Pathoremeds 3 Guide Answers
28
THALASSEMIA Mendelian disorder characterized by a lack of or decreased synthesis of either α or β globin chain of HbA HEREDITARY SPHEROCYTOSIS Intrinsic defect in red cell membrane ankyrin deficiency and other skeletal membrane components Ankyrin deficiency associated with reduced stability and loss of membrane fragments as cells traverse circulation Moderate splenomegaly Clinical Course: Treatment is splenectomy G6PD DEFICIENCY X-linked Impaired or deficient enzyme function which reduce ability of red cells iMMUNOHEMOLYTIC ANEMIA Demonstration of the anti- red cell Antibodies The antibody is of the IgG type, does not usually fix complement and is active at 37 o C Primary (Idiopathic) Secondary The antibodies are IgM and are most active in vitro at 0 o C to 4 o C; Antibodies dissociate at 30 o or above; SICKLE CELL ANEMIA Structurally abnormal hemoglobin Substitution of valine for glutamic acid at the 6 th position of β globin chain Microangiopathic Hemolytic Anemia - abnormally narrowed vessels
-
Upload
stephen-eleserio -
Category
Documents
-
view
233 -
download
0
Transcript of Pathoremeds 3 Guide Answers

THALASSEMIA
Mendelian disorder characterized by a lack
of or decreased synthesis of either α or β
globin chain of HbA
HEREDITARY SPHEROCYTOSIS
Intrinsic defect in red cell membrane
ankyrin deficiency and other skeletal
membrane components
Ankyrin deficiency associated with
reduced stability and loss of membrane
fragments as cells traverse circulation
Moderate splenomegaly
Clinical Course: Treatment is splenectomy
G6PD DEFICIENCY
X-linked
Impaired or deficient enzyme function
which reduce ability of red cells
iMMUNOHEMOLYTIC ANEMIA
Demonstration of the anti-red cell
Antibodies
The antibody is of the IgG type, does
not usually fix complement and is
active at 37 o C
Primary (Idiopathic)
Secondary
The antibodies are IgM and are most
active in vitro at 0 o C to 4 o C; Antibodies
dissociate at 30 o or above;
SICKLE CELL ANEMIA
Structurally abnormal hemoglobin
Substitution of valine for glutamic acid at
the 6 th position of β globin chain
Microangiopathic Hemolytic Anemia -
abnormally narrowed vessels
In DIC, Malignant HPN, SLE, TTP,
Hemolytic-uremic syndrome,
disseminated cancer
See schistocytes, burr, helmet cells,
and triangle cells
IRON DEFICIENCY ANEMIA
Most common nutritional deficiency
Storage pool of Iron: Hemosiderin and
Ferritin
PERNICIOUS ANEMIA
Autoimmune destruction of gastric mucosa
Chronic atrophic gastritis lack of
intrinsic factor
Achlorydia even after histamine
stimulation
Inability to absorb oral dose of

cobalamine – “Schilling
FOLATE DEFICIENCY
Same as B12 deficiency but without
neurologic changes
APLASTIC ANEMIA
Pancytopenia characterized by anemia,
neutropenia and thrombocytopenia
HEMOPHILIA A
X-linked recessive trait; in male and
homozygous female
Reduction in amount or activity of Factor
VIII
VON WILLEBRANDS DISEASE
Autosomal dominant
Characterized by spontaneous bleeding
from mucous membranes; excessive
bleeding from wounds, menorrhagia
Prolonged BT, PTT, normal platelet count,
reduced vWF and Factor VIII levels
May have quantitative or qualitative effects
in vWF
DISSEMINATED INTRAVASCULAR
COAGULATION (DIC)
Acute, subacute, and chronic
thrombohemorrhagic disorder occurring as
a secondary complication in a variety of
disease
Characterized by activation of the
coagulation sequence that leads to
formation of microthrombi throughout the
microcirculation
“Consumptive Coagulopathy”
B.
PERIPHERAL B CELL NEOPLASMS
A. Chronic lymphocytic leukemia/Small
lymphocytic lymphoma
Features:
CLL and SLL are morphologically,
phenotypically and genotypically
indistinguishable; CLL if
>4,000/mm3 blood lymphocytosis
CLL and SLL less common in Asian
countries compared to Western
countries
Tumor composed of lymphocytes
that express CD19, CD20 and CD5
Lymph node effaced by diffuse
proliferation of small lymphocytes
with proliferation centers

Bone marrow involved in 100% of
cases of CLL and in most cases of
SLL
Clinically:
Median age, 60; male > female
Patients are often
asymptomatic or with non-
specific symptoms
Generalized lymphadenopathy
in 50-60% of cases
WBC count slightly increased or
exceed 200,000/mm3
Hypogammaglobulinemia and
AIHA in some patients
Most indolent type of leukemia,
median survival 4-6 years
CLL and SLL may progress to
prolymphocytic transformation
vs Diffuse Large B cell Lymphoma
Features:
20% of NHL, 60-70% of aggressive
lymphoid neoplasms
Median age: 60 years, but wide age
range
5% of childhood lymphoma
Composed of a diffuse proliferation
of large cells 4-5x small
lymphocytes with vesicular nuclei,
prominent nucleoli (centroblastic
or immunoblastic)
Special subtypes:
Immunodeficiency associated
large B cell lymphoma seen in
severe T cell
immunodeficiencies (e.g. end
stage HIV infection), neoplastic
B cells are often latently
infected with EBV
Body cavity large B cell
lymphoma – arise in malignant
pleural or ascitic effusions,
mostly in advanced HIV
infection; tumor cells are
infected with herpes virus 8
Clinically:
Rapidly enlarging node
Extranodal involvement,
common: GIT, skin, bone,
brain, Waldeyer’s ring
Bone marrow involvement

occurs late in the disease
Aggressive tumors that are
rapidly fatal if untreated
With treatment, remission in up
to 80%; cure in 50%
2. PRECURSOR B CELL AND T CELL
NEOPLASMS
Acute lymphoblastic leukemia/lymphoma
Features:
Composed of immature, pre-B and
pre-T cells (lymphoblasts)
85% of ALL are pre-B cell, presents
typically as acute leukemia
15% of ALL are pre-T cell, present
in adolescent males as lymphomas
often with thymic involvement
Most cases occur before age 15,
peak incidence 4 years, male >
female
Must differentiate from AML since
similar signs and symptoms but
different response to chemotherapy
Positive TDT in 95% of cases
90% with numerical and structural
changes in the chromosomes, > 75%
hyperdiploidy
Clinically:
Signs and symptoms related to bone
marrow depression:
Fatigue, pallor – anemia
Fever – infections
Bleeding – thrombocytopenia
Bone pain and tenderness –
marrow expansion and
infiltration of subperiosteum
Neurologic symptoms
(headache, vomiting) –
meningeal spread
Hepatomegaly/splenomegaly –
leukemic infiltrates
90% complete remission, with
chemotherapy; 2/3 cured
Poor prognostic factors (require bone
marrow transplantation)
Less than 2 years of age
Presentation in adolescence or
adulthood
5 jcc
© Spidey Transcriptions
Peripheral blasts greater than

100,000/mm3
Presence of Philadelphia
chromosome t(9;22)
vs Acute Myelogenous Leukemia (AML) –
accumulation of immature myeloid
cells in the bone marrow
affects primarily adults, age 15-39 years
Constiture 20% of childhood leukemias
Revised FAB classification
3. Chronic Myelogenous Leukemia
A disease of adults 25-60 years
90% of cases, karyotype reveals the
Philadelphia chromosome t(9;22)
Morphology:
Peripheral blood: WBC count
generally > 100,000/mm 3 showing
the entire spectrum of myeloid
series; increase include eosinophils,
basophils and platelets;
predominance of neutrophils,
metamyelocytes and myelocytes
Bone marrow: 100% cellular, mostly
maturing granulocytes
LAP: 0 or markedly decreased < 10
(N=13-130); in leukemoid reaction or
other MPDs, LAP is elevated
Chromosome analysis: Philadelphia
chromosome t(9;22) resulting in a
fusion gene tyrosine kinase (BCR-ABL)
Clinically:
Insidious onset, anemia, weakness,
fatigue
Massive splenomegaly (may be the
initial finding)
Poor response to treatment; MS 3
years; 50% go into the accelerated
phase terminating in blastic crisis
(acute leukemia like)
50% go directly to blastic crisis (70%
AML; 30% ALL)
Treatment:
Targeted therapy: tyrosine kinase
inhibitor (Imatinid mesilate) and
newer kinase inhibitors, bone
marrow transplantation, interferon
α
vs Primary Myelofibrosis
A neoplastic transformation of a
multipotent stem cell characterized by
early progression to marrow fibrosis

Fibrosis due to fibrogenic factors
secreted by neoplastic megakaryocytes
Morphology:
Peripheral blood: anemia,
leukoerythroblastic reaction, tear
drop erythrocytes
Bone marrow:
Early: tri-lineage
hypercellularity, minimal
fibrosis
Late: hypocellular with diffuse
fibrosis and clusters of atypical
megakaryocytes
Spleen: extramedullary
haematopoiesis (splenomegaly)
Clinically:
Patients 60 years and above
Present with anemia and massive
splenomegaly
MS: 1-5 years
5-20% transform to AML
4. Hodgkin’s Lymphoma (neoplasm of
Reed Sternberg cells and variants)
HODGKIN’S LYMPHOMA
Originate almost always from a single node
or chain of nodes and spreads to contiguous
nodes
Presence of Reed-Sternberg cells admixed
with a variable inflammatory infiltrate
Associated with systemic manifestations
Neoplastic Reed Sternberg cells are derived
from germinal center or post germinal
center B cells, rarely (1-2%), from
transformed T cells
Classification:
Classic Hodgkin’s Lymphoma (similar
immunphenotype): CD 15 (+), CD 30 (+)
Nodular sclerosis
Mixed cellularity
Lymphocyte rich
Lymphocyte depleted
Lymphocyte predominance – B cell
immunophenotype distinct from the
classic subtypes (arise from germinal
center B-cells) – CD 20 (+), CD 15 (+),
CD 30 (-)
Reed Sternberg cell
Common denominator to all
Neoplastic element of Hodgkin’s Lymphoma
Classic Reed Sternberg cell,

binucleate/bilobed → mirror image with
prominent “owl-eye” nucleoli surrounded
by a clear halo abundant, amphophilic
cytoplasm
Variants: mononuclear, lacunar, L and H
pleomorphic
Must be present to diagnose Hodgkin’s
Lymphoma
nn Arbor staging system for Hodgkin’s disease
Stage 1
Involvement of a single node region or
a single extralymphatic organ or site
Stage 2
Involvement of two or more lymph
node regions on the same side of the
diaphragm or localized involvement of
an extralymphatic organ or site and one
or more lymph node regions on the
same side of the diaphragm
10 jcc
© Spidey Transcriptions
Stage 3
Involvement of lymph node regions on
both sides of the diaphragm which may
also be accompanied by localized
involvement of the spleen or both
Stage 4
Diffuse or disseminated involvement of
one or more extralymphatic organs or
tissues with or without associated
lymph node enlargement
The reason for classifying the patient as
stage 4 should be identified further by
defining the site with symbols (e.g. H+
M+: liver and bone marrow involved)
5.Myelodysplastic Syndrome (MDS) –
associated with ineffective
hematopoeisis and associated
cytopenias
Chronic Myeloproliferative Disorders
(MPD) - associated with increased
production of terminally differentiated
myeloid cells

CML
Polycythemia vera
Essential thrombocytosis
Primary Myelofibrosis
MYELODYSPLASTIC SYNDROMES (MDS)
A clonal stem cell disorder characterized by
maturation defects resulting in ineffective
and disordered haematopoiesis and
increased transformation to AML
2 types:
Idiopathic or primary MDS – affects
patients over 60 years of age and
develops insidiously; MS: 9-29 months
Therapy related MDS (TMDS) – a
complication of previous
myelosuppressive drug or radiation,
about 2-8 years after exposure; poorer
prognosis; MS 4-8 months
Morphology:
Peripheral blood: pancytopenia
Bone marrow: hypercellular,
monocellular or hypocellular with
disordered (dysplastic) differentiation
of 3 lineages (erythroid, myeloid and
megakaryocytic)
< 20% blasts in the bone marrow
Clinically:
Primary MDS affects elderly patient’s
older than 60 years
Weakness, infection haemorrhage
(acute leukemia-like) due to
pancytopenia
50% are asymptomatic and discovered
after accidental blood tests
10-40% of patients progress to AML,
particularly with TMDS
vs CHRONIC MYELOPROLIFERATIVE
DISORDERS (MPDS)
A clonal neoplastic proliferation of
multipotent progenitor cell capable of
giving rise to mature erythrocytes,
platelets, granulocytes and monocytes
except CML in which the pluripotent stem
cell that give rise to lymphoid and myeloid
cells is affected
Common pathogenetic factors: mutated
and activated typosine kinases
Includes:
CML
Polycythemia vera

Essential thrombocytosis
Primary myelofibrosis
Rare: systemic mastocytosis, chronic
eosinophilic leukemia, stem cell
leukemia
Common features:
Neoplastic stem cells have the capacity
to circulate and home to secondary
hematopoietic organs particularly the
spleen giving rise to extramedullary
haematopoiesis therefore varying
degrees of splenomegaly
Frequent occurrence of myelofibrosis
and pancytopenia
Similar clinical and pathologic
manifestation at some stage (overlaps
and transitional forms between types)
All can progress to acute leukemia,
most frequent with CML
Diagnosis is based on correlation
between morphologic findings clinical
and laboratory findings and cytogenetic
studies
c. BRIEFLY DISCUSS THE DISTINCTIVE HISTLOGIC AND CLINICAL BEHAVIORS OF DIFERENT TYPES OF HODKIN DISEASE
D.
IDENTIFY THE FORMULA THAT WILL GIVE YOU THE FOLLOWING
Hemoglobin
RBC ( millions ) x 3 = Hb
Rbc count
RBC ( millions ) x 3 = Hb
RBC ( millions ) x 9 = Hct
Platelet count
10 OIF x 2000 =
platelet count
hematocrit

RBC ( millions ) x 9 = Hct
Mcv
MCV = HCT/RBC count
E. WHAT IS THE NORMAL REFERENCE VALUES FOR THE FOLLOWING
WBC
5-10 x 10 9 /L
PLATELET
150 – 450 x 10 9 /L
RBC
Normal Values:
4.5 – 6.0 x 10 12 / L for men
4.0 – 5.5 x 10 12 / L for women
HEMOGLOBIN
Normal Values:
14 – 18 gm / 100 ml for men
12 – 16 gm / 100 ml for women
*100mL = 1Dl
HEMATOCRIT
Normal Values:
40 – 54 % for men
37 – 47 % for women
F. DEFINE THE FOLLOWING AND IN WHAT CONDITION THEY ARE SEEN
RETICULOCYTE COUNT
Stage after the noromoblast ; nucleus is extruded
with cytoplasmic microsomes or ribosomes which
remain for 1-2 days (appreciated in methylene or
cresyl blue stain)
These cells are anucleated but still contatin
nuclear remnants. On regular stains, you will not
see them hence, you need a special stain.
Large RBC with dark blue dots or thin short
irregular linear structures → Polychromatophilic
(bluish pink), megaloblastic
Measures index of production of mature RBC by
bone marrow (how the bone marrow responds to
changes in blood conditions)
shows polychromatophilia (blue gray hue) on
Wright stain
Normal Values:
0.5 - 1.5 % (anything above 1.5% is increased)
Requested in patients suspected of having
hemolytic anemia or when you suspect an
increase in Rct count.
Most Common Causes of Reticulocytosis
Hemolytic anemia, chronic or acute
Acute bleeding

After treatment of vitamin B 12 / folate / iron
Deficiency
Anisochromia
When there is variety in color – normochromic,
hypochromic, hyperchromic.
This can happen in patients with anemia, or being
treated, or reticulocytosis.
Acanthocytes
Appear similar to crenated erythrocytes.
However, the projections in acanthocytes are
irregularly space. At the apex of the projections
are SHARP POINTS, as contrasted to the smooth
or blunt apices of the crenated RBCs.
Patients with acanthocytes frequently exhibit
metabolic dysfunction.
o This dysfunction is usually associated with
decreased levels of β – lipoproteins (β –
lipoproteinemia) which is a highly
important lipid transporting protein.
Patients with this dysfunction do not
absorb lipid in the small intestines.
Consequently, the feces contain an excess
amount of fat, whereas the plasma and
subsequent cellular levels of lipid are
markedly decreased.
o It is speculated that because an
appreciable constituent of the
corpuscular membrane is lipid in nature,
the decreased lipid levels may account for
the erythrocyte assuming such
configuration.
Howell-Jolly Bodies
remnants of DNA and usually occur singly and on
the periphery of the corpuscle.
Seen in hemolytic anemia, post-splenectomy,
megaloblastic anemia
They are SINGLE INCLUSIONS!
Do NOT mistaken them for platelets because they
can stack on top of your RBCs.
Pappenheimer bodies
These are remnants of iron.
You also need a special stain to see this.
This image was taken from the 1997 Cytohematology Proficiency
Test Event - Slide 005. On Wright stained smears, Pappenheimer
bodies appear as violet staining granules usually found along the
periphery of the red cells, often in clusters. They must be confirmed

with an iron stain. These iron-staining granules are found in sideroblastic and megaloblastic anemias, alcoholism, post-
splenectomy, and in some hemoglobinopathies.
Rouleaux Formation
When you see abnormal stacking of RBC like a
pile of coins.
This can be seen in abnormal protein states like
hypergammaglobulinemia (↑protein in blood)
Seen in multiple myeloma (MM).
o Neoplasm of the plasma cell, but is a
monoclonal type – you produce only one
type: either κ or λ (kappa or lambda).
o It is a malignancy, and these plasma cells
synthesize protein, hence
hypergammaglobulinema → rouleaux.
G. WEN DO YOU REQUEST FOR THE FOLLOWING TESTS? GIVE AT LEAST 2 INDICATIONS
RETICULOCYTE COUNT
Stage after the noromoblast ; nucleus is extruded
with cytoplasmic microsomes or ribosomes which
remain for 1-2 days (appreciated in methylene or
cresyl blue stain)
These cells are anucleated but still contatin
nuclear remnants. On regular stains, you will not
see them hence, you need a special stain.
Large RBC with dark blue dots or thin short
irregular linear structures → Polychromatophilic
(bluish pink), megaloblastic
Measures index of production of mature RBC by
bone marrow (how the bone marrow responds to
changes in blood conditions)
shows polychromatophilia (blue gray hue) on
Wright stain
Normal Values:
0.5 - 1.5 % (anything above 1.5% is increased)
equested in patients suspected of having
hemolytic anemia or when you suspect an
increase in Rct count.
Most Common Causes of Reticulocytosis
Hemolytic anemia, chronic or acute
Acute bleeding
After treatment of vitamin B 12 / folate / iron
Deficiency
BONE MARROW ASPIRATION BIOPSY
To confirm diagnosis of megaloblastic anemia,

leukemia, multiply myeloma (MM)
Diagnosis of bone marrow hypoplasia, aplastic
anemia (a pancytopenia where the entire BM
becomes fatty)
To document deficiency in body iron stores -
reticuloendothelial system (i.e. in retractable
anemia)
To demonstrate metastatic / infectious disease
(i.e. myelophthisic anemias)
Usually done on the iliac crest
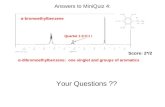
Hemoglobin electrophoresis
Hemoglobin Electrophoresis
- Used to detect abnormal hemoglobin
**examples: Hemoglobin S- sickle cell anemia
Hemoglobin H – thalassemia
Hemoglobin A – normal
Used to diagnose Hemoglobinopathy
- A definitive test
Principle:
H b molecules in alkaline solution have a net (-) charge and migrate toward the anode in an
electrophotometric system
**Hemoglobin = heme + globin
globin (protein) is comprised of amino acids having different migration rates and being amphoteric
which can be charged positively or negatively depending on the medium
o Commonly used mediums: cellulose acetate an alkaline medium and citrate agar an
acidic medium
Usage of cellulose acetate an alkaline medium will allow the amino acid to have a net
negative charge that will migrate towards anode
While usage of an acidic medium will let the amino acid have a net positive charge
and migrate toward the cathode
Procedure:
1. Patient’s hemosylate is placed in a cellulose acetate membrane and immersed on buffered solution.
** A hemosylate is prepared from the patient’s blood sample and placed on the cathode side of the
acetate strip because they have a net negative charge in an alkaline solution so that will migrate
toward the positive side.
2. Electric current is applied and allows Hb to migrate different speeds (slow, intermediate, or fast)
Eg. A2 (slowest) < C < S < F < A (fastest)

**Since each of the different hemoglobin’s has distinctly different amino acid contents, and different
hemoglonins migrate along the acetate strip at different rates of speed for a specific pH.
**The speed at which the hemoglobin travels is directly dependent on the net charge (because of the
amino acid content)
**The different kinds of hemoglobin can be differentiated through the differences in the speed of
migration.
3. Upon separation, Hb’s is stained and quantitated.
4. Unknown identified by comparison with known Hb.
Pathology: Special Hematologic Examinations | 6
**By placing the acetate strip in a densitometer, one is able to quantify the different hemoglobin’s
present
**Cellulose Acetate Method is for screening
**Citrate agar method is for confirmation has an acidic medium
Indication:
- To detect and identify abnormal hemoglobin
H. WHAT TEST IS MOST USEFUL FOR EACH OF THE FOLLOWING
Hereditary spherocytosis- Osmotic fragility Test/Incubated Osmotic Fragility Test
Iron deficiency anemia-Bone marrow examination
Hemoglobin s- Hemoglobin Electrophoresis
Staging of lymphoid neoplasm- Bone marrow examination
aplastic anemia- Core Biopsy Bone marrow examination
paroxysmal nocturnal hemoglobinuria (PNH)-Acid serum (Ham’s) test
I. GIVE THE MAJOR IMPORTANT FACTORS REGULATING HEMOSTASIS
Primary Hemostasis
♠ Platelets bind via glycoprotein Ib (GpIb)
receptors to von Willebrand factor (vWF) on
exposed extracellular matrix (ECM)
♠ Platelets are activated, undergoing a shape
change and granule release.
♠ Released adenosine diphosphate (ADP) and
thromboxane A 2 (TxA 2 ) induce additional
platelet aggregation through platelet GpIIb-IIIa
receptor binding to fibrinogen, and form the
primary hemostatic plug.
C. Secondary Hemostasis
♠ Tissue factor (released due to endothelial
injury) and the phospholipid complex

(expressed at the surface of the platelets
stimulate the coagulation cascade
♠ End result fibrin polymerization, “cementing”
the platelets into a definitive secondary
hemostatic plug
J Vitamin K dependent (for the post-translational
carboxylation):
• Factor II, VII, IX, X
K
Intrinsic Pathway
Pathology : Blood Coagulation | 6
Initiated by the Hageman Factor. Factor
XIIXIIa, which uses HMWK (high molecular
weight kininogen) collagen as a cofactor
The end result of the activation of factor XII
is XIXia and prekallikrein kallikrein
Factor XIa subsequently activates factor IX
to XIa. At the same time there is activation of
factor VIII to VIIIa with the help of factor IIa
(thrombin)
common pathway
Triggered by damaged endothelial lining of
blood vessel when it comes in contact with
foreign antibodies
Evaluated by activated partial thromboplastin
time (aPTT) remember Brad PITT
Factors exclusively involved: XII, XI, IX, VIII
♦ Extrinsic Pathway
Secondary to endothelial injury
Tissue injury induces endothelial cells to
express tissue factor (III) thereby activating
factor VII to VIIa
Triggered by tissue thromboplastin (Factor III)
which is released by damaged endothelial and
body tissues
Evaluated by prothrombin time (PT)
remember PET
Factors exclusively involved: III and VII
L. Low fibrinogen levels may be due to the
presence of fibrinolysins or DIC
In DIC, the coagulation cascade and
platelets are activated so there is formation
of clot. At the same time, the body tries to
degrade the clots because there should be
no thrombus. So there are (+) fibrin
degradation products.
Disorder of Fibrinolysis: Disseminated
intravascular coagulation (DIC) – occurs when
there is a liberation of thromboplastin and other

unknown substances into the bloodstream which
results in the deposition of fibrin and fibrin
precursor substances like fibrinogen.
Disorders which can cause DIC
o Obstetric complications
o Infections
o Neoplasms
o Massive tissue injury
o Miscellaneous
♠ Patients with DIC will present with s/sx of
bleeding, acute renal failure, respiratory failure,
tissue hypoperfusion and infarction (because of
thrombosis)
♠ Laboratory
o Decreased platelet levels
(thrombocytopenia)
o High levels of fibrinogen
(hyperfibrinogenemia)
PT and aPTT abnormalities
o Elevated fibrin degradation products
(FDP
M.Thrombotic thrombocytopenic
purpura (TTP) isolated
consumption of platelets but no
consumption of coagulation factors.
• There is an inherent vascular
wall dysfunction resulting in
excessive deposition of platelet
aggregates in the renal and
cerebral vessels.
• Female>male
• Patient presents with:
(Remember FAT RN)
o Fever
Pathology : Blood Coagulation | 4
o Microangiopatic type of
hemolytic anemia
o Thrombocytopenia
o Renal abnormalities
o Neurological abnormalities
Vasculitis
Hemolytic-Uremic Syndrome also
results from consumption of platelets
(like TTP but less pronounced
neurologic symptoms and a more
pronounced renal symptoms)
• Patient presents with:
(Remember FRAT)
o Fever
o Renal abnormalities

o Anemia
o Thrombocytopenia
HELLP Syndrome (Hemolysis,
Elevated Liver enzymes, Low
Platelet count) commonly seen in
toxemia of pregnancy (e.g. pre-
eclampsia) or delivery. Patients
present with microangiopathic
hemolysis
Immune destruction of platelets
Idiopathic thrombocytopenic purpura
(ITP) an immunologic process
(type II): (+)antibodies against
platelet membrane antigens. ITP can
be of two types:
• Acute ITP more common in
children; sudden onset of
thrombocytopenia following an
infection commonly rubella,
chicken pox, toxoplasmosis or
CMV infection. It typically lasts up
to 6 weeks and follows a
spontaneous remission in 8% of
patients. The platelet count may
reach as low as 20,000/mm 3 .
The mechanism is secondary to
attachment of virus to platelet
membrane resulting in the
alteration of the membrane
proteins.
• Chronic ITP slow onset but
long duration. It can last for
months to years. The platelet
count doesn’t drop as severely as
the acute type. The treatment is
usually splenectomy because this
does not result to spontaneous
remission. (*spleen is removed
because the antibody production
cannot be corrected, so the
treatment is by decreasing
sequestration by the spleen
through splenectomy)
Post-transfusion purpura commonly
occurs after platelet transfusion.
Patients develop antiplatelet
antibodies. But this does not occur in
all patients who receive platelet
transfusion
Drug-induced Ab formation follows

the same principle as ITP. The drug
alters the membrane proteins of the
platelets. Drugs: quinolone and
heparin
COAGULATION FACTORS
Factor I (fibrinogen)
Factor II (prothrombin)
Factor V (labile factor)
Factor VII (stable factor)
Factor VIII (vWF complex)
Factor IX (plasma thromboplastin)
Factor X (Stuart)
Factor XI
Factor XII (Hageman)
Factor XIII (fibrin stabilizing factor)
High-Molecular Weight Kininogen (HMWK;
Fitzgerald factor)
Prekallikrein (Fletcher, PK)
COAGULATION FACTORS
o Factor I (fibrinogen) – synthesized in the liver
so it is decreased in liver damage/disease. It is
an acute phase reactant. It is the final major
step in the coagulation pathway
Acute Phase reactants are substances
which are elevated in immunologic process
but not involved in the reaction. They are
elevated in response to trauma or to onset
of variety of illnesses
o Factor II (prothrombin) is a proenzyme
synthesized also by the liver and is decreased
in liver disease. It becomes thrombin when
activated. It is Vitamin K-dependent. Deficiency
in prothrombin is extremely rare but if it occurs it
is an autosomal recessive trait
o Factor V (labile factor) is also synthesized by
the liver. It is found in plasma, but not serum. It
must be frozen to maintain activity
(labileunstable). Deficiency: Parahemophilia
(associated with bruising and soft tissue
hemorrhage)
o Factor VII (stable factor) is also synthesized
by the liver and Vitamin K dependent. It is found
in both serum and plasma. Deficiency in Factor
VII is inherited as an autosomal recessive trait.
Patients with presents with hemarthroses, large
hemorrhages (in joints, body cavity, intracranial
and intramuscular sites), and delayed post-
surgical bleeding.
o Factor VIII (vWF complex) has 2 subunits:

VIIIR (vWF) and VIIIC (antihemophilic factor)
VIIIC is synthesized by the liver and
deficiency is inherited as an X-linked trait.
The deficiency results to Hemophilia A
• Classic Hemophilia: most
common congenital
COAGULATION FACTOR
DEFICIENCY. Patients presents
with severe bleeding following even
minor trauma, hemarthroses
(bleeding in the joints), mouth, oral
cavity, GIT, intracranial
hemorrhages. Low VIIIC activity,
vWF are normal, normal PT and
bleeding time, aPTT is abnormal
VIIIR is synthesized by endothelial cells,
megakaryocytes and platelets. It has a role
in platelet adhesion and aggregation. The
deficiency in vWF (VIIIR) is called von
Willebrand’s disease
• Willebrand’s disease is an
autosomal dominant trait. Most
common congenital BLEEDING
DISORDER. If there is a decreased
vWF levels there is also a decrease
in VIIIC levels because VIIIR is a
carrier of VIIIC
Factor IX (plasma thromboplastin) is found in
the serum or plasma. It is also Vitamin K
dependent. Its deficiency is inherited as an X-
linked recessive trait. The deficiency is called
Christmas disease or Hemophilia B. Patients
will present with a hemophilia like symptoms
o Factor X (Stuart) is found in the serum and
plasma. It is part of the final common pathway.
It is also vitamin K dependent
o Factor XI
o Factor XII (Hageman) is the surface contact
activator for intrinsic pathway
Deficiency does not cause bleeding, only
increased thrombotic incidence (MI and
thrombosis).
o Factor XIII (fibrin stabilizing factor) The
deficiency is inherited as an autosomal
recessive trait. Infants with the disease present
with bleeding at the umbilical stump. This is
also associated with intracranial hemorrhage,
soft tissue hemorrhage, recurrent abortions and
delayed or poor wound healing. aPTT, PT and
bleeding time are normal. The only way to

diagnose is the 5M-urea clot dissolution
time This measures the time it takes for a clot
to dissolve in urea (normal: 24 hrs; abnormal:
<24 hrs).
o High-Molecular Weight Kininogen (HMWK;
Fitzgerald factor) is part of the kallikrein
system. It converts factor XII to XIIa. The
deficiency of this factor is rare and does not
produce clinical bleeding
o Prekallikrein (Fletcher, PK) – complexes with
HMWK, kallikrein precursor, cleaved by Factor
XIIa (Activated Hageman) to produce kallikrein.
Its deficiency does not produce clinical bleeding
o REMEMBER
9 out of 13 factors are proenzymes and must
be activated except fibrinogen (not an
enzyme), Factor III (a complex rather than a
single protein), Factor IV (Calcium)
Vitamin K dependent (for the post-translational
carboxylation):
• Factor II, VII, IX, X
Many of the factors are decreased at birth
except fibrinogen and platelets (normal level).
Factor VIIIC and VIIIR (vWF) are elevated at
birth. Since many factors are decreased at
birth, PT and aPTT cannot be used in
newborns
Acute phase reactants: Factor VIII, Fibrinogen
(their levels are usually elevated during
inflammation)
O.PLASMA WBC, RBC
P
Q. Blood screening tests

- ABO typing, Rh typing, VDRL; venereal disease
research laboratory test (syphilis), malarial smear,
HBsAg; surface antigen of hepatitis B virus, HCV;
hepatitis C virus, HIV
R.
Transfusion Reactions
- Adverse symptoms produced by red cell
incompatibility between a patient and a unit of
donor blood
- Causes of fatal reactions, most of which are due to
clerical errors: misidentification of patients;
mislabeling of blood samples; error in laboratory
records; mistakes in blood typing; inaccurate
antibody screening or cross matching
- Could wither be acute/delayed,
hemolytic(intravascular or extravascular)/non-
hemolytic, immune/n on-immune
- Types of Transfusion Reactions
a. Acute – occurs within minutes to 24 hours of
the transfusion
b. Delayed – develop within days to months or
even years after the transfusion; sometimes
even on subsequent transfusion
- Factors that influence whether a transfusion will
be acute/delayed:
a. Number of incompatible red cells infused
b. Antibody class or subclass
c. Achievement of optimal temperature for
binding