Mo1001 Nodular Regenerative Hyperplasia: Many Ways to Get There
1
through the down-regulation of integrated signaling pathways involving p-ERK- HIF-1 α- VEGF and p-ERK- c-fos- VEGFR-2. Mo1001 Nodular Regenerative Hyperplasia: Many Ways to Get There Jason L. Eccleston, Mary DeMino, David E. Kleiner, Preeti Reshamwala, Xiongce Zhao, Christopher Koh, Mark T. Gladwin, Harry L. Malech, Dean D. Metcalfe, Warren Strober, Gregory J. Kato, Ivan J. Fuss, Jake Liang, Steven M. Holland, Theo Heller Introduction: Nodular Regenerative Hyperplasia (NRH) is a rare noncirrhotic portal hyperten- sive liver disease characterized by the diffuse transformation of hepatic parenchyma into regenerative nodules without fibrosis. Although the specific etiology has yet to be elucidated, NRH has been associated with various diseases, conditions and medications. Thus, whether NRH occurs from a single unifying pathophysiologic process or multiple different processes is still uncertain. Aims: To characterize biochemical, radiological, and histologic markers of liver disease in patients (pts) with and without NRH in multiple disease cohorts. Methods: Pts with chronic granulomatous disease (CGD), sickle cell disease (SCD), systemic mast cell disease (SMCD), common variable immunodeficiency disease (CVID) and sporadic cases of NRH underwent hepatologic evaluation and liver biopsy for clinical care purposes were evaluated with biomarkers of liver disease, radiologic imaging and histopathologic analysis. Results: 137 pts were evaluated and 56 (41%) were diagnosed with NRH histologically. Of those with NRH, 11 (20%) had CGD, 22 (39%) SCD, 7 (13%) SMCD, 12 (21%) CVID and 4 (7%) sporadic disease. Age at biopsy across all NRH cohorts was significantly older compared to the non-NRH population (mean 40 vs. 33 years, p=0.0128). Patients with NRH had significantly higher alkaline phosphatase (197 vs. 190 U/L, p=0.01), increased liver volumes (2152 vs. 1166 cm3, p=0.01) and increased spleen volumes (after excluding SCD) (1071 vs. 410 cm3, p=0.01), which negatively correlated with platelets ( ρ -0.58, p= 0.002). In the SCD cohort, pts with NRH had increased gamma-glutamyltransferase (128 vs. 67 U/L, p=0.03) and increased lactate dehydrogenase (432 vs. 322 U/L, p=0.01). On histologic evaluation, SCD-NRH pts had increased lobular inflammation (p=0.04). SMCD- NRH pts had increased portal and peri-portal inflammation (p=0.005 and p=0.01, respec- tively), veno-occlusive changes (p=0.04), portal venopathy (p=0.001) and sinusoidal dilation (p=0.03). Conclusions: Despite parallels in clinical disease presentation, histopathologic examination of NRH in separate disease cohorts suggests different mechanistic pathways. Given the potential for multiple etiologies, NRH may be more common than previously thought. Further investigation should focus on the underlying disease process as it may provide a window into biology. Mo1002 MELD Score Is a Risk for First Episode of Spontaneous Bacterial Peritonitis in Patients With Cirrhosis Rashid Khan, Whitney Jennings, Habeeb Salameh, Kirk Russ, Matthew J. Skinner, Sandhya Mudumbi, Yong Fang Kuo, Andrea Duchini, Ashwani K. Singal Purpose: Spontaneous bacterial peritonitis (SBP) occurs in 10-30% of patients with cirrhosis and carries an in-hospital mortality rate of 30 to 50 %. AASLD recommends consideration of primary prophylaxis for SBP amongst patients with low ascitic fluid protein (<1.5 g/dl) along with impaired renal function (creatinine ≥ 1.2 mg/dL, blood urea ≥ 25 mg/dL or serum Na ≤ 130 mEq/l) or liver failure (Child score ≥ 9 and bilirubin ≥3 mg/dL. Model for end-stage disease (MELD) score is accurate in predicting 3 mo. mortality from cirrhosis and is used worldwide for listing patients for liver transplantation. However, there is no data on its predictive ability on initial SBP occurrence. We performed a retrospective case control study from two tertiary care academic centers to examine association of MELD score and risk of SBP. Methods: Cirrhotic patients with a first episode of SBP (cases) were matched to cirrhotics with ascites but without SBP (controls) for age, gender, ethnicity, and calendar year of diagnosis. Diagnosis of SBP was confirmed with culture positivity and/or ascitic fluid cell count. Baseline MELD score was calculated within a month prior to SBP diagnosis for cases and within a month prior to any decompensation for controls. A common spreadsheet was developed for both institutions for collection of patient data of identified study popula- tion. Categorical and continuous variables were compared using chi-square and t-test respec- tively. Conditional logistic regression models with various functional forms of MELD were built. Based on likelihood ratio test, a cut-off MELD score for the risk of SBP was determined. Results: A total of 453 (253 from UTMB with 100 cases and 200 from UAB with 97 cases) patients were analyzed. Proportion of patients with SBP at both the centers increased with increasing MELD scores. As the probabilities were different for the two centers, data were combined for this analysis (Table). Mean probability for SBP occurrence increased linearly with increasing MELD score (Figure). For each unit increase in MELD, the odds ratio (95% CI) for development of SBP were 1.35 (1.24- 1.46) and 1.41 (1.26-1.58) among patients with MELD< 20 and for patients with MELD>/=20 respectively. Conclusion: Our study, suggests an association of MELD score with the risk of initial SBP occurrence in patients with cirrhosis and ascites. Prospective studies are suggested to validate these data, and to assess the cut-off MELD score in patients with cirrhosis who would derive maximum benefit from prophylactic antibiotics for primary prophylaxis of SBP. Prevalence of spontaneous bacterial peritonitis among patients with cirrhosis with various MELD scores S-983 AASLD Abstracts Increasing mean probability of spontaneous bacterial peritonitis with MELD score in patients with cirrhosis Mo1003 The Renal Safety of MRI With Gadolinium in Patients Following Liver Transplantation Thomas Runge, Katherine Shaffer, Mehul Parikh, Sebastian D. Perez, Ram M. Subramanian Introduction: Intravenous contrast enhanced imaging is invaluable in diagnosing pathology following liver transplantation, including vascular and infectious complications. Given the potential risk of contrast nephropathy associated with intravenous iodinated CT contrast, alternate contrast modalities for abdominal imaging need to be examined, especially in the setting of renal insufficiency. Aims: The purpose of this study was to examine the renal safety of MRI with gadolinium during abdominal imaging in patients following liver transplantation. Methods: The study involved a retrospective analysis of 480 cases of abdominal MRI with gadolinium in liver transplant recipients at a single academic center during 2007 to 2011. For each case, a serum creatinine was noted prior to and within one week after the MRI. Patients who underwent hemodialysis or continuous renal replacement prior to the post- MRI creatinine measurement were excluded. Serum creatinine values before and after the MRI were compared using a paired t-test. In addition, the cases were analyzed for the development of nephrogenic systemic fibrosis (NSF), a reported complication of gadolinium in the setting of renal insufficiency. Results: The age of the patients at the time of MRI ranged from 18 to 75 years, with 61% being male. MRIs were obtained between 1 and 3400 days following transplantation, with 67% of MRIs being performed within 8 months of the transplant. The pre-MRI serum creatinine values ranged from 0.32 to 8.69 mg/dL, with 189 cases (39.1%) having values ≥ 1.5 mg/dl. A comparison of the pre and post MRI serum creatinine values did not demonstrate a statistically significant difference, including those cases with a pre-MRI serum creatinine ≥ 1.5 mg/dl. In addition, no cases of NSF were noted. Conclusion: These observations suggest that MRI with gadolinium is a non-nephrotoxic imaging modality in patients following liver transplantation. Importantly, the renal safety of this modality extends to cases with baseline renal insufficiency (defined as Cr ≥ 1.5 mg/ dl), in which contrast enhanced CT may be contraindicated due to the risk of contrast nephropathy. Therefore, gadolinium enhanced IV contrast imaging provides an invaluable imaging modality for the diagnosis of pathology following liver transplantation, especially in the setting of renal insufficiency. Mo1004 Indiscriminate Albumin Use Predisposes to Renal Impairment in Spontaneous Bacterial Peritonitis - Lessons to Learn Jatinder Lachar, Amanda E. Gentry, Mariel Muriel Pastrana, Leroy R. Thacker, Puneet Puri, Arun J. Sanyal Introduction: Intravenous albumin use is recommended with antibiotics on day 1 and day 3 of diagnosis of spontaneous bacterial peritonitis (SBP) as it reduces renal impairment (RI) and mortality. However any deviation from this approach and its impact on SBP related RI in general clinical practice is not known. Our aim was to investigate SBP related renal and mortality outcomes in hospitalized patients with and without IV albumin use. Methods: Hospitalized subjects admitted with ascites in a tertiary care academic center from January 2008-December 2010 were screened for SBP. The diagnosis of SBP was established by >250 ascitic fluid polymorphonuclear (PMN) cells. Demographic, clinical, biochemical and treatment details including IV albumin use were collected. Renal impairment was defined using acute kidney injury criteria of an increase in serum creatinine > 50% or ≥ 0.3 mg/ dL from baseline labs in < 48 hours. For analysis, the subjects were classified following the diagnosis of SBP based on the pattern of IV albumin use as (1) no IV albumin (NIVA), (2) IV albumin on day 1 only (IVAD1), (3) IV albumin on day 3 only (IVAD3) and (4) IV albumin on both day 1 and day 3 (IVAD1+3). Statistical analysis using a logistic regression model with group predicting renal dysfunction and adding dialysis as a potential cofounder was used to evaluate the effects of IV albumin infusion with antibiotic therapy. Results: Of 55 subjects that met the inclusion criteria, 15/55 (27%) had alcoholic cirrhosis and 31/55 (56%) were males. The mean age was 51.89 years. At admission, 7% (4/55) of the patients were undergoing hemodialysis secondary to end stage renal disease and the mean MELD score was 16.16. Interestingly, IVAD1+3 subjects (n=20) when compared to all other groups {NIVA (n=15), IVAD1 (n=15), and IVAD3 (n=5)}, had a significant lower risk of RI between the groups (χ2 = 6.79, p = 0.0221, OR = 0.24, 95% CI=(0.07, 0.85)), indicating that subjects with IVAD1+3 were 4 times less likely to have RI (OR=4.24) than other groups. Adjusting for dialysis by way of a multi-variable logistic regression, IVAD1+3 was still a significant predictor of RI (p = 0.0284, OR = 0.24, 95% CI = (0.07, 0.86)); and 4 times more likely to reduce RI than other groups. In contrast, in-hospital mortality rates were not significantly different among the IVAD1+3 vs. other groups. Conclusions: IV albumin when used as recommended is 4 times more likely to reduce renal impairment (RI) in cirrhotics with SBP. AASLD Abstracts
Transcript of Mo1001 Nodular Regenerative Hyperplasia: Many Ways to Get There

through the down-regulation of integrated signaling pathways involving p-ERK- HIF-1 α-VEGF and p-ERK- c-fos- VEGFR-2.
Mo1001
Nodular Regenerative Hyperplasia: Many Ways to Get ThereJason L. Eccleston, Mary DeMino, David E. Kleiner, Preeti Reshamwala, Xiongce Zhao,Christopher Koh, Mark T. Gladwin, Harry L. Malech, Dean D. Metcalfe, Warren Strober,Gregory J. Kato, Ivan J. Fuss, Jake Liang, Steven M. Holland, Theo Heller
Introduction: Nodular Regenerative Hyperplasia (NRH) is a rare noncirrhotic portal hyperten-sive liver disease characterized by the diffuse transformation of hepatic parenchyma intoregenerative nodules without fibrosis. Although the specific etiology has yet to be elucidated,NRH has been associated with various diseases, conditions and medications. Thus, whetherNRH occurs from a single unifying pathophysiologic process or multiple different processesis still uncertain. Aims: To characterize biochemical, radiological, and histologic markers ofliver disease in patients (pts) with and without NRH in multiple disease cohorts. Methods:Pts with chronic granulomatous disease (CGD), sickle cell disease (SCD), systemic mast celldisease (SMCD), common variable immunodeficiency disease (CVID) and sporadic cases ofNRH underwent hepatologic evaluation and liver biopsy for clinical care purposes wereevaluated with biomarkers of liver disease, radiologic imaging and histopathologic analysis.Results: 137 pts were evaluated and 56 (41%) were diagnosed with NRH histologically. Ofthose with NRH, 11 (20%) had CGD, 22 (39%) SCD, 7 (13%) SMCD, 12 (21%) CVID and4 (7%) sporadic disease. Age at biopsy across all NRH cohorts was significantly oldercompared to the non-NRH population (mean 40 vs. 33 years, p=0.0128). Patients withNRH had significantly higher alkaline phosphatase (197 vs. 190 U/L, p=0.01), increasedliver volumes (2152 vs. 1166 cm3, p=0.01) and increased spleen volumes (after excludingSCD) (1071 vs. 410 cm3, p=0.01), which negatively correlated with platelets ( ρ -0.58, p=0.002). In the SCD cohort, pts with NRH had increased gamma-glutamyltransferase (128vs. 67 U/L, p=0.03) and increased lactate dehydrogenase (432 vs. 322 U/L, p=0.01). Onhistologic evaluation, SCD-NRH pts had increased lobular inflammation (p=0.04). SMCD-NRH pts had increased portal and peri-portal inflammation (p=0.005 and p=0.01, respec-tively), veno-occlusive changes (p=0.04), portal venopathy (p=0.001) and sinusoidal dilation(p=0.03). Conclusions: Despite parallels in clinical disease presentation, histopathologicexamination of NRH in separate disease cohorts suggests different mechanistic pathways.Given the potential for multiple etiologies, NRH may be more common than previouslythought. Further investigation should focus on the underlying disease process as it mayprovide a window into biology.
Mo1002
MELD Score Is a Risk for First Episode of Spontaneous Bacterial Peritonitis inPatients With CirrhosisRashid Khan, Whitney Jennings, Habeeb Salameh, Kirk Russ, Matthew J. Skinner,Sandhya Mudumbi, Yong Fang Kuo, Andrea Duchini, Ashwani K. Singal
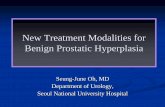
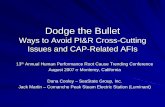
Purpose: Spontaneous bacterial peritonitis (SBP) occurs in 10-30% of patients with cirrhosisand carries an in-hospital mortality rate of 30 to 50 %. AASLD recommends considerationof primary prophylaxis for SBP amongst patients with low ascitic fluid protein (<1.5 g/dl)along with impaired renal function (creatinine ≥ 1.2 mg/dL, blood urea ≥ 25 mg/dL orserum Na ≤ 130 mEq/l) or liver failure (Child score ≥ 9 and bilirubin ≥3 mg/dL. Model forend-stage disease (MELD) score is accurate in predicting 3 mo. mortality from cirrhosis andis used worldwide for listing patients for liver transplantation. However, there is no dataon its predictive ability on initial SBP occurrence. We performed a retrospective case controlstudy from two tertiary care academic centers to examine association of MELD score andrisk of SBP. Methods: Cirrhotic patients with a first episode of SBP (cases) were matchedto cirrhotics with ascites but without SBP (controls) for age, gender, ethnicity, and calendaryear of diagnosis. Diagnosis of SBP was confirmed with culture positivity and/or ascitic fluidcell count. Baseline MELD score was calculated within a month prior to SBP diagnosis forcases and within a month prior to any decompensation for controls. A common spreadsheetwas developed for both institutions for collection of patient data of identified study popula-tion. Categorical and continuous variables were compared using chi-square and t-test respec-tively. Conditional logistic regression models with various functional forms of MELD werebuilt. Based on likelihood ratio test, a cut-off MELD score for the risk of SBP was determined.Results: A total of 453 (253 from UTMB with 100 cases and 200 from UAB with 97 cases)patients were analyzed. Proportion of patients with SBP at both the centers increased withincreasing MELD scores. As the probabilities were different for the two centers, data werecombined for this analysis (Table). Mean probability for SBP occurrence increased linearlywith increasing MELD score (Figure). For each unit increase in MELD, the odds ratio (95%CI) for development of SBP were 1.35 (1.24- 1.46) and 1.41 (1.26-1.58) among patientswith MELD< 20 and for patients with MELD>/=20 respectively. Conclusion: Our study,suggests an association of MELD score with the risk of initial SBP occurrence in patientswith cirrhosis and ascites. Prospective studies are suggested to validate these data, and toassess the cut-off MELD score in patients with cirrhosis who would derive maximum benefitfrom prophylactic antibiotics for primary prophylaxis of SBP.Prevalence of spontaneous bacterial peritonitis among patients with cirrhosis with variousMELD scores
S-983 AASLD Abstracts
Increasing mean probability of spontaneous bacterial peritonitis with MELD score in patientswith cirrhosis
Mo1003
The Renal Safety of MRI With Gadolinium in Patients Following LiverTransplantationThomas Runge, Katherine Shaffer, Mehul Parikh, Sebastian D. Perez, Ram M.Subramanian
Introduction: Intravenous contrast enhanced imaging is invaluable in diagnosing pathologyfollowing liver transplantation, including vascular and infectious complications. Given thepotential risk of contrast nephropathy associated with intravenous iodinated CT contrast,alternate contrast modalities for abdominal imaging need to be examined, especially in thesetting of renal insufficiency. Aims: The purpose of this study was to examine the renal safetyof MRI with gadolinium during abdominal imaging in patients following liver transplantation.Methods: The study involved a retrospective analysis of 480 cases of abdominal MRI withgadolinium in liver transplant recipients at a single academic center during 2007 to 2011.For each case, a serum creatinine was noted prior to and within one week after the MRI.Patients who underwent hemodialysis or continuous renal replacement prior to the post-MRI creatinine measurement were excluded. Serum creatinine values before and after theMRI were compared using a paired t-test. In addition, the cases were analyzed for thedevelopment of nephrogenic systemic fibrosis (NSF), a reported complication of gadoliniumin the setting of renal insufficiency. Results: The age of the patients at the time of MRIranged from 18 to 75 years, with 61% being male. MRIs were obtained between 1 and 3400days following transplantation, with 67% of MRIs being performed within 8 months of thetransplant. The pre-MRI serum creatinine values ranged from 0.32 to 8.69 mg/dL, with 189cases (39.1%) having values ≥ 1.5 mg/dl. A comparison of the pre and post MRI serumcreatinine values did not demonstrate a statistically significant difference, including thosecases with a pre-MRI serum creatinine ≥ 1.5 mg/dl. In addition, no cases of NSF were noted.Conclusion: These observations suggest that MRI with gadolinium is a non-nephrotoxicimaging modality in patients following liver transplantation. Importantly, the renal safetyof this modality extends to cases with baseline renal insufficiency (defined as Cr ≥ 1.5 mg/dl), in which contrast enhanced CT may be contraindicated due to the risk of contrastnephropathy. Therefore, gadolinium enhanced IV contrast imaging provides an invaluableimaging modality for the diagnosis of pathology following liver transplantation, especiallyin the setting of renal insufficiency.
Mo1004
Indiscriminate Albumin Use Predisposes to Renal Impairment in SpontaneousBacterial Peritonitis - Lessons to LearnJatinder Lachar, Amanda E. Gentry, Mariel Muriel Pastrana, Leroy R. Thacker, PuneetPuri, Arun J. Sanyal
Introduction: Intravenous albumin use is recommended with antibiotics on day 1 and day3 of diagnosis of spontaneous bacterial peritonitis (SBP) as it reduces renal impairment (RI)and mortality. However any deviation from this approach and its impact on SBP related RIin general clinical practice is not known. Our aim was to investigate SBP related renal andmortality outcomes in hospitalized patients with and without IV albumin use. Methods:Hospitalized subjects admitted with ascites in a tertiary care academic center from January2008-December 2010 were screened for SBP. The diagnosis of SBP was established by>250 ascitic fluid polymorphonuclear (PMN) cells. Demographic, clinical, biochemical andtreatment details including IV albumin use were collected. Renal impairment was definedusing acute kidney injury criteria of an increase in serum creatinine > 50% or ≥ 0.3 mg/dL from baseline labs in < 48 hours. For analysis, the subjects were classified following thediagnosis of SBP based on the pattern of IV albumin use as (1) no IV albumin (NIVA), (2)IV albumin on day 1 only (IVAD1), (3) IV albumin on day 3 only (IVAD3) and (4) IValbumin on both day 1 and day 3 (IVAD1+3). Statistical analysis using a logistic regressionmodel with group predicting renal dysfunction and adding dialysis as a potential cofounderwas used to evaluate the effects of IV albumin infusion with antibiotic therapy. Results: Of55 subjects that met the inclusion criteria, 15/55 (27%) had alcoholic cirrhosis and 31/55(56%) were males. The mean age was 51.89 years. At admission, 7% (4/55) of the patientswere undergoing hemodialysis secondary to end stage renal disease and the mean MELDscore was 16.16. Interestingly, IVAD1+3 subjects (n=20) when compared to all other groups{NIVA (n=15), IVAD1 (n=15), and IVAD3 (n=5)}, had a significant lower risk of RI betweenthe groups (χ2 = 6.79, p = 0.0221, OR = 0.24, 95% CI=(0.07, 0.85)), indicating that subjectswith IVAD1+3 were 4 times less likely to have RI (OR=4.24) than other groups. Adjustingfor dialysis by way of a multi-variable logistic regression, IVAD1+3 was still a significantpredictor of RI (p = 0.0284, OR = 0.24, 95% CI = (0.07, 0.86)); and 4 times more likelyto reduce RI than other groups. In contrast, in-hospital mortality rates were not significantlydifferent among the IVAD1+3 vs. other groups. Conclusions: IV albumin when used asrecommended is 4 times more likely to reduce renal impairment (RI) in cirrhotics with SBP.
AA
SL
DA
bst
ract
s