Preimplantation genetic diagnosis of β-thalassemia using ... · Preimplantation genetic diagnosis...
9
Preimplantation genetic diagnosis of b-thalassemia using real-time polymerase chain reaction with fluorescence resonance energy transfer hybridization probes Chia-Cheng Hung a,b,1 , Shee-Uan Chen c,1 , Shin-Yu Lin c,d , Mei-Ya Fang b , Li-Jung Chang c , Yi-Yi Tsai c , Li-Ting Lin c , Yu-Shih Yang c , Chien-Nan Lee c, * , Yi-Ning Su a,b,d, * a Graduate Institute of Clinical Genomics, National Taiwan University College of Medicine, Taipei, Taiwan b Department of Medical Genetics, National Taiwan University Hospital, Taipei, Taiwan c Department of Obstetrics and Gynecology, National Taiwan University Hospital, Taipei, Taiwan d Graduate Institute of Clinical Medicine, National Taiwan University College of Medicine, Taipei, Taiwan article info Article history: Received 1 October 2009 Received in revised form 13 December 2009 Accepted 15 December 2009 Available online 24 December 2009 Keywords: Preimplantation genetic diagnosis Fluorescence resonance energy transfer Hybridization probes Melting curve analysis Real-time PCR assay b-Thalassemia HBB gene Primer extension minisequencing abstract Preimplantation genetic diagnosis (PGD) is employed increasingly to allow transfer of embryos to the uterus in assisted reproduction procedures. There are three stages of biopsy: polar bodies, one or two blastomeres from the cleavage-stage embryos, and trophectoderm cells (5 cells) from the blastocyst- stage embryos. Validation of polymerase chain reaction (PCR)-based assays are challenging because only limited genetic material can be obtained for PGD. In the current study, we modified a valid single-cell PCR protocol for PGD using real-time PCR assay with fluorescence resonance energy transfer (FRET) hybrid- ization probes followed by melting curve analysis. We optimized and clinically applied the protocol, per- mitting molecular genetic analysis to amplify a specific region on the beta-globin (HBB) gene for a couple, carriers of two mutations: c.-78A>G and c.52A>T. Among a total of eight embryos obtained after ovarian stimulation, a single blastomere per embryo at the six- to eight-cell stage was biopsied. This PGD method showed that four embryos were unaffected, two embryos were selected for transfer, and one pregnancy was achieved. Finally, a healthy male baby was delivered at 38 weeks’ gestation. The results obtained using the new method, FRET hybridization probes, were compared with findings using an existing method, primer extension minisequencing. Ó 2009 Elsevier Inc. All rights reserved. b-Thalassemia (OMIM no. 141900), one of the most common monogenic genetic diseases in the world, is an autosomal reces- sive inherited disorder with an estimated carrier frequency of 1 in 35 resulting from point mutations, small insertions, or dele- tions in the beta-globin (HBB) gene, resulting in either absence or reduced synthesis of beta-globin chains [1]. The HBB gene is located on chromosome 11 (11p15.5) and contains three exons [2]. Although it is a small gene, more than 200 different muta- tions of the HBB gene cluster are associated with the b-thalasse- mia phenotype [3,4]. Typically, prenatal diagnosis for high-risk pregnancies is per- formed by analysis of fetal cells from chorionic villus sampling at 10 to 12 weeks’ gestation or amniocentesis at 15 to 18 weeks’ ges- tation [5,6]. Recently, preimplantation genetic diagnosis (PGD) 2 is becoming widely used for analysis of monogenic diseases before pregnancy [7–11]. It is an alternative allowing prenatal genetic diag- nosis of embryos for couples at high risk for inherited disorders be- fore intrauterine transfer during assisted reproduction. The advantage of PGD over conventional prenatal diagnosis is the avoid- ance of pregnancy termination. There are three main sources of ge- netic material for PGD: polar bodies (biopsy of the first polar body from oocytes before sperm insemination or biopsy of both polar bodies after fertilization), blastomeres from cleavage-stage embryos, and trophectoderm cells from embryos at the blastocyst stage. In clinical practice, polar body biopsy has been used for aneuploidy screening or for the detection of maternal transmission of single- gene defects. Biopsy of the cleavage embryo at the six- to eight-cell 0003-2697/$ - see front matter Ó 2009 Elsevier Inc. All rights reserved. doi:10.1016/j.ab.2009.12.023 * Corresponding authors. Fax: +886 2 2311 8228 (C.-N. Lee), +886 2 2381 6229 (Y.-N. Su). E-mail addresses: [email protected] (C.-N. Lee), [email protected] (Y.-N. Su). 1 These authors contributed equally to this study. 2 Abbreviations used: PGD, preimplantation genetic diagnosis; PCR, polymerase chain reaction; ADO, allele dropout; RFLP, restriction fragment length polymorphism; ARMS, amplification refractory mutation system; WGA, whole genome amplification; HLA, human leukocyte antigen; FRET, fluorescent resonance energy transfer; GnRH, gonadotropin-releasing hormone; ICSI, intracytoplasmic sperm injection; PBS, phos- phate-buffered saline; BSA, bovine serum albumin; DTT, DL-dithiothreitol; ALB, alkaline lysis buffer; dNTP, deoxynucleoside triphosphate; MBS, multiblock system; LC, LightCycler; T m , melting temperature; ddNTP, dideoxynucleoside triphosphate. Analytical Biochemistry 400 (2010) 69–77 Contents lists available at ScienceDirect Analytical Biochemistry journal homepage: www.elsevier.com/locate/yabio
Transcript of Preimplantation genetic diagnosis of β-thalassemia using ... · Preimplantation genetic diagnosis...

Analytical Biochemistry 400 (2010) 69–77
Contents lists available at ScienceDirect
Analytical Biochemistry
journal homepage: www.elsevier .com/locate /yabio
Preimplantation genetic diagnosis of b-thalassemia using real-time polymerasechain reaction with fluorescence resonance energy transfer hybridization probes
Chia-Cheng Hung a,b,1, Shee-Uan Chen c,1, Shin-Yu Lin c,d, Mei-Ya Fang b, Li-Jung Chang c, Yi-Yi Tsai c,Li-Ting Lin c, Yu-Shih Yang c, Chien-Nan Lee c,*, Yi-Ning Su a,b,d,*
a Graduate Institute of Clinical Genomics, National Taiwan University College of Medicine, Taipei, Taiwanb Department of Medical Genetics, National Taiwan University Hospital, Taipei, Taiwanc Department of Obstetrics and Gynecology, National Taiwan University Hospital, Taipei, Taiwand Graduate Institute of Clinical Medicine, National Taiwan University College of Medicine, Taipei, Taiwan
a r t i c l e i n f o
Article history:Received 1 October 2009Received in revised form 13 December 2009Accepted 15 December 2009Available online 24 December 2009
Keywords:Preimplantation genetic diagnosisFluorescence resonance energy transferHybridization probesMelting curve analysisReal-time PCR assayb-ThalassemiaHBB genePrimer extension minisequencing
0003-2697/$ - see front matter � 2009 Elsevier Inc. Adoi:10.1016/j.ab.2009.12.023
* Corresponding authors. Fax: +886 2 2311 8228 ((Y.-N. Su).
E-mail addresses: [email protected] (C.-N. Lee), yn1 These authors contributed equally to this study.
a b s t r a c t
Preimplantation genetic diagnosis (PGD) is employed increasingly to allow transfer of embryos to theuterus in assisted reproduction procedures. There are three stages of biopsy: polar bodies, one or twoblastomeres from the cleavage-stage embryos, and trophectoderm cells (�5 cells) from the blastocyst-stage embryos. Validation of polymerase chain reaction (PCR)-based assays are challenging because onlylimited genetic material can be obtained for PGD. In the current study, we modified a valid single-cell PCRprotocol for PGD using real-time PCR assay with fluorescence resonance energy transfer (FRET) hybrid-ization probes followed by melting curve analysis. We optimized and clinically applied the protocol, per-mitting molecular genetic analysis to amplify a specific region on the beta-globin (HBB) gene for a couple,carriers of two mutations: c.-78A>G and c.52A>T. Among a total of eight embryos obtained after ovarianstimulation, a single blastomere per embryo at the six- to eight-cell stage was biopsied. This PGD methodshowed that four embryos were unaffected, two embryos were selected for transfer, and one pregnancywas achieved. Finally, a healthy male baby was delivered at 38 weeks’ gestation. The results obtainedusing the new method, FRET hybridization probes, were compared with findings using an existingmethod, primer extension minisequencing.
� 2009 Elsevier Inc. All rights reserved.
2
b-Thalassemia (OMIM no. 141900), one of the most commonmonogenic genetic diseases in the world, is an autosomal reces-sive inherited disorder with an estimated carrier frequency of 1in 35 resulting from point mutations, small insertions, or dele-tions in the beta-globin (HBB) gene, resulting in either absenceor reduced synthesis of beta-globin chains [1]. The HBB gene islocated on chromosome 11 (11p15.5) and contains three exons[2]. Although it is a small gene, more than 200 different muta-tions of the HBB gene cluster are associated with the b-thalasse-mia phenotype [3,4].Typically, prenatal diagnosis for high-risk pregnancies is per-formed by analysis of fetal cells from chorionic villus sampling at10 to 12 weeks’ gestation or amniocentesis at 15 to 18 weeks’ ges-
ll rights reserved.
C.-N. Lee), +886 2 2381 6229
[email protected] (Y.-N. Su).
tation [5,6]. Recently, preimplantation genetic diagnosis (PGD) isbecoming widely used for analysis of monogenic diseases beforepregnancy [7–11]. It is an alternative allowing prenatal genetic diag-nosis of embryos for couples at high risk for inherited disorders be-fore intrauterine transfer during assisted reproduction. Theadvantage of PGD over conventional prenatal diagnosis is the avoid-ance of pregnancy termination. There are three main sources of ge-netic material for PGD: polar bodies (biopsy of the first polar bodyfrom oocytes before sperm insemination or biopsy of both polarbodies after fertilization), blastomeres from cleavage-stage embryos,and trophectoderm cells from embryos at the blastocyst stage. Inclinical practice, polar body biopsy has been used for aneuploidyscreening or for the detection of maternal transmission of single-gene defects. Biopsy of the cleavage embryo at the six- to eight-cell
2 Abbreviations used: PGD, preimplantation genetic diagnosis; PCR, polymerasechain reaction; ADO, allele dropout; RFLP, restriction fragment length polymorphism;ARMS, amplification refractory mutation system; WGA, whole genome amplification;HLA, human leukocyte antigen; FRET, fluorescent resonance energy transfer; GnRH,gonadotropin-releasing hormone; ICSI, intracytoplasmic sperm injection; PBS, phos-phate-buffered saline; BSA, bovine serum albumin; DTT, DL-dithiothreitol; ALB,alkaline lysis buffer; dNTP, deoxynucleoside triphosphate; MBS, multiblock system;LC, LightCycler; Tm, melting temperature; ddNTP, dideoxynucleoside triphosphate.

70 Preimplantation diagnosis of b-thalassemia / C.-C. Hung et al. / Anal. Biochem. 400 (2010) 69–77
stage for one or two blastomeres is a common approach for PGD. Re-cently, trophectoderm biopsy to retrieve approximately five cells atthe blastocyst stage has been used for PGD. The polar body or blas-tomere biopsy provides a very limited amount of genetic material foranalysis and is challenging for accurate diagnosis. The blastocystbiopsy for obtaining more genetic material may have the advantageof reducing the possibility of polymerase chain reaction (PCR) failureor allele dropout (ADO) [12]. Because only limited genetic materialcan be obtained for PGD, it is critical and challenging work to estab-lish the validity of the PGD protocol to make an accurate moleculardiagnosis within a limited time.
Recently, DNA-based analyses have been performed based ondifferent principles to detect single-gene disorders [13–16]. Tradi-tional genotype analysis for PGD takes three steps. Initially, it in-volves a first round of PCR to preamplify the selected genes. Thatis followed by nested PCR to produce sufficient DNA fragmentsfor subsequent mutation analysis. Restriction fragment lengthpolymorphism (RFLP) [17–19], amplification refractory mutationsystem (ARMS) [20], and primer extension minisequencing[21,22] are used for differentiation between mutant and wild-typealleles. In our laboratory, we used whole genome amplification(WGA) combined with PCR and primer extension for PGD of sin-gle-gene disorders and human leukocyte antigen (HLA) haplotypeanalysis [23]. After WGA, the quality and quantity of DNA from asingle blastomere can sufficiently facilitate analysis of multiple loci[14,24]. However, prior to embryo transfer, the time allowed forPGD is limited. It would be helpful to have simple, rapid, inexpen-sive, and reliable diagnostic methods for PGD.
There is increasing need for the development of alternative pre-implantation genetic diagnostic tools in medical laboratories. Real-time PCR with molecular beacons provides a highly accurate assayfor detection in single cells [25,26]. Moreover, real-time PCR incombination with hybridization probes designed for fluorescentresonance energy transfer (FRET) is a powerful tool for detectionof genetic variants with high efficiency and sensitivity [27]. Theprinciple is based on fluorescence-labeled oligonucleotide probesused for sequence variant detection. When the two probes are inclose proximity, FRET leads to excitation and thus fluorescence ofthe second fluorophore by the energy emitted by the firstfluorophore.
Here we present an alternative method with a single-cell PCRprotocol for PGD of b-thalassemia using real-time PCR with FREThybridization probes followed by melting curve analysis. We opti-mized and clinically applied the protocol, permitting molecular ge-netic analysis to amplify a specific region on the HBB gene byanalyzing a single blastomere of eight embryos for a couple, carri-ers of two mutations: c.-78A>G and c.52A>T. The results obtainedusing the new method, FRET hybridization probes, were comparedwith findings using an existing method, primer extension minis-equencing.
Materials and methods
Patients
The couple, a 36-year-old man and a 33-year-old woman (bothwith b-thalassemia trait), was referred to our laboratory. The fathercarried the c.52A>T mutation (CD17), and the mother carried thec.-78A>G mutation (�28), of the HBB gene. In her first and secondpregnancies, the woman underwent dilatation and curettage be-cause both fetuses had b-thalassemia major, as identified on chori-onic villus sampling for DNA testing [28]. To avoid a pregnancywith an affected fetus, the couple requested that PGD be done inthe Reproductive Medicine Laboratory (Department of Obstetricsand Gynecology, National Taiwan University Hospital).
Genetic counseling
A geneticist provided comprehensive genetic counseling to thecouple to explain the risks and that three-quarters of the embryoswould be theoretically unaffected by b-thalassemia. The possibilityof a misdiagnosis using single-cell PCR was also discussed. Thedefinitive genotype of the fetus would need to be confirmed usingconventional prenatal diagnostics such as chorionic villus samplingor amniocentesis. The informed consent given by the couple waswritten, and the study was approved by the ethics committee ofNational Taiwan University Hospital.
Testing of single lymphocytes
To evaluate the reliability of the protocol before PGD, the firstround of PCR and real-time PCR with FRET hybridization weretested on single lymphocytes collected from the husband and wife.Lymphocytes were isolated from 5 ml of unclotted blood. The col-lection of single cells was transferred into 0.2-ml PCR tubes foranalysis. Blank controls were also processed under the same condi-tions to check for the presence of contamination. The amplificationefficiency, ADO rate, and contamination rate were measured.
Cleavage-stage embryo biopsy
Ovarian stimulations were performed using a long gonadotro-pin-releasing hormone (GnRH) agonist protocol as described previ-ously [29]. Intracytoplasmic sperm injection (ICSI) was used toavoid contamination with sperm and surrounding cumulus cells.
Embryos that had six to eight cells on day 3 after fertilizationwere placed into 5-ll droplets of human tubal fluid medium consist-ing of 0.01 M Hepes buffer (Sigma–Aldrich, St. Louis, MO, USA) undermineral oil. Micromanipulation was performed with the aid of twomicromanipulators (Narishige, Tokyo, Japan) mounted on an in-verted microscope (Nikon, Tokyo, Japan). The microscope was fittedwith a noncontact microdrill laser system (Fertilase Medical Tech-nologies, Montreux, Switzerland). The laser system emitted an invis-ible diode beam at a wavelength of 1.48 lm. The embryo was keptusing a holding pipette (Humagen Fertility Diagnostics, Charlottes-ville, VA, USA), and zona was drilled by the laser at a power of47 mW with 10 ms exposure. A hole of approximately 30 lm wasmade. The biopsy pipette (Humagen Fertility Diagnostics) was theninserted to remove a blastomere from each embryo. Following thebiopsy, embryos were further cultured until day 5 after fertilization,and unaffected blastocysts were transferred to the patient’s uterus.
Each blastomere was washed with wash buffer (phosphate-buf-fered saline [PBS] without calcium and magnesium [Sigma Chem-ical, St. Louis, MO, USA] and 0.5% bovine serum albumin [BSA,Sigma Chemical]) and was transferred to a separate 0.2-ml PCRtube containing 3 ll of lysis buffer (200 mM KOH [Sigma Chemical]and 50 mM DL-dithiothreitol [DTT, Sigma Chemical]). The last washdrop of each blastomere served as a blank control. Embryo transferwas carried out at the blastocyst stage.
Lysis of blastomeres and PCR
A singe blastomere was placed in the alkaline lysis buffer (ALB,containing 50 mM DTT and 200 mM KOH) [30] and was incubatedat 65 �C for 10 min, followed by incubation at 94 �C for 10 min. Thesubsequent PCR encompassing both mutation sites of the HBB genegenerated a fragment of 364 bp. Primer sequences were 50-ACGGCT GTC ATC ACT TAG AC-30 (sense) and 50-GTC AGT GCC TATCAG AAA CC-30 (antisense). PCR was performed in a total volumeof 25 ll containing 3 ll of lysis buffer with the lysed blastomere,0.12 lM of each primer, 2.5 mM deoxynucleoside triphosphates(dNTPs), 0.5 U of AmpliTaq Gold enzyme (Applied Biosystems, Fos-

Preimplantation diagnosis of b-thalassemia / C.-C. Hung et al. / Anal. Biochem. 400 (2010) 69–77 71
ter City, CA, USA), and 2.5 ll of GeneAmp 10� buffer II (10 mM Tris–HCl [pH 8.3] and 50 mM KCl) in 2 mM MgCl2, as provided by themanufacturer. PCR was performed in a multiblock system (MBS)thermocycler (ThermoHybaid, Ashford, UK) using a touchdownPCR program with an initial denaturation at 95 �C for 10 min fol-lowed by 14 cycles consisting of denaturation at 94 �C for 30 s,annealing at 64 �C for 30 s (decreased by 0.5 �C/cycle), and extensionat 72 �C for 30 s. Immediately following the initial program, an addi-tional program was run and consisted of 26 cycles of denaturation at94 �C for 30 s, annealing at 57 �C for 30 s, and extension at 72 �C for30 s, followed by a final extension at 72 �C for 10 min.
Real-time PCR with FRET
The first-round PCR product was further amplified by real-timePCR in a LightCycler 480 instrument (Roche, Branchburg, NJ, USA).Real-time PCR was performed using two primers and two adjacentfluorescent hybridization probes for the known HBB genotypes.The primers, 50-ACT TAG ACC TCA CCC TGT GGA-30 (sense) and50-AGG TTG CTA GTG AAC ACA GTT GT-30 (antisense), were usedfor the c.-78A>G mutation. One probe was labeled with fluoresceinat the 30 end (50-TGG GCA TAA AAG TCA GGG C-30) as the donor,and another probe (acceptor) was labeled with the LightCycler(LC) Red fluorophore at the 50 end (50-GAG CCA TCT ATT GCT TACATT TGC TTC TGA-30), which phosphorylated at the 30 end. Primersfor the c.52A>T mutation were 50-ACT TAG ACC TCA CCC TGT GGA-30 (sense) and 50-GTT CTA TTG GTC TCC TTA AAG GTG-30 (anti-sense). The FRET donor probe was fluorescein labeled (50-TCCACG TTC ACC TAG CCC CA-30), and the FRET acceptor probe wasLC Red labeled (50-AGT CTG CCG TTA CTG CTC TGT-30).
Real-time PCR was performed in a total volume of 10 ll con-taining 1 ll of PCR products, 3 mM MgCl2, 0.25 lM of each primer,0.25 lM fluorescein probe, 0.25 lM LC Red fluorophore probe, and1� LightCycler FastStart DNA Master Hybridization Probes Mix(Roche), as provided by the manufacturer. The cycling conditionsfor real-time PCR in the LiC480 were as follows: 95 �C for 10 min,followed by 50 cycles of denaturation at 95 �C for 10 s with a tem-perature transition rate of 4.4 �C/s, annealing at 53 �C for 10 s witha temperature transition rate of 2.2 �C/s, and extension at 72 �C for10 s, with a temperature transition rate of 4.4 �C/s.
Melting curve assay
The subsequent melting curve analysis was appended to theamplification step, which was performed by completely denatur-ing the PCR products at 95 �C for 1 min, with a ramping rate of4.4 �C/s, cooling to 40 �C, with a ramping rate of 1.5 �C/s, and thenheating to 95 �C, with a ramping rate of 2.2 �C/s, with continuousfluorescence monitoring [31]. The melting curve data were ana-lyzed using gene scanning module software (version 1.3, Roche).
Primer extension minisequencing
The PCR–FRET results were compared with primer extensionminisequencing as described previously [32]. Briefly, nested PCRwas performed for further amplification of the specific regions onthe HBB genes. Nested PCR was performed in a total volume of25 ll containing 2 ll of first-round PCR product, 0.12 lM of eachprimer (sense: 50-gac agg tac ggc tgt ca-30; antisense: 50-gtc tccaca tgc cca gtt tc-30), 2.5 mM dNTPs, 0.5 U of AmpliTaq Gold en-zyme (Applied Biosystems), and 2.5 ll of GeneAmp 10� buffer II(10 mM Tris–HCl [pH 8.3] and 50 mM KCl) in 2 mM MgCl2, as pro-vided by the manufacturer. Nested PCR was performed under thesame conditions as first-round PCR. The subsequent primer exten-sion reaction was performed using a GenomeLab SNPStart PrimerExtension Kit (Beckman Coulter, Brea, CA, USA) in a volume of
10 ll containing 1 ll of nested PCR product, 1 mM primer, and1� SNP Start Master Mix (Beckman Coulter). The primer extensionprimers were used to detect the mutation sites causing b-thalasse-mia (50-atg gct ctg ccc tga ctt-30 for the c.-78A>G mutation and 50-aac ttc atc cac gtt cac ct-30 for the c.52A>T mutation). The reactionwas performed in an MBS thermocycler (ThermoHybaid) with 25cycles of 90 �C for 10 s and 45 �C for 20 s. Postreaction samplecleanup was done to avoid contamination by unincorporated dyefollowing the manufacturer’s protocol. Primer extension productswere analyzed using the Beckman CEQ-8000 genetic analysis sys-tem (Beckman Coulter) with CEQ software using D-1-labeled 80DNA size standard (Beckman Coulter).
Results
Results from genomic DNA
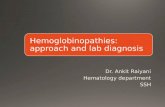
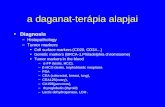
The maternal mutation (c.-78A>G) and the paternal mutation(c.52A>T) were detected by FRET hybridization probes and meltingtemperature (Tm) analysis based on genomic DNA. In the genomicDNA sample of the mother, the peak at the lower temperature(54 �C) corresponded to the mutated allele (G), whereas the peakat the higher temperature (62 �C) corresponded to the wild-typeallele (A), as shown in Fig. 1A. Similarly, the genomic DNA of thefather showed a peak at the lower temperature (61 �C) correspond-ing to the wild-type allele (A) and a peak at the higher temperature(66 �C) belonging to the mutated allele (T), as shown in Fig. 2A.
Amplification efficiency on single lymphocytes
Prior to performing the PGD cycle, 50 single lymphocytes wereisolated and the complete procedure was performed for the twomutated loci. The amplification efficiency of the HBB gene was 92to 96% with a mean of 95%. ADO was measured at 6 to 8% with amean of 7%. There was no contamination of the 100 reactions.The duration of the procedures was 4 h and included the first-round PCR (3 h) and real-time PCR with FRET hybridization plusmelting curve analysis (1 h).
Mutation analysis of blastomeres
After ovarian stimulation and ICSI, a total of eight embryos werebiopsied. Results for amplification and genotyping of the c.-78A>Gsite from the single blastomeres of the eight embryos are illus-trated in Fig. 1B. The mutated allele lowered the Tm of the probeby 8 �C. Genotyping analyses for the c.52A>T site of the eight blas-tomeres from the embryos are shown in Fig. 2B. The mutated alleleresulted in a Tm shift of 5 �C. The overall results are shown inTable 1, and each blastomere was analyzed in triplicate. Based onreal-time PCR with FRET hybridization probes, four embryos(embryos 3, 4, 5, and 7) were diagnosed definitively unaffectedby b-thalassemia. Two were not diagnosed due to amplificationfailure. The remaining two embryos were diagnosed as affectedcases. The amplification rates were 81.25% (13/16), 87.50% (14/16), and 93.75% (15/16), respectively (Table 1). There was no con-tamination of the 24 reactions.
Primer extension minisequencing
All embryos were processed for genetic analysis by primer exten-sion minisequencing to confirm and compare with the melting anal-ysis results, as described previously. Using the primer extensionassay with different dideoxynucleoside triphosphate (ddNTP)-la-beled dyes, we accurately determined the mutated/wild-type allelesof the primer extension products by their different dyes.

Fig. 1. Melting curve analysis of real-time hybridization with FRET probes for c.-78 mutation of the HBB gene. (A) Upper panel: For the wild-type control with homozygous c.-78A, the Tm of the matched DNA duplex was 62 �C. Lower panel: For the heterozygous c.-78A and c.-78G, the peak Tm of 54 �C was from mismatched DNA duplex of themutant allele with c.-78G. The other peak of Tm at 62 �C resulted from the wild-type allele with c.-78A. (B) Embryos 1 to 8.
72 Preimplantation diagnosis of b-thalassemia / C.-C. Hung et al. / Anal. Biochem. 400 (2010) 69–77

Fig. 2. Genotyping of the c.52 mutation site by FRET hybridization probing. (A) Upper panel: For the wild-type control with homozygous c.52A, the Tm of the mismatchedDNA duplex was 61 �C. Lower panel: For the heterozygous c.52T and c.52A, the peak Tm occurred at 66 �C was from matched DNA duplex of the mutant allele with c.52T. Theother peak of Tm at 61 �C resulted from the wild-type allele with c.52A. (B) Results of the FERT hybridization for embryos 1 to 8.
Preimplantation diagnosis of b-thalassemia / C.-C. Hung et al. / Anal. Biochem. 400 (2010) 69–77 73

Table 1Summary of results of the PGD for the HBB gene with FRET hybridization probes and primer extension.
FRET hybridization probes Primer extension
First time Second time Third timeEmbryo Mutation site Mutation site Mutation site Mutation site
c.-78 c.52 c.-78 c.52 c.-78 c.52 c.-78 c.52
1 G A G A G A G A2 No signal A No signal A No signal A No signal No signal3 A A A A A A A A4 A A A A A A A A5 A A A A A A A A6 A T A T A T A T7 A A A A A A A A8 A A A No signal No signal No signal No signal No signal
74 Preimplantation diagnosis of b-thalassemia / C.-C. Hung et al. / Anal. Biochem. 400 (2010) 69–77
In Fig. 3, for each example of an electropherogram from the pri-mer extension analysis, the first peak corresponded to the unex-tended primer extension primer and always presented the sameretention time in each electropherogram. There were two extendedpeaks that were identified for individuals with A (wild-type) and G(mutation) alleles. Likewise, in Fig. 4, there were two extendedpeaks that were identified for individuals with A (wild-type) andT (mutation) alleles. Embryos 2 and 8 failed at amplification onboth mutation sites. The amplification rate for primer extensionwas 75% (12/16). Embryos 3, 4, 5, and 7 were confirmed as unaf-fected by b-thalassemia.
Embryo transfer and follow-up of pregnancy
Two unaffected embryos (embryos 5 and 7) were transferredinto the uterus at the blastocyst stage. The other two unaffectedembryos (embryos 3 and 4) were cryopreserved for future use.The remaining four embryos stopped growing and were discarded.The patient had a singleton pregnancy. Prenatal diagnosis was per-formed by chorionic villus sampling at 11 weeks’ gestation. Direct
Fig. 3. Electropherograms of primer extension minisequencing corresponding to negativeach example of an electropherogram from the primer extension analysis, the first peaksame retention time in each electropherogram. There were two extended peaks that we
genotype sequencing showed that the fetus was a carrier of thematernal mutation (c.-78A>G). Finally, a healthy male baby wasdelivered at 38 weeks’ gestation.
Discussion
A schematic representation of the single-cell PCR protocol usedfor genotyping the region of interest of the HBB gene is shown inFig. 5. A schematic diagram of the gene structure showing positionsof amplification primers, mutation sites, and hybridization probesis shown in Fig. 6. After embryo biopsy, a single blastomere cellwas lysed. The template was a 364-bp fragment generated fromPCR amplification of the HBB gene using the appropriate forwardand reverse primers. The mutation sites of the HBB gene (c.-78A>G and c.52A>T) were within the region. The FRET hybridiza-tion probes lie immediately adjacent to the mutation target, whichis detected as the emission wavelength of the acceptor fluoro-phore. Finally, the melting curve was used to analyze the PCR prod-ucts for mutation analysis of the HBB genes. The strategy for directanalysis of embryo mutations by FRET hybridization probes and
e control, wild-type, c.-78 A>G/WT, c.-78 A>G/WT, and each of embryos 1 to 8. Forcorresponded to the unextended primer extension primer and always presented there identified for individuals with A (wild-type) and G (mutation) alleles.

Fig. 4. Minisequencing electropherograms of the c.52 A>T mutation corresponding to negative control, wild-type, c.-52 A>T/c.-52 A>T mutation, c.-52 A>T /WT, and each ofembryos 1 to 8. For each example of an electropherogram from the primer extension analysis, the first peak corresponded to the unextended primer extension primer andalways presented the same retention time in each electropherogram. There were two extended peaks that were identified for individuals with A (wild-type) and T (mutation)alleles.
Fig. 5. Design of hybridization probes for real-time FRET detection of the c58.A>Tand c-78.A>G mutations of the HBB gene.
Preimplantation diagnosis of b-thalassemia / C.-C. Hung et al. / Anal. Biochem. 400 (2010) 69–77 75
melting curve analysis was successfully applied to b-thalassemia.The illustrated technique can be used to analyze single-cell sam-ples for a known mutation.
Genotyping by FRET hybridization probes is generally consid-ered as more reliable. The FRET hybridization probes can deter-mine single-base variations by changes in Tm with highsensitivity and resolution. Moreover, FRET hybridization probes
were used in the LightCycler (Roche), which is a PCR-based instru-ment that provides real-time and post-PCR analysis in a closedtube environment. It can also provide high-speed throughput thatcould analyze 96 or 384 samples per hour. We compared the lab-oratory costs of PCR combined with FRET hybridization probes,nested PCR followed by primer extension, and WGA. The costs ofdiagnosis were estimated to be U.S. $6, $10, and $20 for FREThybridization, primer extension, and WGA, respectively. However,it should be noted that the expensive fluorescent probes of FRETassays cannot be used for PGD of other mutations; thus, unlessthere are many other PGD cases involving the same mutationswithin the next 1 or 2 years, the entire cost of the synthesizedprobes (costing hundreds of dollars for each fluorophore–quencherpair) must be borne by the patients regardless of how much probewas used during the PGD cycle. This is unlike the case where pri-mer extension reagents are used because the kits are generic andcan be used for any mutation in any gene and the unlabeled min-isequencing primers are comparatively cheap. In terms of length oftime, the WGA method requires 12 h because it involves a hybrid-ization procedure, primer extension requires 9 h because it in-volves DNA cleanup, and FRET hybridization can be completedwithin 4 h, which includes the time it takes to perform the PCRamplification, FRET hybridization, and melting curve analysis.Our results show that the FRET hybridization strategy is accurate[33,34] and is a good alternative for PGD.
Despite the preclinical validation results suggesting otherwise,there is compelling evidence that significant ADO occurred duringthe PGD cycle analysis. First, none of the eight embryos was het-erozygous at either the c.-78 or c.52 mutation site. Based on allelesegregation and inheritance probabilities, the odds of an embryobeing heterozygous at one or both mutation sites is 0.75, whereasthe corresponding probability that an embryo is not heterozygousat any mutation site is 0.25. Thus, the joint probability that none ofthe eight embryos would be heterozygous at any mutation site is0.25 to the power of 8, or 0.000015, a highly unlikely probability.Second, embryo 1 showed only the mutant G allele at the c.-78

Fig. 6. Human HBB gene sequence (NG_000007), primer sequences, probe positions, and the mutation sites. The first-round primers are labeled in boldface letters and orangefont, the mutation sites are labeled in boldface letters and red font, the sensor probes are marked with arrows and red font, and the anchor probes are marked with arrows andblue font. (For interpretation of the references to color in this figure legend, the reader is referred to the Web version of this article.)
76 Preimplantation diagnosis of b-thalassemia / C.-C. Hung et al. / Anal. Biochem. 400 (2010) 69–77
mutation site, whereas embryo 6 showed only the mutant T alleleat the c.52 mutation site. Because the couple carry different muta-tions, it is impossible for any embryo to inherit a homozygous mu-tant genotype at either mutation site. An apparently homozygousmutant genotype is observed only when ADO of the normal alleleoccurs in an embryo that is heterozygous or compound heterozy-gous for that mutation. The observation of apparently homozygousmutant genotypes in two of the eight embryos is, therefore, com-pelling evidence of ADO of the normal allele at the respectivemutation sites. Third, embryos 3, 4, 5, and 7 were apparentlyhomozygous normal at both the c.-78 and c.52 mutation sites,and embryos 5 and 7 were transferred, resulting in a singletonpregnancy. Subsequent prenatal diagnosis, however, showed thatthe fetus was not homozygous normal but in fact a carrier of thematernal c.-78 mutation. This is further evidence that ADO, thistime of the mutant allele at the c.-78 mutation site, had occurredin at least one of the two transferred embryos. The results asshown in Table 1 strongly suggest that most of the ADO in this casereport occurred during the first PCR round. We think that this highADO is related in some way to the fact that we did not have a neu-tralization step after blastomere lysis to ensure that the final PCRpH conditions are near optimal.
Given the demonstrated occurrence of ADO in three embryos(two involving a normal allele and one involving a mutant allele),the question is whether any ADO occurred in any of the other fiveembryos. Unfortunately, we will not be able to know this becausethe PGD strategy adopted here does not allow for detection of ADOof either or both mutant alleles when an embryo has an apparentlyhomozygous normal genotype at both mutation sites. Nestedlinked PCR of both mutation sites would have been the best wayto prevent serious misdiagnosis of an affected embryo as being acarrier or normal embryo. Otherwise, it should have includedflanking linked markers to mitigate this deficiency. The dangerwith ADO is the failure to detect the mutant alleles when bothare present, which would then result in a serious misdiagnosis.
Aside from lacking a means to detect ADO of the mutant alleles,the assay also does not incorporate a means of monitoring for thepresence of exogenous DNA contamination in the blastomere reac-tions. We performed the 24 secondary PCR blank reactions, and theresults were blank. However, these serve a general purpose ofmonitoring overall DNA contamination, but there is no monitoringof DNA contamination within the tubes containing the blasto-meres. This is another deficiency of the assay design.
The amplification efficiency of real-time PCR with FRET hybrid-ization on single lymphocytes was 94 to 98% with an ADO rate of 6to 10%. The ADO rates for PCR were comparable to those in previ-ous PGD works, which reported PCR amplification efficiencies of 85
to 95% with ADO rates of 5 to 15%, and are within the guidelines setby the Preimplantation Genetic Diagnosis International Society(PGDIS) [35].
In comparing the genetic results by FRET hybridization and pri-mer extension, embryos 3, 4, 5, and 7 were healthy (either wildtypes or carriers). Embryos 1 and 6 were diagnosed with b-thalas-semia major and were rejected for transfer. Embryos 2 and 8 failedprimer extension minisequencing and could not be diagnosed.Reanalysis of these two embryos also failed during the secondand third FRET hybridizations (Table 1). This indicated that thetwo embryos were noninformative. After the couple underwent ge-netic counseling, the woman’s uterus was implanted with embryos5 and 7 at the blastocyst stage. Prenatal diagnostic chorionic villussampling was performed and showed a normal fetus carrying thematernal mutation (c.-78A>G). A normal infant boy was delivered.
We have reported the successful PGD and delivery of a healthyboy to a couple at risk for transmitting b-thalassemia. Using real-time PCR with FRET hybridization for PGD, the entire genotypingprocedure can be accomplished easily in a single working day. Thisrapid and accurate assay is highly desirable for clinical use in PGD.It is imperative for blastocyst biopsy because the time interval per-mitted for molecular diagnosis is stringent so as to transfer a freshembryo. Real-time PCR with FRET hybridization can be successfullyperformed for PGD of other monogenic diseases. It deserves furtherinvestigation in the future.
Acknowledgments
We are very grateful to the couple who participated in this re-search. We thank the National Science Council of Taiwan (GrantsNSC 95-2314-B-002-280-MY3 and NSC 96-2628-B-002-063-MY3)for financial support.
References
[1] T.H. Huisman, M.F. Carver, The b- and d-thalassemia repository (nineth ed.,part I), Hemoglobin 22 (1998) 169–195.
[2] R.V. Lebo, M.C. Cheung, B.D. Bruce, V.M. Riccardi, F.T. Kao, Y.W. Kan, Mappingparathyroid hormone, beta-globin, insulin, and LDH-A genes within the humanchromosome 11 short arm by spot blotting sorted chromosomes, Hum. Genet.69 (1985) 316–320.
[3] R.C. Hardison, D.H. Chui, B. Giardine, C. Riemer, G.P. Patrinos, N. Anagnou, W.Miller, H. Wajcman, HbVar: a relational database of human hemoglobinvariants and thalassemia mutations at the globin gene server, Hum. Mutat. 19(2002) 225–233.
[4] U. Bhardwaj, Y.H. Zhang, F. Lorey, L.L. McCabe, E.R. McCabe, Molecular geneticconfirmatory testing from newborn screening samples for the commonAfrican–American, Asian Indian, Southeast Asian, and Chinese b-thalassemiamutations, Am. J. Hematol. 78 (2005) 249–255.

Preimplantation diagnosis of b-thalassemia / C.-C. Hung et al. / Anal. Biochem. 400 (2010) 69–77 77
[5] T.E. Cohen-Overbeek, W.C. Hop, M. den Ouden, L. Pijpers, M.G. Jahoda, J.W.Wladimiroff, Spontaneous abortion rate and advanced maternal age:consequences for prenatal diagnosis, Lancet 336 (1990) 27–29.
[6] B. Chadefaux, D. Rabier, Y. Dumez, J.E. Oury, P. Kamoun, Eleventh weekamniocentesis for prenatal diagnosis of metabolic diseases, Lancet 1 (1989)849.
[7] R.G. Edwards, P. Hollands, New advances in human embryology: implicationsof the preimplantation diagnosis of genetic disease, Hum. Reprod. 3 (1988)549–556.
[8] C. Coutelle, C. Williams, A. Handyside, K. Hardy, R. Winston, R. Williamson,Genetic analysis of DNA from single human oocytes: a model forpreimplantation diagnosis of cystic fibrosis, Br. Med. J. 299 (1989) 22–24.
[9] M. Adinolfi, P.E. Polani, Prenatal diagnosis of genetic disorders inpreimplantation embryos: invasive and non-invasive approaches, Hum.Genet. 83 (1989) 16–19.
[10] K. Sermon, A. Van Steirteghem, I. Liebaers, Preimplantation genetic diagnosis,Lancet 363 (2004) 1633–1641.
[11] J.D. Delhanty, Preimplantation diagnosis, Prenat. Diagn. 14 (1994) 1217–1227.[12] G. Kokkali, J. Traeger-Synodinos, C. Vrettou, D. Stavrou, G.M. Jones, D.S. Cram,
E. Makrakis, A.O. Trounson, E. Kanavakis, K. Pantos, Blastocyst biopsy versuscleavage stage biopsy and blastocyst transfer for preimplantation geneticdiagnosis of b-thalassaemia: a pilot study, Hum. Reprod. 22 (2007) 1443–1449.
[13] P. Burlet, N. Frydman, N. Gigarel, V. Kerbrat, G. Tachdjian, E. Feyereisen, J.P.Bonnefont, R. Frydman, A. Munnich, J. Steffann, Multiple displacementamplification improves PGD for fragile X syndrome, Mol. Hum. Reprod. 12(2006) 647–652.
[14] S. Coskun, O. Alsmadi, Whole genome amplification from a single cell: a newera for preimplantation genetic diagnosis, Prenat. Diagn. 27 (2007) 297–302.
[15] P.J. Renwick, J. Trussler, E. Ostad-Saffari, H. Fassihi, C. Black, P. Braude, C.M.Ogilvie, S. Abbs, Proof of principle and first cases using preimplantationgenetic haplotyping: a paradigm shift for embryo diagnosis, Reprod. Biomed.Online 13 (2006) 110–119.
[16] C. Spits, C. Le Caignec, M. De Rycke, L. Van Haute, A. Van Steirteghem, I.Liebaers, K. Sermon, Optimization and evaluation of single-cell whole-genomemultiple displacement amplification, Hum. Mutat. 27 (2006) 496–503.
[17] C. Gutierrez-Mateo, J.F. Sanchez-Garcia, J. Fischer, S. Tormasi, J. Cohen, S.Munne, D. Wells, Preimplantation genetic diagnosis of single-gene disorders:experience with more than 200 cycles conducted by a reference laboratory inthe United States, Fertil. Steril. 92 (2008) 1544–1556.
[18] E. Unsal, Y. Aktas, O. Uner, I.A. Baltac, S. Ozcan, F. Turhan, V. Baltaci, Successfulapplication of preimplantation genetic diagnosis for Leigh syndrome, Fertil.Steril. 90 (2008) 2017.e11–2017.e13.
[19] H. Van de Velde, I. Georgiou, M. De Rycke, R. Schots, K. Sermon, W. Lissens, P.Devroey, A. Van Steirteghem, I. Liebaers, Novel universal approach forpreimplantation genetic diagnosis of b-thalassaemia in combination withHLA matching of embryos, Hum. Reprod. 19 (2004) 700–708.
[20] C. Moutou, N. Gardes, J.C. Nicod, S. Viville, Strategies and outcomes of PGD offamilial adenomatous polyposis, Mol. Hum. Reprod. 13 (2007) 95–101.
[21] F. Fiorentino, A. Biricik, A. Nuccitelli, R. De Palma, S. Kahraman, M. Iacobelli, V.Trengia, D. Caserta, M.A. Bonu, A. Borini, M. Baldi, Strategies and clinical
outcome of 250 cycles of preimplantation genetic diagnosis for single genedisorders, Hum. Reprod. 21 (2006) 670–684.
[22] A. Obradors, E. Fernandez, M. Rius, M. Oliver-Bonet, M. Martinez-Fresno, J.Benet, J. Navarro, Outcome of twin babies free of Von Hippel–Lindau diseaseafter a double-factor preimplantation genetic diagnosis: monogeneticmutation analysis and comprehensive aneuploidy screening, Fertil. Steril. 91(2009) 933.e1–933.e7.
[23] S.U. Chen, Y.N. Su, M.Y. Fang, L.J. Chang, Y.Y. Tsai, L.T. Lin, C.N. Lee, Y.S. Yang,PGD of b-thalassaemia and HLA haplotypes using OmniPlex whole genomeamplification, Reprod. Biomed. Online 17 (2008) 699–705.
[24] K. Silander, J. Saarela, Whole genome amplification with Phi29 DNApolymerase to enable genetic or genomic analysis of samples of low DNAyield, Methods Mol. Biol. 439 (2008) 1–18.
[25] K.E. Pierce, J.E. Rice, J.A. Sanchez, L.J. Wangh, Detection of cystic fibrosis allelesfrom single cells using molecular beacons and a novel method of asymmetricreal-time PCR, Mol. Hum. Reprod. 9 (2003) 815–820.
[26] J.E. Rice, J.A. Sanchez, K.E. Pierce, L.J. Wangh, Real-time PCR with molecularbeacons provides a highly accurate assay for detection of Tay–Sachs alleles insingle cells, Prenat. Diagn. 22 (2002) 1130–1134.
[27] C. Vrettou, J. Traeger-Synodinos, M. Tzetis, G. Palmer, C. Sofocleous, E.Kanavakis, Real-time PCR for single-cell genotyping in sickle cell andthalassemia syndromes as a rapid, accurate, reliable, and widely applicableprotocol for preimplantation genetic diagnosis, Hum. Mutat. 23 (2004) 513–521.
[28] C.C. Hung, Y.N. Su, C.Y. Lin, Y.F. Chang, C.H. Chang, W.F. Cheng, C.A. Chen, C.N.Lee, W.L. Lin, Comparison of the mismatch-specific endonuclease method anddenaturing high-performance liquid chromatography for the identification ofHBB gene mutations, BMC Biotechnol. 8 (2008) 62.
[29] C.H. Ho, S.U. Chen, F.S. Peng, C.Y. Chang, Y.R. Lien, Y.S. Yang, Prospectivecomparison of short and long GnRH agonist protocols using recombinantgonadotrophins for IVF/ICSI treatments, Reprod. Biomed. Online 16 (2008)632–639.
[30] H.H. Li, U.B. Gyllensten, X.F. Cui, R.K. Saiki, H.A. Erlich, N. Arnheim,Amplification and analysis of DNA sequences in single human sperm anddiploid cells, Nature 335 (1988) 414–417.
[31] C.C. Hung, C.N. Lee, C.H. Chang, Y.J. Jong, C.P. Chen, W.S. Hsieh, Y.N. Su, W.L. Lin,Genotyping of the G1138A mutation of the FGFR3 gene in patients withachondroplasia using high-resolution melting analysis, Clin. Biochem. 41(2008) 162–166.
[32] Y.N. Su, C.N. Lee, C.C. Hung, C.A. Chen, W.F. Cheng, P.N. Tsao, C.L. Yu, F.J. Hsieh,Rapid detection of beta-globin gene (HBB) mutations coupling heteroduplexand primer-extension analysis by DHPLC, Hum. Mutat. 22 (2003) 326–336.
[33] C.A. Mein, B.J. Barratt, M.G. Dunn, T. Siegmund, A.N. Smith, L. Esposito, S.Nutland, H.E. Stevens, A.J. Wilson, M.S. Phillips, N. Jarvis, S. Law, M. de Arruda,J.A. Todd, Evaluation of single nucleotide polymorphism typing with invaderon PCR amplicons and its automation, Genome Res. 10 (2000) 330–343.
[34] M.P. Reboul, L. Higueret, N. Biteau, A. Iron, Rapid and accurate detection of theCFTR gene mutation 1811+1.6 kbA>G by real-time fluorescence resonanceenergy transfer PCR, Mol. Cell. Probes 19 (2005) 358–362.
[35] Preimplantation Genetic Diagnosis International Society, Guidelines for goodpractice in PGD, Reprod. Biomed. Online 9 (2004) 430–434.