Pharmacotherapy: A Pathophysiologic Approach The McGraw-Hill Companies Chapter 28.
77
Asthma Chapter 33 Pharmacotherapy: A Pathophysiologic Approach The McGraw-Hill Companies Chapter 28
-
Upload
lawrence-benson -
Category
Documents
-
view
241 -
download
0
Transcript of Pharmacotherapy: A Pathophysiologic Approach The McGraw-Hill Companies Chapter 28.
Asthma Chapter 33
Asthma Chapter 33
Pharmacotherapy: A Pathophysiologic Approach The McGraw-Hill Companies
Chapter 281AbbreviationsArg: arginineBHR: bronchial hyperresponsivenessCYP- cytochromeDPI: dry-powder inhalerFEV1: forced expiratory volume in 1 secondFVC: forced vital capacityICS: inhaled corticosteroidIgE: immunoglobulin ELABA: long-acting 2-agonistLTRA: leukotriene receptor antagonistMDI: metered-dose inhalerNAEPP: National Asthma Education and Prevention ProgramPEF: peak expiratory flowSABA: short-acting 2-agonistVHC: valved holding chamber22Key ConceptsAsthma is a disease of increasing prevalencecaused by genetic & environmental factorschronic inflammatory pulmonary disorder No known cure or 1 preventionImmunohistopathologic features include cell infiltration by eosinophils, neutrophils, T-helper type 2 lymphocytes, mast cells, epithelial cells3Key ConceptsIntermittent or persistent airflow obstruction inflammation & bronchial smooth muscle constrictionpersistent changes in airway structure may occurInhaled corticosteroids have the greatest efficacy/safety profile for long-term management across all age groupsBronchial smooth muscle constriction prevented/treated most effectively with inhaled 2-adrenergic receptor agonists
44Key ConceptsVariability in response to medications requires individualization of therapy use lowest dose to maintain controlOngoing patient education for a partnership in asthma care essential for optimal outcomes
55AsthmaChronic inflammatory lung diseasereversible airflow obstructionincrease in bronchial hyperresponsiveness (BHR)Recurrent symptomswheezing breathlessnesschest tightnesscoughing especially at night or early morning66Epidemiology Affects about 23 million Americansmost common childhood chronic diseaseby early adulthood, 30 to 70% will markedly improve or be symptom-freeHigher prevalence in minoritiesurbanizationpoor access to care7American Lung Association. Lung Disease Data: 2008. http://www.lungusa.org. Accessed 5-24.09. 7EpidemiologySignificant burden on healthcare system3rd leading cause of preventable hospitalization> $19 billion direct & indirect costsCan be life-threatening if not properly managednearly 4,000 asthma deaths per year80 to 90% preventableeducation is key to prevention of death from asthma8American Lung Association. Lung Disease Data: 2008. http://www.lungusa.org National Institutes of Health, National Heart, Lung, and Blood Institute. National Asthma Education and Prevention Program. Full Report of the Expert Panel: Guidelines for the diagnosis and management of asthma (EPR-3) 2007. http://www.nhlbi.nih.gov/guidelines/asthma 8Etiology Genetic predispositionatopylinked with metalloproteinase genesEnvironmental exposurerisk factorssocioeconomic statusfamily sizetobacco smokeallergen exposureurbanizationexposure to common childhood infectious agentshygiene hypothesis99Asthma TriggersRespiratory infectionRSV, rhinovirus, influenza, parainfluenza, Mycoplasma pneumoniaAllergensAirborne pollens (grass, trees, weeds), house-dust mites, animal danders, cockroaches, fungal sporesEnvironmentCold air, fog, ozone, sulfur dioxide, nitrogen dioxide, tobacco smoke, wood smokeEmotionsAnxiety, stress, laughterExerciseParticularly in cold, dry environmentsDrugs / preservativesAspirin, NSAIDs (cyclooxygenase inhibitors), sulfites, benzalkonium chloride, nonselective -blockersOccupational stimuliBakers (flour dust); farmers (hay mold); spice and enzyme workers; printers (arabic gum); chemical workers (azo dyes, anthraquinone, ethylenediamine, toluene diisocyanates, polyvinyl chloride); plastics, rubber, and wood workers (formaldehyde, western cedar, dimethylethanolamine, anhydrides)10DiPiro JT, Talbert RL, Yee GC, Matzke GR, Wells BG, Posey LM: Pharmacotherapy: A Pathophysiologic Approach, 7th ed. http://www.accesspharmacy.com10PathophysiologyAirway inflammationBHRAirflow obstructionbronchospasm, edema, mucus hypersecretionAirway remodelingMediated by eosinophils, T cells, mast cells, macrophages, epithelial cells, fibroblasts, bronchial smooth muscle cells1111
12
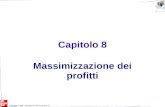
12Pathology Found in Asthmatic Bronchus Compared to Normal Bronchus13
13PathophysiologyEpithelial cells release eicosanoids, peptidases, matrix proteins, cytokines, nitric oxideepithelial sheddingEosinophilsrelease inflammatory mediatorsleukotrienes, granule proteins
1414PathophysiologyTH2 lymphocytes produce cytokines that mediate allergic inflammationTH1/TH2 imbalanceMast cell degranulationrelease histamine, leukotrienes, prostaglandinsMucus plugs epithelial & inflammatory cellsfurther airway obstruction1515
1616
17ECP: eosinophil cationic protein; GM-CSF: granulocyte-macrophage colony-stimulation factor; IAR: immediate asthmatic reaction; IFN: interferon; IL: interleukin ; LAR: late asthmatic response; LT: leukotriene; MBP: major basis protein; PAF: platelet-activating factor; PG:prostaglandin
DiPiro JT, Talbert RL, Yee GC, Matzke GR, Wells BG, Posey LM: Pharmacotherapy: A Pathophysiologic Approach, 7th ed. http://www.accesspharmacy.com17Conditions Affecting Asthma SeverityViral respiratory infectionsEnvironmental/occupational triggersPsychosocial stressorsRhinitis/sinusitisGastroesophageal Reflux Disease (GERD)
1818Clinical PresentationNo single test can diagnose asthmacareful patient historyspirometry demonstrates reversible airway obstructionSymptomschronic asthma: dyspnea, chest tightness, coughing especially at night, wheezingsevere acute asthma: acute respiratory distress
1919Aerosol Therapy2020DevicesMust determine which device is best for each patientMetered-dose inhaler (MDI)spacersvalved holding chamber (VHC)Dry-powder inhaler (DPI)Nebulizersjet ultrasonic 2121Metered-Dose Inhaler22
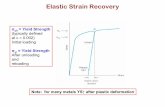
22Factors Determining Lung Deposition of Aerosols 23
DeviceDevice FactorsPatient FactorsMetered-dose inhaler (MDI)Canister held invertedFormulation (HFA, solution, suspension)Actuator cleanlinessAddition of a spacer deviceInspiratory flow (slow, deep)Breath-holdingCoordinating actuation with inhalationPriming and shaking the deviceDry-powder inhaler (DPI)Device cleanlinessResistance to inhalationHumidityInspiratory flow (deep, forceful)Tilting head backMaintaining parallel to ground once activatedJet nebulizer (small volume)Volume fill (36 mL)Gas flow (612 L/min)Dead-space volumeOpen versus closed systemThumb-activating valveMouthpiece versus face maskInspiratory flow (slow, deep)Breath-holdingTapping nebulizerUltrasonic nebulizerVolume fillNot effective for suspensionsMouthpiece versus face maskInspiratory flow (slow, deep)Breath-holdingTapping nebulizerSpacer deviceVolume (650 mL)One-way valvesHolding chamber versus open-endedStatic vs nonstaticMouthpiece versus face maskInspiratory flow (slow, deep)Time between actuation and inhalation (< 5 s)Cleaning with detergent to reduce staticMultiple actuations decrease deliveryCoordination of actuation and inhalation for the simple open-tube spacersDiPiro JT, Talbert RL, Yee GC, Matzke GR, Wells BG, Posey LM: Pharmacotherapy: A Pathophysiologic Approach, 7th ed. http://www.accesspharmacy.com23Patient EducationAppropriate inhalation technique is vital for optimal drug delivery and therapeutic effectup to 30% cannot master MDI techniqueRinse mouth after inhaled corticosteroids (ICS)< 4 years old usually need to attach a face mask to the inhalation device2424Steps for Using Your InhalerRemove the cap and hold inhaler uprightShake the inhalerTilt your head back slightly and breathe out slowlyPosition the inhaler A or B is optimalC is acceptable for those who have difficulty with A or B; required for breath-activated inhalers
25
DiPiro JT, Talbert RL, Yee GC, Matzke GR, Wells BG, Posey LM: Pharmacotherapy: A Pathophysiologic Approach, 7th ed. http://www.accesspharmacy.com25Steps for Using Your Inhaler ContinuedPress down on the inhaler to release medication as you start to breath in slowlyBreathe in slowly (3 to 5 seconds)Hold your breath for 10 seconds to allow the medicine to reach deeply into your lungsRepeat puff as directed. Waiting 1 minute between puffs may permit second puff to penetrate your lungs betterSpacers/holding chambers are useful for all patients. Recommended for young children and older adults and for use with corticosteroids.26DiPiro JT, Talbert RL, Yee GC, Matzke GR, Wells BG, Posey LM: Pharmacotherapy: A Pathophysiologic Approach, 7th ed. http://www.accesspharmacy.com26Steps for Using Your Inhaler ContinuedAvoid common inhaler mistakesbreathe out before pressing your inhalerinhale slowlybreathe in through your mouth, not your nosepress down on your inhaler at the start of inhalation (or within the first second of inhalation)keep inhaling as you press down on inhalerpress your inhaler only once while you are inhaling (one breath for each puff)make sure you breathe in evenly & deeplyDifferent type of inhalers require different techniques27DiPiro JT, Talbert RL, Yee GC, Matzke GR, Wells BG, Posey LM: Pharmacotherapy: A Pathophysiologic Approach, 7th ed. http://www.accesspharmacy.com27Severe Acute Asthma2828Goals of TherapyCorrect significant hypoxemiaRapid reversal of airflow obstructionReduce likelihood of relapse or future recurrence of severe obstructionDevelop written action plan
2929TreatmentEarly recognition of deterioration & aggressive treatment are vitalpatient/family educationPrimary therapyshort-acting 2-agonist (SABA)Additional therapy depending on severitysystemic corticosteroidsinhaled anticholinergicO2303031
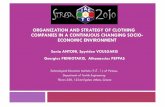
Home Management of Acute Asthma Exacerbations31
Hospital Care of Acute Asthma ExacerbationsContinued on next slide3232
Continued from previous slideHospital Care of Acute Asthma Exacerbations3333Special PopulationsChildren < 4 years old may have higher risk for respiratory failureRequire use of a face mask for aerosolized medicationappropriate size/fitreduces drug delivery to lung by 50%minimal dose is recommended vs weight based dose34342-AgonistsMechanism: bronchodilatorsmooth muscle relaxationskeletal muscle stimulationAerosol route more bronchoselective 3535Inhaled SABAsTreatment of choicemost effective bronchodilator for severe acute asthmaFrequent administrationinhalations every 20 minutescontinuous nebulizationyoung childrenunsatisfactory response to initial 3 doses of inhaled SABAPEF or FEV1 < 30% predicted or personal best3636Inhaled CorticosteroidsMechanism: antiinflammatoryreduce number of mast cells & eosinophilsincrease number of -adrenergic receptors, improve receptor responsivenessreduce mucus production, hypersecretionreduce BHRreduce airway edema/exudation
3737Pharmacokinetics of Inhaled Corticosteroids
3838Systemic CorticosteroidsUseincomplete response to initial inhaled SABA dosesContinue full dose until peak flow 70% of predicted or personal bestAdverse effects dependent on dose & durationshort bursts do not cause serious toxicitiesadrenal suppression less common with shorter-acting corticosteroids (e.g. prednisone)3939AnticholinergicsMechanism: bronchodilatorcompetitively inhibit muscarinic receptorsno effect on BHRLess effective bronchodilator than 2-agonistsNot FDA approved for asthmaAvailable inhaled anticholinergicsipratropiumtiotropium: studies inconclusive for use in asthma
4040IpratropiumUseadjunct when incomplete response to SABA aloneDuration of action4 to 8 hoursduration/intensity of action dose dependentNegligible systemic effects4141Clinical ControversyEmergency departmentunresponsive to standard doses of inhaled 2-agoniststreat with IV magnesium sulfate?Magnesium sulfatemoderately potent bronchodilatoradverse effects include hypotension some require dopamine to treat hypotension
4242Clinical ControversySevere obstructionresponse improves with ipratropium & continuous SABA nebulizationSubset analyses of 2 studiesless hospitalizations for magnesium versus placebo in patients with severe obstructionLarge randomized study did not find less hospitalizations even in severe subset43Rowe BH, Bretzlaff JA, Bourdon C, et al. Intravenous magnesium sulfate treatment for acute asthma in the emergency department: A systematic review of the literature. Ann Emerg Med 2000;36:181-190. 43Clinical ControversyGuideline recommendationsmay consider IV magnesium sulfate in patients with severe exacerbations & poor response to initial inhaled 2-agonists
4444Clinical ControversyInhaled 2-agonists administration MDI plus VHC versus jet nebulizationtreatment outcomes similaris MDI plus VHC more cost effective?no studiesCurrent practice should be based on comfort level of clinic staff Dolovich MB, Ahrens RC, Hess DR, et al. Device selection & outcomes of aerosol therapy: Evidence-based guidelines. Chest 2005;127:335371. Dolovich MA, MacIntyre NR, Dhand R, et al. Consensus conference on aerosols and delivery devices. Respir Care 2000; 45:588776 4545MonitoringFrequency dependent on exacerbation severitylung functionspirometrypeak flowO2 saturation
4646EducationSelf management planwritten action planpeak flow monitoringAsthma educationsigns, symptoms of exacerbationremoval, avoidance of triggers4747Chronic Asthma4848Goals of TherapyReduce impairmentprevent chronic, troublesome symptomsrequire infrequent use ( 2 days a week) of inhaled SABA for quick relief of symptomsmaintain (near-) normal pulmonary functionmaintain normal activity levelsmeet patients & families expectations of and satisfaction with care4949Goals of TherapyReduce riskprevent recurrent exacerbationsminimize need for visits/hospitalizationsprevent loss of lung function prevent reduced lung growth in childrenminimal adverse effects of therapy
5050Nonpharmacologic TreatmentEnvironmental controlManage comorbid conditionsSelf-management skillswritten action plansrecognize early signs of deteriorationEducationasthma, role of medications, inhalation technique, environmental control, how to use action planreinforce every visit5151Pharmacologic TreatmentNational Asthma Education Prevention Program (NAEPP) recommendations categorized by age0 to 4 years5 to 11 years12 yearsStepwise approachinitial therapy based on asthma severitytherapy adjusted based on asthma control
52National Institutes of Health, National Heart, Lung, and Blood Institute. National Asthma Education and Prevention Program. Full Report of the Expert Panel: Guidelines for the diagnosis and management of asthma (EPR-3) 2007. http://www.nhlbi.nih.gov/guidelines/asthma 52TreatmentQuick relief: SABA for all patientsLong-term controlpreferredICS for persistent asthmaincreased ICS dose or addition of long-acting 2-agonist (LABA) for further controlalternativesno to minimal difference in efficacy between alternativescromolyn, nedocromil, leukotriene modifiers, theophyllineomalizumab: severe uncontrolled asthma & atopy
5353Classifying Asthma Severity for Patients Not Currently Taking Long-Term Control Medications (Children 0-4 and 5-11 years)ComponentsIntermittentPersistentMildModerateSevereImpairmentSymptoms2 days/week>2 days/week but not dailyDailyThroughout the dayNighttime awakenings (0-4 yr)None1-2 times/month2-3 times/month> Once a weekNighttime awakenings (5-11 yr)twice/month3-4 times/month> Once per week but not nightlyOften 7 times/weekSABA use for symptom control2 days/week>2 days/week but not dailyDailySeveral times per dayInterference with normal activityNoneMinor limitationSome limitationExtremely limitedLung function (5-11 yr)FEV1 >80%FEV1/FVC >85%FEV1 >80%FEV1/FVC >80%FEV1 60-80%FEV1/FVC 75-80%FEV1 2 in 1 year Recommended step for initiating treatmentStep 1Step 2Step 3 and consider short course of systemic oral corticosteroids54DiPiro JT, Talbert RL, Yee GC, Matzke GR, Wells BG, Posey LM: Pharmacotherapy: A Pathophysiologic Approach, 7th Edition: http://www.accesspharmacy.com/54ComponentsIntermittentPersistentMildModerateSevereImpairmentSymptoms2 days/week>2 days/week but not dailyDailyThroughout the dayNighttime awakenings twice/month3-4 times/month> Once per week but not nightlyOften 7 times/weekSABA use for symptom control2 days/week>2 days/week but not > once per dayDailySeveral times per dayInterference with normal activityNoneMinor limitationSome limitationExtremely limitedLung function (Normal FEV1/FVC: age 8-19 y 85%; 20-39 y 80%; 40-59 y 75%; 60-80 y 70%)FEV1 >80%FEV1/FVC normalFEV1 >80%FEV1/FVC normalFEV1 60-80%FEV1/FVC reduced 5%FEV1 5%
RiskIntermittentPersistentExacerbations0-2/year>2 in 1 year Recommended step for initiating treatmentStep 1Step 2Step 3 and consider short course of systemic oral corticosteroidsStep 4 or 5Classifying Asthma Severity for Patients Not Currently Taking Long-Term Control Medications (12 years old)DiPiro JT, Talbert RL, Yee GC, Matzke GR, Wells BG, Posey LM: Pharmacotherapy: A Pathophysiologic Approach, 7th Edition: http://www.accesspharmacy.com/5555Stepwise Approach for Asthma Management56
56Stepwise Approach for Asthma Management57
57Stepwise Approach for Asthma Management
5858Special PopulationsYoung children, especially 0-4 yearsmany recommendations based on extrapolated datastudies of ICS show improvementcombination therapy inadequately studiedElderlyosteoporosis risk increased with high dose ICSPregnancybudesonide preferred ICSalbuterol preferred for quick relief5959Inhaled Corticosteroids (ICS)Use: cornerstone of chronic asthma therapyimprove lung functionreduce severe exacerbationsonly therapy shown to reduce risk of asthma deathLow systemic activityResponse delayed for several weeks6060Inhaled CorticosteroidsProductsbeclomethasone dipropionatebudesonideflunisolidefluticasone propionatemometasone furoatetriamcinolone acetonideciclesonide
6161Inhaled CorticosteroidsAdverse effects dose dependentsystemic effects can occur at high dosesoropharyngeal candidiasisdysphonia Growth retardation may occurdose-dependenttransientsusceptible populationsstudies suggest reaching predicted adult height not affected62National Institutes of Health, National Heart, Lung, and Blood Institute. National Asthma Education and Prevention Program. Full Report of the Expert Panel: Guidelines for the diagnosis and management of asthma (EPR-3) 2007 Kelly HW. Potential adverse effects of the inhaled corticosteroids. J Allergy Clin Immunol 2003;112:469478. 62LABAsUse: preferred adjunct/ICS combinationadults & most childrenbetter control than increasing ICS dose aloneNot for quick reliefProvide long lasting bronchodilation ( 12 hours)Productsformoterolsalmeterol
6363LABAsSystemic side effects dose dependentNot to be used as monotherapyincreased risk of severe, life threatening exacerbation & asthma related deathpreliminary data suggest concomitant ICS may prevent/decrease risk64Nelson HS, Weiss ST, Bleecker ER, Yancey SW, Dorinsky PM. The Salmeterol Multicenter Asthma Research Trial: A comparison of usual pharmacotherapy for asthma or usual pharmacotherapy plus salmeterol. Chest 2006;129:1526. Kelly HW. Risk versus benefit considerations for the 2-agonists. Pharmacotherapy 2006;26:164S174S. 64MethylxanthinesMechanism: bronchodilationnonselective phosphodiesterase inhibitorisoenzyme III: airway smooth muscleisoenzyme IV: inflammatory cell regulationcompetitively inhibit adenosinestimulate catecholamine releaseUse declined due to risk for toxicityalternative/adjunct therapy
6565TheophyllineRoutine serum concentration monitoringsignificant bronchodilation by 5 mcg/mLmost will not have toxic symptoms when