ppt diabetus millitus
66
DIABETUS MELLITUS Bereket Fantahun Pediatric endocrinology Fellow December ,2010
-
Upload
nur-iswanto -
Category
Documents
-
view
37 -
download
0
description
PPT dm
Transcript of ppt diabetus millitus
-
DIABETUS MELLITUS Bereket FantahunPediatric endocrinology FellowDecember ,2010
-
Diabetes mellitus (DM)Is a common, chronic, metabolic syndrome characterized by hyperglycemia as a cardinal biochemical feature. The major forms of diabetes are classified according to those caused by deficiency of insulin secretion due to pancreatic -cell damage (type 1 DM, or T1DM) and those that are a consequence of insulin resistance occurring at the level of skeletal muscle, liver, and adipose tissue, with various degrees of -cell impairment (type 2 DM, or T2DM).
-
Etiologic Classifications of Diabetes Mellitus
Type I diabetes (-cell destruction, usually leading to absolute insulin deficiency) Immune mediated , IdiopathicType 2 diabetes (may range from predominantly insulin resistance with relative insulin deficiency to a predominantly secretory defect with insulin resistance)Other specific types - Genetic defects of -cell function (MODY 1-6) - Genetic Defects in insulin action -Pancreatitis -Trauma, pancreatectomy -Cystic fibrosis
-
Diabetes mellitusEndocrinopathies-Acromegaly-Cushing disease-Pheochromocytoma-Hyperthyroidism
-
Diabetes mellitus
Drug-or chemical-induced Vacor Pentamidine Glucocorticoids Thyroid hormone -Adrenergic agonists Thiazides
-
Diabetes mellitusInfections Congenital rubella, coxsackie virus Cytomegalovirus Other genetic syndromes associated with diabetes Down syndrome Klinefelter syndrome Turner syndrome prader will syndrome
-
Diabetes mellitusGestational diabetes mellitusNeonatal diabetes mellitus Transientwithout recurrence Transientrecurrence 720 yr later Permanent from onset
-
Type1Diabetes mellitusT1DM is the most common endocrine-metabolic disorder of childhood and adolescence, with important consequences for physical and emotional development. Individuals with T1DM confront serious lifestyle alterations that include -an absolute daily requirement for exogenous insulin - the need to monitor their own glucose level - and the need to pay attention to dietary intake.
-
Type1Diabetes mellitus
Morbidity and mortality is from acute metabolic derangements and from long-term complications (usually in adulthood) that affect small and large vessels . The acute clinical manifestations are due to hypoinsulinemic hyperglycemic ketoacidosis. The long-term complications are related to metabolic disturbances (hyperglycemia).
-
The natural history includes 4 distinct stages:1. preclinical -cell autoimmunity with progressive defect of insulin secretion, 2. onset of clinical diabetes,3. transient remission honeymoon period, and4. established diabetes associated with acute and chronic complications and decreased life expectancy.
-
Natural History of Type 1 Diabetes
ENVIRONMENTALTRIGGERCELLULAR (T CELL) AUTOIMMUNITYLOSS OF FIRST PHASE INSULIN RESPONSE (IVGTT)GLUCOSE INTOLERANCE(OGTT)CLINICALONSETHUMORAL AUTOANTIBODIES(ICA, IAA, GADA etc.)
-
Type1Diabetes mellitus
The onset occurs predominantly in childhood, with median age of 7 to 15 yr, but it may present at any age. Peaks of presentation occur in 2 age groups: at 57 yr of age and at the time of puberty.T1DM is characterized by autoimmune destruction of pancreatic islet cells. T1DM is associated with other autoimmune diseases such as thyroiditis, celiac disease and Addison disease.[Schmidt syndrome (w/o celiac)]
-
Type1Diabetes mellitusThe most important genes are located within the MHC HLA class II region on chromosome 6p21, formally termed (IDDM1), accounting for about 60% genetic susceptibility for the disease.Inheritance of HLA-DR3 or -DR4 antigens appears to confer a 2- to 3-fold increased risk for the development of T1DM. When both DR3 and DR4 are inherited, the relative risk for the development of diabetes is increased by 7- to 10-fold.
-
Diabetes mellitus
The children and adolescents with type 2 diabetes are usually obese but are not insulin dependent and infrequently develop ketosis (during severe infections or other stresses) which is characterized by insulin resistance and often a progressive defect in insulin secretion. This type of diabetes was formerly known as adult-onset diabetes mellitus, non-insulin-dependent diabetes mellitus (NIDDM), or maturity-onset diabetes of the young (MODY).
-
Diabetes mellitusThe presentation of T2DM is typically more insidious than that with T1DM.A history of polyuria and polydipsia is relatively uncommon in these patients. The incidence of T2DM in children has increasedAcanthosis nigricans (dark pigmentation of skin creases/flexural areas), a sign of insulin resistance, is present in the majority of patients with T2DM and is accompanied by a relative hyperinsulinemia at the time of the diagnosis
-
Diabetes mellitusIn MODY, there is no apparent autoimmune destruction of cells and no HLA association. This subclass of T2DM consists of specific genetic disorders involving mutations in the gene encoding either pancreatic -cell and liver glucokinase (GK) or in the nuclear transcription factors hepatocyte nuclear factor (HNF) (1, 4, or 1). A defect in the gene regulating glucose transport into the pancreatic cell, the GLUT2 transporter, may be responsible for other forms of T2DM.
-
Diabetes mellitusOTHER SPECIFIC TYPES OF SECONDARY DIABETES.Examples include diabetes secondary to exocrine pancreatic diseases (cystic fibrosis), other endocrine diseases (Cushing syndrome), and ingestion of certain drugs or poisons (the rodenticide Vacor). Certain genetic syndromes, including those with abnormalities of the insulin receptor, also are included in this category. There are no associations with autoimmunity, or islet cell antibodies among the entities in this subdivision.
-
IMPAIRED GLUCOSE TOLERANCE.The term impaired glucose tolerance (IGT) refers to a metabolic stage that is intermediate between normal glucose homeostasis and diabetes. A fasting glucose concentration of 99 mg/dL is the upper limit of normal. This choice is near the level above which acute-phase insulin secretion is lost in response to intravenous administration of glucose and is associated with a progressively greater risk of the development of microvascular and macrovascular complications.
-
Diabetes mellitusIGT is not a clinical entity but rather a risk factor for future diabetes and cardiovascular disease. IGT is often associated with the insulin resistance syndrome (also known as syndrome X or the metabolic syndrome), which consists of insulin resistance, compensatory hyperinsulinemia to maintain glucose homeostasis, obesity (especially abdominal or visceral obesity), dyslipidemia and hypertension
-
Diabetes mellitusInsulin resistance is directly involved in the pathogenesis of T2DM. IGT appears as a risk marker for this type of diabetes at least in part because of its correlation with insulin resistance. The diagnostic criteria for IGT FBS 110-125 mg/dl
-
Diabetes mellitus
Although most autoimmune diseases are more common in females, there appears to be no gender difference in the overall incidence of childhood type 1 diabetes .Genetic susceptibilityThe risk of type 1 diabetes is significantly increased in close relatives of a patient with type 1 diabetes Environmental factorsIn genetically susceptible individuals, exposure to one or more environmental agents appears to trigger an immune response that ultimately causes destruction of the insulin-producing pancreatic beta cells.
-
Environmental Factors
Viral infections like coxsackie B3, coxsackie B4, cytomegalovirus, rubella, and mumps can infect human cell.Diet especially exposure to cow's milk at an early age. The likely mechanism is the molecular mimicry between a 17-amino-acid peptide of the bovine serum albumin and the islet antigen 69. Drugs like pentamidine and Vacor are directly cytotoxic to cells and cause diabetes
-
Family history of DM10% (only)of the children with diabetes have diabetes type 1 among relativesIf both parents are affected by type 1 diabetes, they will have a child with diabetes in about 20-25 %1 parent: about 5 % (less if the mother has diabetes, higher if the father has diabetes)1 sibling with diabetes: about 5 % risk1 twin (identical): risk 30 -40%
-
PATHOGENESIS
The autoimmune attack on the pancreatic islets leads to a gradual and progressive destruction of cells, with loss of insulin secretion. It is estimated that, at the onset of clinical diabetes, 8090% of the pancreatic islets are destroyed.
-
PATHOGENESISRegeneration of new islets has been detected at onset of T1DM, and it is thought to be responsible for the honeymoon phase (a transient decrease in insulin requirement associated with improved -cell function).
-
PATHOGENESISGenetic markers for type 1 diabetes are present from birth (related to Chromosome 6 HLA types)Immune markers are detectable after the onset of the autoimmune process, (ICA,IAA and IGAD)and Metabolic markers can be detected with sensitive tests once enough -cell damage has occurred, but before the onset of symptomatic hyperglycemia
-
PATHOPHYSIOLOGY.
Insulin performs a critical role in the storage and retrieval of cellular fuel. Its secretion in response to feeding is modulated by the interplay of neural, hormonal, and substrate-related mechanisms to permit controlled disposition of ingested foodstuff as energy for immediate or future use.
-
PATHOPHYSIOLOGY
Insulin is our most important anabolic hormone!Saving, storing and up building of carbohydrate, protein and fat.Carbohydrate -Insulin stimulates the insulin receptor on the cell surface Glut 4 , a glucose transporter, is sent to the cell surface of the muscle to pick up glucose by endocytosis. The more insulin the more transporter!Glucose is phosphorylated and ready for either storing as glycogen or glycolysis and energy production (ATP)
-
PATHOPHYSIOLOGY
Fat -Insulin preserves the fat stores (It antagonizes the adrenaline sensitive lipase in fat tissue)Protein amino acid uptake in the cells is stimulated and breakdown of protein is reduced.
-
PATHOPHYSIOLOGY.
Insulin levels must be lowered to then mobilize stored energy during the fasted state. Thus, in normal metabolism, there are regular swings between the postprandial, high-insulin anabolic state and the fasted, low-insulin catabolic state that affect liver, muscle, and adipose tissue .
-
High Plasma Insulin(post prandial state)Low plasma insulin(Fasted state)Liver-Glucose uptake-glycogen synthesis-lipogenesis-absence of gluconeogenesis and ketogenesis-Glucose production-glycogenolysis-ketogenesis-absence of lipogenesisMuscle -Glucose uptake-Glucose oxidation-Glycogen synthesis-Protein synthesis-Absence of glucose uptake-Fatty acid and ketone oxidation-Glycogenolysis-Protein degradation and aminoacid releaseAdipose tissue-Gulucose uptake-Lipid synthesis-Triglyceride uptake-Absence of glucose uptake-Lipolysis and fatty acid release-Absence of triglyceride uptake.
-
PATHOPHYSIOLOGY.
T1DM is a progressive low-insulin catabolic state in which feeding does not reverse but rather exaggerates these catabolic processes. With moderate insulinopenia, glucose utilization by muscle and fat decreases and postprandial hyperglycemia appears At even lower insulin levels, the liver produces excessive glucose via glycogenolysis and gluconeogenesis, and fasting hyperglycemia begins.
-
PATHOPHYSIOLOGY.
Hyperglycemia produces an osmotic diuresis (glycosuria) when the renal threshold is exceeded (180 mg/dL; 10 mmol/L). The resulting loss of calories and electrolytes, as well as the persistent dehydration, produce a physiologic stress with hypersecretion of stress hormones (epinephrine, cortisol, growth hormone, and glucagon).
-
PATHOPHYSIOLOGY.
These hormones, in turn, contribute to the metabolic decompensation by further impairing insulin secretion (epinephrine) by antagonizing its action (epinephrine, cortisol, growth hormone), and by promoting glycogenolysis, gluconeogenesis, lipolysis, and ketogenesis (glucagon, epinephrine, growth hormone, and cortisol) while decreasing glucose utilization and glucose clearance (epinephrine, growth hormone, cortisol).
-
PATHOPHYSIOLOGY
-
CLINICAL PRESENTATION
Childhood type 1 diabetes can present in several different ways. Classic new onset Diabetic ketoacidosis Silent (asymptomatic) incidental discovery Classic new onset-Hyperglycemia without acidosis is the most common presentation of childhood type 1 diabetes. Symptoms are caused by hyperglycemia and include polyuria, polydipsia, weight loss despite increased appetite initially (polyphagia), and lethargy.
-
CLINICAL PRESENTATION
As diabetes develops, symptoms steadily increase, reflecting the decreasing -cell mass, worsening insulinopenia, progressive hyperglycemia, and eventual ketoacidosis. Initially, when only insulin reserve is limited, occasional hyperglycemia occurs. When the serum glucose increases above the renal threshold, intermittent polyuria or nocturia begins. With further -cell loss, chronic hyperglycemia causes a more persistent diuresis, often with nocturnal enuresis, and polydipsia becomes more apparent. Female patients may develop monilial vaginitis due to the chronic glycosuria
-
Diabetic ketoacidosis
Children with type 1 diabetes often present with diabetic ketoacidosis (hyperglycemia and ketoacidosis). Symptoms are similar but usually more severe than those of patients without acidosis. The reported frequency of diabetic ketoacidosis (DKA) as the initial presentation for childhood type 1 diabetes varies from 15 to 67%. Young children (
-
Diabetic ketoacidosisAs an initial presentation or in a known case of DM when they omit their insulin or when there is infection or stress.Can be classified as mild,moderate and severe DKA
NormalMildModerateSevereCO 2 meq/l(venous)20-2816-2010-15
-
Diabetic ketoacidosisWhen extremely low insulin levels are reached, keto acids accumulate. Keto acids produce abdominal discomfort, nausea, and emesis.Dehydration accelerates, causing weakness and polyuria persists. As in any hyperosmotic state, the degree of dehydration may be clinically underestimated [due to expansion of intravascular volume from intracellular source]Ketoacidosis exacerbates prior symptoms and leads to Kussmaul respirations (deep, heavy, rapid breathing), fruity breath odor (acetone), diminished neurocognitive function, and possible coma.
-
CLINICAL PRESENTATION
Silent presentationSome children will be diagnosed with type 1 diabetes before the onset of clinical symptoms. This presentation is least common and typically occurs in children who have another close family member with type 1 diabetes and are being closely monitored . A rare presentation.
-
DIAGNOSIS
Fasting plasma glucose 126 mg/dL (7 mmol/L) on two occasions Symptoms of hyperglycemia and a random venous plasma glucose 200 mg/dL (11.1 mmol/L) Abnormal oral glucose tolerance test (OGTT) defined as a plasma glucose 200 mg/dL (11.1 mmol/L) measured two hours after a glucose load of 1.75 g/kg (maximum dose of 75 g) Most children and adolescents are symptomatic and have plasma glucose concentrations well above 200 mg/dL (11.1 mmol/L); thus, OGTT is seldom necessary to diagnose type 1 diabetes.
-
DIAGNOSIS
HbA1c determination is said to be a very sensitive diagnostic tool of new onset diabetes and very use full parameter to monitor the management and a good predictor of chronic complication of diabetes
-
Challenges in pediatrics DMThere are unique challenges in caring for children and adolescents with diabetes that differentiate pediatric from adult care. These include the obvious differences in the size of the patients, developmental issues such as the unpredictability of a toddler's dietary intake and activity level, and medical issues such as the increased risk of hypoglycemia and diabetic ketoacidosis. Because of these considerations, the management of a child with type 1 diabetes must take into account the age and developmental maturity of the child.
-
GOALS
Successful management of children with diabetes includes the following : Balancing strict glycemic control, which reduces the risk of long-term sequelae, and avoidance of severe hypoglycemia, which is more likely with stricter control. In children, targeted glycemic goals define what is thought to be the best balance between these long- and short-term complications.
-
GOALS Maintaining normal growth, development, and emotional maturation. Increasing self-independent management as the child grows is an ongoing goal. Training the patient and family to provide appropriate daily diabetes care in order to attain glucose control within the range of predetermined goals, and to recognize and treat hypoglycemia.
-
DKA Management
1.Volume expansion 10-20 ml/kg R/L or N/S over 1 hour2.Insulin therapy and K+ replacement - 0.1u /kg/hr continuous insulin mxt -0.5 u/kg/ every 4-6 hourly intermittent insulin mxt -K + 20-40 meq/L of fluid3. Fluid mxt 85 ml/kg + maintenance fluid bolus/23 hrs(0.45 % N/S and when glucose is < 250 mg/dl change the fluid to 5 % D/W4.Treat the precipitating factors
-
DKA mxt RisksHypoglycemiaCerebral edemaHypokalemiaSo we need to follow the child with V/S, frequent glucose and electrolyte measurement to act accordingly.Bed side mannitol 1gm/kg is important
-
TreatmentInsulin Therapy. Children with long-standing diabetes and no insulin reserve require about 0.7 U/kg/d if prepubertal, 1.0 U/kg/d at midpuberty, and 1.2 U/kg/d by the end of pubertyBasic education about the insulin injection , meal planning ,exercise, about symptoms of hypo/hyperglycemia and importance of SMBG [self-monitoring blood glucose] and the impact of poor control of DM.
-
Normal Endogenous Insulin Secretion
-
Nutritional management55% CHO,30 %fat and 15 % protein and the CHO should be complex CHOThe total daily caloric intake is divided to provide 20% at breakfast, 20% at lunch, and 30% at dinner, leaving 10% for each of the midmorning, mid afternoon, and evening snacks, if they are desired.Monitoring-SMBG, insulin dose adjustment. Ideally, the blood glucose concentration should range from approximately 80 mg/dL in the fasting state to 140 mg/dL after meals. In practice, however, a range of 60220 mg/dL is acceptable
-
Target BG and HbA1c level The non diabetic reference range for HbA1c is 4.55.7%
AgePre meal BG level(mg/dl)30 days average BG level (mg/dl)Target HbA1c
-
HbA1c A reliable index of long-term glycemic control is provided by measurement of glycosylated hemoglobin. HbA1C represents the fraction of hemoglobin to which glucose has been non enzymatically attached in the bloodstream. Will be measured 3-4 x /year.In non diabetic individuals, the HbA1C fraction is usually less than 6%; In diabetics, values of 67.9% represent good metabolic control, values of 8.09.9%, fair control, and values of 10.0% or higher, poor control.
-
ExerciseNo form of exercise, including competitive sports, should be forbidden to the diabetic child.But the risk of hypoglycemia is there during or within hours after exercise so BG measurement is important.They have to take candy or carbonated juice to take immediately if there are symptoms of hypoglycemia
-
Insulin treatment modalities1921-22 to mid thirties: crystalized animal insulin (only rapid acting)Depot insulins (i.e NPH Protamin) and Lente (Zink)Human insulinAnalogues: direct action, Humalog and NovoRapid(max peak in 1 hr)Depot (Glargine and Detemir): more predictable action than intermediate and lente
-
Insulin PreparationsKinetics following s.c. injection
-
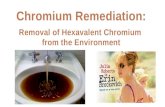
*McMahon G and Dluhy R. N Engl J Med 2007;10.1056/NEJMe078196Schematic Time-Activity Curves for Available Insulin Formulations
-
Insulin injection Conventional way(twice daily injection) Regular insulin with intermediate acting insulin (NPH/Lente insulin)Multiple daily injection using basal(Glargine /Detemir) and bolus insulin(Lispro/Asparte/Regular insulin)CSII (continuous subcutaneous insulin injection or pump therapy) using short acting insulin
-
Other important Issues
1.Hypoglycemic reactions2.The Dawn and somogy phenomenon3.Non Adherance4.Anxiety and depression5.Fear of self injecting and self testing6.Management during infections and surgery
-
T2DM managementWeight loss and physical exercise are said to be the main strategies in controlling glucose level in T2DM patientsOral hypoglycemic agents like metformin [a biguanide] can be triedInsulin if they have ketonuria
-
Why we need good controlAcute diabetic complication is a riskIt predicts the occurrence of chronic complicationIt was not known until 1993 if the degree and duration of hyperglycemia can influence the onset and progression of chronic complications of the diseaseDCCT studies finally proved that complications increased with higher blood sugars, i.e HbA1C
-
Long term complications
-microvascular complications (Retinopathy, nephropathy)-Macrovascular complication-Growth failure and delayed puberty
-
Prognosis
Their life span is 10 yrs shortervisual, renal and neuropathic complications are commonPuberty may be delayed and final Ht is less than the genetic Ht
-
Injection modelsRepeted injectionsFuture intelligent pumps with reliable sensors for glucose levels= mechanical pancreas
-
Glucometers
-
PANCREAS AND ISLET TRANSPLANTATION AND REGENERATION In an attempt to cure T1DM, transplantation of a segment of the pancreas or of isolated islets has been performed. These procedures are both technically demanding and associated with the risks of disease recurrence and complications of rejection or its treatment by immunosuppression. Complications of immunosuppression include the development of malignancy.
****Figure 1. Schematic Time-Activity Curves for Available Insulin Formulations. Biphasic insulin preparations (not shown) combine short-acting insulin with neutral protamine Hagedorn (NPH) insulin.