Fatty Acid Catabolism Caloric Value of Fats and Carbohydrates

Specialty Oils and Fats in Food and Nutrition. http://dx.doi.org/10.1016/B978-1-78242-376-8.00012-0© 2015 Elsevier Ltd. All rights reserved.
12Infant formulaR.P. Happe, L. GambelliIOI Loders Croklaan, Wormerveer, The Netherlands
… a little child, born yesterday,a thing on mother's milk and kisses fed…
Homer, Hymn to Hermes, 1:406.
Abbreviations
AA arachidonic acid (C20:4 n-6)α-LA alpha-linolenic acid (C18:3 n-3)CLA conjugated linoleic acidCCP critical control pointCFR code of federal regulationCVD cardiovascular diseaseDHA docosahexaenoic acid (C22:6 n-3)ESPGHAN European Society of Paediatric Gastroenterology, Hepatology and NutritionEFSA European Food and Safety AuthorityEPA eicosapentaenoic acid (C20:5 n-3)FAC fatty acid compositionFAME fatty acid methyl esters, referring to the most common analytical method to
measure the FACFDA Food and Drug AdministrationFFDCA Federal Food, Drug, and Cosmetic ActFOF follow-on formulaFOS fructo-oligosaccharidesGLA gamma-linolenic acid (C18:3 n-6)GMP good manufacturing practiceGOS galacto-oligosaccharidesGUM growing-up milkHMF human milk fatIF infant formulaISSFAL International Society for the Study of Fatty Acids and LipidsLA linoleic acid (C18:2 n-3)LCT long-chain triglycerideLC-PUFA long-chain polyunsaturated fatty acidMCFA medium-chain fatty acidsMCT mid-chain triglycerideMFGM milk fat globule membraneO oleic acid (C18:1 cis)OPO 1,3-dioleoyl-2-palmitoyl triglycerideP palmitic acid (C16:0)PL phospholipidsn-# stereospecific numbering (i.e., sn-2 refers to the fatty acid esterified to a
glycerol molecule in the 2nd—middle position)

286 Specialty Oils and Fats in Food and Nutrition
WHO World Health OrganizationWIC the special supplemental nutritional program for Women, Infants, and Children
12.1 Introduction
“Breast milk is the best” is written on packages of infant formula almost around the entire globe. And this is not only because legal authorities obligate producers to display this clause on the packaging. Breast milk is the only food naturally “ designed” for babies. It is generally recognized to allow the best growth and devel-opment of young infants, the least dietary-related problems in their early life, and less dietary-related issues such as cardiovascular disease (CVD) and metabolic syndrome later in life. Breast milk contains approximately 3–5% of lipids, 98% of which are triacylglycerols (fats and oils), and they comprise an essential part of young infants’ diet. The key benefits that are provided to the baby by human milk fat (HMF) relate to
1. Energy: almost 50% of the energy required by the fast-growing young infant originates from fat.
2. Physical protection: a layer of stored body fat protects the infant against internal injuries while it starts to explore the world and it acts as an insulant to maintain body heat.
3. Development: HMF provides essential fatty acids required for healthy development of the brain function and visual development, it helps develop and support the immune system, and is an essential component of body tissues and many organs. Furthermore, its hydrophobic nature allows the absorption of fat-soluble vitamins (A, D, E, and K), and therefore HMF is a well-matched vehicle by which vitamins are provided to the infant.
From the early twentieth century onward, infant formula (IF) has become more and more a serious alternative to breast milk for mothers who are not able to breastfeed their baby, or for personal reasons decide to rely on an alternative. The discovery and commercial introduction of infant formula initially was of great help mainly in overcoming the high mortality rates faced until the nineteenth century among infants who could not be breastfed. More than a century of investigations, developments, and supporting (clinical) trials made infant formula evolve into what is nowadays a safe and nutritionally sound food for newborns. During the development of infant formula, breast milk is commonly considered as the reference (or “gold standard”). The goal of the vast majority of IF producers is to mimic the composition and/or to match the functionality of breast milk as closely as possible.
This chapter provides an overview of the most relevant topics related to infant formula, strongly biased to the fat phase. First, an overview of the history is presented: this section gives insights into the discovery of infant formula in the nineteenth century, the main developments during the course of the twentieth century, and the present situ-ation concerning today’s formulas, the global infant formula market, and the main pro-ducers. Subsequently, a brief is handed about the composition of the fat phase, available sources for compounding the fat phase, and legislative requirements and further drivers that determine the selection and combination of fat sources. The chapter then discusses nutritional aspects of infant nutrition, focusing on essential components present in the fat phase (e.g., long-chain fatty acids). The last section guides the reader through the most

Infant formula 287
common processing routes applied for the production of infant formulas. Finally, a short commentary on potential future trends is given. This chapter is intended for readers new to the field, by presenting a broad general overview, as well as to experts, by providing focused information condensed down in schematic representations and tables.
12.2 History of infant formula: Past to present
Papers on the history of infant feeding often start in the late nineteenth century, logically as the invention and the introduction of the first commercial infant formula by Justus von Liebig materialized in that period. In reality, the history goes back to ancient times. Already in 2000 BC, alongside breastfeeding, milk from various mammals (cows, goats, pigs, horses, and camels) was fed to babies. Before the invention of infant formula, there were basically two options: wet nursing (i.e., a baby being fed by a woman other than its mother) or alternative feeding based on mammals’ milk, predigested foods, and wheat-containing porridges (dry nursing). Wet nursing was by far the safest option of the two. Where breast milk was not accessible to the newborn, survival rates neared 0%.
Major breakthroughs in the nineteenth century paved the way for the development of safe and nutritionally sound infant formula and germ-free feeding bottles. The rub-ber teat was invented in 1845. This was the first key breakthrough in feeding devices and significantly reduced health issues caused by microbial contamination of feed-ing bottles. In 1865, the first commercial infant formula was developed. This chief advancement was the basic foundation of the present-day formula for newborns. Nowadays, access to breastfeeding no longer implies a matter of life and death.
The history and evolution of infant formula from ancient history are condensed down in the time line shown in Figure 12.1. The following paragraphs will focus on the pe-riod from the nineteenth century, the era in which infant formula was invented and first marketed, through the present. For the period from 2000 BC to the mid-nineteenth cen-tury the reader is referred to the following valuable reviews: Wickes (1953a–e), Osborn (1979a,b), Schuman (2003), Stevens et al. (2009), and Castilho and Barros Filho (2010).
12.2.1 Era of major breakthroughs
Without any doubt, the nineteenth century can be referred to as the age of the major breakthroughs in infant artificial feeding, which changed the life of many mothers and their babies. In this era new standards were set for feeding devices, both for what con-cerns the substitute nipple and the bottle. Furthermore, control and reduction of micro-bial contamination of foods were drastically improved by the introduction of proper cold storage, pasteurization techniques, and methods to prepare condensed and powdered milk. The invention of infant formula completes the three main highlights of this era.
12.2.1.1 Feeding devices
In the early nineteenth century as many as one-third of all babies who could not be breastfed did not reach their first birthday because of dirty feeding bot-tles (Weinberg, 1993). In conjunction with contaminated milk supplies, very little

288 Specialty O
ils and Fats in Food and Nutrition
1840 1860 1880 1900 1920 1940 1960 1980 2000 2020
1959—Introductionof iron-fortified IF
1962—Whey proteinto caseinate ratioadjusted to becomecloser to that inhuman breast milk
1845—Rubber teat invented andpatented by ElijahPratt
1867—Firstcommercial infantformula launched byJustus von Liebig
1996—Firstcommercial productlaunched includingBetapol®: closer tomother’s milk
2004—First formulasincluding prebiotics,e.g, dietary fibersincluding GOS / FOS
2008—Betapol®
launched in China,igniting a swift growthin IF includingß-palmitate (OPO)
1915—Synthetic milkadapted (SMA), basedon vegetable oils,invented by HenryJohn Gerstenberger
1935—Protein contentwas reduced to bring itin line with that ofhuman milk
1984—Taurinefortification tosupport fatabsorption wasintroduced
1862—Louis Pasteurlaid the basis forpreservation of foodstuffs
1890—Pasteurizationbecame a routineoperation in milkproduction
Late 1990s—Nucleotides wereintroduced as fortifier
1971—Proteinhydrolysate formulaincluding MCT oil
1838—Comparativeanalyses of cow’sand human milk by J.Franz Simon revealedimportant differences
Early 2000s—IFproducts enrichedwith LC-PUFA’s
Figure 12.1 Key events in infant formula development from the industrial revolution until the present.Sources: References cited in the text.

Infant formula 289
knowledge of babys’ dietary needs, and overall lack of hygiene, microbial contam-ination of the feeding device was the main reason for horrendous mortality rates among these infants. Feeding utensils were often dirty because both the material (ceramic, wood, and pewter) and the shape of the device (pap boats, feeding cups, and bottles) hindered appropriate sanitation and bacteria could accumulate (Figure 12.2). Consequently, it is not surprising that the first key advancements in the survival rate of bottle-fed children related to the feeding devices’ shape and material. In 1843, Elijah Pratt invented and patented the India-rubber teat (Osborn, 1979b), which could substitute for rags, small pieces of linen cloths, and sponges or leather used as a teat or nipple.
The rubber teat was superior in mimicking the mother’s nipple in terms of sucking properties and milk flow. Moreover, it set the hygienic standard of the surrogate nipple at an unrivaled high level. An almost coinciding invention, the double-ended feeder of
Figure 12.2 Top panel: ceramic feeding bottle manufactured by Davenport & Co., based in Longport, Staffordshire, UK, in 1840. This type of feeding boat was used up to the second half of the nineteenth century.© Victoria and Albert Museum, London.

290 Specialty Oils and Fats in Food and Nutrition
Allen and Hanbury, improved the sanitary conditions of drinking devices further. Up to the mid-nineteenth century, wood, clay, metal, and animal-derived containers such as horns from ruminants were replaced by pewter or silver. Many of the feeding bottles were hard to clean simply because of their shape. The double-ended glass feeder with a teat on one end and a valve on the other end, not only enabled a constant flow of milk, but more importantly, made cleaning much easier. This feeding device, together with the rubber teat, laid the basis for the further evolution toward a safe surrogate breast (see Figure 12.2).
12.2.1.2 Getting control over microbial food contamination
Louis Pasteur (1822–1895) was not the first to hypothesize, yet the first to verify, the germ theory (Ullmann, 2007). In his experiments, he showed that microorganisms were responsible for food spoilage. Around 1860 he developed a method, called pas-teurization, in which heating was used to effectively kill the vast majority of bacteria and molds. Initially there was hesitation to apply heating for preservation purposes, as it was believed to negatively affect the nutritional benefits of foodstuffs. Not much later, it became a routine process step in food preservation and meant a major step for the safety of infant foods.
The procedure of making condensed milk was patented by Gail Borden in 1856 and provided another option to preserve (cow’s) milk. Milk was subjected to high tem-peratures in the presence of high sugar concentrations. The milk was thus sterilized and the sugar significantly decreased the water activity, resulting in prolonged shelf life and safer milk (Frantz, 1951). The fat content, however, was low and the feeding efficiency was inferior: newborns did not grow well if fed on condensed milk. A better option was provided by Myenberg’s invention for preparing evaporated milk in 1883 (Radbill, 1981). In contrast to condensed milk, it contained proper amounts of fat, sugar was omitted, and the heating process applied resulted in superior digestibility.
12.2.1.3 The first formula: Calculate to formulate
The nineteenth century is also the era in which major advancements were made in analytical sciences. Comparative chemical analyses of cow’s milk and human milk by Johann Franz Simon created the awareness that there were significant differences be-tween the two milks; for example, in protein and carbohydrate levels and type. It gave an explanation for the fact that, despite the improvements in the hygiene standards, babies fed with diluted animal milk products available at that time did not grow as well as breastfed babies.
It also was the start of striving for improved products for newborn infants. An illustrative example of that is Thomas Morgan Botch’s approach referred to as “ percentage feeding.” In the mid-nineteenth century, he tried to define the optimal mix of various constituents to make “fit” baby milk products. This was a complex pro-cess that became routine in the early twentieth century, for which he proposed a term that is still used today: infant formula (Schuman, 2003). American pediatrician Henry John Gerstenberg (1881–1954) recognized that in spite of all attempts up to then, absorption of formula remained suboptimal (Sidnell and Greenstreet, 2011). He then

Infant formula 291
combined several oils to match the fatty acid composition (FAC) of HMF, an approach that is currently common practice in infant formula manufacturing.
German chemist Justus von Liebig (1803–1873) is recognized as the first to have made infant formula available to the public (Radbill, 1981). The first generation infant formula products were launched in 1867 and known as “Liebig’s Perfect Infant Food” and “Liebig’s Soluble Food for Babies” (Levenstein, 1983). Initially, Von Liebig’s product was sold as a bovine milk-based liquid for $1 per can and shortly after in powdered form, which was to be mixed with diluted milk. The product in powder form was based on wheat and malt flour and potassium carbonate.
The success did not come without notice and initiated other producers to develop their own commercial formula. Henri Nestlé, a Swiss confectioner born Heinrich Nestle (1814–1890), launched Nestlé’s milk. It was sold for half the price of Liebig’s formula (i.e., approximately $0.5 per can of 1 lb = 454 g; Albanesi and Olivetti, 2009) and it was more convenient as it could be dissolved in water instead of cow’s milk. Nestlé was the first brand to become internationally known and sold. Therefore, Henri Nestlé is often seen as the godfather of infant formula. Innumerable imitations fol-lowed: the race to develop the best infant formula had begun.
12.2.2 The evolution of infant formula
Much research in infant nutrition followed to develop products for infants that were closer to human milk. Key innovations in the early twentieth century by pediatrician Dr. Henry John Gerstenberger (1881–1954) led to the so-called humanized products: SMA (synthetic milk adapted) was the first product without milk fat and based on vegetable oils (Fomon, 1993). Soon afterwards, Similac (similar to lactation) was in-troduced in the US market. SMA and Similac products are still being sold today by Nestlé (previously Wyeth Nutrition and Pfizer Nutrition) and Abbott Laboratories, respectively. The products are characterized in matching the protein:carbohydrate:fat ratio of breast milk much closer than bovine milk does.
An array of inventions followed and infant formula transformed into high-value products with great nutritional value, mimicking human milk in a stepping-stone man-ner. In 1935, protein levels in infant formulas were reduced to compensate for earlier overestimations of protein levels in breast milk. Fortification of formula with iron followed in 1959. Shortly after, it was recognized that a significant difference existed in the whey:caseinate of breast milk as compared to formula. To achieve a closer match to breast milk, adjustments were made as of 1962 and formula became whey protein-based. In 1984, fortification of infant formula with taurine, a conditionally essential amino acid (Chesney et al., 1998) was established. Before the arrival of the new millennium, formula started being supplemented with long-chain polyunsaturated fatty acids (LC-PUFAs), that is, docosahexaenoic acid (DHA), eicosapentaenoic acid (EPA), and/or arachidonic acid (AA), and these have become obligatory constituents according to different legislation.
Matching of the fatty acid profile was already common practice when it was also recognized that the position of fatty acids on the triglyceride was of importance (Freeman et al., 1965; Tomarelli et al., 1968; Filer et al., 1969). It was shown that

292 Specialty Oils and Fats in Food and Nutrition
HMF was highly enriched in palmitic acid in the middle position of the triglyceride (sn-2 position), whereas in vegetable oils the sn-2 palmitic was low (<10%). It was then understood that the absorption of breast milk was substantially better because of the high sn-2 palmitate. This discovery led to a significant innovation for infant formula in the twentieth century.
In 1986, IOI Loders Croklaan was the first to develop a product to mimic the unique fat composition and structure of HMF. A position-specific enzymatic inter-esterification process (sn-1,3-specific lipase) allows the production of a vegetable oil blend matching breast milk not only on fatty acid profile very closely but also on positional distribution thereof (i.e., high sn-2 palmitic acid). The product, Betapol®, has been commercially used in infant formulas globally since 1995; following several conclusive studies that proved its health benefits to newborn babies. Details will be elaborated on further in Section 12.4.
12.2.3 Today’s formulas
12.2.3.1 Product types and stages
Today’s infant formula is a multifaceted mixture of some 30 to over 50 components and hundreds, if not thousands of different recipes exist worldwide. It is among the most complex foods around and often considered to be an interface between food and pharma. However, the basic composition of infant formula products is the same: a straightforward combination of five constituents: fat, protein, carbohydrates, vitamins, and minerals.
The fat phase of formulas generally contains blends of oils and fats derived from a wide range of vegetable sources as well as from animal sources (i.e., goats and bovine milk fat). In a few cases, for instance in Japan, lard is still being used in formula. Lard has the advantage of containing high sn-2 C16:0; however, it has been banned by most IF-producing companies because of safety, image, and labeling issues. More details on oils and fats applied in present-day formulas are presented in Section 12.3. The diversity of products offered via supermarkets and pharmacies is very extensive (Figure 12.3).
Infant food is segmented into stages, from 1 up to 4 or 5. Stage 1 food targets newborns from birth up to 6 months of age, and the products are referred to as infant formula (IF). The regulation on infant formula is very strict and advertising is prohibited. Stage 2, or follow-on formula (FOF), is intended to be used for babies from 6 up to 12 months. Often, similar legislation as for stage 1 formula is in place. The main difference between stage 1 and stage 2 formulas is that stage 2 formulas are somewhat less energy dense because babies start eating other foods (fruits, vegetables, potatoes, bread, etc.). Stages 3–5 products target toddlers and young children from 1 to 3 years of age, 3–6 years of age, and older than 6 years of age, respectively. The main product category for the higher stages is growing-up milk (GUM). Because the diet is increasingly becoming more diverse, products re-lated to stages 3–5 encompass less strict regulation for what concerns both infant food legislation and advertising. This chapter will focus on IF and FOF products (stages 1 and 2).

Infant formula 293
12.2.3.2 The world market and main players
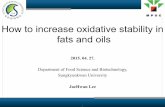
The total world market for infant food is valued at over US$50 million (Renfrew, 2014), approximately 70% of which relates to infant formula. This highly consoli-dated market is dominated by five multinational companies, who account for almost two-thirds of total infant formula business: Nestlé, Danone, Mead Johnson, Abbott, and Heinz (Figure 12.4). In the vast majority of the geographical areas the market is dominated by these five producers. The Chinese market situation, however, appears to be different from all others (Coriolis Research, 2014).
North America and Europe are considered to have an equal-sized market, and combined they account for 33% of the world’s sales of infant formula. The North American market is characterized as oligopolistic, that is, Abbott and Mead Johnson together cover 80% of the infant formula demand. One-third of all products are offered via subsidiary governmental programs, such as WIC (the special supplemental nutri-tional program for Women, Infants, and Children). In Europe, the main players are Nestlé and Danone, but a larger number of players are active and grasping a share. It is a more segmented market than North America, yet a mature one with room for growth expected only in follow-on and GUM.
Figure 12.3 Supermarkets and pharmacies today offer a wide range of IF products; various brands, different stages, and specialty products for low-birth weight preterm infants and term babies suffering from, for example, allergies, lactose intolerance, or congestions and cramps.

294 Specialty Oils and Fats in Food and Nutrition
By far the largest retail value is found in the Asian Pacific region, with around 53%. China is by far the largest single market and accounts for around 30% of the global market. What distinguishes China from the rest of the world is a highly fragmented market, dominated by a large number of players. The above-mentioned top-5 global players, complemented with FrieslandCampina, possessed no more than 40% of the Chinese market in 2013 (Coriolis Research, 2014). The major local producers include Beingmate, Biostime, Mengiu, Yili, and Synutra (approximately 3–10% market share each) and the total number of players is well over a 100. Beingmate is equal in size to the fifth largest multinational player, Heinz, both having a ~3% share of the global IF market. Governmental actions in China are aimed at further strengthening the quality and safety of infant foods (Askew, 2013; Astley, 2014). Measures include decreasing the number of manufacturers permitted to produce infant formula.
Volume-wise the global infant milk market is estimated at ~2.3 million metric tons. Assuming an average fat content of 22% on and end product basis, the global volume of fats and oils for infant milks approaches 500,000 metric tons. A vast array of oils and fats are being used in infant product manufacturing and will be elaborated in detail in Section 12.3. Oils and fats suppliers are an integral part of the infant formula value chain. Logically, their products have to meet the highest quality standards to align with the infant formula producers’ demands and to comply with applicable legislation. Most infant formula producers purchase mixtures of oils and fats to readily use them as a
0
5
Nestle
Danon
e
Mea
d Jo
hnso
n
Abbot
t
Heinz
Friesla
ndCam
pina
HIPP
Hero
Hain C
elesti
al
Mor
inaga
Meij
i
Chines
e loc
al pla
yers
10
15
20
25Multinational manufacturers
Regional playersMajor chinese manufacturers
Sha
re o
f the
glo
bal m
arke
t for
infa
ntnu
triti
on (
%)
Figure 12.4 Global market of IF and baby food based on indicative value share per manufacturer (in %); only major players are included. Of the global baby food category, approximately 70% is IF.Source: Coriolis Research (2014).

Infant formula 295
complete fat phase for their products. Only a handful of producers possess in-house oil blending facilities enabling the application of single oils in their daily operation.
12.3 Composition of the fat phase of infant formula
There exists no such thing as a generic recipe for the fat phase of infant formula prod-ucts. However, the FAC as found in human breast milk fat often serves as a template on which to base infant formulas. Many studies elaborate in detail on this general quest for the best possible IF products; for example, Koletzko et al. (1992), Goedhart and Bindels (1994), Gurr (1997), Forsyth (1998), Jensen (2001), Koo et al. (2006), and Long et al. (2013). In this section, it will be explained that other routes are also chosen and additional drivers come into play when defining the composition of an IF fat phase.
12.3.1 Drivers determining the fat phase of infant formula: Nature leads the way?
As indicated above, mimicking mother’s milk is still the ultimate goal for many infant formula manufacturers. This challenge starts with defining which HMF composition is to be used as a model to copy. Hence, breast milk is not of constant composition; variation is observed in the composition of the fat. First of all, during lactation changes are seen in the fatty acid profile when comparing the milk obtained just after birth (colostrum), transitional milk, and mature milk (López-López et al., 2002). Moreover, variations are seen between mothers, among others originating from differences in the diet (Jensen, 1999). For instance, the linoleic acid (C18:2; LA) content is substan-tially higher in breast milk of mothers in Mexico and Chile, because of the traditional high consumption of maize-based products. Exceptionally high lauric and myristic acid levels (C12:0 and C14:0) are observed in milk from mothers in the Philippines (Yuhas et al., 2006), possibly because of a diet limited in total fat. Such a diet results in increased endogenous mammary gland synthesis of fatty acids, which in this tissue terminates at C14:0. LC-PUFAs in breast milk find their origin mainly in fish prod-ucts; this is reflected in the high DHA levels observed in countries recognized by their traditional high consumption of marine products (e.g., Japan) (Yuhas et al., 2006). Table 12.1 presents the average fatty acid profile observed in breast milk from mothers on a Western or a non-Western diet.
Hence, the choice for manufacturers for the design of a fatty acid profile is not straightforward. Important factors that are being consulted include the composi-tion of HMF in the country/region in which the product will be sold, and insights from the literature and (own) clinical trials. There is an increasing awareness that to mimic mother’s milk as closely as it is possible, matching the fatty acid profile is not sufficient. Addition of a specialty fat such as Betapol®, enriched in palmitic acid in the sn-2 position as in breast milk, provides a better match to HMF than the common palm olein-including products do, and it is recommended (Koo et al., 2006).

296 Specialty Oils and Fats in Food and Nutrition
A vivid example that the HMF composition does not always stand as a model for IF products is mid-chain triglyceride (MCT)-based products commonly sold in the United States. MCT-containing products often omit palm olein as a component; hence, the fatty acid profile is dissimilar to that of breast milk. Manufacturers of such prod-ucts argue that these products mimic mother’s milk in terms of functionality rather than by composition (see also Section 12.4.2).
Further reasons to select a certain combination of oils to obtain an IF fat phase are manifold. Local availability and quality of oils, their combined shelf life, cost, image, nutrition aspects, and cultural habits favoring oils from a certain origin, are among these reasons; for example, in the Western world, the requirement of alpha-linolenic acid (α-LA) is often met by the inclusion of low-erucic rapeseed oil (canola), whereas in China a preference exists to apply soybean oil for that purpose. The vast majority of formulas in China are based on fresh milk, partly because of its taste, and the fat phase is implicitly built up from milk-based fat in combination with vegetable oils; that is, the latter are a required addition in order to meet the legislative requirements on the FAC, which cannot be met with milk fat exclusively. Also, the addition of specialty oils such as AA and DHA or high sn-2 palmitate fats is used by manufacturers as a discriminator. Apart from the above-mentioned factors, ensuring that an IF product is in compliance with prevailing legislation is a must-have rather than a driver during the design of the fat phase.
FA Name Western mean range Non-Western mean range
C10:0 Capric 1.4 0.1–2.2 1.0 0.0–1.7C12:0 Lauric 5.7 2.0–11.8 6.1 1.6–12.2C14:0 Myristic 6.6 2.3–11.7 7.2 4.3–17.7C16:0 Palmitic 21.6 12.9–27.5 19.6 16.1–29.8C18:0 Stearic 6.0 3.5–10.7 5.9 5.0–11.0C18:1 Oleic 31.1 23.6–55.3 27.1 21.5–39.2C18:2 Linoleic (LA) 11.7 5.8–27.6 18.1 9.3–32.7C18:3 α-Linolenic (α-LA) 1.1 0.3–1.9 2.1 0.2–3.0C20:4 Arachidonic (ARA) 0.4 0.1–0.9 0.9 0.3–1.12C20:5 Eicosapentaenoic (EPA) 0.1 0.0–0.7 0.5 0.0–1.07C22:6 Docosahexaenoic (DHA) 0.5 0.0–1.0 0.9 0.0–2.7
sn-2 (fraction of C16:0 esterified in the sn-2 position)
59–88
Table 12.1 Fatty acid composition (in wt%) and relative sn-2 of palmitic acid (in %) as determined in human breast milk fat from mothers on a Western or non-Western diet
FAC data adapted from Jensen (1999); definition of “Western” and “non-Western” diet provided in this publication. sn-2 data adapted from Breckenridge et al. (1969), Jensen (1999), López-López et al. (2002), Straarup et al. (2006), and Haddad et al. (2012).

Infant formula 297
12.3.2 Most commonly used fats and oils
Most fat phases of IF products consist of a blend of three or more vegetable and/or mammal fats and oils. A practical example is a blend of palm olein, sunflower oil, palm kernel, and rapeseed oil, enabling a match with the FAC found in HMF. In this case, palm olein provides mainly palmitic, oleic acid, and some LA. If palm olein is replaced by a high sn-2 palmitate fat such as Betapol®, in addition to the FAC, the structure of the triglycerides that is highly desired in breast milk can also be mimicked. Sunflower oil is responsible for adding a large amount of LA in addition to oleic acid. Palm kernel oil, like coconut oil, is often referred to as a “lauric fat” because of its high content of lauric and myristic acid (C12:0 and C14:0, respectively). Addition of α-LA is a common legislative requirement and for that purpose rapeseed oil may be included. Soybean oil is an alternative source of α-LA and in a few cases linseed oil (or “flax-seed oil”), the richest known α-LA source with a content above 50%, is used. Small amounts of fish oil could be added; oil derived from cold-water fishes such as salmon, sardines, anchovy, and tuna form rich sources of EPA and DHA. Today, several marine microalgae (e.g., Schizochytrium sp. and Crypthecodinium cohnii) and soil fungi (e.g., Mortierella alpina) are used in large-scale production of single cell LC-PUFAs, being an alternative to fish oil in IF to meet requests for sustainable and vegetarian products. Table 12.2 presents the typical FACs of the most commonly used blend oils.
Database sources, as mentioned, can be consulted in order to calculate the ratio of blending the various oils and fats to meet the targeted FAC specifications. It is recom-mended, however, to use actual FACs of the available components (as measured by high-resolution FAME), in order to determine the optimal blend ratio.
12.3.3 Legislative aspects and guidelines
This section touches upon regulatory and expert advice on the IF and FOF, with focus on the fat phase and on Europe only. As legislation per country may differ, even within Europe, Table 12.3 presents an overview of the requirements for IF and FOF, as based on the current EC Directive 2006/141/EC.
The directive sets essential requirements for the composition of infant formula and FOF that are based on the opinion of the Scientific Committee on Food (SCF/CS/NUT/IF/65) and expert opinions from other bodies such as the European Society of Paediatric Gastroenterology, Hepatology and Nutrition (ESPGHAN; Koletzko et al., 2005), the International Society for the Study of Fatty Acids and Lipids (ISSFAL; 2008), and the Codex Alimentarius Commission (CODEX STAN 72-1981). The Codex Alimentarius Commission, as well as international expert opinions, guide reg-ulations not only in Europe but also in other countries.
In the United States, because infant formula is a food, the laws and regulations governing foods apply to infant formula. Nevertheless, additional regulatory require-ments have to be met, which can be found in Section 412 of the FFDCA (Federal Food, Drug, and Cosmetic Act) and in the FDA (Food and Drug Administration) 21 CFR Parts 106 and 107.

298 Specialty O
ils and Fats in Food and Nutrition
FA Name CoconutPalm kernel Palm
Palm olein (IV ~ 56)
Palm superolein (IV ~ 62) Sunflower
High-oleic sunflower
Rapeseed low-erucic Soybean Linseed
Fish oil anchovy
C6:0 Caproic nd–0.7 nd–0.6 C8:0 Caprylic 4.6–10.0 2.4–6.2 C10:0 Capric 5.0–8.0 2.6–5.0 C12:0 Lauric 45.1–53.2 45.0–55.0 nd–0.5 0.1–0.5 0.3 nd–0.1 nd–0.1 C14:0 Myristic 16.8–21.0 14.0–18.0 0.5–2.0 0.5–1.5 1.0 nd–0.2 nd–0.1 nd–0.2 9C16:0 Palmitic 7.5–10.2 6.5–10.0 39.3–47.5 38.0–43.5 35.4 5.0–7.6 2.6–5.0 3.6 8.0–13.5 6.0 17C18:0 Stearic 2.0–4.0 1.0–3.0 3.5–6.0 3.5–5.0 3.8 2.7–6.5 2.9–6.2 1.5 2.0–5.4 2.5 C18:1 Oleic 5.0–10.0 12.0–19.0 36.0–44.0 39.8–46.0 45.1 14.0–39.4 75.0–90.7 61.6 17.0–30.0 19.0 10C18:2 Linoleic
(LA)1.0–2.5 1.0–3.5 9.0–12.0 10.0–13.5 13.4 48.3–74.0 2.1–17.0 21.7 48.0–59.0 24.1
C18:3 α-Linolenic (α-LA)
nd–0.2 nd–0.2 nd–0.5 nd–0.6 0.3 nd–0.3 nd–0.3 9.6 4.5–11.0 47.4
C20:0 Arachidic nd–0.2 nd–0.2 nd–1.0 nd–0.6 0.3 0.1–0.5 0.5–0.5 0.1–0.6 C20:1 Paullinic nd–0.2 nd–0.2 nd–0.4 nd–0.4 nd–0.3 0.1–0.5 1.4 nd–0.5 1C20:5 Eicos-
apentaenoic (EPA)
22
C22:1 Erucic nd–0.1 nd–0.3 0.2 nd–0.3 1C22:5 Docos-
apentaenoic 2
C22:6 Docos-ahexaenoic (DHA)
9
Table 12.2 Indicative fatty acid composition (range or typical) of fats and oils commonly used in infant formulas (in wt%)
nd, not detected. Values in bold indicate the FAs for which the respective oil is primarily added to the IFs fat phase.Adapted from Gunstone and Harwood (2007).

Infant formula
299
Min IF max Units Min FOF max Units
Compulsory composition
Total fat 1.05 1.4 g/100 kJ 0.96 1.4 g/100 kJTrans fatty acids 3 % 3 %Lauric + myristic acid C12:0;
C14:0 20 % 20 %
Linoleic acid (LA) C18:2 n-6 70 285 mg/100 kJ 70 285 mg/100 kJα-Linolenic acid (α-LA) C18:3 n-3 12 mg/100 kJ 12 mg/100 kJRatio LA/ALA 5 15 5 15 Erucic acid C22:1 cis 1 % 1 %
Facultative additions
Total n-3 LC-PUFA’s 1 % 1 %Total n-6 LC-PUFA’s 2 % 2 %Arachidonic acid (AA) C20:4 n-6 1 % 1 %Eicosapentaenoic acid (EPA) C20:5 n-6 ≤DHA ≤DHA Docosahexaenoic acid (DHA) C22:6 n-3 ≤Total n-6
LC-PUFA’s≤Total n-6 LC-PUFA’s
Nutritional claim related to DHA
0.2 %
Phospholipids 2 g/L 2 g/L
Exclusions
Sesame seed oil Not allowed Not allowed Cotton seed oil Not allowed Not allowed
Table 12.3 Legislation on infant formula and follow-on formula in Europe: compositional requirements of the fat phase
% refers to percentage of total fat content.Source: EC Directive 2006/141/EC.

300 Specialty Oils and Fats in Food and Nutrition
In China, infant formula composition is regulated by the National Standards on Food Safety of PR China (GB 10765-2010), issued by the Ministry of Health of the People’s Republic of China in 2010 and implemented on April 1, 2011.
In the last 10 years, scientific and technological developments on the essential com-position of infant formulas have progressed, and in Europe there are increasing calls for a review of the legislation to reflect such developments. Negotiations are currently in place on the proposal for a Regulation of the European Parliament and the Council on foods intended for infants and young children and on food for special purposes. With the aim of capturing the most updated scientific information on nutrients for infants, the European Food and Safety Authority (EFSA) has recently published their updated scientific opinion on infant formula and FOF (EFSA, 2014a). Concerning the fat phase, their main conclusions embrace the view that cow’s and goat’s milk as well as several vegetable oils are suited for IF. As a precautionary measurement, DHA is now recommended as a required constituent (4.8–12 mg/100 kJ), whereas the addition of EPA and AA is safe yet not needed. The beneficial physiological effect of DHA for infants and children was also highlighted a few months later when the EFSA gave the green light for a claim linking DHA and infant brain development (EFSA, 2014b). In the EC directive (EC, 2006), LC-PUFAs including DHA may be added on a voluntary basis. Furthermore, the panel considers that specifying a range of the ratio LA/α-LA, as currently in place (EC, 2006), is not necessary in the presence of LC-PUFAs in the IF and FOF. The addition of phospholipids (PLs) or sources with palmitic acid pre-dominantly esterified in the middle position has also been judged as not essential, in view of the lack of convincing evidence.
12.4 Nutritional aspects
Human milk is uniquely suited to the human infant. Its nutritional composition pro-motes the healthy physical and intellectual development of the child and its com-plex array of lipids maximizes energy intake and calcium absorption (Innis, 2007a; Ballard and Morrow, 2013). Even though small variations in breast milk fatty acids composition occur due to factors such as genetics, mother’s diet, season, lactating stage, physiology, and even psychology, all human milks are characterized by the dominance of triglycerides (>98% of HMF), palmitic acid in the sn-2 position of the glycerol backbone (70% of palmitic acid), and unsaturated fatty acids in the sn-1 and -3 positions. Human milk also provides small quantities of omega-3 fatty acids (EPA and DHA), usually <1% of total fatty acids, and omega-6 fatty acids (LA and AA; Sahin et al., 2006; Brenna et al., 2007; López-López et al., 2002). Human milk from mothers of full term and of preterm infants also contains 10% and 15% MCTs, respectively (Bitman et al., 1983).
The remaining 2% of the lipids in human milk include PLs (0.8%), consisting mainly of phosphatidylethanolamine, phophatidylcholine, and sphingomyelin, a “sphingolipid” (each comprising approximately 30% of the total PLs); free sterols and sterol esters (0.5%), being mostly cholesterol; and, some mono- and diacylglycerols

Infant formula 301
and nonesterified fatty acids (Jensen, 1996). The major part of the PLs, among which are the sphingomyelins, is associated with the milk fat globule membrane (MFGM). The biological function of the polar lipids in MFGM is presently unknown; as is the function of cholesterol, which is present in HMF in higher levels than in IF products (see also Long et al., 2013). This chapter will focus mainly on the triglycerides.
12.4.1 Omega-3 and omega-6 fatty acids
Among the LC-PUFA, DHA has been the most intensively studied and for several reasons:
● DHA is present in relatively high concentrations in all neural tissue, particularly in the brain (up to 40% of fatty acids in some brain areas), and retina (comprising approximately 30–65% of the cell membrane fatty acids of the rods and cones) (Brenna and Carlson, 2014).
● The infant brain goes through extensive development from birth (~360 g) to 1 year of age (925 g), raising several questions on what the consequences might be if DHA is not provided in sufficient amounts (Innis, 2014; Agostoni, 2005; Martinez, 1992).
● Little evidence is available that the mammary gland can maintain a balance between the secretion of AA and DHA or other omega-3 and omega-6 fatty acids in human breast milk, making scientists and regulatory bodies active in finding the best nutritional guidance for gestating and lactating women and formula-fed infants (Innis, 2014).
Human brains accumulate DHA up to age 18, most aggressively from about half-way through gestation to about 2 years of age, during the “brain growth spurt” (Brenna and Carlson, 2014). The mean concentration of DHA in breast milk is 0.32 ± 0.22%, its variation being associated with maternal DHA stores and marine food consump-tion, consequently with the highest concentrations in coastal populations (Brenna et al., 2007) and the lowest in vegans (Sanders, 1999).
Research suggests that dietary DHA benefits an infant’s eye and brain development via several mechanisms. Several lines of evidence suggest that the concentration of DHA can alter the neuronal membrane fluidity and physical structure of neurons, is involved in the production of neurotransmitters affecting synaptic transmission and sub-strate binding to membrane receptors, and it may improve learning and memory and subsequent performance via its role in the development of pre- and postsynaptic proteins (Heaton et al., 2013). Although new well designed and conducted studies are being pub-lished and there is no doubt that DHA is critical in the developing brain, evidence from human randomized controlled trials addressing DHA intakes still do not demonstrate a clear and consistent benefit of DHA supplementation during pregnancy and/or lactation on term infants’ growth, neurodevelopment, and visual acuity (Campoy et al., 2012; Innis, 2014; Tijhuis et al., 2014). It is possible that DHA is not required in humans ap-propriately nourished with the correct LA and α-LA or that DHA may be critical, but for reasons other than those as yet addressed with human studies (Innis, 2007b). Whatever the reason is, it still remains that the evidence that DHA deficiency is detrimental to neu-rocognitive development is by now well established in animal models where impaired visual, motor, and cognitive deficits are observed (Heaton, 2013).

302 Specialty Oils and Fats in Food and Nutrition
Omega-6 fatty acids, LA, and AA, are also important nutritional components. Like DHA, AA plays an important role for infant growth and development; it is a key component of cell membranes and serves as a precursor to prostaglandins and leukotrienes formation (Figure 12.5). Studies in rats, monkeys, and humans have es-tablished a nutritional requirement for LA. The effect of dietary deficiency includes reduced growth and feed efficiency, reproductive failure, skin and hair changes, and liver pathology (Davis-Bruno and Tassinari, 2011). The mean concentration of AA in breast milk is 0.47 ± 0.13%, which indicates lower variability compared to that of DHA (Brenna et al., 2007).
Infant formulas with DHA and AA have gained great interest in the last 30 years, despite the lack of a final consensus on the need to supply DHA and AA to infants (Tijhuis et al., 2014). As the number of breastfeeding women is decreasing, provid-ing an adequate supply of LC-PUFA is more than ever believed to be important for infants during the first year after birth, and mother’s milk is viewed as the best point of reference when breastfeeding is not an option (Sahin et al., 2006). The level of DHA used in formula is based on the level of DHA typically found in human milk from the region of commercialization (Davis-Bruno and Tassinari, 2011). AA can be voluntarily added up to a maximum of 1% (Commission Directive 2006/141/EC).
An optimized ratio of LA:α-LA acids, precursors of AA and DHA, respectively, represents a less costly option to improve DHA and AA status in infants. Nevertheless, studies in modern humans and nonhuman primates show that modern infants consum-ing infant formulas that include only DHA and AA precursors have lower LC-PUFA levels than for those with a source of preformed DHA or AA (Brenna and Carlson, 2014). In fact humans have a limited “conversion” capacity (<1%), it being somewhat dependent on an individual’s genetic profile and sex, with conversion factors signifi-cantly greater in females than in males (Heaton et al., 2013).
Constituents of cellmembrane
Modulation of signaltransmission
Support optimal growth and development
Visualdevelopment
Cognitivedevelopment
Potential long-termbenefits
Low bloodpressure
Low allergyincidence
Improved lipidmetabolismand weight
DHA and AA
Figure 12.5 Potential effects and function of DHA and AA supplementation in infants.Adapted from Tai et al. (2013).

Infant formula 303
12.4.2 MCTs
MCTs are relatively soluble in water, and their molecular weight being lower than long-chain triglycerides (LCTs) facilitates digestion by lipase and intestinal absorp-tion even in the presence of low intraluminal bile salts and reduced levels of pancreatic lipase (Bach and Babayan, 1982).
Studies comparing fat adsorption with preterm formulas, with adding MCTs at different concentrations, found a nearly complete intestinal absorption of MCFAs (Jensen et al., 1986). The comparison between formulas with and without MCTs doc-uments an improvement in fat absorption in infants fed with MCTs (Spenser et al., 1992). Because MCTs, differently from LCTs, pass directly into the portal venous system without forming chylomicrons, a rapid production of energy for immediate use by organs and muscles is expected. It has also been reported that the mineral balance of preterm infants can be improved with the use of MCTs in formulas because MCTs reduce the formation of insoluble calcium and magnesium soaps and thereby increase their absorption (Sulkers et al., 1992). Nevertheless, in terms of fat absorption, gas-trointestinal tolerance or short-term growth of low-birth weight infants, the use of MCTs in formulas for premature infants has shown no advantage over that of LCTs (Klenoff-Brumberg and Genen, 2003). High MCFA has also shown to potentially lead to diarrhea and dicarboxylic aciduria (EFSA, 2014a).
12.4.3 Palmitic acid and the importance of its position on triglycerides
Palmitic acid is not an essential fatty acid as the infant is capable of de novo synthesis of palmitic acid via glucose. Still, in human breast milk triglycerides, palmitic acid is very abundant (20–25% of total milk fatty acids). Furthermore, the human mammary gland has evolved with unusual pathways for acylation of fatty acids into triglycerides for se-cretion in milk, with these pathways resulting in the preferential position of palmitic acid at the sn-2 position (70–75%), a different triglyceride structure observed in other human tissues and plasma, common dietary fats and oils (with the exception of lard) or in the fat blends used in the manufacture of infant formula (Bar-Yoseph, 2013; Bracco, 1994).
Studies over the last 2–3 decades have provided increasing evidence that this un-usual positioning of C16:0 in human milk triglycerides promotes the absorption of both C16:0 and calcium in term and preterm infants (Carnielli et al., 1995a,b, 1996; Lucas et al., 1997; Kennedy et al., 1999), with potential long-term benefits linked to bone mineralization and bone strength (Litmanovitz et al., 2013). Lipid absorption is essential for the energy requirements of the growing infant. The rate of lipid absorp-tion is influenced by both the type of fatty acid and the position of fatty acid on the triglyceride backbone.
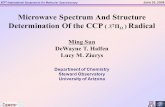
When triglycerides are consumed, the fatty acids bound in the sn-1 and -3 posi-tions are freed by digestive enzymes, leaving the fatty acid in the sn-2 position as a monoglyceride (Figure 12.6). Palmitic acid is favorably absorbed in the sn-2 position as a monoglyceride rather than as free fatty acid because it tends to form insoluble calcium soaps that cannot be absorbed in the small intestine and are thus excreted in

304 Specialty Oils and Fats in Food and Nutrition
the feces (Scott, 2010). The presence of fecal palmitic acid represents a needless loss of available dietary energy and calcium for the infant, especially preterm infants who, in view of their less-developed digestion system and lower weight compared to full-term infants, need to maximize feed efficiency. Furthermore, palmitic acid calcium soaps can accumulate in the feces, resulting in harder stools, which may lead to con-stipation, obstruction, and overall discomfort in the infants. Trials have indeed shown beneficial effects on stool softness and constipation (Carnielli et al. 1996; Kennedy et al. 1999; Bongers et al., 2007) and reduction in crying episodes (Bar-Yoseph et al., 2014; Litmanovitz et al., 2014) when infants were fed high β-palmitate IF. Despite the very promising results, clear benefits of β-palmitate as expressed as bone strength and bone mass have still to be shown (Tijhuis et al., 2014).
Palmitic acid in the sn-2 position has also been associated with intestinal develop-ment and health, as it has been shown to increase the number of the probiotic bacteria Bifidobacteria and Lactobacilli in the gut (Schmelzle et al., 2003; Yaron et al., 2013; Yao et al., 2014). Lactobacilli and Bifidobacteria have been associated with promotion of gut maturation and integrity, antagonism against pathogens, and immune modula-tion in infants (Kaplan et al., 2011). Finally, recent developments in OPO research have shown that palmitic acid in the sn-2 position might have beneficial effects beyond the well-known effects on calcium absorption and bone mineralization. In rats, it was shown that dietary high β-palmitate fat could modify the concentration and type of endocannabinoids and congeners being synthesized in tissues. These changes may
Fatty acids andcalcium from diet
Fatty acids andcalcium from diet
Fatty acidsreleased from sn-1and -3 position
Fatty acidsreleased from sn-1and -3 position
Unsaturated fattyacids at positionssn-2 are absorbed
Unsaturated fattyacids at positionssn-2 are absorbed
Calcium salts areformed
Calcium salts areexcreted
Palmitate at the sn-1 and -3 positions Palmitate at the sn-2 position (e.g. Betapol®)
Unsaturated fattyacids and calciumsalts are absorbed
Palmitic acid Unsaturated fatty acid Calcium
Figure 12.6 Lipid digestion and fatty acid and calcium absorption.

Infant formula 305
potentially favor brain function and fat distribution (subcutaneous rather than visceral) thus improving insulin sensitivity and preventing ectopic fat accumulation in children (Banni et al., 2014).
12.5 Infant formula processing
Meeting the high-quality standards compulsory to protect our precious infants and to comply with the strict legislation in place for infant formula, is a daily challenge for producers of infant foods. Moreover, parents want what is best and safe for their children, but the product also has to guarantee a long shelf life, have good appearance and acceptable dissolubility, and has to taste good. This sets high demands for the ingredients used, the manufacturing lines, packaging and storage, and quality control/assurance. It is, therefore, explicable that infant formula production is occasionally compared to pharmaceutical compounds manufacture. High quality standards with good manufacturing practice (GMP) and sanitary environments are by default in place. This section provides an insight into state-of-the-art IF manufacturing. Infant milk products for children up to 1 year (IF and FOF) basically come in two shapes; in dry powder or as a liquid.
12.5.1 Powdered products
The major part of infant formulas and FOFs comprise powdered products. Commonly sold in tins/cartons of a few 100 g up to >1 kg, the product is to be dissolved in (pres-terilized) lukewarm water prior to feeding. There are basically two processing routes to obtain powdered infant foods. The first and most used route uses an emulsion of the ingredient mix as input material to which spray drying is applied (liquid to powder). The other option is the so-called dry blending technique, in which prefabricated pow-dered ingredients are mixed (powder to powder). A hybrid of the two basic techniques is known as semiintegral spray drying: the majority of the components are spray dried and powdered ingredients are blended in subsequently.
12.5.1.1 Integral spray drying (liquid → powder)
The common basic steps in integral spray drying are outlined below; see also Figure 12.7. The starting point of GMP is the availability of a proper recipe and high-quality ingredients (Zink, 2003). A wet mixture is prepared by blending the liquid ingredients, according to the recipe, in a proper ratio, this being assured by using weighing devices and/or flow meters. The mixture may be preheated, after which powdered ingredients are added and dissolved/dispersed. An emulsion is pre-pared from this mixture by passing the mixture through a high-pressure homogenizer. Subsequently, the product is sterilized or pasteurized. In some cases, heat-sensitive ingredients (e.g., vitamins or PUFAs) are added after sterilization/pasteurization. The decontaminated product is thereafter used to manufacture the powder by means of spray drying. The process to obtain a dry powder from a liquid is typically a two-stage

306 Specialty Oils and Fats in Food and Nutrition
process. The first stage is the spray drying of the liquid in the drying chamber; the sec-ond step is the final drying/cooling of the powder in the external vibrating fluid bed.
The spray-drying stage is characterized by three fundamental steps: (1) atomization of a liquid resulting in the formation of small droplets, (2) evaporation of liquids by subjecting the droplets to a heated gas flow resulting in partially dried solids, and (3) separating the particles from the gas stream (Gohel, 2009; Zuidam and Shimoni, 2010; Singh and Dixit, 2014). A homogenized mixture is atomized into a hot air stream (ranging approximately 140–200 °C). The atomizer may be a pressured nozzle or a centrifugal disc (rotary atomizer). Exposure of the developing powder to high tem-peratures can be prevented by controlling the droplet size and air temperature and residence time in the drying tower. These are also the parameters that determine the powder size and distribution. At the outlet of the spray dryer the temperature is around 100 °C; the powder at that stage typically has a temperature of 45–80 °C. The moist powder thereafter enters the vibrating fluid bed and the powder is further dried and
…………………………….....................…………………………….....................
A
B
C
D
E
F
G
Liquidemulsion
Atomization
I. Drying stage:liquid evaporation
H
II. Drying stage III. Drying stage
Dry-powdered product
Powderseparation
IV. Drying stage
Figure 12.7 Schematic representation of a general process set-up for the manufacture of powdered infant formula (integral spray drying). Process hardware: (A) liquid emulsion buffer tank; (B) liquid feed inlet; (C) rotary atomizer or spray nozzle atomizer; (D) spray dryer; (E) fluid bed drier; (F) conveyer belt; (G) dried powder collector; and (H) sieve or rotary valve. After the dry-powdered product has been obtained, it will be conveyed to an aseptic packaging line for filling of cans or bulk packaging. Dotted lines: product stream. Solid lines: hot air inlet (thick lines) or cold air inlet (thin lines).

Infant formula 307
cooled in a step-wise manner down to ambient temperatures. The product is then sub-jected to a thorough and final quality check prior to release. Finally, the powder is canned in an aseptic packaging line. Preferably, the powdered product is packed un-der modified atmosphere such as nitrogen, to prevent the product from oxidizing and thereby extending the shelf life. A schematic representation of the drying process of liquid droplet to solid particles is depicted in Figure 12.8.
12.5.1.2 Semiintegral spray drying (liquid → powder + powder)
Basically, semiintegral spray drying relies on the same procedures described for inte-gral spray drying. The key difference is that after spray drying, additional powdered components are being mixed in with the powdered IF. This technique is especially applied for adding minor ingredients that are heat sensitive/susceptible to oxidation. Examples of such ingredients are LC-PUFAs and premixes containing vitamins, min-erals, and/or amino acids. Their stability is secured by mixing in as powder end-of-pipe; quality assurance is often what drives producers to use this way of manufacturing.
Nevertheless, this routing also offers profound economical advantages. Changing recipes for different formulas on a spray-drying tower is a laborious operation. It
Dro
plet
/par
ticle
tem
pera
ture
Drying time
Drying gastemperature
Boilingtemperature
Wet-bulbtemperature
A B
C
E
Dry particleWet particleWet droplet
D
12
3
4
5
6
Figure 12.8 Schematic representation of the droplet drying process over the different stages of drying. (A) Atomized droplet obtained at high temperature, which heats up rapidly to the wet-bulb temperature; (B) moisture evaporates gradually until a certain concentration of emulsion particles is reached, the moisture vapor pressure drops and moisture can no longer migrate in sufficient rates to the surface; (C) as the surface temperature rises further crust formation starts and moisture in the wet particle reaches boiling point; (D) the temperature will increase strongly after moisture has evaporated from the particle; and (E) the drying process terminates when the temperature of the particle becomes equal to that of the drying gas. Final dried particles come in different shaped, e.g., solid (1), hollow (2), blistered (3), inflated (4), buckling (5), or shattered (6).Adapted from Singh and Dixit (2014), Handscomb (2008), and references cited herein.

308 Specialty Oils and Fats in Food and Nutrition
often involves cleaning and intrinsically leads to production downtime. Minimizing the number of formulas and thereby simplifying the daily operation, is often a tar-get for manufacturers. Semiintegral spray drying can add positively to this endeavor. The use of a single recipe in the spray-drying step not only offers the opportunity to easily manufacture standard basic formulas but it also enables the cost-efficient making of line-extension products by adding specialty ingredients in a separate step. By this means, various specialty products can be prepared on demand by adding, for example, LC-PUFAs, nucleotides, and/or prebiotic dietary fibers, such as galacto- oligosaccharides (GOS) and fructo-oligosaccharides (FOS).
12.5.1.3 Dry powder blending (powder → powder)
The flexibility indicated in the previous section also applies for the dry powder blending operation, as will be explained below. Dry blending is used to manufacture 10–20% of the global demand for infant formula, mainly in the south of China. The basic principle of dry powder blending is straightforward: powdered ingredients (sin-gle components or premixed blends) are received from the suppliers and ingredients are blended according to the recipe and to meet the final specifications. A powder blend is obtained by extensive mixing in a (ribbon) blender, in which uniform distribu-tion of the components needs to be assured. The homogeneous powder is then passed through a sieve for the removal of powder aggregates. Finally, the powder blend is stored in intermediate packaging (e.g., totes or bag-in-boxes) or transferred directly to a can filling line (Zink, 2003). As previously described, packaging under modified atmosphere is preferable.
The advantages of dry blending over the spray-drying processes are obvious. Processing is economically attractive; that is, no investments are required for a spray-drying tower and less energy is consumed as no heating is applied. Furthermore, because water is not required, intervals between cleaning and maintenance stops are regularly longer than in factories employing spray drying. Also, there is more flexi-bility toward producing different recipes. In many cases, a so-called base powder is used that contains the basic ingredients and makes up 40–70% of the final product. The remaining part can be employed to diversify; for example, specialty products can be manufactured by the addition of nucleotides, LC-PUFAs, and/or dietary fibers. By adjusting the ratios of the ingredients in the remaining part, it also allows the prepara-tion of products for the different stages of formula (see also Section 12.2.3.1).
The downside of dry blending is the risk of contamination with pathogenic bac-teria. As there is no heat treatment in the dry blending operation, this risk is higher than for the earlier discussed processing routes. The main microbiological issues with powdered infant formulas are related to the presence of Enterobacter sakazakii and Salmonella enterica, which can cause serious infections and in a few cases even be fatal. Especially infants under 2 months of age and preterm babies are at higher risk. About 70 incidents related to E. sakazakii were reported between 1958 and 2006 (Drudy et al., 2006); the World Health Organization (WHO), however, assumes this to be an underestimation (WHO, 2007). Therefore, during the dry blending opera-tion several checks and measures are in place to control microbiological status. Small contaminations in one ingredient can lead to serious issues because this ingredient is

Infant formula 309
uniformly distributed over a large batch of product. Hence, suppliers of powdered in-gredients are held to meticulous processing procedures (e.g., including critical control points (CCPs) on the sterilization step) and strict specifications. Other disadvantages of dry blending are the lower mixing quality and the possibility of segregation during storage and transport, caused by possible differences in the density of the ingredients. Dry blended powders may, therefore, be less homogeneous and batch-to-batch varia-tion is more likely to occur.
12.5.2 Ready-to-drink liquid formula
Ready-to-drink/feed products (and liquid concentrates) represent a small minority of global volume of infant formulas. This type of product is often seen in relation to convenience for the parents, as only warming up is needed prior to feeding. Yet in particular, this is the format used widely for feeding preterm (born before 37 weeks gestational age) or low-birth weight infants (weighing less than 2500 g at birth) and for enteral medical nutrition or pediatric formulas. The logic for that originates from the applied processing route, resulting in products that are sterile by default. The basic principles of manufacture are comparable to integral spray drying, up to and including the sterilization step. After sterilization, the liquid product is aseptically packed in single-shot sachets. Manufacturers of ready-to-feed formulas include Danone, Mead Johnson, Abbott, and Vitaflo/Nestlé.
12.6 Future outlook
The near universal aim to develop infant formulas that match human breast milk as closely as possible is anticipated to remain at the forefront in the coming years. Important themes that both IF manufacturers and researchers will explore (further) include healthy growth, proper development of vital functions (e.g., cognitive func-tion and development of the immune system), optimal digestion and comfort for the baby, and metabolic imprinting. The latter is receiving increasing attention; it has been recognized that adequate maternal nutrition during pregnancy and the fatty acids in the infant diet play a key role in guiding the neural receptors that regulate energy homeostasis and expression of genes that control energy storage and oxidation. Early deviations in these pathways have the potential to lead to lasting adaptations, known as “metabolic programming,” which may contribute to increased risk of metabolic syndrome in later life (Innis, 2011; Patel and Srinivasan, 2002) with potential gener-ational effect on metabolic programming (Patel and Srinivasan, 2002). It is then clear why understanding of the importance of dietary fatty acids has grown beyond a simple source of energy to complex roles in regulating gene expression and cell and intra-cellular communication. As infancy is an extremely vulnerable period for metabolic programming, appropriate nutrition could help in reducing the risk of diseases later in life, in particular obesity, diabetes, hypertension, and CVDs. Pending the outcome of human clinical trials, infant nutrition may be developed that supports appropriate tuning of the young infant’s metabolism.

310 Specialty Oils and Fats in Food and Nutrition
The fat composition of HMF and translating that into IF is a common practice that has been employed for over a century. Until now, the focus has been mainly on the triglyceride part (98% of HMF) and the composition of the major fatty acids. It is fore-seen that minor lipids present in HMF, particularly cholesterol, sphingolipids, PLs, and minor fatty acids such as conjugated linoleic acid (CLA) and gamma-linolenic acid (GLA), will be studied more intensively. Depending on their (proven) benefits for the young infant, fortification with minor lipids may be expected in the coming decade.
The unique triglyceride structure of HMF with palmitic acid primarily esterified in the sn-2 position, and the importance thereof, was already acknowledged in the 1960s. Products including high β-palmitate or “OPO” fats have been on the market since 1996 and, until recently, have been gaining market share gradually. The introduction of OPO fats in China resulted in a serious expansion of IF products including β- palmitate fats. A further global expansion is expected, as well as intensified efforts to collect additional evidence of its role in calcium absorption and metabolic imprinting, among others, to convince legal authorities of the importance of this unique triglycer-ide structure.
The physical properties of HMF have only received attention over the last few years. The fat globule structure (MFGM) of HMF has a different physical nature from the fat in IF products, in which the fat phase is stabilized in dispersion using emulsi-fiers. The precise advantages of the MFGM that includes PLs are still to be revealed (Long et al., 2013). Recent rat studies, including Danone’s Nuturis®, have shown that the physical properties of early dietary lipids contribute positively to metabolic imprinting (Oosting et al., 2012). Clinical studies are ongoing in infants (e.g., the study of Timbly at the Umeå University in Sweden, initiated in 2008) and a few for-tifiers including MFGM for addition to IF are already commercially available (e.g., Lacprodan® “MFGM-10” (i.e., Lacprodan® MFGM-10) from Arla Foods). As for all new developments in this segment, conclusive evidence regarding the efficacy and safety as obtained from (human) trials is required prior to introduction in new innova-tive IF products.
References
Agostoni, C., 2005. Polyunsaturated fatty acids in human milk and neurological development in breastfed infants. Curr. Pediatr. Rev. 1, 25–30.
Albanesi, S., Olivetti, C., 2009. Infant formula appendix for: gender roles and medical progress. National Bureau of Economic Research, Cambridge, MA, Appendix to ‘Gender roles and medical progress’. NBER working paper no. 14873.
Askew, K., 2013. China pushes for consolidation of domestic infant formula market. Just-Food, August 16.
Astley, M., 2014. China cuts the number of permitted imported infant formula brands to less than 100. http://www.dairyreporter.com/Markets/China-cuts-number-of-permitted-imported-infant-formula-brands-to-94 (accessed 08.04.15.).
Bach, A.C., Babayan, V.K., 1982. Medium-chain triglycerides: an update. Am. J. Clin. Nutr. 36 (5), 950–962.

Infant formula 311
Ballard, O.J.D., Morrow, A.L., 2013. Human milk composition: nutrients and bioactive factors. Pediatr. Clin. North Am. 60 (1), 49–74.
Banni, S., Carta, G., Collu, M., Gambelli, L., Happe, R.P., Lisai, S., Murru, E., Piras, A., Sirigu, A., 2014. Dietary triacylglycerols with palmitic acid in the sn-2 position modulate levels of endocannabinoids and congeners in rat tissues. In: Abstract from the 11th Biennial Meeting of the International Society for the Study of Fatty Acids and Lipids, 28 June–2 July 2014, Stockholm, Sweden.
Bar-Yoseph, F., 2013. Reviews of sn-2 palmitate oil implications for infant health. Prostaglandins Leukot. Essent. Fatty Acids 89 (4), 139–143.
Bar-Yoseph, F., Lifshitz, Y., Cohen, T., Malard, P., Li, Z., Cui, H., Zhang, A., Yang, H., Wu, J., Xu, C., 2014. sn-2 Palmitate reduces crying and soaped fatty acids excretion in Chinese infants fed formula enriched with prebiotics: a double-blind randomised clinical trial. In: ESPGHAN 2014, Abstract from the 47th Annual Meeting of the European Society for Paediatric Gastroenterology, Hepathology and Nutrition, 9–12 June 2014, Jerusalem, Israel.
Bitman, J., Wood, L., Hamosh, M., Mehta, N.R., 1983. Comparison of the lipid composition of breast milk from mothers of term and preterm infants. Am. J. Clin. Nutr. 38 (2), 300–312.
Bongers, M.E.J., De Lorijn, F., Reitsma, J.B., Groeneweg, M., Jaminiau, J.A.J.M., Benninga, A.M., 2007. The clinical effect of a new infant formula in term infants with constipation: a double-blind, randomized cross-over trial. Nutr. J. 6, 8.
Bracco, U., 1994. Effect of triglyceride structure on fat absorption. Am. J. Clin. Nutr. 60 (6 Suppl.), 1002S–1009S.
Breckenridge, W.C., Marai, L., Kuksis, A., 1969. Triglyceride structure of human milk fat. Can. J. Biochem. 47, 761–769.
Brenna, J.T., Carlson, S.E., 2014. Docosahexaenoic acid and human brain development: evi-dence that a dietary supply is needed for optimal development. J. Hum. Evol. 77, 99–106. http://dx.doi.org/10.1016/j.jhevol.2014.02.017.
Brenna, J.T., Varamini, B., Jensen, R.G., Diersen-Schade, D.A., Boettcher, J.A., Arterburn, L.A., 2007. Docosahexaenoic and arachidonic acid concentrations in human breast milk worldwide. Am. J. Clin. Nutr. 85, 1457–1464.
Campoy, C., Escolano-Margarit, M.V., Anjos, T., Szajewska, H., Uauy, R., 2012. Omega 3 fatty acids on child growth, visual acuity and neurodevelopment. Br. J. Nutr. 107 (Suppl. 2), 85–106. http://dx.doi.org/10.1017/S0007114512001493.
Carnielli, V.P., Sulker, E.J., Moretti, C., Wattimena, J.L.D., Van Goudoever, J.B., Degenhart, H.J., Zachello, F., Sauer, P.J.J., 1994. Conversion of octanoic acid into long-chain satu-rated fatty acids in premature infants fed a formula containing medium-chain triglycerides. Metabolism 43 (10), 1287–1292.
Carnielli, V.P., Ingrid, H.T., Luijendijk, I.H.T., van Goudoever, J.B., Sulkers, E.J., Boerlage, A.A., Degenhart, H.J., Sauer, P.J.J., 1995a. Feeding premature newborn infants palmitic acid in amounts and stereoisomeric position similar to that of human milk: effects on fat and mineral balance. Am. J. Clin. Nutr. 61, 1037–1042.
Carnielli, V.P., Ingrid, H.T., Luijendijk, I.H.T., van Seek, R.H.T., Soerma, G.J.M., Degenhart, H.J., Sauer, P.J.J., 1995b. Effect of dietary triacylglycerol fatty acid positional distribution on plasma lipid classes and their fatty acid composition in preterm infants. Am. J. Clin. Nutr. 62, 776–781.
Carnielli, V.P., Luijendijk, I.H., Van Goudoever, J.B., Sulkers, E.J., Boerlage, A.A., Degenhart, H.J., Sauer, P.J.J., 1996. Structural position and amount of palmitic acid in infant formu-las: effects on fat, fatty acid, and mineral balance. J. Pediatr. Gastroenterol. Nutr. 23 (5), 553–560.

312 Specialty Oils and Fats in Food and Nutrition
Castilho, S.D., Barros Filho, A.A., 2010. The history of infant nutrition. J. Pediatr. 86 (3), 179–188.
Chesney, R.W., Helms, R.A., Christensen, M., Budreau, A.M., Han, X., Sturman, J.A., 1998. The role of taurine in infant nutrition. Adv. Exp. Med. Biol. 442, 463–472.
Codex Alimentarius, 2011. CODEX STAN 72-1981.Coriolis Research, 2014. Infant Formula Value Chain. Coriolis Research, Auckland. Available
from, http://nzpecc.org.nz/media/f3c9cc3577fc96acffff80caffffd502.pdf (accessed 16.04.14).
Davis-Bruno, K., Tassinari, M.S., 2011. Essential fatty acid supplementation of DHA and ARA and effects on neurodevelopment across animal species: a review of the literature. Birth Defects Res. B 92, 240–250.
Drudy, D., Mullane, M.R., Quinn, T., Wall, P.G., Fanning, S., 2006. Enterobacter sakazakii: an emerging pathogen in powdered infant formula. Clin. Infect. Dis. 42 (7), 996–1002.
EC, 2006. Commission Directive 2006/141/EC of 22 December 2006 on infant formulae and follow-on formulae and amending Directive 1999/21/EC. Off. J. Eur. Union L 401, 1–33.
EFSA, 2014a. Scientific opinion on the essential composition of infant and follow-on formulae. EFSA J. 12 (7), 3760.
EFSA, 2014b. Scientific opinion on the substantiation of a health claim related to DHA and contribution to normal brain development pursuant to Article 14 of Regulation (EC) No 1924/2006. EFSA J. 12 (10), 3840.
Filer, L.J., Mattson, F.H., Fomon, S.J., 1969. Triglyceride configuration and fat absorption by the human infant. J. Nutr. 99, 335–344.
Fomon, S.J., 1993. Nutrition of Normal Infants. Mosby, St. Louis.Forsyth, J.S., 1998. Lipids and infant formulas. Nutr. Res. Rev. 11, 255–278.Frantz, J.F., 1951. Gail Borden: Dairyman to a Nation. Oklahoma University Press, Norman.Freeman, C.P., Jack, E.L., Smith, L.M., 1965. Intramolecular fatty acid distribution in the milk
fat triglycerides of several species. J. Dairy Sci. 48 (7), 853–858.Goedhart, A.C., Bindels, J.G., 1994. The composition of human milk fat as a model for
the design of infant formulas: recent findings and possible application. Nutr. Res. Rev. 7, 1–23.
Gohel, M., 2009. Spray Drying: A Review. http://www.pharmainfo.net/reviews/spray-dry-ing-review (accessed 10.10.14).
Gunstone, F.D., Harwood, J.L., 2007. Occurrence and characterisation of oils and fats. In: Gunstone, F.D., Harwood, J.L., Dijkstra, A.J. (Eds.), The Lipid Handbook with CD-ROM. third ed. CRC press, Taylor and Francis group, Boca Raton, FL, pp. 37–141(chapter 2).
Gurr, M., 1997. Lipids in infant nutrition. Lipid Technol. 9 (1), 14–17.Haddad, I., Mozzon, M., Frega, N.G., 2012. Trends in fatty acids positional distribution in
human colostrum, transitional and mature milk. Eur. Food Res. Technol. 235, 325–332.Handscomb, C.S., 2008. Simulated droplet drying and particle formation in spray towers. Ph.D.
thesis. University of Cambridge.Heaton, A.E., Meldrum, S.J., Koster, J.K., Prescott, S.L., Simmer, K., 2013. Does docosahexae-
noic acid supplementation in term infants enhance neurocognitive functioning in infancy? Front. Hum. Neurosci. 7 (774), 1–12 Art.
Innis, S.M., 2007a. Human milk: maternal dietary lipids and infant development. Proc. Nutr. Soc. 66, 397–404.
Innis, S.M., 2007b. Dietary (n-3) fatty acids and brain development. J. Nutr. 137, 855–859.Innis, S.M., 2011. Metabolic programming of long-term outcomes due to fatty acid nutrition in
early life. Matern. Child Nutr. 7 (Suppl. 2), 112–113.

Infant formula 313
Innis, S.M., 2014. Impact of maternal diet on human milk composition and neurological devel-opment of infants. Am. J. Clin. Nutr. 99 (Suppl.), 734S–741S.
ISSFAL, 2008. ISSFAL Statement on Dietary Fats in Infant Nutrition. http://www.issfal.org/statements/pufa-recommendations/statement-2 (accessed 02.10.14).
Jensen, R.G., 1996. The lipids in human milk. Prog. Lipid Res. 35, 53–92.Jensen, R.G., 1999. Lipids in human milk. Lipids 34 (12), 1243–1271.Jensen, R.G., 2001. Infant formulas. In: Gunstone, F.D. (Ed.), Structured and Modified Lipids.
Dekker, New York, pp. 455–464 (chapter 16).Jensen, C., Buist, N.R.M., Wilson, T., 1986. Absorption of individual fatty acids from long
chain or medium chain triglycerides in very small infants. Am. J. Clin. Nutr. 43 (5), 745–751.
Kaplan, J.L., Shi, H.N., Walker, W.A., 2011. The role of microbes in developmental immuno-logic programming. Pediatr. Res. 69, 465–472.
Kennedy, K., Fewtrell, M.S., Morley, R., Abbott, R., Quinlan, P.T., Wells, J.C.K., Bindels, J.G., Lucas, A., 1999. Double-blind, randomized trial of a synthetic triacylglycerol in formula-fed term infants: effects on stool biochemistry, stool characteristics, and bone mineralization. Am. J. Clin. Nutr. 70 (5), 920–927.
Klenoff-Brumberg, H.L., Genen, L.H., 2003. High versus low medium chain triglyceride con-tent of formula for promoting short term growth of preterm infants. Cochrane Database Syst. Rev.CD002777.
Koletzko, B., Thiel, I., Springer, S., 1992. Lipids in human milk: a model for infant formulae? Eur. J. Clin. Nutr. 46 (Suppl. 4), S45–S55.
Koletzko, B., Baker, S., Cleghorn, G., Fagundes Neto, U., Gopalan, S., Hernell, O., Seng Hock, Q., Jirapinyo, P., Lonnerdal, B., Pencharz, P., Pzyrembel, H., Ramirez-Mayans, J., Raanan, S., Turck, D., Yamashiro, Y., Zong-Yi, D., 2005. Global standard for the composition of infant formula: recommendations of an ESPGHAN coordinated international expert group. J. Pediatr. Gastroenterol. Nutr. 41, 584–599.
Koo, W.W.K., Hockman, E.M., Dow, M., 2006. Palm olein in the fat blend of infant formulas: effect on the intestinal absorption of calcium and fat, and bone mineralization. J. Am. Coll. Nutr. 25 (2), 117–122.
Levenstein, H., 1983. ”Best for babies” or “preventable infanticide”? The controversy over arti-ficial feeding of infants in America, 1880–1920. J. Am. Hist. 70 (1), 75–94.
Litmanovitz, I., Davidson, K., Eliakim, A., Regev, R.H., Dolfin, T., Arnon, S., Bar-Yoseph, F., Goren, A., Lifshitz, Y., Nemet, D., 2013. High beta-palmitate formula and bone strength in term infants: a randomised, double-blind, controlled trial. Calcif. Tissue Int. 92, 35–41.
Litmanovitz, I., Bar-Yoseph, F., Lifshitz, Y., Davidson, K., Eliakim, A., Regev, R.H., Nemet, D., 2014. Reduced crying in term infants fed high beta-palmitate formula: a double-blind ran-domized clinical trial. BMC Pediatr. 14, 152.
Long, A.C., Kaiser, J.L., Katz, G.E., 2013. Lipids in infant formula: current and future innova-tions. Lipid Technol. 25 (6), 127–129.
López-López, A., López-Sabatar, M.C., Campoy-Folgoso, C., Rivero-Urgell, M., Castelotte-Bargalló, A., 2002. Fatty acid and sn-2 fatty acid composition in human milk from Granada (Spain) and in infant formulas. Eur. J. Clin. Nutr. 56 (12), 1242–1254.
Lucas, A., Quinlan, P., Abrams, S., Ryan, S., Meah, S., Lucas, P.J., 1997. Randomised con-trolled trial of a synthetic triglyceride milk formula for preterm infants. Arch. Dis. Child. Fetal Neonatal Ed. 77, F177–F184.
Martinez, M., 1992. Tissue levels of polyunsaturated fatty acids during early human develop-ment. J. Pediatr. 120 (4 Pt 2), S129–S138.

314 Specialty Oils and Fats in Food and Nutrition
Oosting, A., Kegler, D., Wopereis, H.J., Teller, I.C., Van de Heijning, B.J., Verkade, H.J., Van der Beek, E.M., 2012. Size and phospholipid coating of lipid droplets in the diet of young mice modify fat accumulation in adulthood. Pediatr. Res. 72 (4), 362–369.
Osborn, M.S., 1979a. The rent breast: a brief history of wet-nursing. Midwife Health Visit. Community Nurse 15 (8), 302–306.
Osborn, M.S., 1979b. The rent breast. Part II. Midwife Health Visit. Community Nurse 15 (9), 347–348.
Patel, M.S., Srinivasan, M., 2002. Metabolic programming: causes and consequences. J. Biol. Chem. 277 (3), 1629–1632.
Radbill, S., 1981. Infant feeding through the ages. Clin. Pediatr. 20 (10), 613–621.Renfrew, E., 2014. 7% Growth for $50 Billion Global Infant Formula Market. Zenith
International Ltd., Bath. Available from, http://www.zenithinternational.com/articles/1355 (accessed 23.10.14).
Sahin, N., Akoh, C.C., Karaalí, A., 2006. Human milk fat substitutes containing omega-3. J. Agric. Food Chem. 54, 3717–3722.
Sanders, T.A.B., 1999. Essential fatty acid requirements of vegetarians in pregnancy, lactation, and infancy. Am. J. Clin. Nutr. 70 (Suppl.), 555S–559S.
SCF/CS/NUT/IF/65, 2003. Report of the scientific committee on food on the revision of essen-tial requirements of infant formulae and follow-on formulae. Adopted on April 04, 2003, SCF/CS/NUT/IF/65 Final, May 18, 2003.
Schmelzle, H., Wirth, S., Skopnik, H., Radke, M., Knol, J., Böckler, H.-M., Brönstrup, A., Wells, J., Fusch, C., 2003. Randomized double-blind study of the nutritional efficacy and bifidoge-nicity of a new infant formula containing partially hydrolyzed protein, a high beta-palmitic acid level, and nondigestible oligosaccharides. J. Pediatr. Gastroenterol. Nutr. 36, 343–351.
Schuman, A.J., 2003. A concise history of infant formula (twist and turns included). Contemp. Pediatr. 20, 91–103.
Scott, C.E., 2010. Structured lipid: a functional ingredient to closely match infant formula to breast milk. Nutrafoods 9 (3), 7–13.
Sidnell, A., Greenstreet, E., 2011. Infant nutrition—review of lipid innovation in infant formula. Nutr. Bull. 36, 373–380.
Singh, S., Dixit, D., 2014. A review on spray drying: emerging technology in food industry. Int. Appl. Eng. Technol. 4 (1), 1–8. ISSN: 227-212X. An open access, online international journal available from, http://www.cibtech.org/jet.htm (accessed 10.10.14).
Spenser, S.A., McKenna, S., Stammers, J., Hull, D., 1992. Two different low birth weight for-mulae compared. Early Hum. Dev. 30 (1), 21–31.
Stevens, E.E., Patrick, T.E., Pickler, R., 2009. A history of infant feeding. J. Perinat. Educ. 18 (2), 32–39.
Straarup, E.M., Lauritzen, L., Faerk, J., Hoy, C.E., Michaelsen, K.F., 2006. The stereospecific triacylglycerol structures and fatty acid profiles of human milk and infant formulas. J. Pediatr. Gastroenterol. Nutr. 42, 293–299.
Sulkers, E.J., Van Goudoever, J.B., Leunisse, C., Wattimena, J.L.D., Sauer, P.J.J., 1992. Comparison of two preterm formulas with or without addition of medium-chain tri-glycerides (MCTs). I: effects on nitrogen and fat balance and body composition changes. J. Pediatr. Gastroenterol. Nutr. 15 (1), 42–47.
Tai, E.K.K., Wanga, X.B., Chen, Z.-Y., 2013. An update on adding docosahexaenoic acid (DHA) and arachidonic acid (AA) to baby formula. Food Funct. 4, 1767–1775.

Infant formula 315
Tijhuis, M.J., Doets, E.L., Vonk Noordegraaf-Schouten, M., 2014. Extensive Literature Search and Review as Preparatory Work for the Evaluation of Essential Composition of Infant and Follow-On Formulae and Growing-Up Milk. EFSA Supporting Publication, Rotterdam, The Netherlands. EN-551.
Timbly, M., 2008. Effects of Milk Fat Globule Membrane (MFGM)—Enriched Formula with Reduced Energy and Protein Content on Growth and Development (TUMME). Umeå University, Sweden Clinicaltrials.gov identifier: NCT00624689. Study started 15 February 2008 and is ongoing.
Tomarelli, R.M., Meyer, B.J., Weaber, J.R., 1968. Effect of positional distribution on the ab-sorption of the fatty acids of human milk and infant formulas. J. Nutr. 95, 583–590.
Ullmann, A., 2007. Pasteur–Koch: distinctive ways of thinking about infectious diseases. Microbe 2 (8), 383–387.
Weinberg, F., 1993. Infant feeding through the ages. Can. Fam. Phys. 39, 2016–2020.Wickes, I.G., 1953a. A history of infant feeding. Part I. Primitive peoples: ancient works: renais-
sance writers. Arch. Dis. Child. 28, 151–158.Wickes, I.G., 1953b. A history of infant feeding. Part II. Seventeenth and eighteenth centuries.
Arch. Dis. Child. 28, 232–240.Wickes, I.G., 1953c. A history of infant feeding. Part III. Eighteenth and nineteenth century
writers. Arch. Dis. Child. 28, 332–340.Wickes, I.G., 1953d. A history of infant feeding. Part IV. Nineteenth century continued. Arch.
Dis. Child. 28, 416–422.Wickes, I.G., 1953e. A history of infant feeding. Part V. Nineteenth century concluded and
twentieth century. Arch. Dis. Child. 28, 495–502.World Health Organization, 2007. Guidelines for the Safe Use Preparation, Storage and
Handling of Powdered Infant Formula. WHO, Geneva. Available from, http://www.who.int/foodsafety/publications/micro/pif2007/en/ (accessed 09.07.14).
Yao, M., Lien, E.L., Capeding, M.R.Z., Fitzgerald, M., Ramanujam, K., Yuhas, R., Northington, R., Lebumfacil, J., Wang, L., DeRusso, P.A., 2014. Effects of term infant formulas con-taining high sn-2 palmitate with and without oligofructose on stool composition, stool characteristics, and bifidogenicity: a randomized, double-blind, controlled trial. J. Pediatr. Gastroenterol. Nutr. 59 (4), 440–448. PMID: 24840511.
Yaron, S., Shachar, D., Abramas, L., Riskin, A., Bader, D., Litmanovitz, I., Bar-Yoseph, F., Cohen, T., Levi, L., Lifshitz, Y., Shamir, R., Shaoul, R., 2013. Effect of high β- palmitate content in infant formula on the intestinal microbiota of term infants. J. Pediatr. Gatroenterol. Nutr. 56 (4), 376–381.
Yuhas, R., Pramuk, K., Lien, E.L., 2006. Human milk fatty acid composition from nine coun-tries varies most in DHA. Lipids 41 (9), 851–858.
Zink, D., 2003. Powdered infant formula: an overview of manufacturing processes. In: Food Advisory Committee, Contaminants and Natural Toxicants Subcommittee, Meeting on Enterobacter sakazakii contamination in powdered infant formula, FDA, USA, 18–19 March 2003.
Zuidam, N.J., Shimoni, E., 2010. Overview of microencapsulates for use in food products and processes and methods to make them. In: Zuidam, N.J., Nedovic, V. (Eds.), Encapsulation Technologies for Active Food Ingredients and Food Processing. Springer, New York, pp. 3–29 (chapter 2).

This page intentionally left blank