![Research Paper Deguelin Attenuates Allergic Airway ...Asthma is a chronic respiratory disease characterized by airway inflammation and remodeling, ... pathophysiology of asthma [4].](https://static.fdocument.org/doc/165x107/6021eed39e87047b88365ced/research-paper-deguelin-attenuates-allergic-airway-asthma-is-a-chronic-respiratory.jpg)
Rosens Asthma
18
941 CHAPTER 73 Asthma Richard M. Nowak and Glenn F. Tokarski PERSPECTIVE The word asthma is derived from the Greek ασυµα, signifying panting, and was used initially as a synonym for “breathlessness.” In 1698, Floyer published A Treatise of the Asthma, in which he attempted to differentiate asthma more clearly from other pul- monary disorders. Subsequent definitions of asthma highlight concepts of airway hyper-responsiveness, bronchospasm, and reversible airway obstruction but fail to encompass the many facets of this complex disease. The National Heart, Lung, and Blood Institute summarizes our current understanding of asthma as “a chronic inflammatory dis- order of the airways in which many cells and cellular elements play a role … this inflammation causes recurrent episodes of wheezing, breathlessness, chest tightness, and coughing … episodes are usually associated with widespread but variable airflow obstruc- tion that is often reversible either spontaneously or with treat- ment. The inflammation also causes an associated increase in the existing bronchial hyper-responsiveness to a variety of stimuli. Reversibility … may be incomplete in some patients.” 1 Asthma is thus a chronic inflammatory disease, and control of symptoms ultimately depends on ameliorating the inflammatory reaction that produces alterations in airway function and structure. Irre- versible structural airway changes occurring in response to chronic airway inflammation may influence emergency department (ED) asthma therapies. EPIDEMIOLOGY In 2008, it was estimated that 38.1 million Americans had been diagnosed with asthma by a health professional within their life- time. 2 The prevalence of asthma (defined as individuals who have been diagnosed and currently have asthma) in 2009 was 24.6 million (17.5 million adults and 7.1 million children), and the asthma attack prevalence (the number of persons who had had at least one asthma attack in the previous year) was 12.8 million, representing 52% of persons who had asthma. 2,3 Asthma is more prevalent in children than adults, in females than males, and in blacks than whites or Hispanics (Fig. 73-1). 4 Puerto Ricans have a current asthma prevalence 100% higher than non-Hispanic whites and 50% higher than non-Hispanic blacks. Females have a 33% higher prevalence than males (this pattern is reversed in children). Asthma is more prevalent in the impoverished and in those resid- ing in nonmetropolitan locales. The northeastern states have the highest asthma prevalence (Fig. 73-2). 3,5 Asthma was responsible for more than 1.75 million ED visits and 456,000 hospitalizations in the United States in 2007 (Fig. 73-3). 3 Females were 1.08 times more likely to require hos- pitalization and had a death rate 1.29 times greater than males. African Americans had an ED visit rate 3.32 times higher, a hos- pitalization rate 2.22 times higher, and a death rate 1.93 times higher than whites. Children (ages 0-17) accounted for more than 640,000 ED visits and had a hospitalization rate 1.23 times higher than adults. Decreases in hospitalization rates have been noted in those older than 45 years from the late 1980s into the early 2000s. 6 Between 1995 and 2006, hospital discharges for asthma decreased by 13%. The only age group that did not experience a decrease in hospital discharge rates was patients older than 65 years. 2 The estimated financial burden of asthma totaled $20.7 billion in the United States in 2010, with approximately 75% attributable to direct costs (hospital care and physician services). 2 Prescription drugs represented the highest single direct cost at $5.9 billion. Less than 20% of asthma patients account for 80% of the direct costs. 7 Indirect costs attributable to asthma are reflected by decreased productivity. In 2008, asthma accounted for an estimated 14.2 million lost work days and 14.4 million lost school days. In those not currently employed, 22 million days of housework or other activities were missed. 3,8 Asthma ranks within the top 10 prevalent conditions causing limitation of activity. The United States has one of the lowest rates of asthma mortal- ity in the world. 9 A downward trend in asthma-related deaths has occurred since 2003, when 4055 deaths from asthma were reported 10 ; 3447 deaths from asthma occurred in 2007, and 3395 in 2008. 11 Despite these positive indicators, asthma mortality is 44% higher in females than in males and three times higher in blacks than in whites. 2 Asthma death rates are higher in Puerto Rico than in the U.S. general population. 12 Deaths from asthma are rare in children. 3 Developed nations have higher rates of asthma, which suggests that urbanization and westernization are correlated with increased asthma prevalence. It is interesting to note that migrants who move from an area of low asthma prevalence to an area of high asthma prevalence assume an increased asthma prevalence, sug- gesting that environmental factors play a role. Urban areas in the United States (New York City, Los Angeles, and Chicago) have high mortality rates associated with asthma, indicating that poverty and lack of access to medical care may also be major determinants of asthma complications. Factors that contribute to asthma morbidity and mortality include inadequate patient and physician assessment of an acute episode resulting in undertreatment; overuse of prescribed or over-the-counter medications leading to delays in seeking treat- ment; failure of physicians to consider previous ED visits, hospi- talizations, or life-threatening episodes of asthma; and failure to initiate corticosteroid therapy early in the course of an exacerba- tion. Socioeconomic factors, environmental influences, and over- reliance on emergency facilities for all asthma care are also contributing factors. Initiatives to educate physicians and patients Section Two PULMONARY SYSTEM
-
Upload
papermate9293 -
Category
Documents
-
view
216 -
download
2
description
Asthma
Transcript of Rosens Asthma
-
941
CHAPTER 73
AsthmaRichard M. Nowak and Glenn F. Tokarski
PERSPECTIVE
The word asthma is derived from the Greek , signifying panting, and was used initially as a synonym for breathlessness. In 1698, Floyer published A Treatise of the Asthma, in which he attempted to differentiate asthma more clearly from other pul-monary disorders. Subsequent definitions of asthma highlight concepts of airway hyper-responsiveness, bronchospasm, and reversible airway obstruction but fail to encompass the many facets of this complex disease.The National Heart, Lung, and Blood Institute summarizes our
current understanding of asthma as a chronic inflammatory dis-order of the airways in which many cells and cellular elements play a role this inflammation causes recurrent episodes of wheezing, breathlessness, chest tightness, and coughing episodes are usually associated with widespread but variable airflow obstruc-tion that is often reversible either spontaneously or with treat-ment. The inflammation also causes an associated increase in the existing bronchial hyper-responsiveness to a variety of stimuli. Reversibility may be incomplete in some patients.1 Asthma is thus a chronic inflammatory disease, and control of symptoms ultimately depends on ameliorating the inflammatory reaction that produces alterations in airway function and structure. Irre-versible structural airway changes occurring in response to chronic airway inflammation may influence emergency department (ED) asthma therapies.
EPIDEMIOLOGY
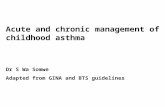
In 2008, it was estimated that 38.1 million Americans had been diagnosed with asthma by a health professional within their life-time.2 The prevalence of asthma (defined as individuals who have been diagnosed and currently have asthma) in 2009 was 24.6 million (17.5 million adults and 7.1 million children), and the asthma attack prevalence (the number of persons who had had at least one asthma attack in the previous year) was 12.8 million, representing 52% of persons who had asthma.2,3 Asthma is more prevalent in children than adults, in females than males, and in blacks than whites or Hispanics (Fig. 73-1).4 Puerto Ricans have a current asthma prevalence 100% higher than non-Hispanic whites and 50% higher than non-Hispanic blacks. Females have a 33% higher prevalence than males (this pattern is reversed in children). Asthma is more prevalent in the impoverished and in those resid-ing in nonmetropolitan locales. The northeastern states have the highest asthma prevalence (Fig. 73-2).3,5
Asthma was responsible for more than 1.75 million ED visits and 456,000 hospitalizations in the United States in 2007 (Fig. 73-3).3 Females were 1.08 times more likely to require hos-pitalization and had a death rate 1.29 times greater than males.
African Americans had an ED visit rate 3.32 times higher, a hos-pitalization rate 2.22 times higher, and a death rate 1.93 times higher than whites. Children (ages 0-17) accounted for more than 640,000 ED visits and had a hospitalization rate 1.23 times higher than adults. Decreases in hospitalization rates have been noted in those older than 45 years from the late 1980s into the early 2000s.6 Between 1995 and 2006, hospital discharges for asthma decreased by 13%. The only age group that did not experience a decrease in hospital discharge rates was patients older than 65 years.2 The estimated financial burden of asthma totaled $20.7 billion in the United States in 2010, with approximately 75% attributable to direct costs (hospital care and physician services).2 Prescription drugs represented the highest single direct cost at $5.9 billion. Less than 20% of asthma patients account for 80% of the direct costs.7 Indirect costs attributable to asthma are reflected by decreased productivity. In 2008, asthma accounted for an estimated 14.2 million lost work days and 14.4 million lost school days. In those not currently employed, 22 million days of housework or other activities were missed.3,8 Asthma ranks within the top 10 prevalent conditions causing limitation of activity.The United States has one of the lowest rates of asthma mortal-
ity in the world.9 A downward trend in asthma-related deaths has occurred since 2003, when 4055 deaths from asthma were reported10; 3447 deaths from asthma occurred in 2007, and 3395 in 2008.11 Despite these positive indicators, asthma mortality is 44% higher in females than in males and three times higher in blacks than in whites.2 Asthma death rates are higher in Puerto Rico than in the U.S. general population.12 Deaths from asthma are rare in children.3
Developed nations have higher rates of asthma, which suggests that urbanization and westernization are correlated with increased asthma prevalence. It is interesting to note that migrants who move from an area of low asthma prevalence to an area of high asthma prevalence assume an increased asthma prevalence, sug-gesting that environmental factors play a role. Urban areas in the United States (New York City, Los Angeles, and Chicago) have high mortality rates associated with asthma, indicating that poverty and lack of access to medical care may also be major determinants of asthma complications.Factors that contribute to asthma morbidity and mortality
include inadequate patient and physician assessment of an acute episode resulting in undertreatment; overuse of prescribed or over-the-counter medications leading to delays in seeking treat-ment; failure of physicians to consider previous ED visits, hospi-talizations, or life-threatening episodes of asthma; and failure to initiate corticosteroid therapy early in the course of an exacerba-tion. Socioeconomic factors, environmental influences, and over-reliance on emergency facilities for all asthma care are also contributing factors. Initiatives to educate physicians and patients
Section TwoPULMONARY SYSTEM
-
942 PART III Medicine and Surgery / Section Two Pulmonary System
Figure 73-1. Asthmaprevalencepercentagesbyage,sex,andrace,UnitedStates,2008.(AdaptedfromNationalHealthInterviewSurvey,NationalCenterforHealthStatistics,CentersforDiseaseControlandPrevention.www.cdc.gov/asthma/asthmadata.htm.)
Age
Child
9.4
%
Adul
t 7.3
%
Sex
Mal
e 7.
1%
Fem
ale
8.5%
Race/Ethnicity
Whi
te 7
.8%
Blac
k 10
.3%
His
pani
c 5.
8%
CURRENT ASTHMA PREVALENCE PERCENTS BYAGE, SEX, AND RACE, UNITED STATES, 2008
0
8
6
4
2
10
12
Figure 73-2. Prevalenceofasthmabyselectedcharacteristics,UnitedStates,2009.Note:Estimates(exceptage-groupspecificestimates)areage-adjustedtotheyear2000U.S.standardpopulation.(AdaptedfromAkinbamiLJ,MoormanJE,LiuX:Asthmaprevalence,healthcareuse,andmortality:UnitedStates2005-2009.Nationalhealthstatisticsreports:no32.Hyattsville,Md,NationalCenterforHealthStatistics,2011.)
0 2 4 6 8 10 12 14 16 18
7.0
Percent
Male9.3
Total current asthmaprevalence: 8.2%
Female
9.60-17 years18 years and older
White11.1Black
8.8American Indian or Alaska Native5.3Asian
9.3Northeast8.8Midwest
SouthWest
11.6Below poverty8.5100% 199% poverty
200% poverty and above
8.1Metropolitan8.7Nonmetropolitan
8.2Non-Hispanic white11.1Non-Hispanic black
6.3Total Hispanic16.6Puerto Rican
4.9Mexican
7.57.7
7.7
7.8
7.3
PRINCIPLES OF DISEASE
Pathophysiology
A variety of airway alterations occur in asthma, but airway inflam-mation is the final common pathway limiting airflow. Allergens and nonallergic stimuli (e.g., exercise; aspirin-induced and menstrual-related asthma) induce bronchoconstriction via release of mediators and metabolic products from inflammatory cells. Compared with healthy individuals, patients with asthma show bronchial hyper-reactivity (hyper-responsiveness) in response to bronchoconstricting stimuli (e.g., methacholine). Edema, inflam-mation, mucous production, and airway smooth muscle hypertro-phy contribute to bronchoconstriction and hyper-reactivity and further airway obstruction and airflow limitation. Permanent structural airway changes (airway remodeling) may contribute to increased airway obstruction and hyper-responsiveness and decrease the response to therapy. The interaction of these features determines the clinical manifestations and severity of asthma and significantly influences the response to therapy.Evidence that inflammation is a component of asthma physiol-
ogy was initially derived from autopsy findings in patients with fatal asthma. The airways revealed infiltration by neutrophils, eosinophils, and mast cells and the presence of subbasement membrane thickening, loss of epithelial cell integrity, goblet cell hyperplasia, and mucous plugs. Antemortem bronchial biopsy findings in patients with even mild degrees of asthma also dem-onstrate inflammatory changes in the central and peripheral airways that correlate with disease severity.13 Inflammatory and
about asthma pathophysiology, monitoring, and therapy (e.g., National Asthma Education and Prevention Program [NAEPP], Global Initiative for Asthma [GINA], and Healthy People 2010) may be in part responsible for the moderation of asthma morbid-ity and mortality rates.
-
Chapter 73 / Asthma 943
cells release proteases that damage airway epithelium and contrib-ute to airway remodeling. Tumor necrosis factor alpha (TNF-) is a potent bronchoconstrictor produced by mast cells. In chronic asthma there is evidence of persistent mast cell activation resulting in continuous mediator release, cytokine production, and ampli-fication of airway inflammation.18 The presence of mast cells in airway smooth muscle contributes to propagation of the inflam-matory response, persistent bronchoconstriction, and over time, airway smooth muscle hypertrophy that plays a role in airway remodeling.19,20
Eosinophils are major effector cells in asthma, and their pres-ence is evidence of the allergic nature of this disease. Increased numbers of eosinophils are found in the airways of most but not all asthmatics.21 Eosinophils contain granules that release inflam-matory mediators, including major basic protein, eosinophil cat-ionic protein, and eosinophil peroxidase. Major basic protein is a potent bronchoconstrictor. Eosinophil cationic protein increases airway mucous production and causes histamine release from mast cells. Leukotrienes (LTs) produced by eosinophils are bron-choconstrictors and promote the secretion of thick viscid mucus, leading to airway plugging, LTs also enhance airway vascular per-meability, leading to airway edema. Platelet-activating factor, superoxides, and free radicals produced by eosinophils also cause bronchospasm and bronchial tissue injury. Eosinophilic mediators damage and cause desquamation of the airway epithelium, expose nerve endings, provide submucosal access for inflammatory cells and mediators, and negate epithelial cell regulation of the inflammatory process.Although eosinophils appear to be important in airway allergic
and inflammatory processes, eosinophilia is not universal in asth-matics. Confounding the role of the eosinophil are studies with antiIL-5 that significantly reduced sputum and blood eosino-philia but did not significantly affect asthma control.22,23 Clinically, eosinophils are important biomarkers in predicting response to corticosteroid therapy. Steroid-nave asthmatics with sputum eosinophilia have a good response to inhaled corticosteroid (ICS) therapy, whereas those without sputum eosinophilia do not.24-26 Suppressing sputum eosinophilia with oral or inhaled steroids reduces the number of acute exacerbations in patients with severe asthma.17,27
Mediator and cytokine release from mast cells, eosinophils, and other airway inflammatory cells (macrophages, lymphocytes, basophils, neutrophils) contributes to prolonged bronchial smooth muscle spasm, edema, and mucous production (the late asthmatic response). Ongoing synthesis and release of cytokines, prostaglan-dins (PGs), and LTs (Fig. 73-4) are responsible for propagation and intensification of airway inflammation and disruption of the airway epithelial border.28 Airway epithelial cells are more than a passive barrier and are recognized to produce proinflammatory mediators. Tight junctions between airway epithelial cells are altered in asthma, which may allow access of allergens, microbes, and viruses into the airway submucosa. Inflammatory cells, medi-ators, and airway viruses can directly damage the epithelial barrier and stimulate airway epithelial cells to produce inflamma-tory mediators. Abnormal repair processes may further airway inflammation and obstruction and contribute to airway remodel-ing.29,30 Nitric oxide (NO) produced by airway epithelial cells in the large and small airways and alveoli is a reflection of ongoing airway inflammation. Measurements of fractional exhaled nitric oxide (FENO) may prove useful for monitoring the response to asthma therapy.31
Airway remodeling refers to the persistent structural changes in airways seen in patients with asthma and is caused by the presence of repetitive or chronic airway inflammation. Microscopic remod-eling features include epithelial thickening, subepithelial fibrosis, mucous gland metaplasia, increases in airway smooth muscle, angiogenesis, and loss of cartilage integrity.32 Airway remodeling
Figure 73-3. Relativeburdenofasthmahealthcareuseandmortality:UnitedStates,annualaverage2005-2007.Note:Arateratioof1.0(dashed line)indicatesequalratesbetweenthegroupsbeingcompared.(AdaptedfromAkinbamiLJ,MoormanJE,LiuX:Asthmaprevalence,healthcareuse,andmortality:UnitedStates2005-2009.Nationalhealthstatisticsreports:no32.Hyattsville,Md,NationalCenterforHealthStatistics,2011.)
0 1 2 3 4Rate ratio
0.98
Black vs. white 3.322.221.93
1.77
-
944 PART III Medicine and Surgery / Section Two Pulmonary System
Figure 73-4. Thephysiologicmechanismofasthma.DC,dendriticcell;MC,mastcell;Th,T-helper;TLR,toll-likereceptor.(FromMurphyDM,OByrnePM:Recentadvancesinthepathophysiologyofasthma.Chest137:1417,2010.)
Remodeledand
inflamedairway
Cellattraction
Secondary Th2response
T cells andmediators
T-cellstimulatedeosinopoiesis
Antigentransport by
dendritic cellsAntigen
presentation
Regionallymph node
Distribution of antigenspecific T cells
Delivery ofinflammatory
cells andprogenitors
Immediatesmooth muscle
contraction
Airwaylumen
Lamina propria
Epithelium
Smoothmuscle
Systemicprocesses
DC
Allergen Virus
MC
TLR
occurs very early in asthma (childhood) and may precede clinical symptoms.14,33 Remodeling features are prominent in patients with severe asthma.34 Basement membrane thickening may be protective by preventing inflammatory cells and proteins from entering the airway submucosa through a damaged epithelium; simultaneously, this process may be counterproductive by reduc-ing the elasticity of the small airways. Airway remodeling may explain the resistance to therapy observed in patients with pro-longed asthma histories and the decline in pulmonary function noted with age. Airway remodeling induced by chronic inflamma-tion may lead to the development of chronic irreversible airflow limitation and increased asthma mortality.The clinical implications of the immune and inflammatory
nature of the early and late asthmatic responses are crucial because therapy may be directed differently toward each phase. Mast cell stabilizers (e.g., beta-agonists) are more effective in the early asthmatic response but are of less use later in the course of an exacerbation. Anti-inflammatory therapy (e.g., corticosteroids, LT antagonists) is more effective in the late asthmatic response. Inter-ference with or inhibition of cytokine activities, suppression of chronic inflammation, and modulation of airway remodeling are potential therapeutic targets.
Miscellaneous Situations
Aspirin-exacerbated respiratory disease (AERD) was first described more than 100 years ago. Clinically, AERD includes the tetrad of nasal polyps, eosinophilic sinusitis, asthma, and sensitivity to cyclooxygenase (COX)-1 inhibitor drugs (e.g., aspirin).The prevalence of AERD is 21% in adults with asthma and 5% in children with asthma.35 Ethnic and familial associations are rare,
and it occurs more frequently in females.36 Nonsteroidal anti-inflammatory drugs (NSAIDs) also precipitate AERD. AERD is a common precipitant of life-threatening asthma; one survey notes that 25% of asthmatics who require mechanical ventilation have AERD.37
Clinically, most patients with AERD develop symptoms in the third decade (average age of onset is 34 years), frequently after a viral respiratory illness. A previous history of asthma or allergic rhinitis may be noted, but many patients have no prior respiratory disease. Chronic rhinitis, nasal polyps, and anosmia develop and are often followed by chronic pansinusitis. Bronchial asthma and sensitivity to aspirin (acetylsalicylic acid [ASA]) then results. After ingestion of aspirin or a nonsteroidal drug, acute asthma symp-toms occur within 3 hours, usually accompanied by profuse rhinorrhea, conjunctival injection, periorbital edema, and occa-sionally a scarlet flushing of the head and neck.38
The pathogenesis of AERD is detailed in Figure 73-5. ASA inhibits COX,39 of which two isoforms have been identified. COX-1 produces PGs that are involved in normal physiologic maintenance of renal function, gastric mucosal integrity and hemostasis, and inflammatory states. COX-2 is not expressed in normal physiologic circumstances but produces PGs only in response to inflammatory stimuli. COX is necessary for the production of PGE2 in mast cells and eosinophils. PGE2 has a stabilizing effect on these cells via blockade of the enzyme 5-lipoxygenase and the subsequent production of proinflamma-tory LTs (LTC4, LTD4, and LTE4). AERD occurs as a result of ASA inhibition of COX and a decrease in the production of PGE2. The end results are an increase in production of LTs, some of which are potent bronchoconstrictors, and inflammatory mediator release from mast cells and eosinophils. Most patients with AERD
-
Chapter 73 / Asthma 945
Prophylaxis for EIA with warm-up and a short-acting inhaled beta-agonist is the therapy of choice. Pretreatment with cromolyn, LT antagonists (montelukast), and inhaled parasympatholytics is also effective.42,43 Breathing through the nose may allow warming and humidification of cool dry air during exercise. Long-acting beta-agonists are usually effective, but tachyphylaxis and loss of efficacy may occur if these agents are used regularly.44
Menstruation-associated asthma affects up to 40% of asthmatic women yet receives little emphasis in asthma treatment guide-lines.1 The ratio of female-to-male asthma prevalence increases dramatically after puberty, and health care for asthma increases in the perimenstrual phase. Perimenstrual reductions in peak expira-tory flow rates (PEFRs) of 35 to 80% are reported. Fluctuations in estrogen and progesterone levels are postulated as causal factors.45,46 Estradiol inhibits eosinophil degranulation and sup-presses LT activity; estrogen withdrawal in the luteal phase may enhance these actions. Progesterone may also have bronchodilator and anti-inflammatory activity, and the rapid decline in proges-terone levels before menstruation may contribute to increased bronchospasm. Beneficial therapies for perimenstrual asthma include LT antagonists, long-acting beta-agonists, and oral contraceptives.46,47
Psychological factors may precipitate bronchospasm. Panic dis-order, generalized anxiety disorder, and mood disorders are more common in asthmatics than the general population. An associa-tion between asthma, anxiety, and depression is noted. The mech-anisms of bronchospasm associated with chronic stress may be related to the cholinergic nervous system or the hypothalamus-pituitary-adrenal axis, resulting in decreased cortisol secretion.48,49 Compliance may be adversely affected by psychological factors. Relaxation as a therapy for asthma has inconsistent effects; hyp-nosis may be beneficial.50
Genetics and Asthma
It is likely that asthma is not a single disease but a syndrome with various phenotypes. The natural history of asthma is highly vari-able. Most asthma begins in childhood and resolves with age. Remissions of variable duration may occur, whereas others experience progressive severe disease. Many aspects of asthma (e.g., atopy susceptibility, IgE levels, degree of bronchial hyper-reactivity, asthma severity) have identifiable genetic associations. Family history of both atopy and asthma are associated with lower rates of remission. Environmental influences (e.g., allergens, pol-lutants, tobacco, and occupational exposures) are associated with asthma, and the interaction of genetic variability and environ-mental factors may allow prediction of future disease risk, expres-sion, and severity.51,52
Pathology
The pathology of the asthmatic airway reflects the inflammatory process described earlier. Mucous gland hyperplasia and viscous mucous plugs in the smaller airways are present. Airway secretions reveal increased numbers of inflammatory cells. Airway epithelial damage and remodeling are evident. In contrast to patients with mild to moderate asthma, patients with acute severe asthma have extensive mucous hyperplasia, subepithelial thickening, and infil-tration of inflammatory cells (particularly eosinophils).53
Necropsies of patients with status asthmaticus reveal grossly inflated lungs that may fail to collapse on opening of the pleural cavities. Histologic examination reveals luminal plugs consisting of inflammatory cells, desquamated epithelial cells, and mucus. Marked thickening of the airway basement membrane, submuco-sal inflammatory cells, increased deposition of connective tissue, mucous gland hyperplasia, and hypertrophy of airway smooth muscle are also observed. Reports of slow-onset asthma fatalities
benefit from anti-LT treatment. These agents block synthesis of LTs (e.g., zileuton) or block specific LT receptors (e.g., zafirlukast, montelukast). Desensitization with slowly increased doses of oral aspirin may be used when aspirin avoidance is not possible (e.g., in patients with cardiovascular disease).39
COX-2 inhibitors have the advantage of inhibiting inflamma-tion without renal, gastrointestinal, or hematologic side effects. AERD is not reported after administration of COX-2 inhibitors. These agents provide a potentially safe alternative for treatment of inflammatory conditions in patients with AERD.39,40
Acetaminophen is a poor COX inhibitor. Most patients with AERD can tolerate up to 500 mg of acetaminophen safely, but 28 to 34% experience mild respiratory reactions when administered 1000 to 1500 mg. Reactions to acetaminophen tend to be milder than those to NSAIDs.39
Exercise-induced asthma (EIA) has been recognized since the first Olympic Games. It occurs in 5 to 20% of the general popula-tion, 30 to 70% of elite winter and summer endurance athletes, and up to 90% of patients with persistent asthma.41 Atopy is strongly associated with EIA, and up to 40% of patients with allergic rhinitis have EIA. EIA may be another reflection of chronic airway inflammation. Clinically, EIA is usually preceded by 3 to 8 minutes of exercise. Peak symptoms usually occur 8 to 15 minutes after exercise is complete and then begin to remit spontaneously; recovery occurs within 60 minutes.The cause of EIA remains unclear. In the osmotic hypothesis,
airway cooling leads to mucosal drying and increased surface osmolality that causes mast cell degranulation and release of inflammatory mediators. The thermal hypothesis suggests that airway cooling during exercise followed by rapid rewarming after exercise causes airway vascular congestion and increased perme-ability, resulting in airway edema and obstruction. Another exercise-specific factor is autonomic deregulation associated with prolonged high-intensity physical training. The predominantly parasympathetic drive of athletes (evidenced by low heart rates) may also increase bronchomotor tone and increase the risk of EIA.41
Figure 73-5. Mechanismofaspirin-exacerbatedrespiratorydisease.Inhibitionofcyclooxygenase(COX)decreasesproductionofprostaglandinE2(PGE2).PGE2hasaninhibitoryeffectonleukotriene(LT)synthesis.5-HPETE,5-hydroperoxyeicosatetraenoicacid.
Arachidonicacid Aspirin
NegativeCOX
Negative5-Lipoxygenase
PGE2
Stabilizingeffect
Mast cells Eosinophils
LTA4
LTC4
LTD4
LTE4
5-HPETE
Inflammation
-
946 PART III Medicine and Surgery / Section Two Pulmonary System
severe airway obstruction, it decreases or vanishes because air movement velocity is insufficient to produce sound.Many asthmatics report symptoms of gastroesophageal reflux
that may cause airway narrowing through a vagally mediated pathway or microaspiration. Proton pump inhibitor therapy decreases asthma symptoms in these patients. Approximately 80% of patients with asthma have symptoms of rhinitis. Approximately 5 to 15% of patients with perennial rhinitis have asthma, and control of sinonasal inflammation can lead to asthma improve-ment. Overweight (body mass index [BMI] of 25 kg/m2 or higher) asthmatics have poorer asthma control, higher admission rates, and a greater risk of complications, possibly secondary to a differ-ence in the perception of dyspnea or in response to asthma con-troller agents.60,61 In addition, obese patients have different bronchial and systemic inflammatory characteristics and a specific pattern of pulmonary function changes, suggesting a different asthma phenotype.62
One third of patients who come to the ED with acute asthma are current cigarette smokers, and these patients have poorer asthma control and greater acute care needs than lifelong non-smokers or former smokers.63,64 African Americans with acute asthma have lower flow rates and more potentially life-threatening episodes than whites, but they respond equally well to albuterol.65 There are no racial disparities in inpatient asthma care when com-paring whites, blacks, and Hispanics.66
Lastly, as asthma can appear at any age, including the ninth decade, wheezing and dyspnea may be misascribed by both patients and physicians to heart failure, bronchitis, chronic obstructive pulmonary disease (COPD), occupational lung disease, or poor exercise capacity.
Historical Components
Slow-onset asthma with progressive deterioration over a period of at least 6 hours (usually days) occurs in over 80% of cases. This type has a female predominance, is triggered by upper respiratory tract infections, and has an airflow inflammation mechanism that results in a slower response to treatment. Sudden-onset asthma with rapid deterioration in less than 6 hours occurs in less than 20% of cases. This type has a male predominance, is triggered by respiratory allergens, exercise, and psychosocial stress, and has a bronchospastic cause resulting in more severe airway obstruction with a faster response to therapy.67
Risk factors for death from asthma are important to determine and are listed in Box 73-1.1,68-71 In urban areas, heroin and cocaine abuse are commonly associated with life-threatening asthma requiring noninvasive positive-pressure ventilation (NIPPV) or intubation in the ED.70,71
The brief history pertinent to the current exacerbation should include onset and possible triggers, severity of symptoms espe-cially as compared with previous exacerbations, and other comor-bidities (especially those that may be worsened by systemic corticosteroids such as diabetes, peptic ulcer, hypertension, and psychosis). In addition, all current asthma medications should be noted, including times and amounts recently used, and any poten-tial asthma exacerbators such as aspirin or NSAIDs, beta-blockers (including topical agents used for glaucoma), and angiotensin-converting enzyme inhibitors. Cardioselective and nonselective beta-blocker use increases hospitalizations and ED visits.72
Physical Assessment
Patients with mild acute asthma usually speak in sentences, those moderate asthma in phrases, and those with severe asthma in words. Although alterations in mentation indicate severe asthma, restlessness and agitation do not reliably indicate hypoxia or hypercapnia. Patients who sit upright have severe airway
reveal greater bronchial eosinophilia and basement membrane thickening when compared with rapid-onset fatal asthma.54,55 Reports of rapid-onset fatal asthma describe less mucus in the airway lumens, suggesting that terminal events may be dominated by bronchoconstriction without excessive luminal plugging; however, an alternative view is that dry airways are more reflec-tive of postmortem tissue processing.55
CLINICAL FEATURES
National and International Guidelines for the Diagnosis and Management of Asthma
In response to the increasing prevalence of asthma, many coun-tries publish guidelines. Some of these, including NAEPP (National Institutes of Health [NIH]) Expert Panel Report 3 (EPR-3), devote specific portions to the management of acute exacerbations of asthma.1 A task force of physicians representing the American Academy of Asthma, Allergy and Immunology, the American Academy of Emergency Medicine, and the American Thoracic Society (ATS) have summarized the aspects of the EPR-3 that are relevant for the ED and have developed evidence-based recom-mendations for acute care gaps in the NIH national guidelines. These include (1) use of noninvasive ventilation, (2) use of intuba-tion and mechanical ventilation, (3) appropriate discharge medi-cations, and (4) techniques for ensuring proper follow-up after an ED visit. These additional acute care recommendations were simultaneously published in 2009 in supplemental issues of Journal of Allergy and Clinical Immunology (volume 124, issue 2), Journal of Emergency Medicine (volume 37, issue 2), and Proceed-ings of the American Thoracic Society (volume 6, issue 4). The EPR-3 and task force recommendations are graded from levels A through D based on the strength of the scientific evidence.ED concordance with the EPR-3 treatment recommendations
is reported as moderate, with significant regional variations in quality of care.56 In addition, ED overcrowding is associated with longer lengths of stay for acute asthma exacerbations.57
Symptoms
Most patients with acute asthma have a constellation of symptoms, including cough, dyspnea, and wheezing. Cough often begins early in the attack, may be the sole manifestation of the disease in cough-variant asthma and elder patients, can be associated with sputum production, and is probably the result of subepithelial vagal stimulation. Nocturnal worsening is common, with most patients reporting cough or wheeze at least once per week. Night-time mortality is higher than in the general population.Although increased airway resistance, diminished flow rates,
and increased bronchial hyperactivity are contributing factors, asthmatic patients who come to the ED with nocturnal asthma attacks have disease severity similar to that of other asthmatics. Up to 40% of asthmatic women experience premenstrual worsen-ing of symptoms, which peak 2 to 3 days before menses and are associated with more severe disease; ED visits increase during the preovulatory and perimenstrual intervals.58
There are interindividual differences in the dyspnea perceived by asthmatic subjects for the same level of airway narrowing. This difference results in poor correlation of symptoms with airway obstruction as determined by pulmonary function testing (PFT), both chronically and on presentation to the ED. Patients with a blunted perception of dyspnea (the poor perceivers) have more ED visits, hospitalizations, and near-fatal and fatal asthma attacks.59
Wheezing reflects air movement velocity and turbulence, and its intensity varies according to the radius of the bronchi. With
-
Chapter 73 / Asthma 947
assessments in the ED use single-patient-use portable peak flow meters because PEFR is easier to measure. The identical device should be used to assess then reassess an individual patient, and different portable meters should not be used interchangeably. Lastly, the FEV1 and PEFR measurements are not interchangeable in assessing acute airway obstruction, which is not addressed in all management guidelines. Although absolute PFT measurements can be used, percentage of predicted performance (% predicted) values are preferable to account for age (now to age 85), sex, and height.
Arterial Blood Gas Analysis
Equilibration of oxyhemoglobin saturation occurs within 3 to 4 minutes of initiation or alteration of supplemental oxygen during an acute asthma attack. Stimulated hyperventilation leads to a modest fall in the partial pressure of carbon dioxide in arterial blood (Paco2). As airway obstruction increases, the Paco2 normal-izes (PFT values 15-25% predicted) and then increases (PFT values
-
948 PART III Medicine and Surgery / Section Two Pulmonary System
DIFFERENTIAL CONSIDERATIONS
See Box 73-2. Of note, vocal cord dysfunction may mimic or coexist with asthma and is gaining recognition as a common cause of respiratory symptoms often misdiagnosed as steroid-refractory asthma.79
MANAGEMENT OF ACUTE EXACERBATIONS
Home and First-Responder Strategies
Subacute lack of asthma control (more than four outpatient visits or more than five short-acting beta2-agonist prescriptions per year) is associated with increased risk of acute asthma exacerba-tion.80 Thus patients should be provided a plan to monitor their symptoms, signs, and PEFR to recognize early deterioration in the event of an exacerbation. Early therapy can prevent progression to severe attacks. Home management includes increased use of inhaled beta2-agonists, early administration of systemic cortico-steroids (not simply doubling the dose of current ICSs), and spe-cific instructions regarding emergency care.1 Emergency medical service providers should provide albuterol inhalation therapy by protocol, and basic emergency medical technicians can be autho-rized to administer the patients own inhaler.81,82 Further studies are needed to determine whether paramedics should be trained to administer continuous positive airway pressure ventilation in asthmatics with severe respiratory failure to decrease tracheal intubation and mortality rates.83
Management of Acute Asthma in the Emergency Department
The rapidity of reversal of the acute airflow obstruction is directly predictive of the outcome. Effective bronchodilation often results in a decreased need for hospitalization with significant cost
admission have a higher likelihood of radiographically identifi-able, unsuspected, clinically significant pulmonary complications of asthma (15% of cases).
Electrocardiogram and Cardiac Monitoring
The electrocardiogram (ECG) is selectively helpful in assessing patients with chest pain or a history of significant cardiovascular disease, in whom the asthma attack may be a physiologic stress test. In patients with severe asthma, the ECG may show a right ventricular strain pattern that reverses with improvement in airflow. Older patients, especially those with coexistent heart disease or with severe exacerbation, could require continuous cardiac monitoring to detect dysrhythmias. All patients with severe hypoxemia, and those for whom intubation is contem-plated, should receive continuous cardiac monitoring.
Future Monitoring Strategies
Noninvasive monitoring of bronchial inflammation may custom-ize the ED assessment of acute asthma. This may include measure-ment of biologic biomarkers, such as cytokine profiles in the blood, evaluation of LTE4 in the urine, and the monitoring of exhaled pentane, hydrogen peroxide, NO, or carbon monoxide levels. Of these measurements, exhaled NO, a marker of airway inflammation, shows the most promise, as studies show that FENO can be measured in the ED with good reproducibility, and levels measured after 6 hours of care are associated with better asthma control after discharge.77,78
Assessment Summary
The severity of airflow obstruction cannot be accurately judged by patients symptoms, physical examination findings, and labora-tory test results. Serial measurements of airflow obstruction (FEV1 or PEFR) are key components of disease assessment and response to therapy (Table 73-1).
FACTOR SEVERE ASTHMA (FEV1 20, therefore nondiscriminating
Pulsus paradoxus (mm Hg) 10 but may be absent with equally severe asthma in 50% of cases
Pulse rate 120, respiratory rate 20, pulsus paradoxus 10
If all three abnormal, 90% with severe asthma, but only 40% with FEV1
-
Chapter 73 / Asthma 949
MILD TO MODERATE SEVERE
FEV1 or PEFR (% predicted/personal best) 40% Unable or
-
950 PART III Medicine and Surgery / Section Two Pulmonary System
could evolve as acute rescue medications with extended length of action (12 hours) and similar safety profiles.103,104 The controver-sies regarding the safety of regular use of short-acting beta-agonists extend to the long-acting classes. The U.S. Food and Drug Admin-istration (FDA) has changed the labeling for LABAs to contrain-dicate their chronic use in patients of all ages without concomitant use of an asthma controller medication such as an ICS.105
Corticosteroids
Corticosteroids inhibit recruitment of inflammatory cells and release of proinflammatory mediators and cytokines. Corticoste-roids activate cytoplasmic glucocorticoid receptors to regulate the transcription of certain target genes, resulting in the synthesis of new proteins.Despite decades of corticosteroid use, controversy persists
regarding the types and quantities required to induce a rapid remission, the time needed for drug action, the route of adminis-tration, the existence of dose-response effects, and the determina-tion of which patient populations respond to this therapy.106
Systemic Corticosteroids in the Emergency Department. Cortico-steroids are indicated for all patients with moderate to severe attacks or those experiencing an incomplete response to initial beta-agonist therapy. In addition, early systemic corticosteroids should be considered for patients who are taking oral corticoste-roids or ICSs, have relapsed after a recent exacerbation, or have prolonged symptoms. Steroid effects begin within hours (not minutes) in acute asthma and peak at about 24 hours. Use of systemic steroids speeds the resolution of airflow obstruction, reduces the rate of relapse, and may decrease admissions in severe but not in mild to moderate attacks.1,106 The PEFR may improve within 2 hours of steroid therapy in those not responding to initial albuterol inhalation.107
Many studies clearly demonstrate that oral corticosteroids are as beneficial as intravenous corticosteroids in the ED. The initial oral dose is usually 60 mg of prednisone. If intravenous methyl-prednisolone is used, the dose is 40 to 80 mg/day in one or two divided doses until the switch to oral therapy or until PEFR reaches 70% of predicted or personal best.Continuing therapy with oral prednisone or prednisolone is
given in an adult dose of 40 to 80 mg/day, usually as a single dose. No study demonstrates the superiority of intravenous cor-ticosteroids over oral preparations. Oral steroid therapy is pre-ferred unless the patient is very ill, is unable to swallow or is vomiting, or is thought to have impaired gastrointestinal transit or absorption.Side effects of short-term (hours or days) steroid use include
reversible increases in glucose (important in diabetics) and decreases in potassium, fluid retention with weight gain, mood alterations including rare psychosis, hypertension, peptic ulcers, aseptic necrosis of the femur, and rare allergic reactions.
Inhaled Corticosteroids in the Emergency Department. Use of ICSs, either alone or in addition to systemic steroids, to treat acute asthma has the potential benefits of reducing systemic side effects, directly delivering medication to the airway, and reducing airway reactivity and edema more effectively. Patients treated with ICSs are less likely to be admitted whether they received systemic ste-roids or not, and no increased cough or bronchospasm is seen with the use of ICSs.108,109 Patients treated with these agents have early improvement in outcomes (
-
Chapter 73 / Asthma 951
patients with more severe disease. Treatment recommendations (see Table 73-2) include adding ipratropium (0.5 mg) with the first three albuterol treatments in severe acute asthma (PEFR/FEV1 24 hours) anti-
cholinergic agent (FDA approved for treatment of COPD) that improves symptoms and lung function when added to an inhaled glucocorticoid with inadequately controlled asthma.118 The role of tiotropium in acute disease therapy is undetermined.
Magnesium Sulfate
Magnesium relaxes bronchial smooth muscle and dilates asth-matic airways in vitro. Mechanisms include calcium channelblocking properties, inhibition of cholinergic neuromuscular transmission, stabilization of mast cells and T lymphocytes, and stimulation of NO and prostacyclin. Intracellular magnesium levels are lower in acute asthma,119 and the level correlates with airway reactivity in chronic disease.There is evidence that intravenous magnesium therapy for
severe attacks might obviate the need for intubation. Magnesium adjunctive administration in severe asthma attacks (FEV1
-
952 PART III Medicine and Surgery / Section Two Pulmonary System
the pregnant asthmatic in the mild severity range is recommended. ICSs are not associated with adverse perinatal outcomes and are recommended for all pregnant patients with asthma (budesonide is preferred). Inhaled beta-agonists, ipratropium, oral or intrave-nous corticosteroids, magnesium sulfate (MgSO4), cromolyn, the-ophylline, and LT antagonists are safe during pregnancy.139 Acute exacerbations should be treated in the ED as in any nonpregnant patient. Oxygen saturation should be maintained at 95% or above. Intensive care unit (ICU) admission and mechanical ventilation are recommended as in any other patient, with the caveat that a Pco2 of 40 to 45 represents early respiratory failure in the pregnant patient. Refractory status asthmaticus may be improved by deliv-ery. Fetal monitoring is recommended for third-trimester ED patients with moderate or severe asthma exacerbations. There are no contraindications to any asthma medication in the breast-feeding patient.
Severe, Near-Fatal, and Fatal Asthma
The ATS has developed a consensus definition for identifying severe and refractory asthma that is unresponsive to conventional therapies (Fig. 73-6).140 This condition is termed severe asthma; patients with these symptoms represent only about 10% of all asthmatics yet account for 30% of asthma-related health care costs. For the definition to be met, medical conditions that mimic asthma must be excluded, exacerbating factors (e.g., allergens) identified and treated, and patients compliant.Cellular features of severe asthma include persistent eosino-
philic inflammation unresponsive to high-dose corticosteroids plus the presence of neutrophilic inflammation in the distal airways. TNF-, an inflammatory cytokine produced by mast cells, is present in increased concentration in bronchoalveolar lavage fluid with severe asthma. The potential role of TNF- antagonists such as etanercept and infliximab, and antiTNF- antibodies such as golimumab, is unclear.141-143 Studies in which monoclonal antibodies have been used against IL-5, IL-4, and IL-13 show promise, but large definitive trials are lacking.144,145
Clinical features of severe asthma include a lesser prevalence of atopy, a history of aspirin sensitivity, and a higher incidence of sinusitis and use of nasal corticosteroids (suggesting involvement of the upper as well as the lower respiratory tract). Exacerbations are also associated with menses.146 Other clinical features that
Asthmatics generally produce elevated levels of LTs, and in acute attacks the levels in the urine can be markedly increased. The addition of either 7 or 14 mg of intravenous montelukast (not available in the United States) to standard therapy for acute asthma causes a 15% nonbeta2-mediated increase in FEV1 over placebo.127 The onset of action is as early as 10 minutes and persists throughout the 2 hours after admission.128 Oral zafirlukast, when given as adjunctive therapy (20 or 160 mg) for acute asthma in the ED, improves PFT results and dyspnea but does not decrease admission rates.129 Oral montelukast (10 mg) given during acute asthma in the ED results in significantly increased PEFR the morning after admission when compared with standard treat-ment.130 The rapid onset and sustained nonbeta-mediated bron-chodilating effects of these medications may help manage acute disease.
Other and Future Therapies
In patients without dehydration or hypovolemia, vigorous admin-istration of fluids does not clear airway secretions. Mucolytics may worsen cough or airflow obstruction, and chest physical therapy is not beneficial. Sedatives are contraindicated in acute disease because of their respiratory depression.Bacterial, chlamydial, and mycoplasmal respiratory tract infec-
tions infrequently contribute to acute asthma. Antibiotics should generally be reserved for patients with fever, purulent sputum, pneumonia, or evidence of bacterial sinusitis, to prevent inap-propriate ED prescription of antibiotics for acute asthma.131
Neurokinin antagonists, inhaled loop diuretics (furosemide in acute attacks), and lidocaine may inhibit neurogenic inflamma-tion, and heparin may have a role in the inhibition of mast cell products. Infused BNP can cause significant bronchodilation.132 Specific cytokine antagonists, agonists, inhibitors of T-cell func-tion, selective inducible NO synthetase inhibitors, and possibly gene-directed therapies may become novel treatments. There are currently biologic therapies available for the management of chronic asthma. Omalizumab, a recombinant humanized mono-clonal anti-IgE antibody, is indicated for the treatment of severe allergic asthma.133 Lastly, the use of rescue therapy with an inhaled combination of a rapid-onset beta-agonist and a corticosteroid might provide both bronchodilation and self-titrated anti-inflammatory therapy.134
Pregnancy and Acute Asthma
Asthma complicates 3.7 to 8.4% of pregnancies, and hospitaliza-tions for acute exacerbations are reported in 9 to 11% of pregnant women.135 The effect of pregnancy on asthma is unpredictable. Asthma exacerbation rates and hospitalizations are directly pro-portional to the severity of asthma control (according to NAEPP guidelines),1 and pregnant patients with severe asthma have an exacerbation rate of 51.9% and a hospitalization rate of 26.9%.136 Knowledge of a pregnant patients baseline asthma severity is thus important to predict the risk of severe exacerbation. Obesity and female fetal sex are also associated with an increased risk of exac-erbation.137 Maternal and neonatal outcome are excellent in patients with mild or moderate asthma; severe asthma during pregnancy is associated with gestational diabetes and delivery before 37 weeks.135,138
The hyperventilation of pregnancy is compensated for by a metabolic acidosis. Typical pregnant patients have ABGs with a pH of 7.40 to 7.45, Po2 of 106 to 110, and Pco2 of 28 to 32 mm Hg; therefore when ABG values in a pregnant patient are interpreted, a normal Pco2 actually represents hypercarbia. Maternal hypox-emia quickly results in fetal hypoxemia. PEFR remains unchanged during pregnancy, and monitoring in the ED is strongly recom-mended. The smallest amount of medication needed to maintain
Figure 73-6. AmericanThoracicSocietyworkshopconsensusfordefinitionofsevereorrefractoryasthma(requiresoneorbothmajorandtwominorcriteriaandthatotherconditionshavebeenexcluded,exacerbatingfactorshavebeentreated,andpatientisgenerallycompliant).
Major characteristics Treatment with continuous or near-continuous (50% of year) oral corticosteroids Requirement for treatment with high-dose intravenous corticosteroids
Minor characteristics Requirement for additional daily treatment with a controller medication (e.g., long-acting beta-agonist, theophylline, or leukotriene antagonist) Asthma symptoms requiring short-acting beta-agonist use on a daily or near-daily basis Persistent airway obstruction (FEV1 < 80% predicted, diurnal peak expiratory flow variability > 20%) One or more urgent care visits for asthma per year Three or more oral steroid bursts per year Prompt deterioration with 25% reduction in oral or intravenous corticosteroid dose Near-fatal asthma event in the past
-
Chapter 73 / Asthma 953
decrease the work of breathing long enough to abort intubation by carrying bronchodilators to the distal airways and allowing anti-inflammatory agents time to achieve their effects. The results when heliox is used to drive nebulized beta-agonist therapies in both children and adults are mixed.150-152 No data indicate that heliox reduces the need for intubation or hospital admission, length of hospital stay, or mortality rates.152-154 Heliox is adminis-tered by nonrebreather mask and may be an adjunctive strategy to mechanical ventilation in selected asthmatics. Close monitoring of oxygen saturation and continuous capnography are advisable. Considerations for heliox include cases of severe airflow obstruc-tion (PEFR
-
954 PART III Medicine and Surgery / Section Two Pulmonary System
tion occurs. Compression delivered too early (i.e., during inspira-tion) may increase airway pressure and result in barotrauma.Unrecognized barotrauma may cause cardiac arrest. Rapid
bedside ultrasound may identify occult pneumothorax and reveal nonpalpable cardiac contractions. Empirical bilateral tube thora-costomy should be performed if unexplained cardiac arrest occurs, especially in the context of dramatic increases in peak inspiratory pressure. Intravenous epinephrine is a logical agent in the setting of cardiopulmonary arrest because it has inotropic, chronotropic, and bronchodilatory properties.164 Isoproterenol, a pure beta-agonist, may increase heart rate and provide bronchodilation but decreases coronary perfusion pressure. Cardiopulmonary bypass and extracorporeal lung assist are also used in the treatment of near-fatal asthma.
DISPOSITION
Prediction of Relapse
Asthmatic patients discharged from the ED have rates of relapse that vary from 11% over 3 days to 45% at 8 weeks. In a multicenter study, the relapse rate was 17% in the 2 weeks after ED discharge. The risk for relapse increases in those with numerous asthma-related ED visits within the previous year, with more outpatient medications, and with longer duration of symptoms before the ED visit.165 Other studies find similar out-of-control indices pre-dicting relapse but have also included insufficient improvement in PFTs with hospital-based treatment for an attack.166
Inpatient versus Observation or Clinical Decision Unit
Patients requiring extended care who are without life-threatening exacerbations, pregnancy, or complications of asthma can gener-ally be treated in a clinical decision unit (CDU) or observation unit with 8-week outcomes equal to those of patients admitted and with significant cost savings.167 The ability to predict discharge from the CDU can be assessed by the ED PEFR response to the third beta2-agonist treatment (PEFR >40% predicted is often associated with successful CDU discharge).165 In addition, patients prefer CDU treatment of acute attacks over routine inpa-tient care.168
Table 73-4 summarizes disposition guidelines.
a ketamine emergence reaction. Alternatively, propofol (1.5- 2 mg/kg) offers rapid-onset deep sedation and also possesses bronchodilating properties. Continued deep sedation with propo-fol or an equivalent agent (e.g., long-acting benzodiazepine) usually avoids the need for muscle paralysis. After intubation, an opioid that does not release histamine, such as fentanyl, can improve the patients comfort.A ventilator strategy providing adequate oxygenation and ven-
tilation while minimizing high airway pressure, barotrauma, and systemic hypotension must be instituted. The technique of per-missive hypercapnia (also known as controlled hypoventilation) is common (see Chapter 2). Oxygenation is maintained by use of a high fraction of inspired oxygen (Fio2); hypercarbia and respira-tory acidosis (pH maintained at 7.15-7.2 with sodium bicarbon-ate) are tolerated. Airway pressure is kept low by providing low tidal volumes (6-8 mL/kg), thus preventing excessive increases of intrinsic positive end-expiratory pressure (auto-PEEP), stacking of ventilations, and barotrauma. Low ventilation rates (below 10 breaths/min) and high inspiratory flow rates (above 60 L/min) provide prolonged time for expiration. Adjunctive therapies (in-line beta-agonists and anticholinergics, intravenous corticoste-roids, intravenous ketamine, and possibly intravenous magnesium) to decrease airway pressure and airway obstruction are delivered simultaneously.Continuous capnography is advisable. Moderate levels of
hypercapnia are well tolerated and have few deleterious effects. Elevated CO2 levels have vasodilatory effects on cerebral vessels. Cerebral blood flow reaches its maximum at a Paco2 level of 120 mm Hg, which may increase intracranial pressure. Although there is no consensus on what constitutes a safe level of hypercap-nia, Paco2 levels above 100 mm Hg should be avoided.
160 Hyper-capnia can decrease cardiac contractility and produce cardiovascular collapse; thus permissive hypercapnia should be supplemented by generous repletion of intravascular volume through intravenous fluid administration.Neuromuscular blockade, once widely used for ventilation of
asthmatic patients to rest fatigued airway muscles, is now used only in cases in which deep sedation with adequate analgesia fails to provide sufficient patient relaxation for successful mechanical ventilation (see Chapter 1). Myopathy attributed to the prolonged use of competitive neuromuscular blocking agents occurs in about 30% of asthmatic patients with neuromuscular blockade.159 Although hazards of mechanical ventilation (nosocomial infec-tion, barotrauma) may occur, the treatment of critically ill asth-matics with mechanical ventilation is associated with low mortality and few complications. Complications of mechanical ventilation in the asthmatic patient include hypoxemia, hypotension, and barotrauma. Hypotension is almost uniformly secondary to increased intrathoracic pressure with a subsequent decrease in venous return and cardiac output. Slowing the rate of mechanical ventilation or removing the patient from the ventilator for a short time (20-30 seconds) allows more time for expiration, thereby decreasing intrathoracic pressure. Volume depletion and medica-tion effects (e.g., narcotic agents used for sedation) are other potential explanations for hypotension. Pneumothorax should be considered whenever sudden deterioration occurs or when hypo-tension is accompanied by a significant rise in peak inspiratory ventilator pressures.
Treatment of the Refractory Critically Ill Asthmatic. If the inten-sively treated, intubated critically ill asthmatic continues to have elevated airway pressures, persistent hypoxemia, and continued bronchospasm, general anesthesia should be considered. Isoflu-rane, a bronchodilator, has lower arrhythmogenic and hypotensive properties than halothane.163
External lateral chest compression may be of assistance when patients cannot exhale. Chest compression is delivered by bilateral squeezing of the lower chest walls immediately after end inspira-
GOOD RESPONSE
INCOMPLETE RESPONSE POOR RESPONSE
FEV1 or PEFR (% predicted/ personal best)
70% 40% but
-
Chapter 73 / Asthma 955
medications, transportation vouchers, and appointment assis-tance significantly increase the likelihood that discharged asthma patients will obtain primary care follow-up. These assistances, however, may not affect long-term outcomes.169
Patients that follow up and are managed by asthma specialists have fewer symptoms, less beta-agonist use, improved quality of life, and reduced ED visits and hospitalizations than those managed by generalists. Patients with severe persistent asthma or prior severe exacerbations should be referred from the ED to an asthma specialist.169
The asthma patient can be provided written education about discharge medications, medication adjustment if the condition is not improving (such action plans are not often created and when done are often inadequate),171 and a peak flow meter for daily measurements, especially for those who have difficulty perceiving airflow obstruction or who have symptoms of worsen-ing asthma. At a minimum, focused education should address the need for follow-up and for understanding the difference between controller and rescue medications and their use.169 Lastly, smoking asthmatics have more respiratory symptoms, lower lung function, and more parenchymal abnormalities noted on chest computed tomography, so the need for smoking cessation should be discussed.172
Inhaledandsystemicsteroidmedicationsareeffectiveincontrollingairwayinflammationandhaveimportantrolesinmanagementofasthmaexacerbations.
Single-isomeralbuterol(levalbuterol),theresultofimprovingisomertechnology,isabetterbronchodilatorinacuteasthmathanthetraditionalracemicform.
Severeandrefractoryasthmaexacerbationsrequirerapididentification.Treatmentmustbeaggressiveandmayusestrategiesnotusedinmildtomoderateexacerbations.
AnormalPCO2inapregnantpatientrepresentshypercarbia. EDmanagementofacuteasthmaisexpanding(upto24
hours)asmorenoncriticallyillasthmaticsaretreatedintheclinicaldecisionunits.
IntegrationofdischargedpatientswithacuteasthmaintochronicmanagementstrategiestopreventrelapserequiresthatasthmapatientsphysiciansbefamiliarwithcontrollingmedicationssuchasICSsandLTmodifiers.
KEY CONCEPTS
BOX 73-3
1. RemovecapfromtheMDIcontainer.2. AssembletheMDIandholditupright.3. Shakethecanister.4. Placethemouthpiecelooselybetweentheteeth(orholdit
3-4cminfrontoftheopenmouth).5. Exhalefully(tofunctionalresidualcapacity).6. Actuatetheinhaleratthebeginningofaslowandfull
inhalation(asifsippinghotsoup)lasting5or6seconds.7. Holdbreathforatleast10seconds.8. Wait1minutebeforereuse.
Instructions for Metered-Dose Inhaler (MDI) Use
Planning Discharge from the Emergency Department
An asthma exacerbation does not end on ED discharge; airway inflammation and peripheral obstruction may take hours to days to resolve. Patients are likely to need continued beta2-agonist rescue therapy, and they should demonstrate the correct use of their inhalers (Box 73-3). If the patient is having difficulty coor-dinating the canister activation with inhalation, a breath-activated inhaler or spacer device can be prescribed or the need for a home nebulizer discussed. A patient using a portable, preloaded, multi-dose DPI must be able to inhale from the mouthpiece in a rapid and forceful inhalation to total lung capacity.Patients receiving systemic corticosteroids in the ED should
continue these orally for 5 to 10 days. Asthma patients treated in the ED are more likely to have moderate to severe disease; not receive controller therapy; and be younger, poorer, and less edu-cated. They have reduced asthma management skills and are more likely to miss school or work. If the patient was not using control-ler medications before the acute ED visit and has characteristics of persistent asthma (symptoms or rescue therapy more than twice per week, interference with sleep more than twice per month, activity limitation caused by asthma or exacerbations requiring oral corticosteroids more than once in the past year), moderate-dose inhaled steroids or a combination inhaled steroid and long-acting beta-agonist should be started.169,170 A less preferred option is to prescribe an LT modifier (e.g., zafirlukast 20 mg twice a day or montelukast 10 mg daily) to decrease relapse and improve asthma control.169
Patients should contact their physician for asthma-related prob-lems within the following 3 to 5 days and should make a follow-up medical appointment (ideally done while the patient is still in the ED) within 1 to 4 weeks. Interventions that include free
The references for this chapter can be found online by accessing the accompanying Expert Consult website.
-
Chapter 73 / Asthma 955.e1
References
1. National Asthma Education and Prevention Program Expert Panel: Report 3: Guidelines for the Diagnosis and Management of Asthma. NIH Publication No. 08-5846. Washington, DC: U.S. Department of Health and Human Services, National Institutes of Health, National Heart, Lung and Blood Institute; 2007.
2. American Lung Association Epidemiology and Statistics Unit Research and Program Services Division: Trends in Asthma Morbidity and Mortality, February 2010. Available at www.lungusa.org/finding-cures/our-research/trend-reports/asthma-trend-report.pdf. Accessed March 2011.
3. Akinbami LJ, Moorman JE, Liu X: Asthma prevalence, health care use, and mortality: United States, 2005-2009. Natl Health Stat Report 2011; 32:1-14
4. Centers for Disease Control and Prevention: Asthma Data and Surveillance. Available at www.cdc.gov/asthma/asthmadata.htm. Accessed April 2011.
5. Moorman JE, Zahran H, Truman BI, Molla MT, Centers for Disease Control and Prevention (CDC): Current asthma prevalenceUnited States, 2006-2008. MMWR Surveill Summ 2011; 60(Suppl):84.
6. National Institutes of Health, National Heart, Lung, and Blood Institute: Morbidity and Mortality: 2007 Chart Book on Cardiovascular, Lung, and Blood Diseases. Available at www.nhlbi.nih.gov/resources/docs/07-chtbk.pdf. Accessed March, 2011.
7. Weiss KB, Sullivan SD: The health economics of asthma and rhinitis. I. Assessing the economic impact. J Allergy Clin Immunol 2001; 107:3.
8. Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion: Healthy Youth! Health Topics: Asthma. August 14, 2009. Available at http://www.nhlbi.nih.gov/guidelines/asthma/index.htm. Accessed April 2011.
9. National Institutes of Health, National Heart, Lung, and Blood Institute: Morbidity and Mortality: 2009 Chart Book on Cardiovascular, Lung, and Blood Diseases. Available at www.nhlbi.nih.gov/resources/docs/2009_ChartBook.pdf. Accessed April 2011.
10. National Center for Health Statistics: Asthma Prevalence, Health Care Use and Mortality: United States, 2003-05. Available at http://www.cdc.gov/nchs/data/hestat/asthma03-05/asthma03-05.htm. Accessed April, 2011.
11. Minio AM, Xu J, Kochanek KD: Deaths: Preliminary data for 2008. Natl Vital Stat Rep 2010; 59:1.
12. Bartolomei-Daz JA, Amill-Rosario A, Claudio L, Hernndez W: Asthma mortality in Puerto Rico: 1980-2007. J Asthma 2011; 48:202.
13. Hamid QA, Minshall EM: Molecular pathology of allergic disease. 1. Lower airway disease. J Allergy Clin Immunol 2000; 105:20.
14. Murphy DM, OByrne PM: Recent advances in the pathophysiology of asthma. Chest 2010; 137:1417.
15. Von Hertzen L, Haahtela T: Disconnection of man and the soil: Reason for the asthma and atopy epidemic? J Allergy Clin Immunol 2006; 117:334.
16. Roduit C, et al: Asthma at 8 years of age in children born by caesarean section. Thorax 2009; 64:107.
17. Bradding P: Asthma: Eosinophil disease, mast cell disease or both? Allergy Asthma Clin Immunol 2008; 4:84.
18. Bradding P, Walls AF, Holgate ST: The role of the mast cell in the pathophysiology of asthma. J Allergy Clin Immunol 2006; 117:277.
19. Brightling CE, et al: Mast cell infiltration of airway smooth muscle in asthma. N Engl J Med 2002; 346:199.
20. Black J: The role of mast cells in the pathophysiology of asthma. N Engl J Med 2002; 346:1742.
21. Williams TJ: The eosinophil enigma. J Clin Invest 2004; 113:507.22. Leckie MJ, et al: Effects of an interleukin-5 blocking monoclonal
antibody on eosinophils, airway hyper-responsiveness, and the late asthmatic response. Lancet 2000; 356:2144.
23. OByrne PM: Cytokines or their antagonists for the treatment of asthma. Chest 2006; 130:244.
24. Green RH, et al: Asthma exacerbations and sputum eosinophil counts: A randomised controlled trial. Lancet 2002; 360:1715.
25. Green RH, et al: Analysis of induced sputum in adults with asthma: Identification of subgroup with isolated sputum neutrophilia and poor response to inhaled corticosteroids. Thorax 2002; 57:875.
26. Berry M, et al: Pathological features and inhaled corticosteroid response of eosinophilic and non-eosinophilic asthma. Thorax 2007; 62:1043.
27. Barnes PJ: How corticosteroids control inflammation. Br J Pharmacol 2006; 148:245.
28. Fireman P: Understanding asthma pathophysiology. Allergy Asthma Proc 2003; 24:79.
29. Holgate ST, Roberts G, Arshad HS, Howarth PH, Davies DE: The role of the airway epithelium and its interaction with environmental factors in asthma pathogenesis. Proc Am Thorac Soc 2009; 6:655.
30. Holgate ST: Epithelium dysfunction in asthma. J Allergy Clin Immunol 2007; 120:1233.
31. Barnes PJ, et al: Exhaled nitric oxide in pulmonary diseases: A comprehensive review. Chest 2010; 138:682.
32. Bergeron C, Al-Ramli W, Hamid Q: Remodeling in asthma. Proc Am Thorac Soc 2009; 6:301.
33. Barbato A, et al: Epithelial damage and angiogenesis in the airways of children with asthma. Am J Respir Crit Care Med 2006; 174:975.
34. Cohen L, et al: Epithelial cell proliferation contributes to airway remodeling in severe asthma. Am J Respir Crit Care Med 2007; 176:138.
35. Jenkins C, Costello J, Hodge L: Systematic review of prevalence of aspirin induced asthma and its implications for clinical practice. BMJ 2004; 328:434.
36. Lee RU, Stevenson DD: Aspirin-exacerbated respiratory disease: Evaluation and management. Allergy Asthma Immunol Res 2011; 3:3.
37. Marquette CH, et al: Long-term prognosis for near fatal asthma: A 6 year follow-up study of 145 asthmatic patients who underwent mechanical ventilation for near-fatal attack of asthma. Am Rev Respir Dis 1992; 146:76.
38. Jawien J: A new insight into aspirin-induced asthma. Eur J Clin Invest 2002; 32:134.
39. Stevenson DL, Szczeklik A: Clinical and pathologic perspectives on aspirin sensitivity and asthma. J Allergy Clin Immunol 2006; 118:773.
40. Knowles SR, Drucker AM, Weber EA, Shear NH: Management options for patients with aspirin and nonsteroidal anti-inflammatory drug sensitivity. Ann Pharmacother 2007; 41:1191.
41. Weiler JM, et al: American Academy of Allergy, Asthma and Immunology Work Group report: Exercise-induced asthma. J Allergy Clin Immunol 2007; 119:1349.
42. Hallstrand TS, Henderson WR: An update on the role of leukotrienes in asthma. Curr Opin Allergy Clin Immunol 2010; 10:60.
43. Grzelewski T, Stelmach I: Exercise-induced bronchoconstriction in asthmatic children: A comparative systematic review of the available treatment options. Drugs 2009; 69:1533.
44. Anderson SD: Single-dose agents in the prevention of exercise-induced asthma: A descriptive review. Treat Respir Med 2004; 3:365.
45. Vrieze A, Postma DS, Kerstjens HA: Perimenstrual asthma: A syndrome without known cause or cure. J Allergy Clin Immunol 2003; 112:271.
46. Dratva J, et al: Perimenstrual increase in bronchial hyperreactivity in premenopausal women: Results from the population-based SAPALDIA 2 cohort. J Allergy Clin Immunol 2010; 125:823.
47. Redmond AM, James AW, Nolan SH, Self TH: Premenstrual asthma: Emphasis on drug therapy options. J Asthma 2004; 41:687.
48. Ritz T, et al: Airway response to emotional stimuli in asthma: The role of the cholinergic pathway. J Appl Physiol 2010; 108:1542.
49. Di Marco F, Santus P, Centanni S: Anxiety and depression in asthma. Curr Opin Pulm Med 2011; 17:39.
50. Anbar RD: Hypnosis in pediatrics: Applications at a pediatric pulmonary center. BMC Pediatr 2002; 2:11.
51. Postma DS, Koppelman GH: Genetics of asthma: Where are we and where do we go? Proc Am Thorac Soc 2009; 6:283.
52. Holloway JW, Arshad SH, Holgate ST: Using genetics to predict the natural history of asthma? J Allergy Clin Immunol 2010; 126:200.
53. Hamid Q: Gross pathology and histopathology of asthma. J Allergy Clin Immunol 2003; 111:431.
54. Chen FH, et al: Airway remodeling: A comparison between fatal and nonfatal asthma. J Asthma 2004; 41:631.
55. Hyzy RC, et al: Slow-onset asthma deaths have more eosinophils and health care utilization than rapid-onset deaths. Respir Med 2008; 102:1819.
56. Tsai CL, et al: Quality of care for acute asthma in 63 U.S. emergency departments. J Allergy Clin Immunol 2009; 123:3549.
57. Pines JM, Prabhu A, Hilton JA, Hollander JE, Datner EM: The effect of emergency department crowding on length of stay and medication treatment times in discharged patients with acute asthma. Acad Emerg Med 2010; 17:834.
58. Zimmerman JL, Woodruff PG, Clark S, Camargo CA: Relation between phase of menstrual cycle and emergency department visits for acute asthma. Am J Respir Crit Care Med 2000; 162:512.
59. Magadle R, Berar-Yanny N, Weiner P: The risk of hospitalization and near-fatal and fatal asthma in relation to the perception of dyspnea. Chest 2002; 121:329.
60. Rodrigo GJ, Plaza V: Body mass index and response to emergency department treatment in adults with severe asthma exacerbations. Chest 2007; 132:1513.
-
955.e2 PART III Medicine and Surgery / Section Two Pulmonary System61. Peters-Golden M, et al: Influence of body mass index on the response
to asthma controller agents. Eur Respir J 2006; 27:495.62. Lessard A, Turcotte H, Cornier Y: Obesity and asthma: A specific
phenotype? Chest 2008; 134:317.63. Patel SN, et al: Multicenter study of cigarette smoking among patients
presenting to the emergency department with acute asthma. Chest 2009; 103:121.
64. Boulet LP, FitzGerald JM, McIvor RA, Zimmerman S, Chapman KR: Influence of current or former smoking on asthma management and control. Can Respir J 2008; 15:275.
65. El-Ekiaby A, et al: Impact of race on the severity of acute episodes of asthma and adrenergic responsiveness. Am J Respir Crit Care Med 2006; 174:508.
66. Chandra D, Clark S, Camargo CA: Race/ethnicity differences in the inpatient management of acute asthma in the United States. Chest 2009; 135:1527.
67. Rodrigo GJ, Rodrigo C, Hall JB: Acute asthma in adults. Chest 2004; 125:1081.
68. Levine M, Iliescu ME, Margellos-Anast H, Estarziau M, Ansell DA: The effects of cocaine and heroin use on intubation rates and hospital utilization in patients with acute asthma exacerbations. Chest 2005; 128:1951.
69. Krantz AJ, et al: Heroin insufflation as a trigger for patients with life-threatening asthma. Chest 2003; 123:510.
70. Corbridge T, Cygan J, Greenberger P: Substance abuse and acute asthma. Intensive Care Med 2000; 26:347.
71. Elia D, Marinou A, Chetta A: Life-threatening asthma after heroin inhalation. A case report and a review of the literature. Acta Biomed 2010; 81:63.
72. Brooks TW, et al: Rates of hospitalizations and emergency department visits in patients with asthma and chronic obstructive pulmonary disease taking beta-blockers. Pharmacotherapy 2007; 27:684.
73. Silverman RA, Flaster E, Enright PL, Simonson SG: FEV1 performance among patients with acute asthma: Results from a multicenter clinical trial. Chest 2007; 131:164.
74. Nowak RM, Tomlanovich MC, Sarkar DD: Arterial blood gases and pulmonary function testing in acute bronchial asthma: Predicting patient outcomes. JAMA 1983; 249:2043.
75. Corbo J, Bijur P, Lahn M, Gallagher EJ: Concordance between capnography and arterial blood gas measurements of carbon dioxide in acute asthma. Ann Emerg Med 2005; 46:323.
76. Nik Hisamuddin NA, et al: Correlations between capnographic waveforms and peak flow meter measurements in emergency department management of asthma. Int J Emerg Med 2009; 2:83.
77. Baptist AP, Sengupta R, Pranathiageswaran S, Wang Y, Ager J: Evaluation of exhaled nitric oxide measurements in the emergency department for patients with acute asthma. Ann Allergy Asthma Immunol 2008; 100:415.
78. Delclaux C, et al: Offline exhaled nitric oxide in emergency department and subsequent acute asthma control. J Asthma 2008; 45:867.
79. Stephenson JJ, Quimbo RA, Gutierrez B: Subacute lack of asthma control as a predictor of subsequent acute asthma exacerbation in a managed care population. Am J Manag Care 2010; 16:108.
80. Kenn K, Balkissoon R: Vocal cord dysfunction: What do we know? Eur Respir J 2011; 37:194.
81. Camargo CA Jr: A model protocol for emergency medical services management of asthma exacerbations. Prehosp Emerg Care 2006; 10:418.
82. Richmond NJ, Silverman R, Kusick M, Matallana L, Winokur J: Out-of-hospital administration of albuterol for asthma by basic life support providers. Acad Emerg Med 2005; 12:396.
83. Thompson J, Petrie DA, Ackroyd-Stolarz S, Bardua DJ: Out-of hospital continuous positive airway pressure ventilation versus usual care in acute respiratory failure: A randomized controlled trial. Ann Emerg Med 2008; 52:232.
84. Moloney E, OSullivan S, Hogan T, Poulter LW, Burke CM: Airway dehydration: A therapeutic target in asthma? Chest 2002; 121:1806.
85. Spitzer WO, et al: The use of beta-agonists and the risk of death and near death from asthma. N Engl J Med 1992; 326:501.
86. Nowak RM: Single-isomer levalbuterol: A review of the acute data. Curr Allergy Asthma Rep 2003; 3:172.
87. Jenne JW: The debate on S-enantiomers of beta-agonists: Tempest in a teapot or gathering storm? J Allergy Clin Immunol 1998; 102:893.
88. Nowak RM, et al: Levalbuterol compared with racemic albuterol in the treatment of acute asthma: Results of a pilot study. Am J Emerg Med 2004; 22:29.
89. Nowak R, et al: A comparison of levalbuterol with racemic albuterol in the treatment of acute severe asthma exacerbations in adults. Am J Emerg Med 2006; 24:259.
90. Carl CC, Myers TR, Kirchner HL, Kercsmar CM: Comparison of racemic albuterol and levalbuterol for treatment of acute asthma. J Pediatr 2003; 143:731.
91. Peters SG: Continuous bronchodilator therapy. Chest 2007; 131:286.92. Truitt T, Witko J, Halpern M: Levalbuterol compared to racemic
albuterol: Efficacy and outcomes in patients hospitalized with COPD or asthma. Chest 2003; 123:128.
93. Rodrigo GJ: Predicting response to therapy in acute asthma. Curr Opin Pulm Med 2009; 15:35.
94. Carroll CL, Stoltz P, Schramm CM, Zucker AR: Beta2-adrenergic receptor polymorphisms affect response to treatment in children with severe asthma exacerbations. Chest 2009; 135:1186.
95. Newman KB, Milne S, Hamilton C, Hall K: A comparison of albuterol administered by metered-dose inhaler and spacer with albuterol by nebulizer in adults presenting to an urban emergency department with acute asthma. Chest 2002; 121:1036.
96. Osmond MH, et al: Barriers to metered-dose inhaler/spacer use in Canadian pediatrics emergency department: A national survey. Acad Emerg Med 2007; 14:1106.
97. Hurley KF, et al: Perceptual reasons for resistance to change in the emergency department use of holding chambers for children with asthma. Ann Emerg Med 2008; 51:70.
98. Mason N, Roberts N, Yard N, Partridge MR: Nebulisers or spacers for the administration of bronchodilators to those with asthma attending emergency departments? Respir Med 2008; 102:993.
99. Dhuper S, et al: Efficacy and cost comparisons of bronchodilatator administration between metered dose inhalers with disposable spacers and nebulizers for acute asthma in an inner-city adult population. J Emerg Med 2008; 40:247.
100. Travers AH, Rowe BH, Barker S, Jones A, Camargo CA Jr: The effectiveness of IV beta-agonists in treating patients with acute asthma in the emergency department: A meta-analysis. Chest 2002; 122:1200.
101. Putland M, Kerr D, Kelly AM: Adverse events associated with the use of intravenous epinephrine in emergency department patients presenting with severe asthma. Ann Emerg Med 2006; 47:559.
102. Liao MM, Ginde AA, Clark S, Camargo CA Jr: Salmeterol use and risk of hospitalization among emergency department patients with acute asthma. Ann Allergy Asthma Immunol 2010; 104:478.
103. Rodrigo GJ, Neffen H, Colodenco FD, Castro-Rodriguez JA: Formoterol for acute asthma in the emergency department: A systematic review with meta-analysis. Ann Allergy Asthma Immunol 2010; 104:247.
104. Najafizadeh K, et al: A randomised, double-blind, placebo-controlled study to evaluate the role of formoterol in the management of acute asthma. Emerg Med J 2007; 24:317.
105. Chowdhury BA, Dal Pan G: The FDA and safe use of long-acting beta-agonists in the treatment of asthma. N Engl J Med 2010; 362:1169.
106. Rowe BH, Spooner C, Ducharme FM, Bretzlaff JA, Bota GW: Early emergency department treatment of acute asthma with systemic corticosteroids. Cochrane Database Syst Rev 2000; 2:CD002178.
107. Lin RY, et al: Rapid improvement of peak flow in asthmatic patients treated with parenteral methylprednisolone in the emergency department: A randomized controlled study. Ann Emerg Med 1999; 33:487.
108. Edmonds ML, Camargo CA, Pollack CV, Rowe BH: Early use of inhaled corticosteroids in the emergency department treatment of acute asthma. Cochrane Database Syst Rev 2003; 3:CD002308.
109. Edmonds ML, Camargo CA Jr, Pollack CV Jr, Rowe BH: The effectiveness of inhaled corticosteroids in the emergency department treatment of acute asthma: A meta-analysis. Ann Emerg Med 2002; 40:145.
110. Rodrigo GJ: Comparison of inhaled fluticasone with intravenous hydrocortisone in the treatment of adult acute asthma. Am J Respir Crit Care Med 2005; 172:1231.
111. Rowe BH, Vethanayagam D: The role of inhaled corticosteroids in the management of acute asthma. Eur Respir J 2007; 30:1035.
112. Schuckman H, et al: Comparison of intramuscular triamcinolone and oral prednisone in the outpatient treatment of acute asthma: A randomized controlled trial. Ann Emerg Med 1998; 31:333.
113. Lahn M, Bijur P, Gallagher EJ: Randomized clinical trial of intramuscular vs oral methylprednisolone in the treatment of asthma exacerbations following discharge from an emergency department. Chest 2004; 126:362.
114. Rowe BH, et al: Inhaled budesonide in addition to oral corticosteroids to prevent asthma relapse following discharge from the emergency department: A randomized controlled trial. JAMA 1999; 281:2119.
-
Chapter 73 / Asthma 955.e3
115. Krishnan JA, Nowak R, Davis SQ, Schatz M: Anti-inflammatory treatment after discharge home from the emergency department in adults with acute asthma. Proc Am Thoracic Soc 2009; 6:380.
116. Rodrigo G, Rodrigo C, Burschtin O: A meta-analysis of the effects of ipratropium bromide in adults with acute asthma. Am J Med 1999; 107:363.
117. Rodrigo GJ, Rodrigo C: The role of anticholinergics in acute asthma treatment: An evidence-based evaluation. Chest 2002; 121:1977.
118. Peters SP, et al: Tiotropium bromide step-up therapy for adults with uncontrolled asthma. N Engl J Med 2010; 363:1715.
119. Zervas E, et al: Reduced intracellular Mg concentrations in patients with acute asthma. Chest 2003; 123:113.
120. Silverman RA, et al: IV magnesium sulfate in the treatment of acute severe asthma: A multicenter randomized controlled trial. Chest 2002; 122:489.
121. Alter HJ, Koepsell TD, Hilty WM: Intravenous magnesium sulfate as an effective adjunct in acute bronchospasm: A meta-analysis. Acad Emerg Med 1999; 6:521.
122. Cheuk DK, Chau TC, Lee SL: A meta-analysis on intravenous magnesium sulfate for treating acute asthma. Arch Dis Child 2005; 90:74.
123. Jones LA, Goodacre S: Magnesium sulphate in the treatment of acute asthma: Evaluation of current practice in adult emergency departments. Emerg Med J 2009; 26:783.
124. Nannini LJ Jr, Pendino JC, Corna RA, Mannarino S, Quispe R: Magnesium sulfate as a vehicle for nebulized salbutamol in acute asthma. Am J Med 2000; 108:193.
125. Mahajan P, Haritos D, Rosenberg N, Thomas R: Comparison of nebulized magnesium sulfate plus albuterol to nebulized albuterol plus saline in children with acute exacerbations of mild to moderate asthma. J Emerg Med 2004; 27:21.
126. Blitz M, et al: Aerosolized magnesium sulfate for acute asthma: A systematic review. Chest 2005; 128:337.
127. Camargo CA Jr, Smithline HA, Malice MP, Green SA, Reiss TF: A randomized controlled trial of intravenous montelukast in acute asthma. Am J Respir Crit Care Med 2003; 167:528.
128. Camargo CA Jr, et al: A randomized placebo-controlled study of intravenous montelukast for the treatment of acute asthma. J Allergy Clin Immunol 2010; 125:374.
129. Silverman RA, et al: Zafirlukast treatment for acute asthma: Evaluation in a randomized, double-blind multicenter trial. Chest 2004; 126:1480.
130. Ramsay CF, Pearson D, Mildenhall S, Wilson AM: Oral montelukast in acute asthma exacerbations: A randomised, double-blind, placebo-controlled trial. Thorax 2011; 66:7.
131. Vanderweil SG, et al: Inappropriate use of antibiotics for acute asthma in United States emergency departments. Acad Emerg Med 2008; 15:736.
132. Akerman MJ, et al: Bronchodilator effect of infused B-type natriuretic peptide in asthma. Chest 2006; 130:66.
133. Rodrigo GJ, Neffen H, Castro-Rodriquez JA: Efficacy and safety of subcutaneous omalizumab vs placebo as add-on therapy to corticosteroids for children and adults with asthma. Chest 2011; 139:28.
134. Papi A, Caramori G, Adcock IM, Barnes PJ: Rescue treatment in asthma: More than as-needed bronchodilation. Chest 2009; 135:1628.
135. Hardy-Fairbanks AJ, Baker ER: Asthma in pregnancy: Pathophysiology, diagnosis and management. Obstet Gynecol Clin North Am 2010; 37:159.
136. Schatz M, et al: Asthma morbidity during pregnancy can be predicted by severity classification. J Allergy Clin Immunol 2003; 112:283.
137. Tamsi L, et al: Asthma in pregnancyimmunological changes and clinical management. Respir Med 2011; 105:159.
138. Enriquez R, et al: Effect of maternal asthma and asthma control on pregnancy and perinatal outcomes. J Allergy Clin Immunol 2007; 120:625.
139. Schatz M, et al: The relationship of asthma medication use to perinatal outcomes. J Allergy Clin Immunol 2004; 113:1040.
140. Holgate ST, et al: Understanding the pathophysiology of severe asthma to generate new therapeutic opportunities. J Allergy Clin Immunol 2006; 117:496.
141. Howarth PH, et al: Tumour necrosis factor (TNFalpha) as a novel therapeutic target in symptomatic corticosteroid dependent asthma. Thorax 2005; 60:1012.
142. Erin EM, et al: The effects of a monoclonal antibody directed against tumor necrosis factoralpha in asthma. Am J Respir Crit Care Med 2006; 174:753.
143. Wenzel SE, et al: A randomized double-blind placebo-controlled study of tumor necrosis factoralpha blockade in severe persistent asthma. Am J Respir Crit Care Med 2009; 179:549.
144. Clienti S, Morjaria JB, Basile E, Polosa R: Monoclonal antibodies for the treatment of severe asthma. Curr Allergy Asthma Rep 2011; 11:253.
145. Corren J: Cytokine inhibition in severe asthma: Current knowledge and future directions. Curr Opin Pulm Med 2011; 17:29.
146. Wenzel SE, Busse WW: Severe asthma: Lessons for the severe asthma research program. J Allergy Clin Immunol 2007; 119:14.
147. Wenzel S, Szefler SJ: Managing severe asthma. J Allergy Clin Immunol 2006; 117:508.
148. Romagnoli M, et al: Near fatal asthma phenotype in the ENFUMOSA cohort. Clin Exp Allergy 2007; 37:552.
149. Kass JE: Heliox redux. Chest 2003; 123:673.150. Lee DL, Hsu CW, Lee H, Chang HW, Huang YC: Beneficial effects of
albuterol therapy driven by heliox versus by oxygen in severe asthma exacerbation. Acad Emerg Med 2005; 12:820.
151. Brando DC, et al: Heliox and posture optimize action of nebulization with bronchodilators for asthma attacks. Randomized trial. Respir Med 2011; 56:947-952. DOI:10.4187/respcare.00963.
152. Bigham MT, et al: Helium/oxygen-driven albuterol nebulization in the management of children with status asthmaticus: A randomized placebo-controlled trial. Pediatr Crit Care Med 2010; 11:356.
153. Rodrigo G, Pollack C, Rodrigo C, Rowe BH: Heliox for nonintubated acute asthma patients. Cochrane Database Syst Rev 2006; 4:CD002884.
154. Hurford WE, Cheifetz IM: Respiratory controversies in the critical care setting: Should heliox be used for mechanically ventilated patients? Respir Care 2007; 52:582.
155. Beers SL, Abramo TJ, Bracken A, Wiebe RA: Bilevel positive airway pressure in the treatment of status asthmaticus in pediatrics. Am J Emerg Med 2007; 25:6.
156. Fernndez MM, Villagr A, Blanch L, Fernndez R: Non-invasive mechanical ventilation in status asthmaticus. Intensive Care Med 2001; 27:486.
157. Soroksky A, Stav D, Shpirer I: A pilot prospective, randomized placebo-controlled trial of bilevel positive airway pressure in acute asthma attack. Chest 2003; 123:1018.
158. Nowak R, Corbridge T, Brenner B: Noninvasive ventilation. J Emerg Med 2009; 37(Suppl 2):S18.
159. Phipps P, Garrard CS: The pulmonary physician in critical care. 12: Acute severe asthma in the intensive care unit. Thorax 2003; 58:81.
160. Mutlu GM, Factor P, Schwartz DE, Sznajder JI: Severe status asthmaticus: Management with permissive hypercapnia and inhalation anesthesia. Crit Care Med 2002; 30:477.
161. Brenner B, Corbridge T, Kazzi A: Intubation and mechanical ventilation of the asthmatic patient in respiratory failure. J Emerg Med 2009; 37(Suppl 2):S23.
162. Maslow AD, et al: Inhaled albuterol, but not intravenous lidocaine, protects against intubation-induced bronchoconstriction in asthma. Anesthesiology 2000; 93:1198.
163. Tobias JD: Inhalational anesthesia: Basic pharmacology, end organ effects, and applications in the treatment of status asthmaticus. J Intensive Care Med 2009; 24:361.
164. Smith D, et al: Intravenous epinephrine in life-threatening asthma. Ann Emerg Med 2003; 41:706.
165. McCarren M, et al: Prediction of relapse within eight weeks after an acute asthma exacerbation in adults. J Clin Epidemiol 1998; 51:107.
166. McDermott MF, et al: A comparison between emergency diagnostic and treatment unit and inpatient care in the management of acute asthma. Arch Intern Med 1997; 157:2055.
167. McCarren M, Zalenski RJ, McDermott M, Kaur K: Predicting recovery from acute asthma in an emergency diagnostic and treatment unit. Acad Emerg Med 2000; 7:28.
168. Rydman RJ, Roberts RR, Albrecht GL, Zalenski RJ, McDermott M: Patient satisfaction with an emergency department asthma observation unit. Acad Emerg Med 1999; 6:178.
169. Schatz M, Rachelefsky G, Krishnan JA: Follow-up after acute asthma episodes: What improves future outcomes? Proc Am Thorac Soc 2009; 6:386.
170. Rowe BH, et al: Adding long-acting beta-agonists to inhaled corticosteroids after discharge from the emergency department for acute asthma: A randomized controlled trial. Acad Emerg Med 2007; 14:833.
171. Camargo CA Jr, et al: A prospective multicenter study of written action plans among emergency department patients with acute asthma. J Asthma 2008; 45:532.
172. Boulet LP, et al: Smoking and asthma: Clinical and radiologic features, lung function, and airway inflammation. Chest 2006; 129:661.
73 AsthmaPerspectiveEpidemiologyPrinciples of DiseasePathophysiologyMiscellaneous SituationsGenetics and Asthma
Pathology
Clinical FeaturesNational and International Guidelines for the Diagnosis and Management of AsthmaSymptom