INVESTIGATOR’S BROCHURE (VERSION 12.0, 16 … 031-2101-09: ... Completed Clinical Trials by Age...
130
Teplizumab MacroGenics, Inc. Investigator's Brochure Version 12.0, 16 November 2016 INVESTIGATOR’S BROCHURE Product Name: Teplizumab [MGA031, hOKT3γ1(ala,ala)] Sponsor: MacroGenics, Inc. 9704 Medical Center Drive Rockville, Maryland 20850 USA Telephone: 301-251-5172 Release Date: 16 November 2016 Version: Version 12.0 Supersedes version: 11.0, dated 05 April 2016 Confidentiality Statement The information contained in this document is the property of MacroGenics, Inc. It is provided in confidence by MacroGenics to the Investigator, potential Investigator, or consultant for review. This document and its contents may only be shared with the Investigator’s team and the appropriate institutional review board and/or independent ethics committee. Confidential Page 1 of 130
Transcript of INVESTIGATOR’S BROCHURE (VERSION 12.0, 16 … 031-2101-09: ... Completed Clinical Trials by Age...

Teplizumab MacroGenics, Inc.
Investigator's Brochure Version 12.0, 16 November 2016
INVESTIGATOR’S BROCHURE
Product Name: Teplizumab [MGA031, hOKT3γ1(ala,ala)]
Sponsor: MacroGenics, Inc. 9704 Medical Center Drive Rockville, Maryland 20850 USA Telephone: 301-251-5172
Release Date: 16 November 2016
Version: Version 12.0
Supersedes version: 11.0, dated 05 April 2016
Confidentiality Statement
The information contained in this document is the property of MacroGenics, Inc. It is provided in confidence by MacroGenics to the Investigator, potential Investigator, or consultant for review. This document and its contents may only be shared with the Investigator’s team and the appropriate institutional review board and/or independent ethics committee.
Confidential Page 1 of 130

Teplizumab MacroGenics, Inc.
Investigator's Brochure Version 12.0, 16 November 2016
SUMMARY OF CHANGES FROM PREVIOUS VERSION (VERSION 11.0)
Summary of Major Changes for Teplizumab Investigator's Brochure Version 12; Data Cut-off: 23 August 2016
Section Summary of Changes
1. summary The summary of safety and the number of treated subjects was updated for the “TN-10 At-Risk” study. Modifications were made consistent with the Section 6.7 update: previously included non-serious adverse drug reactions (ADRs) were removed and only serious ADRs retained.
2. Introduction No changes
3. physical, chemical, and pharmaceutical properties of Teplizumab
No changes
4. Nonclinical Studies with teplizumab OR teplizumab ANALOGS
No changes
5. Effects in Humans of teplizumab
The summary of safety and the number of treated subjects was updated for the SCT-MGA031-005 (“TN-10 At-Risk”) study.
6. summary of data and guidance for the investigator
Section 6.7 “Undesirable Effects/Adverse Drug Reactions” was replaced with “Reference Safety Information”, removing the previously included non-serious ADRs, for internal process consistency for Sponsor determination of expectedness. In Table 27 all previously included non-serious ADRs (leukopenia, thrombocytopenia, eosinophilia, vomiting, chills, infusion-site reaction, herpes zoster, blood bilirubin increased, EBV viremia, headache, and pruritus) were removed. Additionally, the previously included serious ADRs of nausea, pyrexia, and rash were removed. The serious expected ADRs of lymphopenia, neutropenia, cytokine-release syndrome, and AST/ALT increased were retained.
7. References Literature references that are no longer referenced in the document were removed.
Appendix Appendix 1 Table 28 was updated to include Canada, Germany, Italy, and Australia; planned enrollment was decreased from 140 - 170 to 70 – 80 (the amended Protocol [dated 25 June 2014] was submitted to FDA as Serial No. 0060 on 01 July 2014); and subject exposure was increased from 54 to 64 subjects. Appendix 2: Table 30 was added in conjunction with the revised content in Section 6.7.
Note: Minor editorial, formatting and typographical changes were also made.
Confidential Page 2 of 130

Teplizumab MacroGenics, Inc.
Investigator's Brochure Version 12.0, 16 November 2016
TABLE OF CONTENTS
SUMMARY OF CHANGES FROM PREVIOUS VERSION (VERSION 11) ...................... 2
LIST OF ABBREVIATIONS ................................................................................................... 9
1 SUMMARY ................................................................................................................ 12
2 INTRODUCTION ...................................................................................................... 15
2.1 Immunosuppressive Therapy Versus Reestablishment of Immunologic Tolerance or Reprogramming for Treatment of Immune-Mediated Diseases.............................................................................................................. 15
2.2 Development of Teplizumab .............................................................................. 17
2.3 Mechanism of Action of Teplizumab ................................................................. 18
3 PHYSICAL, CHEMICAL, AND PHARMACEUTICAL PROPERTIES OF TEPLIZUMAB ........................................................................................................... 20
3.1 Active Drug Substance ...................................................................................... 20
3.2 Drug Product ...................................................................................................... 20
3.3 Storage, Handling, and Preparation ................................................................... 20
4 NONCLINICAL STUDIES WITH TEPLIZUMAB OR TEPLIZUMAB ANALOGS ................................................................................................................. 22
4.1 Introduction ........................................................................................................ 22
4.2 Nonclinical Pharmacology and Pharmacokinetics ............................................. 22
4.2.1 Alegre et al. Mouse Study: Assessment of Immunological Properties in hu-SPL-SCID Mice ............................................................ 22
4.2.2 Centocor Study T-2002-009: Dose-ranging Safety and Pharmacokinetic Study in Chimpanzees .................................................. 23
4.2.3 031-2101-09: Comparison of CD3 Epsilon Protein Sequences Between Species ...................................................................................... 25
4.2.4 031-2102-09: Binding of Teplizumab to Human CD3 and Binding of 2C11-mG2a(ala,ala) (Surrogate Antibody) to Mouse CD3 .......................................................................................................... 26
4.2.5 MGA031-HL003: Cytokine Release In Vitro in Peripheral Blood Mononuclear Cells ................................................................................... 26
4.3 Toxicology ......................................................................................................... 26
4.3.1 Bluestone Mouse Study: Single-Dose Toxicity Study in Mice ................ 26
4.3.2 PAI Study IM187: Human Tissue Cross-Reactivity ................................ 26
4.3.3 7608-796: Cytokine Release in Mice Given Single-dose 2C11-mG2a(ala,ala) (Surrogate Anti-CD3 Antibody) ............................. 27
4.3.4 7608-797: Repeat-dose Toxicity, Toxicokinetic, and Immunotoxicology Study of 2C11-mG2a(ala,ala) (Surrogate Anti-CD3 Antibody) in Mice ................................................................... 27
Confidential Page 3 of 130

Teplizumab MacroGenics, Inc.
Investigator's Brochure Version 12.0, 16 November 2016
4.3.5 M00255: Dose-ranging Study of 2C11-mG2a(ala,ala) (Surrogate Anti-CD3 Antibody) in Mice ................................................................... 27
4.3.6 WIL-353187: Embryo-Fetal Development, Toxicokinetic and Immunophenotyping Study in Mice of 2851055 [2C11-mG2a(ala,ala)] (Surrogate Anti-CD3 Antibody) Administered SC on Gestation Days 6, 10, and 14 .............................................................. 28
4.3.7 WIL-353209: A Female Fertility and Early Embryonic Development, Toxicokinetic and Immunophenotyping Study in Mice of 2851055 [2C11-mG2a(ala,ala)] (Surrogate Anti-CD3 Antibody) Administered via SC Injection ................................................ 28
4.3.8 WIL-353210: A Male Fertility, Toxicokinetic and Immunophenotyping Study in Mice of 2851055 [2C11-mG2a(ala,ala)] (Surrogate Anti-CD3 Antibody) Administered via SC Injection ............................................................................................. 29
4.3.9 WIL-353232: A Prenatal and Postnatal Development, Including Maternal Function, Toxicokinetic, Immunophenotyping and Antibody Assessment Study of 2851055 Administered Via Subcutaneous Injection in Mice ............................................................... 29
4.3.10 8233170: A Repeat-Dose Toxicity, Toxicokinetic, and Immunotoxicology Study in Mice Given Compound 2851055 by Intravenous Injection Every 3 Days for 1 Month with a 3 Month Recovery .................................................................................................. 32
4.3.11 Discussion and Conclusions .................................................................... 33
5 EFFECTS IN HUMANS OF TEPLIZUMAB ............................................................ 35
5.1 Exposure to Teplizumab ..................................................................................... 35
5.2 Clinical Pharmacology ....................................................................................... 36
5.2.1 Study 1 (Dr. Kevan Herold, Sponsor-Investigator) .................................. 36
5.2.2 Study 2 (Protocol ITN007AI [NDB01], Dr. Kevan Herold, Sponsor-Investigator) ............................................................................... 38
5.2.3 Study 3 (Protocol ITN017AI, Dr. Kevan Herold, Sponsor-Investigator) ............................................................................................. 40
5.2.4 Protégé Study (Protocol CP-MGA031-01) .............................................. 42
5.2.5 Anti-drug Antibodies in Humans ............................................................. 45
5.2.6 Overall Conclusions about PK in Humans .............................................. 47
5.3 Clinical Studies with Teplizumab ...................................................................... 48
5.3.1 Type I Diabetes Mellitus (T1DM) ........................................................... 48
5.3.1.1 Completed Studies in T1DM .......................................................... 49
5.3.1.2 Current Ongoing Study with Teplizumab ...................................... 54
5.3.2 Psoriasis ................................................................................................... 55
5.3.2.1 Protocol CP-MGA031-04 (MacroGenics, Sponsor) ...................... 55
5.4 Summary of Efficacy ......................................................................................... 55
Confidential Page 4 of 130

Teplizumab MacroGenics, Inc.
Investigator's Brochure Version 12.0, 16 November 2016
5.4.1 Type 1 Diabetes Mellitus ......................................................................... 55
5.4.1.1 Protégé Study Results .................................................................... 55
5.4.2 Insulin Use ............................................................................................... 61
5.4.3 HbA1c Analysis ....................................................................................... 62
5.5 Summary of Safety ............................................................................................ 63
5.5.1 Safety Results from Protégé, Protégé Extension, and Protégé Encore Studies ......................................................................................... 63
5.5.1.1 Summary of Key Safety Results from the Protégé, Protégé Extension and Protégé Encore Studies ........................................... 64
5.5.1.2 Most Common Adverse Events in Protégé, Protégé Extension, and Protégé Encore Studies .......................................... 64
5.5.1.3 Serious Adverse Events in Protégé, Protégé Extension and Protégé Encore Studies................................................................... 68
5.5.1.4 Adverse Events of Special Interest ................................................ 72
5.5.2 Safety Summary in ISCT-MGA031-005 (“TN-10 At-Risk”) Trial ......... 88
5.5.2.1 Overall Summary From the TN-10 At-Risk Trial .......................... 88
5.5.2.2 Serious Adverse Events in the TN-10 At-Risk Trial ...................... 89
5.5.3 Overall Evaluation of the Risks ............................................................... 90
5.5.3.1 Hematologic Events ....................................................................... 90
5.5.3.2 Malignancy-Carcinogenesis ........................................................... 95
5.5.3.3 Summary of Pregnancies ................................................................ 95
5.5.3.4 Deaths ............................................................................................. 97
5.5.4 Risk/Benefit Assessment .......................................................................... 97
5.6 Post-Marketing Experience ................................................................................ 98
6 SUMMARY OF DATA AND GUIDANCE FOR THE INVESTIGATOR ................ 99
6.1 Product Name and Pharmacotherapeutic Group ................................................ 99
6.2 Proposed Indications .......................................................................................... 99
6.3 Posology/Dosing and Administration ................................................................ 99
6.3.1 Regimens for Current T1DM Studies ...................................................... 99
6.3.2 Premedication and Drug Administration Instructions ............................ 100
6.3.3 Storage and Handling ............................................................................. 100
6.4 Contraindications ............................................................................................. 101
6.5 Special Warnings and Precautions ................................................................... 101
6.5.1 Cytokine-Release Syndrome .................................................................. 101
6.5.2 Abnormal Liver Function Laboratory Tests ........................................... 101
6.5.3 Lymphopenia .......................................................................................... 101
6.5.4 Hypoglycemia ........................................................................................ 102
6.5.5 Active Infections .................................................................................... 102
Confidential Page 5 of 130

Teplizumab MacroGenics, Inc.
Investigator's Brochure Version 12.0, 16 November 2016
6.5.6 Vaccinations ........................................................................................... 102
6.6 Interactions with Other Drugs and Food .......................................................... 102
6.7 Reference Safety Information .......................................................................... 102
6.8 Postmarketing .................................................................................................. 103
6.9 Carcinogenesis, Mutagenesis, and Impairment of Fertility ............................. 103
6.10 Pharmacokinetics/Pharmacodynamics in Special Populations ........................ 104
6.11 Overdose .......................................................................................................... 104
6.12 Effects on Ability to Drive Vehicles and Operate Machinery .......................... 104
7 REFERENCES ......................................................................................................... 105
LIST OF TABLES
Table 1 Description of Test Articles .......................................................................... 23
Table 2 Summary of the Pharmacokinetic Parameters for CNTO311 in Chimpanzees after a Single SC Injection at 0.1, 1.0, or 10 mg/kg ............... 25
Table 3 Estimated Cumulative Subject Treatment Exposure from Intravenous Teplizumab Completed and Ongoing Studies .......................... 35
Table 4 Cumulative Subject Exposure to Intravenous Teplizumab from Completed Clinical Trials by Age and Sex a,b .............................................. 36
Table 5 Study 1 in T1DM: Serum Trough Levels a from Study Days 8–12 .............. 37
Table 6 Study 2 (ITN007AI) in T1DM: Serum Trough Levels a from Study Days 8–12 ........................................................................................... 39
Table 7 Study 3 (ITN017AI) in T1DM: Serum Trough Levelsa from Study Days 8–12 ........................................................................................... 41
Table 8 Incidence of Subjects Who Developed ADA and the Extent of ADA Response (Protégé Study) ............................................................................. 46
Table 9 Maximum ADA by Quartile of C-peptide Change from Baseline – Days 364 and 728, Full 14-Day Regimen .................................................... 46
Table 10 Summary of Teplizumab Pharmacokinetic Data in Humans ........................ 47
Table 11 T1DM Dosing Regimens .............................................................................. 49
Table 12 Primary Endpoint: Proportion of Subjects with Composite Endpoint of HbA1c < 6.5% and Insulin < 0.5 U/kg/day (Protégé Study, ITT/Safety Population) ................................................................................. 56
Table 13 Number of Subjects in T1DM Intravenous Teplizumab Trials .................... 64
Table 14 Most Frequent Adverse Events (>=10%) by Pooled Treatment Group Pooled Safety Population, Protégé, Protégé Extension and Protégé Encore (CP-MGA031-01, -02, and -03) .......................................... 65
Table 15 Number (%) of Subjects Who Had AEs Satisfying Comparison Criteria (Double-Blind Segment, Protégé Study, Safety Population) .......... 67
Confidential Page 6 of 130

Teplizumab MacroGenics, Inc.
Investigator's Brochure Version 12.0, 16 November 2016
Table 16 Number (%) of Subjects Who Had AEs Satisfying Comparison Criteria (Double-Blind Segment, Encore Study, Safety Population) ........... 68
Table 17 Number (%) Subjects Who Had Serious AEs, Pooled Safety Population, Protégé, Protégé Extension and Protégé Encore, (CP-MGA031-01, -02, -03) ................................................................................. 69
Table 18 Summary of Herpes-like Infection Terms by Treatment Groups (Double-Blind Segment, Protégé Study, Safety Population) ........................ 77
Table 19 Summary of Herpes-like Infection Terms by Treatment Groups (Double-Blind Segment, Protégé Encore Study, Safety Population) ........... 78
Table 20 List of Subjects with Herpes Zoster (Protégé, Double-Blind and Open-Label Segments and Protégé Encore, Double Blind Segment) .......... 79
Table 21 Number and Percent of Subjects with Above-Normal Clinical Laboratory Test Results for ALT, AST, GGT and Bilirubin (Protégé Study, Double-Blind Segment, Safety Population) ...................................... 82
Table 22 Number and Percent of Subjects with Above-Normal Clinical Laboratory Test Results for ALT, AST, GGT and Bilirubin (Protégé Encore Study, Double-Blind Segment, Safety Population) .......................... 84
Table 23 Serious Adverse Events in the TN-10 At-Risk Trial..................................... 89
Table 24 Summary of Pregnancies .............................................................................. 96
Table 25 Summary of Deaths (All Teplizumab Clinical Studies) ............................... 97
Table 26 T1DM Dosing Regimens for the TN-10 At-Risk Study ............................... 99
Table 27 Expected ADRs for Regulatory Reporting Purposes .................................. 103
Table 28 Overview of Ongoing Studies for Teplizumab as of 23 August 2016 ........ 110
Table 29 Overview of Studies Completed for Teplizumab as of 23 August 2016 ............................................................................................................. 111
Table 30 Teplizumab Adverse Drug Reactions1 from Completed Trials with Expectedness .............................................................................................. 115
LIST OF FIGURES
Figure 1 Immunologic Tolerance ................................................................................ 16
Figure 2 The Two-Signal Model of T-Cell Activation ................................................ 18
Figure 3 The Two-Signal Model of T-Cell Activation: Effects of OKT®3 ............... 19
Figure 4 Simulated Concentration-Time Course in Cycle 1 following the Full 14-Day Regimen ........................................................................................... 44
Figure 5 Simulated Concentration-Time Course in Cycle 2 Following the Full 14-Day Regimen: Subjects with Strong Immune Response ......................... 45
Figure 6 Mean Changes from Baseline in C-peptide AUC – Full 14-Day Regimen versus Placebo (Protégé Study, Double-Blind Segment, ITT Population) ............................................................................................ 57
Confidential Page 7 of 130

Teplizumab MacroGenics, Inc.
Investigator's Brochure Version 12.0, 16 November 2016
Figure 7 Mean Change from Baseline for C-peptide in Adolescents (8-17 years old)-Protégé Study, Full 14-Day Regimen versus Placebo ................. 58
Figure 8 Mean Change from Baseline for C-peptide in Adults (18-35 years old)-Protégé Study, Full 14-Day Regimen versus Placebo .......................... 59
Figure 9 Mean Change from Baseline for C-peptide in USA Subjects (all age groups)- Protégé Study, Full 14-Day Regimen versus Placebo.................... 60
Figure 10 Change from Baseline for C-peptide in Subjects ≤6 Weeks from First Symptoms to Randomization- Protégé Study, Full 14-Day Regimen versus Placebo ............................................................................... 61
Figure 11 Mean Change in Average Daily Insulin Use – Protégé Study, Full 14-Day Regimen versus Placebo .................................................................. 62
Figure 12 Mean Changes from Baseline in HbA1c – Protégé Study, Full 14-Day Regimen vs. Placebo ............................................................................. 63
Figure 13 Rash Adverse Events Onset Study Day (Up to Day 728 – All Teplizumab vs. Placebo, Protégé Study, Double-Blind Segment, Safety Population) ........................................................................................ 74
Figure 14 Rash Adverse Events Onset Study Day (Cycle 1 – Teplizumab Subjects, Protégé Study, Double Blind Segment) ........................................ 75
Figure 15 All Cytokine Release Syndrome Events (Protégé, Double-Blind Segment, Teplizumab Safety Population) .................................................... 80
Figure 16 Mean ALT and AST Values Through Study Day 91 (Protégé Study, Safety Population) ........................................................................................ 85
Figure 17 Mean Bilirubin Values Through Study Day 91 (Protégé Study, Safety Population) ........................................................................................ 86
Figure 18 Mean (± SD) Leukocyte Values Up to and Including Day 28 (Protégé Study, Safety Population) ............................................................... 91
Figure 19 Mean (± SD) Lymphocyte Values Up to and Including Day 28 (Protégé Study, Safety Population) ............................................................... 92
Figure 20 Mean (± SD) Neutrophil Values Up to and Including Day 28 (Protégé Study, Safety Population) ............................................................... 93
Figure 21 Mean (± SD) Platelet Levels Up to and Including Day 28 (Protégé Study, Safety Population) ............................................................................. 94
Figure 22 Mean (± SD) Eosinophil Values Up to and Including Day 28 in the Protégé Study ................................................................................................ 95
LIST OF APPENDICES
Appendix 1 Status of Ongoing and Completed Clinical Teplizumab Studies in Type 1 Diabetes Mellitus
Appendix 2 Adverse Drug Reactions
Confidential Page 8 of 130

Teplizumab MacroGenics, Inc.
Investigator's Brochure Version 12.0, 16 November 2016
LIST OF ABBREVIATIONS
Abbreviation Definition
ADA Anti-drug antibody
ADR Adverse drug reaction
AE Adverse event
Ag Antigen
Ala Alanine
ALT Alanine aminotransferase
APC Antigen-presenting cell
AST Aspartate aminotransferase
AUC Area under the curve (a measure of drug exposure)
AVG Average
BQL Below quantitation limit
BSA Body surface area
C Celsius/Centigrade
CD3 A complex of at least 5 membrane-bound proteins on the surface of mature T lymphocytes associated with the T-cell receptor
CD3-ε A polypeptide subunit of CD3 essential in the development of the T-cell complex
CHO Chinese hamster ovary
Cmax Maximum plasma concentration
CMV Cytomegalovirus
CRS Cytokine-release syndrome
CTCAE Common Terminology Criteria for Adverse Events
DCO Detailed clinical observation
DKA Diabetes ketoacidosis
DMC Data monitoring committee
EBV Epstein-Barr virus
F Fahrenheit
Fab Fragment antigen binding
Fc Fc component of an antibody/immunoglobulin molecule
FcR Receptors that bind the Fc component of antibody molecules
GD Gestation day
GGT Gamma-glutamyl transpeptidase
GLP Good laboratory practice
Confidential Page 9 of 130

Teplizumab MacroGenics, Inc.
Investigator's Brochure Version 12.0, 16 November 2016
Abbreviation Definition
GMP Good manufacturing practice
HbA1c Hemoglobin A1c
hr Hour
IFN-γ Interferon-gamma
IgG Immunoglobulin G
IL Interleukin
IND U.S. Investigational New Drug
INN International Nonproprietary Name
IP Intraperitoneal
IRB Institutional Review Board
ITN Immune Tolerance Network
iTreg Inducible T regulatory
IV Intravenous
LFT Liver function test
M Molar
mAb Monoclonal antibody
MedDRA Medical dictionary for regulatory activities
MHC Major histocompatibility complex
mM Millimole
MMRM Mixed model repeated measurement
nTreg Naturally occurring T regulatory
NaCl Sodium chloride
NIH National Institutes of Health
NOAEL No observed adverse effect level
NOD Non-obese diabetic mouse (mouse strain that spontaneously develops autoimmune diabetes)
NOS Not otherwise specified
NSAID Non-steroidal anti-inflammatory drug
NS0 Non-secreting 0, murine myeloma cell line
OKT®3 Designation of muromonab-CD3 (Ortho) anti-lymphocyte monoclonal antibody
PBMC Peripheral blood mononuclear cells
pbo Placebo
PCR Polymerase chain reaction
Confidential Page 10 of 130

Teplizumab MacroGenics, Inc.
Investigator's Brochure Version 12.0, 16 November 2016
Abbreviation Definition
PD Pharmacodynamic(s)
PK Pharmacokinetic(s)
PND Post natal day
PRO Patient reported outcomes
PsA Psoriatic arthritis
RA Rheumatoid arthritis
rad Radiation absorbed dose
RPM Revolutions per minute
RSI Reference safety information
SAE Serious adverse event
SC Subcutaneous
SCID Severe combined immunodeficiency
SD Standard deviation
SOC System organ class
TEAE Treatment-emergent adverse event
T1DM Type 1 diabetes mellitus
TCR T-cell receptor
tmax Time of maximal concentration
TNF Tumor necrosis factor-alpha
Teff T effector
Treg T regulatory
ULN Upper limit of normal
USAN United States Adopted Name
WBC White blood cell
WHO World Health Organization
yr Year
Confidential Page 11 of 130

Teplizumab MacroGenics, Inc.
Investigator's Brochure Version 12.0, 16 November 2016
1 SUMMARY
This Investigator’s Brochure (IB) describes information about teplizumab, a humanized anti-CD3 monoclonal antibody (mAb) with no or minimal capacity to bind Fc receptors, that is being evaluated for treatment and prevention of type 1 diabetes mellitus (T1DM). Teplizumab has also been evaluated for treatment of renal allograft rejection, for induction therapy in islet transplant recipients, and psoriatic arthritis. Teplizumab is the International Nonproprietary Name (INN) for hOKT3γ1 (ala,ala), accepted by the World Health Organization (WHO) and adopted by the United States Adopted Name (USAN) Council. Teplizumab is also called MGA031 and is produced by MacroGenics, Inc.
Teplizumab is a 150-kiloDalton (kD) humanized IgG1 mAb that specifically recognizes the CD3-ε chain of the T-cell receptor (TCR) complex on human T cells. Teplizumab binds minimally or not at all to Fc receptors because its Fc component was modified to eliminate Fc receptor (and complement) binding. The antibody is expressed from a genetically engineered, stable Chinese hamster ovary (CHO) cell line in a chemically defined medium. Harvested mAb is purified and formulated into a sterile injectable solution for human use.
Teplizumab interacts minimally or not at all with Fc receptors because its Fc domain was modified to eliminate Fc receptor (and complement) binding. In vitro and in vivo data suggest that binding of teplizumab to its target triggers events that differentially inhibit auto-reactive T cells compared to regulatory T cells (Tregs). The specific mechanisms involved in therapeutic effects are incompletely understood (19).
As of 23 August 2016, approximately 1093 study subjects have been enrolled into the teplizumab clinical development program and approximately 823 subjects have received teplizumab. This represents data across all teplizumab studies with various doses, formulations, and indications and includes earlier smaller investigator-sponsored studies. The enrollment of subjects by study drug indication is as follows: T1DM (estimated N= 989), renal or renal-pancreatic allograft rejection (N = 8), induction immunotherapy in pancreatic islet transplant recipients (N = 20), psoriatic arthritis (N = 11), plaque psoriasis (N = 1) and the prevention or delay of onset in patients at high risk of developing T1DM (N = 64). The data from the completed Protégé and Protégé Encore trials (total N=808: Protégé N=554 and Protégé Encore N=254) provide the most comprehensive adverse event data for teplizumab-treated subjects from double-blinded, placebo-controlled trials and are the basis of the safety profile for teplizumab.
In current clinical studies of T1DM, teplizumab is administered based on body surface area (BSA) according to the full 14-day regimen given intravenously (IV) over 14 consecutive days; escalating doses of 51 to 413 mcg/m2 on days 1–4 and 826 mcg/m2 on Days 5–14; see Section 6.3).
In October 2010, a Data Monitoring Committee (DMC) review of 1-year data from the 2-year CP-MGA031-01 (Protégé) study disclosed that the primary efficacy endpoint (composite of HbA1c < 6.5% and insulin < 0.5 U/kg/day) was not met in the study. However, no unanticipated safety issues were identified. As a result of missing the primary efficacy
Confidential Page 12 of 130

Teplizumab MacroGenics, Inc.
Investigator's Brochure Version 12.0, 16 November 2016
endpoint in this study, the Sponsor and its partner terminated enrollment in Protocol CP-MGA031-02 (Protégé Extension) and enrollment and dosing in Protocols CP-MGA031-03 (Protégé Encore) and CP-MGA031-06 (SUBCUE). In CP-MGA031-01 (Protégé) and CP-MGA031-03 (Protégé Encore), subjects continued in the study for follow-up of safety endpoints and clinical endpoints associated with the standard of care of diabetes (HbA1c, insulin, and fasting C-peptide only), consistent with the DMC recommendations. A study in subjects at risk of developing T1DM (Study ISCT-MGA031-005 [“TN-10 At–Risk”]) and investigator-sponsored studies continued unchanged after disclosure of the DMC finding to the other study investigators and sponsors.
Exploratory analyses in Protégé subjects who received treatment showed effects similar to those seen in a previous, smaller study with teplizumab (25, 26). C-peptide secretion was preserved with the full 14-day teplizumab regimen, allowing glycemic control to be achieved at a lower insulin dose in the teplizumab group than in the placebo group. A greater proportion of subjects in the teplizumab-treated groups were able to discontinue or use very low doses of insulin than in the placebo group. The Protégé study also identified subgroups that might be more likely to respond to treatment. Larger treatment effects were associated with younger age (8-17 years), recruitment from the USA, earlier treatment (≤ 6 weeks), and lower baseline HbA1c.
The pharmacokinetics (PK) of teplizumab following intravenous administration were described by a two-compartment model with saturable binding in central and peripheral compartments. For typical subjects without immunogenic reaction administered the full 14-day regimen, the predicted mean (± SD) total AUC was 6421 ± 1940 ng•day/mL. Day 14 Cmin and Cmax of teplizumab were 418 ± 225 ng/mL, and 826 ± 391 ng/mL, respectively. The accumulation ratio for AUC between Day 5 and Day 14 (the first and the last day with the full-dose administration) was 3.43 ± 1.16. With a body surface area (BSA)-proportional dose, teplizumab AUC, Cmin and Cmax were independent of body weight. The terminal half-life for teplizumab was 4.01 day (SD = 1.75 day). There was no evidence of clinically relevant dependencies of pharmacokinetics on age, gender, race, region, baseline CD4+ and CD8+ cell counts, disease state or disease onset time. Teplizumab pharmacokinetics were influenced by the immunogenic response with clearance increased by up to 194% in subjects with high anti-drug antibody (ADA) concentration (3 mcg/mL) observed during Cycle 2 dosing. Some subjects demonstrated strong immunogenic response, which was described as an abrupt reduction of bioavailability and increase in clearance after about 10 days of the cycle 2 dosing. There did not appear to be a significant correlation, however, between ADA titers and either the changes in C-peptide or with response using the modified composite HbA1c + insulin usage endpoint.
The largest amount of safety data for teplizumab comes from two completed Phase 3 studies: CP-MGA031-01 (Protégé) and CP-MGA031-03 (Protégé Encore). Leukopenia/lymphopenia and rash have been the events experienced most frequently by teplizumab-treated subjects. The rash has usually been mild and easily treated. Lymphopenia is expected based on the mechanism of action of teplizumab. Other laboratory abnormalities observed include hematologic (neutropenia, thrombocytopenia, eosinophilia) and liver function test (LFT) abnormalities (primarily alanine aminotransferase (ALT), aspartate aminotransferase (AST),
Confidential Page 13 of 130

Teplizumab MacroGenics, Inc.
Investigator's Brochure Version 12.0, 16 November 2016
and bilirubin elevations; not gamma-glutamyl transpeptidase (GGT)). These abnormalities resolved usually within 14 days of dose completion and did not have concurrent clinical sequelae. Cytokine release syndrome (CRS), which may include, but not be limited to, rash, headache, nausea, vomiting, and chills/rigors/pyrexia occurred in less than 6% of teplizumab subjects and was usually Grade 1 or 2.
Overall infections were not increased. However, there are several cases of herpes zoster infections in teplizumab subjects in Protégé, possibly dose-related. Although all herpes zoster cases resolved, there was a numeric increase in herpes zoster cases observed in the Protégé study compared to the Protégé Encore study. In the Protégé Encore study, only one case was observed in a subject randomized to placebo treatment. Drug-relationship to herpes infections remains unclear. Other herpes virus infections (e.g., cytomegalovirus [CMV] and Epstein-Barr virus [EBV]) were not increased.
Currently, there is one study in progress: the TN-10 At-Risk Trial being conducted by the National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK) at TrialNet sites, under MacroGenics IND 102,629. The study is enrolling non-diabetic subjects who are relatives of T1DM patients to determine whether teplizumab will prevent or delay the onset of T1DM in these subjects. The objective is to assess the safety, efficacy, and mode of action of intravenous teplizumab for prevention of T1DM in subjects at high risk of developing T1DM. The US FDA approved opening enrollment to children (8–16 years of age) in the TN-10 At-Risk Trial upon review of data from Protégé and data from other teplizumab studies. As of 23 August 2016, 64 subjects have been enrolled in the study using a 1:1 randomization ratio, receiving either teplizumab or placebo.
Adverse drug reactions (ADRs) that the Sponsor has attributed to the use of teplizumab and that reflect current understanding of events that are expected in association with the administration of teplizumab are lymphopenia, neutropenia, cytokine-release syndrome, and AST/ALT increased. Unanticipated events associated with long-term administration of the drug have not been observed in the ongoing review of the safety data.
Confidential Page 14 of 130

Teplizumab MacroGenics, Inc.
Investigator's Brochure Version 12.0, 16 November 2016
2 INTRODUCTION
2.1 Immunosuppressive Therapy Versus Reestablishment of Immunologic Tolerance or Reprogramming for Treatment of Immune-Mediated Diseases
Treatment of immune-mediated diseases has traditionally involved administration of medications, including monoclonal antibodies that are suppressive. That is, medications of various types are administered to maximally tolerated levels to block or suppress ongoing immunologically mediated tissue injury. This immunosuppressive approach to therapy, although effective in ameliorating the unwanted immunological activity, has multiple potential risks. Immunosuppressive therapy—particularly chronic suppression—enhances the risk of developing opportunistic infections, infection-related cancers, and possibly other cancers.
A potentially better approach to treatment of immune-mediated diseases is to employ short-term therapies that harness the basic immune regulatory systems that limit unwanted immune-mediated tissue injury. For alloantigens that are the targets of immune-mediated attack in transplantation, treatments that “educate” the host immune system to recognize and respond to the alloantigens as if they were “self” antigens and not foreign antigens would be ideal. For immune-mediated attack of self-antigens (autoimmune disease), treatments that “reeducate” the immune system to reestablish “self-tolerance” is the goal. In both settings, these treatments would involve induction of a form of immunologic reprogramming to reestablish the immune tolerant state.
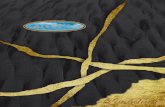
There are several mechanisms involved in the maintenance of immunologic tolerance. One of these mechanisms is operative in the thymus and is referred to as “central tolerance” (Figure 1). This mechanism involves the elimination or deletion in the thymus of T cells that recognize self-antigens and have the potential to destroy self-tissues. The antigen-presenting cell (APC) is central in the presentation of the antigens to which immune competence or tolerance develops.
The other mechanism operates outside the thymus and is known as “peripheral tolerance.” There are a variety of mechanisms involved in peripheral tolerance, but a very important one involves the activity of a class of cells, designated T regulatory (Treg) cells. Treg cells mediate peripheral tolerance through active inhibition of T effector (Teff) cells that destroy or injure self-tissues. A notable feature of this class of Treg cells, some of which emerge from the thymus (Figure 1), is the expression of the transcription factor FoxP3 (45, 46). In addition to Treg, peripheral tolerance may also be mediated through deletion of T cells outside the thymus, through T cell ignorance, unresponsiveness, or anergy to self-antigens. The reestablishment of tolerance has profound implications for treatment of autoimmune, allergic, and other diseases.
Confidential Page 15 of 130

Teplizumab MacroGenics, Inc.
Investigator's Brochure Version 12.0, 16 November 2016
Figure 1 Immunologic Tolerance
Figure 1 reference: (45)
There are 2 general classes of Treg cells, naturally occurring (nTreg) and adaptive (inducible, iTreg) regulatory T cells. nTregs emerge from the thymus (Figure 1) and are characterized as CD3+ CD4+ CD25+ CD62L+, and FoxP3+. iTreg cells (not shown in Figure 1) include CD3+ CD4+ CD25+ CD62L+ FoxP3+ cells, but also include CD3+ CD8+ CD25+ FoxP3+ cells. Both of these cell types have the capacity to inhibit or block the activity of T effector (Teffs) cells. In addition, other cell populations have been described that also have regulatory properties. These cell populations include: a) TGF-β-producing Th3 cells, b) certain Th2 cells, c) NKT cells, d) γδ T cells, and e) anergic T cells.
The relationships among these various types of cells are the focus of extensive current research, but a key concept that has emerged is that Treg numbers and activity can be enhanced with the result that deleterious Teff cell function is checked or inhibited. Available nonclinical and clinical data support the concept that treatment with anti-CD3 mAbs with markedly reduced or absent Fc-receptor binding can achieve these effects. In other words, reestablishing of immunologic tolerance with anti-CD3 mAbs with reduced Fc-receptor binding may be a logical approach for therapy of immune-mediated diseases and may have major advantages over traditional immunosuppressive therapies, particularly chronic immunosuppressive therapies (12). Data on anti-CD3 mAb treatments in humans are reviewed in subsequent sections of this Investigator’s Brochure.
Considerable data on anti-CD3 mAb treatments in animals are available in the literature, as follows:
Nonobese diabetic (NOD) mouse model:(5, 32, 50).
Monoclonal antibodies against murine CD3: (1, 4, 14, 17, 18, 36, 39).
Studies with whole intact anti-CD3 monoclonal antibodies:(6, 13, 14, 21, 22, 24, 50).
Confidential Page 16 of 130

Teplizumab MacroGenics, Inc.
Investigator's Brochure Version 12.0, 16 November 2016
Evidence for beta cell regeneration: (9, 14, 15, 25, 26, 34, 38, 40, 41, 52).
Studies with anti-CD3 F(ab')2 fragments or mAbs engineered for reduced Fc receptor binding: (6, 10-13, 24, 30, 35, 37, 47, 51, 53-55).
Anti-CD3 intervention in systemic lupus erythematosus models (MRL lpr/lpr mouse): (23).
Anti-CD3 intervention in experimental autoimmune encephalomyelitis: (35, 55).
Anti-CD3 intervention in collagen-induced arthritis: (31).
Additional discussion of nonclinical data with the anti-CD3 mechanism occurs in Section 5.
2.2 Development of Teplizumab
The engineering of teplizumab was based on the properties of F(ab')2 fragments or FcR-non-binding versions of anti-murine CD3 antibodies in autoimmune-prone mice: specifically the minimization of the potential for side effects and full preservation of therapeutic activity associated with an expansion of immunoregulatory T cells. OKT®3 is the murine (IgG2a) precursor for the humanized, Fc-engineered (IgG1) mAb teplizumab.
Teplizumab binds an extracellular epitope on the CD3- chain of the TCR complex with affinity equal to OKT®3, but it differs from OKT®3 in that it is humanized (to reduce immunogenicity in humans) and Fc-engineered (to reduce cytokine-mediated toxicity). Two amino acids in the Fc portion of the humanized IgG1 OKT3 were changed (leucine234 to alanine and leucine235 to alanine) to disrupt both Fc receptor and complement component C1q binding (2). Compared with the murine antibody OKT®3, the humanized Fc-engineered antibody teplizumab is 100- to 1,000-fold less potent as an inducer of T-cell activation markers, T-cell proliferation and cytokine release in human peripheral blood mononuclear cell cultures (3); (unpublished MacroGenics data). These in vitro results are consistent with teplizumab retaining the T lymphocyte targeting activity of OKT®3, but exhibiting much reduced activation and mitogenic properties.
This mAb initially was produced by Dr. Bluestone and Tolerance Therapeutics, Inc., a holding company for the Bluestone technology. Bluestone and colleagues, and the Immune Tolerance Network (ITN), directed the earliest phases of clinical development.
MacroGenics acquired the technology for teplizumab from Tolerance Therapeutics in July 2005. An extensive series of in vitro and in vivo assays were conducted, which demonstrated that teplizumab lots manufactured initially by Tolerance Therapeutics and then by MacroGenics are comparable. These data have been submitted to and reviewed by regulatory agencies in all countries in which an Investigational New Drug (IND) or Clinical Trial Application has been filed.
Confidential Page 17 of 130

Teplizumab MacroGenics, Inc.
Investigator's Brochure Version 12.0, 16 November 2016
2.3 Mechanism of Action of Teplizumab
The modified Fc component of teplizumab minimizes the activating capacity of the antibody compared with unmodified murine OKT®3. Although the primary mechanism of action of the antibody involves binding the CD3 antigen target on T cells, subsequent mechanisms involved in the therapeutic effects are incompletely understood, but the mechanisms appear consistent with the biological effects triggered by anti-CD3 interventions with Fc-receptor non-binding antibodies in autoimmune-prone mouse models.
The mechanisms of action of teplizumab appear to involve weak agonistic activity on signaling via the T cell receptor-CD3 complex associated with the development of anergy, unresponsiveness, and/or apoptosis, particularly of unwanted activated Teff cells. In addition, regulatory cytokines are released and regulatory T cells are expanded that may lead to the reestablishment of immune tolerance (7, 12). The details of this activity are illustrated in Figure 2 and Figure 3.
As shown in Figure 2, the mechanism of action of normal T-cell activation involves an interaction between the TCR and antigen-loaded major histocompatibility molecule on the antigen presenting cell (APC). This is called Signal 1. The normal interaction also involves interactions between accessory molecules on the T cell and APC. This is called the 2-signal interaction model and results in full activation of the T cell.
Figure 2 The Two-Signal Model of T-Cell Activation
Source: Dr. Ezio Bonvini, MacroGenics, Inc. Legend: Ag = antigen; MHC = major histocompatibility complex; classes I and II are shown. Note that Signal 1 is mediated by intracellular signaling molecules, Fyn and Lck.
As illustrated in Figure 3, intervention with antibodies such as OKT®3 results in full T-cell activation because the antibody facilitates interactions with the APC and leads to extensive
TCRα
β
T Lymphocyte
TCRα
βTCR
α
β
αα
ββ
T Lymphocyte
ImmuneActivationImmuneActivation
Ag
MHC I/II
APC
CD4/CD8
AgAg
MHC I/II
APC
CD4/CD8
MHC I/II
APC
MHC I/II
APC
CD4/CD8CD4/CD8
Signal 1(Ca2+ Flux)
Lck
CD3ζζ
Fyn Signal 1(Ca2+ Flux)Signal 1(Ca2+ Flux)Signal 1(Ca2+ Flux)
Lck
CD3ζζ
Fyn
LckLck
CD3ζζ
Fyn
CD3ζζCD3ζζ
FynFyn
Signal 2Co-stimulation
Accessorymolecules
Signal 2Co-stimulation
Signal 2Co-stimulation
AccessorymoleculesAccessorymolecules
Confidential Page 18 of 130

Teplizumab MacroGenics, Inc.
Investigator's Brochure Version 12.0, 16 November 2016
cross-linking of CD3 on the T cell surface as well as the potential of interaction between accessory molecules. Consequently, OKT®3 has certain problems associated with its administration, namely T-cell depletion and severe CRS (which produces flu-like symptoms of headache, chills, fever, myalgias and arthralgias; nausea and diarrhea may also occur). Use of OKT®3 is limited to treatment of steroid-resistant transplant rejection.
Figure 3 The Two-Signal Model of T-Cell Activation: Effects of OKT®3
Source: Dr. Ezio Bonvini, MacroGenics, Inc. Legend: APC = antigen presenting cell; FcγR = Fc gamma receptor. This is a receptor that binds to the Fc portion of IgG molecules such as OKT®3. MHC = Major Histocompatibility Complex; Class I and II are shown. TCR = T cell receptor. Note that Signal 1 is mediated by intracellular signaling molecules Fyn and Lck.
In contrast, teplizumab appears to only partially activate through the T-cell receptor (Signal 1). Signal 2 is not activated. Thus, teplizumab may function as a partial agonist that induces apoptosis and anergy among pathogenic Teff cells. Interestingly, teplizumab through the same mechanism also appears to promote adaptive regulatory T cell development and activity. The overall result is consistent, based on analogous studies in NOD mice, with the view of a rebalancing of the immune system and reestablishing immune tolerance.
MHC I/II
APC
MHC I/II
APC
TCRα
β
T Lymphocyte
TCRα
βTCR
α
β
αα
ββ
T Lymphocyte
AccessorymoleculesAccessorymolecules
CD3ζζCD3ζζ
CD4/CD8CD4/CD8
Signal 1(Ca2+ Flux)
Lck
Signal 2Co-stimulation
ImmuneActivation
Fyn Signal 1(Ca2+ Flux)Signal 1(Ca2+ Flux)Signal 1(Ca2+ Flux)
LckLck
Signal 2Co-stimulation
ImmuneActivation
Fyn
Signal 2Co-stimulation
Signal 2Co-stimulation
ImmuneActivationImmuneActivation
FynFyn
OKT®3OKT®3FcγRFcγR
Problems with OKT®3:• Major T cell depletion• CRS: flu-like symptoms, headaches,
chills, fever, nausea, diarrhea• Antibody formation (HAMA response)• Use limited to Tx rescue
Confidential Page 19 of 130

Teplizumab MacroGenics, Inc.
Investigator's Brochure Version 12.0, 16 November 2016
3 PHYSICAL, CHEMICAL, AND PHARMACEUTICAL PROPERTIES OF TEPLIZUMAB
3.1 Active Drug Substance
Teplizumab is expressed in a stable CHO cell line. Column chromatographic procedures and filtration are used to purify the mAb and to facilitate virus removal and inactivation. Teplizumab is formulated for human clinical use under Good Manufacturing Practice (GMP) conditions.
3.2 Drug Product
Teplizumab is provided in 2-mL glass vials with FluroTec®-coated butyl rubber stoppers and flip-off seals. The formulation of teplizumab consists of:
10 mM sodium phosphate, pH 6.1
150 mM sodium chloride
0.05 mg/mL polysorbate 80
Final drug product is provided at a concentration of 1 mg/mL for a total of 2 mg of recoverable drug product per vial.
3.3 Storage, Handling, and Preparation
Vials containing teplizumab should be stored upright under refrigeration at 2°–8°C (36°-46°F), in an appropriate locked room accessible only to pharmacy personnel, principal investigator or duly designated person. Teplizumab must be protected from light and must not be frozen or shaken.
Tepliuzmab is administered intravenously as a very dilute protein in a physiological salt solution near neutral pH. Although not currently being evaluated for subcutaneous administration, teplizumab has been administered subcutaneously as a more concentrated protein in physiological salt solution near neutral pH. Use standard laboratory practices for avoidance of contact. Wear gloves when handling; wash hands when work is finished. Do not commingle storage of teplizumab with food; do not eat while conducting any work with the product. If product is spilled, it can be wiped up with an absorbent towel and disposed as medical waste.
Do not use polyolefin IV bags in the preparation or administration of teplizumab.
Because there is no preservative, infusion of study drug (teplizumab or placebo) should begin no later than 2 hours after preparation and must be completed within 6 hours of preparation. The time of preparation should be written on the infusion bag label. The investigational study drug for IV and/or subcutaneous (SC) administration may be prepared only with 0.9%
Confidential Page 20 of 130

Teplizumab MacroGenics, Inc.
Investigator's Brochure Version 12.0, 16 November 2016
sodium chloride (NaCl). The amount of product to be administered must be consistent with that stipulated in the relevant protocol. It is recommended that the drug not be filtered or administered through a filter to avoid adsorption of teplizumab and possible under-dosing. MacroGenics has tested a limited set of filtered administration sets. If local site or country requirements or other needs require the use of filtered administration sets, the site should contact the study sponsor (or MacroGenics) to verify the acceptability of the proposed filtered administration set.
Confidential Page 21 of 130

Teplizumab MacroGenics, Inc.
Investigator's Brochure Version 12.0, 16 November 2016
4 NONCLINICAL STUDIES WITH TEPLIZUMAB OR TEPLIZUMAB ANALOGS
4.1 Introduction
Teplizumab specifically binds to human CD3+ T cells. It cross-reacts with CD3+ T cells of chimpanzees, an endangered species that is inappropriate for extensive experimentation, but not with CD3+ T cells of any other animal species (3, 8, 43, 44, 48). Because of the limited availability of animal models with cross-reactive target antigens, nonclinical pharmacology, pharmacokinetic, and toxicology studies have been limited, although some recent studies have been conducted using a surrogate antibody [2C11-mG2a(ala,ala)].
Because of the limited availability of animal models with cross-reactive target antigens, the initial clinical studies with teplizumab in T1DM subjects were supported by a limited number of nonclinical studies that evaluated the pharmacology, pharmacokinetics, safety, and toxicology of teplizumab. These studies included a Good Laboratory Practice (GLP) single-dose study in chimpanzees and a GLP tissue cross-reactivity study using human tissues. To further investigate the potential safety issues with teplizumab, a hamster/mouse chimeric mAb was developed that binds to the CD3-ε receptor on mouse T cells. This surrogate mAb for teplizumab, designated as 2C11-mG2a (ala,ala), demonstrated a binding affinity to the murine CD3-ε receptor similar to the binding affinity of teplizumab to human CD3, with equilibrium dissociation constants (Kd) of 2.4 mcM and 2.9 mcM, respectively. The studies conducted in mice using this surrogate antibody [2C11-mG2a(ala,ala)] included two non-GLP single-dose studies, a GLP repeat-dose toxicity study, a GLP embryo-fetal developmental toxicity study, male and female GLP fertility, early embryonic, prenatal/postnatal development and maternal toxicity studies (Section 4.3.3 and Section 4.3.10).
4.2 Nonclinical Pharmacology and Pharmacokinetics
4.2.1 Alegre et al. Mouse Study: Assessment of Immunological Properties in hu-SPL-SCID Mice
The objective of this study was to assess the immunological properties of a humanized Fc-engineered anti-CD3 monoclonal antibody in an in vivo model (hu-SPL-SCID mice) that maintains functional human T cells.
Single-cell suspensions were prepared from fresh human (hu) spleens (SPL) and injected intraperitoneally (108 cells/mouse) into 4- to 6-week old severe combined immunodeficiency (SCID) mice that had been γ-irradiated (200 rad). Animals bearing between 5% and 20% human cells in the peripheral blood were selected for experimentation. Neonatal human foreskin was grafted on the dorsal thorax of mice 11 days after the inoculation of human splenocytes. Mice received monoclonal antibodies (50 µg/day for 5 days, then 10 µg/day for 10 days) or phosphate-buffered saline by intraperitoneal (IP) injection. The grafts were unwrapped at 7 days and the status of the graft was scored blindly and independently by 2
Confidential Page 22 of 130

Teplizumab MacroGenics, Inc.
Investigator's Brochure Version 12.0, 16 November 2016
investigators daily for the first 30 days, and once per week afterward. The scores ranged from 0 to 4: Grade 0, skin grafts intact and soft; Grade 1, skin grafts with a modified pigmentation in a small area; Grade 2, soft skin grafts with larger areas of depigmentation; Grade 3, skin grafts hardened or slightly scrubbed; Grade 4, shrinking or scrubbing skin grafts. Rejection was recorded when scores were Grade 3 or higher.
Research lots of the monoclonal antibodies, shown in Table 1, were prepared from the cell culture supernatant of stably transfected NS0 cells and purified by Protein A column chromatography.
Table 1 Description of Test Articles
Name Alternative name Description
OKT®3 Murine OKT3
hOKT31 209-IgG1 Humanized OKT3 (IgG1)
hOKT34 209-IgG4 Humanized OKT3 (IgG4)
hOKT34(ala,ala) ala,ala-IgG4 Humanized Fc-engineered (A234, A235) OKT3 (IgG4)
Humanized hOKT3γ4(ala,ala), which has similar properties to hOKT3γ1(ala,ala), induced T-cell proliferation inefficiently when compared with OKT®3. Unlike OKT®3, intraperitoneal administration of hOKT3γ4(ala,ala) to hu-SPL-SCID mice did not result in human T-cell activation, as evidenced by the lack of induction of a cell surface marker of activation, CD69, nor did it result in systemic human cytokine production, as evidenced by the lack of induction of human interleukin-2 (IL-2). However, administration of either hOKT3γ4(ala,ala) or OKT®3 resulted in rapid modulation of CD3 molecules from the surface of T cells, caused a reduction of CD3+ T cells, and provided similar prolongation of human allograft survival.
In conclusion, humanized Fc-engineered OKT®3 antibody retained immunomodulatory activity but with reduced side effects, compared with OKT®3, in a chimeric hu-SPL-SCID mouse model.
4.2.2 Centocor Study T-2002-009: Dose-ranging Safety and Pharmacokinetic Study in Chimpanzees
The chimpanzee (Pan troglodytes) is the only relevant animal model for assessing the pharmacokinetics and pharmacodynamics of teplizumab, also referred to as hOKT3γ1(ala,ala) or CNTO311. The primary objectives of this study were to determine the pharmacokinetics and toxicity of CNTO311 in chimpanzees after a single subcutaneous dose (the subcutaneous route was the Centocor planned route of administration in the clinic at that time). Secondary objectives were to evaluate T-cell numbers and cytokine induction.
Twelve animals were assigned to treatment groups (3 animals/group) that received single SC injections of CNTO311 at 0.1, 1.0, or 10.0 mg/kg or saline (control). Cohorts of 4 animals
Confidential Page 23 of 130

Teplizumab MacroGenics, Inc.
Investigator's Brochure Version 12.0, 16 November 2016
were established that contained 1 control animal and 3 animals treated at each of the 3 dose levels. Blood samples were collected pre-study, pre-dose, 0.5, 1, 6, and 24 hours, and on Study Days 3, 4, 8, 15, 36, and 43 for the evaluation of clinical pathology parameters, pharmacokinetics, lymphocyte cell populations, and cytokine production. The hOKT3γ1(ala,ala) test article (CNTO311, lot #5873:64) was produced in murine NS0 cells, purified and formulated at 100 mg/mL in 0.01M sodium phosphate, 8.5% sucrose, 0.01% polysorbate 80, pH 6.0 at the Centocor pilot production facility.
All doses caused a reduction of circulating CD3+ lymphocytes one day after CNTO311 administration. The magnitude of the initial reduction was not dose-level dependent. In the 0.1-mg/kg treatment group, CD3+ cell counts showed partial restoration at 14 days and full restoration by 42 days post-treatment. In the 1.0-mg/kg treatment groups, CD3+ cell counts remained reduced at 14 days, but returned to baseline levels at 42 days post-treatment. In the 10 mg/kg treatment group, depleted CD3+ cell counts persisted at 14 days and at 30–32 days post-treatment, the time at which the animals in this group, including the saline control, developed serious respiratory signs; all but 1 of the animals died or were euthanized. The fact that the saline control animal had the same symptoms suggests that the respiratory signs may not have been caused by the test product. The high dose was lethal, secondary to non-neoplastic B-cell lymphoproliferative disease attributable to T cell immunosuppression and recrudescence of EBV-like lymphocryptovirus infection.
T cells recovered from chimpanzees after CNTO311 treatment were responsive to in vitro re-stimulation by anti-CD3 and anti-CD28 antibodies in terms of cell proliferation and cytokine (interleukin-1 [IL-1], interleukin-10 [IL-10], tumor necrosis factor-alpha [TNF-α) production (data not shown). These responses were similar to those of T-cells from placebo animals. The data suggest that, although CNTO311 reduced the number of circulating T cells, the remaining T cells retained their responsiveness to re-stimulation. Teplizumab-treated animals showed a dose-dependent increase in various cytokines (TNF-α, IL-6, IL-10 and IFN-γ) with peak levels observed 6 hours post-dose. There were no treatment-related effects on body temperature, electrocardiogram (ECG), heart rate, blood pressure, or respiratory rate.
The calculated PK parameters are summarized in Table 2. Drug exposure (maximum plasma concentration [Cmax] and area under the curve [AUC]) increased with dose. The exposure to CNTO311 increased in a greater-than-dose-proportional manner in the dose range of 0.1 to 1.0 mg/kg, and then in a dose-proportional manner between 1.0 mg/kg and 10 mg/kg. No significant dose effect on tmax was detected. The median apparent terminal half-life values were 1.94, 3.68 and 5.20 days, respectively, for the 0.1, 1.0, and 10 mg/kg dose groups.
Confidential Page 24 of 130

Teplizumab MacroGenics, Inc.
Investigator's Brochure Version 12.0, 16 November 2016
Table 2 Summary of the Pharmacokinetic Parameters for CNTO311 in Chimpanzees after a Single SC Injection at 0.1, 1.0, or 10 mg/kg
Dose
(mg/kg)
Cmax
(g/mL)
*tmax
(day)
AUC
(g•day/mL)
AUC (0-t), t=7
(g ̣•̣day/mL)
*t½
(day)
0.1 0.39 ± 0.18 1.00 1.29 ± 0.27 1.17 ± 0.30 1.94
1.0 8.84 ± 2.99 2.00 72.94 ± 41.00 45.65 ± 18.61 3.68
10 60.46 ± 7.14 2.00 788.53 ± 169.13 348.80 ± 40.24 5.20
Values are mean ± SD. Data for tmax and t1/2 are median values.
In conclusion, a single subcutaneous dose of CNTO311 was generally well tolerated in chimpanzees at 0.1 mg/kg and 1.0 mg/kg doses. The highest dose of CNTO311 (10 mg/kg) caused significant morbidity, ultimately leading to the death of the animals in this group before the end of the study period. The high dose was lethal, secondary to non-neoplastic B-cell lymphoproliferative disease attributable to T cell immunosuppression and recrudescence of EBV-like lymphocryptovirus infection.
No adverse effects, except for the expected transient reduction of T cells, were found in the chimpanzees that received single SC injections of CNTO311 at doses of 0.1 or 1.0 mg/kg. These data indicate a no observed adverse effect level (NOAEL) of 1.0 mg/kg, which converts to a BSA normalized dose of 37,876 μg/m2. Relative to the chimpanzee NOAEL, the initial daily dose (51 μg/m2) has a safety factor of 743, and the highest daily dose has a safety factor of 46. The total doses for the full 14-day and full 6-day regimens (9034 μg/m2 and 2426 μg/m2) have safety factors of 4 to 15, respectively.
Substantial exposure to CNTO311 was observed in all drug-treated animals for at least 7 days. CNTO311 exposure (Cmax and AUC) increased with dose. The drug exposure in chimpanzees was observed to increase in a greater-than-dose-proportional manner in the dose range from 0.1 to 1.0 mg/kg, whereas it increased proportionally in the dose range of 1.0 to 10 mg/kg. No significant dose effect on tmax was detected after SC administration of CNTO311 in chimpanzees. The median tmax ranged from 1.00 to 2.00 days for the 3 dose groups (0.1, 1.0, and 10 mg/kg). The median apparent terminal half-life ranged from 1.94 to 5.20 days from 0.1 to 10 mg/kg, respectively, after SC administration; these results are in general agreement with half-life values for teplizumab in humans (see Section 5.2.6). The half-life changed with dose; it appeared to be shorter at the lower doses.
4.2.3 031-2101-09: Comparison of CD3 Epsilon Protein Sequences Between Species
This study evaluated the sequences of the CD3 epsilon protein from different species to assess the likelihood of cross-reactivity with OKT®3, the parent mAb of teplizumab. Human CD3 sequences were compared with published sequences from chimpanzee, rhesus macaque,
Confidential Page 25 of 130

Teplizumab MacroGenics, Inc.
Investigator's Brochure Version 12.0, 16 November 2016
cynomolgus macaque, marmoset, wallaby, sheep, pig, rabbit, dog, woodchuck, cat, rat, and mouse. The results support the conclusion that OKT®3 binding is restricted to humans, apes, and chimpanzees. It is therefore highly unlikely that any reactivity between teplizumab and any of these other species would occur.
4.2.4 031-2102-09: Binding of Teplizumab to Human CD3 and Binding of 2C11-mG2a(ala,ala) (Surrogate Antibody) to Mouse CD3
This study compared the binding of teplizumab to soluble human CD3 and the binding of 2C11-mG2a(ala,ala) (surrogate antibody) to soluble mouse CD3 using 2 methods of direct measurement of affinities between human and mouse CD3 and the corresponding antibody. Both approaches demonstrated a similarity in affinities between human CD3 ectodomain and teplizumab (Kd = 2.9 mcM) and between mouse CD3 ectodomain and 2C11-mG2a(ala,ala) (surrogate antibody) (Kd = 2.4 mcM).
4.2.5 MGA031-HL003: Cytokine Release In Vitro in Peripheral Blood Mononuclear Cells
Peripheral blood mononuclear cells (PBMCs) were obtained from subjects with psoriasis and healthy volunteers and exposed to teplizumab in doses ranging from 1 to 10,000 ng/mL and to positive and negative controls. The positive controls included OKT®3 at 100, 0.1, and 0.0001 ng/mL. Culture supernatants were collected 16 to 20 hours later for determination of IL-2, IL-4, IL-6, IL-10, TNF-α and interferon-gamma (IFN-γ) cytokine levels. There were no significant differences in cytokine induction in PBMCs purified from subjects with psoriasis or healthy volunteers. As expected, and consistent with its modified FcR binding profile, teplizumab induced much lower levels of cytokines than did OKT®3.
4.3 Toxicology
4.3.1 Bluestone Mouse Study: Single-Dose Toxicity Study in Mice
A general safety test was performed in which C57BL/6 mice received single doses of vehicle alone or hOKT3γ1(ala,ala) (teplizumab) test article at 5 or 10 mg/kg by IP injection and were monitored for 14 days. The study was performed at the University of Chicago FMI Animal Facility. No clinical toxicities were observed at either dose level, indicating a NOAEL of 10 mg/kg (the highest dose tested) for hOKT3γ1 (ala,ala) in mice.
4.3.2 PAI Study IM187: Human Tissue Cross-Reactivity
The cross-reactivity of teplizumab with normal human tissues was determined by using a biotinylated secondary goat anti-human IgG1 F(ab')2 and immunoperoxidase staining on a panel of snap-frozen tissue sections. Two concentrations of the mAb (300 and 2400 ng/mL) were tested. This GLP study, which utilized the recommended panel of tissues with 3 donors per tissue, was performed by Charles River Laboratories Preclinical Services – Pathology
Confidential Page 26 of 130

Teplizumab MacroGenics, Inc.
Investigator's Brochure Version 12.0, 16 November 2016
Associates, Frederick, Maryland, USA (PAI study No. IM187). The pattern of binding of the test article teplizumab was to putative T-lymphocytes in multiple tissues as predicted by previous immunohistochemical studies of CD3 distribution, most notably splenic T-cell regions, thymus, lymph nodes, and mucosa-associated lymphoid tissues. No unanticipated reactivity in non-target human tissues was observed.
4.3.3 7608-796: Cytokine Release in Mice Given Single-dose 2C11-mG2a(ala,ala) (Surrogate Anti-CD3 Antibody)
Mice given a single dose of 2C11-mG2a(ala,ala) (surrogate anti-CD3 antibody) at 0.65 or 19.5 mg/kg SC showed transient, slight increases (over baseline) in serum IL-6 and IL-12 levels. No increases were noted in the following cytokines: IL-1β, IL-2, IL-4, IL-5, IL-10, IL-17, granulocyte-macrophage colony-stimulating factor (GM-CSF), IFN-γ, or TNF-α. The current study indicated that 2C11-mG2a(ala,ala) (surrogate anti-CD3 antibody) produces a relatively minor effect on cytokine release in mice at SC doses up to 19.5 mg/kg. All animals survived until the scheduled sacrifice, and no compound-related clinical signs were observed.
4.3.4 7608-797: Repeat-dose Toxicity, Toxicokinetic, and Immunotoxicology Study of 2C11-mG2a(ala,ala) (Surrogate Anti-CD3 Antibody) in Mice
Daily administration of 2C11-mG2a(ala,ala) (surrogate anti-CD3 antibody) was well tolerated by mice when administered daily for 6 days by SC injection at dose levels of 0.0, 0.03, 0.3, or 20 mg/kg or by IV injection at a dose level of 0.3 mg/kg. There were no changes suggestive of target organ toxicity and the majority of the findings appeared to be related to the known pharmacology of 2C11-mG2a(ala,ala) (surrogate anti-CD3 antibody). Drug-related decreases in lymphocytes (T cell subsets) occurred at all dose levels and correlated microscopically with decreased cellularity in the thymus. These changes were still present at the end of the 6-week recovery phase but were not considered adverse because they were consistent with the known pharmacologic activity of 2C11-mG2a(ala,ala) (surrogate anti-CD3 antibody) and there was an indication of reversibility in these parameters at all dose levels. In general, 0.3 mg/kg given by either SC or IV route of administration resulted in similar hematological and microscopic changes. Based on these results, the no-observed-adverse-effect level (NOAEL) is considered to be 20 mg/kg SC.
4.3.5 M00255: Dose-ranging Study of 2C11-mG2a(ala,ala) (Surrogate Anti-CD3 Antibody) in Mice
A single-dose, dose-escalation study (non-GLP) was conducted with 2C11-mG2a(ala,ala) (surrogate anti-CD3 antibody) using SC doses that ranged from 0.03 to 60 mg/kg. In addition, IV doses of 10 and 30 mg/kg were administered during this study. After dosing (3/sex/group), each animal was observed for 72 hours. Results indicated that no treatment-related clinical signs were noted and no mortality occurred during this study. In male mice, T cells in the peripheral circulation were decreased by approximately 30% to 75% at SC doses of 0.1 to 10 mg/kg with a maximal effect (75%) at 0.3 and 1.0 mg/kg. In females,
Confidential Page 27 of 130

Teplizumab MacroGenics, Inc.
Investigator's Brochure Version 12.0, 16 November 2016
T cells were decreased by approximately 50% to 75% at doses of 0.1 to 1.0 mg/kg with a maximal effect (75%) at 0.3 and 1.0 mg/kg. These effects on T cells were not considered adverse since this was the expected pharmacologic action of 2C11-mG2a(ala,ala) (surrogate anti-CD3 antibody) in mice. Thus, the NOAEL for 2C11-mG2a(ala,ala) (surrogate anti-CD3 antibody) in this study was considered to be 60 mg/kg SC and 30 mg/kg IV, whereas the NOAEL for pharmacologic activity was 0.03 mg/kg. A dose of 60 mg/kg in mice is equivalent to 180,000 mcg/m2.
4.3.6 WIL-353187: Embryo-Fetal Development, Toxicokinetic and Immunophenotyping Study in Mice of 2851055 [2C11-mG2a(ala,ala)] (Surrogate Anti-CD3 Antibody) Administered SC on Gestation Days 6, 10, and 14
In an embryo-fetal developmental toxicity study, pregnant mice were administered the surrogate anti-CD3 antibody [2C11-mG2a(ala,ala)] (also designated as 2851055) by SC injection at dose levels of 0, 0.03, 0.3, or 20 mg/kg on Gestation Days (GD) 6, 10, and 14. A treatment-related increase in post-implantation loss occurred in the 20 mg/kg group as indicated by complete resorption of all implantations in 6 out of 26 pregnant mice. The incidences of 100% resorption were 0/26, 1/25, and 0/27 at doses of 0 (control), 0.03, and 0.3 mg/kg, respectively, compared with historical control incidence of 9/771 litters (equivalent to 1/86 litters). Because of the absence of a dose-response and the incidence being within the historical control range, the single animal with complete resorption in the 0.03-mg/kg group is considered a spontaneous event and not treatment related. No effects on fetal weight or fetal external morphology were identified at any dose level. In the 20 mg/kg group, lower mean maternal body weight gain, net body weight change, and food consumption were also observed. There were no effects on fetal weight or fetal external morphology at any dose level of the surrogate anti-CD3 antibody [2C11-mG2a(ala,ala)]. The NOAEL for both maternal toxicity and embryo/fetal developmental toxicity was considered to be 0.3 mg/kg. This is equivalent to a BSA-based dose of 11,157 mcg/m2.
4.3.7 WIL-353209: A Female Fertility and Early Embryonic Development, Toxicokinetic and Immunophenotyping Study in Mice of 2851055 [2C11-mG2a(ala,ala)] (Surrogate Anti-CD3 Antibody) Administered via SC Injection
This study assessed the potential adverse effects of the surrogate anti-CD3 antibody [2C11-mG2a(ala,ala)] on the reproductive process of female mice resulting from treatment from pre-mating, through conception to implantation including deficits in estrous cycling, tubal transport, implantation, and development of the pre-implantation stages of the embryo in the female. Female mice were given the surrogate anti-CD3 antibody [2C11-mG2a(ala,ala)] (also designated as 2851055) via subcutaneous injection at doses of 0, 0.3, 1.0, 3.0, and 20 mg/kg or a G2a(ala,ala) isotype control mAb at a dose of 20 mg/kg. Mice were treated every 3 days for 15 days prior to cohabitation, during the cohabitation period until mating was confirmed, and through Gestation Day 6 (Gestation Days 0, 3, and 6).
Confidential Page 28 of 130

Teplizumab MacroGenics, Inc.
Investigator's Brochure Version 12.0, 16 November 2016
Exposure was demonstrated in all treatment groups. No treatment-related effects were observed on female fertility, reproductive performance, or intrauterine survival up to Gestation Day 15 at any dose of the surrogate anti-CD3 antibody [2C11-mG2a(ala,ala)].
Based on the absence of compound-related effects including female fertility, reproductive performance, and intrauterine survival, the NOAEL for maternal, reproductive, and early embryonic developmental toxicity to the surrogate anti-CD3 antibody [2C11-mG2a(ala,ala)] was 20 mg/kg, the highest dose level evaluated. This is equivalent to a BSA-based dose of 743,800 mcg/m2.
4.3.8 WIL-353210: A Male Fertility, Toxicokinetic and Immunophenotyping Study in Mice of 2851055 [2C11-mG2a(ala,ala)] (Surrogate Anti-CD3 Antibody) Administered via SC Injection
In a study to determine the potential adverse effects of the surrogate anti-CD3 antibody [2C11-mG2a(ala,ala)] (also designated as 2851055) on the reproductive process resulting from treatment of male mice prior to, and during, the mating period male mice were given the surrogate anti-CD3 antibody [2C11-mG2a(ala,ala)] via subcutaneous injection at doses of 0, 0.3, 1.0, 3.0, and 20 mg/kg or the G2a(ala,ala) isotype control at a dose of 20 mg/kg. Male mice were treated every 3 days for 4 weeks prior to cohabitation, throughout the 2-week cohabitation period, and until 1 to 3 days prior to euthanasia (for a total of 15 doses). Female mice were not treated.
Exposure was demonstrated in all treatment groups. No treatment-related effects were observed on male fertility, reproductive performance, spermatogenic parameters, male reproductive organs, and intrauterine survival at any dose of the surrogate anti-CD3 antibody [2C11-mG2a(ala,ala)].
Based on the absence of effects on reproductive endpoints, the NOAEL for male reproductive toxicity and male-mediated embryo toxicity was 20 mg/kg 2C11-mG2a(ala,ala) (surrogate anti-CD3 antibody), the highest dose level evaluated. This is equivalent to a BSA-based dose of 743,800 mcg/m2.
4.3.9 WIL-353232: A Prenatal and Postnatal Development, Including Maternal Function, Toxicokinetic, Immunophenotyping and Antibody Assessment Study of 2851055 Administered Via Subcutaneous Injection in Mice
The purpose of this study was to determine the potential adverse effects of maternal exposure to Compound 2851055, also known as 2C11 mIgG2a(ala,ala), from conceptus implantation through weaning on pregnancy maintenance, parturition, and lactation in the maternal animals, and on the growth, viability, and development of the F1 offspring. Reproductive and behavioral performance of the F1 generation was also assessed. In addition to Compound 2851055, a comparator group was dosed with an IgG2 isotype. A toxicokinetic assessment of
Confidential Page 29 of 130

Teplizumab MacroGenics, Inc.
Investigator's Brochure Version 12.0, 16 November 2016
plasma levels of Compound 2851055 was performed, along with an immunophenotyping assessment of peripheral blood and a T-cell dependent antibody response conducted on the F1 generation. F0 female Crl:CD1(ICR) mice (30/group) were administered either Compound 2851055 at doses of 0, 0.3, 3.0, and 20 mg/kg, the IgG2a(ala,ala) comparator isotype at a dose of 20 mg/kg, or the vehicle control (10 mM NaPO4, 150 mM NaCl, and 0.005% polysorbate 80, pH 6.1) via subcutaneous injection in the scapular region on Gestation Days 6, 9, 12, 15, and 18 and on Lactation Days 1, 4, 7, 10, 13, 16, and 19. An additional 30 females/group, assigned only to the toxicokinetic phase, were given Compound 2851055 at doses of 0, 0.3, 3.0, or 20 mg/kg and were sampled for toxicokinetic evaluation at appropriate intervals following dose administration on Gestation Day 6 and Lactation Day 10 from the dams or Post-natal Day (PND 10) from the pups. Immunophenotyping assessment was conducted on an additional 20 females/group receiving Compound 2851055 at doses of 0, 0.3, 3.0, and 20 mg/kg or the IgG2a(ala,ala) isotype at a dose of 20 mg/kg. Samples were collected at appropriate intervals following dose administration on Gestation Day 6, Lactation Day 10, or PND 10. An additional 1 pup/sex from 10 litters selected from the pre-and postnatal development phase of the F1 generation were sampled for immunophenotyping assessment on PND 84.
All animals were observed twice daily for appearance and behavior. Clinical observations (including injection site observations), body weights, and food consumption were recorded at the protocol-specified intervals. All mated females were allowed to deliver and rear their offspring until Lactation Day 21 (F0) or 1 (F1). Indicators of F1 pup physical and functional development were evaluated as follows. Negative geotaxis assessment was performed on 1 pup/sex/litter beginning on PND 4. One pup/sex/litter from all available litters was selected for detailed clinical observation (DCO) testing on PND 11, 20, and 60, locomotor activity assessment on PND 21 and 61, acoustic startle response on PND 22 and 62, learning and memory assessment beginning on PND 70, while 1 pup/sex/litter from 10 litters were selected for T-cell dependent antibody response on PND 35 and 84. The F1 pups (1 pup/sex/litter) selected for evaluation of developmental landmarks were assigned to an F1 maturational phase, including reproductive functional assessment. The F1 animals in each group (1/sex/litter) were mated, avoiding sibling pairing. All F1 females were allowed to deliver and were housed with their offspring until Lactation Day 1, when the F1 females and F2 pups were euthanized. F1 males were necropsied near the end of the Lactation Day 1 F1 female necropsies. Sperm assessment was conducted on selected F1 males. The brain and reproductive organs were weighed from all F1 parental animals euthanized at the scheduled termination. Histological examination of reproductive and lymphoid tissues was conducted for F1 male animals that were found dead or euthanized in extremis, and for all F1 parental animals that survived to the scheduled necropsy.
In the F0 dams, mean serum concentrations increased with increasing dose between 0.3 and 20 mg/kg of Compound 2851055. Maternal exposure to 2851055 after a single subcutaneous dose was consistent with that previously observed in mice (Section 4.3.6 and Section 4.3.7). By comparing 2851055 serum concentrations following Gestation Day 6 dosing (Gestation Days 7, 8, and 9) to those following Lactation Day 10 dosing (Lactation Days 11, 12, and 13), maternal exposure to 2851055 was observed to decrease over time across treatment groups as expected. The observation that many mice had below the quantitation limit (BQL)
Confidential Page 30 of 130

Teplizumab MacroGenics, Inc.
Investigator's Brochure Version 12.0, 16 November 2016
concentrations on Lactation Day 12 or 13 in either the 0.3 or 3.0 mg/kg dose groups might be due to anti-2851055 antibodies, resulting in assay interference or alterations in Compound 2851055 clearance. Pooled serum samples from male and female pups were assessed for exposure to Compound 2851055 that was a result of placental transfer and/or transfer via maternal milk. Mean serum concentrations were all BQL in the control group of pups, and were mostly BQL in the 0.3 mg/kg group on PND 11 to 13. In both the 3.0 and 20 mg/kg dose groups, pup exposure to Compound 2851055 was observed on PND 11, 12, and 13.
No compound-related effects of administration of Compound 2851055 or the IgG2a(ala,ala) isotype were noted in F0 females during gestation or lactation. Parameters evaluated included F0 survival, clinical condition, body weight, body weight changes, food consumption, gestation length, and the process of parturition. Administration of Compound 2851055 or comparator isotype to F0 dams produced no effects on F1 postnatal survival, body weights, body weight changes, developmental landmarks, auditory startle response, locomotor activity, and learning and memory. The survival and development of the F2 pups were unaffected by administration of Compound 2851055 or comparator isotype to F0 dams at all dose levels.
Compound-related effects related to reproductive endpoints were limited to the F1 generation males and females administered 20 mg/kg of Compound 2851055 and included lower male and female fertility and conception/copulation indices and a lower percentage of motile sperm in F1 males compared to the vehicle control and the IgG2a(ala,ala) isotype groups.
Consistent with the expected pharmacology for this anti-CD3 monoclonal antibody, treatment at all dose levels in the F0 maternal mice caused a non-dose-related decrease in all circulating T lymphocytes and T subsets assessed. This decrease was accompanied by a corresponding increase in circulating B lymphocytes when evaluated on Gestation Day 6 and Lactation Day 10. Maternal exposure to test article had multiple effects on the immune system of the F1 generation. Similar to the maternal effects, decreases were observed in the T cell populations in animals in the F1 generation. In addition to this phenotypic analysis, an evaluation of the humoral immune response was performed. In animals from the 20 mg/kg group, significant decreases in the Primary IgM, Primary IgG, and Secondary IgG humoral responses to the T-dependent antigen (KLH) were observed in the F1 male and F1 female generation. The assessment of the immune system of the F1 generation also included an assessment of lymphoid organ weights and histology. Changes in organ weight histology were limited to the thymus and included increased thymic weights and increased cellularity of the medulla in mice in the 20 mg/kg group. Collectively, the assessments of the immune system indicate that maternal exposure had adverse effects on the developing lymphoid system as demonstrated by functional deficits in the humoral immune response.
Based on the absence of compound-related effects in F0 maternal animals at all dose levels, the no-observed-adverse-effect level (NOAEL) for maternal toxicity was 20 mg/kg of Compound 2851055. Compound-related lower male and female fertility and copulation/conception indices and a lower percentage of motile sperm were noted at 20 mg/kg of Compound 2851055 in the F1 generation. Based upon these results, the NOAEL for F1 reproductive toxicity was 3.0 mg/kg of Compound 2851055. The NOAEL for F1
Confidential Page 31 of 130

Teplizumab MacroGenics, Inc.
Investigator's Brochure Version 12.0, 16 November 2016
systemic toxicity was considered to be 3.0 mg/kg of Compound 2851055 based on the immune function deficits identified in F1 males and females at 20 mg/kg 2851055. Based on the lack of effects noted on survival and development of the F2 generation, 20 mg/kg of Compound 2851055 was considered the NOAEL for F2 developmental toxicity. The 20 mg/kg dose is equivalent to a BSA-based dose of 743,800 mcg/m2.
4.3.10 8233170: A Repeat-Dose Toxicity, Toxicokinetic, and Immunotoxicology Study in Mice Given Compound 2851055 by Intravenous Injection Every 3 Days for 1 Month with a 3 Month Recovery
The purpose of this study was to evaluate the toxicity, determine the toxicokinetics, and evaluate the potential immunomodulatory effects of Compound 2851055, when administered every 3 days by intravenous injection to mice for at least 1 month (10 doses) and to assess the reversibility, persistence, or delayed occurrence of any effects after a 3-month recovery. The study was terminated during Week 9 of the recovery phase.
A previous non-GLP study (2012-AI-100704) had investigated the incidence and severity of anaphylaxis induced by repeat courses of Compound 2851055 [2C11-mG2a(ala,ala)] administration in different strains of mice. In that study, anaphylaxis was observed in female TG1 mice. As TG1 was the preferred strain for toxicology studies, it was decided to proceed with the present study, expecting to observe some level of anaphylaxis upon repeat dosing.
Male and female mice were received from Charles River Laboratories, Raleigh, North Carolina. At initiation, the animals were 6 to 8 weeks old, and their body weights ranged from 26.9 to 38.1 g for males and 21.8 to 30.5 g for females. Each group received dose preparations containing the vehicle control article [10 mM sodium phosphate, 150 mM sodium chloride, and 0.005% (v/v) polysorbate 80 in sterile water for injection] or 0.3, 3.0, or 20 mg of Compound 2851055 per kg of body weight (mg/kg) at a dose volume of 2 mL/kg daily by intravenous injection. Assessment of toxicity was based on mortality, clinical signs, and food consumption. Necropsies were performed at the end of the dosing phase and for animals that died or were sacrificed at an unscheduled interval. Tissues were retained; however, microscopic examination was not conducted. Blood samples were collected for clinical pathology, toxicokinetic, immunophenotyping, and keyhole limpet hemocyanin evaluations. Samples for clinical pathology and immunophenotyping were analyzed but not interpreted, and samples for toxicokinetic and keyhole limpet hemocyanin were discarded without analysis.
A total of 19 compound-related deaths occurred during the dosing phase, including 4 animals given 0.3 mg/kg (3 males and 1 female) and 15 animals given 3.0 mg/kg (2 males and 13 females). Compound-related deaths first occurred following the fourth dose in animals given 0.3 mg/kg and after the fifth dose and continuing to the end of the dosing phase in animals given 3.0 mg/kg. Clinical signs observed in many animals found dead included some combination of swollen nose, irregular respiration, hypoactivity, and recumbency. The onset of clinical signs was within minutes of dose administration, and signs were consistent with an anaphylactic reaction. With the exception of 1 animal given 0.3 mg/kg found dead the
Confidential Page 32 of 130

Teplizumab MacroGenics, Inc.
Investigator's Brochure Version 12.0, 16 November 2016
following day, animals died within minutes or hours of administration of Compound 2851055. In addition, 1 male given 3.0 mg/kg died following the second dose and was replaced. Because the death of this animal was early in the dosing phase and was inconsistent with other deaths and clinical signs, it was not considered compound-related. Compound-related clinical signs included swollen nose, labored or irregular breathing, ataxia, hypoactivity, recumbency, and hunched appearance and occurred during the dosing phase in some animals given 0.3 or 3.0 mg/kg. The first appearance of compound-related clinical signs was on Day 10 of the dosing phase after the fourth dose in some animals given 0.3 mg/kg, followed by some animals given 3.0 mg/kg after subsequent doses. The onset of the majority of clinical signs was within minutes of dose administration and, for animals that survived, resolved within hours of onset.
In future repeat course of dosing studies we may evaluate the use of an allotype-matched host strain such as Balb/C in which less severe effects of the compound were observed. As this anaphylactic reaction was determined to be PAF-mediated and related to IgG antibodies directed at foreign portions of the antibody, it may be possible to administer PAF inhibitor to animals prior to dosing in such a study.
4.3.11 Discussion and Conclusions
The toxicology information that is most germane to the clinical safety of teplizumab was generated in a single-dose SC study in chimpanzees. In that study the highest dose of teplizumab, 10 mg/kg SC (equivalent to 378,758 μg/m2) caused significant morbidity, ultimately leading to the death or euthanasia of all but 1 of the animals in this group approximately 30 days after dosing, including the saline control. The morbidity and mortality at this dose were secondary to non-neoplastic B-cell lymphoproliferative disease attributable to T cell immunosuppression and recrudescence of EBV-like lymphocryptovirus infection. All doses caused a marked reduction in circulating T cells, although T cells at doses of 0.1 and 1.0 mg/kg returned to baseline values by 42 days post dosing. Teplizumab-treated animals showed a dose-dependent increase in various cytokines (TNF-α, IL-6, IL-10 and IFN-γ) with peak levels observed 6 hours post-dose. There were no treatment-related effects on body temperature, electrocardiogram (ECG), heart rate, blood pressure, or respiratory rate. No adverse effects were observed at doses of 0.1 or 1 mg/kg. Thus, the NOAEL for teplizumab in chimpanzees was 1 mg/kg (equivalent to 37,876 μg/m2).
Relative to the chimpanzee NOAEL, the initial daily dose (51 μg/m2) has a safety factor of 743, and the highest daily dose (826 μg/m2) has a safety factor of 46. The total doses for the full 14-day and full 6-day regimens (9034 μg/m2 and 2426 μg/m2, respectively) have safety factors of 4 to 15, respectively.
A human tissue cross-reactivity study demonstrated that teplizumab binds to T lymphocytes in multiple human tissues without unanticipated binding to other cell types. These results indicate that teplizumab has a low probability of producing unexpected, off-target toxicities in human clinical studies.
Confidential Page 33 of 130

Teplizumab MacroGenics, Inc.
Investigator's Brochure Version 12.0, 16 November 2016
A single dose of the surrogate anti-CD3 antibody [2C11-mG2a(ala,ala)] up to 19.5 mg/kg in mice produced only transient, slight increases in 2 (IL-6 and IL-12) of the 11 cytokines measured. This demonstrated that the alanine (ala,ala) substitutions engineered into this anti-CD3 monoclonal antibody were effective in reducing the interaction with Fc receptors and limiting T cell activation and cytokine release.
In the toxicity studies with the surrogate murine anti-CD3 antibody [2C11-mG2a(ala,ala)], there were no new or unexpected adverse effects identified with the exception of post-implantation loss in 6 of 26 pregnant mice given high doses, which were not confirmed in a subsequent study. Single doses of the surrogate anti-CD3 antibody [2C11-mG2a(ala,ala)] were well tolerated up to 60 mg/kg SC and 30 mg/kg IV. In the 6-day repeat-dose toxicity study, the primary observation in mice was a marked reduction in T cell counts within 24 hours after the first dose (at all dose levels), and T cell populations did not return to baseline levels following a 6-week non-dosing period. In the developmental toxicity study, pregnant mice administered the surrogate anti-CD3 antibody [2C11-mG2a(ala,ala)] at a dose of 20 mg/kg (60,000 μg/m2) on Gestation Days 6, 10 and 14 had an increased incidence of 100% resorption of implantations. The NOAEL in the developmental toxicity study was 0.3 mg/kg.
In a prenatal/postnatal development, maternal and reproductive toxicity study in Crl:CD1 (ICR) mice using the surrogate mouse antibody [2C11-mG2a(ala,ala)], there was no F0 maternal toxicity or F2 toxicity [NOAEL: 20 mg/kg administered 12 times for a 240 mg/kg total dose)]. In the F1 generation, compound-related lower male and female fertility, copulation/conception indices and a lower percentage of motile sperm were noted at 20 mg/kg. Consistent with the expected pharmacology for this anti-CD3 monoclonal antibody, treatment at all dose levels in the F0 maternal mice and the F1generation caused a non-dose-related decrease in the percentage of circulating T lymphocytes and T subsets, which was accompanied by a corresponding increase in the percentage of circulating B lymphocytes and impacted thymus size in F1 mice.
In conclusion, considering that the safety factors derived from the chimpanzee study are all 4 or higher and no new or unexpected toxicities were identified in the repeat-dose toxicity study in mice using the surrogate anti-CD3 antibody [2C11-mG2a(ala,ala)], results from the nonclinical studies support the safety of teplizumab for use in human subjects.
Confidential Page 34 of 130

Teplizumab MacroGenics, Inc.
Investigator's Brochure Version 12.0, 16 November 2016
5 EFFECTS IN HUMANS OF TEPLIZUMAB
5.1 Exposure to Teplizumab
A total of approximately 1093 study subjects have been enrolled in teplizumab studies and approximates of treatment groups are as follows (treated subjects= 1069): 823 subjects have received teplizumab, a total of 246 were in either the placebo or no treatment control group, and 24 subjects were enrolled but not treated. These estimates include approximately 32 subjects who have received teplizumab and 32 subjects who have received placebo from the current blinded At-Risk trial, based on a 1:1 randomization ratio of treatment with either teplizumab or placebo. Estimates of cumulative subject treatment exposure in IV teplizumab studies are presented in Table 3.
Table 3 Estimated Cumulative Subject Treatment Exposure from Intravenous Teplizumab Completed and Ongoing Studies
Treatment Number of Subjects a,b
No treatment control 27
Placebo 219 c
Teplizumab 823 c
Total 1069
a Exposure for subjects treated in blinded trials was estimated based on the randomization ratio b Integrated database excludes 5 subjects in the investigator-sponsored hOKT3-002 Islet Cell Transplantation
Trial c It is estimated that approximately 32 subjects have received teplizumab and 32 have received placebo in the
current ongoing, blinded At-Risk trial based on a 1:1 randomization ratio.
For completed studies, 791 subjects received IV teplizumab in studies across various indications: T1DM, renal or renal-pancreatic allograft rejection, induction immunotherapy in pancreatic islet transplant recipients, and psoriatic arthritis studies. Data from 5 subjects in an early investigator-sponsored trial (islet-cell transplant) were not available electronically, have only been provided in abbreviated CSRs, and are not included in the tables below. Data on age and gender are presented in Table 4 and show subjects who received treatment with teplizumab in completed studies.
Confidential Page 35 of 130

Teplizumab MacroGenics, Inc.
Investigator's Brochure Version 12.0, 16 November 2016
Table 4 Cumulative Subject Exposure to Intravenous Teplizumab from Completed Clinical Trials by Age and Sex a,b
Number of Subjects
Age Group Females Males Total
Children (2-11 Years) 73 93 166
Adolescents (12-17 Years) 99 210 309
Adults (18-65 Years) 115 200 315
Elderly (> 65 years) 0 1 1
Total 287 504 791
a Includes subjects from completed or unblinded trials as of 23 August 2016. b Integrated database excludes 5 subjects in the investigator-sponsored hOKT3-002 Islet Cell
Transplantation Trial and 64 subjects in the ongoing blinded ISCT-MGA031-005 “TN-10 At-Risk”) trial.
Information regarding teplizumab activity and safety in these studies is discussed in Sections 5.4 and 5.5, respectively, and in Section 6. For treatment-emergent adverse events (TEAEs) and serious TEAEs that are considered by MacroGenics to be adverse drug reactions (ADRs) for patients receiving teplizumab, see Section 6.7 (Reference Safety Information [RSI]).
5.2 Clinical Pharmacology
Three open-label PK studies were completed in T1DM (Study 1, Study 2, and Study 3). Additional PK data were collected in open-label Segment 1 of the Protégé study (CP-MGA031-01), and limited PK data were captured in the double-blind Segment 2 of the Protégé study. Limited additional PK data were collected in study CP-MGA031-03 (Protégé Encore). Although not included in this IB, one open-label PK study was completed in renal allograft rejection (Study 8223); and one open-label PK study was completed in psoriatic arthritis (Study 8907).
5.2.1 Study 1 (Dr. Kevan Herold, Sponsor-Investigator)
Objective: To assess safety, tolerability, biological effects, PK, and immunogenicity of teplizumab in subjects aged 8–30 years with newly-diagnosed T1DM.
Design: Study 1 was a randomized, controlled, 3-center, Phase 1/2 study. Twenty-two subjects with newly diagnosed (≤ 6 weeks) T1DM were randomized to receive treatment with teplizumab (1 of 2 dosing regimens) plus standard-of-care treatment, and 21 control subjects were randomized to receive standard-of-care treatment only. The teplizumab dosing regimens were as follows:
Group A (n = 12): Study Day 1: 1.42 μg/kg; Study Day 2: 5.7 μg/kg; Study Day 3: 11.3 μg/kg; Study Day 4: 22.6 μg/kg; Study Days 5–14: 45.4 μg/kg.
Confidential Page 36 of 130

Teplizumab MacroGenics, Inc.
Investigator's Brochure Version 12.0, 16 November 2016
Group B (n = 10): Study Day 1: 455 μg/m2; Study Day 2: 919 μg/m2; Study Days 3–12: 1818 μg/m2.
Subjects receiving teplizumab were followed for 24 months to evaluate safety, tolerability, and potential therapeutic activity. Subjects in the control group were followed for metabolic outcomes but were not evaluated for AEs.
Status: Study completed.
Pharmacokinetics/Pharmacodynamics (PK/PD): Subjects in both dosing groups received a mean total dose of 26 mg of teplizumab. The mean steady-state trough level for teplizumab in evaluable subjects from Study Day 8 to Study Day 12 was 129 ng/mL (see Table 5). The level of CD3 coating varied between 57% and 66% (mean levels were 57% for CD4+ cells and 59% for CD8+ cells), and the modulation of CD3 varied between 37% and 57% (mean levels were 50% for CD4+ cells and 53% for CD8+ cells).
Table 5 Study 1 in T1DM: Serum Trough Levels a from Study Days 8–12
Study Day 8 9 10 11 12
Subject No. Daily Maintenance Dose: 1818 μg/m2 Mean (ng/mL)
001/014 80.5 90.4 123.1 179.9 132.6 121
002/021 214.7 267 380 222 407 298
001/015 66.6 41 172 40 35.1 71
001/020 57.1 136.4 27 247 227 139
001/017 27.6 14.2 36.6 12.4 25.4 23
001/013 32.1 36 40.3 44.1 67.3 44
001/016 164 212 274 166 209 205
Mean 92 114 150 130 158 129
Std Dev 71 96 135 96 136
Abbreviations: Std Dev = standard deviation.
a Trough levels were measured by a flow-competition assay before the a.m. dose and are expressed in ng/mL. Serum drug levels were available for 9 of the 10 subjects in Group B. The study drug (Lots Nos. N11007F1 and N11007F2) was heated and filtered before administration. However, the data from 2 subjects were excluded from the table. One subject was excluded because of preexisting antibodies that interfered with the flow competition assay. The other subject was excluded because of receiving a different lot of study drug (Lot Nos. 950907 and 951002) that was not heated or filtered before administration.
Efficacy: The primary metabolic outcome in this study was the proportion of subjects who maintained or increased the total area under the curve (AUC) of the C-peptide response to a mixed meal tolerance test (MMTT). At 12 months, 15 of 21 subjects treated with teplizumab maintained or increased their C-peptide response, whereas only 4 of 19 control subjects showed similar outcomes (p = 0.002). Although C-peptide responsiveness declined beyond 1 year, the statistically significant difference in C-peptide responses persisted for at least
Confidential Page 37 of 130

Teplizumab MacroGenics, Inc.
Investigator's Brochure Version 12.0, 16 November 2016
2 years. Statistically significant differences were also reported for HbA1c levels and total insulin dosage. Both dosage regimens (A and B) produced similar results in terms of pharmacodynamic effects and clinical outcomes.
Safety: All 22 subjects who received teplizumab experienced at least 1 AE. A total of 184 AEs were reported, of which 181 (98%) were either Grade 1 or Grade 2. There were 3 (2%) Grade 3 events (catheter-related infection, hypoglycaemia NOS and thrombocytopenia). No Grade 4 or 5 (fatal) AEs were reported.
The most common AEs were headache, rash, pyrexia, nausea, upper respiratory tract infection, myalgia, dermatitis exfoliative, vomiting, arthralgia, fatigue, rigors, and gastroenteritis viral. Two serious adverse events (SAEs) were reported in 2 subjects (Grade 3 catheter-related infection and Grade 3 thrombocytopenia).
Conclusions: This study provides evidence that teplizumab, administered based on either weight or body-surface area, is generally well tolerated, has biologic effects on immune cell function suggestive of the induction of Treg cells, ameliorates the loss of pancreatic beta cell function, facilitates improved control of blood glucose, and reduces insulin requirements. The study justified continued development of teplizumab for treatment of recent-onset T1DM.
5.2.2 Study 2 (Protocol ITN007AI [NDB01], Dr. Kevan Herold, Sponsor-Investigator)
Objectives: This Phase 2 study was intended to study the clinical and immunological effects of 3 cycles of treatment with teplizumab administered at intervals of 6 months.
Design: The study enrolled subjects aged 9 –20 years to receive teplizumab according to the group B dosing regimen used in Study 1 (see Section 5.2.1).
Status: Study completed. Ten subjects with newly diagnosed T1DM (< 6 weeks) were enrolled at 3 sites before enrollment and treatment were stopped for safety reasons. Of these 10 subjects, 6 received teplizumab.
PK/PD: Subjects received a mean dose of 32.6 mg of teplizumab over 12 days. The mean steady-state trough level for teplizumab in evaluable subjects from Study Day 8 to Study Day 12 was 1038 ng/mL, which is approximately 8-fold higher than in Study 1 (see Table 6). The level of CD3 coating varied between 64% and 83% (mean levels were 78% for CD4+ cells and 78% for CD8+ cells). The mean levels of modulation of CD3 were 64% for CD4+ cells and 63% for CD8+ cells).
Confidential Page 38 of 130

Teplizumab MacroGenics, Inc.
Investigator's Brochure Version 12.0, 16 November 2016
Table 6 Study 2 (ITN007AI) in T1DM: Serum Trough Levels a from Study Days 8–12
Study Day 8 9 10 11 12
Subject No. Daily Maintenance Dose: 1818 μg/m2 Mean (ng/mL)
CUH01/001 642 788 1021 950 534 787
CUH01/002 840 996 948 1265 788 967
CUH01/004 806 820 918 1031 ND 894
VMM01/001 ND 1314 1233 1317 842 1177
VMM01/002 718 1556 792 722 283 814
USF01/001 1662 1735 1711 1716 1462 1657
Mean 934 1202 1104 1167 782 1038
Std Dev 415 395 331 346 441
Abbreviations: ND = not determined; Std Dev = standard deviation. a Trough levels were measured by a flow-competition assay before the a.m. dose and are expressed in ng/mL
Serum drug levels were obtained from the 6 treated subjects. The study drug (Lot Nos. 950907 and 951002) was not heated or filtered before administration.
Further enrollment and study drug administration were discontinued after an increase in the incidence and severity of various side effects, as compared with Study 1. After investigation, these differences in the severity of AEs were ascribed to an unexpected increase in the dose of study drug administered in Study 2 compared with the actual dose administered in Study 1. Investigation revealed that in Study 1, approximately 40% of the drug product was lost during the heating and filtration steps done before preparation of the drug dose. Filtration before preparation of the drug dose in Study 2 was discontinued because the lots of teplizumab used in this study were produced by a process that included two orthogonal downstream robust virus removal/inactivation steps and did not include in-vial heat inactivation of viruses. Therefore, the amount of drug actually given to subjects in Study 1 was closer to 60% of the planned dose. The higher drug levels in Study 2 reflected an approximately 2-fold greater amount of actual IV-administered study drug compared with Study 1.
The finding that mean drug levels in Study 2 were about 8-fold higher than those in Study 1, however, suggests a non-linear relation between administered dose and steady-state drug levels. The non-linear relationship may be explained by saturation of CD3 binding sites on T cells with resulting increased free teplizumab levels. These findings were factored into the dosing amounts used in Study 3, a PK study, and ongoing studies that are described earlier in this report. Study 3 replicated the steady state drug levels obtained in Study 1.
Efficacy: Dr. Herold followed 4 of the 6 teplizumab-treated subjects for 60 months (5 years). While the conclusion was that AEs were increased without improved efficacy as compared with Study 1, there was an insufficient number of subjects to adequately evaluate efficacy.
Confidential Page 39 of 130

Teplizumab MacroGenics, Inc.
Investigator's Brochure Version 12.0, 16 November 2016
The study results indicated that the 4 subjects maintained C-peptide over a 5-year period (27).
Safety: All 6 subjects exposed to teplizumab experienced at least 1 AE, with a total of 205 AEs reported among them. One hundred forty-eight (72%) AEs were Grade 1, 49 (24%) AEs were Grade 2, and 8 (4%) AEs were Grade 3 (4 AEs of lymphopenia, 1 each of tympanic membrane perforation, pyrexia, CD4 lymphocyte decreased, and hyperglycaemia). No Grade 4 or 5 (fatal) AEs were reported. The most common AEs experienced were lymphopenia, nausea, pyrexia, rigors, vomiting, headache, rash, pain, cough, nasopharyngitis, and sweating increased.
Two SAEs were reported in subjects treated with teplizumab: 1 subject experienced tympanic membrane perforation and 1 subject experienced CD4 lymphocytes decreased.
Conclusions: The results of Study 2 demonstrate that increased amounts of administered drug result in higher serum drug levels and probably more severe and frequent AEs. There is a non-linear relationship between administered drug and drug level. Steady state drug levels similar to Study 1 are adequate to produce biological activity with an acceptable AE profile. The steady state drug levels unintentionally produced in Study 2 resulted in excessive CD4+ lymphopenia, which investigators do not consider to be required to produce therapeutic activity.
5.2.3 Study 3 (Protocol ITN017AI, Dr. Kevan Herold, Sponsor-Investigator)
Objective: The goal was to identify a dosing regimen that resulted in predictable steady state drug levels and an AE profile similar to the profile observed in Study 1.
Design: This was a Phase 1 pharmacokinetic and safety study in 6 subjects aged 8–30 years who had been diagnosed with T1DM within the last 12 months. All subjects received teplizumab. The doses used for the first cohort of subjects were as follows:
Study Day 1: 227 μg/m2
Study Day 2: 459 μg/m2
Study Days 3–12: 919 μg/m2
This dosing regimen represents 50% of the dosing regimen for Group B from Study 1. The 50% reduction in dose was the correction factor applied for the 40% drug loss in Study 1 that had occurred due to heating and filtering the study drug, as discussed above. No heating or filtering of study drug was done during study drug preparation for Study 3.
Status: Study completed.
Confidential Page 40 of 130

Teplizumab MacroGenics, Inc.
Investigator's Brochure Version 12.0, 16 November 2016
PK/PD: Five subjects were enrolled in the first cohort, 4 of whom received the full dosing regimen. The mean drug total for these 4 subjects was 18.3 mg. The mean steady state trough level in these subjects from Study Day 8 to Study Day 12 was 99 ng/mL (Table 7), which was similar to the steady state level in Study 1 (see Section 5.2.1). The mean levels of CD3 coating were 67% for CD4+ cells and 66% for CD8+ cells, and the mean levels of modulation of CD3 were 43% for CD4+ cells and 53% for CD8+ cells.
Table 7 Study 3 (ITN017AI) in T1DM: Serum Trough Levelsa from Study Days 8–12
Study Day 8 9 10 11 12
Subject No. Daily Maintenance Dose: 919 μg/m2 Mean (ng/mL)
001/001 31 46 57 106 86 65
001/003 38 73 123 55 86 75
002/001 100 65 112 135 143 111
002/002 102 86 213 160 165 145
Mean 68 68 126 114 120 99
Std Dev 39 17 65 45 40
Abbreviations: Std Dev = standard deviation.
a Trough levels were measured by a flow-competition assay before the a.m. dose and are expressed in ng/mL. Serum drug levels were obtained from the 4 treated subjects. The study drug (Lot Nos. 950907 and 951002) was not heated or filtered before administration.
Efficacy: Not applicable.
Safety: Because the measured drug levels were low and stopping criteria were not met, a sixth subject was enrolled to receive a dose 25% higher than the previous subjects. This subject, a 17-year-old male, developed Grade 4 direct hyperbilirubinemia after receiving the second dose of teplizumab IV 531.0 mcg and 1073 mcg on Day 1 and Day 2, respectively. The event was associated with pyrexia, nausea, vomiting, and headache, and with laboratory evidence of consumptive coagulopathy. The subject was hospitalized, and the event resolved 22 days after its onset. The serum level of study drug measured 1 hour after the first infusion was 509 ng/mL. By comparison, 3 other subjects of the 5 evaluable subjects in this study had undetectable drug levels at the same time point, and the fourth subject had a drug level of 31 ng/mL. These differences in acute drug levels were not explained by dosing error. No other data are available to address this observation. Because this event met criteria for a dose-limiting toxicity, no further subjects were enrolled in this study.
Five of the 6 subjects treated experienced at least 1 AE. A total of 94 AEs were reported. Sixty-three (67%) AEs were Grade 1, 19 (20%) AEs were Grade 2, 11 (12%) AEs were Grade 3 (7 events of lymphopenia in 3 subjects, 1 each of ALT increased, haptoglobin decreased, platelet count decreased, and rash NOS). One event (1%) was a Grade 4 hyperbilirubinaemia. No Grade 5 (fatal) AEs were reported. The most common AEs
Confidential Page 41 of 130

Teplizumab MacroGenics, Inc.
Investigator's Brochure Version 12.0, 16 November 2016
experienced were lymphopenia, headache, nausea, upper respiratory tract infection, monocyte count increased, and pharyngolaryngeal pain.
One SAE, a Grade 4 hyperbilirubinaemia, was reported. This was thought to be cytokine release mediated.
Conclusions: For cohort 1, this study replicated the steady state study drug levels of Study 1. The study showed an overall AE profile similar to that observed in Study 1 and improved compared with Study 2. A single subject in the dose-escalation cohort exhibited a syndrome consistent with severe cytokine release.
5.2.4 Protégé Study (Protocol CP-MGA031-01)
The pharmacokinetics of teplizumab were determined using a population pharmacokinetic analysis (performed by QuantPharm LLC) of 451 diabetic subjects from the Protégé study treated with the full 14-day regimen (53.8%), the 1/3 14-day regimen (23.5%), and the full 6-day regimen (22.8%). In open-label Segment 1, serum teplizumab samples were taken pre- and post-dose, on every dosing day, and on days 14, 28, 56, 196, 210, 224, and 273. In the double-blind Segment 2, serum teplizumab samples were taken pre-dose, days 0 and 182 of dosing, days 5 and 187 of dosing, and on days 14, 28, 56, 196, 210, 224, and 273.
The pharmacokinetics of teplizumab following intravenous administration were described by a two-compartment model with saturable binding in central and peripheral compartments. Clearance of teplizumab was estimated to be 2.3 L/day (33.1% coefficient of variation [CV]); central volume of distribution was 3.4 L, and the peripheral volume of distribution was 6.9 L, resulting in a volume of distribution at steady state of 10.4 L. At concentrations much higher than the binding capacity of the target (129 ng/mL), teplizumab pharmacokinetics were characterized by bi-exponential decay with the distribution and terminal half-lives of t1/2α=0.19 day (SD=0.22 day) and t1/2β = 4.01 days (SD = 1.75 days), respectively. Clearance following 1/3 14-day and full 6-day regimens was higher than following the full 14-day regimen.
For typical subjects without immunogenic reaction administered the full 14-day regimen, the predicted mean (± SD) total AUC was 6421 ± 1940 ng•day/mL. Day 14 Cmin and Cmax of teplizumab were 418 ± 225 ng/mL, and 826 ± 391 ng/mL, respectively. The accumulation ratio for AUC between Day 5 and Day 14 (the first and the last day with the full dose administration) was 3.43 ± 1.16. With a BSA-proportional dose, teplizumab AUC, Cmin, and Cmax were independent of body weight. There was no evidence of clinically relevant dependencies of pharmacokinetics on age, gender, race, region, baseline CD4+ and CD8+ cell counts, disease state or disease onset time.
Teplizumab pharmacokinetics were influenced by immunogenic response. First, teplizumab clearance increased with maximum observed ADA concentrations. Clearance in cycle 1 was increased by up to 67% in subjects with high ADA concentrations (22 mcg/mL) observed after cycle 1 dosing. The effect of immunogenicity on clearance in cycle 2 was stronger, with clearance increasing by up to 105% in subjects with high ADA concentrations observed after
Confidential Page 42 of 130

Teplizumab MacroGenics, Inc.
Investigator's Brochure Version 12.0, 16 November 2016
cycle 1 dosing. In addition, clearance in cycle 2 increased by up to 194% in subjects with high ADA concentration (3 mcg/mL) observed during cycle 2 dosing.
In addition, some subjects demonstrated a strong immunogenic response, which was described as an abrupt reduction of bioavailability and increase in clearance after about 10 days of cycle 2 dosing (cycle 1 pharmacokinetics were not affected by the strong immunogenic response). Among 30 subjects in Segment 1 that had concentration profiles in cycle 2 (with the full 14-day regimen), this strong immunogenicity was observed in 37% of subjects. For the sparse data of Segment 2, strong immunogenicity was estimated to occur in 47.5% (10% RSE) and 65.0% (13% RSE) of subjects administered the full 14-day and 1/3 14-day regimens, respectively. In these subjects, the immunogenic reaction was assumed to be developed after 10 days of dosing and resulted in a decrease of bioavailability to zero and in up to a 438% increase in clearance proportional to the log of maximum ADA concentrations observed after the end of cycle 2 dosing.
The predicted concentration-time courses following the full 14-day regimen are illustrated in Figure 4. The influence of weight and gender on teplizumab exposure is negligible. Teplizumab pharmacokinetics were influenced by an immunogenic response, as measured by presence of ADA, that significantly decreased exposure. The predicted concentration-time courses following the full 14-day regimen for subjects with the strong immunogenic response are shown in Figure 5, which illustrates expected variability of teplizumab concentrations.
Confidential Page 43 of 130

Teplizumab MacroGenics, Inc.
Investigator's Brochure Version 12.0, 16 November 2016
Figure 4 Simulated Concentration-Time Course in Cycle 1 following the Full 14-Day Regimen
The red line illustrates the prediction for a typical 60 kg male subject with no observed ADA.
Confidential Page 44 of 130

Teplizumab MacroGenics, Inc.
Investigator's Brochure Version 12.0, 16 November 2016
Figure 5 Simulated Concentration-Time Course in Cycle 2 Following the Full 14-Day Regimen: Subjects with Strong Immune Response
In each plot, the red line illustrates the prediction for a typical 60 kg male subject with no observed ADA. The blue line illustrates the prediction for a subject with no observed ADA but strong immune response on Day 10.
5.2.5 Anti-drug Antibodies in Humans
Immunogenicity was studied in CP-MGA031-01(Protégé). In both the open-label Segment 1 and double-blind Segment 2, serum ADA samples were taken on days 0, 28, 56, 91, 182, 201, 224, 273, 364, 546, and 728. However, after the DMC determined that the primary endpoint was not met for the Segment 2 subjects in CP-MGA031-01, ADA samples were no longer collected to decrease the burden on the subjects.
Levels of ADA were assayed using a ‘bridging’ (or sandwich) ELISA format where teplizumab was used as both the coating and detecting reagent. Table 8 shows the incidence and extent of ADA levels in subjects that received teplizumab. The proportion of subjects with ADA levels was similar between cycles within a regimen; however, higher levels of immunogenicity were seen in cycle 2 for the three teplizumab regimens.
Confidential Page 45 of 130

Teplizumab MacroGenics, Inc.
Investigator's Brochure Version 12.0, 16 November 2016
Table 8 Incidence of Subjects Who Developed ADA and the Extent of ADA Response (Protégé Study)
ADA titer range (ng/mL)a
Regimen Rx Course Incidence (% subjects) <103 (%) 1-5x103(%) >5×103(%)
Full 14-Day 1st 55.5 92.8 0.03 0.04
2nd 59.5 44.5 36.1 19.3
1/3 Full 14-Day 1st 56 94.6 0.05 0
2nd 64 29.7 34.4 35.9
Full 6-Day 1st 68 82.4 10.3 7.4
2nd 77 33.8 27.3 39.0
a The subjects with positive ADA titer were classified into three classes based on the extent of ADA response; (ng/mL refers to a rabbit polyclonal anti-idiotypic standard not actual human anti-drug antibody).
There did not appear to be a significant correlation, however, between ADA titers and either the changes in C-peptide or with response using the modified composite HbA1c + insulin usage endpoint. Table 9 provides a cross tabulation of C-peptide and ADA levels. ADA levels were categorized as noted in the tables. C-peptide change from baseline was divided into quartiles (lowest = those with the largest negative change) for both Day 364 and Day 728. These results suggest that despite high ADA levels some subjects achieved a change in C-peptide level that placed them in the highest quartile of change from baseline. For example, at Day 364, 40 of the 55 subjects in this highest quartile experienced some level of ADA thought to be neutralizing (ADA>100).
Table 9 Maximum ADA by Quartile of C-peptide Change from Baseline – Days 364 and 728, Full 14-Day Regimen
Quartile C-peptide
(Log AUC+1) ADA<100 100-1000 1000-1500 1500-5000 >5000
Day 364
Lowest 9 11 2 3 10
2nd 7 16 5 5 16
3rd 17 14 5 2 11
Highest 15 19 6 4 11
Day 728
Lowest 18 4 0 1 0
2nd 25 8 1 0 0
3rd 28 5 2 1 0
Highest 26 10 0 1 1
Confidential Page 46 of 130

Teplizumab MacroGenics, Inc.
Investigator's Brochure Version 12.0, 16 November 2016
5.2.6 Overall Conclusions about PK in Humans
Increased amounts of administered teplizumab result in higher serum drug levels (Table 10). However, there is a non-linear relationship between administered drug and drug level, which may be explained by saturation of binding sites and resultant increases in free teplizumab levels at higher dosages concomitant with a reduction in circulating CD3+ T cells.
Table 10 Summary of Teplizumab Pharmacokinetic Data in Humans
Indication: Study Maintenance
dose
Mean trough
level (ng/mL)
Mean CD3
coating in
CD4+; CD8+
cells (%)
Mean CD3
modulation in
CD4+; CD8+
cells (%)
Mean half-
life (days)a
Renal allograft rejection: Study 8223
5–10 mg b ≥1,000 N/A N/A 5.9
Psoriatic Arthritis: Study 8907
4 mg c 215 ~100 50 N/A
T1DM: Study 1 1818 g/m2 129 57; 59 50; 53 0.7–3.0
T1DM: Study 2 (Protocol ITN007AI)
1818 g/m2 1038d 78; 78 64; 63 1.1–1.6
T1DM: Study 3 (Protocol ITN017AI)
919 g/m2 99 67; 66 43; 53 N/A
T1DM: Protégé (Protocol CP-MGA031-01)e
826 g/m2 418 ± 225 N/A N/A 4.0 ± 1.75
Abbreviations: N/A = not available. a Due to the sparsity of data after the completion of dosing, the half-life values are only rough estimates.
b For subjects weighing 70 kg and having a BSA of 1.92 m2, this dose corresponds to 2600–5208 g/m2.
c For subjects weighing 70 kg and having a BSA of 1.92 m2, this dose corresponds to 2083 g/m2.
d Trough levels in Study 2 were unexpectedly elevated. The study drug had been prepared by a procedure that omitted a heating and filtration step utilized in previous studies. Investigation revealed that the heating and filtration steps caused a reduction in the amount of administered study drug. Thus, the amount of actual IV-administered study drug in Study 2 was ~2-fold greater than in Study 1. Because of an apparent non-linear relation between administered drug and steady state drug level, the ~2-fold increase in administered drug led to ~8-fold higher drug levels.
e For a typical 60-kg male subject without immunogenic response receiving the 14-day full regimen.
Subjects in Studies 1 and 3 had similar drug levels despite different nominal dosing regimens, a result explained by a change in the technique for drug preparation between manufactured lots. The similar drug levels in these studies were accompanied by similar pharmacodynamic effects measured by coating and modulation of the CD3 molecule. These findings support the utilization of a dosing strategy, such as the full 14-day regimen, that targets serum trough levels of approximately 100–200 ng/mL.
Confidential Page 47 of 130

Teplizumab MacroGenics, Inc.
Investigator's Brochure Version 12.0, 16 November 2016
In contrast, subjects in Study 2 had distinctly higher drug levels than in Study 1, despite the same nominal dosing regimen. This result is also explained by different techniques for drug preparation between the studies. Coating and modulation were higher in Study 2 (Table 10), but there is no evidence that such degrees of coating and modulation are required for biologic activity. A trend toward higher circulating cytokine levels was observed in Study 2 subjects compared with Study 1 subjects (7).
Population PK analyses from CP-MGA031-01 (Protégé) demonstrate a two-compartment model with saturable binding in central and peripheral compartments. With BSA-proportional dose, teplizumab AUC, Cmin, and Cmax were independent of body weight. There was no evidence of clinically relevant dependencies of PK on age, gender, race, region, disease state or onset. Peak levels occur on Day 14 of dosing. Teplizumab pharmacokinetics were influenced by immunogenic response, but this did not uniformly correlate with change in C-peptide or insulin use.
5.3 Clinical Studies with Teplizumab
A summary of the ongoing and completed studies for Teplizumab are presented in Table 28 and Table 29.
Studies evaluating the efficacy of teplizumab are presented below by indication and study.
5.3.1 Type I Diabetes Mellitus (T1DM)
Type 1 Diabetes Mellitus (T1DM) is an organ-specific autoimmune disorder mediated by T lymphocytes. It is presumed that initial injury to the -cells by an environmental agent, possibly a virus, precipitates a T-lymphocyte-dependent autoimmune attack on the -cells in the pancreas, resulting in progressive destruction of the capacity to produce insulin and, eventually, clinical onset of diabetes and its associated irreversible morbidities and accelerated mortality (33, 42). Data from animal studies (discussed in Section 4) and preliminary data from studies of teplizumab use in humans indicate that the autoimmune attack on the pancreatic beta cells can be slowed with short-term treatment with antibodies that bind CD3 but do not bind Fc receptors (2, 3, 7, 13, 24-26).
Three studies of teplizumab in subjects with recent-onset T1DM (Study 1, Study 2 and Study 3) have been completed under the direction of Dr. Kevan Herold (currently at Yale University) under a single IND (BB-IND #7428) (25, 26). Two additional studies (Study 4 “AbATE” and Study 5 “Delay” (29) were also conducted by Dr. Herold. Studies 2, 3 and 4 were sponsored by the Immune Tolerance Network.
Four additional studies of teplizumab in T1DM were conducted by the Sponsor: 3 with intravenous administration (Protégé, Protégé Extension and Protégé Encore, see Section 5.3.1.1.5) and 1 with subcutaneous administration (SUBCUE, see Section 5.3.1.1.4) of teplizumab. Several dosing regimens were investigated in more than one study and are shown in Table 11.
Confidential Page 48 of 130

Teplizumab MacroGenics, Inc.
Investigator's Brochure Version 12.0, 16 November 2016
In October 2010, a DMC review of 1-year data from the 2-year CP-MGA031-01 study disclosed that the primary efficacy endpoint (a composite of HbA1c < 6.5% and insulin < 0.5 U/kg/day) was not met in the study. However, no unanticipated safety issues were identified. As a result of missing the primary efficacy endpoint in this study, the Sponsor and its partner, terminated enrollment in Protocol CP-MGA031-02 (Protégé Extension) and enrollment and dosing in Protocols CP-MGA031-03 (Protégé Encore) and CP-MGA031-06 (SUBCUE). In CP-MGA031-01 and CP-MGA031-03, subjects continued in the study for follow-up of safety endpoints and clinical endpoints associated with the standard of care of diabetes (HbA1c, insulin, and fasting C-peptide), consistent with the DMC recommendations. Investigator-sponsored studies continued unchanged after disclosure of the DMC finding to the other studies.
Table 11 T1DM Dosing Regimens
Regimen
Name
Former
Name Description
Studies Used
In a
Full 14-day regimen
Herold regimen, or
Classic Herold regimen
14-day course of teplizumab Once-daily IV doses
51 μg/m2 (Day 1), 103 μg/m2 (Day 2), 207 μg/m2
(Day 3), 413 μg/m2 (Day 4), and 826 μg/m2 (Days 5–14)
Total cumulative avg. dose = ~17 mg
AbATE; Delay; Protégé;
Encore; “At Risk” study
One-third 14-day regimen
One-third Herold regimen
14-day course of teplizumab Once-daily doses
17 μg/m2 (Day 0), 34 μg/m2 (Day 1), 68 μg/m2 (Day 2), 136 μg/m2 (Day 3), and 273 μg/m2 (Days 4–13)
Total cumulative avg. dose = ~5.6 mg
Protégé; Encore; Subcue b
Full 6-day regimen
Curtailed Herold regimen
6-day course of teplizumab Once-daily IV doses
51 μg/m2 (Day 0), 103 μg/m2 (Day 1), 207 μg/m2
(Day 2), 413 μg/m2 (Day 3), and 826 μg/m2 (Days 4–5)
Total cumulative avg. dose = ~4.6 mg
Protégé; Encore
Avg = average; IV = intravenous; SC = subcutaneous; T1DM = Type 1 Diabetes Mellitus. a Dosing was IV in these studies, unless otherwise noted. b Dosing was subcutaneous in the Subcue study. Further doses were planned for this study but only this
dose was given to the 1 subject enrolled. Note: Total average dose is the cumulative dose for a subject weighing 70kg with a body surface area (BSA)
of 1.92m2.
5.3.1.1 Completed Studies in T1DM
5.3.1.1.1 Study 1 (Dr. Kevan Herold, Sponsor-Investigator)
Details of this study are presented above in Section 5.2.1.
Confidential Page 49 of 130

Teplizumab MacroGenics, Inc.
Investigator's Brochure Version 12.0, 16 November 2016
5.3.1.1.2 Study 2 (Protocol ITN007AI [NDB01], Dr. Kevan Herold, Sponsor-Investigator)
Details of this study are presented above in Section 5.2.2.
5.3.1.1.3 Study 3 (Protocol ITN017AI, Dr. Kevan Herold, Sponsor-Investigator)
Details of this study are presented above in Section 5.2.3.
5.3.1.1.4 Subcue Protocol CP-MGA031-06 (the “SUBCUE” study, MacroGenics, Sponsor)
Objectives: The primary objectives of this study were to assess the safety and tolerability of subcutaneous (SC) dosing of teplizumab, assess the pharmacodynamic response (relative to placebo) of different SC dosing regimens of teplizumab, as measured by changes in CD4+ and CD8+ T lymphocyte counts, and to assess the pharmacokinetics of teplizumab after SC and IV administration.
Status: This study terminated enrollment subsequent to the DMC finding that the 1-year primary endpoint for study CP-MGA031-01 (Protégé) had not been met. One subject was treated in this study with the 1/3 14-day regimen SC.
Efficacy: Not analyzed as only one study subject was enrolled and dosed.
Safety: No SAEs were reported for the subject. The single subject in the study, a 22-year-old white female, had an AE of Epstein-Barr virus (EBV) infection on Day 28. The subject’s viral load was less than 390 copies/mL at screening (below the lower limit of quantitation) and 17300 copies/mL on Day 28. Adverse events that occurred at approximately the same time as the AE of EBV positive were lymphadenopathy (Days 19 through 28 and 35 through 38) and oropharyngeal pain (Days 44 through 56). The subject experienced an AE of herpes zoster (verbatim term “shingles”) on Day 59, approximately 6 weeks after receiving the last dose of study drug. As of the final study visit, the AEs of herpes zoster and EBV infection were ongoing. At subsequent follow-up contact, approximately 8 months after the subject initially developed herpes zoster, the subject reported “100% resolution” of the AEs of EBV and herpes zoster.
5.3.1.1.5 Protocol CP-MGA031-01 (the Protégé Study, MacroGenics, Sponsor)
Objective: This study was a Phase 2/3, multicenter study designed to compare the efficacy, safety, and tolerability of 3 dose levels of teplizumab relative to placebo in subjects, aged 8-35 years, with recent-onset (within 12 weeks of first visit to any physician for symptoms or signs) of T1DM.
Confidential Page 50 of 130

Teplizumab MacroGenics, Inc.
Investigator's Brochure Version 12.0, 16 November 2016
Design: The study was designed in 3 segments and, under a separate protocol (CP-MGA031-02), included a 3-year extension.
Segment 1 was open-label administration of teplizumab to 38 subjects with recent-onset T1DM. Enrollment in Segment 1 is complete with 11 adult subjects (aged 18 to 35 years), 16 adolescent subjects (aged 12 to 17 years), and 11 children (aged 8 to 11 years).
Segment 2 was double-blind, double-dummy administration of teplizumab or placebo randomly assigned to 1 of 4 study arms, with follow-up to 52 weeks after the first dose. As of 23 June 2009, enrollment was complete with 516 subjects (513 treated).
Segment 3 was a follow-up of all subjects in Segments 1 and 2 for an additional year (104 weeks total) to assess longer-term safety and durability of clinical benefit. Teplizumab was not administered during this segment. All follow-up is complete.
In Segment 1, subjects received two dosing cycles of 14 days each of the full 14-day regimen. In Segment 2, subjects were randomly assigned to receive two dosing cycles, of 14 days each, of either placebo, the full 6-day regimen, 1/3 14 day regimen, or full 14-day regimen (See Table 11 for dosing regimen details). In both segments, dosing cycles were separated by approximately 6 months.
Status: Study is completed and Clinical Study Report was submitted.
Efficacy: The efficacy results for the Protégé study are presented in Section 5.4.
Safety: The safety results for the Protégé study are presented in Section 5.5.
5.3.1.1.6 Protocol CP-MGA031-02 (the Protégé extension study, MacroGenics, Sponsor)
Objective: This study evaluated the durability of efficacy or response and the safety of teplizumab in subjects who participated in CP-MGA031-01. In addition, patient-reported outcomes (PRO), i.e., health-related quality-of-life data were collected. Analysis of efficacy and safety data was planned according to the treatment assignment groups into which the subjects were originally randomized in CP-MGA031-01. Teplizumab was not administered during this study.
Status: The study is completed. CSR dated 05 October 2012 was submitted to FDA on 05 December 2012 as Serial 168 to IND 100,262.
Efficacy: Due to the early termination of this study and the subsequent limited amount of efficacy data obtained, no efficacy conclusions could be drawn.
Safety: The safety results for the Protégé study are presented in Section 5.5.
Confidential Page 51 of 130

Teplizumab MacroGenics, Inc.
Investigator's Brochure Version 12.0, 16 November 2016
5.3.1.1.7 Protocol CP-MGA031-03 (the Protégé Encore study, MacroGenics, Sponsor)
Objectives: The primary objective of this study was to assess, relative to placebo, the efficacy of teplizumab when administered according to 3 different teplizumab dosing regimens in subjects with recent-onset T1DM (within 12 weeks of presentation of first signs and symptoms of disease to a physician). The secondary objectives were to assess the durability of clinical benefit and the safety and tolerability of teplizumab.
Design: The study was a randomized, double-blind, double-dummy, multinational, 4-arm, placebo-controlled, 2-year, dose-ranging study to evaluate the safety and efficacy of teplizumab in subjects aged 8–35 years with recent onset T1DM. A total of 254 subjects were randomized to 1 of 4 study arms (the planned number of subjects was 400):
Arm #1 – Full 14-day regimen (planned n=100)
Arm #2 – 1/3 14-day regimen (planned n=100)
Arm #3 – Full 6-day regimen (planned n=100)
Arm #4 – Placebo (planned n=100)
(See Table 11 for regimen details). Doses were planned to be given in two 14-day courses, separated by approximately 6 months. Not all subjects received both courses, as mentioned below.
As of 20 October 2010, Protégé Encore enrollment and dosing were suspended, based on the DMC findings for the Protégé study. Duration of subjects’ follow-up depended on whether subjects had received 1 or 2 courses of treatment, or portions thereof, before dosing was discontinued. Subjects who received some or all of 1 course of treatment were being followed up for 18 months after randomization; subjects who received some or all of a second course of treatment 6 months after their first course were followed for 24 months after randomization.
Status: The study is completed. CSR dated 10 December 2012 was submitted to FDA on 22 December 2012 as Serial 170 to IND 100,262.
Efficacy: As a result of the premature termination of this study, the planned enrollment of subjects was not completed. Thus, efficacy analyses were under powered, limiting any conclusions and interpretation of outcomes.
Safety: The safety results for the Protégé study are presented in Section 5.5.
Confidential Page 52 of 130

Teplizumab MacroGenics, Inc.
Investigator's Brochure Version 12.0, 16 November 2016
5.3.1.1.8 Study 4 (ITN027AI [the “AbATE” study])
This study was sponsored by the National Institute of Allergy and Infectious Disease (NIAID) and was supported and managed by the Immune Tolerance Network (ITN). Kevan Herold is the protocol chair.
Objective: The main objective of this study was to assess safety, therapeutic activity, and durability of the therapeutic activity of teplizumab.
Design: This was a Phase 2, 2-arm, randomized, open-label, multicenter study of teplizumab in subjects aged 8–30 years with recent-onset (< 8 weeks) T1DM. Subjects in the teplizumab group receive a 14-day course of teplizumab according to the full 14-day regimen (Table 11). The regimen is repeated at 12 months. The subjects were followed through Month 24.
Status: Study concluded in April 2011. The results of the study were published in an article titled “Teplizumab (anti-CD3 mAb) treatment preserves C-peptide responses in patients with new-onset type 1 diabetes in a randomized controlled trial: Metabolic and immunologic features at baseline identify a subgroup of responders” in Diabetes on 8 July 2013 (29). A CSR was submitted on 12 May 2014.
Efficacy: Compared to the untreated control subjects, teplizumab-treated patients had a reduced decline in C-peptide secretion at 2 years ((mean, 95%CI) -0.28 (-0.36, -0.20) nmol/L) vs. control: (-0.46(-0.57, -0.35) nmol/L; p=0.002).
Safety: The most common AEs were rash, transient upper respiratory infections, headaches, and nausea. Drug-related AEs were transient and resolved (29). From AbATE final study data, of the 21 EBV and 16 CMV seropositive individuals in the drug-treated group, 9 and 2, respectively, had a transient increase in the viral load at 1 month after the first course of treatment with anti-CD3 mAb, and 3 and 1 had an increase after the second course of drug. Five subjects with an increase in EBV viral load had possible symptoms of a transient EBV infection. In all subjects, the viral loads were undetectable at 2 months after treatment.
5.3.1.1.9 Study 5 (ISCT-MGA031-001 [the “Delay” study], Dr. Kevan Herold, Sponsor-Investigator)
Objective: The objective of this study was to assess safety and potential therapeutic activity in subjects with residual pancreatic islet cell function who are beyond the time frame defined as recent-onset.
Design: This was a Phase 2, randomized, double-blind, multi-center, placebo-controlled study of teplizumab in subjects with onset of T1DM from 4−12 months before study entry and who had residual pancreatic islet cell function. The study enrolled subjects aged 8–30 years. Subjects were randomized at a 1:1 ratio to receive either the full 14-day regimen of teplizumab or placebo (Table 11). At Month 12, all enrolled subjects had the option to receive an open-label course of teplizumab and to be followed for an additional 12 months.
Confidential Page 53 of 130

Teplizumab MacroGenics, Inc.
Investigator's Brochure Version 12.0, 16 November 2016
Status: The study is completed. Randomization and dosing are complete; follow-up of all subjects was completed in August 2012. A CSR has not been completed; however, the results of the study were published in an article titled “Teplizumab treatment may improve C-peptide responses in participants with type 1 diabetes after the new-onset period: a randomized controlled trial” in Diabetologia on 21 October 2012 (28).
Efficacy: Findings for the primary outcome of comparison of C-peptide responses to a mixed meal tolerance test after 1 year, did not conclusively demonstrate a significant benefit for teplizumab. Nevertheless, secondary outcomes suggest that treatment with teplizumab may modulate the course and reduce the decline of C-peptide in patients with established disease of up to 1-year duration.
Safety: The most common AEs were those typically observed in subjects receiving teplizumab: rash, lymphopoenia and nausea (all of which resolved). These events occurred in at least 40% of participants, and were observed more frequently in teplizumab-treated participants.
5.3.1.2 Current Ongoing Study with Teplizumab
5.3.1.2.1 Protocol ISCT-MGA031-005 (the “TN-10 At-Risk” study, TrialNet, Study Sponsor), Teplizumab for the Prevention or Delay of Onset of T1DM
Objective: To assess the safety, efficacy, and mode of action of teplizumab for prevention of T1DM in subjects at high risk of developing T1DM.
Design: The study is a 2-arm, Phase 2, multicenter, randomized, placebo-controlled, double-blind clinical study, open to enrollment of non-T1DM subjects (aged 8–45 years) who are relatives of T1DM patients and who are identified by the presence of autoantibodies and abnormal glucose tolerance. US FDA approved opening enrollment to children (8–16 years of age) in the TN-10 At-Risk Trial upon review of data from Protégé and data from other teplizumab studies. Subjects in the teplizumab arm will receive the full 14-day regimen. All subjects will receive close monitoring for development of T1DM.
Status: Open for enrollment; 64 subjects were enrolled and received blinded treatment as of 23 August 2016.
Efficacy: Not available.
Safety: In review of clinical adverse event data from the TN-10 At-Risk study, the safety profile of teplizumab remains unchanged. The adverse events most commonly seen in this trial as of 23 August 2016 are lymphopenia, headache, and rash, which have been observed in previous teplizumab trials.
Confidential Page 54 of 130

Teplizumab MacroGenics, Inc.
Investigator's Brochure Version 12.0, 16 November 2016
5.3.2 Psoriasis
Psoriasis is an inflammatory T cell-dependent autoimmune skin disease that is without a known cure and most commonly presents in late adolescence or early adulthood and persists for life. Psoriasis is manifested in its chronic plaque form as well-demarcated, scaly, erythematous plaques, with a predilection for the elbows, knees, and scalp.
5.3.2.1 Protocol CP-MGA031-04 (MacroGenics, Sponsor)
Objective: The main objective was to assess safety and tolerability (including immunogenicity) of ascending SC doses of teplizumab, in subjects with plaque psoriasis.
Design: This was a Phase 2a, multicenter (3 sites), open-label, multiple-dose study to evaluate safety, tolerability, PK, PD, and immunogenicity of teplizumab in adults with moderate or more severe psoriasis.
Status: This study was terminated after the first subject was enrolled and met the protocol-defined criteria for severe injection site reaction. The subject received 2 separate subcutaneous injections of 120 mg of teplizumab (51 mcg/m2) on Study Day 0 and Study Day 1, which was the extent of exposure. CSR completed as of 14 October 2011.
Efficacy: No notable improvements in LS-PGA, PASI, and PGA were documented at Study Day 84 in the single subject enrolled in the study.
Safety: The subject experienced worsening of injection-site reaction on the second day of subcutaneous dosing. The reaction was mainly erythematous and indurated without lymphangitic erythema, lymphadenopathy, blistering, ulceration, or necrosis. The event did not meet the criteria for an SAE, and completely resolved by Study Day 13.
5.4 Summary of Efficacy
5.4.1 Type 1 Diabetes Mellitus
Results on the effectiveness of teplizumab 2 years after commencing administration to subjects with T1DM are available from the Protégé study (CP-MGA031-01)(49).
5.4.1.1 Protégé Study Results
5.4.1.1.1 Data Monitoring Committee Findings at 1 Year of the Protégé Study
After all subjects completed dosing and follow-up through Day 364, the independent DMC performed a planned analysis of 1-year unblinded safety and efficacy data from the Protégé study. The DMC concluded that the primary efficacy endpoint of the study, a composite of a subject’s total daily insulin usage and HbA1c level at 12 months, was not met: 19.8%
Confidential Page 55 of 130

Teplizumab MacroGenics, Inc.
Investigator's Brochure Version 12.0, 16 November 2016
(41/207) in the full 14-day regimen group; 13.7% (14/102) in the 1/3 14-day regimen group; 20.8% (22/106) in the Full 6-day regimen group; and 20.4% (20/98) in the placebo group.
No unanticipated safety issues were identified in the DMC’s review. The DMC recommended continuation of appropriate safety monitoring as well as follow-up of clinical endpoints associated with standard-of-care for diabetes patients such as HbA1c, insulin dose, and other measures (e.g., fasting C-peptide levels). The protocol was subsequently amended to reduce the number of blood draws to decrease the burden on the study subjects and sites, while continuing with the collection of important data. It should be noted that stimulated C-peptide was no longer collected after the amendment. Subject follow-up continued through to the original end of the protocol (Day 728).
5.4.1.1.2 Disposition
A total of 38 subjects were enrolled into the open-label segment, and 516 were randomly assigned to double-blind treatment in the second segment of the study (the double-blind segment).
Five hundred thirteen of the 516 subjects randomly assigned to double-blind treatment in Segment 2 were administered study drug. Of these, 494 subjects (95.7%) completed 52 weeks of follow-up and 462 (89.5%) completed 104 weeks of follow-up, and 54 subjects discontinued from the study, i.e., did not return to the site for 2 full years of follow-up.
5.4.1.1.3 Primary Efficacy Results
In the double-blind segment, the proportion of subjects who had HbA1c < 6.5% and insulin < 0.5 U/kg/day at Weeks 52 and 104 (Day 364 and 728) is shown in Table 12. No difference was observed between any treatment group and placebo in the proportion of subjects who achieved the primary composite endpoint. In addition, no difference was observed between any treatment group and placebo in mean changes in HbA1c values at Week 52.
Table 12 Primary Endpoint: Proportion of Subjects with Composite Endpoint of HbA1c < 6.5% and Insulin < 0.5 U/kg/day (Protégé Study, ITT/Safety Population)
OL segment Double-blind segment
Study Day
Full 14-Day
Regimen
(n=38)
Placebo
(n=98)
Full 6-Day
Regimen
(n=106)
1/3 14-Day
Regimen
(n=102)
Full 14-
Day
Regimen
(n=207)
Day 364 29.0% 20.4% 20.8% 13.7% 19.8%
Day 728 13.2% 9.1% 9.4% 5.9% 8.2%
Confidential Page 56 of 130

Teplizumab MacroGenics, Inc.
Investigator's Brochure Version 12.0, 16 November 2016
5.4.1.1.4 C-peptide Analyses
5.4.1.1.4.1 Primary Analysis of C-peptide at Day 728
C-peptide is a marker for endogenous insulin production and surrogate for beta-cell function. C-peptide was analyzed using change from baseline log (AUC+1). Least square means based on mixed model repeated measurement (MMRM) analyses were determined and displayed in each plot. As a result, groups are equal at baseline in all graphs. The graphs that follow show only placebo and full 14-day regimen groups, since the other groups were not different from placebo.
Figure 6 shows the change in C-peptide over the course of the study for placebo and full 14-day regimen subjects. C-peptide mean change from baseline trended in favor of the full 14-day regimen compared to placebo at each timepoint and overall (Figure 6).
Figure 6 Mean Changes from Baseline in C-peptide AUC – Full 14-Day Regimen versus Placebo (Protégé Study, Double-Blind Segment, ITT Population)
5.4.1.1.5 C-peptide Subgroup Analyses
Further analyses of C-peptide were undertaken based on pre-defined subgroups by age (8–11, 12–17, 18–35), region (USA, India, other), and time from first visit to a physician for symptoms to randomization (≤ 6 weeks, > 6 weeks).
Full 14-Day RegimenPlacebo
Confidential Page 57 of 130

Teplizumab MacroGenics, Inc.
Investigator's Brochure Version 12.0, 16 November 2016
5.4.1.1.5.1 C-peptide AUC Change from baseline by Age Group
Mean changes from baseline in C-peptide log(AUC+1) over time for subjects aged 8 to 17, and 18 to 35 years in full 14-day versus placebo in the double-blind segment (ITT Population) are shown below. Children aged 8 to 17 years are shown in Figure 7. A pattern favoring teplizumab treatment was seen in the 8-17 age range (Figure 7) while not apparent in adults (Figure 8). The placebo group in adults was different from the placebo group in children with less reduction from baseline seen in adults compared to younger subjects.
Figure 7 Mean Change from Baseline for C-peptide in Adolescents (8-17 years old)-Protégé Study, Full 14-Day Regimen versus Placebo
108 100 91 69
# Subjects
p-value
Day 140 0.13
Day 364 0.02
Confidential Page 58 of 130

Teplizumab MacroGenics, Inc.
Investigator's Brochure Version 12.0, 16 November 2016
Figure 8 Mean Change from Baseline for C-peptide in Adults (18-35 years old)-Protégé Study, Full 14-Day Regimen versus Placebo
5.4.1.1.5.2 USA Subjects
Figure 9 shows the change in C-peptide log (AUC+1) for subjects randomized in the USA. Differences favoring the full 14-day regimen were observed at Day 728 and overall.
Placebo Full 14-day regimen
Confidential Page 59 of 130

Teplizumab MacroGenics, Inc.
Investigator's Brochure Version 12.0, 16 November 2016
Figure 9 Mean Change from Baseline for C-peptide in USA Subjects (all age groups)- Protégé Study, Full 14-Day Regimen versus Placebo
5.4.1.1.5.3 Subjects ≤ 6 Weeks from First Symptoms to Randomization
Subjects were categorized by time to entry into the study as ≤6 weeks or >6 weeks from identification of first symptoms of T1DM.
Figure 10 displays the C-peptide log (AUC+1) change from baseline over time. Differences favoring the full 14-day regimen group were observed at all time points.
Placebo Full 14-Day Regimen
Confidential Page 60 of 130

Teplizumab MacroGenics, Inc.
Investigator's Brochure Version 12.0, 16 November 2016
Figure 10 Change from Baseline for C-peptide in Subjects ≤6 Weeks from First Symptoms to Randomization- Protégé Study, Full 14-Day Regimen versus Placebo
5.4.2 Insulin Use
Protégé investigators independently adjusted insulin use during the study for individual subjects. There were no pre-specified regimens to increase or decrease insulin use; however, investigators were instructed to aggressively treat diabetes and attempt to keep HbA1c <6.5% and insulin >0.25 U/kg/day. Insulin use was captured at screening (baseline) and for three days prior to each study visit on a diary card at Days 91, 140, 273, 364, 448, 546, 616 and 728. The average units per kg per day were reported (U/kg/day). In all subjects, change in insulin use from baseline did not differ between the full 14-day group and placebo at Day 364 or 728 (Figure 11).
Full 14-Day Regimen
Placebo
Confidential Page 61 of 130

Teplizumab MacroGenics, Inc.
Investigator's Brochure Version 12.0, 16 November 2016
Figure 11 Mean Change in Average Daily Insulin Use – Protégé Study, Full 14-Day Regimen versus Placebo
It was noted that 19 subjects treated with teplizumab (11 in the full 14-day regimen and 4 in both the 1/3 14-day and full 6-day regimens) were off insulin at Day 364. Fourteen of these 19 subjects had HbA1c of less than 7% (one subject did not have a Day 364 sample). Five of the 19 remained off insulin at Day 728. No subjects receiving placebo were off insulin at Day 364 or 728.
On average, subjects off insulin at 1 year had an average baseline insulin use of 0.32 ± 0.29 U/kg/day. The average baseline use in the overall study population was 0.65 ± 0.40 U/kg/day. Consistent with lower exogenous insulin, C-peptide AUC at baseline was an average of 1.16 ± 0.80 nmol/L. The average baseline C-peptide for the entire study population was 0.67 ± 0.52 nmol/L. Together, these data suggest these subjects had more beta-cell function at baseline and that teplizumab treatment helped to maintain this function compared to placebo.
5.4.3 HbA1c Analysis
Mean changes from baseline are illustrated in Figure 12 for the full 14-day and placebo treatment groups. Mean changes in HbA1c from baseline were essentially identical in the full 14-day and placebo groups at all times. Mean HbA1c values decreased to a nadir at 90 days, with mean HbA1c values of 6.9% in both the full 14-day regimen and placebo groups. Values then slowly increased up to 7.9% and 7.8% in the full 14-day regimen and placebo groups, respectively, at Day 364 and 8.4% in both treatment groups at Day 728.
Confidential Page 62 of 130

Teplizumab MacroGenics, Inc.
Investigator's Brochure Version 12.0, 16 November 2016
Figure 12 Mean Changes from Baseline in HbA1c – Protégé Study, Full 14-Day Regimen vs. Placebo
5.5 Summary of Safety
5.5.1 Safety Results from Protégé, Protégé Extension, and Protégé Encore Studies
Unblinded placebo-controlled data are now available for 805 subjects from protocols CP-MGA031-01 (the Protégé study), CP-MGA031-02 (the Protégé Extension study), CP-MGA031-03 (the Protégé Encore study), including 308 subjects who have received the full 14-day dosing regimen (Protégé open label segment n=38, Protégé double blind segment n=207 and Protégé Encore n=63) (see Table 13). These randomized, placebo-controlled studies are the largest safety experience to date with teplizumab, are the basis for the current safety profile and evaluation of subject risk for teplizumab, and are presented in this IB. Of note, the Protégé Extension Study’s objective was to evaluate the long-term safety and efficacy of teplizumab in subjects with recent-onset of T1DM who completed the CP-MGA031-01 (Protégé) study; no dosing of subjects occurred in this study. There were additional small studies using intravenous administration of teplizumab for the treatment of T1DM; data from these studies was reviewed but is not presented here.
Confidential Page 63 of 130

Teplizumab MacroGenics, Inc.
Investigator's Brochure Version 12.0, 16 November 2016
Table 13 Number of Subjects in T1DM Intravenous Teplizumab Trials
Study Placebo Any Teplizumab All Treatments Number of Subjects
Enrolled
Protégé/Extension (includes open-label segment from Protégé)
98 453 551 554
Protégé Encore 62 192 254 254
Other IV Studies for T1DM 59 130 189 200
Total 219 775 994 1008
5.5.1.1 Summary of Key Safety Results from the Protégé, Protégé Extension and Protégé Encore Studies
No major difference was seen in overall AEs or SAEs between teplizumab and placebo subjects. No difference was seen in the rate of AEs including SAEs in children versus adults. The adverse effects were usually transient, Grade 1 or 2, with the exception of the teplizumab mechanism-based lymphopenia that usually resolves in 14-days and is observed in up to 80% of subjects. Other less common hematologic changes include transient, minimal neutropenia, thrombocytopenia, and eosinophilia not associated with clinical manifestations.
Liver function test abnormalities (primarily ALT, AST, and bilirubin elevations; not GGT), were also seen. These events were transient, usually Grade 1 or 2 with no difference seen in Grade 3 or higher events between teplizumab and placebo subjects. The liver test abnormalities likely represent cytokines in the liver, as the pattern of increase peaks around Day 5 or 6.
The most common clinical adverse experience is transient rash, usually maculopapular, sometimes pruritic, most commonly starting on Day 5 or 6 of dosing. Cytokine release syndrome, most commonly Grade 1 or 2, occurred in < 6% of teplizumab subjects. Symptoms may have included, but were not limited to, rash, headache, nausea, vomiting, and chills/rigors/pyrexia and usually occurred on Day 1 or Day 5 or 6 of dosing. Overall infections were not increased. In the Protégé study, there was a numeric increase in herpes zoster, but not other herpes virus infections in teplizumab-treated subjects. In contrast, the only herpes zoster case reported in Protégé Encore occurred in a subject in the placebo arm, and there were no cases in teplizumab-treated subjects.
5.5.1.2 Most Common Adverse Events in Protégé, Protégé Extension, and Protégé Encore Studies
The most common AEs (incidence of 10% or higher in any treatment group) occurring in subjects at any time during the Protégé, Protégé Extension, and Protégé Encore studies are presented by body system organ class (SOC presented alphabetically) and preferred term (by decreasing frequency) in Table 14. The frequency of AEs was higher in the teplizumab
Confidential Page 64 of 130

Teplizumab MacroGenics, Inc.
Investigator's Brochure Version 12.0, 16 November 2016
groups than in the placebo group, most notably in the SOCs of blood and lymphatic system disorders and skin and subcutaneous tissues disorders. The incidence of infections and infestations and metabolism and nutrition disorders was approximately ≥50%, but did not differ between teplizumab and placebo treatment groups.
Adverse events that began up to 28 days after the first dose in either treatment cycle were also reviewed. Generally, the incidence during the 28-day dosing period during and immediately after dosing was similar to the overall incidence of these events during the entire study period, as most of these AEs were reported during dosing (Table not shown).
Table 14 Most Frequent Adverse Events (>=10%) by Pooled Treatment Group Pooled Safety Population, Protégé, Protégé Extension and Protégé Encore (CP-MGA031-01, -02, and -03)
Treatment Group
System Organ Class
Preferred Term
Placebo a
N=160
n (%)
Full 6-Day and
1/3 14-Day
Dose a
N=337
n (%)
Full 14-Day
Dose
N=308 b
n (%)
Any
Teplizumab
N=645 c
n (%)
AT LEAST ONE ADVERSE EVENT 160 (100.0) 335 (99.4) 308 (100.0) 643 (99.7)
Blood and lymphatic system disorders 64 (40.0) 233 (69.1) 246 (79.9) 479 (74.3)
Lymphopenia 23 (14.4) 195 (57.9) 215 (69.8) 410 (63.6)
Leukopenia 31 (19.4) 122 (36.2) 137 (44.5) 259 (40.2)
Neutropenia 24 (15.0) 69 (20.5) 94 (30.5) 163 (25.3)
Gastrointestinal disorders 44 (27.5) 115 (34.1) 117 (38.0) 232 (36.0)
Nausea 19 (11.9) 46 (13.6) 56 (18.2) 102 (15.8)
Vomiting 9 (5.6) 33 (9.8) 41 (13.3) 74 (11.5)
General disorders and administration site conditions
54 (33.8) 132 (39.2) 131 (42.5) 263 (40.8)
Pyrexia 28 (17.5) 78 (23.1) 67 (21.8) 145 (22.5)
Infections and infestations 79 (49.4) 163 (48.4) 150 (48.7) 313 (48.5)
Upper respiratory tract infection 21 (13.1) 53 (15.7) 39 (12.7) 92 (14.3)
Nasopharyngitis 19 (11.9) 43 (12.8) 34 (11.0) 77 (11.9)
Investigations 146 ( 91.3) 327 ( 97.0) 292 ( 94.8) 619 ( 96.0)
Blood bicarbonate decreased 64 ( 40.0) 166 ( 49.3) 136 ( 44.2) 302 ( 46.8)
White blood cell count decreased 31 ( 19.4) 130 ( 38.6) 140 ( 45.5) 270 ( 41.9)
Aspartate aminotransferase increased 44 ( 27.5) 103 ( 30.6) 111 ( 36.0) 214 ( 33.2)
Haemoglobin decreased 49 ( 30.6) 105 ( 31.2) 103 ( 33.4) 208 ( 32.2)
Alanine aminotransferase increased 23 ( 14.4) 91 ( 27.0) 108 ( 35.1) 199 ( 30.9)
Lymphocyte count decreased 15 ( 9.4) 104 ( 30.9) 90 ( 29.2) 194 ( 30.1)
Confidential Page 65 of 130

Teplizumab MacroGenics, Inc.
Investigator's Brochure Version 12.0, 16 November 2016
Table 14 Most Frequent Adverse Events (>=10%) by Pooled Treatment Group Pooled Safety Population, Protégé, Protégé Extension and Protégé Encore (CP-MGA031-01, -02, and -03)
Treatment Group
System Organ Class
Preferred Term
Placebo a
N=160
n (%)
Full 6-Day and
1/3 14-Day
Dose a
N=337
n (%)
Full 14-Day
Dose
N=308 b
n (%)
Any
Teplizumab
N=645 c
n (%)
Neutrophil count decreased 25 ( 15.6) 81 ( 24.0) 74 ( 24.0) 155 ( 24.0)
Blood sodium decreased 33 ( 20.6) 70 ( 20.8) 57 ( 18.5) 127 ( 19.7)
Blood alkaline phosphatase increased 30 ( 18.8) 54 ( 16.0) 49 ( 15.9) 103 ( 16.0)
Platelet count decreased 15 ( 9.4) 51 ( 15.1) 57 ( 18.5) 108 ( 16.7)
Blood calcium decreased 20 ( 12.5) 49 ( 14.5) 47 ( 15.3) 96 ( 14.9)
Blood potassium increased 17 ( 10.6) 40 ( 11.9) 26 ( 8.4) 66 ( 10.2)
Metabolism and nutrition disorders 93 ( 58.1) 190 ( 56.4) 182 ( 59.1) 372 ( 57.7)
Hyponatraemia 47 ( 29.4) 89 ( 26.4) 80 ( 26.0) 169 ( 26.2)
Hypocalcaemia 34 ( 21.3) 62 ( 18.4) 69 ( 22.4) 131 ( 20.3)
Hyperkalaemia 16 ( 10.0) 43 ( 12.8) 33 ( 10.7) 76 ( 11.8)
Musculoskeletal and connective tissue disorders
13 ( 8.1) 43 ( 12.8) 45 ( 14.6) 88 ( 13.6)
Nervous system disorders 38 (23.8) 93 (27.6) 95 (30.8) 188 ( 29.1)
Headache 29 (18.1) 77 (22.8) 77 (25.0) 154 ( 23.9)
Renal and urinary disorders 15 (9.4) 51 (15.1) 40 (13.0) 91 ( 14.1)
Proteinuria 15 (9.4) 39 (11.6) 36 (11.7) 75 ( 11.6)
Respiratory, thoracic and mediastinal disorders
29 (18.1) 51 (15.1) 66 (21.4) 117 ( 18.1)
Skin and subcutaneous tissue disorders 37 (23.1) 176 (52.2) 181 (58.8) 357 (55.3)
Rash 12 (7.5) 89 (26.4) 91 (29.5) 180 (27.9)
Pruritus 8 (5.0) 40 (11.9) 45 (14.6) 85 (13.2)
a Includes subjects from studies CP-MGA031-01-DB, CP-MGA031-03 b Includes subjects from studies CP-MGA031-01-DB, CP-MGA031-01-Open-label (OL) segment, CP-MGA031-03 c Includes all subjects from studies indicated above who are known to have received an IV dose of Teplizumab. NOTES: Includes all events prior to 24Aug2012. Subjects in both studies CP-MGA031-01 and CP-MGA031-02 are only counted once in the denominators. Events from study hOKT3-002 (Hering) and studies with subcutaneous administration (CP-MGA031-04, CP-MGA031-06) are not included in this summary.
An additional analysis was done to identify AEs that satisfied one of the following 2 sets of criteria: p-value between placebo and teplizumab was less than 0.05 and the teplizumab incidence was ≥ 5% and ≥ 2 times that of placebo (criteria 1), or p-value between placebo
Confidential Page 66 of 130

Teplizumab MacroGenics, Inc.
Investigator's Brochure Version 12.0, 16 November 2016
and teplizumab was less than 0.05 and the teplizumab incidence was greater than that of placebo (criteria 2).
In the Protégé study, the AEs that were more common in the teplizumab full 14-day group compared to in the placebo group, based on comparison criteria, are shown in Table 15 and include: lymphopenia, leukopenia, white blood cell count decreased, neutropenia, alanine aminotransferase increased, rash, lymphocyte count decreased, pruritus, vomiting, chills, bilirubin conjugated increased and CRS. Nausea was numerically increased but did not meet comparison criteria (Table 15).
Table 15 Number (%) of Subjects Who Had AEs Satisfying Comparison Criteria (Double-Blind Segment, Protégé Study, Safety Population)
Preferred Term
Placebo
(N = 98)
Full 14-day
Regimen
(N = 207) p-Value a Comparison b
At least 1 AE 98 (100) 207 (100) -- --
Lymphopenia 17 (17.3) 152 (73.4) p<0.001 1, 2
Leukopenia 22 (22.4) 101 (48.8) p<0.001 1, 2
White blood cell count decreased 18 (18.4) 86 (41.5) p<0.001 1, 2
Neutropenia 19 (19.4) 72 (34.8) 0.007 2
Alanine aminotransferase increased 17 (17.3) 71 (34.3) 0.003 2
Rash 11 (11.2) 66 (31.9) p<0.001 1, 2
Lymphocyte count decreased 9 (9.2) 49 (23.7) 0.003 1, 2
Pruritus 4 (4.1) 32 (15.5) 0.004 1, 2
Vomiting 6 (6.1) 30 (14.5) 0.037 1, 2
Chills 2 (2.0) 20 (9.7) 0.017 1, 2
Bilirubin conjugated increased 2 (2.0) 17 (8.2) 0.042 1, 2
Cytokine release syndrome 0 (0.0) 12 (5.8) 0.011 1, 2
Note: Subjects who experienced the same event multiple times are only counted once. a p-values are obtained from Fisher exact test to determine statistical significance. b Events with the number 1 satisfied the following criteria: p < 0.05 and teplizumab incidence ≥ 5% and
≥ 2 times placebo. Events with the number 2 satisfied the following criteria: p < 0.05 and teplizumab incidence > placebo.
Similarly in Protégé Encore, the AEs that were more common in the teplizumab full 14-day group compared to in the placebo group, based on comparison criteria were (Table 16), white blood cell count decreased, lymphocyte count decreased, neutrophil count decreased, alanine aminotransferase increased, rash, bilirubin conjugated increased, and lymphopenia. In addition, platelet count decreased, blood potassium decreased, rash macular, rash maculopapular and Epstein-Barr Viremia were noted in Protégé Encore but not Protégé, based on comparison criteria. Events that were noted in Protégé but did not meet comparison
Confidential Page 67 of 130

Teplizumab MacroGenics, Inc.
Investigator's Brochure Version 12.0, 16 November 2016
criteria in Protégé Encore included leukopenia, neutropenia, pruritus, vomiting, chills, and CRS.
Table 16 Number (%) of Subjects Who Had AEs Satisfying Comparison Criteria (Double-Blind Segment, Encore Study, Safety Population)
SOC Preferred Term
Placebo
N=62 n (%)
Full 14-Day
Regimen
N= 63 n (%)
p-Value a Comparison b
White blood cell count decreased 13 ( 21.0) 39 ( 61.9) p<0.001 1, 2
Lymphocyte count decreased 6 ( 9.7) 35 ( 55.6) p<0.001 1, 2
Neutrophil count decreased 10 ( 16.1) 23 ( 36.5) .009 1, 2
Alanine aminotransferase increased 6 ( 9.7) 21 ( 33.3) .001 1, 2
Platelet count decreased 6 ( 9.7) 19 ( 30.2) .004 1, 2
Bilirubin conjugated increased 0 5 ( 7.9) .028 1, 2
Blood potassium decreased 0 5 ( 7.9) .028 1,2
Rash macular 2 ( 3.2) 9 ( 14.3) .030 1, 2
Rash 1 ( 1.6) 7 ( 11.1) .033 1, 2
Rash maculo-papular 0 6 ( 9.5) .013 1,2
Epstein-Barr viraemia 3 ( 4.8) 13 ( 20.6) .008 1, 2
Lymphopenia 6 ( 9.7) 27 ( 42.9) p<0.001 1, 2
Note: Subjects who experienced the same event multiple times are only counted once. a p-values are obtained from Fisher exact test to determine statistical significance. b Events with the number 1 satisfied the following criteria: p < 0.05 and teplizumab incidence ≥ 5% and
≥ 2 times placebo. Events with the number 2 satisfied the following criteria: p < 0.05 and teplizumab incidence > placebo.
5.5.1.3 Serious Adverse Events in Protégé, Protégé Extension and Protégé Encore Studies
All SAEs occurring in subjects during the Protégé, Protégé Extension, and Protégé Encore studies are presented by SOC and preferred term in Table 17.
The most common SAEs for subjects in all treatment groups were AEs related to diabetic control, such as, diabetic ketoacidosis, hyperglycemia, and diabetes mellitus inadequate control (consistent with the underlying disorder being studied) and AEs of infections. There was no increase in the overall incidence of SAEs of infections in subjects receiving teplizumab versus those seen in the placebo group. The remainder of events typically occurred in only 1 or 2 study subjects.
Deaths that occurred in the Protégé study are included in Section 5.5.3.4.
Confidential Page 68 of 130

Teplizumab MacroGenics, Inc.
Investigator's Brochure Version 12.0, 16 November 2016
Table 17 Number (%) Subjects Who Had Serious AEs, Pooled Safety Population, Protégé, Protégé Extension and Protégé Encore, (CP-MGA031-01, -02, -03)
System Organ Class
Preferred Term
Placebo/
No-Treatment
Control a
N=160
n (%)
Full 6-Day and
1/3 14-Day
Dose b
N=337
n (%)
Full 14-Day;
Dose c
N=308
n (%)
Any
Teplizumab d
N=645
n (%)
AT LEAST ONE ADVERSE EVENT 15 ( 9.4) 45 ( 13.4) 40 ( 13.0) 85 ( 13.2)
Blood and lymphatic system disorders 1 ( 0.6) 2 ( 0.6) 2 ( 0.6) 4 ( 0.6)
Neutropenia 1 ( 0.6) 1 ( 0.3) 1 ( 0.3) 2 ( 0.3)
Lymphopenia 0 1 ( 0.3) 1 ( 0.3) 2 ( 0.3)
Cardiac disorders 0 2 ( 0.6) 0 2 ( 0.3)
Acute myocardial infarction 0 1 ( 0.3) 0 1 ( 0.2)
Angina pectoris 0 1 ( 0.3) 0 1 ( 0.2)
Cardio-respiratory arrest 0 1 ( 0.3) 0 1 ( 0.2)
Coronary artery disease 0 1 ( 0.3) 0 1 ( 0.2)
Ventricular tachycardia 0 1 ( 0.3) 0 1 ( 0.2)
Ear and labyrinth disorders 0 1 ( 0.3) 0 1 ( 0.2)
Deafness neurosensory 0 1 ( 0.3) 0 1 ( 0.2)
Eye disorders 0 2 ( 0.6) 1 ( 0.3) 3 ( 0.5)
Cataract subcapsular 0 0 1 ( 0.3) 1 ( 0.2)
Corneal erosion 0 1 ( 0.3) 0 1 ( 0.2)
Iritis 0 1 ( 0.3) 0 1 ( 0.2)
Gastrointestinal disorders 0 7 ( 2.1) 3 ( 1.0) 10 ( 1.6)
Gastritis 0 3 ( 0.9) 1 ( 0.3) 4 ( 0.6)
Abdominal pain 0 0 1 ( 0.3) 1 ( 0.2)
Abdominal pain upper 0 0 1 ( 0.3) 1 ( 0.2)
Intestinal obstruction 0 1 ( 0.3) 0 1 ( 0.2)
Nausea 0 1 ( 0.3) 0 1 ( 0.2)
Peritonitis 0 1 ( 0.3) 0 1 ( 0.2)
Vomiting 0 1 ( 0.3) 0 1 ( 0.2)
General disorders and administration site conditions
2 ( 1.3) 1 ( 0.3) 3 ( 1.0) 4 ( 0.6)
Pyrexia 0 0 2 ( 0.6) 2 ( 0.3)
Death 0 0 1 ( 0.3) 1 ( 0.2)
Non-cardiac chest pain 2 ( 1.3) 0 0 0
Pain 0 1 ( 0.3) 0 1 ( 0.2)
Hepatobiliary disorders 0 1 ( 0.3) 2 ( 0.6) 3 ( 0.5)
Biliary dyskinesia 0 0 1 ( 0.3) 1 ( 0.2)
Biloma 0 0 1 ( 0.3) 1 ( 0.2)
Confidential Page 69 of 130

Teplizumab MacroGenics, Inc.
Investigator's Brochure Version 12.0, 16 November 2016
Table 17 Number (%) Subjects Who Had Serious AEs, Pooled Safety Population, Protégé, Protégé Extension and Protégé Encore, (CP-MGA031-01, -02, -03)
System Organ Class
Preferred Term
Placebo/
No-Treatment
Control a
N=160
n (%)
Full 6-Day and
1/3 14-Day
Dose b
N=337
n (%)
Full 14-Day;
Dose c
N=308
n (%)
Any
Teplizumab d
N=645
n (%)
Cholecystitis acute 0 0 1 ( 0.3) 1 ( 0.2)
Hepatosplenomegaly 0 1 ( 0.3) 0 1 ( 0.2)
Immune system disorders 0 1 ( 0.3) 3 ( 1.0) 4 ( 0.6)
Cytokine release syndrome 0 1 ( 0.3) 2 ( 0.6) 3 ( 0.5)
Hypersensitivity 0 0 1 ( 0.3) 1 ( 0.2)
Infections and infestations 4 ( 2.5) 13 ( 3.9) 10 ( 3.2) 23 ( 3.6)
Gastroenteritis 1 ( 0.6) 1 ( 0.3) 2 ( 0.6) 3 ( 0.5)
Gastroenteritis viral 0 1 ( 0.3) 1 ( 0.3) 2 ( 0.3)
Anal abscess 0 1 ( 0.3) 0 1 ( 0.2)
Appendicitis 0 0 1 ( 0.3) 1 ( 0.2)
Appendicitis perforated 0 1 ( 0.3) 0 1 ( 0.2)
Bronchitis 0 1 ( 0.3) 0 1 ( 0.2)
Dengue fever 0 0 1 ( 0.3) 1 ( 0.2)
Gastritis viral 0 1 ( 0.3) 0 1 ( 0.2)
Hepatic amoebiasis 0 1 ( 0.3) 0 1 ( 0.2)
Hepatitis A 0 0 1 ( 0.3) 1 ( 0.2)
Infection 0 1 ( 0.3) 0 1 ( 0.2)
Infectious mononucleosis 0 0 1 ( 0.3) 1 ( 0.2)
Pharyngotonsillitis 0 0 1 ( 0.3) 1 ( 0.2)
Pilonidal cyst 0 1 ( 0.3) 0 1 ( 0.2)
Pneumonia 0 1 ( 0.3) 0 1 ( 0.2)
Pulmonary tuberculosis 0 1 ( 0.3) 0 1 ( 0.2)
Pyelonephritis 0 0 1 ( 0.3) 1 ( 0.2)
Renal abscess 0 1 ( 0.3) 0 1 ( 0.2)
Sepsis 0 1 ( 0.3) 0 1 ( 0.2)
Staphylococcal sepsis 0 1 ( 0.3) 0 1 ( 0.2)
Urinary tract infection 0 0 1 ( 0.3) 1 ( 0.2)
Varicella 0 1 ( 0.3) 0 1 ( 0.2)
Cellulitis 1 ( 0.6) 0 0 0
Paronychia 1 ( 0.6) 0 0 0
Tuberculosis 1 ( 0.6) 0 0 0
Injury, poisoning and procedural complications
1 ( 0.6) 2 ( 0.6) 2 ( 0.6) 4 ( 0.6)
Confidential Page 70 of 130

Teplizumab MacroGenics, Inc.
Investigator's Brochure Version 12.0, 16 November 2016
Table 17 Number (%) Subjects Who Had Serious AEs, Pooled Safety Population, Protégé, Protégé Extension and Protégé Encore, (CP-MGA031-01, -02, -03)
System Organ Class
Preferred Term
Placebo/
No-Treatment
Control a
N=160
n (%)
Full 6-Day and
1/3 14-Day
Dose b
N=337
n (%)
Full 14-Day;
Dose c
N=308
n (%)
Any
Teplizumab d
N=645
n (%)
Caustic injury 0 0 1 ( 0.3) 1 ( 0.2)
Compression fracture 0 1 ( 0.3) 0 1 ( 0.2)
Fall 0 0 1 ( 0.3) 1 ( 0.2)
Fibula fracture 0 0 1 ( 0.3) 1 ( 0.2)
Foot fracture 0 0 1 ( 0.3) 1 ( 0.2)
Splenic rupture 0 0 1 ( 0.3) 1 ( 0.2)
Upper limb fracture 0 1 ( 0.3) 0 1 ( 0.2)
Facial bones fracture 1 ( 0.6) 0 0 0
Investigations 0 2 ( 0.6) 1 ( 0.3) 3 ( 0.5)
Alanine aminotransferase increased 0 1 ( 0.3) 1 ( 0.3) 2 ( 0.3)
Aspartate aminotransferase increased 0 1 ( 0.3) 1 ( 0.3) 2 ( 0.3)
Nuclear magnetic resonance imaging brain abnormal
0 1 ( 0.3) 0 1 ( 0.2)
Metabolism and nutrition disorders 4 ( 2.5) 21 ( 6.2) 19 ( 6.2) 40 ( 6.2)
Diabetic ketoacidosis 0 11 ( 3.3) 10 ( 3.2) 21 ( 3.3)
Hypoglycaemic seizure 0 6 ( 1.8) 1 ( 0.3) 7 ( 1.1)
Hyperglycaemia 3 ( 1.9) 2 ( 0.6) 3 ( 1.0) 5 ( 0.8)
Diabetes mellitus inadequate control 0 2 ( 0.6) 2 ( 0.6) 4 ( 0.6)
Hypoglycaemic unconsciousness 1 ( 0.6) 1 ( 0.3) 1 ( 0.3) 2 ( 0.3)
Hypoglycaemia 0 1 ( 0.3) 1 ( 0.3) 2 ( 0.3)
Dehydration 0 0 1 ( 0.3) 1 ( 0.2)
Ketoacidosis 0 1 ( 0.3) 0 1 ( 0.2)
Ketosis 1 ( 0.6) 0 0 0
Neoplasms benign, malignant and unspecified (incl cysts and polyps)
0 1 ( 0.3) 0 1 ( 0.2)
Metastatic malignant melanoma 0 1 ( 0.3) 0 1 ( 0.2)
Nervous system disorders 1 ( 0.6) 0 1 ( 0.3) 1 ( 0.2)
Hypoglycaemic coma 1 ( 0.6) 0 1 ( 0.3) 1 ( 0.2)
Pregnancy, puerperium and perinatal conditions
1 ( 0.6) 0 1 ( 0.3) 1 ( 0.2)
Abortion spontaneous 0 0 1 ( 0.3) 1 ( 0.2)
Complication of pregnancy 1 ( 0.6) 0 0 0
Psychiatric disorders 0 0 2 ( 0.6) 2 ( 0.3)
Mental disorder 0 0 1 ( 0.3) 1 ( 0.2)
Confidential Page 71 of 130

Teplizumab MacroGenics, Inc.
Investigator's Brochure Version 12.0, 16 November 2016
Table 17 Number (%) Subjects Who Had Serious AEs, Pooled Safety Population, Protégé, Protégé Extension and Protégé Encore, (CP-MGA031-01, -02, -03)
System Organ Class
Preferred Term
Placebo/
No-Treatment
Control a
N=160
n (%)
Full 6-Day and
1/3 14-Day
Dose b
N=337
n (%)
Full 14-Day;
Dose c
N=308
n (%)
Any
Teplizumab d
N=645
n (%)
Suicide attempt 0 0 1 ( 0.3) 1 ( 0.2)
Renal and urinary disorders 1 ( 0.6) 0 2 ( 0.6) 2 ( 0.3)
Intercapillary glomerulosclerosis 0 0 1 ( 0.3) 1 ( 0.2)
Ketonuria 0 0 1 ( 0.3) 1 ( 0.2)
Microalbuminuria 1 ( 0.6) 0 0 0
Reproductive system and breast disorders 0 1 ( 0.3) 0 1 ( 0.2)
Epididymitis 0 1 ( 0.3) 0 1 ( 0.2)
Skin and subcutaneous tissue disorders 0 0 2 ( 0.6) 2 ( 0.3)
Rash 0 0 2 ( 0.6) 2 ( 0.3)
Vascular disorders 0 0 1 ( 0.3) 1 ( 0.2)
Subclavian vein thrombosis 0 0 1 ( 0.3) 1 ( 0.2)
a Includes subjects from studies CP-MGA031-01-DB, CP-MGA031-02-DB, CP-MGA031-03 b Includes subjects from studies CP-MGA031-01-DB, CP-MGA031-02-DB, CP-MGA031-03 c Includes subjects from studies CP-MGA031-01-DB, CP-MGA031-01-OL, CP-MGA031-02-DB, CP-MGA031-
02-OL, CP-MGA031-03 d Includes all subjects from studies indicated above who are known to have received an IV dose of Teplizumab. NOTES: Includes all events prior to 24Aug2012. Subjects in both studies CP-MGA031-01 and CP-MGA031-02
are only counted once in the denominators. Includes all events prior to 24Aug2012. Subjects in both studies CP-MGA031-01 and CP-MGA031-02 are only counted once in the denominators.
5.5.1.4 Adverse Events of Special Interest
In addition to monitoring all AEs and SAEs reported, certain events listed below were pre-defined as adverse events of special interest (AESIs) in the protocol of the Protégé, Protégé Extension, and Protégé Encore studies. Investigative site personnel were to identify AESIs, including laboratory abnormalities, on the AESI electronic Case Report Form (e-CRF) page and complete questionnaire pages about the AESI.
In addition to these pre-defined, specific, AESIs, several patterns in the AE and laboratory data that were not pre-defined were combined for further exploration, including cytopenias and all liver function test changes. For ease of review, these summaries are discussed with the similar pre-specified AESIs. The following AESIs were captured in Protégé, Protégé Extension, and Protégé Encore, unless otherwise noted. Unlike the Protégé and Protégé Encore studies, the Protégé Extension study did not capture AESIs that were related to dosing
Confidential Page 72 of 130

Teplizumab MacroGenics, Inc.
Investigator's Brochure Version 12.0, 16 November 2016
with teplizumab because dosing did not occur in subjects in this trial and the focus was longer-term safety.
Rash (through Study Day 364) (Protégé Extension did not collect AESI of rash; Protégé Encore collected AESI of ≥ Grade 3 Rash through Study Day 364)
All infections (Protégé Extension focused on opportunistic infections, acute mononucleosis-like illness such as EBV and CMV and infections requiring IV antibiotic treatment)
Acute mononucleosis-like illness
≥ Grade 4 CRS (life-threatening requiring pressor or ventilatory support) (AESI not collected in Protégé Extension)
≥ Grade 3 liver function abnormalities (AST or ALT value > 5.0 x upper limit of normal (ULN) or a bilirubin value > 3.0 ULN) (AESI not collected in Protégé Extension)
≥ Grade 3 thrombocytopenia (platelet counts less than 50,000/mcL) (AESI not collected in Protégé Extension)
≥ Grade 3 neutropenia (<1000 PMN/mcL on 2 consecutive evaluations performed on different days) (AESI not collected in Protégé Extension)
Lymphocyte count < 500 mm3 for 7 days or longer (considered important medical event) (AESI not collected in Protégé Extension)
Clinically significant hypoglycemic episodes (required intervention by another individual through the administration of parenteral dextrose, glucagon or equivalent action)
Lymphomas or other malignancies (AESI not collected in Protégé Extension)
≥ Grade 4 allergic/hypersensitivity reaction (anaphylaxis) (AESI not collected in Protégé Extension)
Demyelinating diseases (AESI not collected in Protégé Extension or Protégé Encore)
Other medically important events related to complications of T1DM, such as diabetic ketoacidosis, non-ketotic hyperglycemic-hyperosmolar coma, retinopathy, nephropathy, neuropathy and atherosclerotic coronary heart disease (this AESI was only captured in Protégé Extension)
5.5.1.4.1 Adverse Events of Special Interest of Rash
In Protégé, all AEs of rash were reported as AESIs. Approximately 54% (222/415) of subjects in the all teplizumab group versus 20% (20/98) of subjects in the placebo group reported an AESI of rash. Nearly all rashes were described as mild or moderate (Grade 1 or 2). Approximately 60% (132/222) of subjects with AESIs of rashes in the all teplizumab
Confidential Page 73 of 130

Teplizumab MacroGenics, Inc.
Investigator's Brochure Version 12.0, 16 November 2016
group had a macular/maculopapular rash and approximately 25% (56/222) had a pruritic rash as categorized by the investigator.
Rash events were more common during cycle 1 than cycle 2 dosing. Out of the 187 subjects in the teplizumab treatment group who received both cycles of treatment, 72.2% had rash during cycle 1 only, 6.4% had rash during cycle 2 only, and 20.9% had rash during both cycles.
Figure 13 shows the onset of first occurrence of AESIs of rash during the study. Consistent with a drug-related rash, teplizumab subjects were much more likely to report a rash during dosing compared to placebo subjects. In cycle 1, most rashes began on the fifth or sixth day of dosing, when maximum dosing of the product started (Figure 14). In cycle 1, rash usually lasted 1 to 2 weeks in teplizumab subjects versus 2 to3 weeks in placebo subjects. The teplizumab subjects’ median duration of rash was only 4 to 6 days, reflecting a transient, drug-related rash, in comparison to the placebo subjects’ median duration of 13 days.
Figure 13 Rash Adverse Events Onset Study Day (Up to Day 728 – All Teplizumab vs. Placebo, Protégé Study, Double-Blind Segment, Safety Population)
45.1
2.2 3.11.7 0.7 0.7
11.2
4.1
0.02.0
0.03.1
0.0
5.0
10.0
15.0
20.0
25.0
30.0
35.0
40.0
45.0
50.0
0- 13 14- 28 29-181 182-195 196-224 225-728
Study Day
Perc
ent o
f Sub
ject
s
All TeplizumabPlacebo
Confidential Page 74 of 130

Teplizumab MacroGenics, Inc.
Investigator's Brochure Version 12.0, 16 November 2016
Figure 14 Rash Adverse Events Onset Study Day (Cycle 1 – Teplizumab Subjects, Protégé Study, Double Blind Segment)
0
2
4
6
8
10
12
14
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28
Study Day
Perc
ent o
f Sub
ject
s
The Protégé Encore study collected data for AESI of ≥ Grade 3 Rash through Study Day 364. There were no subjects who experienced Grade 3 or higher rashes in Protégé Encore. In Protégé Encore, the incidence of AEs in the SOC of skin and subcutaneous tissue disorder was 60.3% in the full 14-day dose group vs. 24.2 % in the placebo group. There were no SAEs of rash in the Protégé Encore study.
5.5.1.4.2 Adverse Events of Special Interest of Infections
In Protégé and Protégé Encore, any type or grade of infection was to be considered an AESI. In a few rare instances, investigators may have reported an infection as an AE, but not an AESI when they were not certain there was a “real” infection (e.g. subject had prodromal symptoms of infection, however, did not develop an infection). Overall infections were not increased in either Protégé or Protégé Encore. In Protégé, the incidence of AESIs of infection was 58% in the placebo group and 49% in the all teplizumab group. Over 95% were classified as Grade 1 or 2; 3% to 6% of subjects across all treatment groups had a serious infection. The overall incidence of serious infections in subjects receiving teplizumab was the same as in those receiving placebo (13/415 [3.1%] vs. 3/98 [3.1%], respectively). Similar to Protégé, the incidence of AESIs of infection in Protégé Encore was 34% in the placebo group and 32% in the all teplizumab group. Over 93% were classified as Grade 1 or 2; serious
Confidential Page 75 of 130

Teplizumab MacroGenics, Inc.
Investigator's Brochure Version 12.0, 16 November 2016
AESIs of infection occurred in (0.0%) in the placebo group vs. teplizumab-treated subjected (2.6%).
In both Protégé and Protégé Encore, the most common clinical-based infections reported were upper respiratory infection, sinusitis, nasopharyngitis, and urinary tract infection. In Protégé, 1 subject in the 1/3 14-day regimen group and 1 subject in the placebo group had tuberculosis. Both events met the criteria for serious events. In Protégé Encore, there was an increase in the laboratory-based AE of Epstein-Barr viremia in teplizumab-treated subjects (12.5%) vs. those subjects in the placebo group (4.8%). In the Protégé study, there was a numeric increase in herpes zoster, but not other herpes virus infections in teplizumab-treated subjects. In contrast, the only herpes zoster case reported in Protégé Encore occurred in a subject in the placebo arm, and there were no cases in teplizumab-treated subjects.
5.5.1.4.3 Adverse Events of Special Interest of Acute Mononucleosis-like Illness
In Protégé, the incidence of AESIs of acute mononucleosis-like illness was similar among the treatment groups, occurring in approximately 6% of teplizumab subjects versus 8.2% of placebo subjects. In Protégé Encore, 1.6% of placebo subjects versus 3.6% of teplizumab subjects has an AESI of acute mononucleosis-like illness.
5.5.1.4.4 Herpes-like Infection
Herpes and herpes-like infections were not predefined in the protocol as AESIs in Protégé or Protégé Encore. In review of Protégé and Protégé Encore data, some preferred terms that might be indicative of herpes infection appear in more than one SOC and may or may not have been reported under an AESI term, these preferred terms were combined and counted in Table 18 and Table 19.
In Protégé, the incidence of any type of herpes-like infection was not higher in teplizumab subjects than in placebo subjects; however, the incidence of cases of herpes zoster was numerically higher in the teplizumab groups than in the placebo group (Table 18). Herpes zoster occurred in 10 subjects in the teplizumab-treatment groups (double-blind segment) and no subjects in the placebo group.
There was one additional serious case (important medical event; not hospitalized; not drug related) of varicella reported in a 19-year-old female, participant 3072006, in the 1/3 14-day teplizumab regimen during the Protégé Extension study, approximately 17 months after the last dose of study drug (not included in the table, which shows only Protégé study data). Nine days after developing symptoms, the event was considered resolved.
Confidential Page 76 of 130

Teplizumab MacroGenics, Inc.
Investigator's Brochure Version 12.0, 16 November 2016
Table 18 Summary of Herpes-like Infection Terms by Treatment Groups (Double-Blind Segment, Protégé Study, Safety Population)
Treatment Group, n (%)
Subjects with:
Placebo
N=98
Full 6-Day
Regimen
N=106
1/3 14-Day
Regimen
N=102
Full 14-Day
Regimen
N=207
All
Teplizumab
N=415
Any Herpes-like Infection a 8 (8.2) 7 (6.6) 10 (9.8) 20 (9.7) 37 (8.9)
Epstein-Barr virus antibody positive 5 (5.1) 1 (0.9) 4 (3.9) 6 (2.9) 11 (2.7)
Herpes zoster 0 2 (1.9) 1 (1.0) 7 (3.4) 10 (2.4)
Cytomegalovirus antibody positive 1 (1.0) 2 (1.9) 1 (1.0) 1 (0.5) 4 (1.0)
Oral herpes 0 0 1 (1.0) 3 (1.4) 4 (1.0)
Herpes simplex 1 (1.0) 0 2 (2.0) 0 2 (0.5)
Infectious mononucleosis 1 (1.0) 1 (0.9) 0 1 (0.5) 2 (0.5)
Epstein-Barr virus infection 0 0 0 1 (0.5) 1 (0.2)
Herpes virus infection b 0 1 (0.9) 0 0 1 (0.2)
Mononucleosis syndrome 0 0 0 1 (0.5) 1 (0.2)
Varicella 0 0 1 (1.0) 0 1 (0.2)
a For 33 of the 42 subjects with herpes-like infection AEs, the AEs were reported as AESIs of rash, infection, or mononucleosis-like illness.
b Subject had multiple lesions from cat scratches describe as “herpetic-like” miscoded to herpes virus infection rather than cat scratch fever.
In Protégé Encore, similar to results from Protégé, the incidence of any type of herpes-like infection was not higher in teplizumab subjects than in placebo subjects (Table 19). In contrast to Protégé, the only event of herpes zoster (Grade 3; considered non-serious) reported in Protégé Encore occurred in a subject in the placebo arm, as there were no cases in teplizumab-treated subjects. Other herpes virus infection events were not serious. In Protégé Encore, sites were instructed to capture Epstein-Barr viremia when subjects had an increase in EBV polymerase chain reaction (PCR) values. Epstein-Barr viremia was seen in 24/192 (12.5%) of teplizumab-treated subjects compared to 3/62 (4.8%) of subjects receiving placebo. The increase appeared dose related occurring in 13/63 (20.6%) of subjects receiving the full 14-day dose regimen of teplizumab, (not shown).
Epstein-Barr virus seropositivity was documented by measurement of anti-EBV IgG for evidence of past EBV infection at screening and periodically throughout the Protégé and Protégé Encore studies using an immunoassay. Anti-EBV IgM was assessed for evidence of recent infection, using an immunoassay, which detects IgM class antibody. For subjects seropositive on either the EBV IgG or IgM test, viral load was assessed at designated study visits by semi-quantitative PCR.
Confidential Page 77 of 130

Teplizumab MacroGenics, Inc.
Investigator's Brochure Version 12.0, 16 November 2016
In Protégé, the double-blind study population had a high occurrence of anti-EBV IgG or IgM at baseline (80.5%). Approximately 6.7% of teplizumab and 9.2% of placebo subjects became positive for anti-EBV IgG or IgM during the study. No subjects in the double-blind segment had an increase in EBV viral load. One subject in the open-label group had a small, transient increase in EBV viral load.
There was a high occurrence of anti-EBV IgG or IgM at baseline (78.0%). A total of 217 subjects had high EBV IgG or IgM results during the study. Twenty-two of these subjects were negative at screening. There was no difference between treatment groups in the number of seroconversions during the study; approximately 7.8% of teplizumab and 11.3% of placebo subjects became positive for anti-EBV IgG or IgM during the study. Approximately 8.9% of teplizumab-treated subjects converted from a negative to positive EBV PCR viral load compared to 1.6% of subjects in the placebo group. The number of subjects per dosing regimen who converted to positive were: 8/62 (12.9%) subjects in the full 14-day regimen, 4/63 (6.3%) in the 1/3 14-day regimen, 5/66 (7.6%) in the full 6-day regimen and 1/62 (1.6%) in the placebo group.
Twenty teplizumab subjects had positive viral load on study (these included three subjects who did not have baseline values). Of these 20 subjects, 17 had a transient elevation in viral load on Study Day 28 which resolved by Day 90. One subject converted on Day 190 and 2 subjects on Day 546, including the 1 subject in the placebo arm; these subjects did not have repeat levels drawn. Viral load assay values and number of subjects, respectively, were: <5000 copies/ml in 12 subjects, 5000-10,000 copies/ml in 4 subjects, > 10,000 copies/ml in 4 subjects. There were no subjects with an assay of > 50,000 copies/ml. None of the subject had acute mononucleosis; one subject in the full 14-day regimen had a positive viral load of 39,000 copies/ml on Day 28 and had an AE of pharyngitis starting on Day 28 and resolving by Day 35. Subjects in future studies with elevated EBV DNA viral load should be monitored for asymptomatic infections and/or symptomatic EBV infections (20)
Table 19 Summary of Herpes-like Infection Terms by Treatment Groups (Double-Blind Segment, Protégé Encore Study, Safety Population)
Subjects with:
Placebo
N=62
Full 6-Day
Regimen
N=63
1/3 14-Day
Regimen
N=66
Full 14-Day
Regimen
N=63
All
Teplizumab
N=192
Any Herpes-like Infection a 7 (11.3) 5 (7.9) 12 (18.2) 7(11.1) 14 (12.5)
Epstein-Barr virus test positive 6 (9.7) 4 (6.3) 6 (9.1) 6 (9.5) 16 (8.3)
Cytomegalovirus test positive 0 0 3 (4.5) 0 3 (1.6)
Epstein-Barr virus antibody positive 0 1 (1.6) 1 (1.5) 1 (1.6) 3 (1.6)
Oral herpes 0 0 1 (1.5) 0 1 (0.5)
Varicella 0 0 1 (1.5) 0 1 (0.5)
Herpes zoster 1 (1.6) 0 0 0 0
Cytomegalovirus antibody positive 1 (1.6) 0 0 0 0
a Excludes the term of Epstein-Barr Viremia
Confidential Page 78 of 130

Teplizumab MacroGenics, Inc.
Investigator's Brochure Version 12.0, 16 November 2016
A list of all subjects with herpes zoster infections in the Protégé (open label and double-blind segments) and Protégé Encore studies is shown in Table 20. In Protégé Encore, the only subject with herpes zoster was on placebo; a 14-year-old male experienced a Grade 3 herpes zoster starting on Day 200. In Protégé, the subjects with AEs of herpes zoster range in age from 12 to 34 years and all received teplizumab. Two subjects had Grade 3 events; none of the AEs of herpes zoster were serious. Of these 11 subjects, 3 subjects had herpes zoster within 28 days of starting dosing for cycle 1. However, 6 of the events occurred after Day 270. Three subjects with herpes zoster had the drug permanently withdrawn (one Grade 3, one Grade 2, and one Grade 1 event).
Table 20 List of Subjects with Herpes Zoster (Protégé, Double-Blind and Open-Label Segments and Protégé Encore, Double Blind Segment)
Treatment Group
Subject ID Verbatim Term
Age a/Sex/Race
Start/
Stop Study Day Grade
Action
Taken Country
Protégé Full 14-day Regimen
0092002 Herpes zoster left chest and
shoulder
16/F/White 419/433 2 N/A United States
0122008 Herpes zoster 28/F/White 296/324 2 N/A United States 0362002 Herpes zoster 14/M/White 146/173 1 Dose not
changed United States
4541002 b Herpes Zoster Infection
14/M/Asian 938/947 2 N/A India
4602002 Bullous/vesicular eruptions herpes
zoster
24/F/Asian 12/22 2 Drug Withdrawn
India
4652003 Herpes zoster 12/F/Asian 107/117 3 Drug withdrawn
India
4652007 Herpes zoster 30/M/Asian 562/571 1 N/A India 4652022 Herpes zoster 34/F/Asian 306/372 3 N/A India Full 6-day Regimen
0092012 Herpes zoster left side of back
14/M/White 9/84 1 Drug Withdrawn
United States
3032001 Herpes zoster 14/M/White 329/338 2 N/A Ukraine 1/3 14-day Regimen
0422002 Shingles 13/F/White 18/56 2 N/A United StatesEncore
Placebo 465009 Herpes Zoster 14/M/Asian 200/230 3 Drug
Withdrawn India
a Denotes age of onset of AE. b Denotes subject treated in Open-Label Segment and followed in Protégé Extension Trial.
Confidential Page 79 of 130

Teplizumab MacroGenics, Inc.
Investigator's Brochure Version 12.0, 16 November 2016
Additionally, a subject in the SUBCUE study (CP-MGA031-06), a 22-year-old white female, (1/3 14-day regimen) had an AE of EBV infection on Day 28 and an AE of herpes zoster infection on Day 59. At subsequent follow-up contact, approximately 8 months after the subject initially developed herpes zoster, the subject reported “100% resolution” of the AEs of EBV and herpes zoster.
5.5.1.4.5 Cytokine-release Syndrome
In Protégé, 24/415 (~6%) of teplizumab subjects experienced 39 AEs of CRS, including, but not limited to, rash, headache, nausea, vomiting, and chills/rigors. Fever was not reported as a symptom. There were no events among placebo subjects. None were Grade 4 or higher (the pre-defined AESI) or met the criteria for SAE in the double-blind segment. Of note, one subject in the open-label segment experienced CRS that required hospitalization and that was characterized by rash (Section 5.5.1.4.1). Approximately 70% of CRS events have occurred within the first week of dosing (Figure 15). CRS appears to occur with the initial dose of teplizumab or on Day 4 or 5, when the dose is increased, and may be dose-related. CRS appears more frequently in cycle 1 than cycle 2.
Figure 15 All Cytokine Release Syndrome Events (Protégé, Double-Blind Segment, Teplizumab Safety Population)
0
0.5
1
1.5
2
2.5
0 1 2 3 4 5 6 7 11 13 177 179 180 184 185 186
Study Day
Perc
ent o
f Sub
ject
s
In Protégé Encore, 9/192 (4.7%) of teplizumab subjects experienced CRS, including, but not limited to, rash, headache, nausea, vomiting, and chills/rigors. Unlike Protégé, pyrexia was also noted as a symptom. The incidence of CRS events among Protégé Encore placebo
Confidential Page 80 of 130

Teplizumab MacroGenics, Inc.
Investigator's Brochure Version 12.0, 16 November 2016
subjects was 2/62 (3.2%). None were Grade 4 or higher (the pre-defined AESI); two were considered serious, subjects were treated and the events resolved. 5.5.1.4.6 Liver Function Test Abnormalities
In the Protégé study, transient AEs of ALT and bilirubin conjugated increased were higher in the all teplizumab group than in the placebo group; however, AEs of AST and GGT increased were not different between the teplizumab and placebo treatment groups. Grade 3 or higher liver function abnormalities (AST or ALT values ≥ 5.0x ULN or bilirubin values ≥ 3x ULN) were pre-specified as an AESI and occurred at a similar rate across the treatment groups at 1% to 3%. None of these events were serious AEs.
Table 21 provides a summary of LFT elevations for Protégé subjects by treatment group and toxicity grade for the double-blind segment. Most LFT elevations were Grade 1 or 2. Elevations of ALT and/or bilirubin occurred at a greater incidence in the teplizumab-treated versus placebo- treated subjects and were seen more frequently with higher total doses. Although Grade 1 AST elevations were consistent across all teplizumab and placebo groups (31% to 38%), Grade 2 elevations were more common in the full 14-day regimen group (9.7%) versus the placebo group (1.0%). Grade 1 GGT elevations were more common in the placebo group than the teplizumab-treated group, and Grade 2 elevations were equal in both groups. Of note, baseline LFTs showed approximately 16% (84/513) of subjects had Grade 1 LFT elevations prior to dosing. The percentage of subjects with Grade 1 elevations at baseline were: ALT (3% to 8.5%), AST (2% to 4.9%), bilirubin (6.1% to 8.5%) and GGT (0% to 2.4%) (not displayed).
Confidential Page 81 of 130

Teplizumab MacroGenics, Inc.
Investigator's Brochure Version 12.0, 16 November 2016
Table 21 Number and Percent of Subjects with Above-Normal Clinical Laboratory Test Results for ALT, AST, GGT and Bilirubin (Protégé Study, Double-Blind Segment, Safety Population)
Liver Parameter a
Grade 4
n (%)
Grade 3
n (%)
Grade 2
n (%)
Grade 1
n (%)
Treatment Group B’line Onstudy B’line Onstudy B’line Onstudy B’line Onstudy
Any Abnormality/Any Treatment 0/513 1/513 0/513 13/513 1/513 72/513 84/513 302/513
ALT >20.0 ULN >5.0 - 20.0 ULN >2.5 - 5.0 ULN >ULN - 2.5 ULN
Placebo [N=98] 0 0 0 1 (1.0) 0 1 (1.0) 3 (3.1) 19 (19.4)
Full 6-Day [N=106] 0 0 0 0 0 6 (5.7) 9 (8.5) 40 (37.7)
1/3 14-Day [N=102] 0 0 0 2 (2.0) 0 1 (1.0) 5 (4.9) 32 (31.4)
Full 14-Day [N=207] 0 1 (0.5) 0 4 (1.9) 0 22 (10.6) 17 (8.2) 83 (40.1)
AST >20.0 ULN >5.0 - 20.0 ULN >2.5 - 5.0 ULN >ULN - 2.5 ULN
Placebo [N=98] 0 0 0 1 (1.0) 0 1 (1.0) 2 (2.0) 37 (37.8)
Full 6-Day [N=106] 0 0 0 1 (0.9) 0 3 (2.8) 3 (2.8) 40 (37.7)
1/3 14-Day [N=102] 0 0 0 3 (2.9) 0 3 (2.9) 5 (4.9) 32 (31.4)
Full 14-Day [N=207] 0 0 0 1 (0.5) 0 20 (9.7) 7 (3.4) 73 (35.3)
GGT >20.0 ULN >5.0 - 20.0 ULN >2.5 - 5.0 ULN >ULN - 2.5 ULN
Placebo [N=98] 0 0 0 1 (1.0) 0 1 (1.0) 0 10 (10.2)
Full 6-Day [N=106] 0 0 0 0 0 0 2 (1.9) 9 (8.5)
1/3 14-Day [N=102] 0 0 0 0 0 1 (1.0) 2 (2.0) 9 (8.8)
Full 14-Day [N=207] 0 0 0 2 (1.0) 0 2 (1.0) 5 (2.4) 14 (6.8)
Total Bilirubin >10.0 ULN >3.0 - 10.0 ULN >1.5 - 3.0 ULN >ULN - 1.5 ULN
Placebo [N=98] 0 0 0 0 0 1 (1.0) 6 (6.1) 15 (15.3)
Full 6-Day [N=106] 0 0 0 1 (0.9) 0 6 (5.7) 9 (8.5) 20 (18.9)
1/3 14-Day [N=102] 0 0 0 0 0 6 (5.9) 7 (6.9) 20 (19.6)
Full 14-Day [N=207] 0 0 0 0 1 (0.5) 22 (10.6) 16 (7.7) 46 (22.2)
Each subject’s highest value for each parameter is included in the table. a n = number of subjects with high value. Percentage based on number of subjects in treatment group.
The Protégé Encore study, transient AEs of ALT and bilirubin conjugated increased were higher in the all teplizumab group than in the placebo group and in addition, the events of AST increased were seen more in the teplizumab group. GGT increases were not significantly different between the teplizumab and placebo treatment groups. No Grade 3 or higher liver function abnormalities (AST or ALT values ≥ 5.0x ULN or bilirubin values |≥ 3x ULN) elevations occurred in the placebo group, and AST and ALT elevations occurred at a similar rate across the treatment groups and a higher incidence was see in the full 14-day
Confidential Page 82 of 130

Teplizumab MacroGenics, Inc.
Investigator's Brochure Version 12.0, 16 November 2016
regimen group at 3.2% and 4.8%, respectively. Serious adverse events occurred in 2 (1%) subjects.
Table 22 provides a summary of LFT elevations for Protégé Encore subjects by treatment group and toxicity grade for the double-blind segment. Similar to Protégé, most LFT elevations in Protégé Encore were Grade 1 or 2. Grade 1 elevations of ALT occurred at a greater incidence in the teplizumab-treated subjects (22.7% to 30.2%) versus placebo- treated subjects (14.5%). Grade 1 AST elevations were highest in the 1/3 14-day dosing regimen (31.7%) and were similar in the other treatment groups (21.0 to 25.4%); Grade 2 elevations were more common in the full-14-day group (6.3%) versus the placebo group (1.6%). Grade 1 GGT elevations were more common the teplizumab-treated group (7.9% to 19.0%) than in the placebo group (3.2%), and only one grade 2 GGT elevation was seen in a subject in the full 14-day regimen. Grade 3 elevations of ALT and AST were only seen in teplizumab-treated subjects; none in the placebo group. Grade 3 elevation of bilirubin occurred in one subject in the 1/3 14-day regimen; no subject experienced a Grade 3 GGT elevation. There were no Grade 4 elevations of ALT, AST, bilirubin or GGT.
Confidential Page 83 of 130

Teplizumab MacroGenics, Inc.
Investigator's Brochure Version 12.0, 16 November 2016
Table 22 Number and Percent of Subjects with Above-Normal Clinical Laboratory Test Results for ALT, AST, GGT and Bilirubin (Protégé Encore Study, Double-Blind Segment, Safety Population)
Liver Parameter a
Grade 4
n (0)
Grade 3
n (7)
Grade 2
n (35)
Grade 1
n (123)
Treatment Group B’line Onstudy B’line Onstudy B’line Onstudy B’line Onstudy
Any Abnormality/Any Treatment 0/254 n = 0 a 0/254 n = 7 a 1/254 n = 35 a 28/254 n = 123 a
ALT >20.0 ULN >5.0 - 20.0 ULN >2.5 - 5.0 ULN >ULN - 2.5 ULN
Placebo [N=62] 0 0 0 0 0 2 (3.2) 2 (3.2) 9 (14.5)
Full 6-Day [N=63] 0 0 0 1 (1.6) 0 1 (1.6) 0 19 (30.2)
1/3 14-Day [N=66] 0 0 0 2 (3.0) 0 5 (7.6) 7 (10.6) 15 (22.7)
Full 14-Day [N=63] 0 0 0 3 (4.8) 0 2 (3.2) 2 (3.2) 17 (27.0)
AST >20.0 ULN >5.0 - 20.0 ULN >2.5 - 5.0 ULN >ULN - 2.5 ULN
Placebo [N=62] 0 0 0 0 0 1 (1.6) 0 13 (21.0)
Full 6-Day [N=63] 0 0 0 1 (1.6) 0 1 (1.6) 1 (1.6) 20 (31.7)
1/3 14-Day [N=66] 0 0 0 1 (1.5) 0 3 (4.5) 1 (1.5) 14 (21.2)
Full 14-Day [N=63] 0 0 0 2 (3.2) 0 4 (6.3) 3 (4.8) 16 (25.4)
Total Bilirubin >20.0 ULN >5.0 - 20.0 ULN >2.5 - 5.0 ULN >ULN - 2.5 ULN
Placebo[N=62] 0 0 0 0 0 2 (3.2) 1 (1.6) 6 (9.7)
Full 6-Day [N=63] 0 0 0 0 0 5 (7.9) 3 (4.8) 5 (7.9)
1/3 14-Day [N=66] 0 0 0 1 (1.5) 1 (1.5) 4 (6.1) 3 (4.5) 10 (15.2)
Full 14-Day [N=63] 0 0 0 0 0 6 (9.5) 3 (4.8) 4 (6.3)
GGT >10.0 ULN >3.0 - 10.0 ULN >1.5 - 3.0 ULN >ULN - 1.5 ULN
Placebo[N=62] 0 0 0 0 0 0 0 2 (3.2)
Full 6-Day [N=63] 0 0 0 0 0 0 1 (1.6) 12 (19.0)
1/3 14-Day [N=66] 0 0 0 0 0 0 2 (3.0) 6 (9.1)
Full 14-Day [N=63] 0 0 0 0 0 1 (1.6) 0 5 (7.9)
Each subject’s highest value for each parameter is included in the table. n = number of subjects with high value. Percentage based on number of subjects in treatment group. a Each column N represents number of subjects with Grade for any parameter Percentages are calculated by subjects in each treatment group
When evaluating the time course of mean ALT, AST, and bilirubin values of each treatment group in the double-blind segment in the Protégé study (see Figure 16 and Figure 17), a transient, mild increase is seen in mean ALT and bilirubin. This increase peaked during the first week of infusion, (ALT on Day 7 and bilirubin on Day 3), and generally resolved by Day 28. A similar pattern was observed in the Protégé Encore study.
Confidential Page 84 of 130

Teplizumab MacroGenics, Inc.
Investigator's Brochure Version 12.0, 16 November 2016
Figure 16 Mean ALT and AST Values Through Study Day 91 (Protégé Study, Safety Population)
Alanine Aminotransferase (U/L)
Visit/Study Day
Ala
nine
Am
inot
rans
fera
se (U
/L)
0 6 14 28 91
2025
3035
40
1/3 14-Day RegimenFull 14-Day RegimenFull 6-Day RegimenPlacebo
Aspartate Aminotransferase (U/L)
Visit/Study Day
Asp
arta
te A
min
otra
nsfe
rase
(U/L
)
0 6 14 28 91
2022
2426
2830
3234
1/3 14-Day RegimenFull 14-Day RegimenFull 6-Day RegimenPlacebo
MacroGenics, Inc.Protocol CP-MGA031-01
Confidential
Confidential Page 85 of 130

Teplizumab MacroGenics, Inc.
Investigator's Brochure Version 12.0, 16 November 2016
Figure 17 Mean Bilirubin Values Through Study Day 91 (Protégé Study, Safety Population)
In Protégé, there were 3 serious hepatobiliary events that occurred in 2 subjects in the full 14-day group: biliary dyskinesia and biloma (both occurring in 1 subject) and acute cholecystitis, all assessed as not causally-related to teplizumab. The first subject, a 35-year-old male, experienced biliary dyskinesia, approximately 11 months after receiving the last dose of teplizumab. One month later, the subject underwent a laparoscopic cholecystectomy; biopsy results were benign and confirmed the diagnosis of biliary dyskinesia. The cholecystectomy was complicated by a biloma, which was treated by drainage and resolved. The second subject, a 16-year-old male, experienced abdominal pain and nausea and was hospitalized 8 months after the last dose of study drug. The subject continued to have abdominal pain for the next 3 months, a surgical consult was obtained, and the subject had a laparoscopic cholecystectomy with intraoperative cholangiogram for acalculous cholecystitis, 10 months after the last dose of study drug. The pathology report revealed chronic cholecystitis. The subject was discharged from the hospital the following day, and the event resolved.
In Protégé Encore, there were 2 SAEs of liver enzyme elevations, both occurred during dosing, were transient, resolved and were assessed as causally-related to teplizumab. Both subjects were discontinued from further study drug administration per the defined protocol stopping rules. The first subject a 21-year-old Asian male, randomized to the 1/3 dose 14-day teplizumab regimen, experienced transient elevated ALT and AST which required hospitalization. The subject received 13 of the 14 protocol stipulated study drug infusions. The subject had normal baseline ALT and AST laboratory values. Prior to receiving the 14th study drug infusion, laboratory tests revealed increased levels of AST 166 U/L (Normal range [NR]: 15-37) and ALT 259 U/L (NR: 30-65), total bilirubin of 0.36 mg/dL, alkaline phosphatase of 143 U/L and gamma glutamyl transferase of 27 U/L. The subject was
Bilirubin (MG/DL)
Visit/Study Day
Bili
rubi
n (M
G/D
L)
0 6 14 28 91
0.5
0.6
0.7
0.8 1/3 14-Day Regimen
Full 14-Day RegimenFull 6-Day RegimenPlacebo
Confidential Page 86 of 130

Teplizumab MacroGenics, Inc.
Investigator's Brochure Version 12.0, 16 November 2016
asymptomatic and stable. No treatment was provided. No liver pathology tests were performed. On Study Day 19 the subject was discharged with the following laboratory tests results: AST 201 U/L, ALT 443 U/L, alkaline phosphatase 174 U/L, lactate dehydrogenase 198 U/L, direct bilirubin 0.04 mg/dL and total bilirubin 0.35 mg/dL. Liver function test normalized and the events resolved. Concomitant medications which may have been a contributory factor in the liver enzyme elevations included Combiflam 700 (paracetamol/ibuprofen), Augmentin (amoxicillin/clavulanic acid) and Calpol (paracetamol).
The second SAE of elevated AST and ALT requiring hospitalization occurred in a 10-year old white male who was randomized to the full 14-day teplizumab regimen. The subject received 5 of the 14 protocol-stipulated study drug infusions from for dosing cycle 1. The subject's baseline AST and ALT levels were normal. On Study Day 6, the subject's pre-dosing laboratory tests results showed elevated AST of 120 IU/L (2.7x ULN (Ref: 0-45)) and ALT of 163 IU/L (4.1x ULN (Ref: 0-40)). Follow-up laboratory tests results began to show a downward trend of the subject's AST and ALT levels which were reported as 136 IU/L and 386 IU/L on Study Day 10. Downward trend of laboratory values continued and follow-up laboratory results collected on Study Day 20 revealed an ALT of 45 IU/L; the event was considered resolved. Concomitant medications which may have been a contributory factor in the liver enzyme elevations included cetirizine hydrochloride and ibuprofen, and although uncommon, is a documented effect of these medications.
5.5.1.4.7 Cytopenias
Consistent with the mechanism of action of teplizumab, lymphocytes were expected to decrease in subjects receiving teplizumab. In fact, over 80% of teplizumab-treated subjects had decreased lymphocytes, but none met the AESI criteria of lymphocyte count <500 mm3 for 7 days. Leukocyte counts were at the nadir on Day 4 to 6. Lymphocytes decrease on Day 1 with the maximum lymphopenia typically observed at Study Day 5 and then resolve, despite continued dosing. In most individuals, circulating lymphocytes return to approximately 80% of baseline values 2 weeks after the last dose of drug and to 100% of baseline values by Day 28. This transient decrease is consistent with marginalization of the lymphocytes.
The risk and management of cytopenias in teplizumab-treated subjects is discussed in Section 5.5.3.1.
5.5.1.4.8 Adverse Events of Special Interest of Clinically-significant Hypoglycemia
In Protégé, consistent with the underlying diabetes, AESIs of major hypoglycemic events were reported in 2% to 3% of subjects across all treatment groups; none were fatal.
In the Protégé Encore study, 5.7% of teplizumab-treated subjects had AESIs of major hypoglycemic events versus 1.6% in the placebo group. Serious events occurred in 2.6% of
Confidential Page 87 of 130

Teplizumab MacroGenics, Inc.
Investigator's Brochure Version 12.0, 16 November 2016
the teplizumab-treated subjects and none occurred in the placebo group. None of the serious events were fatal.
5.5.1.4.9 Adverse Events of Special Interest of Lymphoma or Other Malignancies
There were no cases of lymphoma reported in Protégé or Protégé Encore. In Protégé, only one malignancy was reported across the open-label and double-blind study populations. The subject had metastatic malignant melanoma in a pre-existing lesion that was not diagnosed until during the study. Importantly, the subject had a history of dysplastic nevi. The subject underwent excision of the lesion and was in full-remission 2 years post-excision and there has been no recurrence of metastatic malignant melanoma. No subjects in the Protégé Encore study had a malignancy. All malignancies across all teplizumab studies are discussed in Section 5.5.3.2.
5.5.1.4.10 Other Adverse Events of Special Interest Conditions
There were no reports of demyelinating disease or anaphylaxis in the double-blind or open-label segments of the Protégé study. Adverse events of demyelinating disease were not captured as AESIs in the Protégé Encore study.
5.5.2 Safety Summary in ISCT-MGA031-005 (“TN-10 At-Risk”) Trial
5.5.2.1 Overall Summary From the TN-10 At-Risk Trial
The safety profile from the ongoing TN-10 At-Risk study is consistent with the known safety profile for teplizumab noted above from the completed Protege, Protégé Extension and Protégé Encore studies. There have been no deaths and no pregnancies reported for subjects in the At-Risk trial as of 23 August 2016. There are no new safety concerns identified and no changes to the proposed benefit-risk profile of teplizumab based on available data as of 23 August 2016.
Cumulatively, there have been 5 subjects who have discontinued from the At-Risk trial:
Per the protocol definition for discontinuation of infusions, subjects with a total bilirubin of ≥ 2.0 mg/dL will be discontinued from the study. Two subjects discontinued from the blinded At-Risk study due to an increase in total bilirubin:
o One subject had a total bilirubin value of 2.1mg/dL (normal reference range 0.0-1.3 mg/dL) on Study Day 8 and met the protocol requirement of discontinuation of study drug. The subject had mild Grade 1 ALT elevation (50 U/L; normal reference range 0-47 U/L) (considered not clinically significant by the investigator), normal AST, and did not have any adverse events or other laboratory abnormalities.
Confidential Page 88 of 130

Teplizumab MacroGenics, Inc.
Investigator's Brochure Version 12.0, 16 November 2016
o On Study Day 11, one subject had a pre-infusion total bilirubin value of 2.1 mg/dL (normal reference range 0.0-1.0 mg/dL). Direct bilirubin was slightly elevated at 0.3 mg/dL (normal reference range 0.0-0.2 mg/dL). AST and ALT were within normal limits. On Study Day 12, the total bilirubin and direct bilirubin were unchanged, the AST and ALT remained within normal limits.
One patient chose to discontinue treatment in the At-risk trial (not due to adverse event).
One patient from the At-Risk trial was lost to follow-up.
One patient discontinued treatment in the At-risk trial after a non-serious Grade 2 event of increased alanine aminotransferase (ALT), which was assessed by the investigator as probably related to study drug (teplizumab/placebo). Subsequent to this discontinuation, this subject remained an active participant in the At-Risk trial to allow continued assessment of response to study drug and determination of other study endpoints.
5.5.2.2 Serious Adverse Events in the TN-10 At-Risk Trial
Cumulatively, there have been 5 SAEs occurring in 5 subjects in the TN-10 At-Risk Trial as of 23 August 2016 (Table 23).
Table 23 Serious Adverse Events in the TN-10 At-Risk Trial
MG Case ID Reporter’s
Verbatim Term
Preferred Term AE Start
Date
AE End
Date
Outcome
2013000005 Chest wall pain Musculoskeletal chest pain
03-Jul-2013
04-Jul-2013 Recovered
2013000008 Possible serum sickness
Serum sickness 13-Sep-2013
06-Dec-2013
Recovered
2013000014 Uretero-pelvic junction obstruction
Pelvic-ureteric obstruction
28-Oct-2013
08-Nov-2013
Recovered
2014000002 Gastroenteritis Gastroenteritis 21-Dec-2013
08-Jan-2014
Recovered
2016000025 Lung (Pneumonia) Pneumonia 03-Jun-2016
24-Jun-2016
Recovered
Three of the 5 SAEs were assessed as not related to blinded study medication, and 2 SAEs were assessed as possibly related to blinded study medication and are summarized below.
An SAE of immune complex disorder (possible serum sickness), occurred in a 12-year-old male subject and resulted in hospitalization. Relevant medical history included lactose intolerance and eczema. The subject received 14 of 14 scheduled blinded study medication infusions. During the course of blinded study drug administration, the subject experienced
Confidential Page 89 of 130

Teplizumab MacroGenics, Inc.
Investigator's Brochure Version 12.0, 16 November 2016
fever, vomiting (one episode), and rash. Approximately 5 days after the last dose of the blinded study drug, the subject developed arthralgias of the shoulders, hips, wrists, and knees. The arthralgias persisted and began to worsen.
The child’s initial presentation of transient myalgia and arthralgias and positive laboratory tests were compatible with an immune complex disorder. The investigator noted the event was possibly related to blinded study medication and the cause of the arthralgias was most likely serum sickness based on the arthralgias, elevated CRP and ESR, and reduced level of C4 complement. However, both the investigator and sponsor indicated that the low positive (1:80) ANA titer prior to study drug exposure suggests a possible underlying immune process which may have contributed to the clinical outcome. The event is considered recovered as of 06 December 2013.
During the study, an SAE of pneumonia was reported, occurring in a 15-year-old male. This unexpected event was assessed to be possibly related to study drug (teplizumab/placebo) by the investigator and sponsor. Forty-seven days after his last dose of teplizumab/placebo, this subject was found to have developed bilateral pulmonary infiltrates and right-sided pleural effusion after presenting to the hospital with fever, chest pain, and cyanosis. After a 10-day hospitalization, the subject was discharged home on oral antibiotics with the event considered recovered.
5.5.3 Overall Evaluation of the Risks
The current safety profile of teplizumab includes the following 5 types of AEs, which are discussed in this section. Also discussed in this section are malignancies, pregnancies, and deaths observed across all teplizumab studies.
1. Hematologic (lymphopenia, leukopenia, neutropenia, thrombocytopenia, eosinophilia)
2. Rashes
3. Liver function test elevations (primarily ALT and bilirubin)
4. Cytokine release syndrome (may include, but not be limited to, rash, headache, nausea, vomiting, and chills/rigors)
5. Possible herpes zoster infection
The assessment of risk in this section will focus on the full 14-day regimen, as this is the only dose with potential effect (as defined by a treatment effect on C-peptide and insulin use as well as measures of glycemic control) (see Section 5.4.2).
5.5.3.1 Hematologic Events
Hematologic events observed with teplizumab treatment include lymphopenia, leukopenia, neutropenia, thrombocytopenia, and eosinophilia.
Confidential Page 90 of 130

Teplizumab MacroGenics, Inc.
Investigator's Brochure Version 12.0, 16 November 2016
5.5.3.1.1 Leukopenia and Lymphopenia
Consistent with its mechanism of action, teplizumab causes transient leukopenia, greatly manifested by lymphopenia, and the patterns of decrease and duration are similar for these two cytopenias (see Figure 18 and Figure 19). In Protégé and Protégé Encore, lymphopenia or decreased lymphocyte levels occurred in approximately 86% and 92.1% of 14-day full regimen subjects, respectively. Grade 3 (< 500 lymphocytes/mcL) and occasional Grade 4 (< 200 lymphocytes/mcL) lymphopenia should be expected. Grade 3 or higher lymphopenia occurred in > 40% of subjects receiving teplizumab (177/415 [42.7%]) vs. placebo (4/98 [4.1%]) in Protégé. As shown in Figure 19, the pattern observed in Protégé showed lymphocytes decrease on Day 1, with the maximum lymphopenia typically observed at Day 6, and then resolve, despite continued dosing. In most individuals, circulating lymphocytes return to approximately 80% of baseline values 2 weeks after the last dose of drug and to 100% of baseline values by Day 28. This transient decrease is consistent with marginalization of the lymphocytes. A similar pattern was observed in Protégé Encore.
Figure 18 Mean (± SD) Leukocyte Values Up to and Including Day 28 (Protégé Study, Safety Population)
Leukocytes (10^9/L)
Visit/Study Day
Leuk
ocyt
es (1
0^9/
L)
0 3 6 9 14 28
4.5
5.0
5.5
6.0
6.5
7.0
7.5
1/3 14-Day RegimenFull 14-Day RegimenFull 6-Day RegimenPlacebo
Confidential Page 91 of 130

Teplizumab MacroGenics, Inc.
Investigator's Brochure Version 12.0, 16 November 2016
Figure 19 Mean (± SD) Lymphocyte Values Up to and Including Day 28 (Protégé Study, Safety Population)
5.5.3.1.2 Neutropenia
In Protégé and Protégé Encore, neutropenia associated with teplizumab occurred in approximately 45% of full-14-day teplizumab subjects compared to 24-30% of placebo subjects. Neutropenia is more variable and has been generally mild to moderate in contrast to the lymphopenia. Grade 3 or higher neutropenia occurred in similar numbers in the 14-day full regimen teplizumab and placebo groups in both Protégé and Encore. As shown in Figure 20, neutrophils decrease on Day 1 with a biphasic nadir on Day 3 and Day 7 and then resolve by Day 14, despite continued dosing.
The development of transient lymphopenia and/or neutropenia does not appear to be associated with an overall increased risk of infection in subjects receiving teplizumab. During this 28-day period, infections occurred at similar frequencies in the teplizumab (74/415 [17.8%]) and placebo (18/98 [18.4%]) groups in Protégé. In Protégé Encore, there was a slight increase in the frequency of infections of teplizumab subjects versus placebo, (14/63 [22.2%]) and 6/62 [9.7%], respectively. However, the laboratory-based event of Epstein-Barr viremia was the most common infections reported during the 28-day period.
Lymphocytes (10^9/L)
Visit/Study Day
Lym
phoc
ytes
(10^
9/L)
0 3 6 9 14 28
1.0
1.5
2.0
2.5
1/3 14-Day RegimenFull 14-Day RegimenFull 6-Day RegimenPlacebo
Confidential Page 92 of 130

Teplizumab MacroGenics, Inc.
Investigator's Brochure Version 12.0, 16 November 2016
Figure 20 Mean (± SD) Neutrophil Values Up to and Including Day 28 (Protégé Study, Safety Population)
5.5.3.1.3 Thrombocytopenia
Thrombocytopenia parallels the other cytopenias discussed above (see Figure 21). It occurred at a similar incidence in the teplizumab and placebo groups (teplizumab group 24% and placebo group18%) and was mainly mild or moderate (below Grade 3). It generally resolved within 1 week.
Neutrophils (10^9/L)
Visit/Study Day
Neu
troph
ils (1
0^9/
L)
0 3 6 9 14 28
3.0
3.5
4.0
4.5
1/3 14-Day RegimenFull 14-Day RegimenFull 6-Day RegimenPlacebo
Confidential Page 93 of 130

Teplizumab MacroGenics, Inc.
Investigator's Brochure Version 12.0, 16 November 2016
Figure 21 Mean (± SD) Platelet Levels Up to and Including Day 28 (Protégé Study, Safety Population)
5.5.3.1.4 Eosinophils
In Protégé, eosinophilia is more variable and transient, occurs during the first week of dosing, peaks at day 7, and normalizes by day 28 (Figure 22). The incidence of eosinophilia occurs more frequently in the teplizumab-treated subjects (4.1%) vs. the placebo treated subjects (0%). It appears to be dose-related and is statistically significantly higher in the full 14-day treatment group (5.8%) than in the placebo group (0%). A greater increase in eosinophils is seen in the full 14-day treatment group compared to the other teplizumab groups.
In Protégé Encore, the incidence of eosinophilia continues to occur more frequently in the teplizumab-treated subjects (6.3%) vs. the placebo treated subjects (1.6%), however, is seen equally in the full 14-day treatment group (6.3%) and the other teplizumab dose regimens (6.2%). The pattern of mean eosinophil values in Protégé Encore is similar to that observed in Protégé.
Platelet (10^9/L)
Visit/Study Day
Plat
elet
(10^
9/L)
0 3 6 9 14 28
220
260
300
340
1/3 14-Day RegimenFull 14-Day RegimenFull 6-Day RegimenPlacebo
Confidential Page 94 of 130

Teplizumab MacroGenics, Inc.
Investigator's Brochure Version 12.0, 16 November 2016
Figure 22 Mean (± SD) Eosinophil Values Up to and Including Day 28 in the Protégé Study
5.5.3.2 Malignancy-Carcinogenesis
Long-term studies have not been conducted to evaluate the carcinogenic potential of teplizumab. Treatment with T-cell suppressive therapies may secondarily increase cancer risk or tumor progression, especially if significant and persistent immunosuppression occurs. It is unknown if treatment with teplizumab, which causes only transient decreases in lymphocytes, could lead to an increased incidence of lymphoid neoplasms. There were no cases of lymphoma reported. There have been two reports of carcinomas across all studies with teplizumab; these carcinomas were assessed as not related to treatment with teplizumab.
The first case of melanoma is described in Section 5.5.1.4.9.
In another subject from an early, investigator-sponsored open-label teplizumab study, a 37-year-old female developed squamous cell carcinoma, Grade 2 (moderate), 6 months after dosing with teplizumab and was treated with non-drug therapies. The event was considered serious (medically important) by the investigator. The investigator indicated that this event was a recurrence and did not consider the squamous cell carcinoma related to teplizumab.
5.5.3.3 Summary of Pregnancies
As of 23 August 2016, there have been 17 reports of pregnancies across all teplizumab studies (Table 24). Outcomes for the 17 pregnancies include 12 normal neonates, 3 elective terminations of pregnancy, 1 spontaneous abortion, and 1 unknown lost to follow-up. In the
Confidential Page 95 of 130

Teplizumab MacroGenics, Inc.
Investigator's Brochure Version 12.0, 16 November 2016
subject with the spontaneous abortion, the time from last dose of teplizumab to time of conception was approximately 20 months. The investigator assessed the event of spontaneous abortion as unlikely related to the study drug, and suggested the subject’s T1DM and Grave’s disease as an alternate cause of the event.
The outcome of the 2 subjects receiving placebo: one subject delivered a normal neonate, the other subject had an SAE (important medical event) of “complication of pregnancy” (transient abdominal pain and mild vaginal bleeding early in first trimester, resolving within five days). Subsequently, the subject had an elective abortion.
Table 24 Summary of Pregnancies
Assigned Dosing
Regime
Number of
Pregnancies
End of Dosing Until
Conception (approximate)
Outcomes
Full dose; 14-day 10 3 weeks to 4 years; one unknown
6 normal neonates; 2 Elective terminations of pregnancy: 1 spontaneous abortion; 1 unknown outcome (subject lost to follow-up)
Full dose; 6-day 2 (includes one male subject with female partner pregnancy)
4 to 9 months 2 normal neonates
1/3 Dose; 14-day 1 1 month 1 normal neonate
Placebo 4 (includes one male subject with female partner pregnancy)
2.5 to 17 months; one conception while receiving treatment
4 normal neonates 1 elective termination of pregnancy
Total 17
Compound-related lower male and female fertility and copulation/conception indices and a lower percentage of motile sperm were noted at 20 mg/kg 2851055 in the F1 generation of a prenatal/postnatal development, maternal and reproductive toxicity study, conducted in Crl:CD1(ICR) mice using a surrogate mouse antibody (2851055) (Section 4.3.9). Compound 2851055 is the hamster anti-mouse CD3 epsilon chain mAb, 2C11.145, engineered as a chimeric mouse IgG2a (ala,ala). Please note that the mouse IgG2a is the functional equivalent of human IgG1. The relevance of the immune mouse findings for humans is unknown. Thymic function in the mouse is essential even after birth and until about week 5 of age (adult mouse), as shown by the severe immune suppression resulting from early post-natal thymectomy. Humans have postnatal thymus development until adolescence when atrophy occurs; human neonatal thymectomy, however, has not been reported to result in immune suppression or has modest impact on the overall immune function. While these data indirectly suggest that the human fetus would be potentially less sensitive to in utero exposure to thymus-targeted and/or T cell-depleting interventions, caution should still be exercised in order to avoid exposure. As shown in the Protégé trial,
Confidential Page 96 of 130

Teplizumab MacroGenics, Inc.
Investigator's Brochure Version 12.0, 16 November 2016
lymphopenia occurs in over 85% of subjects, but is transient, completely recovering in 2–4 weeks. Given the transient nature of the lymphopenia and the limited dosing (two 14-day cycles – 0.25mg/kg total dose per cycle), this risk is adequately mitigated by having subjects use contraception during the dosing interval.
To manage any potential immune risks during pregnancy and gestation, women with reproductive potential and male subjects with partners of childbearing potential should use highly effective contraceptive precautions during the clinical trial, as described in the study protocol.
5.5.3.4 Deaths
Across all teplizumab studies, there have been 3 deaths (Table 25); 2 in the Protégé study (diabetic glomerulosclerosis/ketoacidosis and extensive anterior wall myocardial infarction with ventricular tachycardia, resulting in sudden cardio-respiratory arrest) and 1 in the Protégé Extension study (unknown cause of death). None of the subjects died during the dosing period of any study and the investigators’ causality assessments in all three cases was not related to study product.
Table 25 Summary of Deaths (All Teplizumab Clinical Studies)
Protocol #/Region Date of Birth
Gender
Adverse Event/
Time to Onset
Post-Last Dose
Cause of Death Relationship
CP-MGA031-01 (Protégé) Ukraine
21 Jan 1990 Female
Diabetic ketoacidosis 9 months
Diabetic ketoacidosis Unlikely
CP-MGA031-01(Protégé) India
26 Jan 1984 Male
Anterior Myocardial Infarction 15 months
Anterior Myocardial Infarction; Ventricular tachycardia; Cardio-
respiratory arrest
Not related
CP-MGA031-02 (Protégé Extension) India
29 Jul 1985 Female
Death 26 months
Unknown None
5.5.4 Risk/Benefit Assessment
Although the primary endpoint was not met in the T1DM Protégé Study, two 14-day courses of teplizumab treatment has been associated with preservation of C-peptide lasting 2 years, especially in younger age groups, or early in the course of Type 1 diabetes mellitus or in US populations or those with lower baseline HbA1c and insulin requirements. There is also evidence of a reduction in insulin use, while maintaining glucose control. It is unknown if teplizumab will result in an improvement in incidence of hypoglycemia a potential benefit of preservation of C-peptide, because it has not been adequately assessed in the initial studies.
Confidential Page 97 of 130

Teplizumab MacroGenics, Inc.
Investigator's Brochure Version 12.0, 16 November 2016
Based on the Protégé study, the main risks of teplizumab over two years consists of transient cytopenias (predominantly lymphopenia), transient, mostly mild, elevations in liver function tests, and if pre-medicated mild to moderate cytokine release and mild to moderate, transient rash. With regard to infection, at the doses used in the Protégé and Protégé Encore studies, EBV reactivation is rare and acute mononucleosis syndrome is not increased. A possible increase in herpes zoster, possibly dose-related is seen, but the number of events is still small and was not confirmed in Protégé Encore. The majority of these cases were in the Protégé study. The one case in the Protégé Encore study occurred in a subject receiving placebo and there were no events in teplizumab subjects. Rigorous, conservative dose stopping rules included in and specific to each protocol have mitigated the potential for the development of SAEs and should be used in future studies. Subjects in teplizumab trials are not exposed to risk from under treatment as they receive teplizumab in addition to insulin and are managed to the standard of care treatment consistent with American Diabetes Association guidelines for patients with T1DM.
Given the potential for important benefit in relation to the expected generally transient and mild to moderate risks, continued investigation of short-term dosing of teplizumab in the treatment of patients with, or at high-risk for developing, T1DM is warranted. Factors for consideration when conducting future studies should include:
1. Recruiting patient populations with greatest benefits observed to date -shortest times from diagnosis, younger age, and higher baseline C-peptide levels
2. Combining anti-CD3 with other immunomodulators or diabetes therapies (concurrently or sequentially)
3. Identifying and enrolling high-risk (clinically, immunologically or genetically defined) subjects in anti-CD3 trials, before insulin dependence (16).
5.6 Post-Marketing Experience
There is no post-marketing experience with teplizumab.
Confidential Page 98 of 130

Teplizumab MacroGenics, Inc.
Investigator's Brochure Version 12.0, 16 November 2016
6 SUMMARY OF DATA AND GUIDANCE FOR THE INVESTIGATOR
6.1 Product Name and Pharmacotherapeutic Group
INN: teplizumab
Pharmacotherapeutic group: humanized IgG1 anti-CD3 monoclonal antibody [hOKT 3γ1 (ala,ala)]
6.2 Proposed Indications
Teplizumab is currently being studied for the prevention or delay of onset of type 1 diabetes mellitus (T1DM) in patients at risk for developing the disease (e.g. family history and autoantibody positive).
6.3 Posology/Dosing and Administration
Dosage form and description: 1 mg teplizumab per mL presented as a 2-mL dosage, and supplied in a 2-mL single-use vial
Route of administration: Teplizumab is available as an intravenous infusion. No studies involving subcutaneous administration are being conducted at this time. Teplizumab should not be administered as IV push.
6.3.1 Regimens for Current T1DM Studies
Dosing regimens for previous T1DM studies is described in Section 5.3. Dosing for the current TN-10 At-Risk Study includes a dosing regimen where patients will receive once daily IV dose of teplizumab for 14 days (Table 26).
Table 26 T1DM Dosing Regimens for the TN-10 At-Risk Study
Regimen Name Description
Full 14-day regimen 14-day course of teplizumab Once-daily IV doses 51 μg/m2 (Day 1) 103 μg/m2 (Day 2) 207 μg/m2 (Day 3) 413 μg/m2 (Day 4) 826 μg/m2 (Days 5-14) Total cumulative avg. dose = ~17 mg
Abbreviations: Avg = average; IV=Intravenous Note: Total average dose is the cumulative dose for a subject weighing 70 kg with a BSA of 1.92 m2
Confidential Page 99 of 130

Teplizumab MacroGenics, Inc.
Investigator's Brochure Version 12.0, 16 November 2016
The IV dosing regimen of teplizumab (MGA031) that is being studied for T1DM is based on BSA in m2.
Tepliuzmab is administered IV as a very dilute protein in a physiological salt solution near neutral pH, prepared with 0.9% sodium chloride (NaCL), and is administered SC as a more concentrated protein in physiological salt solution near neutral pH.
Every effort should be made to prepare the infusion solution immediately before use. No more than 2 hours may elapse between preparation of the solution and the start of the IV infusion. The infusion must be completed within 6 hours of preparation. The infusion solution may only be prepared in IV bags made of PVC (polyvinyl chloride), and the tubing of the IV administration set must also be made of PVC. If a syringe pump is to be used for the infusion, an IV bag is not required for the infusion.
The infusion is prepared by adding a calculated volume from a 1:10 dilution of the study drug to a PVC IV bag containing 25 mL (or 50mL with 25mL removed) 0.9% Sodium Chloride for Injection (if a syringe pump is being used for administration, a 25mL of 0.9% Sodium Chloride for Injection is used as well.)
After the diluted study drug is added to the IV bag, the bag should be kept at room temperature before it is administered to the subject.
Infusion should occur at a constant rate over a minimum of 30 minutes.
The infusion should be started within 2 hours of preparation.
6.3.2 Premedication and Drug Administration Instructions
Premedication with ibuprofen or similar NSAID and with an antihistamine is recommended and may be useful in subjects who develop rashes during drug administration.
Intravenous drug delivery devices, including IV bags and tubing, must be composed of PVC, and syringes of polypropylene, for administration of teplizumab. The use of drug delivery devices other than these may result in adsorption of the teplizumab and under-dosing.
6.3.3 Storage and Handling
Teplizumab is provided at a concentration of 1 mg/mL in 2-mL glass vials with FluroTec®-coated butyl rubber stoppers and flip-off seals. The formulation of teplizumab consists of:
10 mM sodium phosphate, pH 6.1
150 mM sodium chloride
0.05 mg/mL polysorbate 80
Confidential Page 100 of 130

Teplizumab MacroGenics, Inc.
Investigator's Brochure Version 12.0, 16 November 2016
Teplizumab vials should be stored upright at 2°– 8°C (36°– 46°F) and must not be frozen or shaken. Protect from light during storage. Teplizumab should not be stored with food.
Use of standard laboratory practices for avoidance of contact is advised. Wear gloves when handling; wash hands when work is finished. Use standard medical waste procedures for disposal.
6.4 Contraindications
Teplizumab treatment is contraindicated in subjects with a previous history of serious CRS to teplizumab or other humanized anti-CD3 monoclonal antibodies with no or minimal capacity to bind Fc receptors.
6.5 Special Warnings and Precautions
6.5.1 Cytokine-Release Syndrome
Serious CRS has been reported in association with infusion of teplizumab. Signs and symptoms of CRS may include allergic- /hypersensitivity-like reaction, arthralgia, bronchospasm, cough, dizziness, dyspnea, fatigue, headache, myalgia, nausea, pruritus/itching, fever, rash, chills, diaphoresis, tachycardia, urticaria, and vomiting. Appropriate medical treatment should be immediately available in the event of serious CRS during administration of teplizumab. Pre-treatment with NSAID agents, with or without an antihistamine, should be considered for minimization of occurrence or severity of CRS.
6.5.2 Abnormal Liver Function Laboratory Tests
Treatment with teplizumab has been associated with a higher incidence of transaminase and bilirubin elevations. These elevations did not result in apparent permanent or clinically evident hepatic injury in clinical trials.
A transient, mild increase is seen in mean ALT and bilirubin (Figure 16 and Figure 17). This increase peaked during the first week of infusion, (ALT on Day 7 and bilirubin on Day 3), and generally resolved by Day 28.
Teplizumab treatment is not recommended in subjects with elevated ALT or AST > 1.5x ULN. Subjects who develop elevated ALT or AST > 3x ULN should discontinue treatment.
ALT and AST levels should be monitored periodically during treatment with teplizumab. When clinically indicated, other liver function tests such as bilirubin should be considered.
6.5.3 Lymphopenia
Teplizumab causes a transient reduction in the number of circulating lymphocytes, which is directly related to the mechanism of action of the drug. In the Protégé study, lymphopenia
Confidential Page 101 of 130

Teplizumab MacroGenics, Inc.
Investigator's Brochure Version 12.0, 16 November 2016
occurred in just over 85% of 14-day full regimen subjects. Grade 3 (< 500 lymphocytes/mcL) and occasional Grade 4 (< 200 lymphocytes/mcL) lymphopenia should be expected. Maximum lymphopenia is typically observed at the sixth day of treatment and then resolves, despite continued dosing. In most individuals, circulating lymphocytes return to 80% of baseline values 2 weeks after the last dose of drug and to 100% of baseline values shortly thereafter. The development of transient lymphopenia does not appear to be associated with an overall increased risk of infection. Use of teplizumab in subjects with preexisting lymphopenia (< 1000 lymphocytes/μL) is not recommended. Complete blood count with differential should be monitored periodically during treatment with teplizumab.
6.5.4 Hypoglycemia
Subjects receiving teplizumab may require a reduced dosage of insulin and should be monitored closely for hypoglycemia.
6.5.5 Active Infections
Initiation of treatment with teplizumab is not recommended in subjects with active infections, including clinically important localized infections.
Subjects should be closely monitored for the development of symptoms and signs of infection during and after receiving the study drug.
6.5.6 Vaccinations
Live vaccines should not be given concurrently with or within 8 weeks of teplizumab, as clinical safety has not been established. No data are available on the effectiveness of non-live vaccination in subjects receiving teplizumab. Non-live vaccination should not be given concurrently with or within 4 weeks of dosing teplizumab.
6.6 Interactions with Other Drugs and Food
There are no known interactions between teplizumab and other drugs or food. Caution is advised in considering treatment with concomitant medications with AE profiles that may overlap with those of teplizumab, such as drugs associated with liver function abnormalities, cytopenias, hypotension, or other immunosuppressive drugs.
6.7 Reference Safety Information
Based on data up to 23 August 2016, Table 30 in Appendix 2 contains a list of all ADRs for patients receiving teplizumab. The expectedness of an adverse reaction for regulatory reporting is determined by the sponsor in the RSI. The list is based upon evaluation of events previously observed, including data from 645 patients exposed to teplizumab during completed global clinical trials (Phase 1 through Phase 3), and not on the basis of what might be anticipated from the pharmacological properties of a medicinal product.
Confidential Page 102 of 130

Teplizumab MacroGenics, Inc.
Investigator's Brochure Version 12.0, 16 November 2016
The table in this section (Table 27) contains the ADRs that are considered to be expected events for regulatory reporting purposes. For the purpose of safety reporting in clinical trials, only serious adverse reactions can be considered expected. This determination of expectedness is made at the discretion of the sponsor based on medical judgment, nonclinical safety information, and overall reporting frequency.
Table 27 Expected ADRs for Regulatory Reporting Purposes
System Organ Class Preferred Terms
Blood and lymphatic system disorders Lymphopenia a Neutropenia b
Immune system disorders Cytokine-release syndrome c
Investigations AST/ALT increased
a Decreased lymphocyte count, lymphopenia, decreased lymphocyte percentage. b Decreased neutrophil count, decreased neutrophil percent, neutropenia. c As characterized typically by nausea, vomiting, headache, chills/rigors/pyrexia,
and/or rash in teplizumab-treated subjects.
6.8 Postmarketing
Teplizumab has not been approved, marketed, or withdrawn in any country.
6.9 Carcinogenesis, Mutagenesis, and Impairment of Fertility
Carcinogenesis Long-term studies have not been conducted to evaluate the carcinogenic potential of teplizumab. Teplizumab is a potentially immunosuppressive monoclonal antibody. Treatment with T-cell suppressive therapies may secondarily increase cancer risk or tumor progression, especially if significant immunosuppression occurs. Lymphoproliferative changes associated with possible EBV viral recrudescence were observed in chimpanzees following a single subcutaneous dose of 30 mg/kg, but not demonstrated in clinical trials to date. In clinical studies, short-term increases in EBV DNA were observed in fewer than 10% of subjects.
Mutagenesis Genetic toxicity studies with teplizumab, a monoclonal antibody, are not warranted (ICH 1997) and have not been conducted.
Impairment of Fertility Mice were treated with a surrogate antibody [2C11-mG2a (ala,ala)] that binds to the CD3-ε chain of the receptor on mouse T cells. Compound-related lower male and female fertility and copulation/conception indices and a lower percentage of motile sperm were noted at 20 mg/kg 2851055 in the F1 generation of a prenatal/postnatal development, maternal and reproductive toxicity study, conducted in Crl:CD1(ICR) mice using a surrogate mouse antibody (2851055) (Section 4.3.9). The clinical relevance of the reproductive toxicity
Confidential Page 103 of 130

Teplizumab MacroGenics, Inc.
Investigator's Brochure Version 12.0, 16 November 2016
finding is unknown and, despite the required use of contraception in the study, there were several pregnancies with normal gestations, as described in Section 5.5.3.3.
Use During Pregnancy and Lactation Teplizumab should not be used during pregnancy. In pregnant mice given a surrogate antibody [2C11-mG2a (ala,ala)] that binds to the CD3-ε chain of the receptor, there was an increased incidence of embryonic resorptions. However, no fetal malformations or abnormalities occurred in surviving fetuses. In a subsequent study in which the surrogate anti-CD3 antibody [2C11-mG2a(ala,ala)] was administered to pregnant mice at the same time during pregnancy and at the same dose level, there were no effects on embryonic resorption, F2 offspring. Consistent with the expected pharmacology for this anti-CD3 monoclonal antibody, treatment at all dose levels in the F0 maternal mice and the F1 generation caused a non-dose-related decrease in the percentage of circulating T lymphocytes and T subsets; which was accompanied by a corresponding increase in the percentage of circulating B lymphocytes and impacted thymus size in F1 mice. Given the transient nature of lymphopenia and the limited dosing, this risk is mitigated by having subjects use contraception during the dosing interval.
To manage any potential immune risks during pregnancy and gestation, women with reproductive potential should use highly effective contraceptive precautions during the clinical study, as advised by the protocol. Male subjects with partners of child-bearing potential should use barrier contraception in addition to having their partners use another method of contraception, as advised by the protocol.
It is not known if teplizumab is excreted in human milk during lactation. Women who are breastfeeding should not be administered teplizumab.
6.10 Pharmacokinetics/Pharmacodynamics in Special Populations
No data are available.
6.11 Overdose
Overdose of teplizumab has been associated with CRS. In case of overdose, the infusion should be discontinued. There is no known antidote to teplizumab. Management of overdose should include supportive therapy.
6.12 Effects on Ability to Drive Vehicles and Operate Machinery
No studies on the effects on the ability to drive and use machines have been performed. Routine adverse event monitoring did not indicate any effects that may impair the ability to drive or operate heavy machinery.
Confidential Page 104 of 130

Teplizumab MacroGenics, Inc.
Investigator's Brochure Version 12.0, 16 November 2016
7 REFERENCES
1. Alegre ML, Tso JY, Sattar HA, Smith J, Desalle F, Cole M, et al. An anti-murine CD3 monoclonal antibody with a low affinity for Fc gamma receptors suppresses transplantation responses while minimizing acute toxicity and immunogenicity. J Immunol. 1995;155(3):1544-55.
2. Alegre ML, Collins AM, Pulito VL, Brosius RA, Olson WC, Zivin RA, et al. Effect of a single amino acid mutation on the activating and immunosuppressive properties of a "humanized" OKT3 monoclonal antibody. J Immunol. 1992;148(11):3461-8.
3. Alegre ML, Peterson LJ, Xu D, Sattar HA, Jeyarajah DR, Kowalkowski K, et al. A non-activating "humanized" anti-CD3 monoclonal antibody retains immunosuppressive properties in vivo. Transplantation. 1994;57(11):1537-43.
4. Alegre ML, Vandenabeele P, Depierreux M, Florquin S, schodt-Lanckman M, Flamand V, et al. Cytokine release syndrome induced by the 145-2C11 anti-CD3 monoclonal antibody in mice: prevention by high doses of methylprednisolone. J Immunol. 1991;146(4):1184-91.
5. Anderson MS, Bluestone JA. The NOD mouse: a model of immune dysregulation. Annu Rev Immunol. 2005;23:447-85.
6. Belghith M, Bluestone JA, Barriot S, Megret J, Bach JF, Chatenoud L. TGF-beta-dependent mechanisms mediate restoration of self-tolerance induced by antibodies to CD3 in overt autoimmune diabetes. Nat Med. 2003;9(9):1202-8.
7. Bisikirska B, Colgan J, Luban J, Bluestone JA, Herold KC. TCR stimulation with modified anti-CD3 mAb expands CD8+ T cell population and induces CD8+CD25+ Tregs. J Clin Invest. 2005;115(10):2904-13.
8. Boldt DH, Fischbach M, Kuehl TJ. Cellular immunology in the baboon (Papio cynocephalus): examination of structural and functional characteristics of adult and fetal lymphoid cells. J Immunogenet. 1984;11(3-4):219-32.
9. Bresson D, Togher L, Rodrigo E, Chen Y, Bluestone JA, Herold KC, et al. Anti-CD3 and nasal proinsulin combination therapy enhances remission from recent-onset autoimmune diabetes by inducing Tregs. J Clin Invest. 2006;116(5):1371-81.
10. Chatenoud L. CD3-specific antibody-induced active tolerance: from bench to bedside. Nat Rev Immunol. 2003;3(2):123-32.
11. Chatenoud L. CD3-specific antibodies restore self-tolerance: mechanisms and clinical applications. Curr Opin Immunol. 2005;17(6):632-7.
12. Chatenoud L, Bluestone JA. CD3-specific antibodies: a portal to the treatment of autoimmunity. Nat Rev Immunol. 2007;7(8):622-32.
Confidential Page 105 of 130

Teplizumab MacroGenics, Inc.
Investigator's Brochure Version 12.0, 16 November 2016
13. Chatenoud L, Primo J, Bach JF. CD3 antibody-induced dominant self tolerance in overtly diabetic NOD mice. J Immunol. 1997;158(6):2947-54.
14. Chatenoud L, Thervet E, Primo J, Bach JF. Anti-CD3 antibody induces long-term remission of overt autoimmunity in nonobese diabetic mice. Proc Natl Acad Sci U S A. 1994;91(1):123-7.
15. Chong AS, Shen J, Tao J, Yin D, Kuznetsov A, Hara M, et al. Reversal of diabetes in non-obese diabetic mice without spleen cell-derived beta cell regeneration. Science. 2006;311(5768):1774-5.
16. Daifotis AG, Koenig S, Chatenoud L, Herold KC. Anti-CD3 clinical trials in type 1 diabetes mellitus. Clin Immunol. 2013.
17. Ferran C, Dy M, Merite S, Sheehan K, Schreiber R, Leboulenger F, et al. Reduction of morbidity and cytokine release in anti-CD3 MoAb-treated mice by corticosteroids. Transplantation. 1990;50(4):642-8.
18. Ferran C, Sheehan K, Dy M, Schreiber R, Merite S, Landais P, et al. Cytokine-related syndrome following injection of anti-CD3 monoclonal antibody: further evidence for transient in vivo T cell activation. Eur J Immunol. 1990;20(3):509-15.
19. Glandt M, Hagopian W, Herold KC. Treatment of type 1 diabetes with anti-CD3 monoclonal antibody. Rev Endocr Metab Disord. 2003;4(4):361-8.
20. Gulley ML. Molecular diagnosis of Epstein-Barr virus-related diseases. J Mol Diagn. 2001;3(1):1-10.
21. Hayward AR, Shreiber M. Neonatal injection of CD3 antibody into nonobese diabetic mice reduces the incidence of insulitis and diabetes. J Immunol. 1989;143(5):1555-9.
22. Hayward AR, Shriber M. Reduced incidence of insulitis in NOD mice following anti-CD3 injection: requirement for neonatal injection. J Autoimmun. 1992;5(1):59-67.
23. Henrickson M, Giannini EH, Hirsch R. Reduction of mortality and lymphadenopathy in MRL-lpr/lpr mice treated with nonmitogenic anti-CD3 monoclonal antibody. Arthritis Rheum. 1994;37(4):587-94.
24. Herold KC, Bluestone JA, Montag AG, Parihar A, Wiegner A, Gress RE, et al. Prevention of autoimmune diabetes with nonactivating anti-CD3 monoclonal antibody. Diabetes. 1992;41(3):385-91.
25. Herold KC, Gitelman SE, Masharani U, Hagopian W, Bisikirska B, Donaldson D, et al. A single course of anti-CD3 monoclonal antibody hOKT3gamma1(Ala-Ala) results in improvement in C-peptide responses and clinical parameters for at least 2 years after onset of type 1 diabetes. Diabetes. 2005;54(6):1763-9.
Confidential Page 106 of 130

Teplizumab MacroGenics, Inc.
Investigator's Brochure Version 12.0, 16 November 2016
26. Herold KC, Hagopian W, Auger JA, Poumian-Ruiz E, Taylor L, Donaldson D, et al. Anti-CD3 monoclonal antibody in new-onset type 1 diabetes mellitus. N Engl J Med. 2002;346(22):1692-8.
27. Herold KC, Gitelman S, Greenbaum C, Puck J, Hagopian W, Gottlieb P, et al. Treatment of patients with new onset Type 1 diabetes with a single course of anti-CD3 mAb Teplizumab preserves insulin production for up to 5 years. Clin Immunol. 2009;132(2):166-73.
28. Herold KC, Gitelman SE, Willi SM, Gottlieb PA, Waldron-Lynch F, Devine L, et al. Teplizumab treatment may improve C-peptide responses in participants with type 1 diabetes after the new-onset period: a randomised controlled trial. Diabetologia. 2013;56(2):391-400.
29. Herold KC, Gitelman SE, Ehlers MR, Gottlieb PA, Greenbaum CJ, Hagopian W, et al. Teplizumab (Anti-CD3 mAb) Treatment Preserves C-Peptide Responses in Patients With New-Onset Type 1 Diabetes in a Randomized Controlled Trial: Metabolic and Immunologic Features at Baseline Identify a Subgroup of Responders. Diabetes. 2013;62(11):3766-74.
30. Heymann AD, Chodick G, Karpati T, Kamer L, Kremer E, Green MS, et al. Diabetes as a risk factor for herpes zoster infection: results of a population-based study in Israel. Infection. 2008;36(3):226-30.
31. Hughes C, Wolos JA, Giannini EH, Hirsch R. Induction of T helper cell hyporesponsiveness in an experimental model of autoimmunity by using nonmitogenic anti-CD3 monoclonal antibody. J Immunol. 1994;153(7):3319-25.
32. Keymeulen B, Vandemeulebroucke E, Ziegler AG, Mathieu C, Kaufman L, Hale G, et al. Insulin needs after CD3-antibody therapy in new-onset type 1 diabetes. N Engl J Med. 2005;352(25):2598-608.
33. Knip M, Veijola R, Virtanen SM, Hyoty H, Vaarala O, Akerblom HK. Environmental triggers and determinants of type 1 diabetes. Diabetes. 2005;54 Suppl 2:S125-S36.
34. Kodama S, Kuhtreiber W, Fujimura S, Dale EA, Faustman DL. Islet regeneration during the reversal of autoimmune diabetes in NOD mice. Science. 2003;302(5648):1223-7.
35. Kohm AP, Williams JS, Bickford AL, McMahon JS, Chatenoud L, Bach JF, et al. Treatment with nonmitogenic anti-CD3 monoclonal antibody induces CD4+ T cell unresponsiveness and functional reversal of established experimental autoimmune encephalomyelitis. J Immunol. 2005;174(8):4525-34.
Confidential Page 107 of 130

Teplizumab MacroGenics, Inc.
Investigator's Brochure Version 12.0, 16 November 2016
36. Leo O, Foo M, Sachs DH, Samelson LE, Bluestone JA. Identification of a monoclonal antibody specific for a murine T3 polypeptide. Proc Natl Acad Sci U S A. 1987;84(5):1374-8.
37. Luo X, Herold KC, Miller SD. Immunotherapy of type 1 diabetes: where are we and where should we be going? Immunity. 2010;32(4):488-99.
38. Melton DA. Reversal of type 1 diabetes in mice. N Engl J Med. 2006;355(1):89-90.
39. Mottram PL, Murray-Segal LJ, Han W, Maguire J, Stein-Oakley AN. Remission and pancreas isograft survival in recent onset diabetic NOD mice after treatment with low-dose anti-CD3 monoclonal antibodies. Transpl Immunol. 2002;10(1):63-72.
40. Nir T, Melton DA, Dor Y. Recovery from diabetes in mice by beta cell regeneration. J Clin Invest. 2007;117(9):2553-61.
41. Nishio J, Gaglia JL, Turvey SE, Campbell C, Benoist C, Mathis D. Islet recovery and reversal of murine type 1 diabetes in the absence of any infused spleen cell contribution. Science. 2006;311(5768):1775-8.
42. Oldstone MB. Molecular and cellular mechanisms, pathogenesis, and treatment of insulin-dependent diabetes obtained through study of a transgenic model of molecular mimicry. Curr Top Microbiol Immunol. 2005;296:65-87.
43. Parleviet KJ, Jonker M, ten Berge RJ, van Lier RA, Wilmink JM, Strengers PF, et al. Anti-CD3 murine monoclonal isotype switch variants tested for toxicity and immunologic monitoring in four chimpanzees. Transplantation. 1990;50(5):889-92.
44. Rao PE, Olini G, Kille J, Muchmore E, Talle MA, Brake G, et al. OKT3E, an anti-CD3 antibody that does not elicit side effects or antiidiotype responses in chimpanzees. Transplantation. 1991;52(4):691-7.
45. Sakaguchi S. Naturally arising Foxp3-expressing CD25+CD4+ regulatory T cells in immunological tolerance to self and non-self. Nat Immunol. 2005;6(4):345-52.
46. Sakaguchi S, Powrie F. Emerging challenges in regulatory T cell function and biology. Science. 2007;317(5838):627-9.
47. Salomon B, Lenschow DJ, Rhee L, Ashourian N, Singh B, Sharpe A, et al. B7/CD28 costimulation is essential for the homeostasis of the CD4+CD25+ immunoregulatory T cells that control autoimmune diabetes. Immunity. 2000;12(4):431-40.
48. Sandusky GE, Horton PJ, Wightman KA. Use of monoclonal antibodies to human lymphocytes to identify lymphocyte subsets in lymph nodes of the rhesus monkey and the dog. J Med Primatol. 1986;15(6):441-51.
Confidential Page 108 of 130

Teplizumab MacroGenics, Inc.
Investigator's Brochure Version 12.0, 16 November 2016
49. Sherry N, Hagopian W, Ludvigsson J, Jain SM, Wahlen J, Ferry RJ, Jr., et al. Teplizumab for treatment of type 1 diabetes (Protege study): 1-year results from a randomised, placebo-controlled trial. Lancet. 2011.
50. Shoda LK, Young DL, Ramanujan S, Whiting CC, Atkinson MA, Bluestone JA, et al. A comprehensive review of interventions in the NOD mouse and implications for translation. Immunity. 2005;23(2):115-26.
51. Smith JA, Tso JY, Clark MR, Cole MS, Bluestone JA. Nonmitogenic anti-CD3 monoclonal antibodies deliver a partial T cell receptor signal and induce clonal anergy. J Exp Med. 1997;185(8):1413-22.
52. Suri A, Calderon B, Esparza TJ, Frederick K, Bittner P, Unanue ER. Immunological reversal of autoimmune diabetes without hematopoietic replacement of beta cells. Science. 2006;311(5768):1778-80.
53. Tang Q, Henriksen KJ, Bi M, Finger EB, Szot G, Ye J, et al. In vitro-expanded antigen-specific regulatory T cells suppress autoimmune diabetes. J Exp Med. 2004;199(11):1455-65.
54. Tang Q, Adams JY, Tooley AJ, Bi M, Fife BT, Serra P, et al. Visualizing regulatory T cell control of autoimmune responses in nonobese diabetic mice. Nat Immunol. 2006;7(1):83-92.
55. Tran GT, Carter N, He XY, Spicer TS, Plain KM, Nicolls M, et al. Reversal of experimental allergic encephalomyelitis with non-mitogenic, non-depleting anti-CD3 mAb therapy with a preferential effect on T(h)1 cells that is augmented by IL-4. Int Immunol. 2001;13(9):1109-20.
Confidential Page 109 of 130

Teplizumab MacroGenics, Inc.
Investigator's Brochure Version 12.0, 16 November 2016
Appendix 1 Status of Ongoing and Completed Clinical Teplizumab Studies in Type 1 Diabetes Mellitus
Table 28 Overview of Ongoing Studies for Teplizumab as of 23 August 2016
Study ID Phase Status Countries Study Title Study
Design
Dosing
Regimen
Study
Population
FVFP a Planned
Enrollment
Subject
Exposure
ISCT-MGA031-005 (“TN-10 At -Risk”)
2 Ongoing US Canada Germany Italy Australia
Anti-CD3 (teplizumab) for Prevention of Diabetes in Relatives at Risk for Type 1 Diabetes Mellitus
Randomized Double-blind Placebo-controlled
One cycle of Full 14-day regimen
Autoantibody positive relatives of T1DM proband with abnormal Glucose tolerance. Ages 8 – 45 years
18Jul11 70-80 (Planned)
64
a FVFP=first visit first patient
Confidential Page 110 of 130

Teplizumab MacroGenics, Inc.
Investigator's Brochure Version 12.0, 16 November 2016
Table 29 Overview of Studies Completed for Teplizumab as of 23 August 2016
Study ID Phase Status Countries Study Title Study Design Dosing
Regimen
Study
Population
FVFP a Planned
Enrollment
Subject
Exposure
CP-MGA031-01 Protégé
2/3 Completed (CSR complete as of 14Aug12)
Canada Czech Republic Estonia Germany India Israel Latvia Mexico Netherlands Poland Romania Spain Sweden UK Ukraine United States
The Protégé Study - Clinical Trial of Teplizumab (MGA031) in Children and Adults With Recent-Onset Type 1 Diabetes Mellitus
Segment 1: Open-label Segment 2: Randomized; Double-blind; Placebo-controlled; 2:1:1:1 randomization
Segment 1: Two cycles of Full 14-day regimen, six months apart Segment 2: Regimens (Two cycles, six months apart): Full 14-day 1/3 14-day Full 6-day Placebo
Patients aged 8-35 with T1DM, onset within past 12 weeks.
Seg 1: 14Feb2007 Seg 2: 09Aug2007
Seg 1: 38 (actual) Seg 2: 516 (actual)
Seg 1: 38 Seg 2: Full 14-day (n=207) 1/3 14-day (n=102) Full 6-day (n=106) Placebo (n=98)
CP-MGA031-06 (SUBCUE)
1b Completed (CSR complete as of 27Jan12)
US Subcutaneous Administration of Teplizumab in Adults With Type 1 Diabetes (SUBCUE)
Randomized; Double-blind; Placebo-controlled; 1:1:1 randomization
Regimens: 1/3 14-day IV 1/3 14-day SC Full 14-day IV Placebo
Patients aged 18–35, >12 wks and < 52 wks from diagnosis of T1DM
23Sep10 1 (71 Planned- study terminated early, in Oct 2010)
1
Confidential Page 111 of 130

Teplizumab MacroGenics, Inc.
Investigator's Brochure Version 12.0, 16 November 2016
Table 29 Overview of Studies Completed for Teplizumab as of 23 August 2016
Study ID Phase Status Countries Study Title Study Design Dosing
Regimen
Study
Population
FVFP a Planned
Enrollment
Subject
Exposure
CP-MGA031-04 Psoriasis
2a Completed (CSR complete as of 14Oct11)
US Safety Study the Monoclonal Antibody Teplizumab (MGA031) in Subjects With Moderate or More Severe Psoriasis
Open-label 1 (36 Planned, study terminated early)
1
CP-MGA031-02 Protégé Extension
3b
Completed (CSR issued 05 Oct12)
Czech Republic Estonia India Israel Latvia Poland Romania Spain Sweden Ukraine United States
Protégé Extension Trial - Long Term Follow Up Trial for Subjects Who Completed the Protégé Study (CP-MGA031-01)
Follow-up to Study CP-MGA031-01 (Retrospective cohort of Protégé patients)
N/A (no drug administered)
Subjects who completed Protocol CP-MGA031-01
11Feb2009 219 (actual) (554 was target; enrollment terminated early in Oct 2010)
N/A (no drug administered)
Confidential Page 112 of 130

Teplizumab MacroGenics, Inc.
Investigator's Brochure Version 12.0, 16 November 2016
Table 29 Overview of Studies Completed for Teplizumab as of 23 August 2016
Study ID Phase Status Countries Study Title Study Design Dosing
Regimen
Study
Population
FVFP a Planned
Enrollment
Subject
Exposure
CP-MGA031-03 Protégé Encore
3 Completed (CSR issued 10 Dec12)
Belgium Czech Republic Finland Germany India Israel Mexico Poland Romania Spain Ukraine UK United States
Protege Encore Study- Clinical Trial of Teplizumab (MGA031) in Children and Adults With Recent-Onset Type 1 Diabetes Mellitus
Randomized; Double-blind; Placebo-controlled; 1:1:1:1 randomization
Regimens (Two cycles, six months apart): Full 14-day 1/3 14-day Full 6-day Placebo
Patients aged 8-35 with T1DM, onset within past 12 weeks.
15Sep09 254 (400 planned, enrollment/dosing discontinued in Oct 2010)
Regimens Full 14-day (n=63) 1/3 14-day (n=66) Full 6-day (n=63) Placebo (n=62)
ISCT-MGA031-003 ITN027AI; Study 4; AbATE
2 Study completed (CSR submitted on 12 May 2014)
US Phase 2 Multiple-Dose Treatment of Type 1 Diabetes Mellitus with hOKT3γ1 (Ala-Ala)
Open-label Two cycles of Full 14-day regimen or std of care, one year apart
Patients aged 8-30 with T1DM, onset within past 8 weeks.
13Sep05 83 (81 planned)
Full-day regimen (n=52), placebo (n=25), enrolled but did not receive study drug (n=6)
Confidential Page 113 of 130

Teplizumab MacroGenics, Inc.
Investigator's Brochure Version 12.0, 16 November 2016
Table 29 Overview of Studies Completed for Teplizumab as of 23 August 2016
Study ID Phase Status Countries Study Title Study Design Dosing
Regimen
Study
Population
FVFP a Planned
Enrollment
Subject
Exposure
ISCT-MGA031-001 Delay; Study 5
2 Study completed (CSR not completed; however, publication in Diabetologia on 21 October 2012)
US Phase 2 trial of hOKT3γ1(Ala-Ala), teplizumab, for treatment of patients with recent onset Type 1 diabetes mellitus
Randomized Double-blind Placebo-controlled
One cycle of Full 14-day regimen or placebo in blinded segment (yr 1); one cycle of Full 14-day regimen in open-label segment (yr 2)
Patients aged 8-30 T1DM, onset within past 4-12 months with residual pancreatic islet cell function
05Jul07 63 (64 planned)
Full-day regimen (n=31), placebo (n=27), enrolled but did not receive study drug (n=5)
a All study subjects have completed the trial. No additional teplizumab clinical studies were completed as of the cutoff date for this Investigator’s Brochure.
Confidential Page 114 of 130

Teplizumab MacroGenics, Inc.
Investigator's Brochure Version 12.0, 16 November 2016
Appendix 2 Adverse Drug Reactions
Table 30 Teplizumab Adverse Drug Reactions1 from Completed Trials with Expectedness
System Organ Class
Preferred Term (MedDRA v14.0)2
Adverse Drug Reactions Serious Adverse Drug Reactions
Any
Teplizumaba
(N=645)
n (%)
Frequency Category b
Any
Teplizumaba
(N=645)
n (%)
Frequency Category b Expectedness c
Blood and lymphatic system disorders
Lymphopenia 394 (61.1) Very Common 1 (0.2) Uncommon Expected
Leukopenia 244 (37.8) Very Common - - -
Neutropenia 140 (21.7) Very Common 2 (0.3) Uncommon Expected
Anaemia 48 (7.4) Common - - -
Thrombocytopenia 40 (6.2) Common - - -
Eosinophilia 13 (2.0) Common - - -
Monocytopenia 5 (0.8) Uncommon - - -
Leukocytosis 3 (0.5) Uncommon - - -
Lymphadenopathy 2 (0.3) Uncommon - - -
Monocytosis 1 (0.2) Uncommon - - -
Neutrophilia 2 (0.3) Uncommon - - -
Eosinopenia 1 (0.2) Uncommon - - -
Erythropenia 1 (0.2) Uncommon - - -
Hyperglobulinaemia 1 (0.2) Uncommon - - -
Lymph node pain 1 (0.2) Uncommon - - -
Pancytopenia 1 (0.2) Uncommon - - -
Cardiac disorders
Angina pectoris 1 (0.2) Uncommon - - -
Bradycardia 1 (0.2) Uncommon - - -
Confidential Page 115 of 130

Teplizumab MacroGenics, Inc.
Investigator's Brochure Version 12.0, 16 November 2016
Table 30 Teplizumab Adverse Drug Reactions1 from Completed Trials with Expectedness
System Organ Class
Preferred Term (MedDRA v14.0)2
Adverse Drug Reactions Serious Adverse Drug Reactions
Any
Teplizumaba
(N=645)
n (%)
Frequency Category b
Any
Teplizumaba
(N=645)
n (%)
Frequency Category b Expectedness c
Sinus tachycardia 1 (0.2) Uncommon - - -
Tachycardia 1 (0.2) Uncommon - - -
Ear and labyrinth disorders
Deafness 1 (0.2) Uncommon - - -
Deafness neurosensory 1 (0.2) Uncommon 1 (0.2) Uncommon -
Ear pain 1 (0.2) Uncommon - - -
Tinnitus 1 (0.2) Uncommon - - -
Vertigo 1 (0.2) Uncommon - - -
Eye disorders
Vision blurred 3 (0.5) Uncommon - - -
Cataract 1 (0.2) Uncommon - - -
Cataract subcapsular 1 (0.2) Uncommon 1 (0.2) Uncommon -
Conjunctival hyperaemia 1 (0.2) Uncommon - - -
Conjunctivitis 1 (0.2) Uncommon - - -
Diabetic retinopathy 1 (0.2) Uncommon - - -
Eye pain 1 (0.2) Uncommon - - -
Gastrointestinal disorders
Nausea 77 (11.9) Very Common 1 (0.2) Uncommon -
Vomiting 47 (7.3) Common - - -
Diarrhoea 20 (3.1) Common - - -
Abdominal pain 11 (1.7) Common - - -
Abdominal pain upper 11 (1.7) Common - - -
Confidential Page 116 of 130

Teplizumab MacroGenics, Inc.
Investigator's Brochure Version 12.0, 16 November 2016
Table 30 Teplizumab Adverse Drug Reactions1 from Completed Trials with Expectedness
System Organ Class
Preferred Term (MedDRA v14.0)2
Adverse Drug Reactions Serious Adverse Drug Reactions
Any
Teplizumaba
(N=645)
n (%)
Frequency Category b
Any
Teplizumaba
(N=645)
n (%)
Frequency Category b Expectedness c
Aphthous stomatitis 5 (0.8) Uncommon - - -
Dyspepsia 6 (0.9) Uncommon - - -
Hyperchlorhydria 2 (0.3) Uncommon - - -
Mouth ulceration 3 (0.5) Uncommon - - -
Abdominal discomfort 2 (0.3) Uncommon - - -
Cheilitis 2 (0.3) Uncommon - - -
Gastritis 2 (0.3) Uncommon - - -
Abdominal distension 1 (0.2) Uncommon - - -
Dysphagia 1 (0.2) Uncommon - - -
Flatulence 1 (0.2) Uncommon - - -
General disorders and administration site conditions
-
Pyrexia 113 (17.5) Very Common 1 (0.2) Uncommon -
Chills 52 (8.1) Common - - -
Fatigue 48 (7.4) Common - - -
Asthenia 5 (0.8) Uncommon - - -
Influenza like illness 5 (0.8) Uncommon - - -
Pain 5 (0.8) Uncommon 1 (0.2) Uncommon -
Infusion site erythema 4 (0.6) Uncommon - - -
Oedema peripheral 5 (0.8) Uncommon - - -
Infusion site pain 4 (0.6) Uncommon - - -
Malaise 4 (0.6) Uncommon - - -
Confidential Page 117 of 130

Teplizumab MacroGenics, Inc.
Investigator's Brochure Version 12.0, 16 November 2016
Table 30 Teplizumab Adverse Drug Reactions1 from Completed Trials with Expectedness
System Organ Class
Preferred Term (MedDRA v14.0)2
Adverse Drug Reactions Serious Adverse Drug Reactions
Any
Teplizumaba
(N=645)
n (%)
Frequency Category b
Any
Teplizumaba
(N=645)
n (%)
Frequency Category b Expectedness c
Non-cardiac chest pain 2 (0.3) Uncommon - - -
Catheter site pain 1 (0.2) Uncommon - - -
Injection site pain 2 (0.3) Uncommon - - -
Application site erythema 1 (0.2) Uncommon - - -
Application site pruritus 1 (0.2) Uncommon - - -
Application site rash 1 (0.2) Uncommon - - -
Catheter site erythema 1 (0.2) Uncommon - - -
Catheter site haematoma 1 (0.2) Uncommon - - -
Catheter site inflammation 1 (0.2) Uncommon - - -
Catheter site rash 1 (0.2) Uncommon - - -
Catheter site swelling 1 (0.2) Uncommon - - -
Discomfort 1 (0.2) Uncommon - - -
Feeling hot 1 (0.2) Uncommon - - -
Feeling of body temperature change 1 (0.2) Uncommon - - -
Infusion related reaction 1 (0.2) Uncommon - - -
Infusion site irritation 1 (0.2) Uncommon - - -
Infusion site phlebitis 1 (0.2) Uncommon - - -
Infusion site pruritus 1 (0.2) Uncommon - - -
Infusion site rash 1 (0.2) Uncommon - - -
Injection site erythema 1 (0.2) Uncommon - - -
Injection site extravasation 1 (0.2) Uncommon - - -
Injection site pruritus 1 (0.2) Uncommon - - -
Confidential Page 118 of 130

Teplizumab MacroGenics, Inc.
Investigator's Brochure Version 12.0, 16 November 2016
Table 30 Teplizumab Adverse Drug Reactions1 from Completed Trials with Expectedness
System Organ Class
Preferred Term (MedDRA v14.0)2
Adverse Drug Reactions Serious Adverse Drug Reactions
Any
Teplizumaba
(N=645)
n (%)
Frequency Category b
Any
Teplizumaba
(N=645)
n (%)
Frequency Category b Expectedness c
Hepatobiliary disorders
Hyperbilirubinaemia 38 (5.9) Common - - -
Cholestasis 1 (0.2) Uncommon - - -
Immune system disorders
Cytokine release syndrome 37 (5.7) Common 3 (0.5) Uncommon Expected
Hypersensitivity 3 (0.5) Uncommon 1 (0.2) Uncommon -
Food allergy 1 (0.2) Uncommon - - -
Infections and infestations
Upper respiratory tract infection 22 (3.4) Common - - -
Nasopharyngitis 14 (2.2) Common - - -
Epstein-Barr viraemia 9 (1.4) Common - - -
Herpes zoster 7 (1.1) Common - - -
Pharyngitis 6 (0.9) Uncommon - - -
Influenza 4 (0.6) Uncommon - - -
Oral herpes 4 (0.6) Uncommon - - -
Rhinitis 3 (0.5) Uncommon - - -
Sinusitis 4 (0.6) Uncommon - - -
Tinea versicolour 1 (0.2) Uncommon - - -
Bronchitis 2 (0.3) Uncommon - - -
Gastroenteritis viral 2 (0.3) Uncommon - - -
Pharyngitis streptococcal 2 (0.3) Uncommon - - -
Pharyngotonsillitis 2 (0.3) Uncommon 1 (0.2) Uncommon -
Confidential Page 119 of 130

Teplizumab MacroGenics, Inc.
Investigator's Brochure Version 12.0, 16 November 2016
Table 30 Teplizumab Adverse Drug Reactions1 from Completed Trials with Expectedness
System Organ Class
Preferred Term (MedDRA v14.0)2
Adverse Drug Reactions Serious Adverse Drug Reactions
Any
Teplizumaba
(N=645)
n (%)
Frequency Category b
Any
Teplizumaba
(N=645)
n (%)
Frequency Category b Expectedness c
Rotavirus infection 2 (0.3) Uncommon - - -
Acute tonsillitis 1 (0.2) Uncommon - - -
Anal abscess 1 (0.2) Uncommon 1 (0.2) Uncommon -
Anogenital warts 1 (0.2) Uncommon - - -
Bronchiolitis 1 (0.2) Uncommon - - -
Central line infection 1 (0.2) Uncommon - - -
Conjunctivitis infective 1 (0.2) Uncommon - - -
Folliculitis 1 (0.2) Uncommon - - -
Fungal infection 1 (0.2) Uncommon - - -
Fungal skin infection 1 (0.2) Uncommon - - -
Furuncle 1 (0.2) Uncommon - - -
Gastroenteritis 1 (0.2) Uncommon - - -
Helicobacter infection 1 (0.2) Uncommon - - -
Hordeolum 1 (0.2) Uncommon - - -
Impetigo 1 (0.2) Uncommon - - -
Infection 1 (0.2) Uncommon 1 (0.2) Uncommon -
Infectious mononucleosis 1 (0.2) Uncommon - - -
Infusion site infection 1 (0.2) Uncommon - - -
Meningitis viral 1 (0.2) Uncommon - - -
Oral fungal infection 1 (0.2) Uncommon - - -
Otitis media 1 (0.2) Uncommon - - -
Pneumonia bacterial 1 (0.2) Uncommon - - -
Confidential Page 120 of 130

Teplizumab MacroGenics, Inc.
Investigator's Brochure Version 12.0, 16 November 2016
Table 30 Teplizumab Adverse Drug Reactions1 from Completed Trials with Expectedness
System Organ Class
Preferred Term (MedDRA v14.0)2
Adverse Drug Reactions Serious Adverse Drug Reactions
Any
Teplizumaba
(N=645)
n (%)
Frequency Category b
Any
Teplizumaba
(N=645)
n (%)
Frequency Category b Expectedness c
Pulmonary tuberculosis 1 (0.2) Uncommon 1 (0.2) Uncommon -
Rash pustular 1 (0.2) Uncommon - - -
Respiratory tract infection 1 (0.2) Uncommon - - -
Respiratory tract infection viral 1 (0.2) Uncommon - - -
Sialoadenitis 1 (0.2) Uncommon - - -
Staphylococcal sepsis 1 (0.2) Uncommon 1 (0.2) Uncommon -
Urinary tract infection 1 (0.2) Uncommon - - -
Injury, poisoning and procedural complications
Sunburn 1 (0.2) Uncommon - - -
Investigations
White blood cell count decreased 246 (38.1) Very Common - - -
Aspartate aminotransferase increased 175 (27.1) Very Common 2 (0.3) Uncommon Expected
Lymphocyte count decreased 166 (25.7) Very Common - - -
Alanine aminotransferase increased 158 (24.5) Very Common 2 (0.3) Uncommon Expected
Haemoglobin decreased 131 (20.3) Very Common - - -
Neutrophil count decreased 126 (19.5) Very Common - - -
Blood bicarbonate decreased 98 (15.2) Very Common - - -
Platelet count decreased 84 (13.0) Very Common - - -
Blood alkaline phosphatase increased 44 (6.8) Common - - -
Blood sodium decreased 42 (6.5) Common - - -
Blood calcium decreased 35 (5.4) Common - - -
Confidential Page 121 of 130

Teplizumab MacroGenics, Inc.
Investigator's Brochure Version 12.0, 16 November 2016
Table 30 Teplizumab Adverse Drug Reactions1 from Completed Trials with Expectedness
System Organ Class
Preferred Term (MedDRA v14.0)2
Adverse Drug Reactions Serious Adverse Drug Reactions
Any
Teplizumaba
(N=645)
n (%)
Frequency Category b
Any
Teplizumaba
(N=645)
n (%)
Frequency Category b Expectedness c
Blood bilirubin increased 34 (5.3) Common - - -
Gamma-glutamyltransferase increased 26 (4.0) Common - - -
Bilirubin conjugated increased 26 (4.0) Common - - -
Red blood cell count decreased 21 (3.3) Common - - -
Blood albumin decreased 24 (3.7) Common - - -
Haematocrit decreased 18 (2.8) Common - - -
Eosinophil count increased 15 (2.3) Common - - -
Blood potassium increased 15 (2.3) Common - - -
Blood pressure decreased 12 (1.9) Common - - -
Epstein-Barr virus antibody positive 11 (1.7) Common - - -
Blood phosphorus decreased 9 (1.4) Common - - -
Blood chloride decreased 9 (1.4) Common - - -
Blood calcium increased 7 (1.1) Common - - -
Blood chloride increased 8 (1.2) Common - - -
Blood phosphorus increased 8 (1.2) Common - - -
Blood potassium decreased 8 (1.2) Common - - -
Blood pressure increased 8 (1.2) Common - - -
Eosinophil count decreased 7 (1.1) Common - - -
Monocyte count decreased 8 (1.2) Common - - -
Blood albumin increased 7 (1.1) Common - - -
Blood urea increased 5 (0.8) Uncommon - - -
Heart rate increased 5 (0.8) Uncommon - - -
Confidential Page 122 of 130

Teplizumab MacroGenics, Inc.
Investigator's Brochure Version 12.0, 16 November 2016
Table 30 Teplizumab Adverse Drug Reactions1 from Completed Trials with Expectedness
System Organ Class
Preferred Term (MedDRA v14.0)2
Adverse Drug Reactions Serious Adverse Drug Reactions
Any
Teplizumaba
(N=645)
n (%)
Frequency Category b
Any
Teplizumaba
(N=645)
n (%)
Frequency Category b Expectedness c
Body temperature increased 4 (0.6) Uncommon - - -
Neutrophil count increased 4 (0.6) Uncommon - - -
Blood bicarbonate increased 2 (0.3) Uncommon - - -
Monocyte count increased 4 (0.6) Uncommon - - -
White blood cell count increased 4 (0.6) Uncommon - - -
Blood creatinine decreased 3 (0.5) Uncommon - - -
Blood creatinine increased 3 (0.5) Uncommon - - -
Carbon dioxide decreased 3 (0.5) Uncommon - - -
Cytomegalovirus antibody positive 3 (0.5) Uncommon - - -
Mean cell haemoglobin concentration increased
3 (0.5) Uncommon - - -
Red blood cell count increased 1 (0.2) Uncommon - - -
Weight decreased 2 (0.3) Uncommon - - -
Alanine aminotransferase decreased 1 (0.2) Uncommon - - -
Blood alkaline phosphatase decreased 1 (0.2) Uncommon - - -
Blood pressure diastolic decreased 1 (0.2) Uncommon - - -
Blood sodium increased 2 (0.3) Uncommon - - -
Eosinophil percentage increased 2 (0.3) Uncommon - - -
Epstein-Barr virus test positive 2 (0.3) Uncommon - - -
Haemoglobin increased 2 (0.3) Uncommon - - -
Lymphocyte count increased 2 (0.3) Uncommon - - -
Mean cell haemoglobin decreased 2 (0.3) Uncommon - - -
Confidential Page 123 of 130

Teplizumab MacroGenics, Inc.
Investigator's Brochure Version 12.0, 16 November 2016
Table 30 Teplizumab Adverse Drug Reactions1 from Completed Trials with Expectedness
System Organ Class
Preferred Term (MedDRA v14.0)2
Adverse Drug Reactions Serious Adverse Drug Reactions
Any
Teplizumaba
(N=645)
n (%)
Frequency Category b
Any
Teplizumaba
(N=645)
n (%)
Frequency Category b Expectedness c
Mean cell volume decreased 2 (0.3) Uncommon - - -
Basophil count increased 1 (0.2) Uncommon - - -
Blood creatine increased 1 (0.2) Uncommon - - -
Blood glucose decreased 1 (0.2) Uncommon - - -
Blood magnesium decreased 1 (0.2) Uncommon - - -
Blood pH decreased 1 (0.2) Uncommon - - -
Blood urea decreased 1 (0.2) Uncommon - - -
Body temperature fluctuation 1 (0.2) Uncommon - - -
Calcium ionised decreased 1 (0.2) Uncommon - - -
Cytomegalovirus test positive 1 (0.2) Uncommon - - -
Eosinophil morphology abnormal 1 (0.2) Uncommon - - -
Haematocrit increased 1 (0.2) Uncommon - - -
Heart rate decreased 1 (0.2) Uncommon - - -
Heart rate irregular 1 (0.2) Uncommon - - -
Lymphocyte percentage decreased 1 (0.2) Uncommon - - -
Lymphocyte percentage increased 1 (0.2) Uncommon - - -
Mean cell haemoglobin concentration decreased
1 (0.2) Uncommon - - -
Mean cell volume increased 1 (0.2) Uncommon - - -
Mean platelet volume increased 1 (0.2) Uncommon - - -
Monocyte morphology abnormal 1 (0.2) Uncommon - - -
Neutrophil percentage decreased 1 (0.2) Uncommon - - -
Confidential Page 124 of 130

Teplizumab MacroGenics, Inc.
Investigator's Brochure Version 12.0, 16 November 2016
Table 30 Teplizumab Adverse Drug Reactions1 from Completed Trials with Expectedness
System Organ Class
Preferred Term (MedDRA v14.0)2
Adverse Drug Reactions Serious Adverse Drug Reactions
Any
Teplizumaba
(N=645)
n (%)
Frequency Category b
Any
Teplizumaba
(N=645)
n (%)
Frequency Category b Expectedness c
Neutrophil percentage increased 1 (0.2) Uncommon - - -
Platelet count increased 1 (0.2) Uncommon - - -
Protein urine present 1 (0.2) Uncommon - - -
Metabolism and nutrition disorders
Hyponatraemia 72 (11.2) Very Common - - -
Hypocalcaemia 68 (10.5) Very Common - - -
Hyperkalaemia 34 (5.3) Common - - -
Hypoalbuminaemia 28 (4.3) Common - - -
Hypoglycaemia 17 (2.6) Common - - -
Hypokalaemia 16 (2.5) Common - - -
Hypophosphataemia 16 (2.5) Common - - -
Hypercalcaemia 8 (1.2) Common - - -
Hypernatraemia 7 (1.1) Common - - -
Anorexia 7 (1.1) Common - - -
Dehydration 8 (1.2) Common - - -
Decreased appetite 4 (0.6) Uncommon - - -
Hyperchloraemia 2 (0.3) Uncommon - - -
Hypoglycaemic seizure 3 (0.5) Uncommon 3 (0.5) Uncommon -
Hyperphosphataemia 1 (0.2) Uncommon - - -
Hypoglycaemic unconsciousness 1 (0.2) Uncommon 1 (0.2) Uncommon -
Hypochloraemia 1 (0.2) Uncommon - - -
Vitamin B12 deficiency 1 (0.2) Uncommon - - -
Confidential Page 125 of 130

Teplizumab MacroGenics, Inc.
Investigator's Brochure Version 12.0, 16 November 2016
Table 30 Teplizumab Adverse Drug Reactions1 from Completed Trials with Expectedness
System Organ Class
Preferred Term (MedDRA v14.0)2
Adverse Drug Reactions Serious Adverse Drug Reactions
Any
Teplizumaba
(N=645)
n (%)
Frequency Category b
Any
Teplizumaba
(N=645)
n (%)
Frequency Category b Expectedness c
Musculoskeletal and connective tissue disorders
Myalgia 17 (2.6) Common - - -
Arthralgia 9 (1.4) Common - - -
Pain in extremity 6 (0.9) Uncommon - - -
Neck pain 3 (0.5) Uncommon - - -
Muscle spasms 2 (0.3) Uncommon - - -
Arthritis 1 (0.2) Uncommon - - -
Back pain 1 (0.2) Uncommon - - -
Joint swelling 1 (0.2) Uncommon - - -
Muscular weakness 1 (0.2) Uncommon - - -
Musculoskeletal pain 1 (0.2) Uncommon - - -
Pain in jaw 1 (0.2) Uncommon - - -
Nervous system disorders
Headache 99 (15.3) Very Common - - -
Dizziness 14 (2.2) Common - - -
Paraesthesia 4 (0.6) Uncommon - - -
Tremor 4 (0.6) Uncommon - - -
Burning sensation 2 (0.3) Uncommon - - -
Somnolence 2 (0.3) Uncommon - - -
Syncope 2 (0.3) Uncommon - - -
Hypoaesthesia 1 (0.2) Uncommon - - -
Confidential Page 126 of 130

Teplizumab MacroGenics, Inc.
Investigator's Brochure Version 12.0, 16 November 2016
Table 30 Teplizumab Adverse Drug Reactions1 from Completed Trials with Expectedness
System Organ Class
Preferred Term (MedDRA v14.0)2
Adverse Drug Reactions Serious Adverse Drug Reactions
Any
Teplizumaba
(N=645)
n (%)
Frequency Category b
Any
Teplizumaba
(N=645)
n (%)
Frequency Category b Expectedness c
Lethargy 1 (0.2) Uncommon - - -
Migraine with aura 1 (0.2) Uncommon - - -
Psychiatric disorders
Anxiety 2 (0.3) Uncommon - - -
Bruxism 1 (0.2) Uncommon - - -
Confusional state 1 (0.2) Uncommon - - -
Depression 1 (0.2) Uncommon - - -
Renal and urinary disorders
Proteinuria 11 (1.7) Common - - -
Haematuria 2 (0.3) Uncommon - - -
Microalbuminuria 1 (0.2) Uncommon - - -
Dysuria 1 (0.2) Uncommon - - -
Urine odour abnormal 1 (0.2) Uncommon - - -
Reproductive system and breast disorders
Epididymitis 2 (0.3) Uncommon 1 (0.2) Uncommon -
Gynaecomastia 1 (0.2) Uncommon - - -
Respiratory, thoracic and mediastinal disorders
Oropharyngeal pain 14 (2.2) Common - - -
Cough 7 (1.1) Common - - -
Nasal congestion 4 (0.6) Uncommon - - -
Confidential Page 127 of 130

Teplizumab MacroGenics, Inc.
Investigator's Brochure Version 12.0, 16 November 2016
Table 30 Teplizumab Adverse Drug Reactions1 from Completed Trials with Expectedness
System Organ Class
Preferred Term (MedDRA v14.0)2
Adverse Drug Reactions Serious Adverse Drug Reactions
Any
Teplizumaba
(N=645)
n (%)
Frequency Category b
Any
Teplizumaba
(N=645)
n (%)
Frequency Category b Expectedness c
Dyspnoea 2 (0.3) Uncommon - - -
Rhinitis allergic 2 (0.3) Uncommon - - -
Rhinorrhoea 2 (0.3) Uncommon - - -
Epistaxis 1 (0.2) Uncommon - - -
Pleuritic pain 1 (0.2) Uncommon - - -
Tachypnoea 1 (0.2) Uncommon - - -
Throat tightness 1 (0.2) Uncommon - - -
Skin and subcutaneous tissue disorders
Rash 165 (25.6) Very Common 1 (0.2) Uncommon -
Pruritus 75 (11.6) Very Common - - -
Rash macular 33 (5.1) Common - - -
Rash papular 30 (4.7) Common - - -
Rash maculo-papular 22 (3.4) Common - - -
Rash pruritic 14 (2.2) Common - - -
Skin exfoliation 13 (2.0) Common - - -
Urticaria 11 (1.7) Common - - -
Rash erythematous 8 (1.2) Common - - -
Dry skin 8 (1.2) Common - - -
Erythema 6 (0.9) Uncommon - - -
Alopecia 4 (0.6) Uncommon - - -
Dermatitis allergic 4 (0.6) Uncommon - - -
Pruritus generalised 2 (0.3) Uncommon - - -
Confidential Page 128 of 130

Teplizumab MacroGenics, Inc.
Investigator's Brochure Version 12.0, 16 November 2016
Table 30 Teplizumab Adverse Drug Reactions1 from Completed Trials with Expectedness
System Organ Class
Preferred Term (MedDRA v14.0)2
Adverse Drug Reactions Serious Adverse Drug Reactions
Any
Teplizumaba
(N=645)
n (%)
Frequency Category b
Any
Teplizumaba
(N=645)
n (%)
Frequency Category b Expectedness c
Rash generalised 4 (0.6) Uncommon - - -
Dermatitis 3 (0.5) Uncommon - - -
Exfoliative rash 3 (0.5) Uncommon - - -
Hyperhidrosis 3 (0.5) Uncommon - - -
Purpura 3 (0.5) Uncommon - - -
Acne 2 (0.3) Uncommon - - -
Dyshidrosis 2 (0.3) Uncommon - - -
Skin reaction 2 (0.3) Uncommon - - -
Dermatitis atopic 1 (0.2) Uncommon - - -
Dermatitis contact 1 (0.2) Uncommon - - -
Dermatitis exfoliative 1 (0.2) Uncommon - - -
Drug eruption 1 (0.2) Uncommon - - -
Eczema weeping 1 (0.2) Uncommon - - -
Periorbital oedema 1 (0.2) Uncommon - - -
Pityriasis alba 1 (0.2) Uncommon - - -
Psoriasis 1 (0.2) Uncommon - - -
Rash scarlatiniform 1 (0.2) Uncommon - - -
Rash vesicular 1 (0.2) Uncommon - - -
Skin lesion 1 (0.2) Uncommon - - -
Swelling face 1 (0.2) Uncommon - - -
Urticaria chronic 1 (0.2) Uncommon - - -
Confidential Page 129 of 130

Teplizumab MacroGenics, Inc.
Investigator's Brochure Version 12.0, 16 November 2016
Table 30 Teplizumab Adverse Drug Reactions1 from Completed Trials with Expectedness
System Organ Class
Preferred Term (MedDRA v14.0)2
Adverse Drug Reactions Serious Adverse Drug Reactions
Any
Teplizumaba
(N=645)
n (%)
Frequency Category b
Any
Teplizumaba
(N=645)
n (%)
Frequency Category b Expectedness c
Vascular disorders
Flushing 9 (1.4) Common - - -
Hot flush 3 (0.5) Uncommon - - -
Phlebitis 1 (0.2) Uncommon - - -
Vascular rupture 1 (0.2) Uncommon - - -
1 Includes events with causality ratings of 'Possible', 'Probable' or 'Definite'. 2 Bolded and italicized preferred terms denote those events with a history of at least 1 serious adverse drug reaction. a Includes subjects from studies CP-MGA031-01-DB, CP-MGA031-01-OL, CP-MGA031-02-DB, CP-MGA031-02-OL, and CP-MGA031-03 who are
known to have received an IV dose of Teplizumab. Includes all events prior to 24Aug2012. Subjects in both studies CP-MGA031-01 and CP-MGA031-02 are only counted once in the denominators
b Definition of Frequency Category: Very Common: >= 10%, Common: = 1% and < 10%, Uncommon: = 0.1% and < 1%, Rare: = 0.01% and < 0.1% , Very Rare: < 0.01%.
c Denotes “regulatory expectedness” utilized by the sponsor to determine if ICSRs are expeditable to regulatory agencies. A “-” in this column signifies a designation as “unexpected.”
Confidential Page 130 of 130