
Quantification of Radiation Induced DNA Damage Response in ...373627/FULLTEXT01.pdf · whether the...
52
Transcript of Quantification of Radiation Induced DNA Damage Response in ...373627/FULLTEXT01.pdf · whether the...





List of Papers
This thesis is based on the following papers, which are referred to in the textby their Roman numerals.
I Simonsson, M.,† Qvarnström, F.,† Nyman, J., Johansson, K-A., Garmo,H., Turesson, I. (2008) Low-dose hypersensitive γH2AX response andinfrequent apoptosis in epidermis from radiotherapy patients
II Turesson, I., Nyman, J., Qvarnström, F., Simonsson, M., Book, M.,Hermansson, I., Sigurdardottir, S., Johansson, K-A. (2010) A low-dosehypersensitive keratinocyte loss in response to fractionated radiother-apy is associated with growth arrest and apoptosis
III Simonsson, M., Nyman, J., Hermansson, I., Book, M., Sigurdardot-tir, S., Thunberg, U., Qvarnström, F., Johansson, K-A., Turesson, I.(Manuscript) Epidermal keratinocyte loss in response to daily 2 Gy frac-tions for 5 weeks of radiotherapy is associated with DSB-foci, growtharrest, apoptosis and lack of accelerated repopulation
IV Thunberg, U.,† Simonsson, M.,† Qvarnström, F., Nyman, J., Johans-son, K-A., Turesson, I. (Manuscript) Mir-34a, mir-16 and mir-203 inthe DNA damage response of epidermis and dermis to conventional ra-diotherapy
†These authors are considered as joint first authors.Reprints were made with permission from the publishers.


Contents
1 Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 91.1 Background . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 91.2 Radiotherapy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 111.3 Side-effects in the skin . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 121.4 DNA damage response . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 131.5 DNA double strand breaks . . . . . . . . . . . . . . . . . . . . . . . . . . . . 141.6 MicroRNA . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 151.7 Measured endpoints . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 16
1.7.1 Assessment of keratinocyte response . . . . . . . . . . . . . . . . 161.7.2 Assessment of growth arrest . . . . . . . . . . . . . . . . . . . . . . . 161.7.3 Assessment of cell proliferation . . . . . . . . . . . . . . . . . . . . 161.7.4 Assessment of DNA double strand damage . . . . . . . . . . . 161.7.5 Assessment of cell death . . . . . . . . . . . . . . . . . . . . . . . . . 171.7.6 Assessment of microRNAs . . . . . . . . . . . . . . . . . . . . . . . 17
2 Material and Methods . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 192.1 Skin biopsies . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 192.2 Skin biopsy acquisition . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 192.3 Prostate cancer patients . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 192.4 Breast cancer patients . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 202.5 Dosimetry . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 212.6 Histochemistry . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 222.7 Quantification procedures . . . . . . . . . . . . . . . . . . . . . . . . . . . . 222.8 Real-Time qRT-PCR (Real Time quantitative Revers
Transcription PCR) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 233 Results and Discussion . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 25
3.1 γH2AX as a marker for apoptosis . . . . . . . . . . . . . . . . . . . . . . 273.2 Basal keratinocyte density . . . . . . . . . . . . . . . . . . . . . . . . . . . . 27
3.2.1 Fraction dose response . . . . . . . . . . . . . . . . . . . . . . . . . . . 283.2.2 Total dose response . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 28
3.3 Proliferation in terms of Mitosis . . . . . . . . . . . . . . . . . . . . . . . . 293.4 Apoptosis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 303.5 DNA damage . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 313.6 Cell cycle checkpoints . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 32
4 Summary . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 355 Acknowledgements . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 39Bibliography . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 41


1. Introduction
1.1 BackgroundCancer is a leading cause of death worldwide, and as many as one of every tendeaths is caused by cancer. The risk for cancer increases with age, and with anageing population the deaths from cancer worldwide are projected to continuerising.
Lifestyle is an important factor in cancer development and more than athird of cancer is preventable by the avoidance of tobacco and/or alcohol use;low fruit and vegetable intake; physical inactivity; being overweight or obese;exposure to sexually transmitted diseases and inhaled air pollutants. Still in thedeveloped world, one in three people will develop cancer during their lifetime,and in the United States one in four will die of cancer.
From a cellular perspective, cancer is a class of diseases where a singlecell starts to divide and creates a group of abnormal cells with uncontrolledgrowth. These cells grow beyond their normal boundaries, and may invadeneighbouring tissues and spread to other parts of the body.
Treatment aims to completely remove the cancer and this can often be ac-complished with surgery. Since a single cancer cell can regrow into a newtumour a margin of surrounding healthy normal tissue is also removed. Ifthe cancer has spread to other sites in the body, complete surgical excisionis usually impossible. In these cases, other treatment forms may provide analternative approach.
Cancers that reside in the blood or which have metastasised can in manycases be treated with chemotherapy. Since cancer is associated with uncon-trolled growth and often rapidly dividing cells, chemotherapeutic substancescan be applied to target cell division mechanisms and thereby reduce thegrowth of the cancer cells. This can however also affect the cell division ofhealthy normal cells and result in side-effects such as hair loss.
Another commonly used treatment form is radiotherapy. In these treat-ments, ionising radiation is used to damage genetic material, DNA, in can-cer cells. Radiation can be delivered to a target area externally via externalbeam radiotherapy and internally via brachytherapy. The amount of radiation,the absorbed dose, is measured in gray (Gy). The ability to deliver the doseto a precise location makes radiotherapy suitable for solid tumours. Comput-erised treatment planning maximises the dose delivered to the tumour whileminimising the dose to surrounding healthy tissue.
9

Today most cancers are treated with a combination of surgery, chemo-and radiotherapy. Both chemo- and radiotherapy can be given adjuvant, af-ter surgery, to eliminate remaining cancer cells and avoid regrowth. They canalso be given neoadjuvant, before treatment to reduce tumour size and facili-tating less destructive surgery.
Regardless of cancer treatment type, the radiation exposure of normal tis-sue must be taken into consideration. All forms of genotoxic treatment affecthealthy tissues to some degree and these side-effects are often limiting thecurability of cancer. In case of radiotherapy, acute side-effects occur duringtreatment and commonly in tissues with high turnover, such as the gut andskin. Depending on the severity, these effects are usually reversible. However,late side-effects can occur months or even years after treatment. These oftenappear due to damage in more slowly renewing cells such as blood vessels andconnective tissue cells. One of the most severe late side-effects is induction ofcancer, although secondary malignancies are rare and usually appear 20-30years following treatment.
Both chemo- and radiotherapy have most impact on rapidly dividing cells.All dividing cells have to pass through a number of steps that make up the celldivision cycle. The cell cycle can be divided in two main phases: interphaseand mitosis (celldivision, M phase). During interphase, the cell prepares formitosis and accumulates nutrients and duplicates its genetic material. Inter-phase can be further divided into three distinct phases: G1 phase, S phase andG2 phase. Each phase is dependent on the proper execution and completion ofthe previous one. Cells that have temporarily or reversibly stepped out of thecell cycle are said to have entered a reversible state of quiescence called G0phase.
Non-dividing cells, such as fully differentiated cells, generally enter G0/G1from G1 and may remain arrested for long periods of time. Permanently ar-rested senescent cells are metabolically active and differ from quiescent G0cells in this respect. Cellular senescence is a response to genetic damage, andcan in some cases be an alternative to self-destruction by apoptosis.
The cell cycle is governed by several checkpoints that prevent progressionof the cell cycle at specific points. Two main checkpoints exist: one at thetransition from G1 to S and another at G2 to M. The first checkpoint controlswhether the cell should divide or instead delay division and enter G0/G1. Thesecond ensures that the cell is ready for mitosis. An important function ofboth checkpoints is the assessment of DNA damage. When damage is detectedthe checkpoint must stall the cell cycle to allow for repairs. This is to avoidpassing damaged DNA to daughter cells. If the cell is damaged beyond repairthe cell is destined for apoptosis or mitotic failure, or alternatively permanentarrest.
The cellular response to DNA damage is essential for maintaining the nor-mal function of cells and tissues. The cells management of DNA damage isimportant both in the development and treatment of cancer.
10

In this study we have focused on radiation induced DNA damage to variouscell populations in normal skin. The responses have been quantified for severalend points to examine the impact of DNA double-strand breaks on cell cyclecheckpoints and how this translates to the acute and late side-effects seen indifferent parts of the tissue.
1.2 RadiotherapyRadiotherapy is, besides surgery, considered to be the most important cancertreatment [85]. In the clinic, linear accelerators are commonly used to pro-duce megavoltage x-rays, a type of low-LET radiation, which is delivered to atargeted area by external beam therapy. When the ionising radiation (IR) pen-etrates the tissue, DNA-damage is inevitably induced in surrounding healthynormal tissues. Therefore, the radiation fields are meticulously planned to re-duce the risk for side-effects while maximising the dose to the tumour. Bytargeting the tumour with several fields from different directions a highly con-formal dose can be achieved in the tumour with multiple fold lower doses innormal tissue.
To increase the effect of radiotherapy, the total planned dose is commonlydelivered over several weeks of treatment. This treatment approach is referredto as fractionation and allows for the normal tissue to tolerate a higher totaldose and recover between single dose fractions. Fractionation also takes ad-vantage of differences in DNA damage responses between malignant and nor-mal tissue. The cell cycle checkpoints and repair mechanisms are presumed tofunction better in normal cells compared to rapidly dividing tumour cells withuncontrolled growth. Fractionation related changes in cell cycle distributionsmay also favour the relative survival of normal cells over tumour cells [64].
Nevertheless, different cancers respond differently to radiotherapy.Radiosensitivity is the relative susceptibility of cells, tissues and organs tothe harmful effects of ionising radiation. Highly radiosensitive malignanciessuch as lymphomas can be cured with modest doses of radiation. Epithelialcancers, such as breast and prostate cancer, are only moderately radiosensitiveand require higher doses. Radioresistant cancer cells include gliomas andmelanomas, and may require higher doses than considered safe in clinicalpractice.
Radiosensitivity depends on several properties. Rapidly diving cells aregenerally more radiosensitive than quiescent cells [8, 27]. It has also longbeen established that the radiation sensitivity differs quite significantly be-tween various cell cycle phases, with S and G1 being least sensitive and M themost sensitive phase [29, 83]. The radiosensitivity in tumours may also be re-lated to size, with larger tumours being more resistant, sometimes associatedwith hypoxia.
11

The complexity of radiosensitivity is further emphasised by its dose depen-dency. A phenomenon called hyperradiosensitivity (HRS) has been observed,where cells respond more than expected to very low doses [12, 60, 62].
1.3 Side-effects in the skinRegardless of cancer treatment form, healthy normal tissue will inevitably beaffected. Considering radiotherapy, the skin is a normal tissue, which is alwaysaffected as the radiation enters and exits the body. This causes skin reactionsto various degrees common side-effects. The skin is also a tissue that exhibitsboth acute and late effects [26, 59, 89, 91]. The side-effects observed in skinreflect the different tissue components of the skin, with acute effects appearingpredominantly in the epidermis and late effects in the dermis.
The epidermis is a multilayered epithelium consisting of a hierarchicalstructure of basal stem cells and progenitor cells, also known as transit am-plifying cells, and overlying differentiated cells (Fig. 1.1). There is a constantturnover of the epidermis governed by the rate of which terminally differenti-ated keratinocytes are shed from the skin surface [10,99]. The tissue integrityand function is maintained by proliferation of epidermal stem/progenitor cellsthat reside in the basal layer. A population of melanocytes, making up 10 to 15percent of the basal cells, also resides at the basement membrane between theepidermis and dermis. The specific task of cutaneous melanocytes is to pro-duce melanin and transfer it to surrounding keratinocytes in order to protectdeeper tissues from UV-radiation damage.
The early skin response begins with redness of the skin, erythema, followedby shedding of the outer layers of the skin causing dry or moist desquamation.These reactions can be a dose-limiting step and may require a temporary orpermanent cessation of the therapy. Several studies have described skin re-sponses by quantification of basal cell density in skin biopsies from patientsundergoing radiotherapy [37, 48, 66]. A similar but more specific approachhas been described , where only basal kreatinocytes were quantified, therebyavoiding the inclusion of the melanocytic cell compartment [94]. Early effectsthat arise from keratinocyte depletion are reversible if overdosage of radiationis avoided.
Situated directly beneath the epidermis is the dermis (Fig. 1.1). The upperpart of the dermal layer consists mainly of connective tissue interspersed withfibroblasts, immune cells and small blood vessels surrounded by endothelialcells. The epidermis relies on the dermis supporting function of fibroblastsand nutrient supply and waste removal through the capillaries in the dermalpapillae.
The late effects may appear months or even years after treatment and arerepresented by subcutaneous fibrosis, caused by the development of excessfibrous connective tissue. This is usually associated with atrophy, which is
12

keratinocytes
endothelial cell
capillary
epidermis
basal layer
dermis
melanocyte
fibroblast
Figure 1.1: Top layers of human skin. Epidermal stem cells and melanocytes residein the basal layer. Continuous cell divisions in the basal layer re-fill the differenti-ating cell pools further up. In a continuous movement towards the skin surface, thekeratinocytes will finally be incorporated in the top layer, where they eventually areshed. The upper part of the dermal layer consists mainly of connective tissues inter-spersed with fibroblasts, immune cells and small blood vessels coated by endothelialcells.
thinning of the skin. Over time small dilated blood vessels, known as telang-iectasias, may also develop. Late effects progress in a strict dose-dependentmanner [26,59,89,91], and are always irreversible due to lack of proper inter-vention methods.
1.4 DNA damage responseCell cycle checkpoint activation is an important part of the DNA damage re-sponse (DDR) mechanisms, capable of stalling cycling cells and preventingcells with unrepaired DNA damage from continued proliferation. In responseto DNA damage, and especially DNA double-strand breaks (DSBs), the ATMprotein kinase activates molecular pathways essential for coordinating cell cy-cle progression with DNA repair [50].
In normal unirradiated cells, ATM is present as an inactive dimer. Oncetriggered by DSB ATM kinase is activated by autophosphorylation [5]. Cells
13

deficient in ATM activity display hypersensitivity to DSBs [67]. Data suggestthat ATM is fully activated within 15 minutes, but that will occur only if dosesabove ∼0.3–0.5 Gy are reached [5]. This phenomenon has been described toplay an important role for the existence of low-dose hypersensitivity [61].Fully activated ATM phosphorylates several downstream target proteins thatcontribute to initiation checkpoints in the G1, S and G2 phases of the cellcycle.
Within this multitude of checkpoints, which regulate cell cycle progression,the G1-checkpoint is suggested to be the most sensitive in terms of its abil-ity to detect low levels of damage [43, 56, 57]. The G1-checkpoint is initiallytriggered by phosphorylation of p53 by ATM, resulting in an overall increasein transcriptional activity of p53 [6, 17]. The phosphorylated p53 induces anincreased expression of the cyclin dependent kinase inhibitor p21, which inturn directly inhibits the activity of cyclinD-Cdk4/6 and cyclinE-Cdk2, result-ing in cell cycle arrest [28, 38, 100]. Checkpoint-related nuclear p21 expres-sion can then be readily detected in epidermal skin by immunohistochemistry(IHC) [90].
In response to DNA damage, p53 may also induce expression of numerousapoptotic genes involved in the mitochondrial apoptotic pathway and the deathreceptor pathway [52]. However, it is assumed that the default pathway of thep53 response to DNA damage is the induction of cell cycle arrest rather thanapoptosis. What governs the switch between these two outcomes is poorlyunderstood. p53 can act in an anti/pro-apoptotic manner depending on celltype, with cell cycle arrest being more likely in epithelial cells and apoptosisin lymphoid cells [24, 32, 36]. Anti- or pro-apoptotic activity is also regulatedby the severity of DNA damage. At low levels, arrest and repair is favouredand at high levels apoptosis is increased [34].
Cell cycle checkpoints, apoptosis and senesence are factors that have an in-fluence on the overall tissue response to DNA damage. Regulation of thesekey mechanisms influence, to varying degrees, tissue responses observed dur-ing clinical cancer treatments, such as fractionated radiotherapy and multiplecycles of chemotherapy, where tissues are exposed to repeated genotoxic in-sults.
1.5 DNA double strand breaksThe DNA in human cells is wrapped around nuclear histone proteins. Theyform fundamental chromatin units called nucleosomes that are involved inregulation and compaction of eukaryotic DNA [2]. One of the core histonevariants H2AX, has been subject to intensive research since its involvementin DNA DSB-signalling first was discovered [33,74,76]. Following inductionof DSBs, ATM is the main kinase responsible for the rapid phosphorylation
14

Figure 1.2: Foci detection in epidermal cells. Immunofluorescence stainings allow forsimultaneous detection of multiple targets in the same cells. a) γH2AX b) 53BP1 andc) DAPI
of H2AX [15, 86]. Other kinases, such as ATR and DNA-PK, are howevercapable of phosphorylating H2AX [3, 30, 86, 96, 97].
The phosphorylated form of H2AX, referred to as γH2AX, can be visu-alised within individual cell nuclei as distinct foci structures using antibodiesspecific for this phosphorylated form [68, 74] (Fig. 1.2a). Since a single DSBappears to be sufficient for foci formation, γH2AX has been widely employedas a marker for detection of very low levels of DSB damage [13, 20, 78, 81].
Phosphorylated H2AX is not essential for the initial recognition of thebreak. Instead it appears to function as a platform for recruiting other fac-tors involved in the repair process [18, 51, 68]. The kinetics of the removalof γH2AX foci and their connection to DSB repair is still under investiga-ton. It has however been suggested that γH2AX foci, induced by clinicallyrelevant doses, are removed from sites of DSBs shortly after the breaks arerepaired [13, 14, 21, 31, 78].
53BP1 is another protein that signals DSB induction and forms foci at thesites of the lesions within minutes. [4,49,72,80,98] (Fig. 1.2b).Several studieshave thus described co-localisation of γH2AX and 53BP1 foci in a wide rangeof cell types [53, 58, 72, 80]. Phosphorylation of H2AX is not essential for53BP1 foci formation, although γH2AX is necessary to retain 53BP1 at theDSB site, suggesting a parallel but interacting pathway [18, 22, 31, 103].
1.6 MicroRNAMicro RNA is another entity involved in DDR to various genotoxic insults.MicroRNAs (miRNAs) are short non-protein-coding RNAs that negativelyregulate gene expression, and account for 1 to 3% of genes in the mammaliangenome. Estimates suggest that ∼30% of all protein-encoding RNAs are sub-ject to regulation by multiple miRNAs [55, 102]. miRNAs have been impli-cated in the regulation of proliferation, differentiation, and apoptosis [101].
15

To understand the cell-specific functions of miRNAs in DDR, it is importantto define their expression patterns. Several methods have been developed forjust that purpose. We have used real-time quantitative RT-PCR, separately onmicrodissected epidermis and dermis.
1.7 Measured endpointsTo investigate the response to DNA damage in normal tissue we have definedseveral endpoints. These range from the initial induction of DSBs, via cellcycle checkpoints to cell death and cell loss on a tissue level.
1.7.1 Assessment of keratinocyte responseFractionated radiotherapy results in reduction in cell numbers, and a continu-ous thinning out of the epidermal layer. In an effort to quantify this response,tissue sections from biopsies collected from both prostate and breast cancerpatient were histochemically stained, and basal keratinocytes were manuallycounted at high power (100x objective) in a bright-field microscope. Countingwas restricted to interfollicular epidermis and only cells that were attached tothe underlying basement membrane were included. Melanocytes were identi-fied morphologically and counted separately.
1.7.2 Assessment of growth arrestThe cyclin dependent kinase inhibitor p21, directly inhibits the activity ofcyclinD-Cdk4/6 and cyclinE-Cdk2, resulting in cell cycle arrest [28, 38, 100].We have previoulsy reported that checkpoint-related nuclear p21 expressioncan subsequently be readily detected in epidermal skin by immunohistochem-istry (IHC) [90].
1.7.3 Assessment of cell proliferationCell proliferation was quantified in terms of mitotic frequency. The antibodyphospho-H3 staining identified all stages of mitosis in tissue sections [41].
1.7.4 Assessment of DNA double strand damageOne of the primary effects of radiotherapy is the induction of DNA damageand especially DSBs. We have focused on proteins in the DNA damage sig-nalling and repair pathway, which form foci to quantify the initial inductionof DSB and the repair at later time points.
The method we have developed utilises immunofluorescence stainings offoci-forming molecular markers and digital image analysis to quantify them.
16

Figure 1.3: Immunofluorescence stainings of epidermal cells in different stages ofapoptosis.
This method enables us to measure single DSBs within a cell. We then adaptedthe method to work for both γH2AX and 53BP1.
The 53BP1 antibody could also be detected with an enzymatic amplificationsystem to be examined in conventional bright-field microscopy. This allowedus to measure DBSs by manual quantification of 53BP1 foci
1.7.5 Assessment of cell deathIn response to DNA damage, p53 may also induce apoptosis. During apop-tosis the DNA is fragmented, and as a consequence, massive phosphoryla-tion of H2AX occurs [75]. This can be visualised with immunofluorescenceas intensely stained cells (Fig. 1.3). The apoptotic frequency was determinedby manual counting of basal and suprabasal apoptotic cells in γH2AX im-munofluorescence stained sections. Due to the infrequency of the epidermalapoptosis, at least 6 tissue sections per biopsy were counted.
1.7.6 Assessment of microRNAsRecently, members of the miR-34 family (miR-34 a,b,c) have been reportedto be direct targets of the tumor suppressor transcription factor p53. Afterp53 activation miR-34a regulates the molecular pathways leading to apoptosisand reversible or permanent cell cycle arrest. The miR-34a targets a broadspectrum of proteins for down-regulation of the cell cycle progression, whichcan result in different outcomes such as apoptosis, senescence, or terminaldifferentiation [11, 19, 25, 39, 73, 87, 88].
The final outcome in response to DNA damage depends on a multitude ofanti- and pro-apoptotic signals. Bcl-2 is a protein that is expressed in cells toprotect them from apoptosis. Up-regulation of miR-16 has been reported toinduce apoptosis by targeting the Bcl-2 expression [23]. By monitoring miR-16, we investigated its tumour suppressing function in normal tissues, and theconnection with apoptosis as an outcome of radiation induced DNA damage.
17

The delicate balance between proliferating stem cells and progenitor cells,and the subsequent shedding of terminally differentiated keratinocytes is cru-cial to the maintainance of tissue integrity. Terminal differentiation, whichmay be a possible outcome of DNA damage, is a multistep process. The up-regulation of miR-203 in human keratinocytes is an important step in thisprocess [84]. The differentiation is promoted by miR-203, which represses“stemness” by targeting the cell-cycle regulator p63 [54,101]. We assume thatradiation induced supression of proliferation could be reflected by changes indifferentiation [90]. By monitoring miR-203 in skin, the relationship betweenproliferating, and differentiated keratinocytes can be studied as an endpoint ofDNA damage inflicted by radiotherapy.
18

2. Material and Methods
2.1 Skin biopsiesThe accessibility of the skin makes it highly suitable for clinical research. Inaddition to visual inspection, multiple biopsies can be collected at differentdoses and time points from the same patient. Thereby, all the well definedcell-lineages can be explored before, during and after genotoxic treatments,i. e. radiotherapy and chemotherapy. Such a dose and spatiotemporal tissuesampling can provide insights to the interactions between cells from variouscell lineages, i.e the communication between keratinocytes and melanocytes,and epithelial and mesenchymal cells, respectively (Fig. 1.1). In comparisonto more deeply situated tissues of the body, an advantage is that the actualdose of ionising radiation delivered to the skin at a particular location canbe accurately determined. This prerequisite, in combination with its structuralproperties of acutely and late responding cell populations, make skin an ex-cellent clinical model for studying radiation induced DNA damage responsein normal tissues.
2.2 Skin biopsy acquisitionBetween 1993 and 2007 over 2000 skin biopsies were collected from 115prostate and 45 breast cancer patients undergoing curative radiotherapy. Thesamples were 3 mm in diameter, taken under local anaesthesia, immediatelyfixed in 5% formalaldehyde and embedded in paraffin.
2.3 Prostate cancer patientsThe prostate patients received daily fractions throughout a seven week treat-ment course with interruptions over weekends. Each fraction delivered 2 Gyto the prostate target volume, using 3- or 4-field techniques, where the prostateis exposed to photon irradiation from several directions.
The biopsy sets were collected so that dose-response relationships through-out the treatment, as well as between fractions, could be investigated. Thebiopsy sets were taken from areas of the skin exposed to fraction doses of0.05–1.1 Gy, providing a material where individual dose response can be de-termined (Fig. 2.1). To enable assessment of dose response in between frac-
19

0.1 Gy
0.45 Gy0.2 Gy 1.1 Gy
0 Gy
RT �eld
Figure 2.1: Skin punch biopsy collection from prostate cancer patients. Locations forbiopsy collection corresponded to doses of 0.1 Gy, 0.2 Gy and 0.45 Gy, taken withinand just outside one of the lateral fields (shaded area). Regions of the skin within theopposed lateral field provided biopsies corresponding to skin doses of 1.1 Gy, obtainedusing a 5 mm bolus.
tions, biopsy sets were collected at different timepoints following fractions:30 minutes, 3 hours and 24 hours. Unexposed control biopsies were collectedfrom all patients.
2.4 Breast cancer patientsThe breast cancer patients underwent mastectomy followed by standard radio-therapy to the thoracic wall. Radiotherapy was administered either with elec-trons, 6-14 MeV, and 1 cm bolus, or with opposed tangential photon beams,5 MV, and with a bolus of 5 mm in a 5 to 10 cm broad strip covering the surgi-cal scar. In this area the skin received the prescribed dose of 2 Gy per fraction(ICRU 50), given daily Monday to Friday, over 5 weeks, i.e. to a total dose of50 Gy. A homogenous dose to epidermis and dermis was delivered with bothtechniques.
All biopsies collected during treatment were taken from the skin area underthe bolus (Fig. 2.2). One or two control biopsies were collected followed by
20

2.0 Gy
RT �eld
bolus
Figure 2.2: Skin punch biopsy collection from breast cancer patients. Locations forbiopsy collection corresponded to doses of 2 Gy, taken within the field (shaded area)and under a 5 mm bolus in a 5–10 cm broad strip covering the surgical scar.
multiple biopsies sampled at predetermined intervals during and after comple-tion of the treatment, at the longest up to 20 weeks.
2.5 DosimetryAccurate and reliable dose determinations are a prerequisite for dose responsestudies involving low-dose exposures. In this case, modifications of the avail-able clinical dosimetry techniques were applied to ensure optimal accuracy.Doses corresponding to specific biopsy locations were, for each of the pa-tients, initially calculated in the radiotherapy treatment planning system. Thedose determinations were further improved by adjustments derived from a se-ries of ionisation chamber measurements based on the individual field setups.Dose compensations were also made after the biopsies had been taken. Thesewere based on the actual biopsy locations on the skin. The locations werecompared with the dose plan to compensate for possible deviations from theintended biopsy locations.
21

2.6 HistochemistryThe collected biopsies are immediately fixed in formalin to preserve and pro-tect proteins and other tissue structures by creating covalent bonds, anchoringthe different structures to each other. The next step is to remove water fromthe tissues and replace it with a medium that solidifies to allow thin sections tobe cut. Different histochemical staining techniques are then used to enhancecontrast and highlight features of interest in the section.
Hematoxylin is a basic dye that stains the nucleus of the cell blue due to anaffinity to nucleic acids. Eosin is an acidic dye that enhance the structure of thetissue by staining the cytoplasm pink. Eosin can be used in combination withperiodic acid-Schiff (PAS), which detects glycogen in the tissue, to visualisethe basement membrane.
Target-specific primary antibodies are used in immunohistochemistry to de-tect cellular protein expression patterns in the context of their tissue localisa-tion. These primary antibodies can be visualised with secondary antibodiescoupled with an enzymatic amplification system to be examined in conven-tional bright-field microscopy. The secondary antibodies can also be coupledto different fluorophores, which can be detected using different filters in a flu-orescenece microscope. This enables visualisation of several target proteins inthe same section.
2.7 Quantification proceduresThe requirements for quantification of tissue sections should dictate the choiceof of microscopy techniques and histochemical detection system (Fig. 2.3).The simplicity of conventional bright field microscopy can often be advan-tageous for quantifications of distinct staining patterns. The possibility ofarchiving stained sections is a further advantage.
Fluorescence microscopy can use fluorophores with specific excitation andemission spectra to provide a sensitive detection system where several targetsin a tissue can be detected simultaneously. This enables co-localisation analy-sis or other staining pattern comparisons of multiple targets in individual cells.Fluorescence microscopy can however suffer from intensity variations due tofluorophore fading or light source inaccuracies. Fluorophore fading further-more limits long-time storage of tissue sections.
Manual counting is often the most time efficient solution for quantificationof the frequency of positive cells with a distinct staining pattern. Digital imageanalysis (DIA) may however be an option if the staining is ambiguous or addi-tional measurements are required. The use of DIA enables measurement of arange of factors that are difficult to measure by eye: area, intensity and shapesare all quantifiable parameters. DIA is available for both bright field and fluo-rescence microscopy, but impose different requirements for image acquisition.
22

Skin biopsies
Immunohistochemistry
Results
ManualAnalysis
Digital image analysisDigital image analysis
Figure 2.3: Quantification procedures in skin. Molecular targets in cells were targetedand visualised by immunohistochemistry in skin biopsies taken from patients under-going radiotherapy. Histologial sections was quantified manually or with digital imageanalysis.
Bright field microscopy often requires colour separation within the image todistinguish between positive and negative cells. Fluorescence microscopy of-fers a general advantage with different fluorophores to provide easy separationof the stained targets, and superior contrast.
Once the material has been recorded as digital images, it can be re-analysedwith minimal effort. This may also diminish the need to store the actual sec-tions.
2.8 Real-Time qRT-PCR (Real Time quantitativeRevers Transcription PCR)Real-Time qRT-PCR is a major development of PCR, which enables reliabledetection and measurement of products generated during each cycle of thePCR process. There are currently several different chemistry, available forreal-time PCR and all of these allow detection of PCR products via the gener-ation of a fluorescent signal.
TaqMan probes are oligonucleotides that have a fluorescent reporter dyeattached to the 5’ end and a quencher moeity coupled to the 3’ end. Theseprobes are designed to hybridize to an internal region of a PCR product. In
23

the unhybridized state, the proximity of the fluor and the quench moleculesprevents the detection of fluorescent signal from the probe. During PCR, whenthe polymerase replicates a template on which a TaqManTMprobe is bound, the5’- nuclease activity of the polymerase cleaves the probe. This decouples thefluorescent and quenching dyes. Thus, fluorescence increases in each cycle,proportional to the amount of probe cleavage. Since PCR amplifies the targetexponentially, the fluorescence will increase rapidly during the reaction.
The relative amounts of the target during the exponential phase of the re-action are determined by plotting fluorescence against cycle number on a log-arithmic scale (thus an exponentially increasing quantity will give a straightline). A threshold for detection at which the fluorescence rises appreciablyabove the background level is determined. The cycle at which the fluores-cence from a sample crosses the threshold is called the crossing point (CP).The quantity of a target theoretically doubles every cycle during the expo-nential phase and relative amounts of DNA can be calculated, e.g. a samplewhose CP is 3 cycles earlier than another targets has 23 = 8 times more initialamount of DNA. Since all sets of primers don’t work equally well, one has tocalculate the reaction efficiency (E) first. Thus, by using this as the base andthe cycle difference CP as the exponent, the precise difference in starting tem-plate can be calculated. In the previous example, if the efficiency was 1.96,then the sample would have 7.53 times more template.
Amounts of the target can be determined by comparing the CP to a standardcurve produced by known amount of target. This is not always feasible and areference has to be used instead. The reference has to be expressed at constantlevels across a range of different conditions or tissues.
In our study we compared expression levels for micro-RNAs in samplestaken during and after treatment with controls taken before treatment. Thereal-time PCR efficiencies (E) for all probes were determined with linear re-gressions to dilution series. The relative expression ratio (RER) was calculatedwith equation (2.1) as described in [69]. Since all samples were done in fourreplicates an arithmetic mean was used (Eq. 2.3). Two unirradiated controlbiopsies were available for each patient and the mean for both controls wasused (Eq. 2.4).
RER =(Etarget)∆CPtarget
(Ere f erence)∆CPre f erence(2.1)
∆CP = C̄Pcontrol−C̄Psample (2.2)
C̄Pcontrol = ∑4i=1CPcontrol
4(2.3)
C̄Psample =∑
2i=1
∑4i=1 CPcontrol
42
(2.4)
24

3. Results and Discussion
During radiotherapy the skin is inevitably exposed to DNA damaging radia-tion and the treatment course is empirically adapted to cater for the effect innormal tissue. In this thesis we present a detailed study of these effects, andput forth observations that contradict several previous conceptions. In the firstpaper we quantify the DNA damage response in terms of DSB with a pre-viously developed method that measures focus forming proteins associatedwith DNA DSB-recognition and repair [71]. An initial dose-response was de-termined at 30 minutes after the first fraction and revealed a low dose hyper-sensitivity to doses below 0.3 Gy. Low dose hypersensitivity has previouslybeen reported for other end-points such as murine kidney function and skindamage [45, 46]. Similar responses were later also reported for human cellsin vitro [47] and basal keratinocytes in human skin [48]. However, the dose-response for DSB foci has been reported numerous times as being linear overa broad dose range [78, 79]. A second dose-response was determined at 30minutes after the last fraction during the first treatment week, and the lowdose hypersensitive response was persistent even after one week of fraction-ated radiotherapy.
In Paper I we also set out to determine the repair kinetics for DSBs. Themeasurements were made in additional biopsies taken 2 hours after fractiondelivery. However, no reduction in foci levels compared to biopsies taken after30 minutes could be detected. This suggests that the repair kinetics are slowerthan previously reported from several in vitro studies [7, 76, 77].
The method we have developed for DSB quantification is based on im-munofluorescence and proteins associated with DSB recognition, signallingand repair. In the first paper, we focus on γH2AX, a phosphorylated histoneprotein, which is phosphorylated in response to DSB induction. This phos-phorylation is fast but not instant and maximum phosphorylation levels arereported to occur around 30 minutes [75]. Since the initial DNA repair is avery rapid process, a substantial amount of DSB damage is believed to be re-paired within this time-frame. This implies that the foci levels we quantifyat 30 minutes are not the initial amounts of DSBs induced by radiation (Fig-ure 3.1).
We have not found any data that supports a non-linear induction of DSB,and hence we interpret our results to mean that the low dose hypersensitivitywe observe can be traced to dose-dependent repair capacity. The model pro-posed in the literature is a threshold activation of ATM, where low doses fail
25

0.0 0.5 1.0 1.5 2.00.0
0.5
1.0
1.5
2.0
Dose (Gy)
DS
B d
amag
e
0.0 0.5 1.0 1.5 2.00.0
0.5
1.0
1.5
2.0
DSB repair
Damageinduction
30 min
Figure 3.1: Interpretation of the low-dose hypersensitivity effect observed in nor-mal epidermal skin following DNA damage induction. Dose dependent differencesin the initial repair efficiencies could explain the observed dose-response relation-ships where doses below 0.3Gy display elevated levels of DSB-signalling foci. Itis also possible that such an effect could be correlated to dose-dependent activationthresholds of important damage response proteins such as ATM.
to trigger ATM [5, 78]. In our material it was not possible to measure ATMactivity, but we have observed similar threshold activation for protiens in as-sociated DNA damage pathways, such as p21.
It may seem contradictory that we could to detect repair during the first 30minutes, and no further repair during the next 90 minutes. The explanationwe propose is that the DNA damage and the following repair can be dividedinto a fast and slow component. The fast component is able to repair simpleDNA damage during the first 30 minutes, but more complicated breaks maypersist for several hours or even days. In biopsies collected 24h after fractiondelivery, approximately 10% of initial foci levels at 30 minutes remain. Thisimplies that H2AX is dephosphorylated and that foci do disappear over time,even though some foci may persist for more than 24 hours.
26

3.1 γH2AX as a marker for apoptosisSince H2AX is phosphorylated in response to DSB, γH2AX can be used todetect DNA fragmentation associated with apoptosis. In paper I we demon-strate that apoptosis can be quantified in paraffin embedded biopsies. Thisquantification provided an estimation of the dose-response at a time-point oneweek into fractionated radiotherapy. Apoptotic cells were infrequent and un-evenly distributed in the epidermis. The estimation of the apoptotic frequencywas further improved in subsequent articles where the amount of material wasincreased to compensate for the low frequency of apoptotic events.
There is a wide range of markers for apoptosis available on the market, andquite a few have passed through our laboratory without meeting our approval.The IHC markers focus on key proteins in different stages of the apoptoticprogram such as activated caspase-3 and cleaved-PARP-1. The terminal de-oxynucleotidyl transferase dUTP nick and labelling (TUNEL) assay detectsDNA fragmentation by labelling the terminal end of nucleic acids [42].
Markers for activated caspase-3 has been proposed as reliable indicators ofapoptosis that in many cases are more specific than the TUNEL test [44].Theaccuracy of the original TUNEL assay has been debated since necrotic cells insome cases may be inappropriately labeled as apoptotic [35]. Since neither ofthe conventional markers provided reliable apoptotic staining patterns in for-malin fixed epidermal tissue, we investigated the possibility of using γH2AXfor this purpose.
To corroborate the apoptotic status of intensely stained γH2AX positivecells we performed double stainings with cleaved-PARP-1 [16, 70, 82], an-other established marker for apoptosis. From our experience the approach withγH2AX has the benefit of detecting a late and irreversible step such as DNAfragmentation without detecting necrotic cells or DNA damage introduced inthe processing of the biopsy [70]. γH2AX also provides a much more intensestaining pattern compared to all the other apoptotic markers we have tested.The fact that these cells are negative for 53BP1 further supports the notion thatthese cells have reached a state where DNA repair is abolished in favour ofelimination by cell death. The apoptotic staining pattern of γH2AX was fur-ther corroborated by examining the morphology of these intensely γH2AX-stained cells.
3.2 Basal keratinocyte densityThe thinning of the skin is a clearly visible effect during fractionated radio-therapy treatment and is often a limiting factor. On a cellular level, the thin-ning of the skin can be expressed as number of keratinocytes per millimetre ofbasal layer. This measurement has been reported previously from our groupand others for biopsies from patients undergoing RT [37, 48].
27

In paper II we describe the thinning of the skin for 115 prostate cancer pa-tients during RT. Sets of biopsies were collected from the patients to describethe dose-response in the range 0.05–1.1 Gy, for the same patient at differenttime-points throughout the treatment. Additional biopsies were collected tomonitor the total dose-response from repeated fractions of 0.45 and 1.1 Gyfrom the same patient throughout the treatment. In paper III we have extendedthe dose range to 2 Gy by collecting biopsies from 31 breast cancer patientsat several time-points during treatment. Additional follow-up biopsies werecollected up to several weeks after treatment to monitor the regrowth of theskin.
This vast collection of biopsies enables us to describe the response to radia-tion, both as dose-response relationships at several time-points during RT andalso as total dose-response relationships to specific fraction doses during andafter RT.
3.2.1 Fraction dose responseBiopsies taken at the same time and exposed to fraction doses in the range0.05–1.1Gy enables us to determine a dose-response at various time-pointsthroughout the treatment. For this purpose, sets of biopsies were taken at 1,2.5, 3,4,5 and 6.5 weeks. Each of these time-points revealed low dose hyper-sensitivity with regards to basal keratinocyte density. It is worth highlightingthat the effect on the skin after four weeks of fractionated radiotherapy is al-most the same for fraction doses of 0.2, 0.4 and 1.1 Gy. This implies that itis not only the amount of inflicted DNA damage that determines the thinningof the skin, but how the damage is handled in terms of DNA repair, cell cyclecheckpoints and proliferation.
3.2.2 Total dose responseThe thinning of the skin can be described in a log-linear scale where BKD isa function of treatment time. This allows us to monitor the effect of a specificfraction dose sizes throughout the treatment. For fraction doses below 0.5 Gy,we find a linear reduction over time in the log-linear scale. For fraction dosesof 1.1 and 2.0 Gy, an accelerated reduction of keratinocytes is revealed duringthe second half of the treatment. The same result is found if BKD is plottedagainst total dose instead of treatment time. Classic radiobiology leads us toexpect equal effect per fraction, or even some reduced effect during the lat-ter part of treatment due to repopulation [26]. However, in our material wefound the opposite: for fraction doses of 1.1 and 2.0 Gy the effect per fractionincreased during the treatment period and the effect may be doubled towardsthe end of the treatment.
For fraction doses of 2.0 Gy we have collected biopsies at several time-points after treatment. These biopsies revealed that the thinning of the skin
28

continues after treatment cessation and a minimum in basal keratinocyte den-sity was reached one week after treatment. This is followed by a rapid recov-ery during the four following weeks and the skin often overcompensates andreaches higher BKD levels compared to un-irradiated control biopsies.
In healthy skin, the constant shedding of terminally differentiated cells iscompensated by newly produced keratinocytes in the basal layer. If cells areshed more rapidly from the surface than they are produced in the basal layerthe skin will inevitably experience an increased cell depletion. The sheddingfrom the surface is constant, but a number of factors can influence the prolif-eration rate in the basal layer. This process reflects the fact that the epidermaltissue has several possibilities to deal with induced damage. Removal of cellsfrom the proliferating compartments can potentially be handled not only byapoptosis and cell death, but also by sending cells into cell cycle arrest andterminal differentiation. Terminal differentiation may in many cases be ad-vantageous, since these cells, during their travel towards the skin surface, willcontribute to maintain the tissue structure while the risk of passing on badlyrepaired or damaged DNA to daughter cells is eliminated. Our observation ofan increased thickness of the cornfield skin layer towards the end of the treat-ment period suggests that terminal differentiation is an important part of theskin damage management.
3.3 Proliferation in terms of MitosisTo monitor the proliferation capacity in the skin we measured the number ofdividing cells in the basal layer. Dividing cells were identified with antibodiesagainst phospho-H3, a histone protein that is phosphorylated at serine 28, andis present in all stages of mitosis [41].
In the biopsies from prostate cancer patients we can determine the dose-response after one week of RT and after 6.5 weeks of RT. The dose-responseafter one week of RT, just before the first weekend break, displays a very dis-tinct low dose hypersensitivity and the mitotic reduction for 0.2 Gy is larger(even in absolute numbers) than for 0.45 and 1.1 Gy. Additional biopsies,taken after the first week end break, show no recovery in the mitotic frequencyafter the weekend. For 0.45 and 1.1 Gy dose fractions, mitotic frequencies areeven lower after the weekend compared to before. This implies that the 72 hweekend break is not enough to recover the proliferative capacity in the epi-dermis.
The dose-response after 6.5 weeks of RT is also low dose hypersensitiveand the levels are similar to those observed after one week. For fraction sizesof 0.45 and 1.1 Gy we monitored the number of mitotic cells throughout 6.5weeks of treatment. Mitosis was suppressed from week one and a minimumwas reached at three weeks for both 0.45 and 1.1 Gy. During the entire treat-ment the number of mitotic cells was severely repressed compared to un-
29

irradiated control biopsies. This provides a possible explanation for the lackof repopulation observed during the treatment, corroborating our conclusionsregarding the dose-dependent reductions in BKD.
In biopsies taken from breast cancer patients, we monitored the prolifer-ation capacity throughout the treatment and during the recovery phase aftertreatment. Our observations reveal that fraction sizes of 0.2 Gy can be as effec-tive in reducing mitosis as fraction sizes of 2.0 Gy. The mitosis is suppressedthroughout 5 weeks treatment for these breast cancer patients. One week afterthe end of the treatment the number of mitotic cells almost doubled comparedto un-irradiated control biopsies. Two weeks after the treatment, the levelswere four fold. After that, the mitotic cells dropped in number, although re-mained at elevated levels for ten weeks before dropping to normal levels.
3.4 ApoptosisApart from the shedding of terminally differentiated keratinocytes, cell deathdue to DNA damage and apoptosis can contribute to the reduction of the num-ber of cells in the skin during RT. In paper I we developed a method of quanti-fying apoptosis with γH2AX and in paper II we used this method to determinethe dose-response after 6.5 weeks. In paper III, we describe apoptotic levelsduring and after treatment.
The shape of the dose-response for apoptosis at 6.5 weeks resembled thedose-response of DDR foci. Compared with the first treatment week, a gen-eral increase in apoptosis was observed during the treatment period. The re-sponse was low dose hypersensitive with equal levels of apoptosis for fractionsizes of 0.2 Gy and 0.4 Gy. Fraction doses of 2.0 Gy resulted in twice as manyapoptotic cells as fraction doses of 1.1 Gy at the end of treatment, suggestingthat the fraction dose-response is more linear in the higher dose range.
When apoptotic frequency was determined during and after treatment withfraction doses of 2.0 Gy, a doubling of apoptosis was seen after two weeks ofRT. Apoptosis remained at that level until the last week of treatment, where thenumber of apoptotic cells increased dramatically. After treatment, apoptosisdecreases slowly, and even 5 weeks after treatment the levels remained twiceas high as in the un-irradiated control biopsies.
The burst of apoptosis at the last week of treatment preceded the increasein mitosis by more than one week. This suggests that the peak of apoptosisis not primarily a result of mitotic failures, but rather a result of pre-mitoticelimination. This is interesting since the importance of mitotic catastropheshave been emphasised as the dominant mode of cell-killing from ionizing ra-diation [95]. Our observation further stresses the influence of the cell cyclecheckpoints in the epidermal response to radiation. Rather than risking theconsequences of sending damaged cells into mitosis, it appears that damagedcells are efficiently removed from the cycling pool of cells.
30

3.5 DNA damageIn paper I we used γH2AX as a surrogate marker for DSBs. In paper III we ex-tended our study with an additional marker, 53BP1. Upon exposure to ionisingradiation, 53BP1 is hyperphosphorylated in an ATM-dependent manner andrelocalizes rapidly to discrete nuclear foci. These foci colocalise with γH2AXfoci. Furthermore, 53BP1 is required for the accumulation of p53 protein, G2-M checkpoint arrest and the intra-S-phase checkpoint in response to IR dam-age. Although a role for 53BP1 in DNA damage checkpoint has been shown,it is unclear whether 53BP1 plays a direct part in the repair of DNA DSBs [9].
In paper III the DNA damage was quantified extensively during and aftertreatment with three different methods: 1) 53BP1 foci were counted manuallyin a brightfield microscope in 100 consecutive keratinocytes along the basallayer per section. Two sections per biopsy were counted. 2) 53BP1 foci werequantified in immunofluorescence stained sections by digital image analysis.Approximately 250 cells per section and 3 sections per biopsy were analysed.3) γH2AX foci were quantified in immunofluorescence stained sections bydigital image analysis. Approximately 250 cells per section and 3 sections perbiopsy were analysed.
For manually quantified DSBs a decrease in numbers of 53BP1 foci per cellwas observed after the first fraction. The reduced foci numbers remained forthree weeks, but increased during the last week of treatment. After treatment,the foci per cell dropped to background levels.
For immunofluorescence stainings of 53BP1 and digital image analysisthere was no decrease in foci levels at any point during the treatment. Instead,a steady accumulation was found. After treatment, the foci levels dropped tobackground levels.
The digital image analysis of γH2AX stainings resembled the results fromthe 53BP1 analysis. Although the accumulation at the end of the treatment wasnot significant compared to initial levels there was a trend. After treatment thefoci per cell dropped to background levels.
From our experience, the immunofluorescence staining for 53BP1 produceda more distinct and intense signal compared to γH2AX. In terms of inten-sity, the range of individual 53BP1 foci, exceeded the dynamic range of ourCCD camera. This inevitably had the effect that some of the weaker foci re-mained undetected while some of the most intense foci were overexposed.Since 53BP1 is constitutively expressed in the cell nucleus and the antibodyis very sensitive, some foci-like structures may be detected in un-irradiatedcontrols resulting in what would be perceived as higher background.
In theory γH2AX should be superior; since it is a phospho-specific anti-body the background noise should be low. However, from our measurementsthe formalin fixation of the biopsies had a negative impact on the signal andconsequently the signal-to-noise ratio is still lower compared to 53BP1.
31

One should keep in mind when comparing methods using different antibod-ies that anything quantified is a relative measure. In our case, although bothantibodies should detect proteins associated with the same DSB, the amountof protein may differ as may the specificity of the primary and secondary an-tibody. Different fluorophores have different emission spectra and dependingon filter and camera model the sensitivity for different wavelength may differ.However, if great care is taken to optimise or at least standardise as many stepsof the method as possible, the relative measurement will be reliable.
The same 53BP1 antibody was used for both manual scoring and digitalimage analysis. The secondary detection system differs however for the twomethods. Digital image analysis is based on images of immunofluorescencestainings, whereas manual scoring is performed on DAB stained sections in abrightfield microscope. From our experience, the dynamic of the fluorescencesignal is larger and more linear compared to the DAB stainings. In the protocolfor DAB stainings there was an amplification step, which increased the signal.This step has however been shown to introduce some non-linearity.
In the manual analysis we measured the number of foci per cell whereaswith digital image analysis we measured the number of foci per nuclear area.The measurement used in the digital image analysis is independent of differ-ences in cell size due to cell cycle phase. Furthermore only keratinocytes in thebasal layer were scored in the manual analysis, whereas all cells in epidermiswere quantified in the digital image analysis.
3.6 Cell cycle checkpointsThe p21 kinase inhibitor is a key regulator of checkpoints, proliferation, dif-ferentiation, and senescence following radiation induced DNA damage [1,28,63].
In our material we found that p21 activation is very sensitive and fractiondoses of 0.05 Gy after one week radiotherapy was sufficient to trigger an in-creased expression. The dose-response is low dose hypersensitive after oneweek as well as after 6.5 weeks. In biopsies taken before and after the firstweekend break, no decrease in p21 could be detected after 72 hours of recov-ery. This suggests that the cell cycle arrest is persistent and activated over theweekend, which can explain the previously observed suppression of mitosisover weekend breaks.
When comparing biopsies from prostate cancer patients collected at thefirst and last week of treatment, an accumulation is evident. At the last weekof treatment, more than 70% of the basal keratinocytes are p21 positive forfraction doses of 1.1 Gy. For fraction doses of 2.0 Gy given to breast cancerpatients, similar amounts of p21 positive cells were found at the last week oftreatment. For fraction doses of 2.0 Gy, our biopsy material allowed us to studythe p21 response during and after treatment. During the first half of treatment
32

there was a steady accumulation of p21. However during the latter part therewas an accelerated expression of p21 in basal keratinocytes. This acceleratedincrease in p21 mirrored the accelerated reduction of basal keratinocyte den-sity previously described. After treatment, p21 was slowly reduced and even5 weeks after treatment, p21 levels remain above initial levels.
For skin biopsies collected from prostate cancer patients, the quantificationof p21 was done both manually and semi-automated with digital image anal-ysis. The results were in good agreement for both methods. The digital imageanalysis enabled us to measure more parameters, such as staining intensity,and this can provide important information especially if the protein expres-sion is up-regulated and accumulated in a majority of cells.
In the first three papers we used immunohistochemistry and differentmolecular markers in order to analyse the response to DNA damage inparaffin embedded biopsies. In paper IV, we apply an additional technique:Real-Time qRT-PCR to study micro-RNA another entity involved inthe DDR. We have focused on three micro-RNAs involved in cell cyclecheckpoints, apoptosis and differentiation respectively. In this last paper wehave also made an attempt to compare the response in the acute and lateresponding parts of the skin epidermis and dermis. To achieve this, sectionswere taken from skin biopsies collected from breast cancer patients andmicrodissected into epidermis and dermis.
Immunostainings for p53 were made in corresponding sections to monitorthe protein expression. During treatment, p53 was expressed in almost ev-ery cell and the intensity of the staining increased with time and total dose,similarily for both epidermis and dermis. After treatment, the staining pat-tern changed. In epidermis, the cell population became more heterogenous.Intensely stained keratinocytes slowly migrated towards the skin surface, andan increased number of p53 negative cells were observed in the basal layer.In dermis, the p53 expression remained elevated for several weeks after treat-ment, in the majority of the cells.
p53 is phosphorylated at multiple sites in response to DNA DSB and reg-ulates the switch between cell cycle arrest and apoptosis. MiR-34a is up-regulated by p53, which plays a central part in the response to DNA damage.During radiotherapy miR-34a is up-regulated and accumulates in both epider-mis and dermis. No decrease in miR-34a could be seen in biopsies taken be-fore and after weekend breaks during the treatment. After treatment, miR-34alevels slowly decreased, but even 5 weeks after treatment levels were aboveinitial levels. During treatment, no difference could be observed between epi-dermis and dermis. The accumulation is similar both in terms of absolute lev-els and over time. However after treatment, the miR-34a levels in epidermisdropped more rapidly compared to dermis.
An extensive quantification of p21 expression revealed a pattern that cor-responded to that observed for miR-34a. Previous knowledge regarding thesedamage response pathways states that both mir-34a and p21 are regulated, in
33

parallel pathways, by p53, which could explain these similarities [1, 40]. Acomparison between the dermal and epidermal responses revealed an interest-ing difference in the p21 expression levels after treatment. While the inductionof the p21 expression increased continuously for both cellular compartmentsduring treatment, expression levels decreased faster for epidermal cells thanfor dermal cells after treatment.
Persistent dermal expression of both p21 and miR-34a after treatment wasrevealed. It is tempting to speculate that these patterns correlate to the “early”and “late” effects that are observed in these normal tissues during and afterradiotherapy. The persistent p21 response in the dermis could be a sign ofincreased levels of persistent damage and senescence, which at a later stagecould be correlated to the late effects observed in dermal regions of the skin.Future investigations will determine whether this is the case. Our current re-sults do however reveal that the major difference between the epidermal anddermal response is observed during the tissue recovery period rather than dur-ing the damage inducing treatment period.
34

4. Summary
Experience from the clinic has proven that fractionation has a positive effecton normal tissue during radiotherapy. It is however still unclear what factorsgovern this positive effect. The time required for the normal tissue to recoverand cell repopulation have been proposed.
From our biopsies we were able to determine the low dose hypersensitiveeffect on mitosis. The mitosis is almost equally suppressed for fraction dosesof 0.2 Gy and 2.0 Gy, and this effect remains for the entire treatment period.
For basal keratinocyte density depletion we have established low-dose hy-persensitivity for fraction doses below ∼0.3 Gy, i.e the effect per dose unit ishigher than expected in comparison with dose fractions above ∼1.0 Gy. Thedepletion is however greater for a higher total dose. This implies that eventhough proliferation in terms of mitosis is equally suppressed, the skin be-comes thinner for higher fraction doses.
We consider the number of mitotic cells per millimetre as a measure ofproliferation, and an average of how quickly the cell cycle is proceeding. Ifthe mitosis is very low and practically equal for all fraction doses, then thelarger effect on basal keratinocyte depletion for higher fraction doses has tobe explained in terms of cells disappearing through terminal differentiation orapoptosis (Fig 4.1).
Even though suppression of mitosis is not greatly affected by fraction ortotal dose, the number of DSB foci, the p21 expression and the frequency ofapoptosis are dependent on both dose per fraction and total dose. For frac-tion doses of 2.0 Gy, we detected a burst of apoptosis during the last week ofradiotherapy that precedes the up-regulation of mitosis by a week. This sug-gests that pre-mitotic cell death contributes to the basal keratinocyte depletionduring treatment.
In a tissue such as the skin, terminal differentiation may be an alternativeway to apoptosis in the disposal of damaged cells. Through terminal differen-tiation the damaged cell will be stopped from further divisions and the poten-tially faulty DNA will not be multiplied. The cell will however still carry onits role in the tissue and function as a barrier.
In our material we have biopsies taken before and after weekend breaks forfractions doses in the range of 0.05–2.0Gy throughout the treatment. Pairwiseanalysis of these biopsies has not revealed any consistent change for numberof DSB foci, p21, miR-34a, mitosis, apoptosis and BKD. This suggests thatthe amount of recovery during the weekend breaks was limited.
35

S
G2
M
G1
G2arrest
G0arrest
G1arrest
Senescence
Terminaldi�erentiation
Terminaldi�erentiation
Apoptosis
Mitotic failure
Apoptosis
Figure 4.1: The keratinocyte response during radiotherapy is primarily determinedby checkpoints and pre-mitotic cell elimination. Epidermal DNA damage results ina rapid removal of cells from the cell cycle, reflected by an immediate p21 up-regulation. The effective checkpoint regulation is further emphasised by the obser-vation of suppressed of mitotic rates, lasting throughout the treatment period.
In addition to the absence of recovery during weekend breaks, no acceler-ated repopulation during treatment could be observed for any fraction dose.Instead, we found an increased depletion rate of basal keratinocytes duringthe latter part of radiotherapy for fraction doses above 1.0 Gy. This findingwas also reflected in the increasing intensity of DSB foci, p21, miR-34a andapoptosis.
Even though no recovery could be detected during weekend breaks or dur-ing treatment, there was an effective recovery process after treatment. Thebasal keratinocyte density continues to drop one week after treatment, but isfollowed by a dramatic repopulation in epidermis. Although levels of p21,miR-34a and apoptosis remained high for several weeks after treatment basalkeratinocyte density doubled during one week of intense repopulation withmitosis levels being four times as high as in un-irradiated controls.
During treatment the response to radiation induced DNA damage assessedby p21 and miR-34a is similar in epidermis and dermis. However after treat-
36

ment there was a difference, where the DNA damage response is more persis-tent in the dermis compared to epidermis. This suggests that the difference inacute and late responding tissue is not found during treatment, but rather inthe recovery process.
37


5. Acknowledgements
This thesis has been a long journey, and along the way I have met a greatnumber of people. It is a pleasure to convey my gratitude to them all in myhumble acknowledgment.
In the first place I would like to express my gratitude to Fredrik, my con-stant and trusted companion. You have followed me every step of the way,and we have shared triumphs and defeats alike. I cannot imagine someone Iwould rather make this trip with. Lately, Fredrik has been a trailblazer andhas proven to me that there is an end, even to this travel. I am for ever in hisdebt for his help and guidance this last step of the way. I would also like tothank his companion, Fiona. She has helped me navigate the treacherous wa-ters they call the english language. Unfortunately, I could not let her read thisacknowledgements, so I am out on my own on this one.
I would like to thank my supervisor, professor Ingela Turesson, for her tena-cious passion for research and her vast clinical experience. The excellent skinbiopsy material you have collected throughout the years is invaluable. For this,your collaborators in Gothenburg: Jan, Ingegerd, Karl-Axel and Ragnhild de-serve a special thanks.
In Uppsala I have had the privilege to work amongst people with a diverseset of skills and backgrounds. Their accumulated experience has broadenedmy perspective on the practical aspects of research and life in general. Specialthanks to Majlis for numerous talks and your specific knowledge regardingimmunohistochemistry. Thanks to Sunna, for counting endless numbers oftissue sections with infinite patience, and your esoteric wisdom. Thanks alsoto Ulf, for keeping me updated on “blocket.se”-bargains and your contagiouslaughter. Many thanks to Mattias for introducing me to Spanish delicacies,and providing for me and my wife’s food cravings. In particular, I would liketo thank Nognit, for your ways of helping me getting out of rotten bananas.
I am proud to share my last name with Didde, and grateful for all yoursupport. You have a way of making sense of this crazy world and lighteneveryone’s spirit.
On behalf of the oncology department; thanks to Gunilla Enblad and JanNyman for signing up as co-supervisors.
Thanks to everyone, who has sitten down at our coffee table, and madeour “fika”-discussions a bit more interesting. Thanks to Ingrid, Daniel, Marie,Anders, Gustaf, Linda, Xuping and Maryam. I also extend my thanks to ourneighbouring BMS-corridor, in particular to Jörgen, Bosse and Gedda.
39

At times, when I have not been able to meet people in real life, I have hadthe luxury to visit my favourite on-line communities hospaul.net and swedish-simracers.com. To have instant access to this wealth of knowledge and inspi-ration, is truly amazing. You can always depend on knowledgeable responsesand get someone to explain the intricacies of game theory, computer hardware,limited slip differentials and life in general.
For some years, I have played in the bluegrass band Moonshine. They havebecome my second family and helped me express my bottled-up feelings mu-sically. Many thanks to Åse, Uffe, Christer, Per and Svalle.
I am grateful for my newly found friend, career- and lifecoach, Magnus.Together we encourage each other to explore unknown territories, such asrepairing brake servos and the art of home-brewing. I would also like to thankHenkka for his contributions to these excursions, and for sharing my interestto burn digital rubber on laser-scanned tracks.
My deepest gratitude goes to my family for their love and support through-out my life. My parents, for always being there, and our discussions abouteverything in life. My sister Marika, who has given me a valuable and humbleperspective on life.
Endless thanks to my wonderful wife, Anne. I am forever grateful for yourlove.
Last but not least, my amazing daughter Fanny. I love you so much, andyou help me rediscover everything important in life. I promise you, when thisjourney is over we will have more time to indulge ourselves in playing video-games.
40

Bibliography
[1] Tarek Abbas and Anindya Dutta. p21 in cancer: intricate networks and mul-tiple activities. Nature Reviews. Cancer, 9(6):400–414, June 2009. PMID:19440234.
[2] Bruce Alberts, Alexander Johnson, Julian Lewis, Martin Raff, Keith Roberts,and Peter Walter. Chapter 4. chromosomal DNA and its packaging in the chro-matin fiber. In Molecular Biology of the Cell, Fourth Edition. Garland Science,4 edition, March 2002.
[3] Y Andegeko, L Moyal, L Mittelman, I Tsarfaty, Y Shiloh, and G Rotman. Nu-clear retention of ATM at sites of DNA double strand breaks. The Journal of Bi-ological Chemistry, 276(41):38224–38230, October 2001. PMID: 11454856.
[4] L Anderson, C Henderson, and Y Adachi. Phosphorylation and rapid relocal-ization of 53BP1 to nuclear foci upon DNA damage. Molecular and CellularBiology, 21(5):1719–1729, March 2001. PMID: 11238909.
[5] Christopher J Bakkenist and Michael B Kastan. DNA damage activates ATMthrough intermolecular autophosphorylation and dimer dissociation. Nature,421(6922):499–506, January 2003. PMID: 12556884.
[6] S Banin, L Moyal, S Shieh, Y Taya, C W Anderson, L Chessa, N I Smorodin-sky, C Prives, Y Reiss, Y Shiloh, and Y Ziv. Enhanced phosphorylationof p53 by ATM in response to DNA damage. Science (New York, N.Y.),281(5383):1674–1677, September 1998. PMID: 9733514.
[7] Judit P Banáth, Susan H Macphail, and Peggy L Olive. Radiation sensitivity,H2AX phosphorylation, and kinetics of repair of DNA strand breaks in irradi-ated cervical cancer cell lines. Cancer Research, 64(19):7144–7149, October2004. PMID: 15466212.
[8] G W Barendsen, C Van Bree, and N A Franken. Importance of cell prolif-erative state and potentially lethal damage repair on radiation effectiveness:implications for combined tumor treatments (review). International Journal ofOncology, 19(2):247–256, August 2001. PMID: 11445835.
[9] Simon Bekker-Jensen and Niels Mailand. Assembly and function of DNAdouble-strand break repair foci in mammalian cells. DNA Repair, October2010. PMID: 21035408.
[10] Cédric Blanpain and Elaine Fuchs. Epidermal homeostasis: a balancing act ofstem cells in the skin. Nature Reviews. Molecular Cell Biology, 10(3):207–217,March 2009. PMID: 19209183.
41

[11] Guido T Bommer, Isabelle Gerin, Ying Feng, Andrew J Kaczorowski, RorkKuick, Robert E Love, Yali Zhai, Thomas J Giordano, Zhaohui S Qin,Bethany B Moore, Ormond A MacDougald, Kathleen R Cho, and Eric RFearon. p53-mediated activation of miRNA34 candidate tumor-suppressorgenes. Current Biology: CB, 17(15):1298–1307, August 2007. PMID:17656095.
[12] William M Bonner. Phenomena leading to cell survival values which deviatefrom linear-quadratic models. Mutation Research, 568(1):33–39, December2004. PMID: 15530537.
[13] William M Bonner, Christophe E Redon, Jennifer S Dickey, Asako JNakamura, Olga A Sedelnikova, Stéphanie Solier, and Yves Pommier.GammaH2AX and cancer. Nature Reviews. Cancer, 8(12):957–967, December2008. PMID: 19005492.
[14] Fanny Bouquet, Catherine Muller, and Bernard Salles. The loss ofgammaH2AX signal is a marker of DNA double strand breaks repair only atlow levels of DNA damage. Cell Cycle (Georgetown, Tex.), 5(10):1116–1122,May 2006. PMID: 16721046.
[15] S Burma, B P Chen, M Murphy, A Kurimasa, and D J Chen. ATM phospho-rylates histone H2AX in response to DNA double-strand breaks. The Jour-nal of Biological Chemistry, 276(45):42462–42467, November 2001. PMID:11571274.
[16] I Böhm. [The apoptosis marker enzyme poly-(ADP-ribose) polymerase(PARP) in systemic lupus erythematosus]. Zeitschrift Für Rheumatologie,65(6):541–544, October 2006. PMID: 16541210.
[17] C E Canman, D S Lim, K A Cimprich, Y Taya, K Tamai, K Sakaguchi,E Appella, M B Kastan, and J D Siliciano. Activation of the ATM kinaseby ionizing radiation and phosphorylation of p53. Science (New York, N.Y.),281(5383):1677–1679, September 1998. PMID: 9733515.
[18] Arkady Celeste, Oscar Fernandez-Capetillo, Michael J Kruhlak, Duane RPilch, David W Staudt, Alicia Lee, Robert F Bonner, William M Bonner, andAndré Nussenzweig. Histone H2AX phosphorylation is dispensable for theinitial recognition of DNA breaks. Nature Cell Biology, 5(7):675–679, July2003. PMID: 12792649.
[19] Tsung-Cheng Chang, Erik A Wentzel, Oliver A Kent, Kalyani Ramachandran,Michael Mullendore, Kwang Hyuck Lee, Georg Feldmann, Munekazu Ya-makuchi, Marcella Ferlito, Charles J Lowenstein, Dan E Arking, Michael ABeer, Anirban Maitra, and Joshua T Mendell. Transactivation of miR-34a byp53 broadly influences gene expression and promotes apoptosis. MolecularCell, 26(5):745–752, June 2007. PMID: 17540599.
[20] H T Chen, A Bhandoola, M J Difilippantonio, J Zhu, M J Brown, X Tai, E PRogakou, T M Brotz, W M Bonner, T Ried, and A Nussenzweig. Response
42

to RAG-mediated VDJ cleavage by NBS1 and gamma-H2AX. Science (NewYork, N.Y.), 290(5498):1962–1965, December 2000. PMID: 11110662.
[21] Dipanjan Chowdhury, Michael-Christopher Keogh, Haruhiko Ishii, Craig L Pe-terson, Stephen Buratowski, and Judy Lieberman. gamma-H2AX dephospho-rylation by protein phosphatase 2A facilitates DNA double-strand break repair.Molecular Cell, 20(5):801–809, December 2005. PMID: 16310392.
[22] F Chronis and E P Rogakou. Chapter 13. interplay between gammaH2AX and53BP1 pathways in DNA Double-Strand break repair response. In Apoptosis,Senescence and Cancer, pages 243–263. Humana Press, 2 edition, December2007.
[23] Amelia Cimmino, George Adrian Calin, Muller Fabbri, Marilena V Iorio,Manuela Ferracin, Masayoshi Shimizu, Sylwia E Wojcik, Rami I Aqeilan, Si-mona Zupo, Mariella Dono, Laura Rassenti, Hansjuerg Alder, Stefano Volinia,Chang-Gong Liu, Thomas J Kipps, Massimo Negrini, and Carlo M Croce.miR-15 and miR-16 induce apoptosis by targeting BCL2. Proceedings of theNational Academy of Sciences of the United States of America, 102(39):13944–13949, September 2005. PMID: 16166262.
[24] Philip J Coates, Sally A Lorimore, Kirsten J Lindsay, and Eric G Wright.Tissue-specific p53 responses to ionizing radiation and their genetic modifica-tion: the key to tissue-specific tumour susceptibility? The Journal of Pathology,201(3):377–388, November 2003. PMID: 14595749.
[25] David C Corney, Andrea Flesken-Nikitin, Andrew K Godwin, Wei Wang, andAlexander Yu Nikitin. MicroRNA-34b and MicroRNA-34c are targets of p53and cooperate in control of cell proliferation and adhesion-independent growth.Cancer Research, 67(18):8433–8438, September 2007. PMID: 17823410.
[26] Albert Van der Kogel and Michael Joiner. Basic Clinical Radiobiology. AHodder Arnold Publication, 4th edition, May 2009.
[27] E Dikomey. Induction and repair of DNA strand breaks in x-irradiated prolif-erating and quiescent CHO cells. International Journal of Radiation Biology,57(6):1169–1182, June 1990. PMID: 1971842.
[28] W S el-Deiry, T Tokino, V E Velculescu, D B Levy, R Parsons, J M Trent,D Lin, W E Mercer, K W Kinzler, and B Vogelstein. WAF1, a potential medi-ator of p53 tumor suppression. Cell, 75(4):817–825, November 1993. PMID:8242752.
[29] M Elkind and G Whitmore. The radiobiology of cultured mammalian cells.Gordon and Breach, New York, 1967.
[30] Jacob Falck, Julia Coates, and Stephen P Jackson. Conserved modes of re-cruitment of ATM, ATR and DNA-PKcs to sites of DNA damage. Nature,434(7033):605–611, March 2005. PMID: 15758953.
43

[31] Martin Falk, Emilie Lukasova, and Stanislav Kozubek. Higher-order chromatinstructure in DSB induction, repair and misrepair. Mutation Research, 704(1-3):88–100, June 2010. PMID: 20144732.
[32] Peiwen Fei, Eric J Bernhard, and Wafik S El-Deiry. Tissue-specific inductionof p53 targets in vivo. Cancer Research, 62(24):7316–7327, December 2002.PMID: 12499275.
[33] Oscar Fernandez-Capetillo, Alicia Lee, Michel Nussenzweig, and AndréNussenzweig. H2AX: the histone guardian of the genome. DNA Repair, 3(8-9):959–967, September 2004. PMID: 15279782.
[34] Elizabeth Garner and Kenneth Raj. Protective mechanisms of p53-p21-pRbproteins against DNA damage-induced cell death. Cell Cycle (Georgetown,Tex.), 7(3):277–282, February 2008. PMID: 18235223.
[35] B Grasl-Kraupp, B Ruttkay-Nedecky, H Koudelka, K Bukowska, W Bursch,and R Schulte-Hermann. In situ detection of fragmented DNA (TUNEL as-say) fails to discriminate among apoptosis, necrosis, and autolytic cell death:a cautionary note. Hepatology (Baltimore, Md.), 21(5):1465–1468, May 1995.PMID: 7737654.
[36] Andrei V Gudkov and Elena A Komarova. The role of p53 in determiningsensitivity to radiotherapy. Nature Reviews. Cancer, 3(2):117–129, February2003. PMID: 12563311.
[37] Jackie Harney, Nihal Shah, Susan Short, Francis Daley, Nicki Groom,George D Wilson, Michael C Joiner, and Michele I Saunders. The evalua-tion of low dose hyper-radiosensitivity in normal human skin. Radiotherapyand Oncology: Journal of the European Society for Therapeutic Radiology andOncology, 70(3):319–329, March 2004. PMID: 15064019.
[38] J W Harper, G R Adami, N Wei, K Keyomarsi, and S J Elledge. The p21 cdk-interacting protein cip1 is a potent inhibitor of g1 cyclin-dependent kinases.Cell, 75(4):805–816, November 1993. PMID: 8242751.
[39] Lin He, Xingyue He, Lee P Lim, Elisa de Stanchina, Zhenyu Xuan, Yu Liang,Wen Xue, Lars Zender, Jill Magnus, Dana Ridzon, Aimee L Jackson, Peter SLinsley, Caifu Chen, Scott W Lowe, Michele A Cleary, and Gregory J Han-non. A microRNA component of the p53 tumour suppressor network. Nature,447(7148):1130–1134, June 2007. PMID: 17554337.
[40] H Hermeking. The miR-34 family in cancer and apoptosis. Cell Death andDifferentiation, 17(2):193–199, February 2010. PMID: 19461653.
[41] Akihiro Hirata, Ken-Ichi Inada, Tetsuya Tsukamoto, Hiroki Sakai, TsutomuMizoshita, Tokuma Yanai, Toshiaki Masegi, Hidemasa Goto, Masaki Inagaki,and Masae Tatematsu. Characterization of a monoclonal antibody, HTA28, rec-ognizing a histone h3 phosphorylation site as a useful marker of m-phase cells.The Journal of Histochemistry and Cytochemistry: Official Journal of the His-tochemistry Society, 52(11):1503–1509, November 2004. PMID: 15505345.
44

[42] Hana Holubec, Claire M Payne, Harris Bernstein, Katerina Dvorakova, CarolBernstein, Caroline N Waltmire, James A Warneke, and Harinder Garewal. As-sessment of apoptosis by immunohistochemical markers compared to cellularmorphology in ex vivo-stressed colonic mucosa. The Journal of Histochemistryand Cytochemistry: Official Journal of the Histochemistry Society, 53(2):229–235, February 2005. PMID: 15684335.
[43] L C Huang, K C Clarkin, and G M Wahl. Sensitivity and selectivity of theDNA damage sensor responsible for activating p53-dependent g1 arrest. Pro-ceedings of the National Academy of Sciences of the United States of America,93(10):4827–4832, May 1996. PMID: 8643488.
[44] Jera Jeruc, Alenka Vizjak, Blaz Rozman, and Dusan Ferluga. Immunohis-tochemical expression of activated caspase-3 as a marker of apoptosis inglomeruli of human lupus nephritis. American Journal of Kidney Diseases: TheOfficial Journal of the National Kidney Foundation, 48(3):410–418, September2006. PMID: 16931214.
[45] M C Joiner and J Denekamp. The effect of small radiation doses on mouse skin.The British Journal of Cancer. Supplement, 7:63–66, 1986. PMID: 3459542.
[46] M C Joiner and S B Field. The response of mouse skin to irradiation withneutrons from the 62 MV cyclotron at clatterbridge, U.K. Radiotherapy andOncology: Journal of the European Society for Therapeutic Radiology and On-cology, 12(2):153–166, June 1988. PMID: 3406459.
[47] M C Joiner, P Lambin, E P Malaise, T Robson, J E Arrand, K A Skov, andB Marples. Hypersensitivity to very-low single radiation doses: its relation-ship to the adaptive response and induced radioresistance. Mutation Research,358(2):171–183, November 1996. PMID: 8946022.
[48] M C Joiner, B Marples, P Lambin, S C Short, and I Turesson. Low-dose hyper-sensitivity: current status and possible mechanisms. International Journal ofRadiation Oncology, Biology, Physics, 49(2):379–389, February 2001. PMID:11173131.
[49] Gary D Kao, W Gillies McKenna, Matthew G Guenther, Ruth J Muschel,Mitchell A Lazar, and Tim J Yen. Histone deacetylase 4 interacts with 53BP1 tomediate the DNA damage response. The Journal of Cell Biology, 160(7):1017–1027, March 2003. PMID: 12668657.
[50] Michael B Kastan. DNA damage responses: mechanisms and roles in humandisease: 2007 G.H.A. clowes memorial award lecture. Molecular Cancer Re-search: MCR, 6(4):517–524, April 2008. PMID: 18403632.
[51] Andrea Kinner, Wenqi Wu, Christian Staudt, and George Iliakis. Gamma-H2AX in recognition and signaling of DNA double-strand breaks in the con-text of chromatin. Nucleic Acids Research, 36(17):5678–5694, October 2008.PMID: 18772227.
45

[52] Kageaki Kuribayashi and Wafik S El-Deiry. Regulation of programmed celldeath by the p53 pathway. Advances in Experimental Medicine and Biology,615:201–221, 2008. PMID: 18441595.
[53] Alicia C Lee, Oscar Fernandez-Capetillo, Venkat Pisupati, Stephen P Jackson,and André Nussenzweig. Specific association of mouse MDC1/NFBD1 withNBS1 at sites of DNA-damage. Cell Cycle (Georgetown, Tex.), 4(1):177–182,January 2005. PMID: 15611643.
[54] A M Lena, R Shalom-Feuerstein, P Rivetti di Val Cervo, D Aberdam, R AKnight, G Melino, and E Candi. miR-203 represses ’stemness’ by repress-ing DeltaNp63. Cell Death and Differentiation, 15(7):1187–1195, July 2008.PMID: 18483491.
[55] Lee P Lim, Nelson C Lau, Philip Garrett-Engele, Andrew Grimson, Janell MSchelter, John Castle, David P Bartel, Peter S Linsley, and Jason M Johnson.Microarray analysis shows that some microRNAs downregulate large num-bers of target mRNAs. Nature, 433(7027):769–773, February 2005. PMID:15685193.
[56] S P Linke, K C Clarkin, and G M Wahl. p53 mediates permanent arrestover multiple cell cycles in response to gamma-irradiation. Cancer Research,57(6):1171–1179, March 1997. PMID: 9067289.
[57] Markus Löbrich and Penny A Jeggo. The impact of a negligent G2/M check-point on genomic instability and cancer induction. Nature Reviews. Cancer,7(11):861–869, November 2007. PMID: 17943134.
[58] E Marková, N Schultz, and I Y Belyaev. Kinetics and dose-response of residual53BP1/gamma-H2AX foci: co-localization, relationship with DSB repair andclonogenic survival. International Journal of Radiation Biology, 83(5):319–329, May 2007. PMID: 17457757.
[59] Lawrence B Marks, Ellen D Yorke, Andrew Jackson, Randall K Ten Haken,Louis S Constine, Avraham Eisbruch, Søren M Bentzen, Jiho Nam, andJoseph O Deasy. Use of normal tissue complication probability models in theclinic. International Journal of Radiation Oncology, Biology, Physics, 76(3Suppl):S10–19, March 2010. PMID: 20171502.
[60] B Marples, SA Krueger, S J Collis, A J Chalmers, and M C Joiner. Chap-ter 19. low dose Hyper-Radiosensitivity: a historical perspective. In TargetedRadionuclide Tumor Therapy, pages 329–347. Springer, Netherlands, 2008.
[61] B Marples, B G Wouters, S J Collis, A J Chalmers, and M C Joiner. Low-dose hyper-radiosensitivity: a consequence of ineffective cell cycle arrestof radiation-damaged g2-phase cells. Radiation Research, 161(3):247–255,March 2004. PMID: 14982490.
[62] Brian Marples and Spencer J Collis. Low-dose hyper-radiosensitivity: past,present, and future. International Journal of Radiation Oncology, Biology,Physics, 70(5):1310–1318, April 2008. PMID: 18374221.
46

[63] Babak J Mehrara, Tomer Avraham, Marc Soares, John G Fernandez, AlanYan, Jamie C Zampell, Victor P Andrade, Andrew P Cordeiro, and Cristina MSorrento. p21cip/WAF is a key regulator of long-term radiation damage inmesenchyme-derived tissues. The FASEB Journal: Official Publication ofthe Federation of American Societies for Experimental Biology, August 2010.PMID: 20720160.
[64] AJ Mundt, JC Roeske, TD Chung, and RR Weichselbaum. Sect 9:39: Prin-ciples of radiation oncology, biologic basis of radiation therapy. In CancerMedicine 6. B.C. Decker Inc, London, 6 edition, 2003.
[65] Asako J Nakamura, Y Jeffrey Chiang, Karen S Hathcock, Izumi Horikawa,Olga A Sedelnikova, Richard J Hodes, and William M Bonner. Both telom-eric and non-telomeric DNA damage are determinants of mammalian cellularsenescence. Epigenetics & Chromatin, 1(1):6, 2008. PMID: 19014415.
[66] J Nyman and I Turesson. Basal cell density in human skin for various fraction-ation schedules in radiotherapy. Radiotherapy and Oncology: Journal of theEuropean Society for Therapeutic Radiology and Oncology, 33(2):117–124,November 1994. PMID: 7708954.
[67] R B Painter and B R Young. Radiosensitivity in ataxia-telangiectasia: a newexplanation. Proceedings of the National Academy of Sciences of the UnitedStates of America, 77(12):7315–7317, December 1980. PMID: 6938978.
[68] T T Paull, E P Rogakou, V Yamazaki, C U Kirchgessner, M Gellert, and W MBonner. A critical role for histone H2AX in recruitment of repair factors tonuclear foci after DNA damage. Current Biology: CB, 10(15):886–895, August2000. PMID: 10959836.
[69] M W Pfaffl. A new mathematical model for relative quantification in real-timeRT-PCR. Nucleic Acids Research, 29(9):e45, May 2001. PMID: 11328886.
[70] O F Qvarnström, M Simonsson, V Eriksson, I Turesson, and J Carlsson.gammaH2AX and cleaved PARP-1 as apoptotic markers in irradiated breastcancer BT474 cellular spheroids. International Journal of Oncology, 35(1):41–47, July 2009. PMID: 19513550.
[71] Olov Fredrik Qvarnström, Martin Simonsson, Karl-Axel Johansson, Jan Ny-man, and Ingela Turesson. DNA double strand break quantification in skinbiopsies. Radiotherapy and Oncology: Journal of the European Societyfor Therapeutic Radiology and Oncology, 72(3):311–317, September 2004.PMID: 15450730.
[72] I Rappold, K Iwabuchi, T Date, and J Chen. Tumor suppressor p53 bindingprotein 1 (53BP1) is involved in DNA damage-signaling pathways. The Jour-nal of Cell Biology, 153(3):613–620, April 2001. PMID: 11331310.
[73] Nina Raver-Shapira, Efi Marciano, Eti Meiri, Yael Spector, Nitzan Rosenfeld,Neta Moskovits, Zvi Bentwich, and Moshe Oren. Transcriptional activation of
47

miR-34a contributes to p53-mediated apoptosis. Molecular Cell, 26(5):731–743, June 2007. PMID: 17540598.
[74] E P Rogakou, C Boon, C Redon, and W M Bonner. Megabase chromatindomains involved in DNA double-strand breaks in vivo. The Journal of CellBiology, 146(5):905–916, September 1999. PMID: 10477747.
[75] E P Rogakou, W Nieves-Neira, C Boon, Y Pommier, and W M Bonner. Initia-tion of DNA fragmentation during apoptosis induces phosphorylation of H2AXhistone at serine 139. The Journal of Biological Chemistry, 275(13):9390–9395, March 2000. PMID: 10734083.
[76] E P Rogakou, D R Pilch, A H Orr, V S Ivanova, and W M Bonner. DNAdouble-stranded breaks induce histone H2AX phosphorylation on serine 139.The Journal of Biological Chemistry, 273(10):5858–5868, March 1998. PMID:9488723.
[77] Kai Rothkamm and Simon Horn. gamma-H2AX as protein biomarker for radi-ation exposure. Annali dell’Istituto Superiore Di Sanità, 45(3):265–271, 2009.PMID: 19861731.
[78] Kai Rothkamm and Markus Löbrich. Evidence for a lack of DNA double-strand break repair in human cells exposed to very low x-ray doses. Proceed-ings of the National Academy of Sciences of the United States of America,100(9):5057–5062, April 2003. PMID: 12679524.
[79] Claudia E Rübe, Saskia Grudzenski, Martin Kühne, Xiaorong Dong, NicoleRief, Markus Löbrich, and Christian Rübe. DNA double-strand break repair ofblood lymphocytes and normal tissues analysed in a preclinical mouse model:implications for radiosensitivity testing. Clinical Cancer Research: An OfficialJournal of the American Association for Cancer Research, 14(20):6546–6555,October 2008. PMID: 18927295.
[80] L B Schultz, N H Chehab, A Malikzay, and T D Halazonetis. p53 binding pro-tein 1 (53BP1) is an early participant in the cellular response to DNA double-strand breaks. The Journal of Cell Biology, 151(7):1381–1390, December2000. PMID: 11134068.
[81] Olga A Sedelnikova, Emmy P Rogakou, Igor G Panyutin, and William M Bon-ner. Quantitative detection of (125)IdU-induced DNA double-strand breakswith gamma-H2AX antibody. Radiation Research, 158(4):486–492, October2002. PMID: 12236816.
[82] Martin Simonsson, Fredrik Qvarnström, Jan Nyman, Karl-Axel Johansson,Hans Garmo, and Ingela Turesson. Low-dose hypersensitive gammaH2AX re-sponse and infrequent apoptosis in epidermis from radiotherapy patients. Ra-diotherapy and Oncology: Journal of the European Society for TherapeuticRadiology and Oncology, 88(3):388–397, September 2008. PMID: 18524402.
48

[83] W K SINCLAIR and R A MORTON. X-RAY AND ULTRAVIOLET SENSI-TIVITY OF SYNCHRONIZED CHINESE HAMSTER CELLS AT VARIOUSSTAGES OF THE CELL CYCLE. Biophysical Journal, 5:1–25, January 1965.PMID: 14284327.
[84] Enikö Sonkoly, Tianling Wei, Elizabeth Pavez Loriè, Hiroyuki Suzuki, Mit-suyasu Kato, Hans Törmä, Mona Ståhle, and Andor Pivarcsi. Protein kinasec-dependent upregulation of miR-203 induces the differentiation of human ker-atinocytes. The Journal of Investigative Dermatology, 130(1):124–134, Jan-uary 2010. PMID: 19759552.
[85] G G Steel. Chapter 1. introduction: The significance of radiobiology for radio-therapy. In Basic Clinical Radiobiology, pages 1–7. A Hodder Arnold Publi-cation, 3 edition, September 2002.
[86] Tom Stiff, Mark O’Driscoll, Nicole Rief, Kuniyoshi Iwabuchi, MarkusLöbrich, and Penny A Jeggo. ATM and DNA-PK function redundantly tophosphorylate H2AX after exposure to ionizing radiation. Cancer Research,64(7):2390–2396, April 2004. PMID: 15059890.
[87] Valery Tarasov, Peter Jung, Berlinda Verdoodt, Dmitri Lodygin, Alexey Ep-anchintsev, Antje Menssen, Gunter Meister, and Heiko Hermeking. Differen-tial regulation of microRNAs by p53 revealed by massively parallel sequenc-ing: miR-34a is a p53 target that induces apoptosis and g1-arrest. Cell Cycle(Georgetown, Tex.), 6(13):1586–1593, July 2007. PMID: 17554199.
[88] Hiroshi Tazawa, Naoto Tsuchiya, Masashi Izumiya, and Hitoshi Nakagama.Tumor-suppressive miR-34a induces senescence-like growth arrest throughmodulation of the E2F pathway in human colon cancer cells. Proceed-ings of the National Academy of Sciences of the United States of America,104(39):15472–15477, September 2007. PMID: 17875987.
[89] I Turesson. The progression rate of late radiation effects in normal tissue and itsimpact on dose-response relationships. Radiotherapy and Oncology: Journalof the European Society for Therapeutic Radiology and Oncology, 15(3):217–226, July 1989. PMID: 2772250.
[90] I Turesson, R Bernefors, M Book, M Flogegård, I Hermansson, K A Johansson,A Lindh, S Sigurdardottir, U Thunberg, and J Nyman. Normal tissue responseto low doses of radiotherapy assessed by molecular markers–a study of skinin patients treated for prostate cancer. Acta Oncologica (Stockholm, Sweden),40(8):941–951, 2001. PMID: 11845959.
[91] I Turesson and G Notter. The predictive value of skin telangiectasia for lateradiation effects in different normal tissues. International Journal of RadiationOncology, Biology, Physics, 12(4):603–609, April 1986. PMID: 3084405.
[92] I Turesson, G Notter, I Wickström, K A Johansson, and S Eklund. The influ-ence of irradiation time per treatment session on acute and late skin reactions:
49

a study on human skin. Radiotherapy and Oncology: Journal of the Euro-pean Society for Therapeutic Radiology and Oncology, 2(3):235–245, October1984. PMID: 6441973.
[93] I Turesson and H D Thames. Repair capacity and kinetics of human skin duringfractionated radiotherapy: erythema, desquamation, and telangiectasia after 3and 5 year’s follow-up. Radiotherapy and Oncology: Journal of the EuropeanSociety for Therapeutic Radiology and Oncology, 15(2):169–188, June 1989.PMID: 2762590.
[94] Ingela Turesson, Jan Nyman, Fredrik Qvarnström, Martin Simonsson, MajlisBook, Ingegerd Hermansson, Sunna Sigurdardottir, and Karl-Axel Johansson.A low-dose hypersensitive keratinocyte loss in response to fractionated radio-therapy is associated with growth arrest and apoptosis. Radiotherapy and On-cology: Journal of the European Society for Therapeutic Radiology and On-cology, 94(1):90–101, January 2010. PMID: 19931928.
[95] H Vakifahmetoglu, M Olsson, and B Zhivotovsky. Death through a tragedy:mitotic catastrophe. Cell Death and Differentiation, 15(7):1153–1162, July2008. PMID: 18404154.
[96] Hongyan Wang, Minli Wang, Huichen Wang, Wilfried Böcker, and George Il-iakis. Complex H2AX phosphorylation patterns by multiple kinases includingATM and DNA-PK in human cells exposed to ionizing radiation and treatedwith kinase inhibitors. Journal of Cellular Physiology, 202(2):492–502, Febru-ary 2005. PMID: 15389585.
[97] I M Ward and J Chen. Histone H2AX is phosphorylated in an ATR-dependentmanner in response to replicational stress. The Journal of Biological Chem-istry, 276(51):47759–47762, December 2001. PMID: 11673449.
[98] Irene M Ward, Kay Minn, Katherine G Jorda, and Junjie Chen. Accumulationof checkpoint protein 53BP1 at DNA breaks involves its binding to phospho-rylated histone H2AX. The Journal of Biological Chemistry, 278(22):19579–19582, May 2003. PMID: 12697768.
[99] Fiona M Watt, Cristina Lo Celso, and Violeta Silva-Vargas. Epidermal stemcells: an update. Current Opinion in Genetics & Development, 16(5):518–524,October 2006. PMID: 16919447.
[100] Wendy C Weinberg and Mitchell F Denning. P21Waf1 control of epithelial cellcycle and cell fate. Critical Reviews in Oral Biology and Medicine: An OfficialPublication of the American Association of Oral Biologists, 13(6):453–464,2002. PMID: 12499239.
[101] R Yi and E Fuchs. MicroRNA-mediated control in the skin. Cell Death andDifferentiation, 17(2):229–235, February 2010. PMID: 19609273.
[102] Shao-Yao Ying, Donald C Chang, and Shi-Lung Lin. The microRNA(miRNA): overview of the RNA genes that modulate gene function. Molec-ular Biotechnology, 38(3):257–268, March 2008. PMID: 17999201.
50

[103] Omar Zgheib, Kristopher Pataky, Juergen Brugger, and Thanos D Halazonetis.An oligomerized 53BP1 tudor domain suffices for recognition of DNA double-strand breaks. Molecular and Cellular Biology, 29(4):1050–1058, February2009. PMID: 19064641.
51

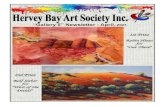





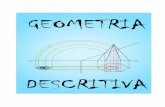








![Introduction€¦ · By the Hitchin-Thorpe inequality [12, 30, 65], the existence of such a metric implies that M has c2 1 =2χ +3τ>0. However, the latter ensures [25, 41] that the](https://static.fdocument.org/doc/165x107/60bd011b2bce7a3a5e3b83fe/by-the-hitchin-thorpe-inequality-12-30-65-the-existence-of-such-a-metric-implies.jpg)

