PowerPoint Presentation 5 Tissue Damage (Infection) Pro-Inflammatory Cytokine release e.g. TNF-α...
11
4/10/2015 1 Joseph Clement, MS, RN, CCNS Clinical Nurse Specialist San Francisco General Hospital and Trauma Center Evidence-Based Care for Sepsis: What’s new in 2015 A case • 77 year old M admitted 5 wks prior for CVA. – PMH: HTN, DM, CAD – Non-verbal, PEG, Foley – Unstageable sacral PU • Baseline VS: T: 37.4 HR: 85 RR: 20 BP: 115/65 SpO2 99 on RA • Awaiting SNF Thursday • Morning Report – WBC 13.5 • 8 am: T: 37 HR: 88 RR: 38 BP: 100/54 SpO2 97 on RA – CXR ordered • 12 pm: T: 37.7 HR: 90 RR: 20 BP: 130/65 SpO2 98 on RA
Transcript of PowerPoint Presentation 5 Tissue Damage (Infection) Pro-Inflammatory Cytokine release e.g. TNF-α...
4/10/2015
1
Joseph Clement, MS, RN, CCNSClinical Nurse Specialist
San Francisco General Hospital and Trauma Center
Evidence-Based Care for Sepsis: What’s new in 2015
A case• 77 year old M admitted 5
wks prior for CVA.
– PMH: HTN, DM, CAD
– Non-verbal, PEG, Foley
– Unstageable sacral PU
• Baseline VS:
T: 37.4 HR: 85 RR: 20 BP: 115/65 SpO2 99 on RA
• Awaiting SNF
Thursday
• Morning Report
– WBC 13.5
• 8 am: T: 37 HR: 88 RR: 38 BP: 100/54 SpO2 97 on RA
– CXR ordered
• 12 pm: T: 37.7 HR: 90 RR: 20 BP: 130/65 SpO2 98 on RA
4/10/2015
2
Thursday cont.
• 4 pm: T: 37.4 HR: 91 RR: 26 BP: 124/61 96% RA
• 8 pm: T: 37.1 HR: 93 RR: 24 BP: 126/63 94% RA
• 12 am: T: 38.8 HR: 96 RR: 28 BP: 128/62 95% RA
– Cultures Drawn
• 4 am (Fri): T: 37 HR: 94 RR: 40 BP: 102/61 96% 4L
– Lacate drawn 5am -> 2.5 mmol/L
Friday• 8:30 am T:38.6 HR:92 RR:45 BP:106/57 96% 2L
– Rapid Response Team Activated, To ICU
• 10 am: T:38.6 HR:92 RR:45 BP:78/45 100% FiO2 1.0– Intubated, Central and Arterial lines placed
– On Phenylephrine, norepinephrine
– Ertapenem and Vancomycin started
– 1 L bolus started over 1 hour
• 12 – 2pm: 2 additional L infused
– BP Stablized on pressors
• 5pm: PEA arrest. Expired
SS Campaign, INLP
4/10/2015
3
Objectives
• Review Sepsis 101
• Explain Early Goal Directed Therapy – the good and the bad
• New Research in 2014-2015
• New Standards of Care
Why is Sepsis Important?• Incidence is rising
– 2000: 11.6 per 10k hospitalization rate
– 2008: 24 per 10k hospitalization rate
• Tenth leading cause of death in US per CDC
• Mortality rate with severe sepsis: 25-35%
• Rapid identification and treatment can decrease mortality
4/10/2015
4
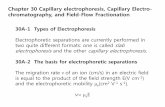
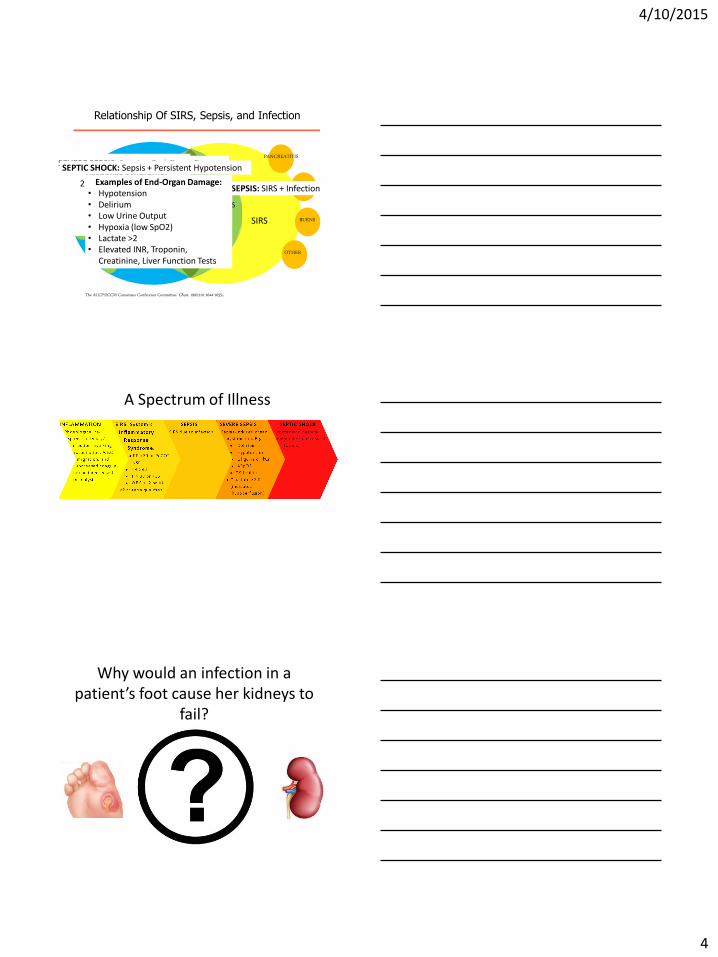
Relationship Of SIRS, Sepsis, and Infection
The ACCP/SCCM Consensus Conference Committee. Chest. 1992;101:1644-1655.
Bacterial
SIRS
PANCREATITIS
TRAUMA
BURNS
OTHER
Fungal
Parasitic
Viral
Other
INFECTION
SEVERE
SEPSIS SEPSISSEPSIS
SEPTICSHOCK
SIRS: Systemic Inflammatory Response Syndrome:
2 or more of:• HR > 90• RR > 20• WBC >12 or <4• Temp >38 or <36
SEPSIS: SIRS + Infection
SEVERE SEPSIS: Sepsis + End-Organ DamageSEPTIC SHOCK: Sepsis + Persistent Hypotension
Examples of End-Organ Damage:• Hypotension• Delirium• Low Urine Output• Hypoxia (low SpO2)• Lactate >2• Elevated INR, Troponin,
Creatinine, Liver Function Tests
A Spectrum of Illness
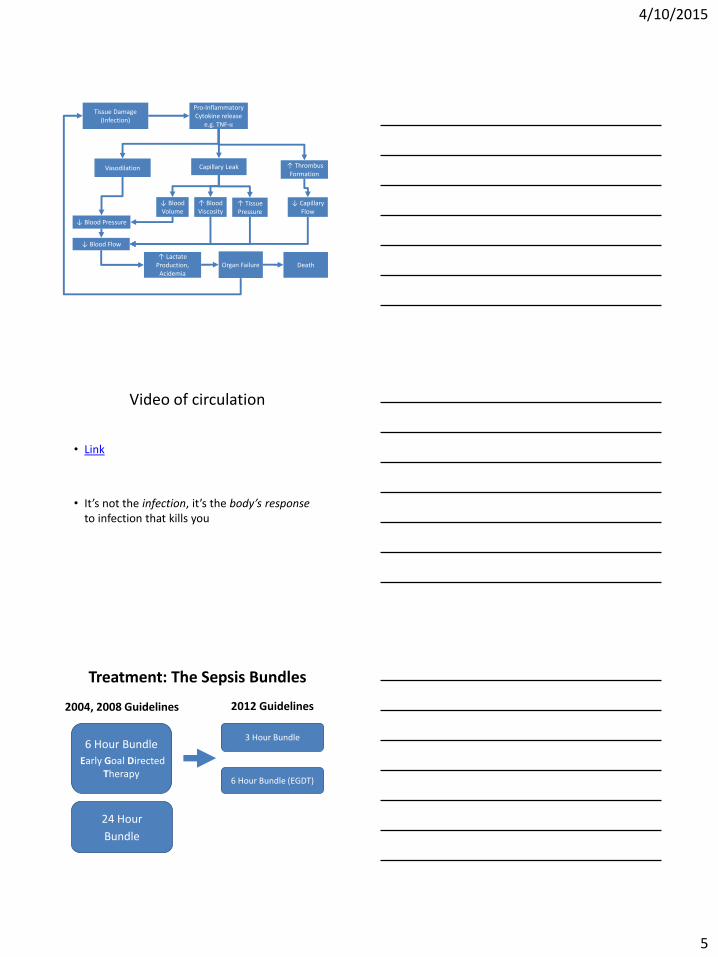
Why would an infection in a patient’s foot cause her kidneys to
fail?
4/10/2015
5
Tissue Damage(Infection)
Pro-Inflammatory Cytokine release
e.g. TNF-α
Vasodilation Capillary Leak ↑ Thrombus Formation
↓ Blood Pressure
↓ Blood Volume
↑ Blood Viscosity
↑ Tissue Pressure
↓ Capillary Flow
↑ Lactate Production,
AcidemiaOrgan Failure Death
↓ Blood Flow
Video of circulation
• Link
• It’s not the infection, it’s the body’s responseto infection that kills you
Treatment: The Sepsis Bundles
6 Hour Bundle
Early Goal Directed Therapy
6 Hour Bundle (EGDT)
3 Hour Bundle
24 Hour
Bundle
2004, 2008 Guidelines 2012 Guidelines
4/10/2015
6
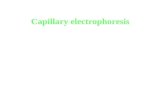
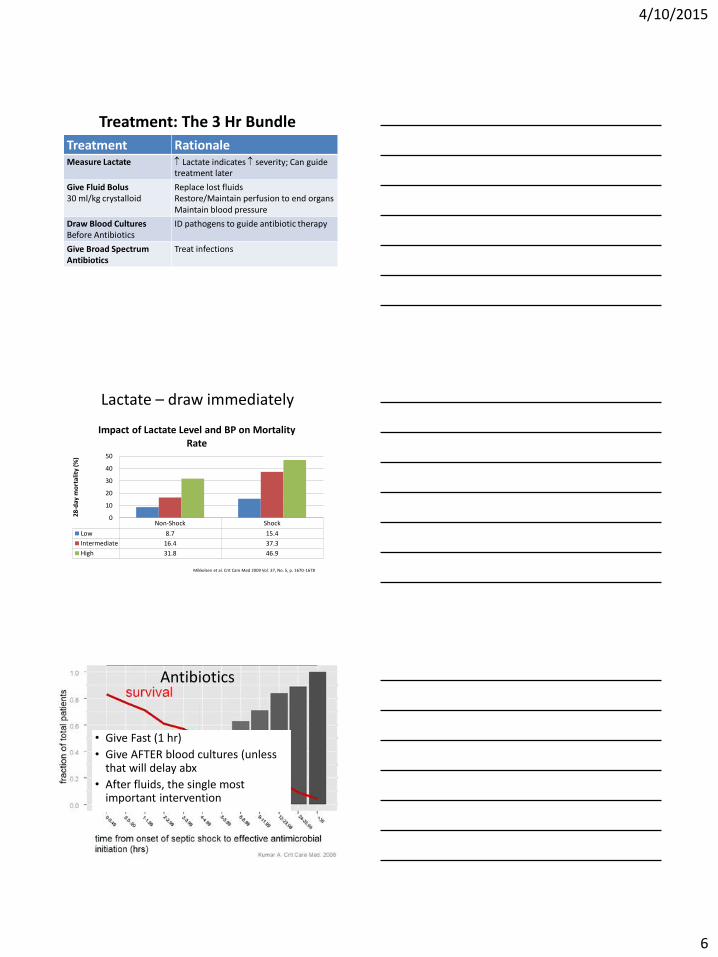
Treatment: The 3 Hr Bundle
Treatment RationaleMeasure Lactate Lactate indicates severity; Can guide
treatment later
Give Fluid Bolus30 ml/kg crystalloid
Replace lost fluidsRestore/Maintain perfusion to end organsMaintain blood pressure
Draw Blood CulturesBefore Antibiotics
ID pathogens to guide antibiotic therapy
Give Broad SpectrumAntibiotics
Treat infections
Non-Shock Shock
Low 8.7 15.4
Intermediate 16.4 37.3
High 31.8 46.9
0
10
20
30
40
50
28-d
ay m
ort
alit
y (%
)
Impact of Lactate Level and BP on Mortality Rate
Lactate – draw immediately
Mikkelsen et al. Crit Care Med 2009 Vol. 37, No. 5, p. 1670-1678
• Give Fast (1 hr)
• Give AFTER blood cultures (unless that will delay abx
• After fluids, the single most important intervention
Antibiotics
4/10/2015
7
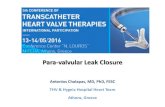
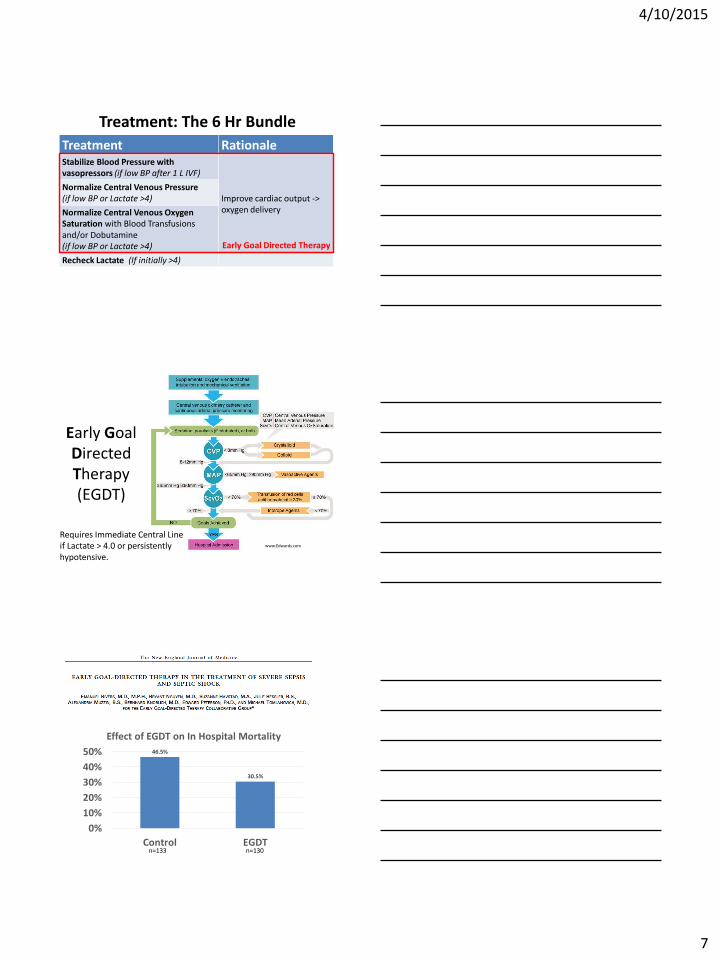
Treatment: The 6 Hr Bundle
Treatment RationaleStabilize Blood Pressure with vasopressors (if low BP after 1 L IVF)
Improve cardiac output -> oxygen delivery
Normalize Central Venous Pressure (if low BP or Lactate >4)
Normalize Central Venous Oxygen Saturation with Blood Transfusions and/or Dobutamine(if low BP or Lactate >4)
Recheck Lactate (If initially >4)
Early Goal Directed Therapy
Early Goal Directed Therapy (EGDT)
www.Edwards.com
Requires Immediate Central Line if Lactate > 4.0 or persistently hypotensive.
46.5%
30.5%
0%
10%
20%
30%
40%
50%
Control EGDT
Effect of EGDT on In Hospital Mortality
n=133 n=130
4/10/2015
8
Controversies with EGDT and Early SSC Guidelines
• Mortality Rate higher than other trials/centers
• Single Center Trial, Single Investigator
• Bundled approach – what was the cause of benefit
• Influence of industry
• Later research questioning individual elements of bundle
• Multi-center/International
• Randomized Controlled Trials
• Testing EGDT against usual care
4/10/2015
9
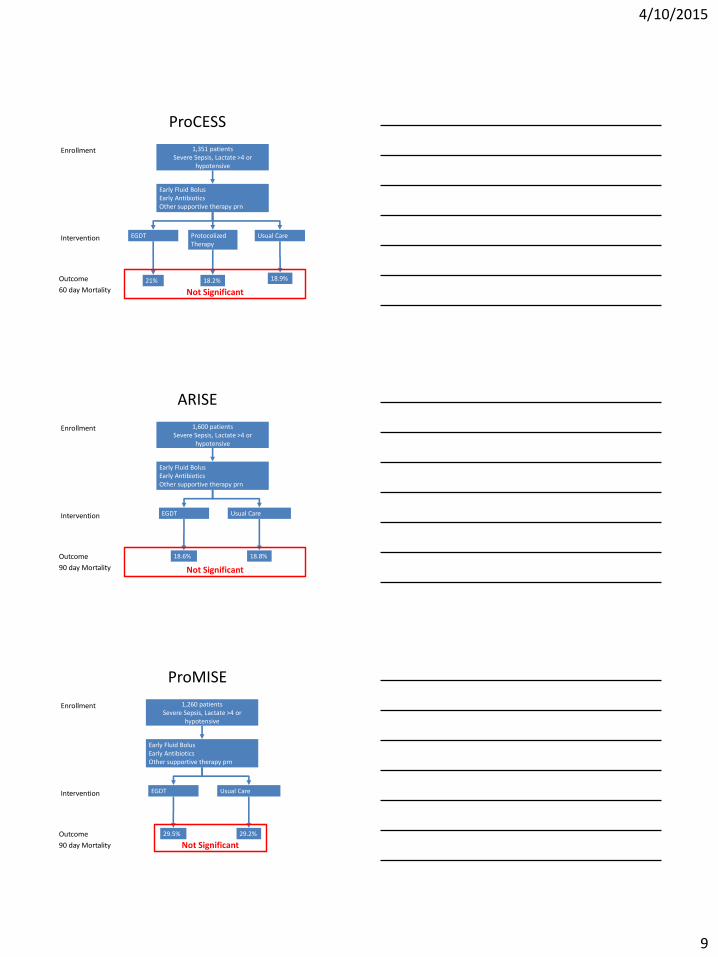
ProCESS
1,351 patientsSevere Sepsis, Lactate >4 or
hypotensive
EGDT ProtocolizedTherapy
Usual Care
Early Fluid BolusEarly AntibioticsOther supportive therapy prn
21% 18.2% 18.9%Outcome
60 day Mortality
Intervention
Enrollment
Not Significant
ARISE
1,600 patientsSevere Sepsis, Lactate >4 or
hypotensive
EGDT Usual Care
Early Fluid BolusEarly AntibioticsOther supportive therapy prn
18.6% 18.8%Outcome
90 day Mortality
Intervention
Enrollment
Not Significant
ProMISE
1,260 patientsSevere Sepsis, Lactate >4 or
hypotensive
EGDT Usual Care
Early Fluid BolusEarly AntibioticsOther supportive therapy prn
29.5% 29.2%Outcome
90 day Mortality
Intervention
Enrollment
Not Significant
4/10/2015
10
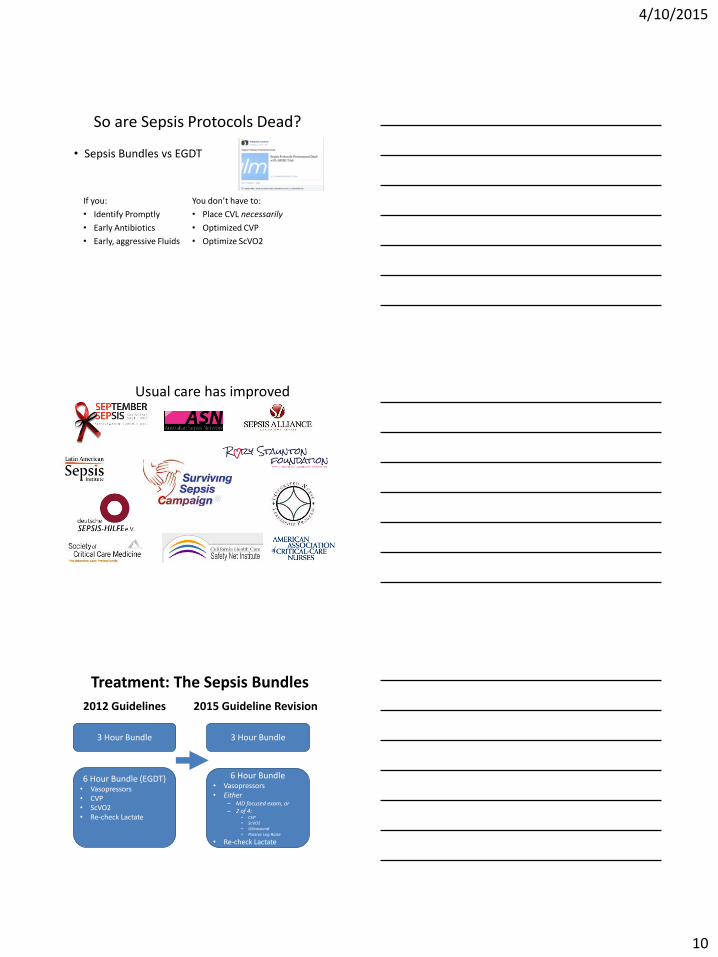
So are Sepsis Protocols Dead?
• Sepsis Bundles vs EGDT
If you:
• Identify Promptly
• Early Antibiotics
• Early, aggressive Fluids
You don’t have to:
• Place CVL necessarily
• Optimized CVP
• Optimize ScVO2
SS Campaign, INLPUsual care has improved
Treatment: The Sepsis Bundles
6 Hour Bundle (EGDT)• Vasopressors• CVP• ScVO2• Re-check Lactate
3 Hour Bundle
2015 Guideline Revision2012 Guidelines
3 Hour Bundle
6 Hour Bundle• Vasopressors• Either
– MD focused exam, or– 2 of 4:
• CVP• ScVO2• Ultrasound• Passive Leg Raise
• Re-check Lactate
4/10/2015
11
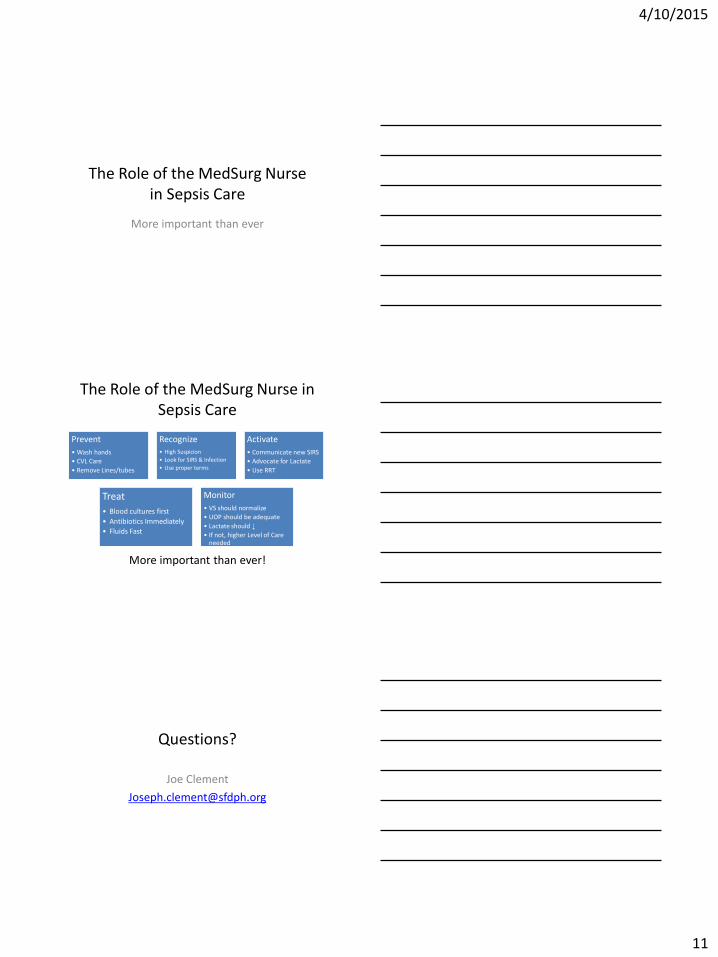
The Role of the MedSurg Nurse in Sepsis Care
More important than ever
The Role of the MedSurg Nurse in Sepsis Care
Prevent
• Wash hands
• CVL Care
• Remove Lines/tubes
Recognize• High Suspicion
• Look for SIRS & Infection
• Use proper terms
Activate
• Communicate new SIRS
• Advocate for Lactate
• Use RRT
Treat
• Blood cultures first
• Antibiotics Immediately
• Fluids Fast
Monitor
• VS should normalize
• UOP should be adequate
• Lactate should ↓
• If not, higher Level of Care needed
More important than ever!
Questions?
Joe Clement