LQT3 Final Presentation
14
LQT Syndrome 3 GROUP 4 Matthew Argentieri Michelle Hung Susan Mathew Sweta Roy Yarden Segal Dikesh Shrestha
-
Upload
matthew-argentieri -
Category
Health & Medicine
-
view
725 -
download
2
Transcript of LQT3 Final Presentation

LQT Syndrome 3
GROUP 4Matthew Argentieri
Michelle HungSusan Mathew
Sweta RoyYarden Segal
Dikesh Shrestha

Background
• LQT3 is an autosomal dominant disease. – This mutation affects the inactivation gate of the
sodium channel and causes a gain of function of sodium current.
– Primary LQT3 mutation is ΔKPQ• ΔKPQ is the deletion of lysine, proline, and glutamine
between domains III and IV.

Background

• Arrhythmia
• Partial or total loss of consciousness
• Abdominal pain and GI complications
Symptoms
• Clinical features– Long ST
segments with a late appearing T wave
– Has QT >490+/-40 ms

Factors
• There was no voltage shift, no change in channel conductance, and no change in ionic concentrations.
• Changes in gate kinetics (time constants) and a new sustained inward current were the only factors discerning LQT3 from wild-type cells.

Time Constants
• Activation gate unaffected
• The time constants for the inactivation gates (fast and slow) changed.
– Wild Type• τ fast : 1.47 +/- 0.11 ms
• τ slow: 8.59 +/- 0.71 ms
– Mutant• τ fast : 0.98 +/- 0.07 ms
• τ slow: 5.40 +/- 0.55 ms

Approach
• Multiplied time constants by a scaling factor
– τfast : 66.67% (2/3)
– τslow : 62.86% (540/859)
• Altered steady-state inactivation curves (minimum probability of inactivation)
– Fast : 1%
– Slow: 3%

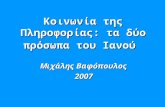
Modified Steady State Curves
BLUE CURVE: Modified fast inactivation steady state curve – levels out at 1% probability of being open (i.e. never reaches 0%)
RED CURVE: Modified slow inactivation steady state curve – levels out at 3% probability of being open (i.e. never reaches 0%)

MATLAB CODE
h_ss(index) = alpha_h/(alpha_h+beta_h);if h_ss(index) <=0.01h_ss(index) = 0.01; end
j_ss(index) = alpha_j/(alpha_j+beta_j); if j_ss(index) <=0.03j_ss(index) = 0.03; end
tau_h = 1.0/(alpha_h+beta_h)*(2/3);
tau_j = 1.0/(alpha_j+beta_j)*(540/859);

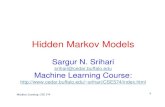
Preview of the GUI

Preview of the GUI
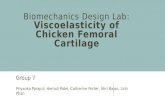
Normal Cardiomyocyte Action Potential
ΔKPQ Mutant Cardiomyocyte Action Potential

Conclusions
• Action potential duration is elongated due to longer repolarization – Increased time of repolarization due to
sustained inward sodium current– Diastolic Interval is reduced
• Time constants for LQT3 are smaller and cause faster inactivation
• Inactivation gates fail to remain inactivated– Leads to bursting mode current

THANK YOU!
Visit our educational website at:
http://mysbfiles.stonybrook.edu/~margentieri

References
• Baars, H. F., Smagt, J. J., & Doevendans, P. (2010). Clinical cardiogenetics. (1st ed., p. 149). Springer.
• Bankston, J., & Kass, R. (2010). Molecular determinants of local anesthetic action of beta-blocking drugs: Implications for therapeutic management of long qt syndrome variant 3. NIH Public Access
• Beinart, R., Michailidis, A., Gurevitz, O., & Gilkson, M. (2009). Is flecainide dangerous in long QT-3 patients? Journal compilation, 32, 143-145.
• Brisbane, J. (2006 (Updated 2009)). Acce review summary: The long qt-syndrome (lqts). Office of Population Health Genomics, Government of Western Australia, Department of Health.
• Moss, A., Windle , J., Hall, W., Zareba, W., Robinson, J., McNitt , S., Severski, P, Rosero, S, et al. (2005). Safety and efficacy of flecainide in subjects with long QT-3 syndrome (ΔKPQ mutation): A randomized, double-blind, placebo-controlled clinical trial. Annals of Noninvasive Electrocardiology, 10(4), 59-66.
• Ruan, Y., Liu, N., Napolitano, C., & Priori, S. (2008). Therapeutic strategies for Long-QT syndrome: Does the molecular substrate matter?. Circ Arrhythm Electrophysiol, 1, 290-297.
• Schwartz, P., Priori, S., Locati, E., Napolitano, C., Cantù, F., Towbin, J., Keating, M., & Hammoude, H, et al. (1995). Long QT syndrome patients with mutations of the
• SCN5A and HERG genes have differential responses to Na channel blockade and• to increases in heart rate. Circulation, (92), 3381-3386.• Sovari, A. (2012, January 10). Long QT syndrome. Retrieved from
http://emedicine.medscape.com/article/157826-overview• Wang , H., Zheng, Y., Yang, Z., Li , C., & Liu, Y. (2003). Effect of mexiletine on long• QT syndrome model. Chinese Pharmacological Society, 4, 316-320.