motor anatomy airway management
121
Motor system Spinal cord
-
Upload
kdiwavvou -
Category
Health & Medicine
-
view
920 -
download
3
Transcript of motor anatomy airway management

Motor system
Spinal cord

Components of spinal motor control system
• Spinal neurons
• Motor unit
• Muscle spindles • Golgi tendon organs

Muscle spindle
muscle
Dorsal root ganglion cell
Upper motor neuron of
corticospinal tract
α-motor neuron in the spinal cord
Neuro muscular junction
Golgi Tendon organ
α-mn is directly responsible for generation of
force by muscle
Upper motor neuron of extrapyramidal tract

Figure 5.28Page 173
Cervical cord
Thoracic cord
Lumbar cord
Sacral cord
VertebraeCervical nerves
Thoracic nerves
Lumbar nerves
Sacral nerves
Coccygealnerve
Cauda equina
50 muscles of the arm innervated
from spinal segments C3-T1
Muscles of the leg innervated from spinal segments
L1-S3

Figure 5.29Page 174
Cell body ofefferent neuron
Cell body ofafferent neuron
Efferent fiber
From receptors
To effectors
Spinal nerve
White matter Gray matter
Interneuron
Dorsal root
Dorsal root ganglion
Ventral root

Figure 5.31 Page 176
Centralcanal
Dorsal horn (cell bodies of interneuronson which afferent neurons terminate)
Lateral horn (cell bodies of autonomicefferent nerve fibers)
Ventral horn (cell bodies of somaticefferent neurons)

Motor neuron pool of a muscle.
• Those motor neurons innervating a single muscle
• The motor neuron pools are segregated into longitudinal columns extending through two to four spinal segments.
• The longitudinal orientation of motor neurons and their dendrites matches that of primary afferent terminals in that zone.
• Thus impulses in a given afferent axon tend to be distributed to motor neurons innervating the same muscle or muscles with similar function.

Figure 8.15Page 269
Spinal cord
= Motor unit 1
= Motor unit 2
= Motor unit 3
A motor unit is one motor neuron and the muscle
fibers it innervates

The size principle: the orderly recruitment of motor units
• The first motor units to be activated are those with smallest motor axons; – these motor units generate the smallest contractile
forces – and allow the initial contraction to be finely graded.
• As more motor units are recruited, – the alpha motor neurons with progressively larger
axons become involved – and generate progressively larger amounts of tension

Motor unit and motor neuron pool

Figure 5.29Page 174
Dorsal root
Dorsal root ganglion
Ventral root

Whole muscle tension depends on • the size of the muscle, • the extent of motor unit recruitment,• the size of each motor unit.
• The number of muscle fibers varies among different motor units.– Muscles performing refined, delicate movements
have few muscle fibers per motor unit. – Muscles performing coarse, controlled movements
have a large number of fibers per motor unit.– The asynchronous recruitment of motor units
delays or prevents muscle fatigue.

• One group of motor neuron pools is located in the medial part of the ventral horn, and the other much larger group lies more laterally.

Somatotopic organization of spinal cord motor neuron
trunk extremities
flexors
extensorsThe ventral root
α-mn: the final common
pathway

Functional rule• The motor neurons located medially project to
axial muscles (muscles of the neck and back): those located more laterally project to limb muscles (arms and legs).
• Within the lateral group the most medial motor neuron pools tend to innervate the muscles of the shoulder and pelvic girdles, while motor neurons located more laterally project to distal muscles of the extremities and digits.
• In addition the motor neurons innervating the extensor muscles tend to lie ventral to those innervating flexors.

Figure 5.30 (1)Page 174
Descending tracts
Dorsal surface
Gray matter
Ventral surface
Lateral corticospinal
Rubrospinal
Ventral corticospinal
Vestibulospinal

Motor neurons
• Alpha motor neuron– Thick myelinated fast conducting axons– Motor end plate of extrafusal skeletal muscle
fibers
• Gamma motor neuron– Thin myelinated slower conducting axons– Supply the intrafusal fibers of Muscle spindles
in skeletal muscles � γ-static� γ-dynamic

Spinal interneurons
• Points of convergence for– most of the input of the brain descending
tracts– Sensory afferents & collaterals of LMN axons
• Intersegmental; same side of spinal cord
• Commissural: cross midline

Spinal reflexes
• Contribute to
• Muscle tone
• Body posture• Locomotion

Muscle spindles
• Lie parallel to regular muscle fibers
• contain nuclear bag and nuclear chain intrafusal muscle fibers.

Capsule
Alpha motorneuron axon
Gamma motorneuron axon
Secondary (flower-spray)endings of afferentfibers
Extrafusal (“ordinary”)muscle fibers
Intrafusal (spindle)muscle fibers
Noncontractilecentral portionof intrafusalfiber
Contractile end portionsof intrafusal fiber
Primary (annulospiral)endings of afferent fibers

Muscle spindles
• Can be stimulated by 2 ways
• Stretching the entire muscle
• Causing contraction of intrafusal fibers while extrafusal fibers remain at the same length.

Muscle spindles
• Group Ia afferent fibers form primary endings on nuclear bag and chain fibers,
• Group II fibers form secondary endings on nuclear chain fibers.
• Dynamic motor axons end on nuclear bag fibers and static motor axons on nuclear chain fibers.

Muscle spindles
• Primary endings demonstrate both static and dynamic responses, which signal muscle length and rate of change in muscle length.
• Secondary endings demonstrate only static responses and signal only muscle length.
• Motor neurons cause muscle spindles to shorten, which prevents the unloading effect of muscle contraction.

Golgi tendon organs
• Located in the tendons of muscles and are arranged in series.
• They are supplied by group Ib afferent fibers and are excited both by stretch and by contraction of the muscle (very sensitive to changes in muscle tension)

Figure 8.26 (1)
Page 287
Extrafusalskeletalmuscle fiber
Intrafusalmusclespindle fiber
Spinalcord
Afferent input from sensory endings of muscle spindle fiber
Alpha motor neuron output to regular skeletal-muscle fiber
Stretch reflex pathway
γ motor-neuron output to contractile end portions of spindle fiber
Descending pathways coactivating α and γ motor neurons

Relaxed muscle; spindlefiber sensitive to stretchof muscle
Contracted muscle inhypothetical situation ofno spindle coactivation;slackened spindle fibernot sensitive to stretchof muscle
Contracted muscle innormal situation of spindle coactivation;contracted spindle fibersensitive to stretch ofmuscle

Primary endings Signal Velocity and amount of change in muscle length
• Nuclear bag fibers• Ia fibers• Show a dynamic
response:– Discharge most rapidly
while the muscle is being stretched & less rapidly during sustained contraction
• Nuclear chain fibers • Ia fibers• Show a Static
response– Discharge at an
increased rate throughout the period when a muscle is stretched
• Signal the amount of displacement

Alpha-gamma linkage
Enhancement of voluntary muscle contraction by co-activation of gamma and alpha motor neurons

The stretch reflex includes
• a monosynaptic excitatory pathway from group Ia (and II) muscle spindle afferent fibers to a motor neurons that supply the same and synergistic muscles and
• a disynaptic inhibitory pathway to antagonistic motor neurons.

Myotatic stretch reflex
• The simplest reflex
• Monosynaptic
• Physiological significance: – Resting muscle tone and thus A key reflex in
maintenance of posture

The tonic stretch reflex
• Physiological significance: Resting muscle tone– Judged by the resistance that a joint offers to
bending
– Receptors: Ia & II from muscle spindle– Triggered by the static responses of group Ia
and II afferents.
– Any slight extension or flexion (during standing) will elicit a tonic stretch reflex in muscles required to oppose the movement, thus helping an individual to stand upright.

Phasic stretch reflex
• Physiological significance:
• Receptors: Ia from muscle spindle
• Triggered by the dynamic responses of group Ia fibers
• Enhancement of voluntary muscle contraction by co-activation of gamma and alpha motor neurons

Myotatic stretch reflex
• Clinical significance in diagnosis of diseases – tendon jerks
– muscle tone

Muscle stretch reflex

Figure 8.27Page 288
Patellar tendon
Extensor muscle of knee(quadriceps femoris)
Musclespindle
Alpha motorneuron

Inverse stretch reflex• Disynaptic (inhibitory interneuron+ α-mn )• Inhibition of α-mn of same muscle• Receptor: Golgi tendon organ (in series with
muscle fibers)
• Stimulus: increase in muscle tension by – excessive stretch – excessive active muscle contraction
• Result: relaxation (sudden stop in contraction)• Safety:
– regulates muscle tension– protects the tendon from tearing


Withdrawal reflex
• Polysynaptic
• Protective
• Painful stimulation of skin, subcutaneous tissue or muscle
• Stimulation of flexorscontraction
• Reciprocal innervation
• Simultaneous inhibition of antagonists relaxation

Figure 5.33Page 178
Stimulus
Biceps(flexor)contracts
Handwithdrawn
Triceps(extensor)relaxes
Ascending pathwayto brain
Response
Components of areflex arc
ReceptorAfferent pathwayIntegrating centerEfferent pathwayEffector organs
Integrating center(spinal cord)
Thermalpain receptor
in finger
Efferent pathway
Effectororgans
= Inhibitory interneuron= Excitatory interneuron= Synapse= Inhibits= Stimulates
AfferentPathway

Crossed extensor reflex
• Supporting reflex, serves to maintain posture
• Polysynaptic • Irradiation of stimulation• Reciprocal innervation
• Flexion and withdrawal of the painfully stimulated limb
• + extension of the other limb

Figure 5.34Page 179
Efferent pathway
Afferentpathway Efferent
pathway
Flexormusclecontracts
Extensormusclerelaxes
Flexormusclerelaxes
Extensormusclecontracts
StimulusResponse
Painreceptorin heel
Injured extremity(effector organ)
Integrating center(spinal cord)
Opposite extremity(effector organ)
Response

Receptor
Effector
Dorsal root ganglion cell Interneuron in
the spinal cord
Upper motor neuron of
corticospinal tract
α-motor neuron in the spinal cord
XU
T
S
V
Y
Z
W



The motor control system
Overview

The Motor system 1
• Cortex
• The Corticospinal tract
• Alpha motor neuron
• Muscles

Motor ControlMotor Cortex
UMN
Corticospinal tract (UMN)
Alpha motor neuron,
LMNMuscle
Alpha motor neuron
axon, LMN

Four Hierarchical Components that Control Movements
• Motor systems consist of separate neural circuits that are linked.
• Ultimately, whether directly or indirectly distributed, all motor processing is focused on a single target ‘the motor neuron’ constituting the ‘final common pathway’ of motor system.

Four Hierarchical Components that Control Movements
Spinal cord BrainstemSubcortical (basal nuclei, thalamus,
cerebellum)Cortical –(primary motor cortex, premotor
and supplementary motor areas)

Motor system 2
• Cortex• corticospinal tract• Alpha motor neuron• Muscles
• Two control circuits that influence the activity of corticospinal tract– Cerebellum – Basal Ganglia

Motor system 2two control circuits

Motor system 3• Cortex• corticospinal tract• Alpha motor neuron• Muscles• + two control circuits influence the corticospinal tract• Cerebellum and BG
• The Indirect brainstem motor control centers and pathways which tonically activate the Lower Motor Neurons especially those that innervate the Axial and Antigravity muscles

Motor system 3

Upper Motor Neuron • The corticospinal tract has its main influence on
LMN that innervate the muscles of the distal extremities, i.e., the hand and the foot
• The corticospinal tract has collaterals that modulate the control of indirect brainstem motor centers, so that we are not as a statue opposing gravity and can move at will and have the right amount of supporting tone
• When there is lesion of UMN, clinical findings are a combination of both direct + indirect effects

Figure
8.24Page 285
Cortical level
Subcortical level
Brain stem level
Spinal cord level
Periphery
Premotor and supplementary motor areas
Sensory areas of cortex
Primary motor cortex
Basal nuclei Thalamus
Brain stem nuclei
Cerebellum
Afferent neuronterminals
Motor neurons
Muscle fibers
Movement

“To move things is all that mankind can do… for such the sole executant is muscle,
whether in whispering a syllable or in felling a forest”.. Charles Sherrington
• The spinal cord contains certain motor programs for the generation of coordinated movements and that these programs are accessed, executed, and modified by descending commands from the brain.

Types of Movements
• Involuntary motor acts– Reflex: the most automatic behaviors (such
as reflexes-organized at spinal cord level)
• Voluntary motor acts– The maintenance of position (posture)– Goal directed movements- skilled voluntary
movements- organized at higher centers

Somatic musculature in relation to the joint they act on
• Axial muscles:– For movements of the trunk
• Proximal muscles (or girdle muscles)– For movements of the shoulder, elbow, pelvis
and knee
• Distal muscles– That move the hands, feet, and digits (fingers
and toes)

Important aspects of hierarchical organization:
• Somatotopic maps – preserved in interconnections at different levels
• each hierarchical level receives information from periphery so that sensory input can modify the action of descending commands
• The higher levels have capacity to control the information that reaches them, allowing or suppressing the transmission of afferent volleys through sensory relays.

Important aspects of hierarchical organization:
• The various motor control levels are also organized in parallel: so that each level can act independently on the final common pathway.
• This allows commands from higher levels either to modify or to supersede lower order reflex behavior.

Upper Motor Neuron Lesion

UMNL loss of direct effect of UMN

UMNL loss of indirect effect of UMN

UMNL is a combination of Loss of regulation
of indirect brainstem motor control centers
Loss of direct CST control
of LM neurons

Upper Motor Neuron Lesion
• Loss of distal extremity strength
• Loss of distal extremity dexterity
• Babinski sign
Loss of direct effect
• Increased tone
• Hyperreflexia
• Clasp-knife phenomenon
Loss of indirect effect

UMNL on opposite side of clinical findings if lesion is above the decussation

UMNL on same side of clinical findings if lesion in the spinal cord after decussation





Figure 9: The brain of a recovered stroke patient relies
on a compensatory neural pathway (dark blue) as
substitution for the damaged neuralpathway (blue dashed).
The cerebello-thalamo -cortical pathway (green) is “teaching” the
supplementary motor area its new function, which is indicated
by abnormal activity in the cerebellum and thalamus.
(Freely adapted from Azari & Seitz, 2000)



Airway Management in the Emergency Department
and ICUMehdi Khosravi, MD Pulmonary/CCM Fellow
Giuditta Angelini, MD Assistant Professor
Jonathan T. Ketzler, MD Associate Professor
Douglas B. Coursin, MD Professor
Departments of Anesthesiology & MedicineUniversity of Wisconsin, Madison

Global Assessment
Assess underlying need for airway control• Duration of intubation
- Nasal intubation less advantageous for potentially prolonged ventilator requirements
• Permanent support- Underlying advanced intrinsic lung or neuromuscular disease
• Temporary support• Anesthesia• Presence of reversible intrinsic lung or neuromuscular disease• Protection of the airway due to depressed mental status • Presence of reversible upper airway pathology• Patient care needs (e.g., transport, CT scan, etc.)• Significant comorbidities
Aspiration potential or increased respiratory secretions Hemodynamic issues such as cardiac disease or sepsis Renal or liver failure

Global Assessment
Pathophysiology of the respiratory failure• Hypoxic respiratory failure
- In case of hypoxic respiratory failure, different noninvasive oxygen delivery devices can be used.
- The severity of hypoxia and presence or absence of underlying disease (such as COPD) will dictate the device of choice.
• Hypercapnic respiratory failure- The noninvasive device of choice for hypercapnic respiratory failure is BIPAP.
Assessment of above mentioned patient characteristics in conjunction with the mechanism of respiratory distress leads the clinician to proper choice and duration of invasive or noninvasive options for airway management.
Code status should be clarified prior to proceeding.

Global AssessmentOxygenation• Respiratory rate and use of accessory muscles
- Is the patient in respiratory distress?• Amount of supplemental oxygen
- What is the patient’s oxygen demand?• Pulse oximeter or arterial blood gas
- Is the patient physiologically capable of providing appropriate supply?
Airway• Anatomy
- Will this patient be difficult to intubate?• Patency
- Is there a reversible anatomical cause of respiratory failure as opposed to intrinsic lung dysfunction?
• Airway device in place- Is there a nasopharyngeal airway or combitube in place?

Oxygen Delivery Devices(In order of degree of support)
Nasal Cannula• 4% increase in FiO2 for each 1 L of flow (e.g., 4 L flow = 37% or 6 L flow
= 45%)
Face tent• At most delivers 40% at 10-15 L flow
Ventimask• Small amount of rebreathing• 8 L flow = 40%, 15 L flow = 60%
Nonrebreather mask• Attached reservoir bag allows 100% oxygen to enter mask with
inlet/outlet ports to allow exhalation to escape - does not guarantee 100% delivery.

Oxygen Delivery DevicesNoninvasive Positive Pressure
CPAP is a continuous positive pressure• Indicated in hypoxic respiratory failure and obstructive sleep apnea
BiPAP allows for an inspiratory and expiratory pressure to support and improve spontaneous ventilation
• Mainly indicated in hypercapnic respiratory failure and obstructive sleep apnea
If use of noninvasive modes of ventilation does not result in improved ventilation or oxygenation in two to three hours, intubation should be considered
These devices can be used if following conditions are met:• Patient is cooperative with appropriate level of consciousness• Patient does not have increased respiratory secretions or aspiration potential• Concurrent enteral feeding is contraindicated.
Facilitates early extubation, especially in COPD patients
Some devices allow respiratory rate to be set.
Up to 10 L of oxygen can be delivered into the mask for 100% oxygen delivery.
Nasal or oral (full face) mask can be used; less aspiration potential with nasal.

Degree of Respiratory DistressRespiratory pattern• Accessory muscle use is an indication of distress.• Rate > 30 can indicate need for more support by noninvasive positive
pressure or intubation
Need for artificial airway• Tongue and epiglottis fall back against posterior pharyngeal wall• Nasopharyngeal airway better tolerated
Pulse oximetry• O2 saturation less than 92% on 60 - 100% oxygen can suggest the need
for intubation based on whether there is anything immediately reversible which could improve ventilation.
Arterial blood gas• pH < 7.3 can indicate need for more support by noninvasive positive
pressure or intubation.

Temporizing Measures
Naloxone for narcotic overdose• 40 mcg every minute up to 200 mcg with:
- 45 minutes to one hour duration of action• 0.4 - 2 mg of naloxone is indicated in patients with respiratory arrest and
history suggestive of narcotic overdose- There is a potential for pulmonary edema, so large dose is reserved
for known overdose and respiratory arrest• Caution in patients with history of narcotic dependence• Naloxone drip can be titrated starting at half the bolus dose used to
obtain an effect- Manufacturer recommended 2 mg in 500 ml of normal saline or D5
gives 0.004 mg/ml concentration

Temporizing Measures (cont'd)
Flumazenil for benzodiazepine overdose• 0.2 mg every minute up to 1 mg• Caution in patients with history of benzodiazepine or alcohol dependence• Caution in patients with history of seizure disorder as it will decrease the
seizure threshold
Artificial airway for upper airway obstruction in patients with oversedation• May be necessary in patients with sleep apnea despite judicious sedation
100% oxygen and maintenance of spontaneous ventilation in patients with pneumothorax• Washout of nitrogen may decrease size of pneumothorax• Positive pressure may cause conversion to tension pneumothorax

Oral/Nasal Airways

Indications for Intubation
Depressed mental status• Head trauma patients with GCS 8 or less is an indication for intubation
- Associated with increased intracranial pressure- Associated with need for operative intervention- Avoid hypoxemia and hypercarbia which can increase morbidity and
mortality• Drug overdose patients may require 24 - 48 hours airway control.
Upper airway edema• Inhalation injuries• Ludwig’s angina• Epiglottitis

Underlying Lung Disease
Chronic obstructive lung disease• Application of controlled ventilation may interfere with complete
exhalation, overdistend alveoli, and impair right heart and pulmonary venous return.
Pulmonary embolus• Pulmonary artery and right ventricle already have high pressure and
dependent on preload• Application of controlled ventilation may deteriorate oxygenation and
systemic pressure.
Restrictive lung disease• May require less than 6 cc/kg Vt to prevent elevated intrapulmonary
pressure• Application of positive pressure may result in barotrauma in addition to
impaired preload.

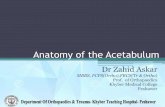
Airway Anatomy Suggesting Difficult Intubation
Length of upper incisors and overriding maxillary teeth
Interincisor (between front teeth) distance < 3 cm (two finger tips)
Thyromental distance < 7 cm• tip of mandible to hyoid bone (three finger breaths)
Neck extension < 35 degrees
Sternomental distance < 12.5 cm• With the head fully extended and mouth closed
Narrow palate (less than three finger breaths)
Mallampati score class III or IV
Stiff joint syndrome• About one third of diabetics characterized by short stature, joint rigidity, and tight waxy skin• Positive prayer sign with an inability to oppose fingers
No sign is foolproof to indicate intubation difficulty
Erden V, et al. Brit J Anesth. 2003;91:159-160.
Prayer Sign

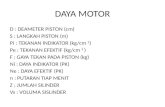
Mallampati Score
Class I: Uvula/tonsillar pillars visibleClass II: Tip of uvula/pillars hidden by tongueClass III: Only soft palate visibleClass IV: Only hard palate visible
Den Herder, et al. Laryngoscope. 2005;115(4):735-739.

ComorbiditiesPotential for aspiration requires rapid sequence intubation with cricoid pressure• Clear liquids < 4 hours• Particulate or solids < 8 hours• Acute injury with sympathetic stimulation and diabetics may have
prolonged gastric emptying time.
Potential for hypotension• Cardiac dysfunction, hypovolemia, and sepsis• May need to consider awake intubation with topical anesthesia
(aerosolized lidocaine) as sedation may precipitate hemodynamic compromise and even arrest.
Organ failure• Renal and hepatic failure will limit medication used.• Potential for preexisting pulmonary edema and airway bleeding from
manipulation

Induction Agents
Sodium Thiopental• 3 - 5 mg/kg IV• Profound hypotension in patients with hypovolemia, histamine release,
arteritis • Dose should be decreased in both renal and hepatic failure.
Etomidate• 0.1 - 0.3 mg/kg IV• Lower dose range for elderly and hypovolemic patients• Hemodynamic stability, myoclonus• Caution should be exercised as even one dose causes adrenal
suppression due to similar steroid hormone structure.• Unlikely to have prolonged effect in organ failure

Induction Agents (cont'd)
Propofol• 2 - 3 mg/kg IV• Hypotension, especially in patients with systolic heart dysfunction,
bradycardia, and even heart block• Unlikely to have prolonged effect in organ failure
Ketamine• 1 - 4 mg/kg IV, 5 - 10 mg/kg IM• Stimulates sympathetic nervous system• Requires atropine due to stimulated salivation and midazolam for
potential of dysphoria• Avoid in patients with loss of autoregulation and closed head injury

Neuromuscular Blockers
Succinylcholine• 1 - 2 mg/kg IV, 4 mg/kg IM• Avoid in patients with malignant hyperthermia, > 24 hours out from burn or
trauma injury, upper motor neuron injury, and preexisting hyperkalemia
Rocuronium • 0.6 - 1.2 mg/kg, highest dose required for rapid sequence• Hemodynamically stable, 10% renal elimination
Vecuronium• 0.1 mg/kg• Hemodynamically stable, 10% renal elimination
Cisatricurium• 0.2 mg/kg• Mild histamine release, Hoffman degradation, not prolonged in renal or
hepatic failure

Rapid Sequence Intubation
Preoxygenate for three to five minutes prior to induction• Wash out nitrogen to avoid premature desaturation during intubation.
Crycoid pressure should be applied from prior to induction until confirmation of appropriate placement.
Succinylcholine 1 - 2 mg/kg IV will achieve intubation conditions in 30 seconds; Rocuronium 1.2 mg/kg IV will achieve intubation conditions in 45 seconds.• Other muscle relaxants do not produce intubation conditions in less than
60 seconds.
Avoid mask ventilation after induction.• Potentially can inflate stomach• Use only if necessary to ensure appropriate oxygenation during
prolonged intubation.

Y BAG PEOPLE (Reference #6)

Cricoid Pressure
Cricoid is circumferential cartilage
Pressure obstructs esophagus to prevent escape of gastric contents
Maintains airway patency
Koziol C, et al. AORN. 2000;72(6):1018-1030.

Sniffing PositionAlign oral, pharyngeal, and laryngeal axes to
bring epiglottis and vocal cords into view.
Hirsch N, et al. Anesthesiology. 2000;93(5):1366.

Mask Ventilation
Mask ventilation crucial, especially in patients who are difficult to intubate
Sniffing position with tight mask fit optimal
May require two hands
Mask ventilation crucial, especially in patients who are difficult to intubate
Sniffing position with tight mask fit optimal
May require two hands

Laryngoscope Blades and Endotracheal Tubes
Miller blade: End of blade should be under epiglottis
Mac blade: End of blade should be placed in front of epiglottis in valecula
ETT for Fastrach LMA
Pediatric uncuffed ETT
ETT for blind nasal
Standard ETT

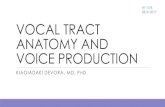
Graded Views on Intubation
Grade 1: Full glottis visibleGrade 2: Only posterior commissureGrade 3: Only epiglottisGrade 4: No glottis structures are visible
Yarnamoto K, et al. Anesthesiology. 1997;86(2):316.

Confirmation of PlacementDirect visualization
Humidity fogging the endotracheal tube
End tidal CO2 which is maintained after > 5 breaths• Low cardiac output results in decreased delivery of CO2
Refill in 5 seconds of self-inflating bulb at the end of the endotracheal tube
Symmetrical chest wall movement
Bilateral breath sounds
Maintenance of oxygenation by pulse oximetry
Absence of epigastric auscultation during ventilation

Additional Considerations
Always have additional personnel and an experienced provider as backup available for potential failed intubation
Always have suction available
Never give a muscle relaxant if difficult mask ventilation is demonstrated or expected
Awake intubation should be considered in the following:• If patient is so hemodynamically unstable that induction drugs cannot be
tolerated (topicalize airway)• If patient has a history or an exam which suggests difficult mask
ventilation and/or direct laryngoscopy

American Society of Anesthesiologistswww.asahq.org

Alternative MethodsBlind nasal intubation
• Bleeding may cause problems with subsequent attempts.• Contraindicated in patients with facial trauma due to cribiform plate disruption or
CSF leak• Avoid in immune suppressed (i.e., bone marrow transplant)
Eschmann styletFiber optic bronchoscopic intubation
• Awake vs. asleep
Laryngeal mask airway• Allows ventilation while bridging to more definitive airway
Light wandRetrograde intubation
• Through cricothyrotomy
Surgical tracheostomyCombitube

Eschman Stylet
Use especially if Grade III view achievedDirect laryngoscopy is performedPlace Eschman where trachea is anticipatedMay feel tracheal rings against stiffness of styletThread 7.0 or 7.5 ETT over stylet with the laryngoscope still in place

Fiberoptic Scope
Essentially what is used to do a bronchoscopyCan be used to thread an endotracheal tube into the trachea either while the patient is asleep or on an awake patient with a topicalized airwayVia laryngeal mask airway in place due to inability to intubate with DL:
• Aintree (airway exchange catheter) can be threaded over the FOB to be placed into trachea upon visualization
• Wire-guided airway exchange catheter can also be used with one more step

The Laryngeal Mask Airway (LMA)

LMA Placement
Guide the LMA along the palate
Eventual position should be underneath the epiglottis, in front of the tracheal opening, with the tip in the esophagus
FOB placement through LMA positions in front of trachea
Martin S, et al. J Trauma Injury, Infection Crit Care. 1999;47(2):352-357.

The FastrachTM Laryngeal Mask Airway
Reinforced LMA allows for passage of ETT without visualization of trachea.
10% failure rate in experienced hands
20% failure rate in inexperienced

The Light WandTransillumination of trachea with light at distal endTrachea not visualized directlyShould not be used with tumors, trauma, or foreign bodies of upper airwayMinimal complication except for mucosal bleed10% failure rate on first attempt in experienced hands

Retrograde Intubation
Puncture of the cricothyroid membrane with retrograde passage of a wire to the trachea
Endotracheal tube guided endoscopically over the wire through the trachea
Catheter through the cricothyroid can be used for jet ventilation if necessary.
Wesler N, et al. Acta Anaes Scan. 2004;48(4):412-416.

CombitubeEmergency airway used mostly by paramedics and emergency physicians for failed endotracheal intubation
Ventilation confirmed through blind blue tube
• Combitube is in the esophagus and salem sump can be placed through white tube
Ventilation confirmed through white (clear) tube with patent distal end
• Combitube is in the trachea and salem sump should be placed outside of combitube into esophagus
• Fiber optic exchange can be accomplished through combitube

Combitube (cont'd)
Should be changed to endotracheal tube (ETT) or tracheostomy to prevent progressive airway edema
If in esophagus, take down pharyngeal cuff and attempt direct laryngoscopy (DL) or fiber optic bronchoscope (FOB) placement around combitube
Failed exchange attempt can be solved with operative tracheostomy
Placement of combitube can produce significant airway trauma
• Removal prior to DL or FOB should be done with caution after thorough airway evaluation
• Cricoid pressure should be maintained and emergency tracheostomy equipment available

Tracheostomy
Surgical airway through the cervical tracheaEmergent procedure carries risk of bleeding due to proximity of innominate arteryCan be difficult and time consuming in emergent situations
Sharpe M, et al. Laryngoscope. 2003;113(3):530-536.

Case Scenario #1
The patient is 70 kg with a 20-year history of diabetes.
On exam, the patient has intercisor distance of 4 cm, thyromental distance is 8 cm, neck extension is 45 degrees, and mallampati score is 1.
Your staff wants to use thiopental and pancuronium.
Do you have any further questions for this patient or would you proceed with your staff?

Case Scenario #1 - Answer
A diabetic for 20 years needs assessment for stiff joint syndrome.
You should have the patient demonstrate the prayer sign.
If the patient is unable to oppose their fingers, you should not give pancuronium.
You may want to proceed with an LMA and FOB at your disposal.
If the patient has a history of gastroparesis, you may want to consider an awake FOB.

Case Scenario #2
43-year-old patient with HIV, likely PCP pneumonia who had been prophylaxed with dapsone
RR is 38, oxygen saturation is 90% on 100% NRB mask
The patient is on his way to get a CT scan.
Is it appropriate to proceed without intubation?

Case Scenario #2 - Answer
Dapsone will produce some degree of methemoglobinemia.
Therefore, some degree of desaturation may not be overcome.
The patient is in significant respiratory distress and will be confined in an area without easy access.
Intubation should be considered as an extra measure of safety, especially as this patient is likely to get worse.

Case Scenario #3
40-year-old, 182-kg man has a history of sleep apnea and systolic ejection fraction of 25%. He has a Strep pneumonia in his left lower lobe and progressive respiratory insufficiency.
He extends his neck to 50 degrees and has a mallampati score of 2.
Would you proceed with an awake FOB?

Case Scenario #3 - Answer
The patient’s airway anatomy is not suggestive of difficulty.
However, with supine position, subcutaneous tissue may impair your ability to visualize or ventilate.
Use of gravity, including a shoulder roll, extreme sniffing position, and reverse trendelenburg may be helpful with asleep DL.
Prudent to have some accessory equipment, including an LMA and FOB, for back up

References
1. Caplan RA, et al. Practice guidelines for management of the difficult airway. Anesthesiology. 1993;78:597-602.
2. Langeron O, et al. Predictors of difficult mask ventilation.Anesthesiology. 2000;92:1229-36.
3. Frerk CM, et al. Predicting difficult intubation. Anaesthesia.1991;46:1005-08.
4. Tse JC, et al. Predicting difficult endotracheal intubation in surgical patients scheduled for general anesthesia. Anesthesia & Analgesia. 1995;81:254-8.
5. Benumof JL, et al. LMA and the ASA difficult airway algorithm. Anesthesiology. 1996;84:686-99.
6. Reynolds S, Heffner J. Airway management of the critically ill patient. Chest. 2005;127:1397-1412.