Regional Anesthesia
43
REGIONAL ANESTHESIA Speaker : Arie Andrianto Consulant : Dr. Purwito Nugroho Sp.An MM
description
adasd
Transcript of Regional Anesthesia
REGIONAL ANESTHESIA
REGIONAL ANESTHESIA
Speaker : Arie AndriantoConsulant : Dr. Purwito Nugroho Sp.An MM
Anesthesia (from Greek -, an-, "without"; and , aisthsis, "sensation").
Anesthesia is the use of medicine to prevent the feeling of pain or sensation during surgery or other procedures that might be painful (such as getting stitches or having a wart removed).WHAT DEFINITION of ANESTHESIA?COMPONENTS OF ANAESTHESIA The famous components of general anaesthesia are TRIAD1. UNCOSCOUSNESS.2. ANALGESIA3. MUSCLE RELAXATION
THE TYPE OF ANESTHESIA
General AnaesthesiaInsensible does not necessary imply loss of consciousness.
General anaesthesiaInhalationalIV ,IM or P/R
LOCAL ANAESTHETICAs anesthesia means no sense, so there are drugs which can block the nerve conduction peripherally with no need of brain depression. So patient will be conscious
REGIONAL ANESTHESIA
Regional anesthesia is the injection of a local anesthetic around major nerves or the spinal cord to block pain from a large region of the body, such as a limb. No CNS depression; patient conscious Regional anesthetic techniques categorized as follows Epidural and spinal anesthesia Peripheral nerve blockades: cervical, brachial, axial
NEURAXIAL BLOCKADE
EPIDURAL AND SPINAL ANESTHESIANEURAXIAL BLOCKADESpinal cord: By injection of local drug in sub-arachnoid space in CSF, this must be bellow L2
Epidural: The drug is injected outside dura [no puncture] to block the nerve roots at its exit from spinal cord.
Anatomy
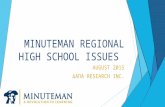
11Epidural Anesthesia Levels
Adapted with permission from Unintended subdural injection: a complication of epidural anesthesia- a case report, AANA Journal, vol. 74, no. 3, 2006.13Spinal vs. Epidural Anesthesia
SpinalEasier to perform Smaller dose of LA required (usually < toxic IV dose) Rapid blockade (onset in 2-5 minutes) Very effective blockade Hyperbaric LA solution - position of patient importantEpidural Technically more difficult; greater failure rate Larger volume/doses of LA (usually > toxic IV dose) Significant blockade requires 10-15 minutes Effectiveness of blockade can be variable Use of catheter allows for continuous infusion or repeat injections Slower onset of side effects Position of patient not as important SG of LA solution not as important
Spinal vs. Epidural Anesthesia
Anetesi SpinalAnestesi EpiduralTempat insersiHanya vertebra lumbal (dibawah L2/3)Sakral, lumbal, thorakdan servicalTempai injeksiRuang subarachnoid (LCS)Ruang epiduralTempat kerjaRuang subarachnoid (saraf dan medulla spinalis)Dosis obat LAKecilBesarOnsetCepatLebih lambatBlok motorikKuatSedangKomplikasiHenti jantung, PDPH, spinal tinggi, total spinal.Intoksikasi local anestetik, hematom epiduralAnalgesi postoptidakYa, dengan kateter
SpinalEpidural
Epidural Anesthesia
Spinal AnesthesiaIndicationsFull stomachAnatomic distortions of upper airwayObstetrical surgery (T4 Level)Decreased post-operative painContinuous infusionContraindications to Regional Anesthesia
Absolute Contraindications for Neuraxial BlockadePatient refusalIschemic Hypertrophic Sub-aortic Stenosis Infection at the site of injectionCoagulopathySevere hypovolemiaIncreased Intracranial pressureSevere Aortic StenosisSevere Mitral Stenosis20Relative ContraindicationsSepsisUncooperative patientsPre-existing neuro deficits/neurological deficits Demylenating lesionsStenotic valuvular heart lesions (mild to moderate Aortic Stenosis/Ischemic Hypertrophic Sub-aortic Stenosis)Severe spinal deformities
21Complications of Neuraxial Blockade
Failure of technique Systemic drug toxicity due to overdose or intravascular injection Peripheral neuropathy due to intraneural injection Pain or hematoma at injection site Epidural anesthesiaSystemic toxicity of LA (accidental intravenous)Catheter complications (shearing, kinking, vascular or subarachnoid placement)
PREPARATION FOR REGIONAL ANESTHESIA
Thorough pre-op evaluation and assessment of patient Technique explained to patient IV sedation may be indicated before block
Neuroaxial TechniquePreparation & MonitoringEKGNBPPulse OximeterPatient PositioningLateral decubitousSittingProne (hypobaric technique)
Spinal NeedlesEpidural NeedlesSpinal NeedlesEpidural Needles
REGIONAL ANESTHESIA DRUGSLidokain The recommended maximum safe doses of lidocaine are as follows: LIDOCAINE WITHOUT EPINEPHRINE ------ 3 mg/kg LIDOCAINE WITH EPINEPHRINE ------ 7 mg/kgBupivakainThe recommended maximum safe doses of bupivacaine are as follows:
BUPIVACAINE WITHOUT EPINEPHRINE ------- 2.0 mg/kg BUPIVACAINE WITH EPINEPHRINE ------- 2.5 mg/kg
Spinal Anesthesia
Epidural AnestesiRoy A. Greengrass, M.D.Associate Professor of AnesthesiologyMayo Clinic, Jacksonville, FL
PERIPHERAL NERVE BLOCKADESCervical, Brachial, AxialIndications for Peripheral BlockadeIn addition to some of the peripheral nerve block indicationsPatient mentally prepared to accept neuraxial blockadeNo contraindicationsNo need for routine labs unless meds or conditions dictate this33Contraindications to Peripheral Nerve BlockPediatric patients, combative patients, demented patientsPre-existing peripheral nerve neuropathiesBleeding disordersLocal anesthetic toxicity riskSepsis34Risks for Peripheral Nerve BlockToxicity of local anestheticsTransient or chronic paresthesiaNerve damageIntra-arterial injection (seizures/cardiac arrest)Block failure (need to supplement or induce general anesthesia)35Advantages of Peripheral Nerve BlocksImproved patient satisfactionLess immunosuppressionLess nausea and vomitingNon-general anesthetic option for patient with malignant hyperthermiaPatient who is hemodynamically unstable or too ill to tolerate a general anesthetic36
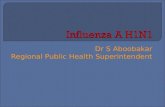
Brachial Plexus
Musculocutaneous NerveMedian NerveUlnar Nerve Radial Nerve
Axillary BlockPositionHead turned away from arm being blockedAbduct to 90Forearm is flexed to 90Palpate brachial artery for pulse
41Other Blocks
Thank you for your attention