Isosteviol ameliorates diabetic cardiomyopathy in rats by ......groups (N =4–6/group) and...
14
https://doi.org/10.1530/JOE-17-0681 http://joe.endocrinology-journals.org © 2018 Society for Endocrinology Printed in Great Britain Published by Bioscientifica Ltd. Journal of Endocrinology 238:1 47–60 S-G Tang et al. Isosteviol attenuates diabetic cardiomyopathy RESEARCH Isosteviol ameliorates diabetic cardiomyopathy in rats by inhibiting ERK and NF-κB signaling pathways Sheng-Gao Tang 1 , Xiao-Yu Liu 1 , Ji-Ming Ye 2 , Ting-Ting Hu 1 , Ying-Ying Yang 1 , Ting Han 1 and Wen Tan 3 1 School of Bioscience and Bioengineering, South China University of Technology, Guangzhou, China 2 Molecular Pharmacology for Diabetes, School of Health and Biomedical Sciences, RMIT University, Melbourne, Victoria, Australia 3 Institute of Biomedical & Pharmaceutical Science, Guangdong University of Technology, Guangzhou, China Correspondence should be addressed to W Tan: [email protected] Abstract Diabetes-induced injury of myocardium, defined as diabetic cardiomyopathy (DCM), accounts for significant mortality and morbidity in diabetic population. Alleviation of DCM by a potent drug remains considerable interests in experimental and clinical researches because hypoglycemic drugs cannot effectively control this condition. Here, we explored the beneficial effects of isosteviol sodium (STVNa) on type 1 diabetes- induced DCM and the potential mechanisms involved. Male Wistar rats were induced to diabetes by injection of streptozotocin (STZ). One week later, diabetic rats were randomly grouped to receive STVNa (STZ/STVNa) or its vehicle (STZ). After 11 weeks of treatment or 11 weeks treatment following 4 weeks of removal of the treatment, the cardiac function and structure were evaluated and related mechanisms were investigated. In diabetic rats, oxidative stress, inflammation, blood glucose and plasma advanced glycation end products (AGEs) were significantly increased, whereas superoxide dismutase 2 (SOD-2) expression and activity were decreased. STVNa treatment inhibited cardiac hypertrophy, fibrosis and inflammation, showed similar ratio of heart to body weight and antioxidant capacities almost similar to the normal controls, which can be sustained at least 4 weeks. Moreover, STVNa inhibited diabetes- inducted stimulation of both extracellular signal-regulated kinase (ERK) and nuclear factor κB (NF-κB) signal pathways. However, blood glucose, plasma AGE and insulin levels were not altered by STVNa treatment. These results indicate that STVNa may be developed into a potent therapy for DCM. The mechanism underlying this therapeutic effect involves the suppression of oxidative stress and inflammation by inhibiting ERK and NF-κB without changing blood glucose or AGEs. Introduction Diabetic cardiomyopathy (DCM) induced by diabetes is increasingly recognized as the most important cause of elevated morbidity and mortality among diabetic patients (Chavali et al. 2013). DCM is characterized by abnormalities of structure and function of the left ventricle (LV), including hypertrophy and fibrosis, as well as diastolic and/or systolic contractile dysfunction. It is generally recognized that hyperglycemia-induced oxidative stress is a critical cause for this in diabetic complication. In fact, DCM is frequently accompanied Key Words f isosteviol f diabetic cardiomyopathy f oxidative stress f advanced glycation end products f extracellular signal- regulated kinase Journal of Endocrinology (2018) 238, 47–60 Downloaded from Bioscientifica.com at 07/06/2021 10:02:16PM via free access
Transcript of Isosteviol ameliorates diabetic cardiomyopathy in rats by ......groups (N =4–6/group) and...
-
https://doi.org/10.1530/JOE-17-0681http://joe.endocrinology-journals.org © 2018 Society for Endocrinology
Printed in Great BritainPublished by Bioscientifica Ltd.
Journal of Endocrinology
238:1 47–60S-G Tang et al. Isosteviol attenuates diabetic cardiomyopathy
-17-0681
RESEARCH
Isosteviol ameliorates diabetic cardiomyopathy in rats by inhibiting ERK and NF-κB signaling pathways
Sheng-Gao Tang1, Xiao-Yu Liu1, Ji-Ming Ye2, Ting-Ting Hu1, Ying-Ying Yang1, Ting Han1 and Wen Tan3
1School of Bioscience and Bioengineering, South China University of Technology, Guangzhou, China2Molecular Pharmacology for Diabetes, School of Health and Biomedical Sciences, RMIT University, Melbourne, Victoria, Australia3Institute of Biomedical & Pharmaceutical Science, Guangdong University of Technology, Guangzhou, China
Correspondence should be addressed to W Tan: [email protected]
Abstract
Diabetes-induced injury of myocardium, defined as diabetic cardiomyopathy (DCM),
accounts for significant mortality and morbidity in diabetic population. Alleviation
of DCM by a potent drug remains considerable interests in experimental and clinical
researches because hypoglycemic drugs cannot effectively control this condition. Here,
we explored the beneficial effects of isosteviol sodium (STVNa) on type 1 diabetes-
induced DCM and the potential mechanisms involved. Male Wistar rats were induced
to diabetes by injection of streptozotocin (STZ). One week later, diabetic rats were
randomly grouped to receive STVNa (STZ/STVNa) or its vehicle (STZ). After 11 weeks
of treatment or 11 weeks treatment following 4 weeks of removal of the treatment,
the cardiac function and structure were evaluated and related mechanisms were
investigated. In diabetic rats, oxidative stress, inflammation, blood glucose and
plasma advanced glycation end products (AGEs) were significantly increased, whereas
superoxide dismutase 2 (SOD-2) expression and activity were decreased. STVNa
treatment inhibited cardiac hypertrophy, fibrosis and inflammation, showed similar
ratio of heart to body weight and antioxidant capacities almost similar to the normal
controls, which can be sustained at least 4 weeks. Moreover, STVNa inhibited diabetes-
inducted stimulation of both extracellular signal-regulated kinase (ERK) and nuclear
factor κB (NF-κB) signal pathways. However, blood glucose, plasma AGE and insulin levels were not altered by STVNa treatment. These results indicate that STVNa may be
developed into a potent therapy for DCM. The mechanism underlying this therapeutic
effect involves the suppression of oxidative stress and inflammation by inhibiting ERK
and NF-κB without changing blood glucose or AGEs.
Introduction
Diabetic cardiomyopathy (DCM) induced by diabetes is increasingly recognized as the most important cause of elevated morbidity and mortality among diabetic patients (Chavali et al. 2013). DCM is characterized by abnormalities of structure and function of the left
ventricle (LV), including hypertrophy and fibrosis, as well as diastolic and/or systolic contractile dysfunction. It is generally recognized that hyperglycemia-induced oxidative stress is a critical cause for this in diabetic complication. In fact, DCM is frequently accompanied
1
Key Words
f isosteviol
f diabetic cardiomyopathy
f oxidative stress
f advanced glycation end products
f extracellular signal-regulated kinase
Journal of Endocrinology (2018) 238, 47–60
238
Downloaded from Bioscientifica.com at 07/06/2021 10:02:16PMvia free access
https://doi.org/10.1530/JOE-17-0681mailto:[email protected]
-
https://doi.org/10.1530/JOE-17-0681http://joe.endocrinology-journals.org © 2018 Society for Endocrinology
Published by Bioscientifica Ltd.Printed in Great Britain
48Isosteviol attenuates diabetic cardiomyopathy
S-G Tang et al. 238:1Journal of Endocrinology
with elevated formation of reactive oxygen species (ROS) (Nishikawa et al. 2000, Haidara et al. 2006) and reduced endogenous antioxidant capacity to clear the excessive ROS (Maritim et al. 2003). Increased ROS exacerbate cardiac inflammation and fibrotic remodeling (Rajesh et al. 2009, Huynh et al. 2013). Additionally, hyperglycemia-induced glycation of proteins, lipids and nucleic acids can generate advanced glycation end products (AGEs). AGEs interact with its receptors (RAGEs) to affect the intracellular signaling pathways, produce free radicals and release pro-inflammatory cytokines (Ma et al. 2009, Bodiga et al. 2014). It has been suggested that extracellular signal-regulated kinase (ERK) and nuclear factor κB (NF-κB) are the key mediators activated by AGEs–RAGEs interaction (Barlovic et al. 2011) to promote the pathophysiological process of DCM (Lorenzo et al. 2011, Xu et al. 2016).
Despite extensive studies in the past decade, the exact mechanisms of hyperglycemia causing DCM are not fully demonstrated (Dobrin & Lebeche 2010, Liu et al. 2014), and there are no effective therapies for this serious condition. Stevioside as well as the analog isosteviol, components of Stevia rebaudiana leaf, whose toxicology and safety were fully investigated, were used as safe conventional noncaloric sweeteners for hundreds of years (Brahmachari et al. 2011). Several researches have shown the anti-type 2 diabetic and cardioprotective effects of isosteviol and related compounds (Ma et al. 2007, Xu et al. 2007). Isosteviol sodium (STVNa) is an improved formulation with higher solubility and bioavailability (Lai et al. 2017), which has been shown by our laboratory to have the ability to alleviate cerebral ischemia injuries (Hu et al. 2016) and ischemia reperfusion-induced mitochondrial dysfunction in vitro (Sun et al. 2017). However, the effects of isosteviol and/or related compounds on DCM have not been investigated.
Since hyperglycemia and AGE-RAGE-stimulated ERK and NF-κB signal pathways play important roles in the formation of oxidative stress and development of DCM, and a previous study showed that isosteviol could improve glucose tolerance (Ma et al. 2007), we hypothesized that STVNa could depress blood glucose, AGEs and inhibit ERK and NF-κB, further attenuate diabetes-induced cardiac injuries and dysfunctions and activate endogenous antioxidant mechanisms. The present study evaluated: (1) whether STVNa could ameliorate or inhibit the development and progression of type 1 diabetes-induced cardiac dysfunction; (2) whether the potential effect of STVNa was related to anti-hyperglycemia and/or AGE-RAGE/ERK/NF-κB inhibiting effects; (3) was there any memory of cardioprotection after stopping the treatment.
Materials and methods
Animals and treatment
The study was performed according to the Guide for the Care and Use of Laboratory Animals published by the US National Institutes of Health (NIH Publication No. 82-23, revised 1996) and was reviewed and approved by the Institutional Animal Care and Use Committee of Sun Yat-sen University. Male Wistar (6- to 8-week-old) rats (N = 80; body weight (BW): 190–220 g) were purchased from the Experimental Animal Center of Sun Yat-sen University (Guangzhou, China) and housed 3–4/cage under 12/12-h light/darkness cycles, kept at constant room temperature of 22 ± 2°C with standard laboratory rat diet and water provided ad libitum. Streptozotocin (STZ; Sigma) was freshly prepared by dissolving it in 0.1 M citrate buffer (pH = 4.5). The rats were fasted overnight after one week of acclimatization, diabetes were induced by single i.p. injection of STZ (55 mg/kg BW). Control animals received an equivalent volume of citrate buffer. One week later, the blood glucose concentrations were measured using a glucometer (AccuSoft) and glucose test strips (Accu-Chek Advantage; Roche Diagnostics), the rats with hyperglycemia (≥11.1 mmol/L) were considered as diabetic and allowed to be assigned to diabetic with or without treatment groups.
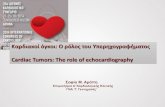
After one week of citrate buffer (Normal control group, N = 10) or STZ injection (N = 40), animals with diabetes (N = 32) successfully induced were randomly assigned into solvent treatment (STZ, N = 16) and STVNa treatment (STZ/STVNa, N = 16). All rats except normal group started treatment accordingly for 11 weeks (total for 12 weeks), cardiac function was measured for 25 rats (N = 5, 10, 10 for each group) and then killed, 17 rats (N = 5, 6, 6 for each group) were further fed without any treatment for another 4 weeks (total for 16 weeks), and cardiac function was measured and killed. The oral dose of STVNa (dissolved in normal saline solvent) was 8 mg/kg/day (twice daily), which optimized by our researches about STVNa on pressure overload induced cardiac hypertrophy (unpublished) and doses previously shown to be neuroprotective in rats (Hu et al. 2016). Additionally, 22 rats were divided into Normal and STZ groups (N = 4–6/group) and sustained for 4 or 8 weeks to study the progress of the DCM. The above research design diagram is shown in Fig. 1. In addition, ten rats were divided into normal group (N = 5) and normal rats treated with STVNa group (N = 5) and sustained for 6 weeks to study the potential effects of STVNa on normal rats.
Downloaded from Bioscientifica.com at 07/06/2021 10:02:16PMvia free access
https://doi.org/10.1530/JOE-17-0681
-
https://doi.org/10.1530/JOE-17-0681http://joe.endocrinology-journals.org © 2018 Society for Endocrinology
Published by Bioscientifica Ltd.Printed in Great Britain
49
Research
S-G Tang et al. Isosteviol attenuates diabetic cardiomyopathy
238:1Journal of Endocrinology
Hemodynamic measurements
Cardiac function was measured in rats anesthetized with 3% pentobarbital sodium (40–50 mg/kg) as previously described (Pacher et al. 2008). Briefly, rats were sedated and mechanically ventilated, the hemodynamic function was recorded by inserting a SPR-838 micro tip catheter (Millar Instruments, Inc., Houston, TX, USA) equipped with MPCU-400 PV signal conditioning hardware into LV via the right carotid artery. LV diastolic and systolic functions were evaluated by assessment maximal rate of pressure rise and pressure fall (dP/dtmax and dP/dtmin), LV end diastolic pressure (LVEDP), LV end systolic pressure (LVESP), heart rate (HR) and mean arterial pressure (MAP) in each study group. The data were analyzed by LabChart software (Millar Instruments, Inc.; version 7.0).
Tissue collection and plasma analysis
After the hemodynamic analysis was performed, hearts were excised surgically and blood was collected and centrifuged to obtain plasma. Hearts were washed totally with ice-cold PBS to clear the blood. HW and BW were weighted and the ratios of HW to BW were calculated. Then, the ventricular portions of the heart were cut into 2 cm sections and fixed or snap frozen in liquid nitrogen for further experiments. Following excision of the heart, plasma was separated from blood collected from the chest cavity and stored at −80°C until use. Rat circulation tumor necrosis factor-α (TNF-α), interleukin-6 (IL-6), insulin and AGEs levels were measured in plasma from every sample by commercially available RATTNF-α, IL-6 and INSULIN ELISA kits (JissKang Biotech, Qingdao, China) and RAT Advanced Glycation End Products ELISA kit (SenBeiJia Biological, Nanjing, China) respectively following the manufacturer’s instructions. As an auxiliary method,
fluorescence measurements of AGEs were monitored using a luminescence spectrometer Berthold LB943 at excitation (ex) and emission (em) wavelengths of 370/440 nm for the total AGEs level, as previous described (Piwowar et al. 2008).
Histological and immunohistochemical evaluation
The ventricles were fixed in 10% formalin for at least 24 h, and then paraffin-embedded and were sectioned at 3 μm for routine staining with hematoxylin and eosin (H&E) to determine cardiomyocyte sizes, as well as 0.1% Sirius Red to measure LV fibrosis, as previously described (Ritchie et al. 2012). All histological analyses were performed by two investigators who had no knowledge of identities of the slides.
Cardiomyocyte cross-sectional areas were assessed by H&E staining of LVs. At least five fields were randomly selected at magnification of 400× containing the capillary profiles and nuclei of myocardium. Images of the heart sections were obtained by an Axisplus image-capturing system (Zeiss) and analyzed by Image-Pro Plus (Media Cybernetics, Bethesda, MD, USA). At least 50 cells per heart were chosen for analysis. For cardiac tissue fibrosis evaluation, cardiac sections were stained with Sirius Red (Huamaike Biotech, Beijing, China). Images were captured by the image-capturing system (Zeiss) at magnification of 200× and analyzed by Image-Pro Plus. The content of tissue fibrosis (expressed as the fibrotic area to the entire cross area) was averaged over all fields.
Immunohistochemical (IHC) analysis of 8-hydroxy-2′-deoxyguanosine (8-OHdG) or CD68 was performed with mouse monoclonal antibody against 8-OHdG (Santa Cruz; #sc-393871, 1:100) or CD68 (Santa Cruz; #sc-20060, 1:100) and a biotinylated goat anti-mouse IgG (Vector Laboratories, Burlingame, CA, USA) as described previously (Yamaleyeva et al. 2012) with some modifications. Briefly, the sections of each heart were dewaxed, hydrated with graded series of ethanol, and then treated with 0.3% H2O2 for 30 min. After washing with Tris buffered solution, the sections were blocked with goat serum to reduce nonspecific reactions and incubated with mouse monoclonal antibody against 8-OHdG or CD68 at 4°C, followed by incubation with biotinylated anti-mouse immunoglobulin for 30 min. The horseradish peroxidase-labeled streptavidin solution was added for 30 min. The peroxidase-binding sites and nuclears were visualized with DAB (Sigma-Aldrich) and hematoxylin, respectively. The density of positive staining was analyzed using Image-Pro Plus.
Figure 1Diagram of the study design for STZ-induced DCM and STVNa treatment. DCM, diabetic cardiomyopathy; STVNa, isosteviol sodium; STZ, streptozotocin.
Downloaded from Bioscientifica.com at 07/06/2021 10:02:16PMvia free access
https://doi.org/10.1530/JOE-17-0681
-
https://doi.org/10.1530/JOE-17-0681http://joe.endocrinology-journals.org © 2018 Society for Endocrinology
Published by Bioscientifica Ltd.Printed in Great Britain
50Isosteviol attenuates diabetic cardiomyopathy
S-G Tang et al. 238:1Journal of Endocrinology
Semi-quantitative PCR and real-time PCR for gene expression analysis
Cardiac tissues were frozen and stored at −80°C until use. Total RNA was extracted using TRIzol reagent (Generay Biotech, Shanghai, China). The concentrations of total RNA samples were determined by NanoDrop ND-2000c spectrophotometer (Thermo Fisher Scientific, Inc.), and agarose gel electrophoresis was used to confirm the purities. First-strand cDNAs were synthesized with 1 μg total RNA in a 20 μL reaction system using RevertAid First Strand cDNA Synthesis Kit (Thermo Fisher Scientific) according to the manufacturer’s protocol.
The levels of gene were determined by semi-quantitative PCR first. The primers, whose sequences were listed in Supplementary Table 1 (see section on supplementary data given at the end of this article), were synthesized by Generay Biotech. The PCR reactions were performed with a 20 μL solution containing 10 μL MasterMix (universal PCR mix solution, Generay), 1 μL cDNA, 2 μL primer (1 μL for forward and reverse, respectively) and 7 μL water, using the ABI 2720 Thermocycler (Life Technologies Corp.). In order to ensure the amplification was within the logarithmic phase, the number of PCR cycles of every gene was optimized. PCR products were resolved on a 1.2–1.5% agarose gel. The intensity of the target gene was calculated using Image Pro Plus (Media Cybernetics) and expressed as fold changes normalized by internal gene control beta actin (Actb). Each experiment was performed in duplicate or triplicate.
The expression of Nppb (BNP), Tgfb1 (TGF-β1), p47 phox, Sod2, interleukin 1-beta (IL-1β) and advanced glycosylation end product-specific receptor (Ager) were confirmed by real-time PCR using SYBR Green PCR Premix HS Taq (Genview, Beijing, China) in the Applied Biosystems Prism 7500 Fast real-time PCR system. The cycling conditions were: 1 cycle of 30 s at 95°C followed by 40 cycles of 15 s at 95°C and 30 s at 60°C. Each RNA sample was analyzed in duplicate. The relative amounts of mRNA were determined by ΔΔCt method with normalization to Actb.
Measurements of total anti-oxidative capacity, SOD activity, total GSH content and malondialdehyde content
Proteins of the heart were collected according to the guidelines of manufacturer (Nanjing Jiancheng Chemical Co, Nanjing, China) and the concentrations were determined by BCA assay (Pierce). Total antioxidant capacity (T-AOC) and SOD activity from tissue were Ta
ble
1
Car
dia
c fu
nct
ion
s o
f d
iab
etic
car
dio
myo
pat
hy
and
th
e th
erap
euti
c ef
fect
s o
f ST
VN
a.
4 w
eeks
8 w
eeks
12 w
eeks
16 w
eeks
(ST
4 w
eeks
)
No
rmal
STZ
(DM
)N
orm
alST
Z (D
M)
No
rmal
STZ
(DM
)ST
Z/ST
VN
aN
orm
alST
Z (D
M)
STZ/
STV
Na
Rat
s n
um
ber
44
66
510
104
66
Bo
dy
wei
gh
t (B
W)
292.
50 ±
12.
5021
7.00
± 1
6.06
**30
7.17
± 1
9.27
261.
30 ±
34.
43*
350.
67 ±
40.
7931
6.00
± 1
5.10
*34
2.60
± 2
9.83
431.
50 ±
53.
1233
2.17
± 1
6.59
**40
1.83
± 2
8.07
$$
HW
/BW
(m
g/g
)2.
85 ±
0.1
22.
99 ±
0.1
62.
74 ±
0.1
43.
23 ±
0.2
6**
2.78
± 0
.09
3.20
± 0
.16*
*3.
04 ±
0.1
0$2.
77 ±
0.1
13.
03 ±
0.0
9**
2.71
± 0
.07$
$$
LVED
P (m
mH
g)
2.83
± 2
.35
5.4
± 2
.20
6.78
± 1
.84
10.1
8 ±
2.2
9#2.
75 ±
0.9
67.
95 ±
3.7
7*3.
25 ±
1.3
3$$
1.94
± 0
.80
6.08
± 1
.39*
*3.
67 ±
1.7
0LV
ESP
(mm
Hg
)12
1.43
± 8
.21
115.
26 ±
18.
0812
4.69
± 1
1.41
112.
88 ±
17.
6013
9.34
± 7
.76
105.
58 ±
16.
38*
135.
35 ±
13.
55$$
140.
10 ±
7.6
011
3.93
± 1
8.56
*13
4.63
± 1
0.93
dP/
dt m
in
(mm
Hg
/s)
−11
260
± 8
83−
9062
± 1
850
−12
570
± 2
061
−85
97 ±
252
9*−
12,8
67 ±
185
6−
8044
± 2
308*
*−
11,0
71 ±
173
5$−
11,0
53 ±
113
7−
7689
± 2
700*
−13
,642
± 5
86$$
dP/
dt m
ax
(mm
Hg
/s)
11,8
06 ±
775
11,6
94 ±
140
210
,176
± 1
168
9034
± 1
579#
11,1
12 ±
548
8079
± 2
059*
,#12
,114
± 1
972$
$11
,955
± 1
517
8258
± 2
298*
,#11
,088
± 1
087
MA
P (m
mH
g)
120.
41 ±
8.0
210
9.67
± 9
.77
126.
53 ±
17.
1212
5.85
± 1
1.03
123.
33 ±
4.7
197
.17
± 1
5.12
*,@
@12
6.83
± 2
6.66
$11
5.15
± 4
.49
92.3
1 ±
16.
71*,
@@
115.
39 ±
9.1
4$
HR
(b
pm
)40
3.03
± 2
7.79
367.
73 ±
33.
5339
7.23
± 3
1.29
372.
85 ±
23.
4042
0.10
± 1
6.24
403.
54 ±
23.
40#,
@41
4.04
± 2
6.41
38
1.10
± 2
4.83
392.
80 ±
32.
7240
1.77
± 1
7.60
*, *
*P <
0.0
5 an
d P
< 0
.01
vs n
orm
al g
rou
p o
f th
e co
rres
po
nd
ing
wee
k; #
P <
0.0
5 vs
STZ
gro
up
of
4 w
eeks
; @, @
@P
< 0
.05
and
P <
0.0
1 vs
STZ
gro
up
of
8 w
eeks
; $, $
$, $
$$P
< 0
.05,
P <
0.0
1 an
d P
< 0
.001
vs
STZ
gro
up
of
the
corr
esp
on
din
g w
eek.
dP/
dt m
ax a
nd
dP/
dt m
in, m
axim
al r
ate
of
pre
ssu
re r
ise
and
pre
ssu
re f
all;
HR
, hea
rt r
ate;
HW
/BW
, hea
rt w
eig
ht-
to-b
od
y w
eig
ht
rati
o; L
VED
P, L
V e
nd
dia
sto
lic p
ress
ure
; LV
ESP,
LV
en
d s
ysto
lic p
ress
ure
; M
AP,
mea
n a
rter
ial p
ress
ure
; STV
Na,
iso
stev
iol s
od
ium
; STZ
, str
epto
zoto
cin
.
Downloaded from Bioscientifica.com at 07/06/2021 10:02:16PMvia free access
https://doi.org/10.1530/JOE-17-0681http://joe.endocrinology-journals.org/cgi/content/full/JOE-17-0681/DC1
-
https://doi.org/10.1530/JOE-17-0681http://joe.endocrinology-journals.org © 2018 Society for Endocrinology
Published by Bioscientifica Ltd.Printed in Great Britain
51
Research
S-G Tang et al. Isosteviol attenuates diabetic cardiomyopathy
238:1Journal of Endocrinology
determined by T-AOC (according to the redox potential of Fe3+-TPTZ) detection kit and SOD activity (WST-1 method) assay kit (Nanjing Jiancheng Chemical Co), respectively according to the manufacturer’s instructions. Enzyme activities were normalized to protein concentration in samples (U/mg protein). Intracellular total glutathione (GSH) was measured using a Total Glutathione Assay Kit (Beyotime, Nantong, China) following the manufacturer’s protocol. Malondialdehyde (MDA), a lipid peroxidation product, was measured using the Malondialdehyde Assay Kit (Beyotime) by thiobarbituric acid assay, which is based on thiobarbituric acid (TBA) reacted with MDA to produce thiobarbituric acid reactive substances. The content of GSH and MDA was normalized to protein concentration and expressed as μmol/mg protein and nmol/mg protein, respectively.
SDS-PAGE/Western blotting
The cardiac tissues were lysed in ice-cold RIPA buffer (Genview) containing 1 mM PMSF and 1× protease inhibitor cocktail (Roche) by 100 mg tissue/1 mL buffer.
The supernatant after centrifugation was collected and the protein concentration was determined by BCA method (Pierce). After separated by 10–12% sodium dodecyl sulfate-polyacrylamide gel electrophoresis (SDS-PAGE), the proteins were transferred to PVDF membrane (Millipore). The membrane was then blocked by 5% (w/v) nonfat milk in Tris-buffered saline with 0.1% Tween 20 at room temperature for 1 h. The primary antibodies, anti-collagen 1 (Abcam #ab7778, 1:1000), anti-collagen 3 (Abcam #ab34710, 1:1000), anti-RAGE (Santa Cruz #sc-365154, 1:1000), anti-phospho-ERK1/2 (CST #4370, 1:2000), anti-ERK1/2 (Abcam #196883, 1:2000), anti-Nuclear factor kappa B subunit p65 (NF-κB p65) anti-NF-κB p65 (ProteinTech #10745-1-AP, 1:1000) and anti-β-actin (CST #3700, 1:1000) were added to react with the proteins on the membrane overnight at 4°C. The membrane was then incubated with secondary HRP-conjugated antibody (Jackson, 1:3000) against primary antibodies at room temperature for 45 min. The bands were detected by ECL chemiluminescence kit (Pierce) and analyzed by ImageLab software (Bio-Rad).
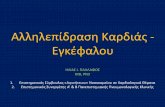
Figure 2Progression of diabetic cardiomyopathy induced by STZ. (A and B) The H&E staining showed cardiac hypertrophy developing process induced by diabetes. The hyperglycemia led to hypertrophy after 8 weeks of STZ injection and further deteriorated at 12 weeks. The scale bar in A represents 50 microns. (C and D) The fibrosis ratios of DCM and normal hearts at different time points (arrows indicated collagen deposition). The heart showed significant fibrosis after 8 weeks of STZ injection and deteriorated at 12 weeks. The scale bar in C represents 100 microns. **P < 0.01, ***P < 0.001 vs normal group of the corresponding week; ##, ###P < 0.01 and P < 0.001 vs STZ group of 4 weeks; $$, $$$P < 0.01 and P < 0.001 vs STZ group of 8 weeks. DCM, diabetic cardiomyopathy; H&E, hematoxylin and eosin; STZ, streptozotocin.
Downloaded from Bioscientifica.com at 07/06/2021 10:02:16PMvia free access
https://doi.org/10.1530/JOE-17-0681
-
https://doi.org/10.1530/JOE-17-0681http://joe.endocrinology-journals.org © 2018 Society for Endocrinology
Published by Bioscientifica Ltd.Printed in Great Britain
52Isosteviol attenuates diabetic cardiomyopathy
S-G Tang et al. 238:1Journal of Endocrinology
Statistical analysis
All data were presented as the mean ± s.d. P < 0.05 was considered as significant. Statistical significance was assessed firstly with one-way ANOVAs for comparisons among multiple groups. When significance existed, two-tailed Student’s t-test between two groups was performed. All statistical analyses were performed using Prism 6.0 GraphPad software (GraphPad).
Results
STZ-induced progressively development of DCM in rats
In order to demonstrate the dynamical process of DCM in rats, the changes of the morphology and cardiac function in rats following induction of diabetes were monitored at several time points. Compared with normal controls, diabetic rats showed cardiac dysfunction and myocardium hypertrophy from 8 weeks after STZ injection, with significant declines in LV diastolic function, increases in the HW/BW ratio (Table 1) and cardiomyocyte cell sizes (Fig. 2A and B). Meanwhile, diabetes significantly induced LV systolic dysfunction from 12 weeks after induction
of diabetes (Table 1). These results were consistent with the previous research showed that DCM characterized by diastolic dysfunction of LV followed by systolic dysfunctions later (Huynh et al. 2014). Furthermore, diabetic animals also had increased fibrosis after 8 weeks of STZ injection (Fig. 2C and D), which further aggravated at 12 and 16 weeks.
Cardiac dysfunction was reversed with STVNa treatment
At the end of animal study, cardiac functions were measured by hemodynamic methods. The results indicated that diabetes induced significant LV diastolic and systolic dysfunction after 12 weeks or 16 weeks of STZ injection. As shown in Table 1, the diabetic rats (STZ) showed an elevated LV end diastolic pressure (LVEDP) and weakened LV −dP/dtmin (indicators of impaired LV diastolic function) compared with normal rats. STVNa administration (STZ/STVNa) for 11 weeks inhibited impairments of LVEDP and −dP/dtmin induced by diabetes. Analysis of end point systolic function showed significantly decreased LVESP and dP/dtmax (indicators of impaired LV contractility) in diabetic rats, and STVNa treatment could attenuate these impairments. Meanwhile, STZ-injected
Figure 3STVNa attenuated STZ-induced cardiac hypertrophy. STVNa can inhibit diabetes-induced cardiomyopathy after treatment. (A) H&E staining of cardiac tissues with the magnification of 400× (the scale bar represents 50 microns). Diabetic hearts showed significant increased CSA (B) and hypertrophic biomarkers ANP and BNP (C and D). STVNa depressed cardiac hypertrophy, decreased the cardiomyocytes sizes and inhibited the expression of hypertrophic biomarkers. **, ***P < 0.01 and P < 0.001 vs normal group of the corresponding week; $, $$, $$$P < 0.05, P < 0.01 and P < 0.001 vs STZ group of the corresponding week; #, ##P < 0.05 and P < 0.01 vs STZ group of 12 weeks. CSA, cross-sectional area; DCM, diabetic cardiomyopathy; H&E, hematoxylin and eosin; STVNa, isosteviol sodium; STZ, streptozotocin.
Downloaded from Bioscientifica.com at 07/06/2021 10:02:16PMvia free access
https://doi.org/10.1530/JOE-17-0681
-
https://doi.org/10.1530/JOE-17-0681http://joe.endocrinology-journals.org © 2018 Society for Endocrinology
Published by Bioscientifica Ltd.Printed in Great Britain
53
Research
S-G Tang et al. Isosteviol attenuates diabetic cardiomyopathy
238:1Journal of Endocrinology
diabetic rats showed decreased MAP and STVNa can reverse this decrease, the heart rates were not changed by diabetes or drug treatment. More importantly, these cardioprotection trends of STVNa lasted at least 4 weeks even after stopping the treatment from the 12th week (16 weeks).
Cardiac hypertrophy was inhibited with STVNa treatment
After 12 weeks or 16 weeks of induction of diabetes, HW/BW ratios were increased in diabetes than normal control groups (Table 1). As shown in the H&E-stained hearts (Fig. 3A and B), cardiomyocyte cross-sectional areas (CSAs) were significantly increased in diabetes than normal groups. Meanwhile, the hypertrophic biomarkers, Nppa (ANP) and Nppb (BNP) mRNA expression were greatly enhanced in diabetic rats (Fig. 3C and D). STVNa treatments for 11 weeks or 11 weeks following 4 weeks without treatment could reverse the effects induced by
DCM, including alleviated cardiac hypertrophy and decreased expressions of Nppa and Nppb mRNAs.
Cardiac fibrotic remodeling was limited by STVNa administration
Diabetes induced significantly increasing in LV interstitial collagen deposition compared to normal rats (Fig. 4A and B). STVNa treatment ameliorated LV fibrosis significantly compared to diabetic rats. Gene expression of Tgfb1 and the downstream signal molecule Smad-3 were similarly elevated in diabetic rats and attenuated with STVNa treatment (Fig. 4C and D). Meanwhile, mRNA levels of collagen 1 (Col1a1) and collagen 3 (Col3a1), the fibrosis and extracellular matrix markers, were significantly increased in diabetic rats (Fig. 4C and D). As shown in Fig. 4E, both collagen 1 and 3 proteins showed trends of increasing in diabetic rats of 12 weeks (although without significance for collagen I, P = 0.058), which to some extent were attenuated by STVNa administration (P = 0.059 for
Figure 4STVNa attenuated STZ-induced cardiac fibrosis. (A) Sirius red staining to show the collagen deposition and the extent of cardiac fibrosis with the magnification of 200× (the scale bar represents 100 microns). (B) The fibrosis percentage of each group. The fibrotic percentage of diabetes rats increased significantly after 12 or 16 weeks of STZ injection, which were significantly mitigated by STVNa treatment. (C) The mRNA levels from each group detected by reverse transcriptase-polymerase chain reaction. (D) The fibrosis signal related genes mRNA expression of TGF-β1, Smad-3, collagen I and collagen III were significantly elevated by diabetes, which were repressed significantly by STVNa treatment. (E) The protein levels of collagen I and collagen III detected by SDS-PAGE/Western blotting. Collagen I and collagen III were elevated in 12-week-old diabetic rats and depressed by STVNa treatment. *, **, ***P < 0.05, P < 0.01 and P < 0.001 vs normal group of the corresponding week; $, $$, $$$P < 0.05, P < 0.01 and P < 0.001 vs STZ group of the corresponding week; #, ###P < 0.05 and P < 0.001 vs STZ group of 12 weeks. STVNa, isosteviol sodium; STZ, streptozotocin.
Downloaded from Bioscientifica.com at 07/06/2021 10:02:16PMvia free access
https://doi.org/10.1530/JOE-17-0681
-
https://doi.org/10.1530/JOE-17-0681http://joe.endocrinology-journals.org © 2018 Society for Endocrinology
Published by Bioscientifica Ltd.Printed in Great Britain
54Isosteviol attenuates diabetic cardiomyopathy
S-G Tang et al. 238:1Journal of Endocrinology
collagen I). STVNa administration significantly attenuated the diabetes-induced elevation in these markers of cardiac fibrosis, which could last at least 4 weeks.
STVNa-attenuated type 1 diabetes-induced cardiac tissue oxidative stress
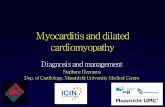
The total antioxidant capacity and total of glutathione (GSH) of cardiac tissues from diabetic rats of 12 weeks decreased significantly, which were reversed by STVNa treatment (Fig. 5A and B). The activity of SOD showed the same trends (P > 0.05, Fig. 5C). Meanwhile, type 1 diabetes markedly promoted LV MDA concentration (Fig. 5D) and NADPH oxidase expression, including increased NADPH oxidase 1 (Nox2) and p47 phox subunits mRNA content and declined expression of superoxide dismutase 2 (Sod2) (Fig. 5E and F), compared to nondiabetic normal rats. Moreover, IHC examinations confirmed the cardiac tissues of 12-week diabetic rats had significantly
elevated 8-OHdG (Fig. 5G and H), another marker of oxidative stress. All these molecular markers of oxidative stress were significantly inhibited by STVNa treatment.
STVNa ameliorated LV inflammation in type 1 diabetes
The expression of Il1b, a pro-inflammatory cytokine (Fig. 6A and B), was significantly upregulated after 12 or 16 weeks of STZ injection. The pro-inflammatory chemokines, including Ccl2 (MCP1), Vcam1, Vcam2 and Icam1 were elevated significantly in diabetic rats (Fig. 6A and B). Meanwhile, the concentration of TNF-α and IL-6 in plasma or cardiac tissues of 12-week-old diabetic rats were increased significantly (Fig. 6C and D). IHC staining showed that CD68, a macrophage cell marker, was notably increased in diabetic rats (Fig. 6E and F). All these inflammation biomarkers were significantly alleviated by treatment with STVNa (including suspending the treatment for 4 weeks) in diabetic rats.
Figure 5STVNa repressed STZ-induced cardiac oxidative stress. Oxidative stress in the myocardial tissues were determined by measuring (A) T-AOC, (B) total GSH content, (C) SOD activity and (D) MDA of 12-week-old diabetic rats, as described in the ‘Methods’ section, and the (E) NADPH oxidase subunits or SOD-2 mRNA expression by reverse transcriptase-PCR. (F) The quantification of the expression of SOD-2, p47phox and Nox-2 from rats of 12 weeks or 16 weeks after STZ injection, respectively. (G and H) IHC measurements of 8-OHdG with the magnification of 200× and 600× (the scale bar represents 100 and 50 microns respectively), which showed significantly augmented in diabetic rats and inhibited by STVNa. *, **, ***P < 0.05, P < 0.01 and P < 0.001 vs normal group of the corresponding week; $, $$, $$$P < 0.05, P < 0.01 and P < 0.001 vs STZ group of the corresponding week; ##, ###P < 0.01 and P < 0.001 vs STZ group of 12 weeks. 8-OHdG, 8-hydroxy-2′-deoxyguanosine; GSH, glutathione; IHC, immunohistochemical; MDA, malondialdehyde; SOD, superoxide dismutase; STVNa, isosteviol sodium; STZ, streptozotocin; T-AOC, total anti-oxidative stress capacity.
Downloaded from Bioscientifica.com at 07/06/2021 10:02:16PMvia free access
https://doi.org/10.1530/JOE-17-0681
-
https://doi.org/10.1530/JOE-17-0681http://joe.endocrinology-journals.org © 2018 Society for Endocrinology
Published by Bioscientifica Ltd.Printed in Great Britain
55
Research
S-G Tang et al. Isosteviol attenuates diabetic cardiomyopathy
238:1Journal of Endocrinology
The alleviation of DCM by STVNa is not related to anti-hyperglycemia, insulin restoration or AGE-RAGE inhibition
Diabetic rats showed elevation of blood glucose levels (Fig. 7A) along with decrease in the plasma insulin levels (Fig. 7B) after STZ injection (12 weeks). STVNa did not lower blood glucose or promote serum insulin levels. Moreover, ELISA and fluorescence methods showed that STZ-induced diabetes caused significant increase in plasma AGE levels compared to normal groups (Fig. 7C and D). However, STVNa did not decrease plasma AGE levels. Meanwhile, diabetes induced increases of the mRNA and protein levels of Ager (RAGE) after 12 weeks of STZ injection (Fig. 7E and F), which cannot be repressed by STVNa administration.
STVNa inhibited ERK1/2 phosphorylation and NF-κB stimulated by DCM
In order to demonstrate the mechanism of STVNa for its anti-inflammation and inhibition of oxidative stress, the related signal pathways were studied by Western blot.
As shown in Fig. 8, STZ-induced diabetic rats (12 weeks) showed significantly increased ERK1/2 phosphorylation (Thr 202/Tyr 204) correlated with elevated NF-κB p65 expression. STVNa-treated diabetic rats had significantly depressed the ERK1/2 and NF-κB pathways.
Effects of STVNa administration on normal rats
To investigate if there were any harmful effects of STVNa treatment on normal rats, we examined the HW/BW, BW increasing and marker genes expression of hypertrophy, fibrosis, oxidative stress and inflammation in cardiac tissues. As summarized in Fig. 9, after 6 weeks of administration of STVNa to normal rats, there were no significant differences between normal rats and rat administrated with STVNa.
Discussion
The present study investigated the effects of STVNa on DCM with an STZ-induced type-1 diabetic rats, a widely accepted animal model for the assessment of new drugs
Figure 6STVNa mitigated STZ-induced cardiac inflammation. (A) The mRNA levels from each group detected by reverse transcriptase-PCR. (B) The inflammatory signal-related genes mRNA expression of IL-1β, MCP-1, VACM-1 and ICAM-1 were significantly induced by diabetes, which were inhibited by STVNa treatment. The concentration of TNF-α and IL-6 of plasma (C) or cardiac tissue (D) were detected by ELISA. (E and F) IHC measurements of CD68 with the magnification of 200× and 600× (the scale bar represents 100 and 50 microns respectively), which was significantly promoted in diabetic rats and attenuated by STVNa. *, **, ***P < 0.05, P < 0.01 and P < 0.001 vs normal group of the corresponding week; $, $$, $$$P < 0.05, P < 0.01 and P < 0.001 vs STZ group of the corresponding week; #, ##P < 0.05 and P < 0.01 vs STZ group of 12 weeks. IHC, immunohistochemical; IL, interleukin; STVNa, isosteviol sodium; STZ, streptozotocin; TNF, tumor necrosis factor.
Downloaded from Bioscientifica.com at 07/06/2021 10:02:16PMvia free access
https://doi.org/10.1530/JOE-17-0681
-
https://doi.org/10.1530/JOE-17-0681http://joe.endocrinology-journals.org © 2018 Society for Endocrinology
Published by Bioscientifica Ltd.Printed in Great Britain
56Isosteviol attenuates diabetic cardiomyopathy
S-G Tang et al. 238:1Journal of Endocrinology
to treat DCM (Bugger & Abel 2009). Many diabetes patients develop cardiomyopathy or cardiac implications because of poor control of hyperglycemia. Once DCM is established, it cannot be easily treated with hypoglycemic drugs (Falcão-Pires & Leite-Moreira 2012). Isosteviol, derived from Stevia by hydrolysis of the β-glycoside, is a known compound but STVNa is an innovative pharmaceutical formulation suitable for injection, which greatly increased the oral bioavailability of isosteviol (Lai et al. 2017). In the present study, for the first time, we demonstrated that application of STVNa (11 weeks) prevented a multitude of cardiac complications of DCM including diastolic and systolic dysfunction, hypertrophy and fibrosis, accompanied with decreased inflammation and oxidative stress in STZ induced diabetic rats. Meanwhile, we discovered that the anti-cardiomyopathy effect of isosteviol was independent of AGE-RAGE levels, glucose lowering or increasing insulin content. More importantly, since ERK 1/2 and NF-κB signals were activated and played critical roles in the pathological processes of DCM, including stimulating hypertrophy, fibrosis and cell apoptosis (Rajesh et al. 2010, Singh et al. 2017), the compounds inactivating ERK1/2 and/or NF-κB would be very effective approaches, which were confirmed
by a few studies (Thomas et al. 2014, Chen et al. 2016, Dong et al. 2016). The present study firstly showed that the beneficial effects of STVNa on DCM were attributed to inhibition of ERK 1/2 and NF-κB signaling pathways, which would be of great clinic significance.
We set up two time points to evaluate the protective effects of STVNa on DCM rats, in which some rats were treated with STVNa for 11 weeks followed by non-treatment for 4 weeks. The diabetes-induced cardiac injuries were significantly attenuated for the 11 weeks by treatment with STVNa, which sustained for additional 4 weeks after the 11-week treatment. This memory of cardioprotection indicated a great therapeutic potential of our preparation of STVNa for cardiomyopathy in diabetes. More importantly, STVNa treatment did not alter relative HW and cardiac genes expression of hypertrophy, fibrosis, oxidative and inflammation in nondiabetic normal rats, suggesting these beneficial effects of STVNa were functional only under high fibrosis, oxidative stress and inflammation in the diabetes hearts.
DCM is a complex multifactorial pathological process characterized by early impairments in cardiac diastolic followed by systolic dysfunction (Boudina & Abel 2010), as well as notably structural abnormalities including
Figure 7Effects of STVNa on circulating levels of glucose, insulin and AGEs and RAGE expression in heart. (A) Diabetes-induced hyperglycemia and STVNa showed no any lowering effects on blood glucose level. (B) The plasma insulin levels of each group after 12 weeks of STZ injection. Insulin decreased significantly in diabetic group, STVNa had no effects on insulin concentration. ELISA (C) and fluorescence methods (D) showed that diabetes induced significant increase of advanced glycation end products in plasma after 12 weeks of STZ injection. STVNa did not show any effects on AGEs. (E) The mRNA expression and protein expression (F) of RAGE measured by semi-quantitative PCR was elevated in diabetic rats of 12 weeks, which cannot be reversed by STVNa administration. *, **, ***P < 0.05, P < 0.01 and P < 0.001 vs normal group. AGE, advanced glycation end product; RAGE, AGEs interact with its receptors; STVNa, isosteviol sodium; STZ, streptozotocin.
Downloaded from Bioscientifica.com at 07/06/2021 10:02:16PMvia free access
https://doi.org/10.1530/JOE-17-0681
-
https://doi.org/10.1530/JOE-17-0681http://joe.endocrinology-journals.org © 2018 Society for Endocrinology
Published by Bioscientifica Ltd.Printed in Great Britain
57
Research
S-G Tang et al. Isosteviol attenuates diabetic cardiomyopathy
238:1Journal of Endocrinology
cardiac hypertrophy and myocardial fibrosis (Asbun & Villarreal 2006). High intensity of oxidative stress and overwhelming inflammatory response play key roles in the pathogenesis of DCM, which can induce cardiac injuries and further lead to disturbance of extracellular matrix (ECM) homeostasis and collagen deposition in cardiac tissue (Falcão-Pires & Leite-Moreira 2012). Given the multi-factorial development and progression of DCM, an ideal therapy to prevent this disease should suppress cardiac hypertrophy, fibrosis, oxidative stress and inflammation. Currently, treatments specific for DCM patients were in urgent need. However, the traditional therapies including anti-diabetic agents cannot effectively target all deleterious aspects of this complex condition. Therefore, an alternative therapy inhibiting multiple pathological factors of DCM can be a potential supplement to meet the unmet medical need of this complication. The beneficial effects of STVNa against DCM of this study have never been reported. This innovative discovery is of great significance since cardiomyopathy, remodeling and failure are the major complications of diabetes, and no pharmaceutical treatment is available so far.
Interstitial fibrosis is a histological hallmark of DCM, accompanied with pathological hypertrophy of
cardiomyocytes as well as upregulation of Nppa/Nppb expression (Huynh et al. 2014, Mátyás et al. 2015). Our data demonstrated that STVNa had anti-hypertrophic and anti-fibrotic effects by histological methods (decreased cardiomyocyte size, cardiac fibrosis area) and molecular analysis (significantly reduced hypertrophic and fibrotic genes expression). Endothelial activation and increased monocyte adhesion molecules including Ccl2, Vcam1 and Vcam2, along with macrophage infiltration, represent the key early events that trigger vascular inflammation as a part of the pathophysiology of DCM (Potenza et al. 2009). Meanwhile, various studies showed that high glucose promoted NADPH oxidase subunits such as Nox2 and p47 phox expression, which increased or prolonged ROS production in response (Thallas-Bonke et al. 2008). Our data confirmed superoxide formation and significant inflammation responses in the cardiac tissue of diabetic rats. Moreover, increasing evidence indicated the enhanced ERK and NF-κB signaling pathways during DCM development with the promotion of much oxidative stress, inflammatory, hypertrophy and fibrosis factors (Rajesh et al. 2010, Gao et al. 2016, Singh et al. 2017). Our results showed that administration of STVNa did not depress AGEs, RAGEs and glucose, but efficiently inhibited DM-induced phosphorylation of ERK and NF-κB p65 expression. Therefore, STVNa treatment could ameliorate cardiac dysfunction in type 1 diabetes, attenuate cardiac hypertrophy and fibrosis, possibly by inhibiting the oxidative stress and inflammation-related ERK and NF-κB signal pathways rather than anti-hyperglycemic effects. However, besides glucose, the disturbance of free fatty acids (FFAs) metabolism plays a critical role in the development of DCM (Ritchie et al. 2017), and the expression of some genes related FFAs metabolism were altered in DCM (Inoue T et al. 2015). We will investigate the effects of STVNa on FFAs metabolism and related pathways in our future study.
In a previous study using Zucker diabetic fatty (ZDF) rats, administration of isosteviol at 5 and 10 mg/kg could significantly decrease the AUC of glucose during the intravenous glucose tolerance test (IVGTT), without any effect on plasma insulin concentration (Ma et al. 2007). Another team demonstrated in vivo acute anti-hyperglycemic effects of a series of novel isosteviol and derivatives (Chen et al. 2010). However, our study showed that STVNa treatment did not show any depression of hyperglycemia or AGEs in plasma. These differences may be probably due to different animal models. Insulin-dependent STZ-induced type 1 diabetes was used in our study while the type 2 diabetic Zucker rats are insulin
Figure 8STVNa inhibited STZ-induced activation of ERK1/2 and NF-κB signaling pathways. (A) Western blot to detect the phosphorylated and total ERK 1/2 as well as NF-κB p65 expression. The phosphorylated ERK 1/2 to total ERK1/2 (B) and the expression of NF-κB p65 (C) were increased significantly in diabetic rats, which were reversed by STVNa treatment. ***P < 0.001 vs normal group; $P < 0.05 vs STZ group. ERK, extracellular signal-regulated kinase; NF, nuclear factor; STVNa, isosteviol sodium; STZ, streptozotocin.
Downloaded from Bioscientifica.com at 07/06/2021 10:02:16PMvia free access
https://doi.org/10.1530/JOE-17-0681
-
https://doi.org/10.1530/JOE-17-0681http://joe.endocrinology-journals.org © 2018 Society for Endocrinology
Published by Bioscientifica Ltd.Printed in Great Britain
58Isosteviol attenuates diabetic cardiomyopathy
S-G Tang et al. 238:1Journal of Endocrinology
independent. Our study showed that STVNa could not promote insulin level of plasma, which is consistent with the previous study (Ma et al. 2007).
In addition, many previous studies of STZ-induced diabetic rats used various time spans from 2 to 24 weeks and showed different and inconsistent findings (Becher et al. 2013, Gupta et al. 2015, Harasiuk et al. 2016); therefore, the precise time course of DCM development is vital for elaborating and explaining varieties between findings. In the present study, we described the time course of DCM development, including the impairment in systolic and diastolic LV performance as well as cardiac hypertrophy and fibrosis over a long period of 4–16 weeks in diabetic Wistar rats, indicated by a progressive decrease in LV relaxation (from 8th week), contractility (from 12th week) and an increase in cardiac hypertrophy (from 8th week) and fibrosis (from 8th week).
In summary, the results presented here suggested that STVNa treatment was able to improve impaired cardiac function by attenuating hypertrophy and fibrosis as well as decreasing the oxidative stress, and inhibiting inflammatory responses, and the cardioprotective effects lasted at least 4 weeks after suspending of treatment. Meanwhile, the diabetes stimulated ERK and NF-κB signal pathways were inhibited by STVNa treatment. Therefore, STVNa, whose effects were not related to glucose lowering or AGE-RAGE inhibition, could be
pursued as a novel therapeutic approach specific to DCM. However, additional in vitro researches will be required to definitively identify molecular mechanisms of STVNa.
Conclusions
This study shows the efficacies of STVNa on DCM by prevention of cardiac dysfunction, restriction on cardiac hypertrophy and fibrosis, as well as inhibition of oxidative stress and inflammation. Moreover, our study shows that the cardioprotective mechanism of STVNa in STZ-induced type 1 diabetes is not dependent on alleviating hyperglycemia and inhibiting AGEs formation, but through inhibition of ERK and NF-κB signal pathways. To our knowledge, this is the first study demonstrating the anti-hypertrophic and anti-fibrotic effects of pharmacological STVNa on DCM type-1 diabetes.
Supplementary dataThis is linked to the online version of the paper at https://doi.org/10.1530/JOE-17-0681.
Declaration of interestThe authors declare that there is no conflict of interest that could be perceived as prejudicing the impartiality of the research reported.
Figure 9STVNa had no adverse effects in normal rats. (A) Heart weight to body weight of normal rats and normal rats administration of STVNa. (B) The body weight gaining during the test. (C) The hypertrophy, oxidative stress, inflammation and fibrosis signal related genes mRNA expression of ANP and BNP (D), TGF-β1 and Smad-3 (E), SOD-2 and Nox-2 (F), IL-1β and VACM-1 (G) were not changed after STVNa treatment. STVNa, isosteviol sodium; STZ, streptozotocin.
Downloaded from Bioscientifica.com at 07/06/2021 10:02:16PMvia free access
https://doi.org/10.1530/JOE-17-0681https://doi.org/10.1530/JOE-17-0681https://doi.org/10.1530/JOE-17-0681
-
https://doi.org/10.1530/JOE-17-0681http://joe.endocrinology-journals.org © 2018 Society for Endocrinology
Published by Bioscientifica Ltd.Printed in Great Britain
59
Research
S-G Tang et al. Isosteviol attenuates diabetic cardiomyopathy
238:1Journal of Endocrinology
FundingThis project was financed in part by the Fundamental Research Funds for the Central Universities (No. 2015ZM165); the Special Fund for Public Welfare Research and Capacity Building of Guangdong Province (2014B020210001); and The Major Scientific and Technological Project of Guangzhou Science and Technology Bureau (201300000051).
Author contribution statementProf. Tan and Ye conceived and directed the project. Sheng-Gao Tang and Xiao-Yu Liu directed rats diabetic cardiomyopathy and tissue analysis related studies. Sheng-Gao Tang designed the experiments of molecular biology. Sheng-Gao Tang and Ying-Ying Yang carried out biochemical and molecular biological experiments. Ting-Ting Hu helped analyze some data of the experiments. Ting Han helped animal care and treatments.
ReferencesAsbun J & Villarreal FJ 2006 The pathogenesis of myocardial fibrosis in
the setting of diabetic cardiomyopathy. Journal of the American College of Cardiology 47 693–700. (https://doi.org/10.1016/j.jacc.2005.09.050)
Barlovic DP, Soro-Paavonen A & Jandeleit-Dahm KA 2011 RAGE biology, atherosclerosis and diabetes. Clinical Science 121 43–55. (https://doi.org/10.1042/CS20100501)
Becher PM, Lindner D, Fröhlich M, Savvatis K, Westermann D & Tschöpe C 2013 Assessment of cardiac inflammation and remodeling during the development of streptozotocin-induced diabetic cardiomyopathy in vivo: a time course analysis. International Journal of Molecular Sciences 32 158–164. (https://doi.org/10.3892/ijmm.2013.1368)
Bodiga VL, Eda SR & Bodiga S 2014 Advanced glycation end products: role in pathology of diabetic cardiomyopathy. Heart Failure Reviews 19 49–63. (https://doi.org/10.1007/s10741-013-9374-y)
Boudina S & Abel ED 2010 Diabetic cardiomyopathy, causes and effects. Reviews in Endocrine and Metabolic Disorders 11 31–39. (https://doi.org/10.1007/s11154-010-9131-7)
Brahmachari G, Mandal LC, Roy R, Mondal S & Brahmachari AK 2011 Stevioside and related compounds – molecules of pharmaceutical promise: a critical overview. Archiv der Pharmazie 344 5–19. (https://doi.org/10.1002/ardp.201000181)
Bugger H & Abel ED 2009 Rodent models of diabetic cardiomyopathy. Disease Models and Mechanisms 2 454–466. (https://doi.org/10.1242/dmm.001941)
Chavali V, Tyagi SC & Mishra PK 2013 Predictors and prevention of diabetic cardiomyopathy. Diabetes, Metabolic Syndrome and Obesity 6 151–160. (https://doi.org/10.2147/DMSO.S30968)
Chen JQ, Zha XM, Sun M, Cai J, Zhou W & Ji M 2010 Synthesis and in vivo acute antihyperglycemic evaluation of novel isosteviol derivatives. Letters in Drug Design and Discovery 7 686–693. (https://doi.org/10.2174/157018010792929522)
Chen M, Li H, Wang G, Shen X, Zhao S & Su W 2016 Atorvastatin prevents advanced glycation end products (AGEs)-induced cardiac fibrosis via activating peroxisome proliferator-activated receptor gamma. Metabolism 65 441–453. (https://doi.org/10.1016/j.metabol.2015.11.007)
Dobrin JS & Lebeche D 2010 Diabetic cardiomyopathy: signaling defects and therapeutic approaches. Expert Review of Cardiovascular Therapy 8 373–391. (https://doi.org/10.1586/erc.10.17)
Dong WQ, Chao M, Lu QH, Chai WL, Zhang W, Chen XY, Liang ES, Wang LB, Tian HL, Chen YG, et al. 2016 Prohibitin overexpression improves myocardial function in diabetic cardiomyopathy. Oncotarget 7 66–80. (https://doi.org/10.18632/oncotarget.6384)
Falcão-Pires I & Leite-Moreira AF 2012 Diabetic cardiomyopathy: understanding the molecular and cellular basis to progress in diagnosis and treatment. Heart Failure Reviews 17 325–344. (https://doi.org/10.1007/s10741-011-9257-z)
Gao Y, Kang L, Li C, Wang X, Sun C, Li Q, Liu R & Wang J 2016 Resveratrol ameliorates diabetes-induced cardiac dysfunction through AT1R-ERK/p38 MAPK signaling pathway. Cardiovascular Toxicology 16 130–137. (https://doi.org/10.1007/s12012-015-9321-3)
Gupta SK, Dongare S, Mathur R, Mohanty IR, Srivastava S, Mathur S & Nag TC 2015 Genistein ameliorates cardiac inflammation and oxidative stress in streptozotocin-induced diabetic cardiomyopathy in rats. Molecular and Cellular Biochemistry 408 63–72. (https://doi.org/10.1007/s11010-015-2483-2)
Haidara MA, Yassin HZ, Rateb M, Ammar H & Zorkani MA 2006 Role of oxidative stress in development of cardiovascular complications in diabetes mellitus. Current Vascular Pharmacology 4 215–227. (https://doi.org/10.2174/157016106777698469)
Harasiuk D, Baranowski M, Zabielski P, Chabowski A & Górski J 2016 Liver X receptor agonist TO901317 prevents diacylglycerols accumulation in the heart of streptozotocin-diabetic rats. Cellular Physiology and Biochemistry 39 350–359. (https://doi.org/10.1159/000445629)
Hu H, Sun Xo, Tian F, Zhang H, Liu Q & Tan W 2016 Neuroprotective effects of isosteviol sodium injection on acute focal cerebral ischemia in rats. Oxidative Medicine and Cellular Longevity 2016 1379162. (https://doi.org/10.1155/2016/1379162)
Huynh K, Kiriazis H, Du XJ, Love JE, Gray SP, Jandeleit-Dahm KA, McMullen JR & Ritchie RH 2013 Targeting the upregulation of reactive oxygen species subsequent to hyperglycemia prevents type 1 diabetic cardiomyopathy in mice. Free Radical Biology and Medicine 60 307–317. (https://doi.org/10.1016/j.freeradbiomed.2013.02.021)
Huynh K, Bernardo BC, McMullen JR & Ritchie RH 2014 Diabetic cardiomyopathy: mechanisms and new treatment strategies targeting antioxidant signaling pathways. Pharmacology and Therapeutics 142 375–415. (https://doi.org/10.1016/j.pharmthera.2014.01.003)
Inoue T, Inoguchi T, Sonoda N, Hendarto H, Makimura H, Sasaki S, Yokomizo H, Fujimura Y, Miura D & Takayanagi R 2015 GLP-1 analog liraglutide protects against cardiac steatosis, oxidative stress and apoptosis in streptozotocin-induced diabetic rats. Atherosclerosis 240 250–259. (https://doi.org/10.1016/j.atherosclerosis.2015.03.026)
Lai W, Kang Q, Zou C, Li Q, Sun H & Tan W 2017 Development of a liquid formulation of poorly water-soluble isosteviol sodium using the co-solvent technology. Pharmaceutical Development and Technology 22 275–282. (https://doi.org/10.1080/10837450.2016.1226900)
Liu Q, Wang SD & Cai L 2014 Diabetic cardiomyopathy and its mechanisms: role of oxidative stress and damage. Journal of Diabetes Investigation 5 623–634. (https://doi.org/10.1111/jdi.12250)
Lorenzo O, Picatoste B, Ares-Carrasco S, Ramírez E, Egido J & Tuñón J 2011 Potential role of nuclear factor κB in diabetic cardiomyopathy. Mediators of Inflammation 2011 652097. (https://doi.org/10.1155/2011/652097)
Mátyás C, Németh BT, Oláh A, Hidi L, Birtalan E, Kellermayer D, Ruppert M, Korkmaz-Icöz S, Kökény G, Horváth EM, et al. 2015 The soluble guanylate cyclase activator cinaciguat prevents cardiac dysfunction in a rat model of type-1 diabetes mellitus. Cardiovascular Diabetology 14 145. (https://doi.org/10.1186/s12933-015-0309-x)
Ma J, Ma Z, Wang J, Milne RW, Xu D, Davey AK & Evans AM 2007 Isosteviol reduces plasma glucose levels in the intravenous glucose tolerance test in Zucker diabetic fatty rats. Diabetes, Obesity and Metabolism 9 597–599. (https://doi.org/10.1111/j.1463-1326.2006.00630.x)
Ma H, Li SY, Xu P, Babcock SA, Dolence EK, Brownlee M, Li J & Ren J 2009 Advanced glycation endproduct (AGE) accumulation and AGE receptor (RAGE) up-regulation contribute to the onset of diabetic cardiomyopathy. Journal of Cellular and Molecular Medicine 13 1751–1764. (https://doi.org/10.1111/j.1582-4934.2008.00547.x)
Downloaded from Bioscientifica.com at 07/06/2021 10:02:16PMvia free access
https://doi.org/10.1530/JOE-17-0681https://doi.org/10.1016/j.jacc.2005.09.050https://doi.org/10.1042/CS20100501https://doi.org/10.1042/CS20100501https://doi.org/10.3892/ijmm.2013.1368https://doi.org/10.3892/ijmm.2013.1368https://doi.org/10.1007/s10741-013-9374-yhttps://doi.org/10.1007/s11154-010-9131-7https://doi.org/10.1007/s11154-010-9131-7https://doi.org/10.1002/ardp.201000181https://doi.org/10.1002/ardp.201000181https://doi.org/10.1242/dmm.001941https://doi.org/10.1242/dmm.001941https://doi.org/10.2147/DMSO.S30968https://doi.org/10.2174/157018010792929522https://doi.org/10.2174/157018010792929522https://doi.org/10.1016/j.metabol.2015.11.007https://doi.org/10.1016/j.metabol.2015.11.007https://doi.org/10.1586/erc.10.17https://doi.org/10.18632/oncotarget.6384https://doi.org/10.1007/s10741-011-9257-zhttps://doi.org/10.1007/s10741-011-9257-zhttps://doi.org/10.1007/s12012-015-9321-3https://doi.org/10.1007/s11010-015-2483-2https://doi.org/10.1007/s11010-015-2483-2https://doi.org/10.2174/157016106777698469https://doi.org/10.2174/157016106777698469https://doi.org/10.1159/000445629https://doi.org/10.1159/000445629https://doi.org/10.1155/2016/1379162https://doi.org/10.1016/j.freeradbiomed.2013.02.021https://doi.org/10.1016/j.pharmthera.2014.01.003https://doi.org/10.1016/j.atherosclerosis.2015.03.026https://doi.org/10.1080/10837450.2016.1226900https://doi.org/10.1111/jdi.12250https://doi.org/10.1155/2011/652097https://doi.org/10.1155/2011/652097https://doi.org/10.1186/s12933-015-0309-xhttps://doi.org/10.1111/j.1463-1326.2006.00630.xhttps://doi.org/10.1111/j.1463-1326.2006.00630.xhttps://doi.org/10.1111/j.1582-4934.2008.00547.x
-
https://doi.org/10.1530/JOE-17-0681http://joe.endocrinology-journals.org © 2018 Society for Endocrinology
Published by Bioscientifica Ltd.Printed in Great Britain
60Isosteviol attenuates diabetic cardiomyopathy
S-G Tang et al. 238:1Journal of Endocrinology
Maritim AC, Sanders RA & Watkins JB 3rd 2003 Diabetes, oxidative stress, and antioxidants: a review. Journal of Biochemical and Molecular Toxicology 17 24–38. (https://doi.org/10.1002/jbt.10058)
Nishikawa T, Edelstein D, Du XL, Yamagishi S, Matsumura T, Kaneda Y, Yorek MA, Beebe D, Oates PJ, Hammes HP, et al. 2000 Normalizing mitochondrial superoxide production blocks three pathways of hyperglycaemic damage. Nature 404 787–790. (https://doi.org/10.1038/35008121)
Pacher P, Nagayama T, Mukhopadhyay P, Bátkai S & Kass DA 2008 Measurement of cardiac function using pressure-volume conductance catheter technique in mice and rats. Nature Protocols 3 1422–1434. (https://doi.org/10.1038/nprot.2008.138)
Piwowar A, Knapik-Kordecka M, Szczecińska J & Warwas M 2008 Plasma glycooxidation protein products in type 2 diabetic patients with nephropathy. Diabetes/Metabolism Research and Reviews 24 549–553. (https://doi.org/10.1002/dmrr.885)
Potenza MA, Gagliardi S, Nacci C, Carratu’ MR & Montagnani M 2009 Endothelial dysfunction in diabetes: from mechanisms to therapeutic targets. Current Medicinal Chemistry 16 94–112. (https://doi.org/10.2174/092986709787002853)
Rajesh M, Mukhopadhyay P, Bátkai S, Mukhopadhyay B, Patel V, Haskó G, Szabó C, Mabley JG, Liaudet L & Pacher P 2009 Xanthine oxidase inhibitor allopurinol attenuates the development of diabetic cardiomyopathy. Journal of Cellular and Molecular Medicine 13 2330–2341. (https://doi.org/10.1111/j.1582-4934.2008.00564.x)
Rajesh M, Mukhopadhyay P, Bátkai S, Patel V, Saito K, Matsumoto S, Kashiwaya Y, Horváth B, Mukhopadhyay B, Becker L, et al. 2010 Cannabidiol attenuates cardiac dysfunction, oxidative stress, fibrosis, and inflammatory and cell death signaling pathways in diabetic cardiomyopathy. Journal of the American College of Cardiology 56 2115–2125. (https://doi.org/10.1016/j.jacc.2010.07.033)
Ritchie RH, Love JE, Huynh K, Bernardo BC, Henstridge DC, Kiriazis H, Tham YK, Sapra G, Qin C, Cemerlang N, et al. 2012 Enhanced phosphoinositide 3-kinase (p110 α) activity prevents diabetes-induced cardiomyopathy and superoxide generation in a mouse model of diabetes. Diabetologia 55 3369–3381. (https://doi.org/10.1007/s00125-012-2720-0)
Ritchie RH, Zerenturk EJ, Prakoso D & Calkin AC 2017 Lipid metabolism and its implications for type 1 diabetes-associated cardiomyopathy. Journal of Molecular Endocrinology 58 R225–R240. (https://doi.org/10.1530/JME-16-0249)
Singh GB, Raut SK, Khanna S, Kumar A, Sharma S, Prasad R & Khullar M 2017 MicroRNA-200c modulates DUSP-1 expression in diabetes-induced cardiac hypertrophy. Molecular and Cellular Biochemistry 424 1–11. (https://doi.org/10.1007/s11010-016-2838-3)
Sun X, Yang Y, Xie Y, Shi X, Huang L & Tan W 2017 Protective role of STVNa in myocardial ischemia reperfusion injury by inhibiting mitochondrial fission. Oncotarget 9 1898–1905. (https://doi.org/10.18632/oncotarget.22969)
Thallas-Bonke V, Thorpe SR, Coughlan MT, Fukami K, Yap FY, Sourris KC, Penfold SA, Bach LA, Cooper ME & Forbes JM 2008 Inhibition of NADPH oxidase prevents advanced glycation end product-mediated damage in diabetic nephropathy through a protein kinase C-alpha-dependent pathway. Diabetes 57 460–469. (https://doi.org/10.2337/db07-1119)
Thomas CM, Yong QC, Rosa RM, Seqqat R, Gopal S, Casarini DE, Jones WK, Gupta S, Baker KM & Kumar R 2014 Cardiac-specific suppression of NF-κB signaling prevents diabetic cardiomyopathy via inhibition of the renin-angiotensin system. American Journal of Physiology: Heart and Circulatory Physiology 307 H1036–H1045. (https://doi.org/10.1152/ajpheart.00340.2014.)
Xu D, Li Y, Wang J, Davey AK, Zhang S & Evans AM 2007 The cardioprotective effect of isosteviol on rats with heart ischemia-reperfusion injury. Life Sciences 80 269–274. (https://doi.org/10.1016/j.lfs.2006.09.008)
Xu Z, Sun J, Tong Q, Lin Q, Qian L, Park Y & Zheng Y 2016 The role of ERK1/2 in the development of diabetic cardiomyopathy. International Journal of Molecular Sciences 17 E2001. (https://doi.org/10.3390/ijms17122001)
Yamaleyeva LM, Lindsey SH, Varagic J, Zhang LL, Gallagher PE, Chen AF & Chappell MC 2012 Amelioration of renal injury and oxidative stress by the nNOS inhibitor L-VNIO in the salt-sensitive mRen2.Lewis congenic rat. Journal of Cardiovascular Pharmacology 59 529–538. (https://doi.org/10.1097/FJC.0b013e31824dd15b)
Received in final form 14 March 2018Accepted 16 April 2018Accepted Preprint published online 2 May 2018
Downloaded from Bioscientifica.com at 07/06/2021 10:02:16PMvia free access
https://doi.org/10.1530/JOE-17-0681https://doi.org/10.1002/jbt.10058https://doi.org/10.1038/35008121https://doi.org/10.1038/35008121https://doi.org/10.1038/nprot.2008.138https://doi.org/10.1002/dmrr.885https://doi.org/10.2174/092986709787002853https://doi.org/10.2174/092986709787002853https://doi.org/10.1111/j.1582-4934.2008.00564.xhttps://doi.org/10.1016/j.jacc.2010.07.033https://doi.org/10.1007/s00125-012-2720-0https://doi.org/10.1007/s00125-012-2720-0https://doi.org/10.1530/JME-16-0249https://doi.org/10.1530/JME-16-0249https://doi.org/10.1007/s11010-016-2838-3https://doi.org/10.18632/oncotarget.22969https://doi.org/10.18632/oncotarget.22969https://doi.org/10.2337/db07-1119https://doi.org/10.2337/db07-1119https://doi.org/10.1152/ajpheart.00340.2014.https://doi.org/10.1016/j.lfs.2006.09.008https://doi.org/10.1016/j.lfs.2006.09.008https://doi.org/10.3390/ijms17122001https://doi.org/10.3390/ijms17122001https://doi.org/10.1097/FJC.0b013e31824dd15b
AbstractIntroductionMaterials and methodsAnimals and treatmentHemodynamic measurementsTissue collection and plasma analysisHistological and immunohistochemical evaluationSemi-quantitative PCR and real-time PCR for gene expression analysisMeasurements of total anti-oxidative capacity, SOD activity, total GSH content and malondialdehyde contentSDS-PAGE/Western blottingStatistical analysis
ResultsSTZ-induced progressively development of DCM in ratsCardiac dysfunction was reversed with STVNa treatmentCardiac hypertrophy was inhibited with STVNa treatmentCardiac fibrotic remodeling was limited by STVNa administrationSTVNa-attenuated type 1 diabetes-induced cardiac tissue oxidative stressSTVNa ameliorated LV inflammation in type 1 diabetesThe alleviation of DCM by STVNa is not related to anti-hyperglycemia, insulin restoration or AGE-RAGE inhibitionSTVNa inhibited ERK1/2 phosphorylation and NF-κB stimulated by DCMEffects of STVNa administration on normal rats
DiscussionConclusionsSupplementary dataDeclaration of interestFundingAuthor contribution statementReferences




![· Web viewfollowed by reduced risk of disease deterioration [11–13]. However, only . a small portion of. HBeAg-negative patients achieve sustained response when treated with](https://static.fdocument.org/doc/165x107/5eae10bc3ad54c1225494ffa/web-view-followed-by-reduced-risk-of-disease-deterioration-11a13-however-only.jpg)