of SC • Boston Medical Center Healthnet Health Plan • CareSource • Community Partners • Louisiana Dept of Health & Hospitals • Medica Health Plans • Molina Healthcare of Ohio • Neighborhood Health Plan • Oklahoma Healthcare Authority/SoonerCare • OmniCare • Passport Health Plan • Priority Health • State of Maryland • UCare • UC Berkeley • UPMC Health Plan

3
QUALITY AND INNOVATION NEWS
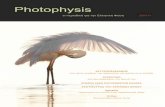
Very few doctors see enough Medicare patients to report reliable quality metrics
CMS releases meaningful use regs for EHRs
‐ Kristin Patterson and MM Staff
Sample size does not compute
The whole world may be abuzz with using
quality metrics to reform payment ‐ there's
just one big problem. According to a study
published in JAMA in December 2009, most
primary care physicians don't even see
enough Medicare patients to calculate the
current Medicare quality measures with
statistical validity. Put simply, their Medicare
patient traffic is too low to tell if they are
improving quality or cost. The lowest sample size needed is 328 patients (for mammography) and the
highest needed is more than 19,000 patients (for hospital prevention). Most physicians see less than 180
Medicare patients each year. If Medicare quality and cost measurement are to be the standards moving
forward, this ain't looking good.1
Regulations Defining Meaningful Use of Electronic Health Records Released
When the American Recovery and Reinvestment Act of 2009 was signed, the law included the Health
Information Technology for Economic and Clinical Health Act (HITECH). HITECH gives CMS the authority
to establish criteria for the utilization of EHR technology within the healthcare system. Under the
proposed regulation, meaningful use is defined by CMS and ONC as “an eligible professional or eligible
Calculating Medicare Quality Metrics - Not Enough Patients Seen to be Accurate
180
328
Average Seen by Physicians Mammography Sample Size Needed

4
hospital that, during the specified reporting period, demonstrates meaningful use of certified EHR
technology in a manner that improves quality, safety, and efficiency of health care delivery, reduces
health care disparities, engages patients and families, improves care coordination, improves
population and public health, and ensures adequate privacy and security protections for personal
health information.”2
During the first year of participation in
the program both eligible professionals
and hospitals must demonstrate they
have performed one or all of the
following criteria: 1) acquired and
installed an EHR system 2) trained staff,
deployed tools and exchanged data or 3)
upgraded a certified EHR system by
expanding its functionality and
interoperability.3
Furthermore, participants must also
satisfy additional annual requirements
such as 30 percent Medicaid patient volume (for professionals), average length of stay of 25 days or
fewer and 10 percent Medicaid patient volume (for hospitals).4
At first glance, the initial cost of implementing an EHR system might be too expensive for operating
budgets; however, eligible professionals can receive up to $63,750 over a six year period while hospital
payments are determined by a formula that benefits those with a high Medicaid patient volume. If the
proposed regulation is passed, providers should consider this an opportunity to implement an EHR
system at a lower cost. Moreover, incentive payments could begin as early as October 2010 to eligible
hospitals and January 2011 to other providers which would help ease the immediate cost burden of
implementing or upgrading a system.5
The proposed regulation contains many incentives to accelerate and facilitate the adoption of health
information technology by individual providers and organizations throughout the healthcare system.
More news over at the Mostly Medicaid Blogs
blog.mostlymedicaid.com where the best Medicaid minds mingle.

5
Participants will see that the costs of implementation will be offset by improvements to patient safety
and quality, reduction of medical errors and acquisition of a loyal patient base.
HEALTH REFORM NEWS Updates on the madness
States that have already broadened health care coverage say that the Senate overhaul bill
unfairly penalizes them
Looking at managed care firms and incentives for reform
Medicaid expansion by having Medicare pick up the full tab for duallies
‐Brendan Stern, Clay Farris, and Kristin Patterson
Given the direction of current political winds, the Great Health Reform Debate may be over
soon – so we thought we’d talk about it one more time.
Updates on the madness
It has truly been head‐spinning to try to keep up with the health reform changes / ideas proposed each
day. In December, some senators were trying to lower the Medicare eligible age to 55 as well as extend
mandatory Medicaid coverage to families with incomes up to $33,075. Those wacky politicians also
proposed requiring insurance companies to spend 90% of premiums on services, building in a profit
limit. Sort of like only giving to charities who have lower admin costs?
Oh, before we forget ‐ Harry Reid (who's admittedly on
our naughty list for his shameful pork slinging ‐ see last "We are, in a sense, being punished for our own charity."

6
issue) compared opposition to passing his health
reform opus to opposition to abolition. We know
that all's fair in love, war and US politics but that
low‐blow is just downright disgusting.
States have been aware for a while that they
would be the one paying for the grand federal
vision of healthcare being crafted in DC right
now‐ but now states are also starting to realize
that the new financing model of Medicaid will be
pretty unfair. Unfair, you say? Oh yeah‐ especially if you're a state that's already been working to
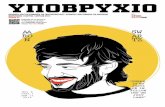
expand coverage. If you have already worked to increase your own Medicaid rolls, you'll get about 80‐
95% of any new expansion efforts under health reform paid for by the feds. If you have not been
expanding coverage up until now, you'll get back 95%. Taxes from states like Arizona, California, and
New York will be going to bring other states up to speed.
And that's the same story for about 20 states that have already been expanding coverage before now.
NY's Governor Peterson has said that "We are, in a sense ,being punished for our own charity." Arizona
has calculated that the new taxes that the health reform package will exact from its state will be about
$17B. If it would not have expanded coverage already (it did so back in 2001), the health reform bill
today for AZ would be about $1.4B. In this formulation of the costs, Arizona would be overpaying for
health reform by about $16B.
Finally, EVERYONE will be paying for Nebraska Medicaid if sleezeball Ben Nelson's deal to get his state
exempted from paying for health reform goes through. In case you've been living under a rock ‐ the
Senator from Nebraska held out his vote for safe passage of the bill so he could bargain it for one huge
piece of pork. 6
It Pays to Wait Costs to Your State Under Health Reform
Proposals What you pay if you have already worked to expand Medicaid in your state
20%
What you pay if you have NOT already worked to expand Medicaid in your state
5%

7
"The special deal for Nebraska was wrong; expanding it makes it even worse. Even today, Medicaid
struggles to serve those already on its rolls, and a full 40 percent of doctors refuse Medicaid patients
because the federal government can't foot the bill. Adding 18 million more people to an already limping
program is not the reform Americans want and would have tremendously serious consequences." –
Senator Mike Johanns (R), Nebraska
Managed Care Firms and the Incentives for Medicaid Expansion
Managed Care Organizations are chomping at the bit as the prospect of expanded state Medicaid
programs, positioning themselves to reap the benefits that such an expansion would create for
capitated health management businesses. In 2009 the health insurance industry lobby, America’s Health
Insurance Plans, released a Lewin Group report to substantiate cost‐saving claims made by MCO’s in
various Medicaid programs. The report, Medicaid Managed Care Cost Savings – A Synthesis of 24
Studies, while not the most unbiased document ever written on the topic of Medicaid cost savings,
nonetheless reveals a great deal about the strategic aims of the managed care industry as it seeks to
position itself to favorably benefit from potential changes to the public insurance market.
Unsurprisingly, many of the current woes experienced by MCO’s serving Medicaid populations would
be redressed to varying degrees by expanding Medicaid:
1. Transitory Enrollment – Since many Medicaid MCO enrollees are covered by the Transitional Assistance to Needy Families program (TANF), their short enrollment periods cause churning and raise administrative costs for the group as a whole. Expanded Medicaid ranks would obviously reduce this churning and help to flatten the cost curve beyond the few months of eligibility currently enjoyed by TANF beneficiaries.
2. Oddly enough, AHIP lists poverty as a
barrier to MCO’s ability to coordinate care – Language barriers, lack of transportation, and other poverty‐related issues pose a hindrance to care management in the opinion of the Lewin Group. The Senate
Democratic bill in its current form would standardize Medicaid eligibility at 133% of the Federal poverty line, combined with the increased overhead from such an expansion, this could help dedicate more resources to the neediest enrollees.
3. Prescription Drug Rebates – MCO’s do not
qualify under the Medicaid Drug Rebate Program, meaning drug companies don’t need to grant them the ‘lowest price,’ as a state Medicaid agency would be able to obtain. Expanding Medicaid, along with granting MCO’s ‘most favored’ status, would give MCO’s more bargaining power and lead to reduced pharmaceutical costs. 7

8
Another Way of Looking at All of This
With all the talk over healthcare
expenditures breaking the bank,
the funny thing is spending on
Medicaid has not really increase
proportionately to GDP. The
punchline – WE’RE SPENDING
WAY MORE ON EVERYTHING.
Have Medicare Pick up the Full Tab for Duallies to Finance Medicaid Expansion
Medicaid expansion has been one of the leading health reform proposals in both the House and Senate.
But with states facing budget gaps of at least $350 billion from 2010through 2011, having states fund
the expansion seems insane.8
The American Recovery and Reinvestment Act provided $87 billion from October 2008 through 2010 for
states in the form of an increase in the federal share of Medicaid. However these stop gap funds will
expire at the end of 2010 and a number of states have yet to experience a full economic recovery.9

9
The House bill could expand Medicaid eligibility to 150 percent of the FPL and the Senate Bill could
expand Medicaid eligibility to 133 percent of the FPL. Both bills plan to finance Medicaid expansion with
high federal match rates for new enrollees and current match rates for current enrollees and new
participation of those currently eligible.10
The result, however, would be continued state and regional variation in terms of costs and eligibility,
with higher costs and coverage in Southern and Western states compared to the Northeast and
Midwest. There are different approaches to finance Medicaid expansion that argue for improvements
to the current system. Many of these actions, if undertaken, would be enough to cover the costs of new
enrollees.
Dual eligibles (those receiving both Medicaid and Medicare benefits), for
example, makeup nearly 8.8 million of the Medicaid population and account for
over 40 percent of overall Medicaid spending. Although dual eligibles constitute just 17
percent of the Medicaid population, their care is split between programs, with Medicare responsible for
acute care while Medicaid pays for long‐term care services, dental care and other benefits not covered
under Medicare.11
If the federal government assumed all costs for dual eligibles through Medicare, including premiums and
other services not currently covered by Medicare, states would save approximately $69.8 billion dollars.
If Medicaid expansion is passed, this cost saving measure would be able to cover new enrollees and
avoid perpetuation of inequities within the current system. This suggestion is only one of many that
question the relationship between Medicare and Medicaid. Rather than working independently, the
benefits of some Medicare enrollees are being financed by Medicaid funds which forces states to
continually restrict Medicaid eligibility requirements and
reduce benefits. The opportunity to reform the allocation
of funds and sever the relationship between Medicare
and Medicaid systems is here. Hopefully, the federally
government would look at alternative financing options
like this one before a bill is passed.
If the federal government assumed all costs for dual eligibles through Medicare, including premiums and other services not currently covered by Medicare, states would save approximately $69.8 billion dollars.

10
SPECIAL ANALYSIS
MEDICAID FINANCIAL REALITY‐ A SCARY STORY TOLD WITH PICTURES ‐Brendan Stern
Much has been said about the fiscal pressure states face when they have to balance their
budgets in tough times. Here’s a sobering visual depiction of what that means.
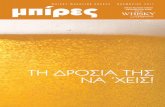
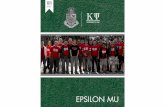
Figure 1 shows total revenues from state and local taxes for all states between 1997 and 2009. Despite
the dot‐com crash in early 2000 and two subsequent wars, state revenues held strong for most of the
past decade before taking a dive in tandem with the housing market. To be fair, much of the increase in
tax revenues could be attributed to the housing bubble itself. Yet there is no denying that the
pie grew between 1997 and 2008: 78% according to the Census. Rarely does one see
a truly state‐centric illustration of the Medicaid equation, but Figure 2 depicts only the state’s share of
Medicaid expenditures over the same time period:
Figure 1: Total Revenues from State and Local Taxes
0
200
400
600
800
1,000
1,200
1,400
2009 2008 2007200620052004200320022001 2000 1999 1998 1997
Billions
Source: www.census.gov/govs/www/qtax.html
Total Revenues from State and Local Taxes

11
Total State Medicaid Expenditures
0
20
40
60
80100
120
140
160
180
2009200820072006200520042003200220012000199919981997
Bill
ions
Source: CMS
Total State Medicaid Expenditures
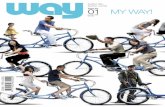
As the revenue pie grew, so too did state Medicaid expenditures: staying between 10% and 12 % of total
revenues until 2009. As Figure 3 illustrates, 2009 marks the first time that state Medicaid expenditures
grew significantly when compared to state tax revenues: from an average of about 10% from 1997 –
2008 to 18% in 2009.
0
200
400
600
800
1,000
1,200
1,400
2009200820072006200520042003200220012000199919981997
Bill
ions
Source: www.census.gov/govs/www/qtax.html
0%
2%
4%
6%
8%
10%
12%
14%
16%
18%
20%
Total Revenues from State and Local TaxesState Medicaid Expenditures as Percent of Total State Revenues
Figure 2: Total State Medicaid Expenditures
Figure 3: Total State Medicaid Expenditures vs State Revenues

12
Obviously there has been increased federal assistance made available to states to help cope with the
effects of rising unemployment and bulging Medicaid rolls, but if tax revenues do not rebound in short
order states will have difficulty navigating the post‐ARRA world without some type of reforms made to
the joint state and federal program. As a final illustration, Figure 4 depicts the percent change in state
tax revenues alongside the percent change in state Medicaid expenditures: something (or more
accurately, some people) must give.
-40%
-30%
-20%
-10%
0%
10%
20%
2009200820072006200520042003200220012000199919981997
Source: CMS & U.S. Census Data
Percent Change in State Tax Revenues Percent Change in State Medicaid Expenditures
Figure 4: Change in State Medicaid Expenditures vs Change in State Revenues

13
Pharmacy Update
The Atypicals Battle: Version 2.0
The atypicals issue we've been covering for 2 years now is back in the Medicaid news cycle. Rutgers and
Columbia just released a study showing that Medicaid kids are more likely to get atypical antipsychotics
(very powerful drugs with high off‐label usage) than privately‐insured kids. The disparity is especially
concerning given the severe weight gain and other common side‐
effects. The drugs are designed for severe mental health issues like
bipolar disorder, but often kids are being prescribed these drugs
without meeting the indications for such conditions. These drugs are big
money for pharma ‐ raking in nearly $8B in Medicaid sales alone for
2006. The Rutgers/Columbia study looked at data for seven state
Medicaid programs between 2001 and 2004. According to the study,
Medicaid kids are 4 times more likely to get the drugs.12
According to the study, Medicaid kids are 4 times more likely to get the drugs.

14
We’re on Facebook and Twitter, too! Look us up searching “medicaid”
or “mostly medicaid”

15
FRAUD NEWS
NY Medicaid thinks $53M in overpayments is not worth going after
Gettin’ High on the Taxpayer’s Dime
And Other Fun Fraud Facts
We all know some money is going to get wasted when you're slinging
around billions (soon to be trillions) of taxpayers' dollars ‐ but come on!
These nuggets from NY Medicaid seem like the punchline of some really
bad jokes (see the nuggets sidebar). Keep in mind all this happened in only
a five year period according to the state comptrollers report. The state
comptroller DiNapoli‐ said "The state's Medicaid system is leaking millions
of taxpayer dollars." And that's just the waste identified in his most recent
audit. DiNapoli has ID'd more than $400M in improper payments (including
fraud) over the past 3 years. When he tried to get the NY
Medicaid agency to go after the $53M lost to
duplicate member numbers, he was told that that
was not a lot of money compared to the billions
spent each year. Makes you feel good, right?
Putting it in context
In 2007, the median household income in the Bronx was $34,156. That $53M equals the annual income
of 1,531 people living in the Bronx. Bet they wouldn't mind if NY government officials tried to get some
of that back and give it to them, huh?13
A few nuggets from a recent NY Comptroller Report
‐ NY spent almost $200,000 in taxi fare for one woman to go see her kid in a long‐term care facility. That's 300 bucks a day round trip. ‐$53M was blown because of duplicate member IDs for 26,000 members ‐$20M was lost because someone input the wrong payment rate into the claims system

16
Gettin’ High on the Taxpayer Dime
As part of the American Recovery
and Reinvestment Act of 2009
(ARRA), the Medicaid program will
receive about $87 billion in federal
assistance due to a greater federal
share of Medicaid spending.
However, with an increase in
federal aid to state Medicaid
programs, fraud and abuse of the
system is likely to increase due to
loopholes exploited by beneficiaries, providers, criminals and pharmacies. An area of great concern for
the Centers for Medicare and Medicaid Services (CMS) focuses on the fraudulent and abusive purchases
of controlled substances by tens of thousands of Medicaid beneficiaries and providers.
A recent report by the Government Accountability Office (GAO) discovered about 65,000 Medicaid
beneficiaries from five selected states (California, Illinois, New York, North Carolina and Texas) obtained
the same type of controlled substance from six or more different medical providers during 2006 and
2007. Prescription drug payments to these particular states accounted for 40 percent of all Medicaid
prescription drug payments in 2006 and 2007. GAO determined that these beneficiaries were employing
techniques such as doctor shopping, falsifying Medicaid enrollment using the identity of dead
individual(s) and attributing prescriptions to dead doctors by pharmacies barred from receiving federal
funds, to obtain excessive amounts of controlled substances.
Investigations by GAO also uncovered other issues, such as doctors over prescribing medication and
writing controlled substance prescriptions without having required DEA authorization. Such
activities have caused the Medicaid system to overpay about $63 million. The $63
million in overpayments, however, does not include the additional cost to other related medical services
You Just Can't Get Ahead These Days- Must Be the Tough
Economy, Right?
-$53,000,000
$53,000,000
Waste due to duplicate IDs that NY Medicaid agency said was notworth recoveringAnnual Income for 1,551 Bronx Residents

17
and personnel, such as doctor and emergency room visits, that precede the distribution of these
prescription drugs.14
In some instances, beneficiaries used the aforementioned activities to either support their own
addiction or profit from the illegal sale of these drugs on the street. The most frequently abused
controlled substances by Medicaid beneficiaries were: narcotic painkillers (e.g. Lortab, Vicodin,
OxyContin and Percocet), non‐narcotic stimulants (e.g. Adderall and Ritalin) and non‐narcotic sedatives
(Lunesta, Ambien). Most of these drugs are categorized as Schedule II or higher and have a potential for
abuse and physical dependence. With an estimated 20 percent of the U.S. population having used
prescription drugs for non‐medical purposes, the demand
for prescription drugs is steadily rising. This new market as
well as the potential profits will help spur an increase in
fraud and abuse cases for CMS. Unfortunately, states and
CMS have yet to standardize criteria to prevent fraud and
abuse of the system.
Although the Controlled Substance Act of 1970 requires
that any person who manufactures, distributes, imports,
exports or conducts research with controlled substance
must register with the DEA, it does not require pharmacies
to report dispensing information at the patient level. This
loophole makes it difficult to catch and prosecute abusers
of the system immediately. Failure points in the national
and state systems include:
1. Medicaid officials (in the five selected states) were not following federal regulations by checking both federal debarment (EPLS) and HHS OIG lists to determine if an individual or entity was barred from federal contracts and/or excluded from Medicare and Medicaid programs
2. States are not required to purchase the DEA’s registrant database
3. State offices do not periodically compare Medicaid beneficiary database to death records
4. No uniformity in the application process into the Medicaid program. Duplicate enrollment is likely to occur, which in turn, makes fraud more difficult to identify.15
The Empire STRIKES Back
The results of the birth of the Medicare STRIKE force are in. Although the program only recently begun, OIG reports that the STRIKE force has lead to charges against 138 people, 44 convictions and $40.7M in identified funds that could be recovered (see our Summer 2009 issue for background on the STRIKE force, a special team used to target Medicare fraudsters). SOURCE: OIG Releases Semi‐Annual Report to Congress.'Medicare Update. Dec 3, 2009 http://medicareupdate.typepad.com/medicare_update/2009/12/oigsemiannualreport.html?utm_source=feedburner&utm_medium=feed&utm_campaign=Feed%3A+MedicareUpdate+%28Medicare+Update%29&utm_content=Google+Reader

18
Job Listings Hey‐ We know it’s tough out there. Here’s
a few Medicaid‐specific opportunities.
Join our LinkedIn group for more contact info on job posters.
Position / Description Contact Info
Healthcare Analytic Consultant Dan Lefeld [email protected]
Medicaid Guru needed! (Northeast) Medicaid Payer Relations Specialist Have you managed Medicaid payer relations for a clinical lab? If so, we need to talk!
Mamie Woods [email protected]
Lead Medicaid Program Analyst
Lou Boozer [email protected]
Sr. Account Executive (Managed Care) To view details and apply referencing req #1587, visit our web site at www.apshealthcare.com
Jason Foss
PBM Project Manager for a >3 yrs long term State Healthcare(PBM) assignment(Boston, MA)
Srinivasa Reddy [email protected] 636‐442‐1000(Ext 225)
"Medicaid Programmer Analyst" for one of the long term State Healthcare(MMIS) Project(Raleigh, NC)
Srinivasa Reddy [email protected] 636‐442‐1000(Ext 225)
"Medicaid Programmer Analyst with Provider Exp" for one of the long term State Healthcare(MMIS) Project(Raleigh, NC)
Srinivasa Reddy [email protected] 636‐442‐1000(Ext 225)
“Project Lead” AND “Team Lead/Tech Lead” positions for a State Healthcare(MMIS) project(Jefferson City, MO)
Srinivasa Reddy [email protected] 636‐442‐1000(Ext 225)
MANAGED CARE EXECUTIVES ‐ SC, MS, GA, MA
Pamela Ratz DeVille [email protected]
Vice President of Operations
Peter Blau, Healthcare Executive Search
Organizational Change Management Leader
Steve Kinnear 727‐446‐8494 [email protected]
Software Quality Assurance Analyst / Tester ‐ State Healthcare Project.
Kiran V 636‐ 489‐0157 EXT ‐‐ 219 Fax : 314‐754‐9839 [email protected]
Mainframe Programmer Analyst ‐ State Project ‐ Long‐term
Kiran V 636‐ 489‐0157 EXT ‐‐ 219 Fax : 314‐754‐9839 [email protected]
MICROFOCUS COBOL Programmer Analyst – State HealthCare Project Kiran V

19
Position / Description Contact Info 636‐ 489‐0157 EXT ‐‐ 219
Fax : 314‐754‐9839 [email protected]
Boston–Looking for a Consultant familiar with Medicare/Medicaid Cost Principals,cost allocation methodologies, knowledge of the federal Medicaid program and other health and human services programs.
Matt McLaughlin [email protected]
Director Public Sector Claims ‐ New Mexico Peter Peterson Executive Recruitment Strategist at UnitedHealth Group
Contract Operations and Specialty Health Plan Specialist ‐ Medicaid Division Colorado Department of Health Care Policy & Financing
Jim Vogel Program Performance ‐ Colorado Medicaid
Exciting Facets Configuration Analyst / Facets Business Analyst/Facets PM and Facets Architects
Michael Brown [email protected]
Physical Managed Care Contracts Specialist ‐ Medicaid Division Colorado Department of Health Care Policy & Financing
Jim Vogel Program Performance ‐ Colorado Medicaid

20
REFERENCES
1 'Liberal Senators Press for Expansion of Medicare.'NYT. OBERT PEAR and DAVID M. HERSZENHORN. December 7, 2009 ; Relationship of Primary Care Physicians’ Patient Caseload with Measurement of Quality and Cost Performance. JAMA.December 15, 2009 http://www.commonwealthfund.org/Content/Publications/In‐the‐Literature/2009/Dec/Relationship‐of‐Primary‐Care‐Physicians‐Patient‐Caseload‐with‐Measurement‐of‐Quality.aspx?utm_source=feedburner&utm_medium=feed&utm_campaign=Feed%3A+TheCommonwealthFund+%28The+Commonwealth+Fund%29&utm_content=Google+Reader 2"CMS AND ONC ISSUE REGULATIONS PROPOSING A DEFINITION OF MEANINGFUL USE AND SETTING STANDARDS FOR
ELECTRONIC HEALTH RECORD." Cms.hhs.gov. CMS, 30 Dec. 2009. Web. 29 Jan. 2009. 3 "CMS Information Related to the Economic Recovery Act of 2009." Health Information Technology. CMS, 15 Jan. 2010. Web.
30 Jan. 2010. <cms.hhs.gov/Recovery>. 4"CMS PROPOSES REQUIREMENTS FOR THE ELECTRONIC HEALTH RECORDS (EHR) MEDICAID INCENTIVE PAYMENT PROGRAM."
Details for: CMS PROPOSES REQUIREMENTS FOR THE ELECTRONIC HEALTH RECORDS (EHR) MEDICAID INCENTIVE PAYMENT
PROGRAM. CMS, 30 Dec. 2009. Web. 28 Jan. 2010. <http://www.cms.hhs.gov/apps/media/press/factsheet>. 5"Medicare and Medicaid Programs; Electronic Health Record Incentive Program; Proposed Rule." Federal Proposed Rules.
Regulations.gov, 13 Jan. 2010. Web. 29 Jan.
2010.<http://http://www.regulations.gov/search/Regs/home.html#documentDetail?R=0900006480a7c4a8>. 6 "States With Expanded Health Coverage Fight Bill." KATE ZERNIKE.December 26, 2009 http://www.nytimes.com/2009/12/27/health/policy/27states.html?pagewanted=2&_r=1&partner=rssnyt&emc=rss 7http://www.californiahealthline.org/articles/2009/10/13/california‐could‐incur‐high‐costs‐from‐plans‐to‐expand‐
medicaid.aspx; http://www.ahip.org/content/default.aspx?docid=27090;
http://www.google.com/hostednews/ap/article/ALeqM5gm81TTE7a0EUL9JlzVML1dnH2N2gD9BL9MB80 8Bowen Garrett, John Holahan, Lan Doan andIrene Headen. “The Cost of Failure to Enact Health Reform: Implications
forStates.” Robert Wood Johnson Foundation and Urban Institute, September 2009. 9"American Recovery and Reinvestment Act(ARRA): Medicaid and Healthcare Provisions.” Medicaid Spending and
Budgets.Kaiser Family Foundation, Oct. 2009. Web. 1 Feb. 2010. <kff.org>. 10Holahan, John. "Alternatives for Financing Medicaid Expansions in Health Reform." Medicaid/CHIP. Kaiser Family Foundation,
11 Dec. 2009. Web. 1 Feb. 2010. <kff.org>. 11"Dual Eligibles: Medicaid’s Role forLow‐Income Medicare Beneficiaries." Resources on Dual Eligibles and Issues Related to
Their Transition to the New Medicare Drug Benefit. Kaiser Family Foundation, Aug. 2009. Web. 2 Feb. 2010. <kff.org>. 12 'Poor Children Likelier to Get Antipsychotics'. DUFF WILSON December 11, 2009. NYT 13 'Audit Says State Wasted $92 Million on Medicaid,'NYT. December 22, 2009 14Fraud and Abuse Related to Controlled Substances Identified in Selected States. Government Accountability Office.
Congressional Request, Sept. 2009. Web. 16 Jan.2010.
www.smpresource.org/.../HealthCareFraud/Medicaid/GAO_Medicaid_controlled_substances.pdf‐; Kiely, Kathy. "GAO report:
Millions in fraud, drug abuse clogs Medicaid." Usatoday.com. USA TODAY, 29 Sept. 2009. Web.17 Jan. 2010.
<http://www.usatoday.com/news/health/2009‐09‐29‐Medicaid‐drug‐abuse‐fraud‐Michael‐Jackson_N.htm>.

21
15 "In U.S., Prescription Drug Abuse Is Growing." MedlinePlus. Ed. Wilson M. Compton. National Institutes of Health, 30 Dec.
2009.Web. 15 Jan. 2010; "Medicaid Fraud and Detection." Detection and Reporting Fraud. U.S. Department of Health and
Human Services, 5 Aug. 2009.Web. 18 Jan. 2010; "Prescription Drug Abuse." Medline Plus. National Institutes of Health, 31 Dec.
2009. Web. 18 Jan. 2010.