INTRODUCTION · class i antiarrhythmics: fast sodium channel blockers Class I agents block fast...
36
9/12/2019 1/36 Tintinalli’s Emergency Medicine: A Comprehensive Study Guide, 8e Chapter 19: Pharmacology of Antiarrhythmics and Antihypertensives Sara H. Shields; Rachel M. Holland; R. Dustin Pippin; Benjamin Small INTRODUCTION This chapter reviews the pharmacology of selected antiarrhythmics and antihypertensives (β-blockers and calcium channel blockers) used in the ED. Discussion of additional antihypertensives can be found in chapter 57, "Systemic Hypertension." Antiarrhythmic medications treat cardiac rhythm abnormalities by modifying autonomic function or myocardial ion channels, leading to changes in conduction velocity or duration of the eective refractory period. 1 Failure to reduce mortality has been a criticism of many agents in this class of drugs. 2,3,4,5 In general, electrical cardioversion is preferable to pharmacologic conversion in patients who are hemodynamically unstable. The majority of antiarrhythmics are organized based on the Vaughan-Williams classification system (Classes I to IV) ( Table 19-1). Other medications used to treat arrhythmias include digoxin, atropine, adenosine, magnesium, and isoproterenol.
Transcript of INTRODUCTION · class i antiarrhythmics: fast sodium channel blockers Class I agents block fast...
9/12/2019
1/36
Tintinalli’s Emergency Medicine: A Comprehensive Study Guide, 8e
Chapter 19: Pharmacology of Antiarrhythmics and Antihypertensives Sara H. Shields; Rachel M. Holland; R. Dustin Pippin; Benjamin Small
INTRODUCTION
This chapter reviews the pharmacology of selected antiarrhythmics and antihypertensives (β-blockers andcalcium channel blockers) used in the ED. Discussion of additional antihypertensives can be found in chapter57, "Systemic Hypertension."
Antiarrhythmic medications treat cardiac rhythm abnormalities by modifying autonomic function ormyocardial ion channels, leading to changes in conduction velocity or duration of the e�ective refractory
period.1 Failure to reduce mortality has been a criticism of many agents in this class of drugs.2,3,4,5 Ingeneral, electrical cardioversion is preferable to pharmacologic conversion in patients who arehemodynamically unstable. The majority of antiarrhythmics are organized based on the Vaughan-Williamsclassification system (Classes I to IV) (Table 19-1). Other medications used to treat arrhythmias includedigoxin, atropine, adenosine, magnesium, and isoproterenol.
9/12/2019
2/36
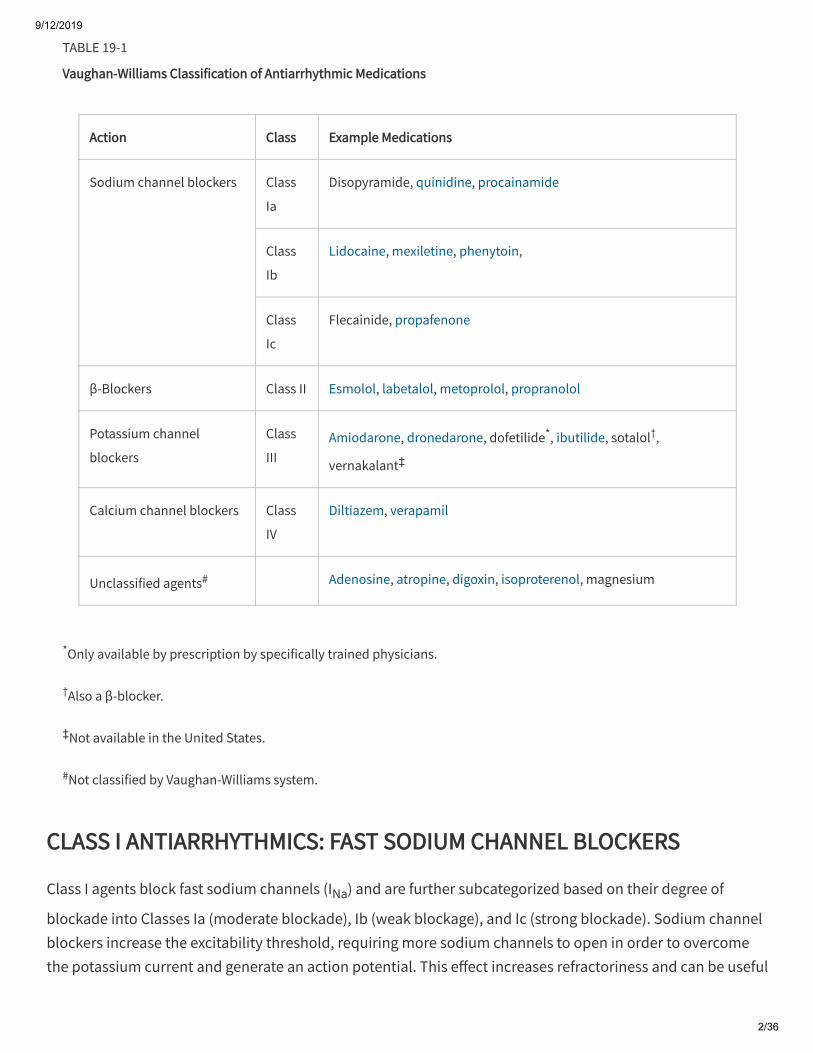
*Only available by prescription by specifically trained physicians.
†Also a β-blocker.
‡Not available in the United States.
#Not classified by Vaughan-Williams system.
TABLE 19-1
Vaughan-Williams Classification of Antiarrhythmic Medications
Action Class Example Medications
Sodium channel blockers Class
Ia
Disopyramide, quinidine, procainamide
Class
Ib
Lidocaine, mexiletine, phenytoin,
Class
Ic
Flecainide, propafenone
β-Blockers Class II Esmolol, labetalol, metoprolol, propranolol
Potassium channel
blockers
Class
IIIAmiodarone, dronedarone, dofetilide*, ibutilide, sotalol†,
vernakalant‡
Calcium channel blockers Class
IV
Diltiazem, verapamil
Unclassified agents# Adenosine, atropine, digoxin, isoproterenol, magnesium
CLASS I ANTIARRHYTHMICS: FAST SODIUM CHANNEL BLOCKERS
Class I agents block fast sodium channels (INa) and are further subcategorized based on their degree of
blockade into Classes Ia (moderate blockade), Ib (weak blockage), and Ic (strong blockade). Sodium channelblockers increase the excitability threshold, requiring more sodium channels to open in order to overcomethe potassium current and generate an action potential. This e�ect increases refractoriness and can be useful
9/12/2019
3/36
in terminating reentry currents. In addition, some Class I agents block potassium channels (IK) and exhibit
antimuscarinic e�ects.
CLASS Ia AGENTS
Class Ia antiarrhythmics block open sodium channels and have a slow dissociation from their target, causingan increase in the refractory period. The use of these agents is limited by their side e�ect profile andproarrhythmic nature. Quinidine and disopyramide are Class Ia agents but are not discussed here becausethey are infrequently used in the ED. Quinidine can cause torsades de pointes. Disopyramide is used orally inpatients with hypertrophic cardiomyopathy due to its negative inotropic properties; however, its associationwith heart failure and hypotension and its anticholinergic e�ects, including urinary retention, limit its use.
PROCAINAMIDE
Actions
Procainamide is a Class Ia agent that increases the refractory period, decreases automaticity andconduction, and prolongs cardiac action potentials through intermediate blockade of open sodium andpotassium channels. NAPA, the active metabolite of procainamide, lacks sodium channel e�ects but doesblock potassium channels, which can lead to QT prolongation.
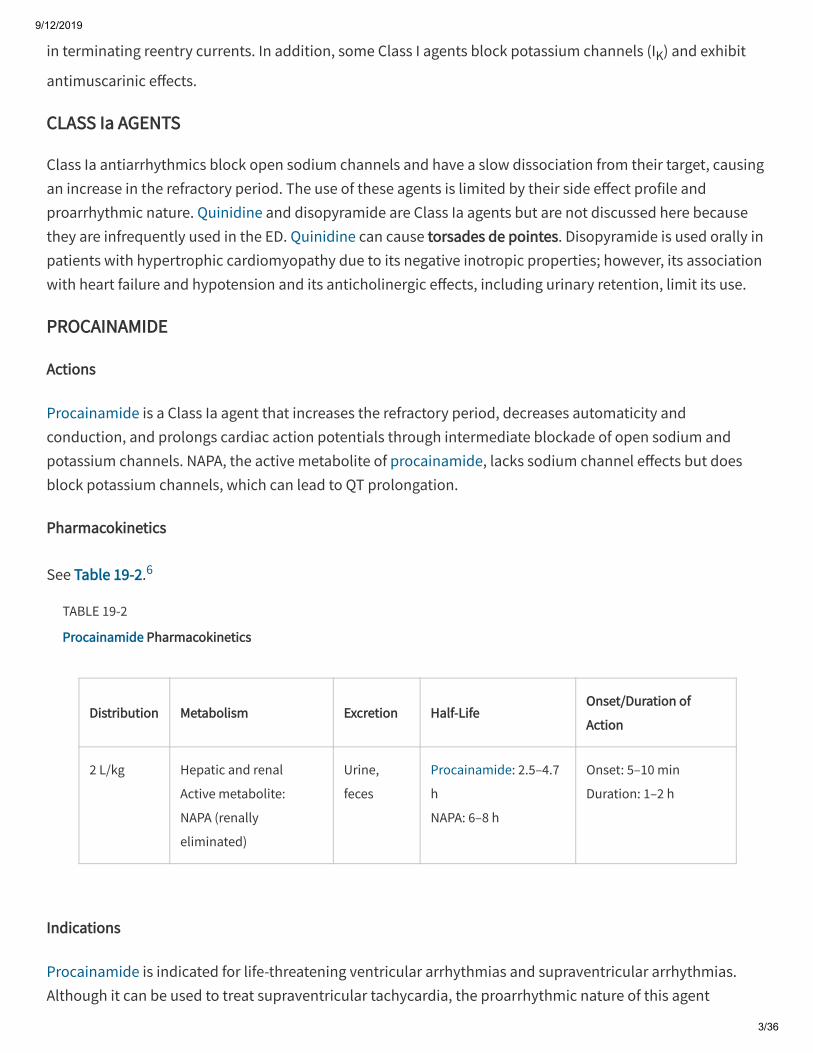
Pharmacokinetics
See Table 19-2.6
TABLE 19-2
Procainamide Pharmacokinetics
Distribution Metabolism Excretion Half-LifeOnset/Duration of
Action
2 L/kg Hepatic and renal
Active metabolite:
NAPA (renally
eliminated)
Urine,
feces
Procainamide: 2.5–4.7
h
NAPA: 6–8 h
Onset: 5–10 min
Duration: 1–2 h
Indications
Procainamide is indicated for life-threatening ventricular arrhythmias and supraventricular arrhythmias.Although it can be used to treat supraventricular tachycardia, the proarrhythmic nature of this agent
9/12/2019
4/36
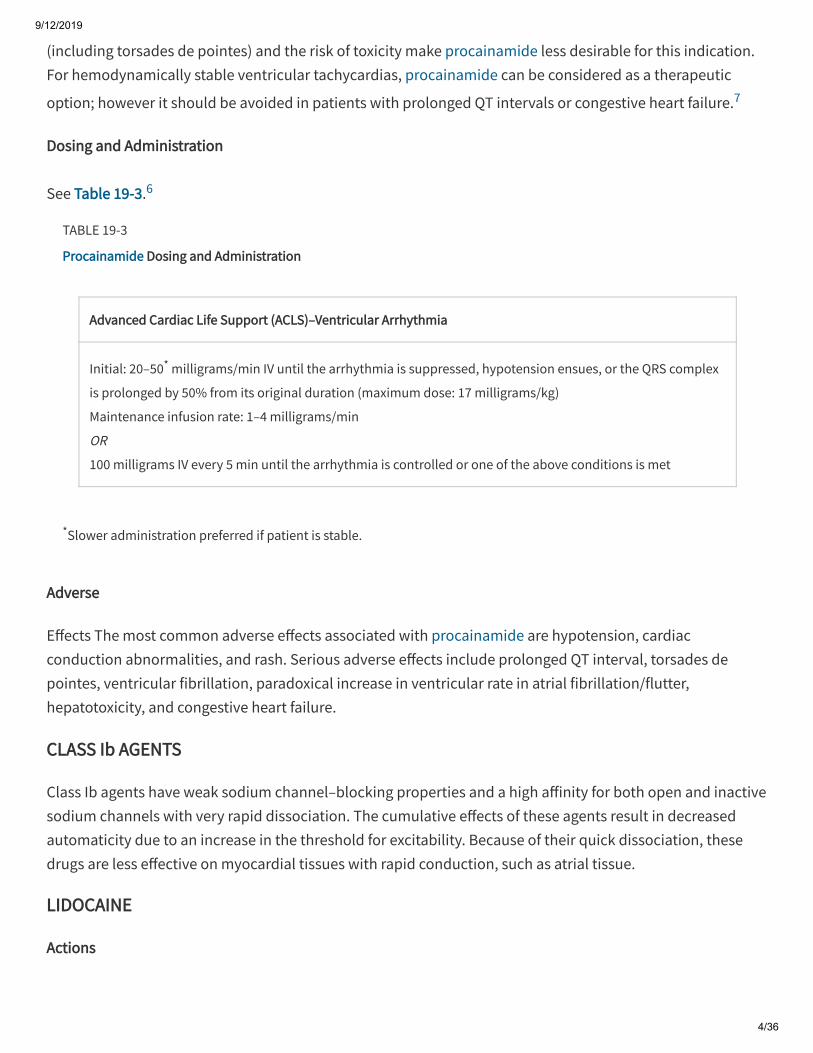
*Slower administration preferred if patient is stable.
(including torsades de pointes) and the risk of toxicity make procainamide less desirable for this indication.For hemodynamically stable ventricular tachycardias, procainamide can be considered as a therapeutic
option; however it should be avoided in patients with prolonged QT intervals or congestive heart failure.7
Dosing and Administration
See Table 19-3.6
TABLE 19-3
Procainamide Dosing and Administration
Advanced Cardiac Life Support (ACLS)–Ventricular Arrhythmia
Initial: 20–50* milligrams/min IV until the arrhythmia is suppressed, hypotension ensues, or the QRS complex
is prolonged by 50% from its original duration (maximum dose: 17 milligrams/kg)
Maintenance infusion rate: 1–4 milligrams/min
OR
100 milligrams IV every 5 min until the arrhythmia is controlled or one of the above conditions is met
Adverse
E�ects The most common adverse e�ects associated with procainamide are hypotension, cardiacconduction abnormalities, and rash. Serious adverse e�ects include prolonged QT interval, torsades depointes, ventricular fibrillation, paradoxical increase in ventricular rate in atrial fibrillation/flutter,hepatotoxicity, and congestive heart failure.
CLASS Ib AGENTS
Class Ib agents have weak sodium channel–blocking properties and a high a�inity for both open and inactivesodium channels with very rapid dissociation. The cumulative e�ects of these agents result in decreasedautomaticity due to an increase in the threshold for excitability. Because of their quick dissociation, thesedrugs are less e�ective on myocardial tissues with rapid conduction, such as atrial tissue.
LIDOCAINE
Actions
9/12/2019
5/36
Lidocaine is a Class Ib agent with weak sodium channel blocker properties that preferentially acts onischemic myocardial tissue to decrease conduction; in addition, it has local anesthetic properties. E�ectsexerted on the cardiac action potential are negligible, with very minimal decrease to no e�ect on the QTinterval and the refractory period.
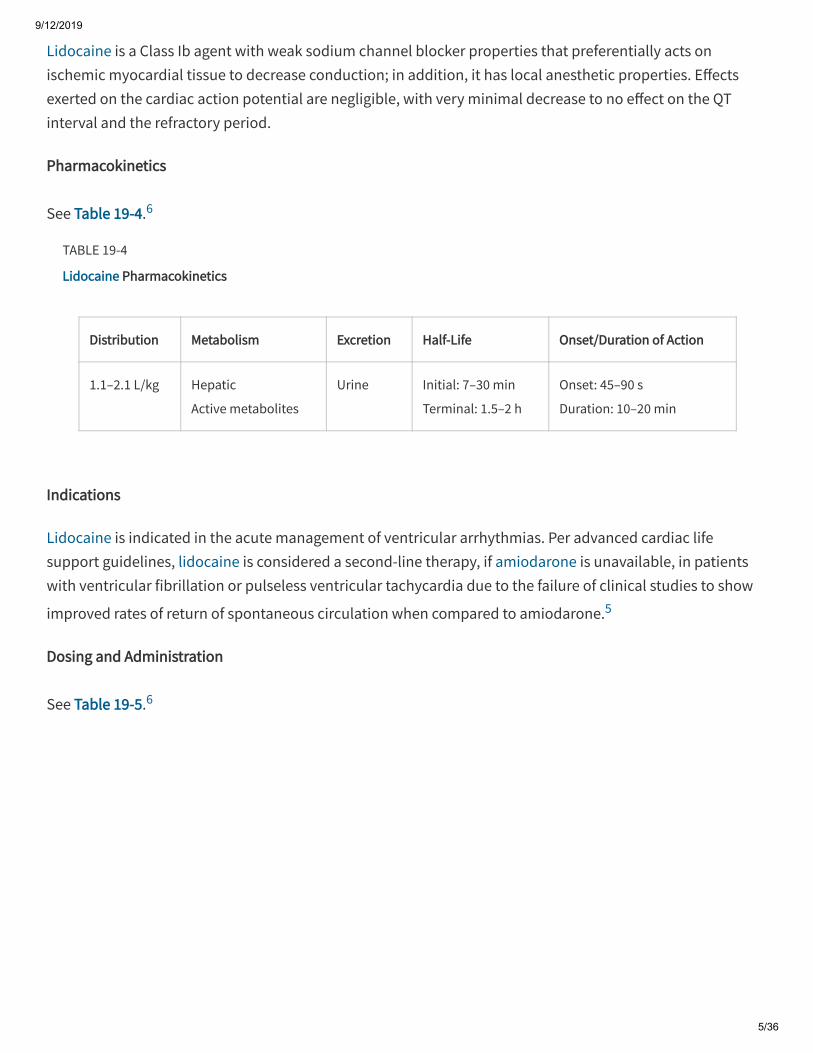
Pharmacokinetics
See Table 19-4.6
TABLE 19-4
Lidocaine Pharmacokinetics
Distribution Metabolism Excretion Half-Life Onset/Duration of Action
1.1–2.1 L/kg Hepatic
Active metabolites
Urine Initial: 7–30 min
Terminal: 1.5–2 h
Onset: 45–90 s
Duration: 10–20 min
Indications
Lidocaine is indicated in the acute management of ventricular arrhythmias. Per advanced cardiac lifesupport guidelines, lidocaine is considered a second-line therapy, if amiodarone is unavailable, in patientswith ventricular fibrillation or pulseless ventricular tachycardia due to the failure of clinical studies to show
improved rates of return of spontaneous circulation when compared to amiodarone.5
Dosing and Administration
See Table 19-5.6
9/12/2019
6/36
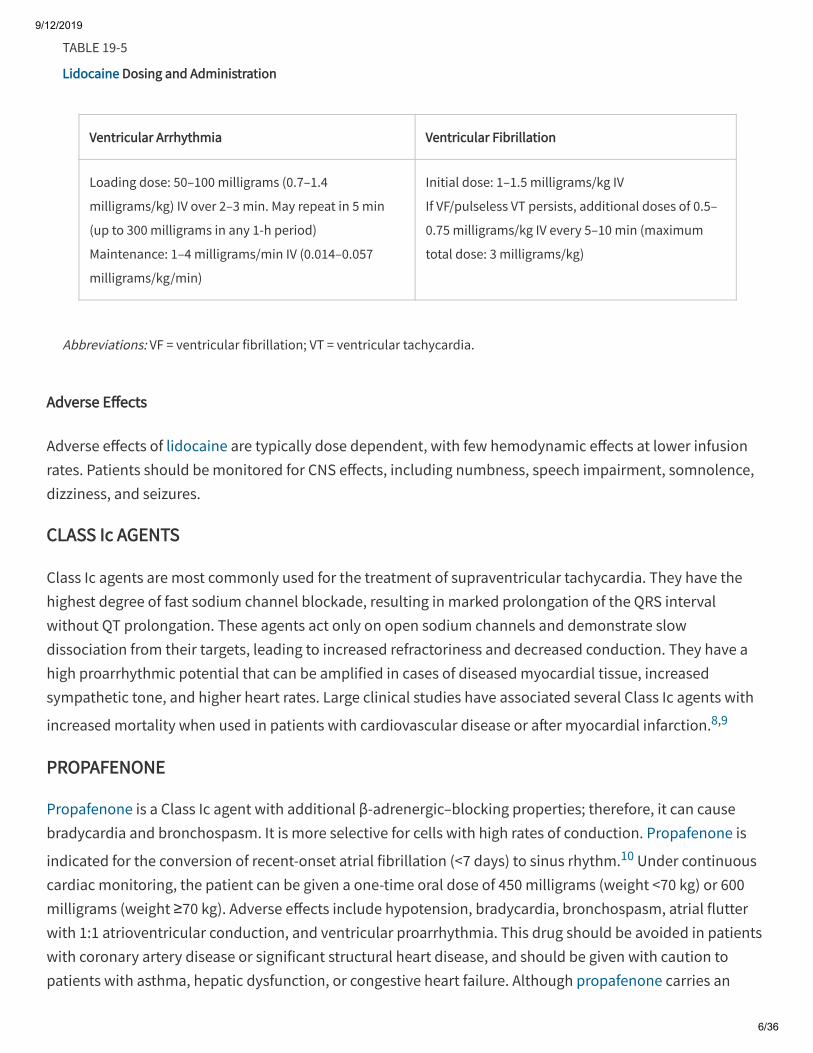
Abbreviations: VF = ventricular fibrillation; VT = ventricular tachycardia.
TABLE 19-5
Lidocaine Dosing and Administration
Ventricular Arrhythmia Ventricular Fibrillation
Loading dose: 50–100 milligrams (0.7–1.4
milligrams/kg) IV over 2–3 min. May repeat in 5 min
(up to 300 milligrams in any 1-h period)
Maintenance: 1–4 milligrams/min IV (0.014–0.057
milligrams/kg/min)
Initial dose: 1–1.5 milligrams/kg IV
If VF/pulseless VT persists, additional doses of 0.5–
0.75 milligrams/kg IV every 5–10 min (maximum
total dose: 3 milligrams/kg)
Adverse E�ects
Adverse e�ects of lidocaine are typically dose dependent, with few hemodynamic e�ects at lower infusionrates. Patients should be monitored for CNS e�ects, including numbness, speech impairment, somnolence,dizziness, and seizures.
CLASS Ic AGENTS
Class Ic agents are most commonly used for the treatment of supraventricular tachycardia. They have thehighest degree of fast sodium channel blockade, resulting in marked prolongation of the QRS intervalwithout QT prolongation. These agents act only on open sodium channels and demonstrate slowdissociation from their targets, leading to increased refractoriness and decreased conduction. They have ahigh proarrhythmic potential that can be amplified in cases of diseased myocardial tissue, increasedsympathetic tone, and higher heart rates. Large clinical studies have associated several Class Ic agents with
increased mortality when used in patients with cardiovascular disease or a�er myocardial infarction.8,9
PROPAFENONE
Propafenone is a Class Ic agent with additional β-adrenergic–blocking properties; therefore, it can causebradycardia and bronchospasm. It is more selective for cells with high rates of conduction. Propafenone is
indicated for the conversion of recent-onset atrial fibrillation (<7 days) to sinus rhythm.10 Under continuouscardiac monitoring, the patient can be given a one-time oral dose of 450 milligrams (weight <70 kg) or 600milligrams (weight ≥70 kg). Adverse e�ects include hypotension, bradycardia, bronchospasm, atrial flutterwith 1:1 atrioventricular conduction, and ventricular proarrhythmia. This drug should be avoided in patientswith coronary artery disease or significant structural heart disease, and should be given with caution topatients with asthma, hepatic dysfunction, or congestive heart failure. Although propafenone carries an
9/12/2019
7/36
indication for paroxysmal supraventricular tachycardia and ventricular tachycardia, it is rarely used for theseindications in the ED.
FLECAINIDE
Flecainide is a Class 1c agent that reduces excitability, primarily in the His-Purkinje system and ventricularmyocardium. Flecainide is indicated for the conversion of recent-onset atrial fibrillation (<7 days) to sinus
rhythm.10 Under continuous cardiac monitoring, the patient can be given a one-time oral dose of 200milligrams (weight <70 kg) or 300 milligrams (weight ≥70 kg). Adverse e�ects include hypotension, atrialflutter with 1:1 atrioventricular conduction, and ventricular pro-arrhythmia. This drug should be avoided inpatients with coronary artery disease, significant structural heart disease, congestive heart failure, orhypokalemia. Although flecainide carries an indication for paroxysmal supraventricular tachycardia andventricular tachycardia, it is rarely used for these indications in the ED.
CLASS II ANTIARRHYTHMICS: β-BLOCKERS
β-Blockers are used for the treatment of various indications including hypertension, supraventriculartachycardia and ventricular arrhythmias, recurrent atrial fibrillation (rate control), and thyrotoxicosis(symptom control). Although these medications share the principal characteristic of blocking catecholaminee�ects on β-receptors, individual agents di�er with respect to their cardioselectivity, α-adrenergic blockingactivity, intrinsic sympathomimetic activity, membrane-stabilizing e�ect, and pharmacokinetic properties(Table 19-6). β-Receptors are divided into two subtypes. β1-Receptors are found in heart muscle, and β2-
receptors are found in bronchial and vascular smooth muscle. Nonselective β-blocking medications target allβ-receptors, thereby a�ecting heart rate, conduction, and contractility, as well as smooth musclecontraction, thus increasing the risk of bronchospasm. In contrast, cardioselective agents have relativeselectivity for β1-receptors and decrease heart rate and blood pressure. These agents may be a better option
for patients with a history of asthma, chronic obstructive pulmonary disease, or insulin-dependent diabetesbecause they are less likely to act on β2-receptors. Because cardioselectivity is dose-dependent, it decreases
or is lost at higher doses. This is variable between agents, and the dose at which this occurs has not beenclearly established.
9/12/2019
8/36
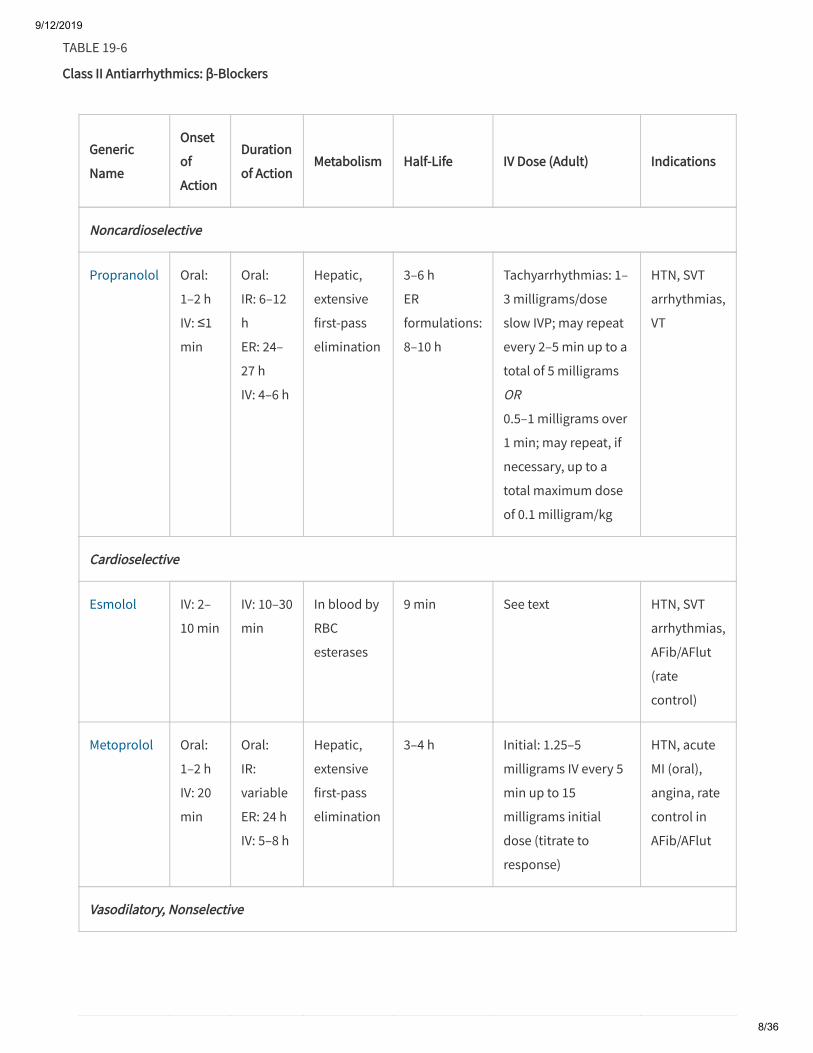
TABLE 19-6
Class II Antiarrhythmics: β-Blockers
Generic
Name
Onset
of
Action
Duration
of ActionMetabolism Half-Life IV Dose (Adult) Indications
Noncardioselective
Propranolol Oral:
1–2 h
IV: ≤1
min
Oral:
IR: 6–12
h
ER: 24–
27 h
IV: 4–6 h
Hepatic,
extensive
first-pass
elimination
3–6 h
ER
formulations:
8–10 h
Tachyarrhythmias: 1–
3 milligrams/dose
slow IVP; may repeat
every 2–5 min up to a
total of 5 milligrams
OR
0.5–1 milligrams over
1 min; may repeat, if
necessary, up to a
total maximum dose
of 0.1 milligram/kg
HTN, SVT
arrhythmias,
VT
Cardioselective
Esmolol IV: 2–
10 min
IV: 10–30
min
In blood by
RBC
esterases
9 min See text HTN, SVT
arrhythmias,
AFib/AFlut
(rate
control)
Metoprolol Oral:
1–2 h
IV: 20
min
Oral:
IR:
variable
ER: 24 h
IV: 5–8 h
Hepatic,
extensive
first-pass
elimination
3–4 h Initial: 1.25–5
milligrams IV every 5
min up to 15
milligrams initial
dose (titrate to
response)
HTN, acute
MI (oral),
angina, rate
control in
AFib/AFlut
Vasodilatory, Nonselective
9/12/2019
9/36
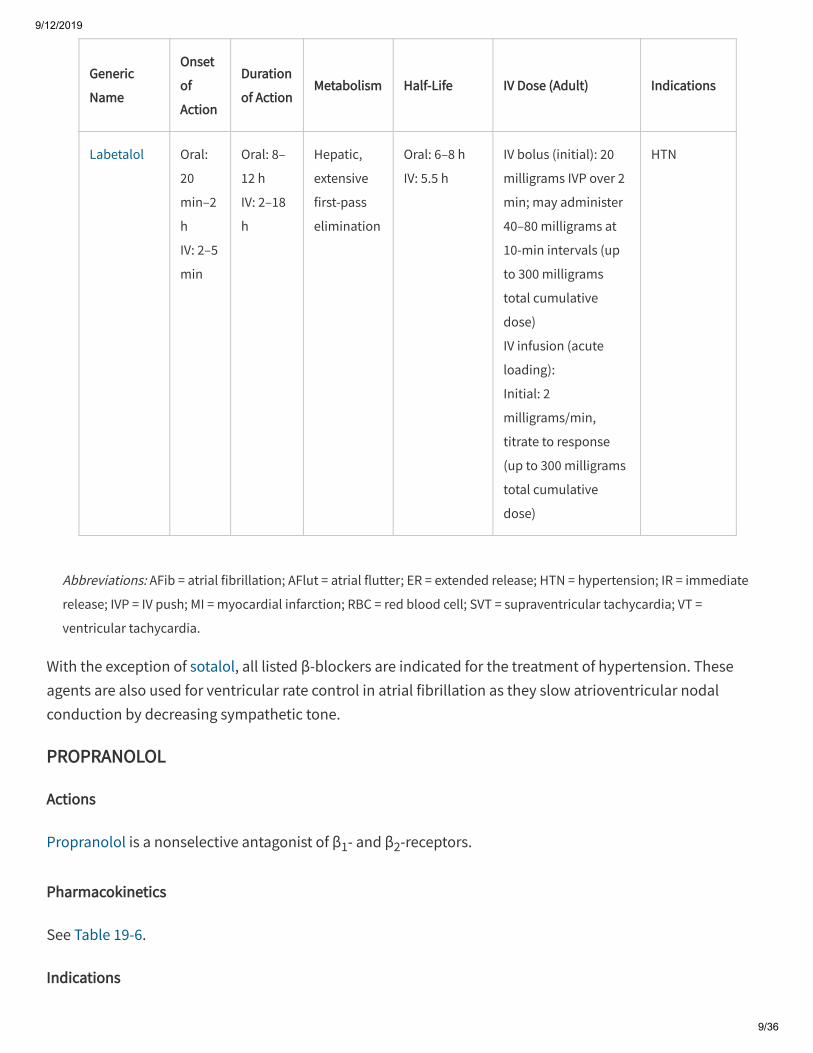
Abbreviations: AFib = atrial fibrillation; AFlut = atrial flutter; ER = extended release; HTN = hypertension; IR = immediate
release; IVP = IV push; MI = myocardial infarction; RBC = red blood cell; SVT = supraventricular tachycardia; VT =
ventricular tachycardia.
Generic
Name
Onset
of
Action
Duration
of ActionMetabolism Half-Life IV Dose (Adult) Indications
Labetalol Oral:
20
min–2
h
IV: 2–5
min
Oral: 8–
12 h
IV: 2–18
h
Hepatic,
extensive
first-pass
elimination
Oral: 6–8 h
IV: 5.5 h
IV bolus (initial): 20
milligrams IVP over 2
min; may administer
40–80 milligrams at
10-min intervals (up
to 300 milligrams
total cumulative
dose)
IV infusion (acute
loading):
Initial: 2
milligrams/min,
titrate to response
(up to 300 milligrams
total cumulative
dose)
HTN
With the exception of sotalol, all listed β-blockers are indicated for the treatment of hypertension. Theseagents are also used for ventricular rate control in atrial fibrillation as they slow atrioventricular nodalconduction by decreasing sympathetic tone.
PROPRANOLOL
Actions
Propranolol is a nonselective antagonist of β1- and β2-receptors.
Pharmacokinetics
See Table 19-6.
Indications
9/12/2019
10/36
See Table 19-6.
Dosing and Administration
See Table 19-6.
Adverse E�ects
Serious adverse e�ects associated with IV propranolol administration include bradycardia, heart block,hypotension, worsening heart failure, and bronchospasm.
ESMOLOL
Actions
Esmolol is a short-acting, selective β1-antagonist that exhibits negative inotropic and chronotropic e�ects. By
blocking β1-receptors, esmolol prevents excessive adrenergic stimulation of the myocardium, thus causing
an increase in sinus cycle length, prolongation of sinoatrial nodal recovery time, and a decrease inconduction through the atrioventricular node.
Pharmacokinetics
See Table 19-6.6 Esmolol is available as a parenteral formulation only and has a rapid onset of action andshort duration of action, with complete reversal of medication e�ects seen within 10 to 30 minutes a�erdiscontinuation.
Indications
See Table 19-6.4
Dosing and Administration
All listed doses are in micrograms. For the treatment of supraventricular tachycardia, the dose of esmolol is a500 microgram/kg bolus (optional) over 1 minute, followed by an infusion starting at 50 micrograms/kg/mintitrated to therapeutic e�ect in 50 microgram/kg/min increments every 4 minutes. To achieve a more rapidresponse, two additional 500 microgram/kg bolus doses may be given prior to increasing the infusion rate to100 micrograms/kg/min (a�er second bolus) and 150 micrograms/kg/min (a�er third bolus), as required.A�er 4 minutes at the rate of 150 micrograms/kg/min, the infusion rate may be increased to a maximum rateof 200 micrograms/kg/min (without an additional bolus dose).
Adverse E�ects
9/12/2019
11/36
Cardiovascular adverse e�ects of esmolol include hypotension (most common), bradycardia, and heartblock. Abrupt discontinuation may cause rebound hypertension or angina. Other adverse e�ects may includeinjection site reaction, nausea, bronchospasm, and pulmonary edema.
METOPROLOL
Actions
Metoprolol is a selective antagonist of β1-receptors and exerts its antihypertensive e�ects by decreasing
cardiac output, reducing sympathetic outflow, and suppressing renin activity.
Pharmacokinetics
See Table 19-6.
Indications
See Table 19-6.
Dosing and Administration
See Table 19-6 and Table 19-7.
TABLE 19-7
IV to PO Conversion of Metoprolol
Medication IV to PO Conversion
Metoprolol 5 milligrams IV = 12.5 milligrams PO
Adverse E�ects
Significant adverse e�ects associated with metoprolol include bradycardia, heart block, hypotension, andbronchospasm.
LABETALOL
Actions
Labetalol is a combined selective α1-blocking and nonselective β-blocking agent with direct vasodilatory
action. The β-blocking e�ects of labetalol are greater than the α1-blocking e�ects, with ratios of 3:1 in the
9/12/2019
12/36
oral and 7:1 in the parenteral formulation. Labetalol is useful as an antihypertensive agent because itdecreases heart rate, contractility, cardiac output, and total peripheral resistance.
Pharmacokinetics
See Table 19-6.
Indications
Labetalol is used primarily for its antihypertensive e�ects. It is used in patients with acute hypertensiveemergencies where rapid blood pressure reduction is indicated (see chapter 57, "Systemic Hypertension")and is considered safe for use in the treatment of hypertension in pregnancy (see chapters 99, "ComorbidDisorders in Pregnancy" and 100, "Maternal Emergencies a�er 20 Weeks of Pregnancy and in the PostpartumPeriod").
Dosing and Administration
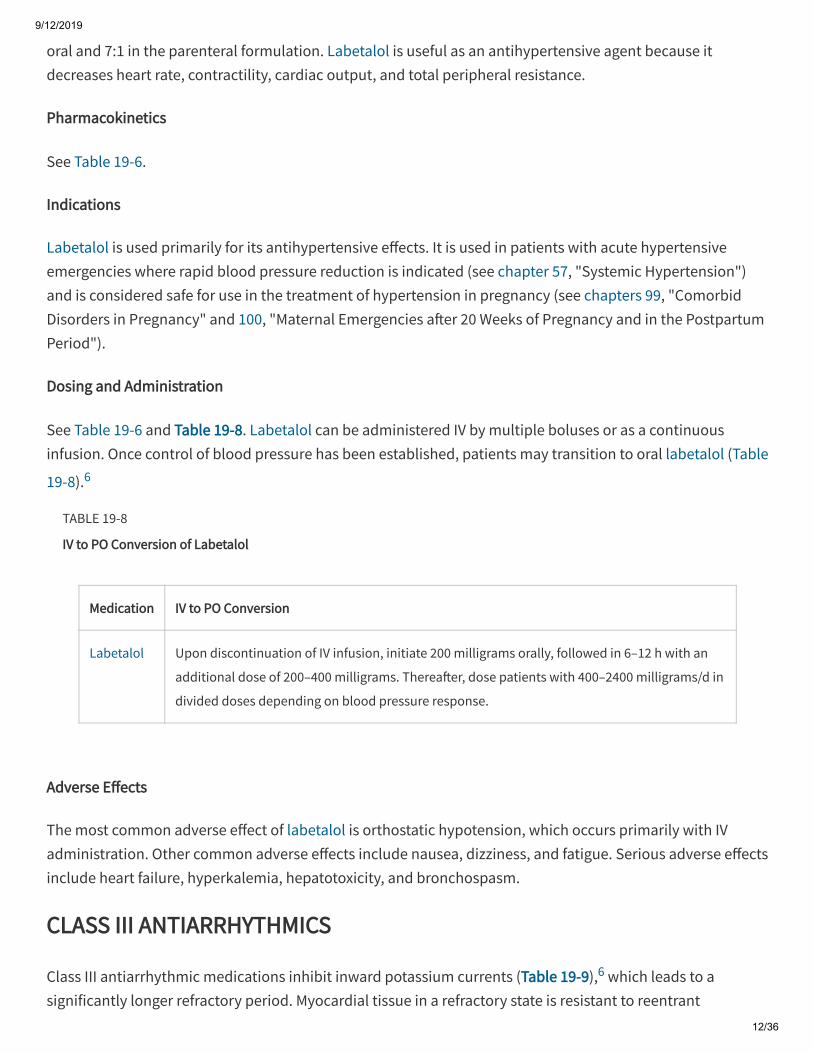
See Table 19-6 and Table 19-8. Labetalol can be administered IV by multiple boluses or as a continuousinfusion. Once control of blood pressure has been established, patients may transition to oral labetalol (Table
19-8).6
TABLE 19-8
IV to PO Conversion of Labetalol
Medication IV to PO Conversion
Labetalol Upon discontinuation of IV infusion, initiate 200 milligrams orally, followed in 6–12 h with an
additional dose of 200–400 milligrams. Therea�er, dose patients with 400–2400 milligrams/d in
divided doses depending on blood pressure response.
Adverse E�ects
The most common adverse e�ect of labetalol is orthostatic hypotension, which occurs primarily with IVadministration. Other common adverse e�ects include nausea, dizziness, and fatigue. Serious adverse e�ectsinclude heart failure, hyperkalemia, hepatotoxicity, and bronchospasm.
CLASS III ANTIARRHYTHMICS
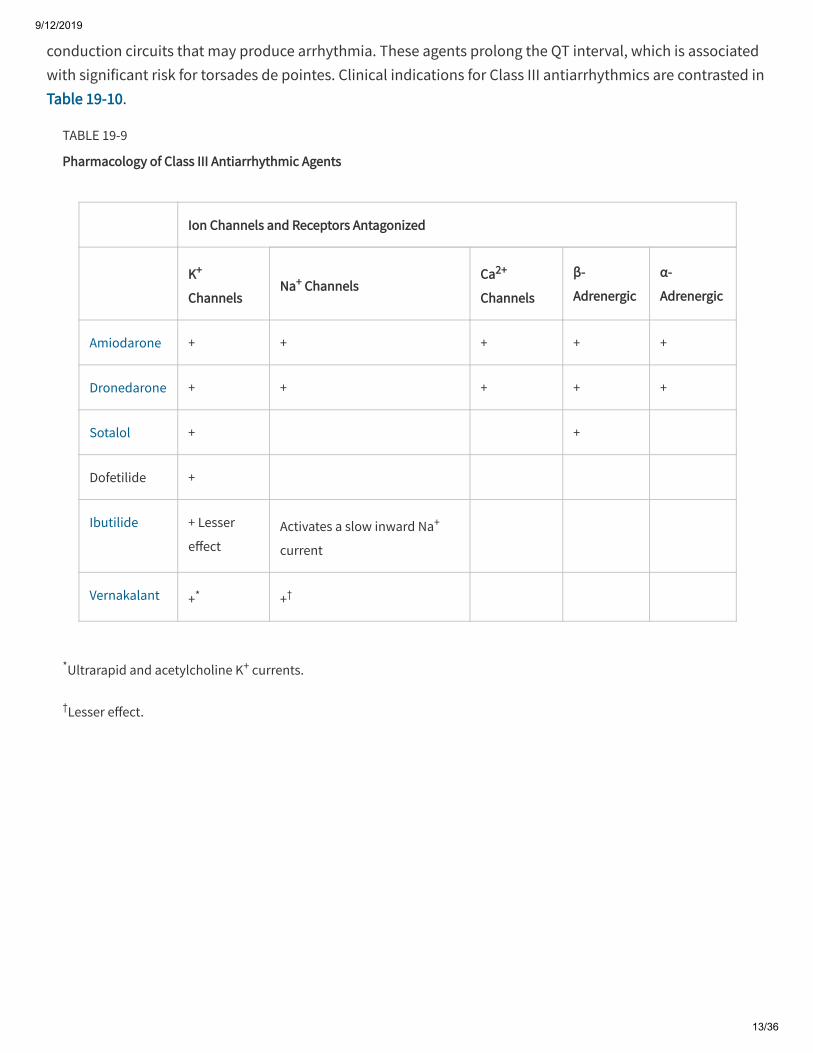
Class III antiarrhythmic medications inhibit inward potassium currents (Table 19-9),6 which leads to asignificantly longer refractory period. Myocardial tissue in a refractory state is resistant to reentrant
9/12/2019
13/36
*Ultrarapid and acetylcholine K+ currents.
†Lesser e�ect.
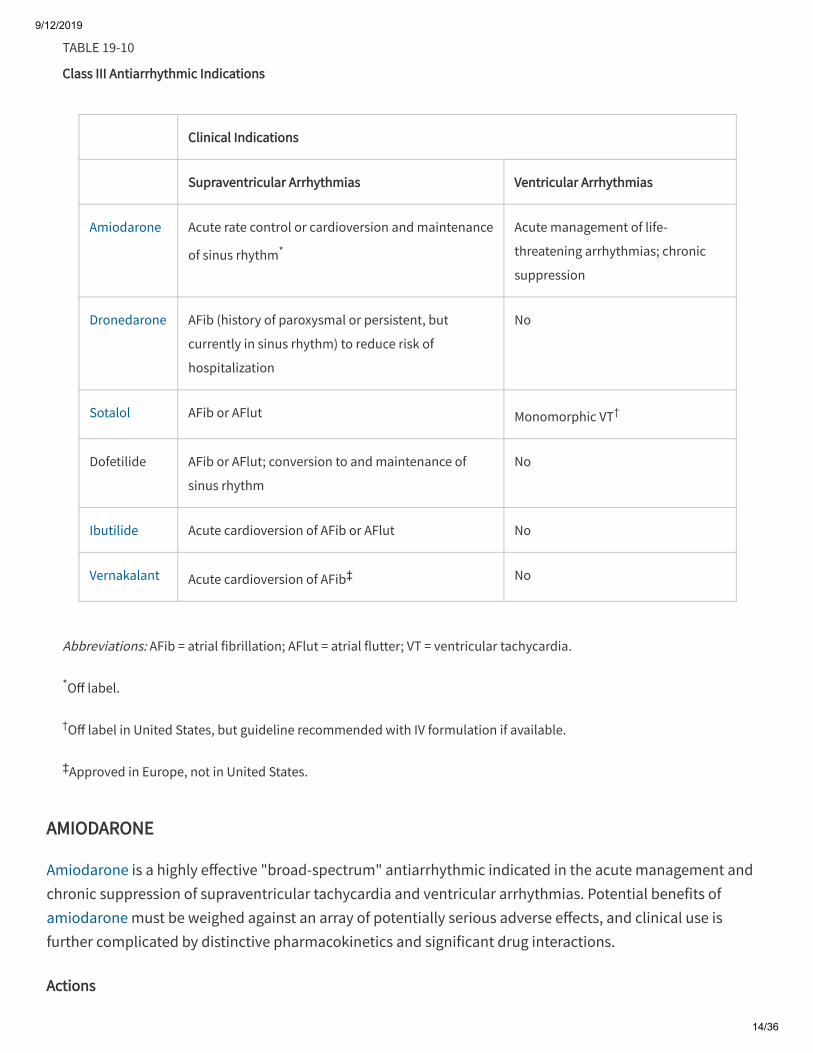
conduction circuits that may produce arrhythmia. These agents prolong the QT interval, which is associatedwith significant risk for torsades de pointes. Clinical indications for Class III antiarrhythmics are contrasted inTable 19-10.
TABLE 19-9
Pharmacology of Class III Antiarrhythmic Agents
Ion Channels and Receptors Antagonized
K+
ChannelsNa+ Channels
Ca2+
Channels
β-
Adrenergic
α-
Adrenergic
Amiodarone + + + + +
Dronedarone + + + + +
Sotalol + +
Dofetilide +
Ibutilide + Lesser
e�ectActivates a slow inward Na+
current
Vernakalant +* +†
9/12/2019
14/36
Abbreviations: AFib = atrial fibrillation; AFlut = atrial flutter; VT = ventricular tachycardia.
*O� label.
†O� label in United States, but guideline recommended with IV formulation if available.
‡Approved in Europe, not in United States.
TABLE 19-10
Class III Antiarrhythmic Indications
Clinical Indications
Supraventricular Arrhythmias Ventricular Arrhythmias
Amiodarone Acute rate control or cardioversion and maintenance
of sinus rhythm*
Acute management of life-
threatening arrhythmias; chronic
suppression
Dronedarone AFib (history of paroxysmal or persistent, but
currently in sinus rhythm) to reduce risk of
hospitalization
No
Sotalol AFib or AFlut Monomorphic VT†
Dofetilide AFib or AFlut; conversion to and maintenance of
sinus rhythm
No
Ibutilide Acute cardioversion of AFib or AFlut No
Vernakalant Acute cardioversion of AFib‡ No
AMIODARONE
Amiodarone is a highly e�ective "broad-spectrum" antiarrhythmic indicated in the acute management andchronic suppression of supraventricular tachycardia and ventricular arrhythmias. Potential benefits ofamiodarone must be weighed against an array of potentially serious adverse e�ects, and clinical use isfurther complicated by distinctive pharmacokinetics and significant drug interactions.
Actions
9/12/2019
15/36
*More common with chronic oral administration than with acute IV use.
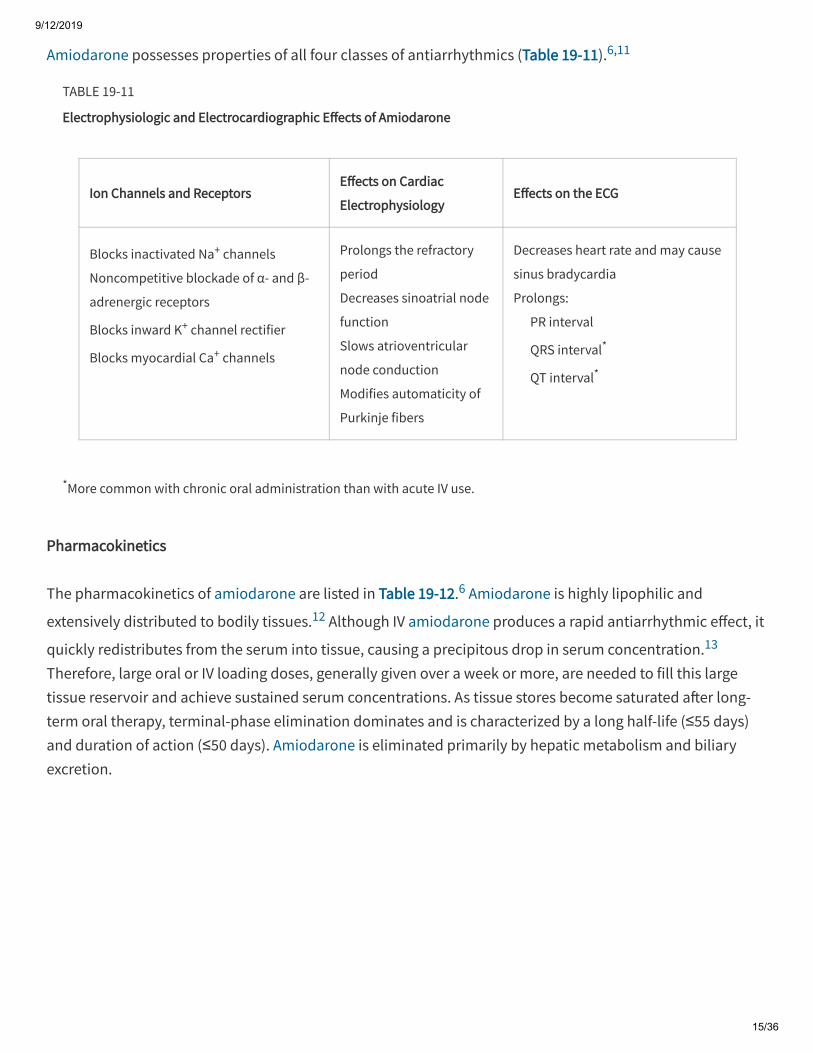
Amiodarone possesses properties of all four classes of antiarrhythmics (Table 19-11).6,11
TABLE 19-11
Electrophysiologic and Electrocardiographic E�ects of Amiodarone
Ion Channels and ReceptorsE�ects on Cardiac
ElectrophysiologyE�ects on the ECG
Blocks inactivated Na+ channels
Noncompetitive blockade of α- and β-
adrenergic receptors
Blocks inward K+ channel rectifier
Blocks myocardial Ca+ channels
Prolongs the refractory
period
Decreases sinoatrial node
function
Slows atrioventricular
node conduction
Modifies automaticity of
Purkinje fibers
Decreases heart rate and may cause
sinus bradycardia
Prolongs:
PR interval
QRS interval*
QT interval*
Pharmacokinetics
The pharmacokinetics of amiodarone are listed in Table 19-12.6 Amiodarone is highly lipophilic and
extensively distributed to bodily tissues.12 Although IV amiodarone produces a rapid antiarrhythmic e�ect, it
quickly redistributes from the serum into tissue, causing a precipitous drop in serum concentration.13
Therefore, large oral or IV loading doses, generally given over a week or more, are needed to fill this largetissue reservoir and achieve sustained serum concentrations. As tissue stores become saturated a�er long-term oral therapy, terminal-phase elimination dominates and is characterized by a long half-life (≤55 days)and duration of action (≤50 days). Amiodarone is eliminated primarily by hepatic metabolism and biliaryexcretion.
9/12/2019
16/36
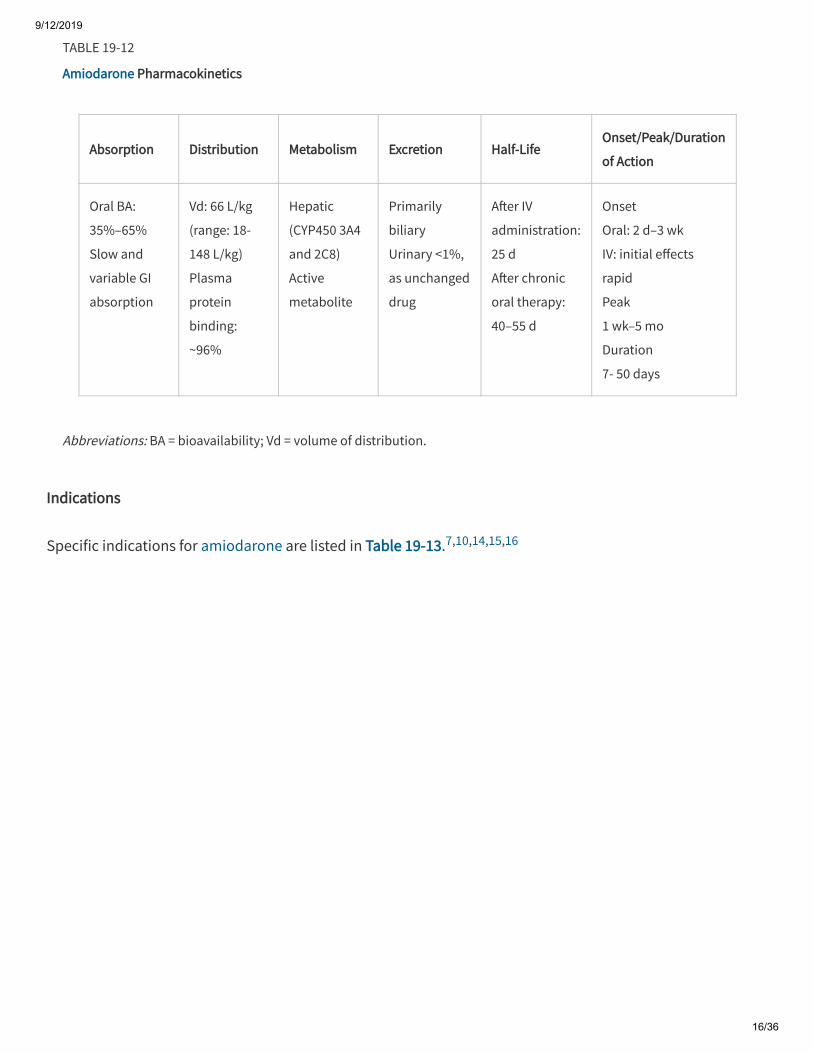
Abbreviations: BA = bioavailability; Vd = volume of distribution.
TABLE 19-12
Amiodarone Pharmacokinetics
Absorption Distribution Metabolism Excretion Half-LifeOnset/Peak/Duration
of Action
Oral BA:
35%–65%
Slow and
variable GI
absorption
Vd: 66 L/kg
(range: 18-
148 L/kg)
Plasma
protein
binding:
~96%
Hepatic
(CYP450 3A4
and 2C8)
Active
metabolite
Primarily
biliary
Urinary <1%,
as unchanged
drug
A�er IV
administration:
25 d
A�er chronic
oral therapy:
40–55 d
Onset
Oral: 2 d–3 wk
IV: initial e�ects
rapid
Peak
1 wk–5 mo
Duration
7- 50 days
Indications
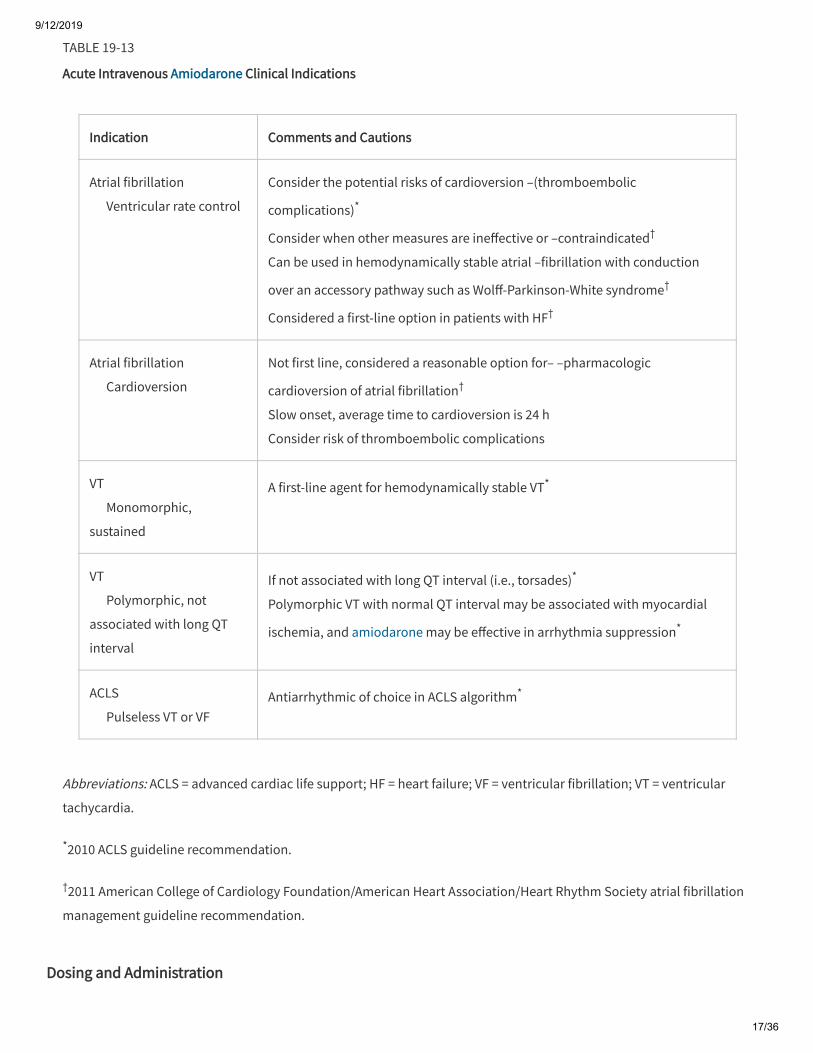
Specific indications for amiodarone are listed in Table 19-13.7,10,14,15,16
9/12/2019
17/36
Abbreviations: ACLS = advanced cardiac life support; HF = heart failure; VF = ventricular fibrillation; VT = ventricular
tachycardia.
*2010 ACLS guideline recommendation.
†2011 American College of Cardiology Foundation/American Heart Association/Heart Rhythm Society atrial fibrillation
management guideline recommendation.
TABLE 19-13
Acute Intravenous Amiodarone Clinical Indications
Indication Comments and Cautions
Atrial fibrillation
Ventricular rate control
Consider the potential risks of cardioversion –(thromboembolic
complications)*
Consider when other measures are ine�ective or –contraindicated†
Can be used in hemodynamically stable atrial –fibrillation with conduction
over an accessory pathway such as Wol�-Parkinson-White syndrome†
Considered a first-line option in patients with HF†
Atrial fibrillation
Cardioversion
Not first line, considered a reasonable option for– –pharmacologic
cardioversion of atrial fibrillation†
Slow onset, average time to cardioversion is 24 h
Consider risk of thromboembolic complications
VT
Monomorphic,
sustained
A first-line agent for hemodynamically stable VT*
VT
Polymorphic, not
associated with long QT
interval
If not associated with long QT interval (i.e., torsades)*
Polymorphic VT with normal QT interval may be associated with myocardial
ischemia, and amiodarone may be e�ective in arrhythmia suppression*
ACLS
Pulseless VT or VFAntiarrhythmic of choice in ACLS algorithm*
Dosing and Administration
9/12/2019
18/36
Abbreviations: ACLS = advanced cardiac life support; D5W = dextrose in 5% water; SVT = supraventricular tachycardia;
VF = ventricular fibrillation; VT = ventricular tachycardia.
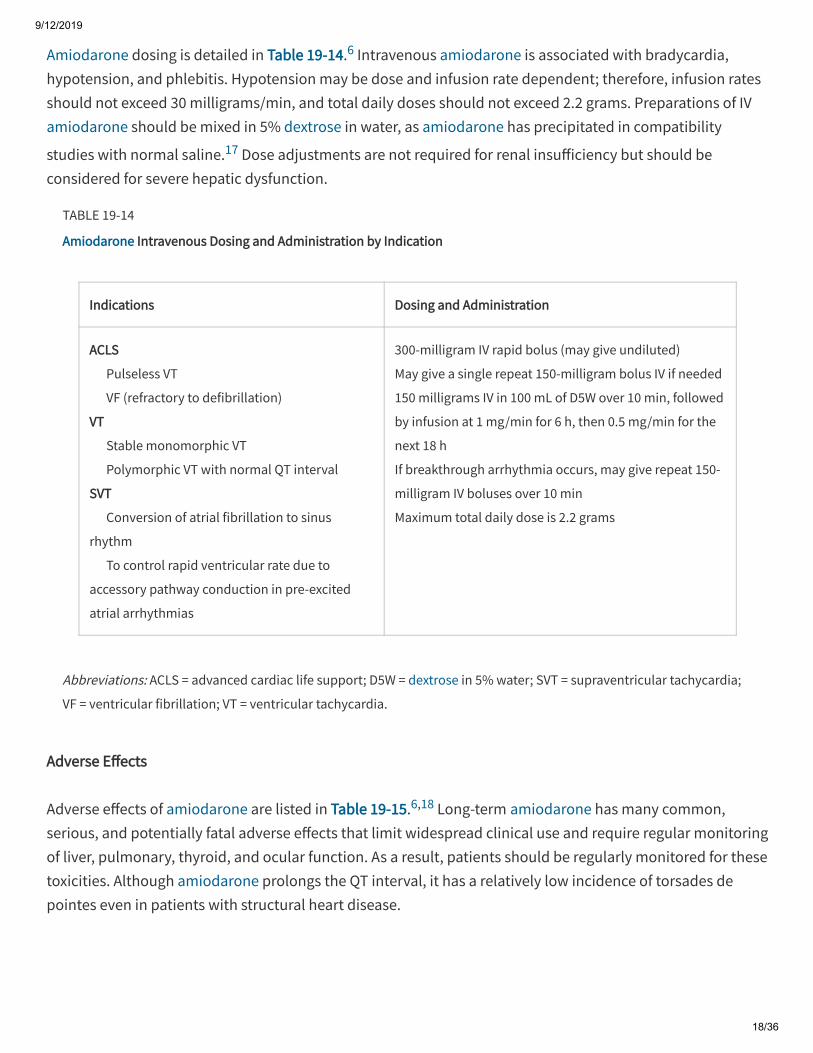
Amiodarone dosing is detailed in Table 19-14.6 Intravenous amiodarone is associated with bradycardia,hypotension, and phlebitis. Hypotension may be dose and infusion rate dependent; therefore, infusion ratesshould not exceed 30 milligrams/min, and total daily doses should not exceed 2.2 grams. Preparations of IVamiodarone should be mixed in 5% dextrose in water, as amiodarone has precipitated in compatibility
studies with normal saline.17 Dose adjustments are not required for renal insu�iciency but should beconsidered for severe hepatic dysfunction.
TABLE 19-14
Amiodarone Intravenous Dosing and Administration by Indication
Indications Dosing and Administration
ACLS
Pulseless VT
VF (refractory to defibrillation)
VT
Stable monomorphic VT
Polymorphic VT with normal QT interval
SVT
Conversion of atrial fibrillation to sinus
rhythm
To control rapid ventricular rate due to
accessory pathway conduction in pre-excited
atrial arrhythmias
300-milligram IV rapid bolus (may give undiluted)
May give a single repeat 150-milligram bolus IV if needed
150 milligrams IV in 100 mL of D5W over 10 min, followed
by infusion at 1 mg/min for 6 h, then 0.5 mg/min for the
next 18 h
If breakthrough arrhythmia occurs, may give repeat 150-
milligram IV boluses over 10 min
Maximum total daily dose is 2.2 grams
Adverse E�ects
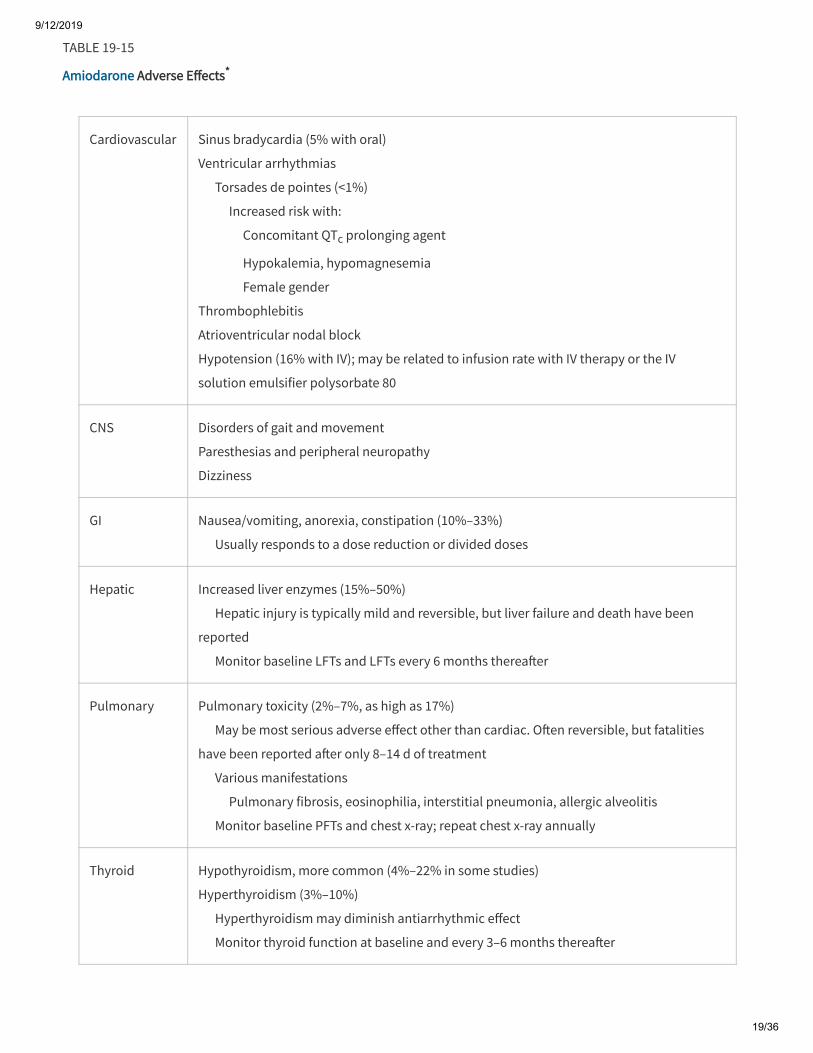
Adverse e�ects of amiodarone are listed in Table 19-15.6,18 Long-term amiodarone has many common,serious, and potentially fatal adverse e�ects that limit widespread clinical use and require regular monitoringof liver, pulmonary, thyroid, and ocular function. As a result, patients should be regularly monitored for thesetoxicities. Although amiodarone prolongs the QT interval, it has a relatively low incidence of torsades depointes even in patients with structural heart disease.
9/12/2019
19/36
TABLE 19-15
Amiodarone Adverse E�ects*
Cardiovascular Sinus bradycardia (5% with oral)
Ventricular arrhythmias
Torsades de pointes (<1%)
Increased risk with:
Concomitant QTc prolonging agent
Hypokalemia, hypomagnesemia
Female gender
Thrombophlebitis
Atrioventricular nodal block
Hypotension (16% with IV); may be related to infusion rate with IV therapy or the IV
solution emulsifier polysorbate 80
CNS Disorders of gait and movement
Paresthesias and peripheral neuropathy
Dizziness
GI Nausea/vomiting, anorexia, constipation (10%–33%)
Usually responds to a dose reduction or divided doses
Hepatic Increased liver enzymes (15%–50%)
Hepatic injury is typically mild and reversible, but liver failure and death have been
reported
Monitor baseline LFTs and LFTs every 6 months therea�er
Pulmonary Pulmonary toxicity (2%–7%, as high as 17%)
May be most serious adverse e�ect other than cardiac. O�en reversible, but fatalities
have been reported a�er only 8–14 d of treatment
Various manifestations
Pulmonary fibrosis, eosinophilia, interstitial pneumonia, allergic alveolitis
Monitor baseline PFTs and chest x-ray; repeat chest x-ray annually
Thyroid Hypothyroidism, more common (4%–22% in some studies)
Hyperthyroidism (3%–10%)
Hyperthyroidism may diminish antiarrhythmic e�ect
Monitor thyroid function at baseline and every 3–6 months therea�er
9/12/2019
20/36
Abbreviations: LFTs = liver function tests; PFTs = pulmonary function tests.
*Incomplete listing; excludes nonacute/non–life-threatening dermatologic, ocular, and other e�ects.
Amiodarone is responsible for many clinically significant drug interactions. As a strong inhibitor of liverenzymes, amiodarone increases serum concentrations of many other medications. Amiodarone may alsoaugment the e�ects of medications that concomitantly prolong the QTc interval or cause bradycardia.
Specific dose reductions are required for digoxin, warfarin, procainamide, quinidine, simvastatin, andlovastatin when used concomitantly with amiodarone. Given amiodarone's extremely long half-life, druginteractions may persist for months a�er discontinuation of therapy.
DRONEDARONE
Actions
Dronedarone is a noniodinated, less lipophilic derivative of amiodarone, designed to have a more favorableadverse e�ect profile than its predecessor. Dronedarone is categorized as a Class III antiarrhythmic but hasall four antiarrhythmic class e�ects and blocks α-adrenergic receptors. Electrophysiologic action is primarily
mediated through Class III antiarrhythmic e�ects by prolonging the refractory period.6
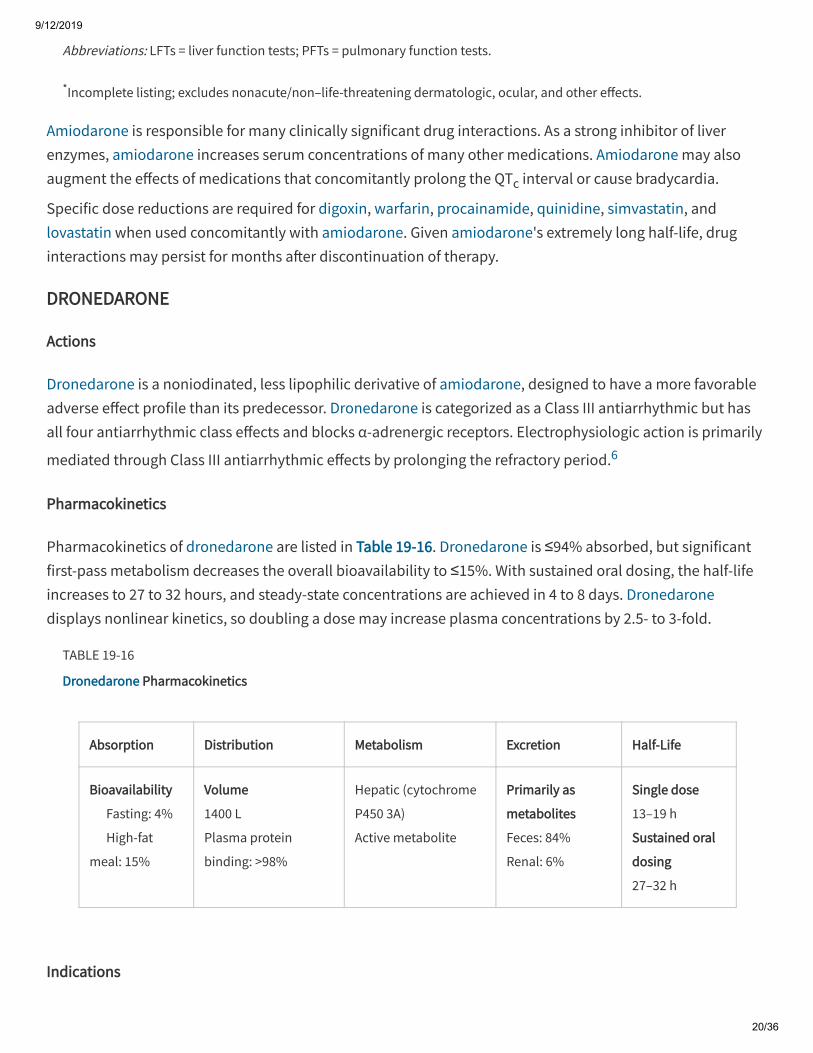
Pharmacokinetics
Pharmacokinetics of dronedarone are listed in Table 19-16. Dronedarone is ≤94% absorbed, but significantfirst-pass metabolism decreases the overall bioavailability to ≤15%. With sustained oral dosing, the half-lifeincreases to 27 to 32 hours, and steady-state concentrations are achieved in 4 to 8 days. Dronedaronedisplays nonlinear kinetics, so doubling a dose may increase plasma concentrations by 2.5- to 3-fold.
TABLE 19-16
Dronedarone Pharmacokinetics
Absorption Distribution Metabolism Excretion Half-Life
Bioavailability
Fasting: 4%
High-fat
meal: 15%
Volume
1400 L
Plasma protein
binding: >98%
Hepatic (cytochrome
P450 3A)
Active metabolite
Primarily as
metabolites
Feces: 84%
Renal: 6%
Single dose
13–19 h
Sustained oral
dosing
27–32 h
Indications
9/12/2019
21/36
Dronedarone is indicated to reduce the risk of hospitalization for atrial fibrillation in patients in sinus rhythmwith a history of paroxysmal or persistent atrial fibrillation. It is less e�icacious than amiodarone formaintenance of sinus rhythm.
Dosing and Administration
The dose of dronedarone is 400 milligrams orally twice daily and should be given with the morning andevening meal to increase bioavailability. Coadministration with grapefruit or grapefruit juice iscontraindicated, as this may increase serum concentrations.
Adverse E�ects
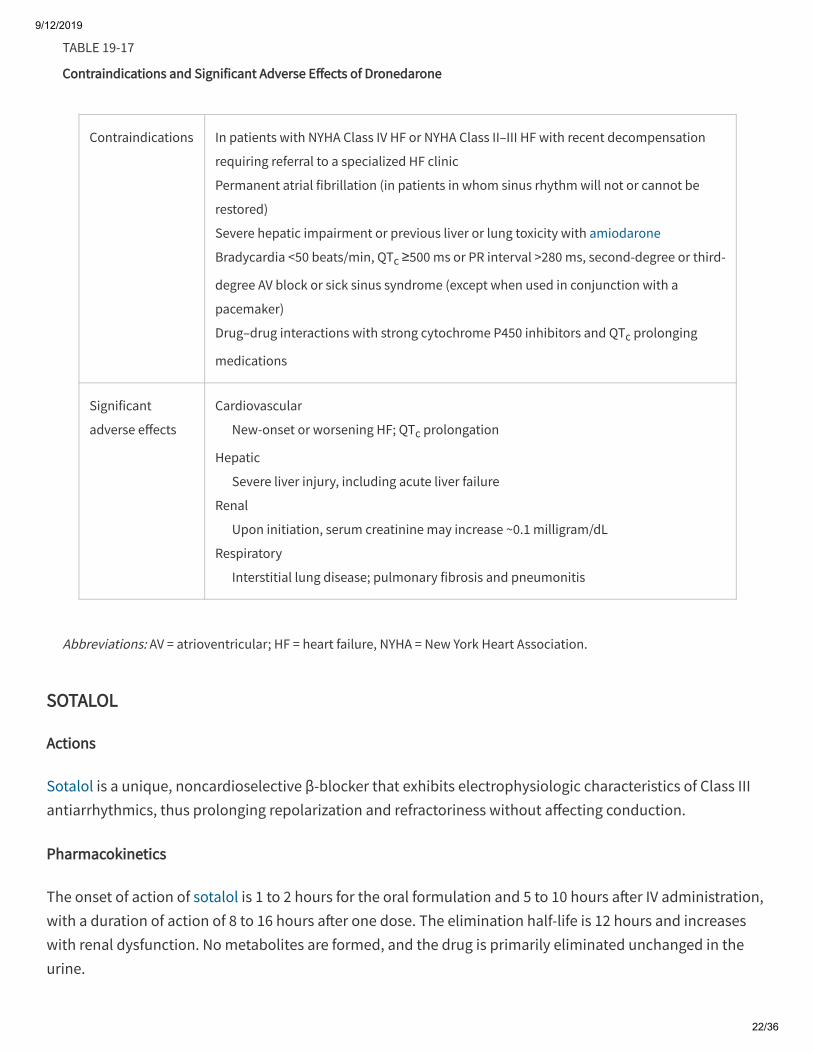
Contraindications and significant adverse e�ects of dronedarone are highlighted in Table 19-17. Comparedto amiodarone, dronedarone has lower rates of pulmonary toxicity and has not demonstrated adverse e�ectson thyroid function. Two clinical trials with dronedarone were prematurely discontinued due to significantlyhigher rates of serious adverse events in the dronedarone treatment groups, prompting black box warningsthat dronedarone is contraindicated in severe or decompensated heart failure and in patients with
permanent atrial fibrillation.5,19 ECGs should be monitored at least every 3 months while on dronedarone. Ifthe patient is found to be in atrial fibrillation, he or she should be cardioverted (if clinically indicated) ordronedarone should be discontinued. Liver function should also be monitored periodically, especially duringthe first 6 months of therapy.
9/12/2019
22/36
Abbreviations: AV = atrioventricular; HF = heart failure, NYHA = New York Heart Association.
TABLE 19-17
Contraindications and Significant Adverse E�ects of Dronedarone
Contraindications In patients with NYHA Class IV HF or NYHA Class II–III HF with recent decompensation
requiring referral to a specialized HF clinic
Permanent atrial fibrillation (in patients in whom sinus rhythm will not or cannot be
restored)
Severe hepatic impairment or previous liver or lung toxicity with amiodarone
Bradycardia <50 beats/min, QTc ≥500 ms or PR interval >280 ms, second-degree or third-
degree AV block or sick sinus syndrome (except when used in conjunction with a
pacemaker)
Drug–drug interactions with strong cytochrome P450 inhibitors and QTc prolonging
medications
Significant
adverse e�ects
Cardiovascular
New-onset or worsening HF; QTc prolongation
Hepatic
Severe liver injury, including acute liver failure
Renal
Upon initiation, serum creatinine may increase ~0.1 milligram/dL
Respiratory
Interstitial lung disease; pulmonary fibrosis and pneumonitis
SOTALOL
Actions
Sotalol is a unique, noncardioselective β-blocker that exhibits electrophysiologic characteristics of Class IIIantiarrhythmics, thus prolonging repolarization and refractoriness without a�ecting conduction.
Pharmacokinetics
The onset of action of sotalol is 1 to 2 hours for the oral formulation and 5 to 10 hours a�er IV administration,with a duration of action of 8 to 16 hours a�er one dose. The elimination half-life is 12 hours and increaseswith renal dysfunction. No metabolites are formed, and the drug is primarily eliminated unchanged in theurine.
9/12/2019
23/36
Indications
Sotalol is an e�ective agent for the suppression of life-threatening ventricular arrhythmias refractory to otherantiarrhythmic drugs. It can suppress supraventricular tachycardia and atrial fibrillation but is not indicated
for cardioversion of atrial fibrillation.10
Dosing and Administration
The usual starting dose is 80 milligrams PO twice daily (which can be titrated), and the usual maintenancedose is 160 to 320 milligrams/d; the dose should be reduced by 50% or more in patients with renalinsu�iciency (creatinine clearance <60 mL/min), and sotalol should not be used (except in special cases) ifcreatinine clearance is <40 mL/min. IV sotalol is indicated in the current advanced cardiac life supportguidelines for hemodynamically stable monomorphic ventricular tachycardia at 1.5 milligrams/kg infusedover 5 min. Monitoring of cardiac and renal function is recommended when sotalol is started. Duringinitiation of sotalol therapy (pretreatment QTc should be <450 milliseconds), QTc intervals are measured 2 to
4 hours a�er each oral dose or at the end of an infusion, and therapy is discontinued if QTc measures ≥500
milliseconds.
Adverse E�ects
The most common adverse e�ects of sotalol are bradycardia and hypotension. Sotalol does possess asignificant proarrhythmic e�ect with a 4.3% rate of new or worsened ventricular arrhythmias and a 2.4% rate
of torsades de pointes.20
DOFETILIDE
Actions/Indications/Dosing
Dofetilide is a pure Class III antiarrhythmic and is indicated for the conversion to, and maintenance of,normal sinus rhythm in patients with atrial fibrillation or flutter. Because dofetilide has a significantproarrhythmic e�ect, it is reserved for patients in whom atrial fibrillation or flutter is highly symptomatic.Dofetilide prescribing is restricted to physicians who have received specific education on dosing and
administration and, therefore, is not covered here in detail.21
Adverse E�ects
Serious adverse e�ects of dofetilide are ventricular tachycardia and QTc interval prolongation, which can
result in torsades de pointes. The risk of developing torsades de pointes is associated with higher dofetilidedoses, initiation of therapy, and electrolyte abnormalities.
IBUTILIDE
9/12/2019
24/36
Actions/Pharmacokinetics
Ibutilide prolongs the refractory period in atrial and ventricular cardiac tissues. This action is caused byactivation of a slow inward sodium current, as opposed to inhibition of outward potassium currents.Blockade of the delayed rectifier potassium current, which slows repolarization, may also contribute to itsclinical e�ects. The onset of action of ibutilide is ~90 minutes a�er starting the infusion. Ibutilide ismetabolized in the liver, is excreted in the urine and feces, and has a half-life of 2 to 12 hours a�er IVadministration.
Indications/Dosing and Administration/Adverse E�ects
Ibutilide is indicated for the rapid conversion of recent-onset atrial fibrillation or flutter (greater e�icacy) to
sinus rhythm.10 If e�ective, cardioversion is expected to occur within 1 hour of administration. For patientswith atrial fibrillation and an accessory pathway, ibutilide is considered a reasonable option for
pharmacologic cardioversion.16 Serum magnesium and potassium levels should be evaluated andresuscitation equipment made available before ibutilide administration. The loading dose is 1 milligram IV(weight ≥60 kg) or 0.01 milligram/kg IV (weight <60 kg) over 10 minutes and may be repeated once every 10minutes a�er completion of the first dose. Electrocardiographic monitoring is continued for at least 4 hoursor until the QTc interval returns to baseline (longer if arrhythmias are observed). Cardiovascular adverse
e�ects of ibutilide include hypotension, hypertension, bradycardia, sinus arrest, syncope, QTc interval
prolongation, congestive heart failure, and torsades de pointes.
VERNAKALANT
Vernakalant is a Class III antiarrhythmic that inhibits sodium and potassium currents. The atria are moresusceptible to vernakalant-induced refractory period prolongation. Vernakalant is not U.S. Food and DrugAdministration approved for use in the United States. In Europe, vernakalant is indicated for rapid conversion
of recent-onset atrial fibrillation in adults.22
CLASS IV ANTIARRHYTHMICS: CALCIUM CHANNEL BLOCKERS
Calcium channel blockers inhibit L-type calcium channels, resulting in slowing of atrioventricular nodalconduction and an increase in the refractory period of nodal tissue. In the myocardium, calcium channelsprimarily a�ect the action potential plateau and modulate the strength of muscle contraction. Calciumchannel blockers are divided into two categories, dihydropyridine and nondihydropyridine.Nondihydropyridine calcium channel blockers have greater cardioselectivity and are generally used forparoxysmal supraventricular tachycardia and rate control in atrial fibrillation, whereas dihydropyridinecalcium channel blockers are more selective for the vasculature and are used to treat hypertension.
DILTIAZEM/VERAPAMIL
9/12/2019
25/36
Abbreviations: BA = bioavailability; ER = extended release (controlled release); IR = immediate release; Vd = volume of
distribution.
Actions
Diltiazem and verapamil are nondihydropyridine calcium channel blockers that slow atrioventricular nodalconduction, increase the atrioventricular node's refractory period, decrease automaticity, and prolong thePR interval. Verapamil is more potent than diltiazem resulting in greater atrioventricular nodal depression;therefore, verapamil is used more frequently to abort supraventricular tachycardia than diltiazem.
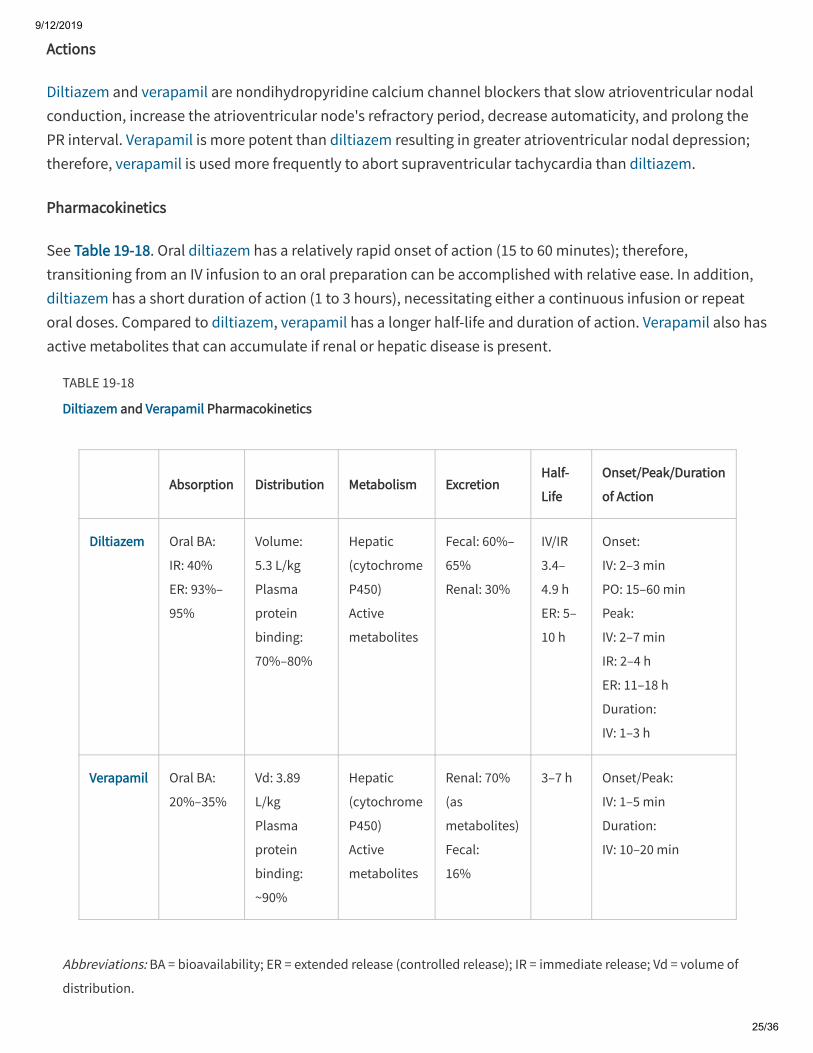
Pharmacokinetics
See Table 19-18. Oral diltiazem has a relatively rapid onset of action (15 to 60 minutes); therefore,transitioning from an IV infusion to an oral preparation can be accomplished with relative ease. In addition,diltiazem has a short duration of action (1 to 3 hours), necessitating either a continuous infusion or repeatoral doses. Compared to diltiazem, verapamil has a longer half-life and duration of action. Verapamil also hasactive metabolites that can accumulate if renal or hepatic disease is present.
TABLE 19-18
Diltiazem and Verapamil Pharmacokinetics
Absorption Distribution Metabolism ExcretionHalf-
Life
Onset/Peak/Duration
of Action
Diltiazem Oral BA:
IR: 40%
ER: 93%–
95%
Volume:
5.3 L/kg
Plasma
protein
binding:
70%–80%
Hepatic
(cytochrome
P450)
Active
metabolites
Fecal: 60%–
65%
Renal: 30%
IV/IR
3.4–
4.9 h
ER: 5–
10 h
Onset:
IV: 2–3 min
PO: 15–60 min
Peak:
IV: 2–7 min
IR: 2–4 h
ER: 11–18 h
Duration:
IV: 1–3 h
Verapamil Oral BA:
20%–35%
Vd: 3.89
L/kg
Plasma
protein
binding:
~90%
Hepatic
(cytochrome
P450)
Active
metabolites
Renal: 70%
(as
metabolites)
Fecal:
16%
3–7 h Onset/Peak:
IV: 1–5 min
Duration:
IV: 10–20 min
9/12/2019
26/36
Indications
Diltiazem and verapamil are indicated for paroxysmal supraventricular tachycardia as well as for rate control
in atrial fibrillation10; however, verapamil is used more commonly to abort supraventricular tachycardia with
a conversion rate to sinus similar to adenosine (90%),23 whereas diltiazem is used more commonly to control
rapid ventricular rate in atrial fibrillation.10 Both agents are contraindicated for wide-complextachyarrhythmias, which may be a result of Wol�-Parkinson-White syndrome, due to the high risk of life-threatening ventricular arrhythmia when given to these patients. Other contraindications include sick sinussyndrome, second- or third-degree atrioventricular block, severe hypotension, cardiogenic shock,administration concomitantly or within a few hours of IV β-blockers, and ventricular tachycardia.
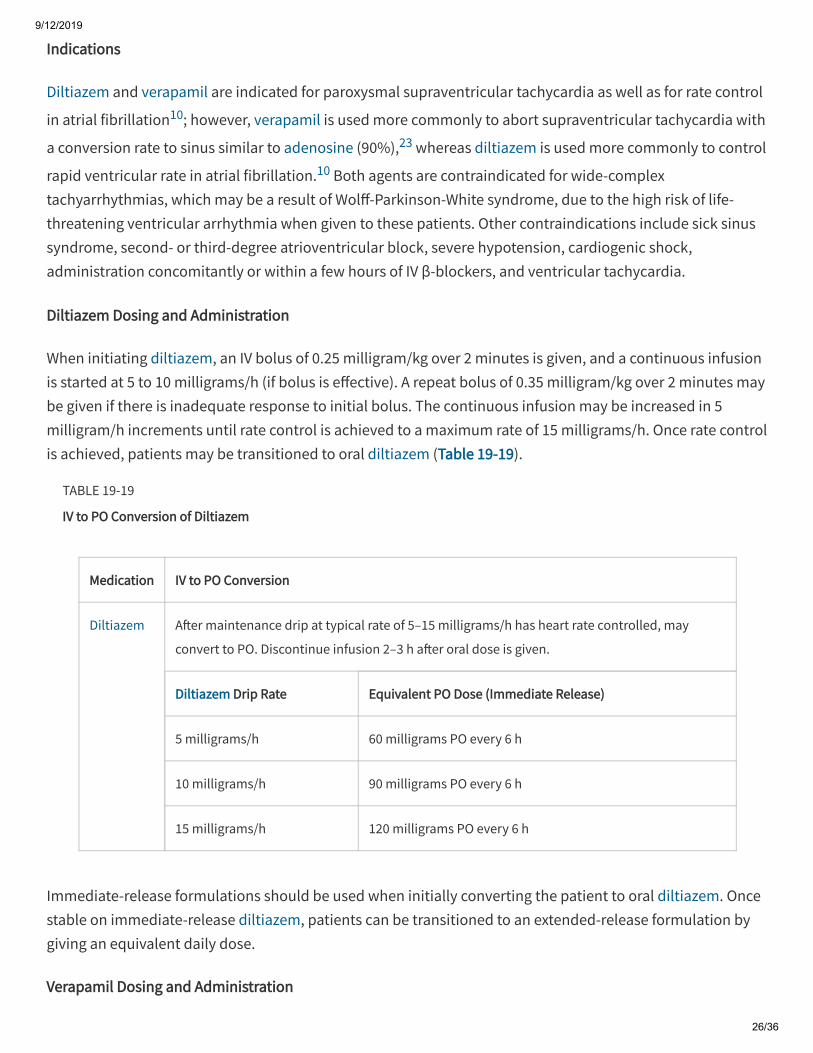
Diltiazem Dosing and Administration
When initiating diltiazem, an IV bolus of 0.25 milligram/kg over 2 minutes is given, and a continuous infusionis started at 5 to 10 milligrams/h (if bolus is e�ective). A repeat bolus of 0.35 milligram/kg over 2 minutes maybe given if there is inadequate response to initial bolus. The continuous infusion may be increased in 5milligram/h increments until rate control is achieved to a maximum rate of 15 milligrams/h. Once rate controlis achieved, patients may be transitioned to oral diltiazem (Table 19-19).
TABLE 19-19
IV to PO Conversion of Diltiazem
Medication IV to PO Conversion
Diltiazem A�er maintenance drip at typical rate of 5–15 milligrams/h has heart rate controlled, may
convert to PO. Discontinue infusion 2–3 h a�er oral dose is given.
Diltiazem Drip Rate Equivalent PO Dose (Immediate Release)
5 milligrams/h 60 milligrams PO every 6 h
10 milligrams/h 90 milligrams PO every 6 h
15 milligrams/h 120 milligrams PO every 6 h
Immediate-release formulations should be used when initially converting the patient to oral diltiazem. Oncestable on immediate-release diltiazem, patients can be transitioned to an extended-release formulation bygiving an equivalent daily dose.
Verapamil Dosing and Administration
9/12/2019
27/36
For treatment of supraventricular tachycardia, give 2.5 to 5 milligrams IV over 2 minutes. A second dose of 5to 10 milligrams (~0.15 milligram/kg) may be given 15 to 30 minutes a�er the initial dose if the patient does
not respond to the initial dose and can tolerate a second dose (maximum total dose: 20 to 30 milligrams).6
Adverse E�ects
Diltiazem is generally well tolerated by patients and has a favorable safety profile when compared to otherantiarrhythmic agents. Adverse e�ects associated with diltiazem and verapamil administration arebradyarrhythmia, asystole, fatigue, headache, hypotension, atrioventricular block, peripheral edema,syncope, and dizziness.
NICARDIPINE
Actions
Nicardipine is a dihydropyridine calcium channel antagonist that causes relaxation of smooth muscle,thereby lowering blood pressure. It has no antiarrhythmic properties and little to no e�ect on themyocardium.
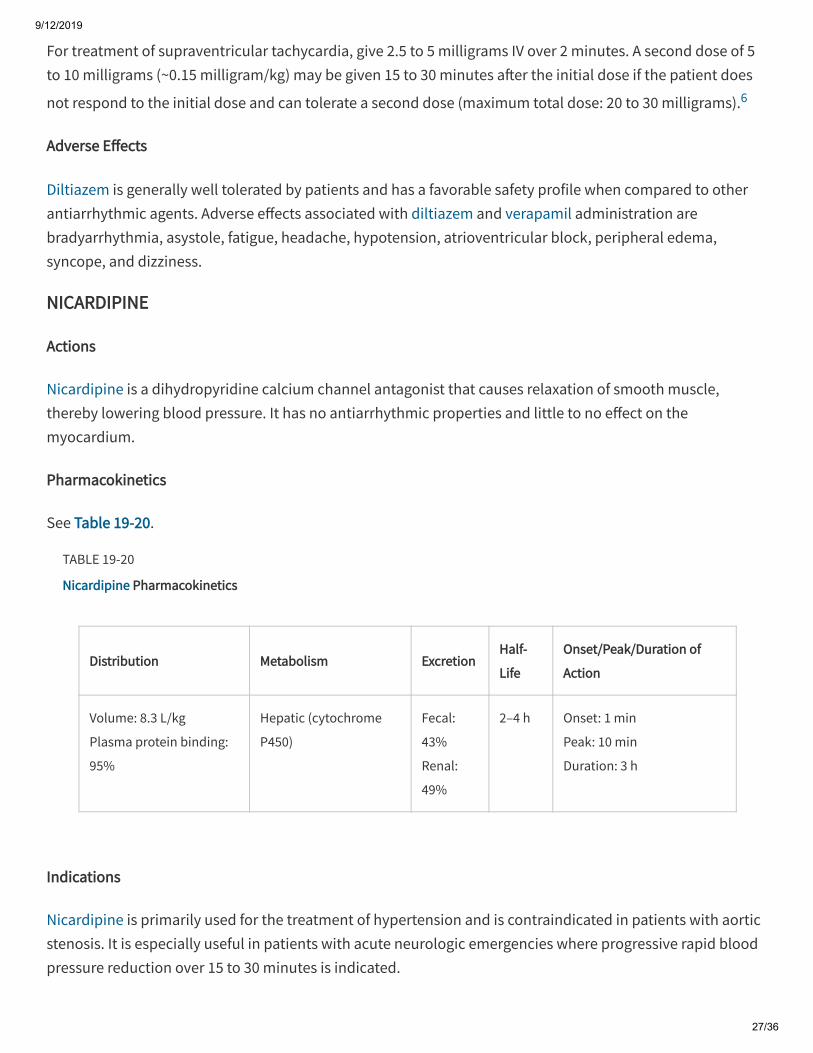
Pharmacokinetics
See Table 19-20.
TABLE 19-20
Nicardipine Pharmacokinetics
Distribution Metabolism ExcretionHalf-
Life
Onset/Peak/Duration of
Action
Volume: 8.3 L/kg
Plasma protein binding:
95%
Hepatic (cytochrome
P450)
Fecal:
43%
Renal:
49%
2–4 h Onset: 1 min
Peak: 10 min
Duration: 3 h
Indications
Nicardipine is primarily used for the treatment of hypertension and is contraindicated in patients with aorticstenosis. It is especially useful in patients with acute neurologic emergencies where progressive rapid bloodpressure reduction over 15 to 30 minutes is indicated.
9/12/2019
28/36
Dosing and Administration
Nicardipine is administered as an IV infusion with an initial rate of 5 milligrams/h. The infusion may betitrated in 2.5 milligram/h increments every 5 to 15 minutes based on blood pressure response with amaximum infusion rate of 15 milligrams/h.
Adverse E�ect Profile
Nicardipine is generally well tolerated by patients. Common side e�ects associated with nicardipineadministration include hypotension/orthostatic hypotension, edema, flushing, tachycardia, palpitations, andnausea.
OTHER ANTIARRHYTHMIC MEDICATIONS
DIGOXIN
Actions
Digoxin, a cardiac glycoside, has positive inotropic, negative chronotropic, and negative dromotropic e�ectson the myocardium due to inhibition of the sodium-potassium ATPase.
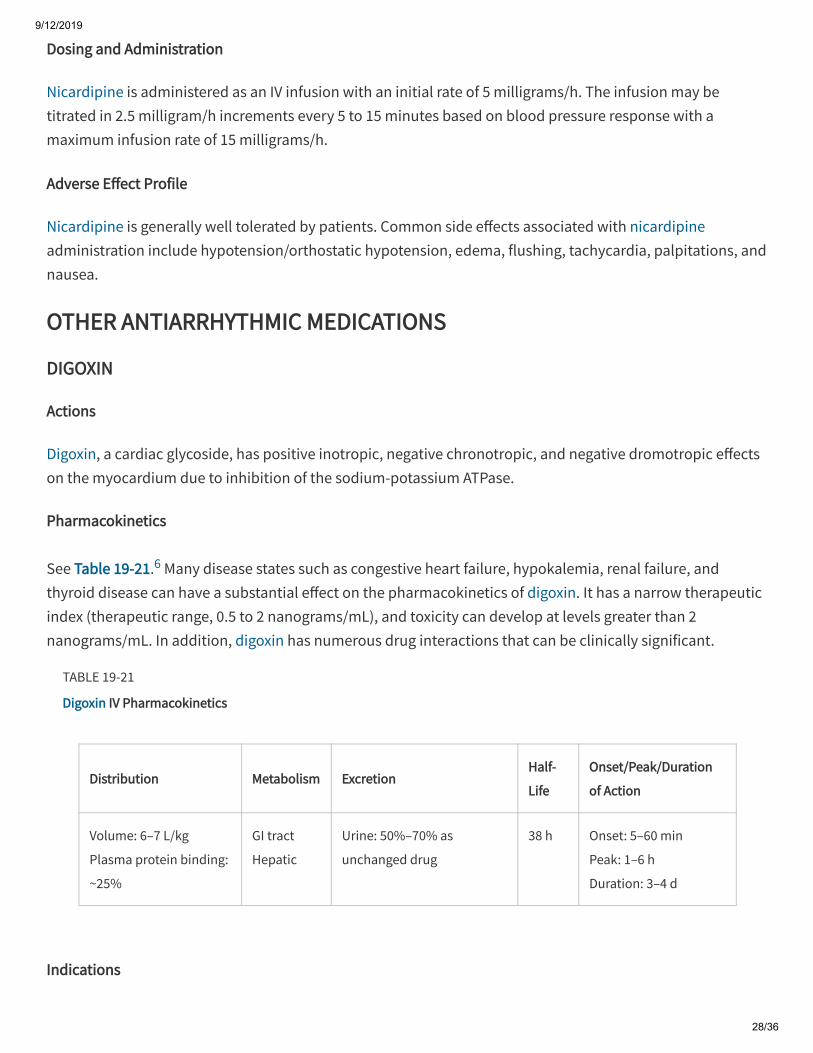
Pharmacokinetics
See Table 19-21.6 Many disease states such as congestive heart failure, hypokalemia, renal failure, andthyroid disease can have a substantial e�ect on the pharmacokinetics of digoxin. It has a narrow therapeuticindex (therapeutic range, 0.5 to 2 nanograms/mL), and toxicity can develop at levels greater than 2nanograms/mL. In addition, digoxin has numerous drug interactions that can be clinically significant.
TABLE 19-21
Digoxin IV Pharmacokinetics
Distribution Metabolism ExcretionHalf-
Life
Onset/Peak/Duration
of Action
Volume: 6–7 L/kg
Plasma protein binding:
~25%
GI tract
Hepatic
Urine: 50%–70% as
unchanged drug
38 h Onset: 5–60 min
Peak: 1–6 h
Duration: 3–4 d
Indications
9/12/2019
29/36
Digoxin is indicated for rate control in atrial fibrillation (not first line)10 and for symptom reduction incongestive heart failure unrelieved by diuretics and angiotensin-converting enzyme inhibitors. Althoughdigoxin is only contraindicated in patients with ventricular arrhythmias, its use should be avoided in patientswith Wol�-Parkinson-White syndrome (potential for ventricular fibrillation), acute myocardial infarction,beri-beri heart disease, electrolyte imbalances, sinus node disease, atrioventricular block, and renal
impairment. Studies on the mortality associated with digoxin use report conflicting results.24,25,26,27,28
Dosing and Administration
There are many dosing strategies for digoxin initiation. For atrial fibrillation, current guidelines recommend0.25 milligram IV every 2 hours up to 1.5 milligrams total. Repeat dosing is necessary when loading digoxindue to the prolonged distribution phase. Maintenance dosing is 0.125 to 0.375 milligram daily. Doseadjustments are o�en necessary based on age, comorbidities, concomitant medications, and renaldysfunction. Digoxin levels should be monitored for safety and e�icacy.
Adverse E�ects
Adverse e�ects of digoxin are generally GI. Other more rare adverse e�ects may include gynecomastia, skinrash, eosinophilia, and thrombocytopenia. Digoxin can also cause cardiac arrhythmias, such as sinusbradycardia, atrioventricular or sinoatrial nodal block, and ventricular arrhythmias.
Symptoms of digoxin toxicity include mental status changes, visual disturbances, delirium, and seizures.Many types of arrhythmias can occur as a result of digoxin toxicity, and the clinician must be able torecognize the signs and symptoms associated with toxicity and treat accordingly.
ATROPINE
Actions
Atropine blocks the e�ects of acetylcholine at parasympathetic sites in smooth muscle thus increasing
cardiac output.6
Pharmacokinetics
See Table 19-22.
9/12/2019
30/36
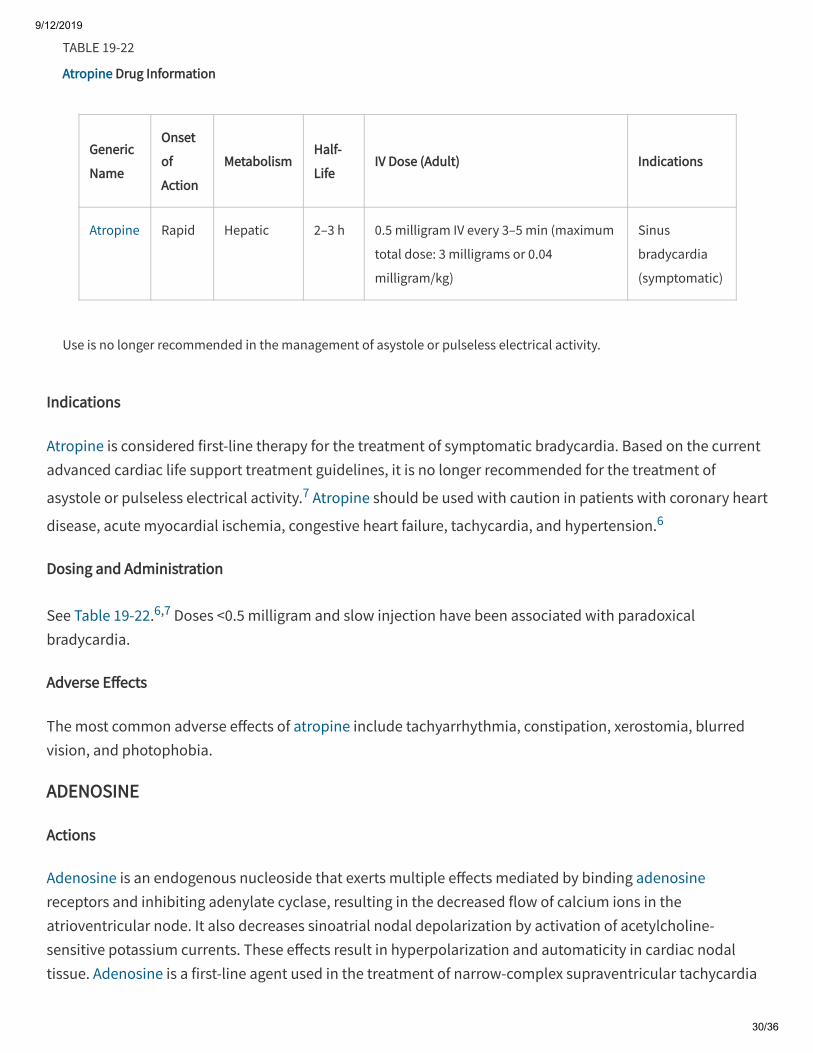
Use is no longer recommended in the management of asystole or pulseless electrical activity.
TABLE 19-22
Atropine Drug Information
Generic
Name
Onset
of
Action
MetabolismHalf-
LifeIV Dose (Adult) Indications
Atropine Rapid Hepatic 2–3 h 0.5 milligram IV every 3–5 min (maximum
total dose: 3 milligrams or 0.04
milligram/kg)
Sinus
bradycardia
(symptomatic)
Indications
Atropine is considered first-line therapy for the treatment of symptomatic bradycardia. Based on the currentadvanced cardiac life support treatment guidelines, it is no longer recommended for the treatment of
asystole or pulseless electrical activity.7 Atropine should be used with caution in patients with coronary heart
disease, acute myocardial ischemia, congestive heart failure, tachycardia, and hypertension.6
Dosing and Administration
See Table 19-22.6,7 Doses <0.5 milligram and slow injection have been associated with paradoxicalbradycardia.
Adverse E�ects
The most common adverse e�ects of atropine include tachyarrhythmia, constipation, xerostomia, blurredvision, and photophobia.
ADENOSINE
Actions
Adenosine is an endogenous nucleoside that exerts multiple e�ects mediated by binding adenosinereceptors and inhibiting adenylate cyclase, resulting in the decreased flow of calcium ions in theatrioventricular node. It also decreases sinoatrial nodal depolarization by activation of acetylcholine-sensitive potassium currents. These e�ects result in hyperpolarization and automaticity in cardiac nodaltissue. Adenosine is a first-line agent used in the treatment of narrow-complex supraventricular tachycardia
9/12/2019
31/36
in patients who have failed vagal maneuvers, and it may also be used in the setting of stable monomorphic,wide-complex tachycardias as a diagnostic tool.
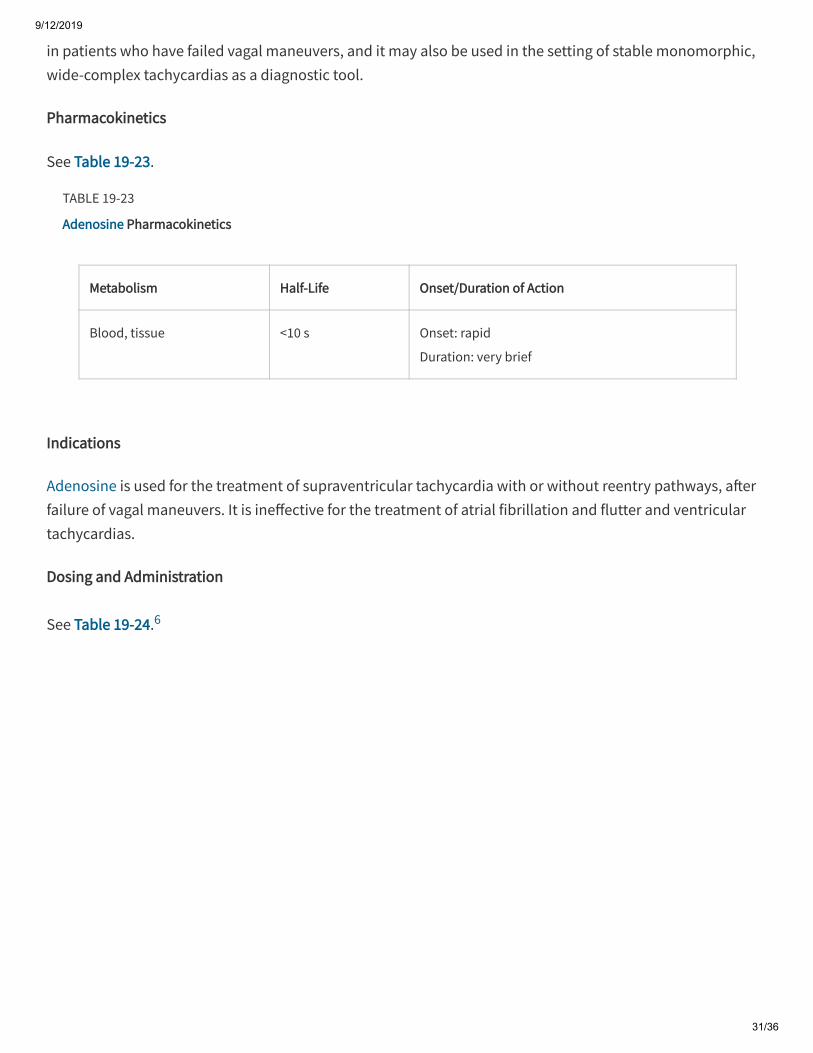
Pharmacokinetics
See Table 19-23.
TABLE 19-23
Adenosine Pharmacokinetics
Metabolism Half-Life Onset/Duration of Action
Blood, tissue <10 s Onset: rapid
Duration: very brief
Indications
Adenosine is used for the treatment of supraventricular tachycardia with or without reentry pathways, a�erfailure of vagal maneuvers. It is ine�ective for the treatment of atrial fibrillation and flutter and ventriculartachycardias.
Dosing and Administration
See Table 19-24.6
9/12/2019
32/36
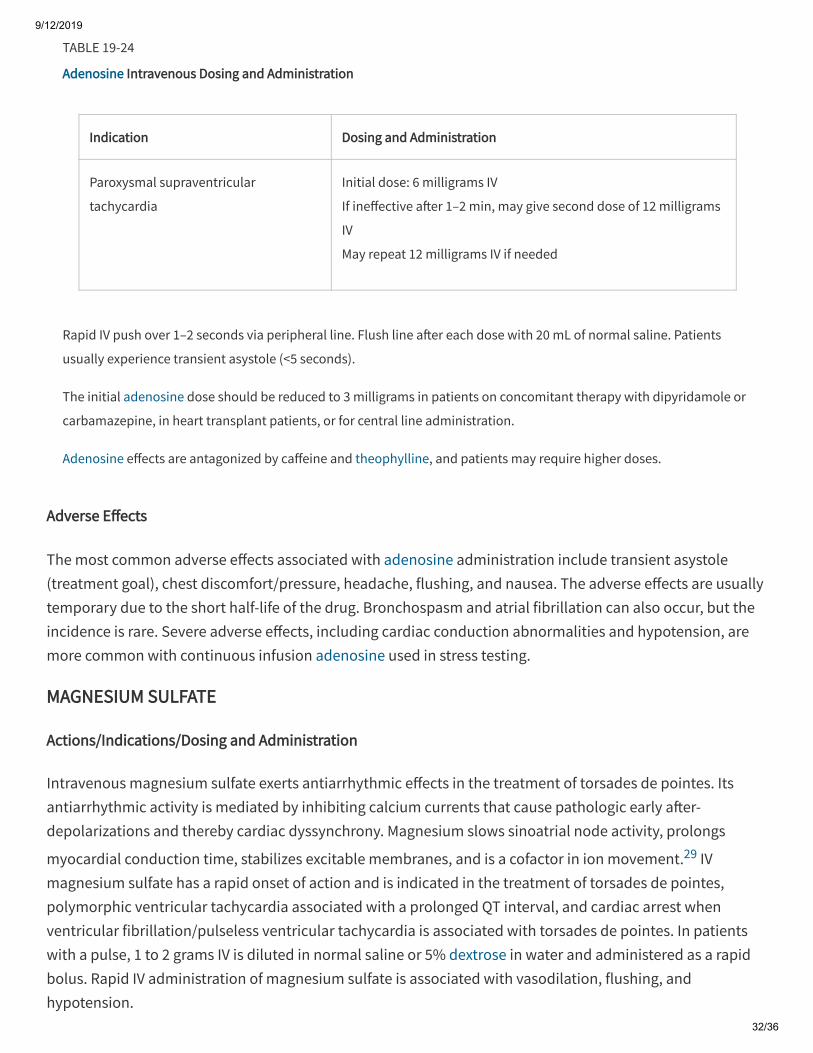
Rapid IV push over 1–2 seconds via peripheral line. Flush line a�er each dose with 20 mL of normal saline. Patients
usually experience transient asystole (<5 seconds).
The initial adenosine dose should be reduced to 3 milligrams in patients on concomitant therapy with dipyridamole or
carbamazepine, in heart transplant patients, or for central line administration.
Adenosine e�ects are antagonized by ca�eine and theophylline, and patients may require higher doses.
TABLE 19-24
Adenosine Intravenous Dosing and Administration
Indication Dosing and Administration
Paroxysmal supraventricular
tachycardia
Initial dose: 6 milligrams IV
If ine�ective a�er 1–2 min, may give second dose of 12 milligrams
IV
May repeat 12 milligrams IV if needed
Adverse E�ects
The most common adverse e�ects associated with adenosine administration include transient asystole(treatment goal), chest discomfort/pressure, headache, flushing, and nausea. The adverse e�ects are usuallytemporary due to the short half-life of the drug. Bronchospasm and atrial fibrillation can also occur, but theincidence is rare. Severe adverse e�ects, including cardiac conduction abnormalities and hypotension, aremore common with continuous infusion adenosine used in stress testing.
MAGNESIUM SULFATE
Actions/Indications/Dosing and Administration
Intravenous magnesium sulfate exerts antiarrhythmic e�ects in the treatment of torsades de pointes. Itsantiarrhythmic activity is mediated by inhibiting calcium currents that cause pathologic early a�er-depolarizations and thereby cardiac dyssynchrony. Magnesium slows sinoatrial node activity, prolongs
myocardial conduction time, stabilizes excitable membranes, and is a cofactor in ion movement.29 IVmagnesium sulfate has a rapid onset of action and is indicated in the treatment of torsades de pointes,polymorphic ventricular tachycardia associated with a prolonged QT interval, and cardiac arrest whenventricular fibrillation/pulseless ventricular tachycardia is associated with torsades de pointes. In patientswith a pulse, 1 to 2 grams IV is diluted in normal saline or 5% dextrose in water and administered as a rapidbolus. Rapid IV administration of magnesium sulfate is associated with vasodilation, flushing, andhypotension.
9/12/2019
33/36
1.
2.
3.
4.
ISOPROTERENOL
Actions/Pharmacokinetics/Indications
Isoproterenol exerts antiarrhythmic e�ects by stimulating β1- and β2-receptors. The β1-receptor interaction
results in increased chronotropic and inotropic activities in the myocardium and vasodilation by β2-
receptor–mediated relaxation of smooth muscle. Isoproterenol has an immediate onset of action, a half-lifeof 2.5 to 5 minutes, and a duration of 10 to 15 minutes. It is indicated for refractory bradyarrhythmias,atrioventricular nodal block, and refractory torsades de pointes. Isoproterenol is contraindicated in patientswith angina, preexisting ventricular arrhythmias, tachyarrhythmias, or digoxin toxicity.
Dosing and Administration
Isoproterenol should be initiated at 2 micrograms/min (maximum rate, 10 micrograms/min) and titratedevery 5 to 10 minutes based on patient response.
Adverse E�ect Profile
Serious adverse e�ects of isoproterenol include hypotension, premature ventricular beats, tachyarrhythmia,ventricular arrhythmia, dyspnea, and pulmonary edema.
REFERENCES
Sampson KJ, Kass RS: Chapter 29. Anti-arrhythmic drugs, in Brunton LL, Chabner BA, Knollmann BC(eds): Goodman & Gilman's The Pharmacological Basis of Therapeutics , 12th ed. New York: McGraw-Hill;2011.
Nattel S, Andrade J, Macle L et al.: New directions in cardiac arrhythmia mangement: present challengesand future solutions. Can J Cardiol 30: S420, 2014. [PubMed: 25432137]
The Cardiac Arrhythmia Suppression Trial (CAST) Investigators: Preliminary report: e�ect of encainide andflecainide on mortality in a randomized trial of arrhythmia suppression a�er myocardial infarction. N Engl JMed 321: 406, 1989. [PubMed: 2473403]
Waldo AL, Camm AJ, deRuyter H et al.: E�ect of d-sotalol on mortality in patients with le� ventriculardysfunction a�er recent and remote myocardial infarction. The SWORD Investigators. Survival with oralsotalol. Lancet 348: 7, 1996. [PubMed: 8691967]
9/12/2019
34/36
5.
6.
7.
8.
9.
10.
11.
12.
13.
14.
15.
16.
Connolly SJ, Camm AJ, Halperin JL et al.: Dronedarone in high-risk permanent atrial fibrillation. N Engl JMed 365: 2268, 2011. [PubMed: 22082198]
Drug Monograph, Access Emergency Medicine, McGraw-Hill.http://accessemergencymedicine.mhmedical.com/drugs.aspx. Accessed December 12, 2014.
Neumar RW, Otto CW, Link MS et al.: Part 8: Adult Advanced Cardiovascular Life Support: 2010 AmericanHeart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care.Circulation 122: S729, 2010. [PubMed: 20956224]
Preliminary report: e�ect of encainide and flecainide on mortality in a randomized trial of arrhythmiasuppression a�er myocardial infarction. N Engl J Med 121: 406, 1989. [PubMed: 2473403]
Myerburg RJ, Mitrani R, Interian A Jr: Interpretation of outcomes of antiarrhythmic clinical trials. Designfeatures and population impact. Circulation 97: 1514, 1998. [PubMed: 9576433]
January CT, Wann LS, Alpert JS et al.: 2014 AHA/ACC/HRS guideline for the management of patients withatrial fibrillation: a report of the American College of Cardiology/American Heart Association Task Force onPractice Guidelines and the Heart Rhythm Society. J Am Coll Cardiol 64: e1, 2014. [PubMed: 24682348]
Desai AD, Chun S, Sung RJ: The role of intravenous amiodarone in the management of cardiacarrhythmias. Ann Intern Med 127: 294, 1997. [PubMed: 9265430]
Product Information: Cordarone(R) IV, amiodarone. Philadelphia, PA: Wyeth Laboratories; 2002.
Nexterone Amiodarone IV (R) [package insert]. Deerfield, IL: Baxter Healthcare Corporation; 1985.
Dorian P, Cass D, Schwartz B et al.: Amiodarone as compared with lidocaine for shock-resistantventricular fibrillation. N Engl J Med 346: 884, 2002. [PubMed: 11907287]
Kudenchuk PJ, Cobb LA, Copass MK et al.: Amiodarone for resuscitation a�er out-of-hospital cardiacarrest due to ventricular fibrillation. N Engl J Med 341: 871, 1999. [PubMed: 10486418]
Heldal M, Atar D: Pharmacologic conversion of recent-onset atrial fibrillatoin: a systematic review. ScandCardiovasc J 47: 2, 2013.
9/12/2019
35/36
17.
18.
19.
20.
21.
22.
23.
24.
25.
26.
27.
28.
[PubMed: 23067130]
Trissel LA. Handbook on Injectable Drugs. Bethesda, MD: American Society of Health-SystemPharmacists; 2005.
Goldschlager N, Epstein AE, Naccarelli GV et al.: Practical guide for clinicians who treat patients withamiodarone. Heart Rhythm 4: 1250, 2007. [PubMed: 17765636]
Multaq® [package insert]. Bridgewater, NJ: Sanofi-Aventis U.S., LLC; 2009.
Sotalol® [package insert]. Weston, FL: Apotex Corp.; 2004.
Product Information: Tikosyn (Dofetilide). New York: Pfizer, Inc.; 2011.
Brinavess® [package insert]. London: Cardiome UK Limited; 2012.
Holdgate A, Foo A: Adenosine versus intravenous calcium channel antagonists for the treatment ofsupraventricular tachycardia in adults. Cochrane Database Syst Rev 4: CD005154, 2006. [PubMed: 17054240]
Reynolds MR: Outcomes with digoxin in atrial fibrillation: more data, no answers. J Am Coll Cardiol 64:669, 2014. [PubMed: 25125297]
Friberg L, Hammar N, Rosenqvist M: Digoxin in atrial fibrillation: report from the Stockholm Cohort studyof Atrial Fibrillation (SCAF). Heart 96: 275, 2010. [PubMed: 19710030]
Gheorghiade M, Fonarow GC, van Veldhuisen DJ et al.: Lack of evidence of increased mortality amongpatients with atrial fibrillation taking digoxin: findings from post hoc propensity-matched analysis of theAFFIRM trial. Eur Heart J 34: 1489, 2013. [PubMed: 23592708]
Turakhia MP, Santangeli P, Winkelmayer WC et al., Increased mortality associated with digoxin incontemporary patients with atrial fibrillation: findings from the TREAT-AF study. J Am Coll Cardiol 64: 660,2014. [PubMed: 25125296]
Shah M, Avgil Tsadok M, Jackevicius CA et al.: Relation of digoxin use in atrial fibrillation and the risk ofall-cause mortality in patients ≥65 years of age with versus without heart failure. Am J Cardiol 114: 401, 2014.
9/12/2019
36/36
29.
[PubMed: 24950677]
Herroeder S, Scho ME, De Hert SG, Hollmann MW: Magnesium—essentials for anesthesiologists.Anesthesiology 114: 971, 2011. [PubMed: 21364460]
McGraw HillCopyright © McGraw-Hill EducationAll rights reserved.Your IP address is 75.148.241.33 Terms of Use • Privacy Policy • Notice • Accessibility
Access Provided by: Brookdale University Medical CenterSilverchair