Modelling of Cardiac β- adrenoceptor desensitisation to understand heart failure therapy

Accepted Manuscript
Selective β3-Adrenoceptor Agonists in the Treatment of the Overactive Bladder
Karl-Erik Andersson, Nancy Martin, Victor Nitti
PII: S0022-5347(13)00380-7 DOI: 10.1016/j.juro.2013.02.104
Reference: JURO 9999
To appear in: The Journal of Urology Accepted date: 20 February 2013 Please cite this article as: Andersson, K.E., Martin, N., Nitti, V., Selective β3-Adrenoceptor Agonists in the Treatment of the Overactive Bladder, The Journal of Urology® (2013), doi: 10.1016/j.juro.2013.02.104. DISCLAIMER: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our subscribers we are providing this early version of the article. The paper will be copy edited and typeset, and proof will be reviewed before it is published in its final form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to The Journal pertain. All press releases and the articles they feature are under strict embargo until uncorrected proof of the article becomes available online. We will provide journalists and editors with full-text copies of the articles in question prior to the embargo date so that stories can be adequately researched and written. The standard embargo time is 12:01 AM ET on that date.

1
February 28, 2013
Selective β3−Adrenoceptor Agonists in the Treatment
of the Overactive Bladder
Karl-Erik Andersson1, Nancy Martin2, Victor Nitti3
1Institute for Regenerative Medicine, Wake Forest University School of Medicine, NC,2Astellas Scientific and Medical Affairs, Northbrook, IL, 3New York University Urology Associates, New York, New York
Correspondence:
K-E Andersson, MD, PhD
Institute for Regenerative Medicine
Wake Forest University School of Medicine
Medical Center Boulevard
Winston Salem, NC 27157
Tel 336.713.1195
Fax 336.713.7290
e-mail: [email protected]

2
Key words: adrenoceptors, detrusor smooth muscle, urodynamics, controlled clinical trials
Abbreviations and Acronyms
OAB = overactive bladder
RCT = randomized controlled clinical trial
AR = adrenoceptor
DO = detrusor overactivity
RT -PCR = reverse transcription polymerase chain reaction
ATP = adenosine triphosphate
NO = nitric oxide
PG = prostaglandin
BKca = calcium activated big potassium channel
PKA = protein kinase A
cAMP = cyclic adenosine monophosphate

3
Abstract
Background and Purpose. Bladder effects of isoprenaline and selective β1− and β2−adrenoceptor
(AR) agonists reported in early studies suggested that bladder β−ARs are "atypical". Since there
is a lack of alternatives to antimuscarinics in the treatment of overactive bladder (OAB)
symptoms, there has been an intensive search for new drug targets. The discovery of the β3−AR
with high expression in the bladder, suggested that this receptor, mediating detrusor relaxation,
could be a target for treatment of patients with OAB symptoms. Methods. An overview of
published literature on β−ARs and bladder (MEDLINE) was performed. The US Food and Drug
Administration web site, clinicaltrials.gov, and controlled-trials.com online trial registries were
searched for English-language articles containing the terms β3−ARs and β3−AR agonists. In
addition, abstracts from recent international scientific meetings were searched for randomised
controlled trials (RCTs) on β3−AR agonists. Results. Stimulation of β3-ARs relaxes detrusor
smooth muscle, decreases afferent signaling from the bladder, improves bladder compliance on
filling, and increases bladder capacity. RCTs show that the selective β3-AR agonist,
mirabegron, for which most information is available and which is approved in Japan, USA, and
Europe, reduces the number of micturitions and incontinence episodes in a 24-h period
compared with placebo. The most common adverse effects recorded are dry mouth (placebo
level) and gastrointestinal disturbances rated as mild to moderate. Small rises in mean heart rate
(1 beat /minute) and blood pressure (1 mm Hg) have been demonstrated in OAB patients.
Conclusions. Available information suggests that β3−AR agonists may be a promising
alternative to antimuscarinics in the treatment of OAB. However, further clinical experiences
outside clinical trials, and information on the long-term use in terms of efficacy, safety, and

4
tolerability are warranted to optimally characterize the position of β3−AR agonists in the
treatment algorithm for OAB.

5
Background.
In 1948, the existence of two broad subtypes of adrenoceptors (AR), α-ARs and β-ARs, were first
demonstrated.1 In the late 1960, two subtypes of β-ARs, β1 and β2, were identified and
characterized,2 while a third, β3, was isolated and cloned in 1989.3 β3-ARs are widely distributed in
the body, including adipose tissue, the heart and vascular system, and the urinary bladder, however,
the distribution is highly species dependent.4, 5 In isolated human bladder, non-subtype selective β-
AR agonists like isoprenaline have a pronounced inhibitory effect, and administration of such drugs
can increase bladder capacity in man.6 Early functional studies on bladders from animals (cat) and
humans suggested that such effects may be mediated by an "atypical' β-AR, since the β-ARs had
functional characteristics typical of neither β1-, nor β2- ARs.7, 8 Thus, the effects could be blocked by
propranolol (non-subtype selective), but not by practolol (β1) or metoprolol (β1) or butoxamine (β2).
Despite these functional data, it was suggested, based on receptor binding studies using subtype
selective ligands, that the β-ARs of the human detrusor were primarily of β2 subtype.6 Favourable
effects in patients with detrusor overactivity (DO) were reported in open studies with selective β2-
AR agonists such as terbutaline.9 However, further studies were unable to show that non-subtype or
β2-AR selective agonists represent an effective therapeutic principle in the treatment of the
overactive bladder (OAB).10
All three β-AR subtypes (β1, β2, and β3) have been identified in the detrusor of most species,
including humans.11 In addition, the human urothelium contains the three receptor subtypes,12
Studies using real-time RT-PCR have revealed a predominant expression of β3-AR mRNA in human
detrusor muscle.11, 13 As pointed out by Frazier et al.14 studies at the protein level have been difficult

6
to interpret because none of the available radioligands is suited to detect β3-ARs. However, the
preclinical functional evidence for an important role of β3-ARs in both normal and neurogenic
bladders is convincing.15 The human detrusor also contains β2-ARs, and most probably both
receptors are involved in the physiological detrusor effects (relaxation) of noradrenaline.11
Rationale for use of selective β3-AR agonists in OAB. Several factors may contribute to OAB,
defined either based on symptoms (the OAB syndrome) or urodynamics (DO). Various theories
have been put forward and are discussed in detail elsewhere.16 OAB is a filling disorder, and
recent research has focused on afferent bladder function. Two signaling pathways by which
afferent information is generated and conveyed to the central nervous system, the myogenic and
the urothelial pathways, have been defined.17 (Figures 1 and 2)
It is well established that β-AR stimulation has relaxant effects on detrusor muscle, either from
basal tone or when contracted by KCl or various agonists.15 However, two types of detrusor
contraction can be observed. One is the voiding contraction, which is a well coordinated bladder
contraction caused by release of acetylcholine and other contractant transmitters (e.g., ATP)
from cholinergic nerves. This contraction requires parasympathetic output from the sacral spinal
cord. The other type of contraction is the spontaneous (autonomous) contractile activity
occurring during bladder filling, which can be demonstrated in vitro and in vivo, 21 Both
preclinical and clinical studies have shown that β3-AR agonists have no significant negative
effects on the voiding contraction,15 suggesting a more limited potential for urinary retention.
The normal stimulus for activation of the micturition reflex is considered to be distension of the
bladder, initiating activity in ‘‘in series’’-coupled, low-threshold mechanoreceptive (Aδ)

7
afferents.19 It is obvious that if this response to distension is decreased by the detrusor muscle
being relaxed and more compliant, the afferent activity needed to initiate micturition will be
delayed and bladder capacity increased. Such an effect may be obtained by stimulating the β3-
ARs on the detrusor muscle. There are reasons to believe that the spontaneous contractile, phasic
activity of the detrusor smooth muscle during filling not only can create tone in the detrusor
muscle, but also generate afferent input (‘‘afferent noise’’), contributing to OAB/DO. In fact.
Aizawa et al.20 showed in rats that the β3-AR agonist, CL316,243, could inhibit filling-induced
activity not only in mechano-sensitive Aδ-fibers, but also in C-fiber primary bladder afferents
provided that these fibers were stimulated by prostaglandin (PG) E2. A more recent study from
the same group confirmed similar findings with mirabegron.21 β3-AR agonists have a
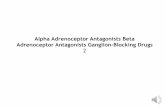
pronounced effect on spontaneous contractile activity in detrusor muscle in vitro (Figure 3),22
which may be an important basis for their clinical effects.
Changes in urothelial receptor function and neurotransmitter release, may lead to changes of
bladder contraction.23, 24 The urothelium interacts closely with underlying structures, e.g., the
interstitials cells and afferent nerves, and these structures appear to work together as a functional
unit.23, 24 The detrusor muscle, the urothelium, interstitial cells, and the afferent nerves all contain
β3-ARs, 12, 25, 26 which may be targeted and when stimulated may contribute to the effects of β3-
AR agonists. The possible role of urothelial β3-ARs in bladder relaxation has been investigated
by several investigators.12, 25 Murakami et al.25 found in human bladder strips that the presence of
urothelium caused a parallel rightward shift of the concentration-response curve to isoprenaline
and suggested that urothelial β3-AR stimulation could induce the release of a urothelium-derived
factor which inhibited the β3-AR agonist-induced relaxation of the detrusor smooth muscle.
However, to what extent a urothelial signaling pathway contributes in vitro and in vivo to the

8
relaxant effects of β-AR agonists in general, and β3-AR agonists specifically, remains to be
elucidated.
The generally accepted molecular mechanism by which β-ARs mediate detrusor relaxation in most
species, is activation of adenylyl cyclase and subsequent formation of cAMP, which activates
protein kinase A (PKA). This enzyme, in turn, phosphorylates specific proteins resulting in detrusor
relaxation. However, there is evidence suggesting that in the bladder K+ channels, particularly BKCa
channels, may be more important in β3-AR mediated relaxation than cAMP.14, 27, 28 To what extent
each of these downstream signal cascade mechanisms contribute to the overall effect of the β-AR
agonists remains to be established.
The in vivo effects of β3-AR agonists on bladder function have been studied in several animal
models. It has been shown that compared with other agents (including antimuscarinics), β3-AR
agonists increase bladder capacity with no change in micturition pressure and the residual volume.17
For example, Hicks et al.29 studied the effects of the selective β3-AR agonist, GW427353
(solabegron), in the anesthetized dog and found that the β3−AR agonist evoked an increase in
bladder capacity under conditions of acid evoked bladder hyperactivity, without affecting voiding.
Effects of β3-ARs outside the bladder
Since the presence β3-ARs have been demonstrated in several tissues outside the bladder, such
as adipose tissues, heart, blood vessels, gastrointestinal, tract, prostate, brain, and near-term
myometrium,4 there is a consideration of "off target" effects of β3-AR stimulation when treating
OAB. Possible effects on the heart and vasculature have been the main concerns.

9
There is evidence for expression of β3-AR mRNA in the human heart, but the receptor protein
does not seem to have been consistently demonstrated, and the functional role of β3-ARs has not
been established.30 In the normal heart, β3-ARs may mediate a moderate negative inotropic
effect, but in heart failure, it may protect against adverse effects of excessive catecholamine
stimulation by action on excitation-contraction coupling, electrophysiology, or remodeling.31 No
negative effects on cardiac contractility have been reported in the treatment of OAB patients.32
Cardiac electrophysiology has been extensively evaluated.31,33 There seems to be no evidence for
a direct effect of β3-AR agonists on the sinus node and consequent changes in heart rate.31
However, in a study on healthy volunteers,32 mirabegron increased heart rate in a dose-dependent
manner. Maximum mean increases in heart rate from baseline for the 50 mg, 100 mg, and 200
mg dose groups compared to placebo were 6.7 beats per minutes (bpm), 11 bpm, and 17 bpm,
respectively.32 However, in the clinical efficacy and safety studies, the change from baseline in
mean pulse rate for mirabegron 50 mg was approximately 1 bpm and reversible upon
discontinuation of treatment. Whether this discrepancy is dependent on the use of different
administration forms (rapid vs extended release) is unclear.
So far, there is no clinical evidence that β-AR agonists are causing QT-prolongation and
ventricular arrhythmia at therapeutic doses (see below).
In some vascular beds β-AR stimulation has been demonstrated to cause dilatation both directly
and via release of NO,31, 34 which could be expected to reduce blood pressure. This is in contrast
to what has been observed clinically. In healthy subjects, mirabegron (50-300 mg/day for 10
days) increased blood pressure dose-dependently.32 However, in the studies on OAB patients the
mean increases (compared to placebo) in systolic/diastolic blood pressure after therapeutic doses

10
of mirabegron once daily was approximately 0.5 - 1 mmHg and reversible upon discontinuation
of treatment.32 Again, whether this discrepancy is dependent on the use of different
administration forms is unclear.
Pharmacology of selective β3-adrenoceptor agonists.
The selective β3-AR agonist, mirabegron,35 has been approved for treatment of OAB in Japan
(Betanis®), USA (Myrbetriq®), and Europe (Betmiga®). There are proof of concept studies for
other β3-AR selective agonists such as and solabegron and ritobegron.36 However, the
development of ritobegron has been ceased since in failed to reach the primary efficacy endpoint
in phase III studies. Other agents, e.g., TRK-380, 37 is in pre-clinical development for the
treatment of OAB.
Mirabegron. Takusagawa et al. found that mirabegron was rapidly absorbed after oral
administration. It circulates in the plasma as the unchanged form, its glucuronic acid conjugates
and other metabolites, the metabolites being inactive.38 Of the administered dose, 55% is
excreted in urine, mainly as the unchanged form, and 34% is recovered in feces, almost entirely
as the unchanged form. Mirabegron is highly lipophilic and is metabolized in the liver via
multiple pathways, mainly by cytochrome P450 3A4 and 2D6 (CYP2D6).39, 40 In a Phase I
pharmacokinetic study, sixteen healthy volunteers, phenotyped as either poor or extensive
metabolizers of CYP2D6 were enrolled. The volunteers received a 160 mg single oral dose after
overnight fasting. Poor metabolizers excreted a slightly higher urinary fraction of mirabegron
(15.4±4.2%) than extensive metabolizers (11.7±3.0%). Tmax in both extensive and poor

11
metabolizers was about 2 hours and the terminal elimination half-life (t1/2) approximately 23-25
hours.41,42
The cardiac safety of mirabegron was evaluated in a thorough QT/QTc (heart rate (HR)-
corrected QT interval) study, including supratherapeutic doses. This was a randomized, placebo-
and active- controlled (moxifloxacin 400 mg) four-treatment-arm parallel crossover study 43 and
the design followed the recommendations of The International Conference on Harmonisation
(ICH). The effect of multiple doses of mirabegron 50 mg, 100 mg and 200 mg once daily on
QTc interval was studied, and according to ICH E14 criteria, mirabegron did not cause QTcI
prolongation at the 50-mg therapeutic and 100-mg supratherapeutic doses in either sex.
Mirabegron prolonged QTcI interval at the 200-mg supratherapeutic dose (upper one-sided 95%
CI >10 ms) in females, but not in males.
Clinical experiences with mirabegron. Chapple et al.44 reported the results of a phase IIA trial of
mirabegron in patients with OAB - the "Blossom trial", which was conducted in several
European countries, as a proof of concept study. It enrolled 314 patients with OAB symptoms -
262 patients were randomly assigned to 4 groups: placebo, mirabegron 100 mg bid, mirabegron
150 mg bid, and tolterodine 4 mg qd for a 4-week treatment period. The primary endpoint was
efficacy, and the primary efficacy variable was the change in the mean number of micturitions
per 24 hours as recorded on a frequency/volume chart. In both mirabegron groups significant
improvements in the mean number of micturitions per 24 hours were found compared with the
placebo group (−2.19 and −2.21 vs. −1.18, respectively). Mean volume voided was dose-
dependently increased in the mirabegron groups, and the change reach significance in the
mirabegron 150 mg group. Urgency episodes per 24 hours decreased significantly in both

12
mirabegron groups compared with the placebo group. No severe adverse events were reported
and treatment was generally well tolerated. A mean increase in pulse rate with mirabegron 150
mg (5 beats per minute) was demonstrated, but this was not associated with a clinically
significant increase in adverse events such as tachycardia and palpitations. The effect of
mirabegron was numerically better than that of tolterodine, but the study was not powered for a
direct comparison. This successful phase IIA study was followed by a phase IIB trial in OAB
patients carried out in Europe.45 This trial was a dose-ranging study of once-daily mirabegron (an
extended release formula of mirabegron) with multiple arms (placebo, mirabegron 25 mg, 100
mg, 150 mg, and 200 mg qd, for a 12-week treatment period), and the primary endpoint was to
evaluate the dose-response relationship on efficacy. The mean number of micturitions per 24
hours decreased dose-dependently, and the decreases were statistically significant with
mirabegron 50, 150 and 200 mg compared with placebo. The mean volume voided per
micturition increased dose-dependently, and the increases were significant with mirabegron 50
mg and more. Adverse events were experienced by 45.2% of the patients - the incidence of
adverse events was similar among all treatment groups (placebo 43.2% vs. mirabegron 43.8-
47.9%). The overall discontinuation rate owing to adverse events was 3.2% (placebo 3.0% vs.
mirabegron 2.4-5.3%). The most commonly reported adverse events considered treatment-related
was gastrointestinal disorders, including constipation, dry mouth, dyspepsia, and nausea. There
was no patient-reported acute retention. No significant difference in ECG parameters between
the groups was demonstrated. However, a small but significant increase in mean pulse rate was
observed after mirabegron 100 and 200 mg (1.6 and 4.1 beats per minute, respectively), although
this was not associated with an increase in cardiovascular adverse events in this study.

13
Three pivotal phase III studies have been performed.46-48 Nitti et al.46 reported on a phase III
multicenter, randomized, double-blind, parallel-group, placebo-controlled trial of mirabegron in
North America. They enrolled 1329 patients ≥18 years with OAB symptoms for ≥3 months.
Patients who completed a 2-week, single-blind, placebo run-in and had ≥8 micturitions/24 h and
≥3 urgency episodes/72 h (with or without incontinence) during a 3-day micturition diary period,
were randomized to receive placebo, or mirabegron 50 or 100 mg once daily for 12 weeks. Co-
primary endpoints were change from baseline to final visit (study end) in the mean number of
incontinence episodes/24 h and micturitions/24 h. Efficacy was assessed according to patient
micturition diaries and safety assessments included adverse event reporting. Patients were
randomized and received study drug (placebo: n=453; mirabegron 50 mg: n=443; mirabegron
100 mg: n=433). Mean age was 60.1 years, 74.3% were female, 29.7% had urgency
incontinence, 38.3% had mixed stress/urgency incontinence with urgency predominant and
32.2% had frequency without incontinence. At the final visit, mirabegron 50 and 100 mg showed
statistically significant improvements in the co-primary efficacy endpoints and mean volume
voided/micturition compared with placebo. Statistically significant benefits were achieved at the
first-measured time point of week 4. The incidence of adverse effects was similar across the
placebo and mirabegron 50 and 100 mg groups (50.1, 51.6 and 46.9%, respectively). The most
common (≥3%) adverse effects in any treatment group were hypertension (6.6, 6.1 and 4.9%,
respectively), urinary tract infection (1.8, 2.7 and 3.7%), headache (2.0, 3.2 and 3.0%) and
nasopharyngitis (2.9, 3.4 and 2.5%).
Khullar et al.47 performed a similarly designed study in Europe and Australia, enrolling 1978
patients, which included a fourth arm in which tolterodine SR 4 mg was used as a comparator.
Like the American study, Khullar et al. found that mirabegron caused a statistically significant

14
improvements from baseline compared with placebo in the number of urgency incontinence
episodes and number of micturitions per 24 hours. Mirabegron 50 and 100 mg was statistically
superior to placebo, whereas tolterodine was not, in these two key OAB symptoms, but the
study was not powered for head-to-head evaluation. Mirabegron 50 and 100 mg was well
tolerated. In particular, the incidence of hypertension or UTI were generally similar across
treatments within this study. In contrast with tolterodine, no increased dry mouth incidence was
observed with mirabegron relative to placebo.
In a third phase 3 study48, evaluating the effects of 25 and 50 mg mirabegron, both doses were
associated with significant improvements in efficacy measures of incontinence episodes and
micturition frequency. In mirabegron-treated patients, the overall incidence/severity of adverse
effects was similar to that of placebo.
In a 12-month study to assess safety and efficacy of mirabegron, Chapple et al.49 randomized a
total of 812, 820, and 812 patients to receive mirabegron 50 mg, mirabegron 100 mg, and
tolterodine ER 4 mg, respectively. The primary variable was incidence and severity of treatment-
emergent adverse, and secondary variables were change from baseline at months 1, 3, 6, 9, and
12 in key OAB symptoms. The study had no placebo control. It was found that mirabegron and
the active control, tolterodine, improved key OAB symptoms from the first measured time point
of 4 wk, and efficacy was maintained throughout the 12-mo treatment period.
Clinical experiences with solabegron. Ohlstein et al.50 evaluated the efficacy and tolerability of
solabegron in a clinical proof-of-concept study in 258 incontinent (one or more 24-h
incontinence episodes and eight or more average 24-h micturitions) women with OAB
symptoms. The study was randomized, and double-blinded and the patients were given

15
solabegron 50 mg (n = 88), 125 mg (n = 85), or placebo (n = 85) twice daily. The primary
efficacy parameter was percentage change from baseline by week 8 in the number of
incontinence episodes over 24 h. Secondary end points included actual change in micturitions
and urgency episodes per 24 h, and volume voided per micturition. Solabegron 125 mg produced
a statistically significant difference in percent change from baseline by week 8 in incontinence
episodes over 24 h when compared with placebo (p = 0.025), and showed statistically significant
reductions from baseline by weeks 4 and 8 in micturitions over 24 h and a statistically significant
increase from baseline to week 8 in urine volume voided. The drug was well tolerated, with a
similar incidence of adverse effects in each treatment group. Systolic blood pressure, diastolic
blood pressure, mean arterial pressure, or heart rate during the 24-h ambulatory measurement,
were not reported as significantly changed.
The promise of selective β3−adrenoceptor agonists in the treatment of OAB
The published evidence for mirabegron and solabegron appears to favor selective β3-AR agonists
as a new effective and well-tolerated class of drug for patients with OAB symptoms. In
comparison with antimuscarinics, only a relatively small number of patients have been studied so
far. In view of its pharmacokinetics, mirabegron has the potential for adverse drug interactions
with other CYP2D6 substrates with narrow therapeutic index. This, in addition to the effect on
the cardiovascular system, needs careful evaluation, especially in the elderly population.
Prospective evaluation of co-administration of β3-AR agonists with antimuscarinics seems
attractive for treatment of the OAB syndrome and is reasonable to examine. However, such
information is not yet available. Although available long-term data are limited, β3-AR agonists
as a class can be considered an attractive alternative to antimuscarinics for treatment of OAB.

16
References
1. Ahlquist RP. A study of the adrenotropic receptors. Am J Physiol 1948; 153:586
2. Lands AM, Arnold A, McAuliff JP et al. Differentiation of receptor systems activated by
sympathomimetic amines. Nature 1967; 214:597
3. Emorine LJ, Marullo S, Briend-Sutren MM et al. Molecular characterization of the human
beta 3-adrenergic receptor. Science 1989;245:1118
4. Ursino MG, Vasina V, Raschi E et al. The beta3-adrenoceptor as a therapeutic target: current
perspectives. Pharmacol Res 2009;59(4):221
5. Michel MC, Ochodnicky P, Summers RJ. Tissue functions mediated by beta(3)-
adrenoceptors-findings and challenges. Naunyn Schmiedebergs Arch Pharmacol
2010;382(2):103
6. Andersson KE. Pharmacology of lower urinary tract smooth muscles and penile erectile
tissues. Pharmacol Rev 1993;45(3):253
7. Nergårdh A, Boréus LO, Naglo AS. Characterization of the adrenergic beta-receptor in the
urinary bladder of man and cat. Acta Pharmacol Toxicol (Copenh) 1977;40(1):14
8. Larsen JJ. alpha And beta-adrenoceptors in the detrusor muscle and bladder base of the pig
and beta-adrenoceptors in the detrusor muscle of man. Br J Pharmacol 1979;65(2):215
9. Lindholm P, Lose G. Terbutaline (Bricanyl) in the treatment of female urge incontinence. Urol
Int 1986;41(2):158
10. Andersson KE, Chapple CR, Cardozo L et al. Pharmacological treatment of
overactive bladder: report from the International Consultation on Incontinence. Curr Opin
Urol. 2009; 19(4):380

17
11. Michel MC, Vrydag W. Alpha1-, alpha2- and beta-adrenoceptors in the urinary bladder,
urethra and prostate. Br J Pharmacol. 2006;147 Suppl 2:S88
12. Otsuka A, Shinbo H, Matsumoto R et al. Expression and functional role of beta-
adrenoceptors in the human urinary bladder urothelium. Naunyn Schmiedebergs Arch Pharmacol
2008; 377(4-6):473
13. Nomiya M, Yamaguchi O. A quantitative analysis of mRNA expression of alpha 1 and beta-
adrenoceptor subtypes and their functional roles in human normal and obstructed bladders. J
Urol 2003;170(2 Pt 1):649
14. Frazier EP, Peters SL, Braverman AS et al. Signal transduction underlying the control of
urinary bladder smooth muscle tone by muscarinic receptors and beta-adrenoceptors. Naunyn
Schmiedebergs Arch Pharmacol 2008; 377(4-6):449
15. Michel MC, Ochodnicky P, Homma Y et al. β-adrenoceptor agonist effects in experimental
models of bladder dysfunction. Pharmacol Ther. 2011; 131(1):40
16. Roosen A, Chapple CR, Dmochowski RR, et al. A refocus on the bladder as the originator of
storage lower urinary tract symptoms: a systematic review of the latest literature. Eur Urol 2009;
56(5):810
17. Kanai A, Andersson KE. Bladder afferent signaling: recent findings. J Urol 2010;
183(4):1288
18. Gillespie JI. The autonomous bladder: a view of the origin of bladder overactivity and
sensory urge. BJU Int. 2004; 93(4):478
19. Iggo A. Tension receptors in the stomach and the urinary bladder. J Physiol. 1955;128(3):593

18
20. Aizawa N, Igawa Y, Nishizawa O et al. Effects of CL316,243, a beta 3-adrenoceptor agonist,
and intravesical prostaglandin E2 on the primary bladder afferent activity of the rat. Neurourol
Urodyn 2010; 29(5):771
21. Aizawa N, Homma Y, Igawa Y. Effects of mirabegron, a novel β3-adrenoceptor agonist, on
primary bladder afferent activity and bladder microcontractions in rats compared with the effects
of oxybutynin. Eur Urol. 2012;62(6):1165
22. Biers SM, Reynard JM, Brading AF. The effects of a new selective beta3-adrenoceptor
agonist (GW427353) on spontaneous activity and detrusor relaxation in human bladder. BJU Int.
2006; 98(6):1310 2
3. Andersson KE. Bladder activation: afferent mechanisms. Urology. 2002; 59(5 Suppl 1):43
4. Birder LA, de Groat WC. Mechanisms of disease: involvement of the urothelium in bladder
5. Murakami S, Chapple CR, Akino H et al. The role of the urothelium in mediating bladder
6. Limberg BJ, Andersson KE, Aura Kullmann F et al. β-Adrenergic receptor subtype
2010;
7. Frazier EP, Mathy MJ, Peters SL et al. Does cyclic AMP mediate rat urinary bladder
8. Petkov GV. Role of potassium ion channels in detrusor smooth muscle function and
2
dysfunction. Nat Clin Pract Urol. 2007; 4(1):46
2
responses to isoprenaline. BJU Int. 2007; 99(3):669
2
expression in myocyte and non-myocyte cells in human female bladder. Cell Tissue Res.
342(2):295
2
relaxation by isoproterenol? J Pharmacol Exp Ther. 2005; 313(1):260
2
dysfunction. Nat Rev Urol. 2011; 9(1):30

19
29. Hicks A, McCafferty GP, Riedel E et al. GW427353 (solabegron), a novel, selective beta3-
adrenergic receptor agonist, evokesbladder relaxation and increases micturition reflex threshold
in the dog. J Pharmacol Exp Ther. 2007; 323(1):202
30. Michel MC, Harding SE, Bond RA. Are there functional β₃-adrenoceptors in the
human heart? Br J Pharmacol. 2011;162(4):817
31. Gauthier C, Rozec B, Manoury B et al. Beta-3 adrenoceptors as new therapeutic targets for
cardiovascular pathologies. Curr Heart Fail Rep. 2011; 8(3):184
32. Mirabegron prescribing information. Available at
http://www.us.astellas.com/docs/myrbetriq-full-pi.pdf. Accessed February 17, 2013.
33. Christ T, Molenaar P, Klenowski PM, Ravens U, Kaumann AJ. Human atrial β(1L)-
adrenoceptor but not β₃-adrenoceptor activation increases force and Ca(2+) current at
physiological temperature. Br J Pharmacol. 2011;162(4):823
34. Dessy C, Balligand JL.. Beta3-adrenergic receptors in cardiac and vascular tissues emerging
concepts and therapeutic perspectives. Adv Pharmacol. 2010;59:135
35. Takasu T, Ukai M, Sato S et al. Effect of (R)-2-(2-aminothiazol-4-yl)-4'-{2-[(2-hydroxy-2-
phenylethyl)amino]ethyl} acetanilide (YM178), a novel selective beta3-adrenoceptor agonist,
on bladder function. J Pharmacol Exp Ther. 2007; 321(2):642

20
36. Igawa Y, Michel MC. Pharmacological profile of β(3)-adrenoceptor agonists in clinical
development for the treatment of overactive bladder syndrome. Naunyn Schmiedebergs Arch
Pharmacol. 2013;386(3):177
37. Kanie S, Otsuka A, Yoshikawa S et al. Pharmacological effect of TRK-380, a novel selective
human β3-adrenoceptor agonist, on mammalian detrusor strips. Urology. 2012; 79(3):744.
38. Takusagawa S, van Lier JJ, Suzuki K et al. Absorption, metabolism and excretion of
[(14)C]mirabegron (YM178), a potent and selective β(3)-adrenoceptor agonist, after oral
administration to healthy male volunteers. Drug Metab Dispos. 2012; 40(4):815
39. Takusagawa S, Yajima K, Miyashita A et al. Identification of human cytochrome P450
isoforms and esterases involved in the metabolism of mirabegron, a potent and selective β(3)-
adrenoceptor agonist. Xenobiotica. 2012;42(10):957
40. Takusagawa S, Miyashita A, Iwatsubo T et al. In vitro inhibition and induction of human
cytochrome P450 enzymes by mirabegron, a potent and selective β3-adrenoceptor agonist.
Xenobiotica. 2012;42(12):1187
41. Eltink C, Lee J, Schaddelee M et al. Single dose pharmacokinetics and absolute
bioavailibility of mirabegron, a β3-adrenoceptor agonist for treatment of overactive bladder. Int J
Clin Pharmacol Ther. 2012;50(11):838
42. Krauwinkel W, van Dijk J, Schaddelee M. et al. Pharmacokinetic Properties of Mirabegron, a
β3-Adrenoceptor Agonist: Results From Two Phase I, Randomized, Multiple-Dose Studies in
Healthy Young and Elderly Men and Women. Clin Ther. 2012; 34(10):2144
43. Malik M, van Gelderen EM, Lee JH et al. Proarrhythmic Safety of Repeat Doses
of Mirabegron in Healthy Subjects: A Randomized, Double-Blind, Placebo-, and Active-
Controlled Thorough QT Study. Clin Pharmacol Ther. 2012; 92(6):696

21
44. Chapple CR, Yamaguchi O, Ridder A et al. Clinical proof of concept study (BLOSSOM)
shows novel Beta3 adrenoceptor agonist YM178 is effective and well tolerated in the treatment
of symptoms of overactive bladder. Eur Urol Suppl 2008; 7(3): 239
45. Chapple C, Wyndaele JJ, Van Kerrebroeck P et al. Dose-ranging study of once-daily
mirabegron (YM178), a novel selective β3-adrenoceptor agonist, in patients with overactive
bladder (OAB). Eur Urol Suppl 2010; 9(2): 249.
46. Nitti VW, Auerbach S, Martin N et al. Results of a Randomized Phase III Trial
of Mirabegron in Patients with Overactive Bladder. J Urol. 2013; 189: 1388.
47. Khullar V, Amarenco G, Angulo JC, Cambronero J, Høye K, Milsom I et al. Efficacy and
Tolerability of Mirabegron, a β(3)-Adrenoceptor Agonist, in Patients with Overactive Bladder:
Results from a Randomised European-Australian Phase 3 Trial. Eur Urol. 2013;63(2):283
48. Van Kerrebroeck P, Barkin J, Castro-Diaz D et al. Randomised, double-blind, placebo-
controlled Phase III study to assess the efficacy and safety of mirabegron 25 mg and 50 mg once
daily in overactive bladder (OAB). Presented at the International Continence Society Meeting,
Beijing, China, 2012. Available at http://www.icsoffice.org/Abstracts/Publish/134/000359.pdf.
Accessed February 17, 2013.
49. Chapple CR, Kaplan SA, Mitcheson D, Klecka J, Cummings J, Drogendijk T et al.
Randomized Double-blind, Active-controlled Phase 3 Study to Assess 12-Month Safety and
Efficacy of Mirabegron, a β(3)-Adrenoceptor Agonist, in Overactive Bladder. Eur Urol.
2013;63(2):296
50. Ohlstein EH, von Keitz A, Michel MC. A Multicenter, Double-blind, Randomized, Placebo-
controlled Trial of the β3-Adrenoceptor Agonist Solabegron for Overactive Bladder. Eur
Urol. 2012;62(5):834

22
Legends to figures
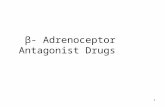
Figure 1
When activated by mechanical or chemical stimuli, the urothelium generates and releases
different agents (e.g., ATP: adenosine triphosphate, ACh: acetylcholine; PGs: prostanoids; NO:
nitric oxide) with stimulating (+) or inhibitory (-) effects on underlying structures, resulting in
modification of the activity in the afferent nerves
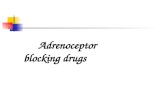
Figure 2
During bladder filling, there is no activity in the parasympathetic outflow from the bladder.
However, the myocytes have a spontaneous (autonomous) contractile activity that generates
afferent nerve activity (C-fibers and Aδ-fibers).
Figure 3
The effect on resting tone of solabegron(GW427353; 10−6 M) in a human detrusor strip showing
spontaneous activity (A), and in a ‘normal’ human detrusor strip (B). Values are expressed as the
mean (SEM) percentage of the control tone. ***P < 0.001. (from reference 22)