Pharma Report Asthma
21
Comparison of a β2 – Agonist, Terbutaline, with an inhaled Corticosteroid, Budesonide, in newly detected asthma
description
journal on asthma
Transcript of Pharma Report Asthma
Comparison of a β2 – Agonist, Terbutaline, with an inhaled Corticosteroid, Budesonide, in newly detected asthma
Background
• The main goal of asthma treatment has usually been to maintain normal airway patency with bronchodilators.
• Asthma is also characterized by inflammatory changes in the airway mucosa which points to the potential value of anti-inflammatory therapy.
• Extravasation of fluid from bronchial circulation, which leads to mucosal edema and appearance of inflammatory cells.
• Increased bronchial responsiveness
Theophylline Inhaled steroids
• Aim is to suppress inflammation
Methods
• Study design• Multicenter, double-blind, randomized, parallel-group trial
• Five centers
• Pretreatment period
• Two-week run-in period
• Four-week baseline period
• Block randomization (4)
Study Protocol
• DRUGS: Budesonide and Terbutaline
• Pressurized metered-dose inhaler through a large volume spacer
• Pretreatment period: Terbutaline 375μg twice a day
• Treatment period:• Budesonide 600μg twice a day
• Terbutaline 375μg twice a day
• Supplemental:• Terbutaline 250μg per puff
• Oral Theophylline 300mg twice a day
• Oral prednisolone for six days in decreasing doses (35, 25, 20, 15, 10 and 5 mg per day)
Patients
• Adult (15 or older)
• Non-smoking
• With newly detected bronchial asthma
• FEV1: inc. by more than 15% after inhalation of a β2-agonist or decrease by more than 15% after exercise tolerance test
• FVC and FEV1 had to be at least 80% of predicted values after treatment with β2-agonist
Patients (c..)
• FEV1 had to fall by more than 15% after the patient inhaled 10 breaths of histamine nebulized from a solution containing less than 32mg/ml
• Patients with a history of regular treatment or treatment with corticosteroid or cromolyn were excluded.
• 103 patients were enrolled and randomized
• 6 were later found not to have fulfilled all the criteria• 3 – treated with oral prednisolone during pretreatment
period
• 1 – irreversible pulmonary obstruction
• 2 – FEV1 values during the baseline period that were too low
• Informed consent
• Finnish Medical Board and local ethics committees
Recording outcomes
• Pretreatment and subsequent 12 weeks – PEF – medication in the morning and evening
• Use of supplemental medication and adverse reactions
• Symptoms of asthma (dyspnea, cough, and sputum production)
• Daily activities
Recording outcomes
• The assessments performed at the clinic at the start of the pretreatment and active treatment periods and then after 6, 12, 28, 44, 48, 72, 92, and 96 weeks of treatment included spirometry, bronchial responsiveness and checks of the patient’s diaries.
• Last dose of the study medication in the evening
• not to use supplemental medication six hours before the appointment
Assessment of Bronchial Responsiveness
• Histamine diphosphate in phosphate-buffered saline
• Six doubling concentration, or dose steps – 1, 2, 4, 8, 16, and 32 mg/ml
• Nebulizers at an airflow of 5 liters/min.
• 0.125 and 0.250 ml/min
• 10 tidal breaths of nebulized saline and continued with histamine solutions of successively higher concentrations
Assessment of Bronchial Responsiveness
• FEV1 was measured 1.5mins after each challenge
• Challenge testing was discontinued when FEV1 fell by 15% or more
• The concentration of histamine that produced the drop was calculated by interpolation and called the “provocative concentration” (PC15)
• If FEV1 dropped less than 15% even when the highest concentration of histamine diphosphate (32mg/ml) was used, the PC15 was considered to be 64mg/ml
RESULTS
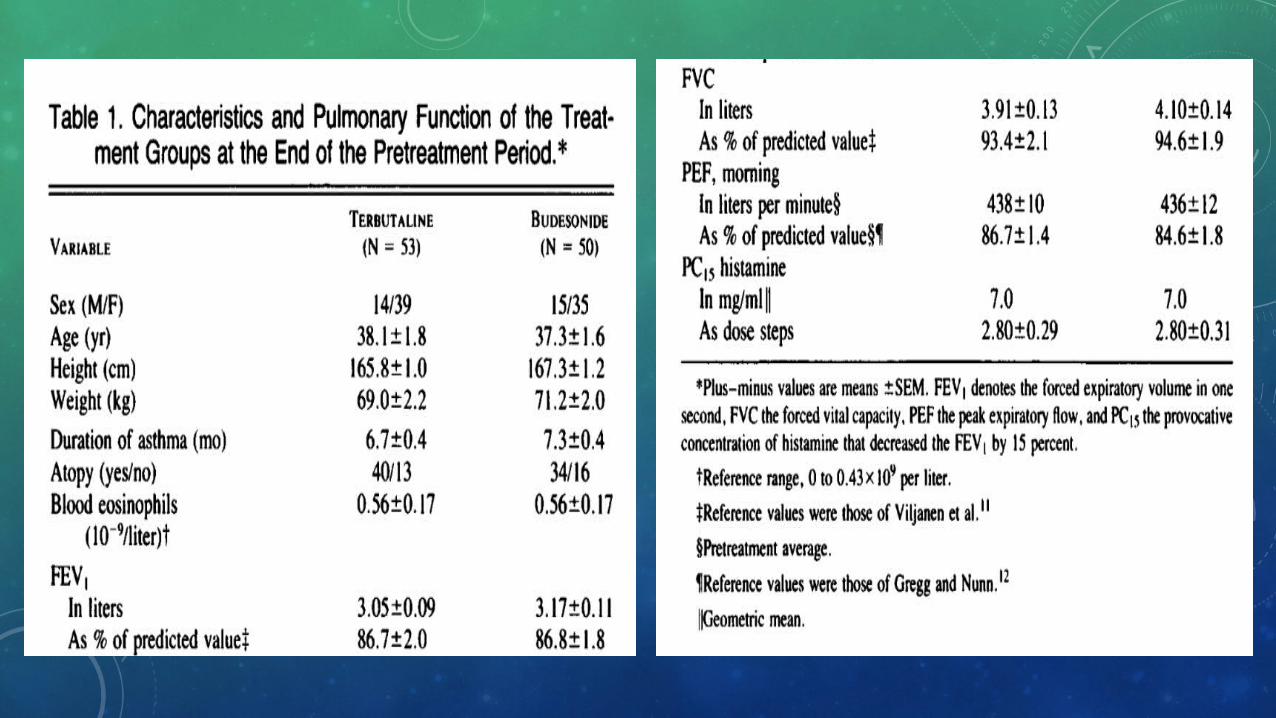
Lung function
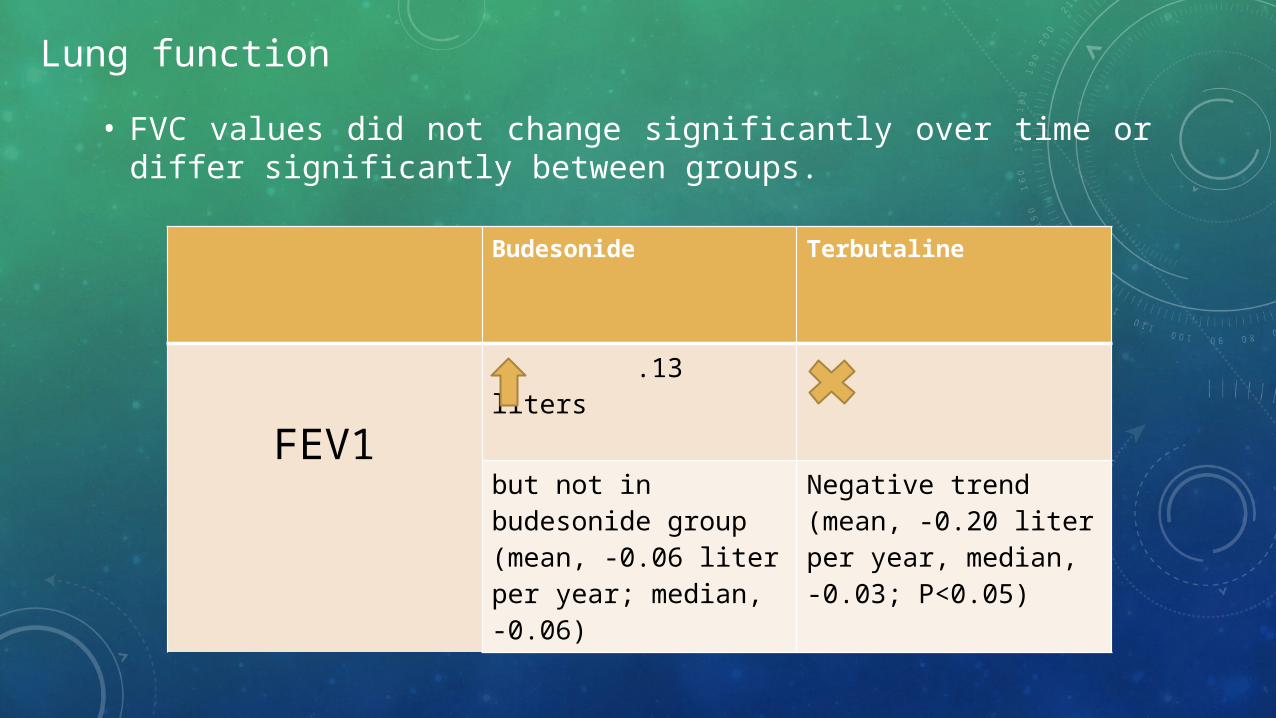
• FVC values did not change significantly over time or differ significantly between groups.
Budesonide Terbutaline
FEV1 .13 liters
but not in budesonide group (mean, -0.06 liter per year; median, -0.06)
Negative trend (mean, -0.20 liter per year, median, -0.03; P<0.05)
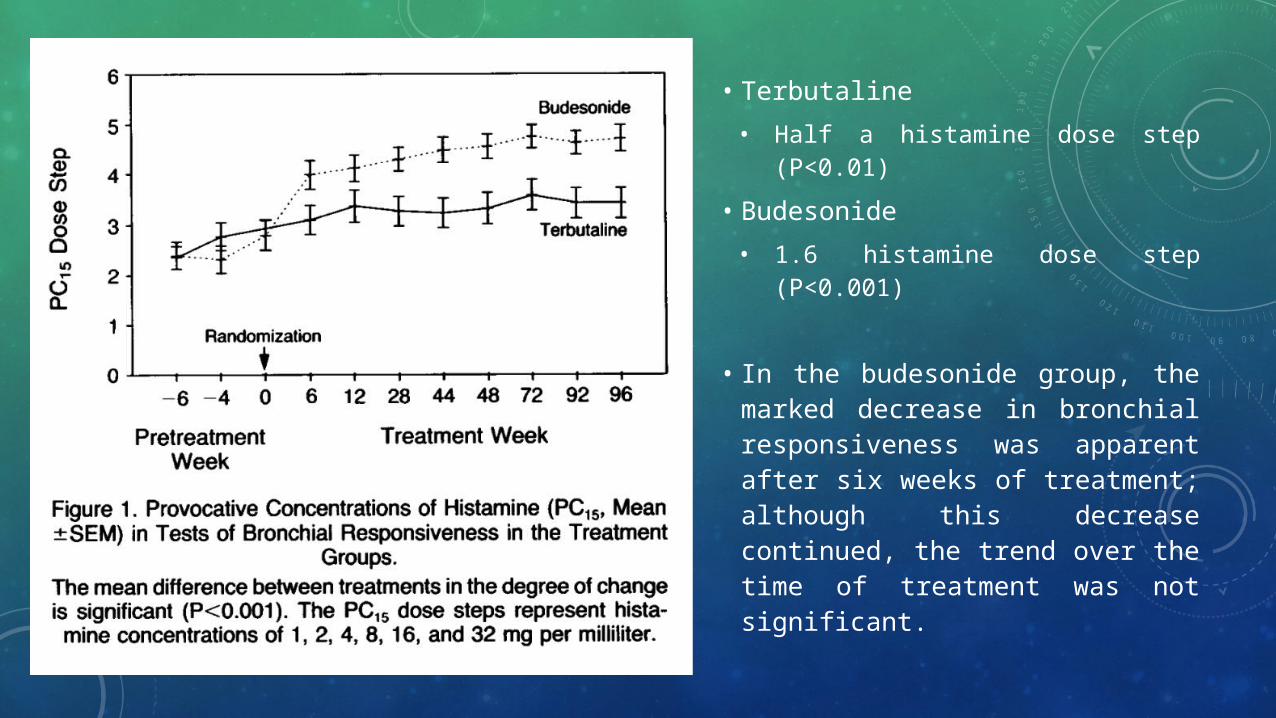
• Terbutaline• Half a histamine dose step
(P<0.01)
• Budesonide• 1.6 histamine dose step
(P<0.001)
• In the budesonide group, the marked decrease in bronchial responsiveness was apparent after six weeks of treatment; although this decrease continued, the trend over the time of treatment was not significant.
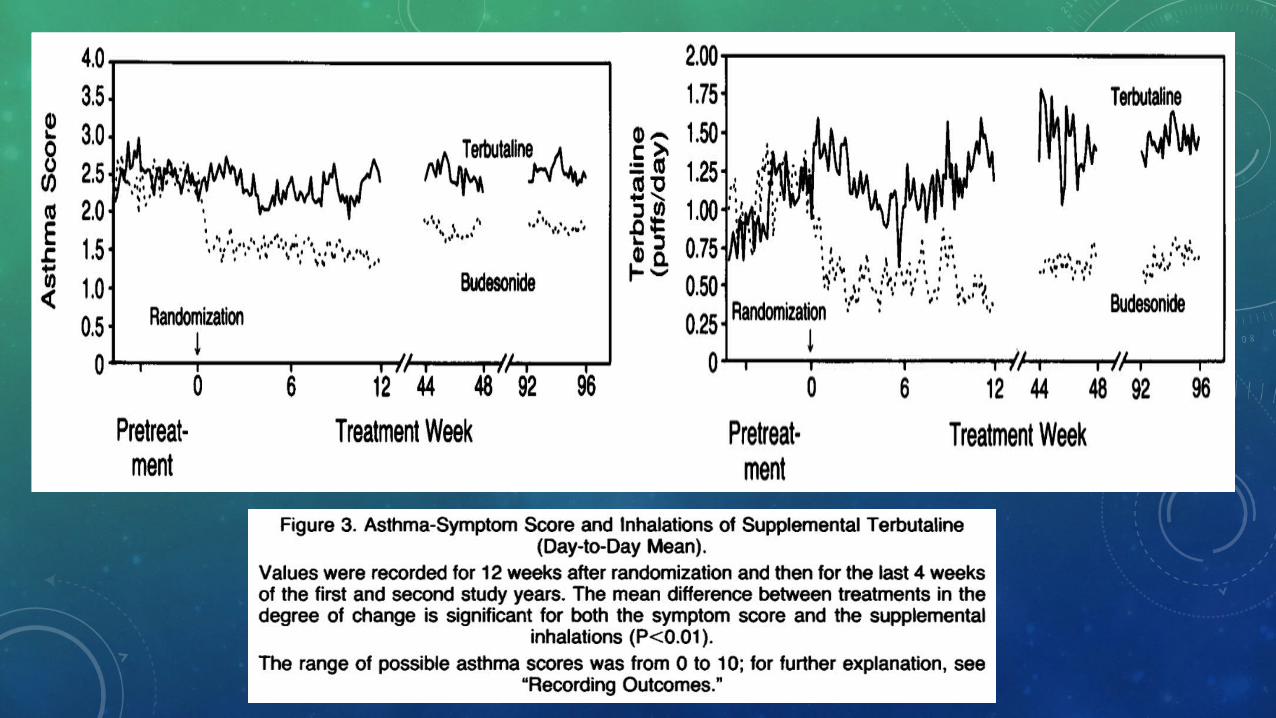
Other variables
• PEF values
• Symptoms of asthma
• Use of supplemental terbutaline
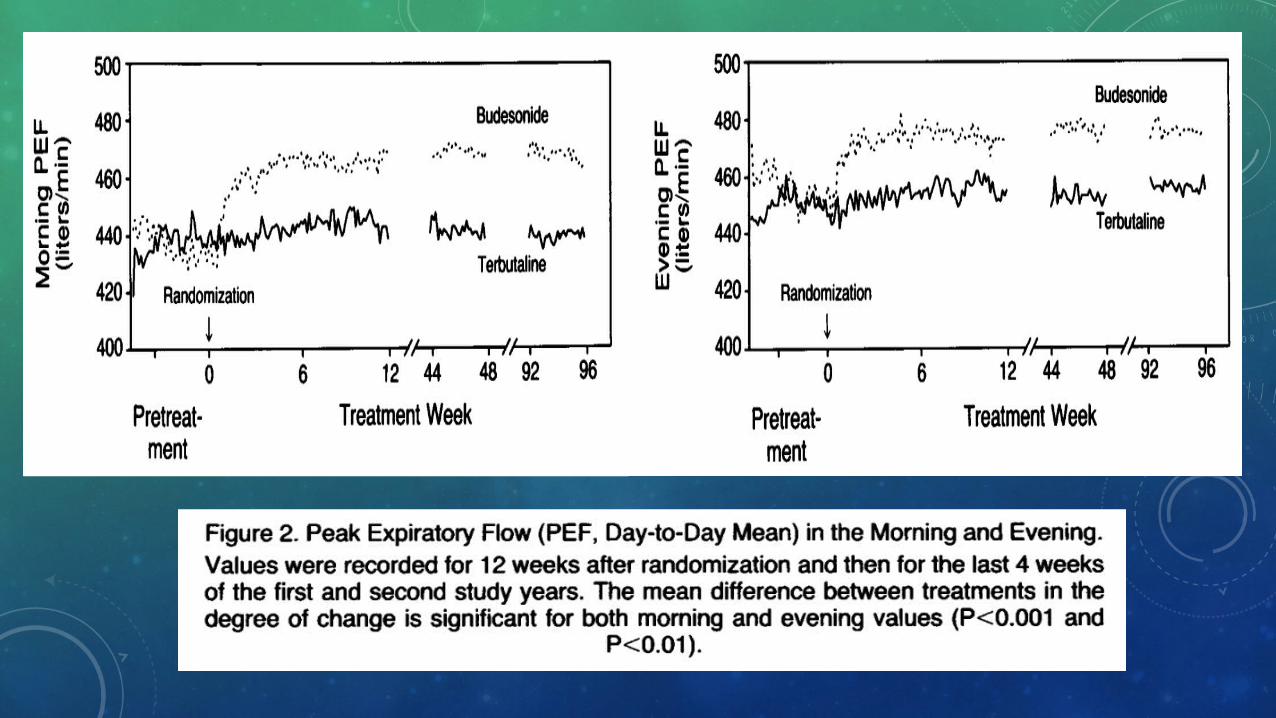
• The average increase over the pretreatment value in PEF in the morning was 32.8 liters per minute for budesonide and 4.8 liters per minute for terbutaline.
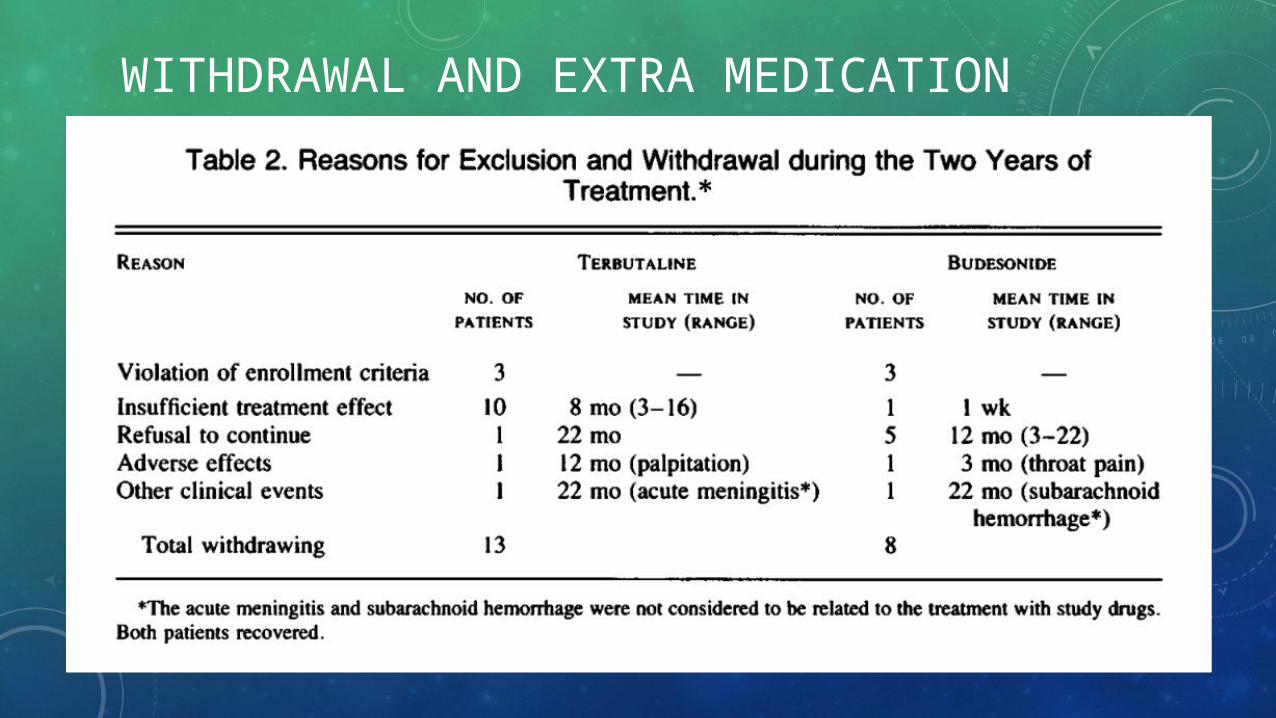
WITHDRAWAL AND EXTRA MEDICATION
CONCLUSION
• Antiinflammatory therapy with inhaled budesonide is an effective first-line treatment for patients with newly detected, mild asthma, and it is superior to the use of terbutaline in such patients.